UnitedHealthcare LIJ EPO 2nd qtr 2013 Benefits Proposal clifford grekin Clifford Grekin Inc. 225 Wireless Blvd. Hauppauge, NY 11788 Phone: (631)963-6020 Fax: (631)656-2512 Email: [email protected] Prepared On: 3/3/2013 Report Id: 22187515

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript
UnitedHealthcare LIJ EPO 2nd qtr 2013
Benefits Proposal
clifford grekinClifford Grekin Inc.225 Wireless Blvd.Hauppauge, NY 11788Phone: (631)963-6020Fax: (631)656-2512Email: [email protected] On: 3/3/2013Report Id: 22187515
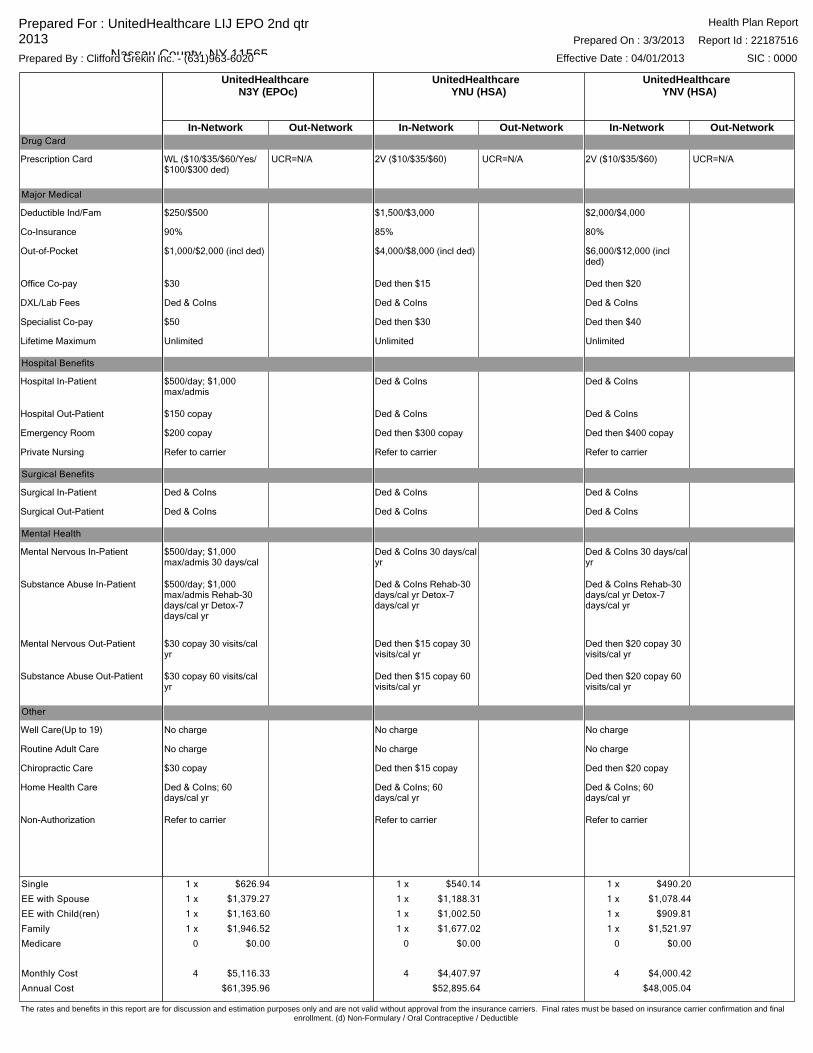
UnitedHealthcareYNV (HSA)
In-Network Out-Network
2V ($10/$35/$60) UCR=N/A
$2,000/$4,000
80%
$6,000/$12,000 (incl ded)
Ded then $20
Ded & CoIns
Ded then $40
Unlimited
Ded & CoIns
Ded & CoIns
Ded then $400 copay
Refer to carrier
Ded & CoIns
Ded & CoIns
Ded & CoIns 30 days/cal yr
Ded & CoIns Rehab-30 days/cal yr Detox-7 days/cal yr
Ded then $20 copay 30 visits/cal yr
Ded then $20 copay 60 visits/cal yr
No charge
No charge
Ded then $20 copay
Ded & CoIns; 60 days/cal yr
Refer to carrier
UnitedHealthcareYNU (HSA)
In-Network Out-Network
2V ($10/$35/$60) UCR=N/A
$1,500/$3,000
85%
$4,000/$8,000 (incl ded)
Ded then $15
Ded & CoIns
Ded then $30
Unlimited
Ded & CoIns
Ded & CoIns
Ded then $300 copay
Refer to carrier
Ded & CoIns
Ded & CoIns
Ded & CoIns 30 days/cal yr
Ded & CoIns Rehab-30 days/cal yr Detox-7 days/cal yr
Ded then $15 copay 30 visits/cal yr
Ded then $15 copay 60 visits/cal yr
No charge
No charge
Ded then $15 copay
Ded & CoIns; 60 days/cal yr
Refer to carrier
UnitedHealthcareN3Y (EPOc)
In-Network Out-Network
WL ($10/$35/$60/Yes/$100/$300 ded)
UCR=N/A
$250/$500
90%
$1,000/$2,000 (incl ded)
$30
Ded & CoIns
$50
Unlimited
$500/day; $1,000 max/admis
$150 copay
$200 copay
Refer to carrier
Ded & CoIns
Ded & CoIns
$500/day; $1,000 max/admis 30 days/cal yr
$500/day; $1,000 max/admis Rehab-30 days/cal yr Detox-7 days/cal yr
$30 copay 30 visits/cal yr
$30 copay 60 visits/cal yr
No charge
No charge
$30 copay
Ded & CoIns; 60 days/cal yr
Refer to carrier
Drug Card
Prescription Card
Major Medical
Deductible Ind/Fam
Co-Insurance
Out-of-Pocket
Office Co-pay
DXL/Lab Fees
Specialist Co-pay
Lifetime Maximum
Hospital Benefits
Hospital In-Patient
Hospital Out-Patient
Emergency Room
Private Nursing
Surgical Benefits
Surgical In-Patient
Surgical Out-Patient
Mental Health
Mental Nervous In-Patient
Substance Abuse In-Patient
Mental Nervous Out-Patient
Substance Abuse Out-Patient
Other
Well Care(Up to 19)
Routine Adult Care
Chiropractic Care
Home Health Care
Non-Authorization
1 x $490.20
1 x $1,078.44
1 x $909.81
1 x $1,521.97
0 $0.00
4 $4,000.42
$48,005.04
1 x $540.14
1 x $1,188.31
1 x $1,002.50
1 x $1,677.02
0 $0.00
4 $4,407.97
$52,895.64
Single
EE with Spouse
EE with Child(ren)
Family
Medicare
Monthly Cost
Annual Cost
1 x $626.94
1 x $1,379.27
1 x $1,163.60
1 x $1,946.52
0 $0.00
4 $5,116.33
$61,395.96
Prepared For : UnitedHealthcare LIJ EPO 2nd qtr 2013 Nassau County, NY 11565Prepared By : Clifford Grekin Inc. - (631)963-6020
Prepared On : 3/3/2013
Effective Date : 04/01/2013
Report Id : 22187516
SIC : 0000
Health Plan Report
The rates and benefits in this report are for discussion and estimation purposes only and are not valid without approval from the insurance carriers. Final rates must be based on insurance carrier confirmation and finalenrollment. (d) Non-Formulary / Oral Contraceptive / Deductible
FootNote Report
Disclosure
NY Commission Disclosure New York Regulation 194 (11 NYCRR 30)) requires disclosure of the compensation a licensed agent or broker (producer) receives from your purchase or renewal of health coverage. Compensation may be in the form of a commission, fee(s), or possibly other valuable consideration, or a combination of all three. Total commission levels per carrier are as follows: Aetna HMO - 4%, Non-HMO business -Based on a tiered per employee, per month (PEPM) model, ranging from $24-$30 PEPM. ; Emblem/HIP 3%-4% depending on selected plan, %6 for HIP EPO/PPO; 4%; HealthPass -same as commission paid by carrier; Oxford -4%. An additional override will be paid to a general agent if they are involved in the sale; this amount may vary based on carrier and plan design. The commissions do not directly affect the premium paid for the plan and no plan can be purchased through another distributor or from the carrier directly with a different commission amount or at a lower cost. Final commission dollar amounts cannot be determined until enrollment is complete and is subject to change based on the number of members covered each month.
UnitedHealthcare
Medical Rates UnitedHealthcare Medical plan rates generated on this quoting tool may not reflect final rates for groups subject to the Federal Mental Health Parity (MHP) Statute effective 7/1/10. Groups in the 2-50 business segment that are subject to Federal Mental Health Parity, and are located in MD, VA, DE and WV, will be subject to an approximate 2% increase. Group sitused outside the MidAtlantic region may be subject to a similar rate increase contingent upon rate approval in each state. These are groups that employ 51 or more total persons, including seasonal and/or part-time employees, and have 50 or less eligible persons. Please contact your General Agent or local sales office for questions regarding these guidelines and any applicable impact to rates.
Medical Proposal rates are valid through the 15th of the month, which includes the requested effective date.
All plans are available subject to NY DOI approval.
If the employer offer consists of more than one medical plan, we require the policy year, or calendar year basis selection be the same for each sold policy if the employees have the option to choose from among the plans offered.
The N3Y, YNU, and YNV plans feature split physician office visit copayments. Enrollees in these plans will pay a higher copayment when they see specialists than when they see primary care physicians.
Disclaimers Due to Federal Mental Health Parity, groups in the 2-50 business segment with UHC may be subject to a 2% increase in their final rate. UHC guidelines reflects that this applies to groups that employ 51 or more total persons, including seasonal and/or part-time employees and have 50 or less eligible persons.
The above rates and benefits are for general information and discussion purposes only and not valid unless approved by UnitedHealthcare. This rate quote is not an offer or a guarantee of coverage. The rates quoted are applicable to the plan design selected. We reserve the right to modify your rates in the event your plan design must be modified as a result of any change, modification or clarification in law, including the Patient and Affordable Care Act. This group should not, under any circumstances, cancel its existing coverage unless and until coverage is offered by us and final rates have been accepted by and initial premium paid by the group. Final rates are determined by UnitedHealthcare's underwriting guidelines and final enrollment. The insurance policy, not general rates and descriptions in this Web site or printed output, will form the contract between the insured and UnitedHealthcare, and the Certificate of Coverage issued to the subscriber will provide the legal description of coverage.
Benefit Reporting The Advantage Series plan designs includes two levels of network benefits, this quote report identifies the tier one network benefits only. A benefit summary report will need to be generated in order to see both tier one and tier two network benefits for an Advantage plan design.
Prepared For : UnitedHealthcare LIJ EPO 2nd qtr 2013 Nassau County, NY 11565Prepared By : Clifford Grekin Inc. - (631)963-6020
Prepared On : 3/3/2013
Effective Date : 04/01/2013
Report Id : 22187517
SIC : 0000
Footnote Report
All Information Contained Within This Report Is For Illustration Purposes Only. Final Binding Information Must Be Provided By The Respective Insurance Carrier.
Page 1 of 12
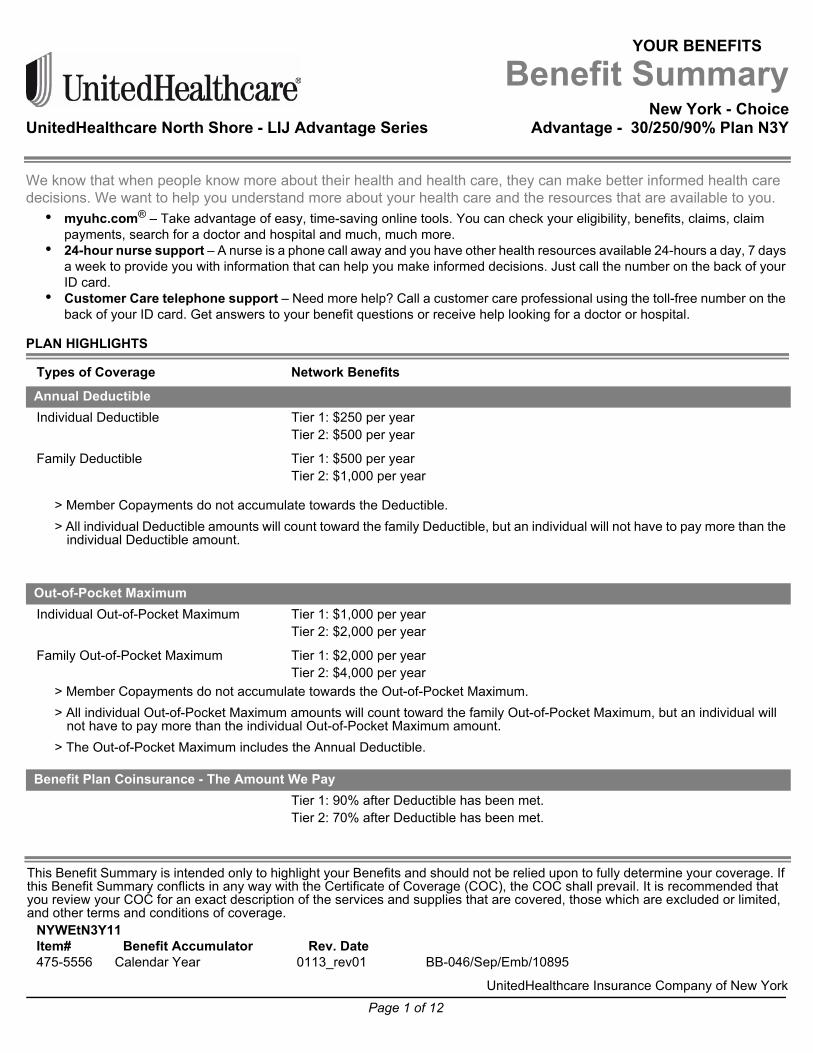
YOUR BENEFITS
Benefit SummaryNew York - Choice
UnitedHealthcare North Shore - LIJ Advantage Series Advantage - 30/250/90% Plan N3Y
We know that when people know more about their health and health care, they can make better informed health care decisions. We want to help you understand more about your health care and the resources that are available to you.• myuhc.com® – Take advantage of easy, time-saving online tools. You can check your eligibility, benefits, claims, claim
payments, search for a doctor and hospital and much, much more. • 24-hour nurse support – A nurse is a phone call away and you have other health resources available 24-hours a day, 7 days
a week to provide you with information that can help you make informed decisions. Just call the number on the back of your ID card.
• Customer Care telephone support – Need more help? Call a customer care professional using the toll-free number on the back of your ID card. Get answers to your benefit questions or receive help looking for a doctor or hospital.
PLAN HIGHLIGHTS
> Member Copayments do not accumulate towards the Deductible.> All individual Deductible amounts will count toward the family Deductible, but an individual will not have to pay more than the
individual Deductible amount.
> Member Copayments do not accumulate towards the Out-of-Pocket Maximum.> All individual Out-of-Pocket Maximum amounts will count toward the family Out-of-Pocket Maximum, but an individual will
not have to pay more than the individual Out-of-Pocket Maximum amount.> The Out-of-Pocket Maximum includes the Annual Deductible.
Types of Coverage Network Benefits
Annual DeductibleIndividual Deductible Tier 1: $250 per year
Tier 2: $500 per year
Family Deductible Tier 1: $500 per yearTier 2: $1,000 per year
Out-of-Pocket MaximumIndividual Out-of-Pocket Maximum Tier 1: $1,000 per year
Tier 2: $2,000 per year
Family Out-of-Pocket Maximum Tier 1: $2,000 per yearTier 2: $4,000 per year
Benefit Plan Coinsurance - The Amount We PayTier 1: 90% after Deductible has been met.Tier 2: 70% after Deductible has been met.
This Benefit Summary is intended only to highlight your Benefits and should not be relied upon to fully determine your coverage. If this Benefit Summary conflicts in any way with the Certificate of Coverage (COC), the COC shall prevail. It is recommended that you review your COC for an exact description of the services and supplies that are covered, those which are excluded or limited, and other terms and conditions of coverage.
NYWEtN3Y11Item# Benefit Accumulator Rev. Date475-5556 Calendar Year 0113_rev01 BB-046/Sep/Emb/10895
UnitedHealthcare Insurance Company of New York

Page 2 of 12
Prescription drug benefits are shown under separate cover.
> The Annual Deductible, Out-of-Pocket Maximum and Benefit limits are calculated on a calendar year basis.> All Benefits are reimbursed based on Eligible Expenses. For a definition of Eligible Expenses, please refer to your Certificate
of Coverage.
MOST COMMONLY USED BENEFITS
> In addition to the visit Copayment, the applicable Copayment and any Deductible/Coinsurance applies when these services are done: Lab, X-Ray, CT, PET, MRI, MRA, Nuclear Medicine; Pharmaceutical Products, Scopic Procedures; Surgery; Therapeutic Treatments.
The health care reform law provides for coverage of certain preventive services, based on your age, gender and other health factors, with no cost-sharing. The preventive care services covered under this section are those preventive services specified in the health care reform law. UnitedHealthcare also covers other routine services as described in other areas of this summary, which may require a copayment, coinsurance or deductible. Always refer to your plan documents for your specific coverage.
> In addition to the visit Copayment, the applicable Copayment and any Deductible/Coinsurance applies when these services are done: Lab, X-Ray, CT, PET, MRI, MRA, Nuclear Medicine; Pharmaceutical Products, Scopic Procedures; Surgery; Therapeutic Treatments.
Prescription Drug Benefits
Information on Benefit Limits
Types of Coverage Network Benefits
Physician’s Office Services - Sickness and InjuryPrimary Physician Office Visit Tier 1: 100% after you pay a $30 Copayment per visit.
Tier 2: 100% after you pay a $60 Copayment per visit.
Specialist Physician Office Visit Tier 1: 100% after you pay a $50 Copayment per visit.Tier 2: 100% after you pay a $100 Copayment per visit.
Preventive Care ServicesCovered Health Services include but are not limited to:
Primary Physician Office Visit Tier 1: 100%, Copayments and Deductibles do not apply.Tier 2: 100%, Copayments and Deductibles do not apply.
Specialist Physician Office Visit Tier 1: 100%, Copayments and Deductibles do not apply.Tier 2: 100%, Copayments and Deductibles do not apply.
Lab, X-Ray or other preventive tests
Tier 1: 100%, Copayments and Deductibles do not apply.Tier 2: 100%, Copayments and Deductibles do not apply.
Urgent Care Center ServicesTier 1: 100% after you pay a $50 Copayment per visit.Tier 2: 100% after you pay a $100 Copayment per visit.
Emergency Health Services - OutpatientTier 1: 100% after you pay a $200 Copayment per visit.Tier 2: 100% after you pay a $200 Copayment per visit.
Notification is required if confined in a non-Network Hospital.
Hospital - Inpatient Stay Tier 1: 100% after you pay a $500 Copayment per day to a maximum $1,000
Copayment per Inpatient Stay.Tier 2: 100% after you pay a $1,000 Copayment per day to a maximum $5,000 Copayment per Inpatient Stay.
Page 3 of 12
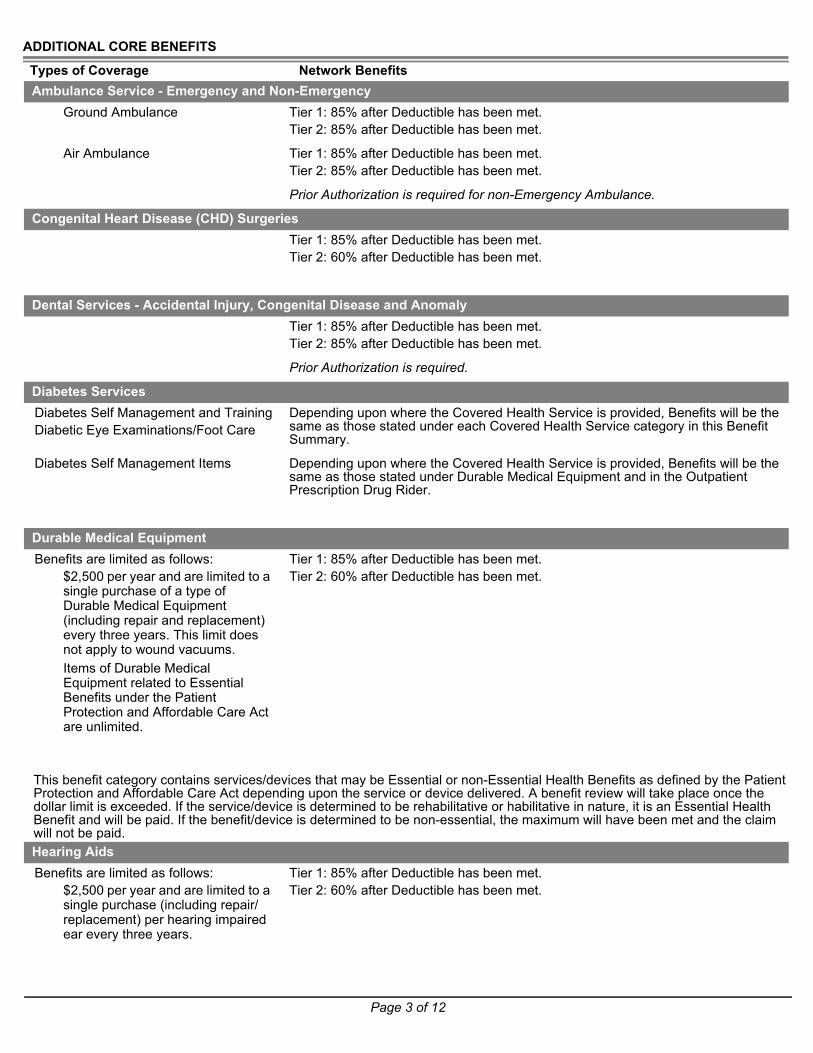
ADDITIONAL CORE BENEFITS
Types of Coverage Network Benefits
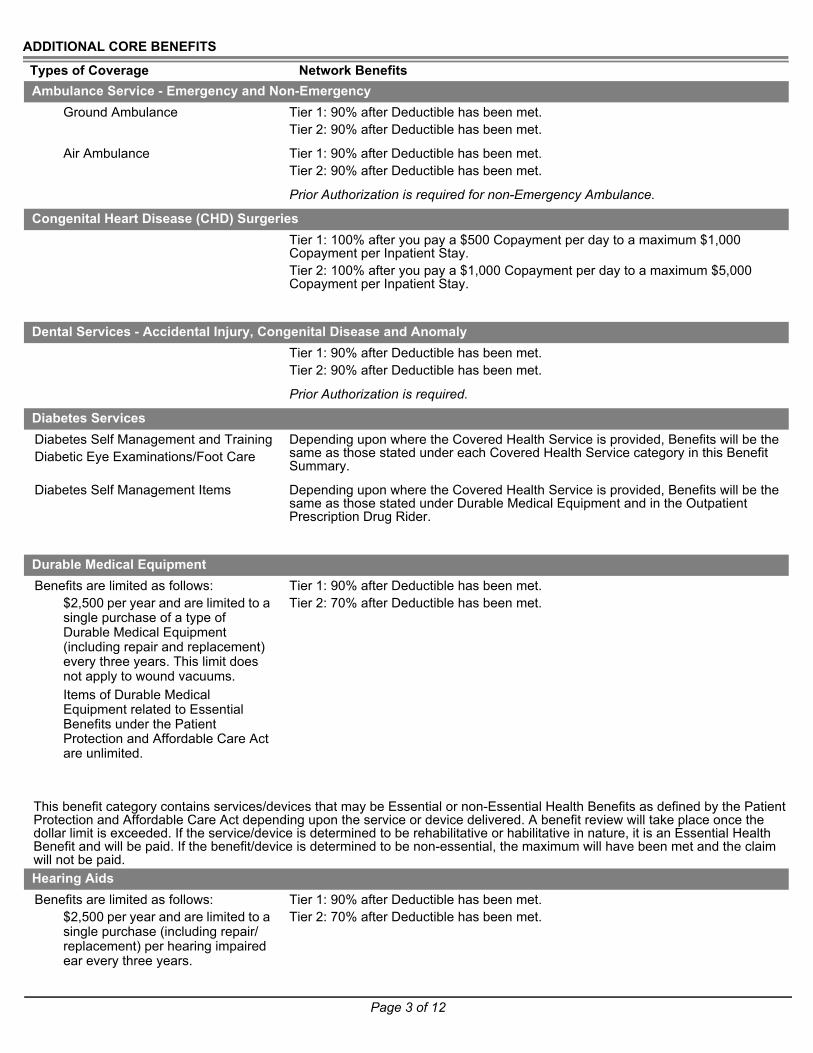
This benefit category contains services/devices that may be Essential or non-Essential Health Benefits as defined by the Patient Protection and Affordable Care Act depending upon the service or device delivered. A benefit review will take place once the dollar limit is exceeded. If the service/device is determined to be rehabilitative or habilitative in nature, it is an Essential Health Benefit and will be paid. If the benefit/device is determined to be non-essential, the maximum will have been met and the claim will not be paid.
Ambulance Service - Emergency and Non-EmergencyGround Ambulance Tier 1: 90% after Deductible has been met.
Tier 2: 90% after Deductible has been met.
Air Ambulance Tier 1: 90% after Deductible has been met.Tier 2: 90% after Deductible has been met.
Prior Authorization is required for non-Emergency Ambulance.
Congenital Heart Disease (CHD) SurgeriesTier 1: 100% after you pay a $500 Copayment per day to a maximum $1,000 Copayment per Inpatient Stay.Tier 2: 100% after you pay a $1,000 Copayment per day to a maximum $5,000 Copayment per Inpatient Stay.
Dental Services - Accidental Injury, Congenital Disease and AnomalyTier 1: 90% after Deductible has been met.Tier 2: 90% after Deductible has been met.
Prior Authorization is required.
Diabetes ServicesDiabetes Self Management and TrainingDiabetic Eye Examinations/Foot Care
Depending upon where the Covered Health Service is provided, Benefits will be the same as those stated under each Covered Health Service category in this Benefit Summary.
Diabetes Self Management Items Depending upon where the Covered Health Service is provided, Benefits will be the same as those stated under Durable Medical Equipment and in the Outpatient Prescription Drug Rider.
Durable Medical EquipmentBenefits are limited as follows:
$2,500 per year and are limited to a single purchase of a type of Durable Medical Equipment (including repair and replacement) every three years. This limit does not apply to wound vacuums.Items of Durable Medical Equipment related to Essential Benefits under the Patient Protection and Affordable Care Act are unlimited.
Tier 1: 90% after Deductible has been met.Tier 2: 70% after Deductible has been met.
Hearing AidsBenefits are limited as follows:
$2,500 per year and are limited to a single purchase (including repair/replacement) per hearing impaired ear every three years.
Tier 1: 90% after Deductible has been met.Tier 2: 70% after Deductible has been met.
Page 4 of 12
ADDITIONAL CORE BENEFITS
Types of Coverage Network Benefits
YOUR BENEFITS
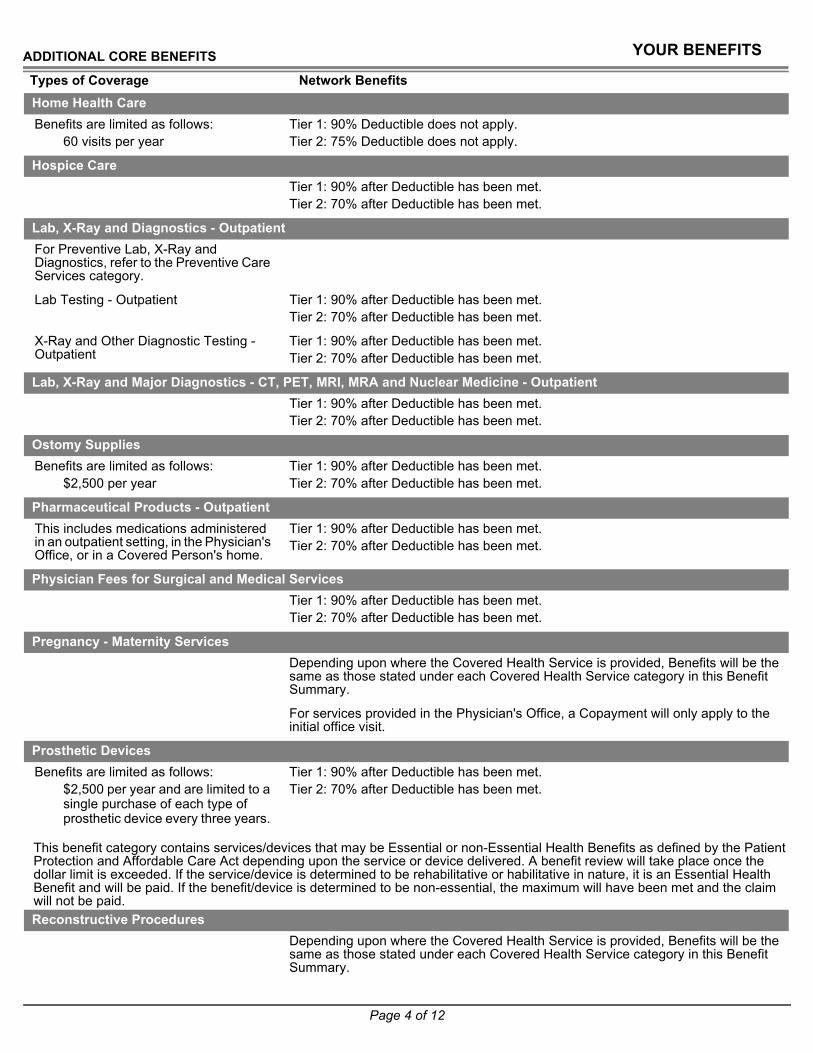
This benefit category contains services/devices that may be Essential or non-Essential Health Benefits as defined by the Patient Protection and Affordable Care Act depending upon the service or device delivered. A benefit review will take place once the dollar limit is exceeded. If the service/device is determined to be rehabilitative or habilitative in nature, it is an Essential Health Benefit and will be paid. If the benefit/device is determined to be non-essential, the maximum will have been met and the claim will not be paid.
Home Health CareBenefits are limited as follows:
60 visits per year Tier 1: 90% Deductible does not apply.Tier 2: 75% Deductible does not apply.
Hospice CareTier 1: 90% after Deductible has been met.Tier 2: 70% after Deductible has been met.
Lab, X-Ray and Diagnostics - OutpatientFor Preventive Lab, X-Ray and Diagnostics, refer to the Preventive Care Services category.
Lab Testing - Outpatient Tier 1: 90% after Deductible has been met.Tier 2: 70% after Deductible has been met.
X-Ray and Other Diagnostic Testing - Outpatient
Tier 1: 90% after Deductible has been met.Tier 2: 70% after Deductible has been met.
Lab, X-Ray and Major Diagnostics - CT, PET, MRI, MRA and Nuclear Medicine - Outpatient
Tier 1: 90% after Deductible has been met.Tier 2: 70% after Deductible has been met.
Ostomy SuppliesBenefits are limited as follows:
$2,500 per yearTier 1: 90% after Deductible has been met.Tier 2: 70% after Deductible has been met.
Pharmaceutical Products - OutpatientThis includes medications administered in an outpatient setting, in the Physician's Office, or in a Covered Person's home.
Tier 1: 90% after Deductible has been met.Tier 2: 70% after Deductible has been met.
Physician Fees for Surgical and Medical ServicesTier 1: 90% after Deductible has been met.Tier 2: 70% after Deductible has been met.
Pregnancy - Maternity Services Depending upon where the Covered Health Service is provided, Benefits will be the same as those stated under each Covered Health Service category in this Benefit Summary.
For services provided in the Physician's Office, a Copayment will only apply to the initial office visit.
Prosthetic DevicesBenefits are limited as follows:
$2,500 per year and are limited to a single purchase of each type of prosthetic device every three years.
Tier 1: 90% after Deductible has been met.Tier 2: 70% after Deductible has been met.
Reconstructive ProceduresDepending upon where the Covered Health Service is provided, Benefits will be the same as those stated under each Covered Health Service category in this Benefit Summary.
Page 5 of 12
ADDITIONAL CORE BENEFITS
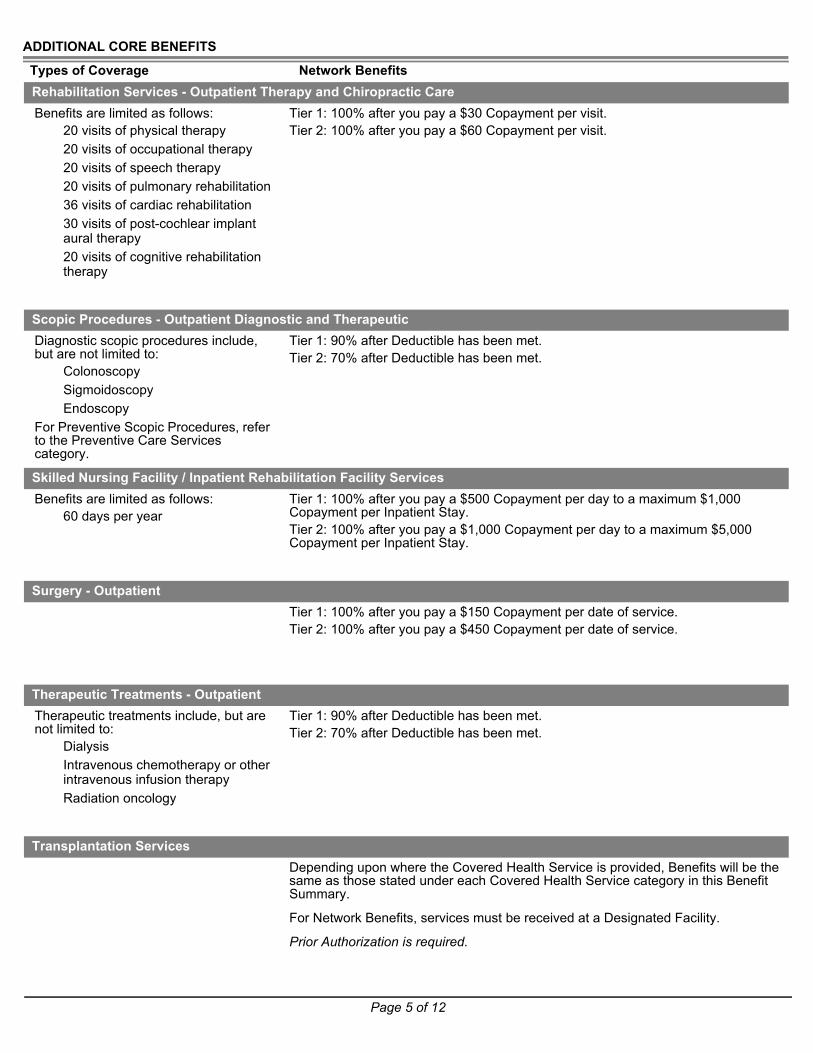
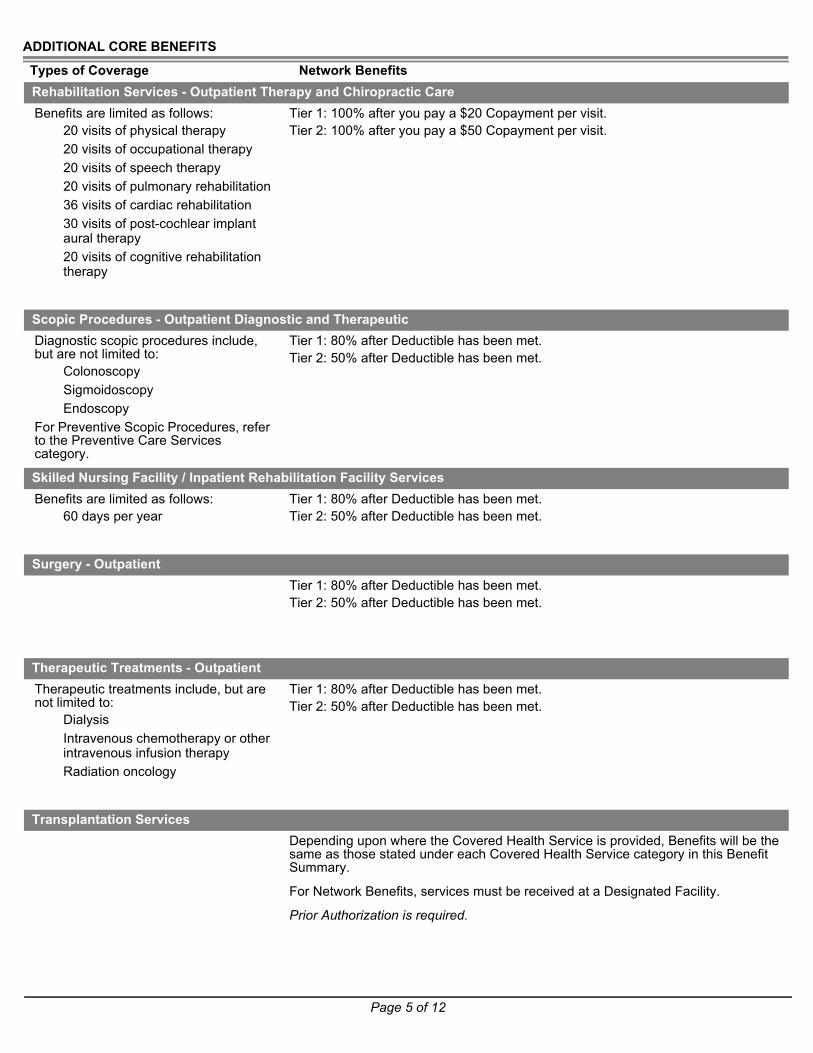
Types of Coverage Network BenefitsRehabilitation Services - Outpatient Therapy and Chiropractic CareBenefits are limited as follows:
20 visits of physical therapy20 visits of occupational therapy20 visits of speech therapy20 visits of pulmonary rehabilitation36 visits of cardiac rehabilitation30 visits of post-cochlear implant aural therapy20 visits of cognitive rehabilitation therapy
Tier 1: 100% after you pay a $30 Copayment per visit.Tier 2: 100% after you pay a $60 Copayment per visit.
Scopic Procedures - Outpatient Diagnostic and TherapeuticDiagnostic scopic procedures include, but are not limited to:
ColonoscopySigmoidoscopyEndoscopy
For Preventive Scopic Procedures, refer to the Preventive Care Services category.
Tier 1: 90% after Deductible has been met.Tier 2: 70% after Deductible has been met.
Skilled Nursing Facility / Inpatient Rehabilitation Facility ServicesBenefits are limited as follows:
60 days per year Tier 1: 100% after you pay a $500 Copayment per day to a maximum $1,000 Copayment per Inpatient Stay.Tier 2: 100% after you pay a $1,000 Copayment per day to a maximum $5,000 Copayment per Inpatient Stay.
Surgery - OutpatientTier 1: 100% after you pay a $150 Copayment per date of service.Tier 2: 100% after you pay a $450 Copayment per date of service.
Therapeutic Treatments - OutpatientTherapeutic treatments include, but are not limited to:
DialysisIntravenous chemotherapy or other intravenous infusion therapyRadiation oncology
Tier 1: 90% after Deductible has been met.Tier 2: 70% after Deductible has been met.
Transplantation ServicesDepending upon where the Covered Health Service is provided, Benefits will be the same as those stated under each Covered Health Service category in this Benefit Summary.
For Network Benefits, services must be received at a Designated Facility.
Prior Authorization is required.

Page 6 of 12
ADDITIONAL CORE BENEFITS
Types of Coverage Network Benefits
YOUR BENEFITS
Vision ExaminationsBenefits are limited as follows:
1 exam every 2 yearsTier 1: 100% after you pay a $30 Copayment per visit.Tier 2: 100% after you pay a $30 Copayment per visit.
Page 7 of 12
STATE MANDATED BENEFITS
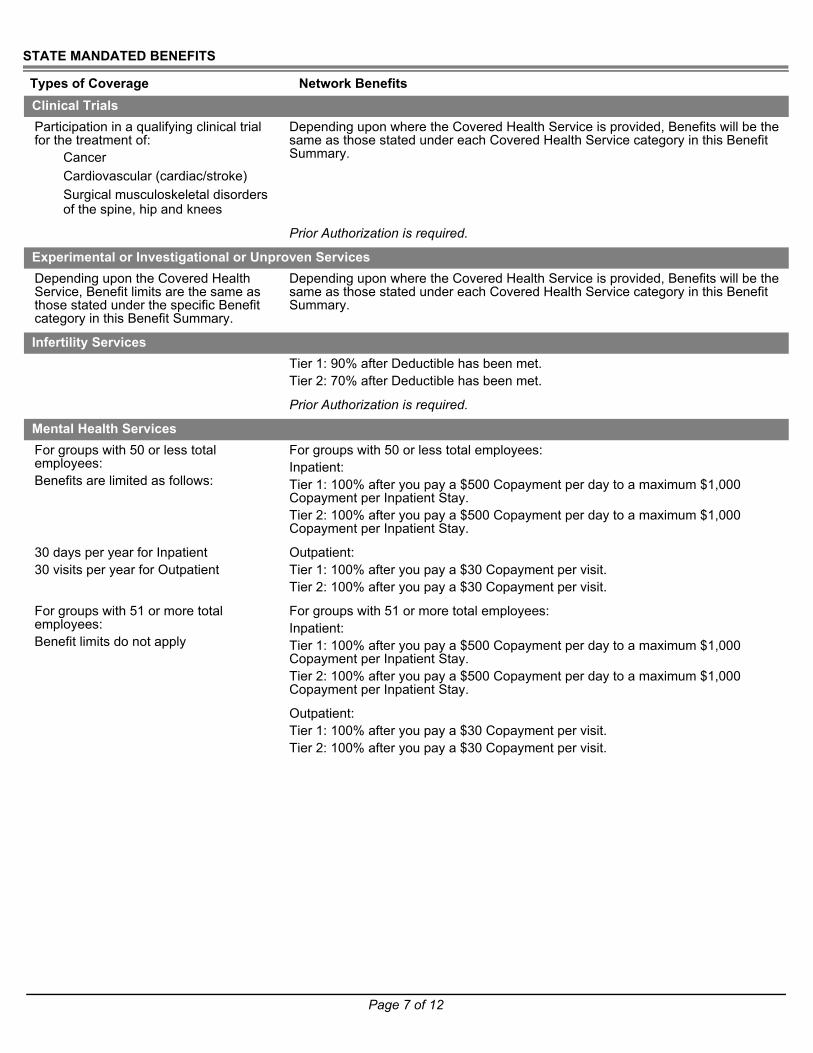
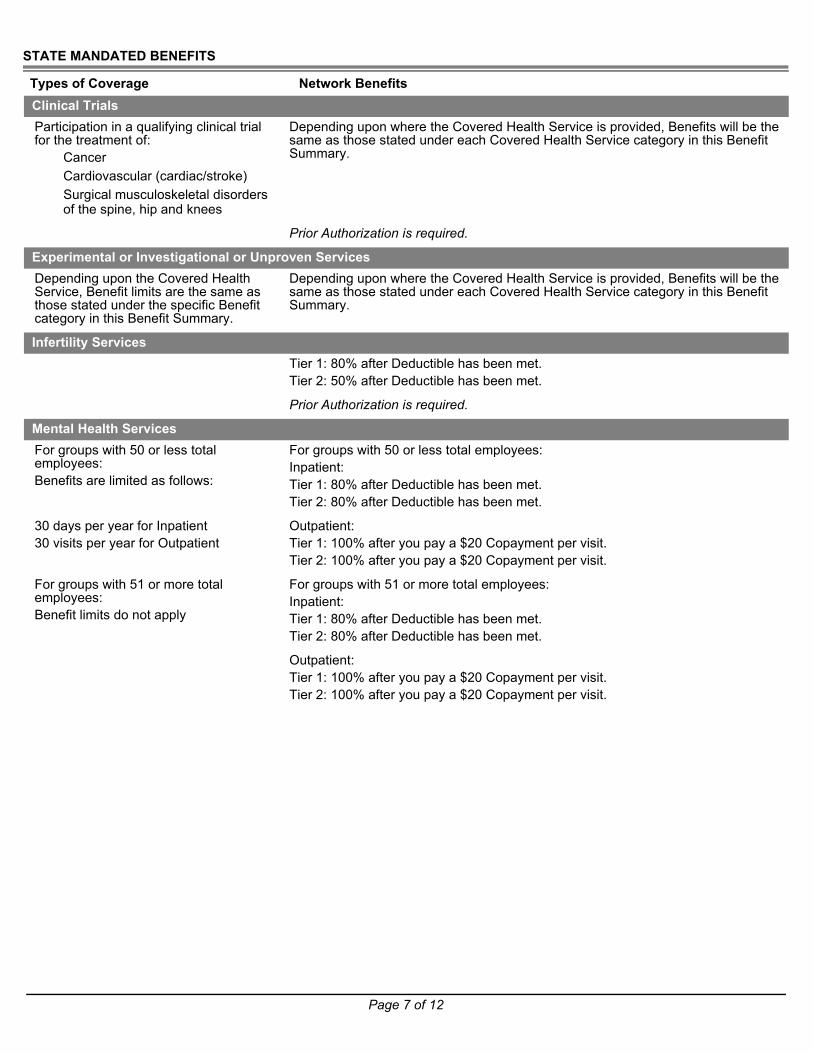
Types of Coverage Network BenefitsClinical TrialsParticipation in a qualifying clinical trial for the treatment of:
CancerCardiovascular (cardiac/stroke)Surgical musculoskeletal disorders of the spine, hip and knees
Depending upon where the Covered Health Service is provided, Benefits will be the same as those stated under each Covered Health Service category in this Benefit Summary.
Prior Authorization is required.
Experimental or Investigational or Unproven ServicesDepending upon the Covered Health Service, Benefit limits are the same as those stated under the specific Benefit category in this Benefit Summary.
Depending upon where the Covered Health Service is provided, Benefits will be the same as those stated under each Covered Health Service category in this Benefit Summary.
Infertility ServicesTier 1: 90% after Deductible has been met.Tier 2: 70% after Deductible has been met.
Prior Authorization is required.
Mental Health ServicesFor groups with 50 or less total employees:Benefits are limited as follows:
For groups with 50 or less total employees:Inpatient:Tier 1: 100% after you pay a $500 Copayment per day to a maximum $1,000 Copayment per Inpatient Stay.Tier 2: 100% after you pay a $500 Copayment per day to a maximum $1,000 Copayment per Inpatient Stay.
30 days per year for Inpatient30 visits per year for Outpatient
Outpatient:Tier 1: 100% after you pay a $30 Copayment per visit.Tier 2: 100% after you pay a $30 Copayment per visit.
For groups with 51 or more total employees:Benefit limits do not apply
For groups with 51 or more total employees:Inpatient:Tier 1: 100% after you pay a $500 Copayment per day to a maximum $1,000 Copayment per Inpatient Stay.Tier 2: 100% after you pay a $500 Copayment per day to a maximum $1,000 Copayment per Inpatient Stay.
Outpatient:Tier 1: 100% after you pay a $30 Copayment per visit.Tier 2: 100% after you pay a $30 Copayment per visit.
Page 8 of 12
STATE MANDATED BENEFITS
Types of Coverage Network Benefits
YOUR BENEFITS
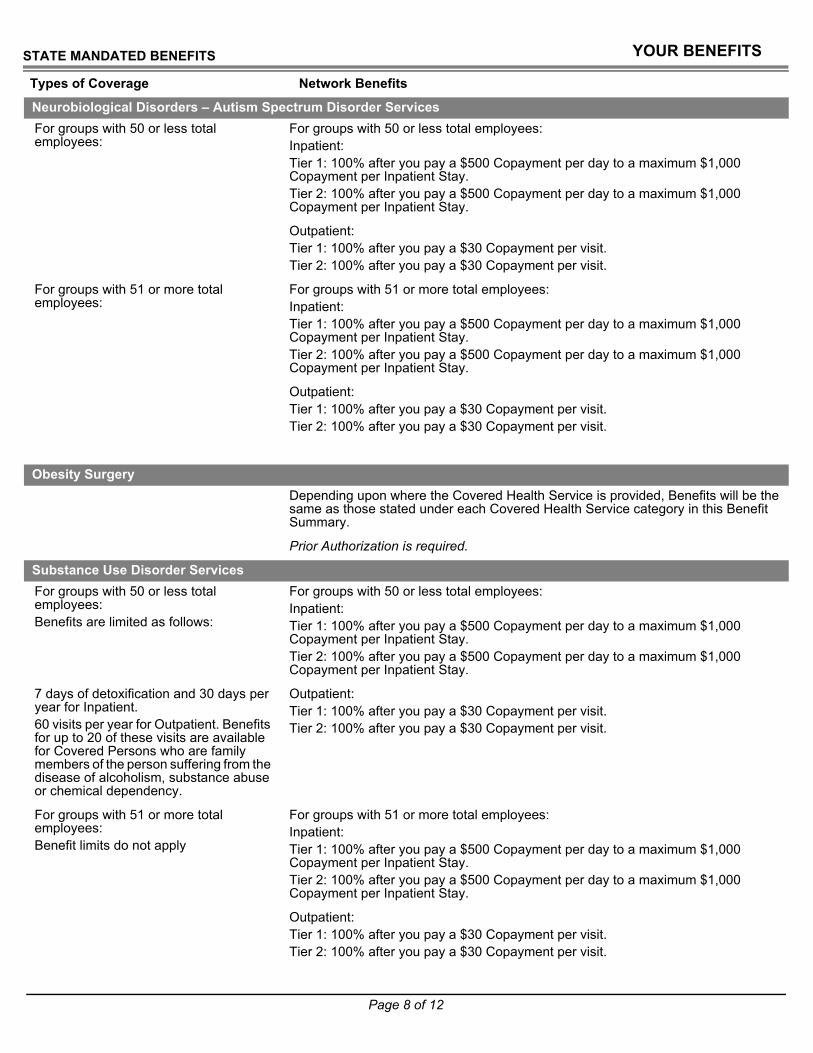
Neurobiological Disorders – Autism Spectrum Disorder ServicesFor groups with 50 or less total employees:
For groups with 50 or less total employees:Inpatient:Tier 1: 100% after you pay a $500 Copayment per day to a maximum $1,000 Copayment per Inpatient Stay.Tier 2: 100% after you pay a $500 Copayment per day to a maximum $1,000 Copayment per Inpatient Stay.
Outpatient:Tier 1: 100% after you pay a $30 Copayment per visit.Tier 2: 100% after you pay a $30 Copayment per visit.
For groups with 51 or more total employees:
For groups with 51 or more total employees:Inpatient:Tier 1: 100% after you pay a $500 Copayment per day to a maximum $1,000 Copayment per Inpatient Stay.Tier 2: 100% after you pay a $500 Copayment per day to a maximum $1,000 Copayment per Inpatient Stay.
Outpatient:Tier 1: 100% after you pay a $30 Copayment per visit.Tier 2: 100% after you pay a $30 Copayment per visit.
Obesity SurgeryDepending upon where the Covered Health Service is provided, Benefits will be the same as those stated under each Covered Health Service category in this Benefit Summary.
Prior Authorization is required.
Substance Use Disorder ServicesFor groups with 50 or less total employees:Benefits are limited as follows:
For groups with 50 or less total employees:Inpatient:Tier 1: 100% after you pay a $500 Copayment per day to a maximum $1,000 Copayment per Inpatient Stay.Tier 2: 100% after you pay a $500 Copayment per day to a maximum $1,000 Copayment per Inpatient Stay.
7 days of detoxification and 30 days per year for Inpatient.60 visits per year for Outpatient. Benefits for up to 20 of these visits are available for Covered Persons who are family members of the person suffering from the disease of alcoholism, substance abuse or chemical dependency.
Outpatient:Tier 1: 100% after you pay a $30 Copayment per visit.Tier 2: 100% after you pay a $30 Copayment per visit.
For groups with 51 or more total employees:Benefit limits do not apply
For groups with 51 or more total employees:Inpatient:Tier 1: 100% after you pay a $500 Copayment per day to a maximum $1,000 Copayment per Inpatient Stay.Tier 2: 100% after you pay a $500 Copayment per day to a maximum $1,000 Copayment per Inpatient Stay.
Outpatient:Tier 1: 100% after you pay a $30 Copayment per visit.Tier 2: 100% after you pay a $30 Copayment per visit.

Page 9 of 12
STATE MANDATED BENEFITS
Types of Coverage Network BenefitsTemporomandibular Joint Services
Depending upon where the Covered Health Service is provided, Benefits will be the same as those stated under each Covered Health Service category in this Benefit Summary.
This Benefit Summary is intended only to highlight your Benefits and should not be relied upon to fully determine your coverage. If this Benefit Summary conflicts in any way with the Certificate of Coverage (COC), the COC shall prevail. It is recommended that you review your COC for an exact description of the services and supplies that are covered, those which are excluded or limited, and other terms and conditions of coverage.

Page 10 of 12
MEDICAL EXCLUSIONS
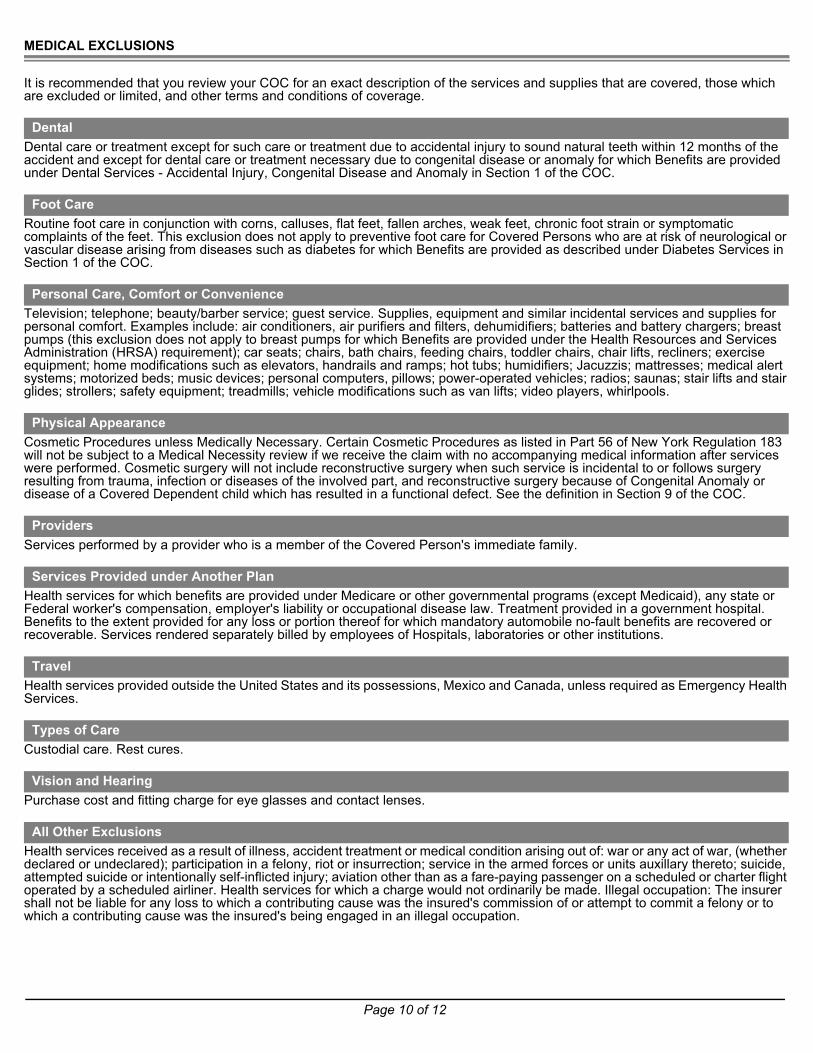
It is recommended that you review your COC for an exact description of the services and supplies that are covered, those which are excluded or limited, and other terms and conditions of coverage.
Dental care or treatment except for such care or treatment due to accidental injury to sound natural teeth within 12 months of the accident and except for dental care or treatment necessary due to congenital disease or anomaly for which Benefits are provided under Dental Services - Accidental Injury, Congenital Disease and Anomaly in Section 1 of the COC.
Routine foot care in conjunction with corns, calluses, flat feet, fallen arches, weak feet, chronic foot strain or symptomatic complaints of the feet. This exclusion does not apply to preventive foot care for Covered Persons who are at risk of neurological or vascular disease arising from diseases such as diabetes for which Benefits are provided as described under Diabetes Services in Section 1 of the COC.
Television; telephone; beauty/barber service; guest service. Supplies, equipment and similar incidental services and supplies for personal comfort. Examples include: air conditioners, air purifiers and filters, dehumidifiers; batteries and battery chargers; breast pumps (this exclusion does not apply to breast pumps for which Benefits are provided under the Health Resources and Services Administration (HRSA) requirement); car seats; chairs, bath chairs, feeding chairs, toddler chairs, chair lifts, recliners; exercise equipment; home modifications such as elevators, handrails and ramps; hot tubs; humidifiers; Jacuzzis; mattresses; medical alert systems; motorized beds; music devices; personal computers, pillows; power-operated vehicles; radios; saunas; stair lifts and stair glides; strollers; safety equipment; treadmills; vehicle modifications such as van lifts; video players, whirlpools.
Cosmetic Procedures unless Medically Necessary. Certain Cosmetic Procedures as listed in Part 56 of New York Regulation 183 will not be subject to a Medical Necessity review if we receive the claim with no accompanying medical information after services were performed. Cosmetic surgery will not include reconstructive surgery when such service is incidental to or follows surgery resulting from trauma, infection or diseases of the involved part, and reconstructive surgery because of Congenital Anomaly or disease of a Covered Dependent child which has resulted in a functional defect. See the definition in Section 9 of the COC.
Services performed by a provider who is a member of the Covered Person's immediate family.
Health services for which benefits are provided under Medicare or other governmental programs (except Medicaid), any state or Federal worker's compensation, employer's liability or occupational disease law. Treatment provided in a government hospital. Benefits to the extent provided for any loss or portion thereof for which mandatory automobile no-fault benefits are recovered or recoverable. Services rendered separately billed by employees of Hospitals, laboratories or other institutions.
Health services provided outside the United States and its possessions, Mexico and Canada, unless required as Emergency Health Services.
Custodial care. Rest cures.
Purchase cost and fitting charge for eye glasses and contact lenses.
Health services received as a result of illness, accident treatment or medical condition arising out of: war or any act of war, (whether declared or undeclared); participation in a felony, riot or insurrection; service in the armed forces or units auxillary thereto; suicide, attempted suicide or intentionally self-inflicted injury; aviation other than as a fare-paying passenger on a scheduled or charter flight operated by a scheduled airliner. Health services for which a charge would not ordinarily be made. Illegal occupation: The insurer shall not be liable for any loss to which a contributing cause was the insured's commission of or attempt to commit a felony or to which a contributing cause was the insured's being engaged in an illegal occupation.
Dental
Foot Care
Personal Care, Comfort or Convenience
Physical Appearance
Providers
Services Provided under Another Plan
Travel
Types of Care
Vision and Hearing
All Other Exclusions
Page 11 of 12
MEDICAL EXCLUSIONS CONTINUED
Benefits for the treatment of a Preexisting Condition are excluded until the earlier of the following: The date you have had Continuous Creditable Coverage for 12 months; or the date you have had Continuous Creditable Coverage for 18 months if you are a Late Enrollee. This exclusion does not apply to Covered Persons under age 19. This exclusion does not apply to pregnancy or an individual, and any dependent of such individual, who is eligible for a federal tax credit under the federal Trade Adjustment Assistance Reform Act of 2002 and who has three months or more of Continuous Creditable Coverage. Note: See the definition of Continuous Creditable Coverage and Preexisting Condition in Section 9 of the COC.
Preexisting Conditions (Applies only to groups of 50 or less employees)
UnitedHealthcare Insurance Company of New York

Page 12 of 12
THIS PAGE INTENTIONALLY LEFT BLANK

Page 1 of 12
YOUR BENEFITS
Benefit SummaryNew York - Choice
UnitedHealthcare North Shore - LIJ Advantage Series Advantage HSA - 20/2000/80% Plan YNV
We know that when people know more about their health and health care, they can make better informed health care decisions. We want to help you understand more about your health care and the resources that are available to you.• myuhc.com® – Take advantage of easy, time-saving online tools. You can check your eligibility, benefits, claims, claim
payments, search for a doctor and hospital and much, much more. • 24-hour nurse support – A nurse is a phone call away and you have other health resources available 24-hours a day, 7 days
a week to provide you with information that can help you make informed decisions. Just call the number on the back of your ID card.
• Customer Care telephone support – Need more help? Call a customer care professional using the toll-free number on the back of your ID card. Get answers to your benefit questions or receive help looking for a doctor or hospital.
PLAN HIGHLIGHTS
> Member Copayments do accumulate towards the Deductible.> No one in the family is eligible for benefits until the family coverage deductible is met.> The Annual Deductible is a single combined Tier 1 and Tier 2 Deductible.
> The Out-of-Pocket Maximum includes the Annual Deductible.> If more than one person in a family is covered under the Policy, the single coverage Out-of-Pocket Maximum stated above
does not apply.> Member Copayments do accumulate towards the Out-of-Pocket Maximum.
Types of Coverage Network Benefits
Annual Deductible - Combined Medical and PharmacyIndividual Deductible Tier 1: $2,000 per year
Tier 2: $2,000 per year
Family Deductible Tier 1: $4,000 per yearTier 2: $4,000 per year
Out-of-Pocket Maximum - Combined Medical and PharmacyIndividual Out-of-Pocket Maximum Tier 1: $6,000 per year
Tier 2: $6,000 per year
Family Out-of-Pocket Maximum Tier 1: $12,000 per yearTier 2: $12,000 per year
Benefit Plan Coinsurance - The Amount We PayTier 1: 80% after Deductible has been met.Tier 2: 50% after Deductible has been met.
This Benefit Summary is intended only to highlight your Benefits and should not be relied upon to fully determine your coverage. If this Benefit Summary conflicts in any way with the Certificate of Coverage (COC), the COC shall prevail. It is recommended that you review your COC for an exact description of the services and supplies that are covered, those which are excluded or limited, and other terms and conditions of coverage.
NYWEyYNV11Item# Benefit Accumulator Rev. Date475-5558 Calendar Year 0113_rev01 HH-010/Comb/NonEmb/10896
UnitedHealthcare Insurance Company of New York

Page 2 of 12
Prescription drug benefits are shown under separate cover.
> The Annual Deductible, Out-of-Pocket Maximum and Benefit limits are calculated on a calendar year basis.> All Benefits are reimbursed based on Eligible Expenses. For a definition of Eligible Expenses, please refer to your Certificate
of Coverage.
MOST COMMONLY USED BENEFITS
> In addition to the visit Copayment, the applicable Copayment and any Deductible/Coinsurance applies when these services are done: Lab, X-Ray, CT, PET, MRI, MRA, Nuclear Medicine; Pharmaceutical Products, Scopic Procedures; Surgery; Therapeutic Treatments.
The health care reform law provides for coverage of certain preventive services, based on your age, gender and other health factors, with no cost-sharing. The preventive care services covered under this section are those preventive services specified in the health care reform law. UnitedHealthcare also covers other routine services as described in other areas of this summary, which may require a copayment, coinsurance or deductible. Always refer to your plan documents for your specific coverage.
> In addition to the visit Copayment, the applicable Copayment and any Deductible/Coinsurance applies when these services are done: Lab, X-Ray, CT, PET, MRI, MRA, Nuclear Medicine; Pharmaceutical Products, Scopic Procedures; Surgery; Therapeutic Treatments.
Prescription Drug Benefits
Information on Benefit Limits
Types of Coverage Network Benefits
Physician’s Office Services - Sickness and InjuryPrimary Physician Office Visit Tier 1: 100% after you pay a $20 Copayment per visit.
Tier 2: 100% after you pay a $50 Copayment per visit.
Specialist Physician Office Visit Tier 1: 100% after you pay a $40 Copayment per visit.Tier 2: 100% after you pay a $100 Copayment per visit.
Preventive Care ServicesCovered Health Services include but are not limited to:
Primary Physician Office Visit Tier 1: 100%, Copayments and Deductibles do not apply.Tier 2: 100%, Copayments and Deductibles do not apply.
Specialist Physician Office Visit Tier 1: 100%, Copayments and Deductibles do not apply.Tier 2: 100%, Copayments and Deductibles do not apply.
Lab, X-Ray or other preventive tests
Tier 1: 100%, Copayments and Deductibles do not apply.Tier 2: 100%, Copayments and Deductibles do not apply.
Urgent Care Center ServicesTier 1: 100% after you pay a $100 Copayment per visit.Tier 2: 100% after you pay a $150 Copayment per visit.
Emergency Health Services - OutpatientTier 1: 100% after you pay a $400 Copayment per visit.Tier 2: 100% after you pay a $400 Copayment per visit.
Notification is required if confined in a non-Network Hospital.
Hospital - Inpatient Stay Tier 1: 80% after Deductible has been met.
Tier 2: 50% after Deductible has been met.

Page 3 of 12
ADDITIONAL CORE BENEFITS
Types of Coverage Network Benefits
This benefit category contains services/devices that may be Essential or non-Essential Health Benefits as defined by the Patient Protection and Affordable Care Act depending upon the service or device delivered. A benefit review will take place once the dollar limit is exceeded. If the service/device is determined to be rehabilitative or habilitative in nature, it is an Essential Health Benefit and will be paid. If the benefit/device is determined to be non-essential, the maximum will have been met and the claim will not be paid.
Ambulance Service - Emergency and Non-EmergencyGround Ambulance Tier 1: 80% after Deductible has been met.
Tier 2: 80% after Deductible has been met.
Air Ambulance Tier 1: 80% after Deductible has been met.Tier 2: 80% after Deductible has been met.
Prior Authorization is required for non-Emergency Ambulance.
Congenital Heart Disease (CHD) SurgeriesTier 1: 80% after Deductible has been met.Tier 2: 50% after Deductible has been met.
Dental Services - Accidental Injury, Congenital Disease and AnomalyTier 1: 80% after Deductible has been met.Tier 2: 80% after Deductible has been met.
Prior Authorization is required.
Diabetes ServicesDiabetes Self Management and TrainingDiabetic Eye Examinations/Foot Care
Depending upon where the Covered Health Service is provided, Benefits will be the same as those stated under each Covered Health Service category in this Benefit Summary.
Diabetes Self Management Items Depending upon where the Covered Health Service is provided, Benefits will be the same as those stated under Durable Medical Equipment and in the Outpatient Prescription Drug Rider.
Durable Medical EquipmentBenefits are limited as follows:
$2,500 per year and are limited to a single purchase of a type of Durable Medical Equipment (including repair and replacement) every three years. This limit does not apply to wound vacuums.Items of Durable Medical Equipment related to Essential Benefits under the Patient Protection and Affordable Care Act are unlimited.
Tier 1: 80% after Deductible has been met.Tier 2: 50% after Deductible has been met.
Hearing AidsBenefits are limited as follows:
$2,500 per year and are limited to a single purchase (including repair/replacement) per hearing impaired ear every three years.
Tier 1: 80% after Deductible has been met.Tier 2: 50% after Deductible has been met.

Page 4 of 12
ADDITIONAL CORE BENEFITS
Types of Coverage Network Benefits
YOUR BENEFITS
This benefit category contains services/devices that may be Essential or non-Essential Health Benefits as defined by the Patient Protection and Affordable Care Act depending upon the service or device delivered. A benefit review will take place once the dollar limit is exceeded. If the service/device is determined to be rehabilitative or habilitative in nature, it is an Essential Health Benefit and will be paid. If the benefit/device is determined to be non-essential, the maximum will have been met and the claim will not be paid.
Home Health CareBenefits are limited as follows:
60 visits per year Tier 1: 80% after Deductible has been met.Tier 2: 75% after Deductible has been met.
Hospice CareTier 1: 80% after Deductible has been met.Tier 2: 50% after Deductible has been met.
Lab, X-Ray and Diagnostics - OutpatientFor Preventive Lab, X-Ray and Diagnostics, refer to the Preventive Care Services category.
Lab Testing - Outpatient Tier 1: 80% after Deductible has been met.Tier 2: 50% after Deductible has been met.
X-Ray and Other Diagnostic Testing - Outpatient
Tier 1: 80% after Deductible has been met.Tier 2: 50% after Deductible has been met.
Lab, X-Ray and Major Diagnostics - CT, PET, MRI, MRA and Nuclear Medicine - Outpatient
Tier 1: 80% after Deductible has been met.Tier 2: 50% after Deductible has been met.
Ostomy SuppliesBenefits are limited as follows:
$2,500 per yearTier 1: 80% after Deductible has been met.Tier 2: 50% after Deductible has been met.
Pharmaceutical Products - OutpatientThis includes medications administered in an outpatient setting, in the Physician's Office, or in a Covered Person's home.
Tier 1: 80% after Deductible has been met.Tier 2: 50% after Deductible has been met.
Physician Fees for Surgical and Medical ServicesTier 1: 80% after Deductible has been met.Tier 2: 50% after Deductible has been met.
Pregnancy - Maternity Services Depending upon where the Covered Health Service is provided, Benefits will be the same as those stated under each Covered Health Service category in this Benefit Summary.
For services provided in the Physician's Office, a Copayment will only apply to the initial office visit.
Prosthetic DevicesBenefits are limited as follows:
$2,500 per year and are limited to a single purchase of each type of prosthetic device every three years.
Tier 1: 80% after Deductible has been met.Tier 2: 50% after Deductible has been met.
Reconstructive ProceduresDepending upon where the Covered Health Service is provided, Benefits will be the same as those stated under each Covered Health Service category in this Benefit Summary.
Page 5 of 12
ADDITIONAL CORE BENEFITS
Types of Coverage Network BenefitsRehabilitation Services - Outpatient Therapy and Chiropractic CareBenefits are limited as follows:
20 visits of physical therapy20 visits of occupational therapy20 visits of speech therapy20 visits of pulmonary rehabilitation36 visits of cardiac rehabilitation30 visits of post-cochlear implant aural therapy20 visits of cognitive rehabilitation therapy
Tier 1: 100% after you pay a $20 Copayment per visit.Tier 2: 100% after you pay a $50 Copayment per visit.
Scopic Procedures - Outpatient Diagnostic and TherapeuticDiagnostic scopic procedures include, but are not limited to:
ColonoscopySigmoidoscopyEndoscopy
For Preventive Scopic Procedures, refer to the Preventive Care Services category.
Tier 1: 80% after Deductible has been met.Tier 2: 50% after Deductible has been met.
Skilled Nursing Facility / Inpatient Rehabilitation Facility ServicesBenefits are limited as follows:
60 days per year Tier 1: 80% after Deductible has been met.Tier 2: 50% after Deductible has been met.
Surgery - OutpatientTier 1: 80% after Deductible has been met.Tier 2: 50% after Deductible has been met.
Therapeutic Treatments - OutpatientTherapeutic treatments include, but are not limited to:
DialysisIntravenous chemotherapy or other intravenous infusion therapyRadiation oncology
Tier 1: 80% after Deductible has been met.Tier 2: 50% after Deductible has been met.
Transplantation ServicesDepending upon where the Covered Health Service is provided, Benefits will be the same as those stated under each Covered Health Service category in this Benefit Summary.
For Network Benefits, services must be received at a Designated Facility.
Prior Authorization is required.

Page 6 of 12
ADDITIONAL CORE BENEFITS
Types of Coverage Network Benefits
YOUR BENEFITS
Vision ExaminationsBenefits are limited as follows:
1 exam every 2 yearsTier 1: 100% after you pay a $20 Copayment per visit.Tier 2: 100% after you pay a $20 Copayment per visit.
Page 7 of 12
STATE MANDATED BENEFITS
Types of Coverage Network BenefitsClinical TrialsParticipation in a qualifying clinical trial for the treatment of:
CancerCardiovascular (cardiac/stroke)Surgical musculoskeletal disorders of the spine, hip and knees
Depending upon where the Covered Health Service is provided, Benefits will be the same as those stated under each Covered Health Service category in this Benefit Summary.
Prior Authorization is required.
Experimental or Investigational or Unproven ServicesDepending upon the Covered Health Service, Benefit limits are the same as those stated under the specific Benefit category in this Benefit Summary.
Depending upon where the Covered Health Service is provided, Benefits will be the same as those stated under each Covered Health Service category in this Benefit Summary.
Infertility ServicesTier 1: 80% after Deductible has been met.Tier 2: 50% after Deductible has been met.
Prior Authorization is required.
Mental Health ServicesFor groups with 50 or less total employees:Benefits are limited as follows:
For groups with 50 or less total employees:Inpatient:Tier 1: 80% after Deductible has been met.Tier 2: 80% after Deductible has been met.
30 days per year for Inpatient30 visits per year for Outpatient
Outpatient:Tier 1: 100% after you pay a $20 Copayment per visit.Tier 2: 100% after you pay a $20 Copayment per visit.
For groups with 51 or more total employees:Benefit limits do not apply
For groups with 51 or more total employees:Inpatient:Tier 1: 80% after Deductible has been met.Tier 2: 80% after Deductible has been met.
Outpatient:Tier 1: 100% after you pay a $20 Copayment per visit.Tier 2: 100% after you pay a $20 Copayment per visit.
Page 8 of 12
STATE MANDATED BENEFITS
Types of Coverage Network Benefits
YOUR BENEFITS
Neurobiological Disorders – Autism Spectrum Disorder ServicesFor groups with 50 or less total employees:
For groups with 50 or less total employees:Inpatient:Tier 1: 80% after Deductible has been met.Tier 2: 80% after Deductible has been met.
Outpatient:Tier 1: 100% after you pay a $20 Copayment per visit.Tier 2: 100% after you pay a $20 Copayment per visit.
For groups with 51 or more total employees:
For groups with 51 or more total employees:Inpatient:Tier 1: 80% after Deductible has been met.Tier 2: 80% after Deductible has been met.
Outpatient:Tier 1: 100% after you pay a $20 Copayment per visit.Tier 2: 100% after you pay a $20 Copayment per visit.
Obesity SurgeryDepending upon where the Covered Health Service is provided, Benefits will be the same as those stated under each Covered Health Service category in this Benefit Summary.
Prior Authorization is required.
Substance Use Disorder ServicesFor groups with 50 or less total employees:Benefits are limited as follows:
For groups with 50 or less total employees:Inpatient:Tier 1: 80% after Deductible has been met.Tier 2: 80% after Deductible has been met.
7 days of detoxification and 30 days per year for Inpatient.60 visits per year for Outpatient. Benefits for up to 20 of these visits are available for Covered Persons who are family members of the person suffering from the disease of alcoholism, substance abuse or chemical dependency.
Outpatient:Tier 1: 100% after you pay a $20 Copayment per visit.Tier 2: 100% after you pay a $20 Copayment per visit.
For groups with 51 or more total employees:Benefit limits do not apply
For groups with 51 or more total employees:Inpatient:Tier 1: 80% after Deductible has been met.Tier 2: 80% after Deductible has been met.
Outpatient:Tier 1: 100% after you pay a $20 Copayment per visit.Tier 2: 100% after you pay a $20 Copayment per visit.

Page 9 of 12
STATE MANDATED BENEFITS
Types of Coverage Network BenefitsTemporomandibular Joint Services
Depending upon where the Covered Health Service is provided, Benefits will be the same as those stated under each Covered Health Service category in this Benefit Summary.
This Benefit Summary is intended only to highlight your Benefits and should not be relied upon to fully determine your coverage. If this Benefit Summary conflicts in any way with the Certificate of Coverage (COC), the COC shall prevail. It is recommended that you review your COC for an exact description of the services and supplies that are covered, those which are excluded or limited, and other terms and conditions of coverage.
Page 10 of 12
MEDICAL EXCLUSIONS
It is recommended that you review your COC for an exact description of the services and supplies that are covered, those which are excluded or limited, and other terms and conditions of coverage.
Dental care or treatment except for such care or treatment due to accidental injury to sound natural teeth within 12 months of the accident and except for dental care or treatment necessary due to congenital disease or anomaly for which Benefits are provided under Dental Services - Accidental Injury, Congenital Disease and Anomaly in Section 1 of the COC.
Routine foot care in conjunction with corns, calluses, flat feet, fallen arches, weak feet, chronic foot strain or symptomatic complaints of the feet. This exclusion does not apply to preventive foot care for Covered Persons who are at risk of neurological or vascular disease arising from diseases such as diabetes for which Benefits are provided as described under Diabetes Services in Section 1 of the COC.
Television; telephone; beauty/barber service; guest service. Supplies, equipment and similar incidental services and supplies for personal comfort. Examples include: air conditioners, air purifiers and filters, dehumidifiers; batteries and battery chargers; breast pumps (this exclusion does not apply to breast pumps for which Benefits are provided under the Health Resources and Services Administration (HRSA) requirement); car seats; chairs, bath chairs, feeding chairs, toddler chairs, chair lifts, recliners; exercise equipment; home modifications such as elevators, handrails and ramps; hot tubs; humidifiers; Jacuzzis; mattresses; medical alert systems; motorized beds; music devices; personal computers, pillows; power-operated vehicles; radios; saunas; stair lifts and stair glides; strollers; safety equipment; treadmills; vehicle modifications such as van lifts; video players, whirlpools.
Cosmetic Procedures unless Medically Necessary. Certain Cosmetic Procedures as listed in Part 56 of New York Regulation 183 will not be subject to a Medical Necessity review if we receive the claim with no accompanying medical information after services were performed. Cosmetic surgery will not include reconstructive surgery when such service is incidental to or follows surgery resulting from trauma, infection or diseases of the involved part, and reconstructive surgery because of Congenital Anomaly or disease of a Covered Dependent child which has resulted in a functional defect. See the definition in Section 9 of the COC.
Services performed by a provider who is a member of the Covered Person's immediate family.
Health services for which benefits are provided under Medicare or other governmental programs (except Medicaid), any state or Federal worker's compensation, employer's liability or occupational disease law. Treatment provided in a government hospital. Benefits to the extent provided for any loss or portion thereof for which mandatory automobile no-fault benefits are recovered or recoverable. Services rendered separately billed by employees of Hospitals, laboratories or other institutions.
Health services provided outside the United States and its possessions, Mexico and Canada, unless required as Emergency Health Services.
Custodial care. Rest cures.
Purchase cost and fitting charge for eye glasses and contact lenses.
Health services received as a result of illness, accident treatment or medical condition arising out of: war or any act of war, (whether declared or undeclared); participation in a felony, riot or insurrection; service in the armed forces or units auxillary thereto; suicide, attempted suicide or intentionally self-inflicted injury; aviation other than as a fare-paying passenger on a scheduled or charter flight operated by a scheduled airliner. Health services for which a charge would not ordinarily be made. Illegal occupation: The insurer shall not be liable for any loss to which a contributing cause was the insured's commission of or attempt to commit a felony or to which a contributing cause was the insured's being engaged in an illegal occupation.
Dental
Foot Care
Personal Care, Comfort or Convenience
Physical Appearance
Providers
Services Provided under Another Plan
Travel
Types of Care
Vision and Hearing
All Other Exclusions

Page 11 of 12
MEDICAL EXCLUSIONS CONTINUED
Benefits for the treatment of a Preexisting Condition are excluded until the earlier of the following: The date you have had Continuous Creditable Coverage for 12 months; or the date you have had Continuous Creditable Coverage for 18 months if you are a Late Enrollee. This exclusion does not apply to Covered Persons under age 19. This exclusion does not apply to pregnancy or an individual, and any dependent of such individual, who is eligible for a federal tax credit under the federal Trade Adjustment Assistance Reform Act of 2002 and who has three months or more of Continuous Creditable Coverage. Note: See the definition of Continuous Creditable Coverage and Preexisting Condition in Section 9 of the COC.
Preexisting Conditions (Applies only to groups of 50 or less employees)
UnitedHealthcare Insurance Company of New York

Page 12 of 12
THIS PAGE INTENTIONALLY LEFT BLANK
Page 1 of 12
YOUR BENEFITS
Benefit SummaryNew York - Choice
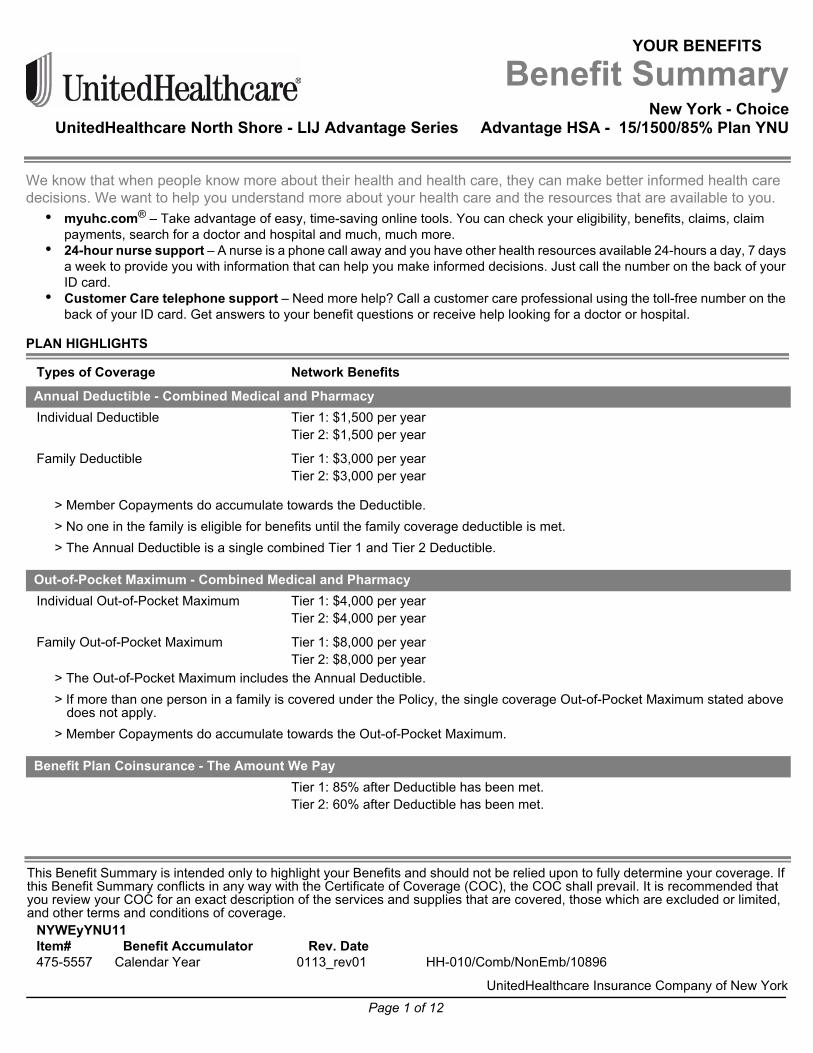
UnitedHealthcare North Shore - LIJ Advantage Series Advantage HSA - 15/1500/85% Plan YNU
We know that when people know more about their health and health care, they can make better informed health care decisions. We want to help you understand more about your health care and the resources that are available to you.• myuhc.com® – Take advantage of easy, time-saving online tools. You can check your eligibility, benefits, claims, claim
payments, search for a doctor and hospital and much, much more. • 24-hour nurse support – A nurse is a phone call away and you have other health resources available 24-hours a day, 7 days
a week to provide you with information that can help you make informed decisions. Just call the number on the back of your ID card.
• Customer Care telephone support – Need more help? Call a customer care professional using the toll-free number on the back of your ID card. Get answers to your benefit questions or receive help looking for a doctor or hospital.
PLAN HIGHLIGHTS
> Member Copayments do accumulate towards the Deductible.> No one in the family is eligible for benefits until the family coverage deductible is met.> The Annual Deductible is a single combined Tier 1 and Tier 2 Deductible.
> The Out-of-Pocket Maximum includes the Annual Deductible.> If more than one person in a family is covered under the Policy, the single coverage Out-of-Pocket Maximum stated above
does not apply.> Member Copayments do accumulate towards the Out-of-Pocket Maximum.
Types of Coverage Network Benefits
Annual Deductible - Combined Medical and PharmacyIndividual Deductible Tier 1: $1,500 per year
Tier 2: $1,500 per year
Family Deductible Tier 1: $3,000 per yearTier 2: $3,000 per year
Out-of-Pocket Maximum - Combined Medical and PharmacyIndividual Out-of-Pocket Maximum Tier 1: $4,000 per year
Tier 2: $4,000 per year
Family Out-of-Pocket Maximum Tier 1: $8,000 per yearTier 2: $8,000 per year
Benefit Plan Coinsurance - The Amount We PayTier 1: 85% after Deductible has been met.Tier 2: 60% after Deductible has been met.
This Benefit Summary is intended only to highlight your Benefits and should not be relied upon to fully determine your coverage. If this Benefit Summary conflicts in any way with the Certificate of Coverage (COC), the COC shall prevail. It is recommended that you review your COC for an exact description of the services and supplies that are covered, those which are excluded or limited, and other terms and conditions of coverage.
NYWEyYNU11Item# Benefit Accumulator Rev. Date475-5557 Calendar Year 0113_rev01 HH-010/Comb/NonEmb/10896
UnitedHealthcare Insurance Company of New York

Page 2 of 12
Prescription drug benefits are shown under separate cover.
> The Annual Deductible, Out-of-Pocket Maximum and Benefit limits are calculated on a calendar year basis.> All Benefits are reimbursed based on Eligible Expenses. For a definition of Eligible Expenses, please refer to your Certificate
of Coverage.
MOST COMMONLY USED BENEFITS
> In addition to the visit Copayment, the applicable Copayment and any Deductible/Coinsurance applies when these services are done: Lab, X-Ray, CT, PET, MRI, MRA, Nuclear Medicine; Pharmaceutical Products, Scopic Procedures; Surgery; Therapeutic Treatments.
The health care reform law provides for coverage of certain preventive services, based on your age, gender and other health factors, with no cost-sharing. The preventive care services covered under this section are those preventive services specified in the health care reform law. UnitedHealthcare also covers other routine services as described in other areas of this summary, which may require a copayment, coinsurance or deductible. Always refer to your plan documents for your specific coverage.
> In addition to the visit Copayment, the applicable Copayment and any Deductible/Coinsurance applies when these services are done: Lab, X-Ray, CT, PET, MRI, MRA, Nuclear Medicine; Pharmaceutical Products, Scopic Procedures; Surgery; Therapeutic Treatments.
Prescription Drug Benefits
Information on Benefit Limits
Types of Coverage Network Benefits
Physician’s Office Services - Sickness and InjuryPrimary Physician Office Visit Tier 1: 100% after you pay a $15 Copayment per visit.
Tier 2: 100% after you pay a $30 Copayment per visit.
Specialist Physician Office Visit Tier 1: 100% after you pay a $30 Copayment per visit.Tier 2: 100% after you pay a $60 Copayment per visit.
Preventive Care ServicesCovered Health Services include but are not limited to:
Primary Physician Office Visit Tier 1: 100%, Copayments and Deductibles do not apply.Tier 2: 100%, Copayments and Deductibles do not apply.
Specialist Physician Office Visit Tier 1: 100%, Copayments and Deductibles do not apply.Tier 2: 100%, Copayments and Deductibles do not apply.
Lab, X-Ray or other preventive tests
Tier 1: 100%, Copayments and Deductibles do not apply.Tier 2: 100%, Copayments and Deductibles do not apply.
Urgent Care Center ServicesTier 1: 100% after you pay a $75 Copayment per visit.Tier 2: 100% after you pay a $125 Copayment per visit.
Emergency Health Services - OutpatientTier 1: 100% after you pay a $300 Copayment per visit.Tier 2: 100% after you pay a $300 Copayment per visit.
Notification is required if confined in a non-Network Hospital.
Hospital - Inpatient Stay Tier 1: 85% after Deductible has been met.
Tier 2: 60% after Deductible has been met.
Page 3 of 12
ADDITIONAL CORE BENEFITS
Types of Coverage Network Benefits
This benefit category contains services/devices that may be Essential or non-Essential Health Benefits as defined by the Patient Protection and Affordable Care Act depending upon the service or device delivered. A benefit review will take place once the dollar limit is exceeded. If the service/device is determined to be rehabilitative or habilitative in nature, it is an Essential Health Benefit and will be paid. If the benefit/device is determined to be non-essential, the maximum will have been met and the claim will not be paid.
Ambulance Service - Emergency and Non-EmergencyGround Ambulance Tier 1: 85% after Deductible has been met.
Tier 2: 85% after Deductible has been met.
Air Ambulance Tier 1: 85% after Deductible has been met.Tier 2: 85% after Deductible has been met.
Prior Authorization is required for non-Emergency Ambulance.
Congenital Heart Disease (CHD) SurgeriesTier 1: 85% after Deductible has been met.Tier 2: 60% after Deductible has been met.
Dental Services - Accidental Injury, Congenital Disease and AnomalyTier 1: 85% after Deductible has been met.Tier 2: 85% after Deductible has been met.
Prior Authorization is required.
Diabetes ServicesDiabetes Self Management and TrainingDiabetic Eye Examinations/Foot Care
Depending upon where the Covered Health Service is provided, Benefits will be the same as those stated under each Covered Health Service category in this Benefit Summary.
Diabetes Self Management Items Depending upon where the Covered Health Service is provided, Benefits will be the same as those stated under Durable Medical Equipment and in the Outpatient Prescription Drug Rider.
Durable Medical EquipmentBenefits are limited as follows:
$2,500 per year and are limited to a single purchase of a type of Durable Medical Equipment (including repair and replacement) every three years. This limit does not apply to wound vacuums.Items of Durable Medical Equipment related to Essential Benefits under the Patient Protection and Affordable Care Act are unlimited.
Tier 1: 85% after Deductible has been met.Tier 2: 60% after Deductible has been met.
Hearing AidsBenefits are limited as follows:
$2,500 per year and are limited to a single purchase (including repair/replacement) per hearing impaired ear every three years.
Tier 1: 85% after Deductible has been met.Tier 2: 60% after Deductible has been met.
Page 4 of 12
ADDITIONAL CORE BENEFITS
Types of Coverage Network Benefits
YOUR BENEFITS
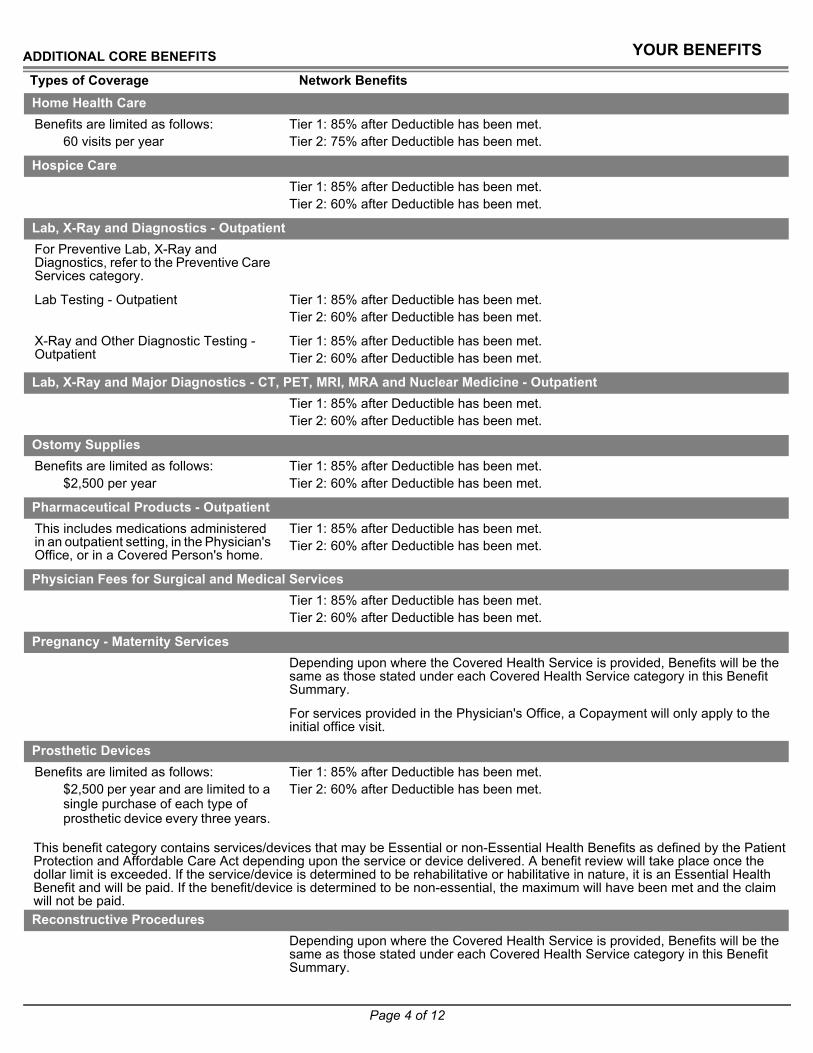
This benefit category contains services/devices that may be Essential or non-Essential Health Benefits as defined by the Patient Protection and Affordable Care Act depending upon the service or device delivered. A benefit review will take place once the dollar limit is exceeded. If the service/device is determined to be rehabilitative or habilitative in nature, it is an Essential Health Benefit and will be paid. If the benefit/device is determined to be non-essential, the maximum will have been met and the claim will not be paid.
Home Health CareBenefits are limited as follows:
60 visits per year Tier 1: 85% after Deductible has been met.Tier 2: 75% after Deductible has been met.
Hospice CareTier 1: 85% after Deductible has been met.Tier 2: 60% after Deductible has been met.
Lab, X-Ray and Diagnostics - OutpatientFor Preventive Lab, X-Ray and Diagnostics, refer to the Preventive Care Services category.
Lab Testing - Outpatient Tier 1: 85% after Deductible has been met.Tier 2: 60% after Deductible has been met.
X-Ray and Other Diagnostic Testing - Outpatient
Tier 1: 85% after Deductible has been met.Tier 2: 60% after Deductible has been met.
Lab, X-Ray and Major Diagnostics - CT, PET, MRI, MRA and Nuclear Medicine - Outpatient
Tier 1: 85% after Deductible has been met.Tier 2: 60% after Deductible has been met.
Ostomy SuppliesBenefits are limited as follows:
$2,500 per yearTier 1: 85% after Deductible has been met.Tier 2: 60% after Deductible has been met.
Pharmaceutical Products - OutpatientThis includes medications administered in an outpatient setting, in the Physician's Office, or in a Covered Person's home.
Tier 1: 85% after Deductible has been met.Tier 2: 60% after Deductible has been met.
Physician Fees for Surgical and Medical ServicesTier 1: 85% after Deductible has been met.Tier 2: 60% after Deductible has been met.
Pregnancy - Maternity Services Depending upon where the Covered Health Service is provided, Benefits will be the same as those stated under each Covered Health Service category in this Benefit Summary.
For services provided in the Physician's Office, a Copayment will only apply to the initial office visit.
Prosthetic DevicesBenefits are limited as follows:
$2,500 per year and are limited to a single purchase of each type of prosthetic device every three years.
Tier 1: 85% after Deductible has been met.Tier 2: 60% after Deductible has been met.
Reconstructive ProceduresDepending upon where the Covered Health Service is provided, Benefits will be the same as those stated under each Covered Health Service category in this Benefit Summary.

Page 5 of 12
ADDITIONAL CORE BENEFITS
Types of Coverage Network BenefitsRehabilitation Services - Outpatient Therapy and Chiropractic CareBenefits are limited as follows:
20 visits of physical therapy20 visits of occupational therapy20 visits of speech therapy20 visits of pulmonary rehabilitation36 visits of cardiac rehabilitation30 visits of post-cochlear implant aural therapy20 visits of cognitive rehabilitation therapy
Tier 1: 100% after you pay a $15 Copayment per visit.Tier 2: 100% after you pay a $30 Copayment per visit.
Scopic Procedures - Outpatient Diagnostic and TherapeuticDiagnostic scopic procedures include, but are not limited to:
ColonoscopySigmoidoscopyEndoscopy
For Preventive Scopic Procedures, refer to the Preventive Care Services category.
Tier 1: 85% after Deductible has been met.Tier 2: 60% after Deductible has been met.
Skilled Nursing Facility / Inpatient Rehabilitation Facility ServicesBenefits are limited as follows:
60 days per year Tier 1: 85% after Deductible has been met.Tier 2: 60% after Deductible has been met.
Surgery - OutpatientTier 1: 85% after Deductible has been met.Tier 2: 60% after Deductible has been met.
Therapeutic Treatments - OutpatientTherapeutic treatments include, but are not limited to:
DialysisIntravenous chemotherapy or other intravenous infusion therapyRadiation oncology
Tier 1: 85% after Deductible has been met.Tier 2: 60% after Deductible has been met.
Transplantation ServicesDepending upon where the Covered Health Service is provided, Benefits will be the same as those stated under each Covered Health Service category in this Benefit Summary.
For Network Benefits, services must be received at a Designated Facility.
Prior Authorization is required.

Page 6 of 12
ADDITIONAL CORE BENEFITS
Types of Coverage Network Benefits
YOUR BENEFITS
Vision ExaminationsBenefits are limited as follows:
1 exam every 2 yearsTier 1: 100% after you pay a $15 Copayment per visit.Tier 2: 100% after you pay a $15 Copayment per visit.

Page 7 of 12
STATE MANDATED BENEFITS
Types of Coverage Network BenefitsClinical TrialsParticipation in a qualifying clinical trial for the treatment of:
CancerCardiovascular (cardiac/stroke)Surgical musculoskeletal disorders of the spine, hip and knees
Depending upon where the Covered Health Service is provided, Benefits will be the same as those stated under each Covered Health Service category in this Benefit Summary.
Prior Authorization is required.
Experimental or Investigational or Unproven ServicesDepending upon the Covered Health Service, Benefit limits are the same as those stated under the specific Benefit category in this Benefit Summary.
Depending upon where the Covered Health Service is provided, Benefits will be the same as those stated under each Covered Health Service category in this Benefit Summary.
Infertility ServicesTier 1: 85% after Deductible has been met.Tier 2: 60% after Deductible has been met.
Prior Authorization is required.
Mental Health ServicesFor groups with 50 or less total employees:Benefits are limited as follows:
For groups with 50 or less total employees:Inpatient:Tier 1: 85% after Deductible has been met.Tier 2: 85% after Deductible has been met.
30 days per year for Inpatient30 visits per year for Outpatient
Outpatient:Tier 1: 100% after you pay a $15 Copayment per visit.Tier 2: 100% after you pay a $15 Copayment per visit.
For groups with 51 or more total employees:Benefit limits do not apply
For groups with 51 or more total employees:Inpatient:Tier 1: 85% after Deductible has been met.Tier 2: 85% after Deductible has been met.
Outpatient:Tier 1: 100% after you pay a $15 Copayment per visit.Tier 2: 100% after you pay a $15 Copayment per visit.

Page 8 of 12
STATE MANDATED BENEFITS
Types of Coverage Network Benefits
YOUR BENEFITS
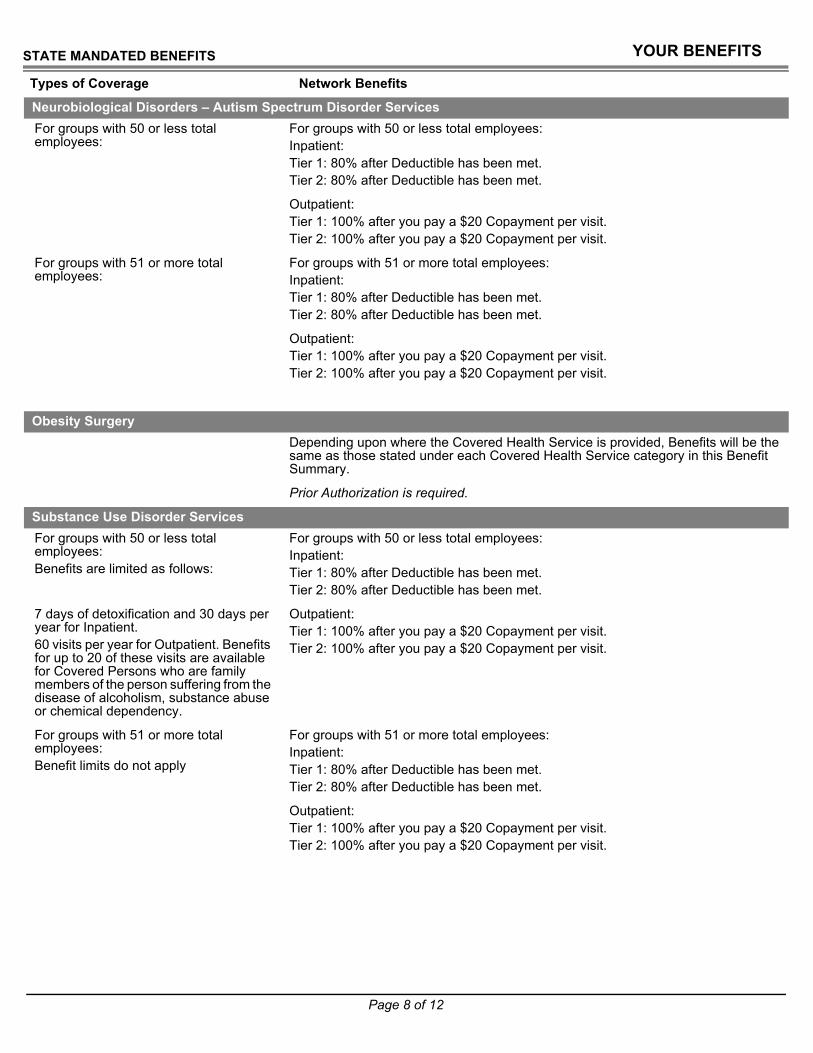
Neurobiological Disorders – Autism Spectrum Disorder ServicesFor groups with 50 or less total employees:
For groups with 50 or less total employees:Inpatient:Tier 1: 85% after Deductible has been met.Tier 2: 85% after Deductible has been met.
Outpatient:Tier 1: 100% after you pay a $15 Copayment per visit.Tier 2: 100% after you pay a $15 Copayment per visit.
For groups with 51 or more total employees:
For groups with 51 or more total employees:Inpatient:Tier 1: 85% after Deductible has been met.Tier 2: 85% after Deductible has been met.
Outpatient:Tier 1: 100% after you pay a $15 Copayment per visit.Tier 2: 100% after you pay a $15 Copayment per visit.
Obesity SurgeryDepending upon where the Covered Health Service is provided, Benefits will be the same as those stated under each Covered Health Service category in this Benefit Summary.
Prior Authorization is required.
Substance Use Disorder ServicesFor groups with 50 or less total employees:Benefits are limited as follows:
For groups with 50 or less total employees:Inpatient:Tier 1: 85% after Deductible has been met.Tier 2: 85% after Deductible has been met.
7 days of detoxification and 30 days per year for Inpatient.60 visits per year for Outpatient. Benefits for up to 20 of these visits are available for Covered Persons who are family members of the person suffering from the disease of alcoholism, substance abuse or chemical dependency.
Outpatient:Tier 1: 100% after you pay a $15 Copayment per visit.Tier 2: 100% after you pay a $15 Copayment per visit.
For groups with 51 or more total employees:Benefit limits do not apply
For groups with 51 or more total employees:Inpatient:Tier 1: 85% after Deductible has been met.Tier 2: 85% after Deductible has been met.
Outpatient:Tier 1: 100% after you pay a $15 Copayment per visit.Tier 2: 100% after you pay a $15 Copayment per visit.

Page 9 of 12
STATE MANDATED BENEFITS
Types of Coverage Network BenefitsTemporomandibular Joint Services
Depending upon where the Covered Health Service is provided, Benefits will be the same as those stated under each Covered Health Service category in this Benefit Summary.
This Benefit Summary is intended only to highlight your Benefits and should not be relied upon to fully determine your coverage. If this Benefit Summary conflicts in any way with the Certificate of Coverage (COC), the COC shall prevail. It is recommended that you review your COC for an exact description of the services and supplies that are covered, those which are excluded or limited, and other terms and conditions of coverage.

Page 10 of 12
MEDICAL EXCLUSIONS
It is recommended that you review your COC for an exact description of the services and supplies that are covered, those which are excluded or limited, and other terms and conditions of coverage.
Dental care or treatment except for such care or treatment due to accidental injury to sound natural teeth within 12 months of the accident and except for dental care or treatment necessary due to congenital disease or anomaly for which Benefits are provided under Dental Services - Accidental Injury, Congenital Disease and Anomaly in Section 1 of the COC.
Routine foot care in conjunction with corns, calluses, flat feet, fallen arches, weak feet, chronic foot strain or symptomatic complaints of the feet. This exclusion does not apply to preventive foot care for Covered Persons who are at risk of neurological or vascular disease arising from diseases such as diabetes for which Benefits are provided as described under Diabetes Services in Section 1 of the COC.
Television; telephone; beauty/barber service; guest service. Supplies, equipment and similar incidental services and supplies for personal comfort. Examples include: air conditioners, air purifiers and filters, dehumidifiers; batteries and battery chargers; breast pumps (this exclusion does not apply to breast pumps for which Benefits are provided under the Health Resources and Services Administration (HRSA) requirement); car seats; chairs, bath chairs, feeding chairs, toddler chairs, chair lifts, recliners; exercise equipment; home modifications such as elevators, handrails and ramps; hot tubs; humidifiers; Jacuzzis; mattresses; medical alert systems; motorized beds; music devices; personal computers, pillows; power-operated vehicles; radios; saunas; stair lifts and stair glides; strollers; safety equipment; treadmills; vehicle modifications such as van lifts; video players, whirlpools.
Cosmetic Procedures unless Medically Necessary. Certain Cosmetic Procedures as listed in Part 56 of New York Regulation 183 will not be subject to a Medical Necessity review if we receive the claim with no accompanying medical information after services were performed. Cosmetic surgery will not include reconstructive surgery when such service is incidental to or follows surgery resulting from trauma, infection or diseases of the involved part, and reconstructive surgery because of Congenital Anomaly or disease of a Covered Dependent child which has resulted in a functional defect. See the definition in Section 9 of the COC.
Services performed by a provider who is a member of the Covered Person's immediate family.
Health services for which benefits are provided under Medicare or other governmental programs (except Medicaid), any state or Federal worker's compensation, employer's liability or occupational disease law. Treatment provided in a government hospital. Benefits to the extent provided for any loss or portion thereof for which mandatory automobile no-fault benefits are recovered or recoverable. Services rendered separately billed by employees of Hospitals, laboratories or other institutions.
Health services provided outside the United States and its possessions, Mexico and Canada, unless required as Emergency Health Services.
Custodial care. Rest cures.
Purchase cost and fitting charge for eye glasses and contact lenses.
Health services received as a result of illness, accident treatment or medical condition arising out of: war or any act of war, (whether declared or undeclared); participation in a felony, riot or insurrection; service in the armed forces or units auxillary thereto; suicide, attempted suicide or intentionally self-inflicted injury; aviation other than as a fare-paying passenger on a scheduled or charter flight operated by a scheduled airliner. Health services for which a charge would not ordinarily be made. Illegal occupation: The insurer shall not be liable for any loss to which a contributing cause was the insured's commission of or attempt to commit a felony or to which a contributing cause was the insured's being engaged in an illegal occupation.
Dental
Foot Care
Personal Care, Comfort or Convenience
Physical Appearance
Providers
Services Provided under Another Plan
Travel
Types of Care
Vision and Hearing
All Other Exclusions
Page 11 of 12
MEDICAL EXCLUSIONS CONTINUED
Benefits for the treatment of a Preexisting Condition are excluded until the earlier of the following: The date you have had Continuous Creditable Coverage for 12 months; or the date you have had Continuous Creditable Coverage for 18 months if you are a Late Enrollee. This exclusion does not apply to Covered Persons under age 19. This exclusion does not apply to pregnancy or an individual, and any dependent of such individual, who is eligible for a federal tax credit under the federal Trade Adjustment Assistance Reform Act of 2002 and who has three months or more of Continuous Creditable Coverage. Note: See the definition of Continuous Creditable Coverage and Preexisting Condition in Section 9 of the COC.
Preexisting Conditions (Applies only to groups of 50 or less employees)
UnitedHealthcare Insurance Company of New York

Page 12 of 12
THIS PAGE INTENTIONALLY LEFT BLANK
Related Documents











