Unit 7: Treatment of TB Unit 7: Treatment of TB Botswana National Tuberculosis Programme Manual Training for Medical Officers

Unit 7: Treatment of TB Botswana National Tuberculosis Programme Manual Training for Medical Officers.
Dec 22, 2015
Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript
Unit 7: Treatment of TBUnit 7: Treatment of TB
Botswana National Tuberculosis Programme Manual Training for Medical Officers
Slide 7-2Unit 7: Treatment of TB
ObjectivesObjectives
At the end of this unit, participants will be able to:
• Explain the principles of TB treatment
• Use the category regimens appropriately
• Properly monitor treatment, follow-up, and end of treatment
• Discuss side effects of drugs and their management
Slide 7-3Unit 7: Treatment of TB
Admission PolicyAdmission Policy
• Admit patients who present with the following: • TB meningitis and miliary TB, until ambulatory • Danger signs (e.g., respiratory distress,
temperature of 39º C or more, inability to walk unaided)
• Spinal TB • Severe adverse events (e.g. hepatitis)
• Observe strict infection control and isolation procedures
Slide 7-4Unit 7: Treatment of TB
Aims of TB Treatment Aims of TB Treatment
• Cure the patient of TB
• Prevent death from active TB or its latent effects
• Prevent relapse of TB
• Prevent the development of acquired resistance
• Prevent transmission of TB to others
Slide 7-5Unit 7: Treatment of TB
Importance of Follow-upImportance of Follow-up
Retrospective analysis in 1997 in Gaborone with 127 patients:• 11.8% had treatment delay• 10.2% had incomplete workup (one smear
performed) & were not registered• 4.5% had 2 or more positive smears and were not
registered for treatment
Source: Creek T, et al., Int J Tuberc Lung Dis, 2000.
Slide 7-6Unit 7: Treatment of TB
Treatment Regimens Treatment Regimens
• Category I regimen for new patients
• Category II regimen for re-treatment patients
• Category III regimen for children with less severe cases of TB
• Category IV for chronic and MDR-TB cases
Slide 7-7Unit 7: Treatment of TB
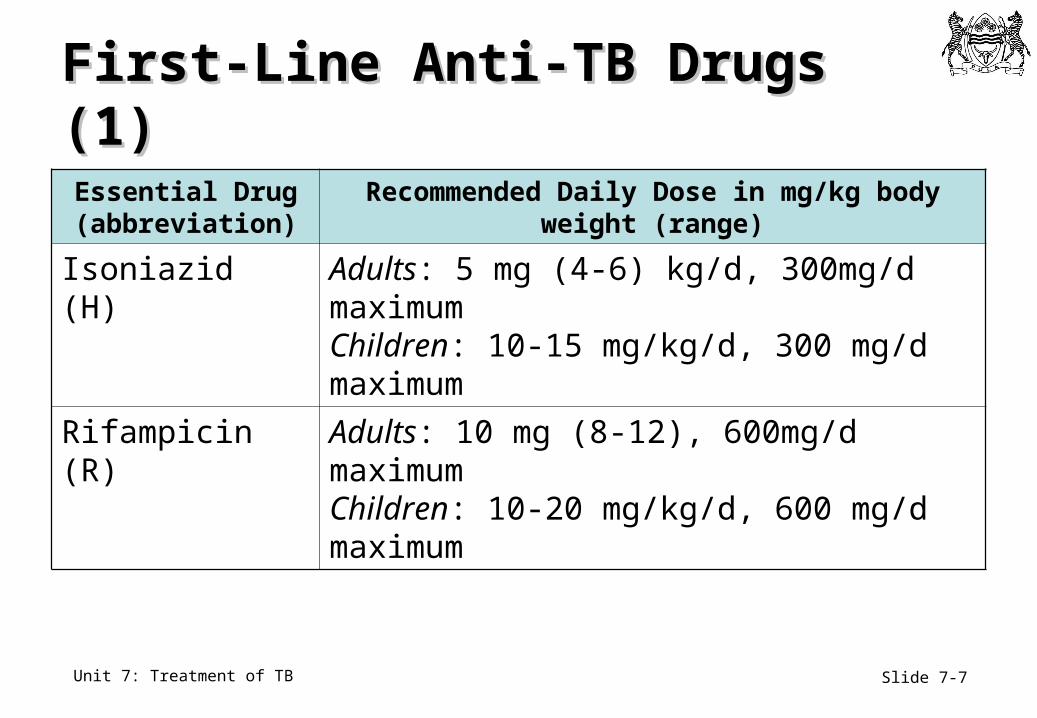
First-Line Anti-TB Drugs (1)First-Line Anti-TB Drugs (1)
Essential Drug (abbreviation)
Recommended Daily Dose in mg/kg body weight (range)
Isoniazid (H) Adults: 5 mg (4-6) kg/d, 300mg/d maximumChildren: 10-15 mg/kg/d, 300 mg/d maximum
Rifampicin (R) Adults: 10 mg (8-12), 600mg/d maximumChildren: 10-20 mg/kg/d, 600 mg/d maximum
Slide 7-8Unit 7: Treatment of TB
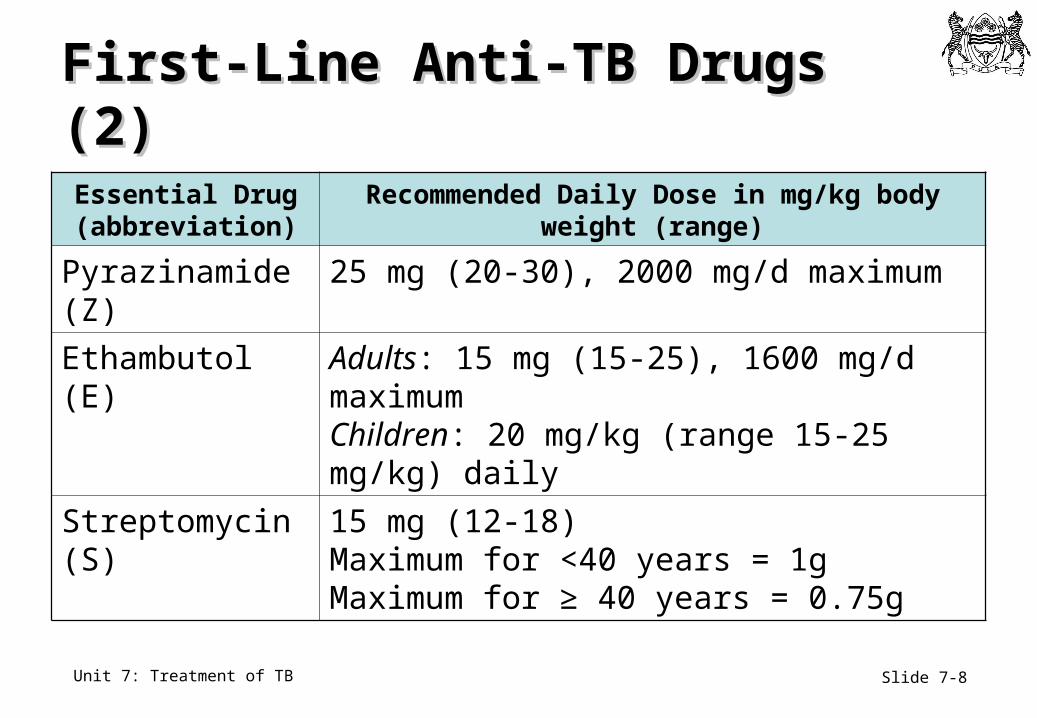
Essential Drug (abbreviation)
Recommended Daily Dose in mg/kg body weight (range)
Pyrazinamide (Z) 25 mg (20-30), 2000 mg/d maximum
Ethambutol (E) Adults: 15 mg (15-25), 1600 mg/d maximumChildren: 20 mg/kg (range 15-25 mg/kg) daily
Streptomycin (S) 15 mg (12-18) Maximum for <40 years = 1g Maximum for ≥ 40 years = 0.75g
First-Line Anti-TB Drugs (2)First-Line Anti-TB Drugs (2)
Slide 7-9Unit 7: Treatment of TB
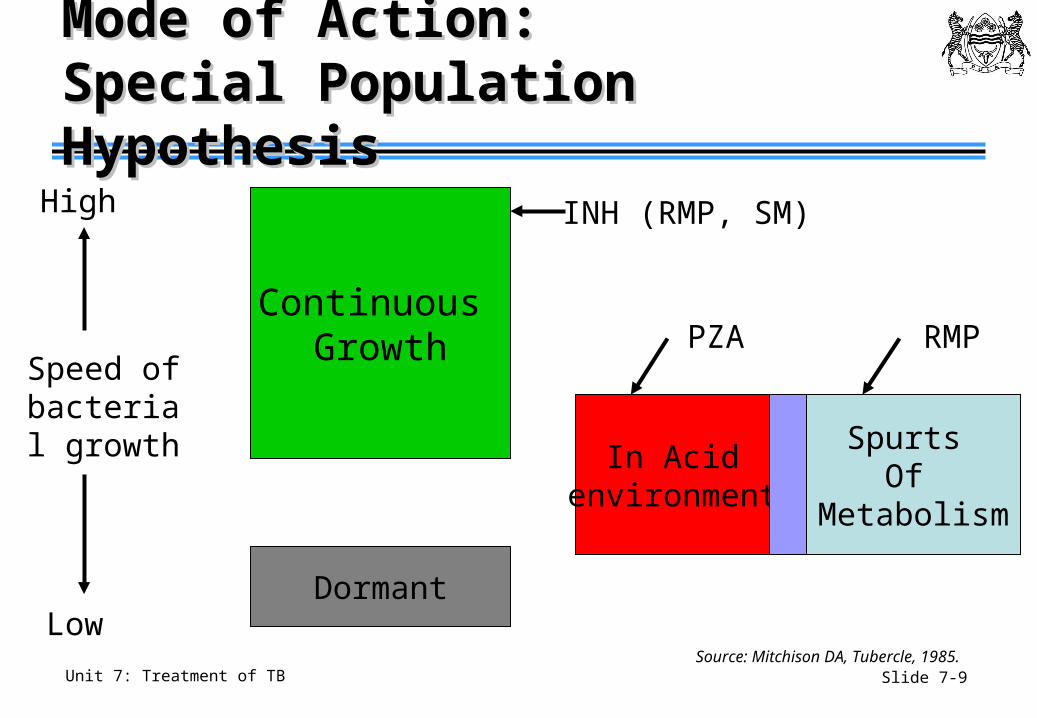
Mode of Action: Mode of Action: Special Population HypothesisSpecial Population Hypothesis
Continuous Growth
Dormant
In Acid environment
Spurts Of
Metabolism
Speed of bacterial growth
High
Low
INH (RMP, SM)
PZA RMP
Source: Mitchison DA, Tubercle, 1985.
Slide 7-10Unit 7: Treatment of TB
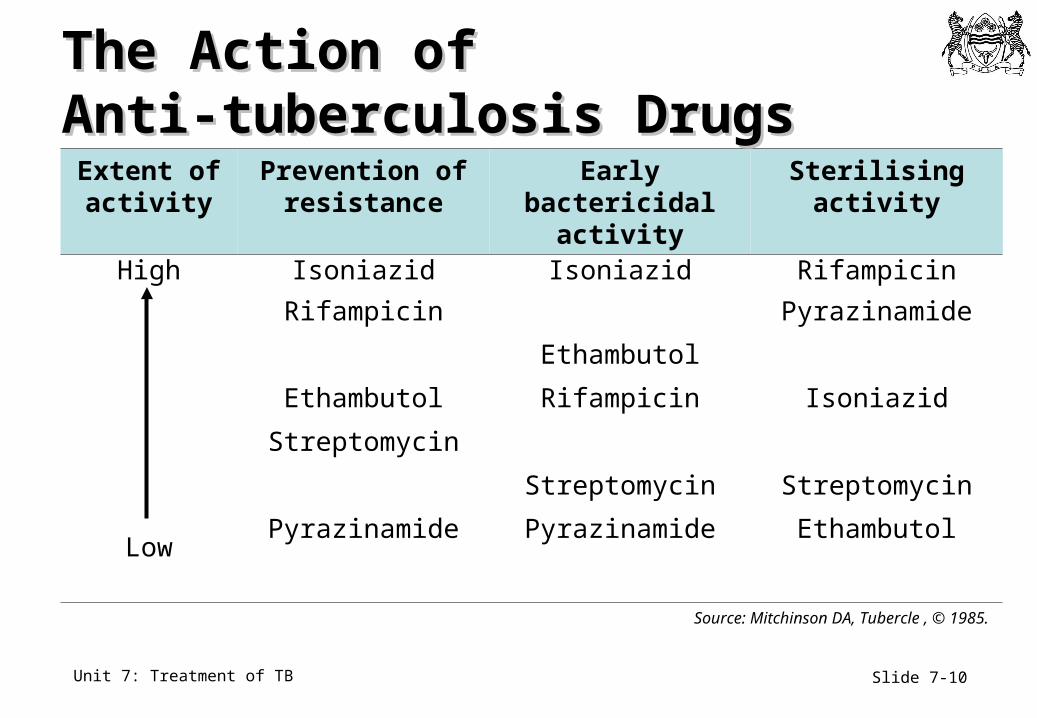
Extent of activity
Prevention of resistance
Early bactericidal activity
Sterilising activity
High Isoniazid Isoniazid Rifampicin
Low
Rifampicin Pyrazinamide
Ethambutol
Ethambutol Rifampicin Isoniazid
Streptomycin
Streptomycin Streptomycin
Pyrazinamide Pyrazinamide Ethambutol
Source: Mitchinson DA, Tubercle , © 1985.
The Action of The Action of Anti-tuberculosis DrugsAnti-tuberculosis Drugs
Slide 7-11Unit 7: Treatment of TB
Modern TB Chemotherapy (1)Modern TB Chemotherapy (1)
• INH – kills rapidly growing organisms (early bactericidal activity)
• INH and RMP protect each other from development of resistance
• Rifampicin and pyrazinamide kill slowly growing organisms• Sterilising activity
Source: Combs D et al., Ann Intern Med., 1990.
Slide 7-12Unit 7: Treatment of TB
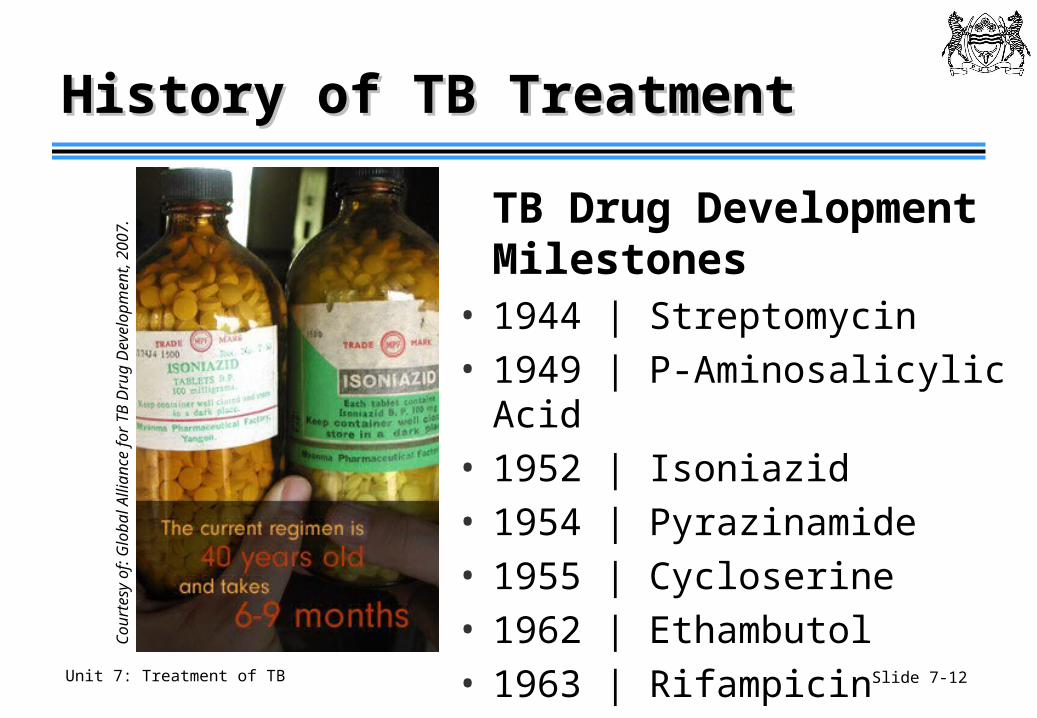
History of TB Treatment History of TB Treatment
TB Drug Development Milestones
• 1944 | Streptomycin• 1949 | P-Aminosalicylic Acid• 1952 | Isoniazid• 1954 | Pyrazinamide• 1955 | Cycloserine• 1962 | Ethambutol• 1963 | RifampicinC
ou
rte
sy o
f: G
lob
al A
llia
nce
fo
r T
B D
rug
De
velo
pm
en
t, 2
00
7.
Slide 7-13Unit 7: Treatment of TB
History of TB History of TB Treatment in BotswanaTreatment in Botswana
• 1975-1986: 2STH/16TH
• 1986-1993: 2SHRZ/4HR
• 1993-present: 2HRZE/4HR
• S= streptomycin
• T= thiacetazone
• H= isoniazid
• R= rifampicin
• Z= pyrazinamide
• E=ethambutol
Slide 7-14Unit 7: Treatment of TB
Modern TB Chemotherapy (2)Modern TB Chemotherapy (2)
British Thoracic Society
No. 2; 1982• Initial 2 months
• HRZE
• Continuation 4 months• HR
• 97% cure rate
US Public Health Service
No. 21; 1990• Initial 2 months
• HRZ+/-E
• Continuation 4 months• HR
• 97% cure rate
Source: Iseman, MD. A Clinician’s Guide to Tuberculosis. 2000.British Thoracic Society, 1982.
Slide 7-15Unit 7: Treatment of TB
Category I RegimenCategory I Regimen
Initial Phase• Normally two months• 4 drugs: 2HRZE
• Isoniazid (H)• Rifampicin (R)• Pyrazinamide (Z)• Ethambutol (E)
• Daily and observed
Continuation Phase• Normally four months• 2 drugs: 4HR
• Isoniazid (H)• Rifampicin (R)
• Daily and observed
Slide 7-16Unit 7: Treatment of TB
Category I Regimen EligibilityCategory I Regimen Eligibility
• New Patients• Sputum smear + PTB• Sputum smear – PTB• Extra-pulmonary TB
• TB Meningitis: streptomycin substitutes for ethambutol
• Streptomycin should not be used if pregnant
Slide 7-17Unit 7: Treatment of TB
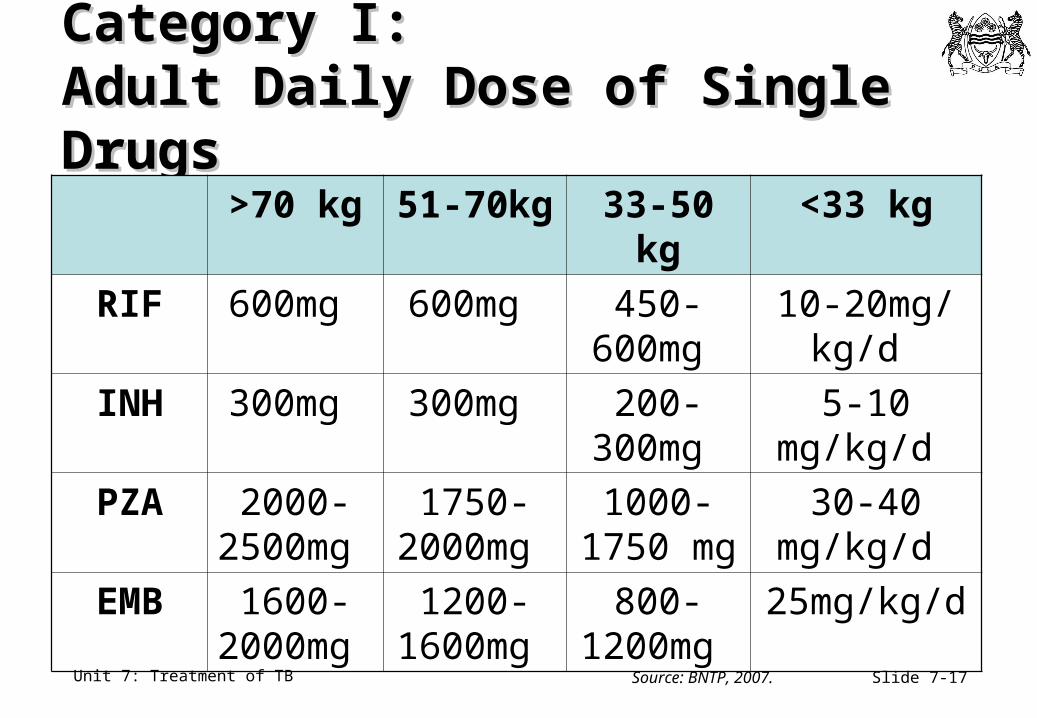
Category I:Category I:Adult Daily Dose of Single DrugsAdult Daily Dose of Single Drugs
>70 kg 51-70kg 33-50 kg <33 kg
RIF 600mg 600mg 450-600mg
10-20mg/kg/d
INH 300mg 300mg 200-300mg
5-10 mg/kg/d
PZA 2000-2500mg
1750-2000mg
1000-1750 mg
30-40 mg/kg/d
EMB 1600-2000mg
1200-1600mg
800-1200mg
25mg/kg/d
Source: BNTP, 2007.
Slide 7-18Unit 7: Treatment of TB
FDC: Fixed DoseFDC: Fixed DoseCombination Tabs (1)Combination Tabs (1)
Courtesy of: STOP TB Partnership
Slide 7-19Unit 7: Treatment of TB
FDC: Fixed Dose FDC: Fixed Dose Combination Tabs (2)Combination Tabs (2)
• Fixed Dose Combination pills include two, three or even four drugs in one pill
• Advantages of FDCs • Reduces the number of pills patients must take• Minimises errors in dosing• Simplifies distribution of pills to patients• Simplifies monitoring adherence
Slide 7-20Unit 7: Treatment of TB
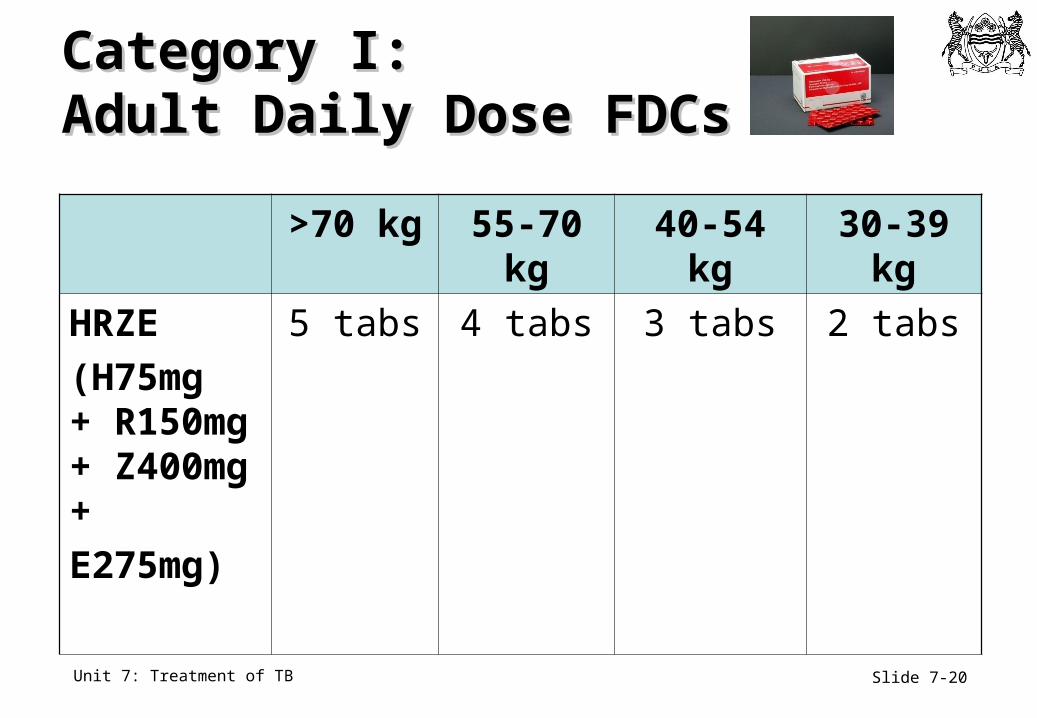
Category I:Category I:Adult Daily Dose FDCsAdult Daily Dose FDCs
>70 kg 55-70 kg 40-54 kg 30-39 kg
HRZE
(H75mg + R150mg + Z400mg +
E275mg)
5 tabs 4 tabs 3 tabs 2 tabs
Slide 7-21Unit 7: Treatment of TB
Treatment Follow-upTreatment Follow-up
• Patients should be assessed monthly during treatment (more frequently, if needed) • Symptoms: cough, weight loss, fever, adverse
effects• Adherence: review the treatment card• Adverse events: enquire about any side effects• Weight measurement: adjust dosages to account
for any weight change• Sputum smear: obtain at 2 and at 5-6 months
Slide 7-22Unit 7: Treatment of TB
The Role of CXR in Follow-UpThe Role of CXR in Follow-Up
• There is no need for routine CXR in follow-up of PTB patients• CXR can be useful for the follow-up of some EPTB
patients (e.g., pleural effusion)
• Treatment decisions in PTB (switching to continuation phase, ending treatment) should generally be based upon sputum smear exams at stated intervals and clinical monitoring
Slide 7-23Unit 7: Treatment of TB
Monitoring Treatment ResponseMonitoring Treatment Response
• Important to tuberculosis control• Allows assessment of
• Infectivity of a patient• Response to treatment• Outcome of treatment
• Assessed through clinical, laboratory and radiological methods
• Relies primarily on sputum conversion • X-rays are not part of routine follow-up of TB cases in
Botswana
Slide 7-24Unit 7: Treatment of TB
Category I: Category I: End of 2 Months of TreatmentEnd of 2 Months of Treatment
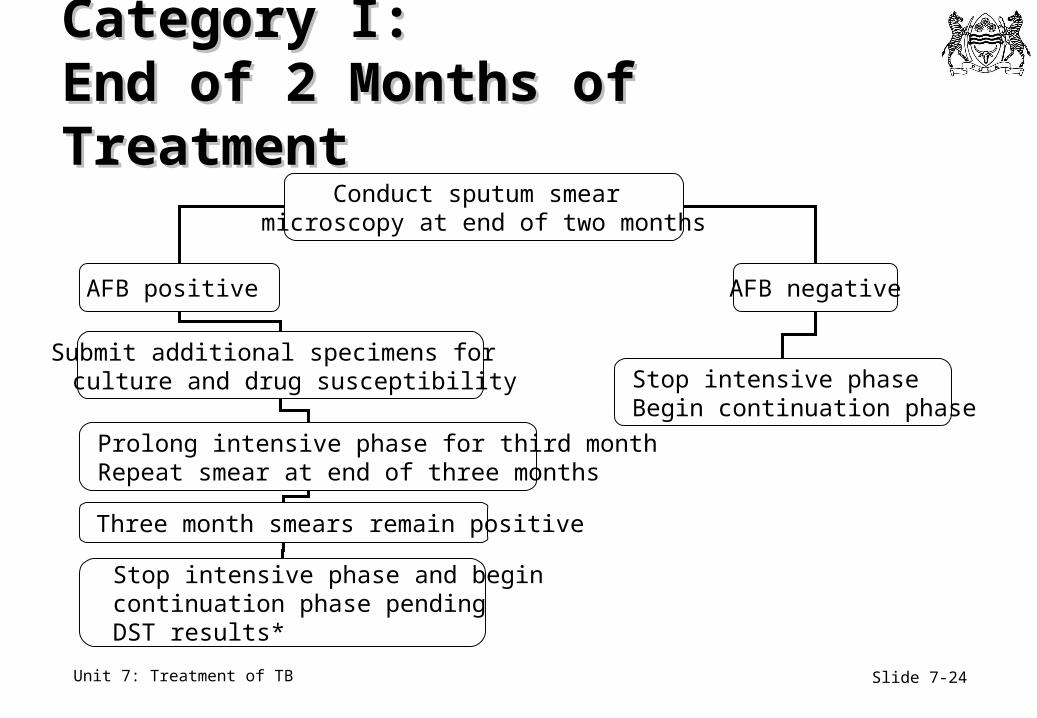
Conduct sputum smear microscopy at end of two months
AFB positive AFB negative
Stop intensive phase Begin continuation phase
Three month smears remain positive
Stop intensive phase and begin continuation phase pending DST results*
Prolong intensive phase for third month Repeat smear at end of three months
Submit additional specimens for culture and drug susceptibility
Slide 7-25Unit 7: Treatment of TB
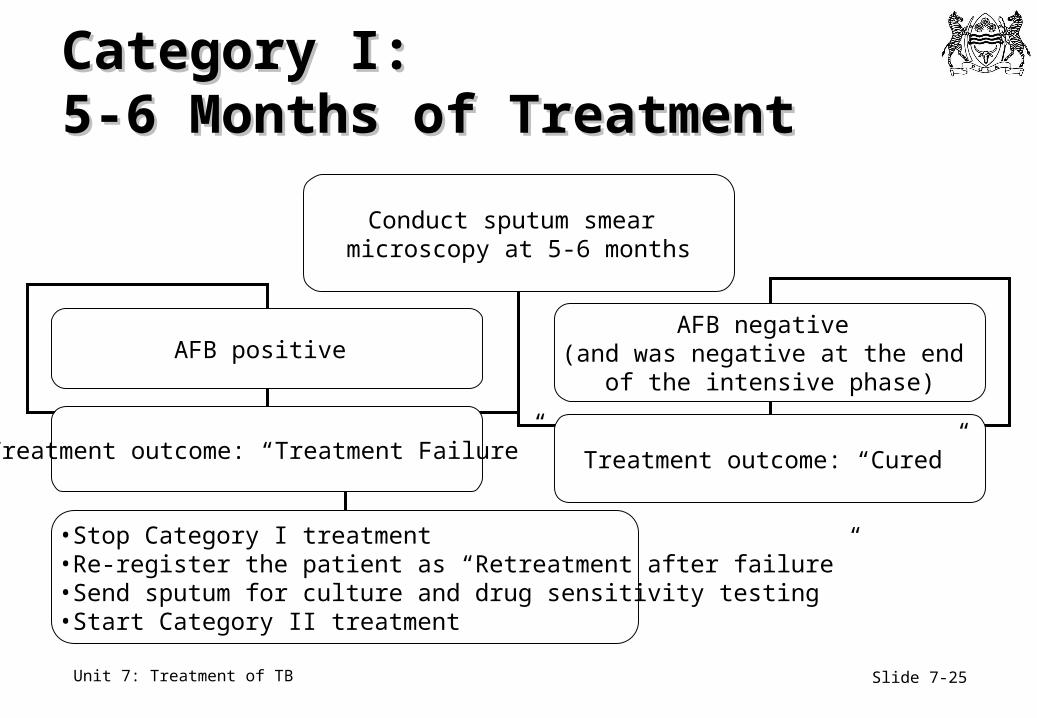
Category I: Category I: 5-6 Months of Treatment5-6 Months of Treatment
Conduct sputum smear microscopy at 5-6 months
AFB positive AFB negative
(and was negative at the end of the intensive phase)
Treatment outcome: “Cured”
•Stop Category I treatment•Re-register the patient as “Retreatment after failure”•Send sputum for culture and drug sensitivity testing•Start Category II treatment
Treatment outcome: “Treatment Failure”
Slide 7-26Unit 7: Treatment of TB
Introduction to Introduction to Category II RegimenCategory II Regimen
• Adds a fifth drug, streptomycin, to the other first-line medications
• Prolongs treatment to 8 months in total
• Initiated and managed by the same clinicians and nurses as category I
• Requires two months of injections (given daily)
Slide 7-27Unit 7: Treatment of TB
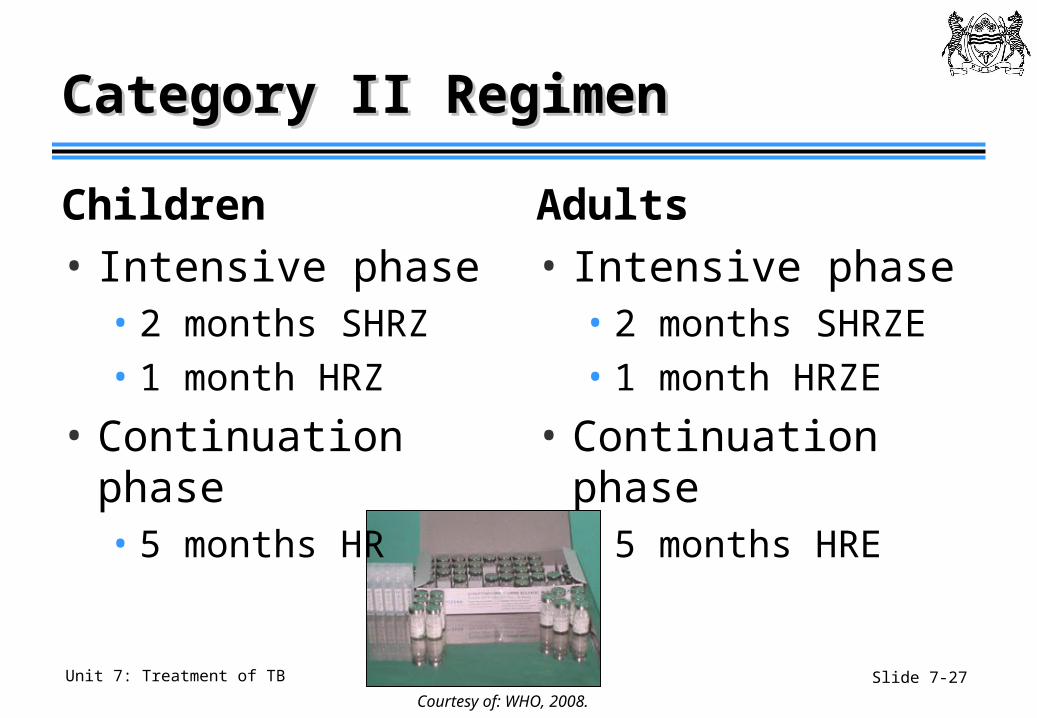
Category II RegimenCategory II Regimen
Adults
• Intensive phase • 2 months SHRZE• 1 month HRZE
• Continuation phase • 5 months HRE
Courtesy of: WHO, 2008.
Children
• Intensive phase• 2 months SHRZ• 1 month HRZ
• Continuation phase• 5 months HR
Slide 7-28Unit 7: Treatment of TB
Category II Regimen EligibilityCategory II Regimen Eligibility
For smear-positive or culture-positive retreatment cases after• Relapse
• Default
• Treatment failure
Slide 7-29Unit 7: Treatment of TB
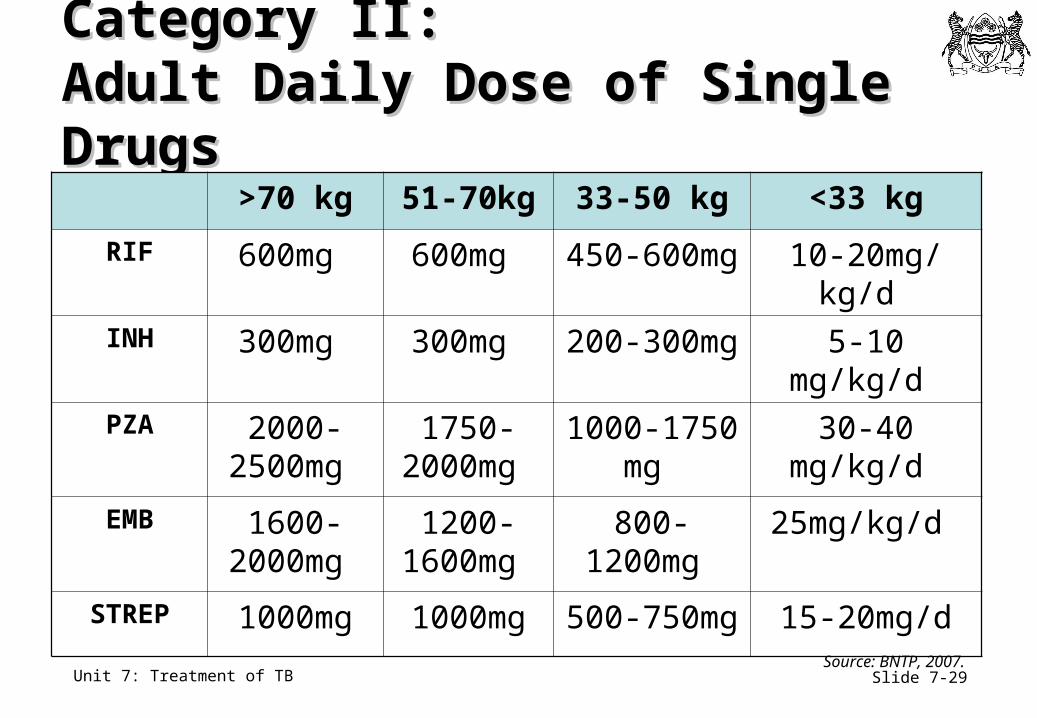
Category II:Category II:Adult Daily Dose of Single DrugsAdult Daily Dose of Single Drugs
>70 kg 51-70kg 33-50 kg <33 kg
RIF 600mg 600mg 450-600mg 10-20mg/kg/d
INH 300mg 300mg 200-300mg 5-10 mg/kg/d
PZA 2000-2500mg
1750-2000mg
1000-1750 mg
30-40 mg/kg/d
EMB 1600-2000mg
1200-1600mg
800-1200mg
25mg/kg/d
STREP 1000mg 1000mg 500-750mg 15-20mg/d
Source: BNTP, 2007.
Slide 7-30Unit 7: Treatment of TB
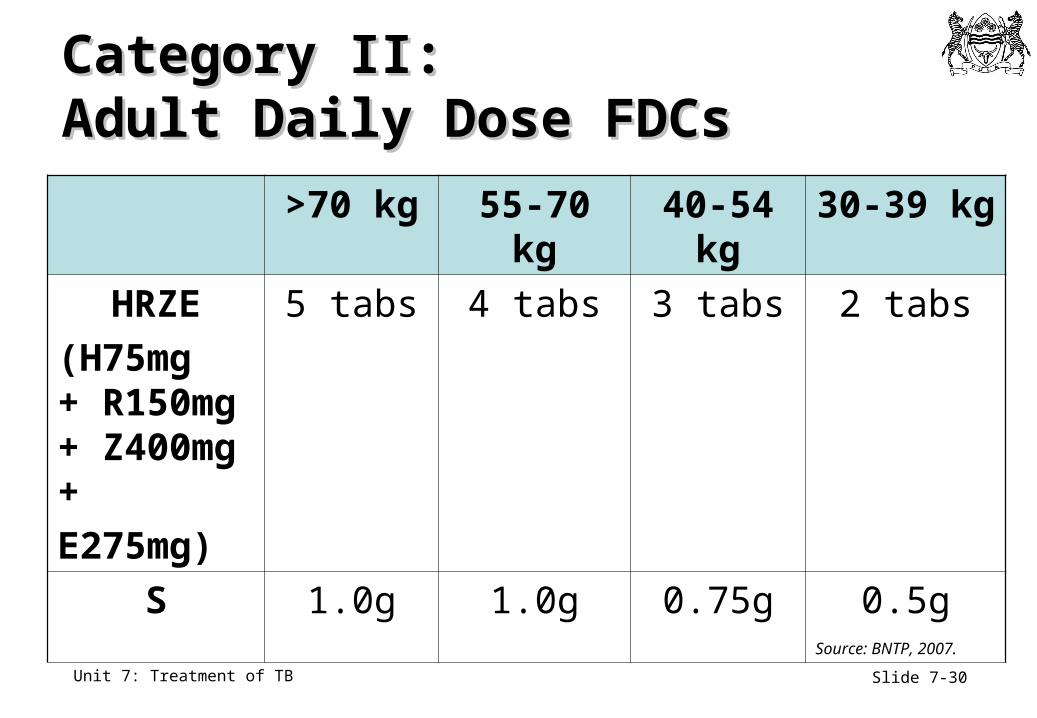
Category II:Category II:Adult Daily Dose FDCsAdult Daily Dose FDCs
>70 kg 55-70 kg 40-54 kg 30-39 kg
HRZE
(H75mg + R150mg + Z400mg +
E275mg)
5 tabs 4 tabs 3 tabs 2 tabs
S 1.0g 1.0g 0.75g 0.5g
Source: BNTP, 2007.
Slide 7-31Unit 7: Treatment of TB
Category II Regimen: PregnancyCategory II Regimen: Pregnancy
• Streptomycin should be avoided in pregnancy if possible• Due to possible foetal ear damage and
nephrotoxicity
• Women of childbearing age should have a pregnancy test prior to starting category II
• If not pregnant, advise contraception
Slide 7-32Unit 7: Treatment of TB
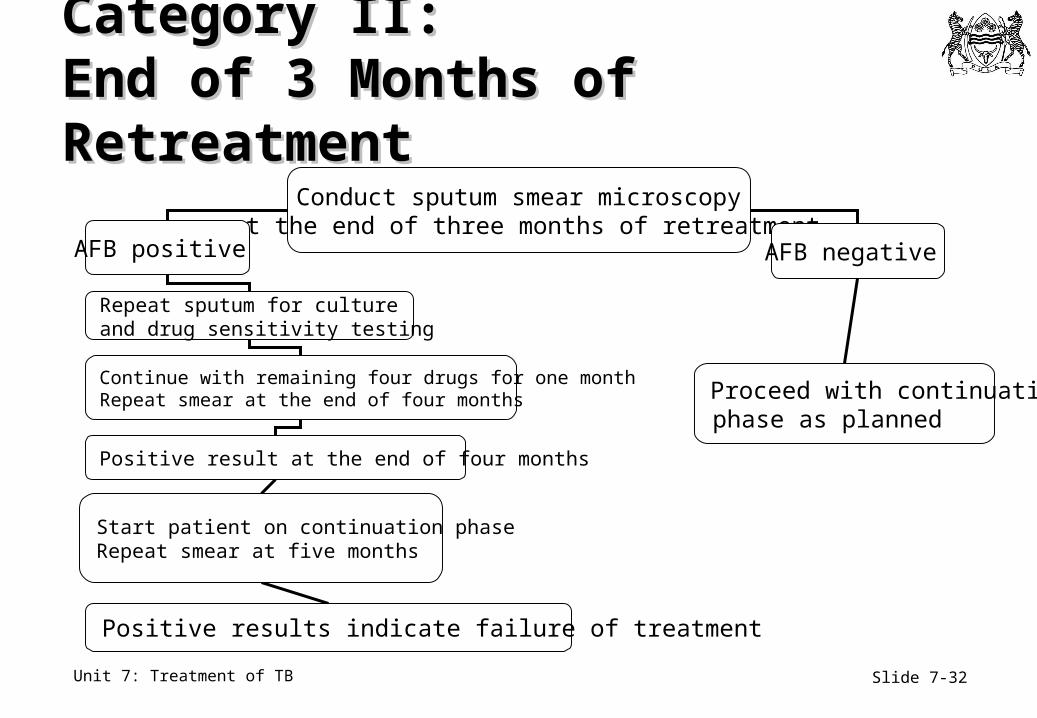
Category II: Category II: End of 3 Months of RetreatmentEnd of 3 Months of Retreatment
Conduct sputum smear microscopy at the end of three months of retreatment
AFB positive AFB negative
Proceed with continuation phase as planned
Positive result at the end of four months
Continue with remaining four drugs for one month Repeat smear at the end of four months
Start patient on continuation phase Repeat smear at five months
Positive results indicate failure of treatment
Repeat sputum for culture and drug sensitivity testing
Slide 7-33Unit 7: Treatment of TB
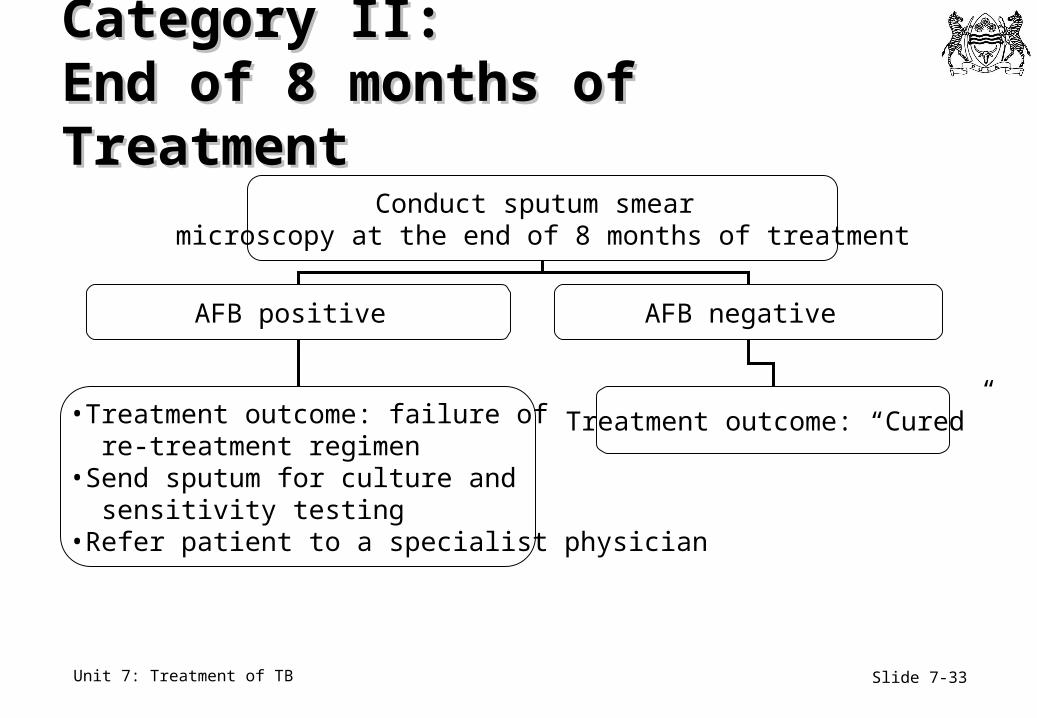
Category II: Category II: End of 8 months of TreatmentEnd of 8 months of Treatment
Conduct sputum smear microscopy at the end of 8 months of treatment
AFB positive AFB negative
Treatment outcome: “Cured”•Treatment outcome: failure of re-treatment regimen•Send sputum for culture and sensitivity testing•Refer patient to a specialist physician
Slide 7-34Unit 7: Treatment of TB
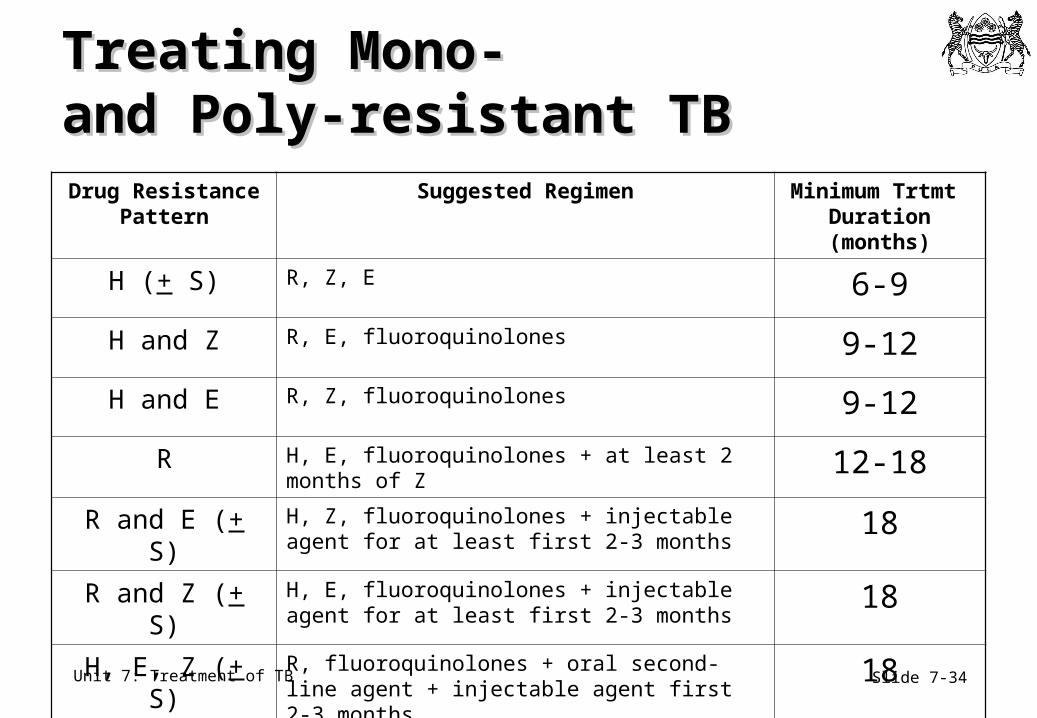
Treating Mono- Treating Mono- and Poly-resistant TBand Poly-resistant TB
Drug Resistance Pattern
Suggested Regimen Minimum Trtmt Duration (months)
H (+ S) R, Z, E 6-9
H and Z R, E, fluoroquinolones 9-12
H and E R, Z, fluoroquinolones 9-12
R H, E, fluoroquinolones + at least 2 months of Z 12-18
R and E (+ S) H, Z, fluoroquinolones + injectable agent for at least first 2-3 months
18
R and Z (+ S) H, E, fluoroquinolones + injectable agent for at least first 2-3 months
18
H, E, Z (+ S) R, fluoroquinolones + oral second-line agent + injectable agent first 2-3 months
18
Slide 7-35Unit 7: Treatment of TB
Category III RegimenCategory III Regimen
• This is the recommended regimen for most children with TB in Botswana
• Intensive phase• 2 months HRZ
• Continuation phase• 4 months HR
Slide 7-36Unit 7: Treatment of TB
Category IV Category IV Regimen and EligibilityRegimen and Eligibility• Specially-designed standardised or
individualised regimens are recommended
• For all patients who remain or become smear positive after completing a fully supervised retreatment regimen
• For chronic and MDR-TB cases
• Second line TB drugs include amikacin, ethionamide, ciprofloxacin and first line drugs with continued activity against M. tuberculosis
Slide 7-37Unit 7: Treatment of TB
Treatment of Severe Forms of TBTreatment of Severe Forms of TB
• Prolong the continuation phase to 6 months for the following sites of disease:• Tuberculous meningitis*• TB percardiditis• Disseminated TB• Spinal disease with neurologic complications
*For tuberculous meningitis: substitute streptomycin for ethambutol during the initial phase of treatment
Source: Basquoz N, 2007.
Slide 7-38Unit 7: Treatment of TB
Treatment of Severe TB: Treatment of Severe TB: Adjuvant CorticosteroidAdjuvant Corticosteroid• Indications:
• TB meningitis, TB pericarditis, Massive lymphadenopathy with airway obstruction
• Recommended dose: usually prednisolone • TB meningitis: 2mg/kg/day up to 60mg/day for 4 weeks,
then taper over several weeks• TB pericarditis: 2mg/kg/day up to 60mg/day for 4 weeks,
then 30mg/day for 4 weeks, then taper over several weeks
• In patients that cannot tolerate oral medication, IV dexamethasone is recommended
Slide 7-39Unit 7: Treatment of TB
Side EffectsSide Effects
• Each TB medication has potential side effects and drug interactions
• Patients should be educated on particulars of potential side effects Courtesy of: Virot P, Lung Health Image Library, 2004.
Slide 7-40Unit 7: Treatment of TB
Clinical Monitoring for ToxicityClinical Monitoring for Toxicity
Symptoms• Nausea• Vomiting• Right upper quadrant
pain• Burning in feet• Change in vision• Joint pain• Dizziness
Signs• Fever• Rash• Jaundice• Pallor
• Other signs of anaemia
• Confusion, psychosis• Seizures
Slide 7-41Unit 7: Treatment of TB
Paradoxical ReactionsParadoxical Reactions
• Apparent clinical worsening of TB on appropriate therapy• Caused by an immunologic reaction to TB as patient improves• Common with TB adenitis
• Also occurs with brain tuberculomas and other manifestations
• Monitor for bacteriologic relapse/failure• Continue TB treatment• Steroid therapy may be helpful for severe paradoxical
reaction, after excluding TB treatment failure and other etiologies of apparent clinical worsening
Slide 7-42Unit 7: Treatment of TB
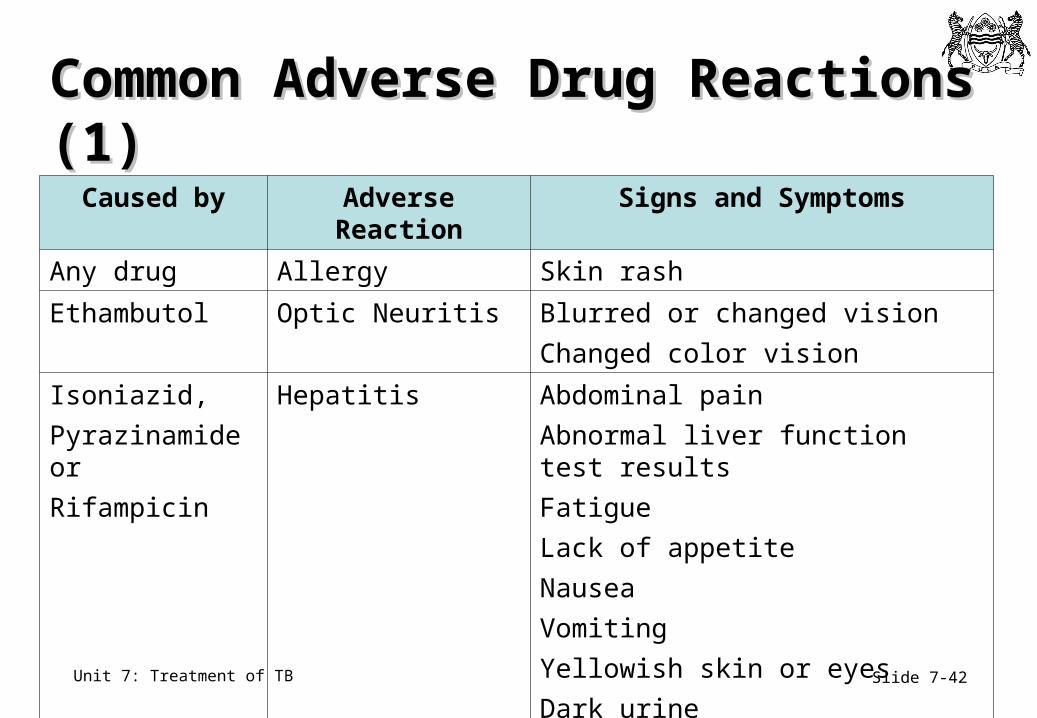
Common Adverse Drug Reactions (1)Common Adverse Drug Reactions (1)
Caused by Adverse Reaction Signs and Symptoms
Any drug Allergy Skin rash
Ethambutol Optic Neuritis Blurred or changed vision
Changed color vision
Isoniazid,
Pyrazinamide or
Rifampicin
Hepatitis Abdominal pain
Abnormal liver function test results
Fatigue
Lack of appetite
Nausea
Vomiting
Yellowish skin or eyes
Dark urine
Slide 7-43Unit 7: Treatment of TB
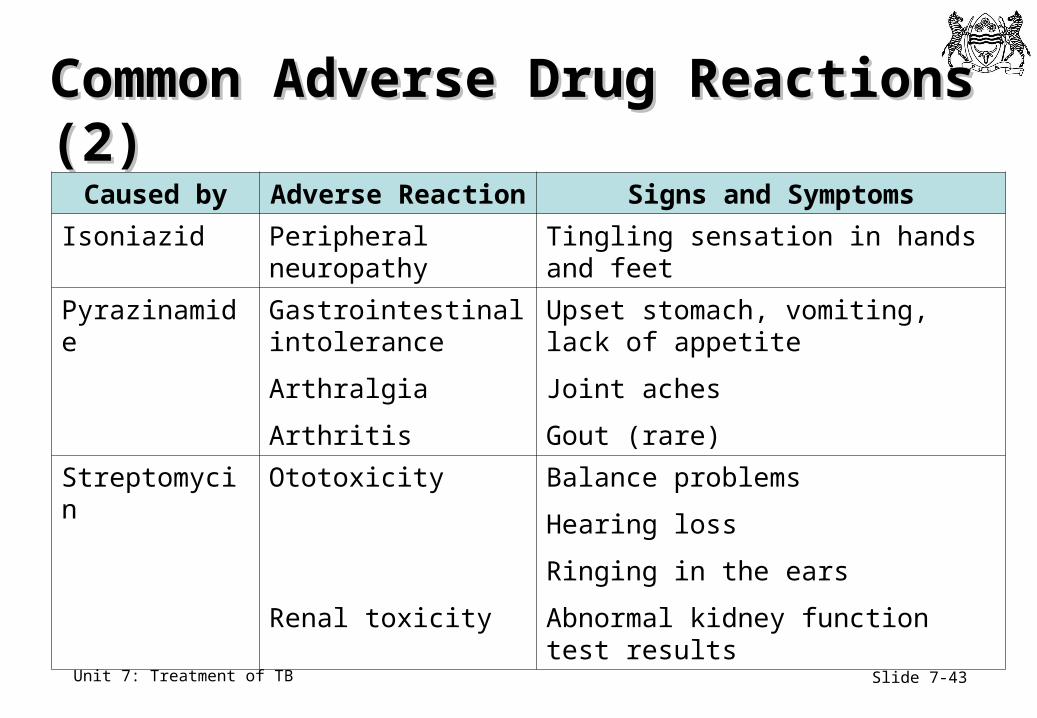
Common Adverse Drug Reactions (2)Common Adverse Drug Reactions (2)
Caused by Adverse Reaction Signs and Symptoms
Isoniazid Peripheral neuropathy
Tingling sensation in hands and feet
Pyrazinamide Gastrointestinalintolerance
Arthralgia
Arthritis
Upset stomach, vomiting, lack of appetite
Joint aches
Gout (rare)
Streptomycin Ototoxicity
Renal toxicity
Balance problems
Hearing loss
Ringing in the ears
Abnormal kidney function test results
Slide 7-44Unit 7: Treatment of TB
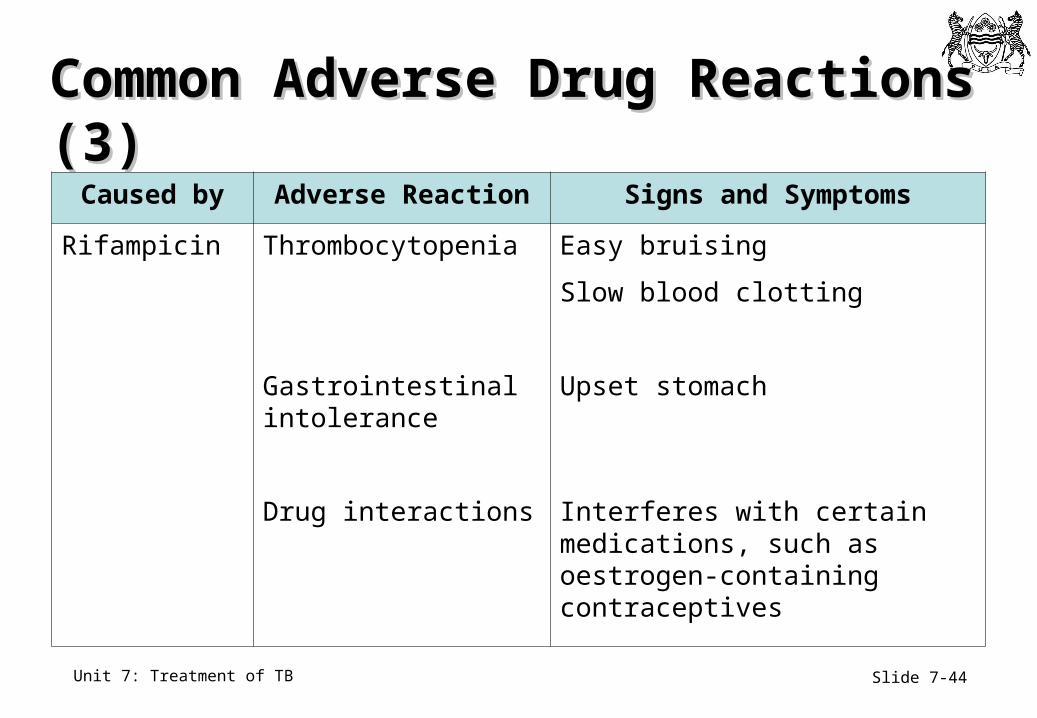
Common Adverse Drug Reactions (3)Common Adverse Drug Reactions (3)
Caused by Adverse Reaction Signs and Symptoms
Rifampicin Thrombocytopenia
Gastrointestinal intolerance
Drug interactions
Easy bruising
Slow blood clotting
Upset stomach
Interferes with certain medications, such as oestrogen-containing contraceptives
Slide 7-45Unit 7: Treatment of TB
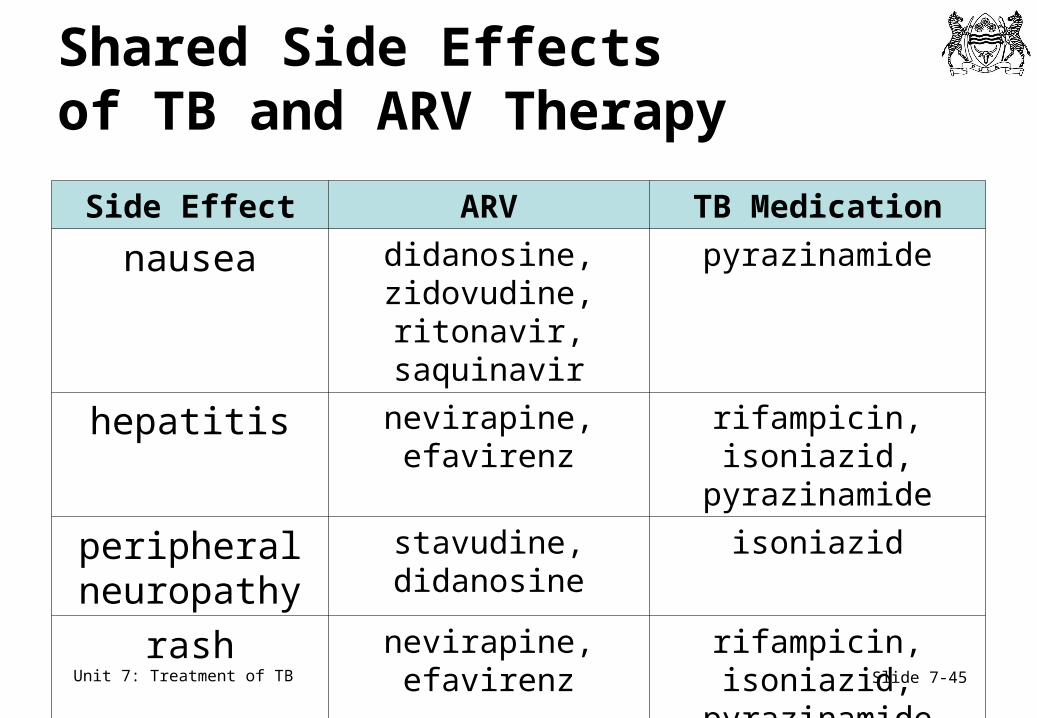
Shared Side Effects of TB and ARV Therapy
Side Effect ARV TB Medication
nausea didanosine, zidovudine, ritonavir,
saquinavir
pyrazinamide
hepatitis nevirapine, efavirenz rifampicin, isoniazid, pyrazinamide
peripheral neuropathy
stavudine, didanosine
isoniazid
rash nevirapine, efavirenz rifampicin, isoniazid, pyrazinamide
Slide 7-46Unit 7: Treatment of TB
Managing Minor Side EffectsManaging Minor Side Effects
• Loss of appetite, nausea, abdominal pain• Provide anti-emetics such as promethazine or
metoclopromide• Check liver function tests or ALT, especially if symptoms
persist• Joint pains
• Aspirin or Non-Steroidal Anti-Inflammatory Drugs (NSAID)• Peripheral Neuropathy
• Give pyridoxine 100-200 mg daily until symptoms disappear and then decrease to preventive dose
• Orange/red urine• Reassurance
Source: WHO, 2004.
Slide 7-47Unit 7: Treatment of TB
Managing Major Side EffectsManaging Major Side Effects
• Severe rash• Stop all drugs; see Unit 8
• Jaundice, vomiting and abdominal pain, confusion• Stop all drugs; see Unit 8
• Visual changes• Stop ethambutol and revise treatment
• Generalised reaction, shock, purpura• Stop all drugs until stable
Slide 7-48Unit 7: Treatment of TB
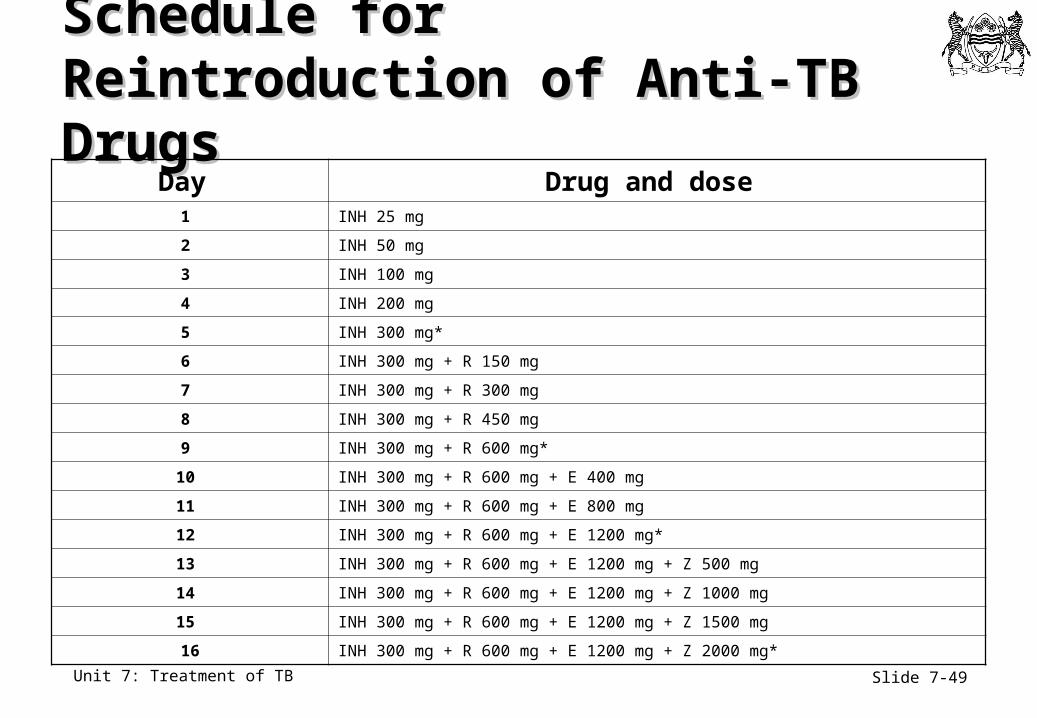
Serial Drug ChallengeSerial Drug Challenge
• When symptoms of a major side effect have subsided, wait two weeks
• Reintroduce TB medicines as described in Table 6.7 in the Botswana National Tuberculosis Programme Manual
Slide 7-49Unit 7: Treatment of TB
Schedule for Schedule for Reintroduction of Anti-TB DrugsReintroduction of Anti-TB Drugs
Day Drug and dose 1 INH 25 mg
2 INH 50 mg
3 INH 100 mg
4 INH 200 mg
5 INH 300 mg*
6 INH 300 mg + R 150 mg
7 INH 300 mg + R 300 mg
8 INH 300 mg + R 450 mg
9 INH 300 mg + R 600 mg*
10 INH 300 mg + R 600 mg + E 400 mg
11 INH 300 mg + R 600 mg + E 800 mg
12 INH 300 mg + R 600 mg + E 1200 mg*
13 INH 300 mg + R 600 mg + E 1200 mg + Z 500 mg
14 INH 300 mg + R 600 mg + E 1200 mg + Z 1000 mg
15 INH 300 mg + R 600 mg + E 1200 mg + Z 1500 mg
16 INH 300 mg + R 600 mg + E 1200 mg + Z 2000 mg*
Slide 7-50Unit 7: Treatment of TB
Drug Interactions Drug Interactions
• With many patients on ARVs also taking ATT, quite common for drug levels to be altered to some degree
• Antituberculosis drugs sometimes change concentrations of other drugs
• Rifampicin can decrease serum concentrations of many drugs (e.g., most of the HIV-1 protease inhibitors) to subtherapeutic levels
• Isoniazid increases concentrations of some drugs (e.g., phenytoin) to toxic levels
Slide 7-51Unit 7: Treatment of TB
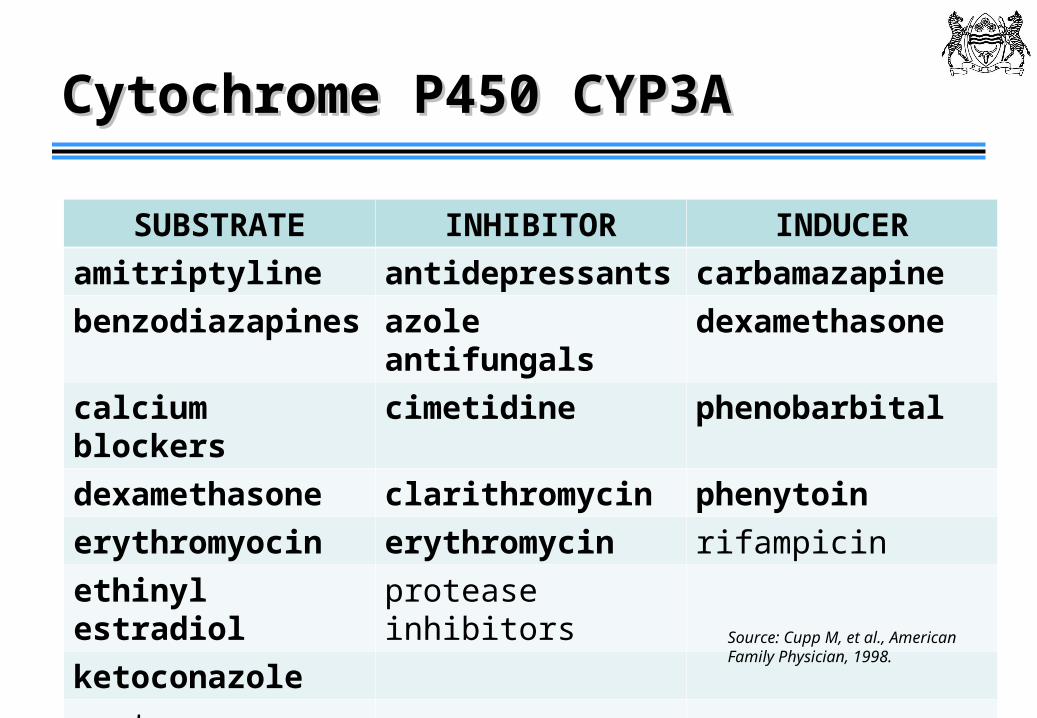
Cytochrome P450 CYP3ACytochrome P450 CYP3A
SUBSTRATE INHIBITOR INDUCER
amitriptyline antidepressants carbamazapine
benzodiazapines azole antifungals dexamethasone
calcium blockers cimetidine phenobarbital
dexamethasone clarithromycin phenytoin
erythromyocin erythromycin rifampicin
ethinyl estradiol protease inhibitors
ketoconazole
protease inhibitorsSource: Cupp M, et al., American Family Physician, 1998.
Slide 7-52Unit 7: Treatment of TB
Treatment of MOTTTreatment of MOTT
• The most common non-tuberculous mycobacteria that cause disease in the US are• MAC, M.kansasii, M.fortuitum
• MAC is treated with clarithromycin, rifampicin, and ethambutol for 18-24 months
• M. kansasii is treated for 1 year after culture conversion with rifampicin, ethambutol and INH
Source: American Thoracic Society, 2007.
Slide 7-53Unit 7: Treatment of TB
MOTT ManagementMOTT Management
• Patients with MOTT are generally not isolated
• These bacteria are widespread in the environment and are typically not spread person-to-person
• MOTT is not MDR TB
• MOTT may be present on culture but not cause disease
Slide 7-54Unit 7: Treatment of TB
Key Points (1)Key Points (1)
• TB treatment rapidly kills growing bacteria, prevents the emergence of drug resistance, and kills persistent organisms to avoid relapse
• Treatment renders adherent and drug-sensitive patients non-infectious, usually within several days to several weeks
• Modern chemotherapy can cure 97% of persons with drug susceptible TB
Slide 7-55Unit 7: Treatment of TB
Key Points (2)Key Points (2)
• There are 4 treatment categories of anti-TB medicines
• First-line anti-TB medicines are isoniazid, rifampicin, pyrazinamide, ethambutol, and streptomycin
• TB treatment should be monitored monthly
• Side effects should be addressed as they occur
Related Documents











