Archrves o/Clmlcrrl /veuropsychology. Vol. 3, pp. 213-225. 1988 0887.6177188 13.00 + .@I Pruned I” the USA. All nghrs rescrvcd. Copyright 0 1988 Narmnal Academy of Necroprychologws Unilateral Spatial Neglect: Biases in Contralateral Search and Fine Spatial Attention Susan Egelko, Ellen Riley, Dvorah Simon, Leonard Diller, and Ora Ezrachi Rusk Institute of Rehabilitation Medicine, New York University Medical Center Contralateral search and fine spatial attentional asymmetries, two aspects of hemispatial neglect, were examined in a total of 91 right brain damaged (RBD) and 40 non-aphasic left brain damaged (LBD) stroke rehabilitation inpatients. Fine spatial attentional asymmetries within a hemispace were found in both RBD and LBD patients on the LAVA figure-match test. This finding is in contrast to Gainotti’s hypothesis that such problems in extracting contralateral visual infor- mation are uniquely characteristic of RBD patients. Furthermore, the study suggests that the gross search and fine attentional aspects of neglect are dissocia- ble and may refrect different underlying mechanisms of hemispatial neglect. Unilateral spatial neglect is generally recognized to be a complex behavioral phenomenon involving the spatial distribution of directed attention, that is, a failure to orient automatically to the side of space contralateral to the lesion. Deficiencies in exploration of space, as seen in tasks involving sac- cadic eye movement to the side contralateral to that of lesion, are observed clinically and experimentally in both right (RBD) and left brain damaged (LBD) patients. However, the frequency and magnitude of the problem are reported to be greater with RBD patients (Heilman, 1983). Gainotti, D’Erme, Monteleone, and Silveri (1986) have proposed that what is unique to the condition of RBD neglecters is an inability to extract This research was supported by designation of the Rusk Institute of Rehabilitation Medicine, New York University Medical Center, as a Rehabilitation Research and Training Center by the National Institute of Disability and Rehabilitation Research (GOO8300039). Requests for reprints should be sent to Director of Training and Dissemination, Rusk Institute of Rehabilitation Medicine, Psychology Department, New York University Medical Center, 400 East 34th Street, New York, NY 10016. 213

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

Archrves o/Clmlcrrl /veuropsychology. Vol. 3, pp. 213-225. 1988 0887.6177188 13.00 + .@I Pruned I” the USA. All nghrs rescrvcd. Copyright 0 1988 Narmnal Academy of Necroprychologws
Unilateral Spatial Neglect: Biases in Contralateral Search and Fine
Spatial Attention
Susan Egelko, Ellen Riley, Dvorah Simon, Leonard Diller, and Ora Ezrachi
Rusk Institute of Rehabilitation Medicine, New York University Medical Center
Contralateral search and fine spatial attentional asymmetries, two aspects of
hemispatial neglect, were examined in a total of 91 right brain damaged (RBD) and 40 non-aphasic left brain damaged (LBD) stroke rehabilitation inpatients. Fine spatial attentional asymmetries within a hemispace were found in both RBD and LBD patients on the LAVA figure-match test. This finding is in contrast to
Gainotti’s hypothesis that such problems in extracting contralateral visual infor- mation are uniquely characteristic of RBD patients. Furthermore, the study
suggests that the gross search and fine attentional aspects of neglect are dissocia- ble and may refrect different underlying mechanisms of hemispatial neglect.
Unilateral spatial neglect is generally recognized to be a complex behavioral phenomenon involving the spatial distribution of directed attention, that is, a failure to orient automatically to the side of space contralateral to the lesion. Deficiencies in exploration of space, as seen in tasks involving sac- cadic eye movement to the side contralateral to that of lesion, are observed clinically and experimentally in both right (RBD) and left brain damaged (LBD) patients. However, the frequency and magnitude of the problem are reported to be greater with RBD patients (Heilman, 1983).
Gainotti, D’Erme, Monteleone, and Silveri (1986) have proposed that what is unique to the condition of RBD neglecters is an inability to extract
This research was supported by designation of the Rusk Institute of Rehabilitation Medicine, New York University Medical Center, as a Rehabilitation Research and Training Center by the
National Institute of Disability and Rehabilitation Research (GOO8300039).
Requests for reprints should be sent to Director of Training and Dissemination, Rusk
Institute of Rehabilitation Medicine, Psychology Department, New York University Medical
Center, 400 East 34th Street, New York, NY 10016.
213

214 S. Egelko et al.
information from the left half of visual stimuli during single eye fixation, which is attributed to a problem of disengagement of attention. This sugges- tion is consistent with only some of the findings based on Posner’s reaction time paradigm (e.g., Morrow & Ratcliff, 1987), in which disengagement of attention from the ipsilateral field in order to attend to the contralateral field has been found to be impaired for RBD, but not LBD, patients. Other studies (e.g., Posner, Walker, Friedrich, & Rafal, i984), have implicated a critical role to the parietal lobe, in both right and left hemispheres, in shifts or disengagement of attention. However, it is still unclear whether dis- engagement of attention may be the underlying phenomenon in difficulties of extracting information from one side of a figure. Furthermore, regions of the brain other than the parietal lobes have been implicated in disorders of spatial attention (Stuss & Benson, 1984). For example, Luria (1973) has deinert and disorganized focusing of attention may contribute to deficient contralateral search behavior as well as disengagement from single points of fixation.
The use of a “bias” score, as developed by Costa, Vaughan, Horwitz, and Ritter (1969) on the original Raven’s Coloured Progressive Matrices (RCPM) test (1962) has been used widely to identify grossly neglecting patients. Specifically, a “position preference” score has been determined by computing for each subject the difference between the number of alterna- tives chosen on the side of the page ipsilateral to the damaged hemisphere and the number chosen on the contralateral side of the page. Position pref- erence scores based on the 36-item test have been found to differentiate RBD and LBD patients at the -005 level in one study (Gainotti, Caltagirone, & Miceli, 1977).
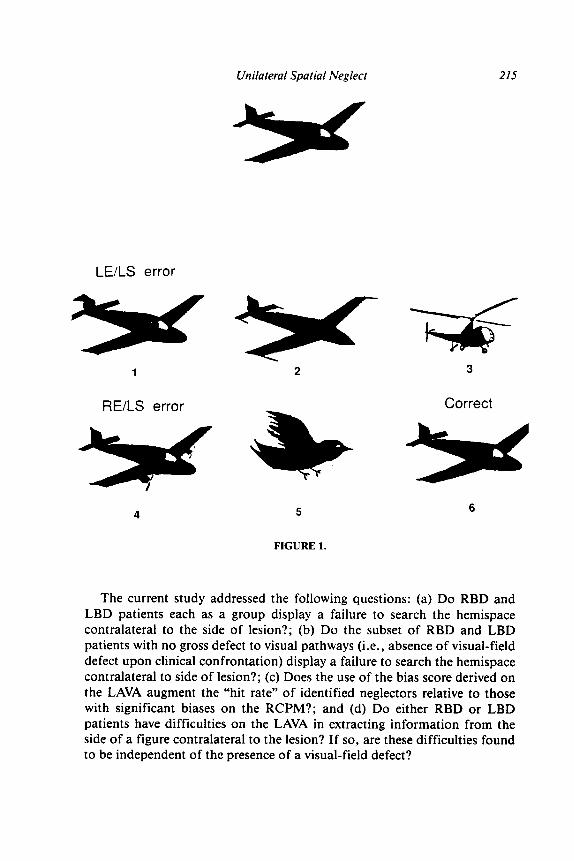
The more recently developed Lateral Asymmetry in Visual Attention (LAVA) Test (Piasetsky, 1981) poses a cognitively simple challenge relative to that of the RCPM. This figure-match test was designed specifically to present compelling, competing visual choices (see Figures 1 and 2) simulta- neously to the right and left of patient’s midline, thereby ferreting out mildly inattentive “covert” neglecters. An attractive feature of this test is that atten- tional preference may be classified not only by which side of the page is preferred but furthermore whether errors are committed for left or right edge details within either the left or right hemispace. This feature of the test thereby permits inquiry into the issues of bias of fine spatial attention. According to Gainotti’s proposal, only RBD patients would be expected to display a fine spatial attentional bias. Thus, the foils selected by RBD patients would be expected to be characterized by a preponderance of left edge to right edge detail errors. By contrast, the foils selected by LBD patients would not be expected to be characterized by a preponderance of right edge detail errors.
Unilateral Spatial Neglect 215
LE/LS error
RE/LS error
w
4 5
FIGURE 1.
Correct
6
The current study addressed the following questions: (a) Do RBD and LBD patients each as a group display a failure to search the hemispace contralateral to the side of lesion ?; (b) Do the subset of RBD and LBD patients with no gross defect to visual pathways (i.e., absence of visual-field defect upon clinical confrontation) display a failure to search the hemispace contralateral to side of lesion ?; (c) Does the use of the bias score derived on the LAVA augment the “hit rate” of identified neglecters relative to those with significant biases on the RCPM?; and (d) Do either RBD or LBD patients have difficulties on the LAVA in extracting information from the side of a figure contralateral to the lesion? If so, are these difficulties found to be independent of the presence of a visual-field defect?

216 S. Egelko et al.
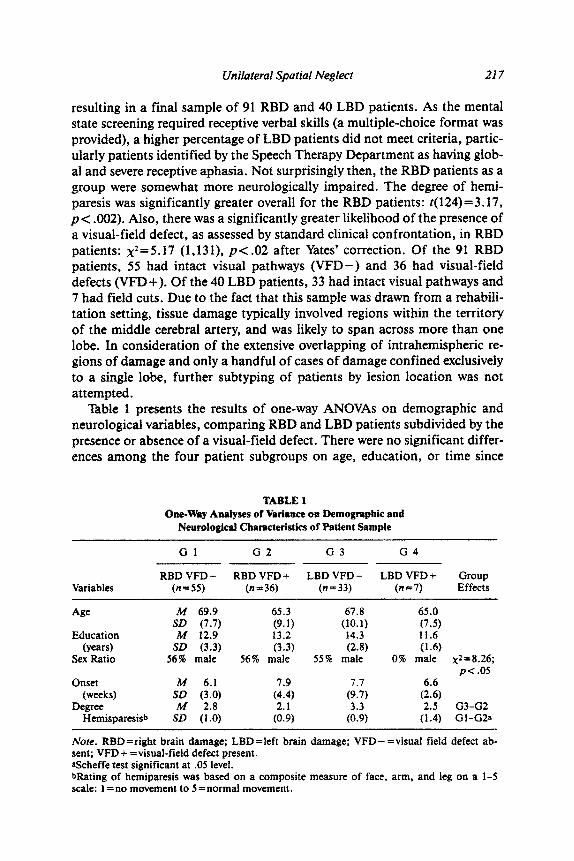
Correct
2
*
5
’ LEiRS error
RElRS error
6
FIGURE 2.
METHODS
Subjects
A total of 131 RBD and 67 LBD consecutively admitted unilateral stroke rehabilitation inpatients were assessed. Criteria for inclusion in the study included: (a) right-handedness for writing; (b) absence of prior CVA (al- though histories of TIA’s were common); (c) at least four weeks post onset of stroke at the time of testing; (d) lateralized documentation of lesion by neuroradiological exam; (e) no other CNS disorder nor psychiatric disturb- ance as determined by medical chart review; and (f) not demented as deter- mined by a score of 20 or greater on a modified Mini-Mental State Exam (MMSE) (Folstein, Folstein, & McHugh, 1975). A total of 27 RBD and 40 LBD patients were ruled out on the basis of the Mini-Mental State Exam,
Unilateral Spatial Neglect 217
resulting in a final sample of 91 RBD and 40 LBD patients. As the mental state screening required receptive verbal skills (a multiple-choice format was provided), a higher percentage of LBD patients did not meet criteria, partic- ularly patients identified by the Speech Therapy Department as having glob- al and severe receptive aphasia. Not surprisingly then, the RBD patients as a group were somewhat more neurologically impaired. The degree of hemi- paresis was significantly greater overall for the RBD patients: t( 124)=3.17, p< .002). Also, there was a significantly greater likelihood of the presence of a visual-field defect, as assessed by standard clinical confrontation, in RBD patients: x*=5.17 (1,131). p< .02 after Yates’ correction. Of the 91 RBD patients, 55 had intact visual pathways (VFD-) and 36 had visual-field defects (VFD-t). Of the 40 LBD patients, 33 had intact visual pathways and 7 had field cuts. Due to the fact that this sample was drawn from a rehabili- tation setting, tissue damage typically involved regions within the territory of the middle cerebral artery, and was likely to span across more than one lobe. In consideration of the extensive overlapping of intrahemispheric re- gions of damage and only a handful of cases of damage confined exclusively to a single lobe, further subtyping of patients by lesion location was not attempted.
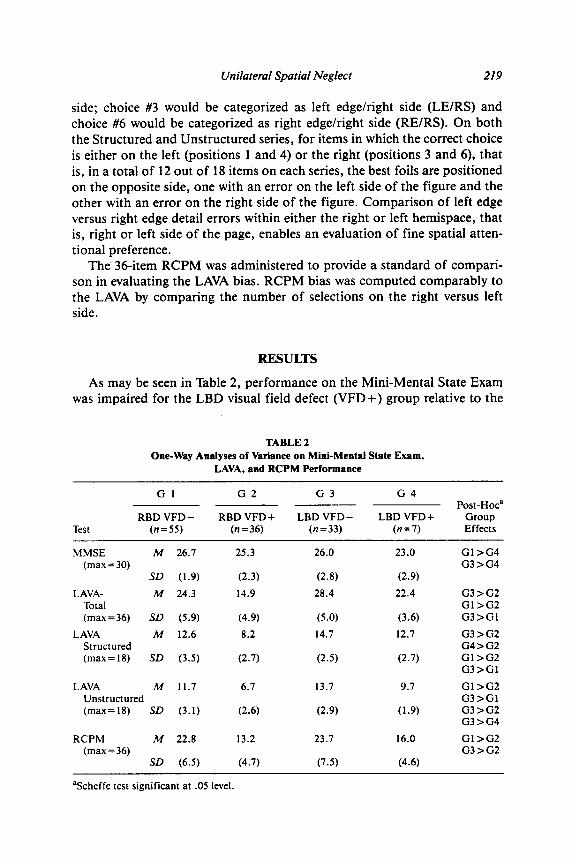
Table 1 presents the results of one-way ANOVAs on demographic and neurological variables, comparing RBD and LBD patients subdivided by the presence or absence of a visual-field defect. There were no significant differ- ences among the four patient subgroups on age, education, or time since
TABLE 1 One-Way Adyses of Variance on ~mog~pbi~ and
Neurological Chsraeteristics of Patient Sample
Gl G2 G3 G4
Variables RBD VFD - RBD VFD + LBD VFD - LBD VFD+ Group
(n=SS) (n=36) (n=33) (n=7) Effects
Age M 69.9 65.3 67.8 65.0 SD (7.7) (9.1) (10.1) (7.5)
Education M 12.9 13.2 14.3 11.6 (years) SD (3.3) (3.3) (2.8) (1.6)
Sex Ratio 56% male 56% male 55% male 0% male x2=8.26; PC.05
Onset 144 6.1 1.7 6.6 (weeks) SD (3.0) (X) (9.7) (2.6)
Degree M 2.8 Hemisparesisb SD (1.0) (Z) ($ (Z) GG:IGG;a
Note. RBD=right brain damage; LBD=left brain damage; VFD- =visuaI fietd defect ab- sent; VFD + =visual-field defect present. aScheffe test significant at .OS level. Qating of hemiparesis was based on a composite measure of face, arm, and leg on a l-5 scale: 1 = no movement to 5 = normal movement.

218 S. Egelko et al.
onset of stroke. However, the sex ratio in the LBD field cut group (all seven were females) was different than that for the other three patient groups, in which males slightly outnumbered females. This discrepancy in sex ratio may be attributable to a higher incidence of severe aphasia in LBD males with more posterior (and hence greater likelihood of testing positive for a visual-field defect) damage. As already mentioned, severely aphasic patients were screened out by the Mini-Mental State Exam.
Procedure
A 36item figure match test, the Lateral Asymmetries in Visual Spatial Attention (LAVA) Test, was administered. The LAVA consisted of evenly divided Structured and Unstructured Match series (see Figures 1 and 2) administered in counterbalanced order. The Structured series entailed the match of common, easily labeled objects and the Unstructured series con- sisted of geometric, not easily labeled objects. On each page a target in top center was positioned at the patient’s midline and was matched to one of six figures below, arranged in the following positions:
1 2 3 4 5 6
In each series correct choices were evenly distributed among these six posi- tions. Each page was 9” x 12” in dimensions, placed on a table at roughly 18” distance, and all seven figures on each page were roughly 20 sq. cm. in area. Patients were instructed to identify their item choice orally, although in a minority of cases in which confusion appeared in identifying the number corresponding to the picture, manual pointing of the choice by the patient was implemented. Thus, the task was relatively motor-free.
A “bias” score was computed by comparing the number of selections on the right (3 and 6 position) versus the number of selections on the left (1 and 4 position). Errors made by subjects were classified not only by side but further by lateral edge of figure (i.e., left or right detail). For example, as may be seen in Figure 1, a sample item from the Structured series, the correct choice is #6 on the right side of the page. If either of the two best foils, both on the left side, were selected as an answer, this choice would be tallied in the bias score as a preference for the left hemispace. Furthermore, the two incorrect choices could be distinguished on the basis of whether the left or right edge detail was faulty relative to the target. Thus, the error in selecting choice #l would be categorized as a left edge/left side (LEILS) of the page error while the error in selecting choice #4 would be categorized as right edge/left side (REILS). Figure 2, a sample item from the Unstructured series, illustrates an example in which a converse situation exists. The correct choice, #4, is located on the left and is balanced by two foils on the right
Unilateral Spatial Neglect 219
side; choice #3 would be categorized as left edge/right side (LE/RS) and choice #6 would be categorized as right edge/right side (RE/RS). On both the Structured and Unstructured series, for items in which the correct choice is either on the left (positions 1 and 4) or the right (positions 3 and 6), that is, in a total of 12 out of 18 items on each series, the best foils are positioned on the opposite side, one with an error on the left side of the figure and the other with an error on the right side of the figure. Comparison of left edge versus right edge detail errors within either the right or left hemispace, that is, right or left side of the page, enables an evaluation of fine spatial atten- tional preference.
The 36-item RCPM was administered to provide a standard of compari- son in evaluating the LAVA bias. RCPM bias was computed comparably to the LAVA by comparing the number of selections on the right versus left side.
RESULTS
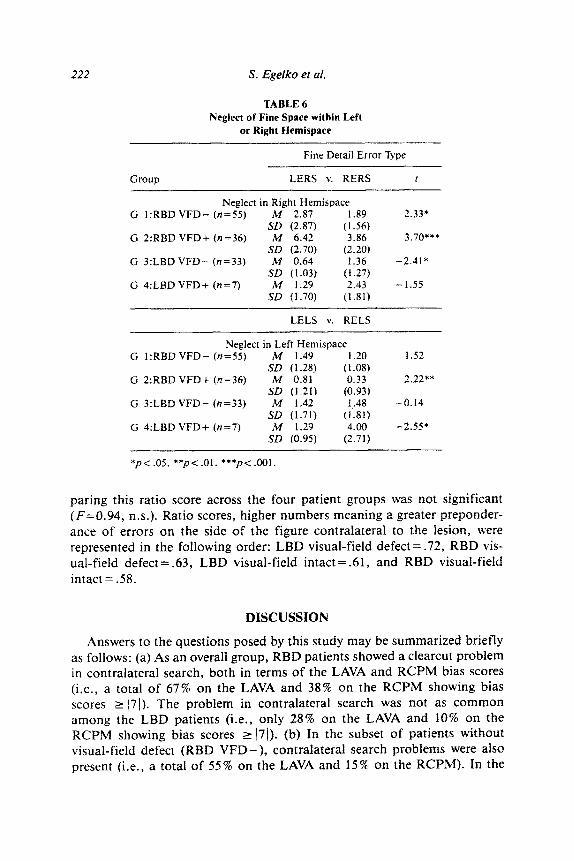
As may be seen in Table 2, performance on the Mini-Mental State Exam was impaired for the LBD visual field defect (VFD+) group relative to the
TABLE 2 One-Way Analyses of Variance on Mini-Mental State Exam,
LAVA, and RCPM Performance
Cl G2 G3 G4 Post-Ho?
RBD VFD- RBD VFD + LBD VFD- LBD VFD + Group Test (n=55) (n=36) (n=33) (n=7) Effects
MMSE M 26.7 25.3 26.0 23.0 Gl>G4 (max = 30) G3>G4
SD (1.9) (2.3) (2.8) (2.9)
LAVA- M 24.3 14.9 28.4 22.4 G3>G2 Total Gl>G2 (max=36) SD (5.9) (4.9) (5.0) (3.6) G3>GI
LAVA M 12.6 8.2 14.7 12.7 G3>G2 Structured G4>G2 (max = 18) SD (3.5) (2.7) (2.5) (2.7) Gl>GZ
G3>Gl
LAVA M 11.7 6.7 13.7 9.7 Gl>G2 Unstructured G3>Gl (max=lE) SD (3.1) (2.6) (2.9) (1.9) G3>G2
G3>G4
RCPM M 22.8 13.2 23.7 16.0 Gl>G2 (max=36) G3>G2
SD (6.5) (4.7) (7.5) (4.6)
‘Scheffe test significant at .05 level.

220 S. Egelko et al.
RBD and LBD visual field intact (VFD-) groups. On the two visual-spatial tasks, LAVA and RCPM, overall performance was generally poorer for the RBD visual field defect (VFD+) group relative to the other three groups. For all four groups, performance on the Unstructured series was more im- paired relative to the Structured series; overall t(130)=5.36, p< .OOl. Com- parison of the RBD and LBD visual-field intact groups showed no signifi- cant difference between the two groups in RCPM while the RBD visual-field intact group was significantly worse on LAVA for overall score, as well as performance on Structured and Unstructured Series. Chi square compari- sons (see Table 3) between all RBD and LBD patients were significant for both the LAVA bias (x2=37.22 [2,131]. p< .OOl) and RCPM bias (x2= 14.66 [2, 1301, p< .OOl). On both tests, RBD patients displayed, as expected, a
-tendency to neglect preferentially the left hemi-space, i.e., 62% and 34% showed a bias score of greater than or equal to +7 on the LAVA and RCPM, respectively. By contrast, LBD patients showed only a slight preferential neglect of the right hemispace (biasr -7), that is, 23% and 08% on the LAVA and RCPM, respectively. (In a sample of 50 normal age-matched controls, only one case showed a positive bias and only one a negative bias on the RCPM for a total of 04%). Comparable chi square analyses (Table 3) comparing RBD and LBD visual-field intact patients indicated no differ- ences between the groups on RCPM bias score, although a significant differ- ence in LAVA bias score was found (x2= 16.80 [2,88], p< .OOl).
As may be seen in Table 4, it is in the RBD visual-field intact group that
TABLE 3 Comparison of Neglect between RBD and LBD Patient Groups
5 -7 -6 to +6 2 +7 Missing
LAVA Bias All RBD 5 30 56 x2=37.22, PC .OOl All LBD 9 29 2
RCPM Bias All RBD 4 56 31 0 x2=14.66, p<.OOl All LBD 3 35 1 1
LAVA Bias RBD VFD- 5 26 24 x2= 16.80, p< ,001 LBD VFD- 6 26 1
RBD VFD- LBD VFD -
RCPM Bias 3 41 5 x2=1.19, n.s. 2 30 I
No/e. There were too few cases (n=7) in the LBD VFD+ group to permit a x2 analysis comparing this group to RBD VFD+.

Unilateral Spatial Neglect 221
TABLE 4
Comparison of Neglect Classification by RCPM versus LAVA Bias
RCPM neglect v. LAVA neglect
n % n % I
G 1:RBD VFD- (n=SS) 8 15 29 53 4.22* G 2:RBD VFD+ (n=36) 27 75 32 89 0.50 G 3:LBD VFD- (n=33) 3 09 7 21 1.37
Note. For both RCPM and LAVA an absolute bias score of 2 7 was the criterion for neglect. *p< .ool.
the hit rate for identifying neglecters is significantly increased by use of the LAVA, 53%, as compared with the 15% so classified by the RCPM. The presence of contralateral search problems in the RBD visual-field defect group is sufficiently gross as to be fairly adequately captured by the RCPM bias score and the addition of the LAVA bias score does not contribute significantly to the hit rate, that is, 89% LAVA v. 75 % RCPM rate. Nor does the LAVA significantly increase classification of neglect in the LBD visual- field intact group, 21% LAVA as compared with a 9% RCPM rate. Table 5 further illustrates the concordant and discordant classifications of neglect according to RCPM and LAVA bias scores for each of the patient sub- groups.
Finally, the issue of fine detail errors on the side contralateral to the lesion, presumably reflective of difficulty in extracting lateralized details during single-eye fixation, was examined. As indicated in Table 6, a signifi- cant preponderance of such lateralized fine detail errors was found in all of the patient groups for either one or both of the hemispaces. In both RBD and LBD patient groups, with and without visual-field defect, neglect of fine space was present. A ratio score of fine detail error type was computed for each group collapsed across hemispace (LE : LE +RE for both RBD groups and RE : RE + LE for both LBD groups). A one-way ANOVA com-
TABLE 5 Percentage of Concordant and Discordant Neglect
Classification on the Basis of RCPM and LAVA Bias
Neglect on Both Neglect on Neglect on Neglect on LAVA+RCPM LAVA Only RCPM Only Neither Measure
G l:RBD VFD- (n=55) 13% 40% 02% 45% G 2:RBD VFD+ (n=36) 69% 19% 06% 06% G 3:LBD VFD- (n=33) 03% 18% 06% 73%
Nofe. For both RCPM and LAVA an absolute bias score value of 2 7 was the criterion for neglect.
222 S. Egelko et al.
TABLE 6 NeglecI of Fine Space within Left
or Right Hemispace
Fine Detaif Error Type
Group LERS v. RERS t
Neglect in Right Hemispace G 1:RBD VFD- (n=55) M 2.87 1.89
SD (2.87) (1.56) G 2:RBD VFD+ (n=36) M 6.42 3.86
SD (2.70) (2.20) G 3:LBD VFD- (n=33) M 0.64 1.36
SD (1.03) (1.27) G 4:LBD VFD+ (n=7) M 1.29 2.43
SD (1.70) (1.81)
2.33*
3.70***
-2.41’
-1.55
LELS v. RELS
Neglect in Left Hemispace G 1:RBD VFD- (n=55) M 1.49 1.20
SD (1.28) (1.08) G 2:RBD VFD+ (n=36) M 0.81 0.33
SD (1.21) (0.93) G 3:LBD VFD- (n=33) M 1.42 1.48
SD (1.71) (1.81) G 4:LBD VFD+ (n=7) M 1.29 4.00
SD (0.95) (2.71)
1.52
2.22**
-0.14
-2.55+
*p<.o5. **p<.o1. ***p<.OO1.
paring this ratio score across the four patient groups was not significant (F=0.94, n.s.). Ratio scores, higher numbers meaning a greater preponder- ance of errors on the side of the figure contralateral to the lesion, were represented in the following order: LBD visual-field defect =.72, RBD vis- ual-field defect = .63, LBD visual-field intact = .61, and RED visual-field intact = .58.
DISCUSSION
Answers to the questions posed by this study may be summarized briefly as follows: (a) As an overall group, RED patients showed a clearcut problem in contralateral search, both in terms of the LAVA and RCPM bias scores (i.e., a total of 67% on the LAVA and 38% on the RCPM showing bias scores L 171). The problem in contralateral search was not as common among the LBD patients (i.e., only 28% on the LAVA and 10% on the RCPM showing bias scores 2 /71). (b) In the subset of patients without visual-field defect (RBD VFD-), contralateral search problems were also present (i.e., a total of 55% on the LAVA and 15% on the RCPM). In the

Unilateral Spatial Neglect 223
LBD visual field intact group, problems of contralateral search were not as common and roughly comparable to the overall group of LBD patients (i.e., only 21% on LAVA and 09% cn RCPM). (c) As these percentages indicate, the LAVA bias is a more sensitive diagnostic tool in detecting spatial neglect than is the RCPM bias score, particularly in ferreting out spatial neglect in RBD visual-field intact patients. (d) Finally, greater difficulties in matching information on the side of a figure contralateral, as compared with ipsila- teral, to the lesion may be detected in RBD and LBD patients, both with and without field defects. This finding is somewhat surprising in view of Gainot- ti’s hypothesis of a uniquely RBD type of difficulty in extracting visual information from the side of a figure contralateral to the lesion.
Recent efforts to determine the underlying mechanism of neglect have pointed to the multi-dimensional nature of neglect phenomena, and the need for assessment procedures which better reflect that complexity. The present study utilized the LAVA, a test which is similar to the RCPM in structure, and which similarly yields a bias score. However, the LAVA is a more sensitive test than the RCPM due to the use of more complex stimuli, competing stimuli in the left and right hemispace, and the use of choices requiring discrimination of fine left and right details within a hemisphere.
The sensitivity of the LAVA to deficiencies of gross scanning behavior, as well as to inattention to fine detail in small space, enabled the exploration of the mechanisms of neglect which are currently discussed in the literature. For example, Heilman and colleagues have proposed that neglect is due to hypokinesis - a failure to search in the hemispace contralateral to the lesion. While our findings of fine spatial inattention to the hemispace contralateral to the lesion might be interpreted as a milder manifestation of hypokinesis (i.e., the patient is searching in the contralateral hemispace, but misses fine details in the far edge of that hemispace), the occurrence of lateralized fine detail errors in the ipsilateral field is difficult to explain by the mechanism of hypokinesia.
Gainotti has proposed a theory which addresses the mechanism of inat- tention to smaller-scale space. His theory posits that, while gross scanning behavior is impaired in both left and right brain damaged patients, the inability to extract information from the side of visual stimuli contralateral to lesion during single eye fixation is unique to RBD patients. While the LAVA paradigm differs from the embedded figures task on which Gainotti et al. (1986) bases his theory, and it is unclear in both cases the degree to which only single fixation is involved, both tasks are sensitive to inattention in smaller-scale space and address an aspect of neglect which appears to be other than a failure to search the contralateral hemispace. Furthermore, the finding of this study of lateralized fine spatial errors in LBD patients sug- gests that this component of neglect is not unique to RBD patients.
Bisiach, Perani, Vallar, and Berti’s (1986) hypothesis of multiple schematic

224 S. Egelko et 01.
systems of space representation involving a formulation of neglect dissocia- ble at different levels of space (i.e., personal, peri-personal, and extraper- sonaf) may be of relevanrz to the current study, According to their schema, variation in a patient’s performance across tasks assessing different compo- nents of neglect may reflect disturbances in one of a number of distinct systems of space representation. While the stimuli in this study did not utilize the same divisions of space as those proposed by Bisiach (i.e., person- al, peri-personal, extrapersonal), we explored the possibility that neglect phenomena in fine and gross space as assessed by the LAVA were the rest& of disturbance in distinct systems of space representation rather than de- grees of disturbance in a unitary mechanism of neglect. To this end, the correlation between fine attentional errors and the bias scores on the LAVA test was examined to assess the degree to which these two aspects of neglect were associated. While not conclusive, the absence of a significant correla- tion between fine and gross neglect within RBD and LBD patient groups, with and without visual-field defects, suggests that these phenomena may result from dissociable mechanisms or systems of representation. For exam- ple, hypokinesia may underlie neglect of space across the body midline while mechanisms such as disturbances of internal space representation and fail- ure to disengage from stimuli during single eye fixation may play a more critical role in neglect of fine space.
In conclusion, the current study supports our contention that use of the LAVA provides a more powerful tool than the RCPM in identifying patients with subtle as well as gross manifestations of neglect, and furthers our ability to discriminate among distinct aspects of neglect phenomena. Rather than pointing to a unitary mechanism of neglect the findings of the present study support a view of neglect as resulting from multiple underlying mech- anisms.
These conclusions are based on the use of the LAVA test in a paper-and- pencil format, and it remains for future research to refine the presentation of these stimulus materials. For example, separate tachistoscopic presenta- tion of the LAVA stimuli to each lateral visual field and use of reaction time measures may further our understanding of the phenomena of neglect, particularly of the subtype confined exclusively to fine spatial asymmetrical errors. Furthermore, these refined procedures may be more appropriate for use with more homogeneous populations, with respect to both size and location of lesion.
REFERENCES
Bisiach, E., Perani, D., Valiar, G., Rr Berti, A. (1986). Unilateral neglect: Personal and extra- personat. ~e~~ps~~~~~~gi~, 24, X9-767.
Costa, L. D., Vaughan, H. G., Jr., Horwitz, M., & Ritter, W. (1969). Patterns of behavioral deficit associated with visual spatial neglect. Carrex, 5, 242-263.
Unilateral Spatial Neglect 225
Folstein, M. F., Folstein, S. E., & McHugh, P. R. (1975). Mini-mental state. Journal of
Psychiatric Research, 12, 189-198.
Gainotti, G., Caltagirone, C., & Mice& G. (1977). Poor performance of right brain-damaged
patients on Raven’s Coloured Matrices: Derangement of general intelligence or of specific
abilities. Neuropsychologiu, 15, 675-680. Gainotti, G., D’Erme, P., Monteleone, D., & Silveri, M. C. (1986). Mechanisms of unilateral
spatial neglect in relation to laterality of cerebral lesions. Bruin, 109, 599-612.
Heilman, K. M. (1983). Localization of lesions in neglect. In A. Kertesz (Ed.), Localization in neuropsychofogy New York: Academic Press.
Luria, A. R. (1973). The working bruin (pp. 210-214). (B. Haigh, Trans.). New York: Basic
Books.
Morrow, L. A., & Ratcliff, G. G. (1987). Attentional mechanisms of clinical neglect. Journal of
Clinical and Experimental Neuropsychology, 9,74-75. Piasetsky, E. (198 1). A study of pathological asymmetries in visual-spatial attention in unilater-
ally bruin-dumged stroke patients. Unpublished doctoral dissertation, City of New York,
New York.
Posner, M. I., Walker, J. A., Friedrich, F. J., & Rafal, R. D. (1984). Effects of parietal injury on
covert orienting of attention. Journul of Neuroscience, 4, 1863-1874.
Raven, J. C. (1962). Coloured Progressive Matrices Sets A, AB, B. London: H. K. Lewis
(Originally published in 1947, revised order in 1956).
Stuss, D. T., & Benson, D. F. (1984). Neuropsychological studies of the frontal lobes. Psycho- logical Bulletin, 95, 3-28.
Related Documents











