Accepted Manuscript Fully Endoscopic Interlaminar and Transforaminal Lumbar Discectomy: Short-term Clinical Results of 163 Surgically Treated Patients Altay Sencer , MD Ali Guven Yorukoglu , MD Mehmet Osman Akcakaya , MD Yavuz Aras , MD Aydin Aydoseli , MD Osman Boyali , MD Fahir Sencan , MD Pulat Akin Sabanci , MD Cengiz Gomleksiz , MD Murat Imer , MD Talat Kiris , MD Kemal Hepgul , MD Omer Faruk Unal , MD Nail Izgi , MD Ali Tuncay Canbolat , MD PII: S1878-8750(14)00539-7 DOI: 10.1016/j.wneu.2014.05.032 Reference: WNEU 2387 To appear in: World Neurosurgery Received Date: 14 September 2013 Revised Date: 7 December 2013 Accepted Date: 29 May 2014 Please cite this article as: Sencer A, Yorukoglu AG, Akcakaya MO, Aras Y, Aydoseli A, Boyali O, Sencan F, Sabanci PA, Gomleksiz C, Imer M, Kiris T, Hepgul K, Unal OF, Izgi N, Canbolat AT, Fully Endoscopic Interlaminar and Transforaminal Lumbar Discectomy: Short-term Clinical Results of 163 Surgically Treated Patients, World Neurosurgery (2014), doi: 10.1016/j.wneu.2014.05.032. This is a PDF file of an unedited manuscript that has been accepted for publication. As a service to our customers we are providing this early version of the manuscript. The manuscript will undergo copyediting, typesetting, and review of the resulting proof before it is published in its final form. Please note that during the production process errors may be discovered which could affect the content, and all legal disclaimers that apply to the journal pertain.

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript
Accepted Manuscript
Fully Endoscopic Interlaminar and Transforaminal Lumbar Discectomy: Short-termClinical Results of 163 Surgically Treated Patients
Altay Sencer , MD Ali Guven Yorukoglu , MD Mehmet Osman Akcakaya , MD YavuzAras , MD Aydin Aydoseli , MD Osman Boyali , MD Fahir Sencan , MD Pulat AkinSabanci , MD Cengiz Gomleksiz , MD Murat Imer , MD Talat Kiris , MD KemalHepgul , MD Omer Faruk Unal , MD Nail Izgi , MD Ali Tuncay Canbolat , MD
PII: S1878-8750(14)00539-7
DOI: 10.1016/j.wneu.2014.05.032
Reference: WNEU 2387
To appear in: World Neurosurgery
Received Date: 14 September 2013
Revised Date: 7 December 2013
Accepted Date: 29 May 2014
Please cite this article as: Sencer A, Yorukoglu AG, Akcakaya MO, Aras Y, Aydoseli A, Boyali O,Sencan F, Sabanci PA, Gomleksiz C, Imer M, Kiris T, Hepgul K, Unal OF, Izgi N, Canbolat AT, FullyEndoscopic Interlaminar and Transforaminal Lumbar Discectomy: Short-term Clinical Results of 163Surgically Treated Patients, World Neurosurgery (2014), doi: 10.1016/j.wneu.2014.05.032.
This is a PDF file of an unedited manuscript that has been accepted for publication. As a service toour customers we are providing this early version of the manuscript. The manuscript will undergocopyediting, typesetting, and review of the resulting proof before it is published in its final form. Pleasenote that during the production process errors may be discovered which could affect the content, and alllegal disclaimers that apply to the journal pertain.
MANUSCRIP
T
ACCEPTED
ACCEPTED MANUSCRIPTFully Endoscopic Interlaminar and Transforaminal Lumbar Discectomy: Short-term Clinical
Results of 163 Surgically Treated Patients
Altay Sencer MD1, Ali Guven Yorukoglu MD2, Mehmet Osman Akcakaya MD3, Yavuz Aras
MD1, Aydin Aydoseli MD1, Osman Boyali MD1, Fahir Sencan MD1, Pulat Akin Sabanci MD1,
Cengiz Gomleksiz MD4, Murat Imer MD1, Talat Kiris MD1, Kemal Hepgul MD1, Omer Faruk
Unal MD1, Nail Izgi MD1, Ali Tuncay Canbolat MD1
1) Department of Neurosurgery, Istanbul School of Medicine, Istanbul University,
Istanbul/ Turkey
2) Department of Neurosurgery, Artvin State Hospital, Artvin/Turkey
3) Department of Neurosurgery, Taksim Training and Research Hospital,
Istanbul/Turkey
4) Department of Neurosurgery, Erzincan University Faculty of Medicine,
Erzincan/Turkey
Corresponding Author:
Mehmet Osman Akcakaya, MD
Taksim Egitim ve Arastırma Hastanesi, Nöroşirürji Klini ği
Sıraselviler Cad. No:112 Beyoglu/Istanbul 34433
E-mail: [email protected]
Phone: 00905322557774
Keywords: endoscopic discectomy, transforaminal discectomy, interlaminar discectomy,
percutaneous discectomy, lumbar disc herniation, minimally invasive spine surgery
Running Head: Sencer et al, Fully Endoscopic Lumbar Discectomy
MANUSCRIP
T
ACCEPTED
ACCEPTED MANUSCRIPTAbstract:
Objective: Due to technical advances, minimally invasive surgical techniques are becoming
increasingly common in an attempt to decrease tissue trauma. In this study, we evaluated the
clinical outcomes of lumbar disc disease patients undergoing fully endoscopic surgery at our
clinic.
Methods: One hundred sixty-three patients underwent fully endoscopic lumbar discectomy
between August 2009 and January 2012. There were 74 male and 89 female patients in our
study. All patients were followed for one year after surgery. The Oswestry Disability Index
(ODI) and the visual analog scale (VAS) were used to analyze outcomes.
Results: During the follow-up period, 114 (70%) patients had no complaints, 30 (18%)
patients had occasional pain, and 19 (12%) had no improvement. During postoperative
follow-up, eight patients required repeat surgery due to recurrence or residual fragments.
Postoperatively, four patients experienced dysesthesia, which completely resolved in time.
Five patients deteriorated neurologically, four of whom recovered completely without any
intervention. Dural tears occurred in six patients.
Conclusions: The results of our study show that fully endoscopic interlaminar or
transforaminal surgeries are safe and effective treatment modalities for lumbar disc
herniations. As our clinical experience indicates, despite the difficulties of acquiring this new
technique, good results can be achieved with sufficient experience.
Keywords: endoscopic discectomy, transforaminal discectomy, interlaminar discectomy,
percutaneous discectomy, lumbar disc herniation, minimally invasive spine surgery
MANUSCRIP
T
ACCEPTED
ACCEPTED MANUSCRIPTIntroduction:
Since the first description of the open lumbar discectomy by Dandy, followed by
Mixter and Barr (9,34), significant improvements have been achieved in the management of
lumbar disc herniation. After the introduction of the surgical microscope, Caspar (7) and
Yasargil (52) defined laminectomy and open microdiscectomy (MD). This technique, with
slight variations, has become the standard surgical procedure for lumbar disc herniations
through the last decade and is still the predominant surgical approach.
In the past three decades, minimally invasive surgery has attracted increasing
attention. With the evolution and refinement of the surgical endoscope, minimally invasive
endoscopic surgical techniques have been widely adopted in different fields of medicine.
However, compared to other surgical fields such as gastrointestinal or orthopedic surgery,
endoscopes have been slow to gain widespread application in spinal surgery. Minimally
invasive procedures in the lumbar spine date back to 1948, when Valls et al. described a
percutaneous technique for aspiration biopsy of vertebral body lesions. (48) In the 1970s,
Hijikata (17) and Kambin (21) separately defined a posterolateral approach for percutaneous
central nucleotomy. Forst and Housmann first visualized the intervertebral disc space with a
modified arthroscope. (15) Mayer, Schreiber and Kambin improved endoscopic lumbar
discectomy techniques. (16,23,33,44,45) In particular, Kambin’s anatomic description of the
neural foramen for the purposes of endoscopic access was one of the cornerstones in the
development of a fully endoscopic transforaminal approach. Major improvements were
achieved by the introduction of the “Yeung Endoscopic Spine System (YESS)” by Yeung
(53,55) and the fully endoscopic interlaminar technique described by Ruetten. (40) Today,
MANUSCRIP
T
ACCEPTED
ACCEPTED MANUSCRIPTendoscopic lumbar discectomy has become an important alternative to conventional MD in
the management of lumbar disc herniations.
Various surgical techniques have been described; however, minimally invasive
endoscopic approaches to the lumbar spine can be classified into two major categories:
transforaminal (TF) and interlaminar (IL). TF approaches can be divided into fully endoscopic
posterolateral and lateral subcategories. IL approaches can be categorized as endoscopy-
assisted techniques or fully endoscopic techniques.
This prospective study presents the surgical results of 163 patients with lumbar disc
herniations who underwent surgery using both fully endoscopic IL and lateral TF approaches.
The indications and limitations of both approaches are described, and the possible difficulties
and complications that may be faced by surgeons who are unfamiliar with these procedures
are presented. The aim of this study is to present our experience with fully endoscopic lumbar
discectomy in an effort to evaluate our clinical results, specifically in terms of the safety and
efficacy of this approach.
Patients and Methods:
Patient Demographics and Diagnoses
One hundred sixty-three consecutive patients who underwent fully endoscopic lumbar
discectomy (FELD) in our department between August 2009 and January 2012 were
evaluated in this study. One hundred seventy-five disc levels were operated upon, as multiple
MANUSCRIP
T
ACCEPTED
ACCEPTED MANUSCRIPTlevel lumbar discectomy was performed in 11 patients. There were 74 male and 89 female
patients. The mean age was 47 years (range 18 to 78 years). All patients had experienced
ongoing symptoms of back and leg pain. The indications for surgery were the same as for
open microsurgery, namely, the presence of any progressive neurological deficit or radicular
pain that was unresponsive to medical therapy. Only patients with cauda equina syndrome did
not undergo endoscopic surgery.
Magnetic resonance imaging (MRI) was performed in all cases. An additional
abdominal computed tomography (CT) scan was performed in order to visualize the
anatomical structures and to prevent retroperitoneal injuries related to the lateral access
techniques used by the TF approach for lumbar disc herniations above the L3-4 level.
Selection Criteria for Surgical Approach
The selection of a lateral TF versus an IL approach was based on the principles
previously defined by Ruetten et al. (39,41,42) The TF approach was the first choice, but it
has known anatomic limitations. Therefore, the IL approach was chosen in patients with the
following characteristics: a) sequestering material had migrated beyond the lower edge of the
cranial pedicle or over the middle of the caudal pedicle, and b) the foramen was overlaid by
the iliac crest on lateral plain radiographs. (39,41,42)
MANUSCRIP
T
ACCEPTED
ACCEPTED MANUSCRIPT
Surgical Technique
We used the same surgical techniques for both approaches that were previously
described by Ruetten et al. (38-42) Operations are performed under general anesthesia. The
patient is placed on the operating table in the prone position. The c-arm is positioned under
the operating table to allow sterile biplanar fluoroscopic control. For both approaches, the skin
incision is first marked. Following marking, the skin and muscle fascia incisions are made.
Normally, in the TF approach, the skin incision is located 8-12 cm from the midline,
but for the lateral TF approach, it must be located more laterally, depending on individual
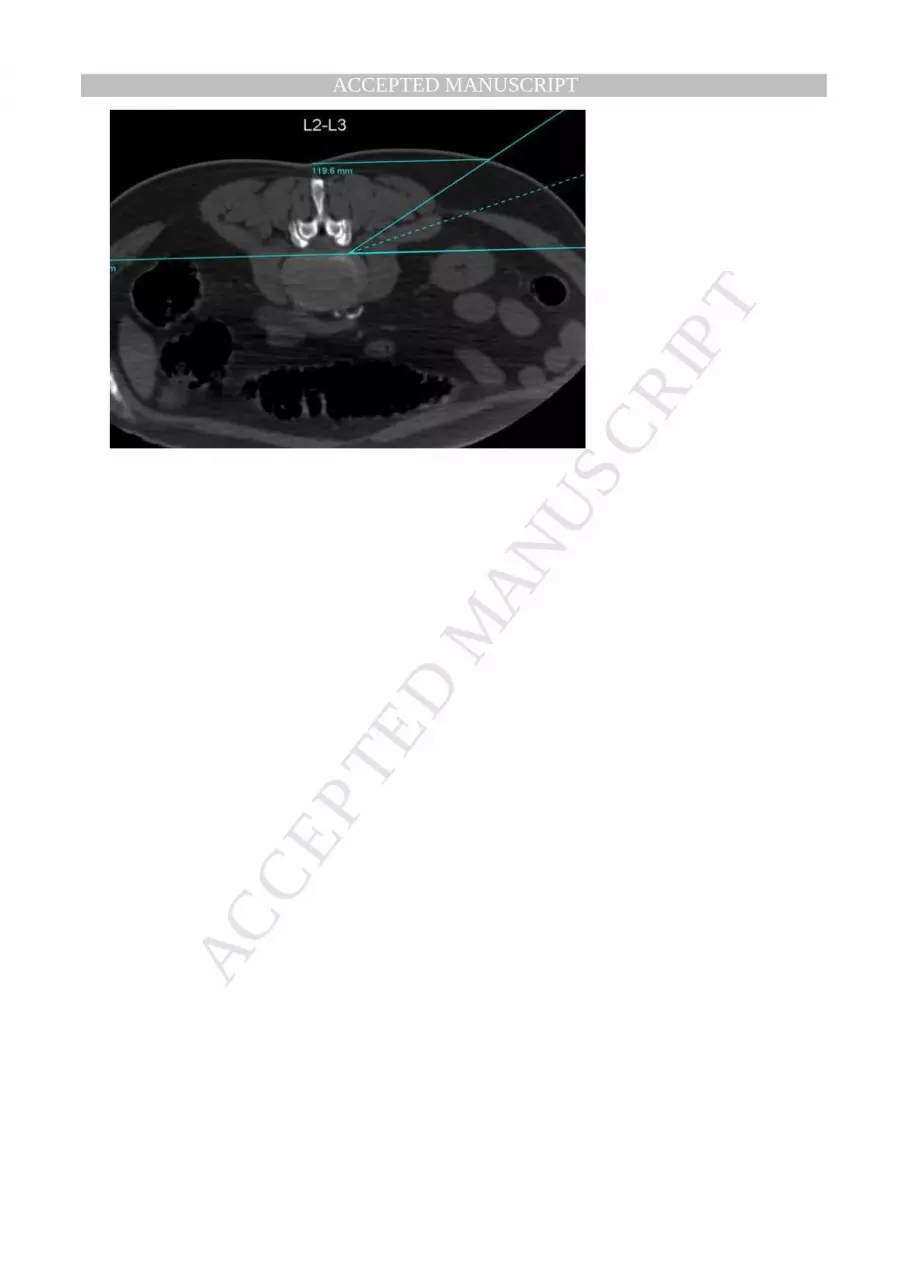
anatomy. The purpose is to obtain tangential access to the spinal canal. (Figure 1) As viewed
on lateral fluoroscopy, the posterior edge of the inferior articular process limits the entry zone
anteriorly for levels L3-4 and below. For levels above L3-4, care must be taken in order to
avoid damage to abdominal and thoracic anatomical structures. As mentioned above, an
additional abdominal CT may be a useful tool for planing the entry approach. Under
fluoroscopic control, a 1.5-mm blunt spinal cannula is inserted; through this, a 0.8 mm
guidewire is then inserted. The cannula is removed, and a cannulated dilator (with an outer
diameter of 6.9 mm) is inserted using the guidewire. The guidewire is then removed, and with
this blunt dilator, the position can be fixed more safely under fluoroscopic control. A surgical
sheath (with an outer diameter of 7.9 mm) with a beveled opening is placed over the dilator.
Then, using a direct endoscopic view and continuous irrigation, decompression is performed
(as shown in Figure 2 and 4a). Cauterization of the surrounding soft tissues allows hemostasis
and a cleaner surgical view. Decompression of the disc space and subsequent exploration of
MANUSCRIP
T
ACCEPTED
ACCEPTED MANUSCRIPTthe posterior longitudinal ligament (PLL) and the epidural space for the herniated disc is more
useful than directly searching for the sequestering material. Free fluctuation of the PLL under
constant irrigation is a good indicator of an adequate decompression.
The skin incision for the IL approach is made as medial to the midline of the targeted
interlaminar space as possible. Again, the dilator (with an outer diameter of 6.9 mm) is
bluntly inserted under fluoroscopic control to the lateral edge of the interlaminar space, and
the surgical sheath (with an outer diameter of 7.9 mm) with a beveled opening is placed over
the dilator. The procedure is continued using a direct endoscopic view and continuous
irrigation. Following cauterization and resection of the surrounding soft tissues, the
ligamentum flavum is exposed and is laterally incised for 3 to 5 mm. This incision can be
enlarged if necessary. After accessing the spinal canal, the dura mater and nerve roots are
exposed (Figure 3). The beveled opening of the surgical sheath can be used as a nerve root
retractor by rotating it. Following cauterization of the epidural veins, discectomy is performed
under fluoroscopic control (Figure 4b). If the bony structures do not allow enough access to
the spinal canal, further bone resection can be performed using a burr or Kerrison rongeur.
Compared to the TF approach, the IL approach is a more mobile access, allowing the
visualization of neighboring levels by using the endoscope like a joystick. With the IL
approach, bony resection can be achieved as necessary, and caudally or cranially migrated
disc herniations can be treated.
Outcome Assessment
MANUSCRIP
T
ACCEPTED
ACCEPTED MANUSCRIPT
If no complications occurred, patients were mobilized three hours after the operation,
and they were discharged from the hospital the next day. An early follow-up examination was
performed three weeks after surgery. The patients also returned for follow-up visits at 3, 6, 9,
and 12 months after surgery. Pre- and postoperative visual analog scale (VAS) testing and the
Turkish version of the “Oswestry Disability Index” (ODI) were used to evaluate clinical
outcomes and pain relief. (12) Additionally, a telephone interview was performed that
included questions assessing the subjective satisfaction of the patients. Clinical follow-up
examinations and interviews were performed by three physicians who were not involved in
the operations.
Statistical Analysis
The t-test was used to compare pre- and postoperative VAS and ODI scores.
Descriptive assessments and analytical statistics were calculated, depending on the group’s
characteristics, using SPSS 16. A positive significance level was assumed at a probability of
less than 0.05.
Results:
In 163 patients, a total of 175 FELDs were performed. One hundred and four patients
(59.5%) underwent surgery using the IL approach, and 71 patients (40.5%) underwent surgery
using the lateral TF approach. Patients with no complications (91%) were mobilized three
hours postoperatively and were discharged from the hospital the next day. The majority of the
MANUSCRIP
T
ACCEPTED
ACCEPTED MANUSCRIPToperations were performed on the L4-5 (93 cases - 53%) and L5-S1 (52 cases – 30%) levels.
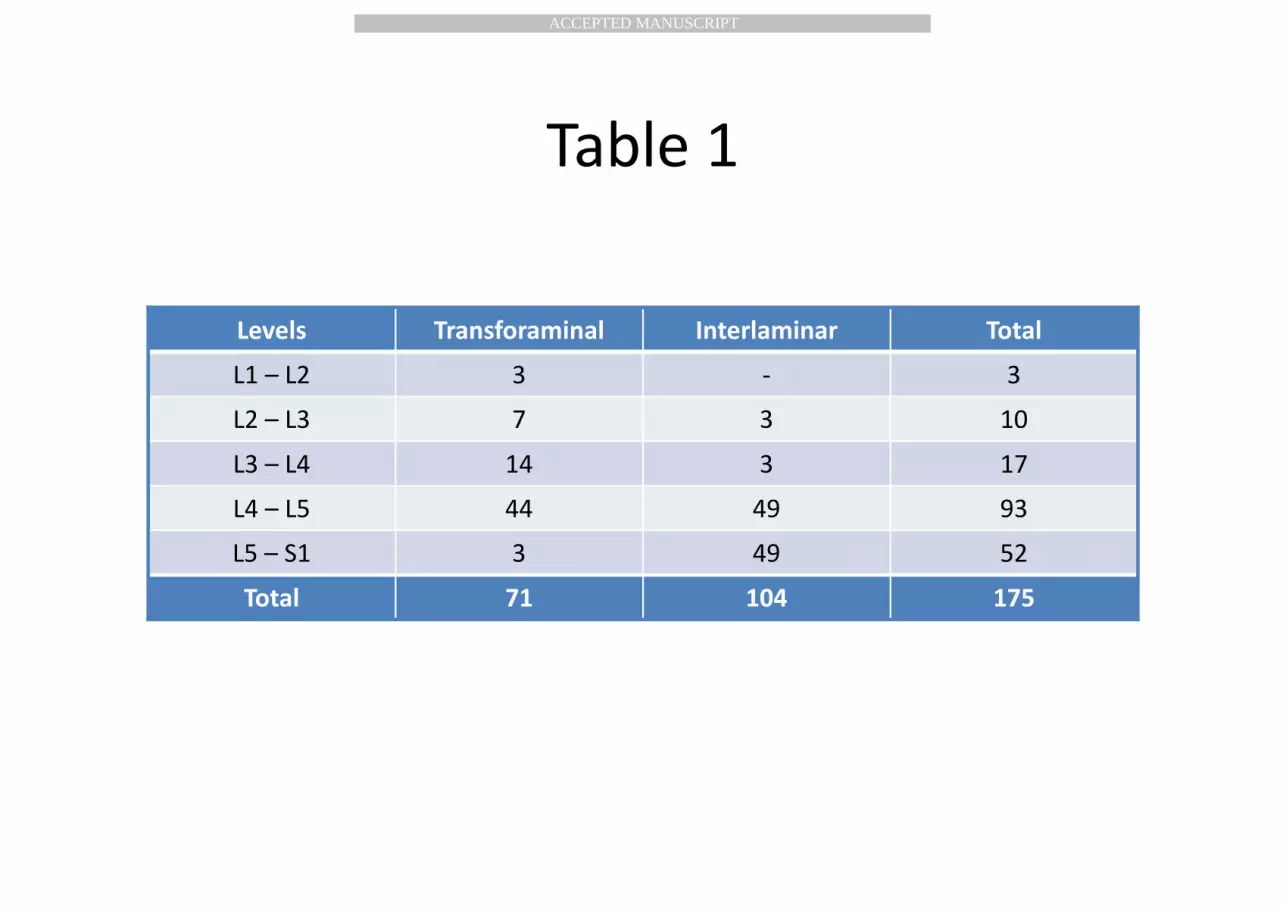
The follow-up time was 12 months. The distribution of the herniated disc levels and surgical
approaches are summarized in Table 1.
Multi-level lumbar discectomy was performed in 11 patients, and single-level
discectomy was performed in 152 patients. Three-level discectomy was performed in one
case, and in 10 cases two-level discectomy was performed. Eleven cases with single-level disc
herniations had a history of previous MD at the same level and the same side. The TF
approach was used in four of these patients, and the IL approach was performed in seven
patients. (L5-S1: 3 IL/1 TF, L4-5: 2 IL/2 TF, L3-4: 1 IL, L2-3: 2 TF) Pain relief was achieved
in all of these 11 patients.
Reoperations
The herniated disc material was removed in all cases. Intraoperative conversion to
conventional MD was not required in our cases. In two cases (1.2%), early pain relief did not
occur; both of these patients underwent surgery via the lateral TF approach. With further
radiological evaluation, the presence of residual herniated disc material was identified, and
these patients underwent reoperation with the same technique. Pain relief was achieved in one
of these cases. The other patient did not experience significant improvement.
There were 6 recurrences (3.7%) among our patients. Following a pain-free interval,
the mean time from the first operation to recurrence was 1.5 months in our series (range 2
weeks to 3 months). The primary surgical approach was IL in four cases and TF in two cases.
Four of these recurrences underwent repeat surgery using the technique described here, and in
MANUSCRIP
T
ACCEPTED
ACCEPTED MANUSCRIPTtwo cases (one IL and one TF), conventional MD was the preferred approach for reoperation.
No further recurrences occurred following the second surgery. In four of these cases, good
pain control was achieved, whereas in two cases (where the IL approach was used for both the
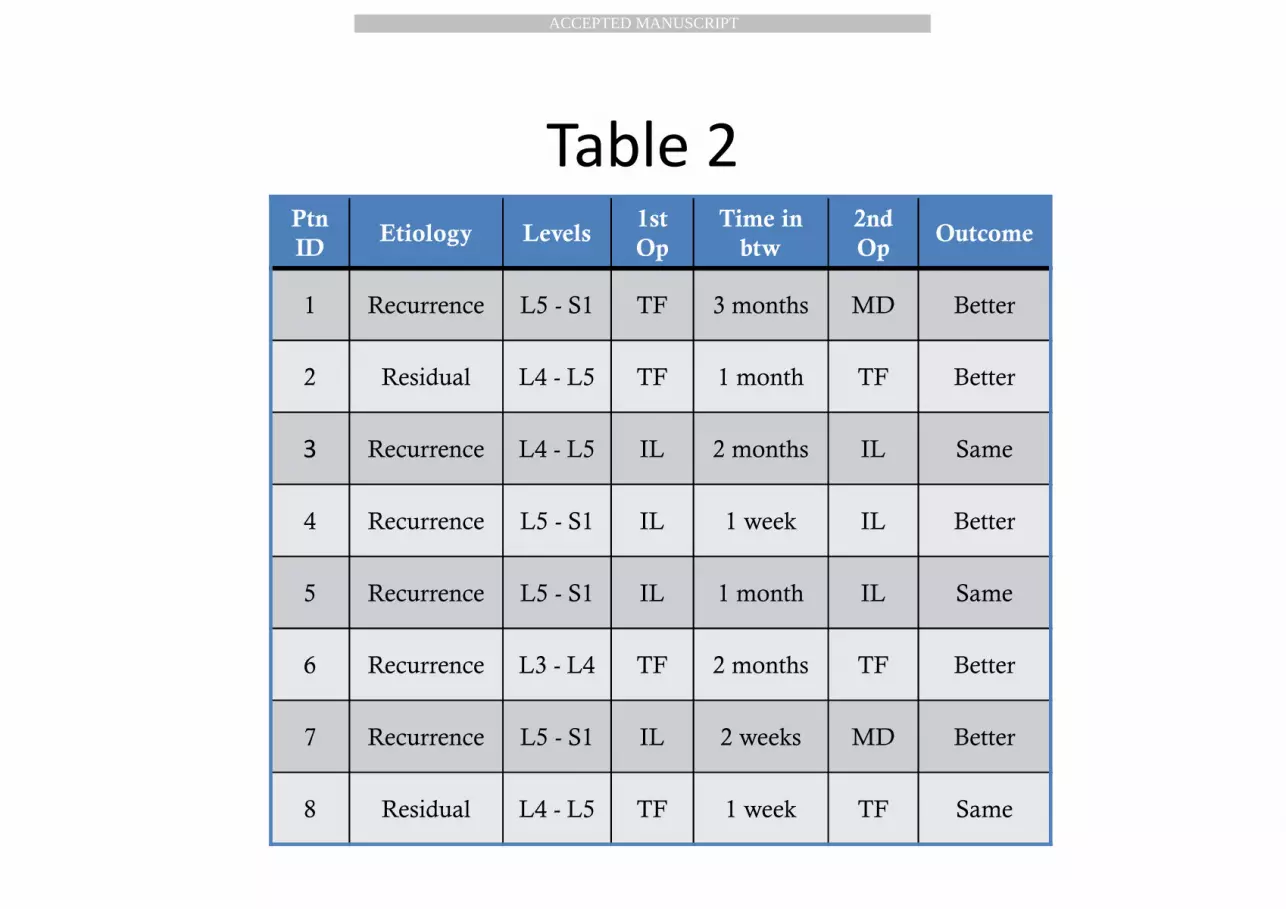
initial and repeat operations), no significant improvement was noted. The distribution of
lumbar disc herniation levels, selected surgical approaches for the initial and the second
operations, time to the second operation, and outcomes are summarized in Table 2.
Complications
Motor deficits occurred in five patients (3%). Most of these deficits occurred in the
early cases of this series and were attributed to possible nerve root injuries due to nerve root
retraction. In two of these cases, two-level discectomy was performed using an IL approach
for one level and a TF approach for the other. In four cases, these motor deficits were
transient, and complete recovery occurred, including the two patients who underwent two-
level discectomies. In only one case (0.6%), there was a permanent postoperative motor
deficit, resulting in “foot drop”.
Four patients experienced dysesthesia after the surgery (2.4%). All of the patients who
developed dysesthesia underwent surgery via the TF approach. Limited relief was achieved in
one patient with epidural and foraminal steroid injections. In the other three cases, this
complaint resolved completely.
Dural tears occurred in six cases (3.6%), but open cerebrospinal fluid (CSF) fistula
occurred in only one of these patients (0.6%). All the patients who experienced dural tears
underwent surgery with the IL approach. There was no attempt at dural repair in five cases; no
MANUSCRIP
T
ACCEPTED
ACCEPTED MANUSCRIPTopen or closed CSF fistula occurred in these cases, probably because of the small surgical
incision. These patients were followed up in the clinic with two additional days of bed rest
and thereafter were mobilized and discharged. The single case of an open CSF fistula was the
first case in our series in which this complication occurred. Unfortunately, we attempted to
repair the dura using an open microsurgical technique immediately after completing the
FELD. This patient had to undergo a second surgery for dural repair, and the fistula was
managed with 5 days of bed rest and lumbar drainage. There were no reports of infection,
secondary spondylodiscitis or abdominal organ injury in our series, except for two superficial
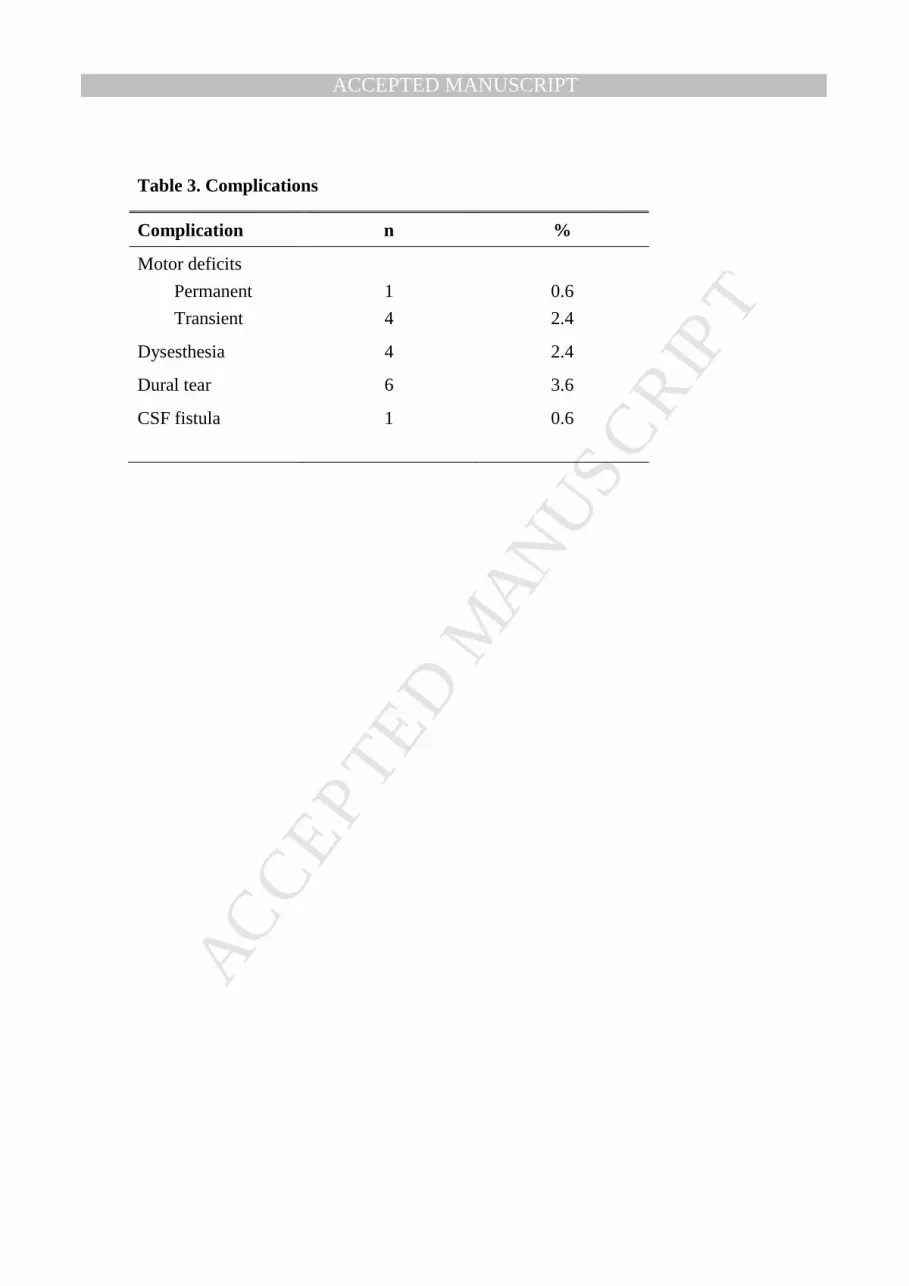
wound infections (1.2%), which were managed with oral antibiotics. Complications are
summarized in Table 3.
Clinical Outcomes
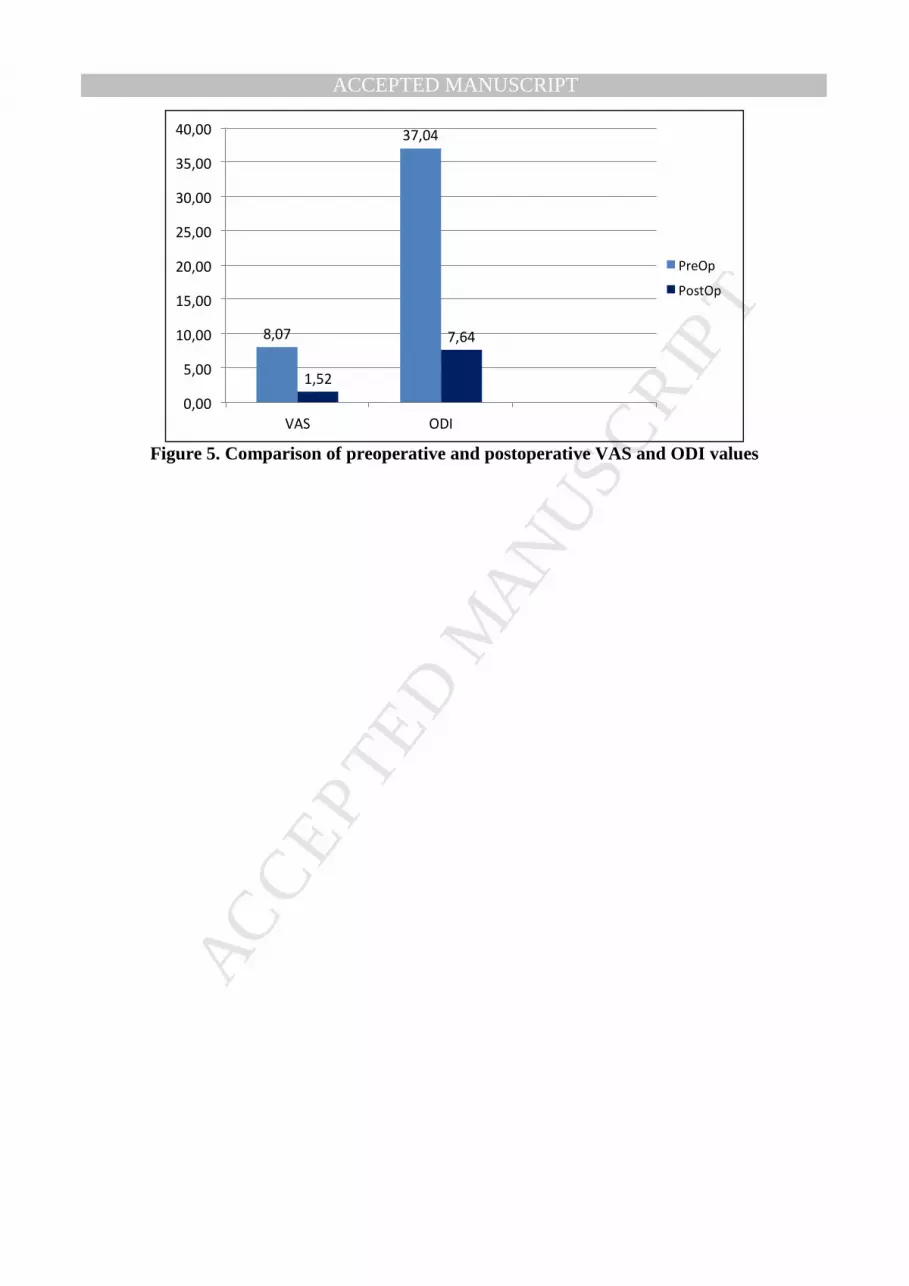
The bar graphs in Figure 5 show the differences in VAS and ODI scores before
surgery and at 12 months after surgery. Preoperatively, most of the patients had severe pain,
rendering them unable to perform their daily activities. As a result, the mean preoperative
VAS and ODI scores were 8,07/10 and 37,04, respectively. There was a significant decrease
in both the VAS and ODI scores after the FELD (p< 0,001). With a follow-up time of 12
months, 114 patients (70%) claimed that they no longer had leg pain, 30 patients (18%) had
occasional leg pain with general pain relief, and 19 patients (12%) experienced no significant
improvement. There were no persisting symptoms following revision surgeries for recurrent
or residual lumbar disc herniations. One hundred thirty-eight patients (85%) had subjective
satisfaction and would undergo the FELD operation again.
Discussion
MANUSCRIP
T
ACCEPTED
ACCEPTED MANUSCRIPT
Today, MD remains the standard surgical treatment for lumbar disc herniation.
Nevertheless, endoscopic surgical techniques have gained considerable attention in various
fields of surgery and have replaced conventional approaches in the management of many
different diseases, especially in gastrointestinal, orthopedic, thoracic and
otorhinolaryngological surgery. However, endoscopic neurosurgical techniques, particularly
for spine surgery, have been slow to gain acceptance. This may be due to the high success rate
of MD (between 75% and 100%; 2,11,13,28,51) and the routine use of microsurgical
techniques in nearly every field of neurosurgery. With such a high success rate, it is hard to
convince neurosurgeons who already have microsurgical skills to learn the endoscopic lumbar
discectomy technique, which is known for its steep learning curve. (20,31,36,43)
Additionally, the reported failure rates (20,26,31,32,43), the need of additional surgical time
(37), the need of strict patient selection (35) and potential complications cut in favor of
skeptics.
Lumbar disc herniation is a major health problem, and successful surgical treatment of
this condition is crucial in order to allow individuals to remain in the work force. Minimally
invasive lumbar disc surgery has attracted growing attention because of a possible reduction
in postoperative pain, earlier mobilization and a shorter recovery period. Although no studies
have provided Level 1 evidence for these advantages of minimally invasive procedures, many
studies, including ours, have shown that minimally invasive surgical treatment of lumbar disc
herniation provides comparable results to the classical surgical approaches. In a study by
Ruetten et al., no significant differences in clinical results were noted between FELD (IL or
lateral TF) and MD. (42) The main advantages of FELD include decreased operative trauma
and reduced epidural scarring (due to the use of an 8-mm cannula and direct visualization and
MANUSCRIP
T
ACCEPTED
ACCEPTED MANUSCRIPTillumination), early postoperative mobilization of patients, and reduced overall costs. (41,42)
In contrast to other publications, shorter operating times and success rates as high as
conventional MD have been reported in recent studies. (40,42) However, these studies were
conducted at a single institution and may be subject to biases related to patient selection, lack
of randomization, and subjective observations. Nellensteijn et al. provide a thorough review
of all studies related to the endoscopic lumbar disc surgery using the lateral TF approach. (35)
Thirty-nine different studies were analyzed; serious design weaknesses and a high risk of
selection bias were found in most of these. (35) Such criticisms also apply to the IL approach.
Given the current literature, objectively drawing such conclusions is not possible, due to a
previously noted lack of Level 1 evidence. Due to a lack of data from patients who underwent
MD at our institution prior to this study and a very small number of patients who underwent
MD during the study period, we did not conduct a study aiming to compare the surgical
results of MD and FELD. This is another weakness of our study. However, our fairly large
series provides some information to surgeons who want to adopt this technique in their
clinical practice. Despite the lack of Level 1 evidence, we still believe that minimally invasive
lumbar disc surgery will become a better alternative to classical surgical techniques, due to
the aforementioned advantages which, although subjective, may be preferred both by patients
and health insurance systems.
At our institution, we have been operating on lumbar disc herniations using an
endoscopic approach since 2009. Either the lateral TF or IL routes have been used, depending
on the characteristics of each individual case. Due to minimal tissue retraction, the lateral TF
approach is the preferred minimally invasive approach, if possible. However, the TF approach
is not preferred when the sequestering material has migrated beyond the lower edge of the
cranial pedicle or over the middle of the caudal pedicle, or in cases where the neural foramen
MANUSCRIP
T
ACCEPTED
ACCEPTED MANUSCRIPTis overlaid by the iliac crest on lateral plain radiographs. Due to the position of the iliac crest,
most of the L5-S1 herniations (49/52) and approximately half of the herniations at the L4-5
level (49/93) in our series were treated using the IL technique. The cranial or caudal migration
of the sequestering material was more decisive for cases above the L4-5 level.
For neurosurgeons who are experienced in conventional MD, the IL approach is easier
to adopt because of similarities in the anatomic orientation. However, the lateral TF approach
may be more demanding. The initial stage of spinal cannula insertion under fluoroscopy is of
the utmost importance, as it leads the surgeon to the optimal target point. Failures at that stage
may result in improper placement of the endoscope, creating a risk of nerve root injury and
inability to remove the herniated disc. Transforaminal steroid injection is a common method
used in the management of radicular pain. (4) Like several other authors (31), we recommend
that all neurosurgeons who wish to use the TF approach perform transforaminal epidural
steroid injections, due to the similarity between the injection procedure and the initial step of
the TF approach. Another good training opportunity is working on cadavers in order to
improve endoscopic surgical skills.
Another serious complication of the lateral TF approach is visceral organ or vascular
injury. Even minor manipulation failures while using the spinal cannula may cause contact
with the contents of the abdominal organs and, consequently, infections. Psoas abcess and
spondylodiscitis following TF procedures have previously been reported. (27) To avoid these
injuries, abdominal CT scans may assist in the visualization of anatomical structures in order
to calculate a safe entrance trajectory.
MANUSCRIP
T
ACCEPTED
ACCEPTED MANUSCRIPTThe IL approach is similar to conventional MD; however, anatomic orientation can
easily be lost with misplacement of the working sheath. (49) If the sheath is placed too far
laterally or medially, placement confusion may occur, complicating the identification of
anatomic structures and leading to prolonged operation times and iatrogenic injuries.
Additionally, inappropriate manipulation of the neural elements may result in transient or
permanent motor deficits. (49)
Good clinical results have been reported for endoscopic discectomies, even with
various TF and IL approaches, different patient selection criteria, and varying surgical
techniques. (1,8,10,14,19,22,24,25,39-41,47,53-56) The overall success rate for conventional
MD ranges from 75% to 100%. (2,11,13,28,51) In our series, the clinical results are consistent
with previously published data for both endoscopic and MD surgeries. An 85% subjective
patient satisfaction rate 12 months after surgery is a considerably good result, and significant
improvements were achieved in both the VAS and ODI scores.
The rate of recurrences in our series is 3.7%, which is in accordance with previously
published data. (3,6,18,30,46,50) Four of these surgeries were performed via the IL approach.
Generally, recurrences are attributable to the type of herniation and the size of the annular
defect. (5,57) Therefore, surgeons should attempt to avoid enlarging the annular defect. A few
patients (1/2%) experienced residual disc herniations in our series, which may be related to
our lack of experience in the early stages of this study. Both of these surgeries were
performed via the TF approach, and repeat surgeries were also performed using the same
approach. As mentioned above, for the TF approach, free fluctuation of the PLL under
constant irrigation is a good indication of an adequate decompression. The PLL and the
MANUSCRIP
T
ACCEPTED
ACCEPTED MANUSCRIPTepidural space should be explored properly in order not to leave any type of free fragments or
residual herniation behind.
There were 15 complications (9%) in our series, with only one significant major
complication (0.6%). Additional motor deficits occurred in five cases (3%), probably related
to inadequate use of the beveled opening of the endoscope as a nerve root retractor.
Fortunately, in four of these cases, these deficits were only transient, and patients experienced
complete neurological recovery. In only one case did a permanent motor deficit occur. In two
cases with two-level disc herniations, motor deficits occurred postoperatively. In both of these
cases, TF and IL approaches were used in the same session for different disc levels. Five of
the six motor deficits occurred within the first 60 cases of our series, including the case where
a permanent deficit occurred and the cases with two-level disc herniations. We believe that
the prolonged operative times and increased manipulation of the neural elements for multi–
level procedures may cause postoperative motor deficits, and therefore we recommend that
surgeons gain sufficient experience with single-level FELD before attempting to operate on
multi-level disc herniations.
Dysaesthesias were encountered in four cases (2.4%), all of which were approached
with a TF technique. This may be due to the relatively large neural foramen, which allows
limited movement of the endoscope. Repeated manipulations and slight movements may
result in the irritation of the dorsal root ganglion. Dural tears (3%) are another complication
that must be mentioned. All of these surgeries were performed with an IL approach. There
was an open CSF fistula in only one case (0.6%), which was related to our attempt to perform
a dural repair via an open microscopic approach. In the other five cases, no attempt at dural
repair was made; the cases were closed normally, and no open or closed CSF fistulas occurred
MANUSCRIP
T
ACCEPTED
ACCEPTED MANUSCRIPTpostoperatively. The complication rates in our series are higher than those reported in the
series of experienced surgeons. (42) However, our institution had no prior experience with
FELD and most of the complications happened in the early stages of this study. Similar
complication rates have been reported by various surgeons during the initial stages of using
this technique. (20, 29, 49)
As our series demonstrates, attention must be paid, especially in the early stages of
learning this new technique. Inadequate manipulation of nerve roots may result in motor
deficits and dural tears, which are primarily related to adhesions that occur secondary to
chronic herniations. Although dural tears are a major problem in conventional MD, based on
our experience, we believe that open or closed CSF fistulas do not readily occur in FELD,
probably due to the limited access, which is a possible advantage of this technique. We
recommend not attempting dural repair if a dural tear occurs.
Conclusions:
Currently, the goal of surgical treatment for lumbar disc herniations is optimal
decompression with minimal tissue trauma and complication. From this perspective, FELD is
a safe and effective method. Minimal operative trauma and consequent early mobilization and
decreased risk of CSF fistula are the advantages of this method. A steep learning curve and
possible complications are disadvantages. As our clinical experience indicates, despite the
difficulties of learning this new technique, considerably good results may be achieved when
enough experience is gained.
MANUSCRIP
T
ACCEPTED
ACCEPTED MANUSCRIPTReferences:
1. Ahn Y, Lee SH, Park WM, Lee HY, Shin SW, Kang HY. Percutaneous endoscopic lumbar
discectomy for recurrent disc herniation: surgical technique, outcome and prognostic factors
of 43 consecutive cases. Spine 29: 326-332, 2004
2. Andrews DW, Lavyne MH. Retrospective analysis of microsurgical and standart lumbar
discectomy. Spine 15: 329-335, 1990
3. Bover P, Srour R, Buchheit F, Krause D, Alberquerque M. [ Lumbar disc hernia. Excision
of hernia with or without complementary discectomy?] Neurochirurgie 40: 259-262, 1994
(Article in French)
4. Cansever T, Kabatas S, Civelek E, Kircelli A, Yılmaz C, Musluman M, Ofluoglu D, Caner
H. Transforaminal epidural steroid injection via a preganglionic approach for the treatment of
lumbar radicular pain. Turk Neurosurg 22(2): 183-188, 2012
5. Carragee EJ, Han MY, Suen PW, Kim D. Clinical outcomes after lumbar discectomy for
sciatica: the effects of fragment type and anular competence. J Bone Joint Surg Am 85: 102-
108, 2003
6. Carragee EJ, Spinnikie AO, Alamin TF, Paraqioudakis S. A prospective controlled study of
limited versus subtotal posterior discectomy: short term outcomes in patients with herniated
lumbar intervertebral discs and large posterior anular defect. Spine 31: 653-657, 2006
7. Caspar W, Iwa H. A microsurgical operation for lumbar disc herniations. Neurol Surg 6:
657-662, 1979
8. Chiu JC. Evolving transforaminal endoscopic microdecompression for herniated lumbar
discs and spinal stenosis. Surg Tech Int 13. 276-286, 2004
9. Dandy WE. Loose cartilage from intervertebral disc simulating tumor of the spinal cord.
Arch Surg 19: 660-672, 1929

MANUSCRIP
T
ACCEPTED
ACCEPTED MANUSCRIPT10. Destandau J. [Technical features of endoscopic surgery for lumbar disc herniation: 191
patients.] Neurochirurgie 50: 6-10, 2004 (Article in French)
11. Ebeling U, Reichenberg W, Reulen HJ. Results of microsurgical lumbar discectomy.
Review on 485 patients. Acta Neurochir (Wien) 81: 45-42, 1986
12. Fairbank JC, Couper J, Davies JB, O’ Brein JP. The Oswestry low back pain
questionnaire. Physiotherapy 66: 271-273, 1980
13. Ferrer E, Garcia-Bach M, Lopez L, Isamat F. Lumbar microdiscectomy: Analysis of 100
consecutive patients. Acta Neurochir Suppl (Wien) 43: 39-43, 1988
14. Foley KT, Smith MM, Rampersaud YR. Microendoscopic approach to far-lateral lumbar
disc herniation. Neurosurg Focus 7(5): e5, 1999
15. Forst R, Hausmann B. Nucleoplasty- a new examination technique. Arch Orthop Trauma
Surg 101: 219-221, 1983
16. Hermantin FU, Peters T, Quartarato IA, Kambin P. A prospective, randomized study
comparing the results of open discectomy with those of video-assisted arthroscopic
microdiscectomy. J Bone Joint Surg Am 81: 958-965, 1999
17. Hijakata S. Percutaneous nucleotomy. A new concept technique and 12 years’ experience.
Clin Ortop Relat Res 238: 9-23, 1989
18. Hirabayashi S, Kumano K, Ogawa Y, Aota Y, Maehiro S. Microdiscectomy and second
operation for lumbar disc herniation. Spine 18: 2206-2211, 1993
19. Hoogland T, Schubert M, Miklitz B, Ramirez A. Transforaminal posterolateral
endoscopic discectomy with or without the combination of a low-dose Chymopapain: a
prospective randomized study in 280 consecutive cases. Spine 24: 890-897, 2006
20. Kafadar A, Kahraman S, Akboru M. Percutaneous endoscopic transforaminal lumbar
discectomy: A critical appraisal. Minim Invas Neurosurg 49: 74-79, 2006
MANUSCRIP
T
ACCEPTED
ACCEPTED MANUSCRIPT21. Kambin P, Gellman H. Percutaneous lateral discectomy of the lumbar spine: a preliminary
report. Clin Orthop 174: 127-132, 1983
22. Kambin P, Sampson S. Posterolateral suction-excision of herniated lumbar intervertebral
discs: report of interim result. Clin Orthop 207: 37-43, 1986
23. Kambin P. Arthroscopic microdiscectomy. Arthroscopy 8: 287-295, 1992
24. Kambin P, Casey K, O’Brein E, Zhou L. Transforaminal arthroscopic decompression of
the lateral recess stenosis. J Neurosurg 84: 462-467, 1996
25. Kambin P, O’Brein E, Zhou L, Schaffer JL. Arthroscopic microdiscectomy and selective
fragmentectomy. Clin Orthop 347: 150-167, 1998
26. Kim JM, Lee SH, Ahn Y, Yoon DH, Lee CD, Lim ST. Recurrence after successful
percutaneous endoscopic lumbar discectomy. Minim Invas Neurosurg 50: 82-85, 2007
27. Kim WJ, Lim ST, Lee SH. Pyogenic psoas abscess and secondary spondylodiscitis as a
rare complication of percutaneous endoscopic lumbar discectomy: a case report. Joint
Diseases and Related Surgery 16: 163-166, 2005
28. Kotilainen E, Valtonen S. Clinical instability of the lumbar spine after microdiscectomy.
Acta Neurochir (Wien) 125: 120-126, 1993
29. Kuonsongtum V, Paiboonsirijit S, Kesornak W, Chaiyosboorana V, Rukskul P,
Chumnanvej S, Ruetten S. Result of full endoscopic uniportal lumbar discectomy: preliminary
report. J Med Assoc Thai 6: 776-780, 2009
30. Lee DY, Ahn Y, Lee SH. Percutaneous endoscopic lumbar discectomy for adoslescent
lumbar disc herniation: surgical outcomes in 46 consecutive patients. Mt Sinai J Med 73: 864-
870, 2006
31. Lee DY, Lee SH. Learning curve for percutaneous endoscopic lumbar discectomy. Neurol
Med Chir 48: 383-389, 2008
MANUSCRIP
T
ACCEPTED
ACCEPTED MANUSCRIPT32. Lee SH, Kang BU, Ahn Y, Choi G, Choi YG, Ahn KU, Shin SW, Kang HY. Operative
failure of percutaneous endoscopic lumbar discectomy: a radiological analysis of 55 cases.
Spine 31: E285-E290, 2006
33. Mayer HM, Brock M, Berlien HP, Weber B. Percutaneous endoscopic laser discectomy
(PELD). A new surgical technique for non-sequestrated lumbar discs. Acta Neurochir Suppl
(Wien) 54: 53-58, 1992
34. Mixter WJ, Barr JS. Rupture of intervertebral disc with involvement of the spinal canal. N
Eng J Med 211: 210-215, 1934
35. Nellenstejn J, Ostelo R, Bartels R, Peul W, van Royen B, van Tulder M. Transforaminal
endoscopic surgery for symptomatic lumbar disc herniations: a systematic review of the
literature. Eur Spine J 19: 181-204, 2010
36. Oertel JMK, Mondorf Y, Gaab MR. A new endoscopic spine system: the first results with
“Easy GO”. Acta Neurochir (Wien) 151: 1027-1033, 2009
37. Righesso O, Falavigna A, Avanzi O. Comprasion of open discectomy with
microendoscopic discectomy in lumbar disc herniations: results of a randomized controlled
trial. Neurosurgery 61: 545-549, 2007
38. Ruetten S. The full-endoscopic interlaminar approach for lumbar disc herniations. In:
Mayer HM (ed), Minimally Invasive Spine Surgery. Berlin: Springer. 2005, pp: 346-355
39. Ruetten S, Komp M, Godolias G. An extreme lateral access for the surgery of lumbar disc
herniations inside the spinal canal using the full-endoscopic uniportal transforaminal
approach: Technique and prospective results of 463 patients. Spine 30: 2570-2578, 2005
40. Ruetten S, Komp M, Godolias G. A new full-endoscopic technique for the interlaminar
operation of lumbar disc herniations using 6-mm endoscope; Prospective 2-year results of 331
patients. Minim Invas Neurosurg 2: 80-87, 2006
MANUSCRIP
T
ACCEPTED
ACCEPTED MANUSCRIPT41. Ruetten S, Komp M, Merk H, Godolias G. Use of newly developed instruments and
endoscopes: full-endoscopic resection of lumbar disc herniations via the interlaminar
approach. J Neurosurg Spine 6: 521-530, 2007
42. Ruetten S, Komp M, Merk H, Godolias G. Full-endoscopic interlaminar and
transforaminal lumbar discectomy versus conventional microsurgical technique: a prospective
randomized, controlled study. Spine 33: 931-939, 2008
43. Sasani M, Ozer AF, Oktenoglu T, Canbulat N, Sarioglu AC. Percutaneous endoscopic
discectomy for far lateral lumbar disc herniations: prospective study and outcome of 66
patients. Minim Invas Neurosurg 50(2): 91-97, 2007
44. Screiber A, Suezawa Y, Leu H. Does percutaneous nucleotomy with discoscopy replace
conventional discectomy? Eight years of experience and results in treatment of herniated
lumbar disc. Clin Orthop Relat Res 238: 35-42, 1989
45. Schreiber A, Leu H. Percutaneous nucleotomy: technique with discoscopy. Orthopedics
14: 439-444, 1991
46. Stambough JL. Lumbar disc herniation: an analysis of 175 surgically treated cases. J
Spinal Disord 10: 488-492, 1997
47. Tsou PM, Yeung AT. Transforaminal endoscopic decompression for radiculopathy
secondary to intracanal noncontained lumbar disc herniations: outcome and technique. Spine J
2: 41-48, 2002
48. Valls J, Ottolenghi CE, Schajowicz F. Aspiration biopsy in diagnosis of lesions of
vertebral bodies. J Am Med Assoc 136(6): 376-382, 1948
49. Wang B, Lu G, Patel AA, Ren P, Cheng I. An evaluation of the learning curve for a
complex surgical technique: the full endoscopic interlaminar approach for lumbar disc
herniations. Spine J 11: 122-130, 2011
MANUSCRIP
T
ACCEPTED
ACCEPTED MANUSCRIPT50. Wenger M, Mariani L, Kalbarczyk A, Groger U. Long-term outcome of 104 patients after
lumbar sequestrectomy according to Williams. Neurosurgery 49: 329-334, 2001
51. Williams RW. Microlumbar discectomy. A 12-year statisticaal review. Spine 11: 851-852,
1986
52. Yasargil MG. Microsurgical operation for herniated disc. In: Wullenweber R, Brock M,
Hamer J, Klinger M, Spoerri O (eds), Advances in Neurosurgery. Berlin: Springer-Verlag,
1977: pp 81-82
53. Yeung AT. Minimally invasive disc surgery with the Yeung Endoscopic Spine System
(YESS). Surg Tech Int 8: 1-11, 1999
54. Yeung AT. The evolution of percutaneous spinal endoscopy and discectomy: state of the
art. Mt Sinai J Med 67: 327-332, 2000
55. Yeung AT, Tsou PM. Posterolateral endoscopic excision for lumbar disc herniation:
Surgical techniques, outcome and complications in 307 consecutive cases. Spine 27: 722-773,
2002
56. Yeung AT, Yeung CA. Advances in endoscopic disc and spine surgery: foraminal
approach. Surg Tech Int 11. 255-263, 2003
57. Yorimitsu E, Chiba K, Toyama Y, Hirabayashi K. Long-term outcomes of Standard
discectomy for lumbar disc herniation. Spine 26: 652-657, 2001
MANUSCRIP
T
ACCEPTED
ACCEPTED MANUSCRIPTFigure Legends:
Figure 1: CT shows calculations for the entry point and entry trajectory for the TF approach in
order to provide safe access to the L2-3 disc level in a fresh cadaver. (Used with the
permission of Burcu Goker, MD, from her unpublished neurosurgery thesis.)
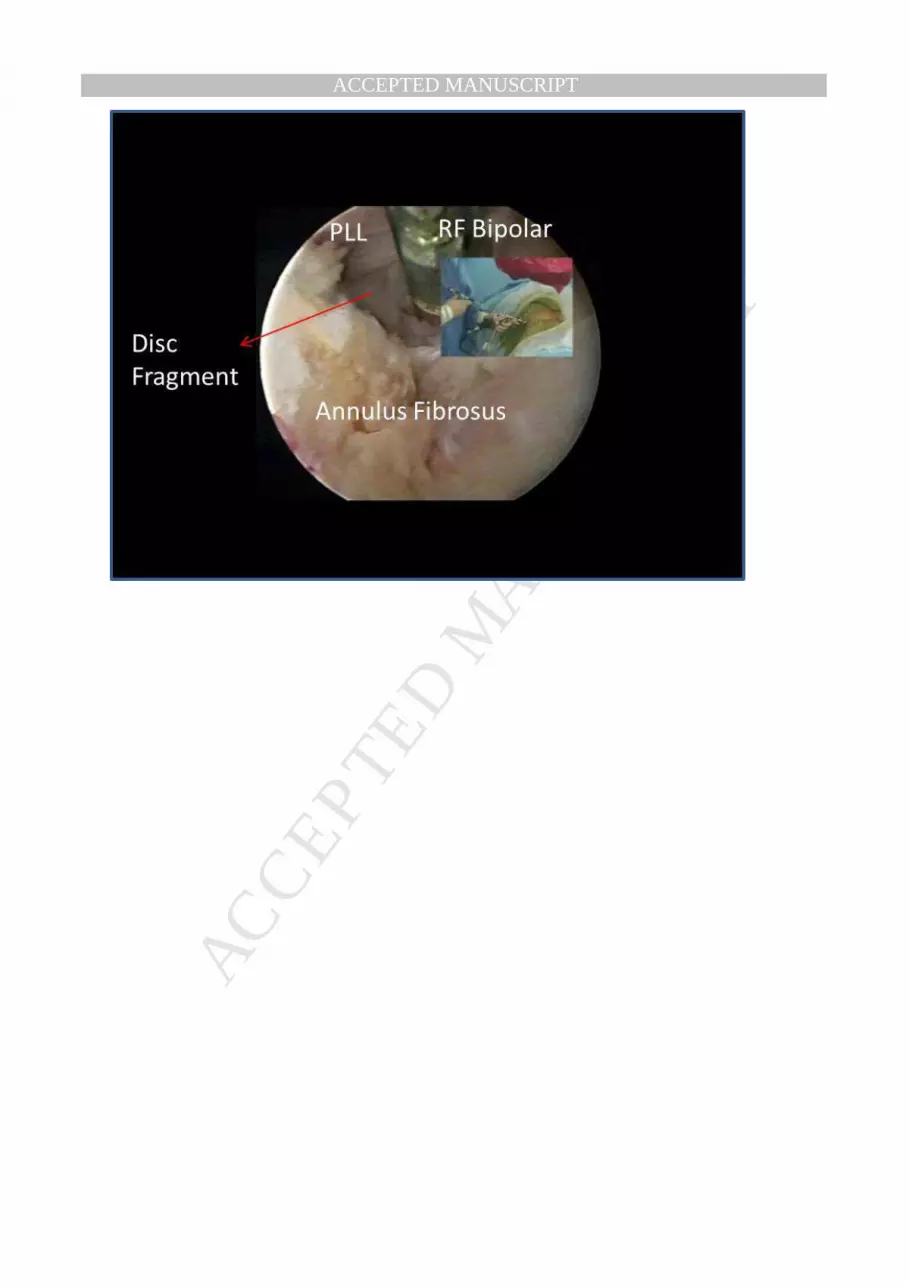
Figure 2: Figure shows the surgeon’s position and the view of the neural foramen from a left
lateral TF approach to the L4-5 disc level. The use of continuous irrigation and RF bipolar
provides a cleaner view (PLL: posterior longitudinal ligament, RF: radiofrequency).
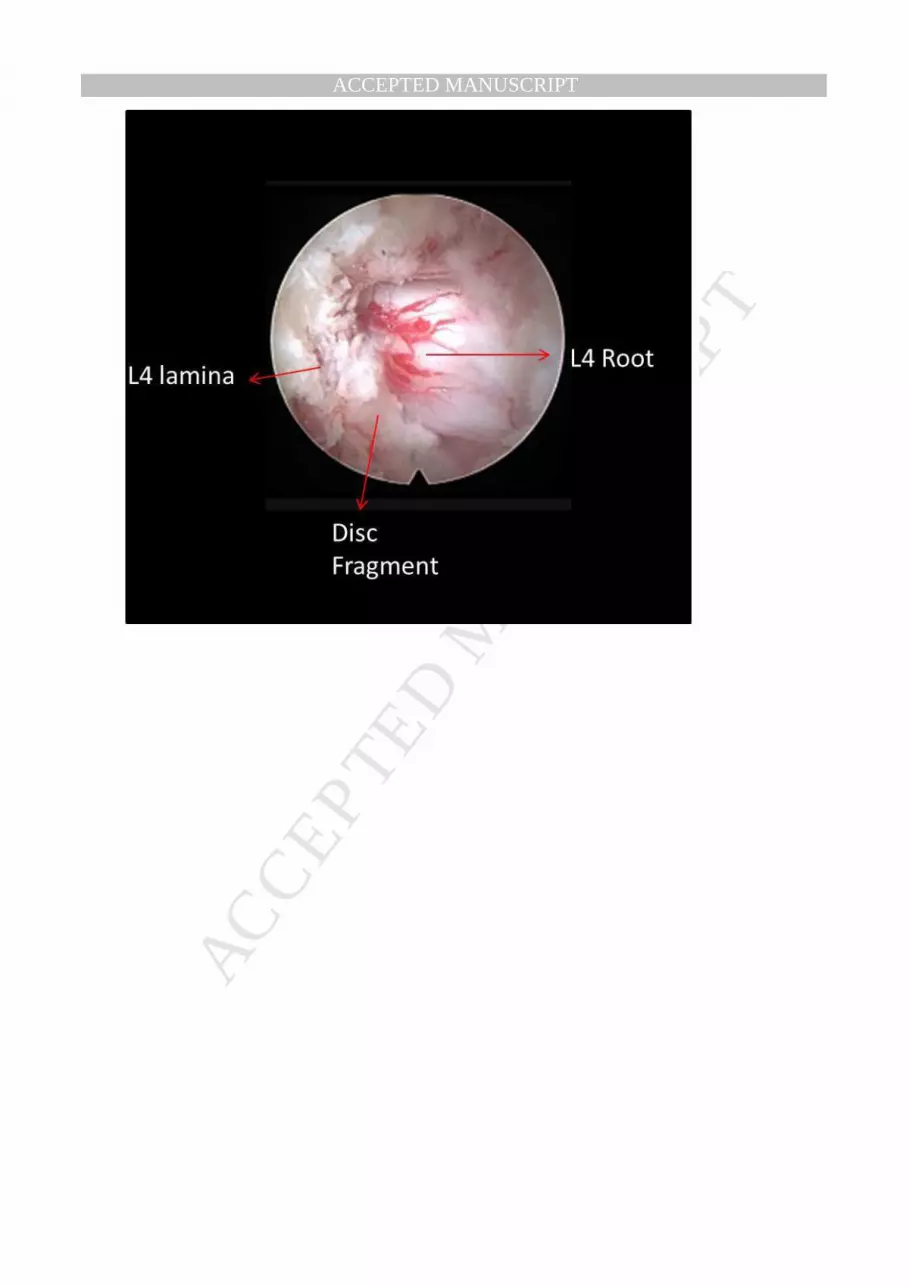
Figure 3: Figure shows the endoscopic view of an IL approach to the L3-4 disc level.
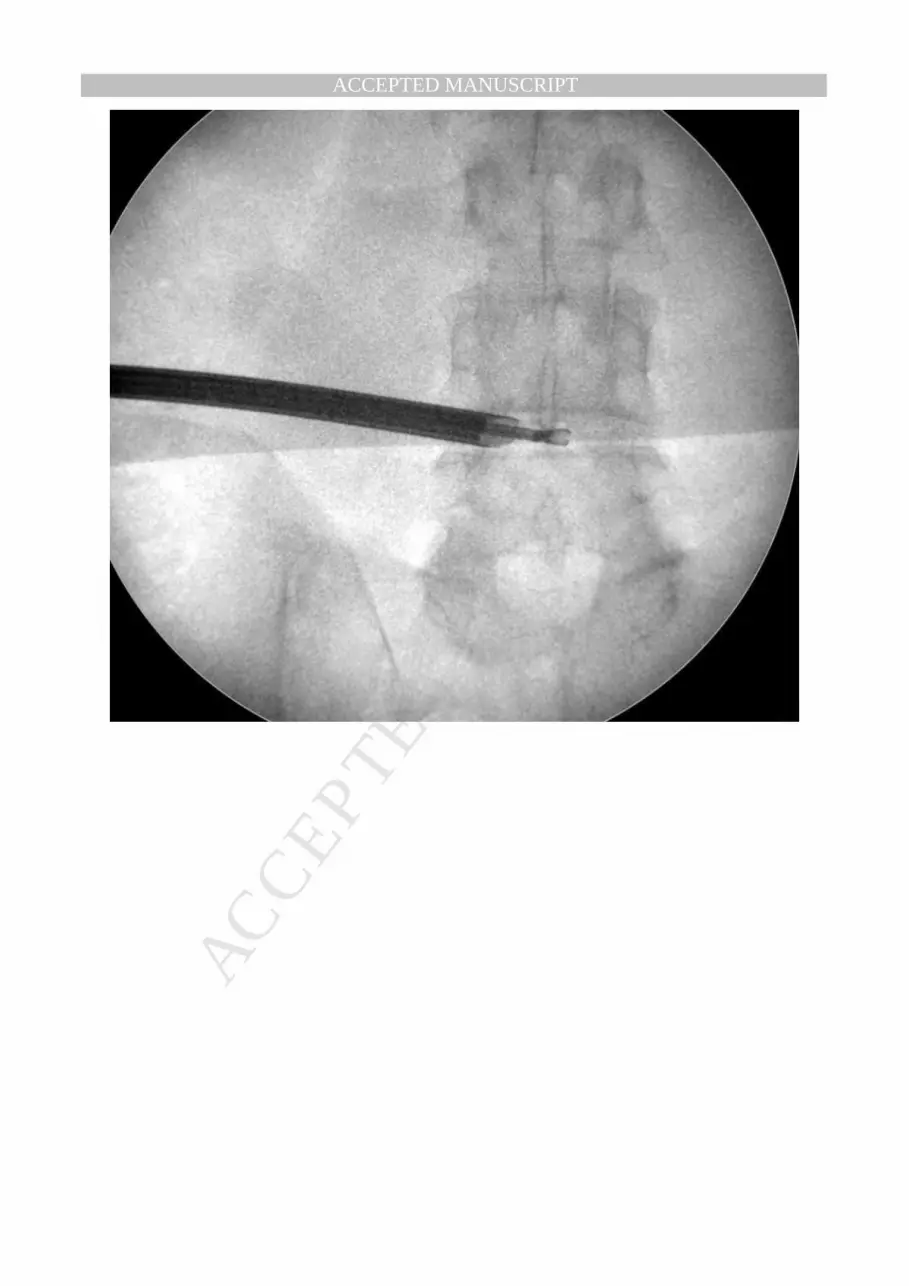
Figure 4a: Usually, only AP fluoroscopic view is used for the TF approach. Figure shows AP
fluoroscopic view of a TF approach to the L4-5 disc level during the disc decompression.
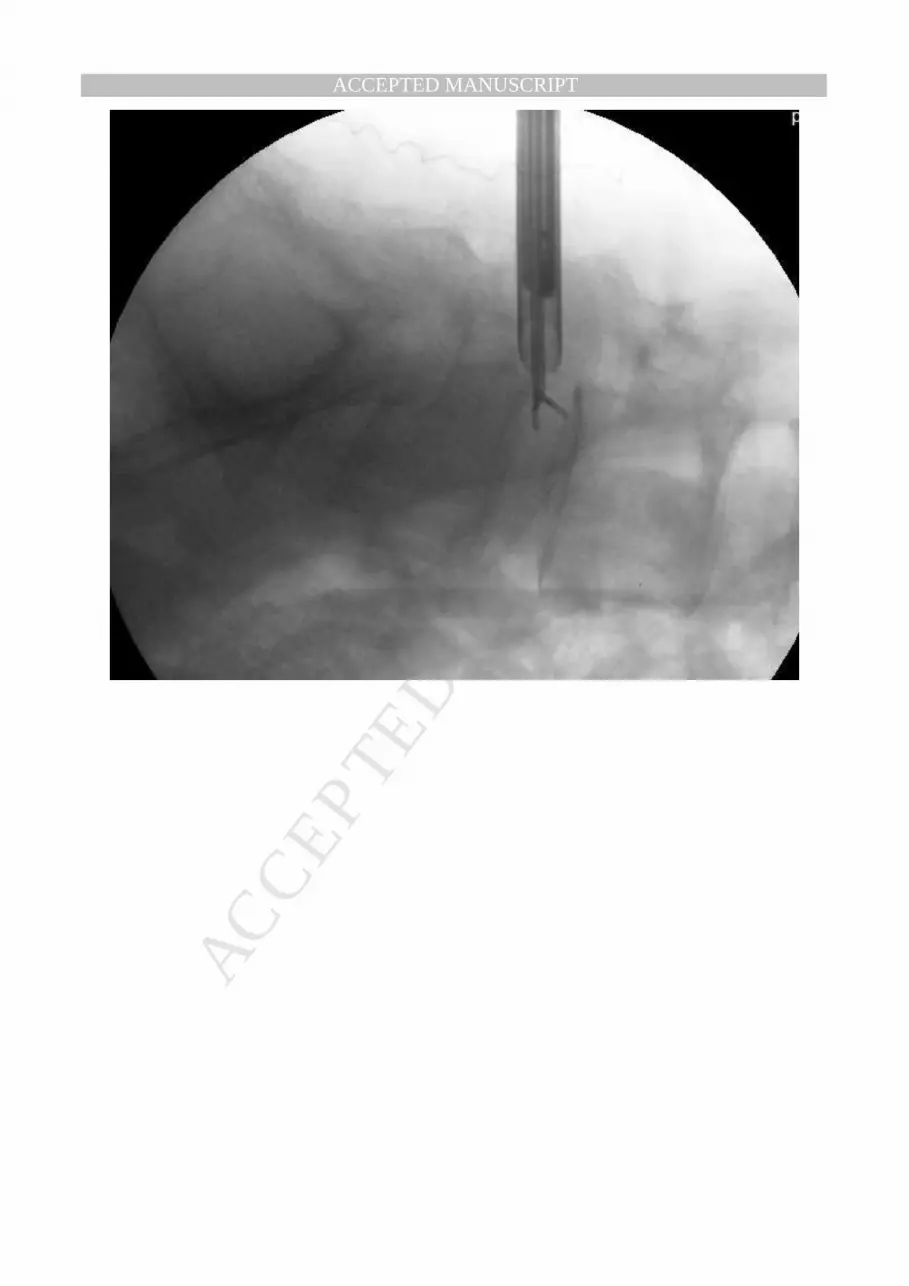
Figure 4b: Only lateral fluoroscopic view is used for the IL approach. Figure shows the
position of the micropunch within the L4-5 level via IL approach.
Figure 5: The bar graph shows the differences between pre- and postoperative ODI and VAS
scores.
Acknowledgments:
We would like to thank our archive officer, Nurcan Uzel, and our clinical secretaries, Kıymet
Gazioglu and Pervin Yuksel, for their help and support.
MANUSCRIP
T
ACCEPTED
ACCEPTED MANUSCRIPT
Table 1
Levels Transforaminal Interlaminar Total
L1 – L2 3 - 3
L2 – L3 7 3 10
L3 – L4 14 3 17
L4 – L5 44 49 93
L5 – S1 3 49 52
Total 71 104 175
MANUSCRIP
T
ACCEPTED
ACCEPTED MANUSCRIPT
Table 2
Ptn
IDEtiology Levels
1st
Op
Time in
btw
2nd
OpOutcome
1 Recurrence L5 - S1 TF 3 months MD Better
2 Residual L4 - L5 TF 1 month TF Better
3 Recurrence L4 - L5 IL 2 months IL Same
4 Recurrence L5 - S1 IL 1 week IL Better
5 Recurrence L5 - S1 IL 1 month IL Same
6 Recurrence L3 - L4 TF 2 months TF Better
7 Recurrence L5 - S1 IL 2 weeks MD Better
8 Residual L4 - L5 TF 1 week TF Same
MANUSCRIP
T
ACCEPTED
ACCEPTED MANUSCRIPT
Table 3. Complications
Complication n %
Motor deficits
Permanent
Transient
1
4
0.6
2.4
Dysesthesia 4 2.4
Dural tear 6 3.6
CSF fistula
1 0.6
MANUSCRIP
T
ACCEPTED
ACCEPTED MANUSCRIPT
MANUSCRIP
T
ACCEPTED
ACCEPTED MANUSCRIPT
MANUSCRIP
T
ACCEPTED
ACCEPTED MANUSCRIPT
MANUSCRIP
T
ACCEPTED
ACCEPTED MANUSCRIPT
MANUSCRIP
T
ACCEPTED
ACCEPTED MANUSCRIPT
MANUSCRIP
T
ACCEPTED
ACCEPTED MANUSCRIPT
8,07
37,04
1,52
7,64
0,00
5,00
10,00
15,00
20,00
25,00
30,00
35,00
40,00
VAS ODI
PreOp
PostOp
Figure 5. Comparison of preoperative and postoperative VAS and ODI values
MANUSCRIP
T
ACCEPTED
ACCEPTED MANUSCRIPTODI: Oswestry disability index
VAS: Visual analog scale
MD: Microdiscectomy
YESS: Yeung Endoscopic Spine System
TF: Transforaminal
IL: Interlaminar
FELD: Full-endoscopic lumbar discectomy
MRI: Magnetic resonance imaging
CT: Computed tomography
PLL: Posterior longitudinal ligament
CSF: Cerebrospinal fluid
Related Documents





![Idiopathic Intracranial Hypertension and the Evaluation of ...Papilledema is the swelling of the optic disc only in the setting of increased intracranial . pressure (ICP) [1]. Swelling](https://static.cupdf.com/doc/110x72/5e638a517c188f5ba85f36a6/idiopathic-intracranial-hypertension-and-the-evaluation-of-papilledema-is-the.jpg)





