Nruropsycholog,a, Vol. 27, No. 3, pp. 353-366. 1989. Prmted in Great Britam. 0028-3932,‘89 S3.00~0 00 \I’ 1989 Pergamon Press plc UNILATERAL ATTENTION DEFICITS AND HEMISPHERIC ASYMMETRIES IN THE CONTROL OF VISUAL ATTENTION ELISABETTA LADAVAS*$, MARIA DEL PESCE~ and LEANDRO PROVINCIALI~ *Dipartimento di Psicologia, Universita di Bologna; and TClinica Neurologica, Universita di Ancona, Italy (Received 11 November 1987; accepted 23 April 1988) Abstract-The present study sought to determine the roles of the two hemispheres in arousal and the selective components ofattention. Ten patients with left and right parietal lesions and ten with left and right temporal lesions participated in the experiment. The hypothesis that posterior parietal lesions, whether left or right, cause two selective attentional deficits, namely, a reduced reactivity to stimuli in the visual field contralateral to the lesion, and a reduced reactivity to any stimulus which occupies a relative contralateral spatial position, was tested by asking the patient to tilt their head either to the left or to the right by 90” and to respond to two stimuli displayed above and on either side of fixation mark. The arousal component of attention was studied by analysing the overall RT to visual stimuli independent of their spatial positions. The results showed that (1) patients with either left or right parietal damage are impaired in shifting attention from the ipsilateral to the contralateral visual field, and, within each visual field, in a direction contraversive to the lesion and (2) these two attentional deficits are more severe after right than after left parietal damage. Furthermore, the results show that the difficulty in maintaining a high level of alertness is a specific deficit of patients with right hemispheric lesion and not of patients with an extinction syndrome, insofar as there is no significant difference in overall RT between patients with parietal and temporal lesions. INTRODUCTION THE AIM of this paper is to investigate the nature of the attentional impairment in patients with an extinction syndrome, as well as the role of the two hemispheres in sustaining attentional activities. Two main components of attention have been considered in the present study: arousal or alertness, e.g. the physiological readiness to respond to external and internal stimuli, and selective visual attention, e.g. the capacity to orient visual attention towards a relevant location in space. In the neuropsychological literature different theories have considered these components of attention in order to explain the hemi-inattention deficits shown by patients with parietal damage. One theory proposes that the deficit concerns the intensive aspects of attention, i.e. the arousal mechanisms [lo, 111. According to this theory each side ofthe brain contains its own activating system. When this system is destroyed half of the brain cannot properly process the incoming sensory information and organize the appropriate motor responses to it. Such a unilateral decrease in arousal is thought to result in the selective loss of the orienting response to the space contralateral to the lesion, since it is assumed that each cerebral hemisphere fCorrespondence to be addressed to: Elisabetta LBdavas, Dipartimento di Psicologia, Viale Berti Pichat 5, Bologna, Italy. 353

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

Nruropsycholog,a, Vol. 27, No. 3, pp. 353-366. 1989. Prmted in Great Britam.
0028-3932,‘89 S3.00~0 00 \I’ 1989 Pergamon Press plc
UNILATERAL ATTENTION DEFICITS AND HEMISPHERIC ASYMMETRIES IN THE CONTROL OF VISUAL ATTENTION
ELISABETTA LADAVAS*$, MARIA DEL PESCE~ and LEANDRO PROVINCIALI~
*Dipartimento di Psicologia, Universita di Bologna; and TClinica Neurologica, Universita di Ancona, Italy
(Received 11 November 1987; accepted 23 April 1988)
Abstract-The present study sought to determine the roles of the two hemispheres in arousal and the selective components ofattention. Ten patients with left and right parietal lesions and ten with left and right temporal lesions participated in the experiment. The hypothesis that posterior parietal lesions, whether left or right, cause two selective attentional deficits, namely, a reduced reactivity to stimuli in the visual field contralateral to the lesion, and a reduced reactivity to any stimulus which occupies a relative contralateral spatial position, was tested by asking the patient to tilt their head either to the left or to the right by 90” and to respond to two stimuli displayed above and on either side of fixation mark. The arousal component of attention was studied by analysing the overall RT to visual stimuli independent of their spatial positions. The results showed that (1) patients with either left or right parietal damage are impaired in shifting attention from the ipsilateral to the contralateral visual field, and, within each visual field, in a direction contraversive to the lesion and (2) these two attentional deficits are more severe after right than after left parietal damage. Furthermore, the results show that the difficulty in maintaining a high level of alertness is a specific deficit of patients with right hemispheric lesion and not of patients with an extinction syndrome, insofar as there is no significant difference in overall RT between patients with parietal and temporal lesions.
INTRODUCTION
THE AIM of this paper is to investigate the nature of the attentional impairment in patients with an extinction syndrome, as well as the role of the two hemispheres in sustaining attentional activities. Two main components of attention have been considered in the present study: arousal or alertness, e.g. the physiological readiness to respond to external and internal stimuli, and selective visual attention, e.g. the capacity to orient visual attention towards a relevant location in space. In the neuropsychological literature different theories have considered these components of attention in order to explain the hemi-inattention deficits shown by patients with parietal damage.
One theory proposes that the deficit concerns the intensive aspects of attention, i.e. the arousal mechanisms [lo, 111. According to this theory each side ofthe brain contains its own activating system. When this system is destroyed half of the brain cannot properly process the incoming sensory information and organize the appropriate motor responses to it. Such a unilateral decrease in arousal is thought to result in the selective loss of the orienting response to the space contralateral to the lesion, since it is assumed that each cerebral hemisphere
fCorrespondence to be addressed to: Elisabetta LBdavas, Dipartimento di Psicologia, Viale Berti Pichat 5, Bologna, Italy.
353

354 ELISAHETTA L~AVAS, MARIA DEL PESCF and LEANDRCI PROVINCIALI
subserves orienting responses to the opposite halfspace. However, in order to explain the fact that neglect occurs more frequently following right than left hemisphere lesions [6, 7, 201, HEILMAN and VAN DEN ABELL [lo, 111 further assume that the left hemisphere only controls orienting to the right side of space, whereas the right hemisphere can produce orienting to both sides. Thus, the etfect of a left hemisphere lesion on orienting can be compensated for by the right hemisphere, whereas a right hemisphere lesion limits orienting response to the right space under the control of the left hemisphere.
Other theories explain the hemi-inattention syndrome as a deficit of the selective attention mechanisms which direct attention to various portions of space according to internal needs or in response to external stimuli [3, 19,23, 241. Selective attention theories propose that the deficit is due to a lesion of a single cerebral attentional mechanism, either localized in a particular brain area or distributed in various cortical areas and subcortical centres 17, 191, or to a lesion of different circuits which contribute to organizing movements toward a certain part of space [25, 261. The selective attention theories seem to provide a more straightforward explanation of the spatial features of hemi-inattention (e.g. dissociations between attentional deficits for personal and extrapersonal space, for the horizontal versus the vertical dimension) than the intensive attention theory (for review, see 1251). But, even if disturbances of activation/arousal alone may be insufficient to explain the spatial features of the hemi-inattention syndrome, they can account for the greater frequency of left than right hemi-inattentive deficits, if we assume that the right hemisphere is specialized for the arousal component of attention. It seems possible that the decrease in general arousal, typical of right hemisphere lesions [7, 8, 9, 121, may also be responsible for the higher incidence and the greater severity of hemi-inattention after right-hemispheric lesions [7, 201.
In order to assess the roles played by the two hemispheres in mediating arousal and the selective components of attention, we tested the ability of patients with left and right parietal lesions to attend to visuai stimuli, and compared these results with those of patients with left and right temporal lesions. The selective component of attention was studied by replicating a recent study by L~DAVAS 1161, where it was shown that patients with right parietal lesions were impaired in directing attention in space according to both the retinal and the physical frame of reference. By asking the patients to turn the head to the left and to the right by 90” [l, 21, the two different systems are dissociated, and therefore it is possible to determine which of the two systems is disturbed by parietal lobe damage. That study showed that when two visual stimuli are presented to one or the other visual field, the stimulus occupying a right position yields faster RTs than the left stimulus in both visual fields, and that responses to LVF stimuli are slower than responses to RVF stimuli. Therefore, that study suggested that the reduced ability to shift attention from one spatial location to another is tied to both gravitational and retinotopic coordinates and that right parietal damage produces deficits in both systems of coordinates.
The present study asks whether these deficits are specific of patients with right parietal damage, or whether symmetric deficits, opposite in sign, can be obtained in patients with left parietal damage. If the two hemispheres exhibit a selective attentional control which is equal in strength, but opposite in sign, we should expect the following results: (I ) in patients with left parietal lesions RTs to RVF stimuli should be shorter than RTs to LVF stimuli, and in each head-tilted condition RTs to stimuli which occupy a right position should be slower than RTs to stimuli which occupy a left position; and (2) those deficits should be comparable in magnitude. though opposite in direction, to those following right parietal lesions.
The arousal component of attention in hemi-inattentive patients was studied by

UNILATERAL ATTENTlON DEFICITS AND HEMISPHERIC ASYMMETRIES IN THE CONTROL OF WSUAL ATTENTION 355
considering the overall reaction time to visual stimuli independent of their spatial positions. More precisely, if the arousal component of attention plays a specific role in determining hemi-inattention, we should expect longer RTs in groups of patients with hemi-inattention (patients with left and right parietal lesions) compared with patients without hemi- inattention (patients with left and right temporal lesions).
METHOD
Subjrcts
A total of 20 patients with CT-confirmed unilateral lesions involving the right or left parietal lobe and the right or left temporal lobe (see Table 1) participated in this study. There were five patients in each of the four groups resulting from the combinations between site and side of the lesion. The average size of the lesions, measured by a special CT scan program, did not vary between left and right parietal, as well as between left and right temporal lesions.
Table 1. Summary of clinical data for patients with parietal and temporal damage
Case Age Sex Hand Onset of illness CT scan
PRl 60 PR2 67 PR3 60 PR4 60 PR5 42
PLl 49 PL2 62 PL3 56 PL4 65 PL5 58
TRl 48 TR2 72 TR3 68 TR4 54 TR5 60
TLl 52 TL2 61 TL3 54 TL4 43 TL5 56
F M F M M
F M M F M
F F M M F
M M M F F
R R R R R
R R R R R
R R R R R
R R R R R
4 yr 3 yr 2 mth 4 mth 3 mth
3 yr 3 mth 10 yr 3 mth 3 mth
1 mth 6 mth 2 mth
5 yr 1 mth
5 mth 9 mth 1 mth
9 yr 3 mth
R parietal infarct R fronto-parictal infarct R parietal infarct R fronto-parietal infarct R posterior parietal tumour
L fronto-parietal tumour L parietal tumour L parietal infarct L parietal infarct L parietal infarct
R temporal infarct R posterior-temporal infarct R temporal infarct R temporal infarct R temporal infarct
L anterior-temporal infarct L temporal infarct L temporal infarct L temporal infarct L temporal glyoma
The patients with parietal lesions extinguished to double simultaneous visual stimulation (see below for the description of the test used for the selection of patients with extinction), and none displayed evidence of neglect, visual impairment, receptive or expressive language disturbance. The patients with temporal lesions did not show any evidence of extinction or neglect and visual impairment, and only two patients out of ten had a mild expressive language disorder. The presence/absence of neglect was tested in a task requiring the crossing out of circles symmetrically arranged around a central circle [41, and in a wide range of tests, including drawing from memory, copying and reading. The presence/absence of visual impairment was detected by campimetry and visual acuity evaluation and this selection defined a group of patients whose cerebral lesions were limited to cortical lesions saving the optic radiation. The presence/absence of language disturbance was tested by the Token test. Furthermore, patients with parietal lesions showed a contralateral hemiplegia or a severe hemiparesis, whereas patients with temporal lesions showed only a light contralateral hypereflexia with or without hemihypoesthesia.
Apparatus
Stimuli were generated by an Apple II microprocessor and displayed on a 15 in. video monitor. For experimental trials, a button response box was fixed to a table under the subject’s hand (right for the right damaged patients and left for the left damaged patients) and connected to the computer. The computer recorded responses and response latencies, and stored these data on a magnetic disk for subsequent analysis. All displays were viewed from a distance

356 ELISAB~TTA L~AVAS, MARIA DEL PESCE and LEANERS PK~VINCIALI
of 40 cm under normal room illumination. Eye movements were monitored by the experimenter throughout the expertmental session.
EXTINCTION TEST Prior to the experiment, the presence of visual extinction was assessed for each subject. The computer-controlled
visual display for this purpose consisted of four 2.5 ‘/side squares forming the four corners of an imaginary 12,5”/side square around a central fixation point. A trial began with a continuously displayed central fixation stimulus followed by the presentation of one of three possible stimulus conditions; either two x’s were briefly displayed centred in two of the squares, or one x was displayed, or no x’s were displayed. A tone sounded immediately afterwards, and the subject was required to indicate, by pointing with the index finger of the hand ipsilateral to the lesion, which of the squares had contained an “x”. Each ‘ix” subtended 0.6 x 1.2’ of visual angle and was displayed for 75 msec.
The extinction test consisted of96 trials: 24 trials in which a single stimulus was presented six times in each of the four squares: 48 trials in which two stimuli were presented simultaneously, equally distributed across each of the six possible between-and within--field combinations; and 24 trials in which no stimulus appeared (catch trials). All patients with parietal damage who participated in the study omitted more than 20% of the stimuli on the side contralateral to the lesion on between-field double presentations, and less than 5% of the stimuli on the side contralateral to the lesion on a single stimulus presentation. On the contrary, they consistently detected single stimuli or within-fields stimuli in the ipsilateral visual field. Patients with temporal lobe damage performed this test without omissions.
(‘onditiom und procedure
The experiment comprised three conditions of head position: upright position (Condition I), head and sagittal midplane of the trunk tilted to the left (Condition 2) or to the right (Condition 3) by 90 and 40”, respectively. In the head tilted condition the head rested on a horizontal wooden board. At the patient’s requests the session could be interrupted for allowing him or her to resume a comfortable posture for a few minutes rest. Each condition consisted of a continuously displayed central fixation stimulus and two horizontally aligned 2.5”/side squares. In all Conditions the squares were displayed symmetrically along a horizontal line, 9” above and lo” on either side of fixation mark. When the head was tilted to the left, the left stimulus was in the upper RVF and the right stimulus in the lower RVF, whereas when the head was tilted to the right, the left stimulus was in the lower LVF and the right stimulus was in the upper LVF.
Each trial began with the instruction to look at the fixation stimulus. Eye movements were monitored by the experimenter who sat in front of the patient in an advantageous position for the detection of eye movements. The patient was aware that the experimenter was monitoring eye movements and he/she was instructed to look at the fixation stimulus whenever an eye shift occurred. When accurate fixation was established, the experimenter initiated the trial from the Apple keyboard, a 100 or 300 or 500 msec variable delay elapsed, and a target “x” appeared centred in one of the squares for 100 msec. Trials in which eye movements occurred were omitted from the analysis but not replaced. The subject was instructed to push the response button upon the appearance of the “X”, independent of its position in the visual field. The order of conditions for each subject was randomized, and the sequences were different for each subject. Reaction times (RTs) were measured from the onset of the stimulus to the appropriate key press.
Each subject attended three experimental sessions that were run on consecutive days. Each session consisted of three blocks (one for each condition) of 30 practice trials and three blocks of 100 experimental trials, with a 20-min rest period bctwccn blocks. The sequence was such that left and right target stimuli were equiprobable, with the restriction that no more than three consecutive right or left stimuli could occur. The subjects were not aware of the run length restriction.
RESULTS
Only RTs between 100 msec and 1500 msec were included in the analysis. Trials in which reaction times fell within this range, but an eye movement occurred, were omitted from the analysis.
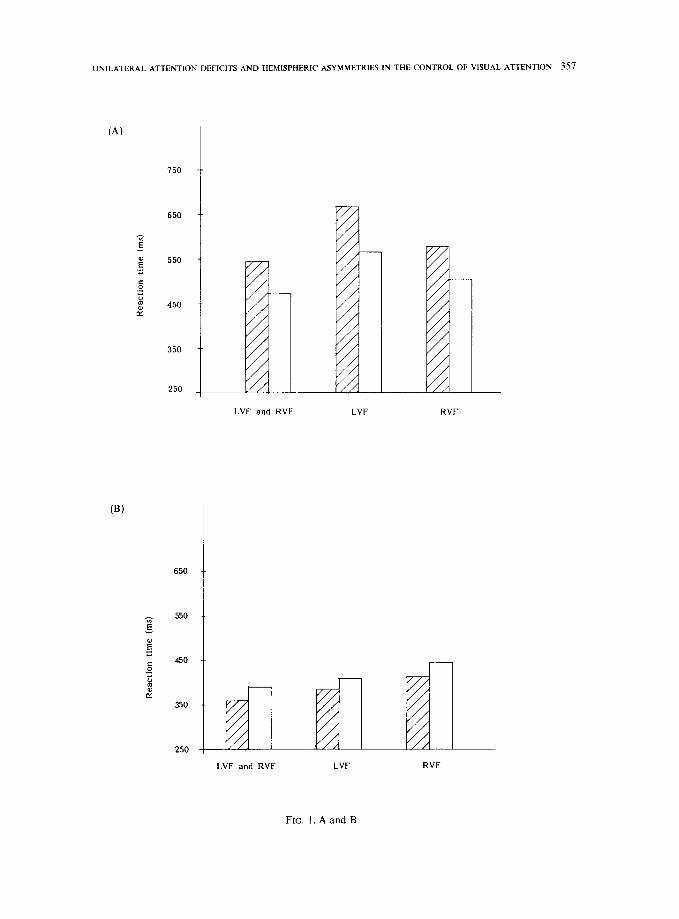
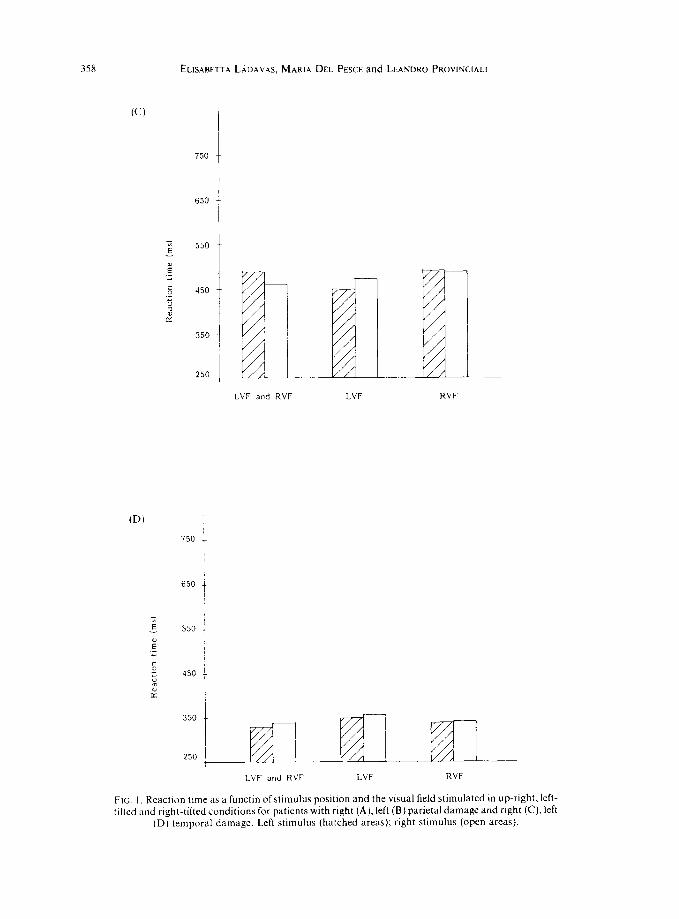
Figure 1 shows the average RTs for each of the three conditions for patients with right and left parietal damage (Fig. lA, B, respectively) and right and left temporal damage (Fig. 1 C, D, respectively).
The mean RTs for each subject and for each condition were submitted to an analysis of variance with repeated measures using group (right parietal, left parietal, right temporal and left temporal) as a between-subjects factor and Condition (upright, left tilted, right tilted) and
UNILATERAL ATTENTION DEFICIT’S AND HEMISPHERIC ASYMMETRIES IN THE CONTROL OF VISUAL ATTENTION 357
(A)
(B)
750
650 1
B 550 ._ Y
5 ._ ; : 450 z
350
250 L
LVF and RVF LVF RVF
LVF and RVF LVF RVF
FIG. l.AandB
358 ELISABETTA L~AVAS, MARIA DEL PESCE and LEAWKO PROVINCIALI
750
650
-z E 550
E” ._
5 450
G ; c:
350
250
c / IdIt p LVF and RVF LVF
750 ;
I
650 ;
-1 /
LVF and RVF LVF RVF
FIG. I. React1011 tlmr as a functin of stimulus position and the visual field stimulated m up-right, left- tilted and right-tilted conditions for patients with right (A), left (B) parietal damage and right (C), left
(D) temporal damage. Left stimulus (hatched areas); right stimulus (open arcas).
UNILATERAL ATTENTION DEFICITS AND HEMISPHERIC ASYMMETRIES IN THE CONTROL OF VISUAL ATTENTION 359
Stimulus Position (left and right) as within-subjects factors. The analysis revealed a significant main effect of group [F (3, 16)= 7.57, P<O.O05]. When the four groups were compared according to the side of the lesion on overall reaction time, independent of the visual field stimulated and the relative position of the stimuli, the results showed that the slowest group was the right parietal group (555 msec; SD = 165) followed by the right temporal (475 msec; SD = 166), left parietal (400 msec; SD = 102) and left temporal (342 msec; SD = 98) groups. The right parietal group did not differ significantly from the right temporal group and the left parietal group did not differ significantly from the left temporal group. On the contrary, when we compared the results of patients with right and left parietal lesions, the 155 msec difference was significant [t (8) = 2.34, PC 0.051, as was the 133 msec difference between patients with right and left temporal lesions [t (8)=4.82. P<O.Ol]. After collapsing RTs across sides of lesion, the difference between parietal and temporal patients (468 msec vs 408 msec) became insignificant; and after collapsing RTs across sites of the lesion, the combined right group (516 msec) was found to be significantly slower than the combined left group (372 msec) [t (18)=3.83, P<O.Ol]. The between- subjects factors Condition and Stimulus Position were not significant.
The interaction between Group and Condition was significant [F (6, 32) = 3.90, P< 0.011. When RTs for the stimulus position within each visual field were combined, independent of the distinction between right and left stimulus, the results showed that in patients with parietal damage RTs to stimuli presented to the visual field ipsilateral to the lesion were faster than RTs to the contralateral visual field stimuli, whereas in patients with temporal damage there was no significant difference between RTs to ipsilateral and contralateral visual fields. In right parietal patients the average RT to RVF stimuli (540 msec; SD= 138, left tilted condition) was 76 msec faster than RTs to LVF stimuli (616 msec; SD= 133, right tilted condition) [t (4) = 2.78, P-C 0.05]. In left parietal patients RT to LVF (397 msec; SD = 106, right tilted condition) was 32 msec faster than RT to RVF (429 msec; SD= 141, left tilted condition) [t (4)=2.78, P<O.O5]. Moreover, in both parietal groups Condition 1 yielded faster RT than Condition 2 (left tilted condition) and 3 (right tilted condition) (P < 0.05 in all comparisons). This effect can be explained by considering that patients with parietal lesions had hemiplegia and therefore they found the head tilted conditions more uncomfortable than the upright tilted condition. A different pattern of results appeared in the temporal damaged patients when we compared RTs of Condition 2 and Condition 3. In left temporal patients RTs to RVF (339 msec; SD =97) were 13 msec faster than RTs to LVF stimuli (352 msec; SD = 109). In right temporal patients RTs to LVF (460 msec; SD = 170) were 27 msec faster than RTs to RVF stimuli (487 msec; SD= 160). None of these differences was significant.
Finally, the interaction between Group and Stimulus Position was significant [F (3, 16)= 19.69, P<O.OOl]. Patients with right parietal lesions were faster in responding to the right stimulus (514 msec, SD= 182) than to the left stimulus (596 msec; SD= 145) [t (4)= 5.46, P<O.Ol] in both visual fields, whereas patients with left parietal lesion were faster in responding to the left stimulus (386 msec; SD= 155) than to the right stimulus (415 msec; SD= 124) [t (4)=4.46, P<O.O2]. On the contrary, patients with left and right temporal lesions showed no significant difference between RTs to left and right stimuli. In patients with right temporal lesions, RTs to left and right stimuli were 474 msec and 475 msec respectively, whereas in patients with left temporal lesions RTs to left stimuli were 338 msec and to right stimuli were 345 msec.
Moreover, in patients with visual extinction, the difference between RT to left and right stimuli was larger in right than in left parietal patients. When we compared the difference

360 ELISABETTA LADAVAS, MARIA DEL PESCE and LEANDRO PROVINCIALI
between RT to left and right stimuli both in LVF (Condition 2) and in RVF (Condition 3) we found that the difference was larger in right than in left parietal damaged patients (88 msec vs 27 msec, respectively) [t (18)=2.75, P-cO.021.
The advantage of the stimulus ipsilateral to the lesion found in patients with parietal damage was present in all experimental conditions. In patients with right parietal damage, when the two target stimuli were presented to different hemifields (Condition 1 ), the average RT to the right stimulus (473 msec; SD= 144) was 71 msec faster than that to the left stimulus (544 msec: SD = 115) [t (4) = 7.52, P<O.Ol]. Similarly, when both stimuli appeared in the LVF (Condition 2) the difference between RTs to right (565 msec; SD = 215) and left (667 msec; SD= 129) stimuli was 102 msec [t (4)=3.42, P<O.O5]. When they appeared in the RVF (Condition 3) the difference between RTs to right (502 msec; SD= 188) and left (577 msec; SD = 191) stimuli was 75 msec [t (4)= 2.78, PcO.051. All patients showed this pattern of results.
Patients with left parietal damage showed a mirror-symmetrical pattern of results, e.g. RT to left stimulus was faster than RT to right stimulus, in all experimental conditions. In Condition 1, RT to LVF stimuli (359 msec; SD = 72) was 32 msec faster than RT to RVF stimuli (391 msec; SD=l20) [t (4)=4.53, P<O.O2]. Similarly, when both stimuli were presented in the LVF (Condition 2) RTs to left stimuli (385 msec; SD= 100) were 24 msec faster than RTs to right stimuli (409 msec; SD= 110) [t (4)= 3.03, P<O.O5]. When both stimuli were presented to RVF (Condition 3), RT to left stimuli (413 msec; SD = 139) was 31 msec faster than RT to right stimuli (444 msec; SD= 144) [t (4)= 3.47, PcO.051. All patients showed this pattern of results.
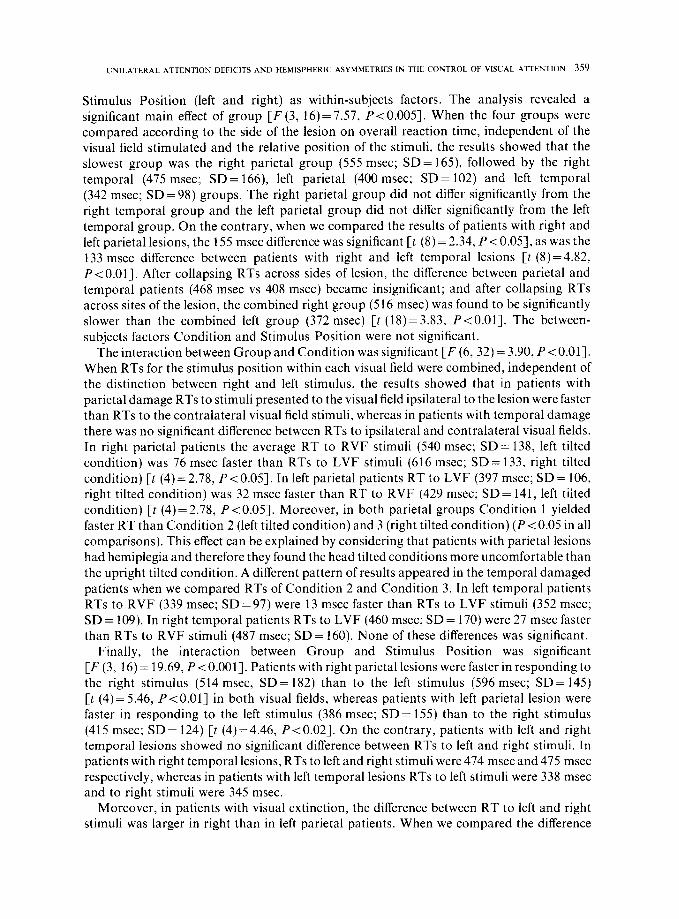
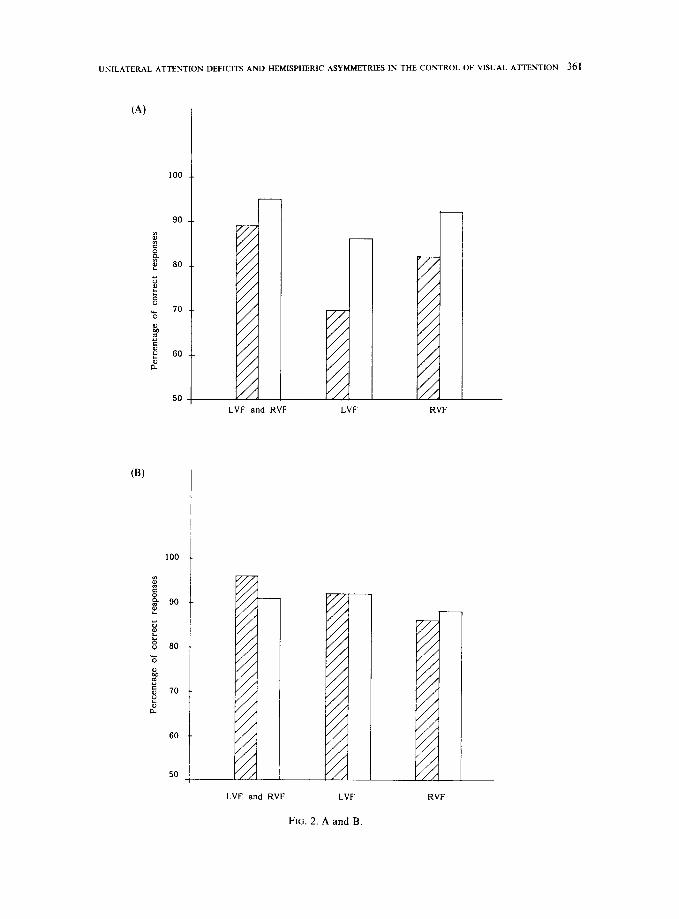
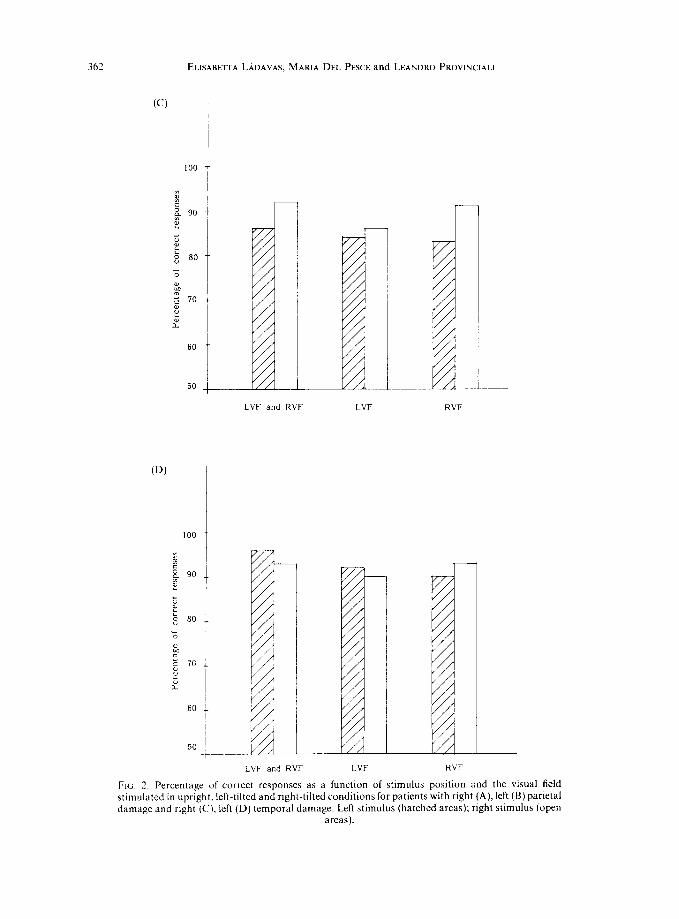
A similar analysis of variance was carried out on the arc-sine transformations of percentages of correct responses. “Incorrect” trials were those in which a response occurred, but RT exceeded 1500 .msec and those in which the subject failed to respond or anticipated the target. The last two types of errors were very rare and did not exceed 2% of trials. These data are depicted graphically in Fig. 2 for each of the three conditions for right and left parietal damaged patients (Fig. 2A, B, respectively) and for right and left temporal damaged patients (Fig. 2C, D, respectively).
The analysis of variance showed only one interesting significant effect, the interaction between Group and Stimulus Position [F (3, 16)=6.2 P<O.Ol], due to the difference in accuracy between responses to ipsilateral and contralateral stimulus positions. In patients with right parietal damage the responses to left stimuli were less accurate than to right stimuli both across (81% vs 92%, respectively) [t (14)=6.50, P<O.OOl] and within conditions [P<O.O5, in all conditions]. The same pattern of results was obtained in patients with right temporal damage, where responses to left stimuli were less accurate than to right stimuli (84 vs 90%) respectively) [t (14) = 2.97, P < 0.011. However, in this group the left-right difference was significant only in Condition 1 [t (4)=4, 22, Pt0.021, because in Conditions 2 and 3 the difference was not significant. On the contrary, in patients with left temporal and parietal damage the difference in favour of the ipsilateral stimulus position was not significant.
DISCUSSION
Attentional deficits following brain damage can be ascribed to impairments of general alerting and arousal functions or to failures of the mechanisms which control orienting and selective attention (see [22] for a recent review). The present experiment has possibly borne out a double dissociation of attentional deficits between left and right hemisphere lesions on
UNILATERAL ATTENTION DEFICITS AND HEMISPHERIC ASYMMETRIES IN THE CONTROL OF VISUAL ATTENTION 361
100
90
50
(B)
60
LVF and RVF LVF
LVF and RVF LVF
FIG. 2. A and B.
RVF
RVF
362 ELHABETTA LADAVAS, MARIA DEL PESCE and LEANDRO PROWNC~AIJ
CD)
100
60
50
f
t
i-
1
L
LVF and RVF LVF RVF
LVF and RVF LVF
FIG. 2. Percentage of correct responses as a [unction of stimulus position and the visual field stimulated in upright, left-tilted and right-tilted conditions for patients with right (A), left (B) parietal damage and right (C), left (D) temporal damage. Left stimulus (hatched areas); right stimulus (open
areas).
UNILATERAL ATTENTION DEFICITS AND HEMISPHERIC ASYMMETRIES IN THE CONTROL OF VISUAL ATTENTION 363
one side, and parietal and temporal lesions on the other. Patients with right hemisphere lesions, whether parietal or temporal, showed an overall increase in reaction time which is best attributed to a disruption of arousal mechanisms localized to this hemisphere [7,9, 10, 11, 133. Patients with parietal lesions, whether right or left, and visual extinction on double stimulation showed direction selective reaction-time effects which were most probably the result of a malfunctioning of some mechanism for selective attention and orienting.
It is known from many clinical investigations [3, 14, 16, 18,22,23,25] that patients with posterior parietal damage in the right hemisphere are frequently affected by deficits in the spatial distribution of attention. By using the reaction-time method two recent studies [16, 241 have shown that right parietal lesions cause difficulties in attending not only to stimulus locations in the visual field contralateral to the lesion (i.e. the left visual field), but also to stimuli which occupy a relative left position in the right visual field. Further, these deficits suggest that “left” and “right” are coded in bodycentric or gravitational in addition to oculocentric or headcentric coordinates, since attention to stimulus locations on the gravitational left is deficient even when the head is tilted to one side and the stimuli are projected to the upper and lower hemiretinae [ 161.
The present reaction-time study has confirmed these results in patients with right parietal lesions and has extended them to patients with left parietal lesions. The latter patients exhibited a reduced speed of reaction both to stimuli in the right visual field and to stimuli occupying a relative right position in the retinotopic as well as in the gravitational frame of reference. No asymmetries in reaction time to the right and left visual fields and to right and left stimulus positions were seen in patients with right or left temporal lesions tested under comparable conditions, suggesting a specific role of unilateral parietal damage in producing such asymmetries.
RIZZOLATTI et al. [26] have reported right-left asymmetries in visual attention in monkeys after unilateral frontal lesions. These asymmetries were similar to those observed in the patients with parietal lesions of this study insofar as reactions to stimuli on the same side as the lesion (ipsilesional stimuli) were faster than reactions to contralesional stimuli, regardless of whether the stimuli were presented in the half field ipsilateral or contralateral to the lesion. RIZZOLATTI et al. [26] have interpreted these deficits in terms of a partial representation of each half of the visual field in attentional areas of both cerebral hemisphere and a gradient of the strength of representation of the whole attentional field in each hemisphere going from a maximum in the extreme contralesional field to a minimum in the extreme ipsilesional field. Because of this pattern of representation, following a unilateral lesion ipsilesional stimuli would excite more neurons in the frontal attentional area than contralesional stimuli, thus inducing an attentional bias in favour of the former stimuli and against the latter stimuli. Since it assumes a fixed relation between the right and left visual hemifields, as projected through the right and left hemiretinae, and the two hemispheres, this representational hypothesis cannot account for the present results in the head-tilted condition, because according to the retinal coordinates the two stimuli fall in the upper and lower visual fie!ds.
KINSBOURNE [14, 151 has postulated that each hemisphere is responsible for shifting attention in a contraversive direction, either in the ipsilateral or contralateral visual field. Damage to one hemisphere would unbalance the attentional system in favour of shifts contraversive to the intact side. His hypothesis would be compatible with the present results to the extent that such unbalanced contraversive tendency is assumed to occur with reference to both the retinotopic and the gravitational coordinates. In other words, a left parietal
364 ELISABETTA LADAVAS, MARIA DEL PESCE and LEANDR~ PROVINCIALI
lesion would be followed by an unbalanced tendency of the intact right parietal system to shift attention contraversively, in a leftward direction, in all frames of references; and the reverse would occur following a right parietal lesion. Experiments on split-brain patients support this interpretation insofar as the isolated left hemisphere can be shown to attend preferentially to stimuli in relative right locations, either in the retinotopic or the gravitational frame of reference and throughout the visual field, whereas the isolated right hemisphere attends preferentially to relative left stimulus locations [ 171.
As a consequence of the asymmetrical directional bias by the two hemispheres and due to a lesion in the parietal lobe patients with visual extinction show a general facilitation of all responses potentially triggered or guided from the most ipsilesional area and a disadvantage or exclusion of reactions to other stimulus locations. The disadvantage or the exclusion of reactions in these patients is due to the fact that attention must be reoriented to the non- attended location of the stimulus before a voluntary response can be emitted. The reorienting response of attention is time-consuming and therefore, when it occurs, causes a delay in response latency. On the contrary, if the reorienting does not occur we have the suppression of reactions because a voluntary response can occur only if the stimulus is within the focus of attention [21]. Furthermore the results of the present study show that orienting attention to a specific point in space involves two distinct operations: the specification of the direction concerning the visual field stimulated and that concerning the spatial position of the stimulus in the visual field. As we noted before, in patients with a right parietal lesion, the orienting response of the patient is under the control of the intact left hemisphere, and, therefore, the essential element which characterizes the preparation to respond to visual stimuli is the specification of the direction “right” as opposed to “left” for both the visual field and spatial position of the stimuli. When a patient with right parietal damage has to respond to the stimulus which occupies a right position in the RVF, the task does not require a readjustment of the ongoing pattern of neural organization, because the system is already prepared to respond to that direction. On the contrary, if the subject has to respond to left stimulus in the RVF, the neural adjustments must involve the correction of the directional bias concerning the spatial position of stimuli, and as a result the emission of the response is retarded. Hence, the cost for RT consistently found for left stimuli in RVF presentation. When the two stimuli are presented to LVF and the subject has to respond to right stimuli, the directional bias for the spatial position has not to be corrected, whereas that for visual field needs to be changed and specified as “left”, with the consequence that the response is retarded. When the subject has to respond to left visual stimuli in the LVF, the directional bias for both the spatial position and visual field have to be changed and specified as “left”. The correction of the directional bias for both visual field and spatial position is reflected in a marked cost for RT to left stimuli in LVF presentation. As it is possible to observe in Fig. 1A this condition yielded the longest reaction time. Of course the same explanation accounts for the results obtained in patients with left parietal lesions, with the exception that in these patients the essential element which characterized their orienting response is the specification of the direction “left” as opposed to “right”.
The directional deficits appeared to be greater after right than left parietal lesions. The results of the present study showed that the difference between reaction times to LVF and RVF stimuli and, within each visual field, between left and right stimuli, were greater when lesions occurred in the right rather than in the left parietal lobe. This could be due to an asymmetry in the hypothetical attentional biases generated by the two hemispheres, the leftward bias from the right hemisphere being weaker than the rightward bias from the left
UNILATERAL ATTENTION DEFICITS AND HEMISPHERIC ASYMMETRIES IN THE CONTROL OF VISUAL ATTENTION 365
hemisphere. The weaker bias would allow the right hemisphere to keep a more balanced control over the entire attentional field, in agreement with its traditionally recognized superior role in spatial orientation and cognition [6, 7,201. A right parietal lesion would thus release a comparatively stronger contraversive bias from the left hemisphere. Split-brain studies provide indirect support to such an interpretation [17] insofar as, using the same experimental procedure as in the present study, the authors showed that the asymmetrical attentional bias by the two hemispheres is bigger for the left than for the right stimulus. In other words, the left stimuli are mainly under the attentional control of the right hemisphere, whereas the right stimuli are under the control of both hemispheres, with the left hemisphere being more efficient than the right.
Alternatively, the greater asymmetry in directional bias found in the present study after right than after left parietal lesions may be linked in some way with the general reduction in speed of reaction following right hemisphere damage, hence with changes in the arousal mechanisms. The hypothesis that the general increase in reaction time in patients with parietal lesions may magnify the asymmetry in reactivity to right vs left stimuli compared to patients with left parietal lesions can only be tested directly by artificially inflating the reaction time of the latter group, for example by reducing the intensity of the stimuli. In this case, one might expect the reaction times for the left-sided group to go up and, as a consequence, we may or may not see differences between right and left stimuli comparable to those shown by the right-sided patients. This experiment remains to be done.
The results of the present study have shown an additional attentional impairment in patients with right-side lesion, which is independent for the spatial location of the stimuli. When we collapsed RTs in all the experimental conditions, we found that RTs of patients with right hemisphere lesions were slower than RTs of patients with left hemisphere lesion. Furthermore, the difficulty in maintaining a high level of alertness seems to be a specific deficit of patients with right hemispheric lesion and not of patients with visual extinction, since there is no significant difference between the overall RT to visual stimuli ofpatients with parietal and temporal lesions. This result is in very good agreement with a recent paper on the difference between alerting and orienting effects [22]. Using a different experimental paradigm POSNER et al. [22] found that patients with right-side lesions have special difficulties in maintaining a high level of alertness and that this difficulty does not affect their ability to shift attention in the cued direction.
Therefore we can conclude that visual extinction is better explained as a deficit of a selective attentional system, which is responsible for directing attention in space rather than as a deficit in the arousal component of attention. On the contrary, the arousal component of attention may play a specific role in determining the greater severity of left over right hemi- inattentive deficit [6, 7,201, although it is not the crucial factor which explains this phenomenon. A more straightforward explanation can be based on differential orienting strength of the two hemispheres in the control of spatial allocation of attention, with the rightward orienting bias of the left hemisphere being stronger than the leftward bias of the right hemisphere.
Acknowledyement-This research has been supported by MPI and Regione Marche.
REFERENCES 1. ATTNEAVE, F. and OLSON, R. K. Discriminability of stimuli varying in physical and retinal orientation. J. exp.
Psychol. 74, 149-157, 1967.
366 ELISABETTA L.&DAVAS, MARIA DEL PESCE and LEANDRO PROVINCIALI
2.
3.
4.
5.
6.
1. 8. 9.
10.
II.
12.
13.
14.
15.
16.
17.
le.
19.
20.
21. 22.
23.
24.
25.
26.
27.
ATTNEAVE, F. and REII), K. W. Voluntary control of frame of reference and slope equivalence under head rotation. J. exp. Psycho/. 78, 153- 159, 1968. BAYNES, K., HOLTZMAN, J. D. and VOLPE, B. T. Components ofvisual attention: alterations in response pattern to visual stimuli following parietal lobe infarction. Brain 109, 99 114, 1986. BISIACH, E., LUZZATTI, C. and PFRA~I, D. LJnilateraI neglect, representational schema and consciousness. Brain
102, 609 ~618, 1979. BOWERS, D. and HEILMAN, K. M. Pseudoneglect: etTects of hemispace on tactile line bisection task. Neuropsycholoyia 18, 491498, 1980. CHEDRU, F. Space representation in unilateral spatial neglect. /. Neural. Neurosury. Psychiat. 39, 1057- 1061, 1976. DE RENZI, E. Disorders of Space E?cploration and Cognition. John Wiley, New York, 1982. DIMOND, S. J. Performance by split-brain humans on lateralized vigilance tasks. Cortex 15, 521-529, 1979. HEILMAN, K. M., SCHWAKTZ, H. D. and WATSON, K. T. Hypoarousal m patients neglect syndrome and emotional indifference. Neurology 28, 229-232, 1978. HCILMAN, K. M. and VAN DEN ABELI., T. Right hemispheric dominance for mediating cerebral activation. Neuropsychologia 17, 315-321, 1979. HEILMAN, K. M. and VAN DEN ABELL, T. Right hemisphere dominance for attention: the mechanism underlying hemispheric asymmetries of inattention (neglect). Neurology 30, 327-330, 1980. HEILMAN, K. M., WATSON, R. T., VALENSTEIN, E. and DAMASIO, A. R. In Localization in Neuropsychologp, A. KERTESZ (Editor). Academic Press, New York, 1983. HOWES, D. and BOLLER, F. Simple reaction time: evidence for focal impairment from !esions of the right hemisphere. Brain 98, 317-332, 1975. KINSBOIJKNE, M. Hemi-neglect and hemisphere rivalry. In Hemi-attention and Hemispheric Specialization, E. A. WEINSTEIN and R. L. FRIEDLAND (Editors). Raven Press, New York, 1973. KINSBOUKSE, M. Mechanisms of unilateral neglect. In Neurophysioloyical and NewopsychologicaI Aspects of SDatial Nealect. M. JEANNEROD (Editor). North-Holland, 1987. L~DAVAS, ‘6. Is the hemispatial deficit produced by right parietal lobe damage associated with retinal or gravitational coordinates? Brain 110, 167-180, 1987. L~DAVAS, E. and GAZZANIGA, M. Different attentional bias in the two disconnected cerebra! hemispheres. in preparation. LAMOTTE, R. H. and ACUNA, C. Defects in accuracy of reaching after removal of posterior parietal cortex in monkeys. Brain Res. 139, 309-326, 1978. MESIJLAM, M-M. A cortical network for directed attention and unilateral neglect. Ann. Neural. 10, 309-325, 1981. OGDEN, J. A. The “neglected” left hemisphere and its contribution to visuospatia! neglect. In Neurophysiological and Neuropsychohqical Aspects qf Spatial Neglect, M. JEANNEROD (Editor). North-Holland, 1987. POSNER, M. I. Orienting of attention. Q. JI exp. Psychol. 32, 3-25, 1980. POSNER, M. I., INHOFF, A. W. and COHEN, A. Isolating attentional systems: a cognitive-anatomical analysis, Psychohioloyy 15, 107-121, 1987. POSNER, M. I., WALKER, J. A., FRIEDRICH, F. J. and RAFAL, R. D. Effects ofparietal injury on covert orienting of attention. J. Neurosci. 4, !863~-1874, 1984. POSNER, M. 1.. WALKER, J. A., FRIEDRICH, F. A. and RAFAL, R. D. How do the parietal lobes direct covert attention? Neuropsycholoyia 25, 135-145, 1987. RIZZOLATTI, G. and CAMARDA, R. Neural circuits for spatial attention and unilateral neglect. In Neurophysiological and Neuropsychological Aspects ofSpatial Neglect, M. JEANNEROD (Editor). North-Holland, 1987. RIZZOLATTI, G., GENTILUCCI, M. and MATELLI, M. Selective spatial attention: one center, one circuit or many circuits? In Attention and Performance IX, M. I. POSNER and 0. S. M. MARIN (Editors). Lawrence Erlbaum, Hillsdale, New Jersey, 1985. TUCKER, D. M. and WILLIAMSON, P. A. Asymmetric neural control systems in human self-regulation. Psycho/. Rev. 91, 185 215, 1984.
Related Documents




![Imagine a mouse and an elephant: Hemispheric asymmetries ......Downloaded by [Izmir Ekonomi Universitesi] at 03:54 23 June 2016 Inventory (Oldfield, 1971) which allows to assess the](https://static.cupdf.com/doc/110x72/60a0a5746a20b8137b0adf95/imagine-a-mouse-and-an-elephant-hemispheric-asymmetries-downloaded-by-izmir.jpg)






