UNHCR’S MENTAL HEALTH AND PSYCHOSOCIAL SUPPORT FOR STAFF July 2013 Courtney E. Welton-Mitchell, Ph.D. Asst. Professor, Graduate School of Professional Psychology International Disaster Psychology, University of Denver PDES 12/2013

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript
UNHCR’S MENTAL HEALTH AND PSYCHOSOCIAL SUPPORT
FOR STAFFJuly 2013
Courtney E. Welton-Mitchell, Ph.D.Asst. Professor, Graduate School of Professional PsychologyInternational Disaster Psychology, University of Denver PDES 12/2013


© United Nations High Commissioner for Refugees Policy Development & Evaluation Service Geneve, July 2013
This document is for general distribution. All rights reserved. Reproductions and translations are authorised, except for commercial purposes, provided the source is acknowledged.
Policy Development and Evaluation ServiceUNHCR’s Policy Development and Evaluation Service (PDES) is committed to the systematic examination and assessment of UNHCR policies, programmes, projects and practices. PDES promotes rigorous research on issues related to the work of UNHCR and encourages an active exchange of ideas and information between humanitarian practitioners, policymakers and the research community. All of these activities are undertaken with the purpose of strengthening UNHCR’s operational effectiveness, thereby enhancing the organization’s capacity to fulfill its mandate on behalf of refugees and other persons of concern to the Office. The work of the unit is guided by the principles of transparency, independence, consultation, relevance and integrity.
All PDES evaluation reports are placed in the public domain. Electronic versions are posted on the UNHCR website and hard copies can be obtained by contacting PDES. They may be quoted, cited and copied, provided that the source is acknowledged. The views expressed in PDES publications are not necessarily those of UNHCR. The designations and maps used do not imply the expression of any opinion or recognition on the part of UNHCR concerning the legal status of a territory or of its authorities.
Cover photo: © UNHCR Back-cover photo: © UNHCR / A. Plotnikov / March 2006
Printed by UNHCR PDES 12/2013
Layout and Design: BakOS DESIGN


Acknowledgement
First and foremost it must be acknowledged that any evaluation of an employer’s impact on the mental health and well-being of its workforce is a sensitive undertaking. When the employer is one of the largest frontline relief agencies in the world and many of its staff has been exposed to human rights abuses, state and militia supported violence, and wide-scale human suffering, the evaluative task is all the more complex. Adding to this complexity is the fact that humanitarian work has evolved significantly in the past few decades owing to the expanded role of information and warfare technology, oversight entities, the media and the consequences of unresolved conflicts in some regions. Humanitarian work has changed and the profile of the humanitarian professional has also noticeably evolved in the past two decades.
It takes curiosity and courage to evaluate how well a humanitarian organization is taking care of its own staff. It also indicates deep concern and care for UNHCR’s staff members and good citizenship in the humanitarian community. This evaluation contributes to a growing body of literature on mental health and psychosocial support for humanitarians. The hope is that the findings and recommendations from these studies will enable both organizations and individuals to stay strong while providing relief for others in a chaotic world.
Critical analysis of such a sensitive topic requires a researcher who is neutral and scientific yet has sufficient knowledge of the subject to be able facilitate genuine and candid data through interviews, focus groups and research tools: an outsider who can understand the insiders. Thankfully, Dr. Courtney Welton-Mitchell was available to research and write this evaluation. In addition to being on faculty in the University of Denver’s Graduate School of Professional Psychology’s International Disaster Psychology program, and holding a M.A. in Counseling, a M.A. in Social Psychology, and a Ph.D. in Affect/Social Psychology, Courtney worked for many years for the UN World Food Programme in Nepal and Tanzania as well as for the Cairo based NGO, African and Middle East Refugee Assistance (AMERA). Through her teaching and research, Courtney was able to articulate the trends and issues relevant to all humanitarian organizations and through her own humanitarian experiences, she was able to capture the nuances of UNHCR staff narratives. The review benefitted from her ability to remain compassionately detached in processing the sensitive data of this evaluation. Courtney’s team of researchers also deserves acknowledgement. We thank Gwen Vogel, Victoria Roeck, Mahaut de Talhouet, Carla Hauer Carrillo and Meghan Hunter for supporting Courtney through data analysis and coding, translations, copy-editing and data reduction.
Thanks to the staff from ICRC, MSF-Holland, MSF-U.S., WFP, OCHA, USAID, CVT and the Antares Foundation for sharing volumes of agency documents and insights. Many thanks to the Staff Health and Welfare Service staff who also shared numerous documents and made time for multiple interviews and answered countless questions. This review benefited also from the critical feedback of steering committee members, Betsy Greve, Marian Schilperoord, and Duda Suzic-Kofi who provided suggestions and corrections to research instruments and draft documents.
Sincere thanks are due to the UNHCR offices in Bangladesh and Pakistan who graciously hosted the field-based interviews and focus groups. Special thanks are extended to the independent support group for UNHCR staff survivors of critical incidents, including sexual assault and bombings; they provided input through interviews, focus groups and survey responses. Over 1,500 staff offered their opinions through the combination of the all staff survey, focus group participation and individual interviews. Thanks to every staff member who shared his or her personal experiences and unique point of view.
Gratefully, MaryBeth Morand Senior Policy & Evaluation Officer
Table of Contents
Acknowledgement.............................................................................................................................5
Executive summary ...........................................................................................................................9
1. Purpose of the study ...................................................................................................................13
2. Methodology ................................................................................................................................14
2.1 Desk Review and Comparison with Other Agencies ............................................................14
2.2 Interviews with Internal and External Stakeholders ..............................................................16
2.3 Field Work: Focus Groups and Interviews ............................................................................17
2.4 Online Survey ........................................................................................................................20
2.5 Methodological Limitations ...................................................................................................21
3. Introduction: Mental Health and Psychosocial Support for Humanitarian Staff ...................22
3.1 Why Prioritize MHPSS for Staff? ...........................................................................................23
3.2 Guidelines .............................................................................................................................24
3.3 Current Literature: Stress and Coping among Humanitarian Staff .......................................25
3.4 Staff Welfare in UNHCR ........................................................................................................30
4. Findings ........................................................................................................................................35
4.1 Good Practice Standards ......................................................................................................35
4.2 Summary Score for Antares Principles .................................................................................49
4.3 Managerial Responsibility for Staff Well-being .....................................................................50
4.4 Stress and Coping .................................................................................................................52
Distress .................................................................................................................................56
Coping ...................................................................................................................................58
4.3 Critical Incidents ....................................................................................................................59
Critical Incident Exposure .....................................................................................................59
Critical Incident related Distress ...........................................................................................60
Critical Incident Response ....................................................................................................61
4.4 Satisfaction with Critical Incident Response .........................................................................62
Service Utilization among Survivors of Critical Incidents......................................................62
Critical Incident Survivors Recommendations ......................................................................64
4.5 Overall Satisfaction ...............................................................................................................65
Overall Service Utilization .....................................................................................................65
Factors influencing service utilization ...................................................................................66
4.6 Overall Staff Preferences and Recommendations ................................................................68
6 UNHCR’S MENTAL HEALTH AND PSYCHOSOCIAL SUPPORT FOR STAFF
5. Recommendations ......................................................................................................................69
5.1 Ensure Appropriate Response and Follow up for Survivors of Critical Incidents .................70
5.2 Increase Availability and Utilization of Formal Mental Health and Psychosocial Support ....71
Antares Foundation, Network of Staff Care Associates Worldwide ......................................72
5.3 Encourage Informal Social Support Among Staff .................................................................75
5.4 Enhance Accountability of Staff Welfare Related Services through Rigorous Evaluations, Clear Staff-Welfare Policies and Roles ..................................................................................77
5.5 Feasibility and Threats to Implementation of Recommendations .........................................78
6. Conclusion ...................................................................................................................................79
7. Management response to the UNHCR’S Mental Health and Psychosocial Support of Staff (MHPSS) evaluation. .........................................................81
List of Acronyms: ........................................................................................................................85
8. References and Bibliography .....................................................................................................86
Additional relevant websites .......................................................................................................92
Annexes ............................................................................................................................................93
7A Global Review

List of Annexes, Tables, Figures and Text Boxes
Annexes:Annex I. - Antares Framework: UNHCR’s Indicator Level Scores .....................................................93Annex II. - UNHCR STAFF WELL-BEING SURVEY ...........................................................................94Annex III. - DEMOGRAPHICS: Survey Respondents compared to UNHCR all staff ......................106Annex IV. - Staff Welfare-related Website Examples .......................................................................107Annex V. - List of Remote Interviewees ...........................................................................................108Annex VI. - Chain of Evidence Supporting Recommendations.......................................................109Annex VII. - Summary of Recommendations ..................................................................................113
Tables:Table 1: Timeline and associated tasks for evaluation ......................................................................14Table 2: Staff Welfare Section Service Delivery 2011 ........................................................................32Table 3: Eight Principles of Good Practice: Comparison of UNHCR with ICRC and MSF ...............35Table 4: Top Stressors for Staff in Bangladesh and Pakistan............................................................55Table 5: Distress Reported by Survey Respondents .........................................................................56Table 6: Coping Strategies ................................................................................................................58Table 7: Unexpected Benefits associated with Stress Exposure as a result of Humanitarian Work ........59Table 8: Critical Incident Exposure (among subgroup of 8 survivors) ...............................................60Table 9: Distress Reported by Subgroup of Critical Incident Survivors (N = 8) .................................60Table 10: Critical Incident Survivors’ (N = 8) Recommendations for Improving Response ...............64Table 11: Staff Preference for Organizational Interventions ..............................................................68
Figures:Figure 1: Managing Stress in Humanitarian Workers – Guidelines for Good Practice ......................26
Figure 2. Connection between Well-being and Engagement ............................................................31
Figure 3: Top Stressors for UNHCR Staff online survey (2012) .........................................................53
Figure 4: Top Stressors for UNICEF, Staff Stress Survey (2003; 2009) .............................................53
Figure 5: Issues raised with the Office of the Ombudsman 2011 .....................................................54
Figure 6: Critical incident survivors’ satisfaction with UNHCR response to critical incidents ..........62
Figure 7: Staff satisfaction with UNHCR efforts to promote staff well-being ....................................65
Text Boxes:Text Box 1: UNHCR Bangladesh, working environment ...................................................................17Text Box 2: UNHCR Pakistan, working environment ........................................................................19Text Box 3: Staff Welfare: Definition, Purpose, Organizational Responsibility ..................................23Text Box 4: Secondary stress, vicarious trauma ...............................................................................29Text Box 5: Psychological First Aid ...................................................................................................47
8 UNHCR’S MENTAL HEALTH AND PSYCHOSOCIAL SUPPORT FOR STAFF

Executive summary
Mental health and psychosocial support (MHPSS) for humanitarian staff, is often referred to as staff welfare, care, or well-being. MHPSS includes institutional responses intended to mitigate distress and enhance resilience of staff in response to stressors encountered during the course of providing humanitarian assistance.
Humanitarian work is risky business. Recent research suggests humanitarians face numerous mental health and psychosocial challenges, including increased risk for depression, anxiety and burnout. Although historically most staff care services have focused on intervention for acute stressors, i.e. in the aftermath of direct exposure to potentially traumatic events such as a bombing or sexual assault, in recent years it has become clear that chronic stress, often a result of environmental stressors, can be just as debilitating. Humanitarian agencies are increasingly concerned about the potential impact of staff stress on effectiveness and efficiency of service delivery.
In the last decade widely supported guidelines for providing mental health and psychosocial support for humanitarian staff have been developed: The Antares Framework, 2004, 2006, 2012; IASC MHPSS Guidelines, 2007; and the Sphere Guidelines, 2011. These guidelines, recent research, and innovative practices on the part of humanitarian agencies, such as those highlighted by Interhealth & PeopleInAid, 2009, have resulted in staff welfare initiatives receiving increased attention, with many organizations modifying their historical approach to MHPSS for staff.
This evaluation was conducted over the course of seven months, from May to November 2012, using various methodologies including an online survey; field visits to Bangladesh and Pakistan; and Skype, phone, and email interviews and correspondence with internal and external stakeholders. The result is a document intended to answer the following questions:
•WhatareUNHCR’scurrentmentalhealthandpsychosocialprogramsandpoliciesforstaffandhowdothesecomparetorecognizedframeworks?
•AreUNHCRstaffinthefieldawareofcurrentMHPSSprogramsforthem?Dotheyhaveaccesstotheseprograms?Aretheyutilizingservices?
•WhatarethecurrentmentalhealthneedsandconcernsofUNHCRstaffandarethesebeingadequatelyaddressed?Areself-identifiedneedsconsistentwiththoseidentifiedbysupportservices,e.g.StaffWelfareSection?
•WhatadjustmentstoUNHCR’smentalhealthandpsychosocialserviceswilllikelyenhanceeffectiveness?
Findings from this evaluation indicate four broad areas of concern:
1. Lack of adequate response to critical incidents;
2. Inadequate utilization of formal MHPSS services, coupled with a lack of options for service utilization outside of UNHCR;
3. Lack of adequate support for informal peer networks, apart from the underutilized peer support network;
4. Lack of accountability for the adequacy of MHPSS services provided, in part due to minimal evaluative efforts, including a lack of formal means of collecting indicators on staff well-being and satisfaction with existing services.
9A Global Review

Recommendations, detailed in the following section, attempt to address these shortcomings.
� Ensure Appropriate Response and Follow up for Survivors of Critical Incidents
In regard to the first finding that responses to critical incidents are inadequate, especially for survivors of sexual assault, and that critical incident survivors don’t consistently receive appropriate psychological care, the following actions are recommended to strengthen UNHCR’s responsibility to affected staff and their colleagues:
a. Provide Psychological First Aid (PFA) for all potential first responders.
b. Disseminate UNDSS Standard Operating Procedures (SOPs) for sexual assault of staff to all field based managerial positions.
c. Conduct internal reviews following critical incidents to determine compliance with protocols, and as a means of soliciting feedback from survivors.
d. Prioritize postings in low to moderate risk areas, at least in the short-term, for survivors of critical incidents.
e. Streamline procedures for recognition of service incurred incidents.
Chad / UNHCR and WFP warehouses were looted by the local population after the rebel attack. © UNHCR / H. Caux, November 30, 2006.
10 UNHCR’S MENTAL HEALTH AND PSYCHOSOCIAL SUPPORT FOR STAFF
� Increase Availability and Utilization of Formal Mental Health and Psychosocial Support
The second finding of this review indicates that there is insufficient availability and utilization of formal mental health and psychosocial support services, especially for those most in need of services. The following recommendations provide suggestions that would enable staff to access appropriate MHPSS options and explore therapeutic arrangements that would meet their specific needs:
a. Provide and promote the option for staff to utilize external mental health therapists remotely, e.g. Skype, telephone interviews.
b. Provide and promote the option for staff to utilize local external mental health therapists and traditional healers or religious figures where these may be preferred options.
c. Disseminate information on what is covered by UNSMIS for international staff and the Medical Insurance Plan (MIP) for national staff for outside therapeutic support, and promote a diverse range of staff support options within these coverage parameters.
d. Invest in an interactive website, including an external confidential component, with links to self-assessment tools such as https://ecouch.anu.edu.au/welcome, and online follow up resources such as a Skype consultation with an internal or external therapist of choice.
e. Annually, or at a minimum during the end of an assignment or another transitional phase, provide a regularly scheduled mental health and psychosocial wellness checkup with the option for staff to decline at their own initiative: an “opt-out” model of compliance. Consider a brief mandatory mental health screen in the annual physical for those who “opt-out” of the more comprehensive evaluation. Use the annual physical as an opportunity to provide psycho-education about stress and coping and referral to external resources.
f. Put in place explicit means to both ensure, and explain limits of, confidentiality. Written informed consent should be obtained for all staff receiving even brief internal or external services. This should include specifying if anyone can be informed of session content without additional express written permission from staff and other limits of confidentiality such as risk of harm to self or others. Staff in positions of authority should sign a confidentiality agreement. Reports of critical incidents should at minimum, be de-identified before being distributed. Critical incident reports should have very restricted distribution even when victim details have been removed.
� Encourage Informal Social Support Amongst Staff
The third finding of the review requests UNHCR to strengthen informal peer to peer support amongst staff since this is the support system UNHCR staff indicated that they rely on most heavily in times of distress. The current Peer Support Personnel (PSP) model is insufficient as a means of promoting informal social support amongst staff. UNHCR can improve by doing the following:
a. Improve selection, accountability, and utilization of existing Peer Support Personnel in operations deciding to retain this model.
b. Channel formal, peer support resources such as training to more broad-based informal low-cost peer support groups and team building activities, including country or office-specific well-being initiatives.
c. Provide corporate managerial support to ad-hoc critical incident survivor peer groups.
11A Global Review

d. Identify senior staff within the organization willing to speak frankly about their struggles with distress and burnout to act as role models.
e. Provide mental health first aid training (MHFA) for all managers.
f. Building on mandatory training on sexual harassment, provide advanced gender sensitivity training for all staff.
g. Investigate peer based support models for alcohol and other forms of substance abuse and consider pilot initiatives to examine receptivity of staff.
� Enhance Accountability of Staff Welfare Related Services through Regular Rigorous Evaluation, Clear Staff Welfare Policies, and Role Distinction between Sections
In response to the final finding calling for increased accountability of staff welfare both within the Division of Human Resources Management (DHRM) and at the line manager level, it is recommended that systematic and rigorous evaluations of functions affecting staff well-being take place along with the wide-scale dissemination of clear policies on roles and responsibilities for staff care.
UNHCR should develop protocols for regular evaluation of staff distress levels and satisfaction with staff support services, e.g. regular online surveys; anonymous online evaluations for SWS mission visits; pre and post measures for specific programs, using indicators such as – “burnout” and other distress symptoms (note: many of these items can be pulled from the online staff survey Annex II).
a. Evaluate managers on staff welfare indicators such as staff perception of support (through anonymous means).
b. Introduce a new UNHCR Staff Care Policy (follow nextstepsrecommendations made by PeopleInAid for UNHCR Duty of Care Project 2011).
c. Clarify the roles of relevant services within DHRM – the Staff Welfare Section (SWS), Medical, and Career Management Services (CMS).
d. Reallocate roles in SWS, with greater emphasis on case management, coordination and referral to external (country-specific and remote web-based therapeutic) resources, capacity building, including support and replication of innovative country-specific pilot initiatives, and decreased emphasis on direct service provision.
Recommendations elaborated in this report are informed by supporting evidence from several sources; please refer to Annex VI, ChainofEvidenceSupportingRecommendations. It is worth noting that nearly half of online survey respondents were national staff, and the overwhelming majority of focus group members in the field were national staff. As such, this data and associated recommendations should reflect the mental health status and associated needs of both national and international staff within UNHCR. It is hoped that these suggestions represent cost-effective solutions designed to mitigate common sources of staff stress and enhance effective coping. However, a cost analysis is recommended.
Humanitarian work is challenging, yet with adequate support there is no reason why those who choose this career cannot be resilient, and even thrive, in the face of adversity.
12 UNHCR’S MENTAL HEALTH AND PSYCHOSOCIAL SUPPORT FOR STAFF

1. Purpose of the study
Inthecontextofthecurrentforceddisplacementemergenciesandtheincreasinglydangerousworkenvironmentsinmanypartsoftheworld,wearedeeplyconcernedaboutthewell-beingofUNHCRstaffacrosstheglobe.ThisrequirescarefulanalysisofhowstaffarecopingwiththechallengesofbeingahumanitarianprofessionalandwhatadditionalstepsUNHCRcantaketofosterstaffwell-being”
T. Alexander Aleinikoff, Deputy High Commissioner, 31 August 2012 email broadcast to all UNHCR staff re: online staff welfare survey component of this global evaluation.
This study was commissioned by UNHCR’s Policy Development and Evaluation Service (PDES), at the request of the Deputy High Commissioner, in an attempt to determine how to better support UNHCR staff. Although heavily focused on the Staff Welfare Section within UNHCR, this is not an evaluation of SWS alone. The mental health and psychosocial well-being of staff is a cross-cutting issue and as such, it is the responsibility of numerous stakeholders, units, and sections within UNHCR - Medical Service,1 Legal Affairs, Office of the Ombudsman, Personnel Administration and Payroll Section, Security. In addition to providing a snapshot of staff well-being and distress, this global evaluation provides recommendations for a way forward, based on staff feedback, taking into account services provided by other humanitarian agencies, and a growing body of research.
1 The medical and staff welfare sections within UNHCR have recently restructured (July, 2012) such that both are now part of ‘Staff Health and Welfare Services.’ Several internal stakeholders mentioned this restructuring, with near unanimous support for the change. Several staff explained coordination between the two sections had been lacking and they were hopeful this would now improve. There are no mental health specialists in the medical section (e.g., clinical psychologists, psychiatrists). However, the medical section is often involved in severe and/or persistent mental health issues (major depression, PTSD, suicidal intent, substance abuse). The involvement of medical staff in such cases includes supporting documentation for sick leave, coordinating medical evacuations, reviewing case details to determine if the mental health issue is ‘service incurred,’ and in referring to and communicating with outside psychiatrists and other mental health specialists.
The mental health and psychosocial needs of staff is a cross-cutting issue that is the responsibility of numerous stakeholders, units, and sections within UNHCR.
13A Global Review

2. Methodology
This global evaluation took place between May and November 2012. In addition to an online survey with 1,341 participating staff, a total of 231 persons were interviewed, consulted, and/or participated in focus groups. One hundred and eighty eight staff members were contacted during the field missions and 43 were contacted via remote interviews.2
Table 1: Timeline and associated tasks for evaluation
Tasks Timeframe (2012 – 2013)
Institutional Review Board (IRB) approval3 May
Desk Review – comparison with guidelines and other agencies May – July
First wave interviews with internal and external stakeholders June-early August
Data collection from critical incident survivors July
Online survey design July
Mission to Bangladesh late August
Mission to Pakistan early to mid-September
Online survey data collection end August – end September
Coding of field data from individual interviews and focus groups September
Second wave interviews with internal and external stakeholders September - October
Coding and analysis of online survey data October – November
Report writing Ongoing through early December
Draft revisions and internal review January - April
2.1 Desk Review and Comparison with Other Agencies
Numerous publications, including internal UNHCR documents, were reviewed (see References and Bibliography for detailed list). As part of this process, UNHCR and staff from the following agencies were interviewed by Skype or phone, although in a few cases, staff were consulted through email:
• United Nations World Food Programme (WFP)
• United Nations Office for Coordination of Humanitarian Affairs (OCHA)
• International Committee for the Red Cross (ICRC)
• Médecins Sans Frontières/ Doctors without Border (MSF-Holland and MSF-U.S.)
• Center for Victims of Torture (CVT)
• United States Agency for International Development (USAID)
As evident from the above list, the group of comparator agencies included two United Nations organizations, WFP, and OCHA, three INGOs, and one governmental organization.3 Staff from the Antares Foundation was also consulted by email about current and forthcoming editions of the guidelines, the Antares network of mental health therapists specializing in work with humanitarians, and for permission to reproduce some of their materials. Documents from several
2 Protocol number 2012-2138, University of Denver (programme evaluation exemption).3 Attempts were also made to contact staff from Norwegian Refugee Council (NRC) to no avail.
14 UNHCR’S MENTAL HEALTH AND PSYCHOSOCIAL SUPPORT FOR STAFF

other humanitarian agencies were reviewed including the International Federation of Red Cross and Red Crescent Societies (IFRC); CARE, and the World Health Organization (WHO). In most cases for comparator agencies, staff welfare officers with a background in clinical psychology, counseling, or social work were interviewed. In a few cases, others in charge of staff care were also interviewed, e.g. Human Resource officers.
External and internal participants in this evaluation were assured of confidentiality, and anonymity in the case of the online survey, to encourage candor. This assurance of confidentiality for information shared during individual interviews and focus groups was especially important in light of recent results from the UNHCR Global Staff Survey in 2011, indicating a fear of speaking up among 57 per cent of survey respondents, and with 50 per cent indicating they believed there is a lack of ‘open and honest communication’ within the organization. As a result, the names of those interviewed are not provided in this document and care has been taken to ensure quotes have been de-identified. The exception to this is information derived from personal correspondence with the UNHCR Chief of the Staff Welfare Section, an important internal stakeholder whose specific contributions must be acknowledged in order to maintain the integrity of this evaluation.
The Antares document ManagingStressinHumanitarianWorkers–GuidelinesforGoodPractice-secondedition (2006) was used for a comparison of UNHCR to ICRC and MSF as agreed with the Steering Committee and other relevant stakeholders. The Antares guidelines focus on eight core principles with 34 associated indicators. This mapping exercise compared UNHCR’s staff welfare activities to the two other organizations at both the principle level and the indicator level.
In order to minimize the subjectivity of this comparative process, the team employed a method that involved external project staff rechecking information provided by the participating agencies. First, a review of compliance with indicators was conducted by project assistants based on extensive documents provided by UNHCR and the comparator agencies. Upon a second review by the consultant, the information was cross-checked with the senior staff with UNHCR, ICRC, and MSF
Burnt shelters in Bulo Elay settlement in Bosasso. © UNHCR/R. Gangale/May 2011
15A Global Review
in charge of staff welfare. In the case of ICRC the health unit also reviewed compliance with the Antares guidelines. After additional comments and associated documents were received from agency contacts, another review was conducted by project assistants and the consultant, making modifications where appropriate. Finally, while writing this report the consultant conducted a final review of compliance criteria to ensure agencies were evaluated in a similar fashion. Compliance with indicators is based on the documents that were provided to the consultant, written information from senior staff in charge of staff welfare, and impressions from the consultant and project assistants based on additional sources of data. The veracity of the statements provided by ICRC and MSF were not assessed directly. However, the information provided by UNHCR staff welfare was cross-checked with information collected during field missions, through the online survey, and stakeholder interviews. This resulted in a more in-depth review of compliance with the Antares framework for UNHCR than for ICRC and MSF.
In the case of other organizations - OCHA, WFP, USAID, and CARE - specific program elements have been highlighted relative to the Antares guidelines, but an Antares framework indicator-based comparison was not made. In part, this is due to limited availability of internal documents from these agencies, time constraints on the part of participating staff from these organizations, and in a few cases, because the organizations are in a transition period with their own staff welfare initiatives.
2.2 Interviews with Internal and External Stakeholders
Interviews with stakeholders were conducted using semi-structured questions associated with content areas consistent with the Antares framework’s eight good practice principles elaborated elsewhere in this report. For senior UNHCR staff in Headquarters, questions were tailored to their specific roles. For UNHCR staff in the first wave of interviews, the Antares guidelines provided a loose framework for questions, for those in the second wave of interviews the Antares framework played a limited role. Instead, feedback was solicited on field data and online survey findings in the interest of developing recommendations. The informal ‘open-ended’ interview approach was used to allow for maximum flexibility, to ensure spontaneity in responding to content generated by interviewees, and to obtain feedback relevant to developing recommendations. This less structured approach4 was intentionally designed as a counterpoint to the more formal and structured online survey and open-ended but standardized focus group questions posed to staff while on mission.
The consultant individually interviewed 37 UNHCR staff and former staff, most of who had been recommended by the evaluation manager in consultation with the steering committee. The steering committee also included a representative from ICRC. External comparator agencies were determined by the consultant in collaboration with the evaluation manager. Eight additional persons from external agencies provided interviews and/or email correspondence.
The initial intention was to record Skype interviews for the remote interviewees, but several people expressed discomfort with this idea based on concerns over confidentiality. Consequently, these interviews were not recorded but were transcribed by hand. All interviews were conducted by the consultant directly, not project assistants.
4 This is consistent with recommendations in the literature (e.g., Turner, 2010).
16 UNHCR’S MENTAL HEALTH AND PSYCHOSOCIAL SUPPORT FOR STAFF

Text Box 1
UNHCR Bangladesh, working environment
“In what constitutes one of the most protracted displacement situations in the world, Bangladesh hosts more than 29,000 refugees from Myanmar's northern Rakhine State. These refugees, who are members of an ethnic, linguistic and religious minority in Myanmar, reside in the two camps of Kutupalong and Nayapara in Bangladesh's south-eastern district of Cox's Bazar…The quality of life for most refugees remains very poor. Moreover, high levels of poverty and illiteracy in Cox's Bazar district contribute to negative attitudes towards the refugees, affecting the unregistered population in particular. This has resulted in some 30,000-40,000 unregistered people of concern from Myanmar settling spontaneously outside Kutupalong Camp, where sanitary conditions are poor, and the malnutrition rate is even higher than in the registered camps….in November 2010, the Bangladesh authorities suspended resettlement…”
Retreived from UNHCR website November 2012: http://www.unhcr.org/pages/49e487546.html
2.3 Field Work: Focus Groups and Interviews
The consultant traveled with the evaluation manager on mission to Bangladesh and Pakistan for ten days in each place. These locations were selected because they represented duty stations dealing with protracted refugee situations and frequent crises. Pakistan and Bangladesh also matched, respectively, the consultant’s criteria for differentials in security risk, restricted compound living vs. freedom of movement for staff, presence of a staff welfare professional vs. none, an established peer support network vs. none, and varying degrees of participation in a formal peer support program. Stakeholder interviews, individual interviews5 and focus groups were conducted while on mission to Bangladesh and Pakistan.
Focus groups were arranged to be relatively homogenous, e.g. gender, grade levels and supervisorial responsibilities, in order to encourage persons who might otherwise feel intimidated to speak up. Focus groups averaged eight persons; a few were as small as three and one was as large as fourteen. Groups of six to eight participants appeared to be the most successful in encouraging contributions from all members. Interpretation was provided for two groups of drivers.
The two groups requiring interpretation selected their own interpreter. All focus groups and individual interviews began with a verbal informed consent. Focus groups were co-facilitated by the consultant and the evaluation manager.6 Permission was requested to audio record in-person focus groups and interviews, ensuring only the consultant would have a copy that would eventually be destroyed. All groups granted this permission with the exception of one focus group and one individual interview participant. In these two cases, the content was transcribed by hand. The structure of the focus group discussions was consistent across all the groups, based on three broad questions:
5 Individualinterviewsrefer to audio recorded interviews with staff who requested a meeting. In contrast, stakeholderinterviews refer to key informants who provided information at the consultant’s request (e.g., regional staff welfare officers; UNDSS stress counselors; peer support volunteers; senior management).
6 Participants were reassured of confidentiality. The UNHCR evaluation manager’s neutral role was emphasized; however, participants were also offered the option of meeting with the consultant without UNHCR staff present. No one selected this option.
17A Global Review

� Stressors - Focus group members were asked about common causes of stress. Most of the time, the group members had no difficulty in generating their own list of stressors. A list of ‘common stressors among humanitarians’ was shared. This list was based on previous research in a large sample of humanitarian workers.7 Participants were asked if any of the items were a common cause of stress:
• Exposure to suffering of persons of concern; • Exposure to incidents when you were seriously injured or your life was threatened; • Political situation in the county where you are presently working; • Relationship with supervisors; • Relationship with work colleagues; • Family concerns; • Health concerns; • Safety concerns; • Financial concerns; • Feeling undervalued; • Feeling unable to contribute to decision making; • Status of employment contract; • Workload; • Working hours; • Ability to achieve work goals and objectives.
� Coping - Next, focus group members were asked what they typically do to manage stress. Again, most groups quickly generated a list of common coping strategies. Some examples were provided to determine if these were in common use, e.g. exercise, prayer, talking to family and friends.
� Organizational supports - Finally, focus group members were asked to comment on organizational solutions used to mitigate stress, both those in use in UNHCR and used by other agencies. During this discussion, the following possibilities were introduced:
• Peer Support Personnel and Respectful Workplace Volunteers; • Staff Welfare Section in HQ – available by phone/Skype; along with missions for training and
counseling; • Regional or locally–based UNHCR Staff Welfare Officers; • Formal complaint mechanisms -- Ombudsman, IGO, Ethics Office; • Critical Incident Response – trained focal points; clear SOPs ; mandatory psychological first
aid ( PFA) training for staff; • Mental health screening, posting preparation, ongoing monitoring of psychosocial well-being
during annual physicals with a mandatory or ‘opt out’ model as opposed to procedures whereby staff are expected to self-identify when in need of services;
• Website or web-based services – with interactive and self- assessment components; access to outside web-based counseling, video testimony from role models, e.g. Representatives talking about stress responses and staff care;
• Annual stress management plans at the office level that have been developed through a consensus process with staff, potentially through an existing staff council, or where none exists, an ad hoc committee of staff with representations from each office and job sector.
Participants were asked if they found any of these relevant or useful for this operation, and if not, what might be more useful.
7 Curling & Simmons (2010).
18 UNHCR’S MENTAL HEALTH AND PSYCHOSOCIAL SUPPORT FOR STAFF

Text Box 2
UNHCR Pakistan, working environment
“Pakistan continues to host approximately 1.7 million refugees. Most are from Afghanistan and live in refugee villages and urban areas…The socio-political and security situation in Pakistan remains challenging. UNHCR endeavours to strike a balance between providing assistance to those in need and ensuring staff security…UNHCR operational activities have further been challenged by the devastating floods that hit Pakistan in 2010 and 2011.
In addition to the approximately 1.7 million refugees in the country, there are currently some 420,500 people displaced due to conflict in Khyber Pakhtunkhwa (KPK) and the Federally Administered Tribal Areas (FATA)….”
Retreived from UNHCR website November 2012: http://www.unhcr.org/pages/49e487016.html
In 2009 three UNHCR staff were killed in separate incidents in Pakistan (kidnapping, bombing, shooting).
All focus groups and individual interviews were coded by two independent project assistants for thematic content, e.g. stressors, coping, staff preferences for various types of well-being initiatives in UNHCR and other agencies such as the formal peer support model. A third independent project assistant merged data in a manner inclusive of content from both coders.
Bangladesh - Thirty-three persons in the UNHCR Cox’s Bazar Sub-office participated in individual interviews and/or focus groups. There were five focus groups with 26 persons total and 14 individual interviews (10 of these individuals also participated in focus groups), resulting in an 88 per cent coverage of the Sub-Office. No focus groups or individual interviews were conducted with staff in Dhaka, although three additional meetings took place with key stakeholders there: the Representative, the Senior Administrative Officer, and a UNDSS trained stress counselor who works for an international health organization as a clinician, supervisor, and trainer. Informal conversations were also had during social gatherings in Dhaka and Cox’s Bazar with other UN and INGO staff working in the area. Focus groups and individual interviews were typically slightly longer in Bangladesh (up to 90 minutes each) than Pakistan (60 minutes) based on time available relative to the size of the office.
Pakistan - One hundred thirty-four persons participated in individual interviews and/or focus groups in UNHCR offices in Pakistan: Islamabad, Peshawar, and Quetta. This represents 43 per cent coverage based on all UNHCR staff with the Pakistan operation, a much larger operation than Bangladesh. An additional 19 stakeholder interviews were conducted with Heads of Office, the Regional Staff Welfare Counselor, two UNDSS Stress Counselors, staff at UN guesthouses, and ten Peer Support Personnel volunteers. The PSP volunteers also participated in focus groups and/or interviews; they are only counted once however in the participant total.
Field visits were beneficial in numerous ways, including allowing for in-person collection of rich qualitative data for comparison with online survey responses and the remote interviews with senior staff. The majority of time was spent speaking to national staff, including typically underrepresented groups such as drivers.
19A Global Review

2.4 Online Survey
The content of the online survey was developed based on: 1) the IASC Guidelines for MHPSS in Emergencies 2007 – Action Sheet 4.4 Preventandmanageproblemsinmentalhealthandpsychosocialwell-beingamongstaffandvolunteers; 2) recent research in the field of mental health and psychosocial well-being for humanitarian workers, including consideration of previously used staff care survey instruments,8 and 3) the Antares ManagingStressinHumanitarianWorkers:GuidelinesforGoodPractice second edition, 2006.
Once the initial draft was complete it was discussed with the evaluation manager, and a slightly modified version was sent on to the steering committee for review. The final version of the survey incorporated steering committee feedback (see Annex II). The questionnaire was translated into French and Spanish by professional translation experts hired by the consultant.
The survey link was sent out by UNHCR in an all-staff email broadcast on 31 August 2012 with a cover letter from the Deputy High Commissioner emphasizing the anonymous nature of the survey and the importance of the topic. A reminder was sent at the survey mid-point. The survey closed at the end of September. Although initially a random stratified sampling technique was recommended by the consultant, UNHCR senior staff preferred an all-staff survey.
The online all staff survey resulted in a lower than ideal response rate of 16 per cent, based on 8,164 staff including ‘affiliate workforce.’ Of these 1,493 staff logged on to view the survey, but only 1,341 responses were deemed valid based on the completion of at least one section. This is substantially less than the recent UNHCR Global Staff Survey response rate of 34 per cent, and response rates of similar online surveys in large humanitarian organizations.9 Of note, a meta-analysis of 199 online surveys10 indicated an average response rate of 32.5 per cent for sample/population size larger than 1,000, and median response of 26.5 per cent. Response rates for all-employee surveys however, are typically lower in general. The response rate for this survey is comparable to a staff care survey with UNHCR several years ago11 resulting in a 17 per cent response rate, although sampling and data collection methods differed. The relatively low response rate is likely due to several factors including: staff not routinely opening UNHCR broadcasts; skepticism about the potential of survey data to influence change; timing of the message- it came out a couple days after the HC sent out a message on reduction in workforce which may have caused apathy or disengagement; misunderstanding on the source and purpose of the survey; and lack of computer proficiency and access for some staff such as drivers, guards, cleaners.
Considering these possibilities, it is especially important to make a determination of who did complete the survey by comparing the survey sample to the population of all UNHCR staff (Annex III). Relative to the population of all UNHCR staff: more women completed the survey (53 per cent of the respondents were women whereas women are only 37 per cent of all UNHCR staff); there were fewer participants from Africa (28 per cent of survey respondents, 45 per cent of all UNHCR staff); more international professional staff participated (42 per cent of survey respondents, 25 per cent of UNHCR staff); fewer national staff participated (just under half of survey respondents, 68 per cent of all UNHCR staff); more Protection staff participated (37 per cent of survey respondents, 25 per cent of all UNHCR staff); fewer Programme and Administrative staff participated (12 per cent and 16 per cent of respondents respectively, 21 per cent and 42 per cent of all UNHCR staff).12 The majority of respondents had between 1-5 years (29 per cent) or 5-10 years of experience with UNHCR (22 per cent). Most were between the ages of 31-40 (36 per cent) or 41-50 (31 per cent).
8 Primary sources: Curling & Simmons (2010) and InterHealth and PeopleInAid study, Approaches to Staff Care in International NGOs (2009), specially the QuestionnaireforStaffCareResearch.
9 Curling & Simmons (2010) 34% response rate.10 Hamilton (2003).11 Stress,Coping,andBurnoutinUNHCRStaff:APilotStudy (2001).12 Drivers, guards, cleaners, receptionists are all classified as administrative staff.
20 UNHCR’S MENTAL HEALTH AND PSYCHOSOCIAL SUPPORT FOR STAFF

Results based on any survey that is not representative of the population in some of the ways outlined above, and that has a low response rate, must be interpreted with caution. Considered in combination with field data and stakeholder interviews however, the online survey data makes significant contributions to understanding the mental health and psychosocial needs of UNHCR staff, and to informing recommendations concerning preferred services.
2.5 Methodological Limitations
As has been highlighted, the response rate for the online survey (16 per cent) is a limitation. In addition, although participation in individual interviews and focus groups in Bangladesh and Pakistan was high, it is possible those participating differed in some way from those unable or unwilling to participate. Participants were not selected at random, but instead participated based on interest and availability.
Remote stakeholder interviews necessarily varied in content, and although transcribed, were not independently coded, but instead were open to subjective interpretation by the consultant. In addition, stakeholders were not randomly selected, but were instead selected by the evaluation manager based in part on advice from the steering committee, in an attempt to represent diverse opinions and experience.
Cultural and language barriers must also be acknowledged. The online survey, although provided in English, French, and Spanish, did not include other languages. Some UNHCR staff, especially national staff, could be more comfortable responding in languages that were not represented. Some staff such as drivers and guards may have had difficulty accessing the survey due to limited computer access and/or a lack of familiarity with online survey instruments. In addition, the survey instrument did not undergo rigorous psychometric testing and development and was not validated for use in specific cultural contexts as this would not have been feasible considering the diversity of UNHCR work locations in over 100 countries. Finally, as has been pointed out by others doing similar work, Western-derived constructs associated with stress and coping are not always relevant in non-Western cultural settings.
As with any evaluation of this nature, and despite efforts to use independent coders, collect anonymous survey data, and multiple sources of data, a consultant’s personal biases and preferences will influence outcomes, including associated recommendations. Taking all this into account, a significant strength of this evaluation is that multiple sources of data were collected using various methodology, and where possible, independent coders were used to minimize subjectivity. Every attempt has been made to allow the data to speak for itself and minimize subjective interpretation.
21A Global Review
3. Introduction: Mental Health and Psychosocial Support for Humanitarian Staff
The document attempts to answer the following questions as outlined in the Inception Report associated with this global review of UNHCR’s Mental Health and Psychosocial Support of Staff.
WhatareUNHCR’scurrentmentalhealthandpsychosocialprogramsandpoliciesforstaffandhowdothesecomparetorecognizedframeworks?
AreUNHCRstaffinthefieldawareofcurrentprogramsforthem?Dotheyhaveaccesstoexistingprograms?Aretheyutilizingservices?
WhatarethecurrentmentalhealthneedsandconcernsofUNHCRstaffandarethesebeingadequatelyaddressed?Areself-identifiedneedsconsistentwiththoseidentifiedbysupportservicese.g.StaffWelfareSection?
WhatadjustmentstoUNHCR’smentalhealthandpsychosocialserviceswilllikelyenhanceeffectiveness?
As the above questions indicate, UNHCR and many other humanitarian organizations have staff welfare programs in place. In recent years there has been increased emphasis on reviewing the efficacy of existing programs. Despite considerable progress that has been made by humanitarian organizations in paying attention to staff welfare in the past 10 to 15 years, including significant resources dedicated to peer support programs, recent research13 suggests many humanitarian staff care programs still lack:
1. Consistency in practices;
2. Adherence to minimum guidelines;
3. Specific staff care policies;
4. Post-assignment psychological reviews;
5. Secure and adequate funds for staff care;
6. Regular monitoring and evaluation mechanisms;
7. Knowledge of best practices and current research.
The humanitarian community at large is grappling with how to provide well-considered and consistent care to their employees. Implementing the ideal staff care program is not a simple undertaking, yet it is not unattainable.
13 InterHealth and PeopleInAid, 2009. Approaches to Staff Care in International NGOs.
22 UNHCR’S MENTAL HEALTH AND PSYCHOSOCIAL SUPPORT FOR STAFF

Text Box 3
Staff Welfare: Definition, Purpose, Organizational Responsibility
DEFINITION: “Staff care refers to self-care and institutional responses to stress among humanitarian workers in particularly difficult and stressful environments” (InterAction, 2008).
PURPOSE: “The purpose of staff care is to create a healthy and productive workforce; to create wellbeing among staff and improve the quality of their work… (by promoting) emotional, cognitive, spiritual, and physical health” (InterHealth & PeopleInAid, 2009).
ORGANIZATIONAL RESPONSIBILITY: Humanitarian aid organizations bear legal liability for ensuring staff welfare (see Kemp & Merkelbach, 2011: Canyougetsued:Legalliabilityofinternationalaidorganizationstowardstheirstaff).
Mental health and psychosocial support for humanitarian staff, often referred to as staffwelfare,care,orwellbeing,will for the purposes of this report, and to minimize potential confusion with the Staff Welfare Section at UNHCR, be referred to asmentalhealthandpsychosocialsupport(MHPSS). This terminology is consistent with the IASC Mental Health and Psychosocial Support in Emergencies guidelines (2007).
“Thecompositetermmentalhealthandpsychosocialsupportisused…todescribeanytypeoflocaloroutsidesupportthataimstoprotectorpromotepsychosocialwell-beingand/orpreventortreatmentaldisorder.Aidagenciesoutsidethehealthsectortendtospeakofsupportingpsychosocialwell-being.Healthsectoragenciestendtospeakofmentalhealth,yethistoricallyhavealsousedthetermspsychosocialrehabilitationandpsychosocialtreatmenttodescribenon-biologicalinterventionsforpeoplewithmentaldisorders.Exactdefinitionsofthesetermsvarybetweenandwithinaidorganisations,disciplinesandcountries…thecompositetermmentalhealthandpsychosocialsupport(MHPSS)servestouniteasbroadagroupofactorsaspossibleandunderscorestheneedfordiverse,complementaryapproachesinprovidingappropriatesupports”
(IASC MHPSS, 2007, 1-2).
3.1 Why Prioritize MHPSS for Staff?
Some humanitarians question whether providing MHPSS for staff should be a priority, especially when there are insufficient resources for Persons of Concern (PoC).14 In comparison, humanitarian staff appears to be well resourced. However, MHPSS for staff is not a luxury; it is essential for humanitarian organizations to function effectively. In an organization like UNHCR, services for PoC may be compromised if staff care is neglected. Humanitarian agencies are increasingly concerned about the potentially debilitating effects of staff stress on effectiveness of relief programs.15 Research with non-governmental organizations (NGOs) indicates stress in the absence of adequate support can also result in staff leaving an agency.16 UNHCR cannot afford attrition or compromises to the integrity of its staff. With its unique leadership role in refugee operations and its cluster obligations, UNHCR needs to maintain a cadre of experienced and healthy staff who can energetically and diplomatically engage in emergencies.
14 For UNHCR this may include refugees, internally displaced, and stateless persons.15 McKay (2012): http://www.headington-institute.org16 Loquercio, Hammersley, & Emmens (2006).
23A Global Review

Workerssufferingfromtheeffectsofstressarelikelytobelessefficientandlesseffectiveincarryingouttheirassignedtasks.Theybecomepoordecisionmakersandtheymaybehaveinwaysthatplacethemselvesorothermembersoftheteamatriskordisrupttheeffectivefunctioningoftheteam.Theyaremorelikelytohaveaccidentsortobecomeill.Aconsequenceforhumanitarianagenciesisthatstaffstressandburnoutmayimpederecruitmentandretentionofqualifiedstaff,increasehealthcarecosts,compromisesafetyandsecurityofstaffandcreatelegalliabilities.”
Antares, Managing Stress in Humanitarian Workers: Guidelines for Good Practice, 2nd ed. (2006).
3.2 Guidelines
In the last decade widely supported guidelines and supporting document for providing mental health and psychosocial support to humanitarian staff have been developed in collaboration with multiple stakeholders:
• “Managing Stress in Humanitarian Workers – Guidelines for Good Practice,” Antares Foundation, 2004; 2006; 2012;
• “Approaches to Staff Care in International NGOs,” Interhealth & PeopleInAid, 2009;
• “The Interagency Standing Committee Guidelines on Mental Health and Psychosocial Support in Emergency Settings,” 2007;
• The Sphere Handbook: HumanitarianCharterandMinimumStandardsinHumanitarianResponse, The Sphere Project, 2011.
Amongst these international guidelines, two in particular set the standard for the field and played a significant role in this evaluation.
Antares: Managing Stress in Humanitarian Workers – Guidelines for Good Practice - The Antares consensus-based guidelines were initially developed in collaboration with the Centers for Disease Control and Prevention, and are the result of several years of work with an international specialist group that included national and international NGOs, experts in human resources, safety and security, psychosocial programs, agency directors, national and international field-based managers, and academic and clinical practitioner experts in managing chronic and acute stress. The second and third editions of the guidelines were used in this evaluation.17 Figure 1 provides an illustration of the eight principles in the Antares guidelines; in part these correspond to the employment stages of a humanitarian staff member.
Inter-agency Standing Committee (IASC) Guidelines on Mental Health and Psychosocial Support (MHPSS) in Emergency Settings - The consensus-based IASC Guidelines on MHPSS in Emergency Settings are seen as a significant accomplishment for the humanitarian field in general and for international disaster psychology specifically.18 The IASC Guidelines on MHPSS include detailed guidance for humanitarian agencies, Action Sheet 4.4 Preventandmanageproblemsinmentalhealthandpsychosocialwell-beingamongstaffandvolunteers. This Action Sheet is consistent with and informed by Antares guidelines.19
Although the Antares and MHPSS IASC Guidelines, Action Sheet 4.4 are the benchmarking documents for this review, the Sphere Project’s minimum standards 2011 and the framework set forth in Interhealth and PeopleInAid’s 2009 document were frequently referenced. It should be noted that the latter collected data on staff care practices from 19 humanitarian organizations along with providing examples of innovative programs. Moreover, the guidelines, reports, and minimum standards are largely consistent across documents, representing broad consensus in the field about what constitutes
17 The third edition Antares Guidelines (2012) became available near the end of this evaluation. Differences between the two editions have been reviewed to ensure recommendations are based on latest updates.
18 Lopez-Cardoza (2008); Barrett et al. (2011).19 Staff from Antares participated in development of Action Sheet 4.4.
24 UNHCR’S MENTAL HEALTH AND PSYCHOSOCIAL SUPPORT FOR STAFF

effective mental health and psychosocial support for humanitarian staff. In addition to providing a framework for this evaluation, these documents influenced the desk review along with the questions for remote and field-based individual interviews and focus groups, and the content of the online survey.
3.3 Current Literature: Stress and Coping among Humanitarian Staff
This is an opportune time for conducting a global evaluation of UNHCR’s MHPSS for staff. In recent years, concerned stakeholders and researchers have amassed a body of knowledge emphasizing distress among humanitarians, and underscoring the need to provide support: “…our knowledge about the psychosocial needs of staff and about factors that affect staff well-being has increased dramatically. In part this reflects an increase in formal studies of staff stress…”20 The resources available today allow humanitarian agencies to make rational, evidence informed decisions on staff care whereas in the past they may have been overly reliant on subjective impressions of a few decision makers.
In the early 1990’s, distress among humanitarians began to be increasingly documented. This initial data, and more recent research, suggests that humanitarians face numerous mental health and psychosocial challenges. A recent longitudinal study indicated humanitarians are at increased risk for depression, anxiety and burnout during deployment and after returning; aid workers also had lower levels of life satisfaction compared with pre-deployment levels, even months after returning from the field.21
This is consistent with other findings. In a 2007 Headington Institute study of distress among humanitarians in Darfur, 42 per cent of respondents rated overall well-being as 5 or below out of 10 (with 1 being ‘very bad’ and 10 being ‘very good’). Various forms of distress were evident in their responses. Within the two weeks prior to taking the survey, over half of survey respondents reported symptoms of being ‘physically stressed’, e.g. headaches, sleep disturbances, stomach upsets, and tight muscles, and just under half reported being ‘emotionally stressed’, e.g. irritability, mood swings, feeling depressed, anxious or numb. Nearly one third of the respondents indicated they were ‘mentally stressed’ e.g. they experienced difficulty concentrating and forgetfulness, and 13 per cent reported feeling ‘interpersonally stressed’ and/or ‘spiritually stressed’. Interpersonal stress was defined as ‘feeling withdrawn, overwhelmed by people, or lonely, and/or avoiding being with people.’ Spiritual stress was defined as ‘feeling empty; feeling as if you have lost your sense of meaning, purpose, hope or connection; and questioning or doubting some of your core beliefs.’22 In short, just about half of the humanitarian respondents felt sub-par, reporting numerous somatic and emotional complaints.
Other studies also indicate that substantial numbers of humanitarians experience poor health. In one study nearly half of a group of repatriated international staff was described as being at moderate or high risk of burnout.23 Studies of former humanitarians indicate approximately 15 per cent have clinically significant levels of depression and a similar percentage (15 per cent) struggle with alcohol abuse.24
20 Antares (2012), p.6.21 Cardoza et al. (2012).22 Headington Institute (2007), p.15.23 Ericksson (2002).24 Cardozo & Salama (2002); Eriksson, Van de Kemp, Gorsuch, Hoke, & Foy (2001).
In recent years “…ourknowledgeaboutthepsychosocialneedsofstaffandaboutfactorsthataffectstaffwellbeinghasincreaseddramatically.Inpartthisreflectsanincreaseinformalstudiesofstaffstress...”(Antares, 2012, p. 6).
25A Global Review

Figure 1: Managing Stress in Humanitarian Workers – Guidelines for Good Practice (reprinted with permission, Antares, 2012)
26 UNHCR’S MENTAL HEALTH AND PSYCHOSOCIAL SUPPORT FOR STAFF

27A Global Review

Post-traumatic stress disorder (PTSD) - In one study nearly 10 per cent of international aid workers surveyed met diagnostic criteria for Post-Traumatic Stress Disorder, and an additional 19 per cent reported clinicallysignificant PTSD symptoms.25 Another study indicated that 46 per cent of repatriated international staff had high or moderate levels of symptoms of PTSD.26 Such symptoms may persist even years after return from field postings in high stress environments. A study examining long-term adjustment indicated that 10 per cent of returned United States aid workers had Post-Traumatic Stress Disorder even three years after having returned home. Comparisons to lifetime prevalence in civilian populations suggest that there is a higher rate of PTSD among humanitarians compared to other professions.27
In addition to high rates of exposure to acute stressors, higher rates of PTSD among humanitarians compared to civilian populations may in part be explained by exposure to high levels of chronic work related stress.28 Findings from a workplace stress survey conducted by a large international humanitarian organization indicated 74 per cent of respondents reported feeling ‘moderately’ to ‘extremely’ stressed. In contrast, a national workplace survey carried out in the United Kingdom revealed that 45 per cent of survey respondents reported finding their jobs ‘moderately’ to ‘extremely’ stressful”.29 In understanding contributing factors to the relatively high rates of reported stress and associated distress symptoms among humanitarians, it’s important to examine common stressors and frequently utilized attempts at coping.
Common stressors - Identifying common sources of stress for humanitarians has become an increasing priority for researchers, including those working in the field of international disaster psychology.30
A few categories of common stressors for humanitarians have emerged across studies: 1) work-related stressors, including team conflict and disorganized work environment; 2) other environmental stressors. such as the local political context; hardship conditions related to food, shelter, insecurity; and 3) traumatic stressors, i.e. - exposure to life-threatening events, and in some cases, vicarious trauma as a result of secondary exposure to traumatic experiences and associated suffering of aid recipients.31
Although historically the bulk of staff care interventions have focused on intervention for acute stressors, i.e. in the aftermath of direct exposure to potentially traumatic events such as a bombing, in recent years it has become clear that chronic stress, often a result of work or other environmental stressors, can be just as debilitating and tends to be more pervasive. Commonly cited sources of chronic stress included: poor leadership, lack of career opportunities, and bureaucracy. These chronic stressors potentially lead to burnout, disillusionment, and frustration, all of which can affect service delivery and, at times, results in staff deciding to leave the organization, or the field of humanitarian work entirely.32
25 Eriksson, Van de Kemp, Gorsuch, Hoke, & Foy (2001).26 Eriksson (2002).27 Eriksson, Vande Kemp, Gorusch, Hoke, & Foy (2001).28 Stress is a normal part of a living organism's response to the inevitable changes in its physical or social
environment. When resources to cope with stressors are inadequate, stress-related illness (physical and/or psychological) may result. Risk factors for stress-related illnesses include person-specific (e.g., genes, personality) and environmental (e.g., stressors) (http://medical-dictionary.thefreedictionary.com/stress).
29 Curling & Simmons (2012), p. 98.30 See Fox, Welton-Mitchell, & Barrett, in press, for a review.31 See Ericksson et al., 2009 for a review.32 Loquercio, Hammersley, & Emmens (2006).
Inrecentyearsithasbecomeclearthatchronicstress,oftenasaresultofworkorotherenvironmentalstressors,canbejustasdebilitatingasexposuretoacutetraumaticstressors.
28 UNHCR’S MENTAL HEALTH AND PSYCHOSOCIAL SUPPORT FOR STAFF

Text Box 4
Secondary stress, vicarious trauma
“When I was 23, I started working in a refugee legal aid clinic in Cairo, Egypt. My job was to record refugees’ stories of persecution, torture, and rape. Since the details of their stories were very important for their legal case, I tried to listen as closely as I could. What I did not realise was that close listening can come with a price. When I first started having intrusive thoughts and flashbacks, I was at a loss and I tried to ‘just get on with it’. There is often an unspoken code in this line of work that says that we are the tough ones, that we can face the harsh realities of war and human suffering. We wear the number of war zones and hunger-stricken countries we have worked in as badges of honor. Self-care is a luxury that no self-respecting aid worker has. I was definitely from that school of thought until I could no longer afford to be…I had wanted to do this work with enthusiasm and compassion but found myself becoming increasingly hard and cynical.”
Lotte Lenaers, Fahamu Refugee Legal Aid Newsletter: http://frlan.tumblr.com
Consistent with this, 2009 findings from a survey of staff in a large front-line humanitarian organization indicated that the following sources of work-related stress were their most common forms of stressors: 1) workload; 2) inability to achieve work goals and objectives; 3) working hours; 4) status of employment contract; and 5) feeling undervalued and/or unable to contribute to decision making.33 “Respondents working in emergency duty stations reported ‘workload’ and ‘working hours’ to be a greater source of stress than their counterparts working in headquarters duty stations…”34 This is consistent with a meta-analysis focused on the influence of the work environment on mental health indicating highdemandsandlowdecisionmakingabilityandhigheffortsandlowrewards are associated with mental health symptoms, underscoring the importance of the work environment for mental health.35
In addition to work stressors, and the possibility of exposure to potentially traumatic events, including bombing and kidnappings, another common source of stress for field-based humanitarian workers arises from their exposure to the suffering of persons they are responsible for assisting. This is typically referred to as secondarystressorvicarioustrauma. In a study in India,36 over half of the aid workers surveyed endorsed the following items from the SecondaryTraumaticStressScale: “It seemed as if I was reliving the trauma experienced by my client; I thought about my work with clients when I didn’t intend to; memories of my work with clients upset me; I had trouble sleeping; I was easily annoyed; I had trouble concentrating”. All in all, a series of studies provides a body of evidence that a substantial proportion of the humanitarian workforce is exposed to both chronic and acute stress, including secondary stress associated with exposure to the suffering of others, and as a result, experiences various forms of distress.
Coping - A focus on stress exposure and distress symptoms amongst humanitarian staff begs analysis of how they cope. Although negative forms of coping are not uncommon, e.g. excessive substance use, positive coping mechanisms also seem to be common among humanitarian workers: “…the degree to which aid workers reported relying on positive coping mechanisms to help them manage stress was on average more than five times greater than the degree to which they reported relying on negative coping mechanisms. A total of 91 per cent of respondents reported that they rely on social activities, 89 per cent on physical activities, and 68 per cent on spiritual or religious practices.”37 In identifying an institutional strategy for psychosocial support to
33 Curling & Simmons (2010), p.95.34 Curling & Simmons (2012) p. 96.35 Standfeld (2006).36 Shah, Garland, & Katz (2007).37 Curling & Simmons (2010), p. 99.
29A Global Review

staff, it is important to identify preferred healthy coping strategies and consider how the organization can enhance use of such strategies.
Although institutional responses to MHPSS for staff have placed less emphasis on informal social support compared to formal counseling by mental health experts, several organizations, including UNHCR, have recognized the importance of all staff retreats, social gatherings, access to loved ones (in-person, during annual leave and R&R cycles, and through remote access such as e-mail or Skype), and formal peer support networks. Informal social support is crucial for effective coping among humanitarians. Longitudinal research with humanitarians indicates social support is associated with lower levels of depression, psychological distress, and burnout, and greater life satisfaction.38
A study of coping amongst humanitarians indicated 84 per cent of respondents found work-related social activities very useful in managing stress. In comparison, 64 per cent rated formal in-house staff counselors as useful.39 Interestingly, the same percentage, 64 per cent, found formal peer support volunteers to be helpful. This suggests work-sponsored informal social activities may be a more effective means of providing support than even formal peer support mechanisms such as designated peer support personnel. Capacity-building and self-help mechanisms, e.g. information on stress and coping via the intranet and stress management workshops were rated as valuable by 78 per cent and 77 per cent respectively.40 This also suggests that staff are eager to utilize self-help resources.
3.4 Staff Welfare in UNHCR
UNHCR staff numbers have increased in recent years, with staff operating in increasingly insecure settings, including places where humanitarian aid workers are at times directly targeted. A large proportion of new staff has been recruited to respond to conflicts in the Middle East and North Africa (MENA). At the start of 2012, there were 7,739 staff, including a combined total of 960 in UNHCR's Geneva headquarters and the Global Service Centre in Budapest. Of the total, 5,871 were nationally recruited staff and 1,868 were internationally recruited staff. The largest concentration of field staff was in Kenya (437) followed by Chad (370), Democratic Republic of the Congo (353) and Afghanistan (333). Increased staff levels conjoined with elevated risks, including hostility directed at aid workers in a variety of insecure settings, e.g. Afghanistan, Somalia, Darfur, Pakistan, Chad,41 suggesting that ensuring staff welfare within UNHCR has become more critical and more challenging than ever.
UNHCR staff, on the whole, are engaged and dedicated to UNHCR’s mission. In the most recent UNHCR Global Staff Survey, 97 per cent of staff agreed with the statement “I fully support the values for which UNHCR stands;” 94 per cent endorsed the statement, “I am proud to work for UNHCR;” and 94 per cent indicated “I work beyond what is required to help UNHCR succeed.” However in the same survey, UNHCR staff well-being (defined within the survey as work/life balance, and working and living conditions) was below external norms. This particular combination is cause for concern as “engagement in the absence of well-being can lead to a burned out
38 Cardozo et al., (2012).39 Twelve percent of staff reported utilizing the staff counselor and 14% the peer support volunteers in the
past six months (Curling & Simmons, 2012, p. 99).40 Curling & Simmons (2010).41 Stoddard & Harmer (2011).
“UNHCRhastwicewontheNobelPeacePrize…staffmemberscurrentlyworkinover100countriesprovidingprotectionandassistanceto20.8millionrefugeesandotherpersonsofconcern”(UNHCR website, retrieved 4 August, 2012).
30 UNHCR’S MENTAL HEALTH AND PSYCHOSOCIAL SUPPORT FOR STAFF
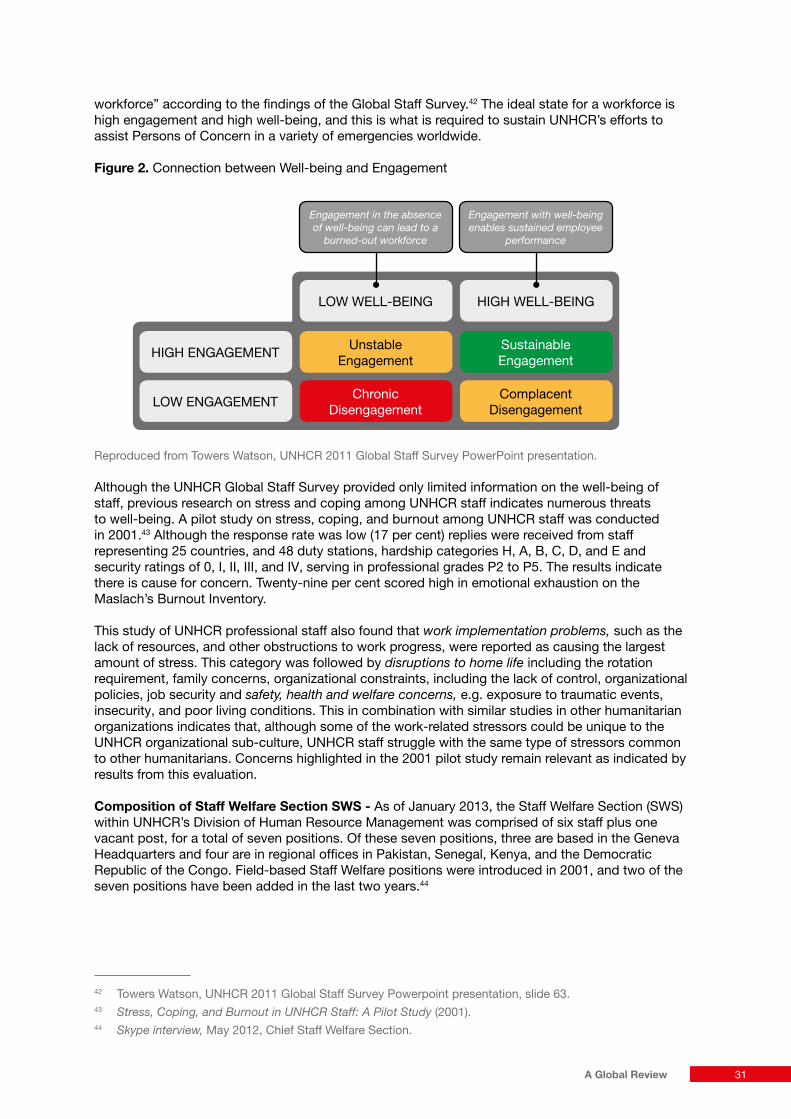
workforce” according to the findings of the Global Staff Survey.42 The ideal state for a workforce is high engagement and high well-being, and this is what is required to sustain UNHCR’s efforts to assist Persons of Concern in a variety of emergencies worldwide.
Figure 2. Connection between Well-being and Engagement
Reproduced from Towers Watson, UNHCR 2011 Global Staff Survey PowerPoint presentation.
Although the UNHCR Global Staff Survey provided only limited information on the well-being of staff, previous research on stress and coping among UNHCR staff indicates numerous threats to well-being. A pilot study on stress, coping, and burnout among UNHCR staff was conducted in 2001.43 Although the response rate was low (17 per cent) replies were received from staff representing 25 countries, and 48 duty stations, hardship categories H, A, B, C, D, and E and security ratings of 0, I, II, III, and IV, serving in professional grades P2 to P5. The results indicate there is cause for concern. Twenty-nine per cent scored high in emotional exhaustion on the Maslach’s Burnout Inventory.
This study of UNHCR professional staff also found that workimplementationproblems, such as the lack of resources, and other obstructions to work progress, were reported as causing the largest amount of stress. This category was followed by disruptionstohomelife including the rotation requirement, family concerns, organizational constraints, including the lack of control, organizational policies, job security and safety,healthandwelfareconcerns, e.g. exposure to traumatic events, insecurity, and poor living conditions. This in combination with similar studies in other humanitarian organizations indicates that, although some of the work-related stressors could be unique to the UNHCR organizational sub-culture, UNHCR staff struggle with the same type of stressors common to other humanitarians. Concerns highlighted in the 2001 pilot study remain relevant as indicated by results from this evaluation.
Composition of Staff Welfare Section SWS - As of January 2013, the Staff Welfare Section (SWS) within UNHCR’s Division of Human Resource Management was comprised of six staff plus one vacant post, for a total of seven positions. Of these seven positions, three are based in the Geneva Headquarters and four are in regional offices in Pakistan, Senegal, Kenya, and the Democratic Republic of the Congo. Field-based Staff Welfare positions were introduced in 2001, and two of the seven positions have been added in the last two years.44
42 Towers Watson, UNHCR 2011 Global Staff Survey Powerpoint presentation, slide 63.43 Stress,Coping,andBurnoutinUNHCRStaff:APilotStudy (2001).44 Skypeinterview, May 2012, Chief Staff Welfare Section.
LOW ENGAGEMENT Chronic Disengagement
LOW WELL-BEING
Complacent Disengagement
HIGH WELL-BEING
HIGH ENGAGEMENT Unstable Engagement
Engagementintheabsenceofwell-beingcanleadtoa
burned-outworkforce
Sustainable Engagement
Engagementwithwell-beingenablessustainedemployee
performance
31A Global Review
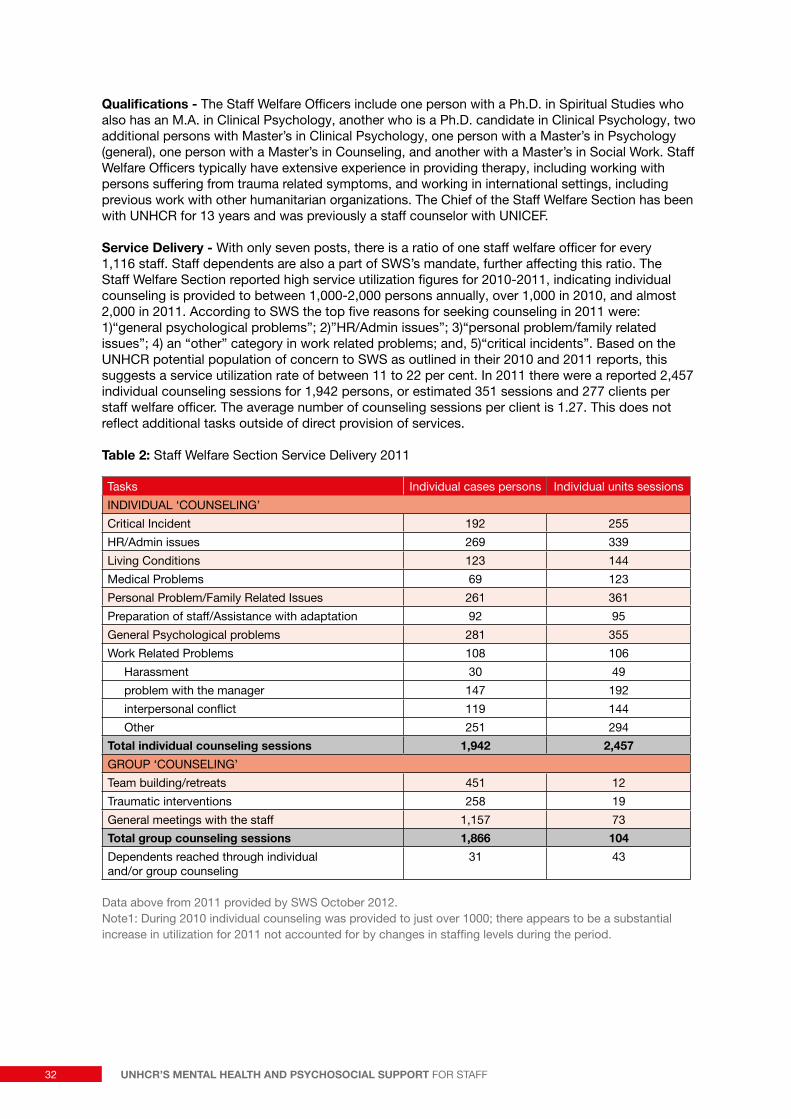
Qualifications - The Staff Welfare Officers include one person with a Ph.D. in Spiritual Studies who also has an M.A. in Clinical Psychology, another who is a Ph.D. candidate in Clinical Psychology, two additional persons with Master’s in Clinical Psychology, one person with a Master’s in Psychology (general), one person with a Master’s in Counseling, and another with a Master’s in Social Work. Staff Welfare Officers typically have extensive experience in providing therapy, including working with persons suffering from trauma related symptoms, and working in international settings, including previous work with other humanitarian organizations. The Chief of the Staff Welfare Section has been with UNHCR for 13 years and was previously a staff counselor with UNICEF.
Service Delivery - With only seven posts, there is a ratio of one staff welfare officer for every 1,116 staff. Staff dependents are also a part of SWS’s mandate, further affecting this ratio. The Staff Welfare Section reported high service utilization figures for 2010-2011, indicating individual counseling is provided to between 1,000-2,000 persons annually, over 1,000 in 2010, and almost 2,000 in 2011. According to SWS the top five reasons for seeking counseling in 2011 were: 1)“general psychological problems”; 2)”HR/Admin issues”; 3)“personal problem/family related issues”; 4) an “other” category in work related problems; and, 5)“critical incidents”. Based on the UNHCR potential population of concern to SWS as outlined in their 2010 and 2011 reports, this suggests a service utilization rate of between 11 to 22 per cent. In 2011 there were a reported 2,457 individual counseling sessions for 1,942 persons, or estimated 351 sessions and 277 clients per staff welfare officer. The average number of counseling sessions per client is 1.27. This does not reflect additional tasks outside of direct provision of services.
Table 2: Staff Welfare Section Service Delivery 2011
Tasks Individual cases persons Individual units sessions
INDIVIDUAL ‘COUNSELING’
Critical Incident 192 255
HR/Admin issues 269 339
Living Conditions 123 144
Medical Problems 69 123
Personal Problem/Family Related Issues 261 361
Preparation of staff/Assistance with adaptation 92 95
General Psychological problems 281 355
Work Related Problems 108 106
Harassment 30 49
problem with the manager 147 192
interpersonal conflict 119 144
Other 251 294
Total individual counseling sessions 1,942 2,457GROUP ‘COUNSELING’
Team building/retreats 451 12
Traumatic interventions 258 19
General meetings with the staff 1,157 73
Total group counseling sessions 1,866 104Dependents reached through individual and/or group counseling
31 43
Data above from 2011 provided by SWS October 2012. Note1: During 2010 individual counseling was provided to just over 1000; there appears to be a substantial increase in utilization for 2011 not accounted for by changes in staffing levels during the period.
32 UNHCR’S MENTAL HEALTH AND PSYCHOSOCIAL SUPPORT FOR STAFF
These numbers may be somewhat misleading. As explained by SWS, these numbers represent: “…the number of people [who] have an individual interaction through meeting in person, on the phone or through an email contact when an email contact results in [a] substantive communication…Double reporting is possible.” SWS went on to explain why a determination of utilization rates relative to all UNHCR staff is difficult to make, “…take into consideration that our services are also available to UNVs, UNOPS staff, and other affiliate workforce as well as to the family members…During the missions, we have a lot of individual sessions.” In 2011 the Geneva and regionally based SWS staff collectively reported the completion of 52 support missions to 28 locations, including relatively insecure settings such as Afghanistan, Pakistan, Libya, Tunisia, Egypt, Syria, Yemen, Ivory Coast, DRC and Somalia. This is a substantial increase from 2010 when “more than 30 support missions” were provided.
Despite challenges in determining utilization rates, the overall SWS caseload is unreasonably large with so few staff welfare officers, all the more when one recognizes SWS’s attempts to increase utilization of their individual counseling services. On top of this, SWS plans to conduct more outreach to dependents of UNHCR staff as stated in their 2011 report, UNHCRFamiliesSpeakOut. In addition to these services, a new initiative was introduced by SWS during the period of this evaluation, PsychologicalPreparationforHardshipAssignmentsandMissions. Objectives of this new program include the provision of individual ‘psychological preparation’ support to all international UNHCR staff deployed to hardship duty stations (D & E hardship categories). As noted in the explanatory document on this initiative, 45 per cent of UNHCR staff work in hardship locations. Although the initiative is focused on international staff only, the support envisaged will potentially result in a considerable increase in SWS’s workload, while maintaining the same number of staff welfare officers. However, “UNHCR is certainly not unique in funding a small staff welfare service in comparison to the size of the workforce and the nature of the work; resources for the range of services required to support staff adequately in the highly demanding context of humanitarian work are generally thought to be limited and even inadequate across the industry.”45 This suggests that although an increase in staff welfare officers may be helpful, especially given the current emphasis on individual support, low cost alternatives should also be explored in order to enhance services and expand care options in the prevailing climate of resource limitations.
Peer Support Personnel - SWS has attempted to extend their reach in a relatively low cost way through the introduction, expansion, and maintenance of peer support personnel (PSP). SWS reports that a network of 269 trained46 peer support personnel/volunteers has provided support to over 1,700 staff to date. Aside from a 2011 Global Learning Centre evaluation comparing the content of the Peer Support Personnel program alongside a similar program, the Respectful Workplace Advisors (RWA), the PSP has not been formally evaluated. Nevertheless the Global Learning Centre’s report included recommendations on harmonizing the two programs and integrating their reporting mechanisms, along with establishing a user evaluation system that focuses on results rather than instances of contact.
A more critical perspective on formal peer support programs has recently become available: GuidelinesforPeerSupportinHighRiskOrganizations:AnInternationalConsensusStudyUsingtheDelphiMethod; Creamer et al., 2012. The impetus for this study was a lack of consensus about the efficacy and ideal components of formal peer support networks, despite widespread adoption of peer-support programs in humanitarian organizations. Although some consensus was reached regarding the way forward, to date there remains of lack of evidence supporting the efficacy of peer support models as currently implemented in many humanitarian organizations.
45 Wigley (2005).46 Two trainings (level I and II) are provided. Of these 140 have only received level I training.
33A Global Review

In summary, UNHCR Staff Welfare Section has prioritized three main areas in recent years:
� Individual and Group Counseling – These sessions are for staff experiencing difficulties that have the potential to interfere with work performance. Reportedly, these sessions focus on areas such as vicarious trauma, addiction, problems with family, and crisis intervention. The mechanisms of delivery include face-to-face, phone, email, and Skype conversations.
� Capacity Building and Training – These activities include expanding on written materials on stress and coping for staff and include joint staff welfare trainings with security. These also involve contributions to the stress management trainings at country-level focusing on vicarious trauma, cumulative stress, interpersonal conflict, and crisis intervention. Training also includes psychological preparation for staff on the emergency roster and team-building interventions.
� Peer Support Personnel Network – According to the Chief of the Staff Welfare Section, maintaining the PSP involves continuous capacity building of selected peers at the country-level to “be a focal point for listening to problems, exploring emotions, encouraging self-reflection…contributing to respectful workplace…”
As noted, budgetary constraints and the small number of staff welfare officers mean priorities must be determined. In-house counseling, capacity building and training, and maintenance of peer support personnel appear to occupy the lion’s share of the staff welfare officers’ time. Yet, determination of priorities and maintenance of some long-standing initiatives does not appear to have been based on a comprehensive needs assessment nor on regular, rigorous evaluations to determine the impact of existing programs.
The findings of this evaluation report, detailed in the following sections, suggest the Staff Welfare Section has not devoted sufficient resources to: 1) keeping pace with recent research and ‘best practice’ guidelines in the field; 2) adequately monitoring staff well-being; 3) measuring the impact of its ongoing initiatives; 4) providing staff with a diverse menu of options for maintaining well-being; 5) responding to specific feedback from staff on needs and preferences (staff needs and preferences have been summarized in other evaluative reports).47 This may be in part a result of resource limitations and the resultant competing priorities. Thus, recommendations have been made with these constraints in mind, emphasizing low cost alternatives to increasing staff welfare officers, the number of field missions annually, and in-person trainings.
The challenges in designing and implementing quality staff welfare programs that adhere to minimum standards and best practice guidelines, including measuring effectiveness, are not unique to UNHCR. UNHCR is to be commended for taking the initiative through this global evaluation to determine what is working and where gaps exist, and for having expressed interest in adapting to fit best practice models based on contemporary research.
47 For example, ImpactEvaluationofthePSPandRWATrainingProgrammes, Global Learning Centre, 2011; GlobalStaffSurvey 2011.
34 UNHCR’S MENTAL HEALTH AND PSYCHOSOCIAL SUPPORT FOR STAFF

4. Findings
4.1 Good Practice Standards
Of UNHCR, ICRC, and MSF, it appears ICRC is the most compliant with current practice standards based on the Antares framework, ManagingStressinHumanitarianWorkers,GuidelinesforGoodPractice.
UNHCR appears less compliant than MSF at the level of the eight Good Practice Principles and individual indicators. In order to receive ‘credit’ for compliance with each good practice principle, the organization needed to comply with at least 50 per cent of the associated indicators. By this criteria ICRC is the most compliant, followed by MSF, and finally UNHCR.
Thanks to recent initiatives, UNHCR is strongest in the policy and crisis intervention sectors, although at only 50 per cent compliance for each. UNHCR does not meet the minimum 50 per cent compliance threshold for the following six principles: screeningandassessing,preparationandtraining,monitoring,ongoingsupport,endofassignmentsupport,andpostassignmentsupport. The narrative section that follows provides explanatory context for some of the results presented below in Table 3. This section also highlights innovative practices and in some cases, future plans, primarily from three agencies interviewed but not mapped against UNHCR: WFP,48 OCHA,49 and USAID.50
Table 3: Eight Principles of Good Practice: Comparison of UNHCR with ICRC and MSF
Good Practice Principle (Antares) UNHCR ICRC MSF
1. Policy - 8 indicators þ (50%) 4/8 þ (63%) 5/8 þ (63%) 5/8
2. Screening and Assessing - 5 indicators ý (20%) 1/5 þ (60%) 3/5 ý (0%) 0/5
3. Preparation and Training - 3 indicators ý (33%) 1/3 þ (67%) 2/3 þ (67%) 2/3
4. Monitoring - 4 indicators ý (25%) 1/4 þ (50%) 2/4 ý (0%) 0/4
5. Ongoing Support - 3 indicators ý (33%) 1/3 þ (67%) 2/3 þ (67%) 2/3
6. Crisis Support - 4 indicators þ (50%) 2/4 þ (50%) 2/4 ý (25%) 1/4
7. End of Assignment Support – 5 indicators ý (40%) 2/5 þ (100%) 5/5 þ (60%) 3/5
8. Post Assignment Support - 2 indicators ý (0%) 0/2 þ (100%) 2/2 ý (0%) 0/2
Total 2 out of 8 (12 out of 34 = 35%)
8 out of 8 (23/34 = 68%)
4 out of 8 (13 out of 34 = 38%)
Note1: A check indicates compliance with at least 50 per cent of the indicators within the principle category. An ‘x’ indicates less than 50 per cent compliance.
Note2: Results differ when considered based on principles, or at the individual indicator level.
Note3: For a detailed description of all indicators associated with each principle see: http://www.antaresfoundation.org/guidelines.htm
Note4: Due to space constraints details for each of the individual indicators for ICRC, and MSF are not provided in this evaluation report. Instead important elements are highlighted in narrative sections below. For UNHCR see Annex I: UNHCR Indicator Level Scores.
48 The WFP information is based on an interview with WFP senior staff in charge of staff welfare, July, 2012, and associated documents.
49 The information in this section is based on an interview with OCHA senior staff in charge of Staff Welfare, June, 2012.
50 The information in this section is based on an interview with USAID senior staff working on staff care issues, June, 2012.
35A Global Review

PRINCIPLE 1: POLICY The agency has a written and active policy to prevent or mitigate the effects of stress.
A clear staff care policy reflects an awareness of the impact staff stress can have on an organization’s ability to fulfill its mandate. Such a policy indicates an organizational commitment to integrate efforts to mitigate stress in all aspects of its operations. UNHCR has struggled to develop a comprehensive staff care policy. By UNHCR’s own admission, “service orientation…impedes the Section’s capacity to deliver as planned in the area of policy…”51 Despite this, UNHCR does have some policy elements relevant to staff well-being in place. The following are examples of UNHCR policies related to staff well-being.
UNHCR Anti-discrimination Policy - The Antares set of eight policy specific indicators (see Annex I for details) includes elements such as policies against discrimination of staff based on sex, race, nationality or sexual orientation, and forbidding sexual harassment of any individual or group of staff. Examples of this in UNHCR include: the Code of Conduct all UNHCR staff are requested to sign; the UNHCR Policy on Harassment (2005); and policies forbidding discrimination on the basis of age, gender disabilities, diversity, ethics and HIV/AIDS.
This Antares policy principle also includes policies and associated strategies for assessing security risks in specific settings. UNHCR has a policy of compliance with United Nations’ Department of Safety and Security (UNDSS) protocols. In addition, UNHCR has other stress mitigation procedures and policies in place such as R&R, and standardized assignment lengths in difficult duty stations.
UNHCR Critical Incident Policy - A specific policy for response to critical incidents apparently does not exist, in part because it was deemed unnecessary by the Staff Welfare Section. “Although we have started working on the protocol on crisis intervention...we never really finished that simply as it sounded self-evident…”52 In 1998 a skeletal policy covering stress management training, counseling and support following critical incidence was established. More recently however, a document providing an overview of coordination during a critical incident between security, medical service, staff welfare and human resources was apparently developed. It is unclear if this was widely disseminated.
UNHCR General Staff Care Policy - Recommendations were made in 1995 to establish a written policy concerning staff stress. Yet, the 1997 ManagingStaffStress report noted there was still no clear organizational policy in place. In July 2011 UNHCR hired PeopleinAid to develop a duty of care policy. This has not yet been implemented, however. The policy report provides six ‘next steps’ for UNHCR to follow, including refining minimum standards and indicators; attempts are being made to make the PeopleInAid document more concrete.53 To the best of the consultant’s knowledge, the roll out has not yet occurred.
In the online staff well-being survey, of the 1,316 respondents to the question, “How familiar are you with UNHCR policies related to staff well-being that help staff or managers cope with stress? “, 52 per cent indicated they were ‘somewhatfamiliar’ with UNHCR policies related to staff well-being. This is likely due to familiarity with policies associated with mandatory rotation and R&R cycles in hardship duty stations. Nevertheless, many staff remain unclear about staff care related policies. This online survey feedback contributed to UNHCR being scored as compliant with only half of the policy associated indicators for this principle.
51 SWS HQ Report, 2008, p. 2.52 Writtencorrespondence, SWS, June, 2012.53 The Director of DHRM explained this directly to the consultant mid-June, 2012.
36 UNHCR’S MENTAL HEALTH AND PSYCHOSOCIAL SUPPORT FOR STAFF

What other agencies are doing to implement this principle
WFP General Staff Care and Critical Incidents Policy - In late 2011 a new Chief of Staff Welfare joined WFP and, as a result, the agency is going through a period of transition with MHPSS for staff. He is introducing some new initiatives and overhauling a few long-standing programs. For example, WFP is spending considerable energy on developing an “occupational safety and health policy” emphasizing work-related stress. They have also selected an occupational health and safety focal point.54 For critical incidents, WFP coordinates with other agencies, including UNDSS stress counselors, to provide services. WFP is working to revise critical incident policies and protocols in collaboration with the security and emergency response division.
OCHA Critical Incidents Policy - There are also efforts amongst Human Resources staff in OCHA to revise some of the existing policy documents to emphasize “the short, medium, and long-term needs of those traumatized…” during critical incidents.
Arecentmulti-agencystudyofstaffcareinhumanitarianorganisationsfound,“Mostorganisationshavepoliciesthatrelatetostaffcarei.e.healthandsafety,leaveallowance,R&R,substanceabuse,occupationalhealth,security,housing,work-lifebalance,flexitime,etc…,butonlyone-thirdhaddesignatedstaffcare/wellnesssectionsorchapterswithintheirwiderorganisationalpolicy.”PeopleinAid/InterHealth, Approaches to Staff Care in International NGOs p. 19
54 WFP, 2012ReportoftheJointInspectionUnitRelevanttotheWorkofWFP, Executive Board document.
Iraq / An American convoy with UNHCR staff arrives in Topzawa village. UNHCR has been providing the returnees with some construction material to rehabiliate their houses or to build new homes. © UNHCR / H. Caux / September 13, 2010
37A Global Review

PRINCIPLE 2: SCREENING AND ASSESSING The agency systematically screens and/or assesses the current capacity of staff members to respond to and cope with the anticipated stressors of an assignment.
Screening is recommended prior to hiring, and comprehensive assessments are recommended on an ongoing basis, especially after work in hardship duty stations. Determining appropriate screening tools and developing exclusion indicators can however, be challenging for an organization.
UNHCR Screening and Assessment - Only minimal mental health or psychosocial screening procedures are in place. Standard medical forms include a section to be completed during the required annual physical, with questions on ‘appearance,’ and ‘behavior.’ The self-report section of the UN standard medical form includes the following questions: “Have you ever consulted a neurologist, psychiatrist, or a psychoanalyst? If yes, please give his/her name and address. Reason for consultation? Date?” This does not constitute a comprehensive screening “with respect to factors possibly affecting the likelihood of adverse or maladaptive response to the risks and stresses of humanitarian work.”55 UNHCR staff confirmed this is not intended to provide a mental health screening. Respondents to the staff well-being survey agreed that mental health or psychosocial screenings do not exist in UNHCR; only 11 per cent of respondents indicated they had received a psychological screening when joining the organization. It is assumed these persons are referring to the aforementioned questions on the medical form.
Although challenges associated with developing the exclusion criteria that is necessarily associated with implementing screening procedures prevent some agencies from pursuing this, recent research examining staff care in humanitarian organizations indicates, “Organisations that undertake psychological screening found them very useful. Rarely were staff members asked to delay their assignment or take a different assignment. After a period of support, e.g. private counseling through bereavement, depression, drug and alcohol rehabilitation, the organisation and staff person felt much more comfortable about working in the high-pressure environment.”56
What other agencies are doing to implement this principleWFP Screening and Assessment - WFP is very interested in enhancing mental health screening procedures. Currently mental health screening is not provided for new hires, apart from minimal questions on the standard medical forms similar to UNHCR. WFP is, however, working to identify what type of screening instruments might be appropriate. The goal is to identify an instrument by the end 2012 and put a screening protocol and associated policy in place during 2013.
ICRC Screening and Assessment - Standardized screening instruments are not the only means for humanitarian agencies to conduct psychological screening. Increasingly humanitarian organizations, e.g. WHO, are using simulation and other training activities as part of the hiring process and, in some cases, to vet candidates. In ICRC new hires, while still considered to be in a ‘trial period,’ are required to participate in an ‘introductory course.’ During the first week of training –
[an]assessment[is]made…todrawupanappraisalreportthatisaddedtotheparticipant’spersonnelfile,alongwiththecommentsmadeonrecruitmentday…participantsareobservedbyRH/RECandapersonnelmanager,whomainlyassesstheirbehaviourwithaviewtomatchingtheirabilitiestopotentialassignments.ThisisanopportunityforRECtoprovideparticipantswithindividualfeedbackontheirbehaviourduringtherecruitmentprocessandenablethemtoadjustit,ifnecessary,tomeettheICRC'srequirements.ThisobservationperiodalsomakesitpossibleforRECtodetectanymajorproblemsthatcouldjeopardizetheICRC'soperationsandcallintoquestionthedecisiontorecruitaparticularindividual.”57
55 Antares (2006).56 PeopleInAid/InterHealth, (2009), p. 24.57 Correspondence with ICRC senior staff.
38 UNHCR’S MENTAL HEALTH AND PSYCHOSOCIAL SUPPORT FOR STAFF

Although it is not for initial recruitment, the UNHCR Emergency Management Workshop, the “WEM”, includes simulated security incidents. SWS participate in these events which include discussion of staff members’ reactions to scenarios that involve potentially disturbing elements, e.g. kidnapping. However, this training is limited to staff on the emergency roster and it is not clear to what extent staff performance during these simulations has been used as a screening tool, although SWS reports that these exercises have indeed been used for screening purposes. Experiential screening is increasingly being used by humanitarian organizations, for initial hiring and on-going assessment, in order to increase the likelihood that appropriate staff are selected and will perform well in these high stress environments. However, as has been noted elsewhere, determination of appropriate screen out criteria is difficult. It is no wonder then -
…only15%oforganisationsrequireapsychologicalscreeningfortheirinternationalstaffpriortodeparture.Another15%oforganisationsreportedusinganon-clinicalbehaviouralscreeningorpersonalityassessment.”PeopleinAid/InterHealth, Approaches to Staff Care in International NGOs p. 20
PRINCIPLE 3: PREPARATION AND TRAINING The agency ensures that all employees have appropriate pre-assignment preparation and training in managing stress.Appropriate pre-departure briefings should include information on stress mitigation techniques and stressors associated with specific settings. Preparation and training should be provided after assignments and when transitioning between locations.
UNHCR Preparation and Training - There is no regular pre-departure training for all staff, although the mandatory UNDSS online security trainings have a brief stress management component. Recent attempts have been made to increase preparation between assignments and during transitions, i.e. when a staff member transitions to a hardship duty station.58
The Staff Welfare Section facilitates the TipsonStress and the Teams,IndividualsandStress sections of the Workshop for Emergency Management and, as noted above, participates in associated training activities involving simulated security incidents. SWS also meet with all new Junior Professional Officers, estimated 25 persons annually, and every Field Security Officer to discuss collaboration between security and Staff Welfare Section.59 The majority of UNHCR staff, however, does not receive comprehensive preparation or training in staff care related issues.
The online staff well-being survey included the question: “Have you ever received information about common stressors of humanitarian work, how to recognize stress reactions, and/or how to cope with stress? (check all that apply).” Only 12 per cent said they received such information prior to their first assignment and fewer (5 per cent) received this information before being posted to a hardship duty station. Almost half said they had received this information atsomeotherpoint since joining UNHCR, yet 24 per cent indicated they have never received this type of information.
An important element of the ‘preparation and training’ principle and associated indicators is training and evaluating managers on their ability to recognize stress, monitor stress, promote activities that reduce stress, and respond appropriately in times of unusual stress, including critical incidents. Since its inception in 2007, UNHCR’s Management Learning Programme (MLP) curriculum includes a module on general stress management and stress management for teams. Self-care and stress management is also emphasized in the MLP’s annual workshop. However, the MLP has only had 224 graduates since it began in 2007. The UNHCRHandbook(2007) also includes a section on TipsforManagersonStressManagement (pg. 515), and is consistent with good practice models.
58 PsychologicalpreparationforD&Edutystations,introducedAugust2012.59 SWS written correspondence, 2012.
39A Global Review

There do not appear to be adequate mechanisms in place for evaluating the efficacy of individual managers in promoting staff well-being. UNHCR’s core competencies associated with performance management do include “…accountability, teamwork and collaboration, communication, commitment to continuous learning, client and result orientation and organizational awareness…” and “… the managerial competencies include empowering and building trust, leadership…,”60 but these are not associated with specific indicators measuring a manager’s capacity and motivation to promote, and not undermine, MHPSS for staff.
It is recognized that it is a challenging task to define and measure the manager’s role in promoting adequate psychosocial care for staff. This limitation is not unique to UNHCR; none of the agencies were doing an adequate job of evaluating MHPSS for staff related competencies in managers. Some agencies are working to change this. For example, WFP is very interested in holding managers accountable for staff care by building concrete components into the performance review process and is working on means of “…spelling it out explicitly.”
What other agencies are doing to implement this principle
MSF Preparation and Training - All MSF staff prior to the first mission receives a PrimaryDeparturePreparationCourse, including a ‘Coping with Stress’ training module (MSF Holland). The course includes content on: 1) individual and team stress; 2) coping; 3) cumulative - day-to-day work stress; 4) critical incident stress; 5) awareness of stressors experienced by others and how to support one another; 6) individual and team stress management; and 7) the role of the organization in supporting people in the field. This “Coping with Stress” module meets the minimum requirements outlined in the Antares Guidelines and as such, can serve as a model for other agencies.
60 Written correspondence, SWS, 2012.
UNHCR team on the road to the Tule village are being stopped at the last army check point, at the exit of the village of Unguia. © UNHCR / B. Heger / May 2010
40 UNHCR’S MENTAL HEALTH AND PSYCHOSOCIAL SUPPORT FOR STAFF

PRINCIPLE 4: MONITORING The agency ensures the monitoring of the response to stress of its staff on an ongoing basis.
Regular monitoring activities allow an agency to examine staff distress following specific stressors, and as a result of cumulative chronic stressors. Monitoring also provides an opportunity to obtain regular feedback about service utilization and satisfaction. None of the agencies scored higher than 50 per cent compliance for monitoring indicators. These indicators include “…assess staff members for signs of stress on a regular,routinebasis as well as in the wake of crises.”
SWS explained its approach to monitoring as follows:
StaffWelfareSectiondoesnotparticipateinglobalmonitoringofstaffwell-being….Monitoringofstaffwell-beingisindeedincludedinourmissions…Wehadconsideredtheapplicationoftheallstaffsurveyonstress,asUNICEFdidit(twice)andwewerejusttakenoverbypriorities.However,itiscleartousthatsuchmonitoringwouldhavemoresoofanadvocacymeasureratherthanatooltoidentifywhereexactlytheproblemsare.Finally,Idonotthinkthatapplicationofclinicalinterviewsformonitoringwouldbethemostappropriateorcost-effectiveforallsituations.”61
Monitoring during missions, while commendable, cannot take the place of comprehensive monitoring systems.62 For example, in 2011 SWS went on mission to 28 locations, a coverage rate of only 22 per cent of UNHCR operations worldwide.
UNHCR Expectations of Staff to Self-monitor - Although the Antares framework recognizes staff must be accountable for monitoring stress in themselves, it is important that they be given the tools to do so, e.g. self-assessment tools, and comprehensive resources for follow up. There does not appear to be any expectation in UNHCR that staff regularly use self-assessment tools or create annual personalized stress management plans. Staff are generally encouraged to come to SWS if they need to talk to someone, but in the absence of specific tools or regular check-ins, e.g. during annual physicals, many staff are unlikely to engage in the type of self-reflection that may be necessary to make a determination that they ‘need to talk to someone,’ never mind taking the initiative to actually make contact.
This ‘passive’ self-monitoring model and its associated expectation that staff in need take the initiative to approach SWS is problematic. There are numerous staff who may benefit from services but who are unfamiliar with counseling or the notion that awareness of one’s stress-related difficulties may be perceived as a sign of strength. It is important to recognize however, that peer support personnel are intended to augment SWS and regional staff welfare officers, encouraging those who might be reticent to contact a staff welfare officer to make contact with a peer. It is not clear whether PSP are actually playing an advocacy and outreach role. Most interviewed for this evaluation indicated availability if needed, but no regular outreach. Despite reports from SWS that peer support personnel have served 1,700 staff to date, this does not address the needs of those reluctant to reach out. Peer support personnel do not appear to be playing any role in monitoring overall well-being and distress of staff in operations where they are based.
Albeit staff report on general well-being in the Global Staff survey, this is an insufficient means of monitoring stress. Nevertheless, a few additional questions concerning MHPSS for staff could be added to the global survey for the generalized monitoring of staff well-being. Other regular low-cost monitoring options could also be put in place e.g. agency-wide online assessments, and/
61 Writtencorrespondence, SWS, 2012.62 While UNHCR is to be commended for putting in place a Special Constraints Panel to address personal
needs associated with rotation, and review of rotational caps in hardship duty stations, this does not take the place of comprehensive screening, monitoring, or ongoing support.
41A Global Review
or anonymous location-specific surveys at the country, sub, field office, or team/unit level. For example, one large international aid organization used online surveys in 2003 and 2009 in order to compare distress at the two time points.63 In addition to monitoring staff stress, the survey results were utilized to examine the needs of sub-groups including women, national staff, and field-based staff, with an eye toward developing services tailored to specific needs.
In addition, this set of Antares indicators includes the need for a written policy stating that the organization will not respond punitively if staff should reveal stress related problems. It appears UNHCR is lacking in such policies and associated procedures. For example, there are no standard procedures in place for informed consent,64 or otherwise explaining limits of confidentiality.65 Such procedures are necessary prior to engaging in ‘counseling’ with staff welfare officers or peer support personnel. It is important for UNHCR staff to know their rights, and for the therapists within the organization to protect themselves and the organization from liability, especially in the event that a staff reveals stress related problems that have the potential to compromise the safety of colleagues, refugees, and other Persons of Concern. In a standard informed consent process these exceptions to confidentiality would be noted. Some striking examples of cases when confidentiality would need to be breeched were raised by internal stakeholders during this evaluation, such as suicidal staff, and a staff member who threatened to harm colleagues.
What other agencies are doing to implement this principle
WFP Monitoring - Like UNHCR, WFP does not mandate regular check-ins; instead they encourage staff to self-monitor and check -in if needed. WFP is also heavily reliant on peer support volunteers, but does not expect them to formally monitor staff well-being. It does not appear that WFP implements regular staff well-being surveys, nor do they appear to have standardized informed consent procedures for staff welfare officers and peer support personnel. WFP is in the process of modifying peer support programs however, so this may change.
On-goingmonitoringandperiodicevaluationhelpstheorganizationenhanceeffectivepracticeandeliminatingunhelpfulandcost-ineffectivepractice.”PeopleinAid/InterHealth, Approaches to Staff Care in International NGOs p. 17
63 Curling & Simmons (2010).64 See Ethical Principles of Psychologists and Code of Conduct for details of required elements of informed
consent in therapeutic relations, including limitations to confidentiality http://www.apa.org/ethics/code/index.aspx
65 Confirmed by skype interview with SWS (2012).
42 UNHCR’S MENTAL HEALTH AND PSYCHOSOCIAL SUPPORT FOR STAFF

PRINCIPLE 5: ONGOING SUPPORT The agency is providing training and support, on an ongoing basis, to help its staff deal with the daily stresses of humanitarian aid work.
Comprehensive ongoing support can serve a preventative function, contributing to an environment with a “proactive culture of stress mitigation.”66
This Antares principle states, “The agency provides training and support on an ongoing basis to help its staff deal with their daily stresses…;” this is consistent with the written objectives of UNHCR’s SWS:
ProvidepsychosocialsupporttotheUNHCRteams,personnelandtheirfamilymembers,inthefieldandattheHQ,whenevertheirprobleminterfereswiththeoutputofthestaffatwork,”andto“Providepsychosocialsupporttothestaffincrisissituationsandemergencyoperations,andfacilitatepsychologicalcrisisinterventionwhenappropriate.”67
As has been noted elsewhere in this report, SWS has contributed to capacity building and various training interventions over the past decade. This includes developing written materials, providing trainings for staff on the emergency roster, joint trainings with security personnel, peer support network trainings, and occasional trainings for the Management Learning Program and at country-level when there have been requests for sessions on vicarious trauma, cumulative stress, interpersonal conflicts, team building, and crisis intervention.
Yet, it appears there is no comprehensive strategy in place for providing ongoingsupportapart from responding to specific requests on an ad hoc basis. SWS has focused on individual and group counseling and peer support for those who self-identity as in need of services.68 Reports indicate the average contact or length of counseling sessions is only one. It is unclear whether SWS or peer support personnel are able to offer anything ongoing.
An internal report indicates that there was once continuous support for UNHCR staff in Jordan perceived to be at risk for vicarious trauma69 but this appears to have been a one-time initiative in one location. Stress management and general well-being sessions have also been provided a few times for staff at headquarters. Although a report in 2008 indicates follow up sessions associated with these were not well attended, SWS staff explained that sessions for staff at headquarters back in 2006 were well attended and were deemed effective based on a “mood measure” administered over four weeks.70
In part because of the difficulty in determining compliance with the three ongoing support indicators, responses to the online staff well-being survey were also considered in measuring UNHCR’s compliance with this principle. To this point, staff members were asked “Overall how would you rate UNHCR’s effort to promote staff well-being (to support staff and promote psychosocial and mental health)?” Of the 1,327 staff who answered this question, the majority, 58 per cent, responded in the range from ‘neutral’ to ‘extremelydissatisfied’(neutral: 15.4 per cent; slightly dissatisfied: 13.8 per cent; somewhat dissatisfied: 17.9 per cent; extremely dissatisfied: 10.9 per cent), suggesting UNHCR may not be providing adequate, regular, ongoing support. Understandably this is difficult, especially given resource constraints, including a lack of permanent on-the-ground presence in all but four field locations.
66 Antares (2012), p. 16.67 HQ report 2009 SWS.68 Occasionally staff are also encouraged by managers or other colleagues to approach peer support
personnel or the staff welfare section.69 SWS HQ Report, 2008.70 Personalcorrespondence, SWS, 2012.
43A Global Review

What other agencies are doing to implement this principle
ICRC Ongoing Support - ICRC provides ongoing support to its national staff through locally available mental health providers. “The ICRC does take into account the specific needs of its national staff…mainly in collaboration with national NGOs, specialized in providing psychosocial support, for example in Haiti, or with specialists available on site.”71
USAID Ongoing Support - In February 2012, USAID launched a new staff welfare initiative. The new initiative includes a staff care welcome center in headquarters,72 and 24/7 services for USAID staff around the globe through anytime phone access to support staff with free phone and reverse charges calling options.73 From the site: “The Staff Care Program is available to support you and your family. Don't hesitate to connect with us. We are available 24/7 and 365 days a year.”
WFP Utilization of Services and ongoing support - WFP counselors can provide services in-person or by phone but would like to expand, emphasizing more online counseling through Skype and live chat. WFP staff explained, “90 percent of staff are self-referred…” and utilization is low: “…approximately 3 to 5 percent are utilizing services out of almost 14,000 staff…” It is noteworthy that this percentage (an estimated 420-700 WFP staff) is substantially lower than the amount of service users reported by UNHCR. WFP also reports that their counselors “carry an ongoing moderate caseload providing psychotherapy….” WFP also maintains and distributes lists of local mental health providers and encourages the use of these local resources.
WFP Peer Support Volunteers - WFP maintains a separate website for peer support. WFP is in the midst of “revamping” the agency’s long-standing peer support program, believing there are some problems with the way the agency has historically implemented the program, including insufficient oversight. WFP is working to implement “quality control” procedures: “a clear selection process, review the training and build a ‘pass/fail’ into the training process to screen out people” that are a poor fit. Currently WFP is concerned that the peer support program isn’t as effective as it should be, stating, “the selection process is problematic.”74
WFP Web-based Materials and ‘Radio Talk show’ - Like UNHCR, WFP has a range of mental health and psychosocial materials on the intranet. However, unlike UNHCR, WFP materials include an emphasis on self-assessment tools, encouraging staff to use these for self-monitoring. WFP is also interested in innovative ideas using modern technology, such as introducing a radio talk-show forum where staff can call in and have a dialogue with the host.
PRINCIPLE 6: CRISIS SUPPORT The agency provides staff with specific and culturally appropriate support in the wake of critical or traumatic incidents and other unusual and unexpected sources of severe stress.Exposure to critical incidents can result in severe distress, the likelihood of which is greater in the absence of support. A comprehensive coordinated agency response is an essential part of efforts to mitigate long-term distress.
UNHCR staff assigned to emergencies currently receive a document entitled, BasicStressManagementforDifficultAssignments:NotesforStaffAssignedtoEmergencies. This document includes criteria for defining and reporting ‘critical events.’75 This suggests compliance with crisis
71 ICRC written correspondence, 2012.72 http://staffcare.usaid.gov/hr_blog.html73 http://www.konterragroup.net/client/united-states-agency-for-international-development-usaid74 WFP interview (2012).75 Personalcorrespondence, SWS, 2012.
44 UNHCR’S MENTAL HEALTH AND PSYCHOSOCIAL SUPPORT FOR STAFF

support principle 6, indicator 1 “All staff members are provided with explicit guidelines as to the kinds of ‘critical incidents’ that should be reported to the agency headquarters.” This principle however, includes three other indicators:
2.Allmanagersandsupervisorsaretrainedinappropriatefrontlineresponsestotraumaticincidents(e.g.psychoeducation,psychologicalfirstaidtoindividuals,managingteamresponsetotraumaticincidents,assessmentofindividualandteamresponses,andreferraltoorrequestsforfollowupsupportandcarewhenappropriate)
3.Theagencymakespsychosocialstaffwithspecifictraininginpsychologicalfirstaidavailable,onan‘asneeded’basis,toconsultwithstaffmembersaftertraumaticincidentsorothersourcesofacutestressinstaff.
4.Theagencyhasstandingarrangementswithspecialistsinsuchinterventionstoprovideassistancewhenitisneeded.”
In response to the fourthindicator, SWS reports they compile lists of regional specialists for referrals in different countries,76 although it is not clear how comprehensive these lists are, or how often they are updated, or how widely they are disseminated. In-country UNDSS stress counselors also exist in many locations. Terms of reference for UNDSS stress counselors include support to all UN staff in the event of a critical incident.
Compliance with indicators two and three is more challenging to ascertain. There are apparently some attempts to include elements of Psychological First Aid in written materials and trainings for peer support personnel (see text box 5. for a description of PFA). However, there does not appear to be any comprehensive PFA training being provided to UNHCR staff, nor is it clear to what extent SWS is actually practicing explicit PFA in the aftermath of a critical incident. Instead, it appears that SWS is continuing to provide general counseling and/or some elements of critical incident stress debriefing, otherwise referred to as ”CISD”. This is evident in SWS statistics which reference 19 ‘group counseling traumatic interventions’ provided in 2011. This suggests that SWS is still apparently using CISD or another non-PFA intervention, since PFA is not typically a group intervention, whereas CISD is. This is furthermore confirmed by SWS, “there is no formal PFA training.”77 However, per SWS correspondence, there appear to be plans to focus increased efforts on PFA-based intervention and training, “…[we find the] WHO manual on PFA very good. UNICEF and WFP have a simple guide on PFA for managers and we are looking at adopting that.”
UNHCR’s tentative adoption of PFA appears typical of the situation in other humanitarian agencies. While several agencies reported adhering to PFA principles and no longer using Critical Incident Stress Debriefing/Management (CISD/M), when they actually described how they provided crisis support, they in fact described the very elements of CISD/M now deemed by a majority of crisis intervention practitioners and researchers to be problematic. In addition, many of the staff welfare officers in humanitarian agencies were unable to clarify to what extent their crisis intervention protocols conformed to explicit elements associated with PFA and not CISD. ICRC stated they provided PFA but referred to a "psychological debriefing," which they offer once a year in collaboration with the University of Nottingham/Nottinghamshire Healthcare NHS. And indeed, NHS’s online training materials reveal that they are still using elements of CISD, not a PFAonly model.78
The confusion between CISD/M and PFA is not surprising considering that PFA only came to be accepted as the standard replacement for CISD in crisis situations a few years ago. In fact, a 2009 PeopleInAid study of 19 humanitarian agencies revealed that only 37 per cent were practicing “strict psychological first aid only,” whereas the remainder was still using CISD/M or a hybrid approach in the aftermath of critical incidents. With the proliferation of PFA manuals in the last few years however, and associated recommendations from influential organizations such as the National
76 Based on various reports and personal correspondence.77 Writtencorrespondence,SWS, 2012.78 CentreforTrauma,ResilienceandGrowth,NottinghamshireHealthcareNHSTrust.CISM Programmme, 2011.
45A Global Review

Child Traumatic Stress Network in the United States and the World Health Organization, it is clear organizations will be increasingly accountable for demonstrating compliance with PFA. In addition, while PFA is currently evidence-informed, the evidence base for PFA will likely grow in the coming years as additional research is conducted in emergency settings worldwide. Those in charge of staff well-being initiatives with humanitarian organizations should keep an eye on these unfolding developments to ensure compliance with the latest PFA protocols.
In order to further examine compliance with this principle, critical incident data from the online survey was reviewed. Support after a crisis and the associated protocols are especially important to UNHCR due to the prevalence of trauma and critical incident exposure. Of respondents to the online staff survey, 45 per cent experienced an incident in which they believed their life was in danger or they thought they would be seriously injured; 38 per cent experienced an incident in which they witnessed someone else being seriously injured, killed, or threatened in a manner that led them to believe their life was in danger. Only 33 per cent of those exposed to a critical incident said they received any type of support within 24 hours of the incident.
Of the 33 per cent who received support within the first 24 hours, support was provided by the following persons (respondents were able to endorse multiple sources of support): Friends – 27 per cent; Family – 22 per cent; UNHCR manager – 11 per cent; Other UN staff – 10 per cent; UNHCR peer support member – 7 per cent; UNHCR Staff Welfare Officer – 6 per cent; UNHCR Administrator – 5 per cent; Staff from other non-UN agencies – 4 per cent; Others- 4 per cent; UNHCR Medical Officer – 3 per cent. Of those only 32 per cent received support consistent with core components of PFA, including elements such as “helping you to feel safe; assisting you by providing up to date information about the situation; providing information on normal psychological reactions you might experience; helping you to make practical arrangements as needed; helping you to connect with social supports; linking you with support services for additional follow up”. This suggests UNHCR is not doing an effective job of providing the recommended crisis intervention (Psychological First Aid) in the aftermath of critical incidents for most survivors. The majority of survey respondents did not
Chad / looted warehouse in Abeche. © UNHCR / N. Ndolde / 26 November 2006
46 UNHCR’S MENTAL HEALTH AND PSYCHOSOCIAL SUPPORT FOR STAFF

receive support within the first 24 hours, a critical time period for survivors. For the minority who did receive this early support, only one third received support consistent with PFA.
What other agencies are doing to implement this principle
OCHA Critical Incidents - OCHA is working to better equip staff for critical incident response and has ordered copies of the WHO Psychological First Aid guidelines for all staff, although there is no formal PFA training offered. There is an interest, however, in building capacity to ensure OCHA staff “can be first responders for one another.”
CARE Critical Incident and PFA Manual - CARE has developed an excellent agency-specific critical incident protocol manual, including an emphasis on psychological first aid for all staff: http: //www.slideshare.net/lcripe/critical-incident-protocol
Text Box 5
Psychological First Aid
“Acuteanxietyafterexposuretoextremestressors(e.g.traumaticevents)isbestmanagedfollowingtheprinciplesofpsychologicalfirstaid…Itentailsbasic,non-intrusivepragmaticcarewithafocusonlisteningbutnotforcingtalk,assessingneedsandconcerns,ensuringthatbasicneedsaremet,encouragingsocialsupportfromsignificantothersandprotectingfromfurtherharm.Psychologicaldebriefing(i.e.thepromotionofventilationbyencouragingthepersontobrieflybutsystematicallyrecountperceptions,thoughtsandemotionalreactionsexperiencedduringarecent,stressfulevent)isatbestineffectiveandshouldnotbeapplied”
(IASCMHPSSguidelines, 2007, p. 335).
Psychological first aid (PFA) has become the psychosocial intervention of choice to address immediate concerns of survivors of critical incidents (Schafer, Snider & van Ommeren, 2008). PFA is a replacement for Critical Incident Stress Debriefing (CISD), which fell out of favor primarily due to research indicating 1) minimal effects, 2) no effects, or in some cases, 3) harmful effects on later distress (Rose, Bisson , Churchill, & Wessely, 2009; see Uhernik & Husson, 2009 for a review). As a result of concerns associated with CISD, trauma experts at the Center for the Study of Traumatic Stress began working to clarify guidelines for disaster response and other forms of crisis intervention. These guidelines eventually evolved into the PFA model we have today (Uhernik & Husson, 2009). WHO released a PFA manual in 2011, PsychologicalFirstAid:GuideforFieldWorkers. WHO and others have come out with statements condemning the use of CISD, including what is often referred to simply as ‘psychological debriefing’ or ‘debriefing’:
“Becauseofthepossibilityofpsychologicalharmtoindividualparticipants,‘PsychologicalDebriefing’shouldNOTbeapartofthestandardmentalhealthresponsetocrisisanddisastersituations…”
Medical Reserve Corps -National Child Traumatic Stress Network - National Center for PTSD: Position Statement on CISD (2006)
According to Sphere (2011) and IASC (2007), Psychological First Aid (PFA) describes an appropriate response to a fellow human being who may be suffering and needs support. Notably, and unlike CISD, PFA is an intervention that does not require mental health professionals, but can instead be used by laypersons, and includes the potential for onward referral to mental health specialists if necessary. PFA is intended to support both short and long-term adaptive functioning and is evidence-informed. In other words, it is consistent with research on risk and resilience following trauma but rigorous outcome research on the efficacy of PFA is still in its infancy (Uhernik & Husson, 2009; NCTSN, 2006). PFA is intended to be flexible, allowing for modification depending on the local context.
47A Global Review
PRINCIPLE 7: END OF ASSIGNMENT SUPPORT The agency provides practical, emotional and culturally appropriate support for staff at the end of an assignment or contract. This includes a personal stress review and an operational debriefing.Several years ago, UNHCR began a pilot program in exit debriefing upon separation from UNHCR, but apparently the scope was limited. Others have suggested UNHCR should perform end of assignment briefings.79
Some career counseling is provided by UNHCR when posts are terminated: this is usually through the Career Management Section, when the cuts affect international staff, and through SWS when an office is being closed and many national posts will be eliminated.80 However, this is limited. In addition, the Antares indicators for this principle also specifically refer to access to a confidentialpersonalstressassessment for all transitioning or existing staff, which does not currently exist in UNHCR.
Some smaller organizations are able to offer this level of personal attention. For example, Tearfund, an agency highlighted in the 2009 PeopleInAid/InterHealth research on staff care in humanitarian organizations “requires all returning field-based staff to attend a ‘returner’s medical check-up’ at a preapproved travel health clinic and has an opt-out policy for a post-assignment psychological debriefing with one of three psychologists or three professional counselors: all of whom have received additional training by Tearfund to provide an appropriate debriefing experience.” An opt-out policy means that the activity is scheduled for everyone unless a staff member indicates in advance that they do not wish to participate.
This principle also refers to transitions from one assignment to another. Survivors of critical incidents, in particular, may need additional follow up and support during such transitions. During the online survey staff endorsing exposure to critical potentially traumatic incidents were asked: “When transitioning to a new job assignment and/or location has any UNHCR staff member, e.g. manager, Staff Welfare Officer, peer support member, Medical Officer, ever talked with you about your stress level and use of coping techniques?”, 82 per cent of critical incident survivors who confirmed having experienced at least one transition to a new assignment or location answered no.
PRINCIPLE 8: POST ASSIGNMENT SUPPORT The agency has clear written policies with respect to the ongoing support they will provide to staff members who have been adversely impacted by exposure to stress and trauma during their assignment.
This principle is comprised of the following two indicators:
1. The agency has a clear policy aimed at protecting the jobs of employees who have job stress-related disabilities such as ‘burnout,’ depression, or PTSD.
2. The agency has policies for employees who are unable to continue working for the agency due to job-related stress or injury. This addresses issues such as continuation of salary and benefits and provision (or financing) of medical and/or psychological services.
When deemed eligible, the 2012 UNHCR sick leave policy allows staff members to take time off for psychological reasons. There are also some associated disability policies in UNHCR that cover mental health disability, e.g. staff can apply for compensation through the compensationboardforserviceincurredinjuries. This requires a psychiatric evaluation. In addition, it appears a staff member
79 SeeStateofUNHCROrganizationalCulture,2005.80 Writtencorrespondence,SWS, 2012.
48 UNHCR’S MENTAL HEALTH AND PSYCHOSOCIAL SUPPORT FOR STAFF

must be formally separated to be eligible for their national disability scheme. SWS shared, “We have developed a strategy for long term support of the survivors of such incidents that includes the admin, HR/work, security, psychological and medical issues,” but this was not consistent with some of the experiences shared by survivors of critical incidents during this evaluation.
Additionally, none of this appears to explicitly address job protection and benefits for staff who have “job-related disabilities such as ‘burnout,’ depression, or PTSD.’” Data from a group of eight UNHCR survivors of critical incidents was used to assist in interpretation of UNHCR’s compliance with this indicator. Several survivors feared for their jobs after they developed mental health symptoms following exposure to traumatic incidents while working for UNHCR. The following quote is relevant to this section; it is from a survivor who worries s/he will have to quit UNHCR because s/he has not been offered a post where s/he can get appropriate treatment for his/her PTSD or feel minimally safe:
Theyclearlydon'tgetit.Isobbeduponreadingthe[post]offer.Nomatterhowmuchwetrytobeheard,theydonotseemtohearorunderstandus.AllIhaverequestedistobeabletoslowlyre-immersemyselfbackintothefieldandtobeinalocationwhereIcansleep...UNHCRclearlyneedssensitizationexercisesforallstafftobetterunderstandthelong-termeffectsoftraumaticincidents,aswellaspoliciesonhowtomanagecareerservicesforaffectedstaff.”
This suggests critical incident survivors do not always find the support they seek, especially support for gradual reintegration. Concern for one’s job is likely to compound the stress associated with trauma exposure and undermine recovery efforts.
4.2 Summary Score for Antares Principles
In summary, UNHCR was compliant with only 2 out of 8 Antares Principles and one-third of the associated indicators (see Annex I: Antares Framework: UNHCR’s Indicator Level Scores). Antares is the not the only reference document utilized. IASC MHPSS Guidelines (2007), Sphere Minimum Standards (2011) and research on staff welfare initiatives by InterHealth and PeopleinAid (2009) were also considered throughout this report. These other documents are largely consistent with Antares principles and associated indicators, and in some cases contributing authors to these reports also contributed to development and revision of the Antares’ framework.
Consistent with initiatives underway at comparator organizations, UNHCR could improve screening procedures. Simulation exercises for provisional new hires are one way of screening out for undesirable characteristics such as an inability to tolerate uncertainty and stressful, ever-changing conditions. More comprehensive screenings, including a clinical interview combined with standardized instruments, would be an improvement over the minimal screening protocol in place currently. More comprehensive information on potential risk factors for developing adverse outcomes following field-based stress exposure, such as prior trauma exposure or a history of PTSD, cannot ethically be used as a screen-out tool. However, this information can be used to provide additional support to staff that may be especially vulnerable.
Systematic monitoring and evaluation of staff mental health and psychosocial well-being should also be introduced. For example, UNICEF conducts online surveys every few years, allowing the agency to monitor well-being over time. Country-specific evaluations could also be conducted, especially in areas considered to be particularly stressful. Although this is not an effective means of planning a given treatment for an individual, it does allow for a cost-effective targeted resource buildup in operations where a significant number of staff are experiencing distress.
Monitoring and evaluative efforts should include rigorous assessment of effectiveness of existing programs. This is particularly important when UNHCR introduces pilot initiatives. An objective
49A Global Review
external review should be conducted to determine if allocating the resources necessary to scale up programming is warranted. Staff preference for programs deemed appropriate by staff welfare should be reviewed. In some cases staff may prefer alternative interventions. Ideally, staff utilizing formal staff welfare services, including peer support personnel, would complete a brief anonymous satisfaction survey online. This information should be processed by an independent third party and staff welfare services should be held accountable for the results.
UNHCR should also offer more comprehensive and diverse ongoing support. Examples already referenced include WFP’s emphasis on utilizing local therapists, online self-assessment tools, Skype consultations; USAID’s 24/7 staff support services; ICRC’s linkages with local NGOs specializing in staff care, etc. UNHCR should also review the UNICEF developed booklet, ‘TipsforManagers:HowtoCreateaSupportiveWorkplace.’ It is inadequate to expect those in need to independently approach SWS or a PSP volunteer; staff welfare personnel must reach out to all staff, ideally emphasizing prevention, and provide a variety of options. Staff should be encouraged to utilize therapeutic supports as a preventative tool for coping with stress, before distress becomes unmanageable.
Comprehensive and explicit critical incident protocols should be in place, widely disseminated, and managers should be trained and held accountable for compliance.81 UNHCR should reference CARE’s critical incident and PFA training materials and protocols. All potential first responders should have basic psychological first aid skills.
Finally, systematic follow up support is lacking after and during transitions between assignments. In light of this, UNHCR should review TearFund’s post-assignment ‘opt-out’ psychological check-up. Again, staff should not be wholly responsible for self-determination of needs, coupled with a willingness to seek services. Such a passive system likely means many of the most severely distressed will slip through the cracks.
4.3 Managerial Responsibility for Staff Well-being
This is a cross-cutting issue associated with Antares’ principles linked to training, monitoring and ongoing support. As such, it is deserving of further consideration and thus warrants this separate section in this report. Although some management training is in place, managers should be evaluated on their ability to promote, and not undermine, staff welfare. This was a concern that figured prominently in stakeholder interviews, during field missions, and in responses to the online survey.
During the field-based research, staff provided examples of former Heads of Sub-Office who encouraged staff care, e.g. walked around at the end of the day encouraging people to go home on time, provided opportunities for work-sponsored social activities, monitored and encouraged regular use of annual leave balances, encouraged staff to contact staff welfare and provided the use of a confidential phone for this purpose. They also provided examples of those who undermined staff well-being, such as those who were verbally abusive toward staff, penalized staff if they went home promptly at the end of the day or didn’t want to come in most weekends, expected staff to be on call 24/7 for even non-emergency personal requests, discouraged staff from taking leave, made statements suggesting that anyone exhibiting symptoms of stress and burnout probably wasn’t suited for this work.
Many internal interviewees, mostly Heads of Units and Representatives, also emphasized similar concerns. Several internal stakeholders mentioned a lack of knowledge, willingness, and accountability of mid-level and senior managers to mitigate staff stress, providing example of the ways in which some managers contribute to staff stress by being verbally abusive, and unwilling to allow national staff in particular to work reasonable hours. Several interviewees indicated that
81 SWS reports that some heads of office in hardship locations received PFA training as a component of the Security Management Learning Programme. The total number of participants could not be verified.
50 UNHCR’S MENTAL HEALTH AND PSYCHOSOCIAL SUPPORT FOR STAFF

for some managers the product appeared to be more important than the process. In other words, “get the work done at any cost”. Some interviewees even reported that some managers appear to believe that encouraging staff well-being will negatively affect productivity. Multiple interviewees mentioned concerns that some managers known to be “difficult” were intentionally sent to hardship duty stations, places where in fact, the best managers are needed and staff well-being is particularly important.
In addition to information collected while on field mission and during remote stakeholder interviews, a bank of questions in the online survey was designed specifically to get at indicators associated with a healthy work environment, including elements of managerial responsibility for promoting staff well-being (see survey questions 7-18, 21-22, Annex II). In response to the question, “Do managers in your current location emphasize the importance of staff well-being?” 17 per cent indicated Yes,mostemphasizestaffwell-being; 54 per cent indicated “Yes, some emphasize staff well-being” and 30 per cent indicated “No, none emphasize staff well-being”.
In response to the open-ended question, “If you are a manager what do you do to emphasize staff well-being?” the majority of responses covered the four categories below:
� Openness and Availability: dialogue, hold meetings, ensure availability, staff involvement in the decision making process;
� Work-Life Balance: encourage staff to take leave, time-off and breaks to ensure work-life balance, and, to provide flexibility in working hours;
� Distribution of Workload: promote fair work distribution amongst staff, demonstrate respect, planning processes, equality, transparency, and recognition;
� Socializing: encourage trainings, social events and activities.
These ideas are consistent with staff feedback on preferred strategies to mitigate stress and current research on common sources of stress, e.g. lack of work/life balance, lack of accessibility to one’s supervisor. UNHCR needs to promote a subculture in which managers who implement these initiatives are rewarded and recognized and those who undermine staff well-being are held accountable.
Additional survey responses underscore some of the challenges associated with promoting staff well-being in a fast-paced organization addressing complex emergencies. Sixty-six per cent of respondents indicated they frequently work overtime. Of those who work overtime, only 23 per cent indicated they receive compensatory time off. Sixty-one per cent indicated the workload is not divided equally among staff based on their jobs. Forty-three per cent indicated they do not have an updated job description. Thirty-seven per cent indicated activities in their operation or work unit are not well defined. Thirty-one per cent indicated the leadership structure in their operation or work unit is not clear. Twenty-seven per cent indicated they do not have regular staff meetings. Twenty-three per cent indicated international and national staff do not have a good working relationship. It is important to note here that 77 per cent of staff indicated they do have a good working relationship. Thirty-seven per cent of respondents indicated members of senior management do not regularly visit their country or operations at the sub and field office level or keep in touch in other ways.
In a demanding, multicultural environment where many staff are working long hours, conflict is perhaps to be expected. When asked about the type of conflict that is common in “your operation or work unit”, the most frequent responses were: 1) Lack of transparency and information sharing; 2) Inequitable treatment by management and an inequitable distribution of the workload; 3) Mistrust and misunderstandings, including disrespect between local and international staff and gossip; and, 4) Human Resource policies and office politics. The survey then went on to ask how to ameliorate these complaints.
When asked how UNHCR might promote team building and mutual respect among colleagues, the most common responses were: 1) Retreats and recreational activities including team-building
51A Global Review

events, meetings and trainings; 2) Inclusion in the decision-making process along with equal treatment and recognition; 3) Maintaining integrity and adherence to the Code of Conduct through professionalism, transparency, trust and respect; 4) Fostering communication and information sharing along with feedback and fair staff rotations; 5) Evaluations and other accountability mechanisms with the provision of external resources; and, finally, 6) An increase in the number of staff or a decrease in the workload, along with improvement of HR policies and hiring processes.
Consistent with these responses to the online survey, teambuilding, including social events, was a common response when asked about preferred coping strategies for managing chronic stress during field missions. Sixty-five per cent of survey respondents had participated in some form of teambuilding exercises with other UNHCR staff in the past two years.
These survey responses underscore the influence of management in maintaining a healthy workplace, including promoting or undermining staff well-being. Holding managers explicitly accountable is crucial in changing the organizational culture and minimizing distress arising from workplace stressors. When only 17 per cent of survey respondents indicate most managers in their current location emphasize staff well-being, managerial accountability toward psychosocial support of staff appears to be neglected in the workplace culture of UNHCR.
Ensuring management accountability when it comes to promoting staff well-being is challenging. This is not something the Staff Welfare Section can address independently, but involves multiple sections and requires high level support within UNHCR. This challenge is recognized by SWS:
TheintroductionoftheGlobalStaffSurveyin2006anditsimplementationthereafterhasintroducedalotofdiscussionaboutmanagement’sinterestinandcommitmenttothestaffwell-beingissues[emphasisadded].Therehasbeenlittleactionfollowingfromthatanditstillnotclearwhatactionwouldtakeplace.”
4.4 Stress and Coping
Stressors - It is essential to understand common sources of stress before developing interventions designed to mitigate stress. In order to identify common stressors in UNHCR, online survey respondents were provided with a list of 16 items that were derived from previous research with humanitarian workers. The top six stressors identified by UNHCR staff in 2012 were nearly identical to those identified by UNICEF staff in 2003 and 2009 (see Figures 3 and 4 below), with a few notable exceptions: for UNHCR staff ‘family concerns’ were rated as the 4th most frequent stressor (29 per cent); for UNICEF staff this wasn’t in the top five in 2003 or 2009. For UNICEF ‘relationship with supervisors’ was cited as one of the top five stressors (in 2003, 44 per cent; relationships with colleagues 26 per cent). For UNHCR relationship with supervisors was ranked as a significant source of stress for 27 per cent of respondents (relationship with colleagues caused significant stress for 15 per cent). Although Figure 3. emphasizes the top five stressors for UNHCR, it is important to note the other frequently endorsed stressors: 1) working hours – 21 per cent; 2) safety concerns – 20 per cent; 3) political situation in country where you’re currently working – 18 per cent; 4) inability to achieve work goals or objectives – 17 per cent; 5) health concerns – 17 per cent; 6) exposure to suffering of persons of concern – 16 per cent; 7) exposure to incidents where you were seriously injured or your life was threatened – 7 percent.
ThetopsourcesofstressidentifiedbyUNHCRstaffwerenearlyidenticaltothoseforUNICEFstaffinsimilarsurveys.
52 UNHCR’S MENTAL HEALTH AND PSYCHOSOCIAL SUPPORT FOR STAFF

Figure 3: Top Stressors for UNHCR Staff online survey (2012)
0
0
10
20
20
40
30
60
40
50
80
Workload
Workload/inability to achieve work
goals
42
76
Status of contract
Feeling undervalued/not able to contribute
to decisions
40
58
Feeling undervalued
Status of contract
40
54
Family concerns
Political situation in-country
29
51
Inability to contribute to
decisions
Relationship with supervisor(s)
28
44
Figure 4: Top Stressors for UNICEF, Staff Stress Survey (2003; 2009)
Note: 2003 data above from “Caring for Us: Stress in Our Workplace,” UNICEF, 2nd edition, MacDonald & Curling (2004). 2009 data from Curling & Simmons (2010): 1) Workload; 2) Ability to achieve work goals and objectives; 3) Working hours; 4) Status of employment contract; 5) Feeling undervalued and/or unable to contribute to decision making.
Twelve per cent of online survey respondents endorsed the ‘other’ category for stressors and provided associated detail. Some of these included mention of specific cases of sexual harassment, however the majority of ‘other’ responses were as follows: 1) Poor management; 2) Lack of delegated authority; 3) Internal policies and bureaucracy that hinder service delivery to persons of concern; 4) Inconsistency in the application of HR rules; 5) Wasted resources; and 6) Inadequate resources to help Persons of Concern. Some of this is consistent with issues raised with the Office of the Ombudsman.
53A Global Review

Figure 5: Issues raised with the Office of the Ombudsman 2011
121
41%
22
7%
60
17
9
1417
23
12
3%
4%6%8%
6%
5%
20%
Job and Career
Peer and Coleague Relationships
Evaluative Relationships
Compensation and Benefits
Value, Ethic and Standards
Organizational, Leadership and ManagementSafety, Health, Wellbeing, Stress and Work/Life
Legal, Regulatory, Financial and Compilance
Services/Admin Issues
Figure above reprinted from Office of the Ombudsman UNHCR 2011 Annual Report.
Qualitative data on significant stressors collected during field missions was largely consistent with these online survey responses. Top stressors in Bangladesh and Pakistan are listed in the order of frequency in Table 4.
It is important to emphasize that the online survey data and field data are fairly consistent, lending credibility to online survey responses, despite the relatively low response rate.
Safety and security is an issue that deserves further examination. Although online survey respondents and those in Bangladesh and Pakistan mentioned security as a significant source of stress, most survey respondents felt they were adequately prepared to deal with security concerns. In response to the question, “Do you think you have adequate training and equipment to deal with potential security concerns?”, 74 per cent indicated ‘yes.’ This suggests some elements of security-related stress may not be mitigated by additional resources.
Sexual harassment is another issue that also warrants further consideration. In cultural settings with rigid gender role expectations, where women entering the workforce are seen as a threat to men’s livelihoods, sexual harassment seems to be particularly common. In more than one office, female staff provided examples of sexual harassment from male colleagues of a chronic and often indirect nature, apparently intended to slowly erode their desire to continue working with UNHCR. Women who adhere to cultural prescriptions, e.g. wear a veil, and those who do not, appear to equally be targeted. Victims of harassment are often reluctant to come forward, making this stressor difficult to address, as has been noted by the office of the Ombudsman:
Sexualharassmentissuesareevenhardertohandleforstaff.Inaddition,staffarereluctanttobringtheirconcernsoutintheopen,forfearofbeingstigmatizedorretaliatedagainst.TheOmbudsmanOfficewasnotveryoftenapproachedinrelationtosexualharassment."2010 Annual Report, Office of Ombudsman
54 UNHCR’S MENTAL HEALTH AND PSYCHOSOCIAL SUPPORT FOR STAFF

Table 4: Top Stressors for Staff in Bangladesh and Pakistan
Category of Stressor Bangladesh Pakistan
focus groups
individual interviews
focus groups
individual interviews
Status of employment contracts, including short-term contracts; late renewal of contracts; lack of long-term job security. 100% 77% 62% 20%
Workload, described as more work than one person can be expected to handle, competing task demands, conflicting deadlines, too much paperwork, bureaucracy, and inequitable distribution of work.
100% 85% 77% 80%
Relationship with supervisors including competing requests from many informal ‘supervisors’ i.e. people of higher authority; along with frequent changes in supervisors and the associated changes in management style and performance expectations.
80% 77% 85% 20%
Family concerns, including family separation and not enough time for family. 80% 69% 46% 20%
Feeling undervalued, described by participants as not feeling appreciated or recognized for one’s contributions to the organization.
60% 77% 62% 40%
Working hours. 60% 54% 69% 60%
Relationships with work colleagues, including team tension and conflicts. 20% 84% 77% 60%
Safety concerns including a fear of travel late at night, the lack of adequate training or equipment to deal with emergencies. 60% 31% 92% 40%
Sexual harassment. 0% 20% 77% 6%
Exposure to suffering of Persons of Concern was noted as a significant cause of stress for some survey respondents and focus groups in Bangladesh and Pakistan. Such ‘vicarious trauma’ or secondary stress may be even more pervasive than this data indicates. This is a stressor that may be difficult for staff to articulate and may function largely outside of conscious awareness. Over time, the cumulative effects of this type of distress, especially if accompanied by associated feelings of helplessness, may contribute to ‘burnout’ and a desire to leave the humanitarian field.
Additional questions were asked during the online survey to tap possible stressors based on existing research and good practice standards on staff care. For example, questions on living conditions were included because environmental stressors have been identified as a common source of stress for humanitarians in previous research. Staff were asked, “Are you able to obtain adequate food and water not only for drinking but also to engage in washing in a manner consistent with your religion and culture?”, and 94 per cent indicated ‘yes.’ Staff were also asked, “Do you have a minimally comfortable and safe place to live?” and again, 94 per cent indicated ‘yes.’ Although recent mission reports indicate inadequate conditions for colleagues in specific locations, e.g. CAR, Ethiopia, South Sudan, the results from the online survey suggest that the majority of respondents feel they have adequate accommodation and resources.
In order to differentiate amongst the duty stations, the online survey included a few questions for those who have served in hardship settings. Staff were asked, “If you have ever worked in a C, D, or E duty station - are ‘entitlements’, e.g. R&R/ STO, annual leave, hardship allowance/danger pay, being implemented?”, and 83 per cent indicated ‘yes,’ while 14 per cent indicated ’no.’ Staff were asked, “If you have ever worked in a C, D, or E duty station - does UNHCR make an effort to manage the security risks facing international and national staff equally?”, and 56 per cent indicated ‘yes,’ while 44 per cent indicated ‘no.’ Although entitlements appear to be implemented, the perception that security risks are not equitable between national and international staff warrants further consideration. Of course, it is often the case that national staff are more frequently in the field monitoring, putting them at increased risk. As numerous sources indicate, the majority of humanitarian workers killed worldwide are national staff. “National humanitarian workers,
55A Global Review

constituting upwards 90 per cent of humanitarian workers in the field, bear the brunt of attacks, due to the nature of their jobs at the frontlines. International staff do face a higher incident rate per capita than national staff, especially in high-risk internationalized contexts. 82”
In summary, some of the sources of stress for UNHCR staff are consistent with stressors in other humanitarian organizations such as UNICEF. Most of the stress is related to the administrative aspects of their working arrangements followed by the relational aspects. For the most part, data collected through the online survey, during field mission to Bangladesh and Pakistan, and through stakeholder interviews is consistent, lending credibility to findings from this evaluation, despite low response rates to the online survey.
Distress
Although an online survey cannot be used for diagnostic purposes, questions were included to tap symptoms commonly associated with depression and post-traumatic stress disorder. Survey respondents were asked, “Please consider, are you currently experiencing, or have you in the past month experienced, any of the following? (check all that apply)”.
Table 5: Distress Reported by Survey Respondents
Frequency Symptom Description
57% Feelings of sadness, unhappiness, or ‘emptiness’
54% Irritability or frustration, even over small matters
50% Fatigue, tiredness and loss of energy — even small tasks may seem to require a lot of effort
47% Difficulty sleeping or sleeping more than usual
38% Loss of interest or pleasure in normal activities
28% Trouble thinking, concentrating, making decisions and remembering things
27% Changes in appetite, less hungry or more hungry than usual
23% Frequent aches or pains, headaches, cramps, or digestive stomach problems that do not ease even with treatment or do not seem to have a clear explanation
22% Feelings of worthlessness or guilt, fixating on past failures or blaming yourself when things aren't going right
20% Slowed thinking, speaking or body movements
19% Restlessness — e.g. pacing, hand-wringing or an inability to sit still
19% Numbing, or feeling emotionally disconnected from others
16% Avoiding thoughts, feelings, conversations, activities, places, people associated with stressful events
15% Feeling “jumpy” when hearing noises e.g. phones, doors, cars, thunder
12% Feeling disconnected from your life, like nothing is real, as if you were in a movie
13% Images, thoughts, dreams, illusions, flashback episodes, or a sense of reliving stressful experiences
10% A reduction in awareness of surroundings e.g. "being in a daze"
8% Crying spells for no apparent reason
6% Frequent thoughts of death, dying or suicide
Note: Eighty-nine per cent of survey respondents endorsed at least one item above.
Again, although not diagnostic, survey respondents endorsed symptoms typically associated with post-traumatic stress disorder and depression at high rates, with almost 60 per cent indicating “feelings of sadness, unhappiness, or ‘emptiness’”. In addition, even 6 per cent of survey
82 OCHA Factsheet.
56 UNHCR’S MENTAL HEALTH AND PSYCHOSOCIAL SUPPORT FOR STAFF
respondents indicating “frequent thoughts of death, dying or suicide” is disconcerting and begs the question, is UNHCR doing enough to address suicidal ideation? Aside from suicidal thoughts, some might suggest these symptoms should only be of concern if clearly interfering with work performance. Some of the online survey items were designed to address this issue.
Staff were asked, “Are any of the items checked interfering with your ability to: Do your job?”, and 42 per cent indicated ‘yes’. Staff responded at an even higher rate to a modification of the question asking whether the checked items are interfering with his or her ability to “Maintain relationships with your family, friends, or colleagues?” Forty nine per cent of the survey respondents indicated ‘yes’ to this question.
The examination of sub-groups of survey respondents indicated a significant difference between national and international staff on a few important items. In response to the question, “Are any of the items checked above interfering with your ability to do your job?”, significantly more national staff replied "yes" than international staff.83 Interestingly, there was no significant difference between national and international staff in their response to a similar question about interference with relationships with family, friends, and colleagues.84
This data highlighting symptoms that may be indicative of depression and PTSD is consistent with UNHCR’s sick leave data suggesting high rates of psychiatric conditions. In 2012 psychiatric conditions were the leading cause of missed work in the form of sick leave globally for UNHCR, representing 18 per cent of the total sick leave days lost in a given year.
83 Chi squared analysis: (c2 (df = 1, N = 849) = 6.30, p = .043).84 Chi squared analysis (c2 (df = 1, N = 849) = 5.57, p = .062). There was no significant difference on either of
these questions based on location of work (HQ v. others).
Indonesia / Tsunami disaster / An impromptu meeting between UNHCR and community leaders on the beach in Tagaule, one of the three submerged villages on Nias Island. © UNHCR / J. Perugia / November 2005
57A Global Review

Coping
Exposure to stress does not necessarily result in long-term distress. Often staff members have effective means of coping with stress. Any intervention to mitigate stress typically involves efforts to enhance healthy coping strategies. Online survey respondents were asked about their preferred coping strategies, with a list provided based on previous research and items derived from common coping measures. The following items were endorsed in order of frequency.
Table 6: Coping Strategies
Frequency Symptom Description
49% I've been trying to see it in a different light, to make it seem more positive
43% I've been taking action to try to make the situation better
42% I've been trying to learn to live with it
37% I've been getting emotional support from others
36% I've been doing something to think about it less, such as watching TV, reading, daydreaming, or sleeping
35% I’ve been trying to get advice or help from other people about what to do
34% I've been making jokes about the situation, using humor
25% I've been trying to find comfort in my religion or spiritual beliefs (praying, meditating)
24% I've been expressing my negative feelings, complaining, venting to get the frustration out
20% I've been working more to try to take my mind off things
12% I’ve been criticizing or blaming myself
12% Other
8% I've given up on trying to deal with it
6% I've been using alcohol or other drugs to make myself feel better
Note: Online survey respondents were asked about their preferred coping strategies. A list was provided based on previous research and items derived from common coping measures.
This suggests a preference among online survey respondents for reframing, active coping, acceptance, social support, distraction, religious support and venting. Although less frequently endorsed, self-blame, disengagement and use of substances were reported by between 6 to 12 per cent of survey respondents.
It is not surprising that 6 per cent of staff noted use of alcohol or other drugs in order to cope. Another question on substance use was asked: “What percentage of UNHCR staff that you have worked with do you think drink alcohol to excess or use substances to excess, in a manner that interferes with their work performance?”, results indicate 48 per cent of survey respondents believe between 10-20 per cent of UNHCR staff drink alcohol or use substances to excess, in a manner that interferes with their work performance. When asked, “Are you satisfied with the way UNHCR addresses substance abuse?”, roughly equal numbers of respondents indicated satisfaction - 51 per cent, and dissatisfaction - 49 per cent.
Research on resilience, benefit finding and post-traumatic growth over the last decade emphasizes the importance of exploring the possibility that persons may perceive some positive aspect from exposure to potentially traumatic or other stressful events. As a result, the following question was included: “Sometimes people report unexpected or surprising benefits associated with stress exposure. In your case, have stressful experiences with UNHCR resulted in any of the following?” The results are provided below.
Forty-eight(48%)ofrespondentsbelievebetween10-20%ofUNHCRstaffdrinkalcoholorusesubstancestoexcess,inamannerthatinterfereswiththeirworkperformance.Sixpercentadmittedusingsubstancestocopewithstress.
58 UNHCR’S MENTAL HEALTH AND PSYCHOSOCIAL SUPPORT FOR STAFF

Table 7: Unexpected Benefits associated with Stress Exposure as a result of Humanitarian Work
Frequency Benefit
37% I changed my priorities about what is important in life
33% I know better that I can handle difficulties; I’m stronger than I thought I was
29% I have a greater appreciation for the value of my own life
18% I have a greater sense of closeness with others
17% I enjoy my work more and am performing better
16% I have a stronger religious faith
15% I established a new path for my life
12% I learned a how wonderful people are
This suggests a significant number of staff perceive some benefit associated with stress exposure during the course of work with UNHCR. Likewise, optimism has been associated with resilience and ‘hardiness.’ In order to determine the prevalence of optimism amongst UNHCR staff, the following statement was included: “I can find something positive in even the most difficult situation.” The results indicate more resilience than not with 48 per cent stating “Usually true”; 30 per cent said “True about half the time”; and 16 per cent said “Always true”.
In summary, in addition to the online survey responses, the coping data from field missions highlighted a number of unique preferred coping strategies including a preference for reframing and engaging informal support systems. Staff said they turn to family and friends, and when they do turn to a coworker, it has to be someone they trust. Staff in Bangladesh and Pakistan also indicated a preference for time off, use of humour, entertaining distractions such as a movie, religious and spiritual activities including praying, talking to a religious leader, going to a mosque/church/temple, exercising, travel, and writing in a diary. Recommendations have been developed to enhance the possibility that staff can access positive coping mechanisms with an eye towards enhancing natural resilience.
4.3 Critical Incidents
The following section includes critical incident information from the online survey and additional data collected from a small group of critical incident survivors. Sections are organized by critical incident exposure; critical incident specific distress; satisfaction with critical incident response; and service utilization among critical incident survivors.
Critical Incident Exposure
Online survey responses suggest exposure to potentially traumatic events is high among UNHCR staff: Forty-five per cent experienced an incident in which they believed their life was in danger or they thought they would be seriously injured; 38 per cent experienced an incident in which they witnessed someone else being seriously injured, killed, or threatened in a manner that led them to believe their life was in danger. Although, as has been emphasized elsewhere in this report, we can’t assume these survey respondents are representative of all staff in UNHCR, this does produce some striking data – based on survey respondents alone, there are at least 498 UNHCR staff who have experienced an incident in which they believed their life was in danger, and 417 who experienced an incident in which they witnessed someone else being seriously injured, killed or seriously threatened. Even if critical incident survivors were more likely to respond to the survey, if exposure prevalence is even half of that reported on the survey that suggests another 1,500 or so UNHCR staff with direct critical incident exposure in the total population. Given the prevalence and types of interpersonal violence worldwide it is likely a significant number of these are survivors of sexual assault.
59A Global Review

In an attempt to better understand the experiences of critical incident survivors within UNHCR, additional data was collected from eight survivors, five women and three men. Three are from North America, four are from Africa, and one did not provide demographic data. This is an experienced group, the mean number of years with UNHCR = 14.5 (range 7 – 21), seven of the eight are above the age of 40. They work in various sectors including Protection, Programme, Management, and other areas. All members of the group have experienced at least one critical incident during which they feared for their life. The incident exposure breakdown is detailed n Table 8. Five of the eight have also witnessed others being killed, seriously injured, or having their lives threated. Survivors answered individual questionnaires and participated in a third party facilitated focus group to solicit recommendations for improvement in critical incident response.
Table 8: Critical Incident Exposure (among subgroup of 8 survivors)
Frequency Category of Incident
5 (63%) Life threatened during violent demonstration/uprising
2 (25%) Kidnapped/held hostage
2 (25%) Bombing
2 (25%) Sexual Assault
2 (25%) Physical Assault/ armed robbery
1 (13%) Motor vehicle or plane accident
Note: Totals are greater than 100 because several persons were exposed to multiple incidents. The majority of incidents in “life threatened during violent demonstration/uprising” includes being shot at or otherwise threatened with a weapon. Several persons experienced more than one incident.
Critical Incident related Distress
This same groups of eight critical incident survivors was asked about distress associated with the potentially traumatic event. The table below provides details indicating a number of symptoms commonly associated with post-traumatic stress disorder, depression, functional impairments in work, and a variety of other long-term consequences.
Table 9: Distress Reported by Subgroup of Critical Incident Survivors (N = 8)
General Category of Distress
Specific Description of Distress
Symptoms commonly associated with post-traumatic stress disorder and/or depression
• Lack of concentration
• Fatigue
• Excessive stress, feeling “stressed out”
• “Emotional weakness”
• “Depression”
• Jumping at loud noises
• Afraid of the dark
Additional physical/ somatic complains
• High blood pressure
Functional impairment in work domain
• Low morale
• Loss of confidence in the organization
• Uncomfortable around UNHCR staff
• Job performance has suffered
• Lost professional experience
• Unable to work
• Difficulty with day to day activities
Additional long-term consequences
• Loss of self-confidence
• Feeling like a different person
• “Emotionally scarred”
• Uncomfortable around men
• Medical bills
• Victim’s family is worried about person’s well-being
• Unemployed
• Lost pension
• “Paying for health insurance because claim for compensation hasn’t been accepted for an extended period”
• No place to live
• “In need of long term therapy”
60 UNHCR’S MENTAL HEALTH AND PSYCHOSOCIAL SUPPORT FOR STAFF
Critical Incident Response
Having extensive input from this subgroup of eight survivors provides a unique opportunity to examine what worked in a given critical incident. Unfortunately, numerous concerns were raised by critical incident survivors indicating: 1) Inadequate information exchange; 2) Minimal short and long-term support; and 3) Discrimination and harassment from colleagues, in the aftermath of the incident.
Information exchange in the immediate aftermath of the critical incident - Four of the eight survivors indicated UNHCR was informed of the incident immediately by themselves or someone else. The other four did not respond to this question. Of those who stated UNHCR was informed, three informed management, one chose to inform a trusted coworker, and one also informed security. Five of the eight indicated relevant persons in headquarters, e.g. security, staff welfare and medical, were informed about the incident by the office. Allbutonepersonindicatedthattheirnamewasusedwithoutaskingtheirpermissionwheninformationabouttheincidentwassharedforreportingpurposes. This includes the sharing of the survivor’s name associated with graphic sexual assault details. In some cases many people were copied on the correspondence.
Despite this disregard for confidentiality, with wide dissemination of incident reports in some cases, the majority of survivors did not receive a copy of the incident report themselves. For those who did, only two received a copy in a timely manner. Another two persons had to advocate for a copy and eventually were provided with information. Four of the eight survivors felt the reporting of the incident was not handled in an appropriate manner primarily due to lack of sensitivity toward the survivors. In half of the cases, a formal investigation was conducted that involved UNDSS, UNHCR security focal points, and/or local authorities. None of these four survivors received a copy of the formal investigation report despite several of them having expressed an interest in obtaining a copy. As a result, most are left wondering about the case outcome to this day.
Support in the immediate aftermath of critical incident - Of the eight critical incident survivors who completed additional surveys and interviews, five stated that they received support from UNHCR within the first 24 hours of the incident, while the remaining three indicated support from UNHCR was delayed, and in some cases never provided. Of those receiving immediate support, two received support from a trusted colleague, two from senior management, two from staff welfare, one from security, one from admin, and one from junior staff (several persons indicated more than one type of support person). The most common forms of support provided were some form of medical assistance, including medical evacuation and time off. Most indicated UNHCR did not help to facilitate contact with loved ones.
Longer-term follow up - Follow up is necessary to check in about distress level and ability to cope with any adverse consequences of the incident (see text box 5 for categories of distress experienced by critical incident survivors). Only 25 per cent of the eight critical incident survivors said UNHCR followed up within one to three months after the incident. Another 50 per cent indicated that UNHCR provided some minimal check-in but deemed it inadequate. Twenty-five per cent indicated no follow up was provided at all.
Discrimination and harassment - Fifty per cent of survivors indicated they had been treated in a discriminatory or harassing manner by at least one colleague after the incident, some elaborating in great detail on the stigma associated with being a “survivor.” This may have been in part due to a lack of concern for survivor privacy, with incident details disseminated throughout the office in some cases. This is yet another reason why long-term follow up with critical incident survivors is crucial.
Sexual assault as distinct from other types of critical incidents - Two sexual assault victims shared detailed information about UNHCR’s response in the immediate and longer-term aftermath of the incident. In both cases UNHCR appears to have failed to provide minimally adequate support. Several stakeholders also commented on the lack of comprehensive protocols in place, and lack of training and accountability for managers, when it comes to sexual assault of staff. In a few cases stakeholders even made comments indicating that UNHCR knows what to do when a refugee is sexually assaulted, but not a staff member. Other stakeholders commented that UNHCR appears
61A Global Review

to do a better job in responding to bombings and other forms of critical incidents than sexual assaults, and that UNHCR is better at addressing concerns with the victim is a male. It is important to note there are some important differences between responses to sexual assaults and other critical incidents. For example, asking a survivor of sexual assault for detailed information about the incident can be invasive. In addition, they may be socially ostracized if colleagues are informed of the event, especially in cultural settings where rape survivors are perceived as “dirty” or “spoiled.”
4.4 Satisfaction with Critical Incident Response
…wearefirsttraumatizedbyourexperiencesand,subsequently,undergosecondarytraumatizationbywayofneglect/abandonment/denialbyouremployer,theUN…”UNHCR staff, survivor of critical incidents
Although the online survey did not include a question on satisfaction with UNHCR response to critical incidents, the group of eight UNHCR critical incident survivors contacted did answer a question regarding satisfaction with UNHCR’s response. Eighty-five per cent said UNHCR’s immediate response to their specific critical incident was inadequate. Of these, one-third said the response was eventually satisfactory, although initially slow. Sixty-two per cent of survivors indicated some level of general dissatisfaction with UNHCR’s response to critical incidents. Over half of survivors indicated they would not tell others to have faith in UNHCR’s response to critical incidents.
Figure 6: Critical incident survivors’ satisfaction with UNHCR response to critical incidents
37%
25%
13%
12%
13%Extremely Dissatisfied
Slightly Dissatisfied
Satisfied
Neutral
Extremely Satisfied
Service Utilization among Survivors of Critical Incidents
In order to enhance understanding of online survey responses and ask additional follow up questions, questions on serviceutilization were also put to the group of eight critical incident survivors.
Staff Welfare - When asked about willingness to contact the Staff Welfare Service should another critical incident occur, only two persons indicated they would do so. One indicated they would consider the option but are not sure if they would choose to engage. Another four stated they would not be willing to engage with staff welfare officers in the aftermath of a critical incident. One survivor stated s/he had no idea such an option was even available.
62 UNHCR’S MENTAL HEALTH AND PSYCHOSOCIAL SUPPORT FOR STAFF
One factor influencing utilization is the perceived efficacy of the staff welfare services. Although critical incident survivors and others participating in this evaluation stated they generally find the staff welfare officers to be very likeable and sincere, they often wondered if the current model of support is the most effective for addressing their individual needs, especially considering concerns about confidentiality. Below is a quote from a critical incident survivor:
Ithinkthey[SWS]aresympathetic,understandingbeingswhodeservesomecreditfortheirempathyandabilitytolisten…however,ifIweretoneedhelpagainorafriendweretocontactmeaskingwhotheyshouldconsult,Iwouldreferthemto[outsidetraumaspecialist].IsthisduetoaculturalissuewithinUNHCRthatsuggeststhatnothingisconfidential?Probably.”
Peer Support - Only one critical incident survivor indicated s/he would be comfortable going to peer support personnel in the aftermath of a critical incident. Two persons clearly indicated they would not engage with peer support volunteers; one other suggested ‘perhaps,’ and finally, one stated s/he did not know this option existed.
A UNHCR staff member comforts a child who was among a group of boat people earlier intercepted at sea by the Italian coastguards. © UNHCR / A. Di Loreto
63A Global Review
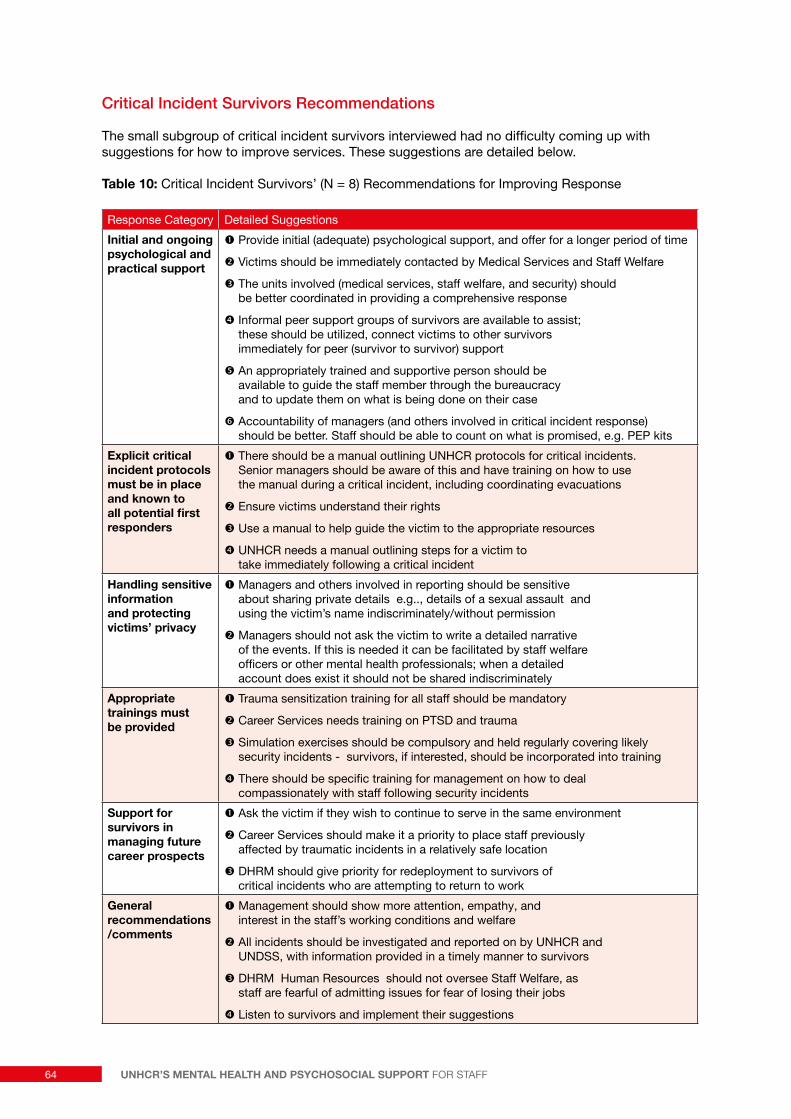
Critical Incident Survivors Recommendations
The small subgroup of critical incident survivors interviewed had no difficulty coming up with suggestions for how to improve services. These suggestions are detailed below.
Table 10: Critical Incident Survivors’ (N = 8) Recommendations for Improving Response
Response Category Detailed Suggestions
Initial and ongoing psychological and practical support
� Provide initial (adequate) psychological support, and offer for a longer period of time
� Victims should be immediately contacted by Medical Services and Staff Welfare
� The units involved (medical services, staff welfare, and security) should be better coordinated in providing a comprehensive response
� Informal peer support groups of survivors are available to assist; these should be utilized, connect victims to other survivors immediately for peer (survivor to survivor) support
� An appropriately trained and supportive person should be available to guide the staff member through the bureaucracy and to update them on what is being done on their case
� Accountability of managers (and others involved in critical incident response) should be better. Staff should be able to count on what is promised, e.g. PEP kits
Explicit critical incident protocols must be in place and known to all potential first responders
� There should be a manual outlining UNHCR protocols for critical incidents. Senior managers should be aware of this and have training on how to use the manual during a critical incident, including coordinating evacuations
� Ensure victims understand their rights
� Use a manual to help guide the victim to the appropriate resources
� UNHCR needs a manual outlining steps for a victim to take immediately following a critical incident
Handling sensitive information and protecting victims’ privacy
� Managers and others involved in reporting should be sensitive about sharing private details e.g.., details of a sexual assault and using the victim’s name indiscriminately/without permission
� Managers should not ask the victim to write a detailed narrative of the events. If this is needed it can be facilitated by staff welfare officers or other mental health professionals; when a detailed account does exist it should not be shared indiscriminately
Appropriate trainings must be provided
� Trauma sensitization training for all staff should be mandatory
� Career Services needs training on PTSD and trauma
� Simulation exercises should be compulsory and held regularly covering likely security incidents - survivors, if interested, should be incorporated into training
� There should be specific training for management on how to deal compassionately with staff following security incidents
Support for survivors in managing future career prospects
� Ask the victim if they wish to continue to serve in the same environment
� Career Services should make it a priority to place staff previously affected by traumatic incidents in a relatively safe location
� DHRM should give priority for redeployment to survivors of critical incidents who are attempting to return to work
General recommendations /comments
� Management should show more attention, empathy, and interest in the staff’s working conditions and welfare
� All incidents should be investigated and reported on by UNHCR and UNDSS, with information provided in a timely manner to survivors
� DHRM Human Resources should not oversee Staff Welfare, as staff are fearful of admitting issues for fear of losing their jobs
� Listen to survivors and implement their suggestions
64 UNHCR’S MENTAL HEALTH AND PSYCHOSOCIAL SUPPORT FOR STAFF
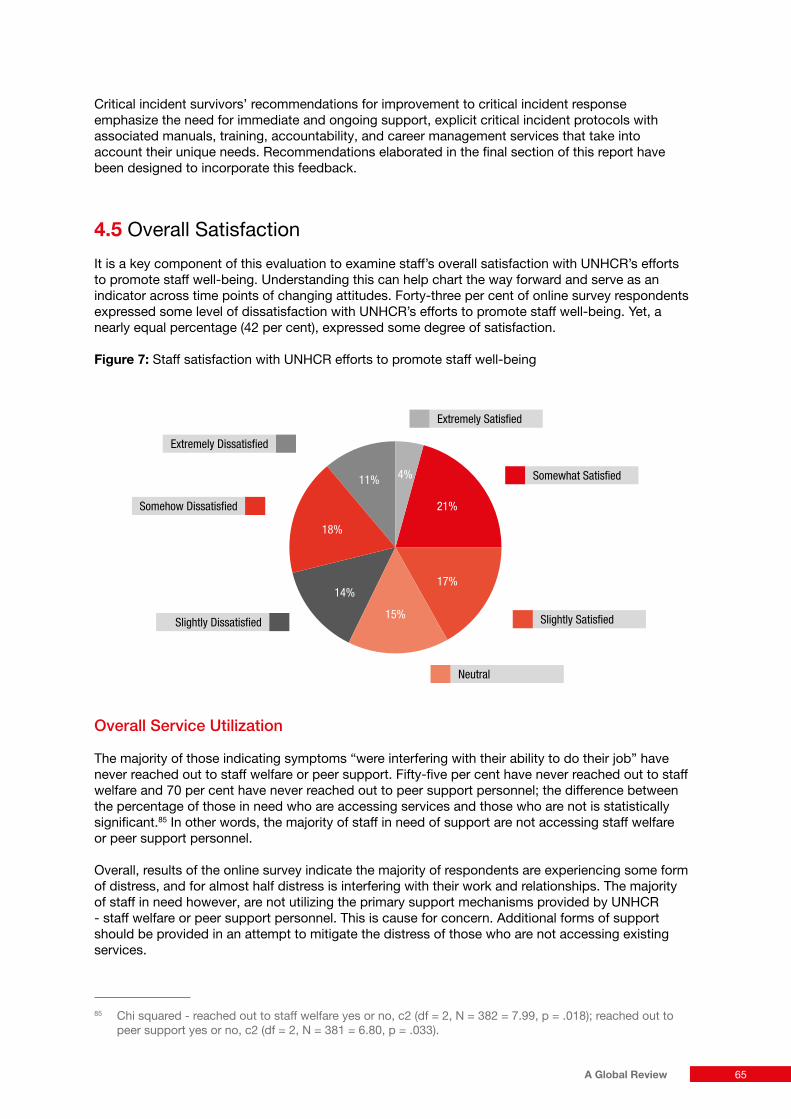
Critical incident survivors’ recommendations for improvement to critical incident response emphasize the need for immediate and ongoing support, explicit critical incident protocols with associated manuals, training, accountability, and career management services that take into account their unique needs. Recommendations elaborated in the final section of this report have been designed to incorporate this feedback.
4.5 Overall Satisfaction
It is a key component of this evaluation to examine staff’s overall satisfaction with UNHCR’s efforts to promote staff well-being. Understanding this can help chart the way forward and serve as an indicator across time points of changing attitudes. Forty-three per cent of online survey respondents expressed some level of dissatisfaction with UNHCR’s efforts to promote staff well-being. Yet, a nearly equal percentage (42 per cent), expressed some degree of satisfaction.
Figure 7: Staff satisfaction with UNHCR efforts to promote staff well-being
Overall Service Utilization
The majority of those indicating symptoms “were interfering with their ability to do their job” have never reached out to staff welfare or peer support. Fifty-five per cent have never reached out to staff welfare and 70 per cent have never reached out to peer support personnel; the difference between the percentage of those in need who are accessing services and those who are not is statistically significant.85 In other words, the majority of staff in need of support are not accessing staff welfare or peer support personnel.
Overall, results of the online survey indicate the majority of respondents are experiencing some form of distress, and for almost half distress is interfering with their work and relationships. The majority of staff in need however, are not utilizing the primary support mechanisms provided by UNHCR - staff welfare or peer support personnel. This is cause for concern. Additional forms of support should be provided in an attempt to mitigate the distress of those who are not accessing existing services.
85 Chi squared - reached out to staff welfare yes or no, c2 (df = 2, N = 382 = 7.99, p = .018); reached out to peer support yes or no, c2 (df = 2, N = 381 = 6.80, p = .033).
Somewhat Satisfied
Extremely Satisfied
Slightly Satisfied
Neutral
Somehow Dissatisfied
Slightly Dissatisfied
Extremely Dissatisfied
21%
4%11%
17%
15%
14%
18%
65A Global Review

As indicated earlier in this document, based on SWS statistics, their service utilization rate is between 11 to 22 per cent. Thus, it is not surprising then that 40 per cent of the survey respondents indicated they had contacted a staff welfare officer at some point in their UNHCR career. Of those who had contacted a staff welfare officer in the past, 83 per cent said they would recommend that other staff contact a staff welfare officer in times of need. Twenty-five per cent of survey respondents have approached a member of the peer support network for assistance, while 75 per cent have not utilized these services. Of those who had contacted peer support personnel, 85 per cent indicated they would recommend other UNHCR staff contact peer support personnel for assistance in managing stress.
For the 60 per cent who had not been in touch with staff welfare when they were asked “why not?” the most common responses were: “I was not aware that a staff welfare officer existed”; “I don’t have a need”; “I didn’t think it would be useful”; “I’m concerned about confidentiality; distance is a limitation; they are not available; I talked to someone else instead”.
Those who had not been in touch with peer support personnel were asked, “why not?” The most common responses were: “Iwasnotawarethatpeersupportpersonnelexisted”; “I don’t have a need”; “I’m concerned about confidentiality - they share with others in the office”; “I don’t think they have the necessary skills”; “They aren’t available”; “I don't have time or don't want to bother”.
The 2011 Global Learning Center evaluation of the PSP and Respectful Workplace Advisor (RWA) program indicated a high perceived need for support – 73 per cent, yet seemingly low utilization rates – 13 per cent in locations with a PSP or RWA in-country. Only 34 per cent of respondents said they felt comfortable discussing a problem with a PSP. Respondents also said they would rather address their problems outside of UNHCR than within it due to concerns over confidentiality and fear of possible retaliation.
This is consistent with the 2005 report on the State of UNHCROrganizationalCulture, indicating staff members fear judgment from colleagues if they expose personal stress-related issues. They are also hesitant to trust their peers because they fear revealing difficulties managing stress may put their job in jeopardy. Those accessing staff welfare and peer support generally find it helpful. However, many are choosing not to access these resources. A lack of awareness of services, concerns over confidentiality, and a lack of satisfaction with general services and critical incident response appear to play a role.
Factors influencing service utilization
Preference for outside support due to confidentiality concerns - Confidentiality concerns were mentioned repeatedly throughout the evaluation as a barrier to accessing services. This is consistent with other sources of data. In the 2011 impact evaluation for the PSP program only 34 per cent of respondents indicated they would be comfortable discussing a problem with Peer Support Personnel. Many respondents indicated a preference for addressing problems outside of UNHCR primarily due to concerns about confidentiality. In order to further investigate staff preference for outside mental health specialists we asked, “Would you prefer to have contact with someone who is not affiliated with UNHCR”, e.g. private counselor, someone from another agency?” 52 per cent indicated ‘yes,’ while 48 per cent were comfortable with in-house services. This, along with previous sources of information, indicates a substantial number of UNHCR staff are not accessing services because services are in-house. For many, in-house is associated with fears of lack of confidentiality and potential adverse career implications.
Thoseaccessingstaffwelfareandpeersupportgenerallyfindithelpful.However,manyarechoosingnottoaccesstheseresources.Lackofawarenessofservicesandconcernsoverconfidentialityappeartoplayarole.
66 UNHCR’S MENTAL HEALTH AND PSYCHOSOCIAL SUPPORT FOR STAFF

Preference for informal social support - Staff were also asked to compare formal and informal support mechanisms to each other: “Comparing informal support - friends, colleagues- and UNHCR's institutional responses -staff welfare officers, peer support network members, how would you rate the effectiveness of each of the two support mechanisms?” The responses indicate that most people, 86 per cent, find informal supports moreorequallyhelpful compared to ‘UNHCR responses’ to providing support.
• 50% I find informal support -friends, colleagues- more useful than UNHCR’s responses.
• 36% I find informal support - friends, colleagues- and UNHCR’s responses equallyuseful.
• 8% I find neither particularly useful.
• 7% I find UNHCR’s responses more useful than informal support - friends, colleagues.
Access to recreational activities - One way of accessing social support is through participation in group recreational activities. Seventy per cent of survey respondents indicated they have access to recreational activities, suggesting promotion of such activities should be relatively simple compared to situations where access is limited.
Engagement with online resources - The majority of survey respondents (56 per cent) indicated they have never looked at any of the well-being or stress management resources on the UNHCR intranet. This may be in part due to time constraints, but lack of interactive elements to make the website more engaging may also be a factor influencing service utilization.
Fifty-six(56%)percentofsurveyrespondentsindicatedtheyhaveneverlookedatanyofthewellbeingorstressmanagementresourcesontheUNHCRintranet.
On the border between DRC and Uganda, in Bunagana, a UNHCR staff leads a group of 21 refugees who just crossed, to the UNHCR truck that will transport them to the Transit Center. © UNHCR / Frederic NOY / November 2012
67A Global Review

4.6 Overall Staff Preferences and Recommendations
This section on ‘staff preferences and recommendations’ has been included in the hope that decision makers will consider this section alongside formal recommendations from the consultant. The consultant has attempted to develop feasible recommendations based primarily on current research, good practice frameworks, online survey responses, field data, and critical incident survivors’ feedback. It is difficult however, for formal recommendations to fully capture some of the details and nuance that is evident when staff are asked directly about whatworksandwhatdoesn’t.
Opinions about existing and proposed organizational means of addressing stressors are detailed in order of frequency/preference below (based on field data collected in Bangladesh and Pakistan).
Table 11: Staff Preference for Organizational Interventions (based on data collected in Bangladesh and Pakistan)
General Category Specifics
IDEAS MOST STAFF SUPPORTED ENTHUSIASTICALLY
Support for informal social support ‘Happy hour,’ team-building, social events with all staff and family
Training for staff (online or in-person) Critical incident response – Psychological First Aid;
Comprehensive Stress Management Training
Delegated authority to staff to develop their own stress management plans
Possibly route through staff council or committee set up for this purpose
IDEAS THAT RECEIVED MIXED REACTIONS (SOME CLEARLY LIKED, OTHERS CLEARLY OPPOSED)
Screening and Monitoring
Web-based Tools
Consultation with outside mental health specialists
Regionally or locally-based mental health specialists
Peer Support Personnel Access informally or have them provide more unsolicited regular check-ins and training
Staff Welfare Section in HQ Individual or group therapeutic intervention, available by phone, Skype, or in-person on mission
Formal complaint mechanisms IGO, Ombudsman
68 UNHCR’S MENTAL HEALTH AND PSYCHOSOCIAL SUPPORT FOR STAFF

5. Recommendations
Formal recommendations are provided in this section, incorporating feedback from:
1. Internal stakeholders, including senior staff from various sections and units, and country representatives;
2. Staff in the field;
3. Online survey respondents;
4. Critical incident survivors.
In most cases, additional justification, explanatory information, and resources have been provided in this section to contextualize these recommendations. However, information already provided throughout this report also serves as justification for recommendations (see Annex VI, ChainofEvidenceSupportingRecommendations).
As has been noted elsewhere, results based on the online survey with a low response rate, must be interpreted with caution, despite the fact that well over 1,000 staff took part in the survey. Considered in combination with field data and stakeholder interviews however, the online survey data makes significant contributions to understanding the mental health and psychosocial needs of UNHCR staff, and to informing recommendations concerning preferred services.
Findings from this evaluation indicate four broad areas of concern:
1. Lack of adequate response to critical incidents;
2. Inadequate utilization of formal MHPSS services, coupled with a lack of options for service utilization outside of UNHCR;
3. Lack of adequate support for informal peer networks, apart from the underutilized peer support network;
4. Lack of accountability for the adequacy of MHPSS services provided, in part due to minimal evaluative efforts, including a lack of formal means of collecting indicators on staff well-being and satisfaction with existing services.
Recommendations, detailed in the following section, attempt to address these shortcomings. It is often the case that staff knows what they need. In addition to reviewing suggestions in this section of the report, UNHCR should solicit feedback regularly from staff and be accountable to respond to staff suggestions for program improvements.
69A Global Review

5.1 Ensure Appropriate Response and Follow up for Survivors of Critical Incidents
In regard to the first finding that responses to critical incidents are inadequate, that this may be especially true for survivors of sexual assault,86 and that critical incident survivors don’t consistently receive appropriate psychological care, the following actions are recommended to strengthen UNHCR’s responsibility to affected staff and their colleagues:
a. Provide Psychological First Aid (PFA) for all potential first responders.
b. Disseminate UNDSS Standard Operating Procedures (SOPs) for sexual assault of staff to all field based managerial positions.
c. Conduct internal reviews following critical incidents to determine compliance with protocols, and as a means of soliciting feedback from survivors.
d. Prioritize jobs in low to moderate risk areas, at least in the short-term, for survivors of critical incidents.
e. Streamline procedures for recognition of service incurred incidents.
PFA for UNHCR Staff - Many of the survivors of critical incidents, both online survey respondents and additional persons interviewed, have described missteps by the agency, with UNHCR failing to explain procedures, contact loved ones, transfer them quickly to a safe location, etc. No comprehensive psychological first aid training is currently offered. PFA should be provided for all potential first responders to critical incidents, e.g. managers, administrators, security officers, anyone who will be on emergency call. Ideally all UNHCR staff should receive PFA, as this will not only be beneficial for staff survivors of critical incidents, but will also enable staff to better respond to persons of concerns in crisis. As mentioned elsewhere in this report, PFA is an early intervention that is appropriate for laypersons and does not require a mental health specialist. Critical incident survivors and staff in Bangladesh and Pakistan expressed enthusiasm about the possibility of PFA training for all UNHCR staff first responders.
In part because it is cost-prohibitive to provide training in person, online trainings should be considered. When financially feasible, live simulations to assess skills are an ideal companion to an online training. Publicly available, free, online PFA trainings87 exist as do mobile PFA phone apps.88 In addition, the Headington Institute offers various free, online training courses, including ones on secondary stress and vicarious trauma for humanitarian workers.89 Although adapting resources to the UNHCR context is useful, there is no reason not to utilize publicly available resources.
For more information on the PFA model in humanitarian settings and recommendations concerning training aid workers in PFA, see Sustainablecommunitymentalhealth:psychologicalfirstaidinhumanitarianemergencies, Deleon, Ditzler, & Hastings, 2009. “The authors propose that making PFA training available to aid workers will enhance their efficacy in helping survivors and provide a natural platform for the creation of a cadre of trained local providers to provide self-sustaining mental health assets…”
86 Based on feedback from a few survivors of sexual assault including detailed examples of breach of confidentiality, lack of available PEP kits, and an apparent lack of awareness on the part of some managers concerning protocol. While it is unclear how pervasive such problems are, this information is disconcerting enough to warrant recommendations specific to sexual assault response.
87 See NCTSN: http://learn.nctsn.org/course/category.php?id=1188 http://www.ptsd.va.gov/professional/pages/pfa_mobile_app.asp89 http://headington-institute.org/Default.aspx?tabid=2258
70 UNHCR’S MENTAL HEALTH AND PSYCHOSOCIAL SUPPORT FOR STAFF

Sexual Assault SOPs - Based on the feedback from a few survivors of sexual assault, it appears that UNHCR is not following existing protocols uniformly. This is likely due in part to a combination of factors, including a lack of awareness of protocols and a lack of accountability when managers fail to comply with protocols. UNDSS has produced the SOP for dealing with sexual assault which has to be followed because sexual assault is a security incident. In addition, SWS section indicates “…in the Security Management Learning Programme for the heads of offices, there is a section on management of stress in security and one of the case-studies we were using has been around sexual assault situation.”90
Internal Reviews - In addition to knowledge of agency-specific and UNDSS critical incident protocols, staff welfare and medical staff should have adequate training in rapid assessment of risk for lethality, e.g. suicide, homicide, and a safety plan in place for how to handle imminent threat. Comprehensive reviews should be conducted in the aftermath of a critical incident and in the event of suicide or homicide of or by a staff member to determine compliance with protocols. Procedures should be revised as needed.
5.2 Increase Availability and Utilization of Formal Mental Health and Psychosocial Support
The second finding of this review indicates that there is insufficient availability and utilization of formal mental health and psychosocial support services, especially for those most in need of services. The following recommendations provide suggestions that would enable staff to access appropriate MHPSS options and explore therapeutic arrangements that would meet their specific needs:
a. Provide and promote the option for staff to utilize external mental health therapists remotely, e.g. Skype, telephone interviews.
b. Provide and promote the option for staff to utilize local external mental health therapists and traditional healer or religious figures where these may be preferred options.
c. Disseminate information on what is covered by UNSMIS for international staff and the Medical Insurance Plan (MIP) for national staff for outside therapeutic support, and promote a diverse range of staff support options within these coverage parameters.
d. Invest in an interactive website, including an external confidential component, with self-assessment tools, and online follow up resources such as a Skype consultation with an internal or external therapist of choice. Provide links to existing eternally administered self-assessment tools such as https://ecouch.anu.edu.au/welcome
e. Annually, or at minimum during the end of an assignment or another transitional phase, provide a regularly scheduled mental health and psychosocial wellness checkup with the option for staff to decline at their own initiative: an “opt-out” model of compliance. Consider a brief mandatory mental health screen in the annual physical for those who “opt-out” of the more comprehensive evaluation. Use the annual physical as an opportunity to provide psycho-education about stress and coping and referral to external resources.
f. Put in place explicit means to ensure, and explain limits of, confidentiality. Written informed consent should be obtained for all staff receiving even brief internal or external services. This should include specifying if anyone can be informed of session content without additional express written permission from staff and other limits of confidentiality such as risk of harm to self or others. Staff in positions of authority should sign a confidentiality agreement. Reports of critical incidents should at minimum, be de-identified before being distributed. Critical incident reports should have very restricted distribution even when victim’s details have been removed.
90 Writtencorrespondence, SWS, 2012.
71A Global Review

In-house Counseling and ‘Outsourcing’ - The following section provides detailed suggestions for diversifying the type of mental health and psychosocial support available, and increasing utilization, especially among those who do not appear to be comfortable accessing in-house resources.
Amajorquestionfacingorganisationsinrecentyearsiswhethertoout-sourcestaffcarepracticeortohavethein-housecapacity…Wefoundthattheanswerisnottypically‘binary’,thatistosayeither/or,ratherthequestionishowmuchshouldbeinhouseorout-sourced...?Themaindisadvantages[ofin-housestaffcare]areconcernsofconfidentiality,costeffectiveness,andproximitytoin-countrylocations.” PeopleinAid/InterHealth, Approaches to Staff Care in International NGOs 2009, p. 17-19 .
…thesolutionisnotindecidingwhetheraninhousecounsellororoutsourcedsupportisbetter,butratherexploringbothchoicesasvalidoptionsanddeterminingwhichaspectsofin-houseandoutsourcedstaffsupportmechanismsarebestsuitedforspecificstaffneeds” Stress and Staff Support Strategies for International Aid Work Curling & Simmons, 2010, p. 101
Below are just a few examples of organizations providing counseling for humanitarian workers by phone, Skype, and sometimes in person.
Antares Foundation, Network of Staff Care Associates Worldwide
Antares has the capacity to provide support for even a large world-wide organization such as UNHCR. They are able to scale-up services within just a few months of a request by a humanitarian agency. In fact, they are in the process of “…finalizing a distance services system, which will enable humanitarian aid workers to have access [ ] to direct support by mail, Skype or phone. Within this system, e-learning modules on stress management on various levels will be made available as well”, personal communication, Antares, 2012. One of the international UNHCR staff interviewed while on field mission had experience using an Antares therapist for almost a year while working with another agency (INGO) in Africa. The therapist provided support by email and phone. The staff member found this remote communication with the therapist very helpful. http://antaresfoundation.org/support.htm
Other examples of organizations specializing in remote support services for humanitarian staff are Headington Institute: http://headington-institute.org, CARD Directory - Counsellors Assisting Relief and Development: http://headington-institute.org/Default.aspx?tabid=2327 and SalusWorld, with options including Skype, phone sessions, and trainings and short term counseling on location: http://salusworld.org/services/staff-welfare.php These are just a few examples, such organizations are not difficult to find. In fact, these types of remote services are increasing rapidly, in line with continuing trends in new technology.
Local Mental Health Providers - Identify and invest in country-specific mental health specialists and collaborators, including persons with culturally-specific knowledge who can provide trainings. UNHCR can consider cost-sharing efforts with other agencies in-country. This strategy has been recommended elsewhere, “…many low cost interventions are capable of providing highly valuable support to humanitarian staff…Creative alternatives include cost-sharing arrangements with local counselors on an inter-organizational basis, or training local counselors who then act as regional referral resources for an organization…the [in-house] staff counselor can identify local counselors while on mission travel and develop a professional relationship with them, facilitating referrals for staff in the field. In addition to being available for ongoing counseling, local counselors have a grasp on local conditions, culture and practices.”91 As part of this, UNHCR should continue to strengthen
91 Curling & Simmons (2010), p.101.
72 UNHCR’S MENTAL HEALTH AND PSYCHOSOCIAL SUPPORT FOR STAFF

collaborative relationships with UNDSS stress counselors in the field, and contribute to capacity-building when necessary.
Although the online survey, field data, and stakeholder interviews indicate many staff would like to have options other than in-house counseling, it was important to the majority that such persons have humanitarian experience, or at minimum, knowledge of the humanitarian context:
Forme,itiscriticalthatthetherapist/clinicianhaveexperiencewithhumanitariansettingsand,inthecaseofUNHCR,ithelpstohavesomeonewhounderstandsUNculture.Mytherapistin[]92livedin[]for12yearsandcompletelyunderstoodme.But,mytherapistin[]worksonlywithUNstaffandknowsthecultureaswell...Thishashelpedmeimmensely.Ithinkit'sabsolutelycritical.”
SWS is already making progress in this direction:
• “Syria avails of the temporary services from an international psychologist.”
• “Lebanon is about to recruit a local psychologist to work with the staff on once-a-week basis.”
• “We are expecting an additional full time position for Somalia emergency next year.”
• “Referrals to the counselors of other UN agencies or NGOs is regular practice in location where we do not have a SWO and in location where we trust the quality of service provided by the sister agency’s counselor or NGO counselors e.g. in Dadaab, there is a Center for treatment of victims of torture.”93
During the course of this evaluation, the office in Bangladesh worked directly with a local UNDSS-trained therapist, contracting her to provide stress management training and individual mental health check-ins. Her training was evaluated favorably by staff and included the following components: overviewofstressandburnout,casestudiesandgroupwork;aself-assessmenttoolforstressand‘burnout;’examplesofstressmanagementstrategies;reviewofrelaxationtechniquesandbreathingexercises;andthedevelopmentofindividualstressmanagementplans.
Utilizing Insurance Benefits to Pursue Outside Support - Information obtained from various sources during the course of this evaluation suggests it may be easy for staff to visit outside mental health specialists for up to 15 sessions94 annually without having to justify themselves to UNHCR, and assuming they agree to pay 20 per cent of the cost of each session. Longer term support is limited. It appears to be the case that if staff wants to continue beyond the 15 sessions they must subject themselves to scrutiny in order to determine if their mental health need is 'severe' enough to warrant continued coverage up to 50 sessions. Rather than go through a process of determination of whether their mental health need warrants coverage, most staff will likely either: 1) Choose not to see anyone, although they think they should; 2) Speak to UNHCR staff welfare unit or peer support volunteers, although many worry about the implications for their career and confidentiality; or, 3) See someone outside of UNHCR whom they pay for directly out of pocket.
During this evaluation one person shared that they had an external, remote therapist when they joined UNHCR, but it was their understanding they were not allowed to continue with this person, instead they were encouraged to use in-house counselors. Another UNHCR staff member explained they had been seeing an outside therapist but when the 15 sessions were up they decided to discontinue therapy rather than have their therapist submit a request for extension with supporting justification to UNHCR.
92 Some identifying information omitted to maintain confidentiality.93 Writtencorrespondence, SWS 2012.94 There is apparently a lower cap (6 sessions) on services from psychiatrists.
73A Global Review

It is still encouraging to think that staff can access counseling outside of UNHCR for up to 15 sessions, with no questions asked or reporting obligations to UNHCR, at the reimbursement rate of 80 per cent. Assuming this is actually the case, it seems staff should be made aware of this possibility; most staff do not appear to understand this.
Interactive websites - Increasingly, agencies are relying on information technology to provide services for remote areas. UNHCR will benefit from website development, adding interactive features such as:
• Skype or other remote means for consultation or therapy
• Self-assessment tools 'burnout,' 'general stress reactions,’ PTSD, depression
• Testimonials from respected senior staff/mentors sharing their experiences with critical incidents and/or chronic stressors video testimonials or quotes. Use Headington as a model for self-help and self-assessment resources and humanitarian workers’ stories - http://www.headington-institute.org/Default.aspx?tabid=1792
• Distribution of social normative data about humanitarian workers' common stress reactions based on recent research
• Referral information for local/ country-specific mental health professionals or other sources of support
• List of suggested healthy coping strategies
• Personalized stress management plan template for use by staff
See Annex IV for examples of interactive, user-friendly web-based staff well-being initiatives. The example of a campaign targeting members of a subculture with a high degree of stigma around mental health and help seeking, “ISTSS Real Warriors campaign for service members” may also be of use in considering similar initiatives for UNHCR: http://www.realwarriors.net
External website - Several people mentioned a concern that the agency could trace their information through the computer IP address and explained that they feel more comfortable using an external site, especially for things like self-assessment and coping tools and consultation with external providers. UNHCR could consider a model similar to USAID’s internal website http://staffcare.usaid.gov with a link to an external private and confidential website with additional tools.
Monitoring and Ongoing Support during Transitions - Information on stress management and general psychological wellness is not collected during annual physicals, resulting in a missed opportunity to engage in ongoing monitoring and to provide ongoing support, especially for those unlikely to reach out on their own. However, mental health and psychosocial wellness should not be assessed solely by the physician providing the annual physical: a separate provider is needed to avoid the impression that medical will use this information in a punitive manner. When staff members show signs of distress and associated functional impairment, this provider could refer them to appropriate local or remote resources. Considering the high rate of critical incident exposure, mental health care providers to UNHCR staff should give particular consideration to screening for signs of PTSD.95
95 “Thisyear’sannualmeetingofUNStaff/StresscounselorswillalsoaddressthequestionofmonitoringthedevelopmentofPTSDespeciallyfollowingmasscasualtyincidents(Haiti,Nigeria...)wherethechallengeofdiagnosingismuchbigger.WehaveChrisBrewinoftheUniversityCollegeLondonwhowillhelpusaddressthisissue…”(written correspondence, SWS, 2012).
74 UNHCR’S MENTAL HEALTH AND PSYCHOSOCIAL SUPPORT FOR STAFF

5.3 Encourage Informal Social Support Among Staff
The third finding of the review requests UNHCR to strengthen peer to peer support amongst staff since this is the support system UNHCR staff indicated that they rely on most heavily in times of distress. The current Peer support personnel (PSP) model is insufficient as a means of promoting informal social support amongst staff. It can be improved through the following:
a. Improve selection, accountability, and utilization of existing peer support network members in operations deciding to retain this model.
b. Channel formal, peer support resources such as training to more broad-based low-cost informal peer support groups and team building activities, including country or office-specific well-being initiatives.
c. Provide corporate (managerial) support to ad-hoc critical incident survivor groups.
d. Identify senior staff within the organization willing to speak frankly about their struggles with distress and ‘burnout’ to act as role models.
e. Provide mental health first aid training (MHFA) for all managers.
f. Building on mandatory training on sexual harassment, provide advanced gender sensitivity training for all staff.
g. Investigate peer based support models for alcohol and other forms of substance abuse and consider pilot initiatives to examine receptivity of staff.
Peer Support Personnel - Field-based discussions with ten peer support personnel, one RWA, and other staff, in addition to online survey responses, suggests peer support personnel would benefit from comprehensive psychological first aid and mental health first aid training. Online survey responses and previous evaluations indicate peer support personnel are likely underutilized. Providing them with specific delegated authority, e.g. for trainings in a train the trainers model and evaluating their performance through anonymous office-level surveys, may address quality control concerns and increase utilization. However, it is clear some people will still be uncomfortable with the specific persons selected as peer support personnel. Consequently, it is essential to enhance the skills of all staff to promote utilization of informal peer support networks.
‘Expert-driven’ Individual Counseling vs. Delegated Authority to Staff - Although mental health experts are required at times, a growing body of evidence indicates informal social support is associated with a variety of well-being indicators. Staff should be encouraged to develop their own well-being initiatives.
Themeansbywhichtheorganizationaddressesthesupportneedsofstaffisvariableand,forsome,inadequate.Giventheindividualnatureoftheexperienceandexpressionofstress,nosinglesolutionsareabletomeettheneedsofall,evenifthestressderivesfromsimilarsources…Accordingtonumerousorganizationalresearchfindings,systemicororganizationlevelinterventionsarelikelytohavefargreaterimpactthanindividualinterventions.”96
When asked during field mission to Bangladesh and Pakistan, staff easily generated their own ideas about maintaining/enhancing staff well-being (see earlier section on recommendationsfromstaff). These typically included opportunities to socialize with work colleagues and include family members. Staff explained they would like to be given the delegated authority to develop Annual Well-being Plans, with the possibility of some small associated budget for implementation. In fact, some are working on this already, independently collecting donations through local staff councils to plan events.
96 State of UNHCR’s Organizational Culture (2005) p.95.
75A Global Review
Ad hoc/Informal Peer Support for Critical Incident Survivors - An ad-hoc peer support group for survivors of critical or traumatic incidents has formed, spearheaded by a few active survivors. This should not be confused with the formal peer support mechanism (PSP) coordinated by UNHCR. This group is independent, although they have been in touch with the Staff Welfare Section. While it is clear that this group may not be representative of survivors within UNHCR as a whole, the group formed to fill a perceived gap in services for survivors and as such, has important contributions to make based on personal experience.
The group has offered to be available to other survivors of critical incidents. They are also developing a peer support website, specifically for critical incident survivors. They have requested this website be independent from UNHCR to ensure confidentiality and increased chance of utilization. This appears to be a small yet vibrant group of motivated members, willing to be a resource for others. SWS should consider how to capitalize on this informal peer support resource for immediate and long-term support for critical incident survivors, especially given staff and other resource limitations within SWS. The group needs managerial support to thrive.
Senior Staff Role Models - Ideally, senior staff, especially those who are well known within the agency, would step forward and admit their own struggles, setting an example for others. This would increase visibility of those who have experienced stress related challenges associated with critical incidents and/or chronic stressors. It is important to formally identify those willing to be role models among senior management, and other survivors of critical incidents, to help with messaging around normal responses to stress and to illustrate that you can come forward and say "I struggled," and still be respected and perceived as competent. This may be challenging to set up due to stigma and fear, but during the course of this evaluation a few country representatives shared personal experiences and indicated that such experiences have resulted in their being highly motivated to help others through similar struggles. Some members of the survivor-led support group have also expressed an interest in participating in such an initiative.
Peer models for alcohol and other forms of substance abuse - Six per cent of online survey respondents endorsed the use of alcohol to cope with stress. Typically such information is underreported. More telling perhaps is that almost half of all survey respondents believe between 10 and 20 per cent of UNHCR staff drink alcohol or use substances to excess in a manner that interferes with their job performance. While punitive agency policies may have limited success in curbing reliance on alcohol and other substances to cope with stress, peer support models have enjoyed some success and may be well received by UNHCR staff, especially if concerns over confidentiality can be addressed. An anonymous online model might be a useful starting place for a pilot initiative.
76 UNHCR’S MENTAL HEALTH AND PSYCHOSOCIAL SUPPORT FOR STAFF

5.4 Enhance Accountability of Staff Welfare Related Services through Rigorous Evaluations, Clear Staff-Welfare Policies and Roles
In response to the final finding calling for increased accountability of staff welfare both within the Division of Human Resources Management (DHRM) and at the line manager level, it is recommended that systematic and rigorous evaluations of functions affecting staff well-being take place along with the wide-scale dissemination of clear policies on roles and responsibilities for staff care.
a. Develop protocols for regular evaluation of staff distress levels and satisfaction with staff support services, e.g. online surveys; pre and post measures for specific programs; anonymous online evaluations for SWS mission visits, using indictors such as – “burnout” surveys, various forms of distress symptoms.
b. Evaluate managers on staff welfare indicators such as staff perception of support through anonymous means.
c. Introduce a new UNHCR Staff Care Policy and follow next steps recommendations made by PeopleInAid for UNHCR Duty of Care Project 2011.
d. Clarify the roles of relevant services within DHRM – the Staff Welfare Section, Medical, and Career Management Services.
e. Reallocate roles in SWS, with greater emphasis on case management; coordination and referral to external, country-specific and remote web-based therapeutic resources; capacity building, including support and replication of innovative country-specific pilot initiatives; and decreased emphasis on direct service provision.
Staff Surveys for Monitoring - Whether through independent comprehensive surveys, e.g. reusing the staff well-being survey created for this evaluation or a few additional questions on the Global Staff Survey, a regular agency-wide monitoring mechanism should be put in place. “Systematic anonymous surveys to review staff morale and staff concerns …are examples of elective resources that improve staff well-being.”97 SWS appears to be making plans to move in the direction of increased monitoring and evaluation: “We have one G5 assistant at the HQ and we have received the support for an additional G6 position. That will help in a number of research activities in the section” (SWS, written correspondence, 2012).
Management Accountability and Healthy Workplace - Research has highlighted the importance of managers’ leadership skills in promoting staff morale and enhancing staff well-being.98 In the Global Staff Survey in 2011, 54 per cent of staff agreed with the statement, “UNHCR’s management is interested in the well-being of employees.” Elsewhere in this report, examples have been provided of managers who promote, and those who undermine, staff well-being. Managers themselves have also provided best practice examples suggesting it may be prudent to utilize managers who are effective to train and mentor others. In addition, critical incident survivors provided several examples of the failure of managers to respond appropriately in the aftermath of critical incidents. Although some managers are trained in staff welfare, they are not evaluated adequately on their actual abilities and demonstrated behaviors.
97 Curling & Simmons (2010), p. 103.98 Bowie, Fisher & Cooper (2005).
77A Global Review

5.5 Feasibility and Threats to Implementation of Recommendations
Recommendations elaborated in this report are informed by supporting evidence from several sources;99 please refer to Annex VI, ChainofEvidenceSupportingRecommendations. It is hoped that these suggestions represent cost-effective solutions to mitigating common sources of staff stress and enhancing effective coping. However, implementation challenges may result from a limited number of Staff Welfare Officers assumed to be responsible for the majority of recommendations. It is hoped that staff in other sections will also assume responsibility for following up with recommendations.
Throughout this evaluation many staff, especially those in headquarters, expressed frustration with what they perceive to be a lack of will within the agency to address staff welfare issues resulting from chronic stressors, notably issues related to management accountability. As such, it is possible that senior staff in positions of authority may not be sufficiently motivated to make changes. In addition, some recommendations may be met with responses such as ‘we are already doing that.’ Pilot and other initiatives benefitting very few staff however, cannot be viewed as evidence of comprehensive services, and should not be viewed as compliance with recommendations.
99 As a compliment to the good practice Antares and other frameworks e.g. IASC Guidelines for MHPSS in Emergencies, 2007, PeopleinAid have outlined core components of a ‘Global Model for Staff Care’ StaffCare:AGlobalApproach, Nowlan, 2012. These elements are: 1. 24/7 helpline; 2. Training for managers in the field; 3. Communication of support systems; 4. Local clinical resources; 5. Employee assistance programme with practical as well as psychological support; and 6. Online / digital access. These areas are consistent with recommendations highlighted in this report. For additional information on innovative programs, see PeopleInAid Case Studies, including a specific section on Staff Welfare: http://www.peopleinaid.org/resources/casestudies.aspx
Kenya / Floods in Dadaab / Airdrops of UNHCR relief items for refugees in Dadaab camps / UNHCR Emergency Supply Officer, Maurice Bisau, helps load airdropped items onto Red Cross trucks. © UNHCR / B. Bannon / 9 December 2006
78 UNHCR’S MENTAL HEALTH AND PSYCHOSOCIAL SUPPORT FOR STAFF

6. Conclusion
The field of humanitarian mental health and psychosocial support has changed rapidly in the last several years. We now have a body of research on common stressors, related distress symptoms, and effective coping strategies. For those working to promote staff well-being amongst humanitarians, it may be reassuring to realize our toolkit now includes creative solutions for providing low cost yet comprehensive support. This includes ensuring adequate resources for both national and international staff working in remote or high risk locations. The field is continuing to grow and it is likely that in another few years we will have amassed an even more comprehensive knowledge base for promoting resilience among humanitarians. Staff in charge of designing and implementing MHPSS for aid workers will need to stay abreast of these developments as they unfold.
UNHCR is to be commended for taking staff well-being seriously and working to put comprehensive services in place despite resources limitations. This evaluation represents an opportunity for UNHCR to reflect not only on what has been achieved, but more importantly, to address gaps in services. UNHCR is not compliant with good practice standards, and in fact, performs worse than comparator agencies. More must be done to standardize and expand efforts with regard to policy; screening and assessing; preparation and training; monitoring; ongoing support; crisis support; and, end of assignment and post assignment support. Although the initial good practice comparison was conducted based on desk review and interviews with staff in headquarters, this information was cross-referenced with online survey data, field data, and internal stakeholder interviews, painting a clear picture that suggests UNHCR is falling short of meeting good practice standards.
Chronic stressors are impacting work performance. UNHCR staff are most stressed by workload; the status of their contracts; feeling undervalued; family concerns; inability to contribute to decisions; and relationships with supervisors. This is consistent with data from the Global Staff Survey in 2011, emphasizing staff frustration with various aspects of career development and job and organizational culture, noting well-being is below external norms. Data from comparator agencies such as UNICEF suggests these stressors are not unique to UNHCR, but may be typical of humanitarian work, especially with a largely field-based U.N. agency. This should not be taken to suggest that such stressors are an unavoidable aspect of humanitarian work. Instead remedial measures should be taken to mitigate such stressors. Prevention is far more effective than efforts to intervene after distress levels have already become problematic. Nearly half of survey respondents indicated distress symptoms were interfering with their work and relationships. This suggests distress associated with common stressors may be compromising service delivery for Persons of Concern.
In addition to addressing chronic stressors, UNHCR has a responsibility to protect staff from harm associated with critical incidents such as bombing, kidnapping, and sexual assault. This evaluation indicates critical incident exposure is high among UNHCR staff. Nearly half of the survey respondents have experienced an incident in which they believed their life was in danger or thought they would be seriously injured. Almost 40 per cent have experienced an incident in which they witnessed someone else being seriously injured, killed, or threatened in a manner that led them to believe their life was in danger. This is a substantially higher rate of exposure to potentially traumatic events than among those outside of the humanitarian sector. Amongst the smaller subgroup of critical incident survivors interviewed, most had experienced incidents involving threat of death or injury in the form of being shot at or threatened with a weapon during violent demonstrations. Others had been kidnapped, held hostage, sexually or physically assaulted, robbed, or involved in serious motor vehicle accidents.
Given the combination of chronic work-related stressors and high rates of critical incident exposure, it is not surprising that one-sixth to one-half of survey respondents indicated that they experienced symptoms in the last month consistent with some aspects of depression and post-traumatic stress disorder. While it is important to acknowledge that the online survey used during this evaluation is not diagnostic of prevalence rates of PTSD or depression, the frequency of reported distress symptoms
79A Global Review

is alarming, especially in light of the high reported impact on job performance. Furthermore, for an estimated ten per cent of survey respondents, efforts to cope include primarily ‘negative’ coping, such as criticizing or blaming oneself, or using alcohol or drugs. These findings are consistent with other research examining common forms and prevalence of distress in humanitarians.
Although this seems to paint quite a bleak picture, information on resilience, hardiness, and ‘positive’ coping suggests most staff have some resources at their disposal. This is important to note because this provides an opportunity for UNHCR to capitalize on preferred forms of positive coping, including informal social support, and thus potentially minimize the need for expensive individual formal therapeutic services. One-third to one-half of survey respondents indicated use of informal social support and/or reframing difficult situations in a more positive or optimistic light to cope. Approximately one-third also indicated some unexpected benefits associated with stress exposure during the course of humanitarian work, including realizing they are stronger than they thought, feeling closer to others, deriving more enjoyment from work, and developing stronger religious faith. Field data was consistent with online responses in that the overwhelming coping strategy of choice was informal social support from family, friends, and trusted coworkers.
Service utilization is far from ideal, despite high rates of utilization reported by staff welfare services. The majority of online survey respondents indicating distress symptoms were interfering with their ability to do their job have never reached out to staff welfare or formal peer support personnel. This is consistent with data from other sources such as the Global Learning Center evaluation of the Peer Support Personnel and the Respectful Workplace Advisor program indicating high perceived need yet low utilization rates. This suggests the majority of those in need may not be accessing services. In addition, over half of survey respondents indicated they have never looked at any of the well-being or stress management resources on the intranet.
In contrast, those who do use services appear to feel supported. Nearly all of those who have used services stated they would recommend other UNHCR staff use staff welfare and peer support personnel. This warrants further examination. Perhaps those with certain types of needs are using services and finding these helpful, while those with more severe distress symptoms are not. For example, “HR/admin issues” and “personal/family problems” appear to represent a large proportion of those using formal staff welfare services according to UNHCR internal reports. These categories may not be comprised of those experiencing the greatest distress and associated interference with work performance. It is worth considering how to maximize service utilization among those not using services. Concerns about confidentiality and lack of awareness of available services appear to be two factors limiting utilization. A lack of confidence in UNHCR’s perceived commitment to staff well-being may also play a role. This was mentioned as a concern during multiple stakeholder interviews. Overall dissatisfaction may also explain low rates of utilization amongst those in greatest need.
Almost half of the online survey respondents reported some level of dissatisfaction with UNHCR’s efforts to promote staff well-being. In addition, of a small subgroup of critical incident survivors interviewed, nearly all said UNHCR’s immediate response to the incident was inadequate. Over half of survivors indicated they would not tell others to have faith in UNHCR’s ability to respond to critical incidents, although several did suggest UNHCR does a better job in responding to bombings than sexual assault. It is critical that UNHCR address the dissatisfaction amongst staff as one step in increasing service utilization. For a start, UNHCR needs to consider staff preferences and recommendations. Throughout this review staff clearly indicated a preference for options for formal support, including a choice of service providers outside of UNHCR, and increased opportunities for accessing informal social support, including social events with colleagues.
This evaluation provides a roadmap for addressing critical incident response, the under-utilization of formal services among those most in need, inadequate support for informal peer networks, and the lack of accountability in monitoring staff well-being and measuring satisfaction with staff welfare services. Detailed suggestions are provided consistent with recent intervention research, good practice standards, and staff suggestions for improvement.
At this point it bears reiteration that MHPSS for staff is not a luxury; instead it is essential for humanitarian organizations to function effectively. In an organization like UNHCR, services for Persons of Concern may be compromised if staff care is neglected. Humanitarian agencies are increasingly obliged to be concerned about the potentially debilitating effects of staff stress on the effectiveness of relief programs.
80 UNHCR’S MENTAL HEALTH AND PSYCHOSOCIAL SUPPORT FOR STAFF
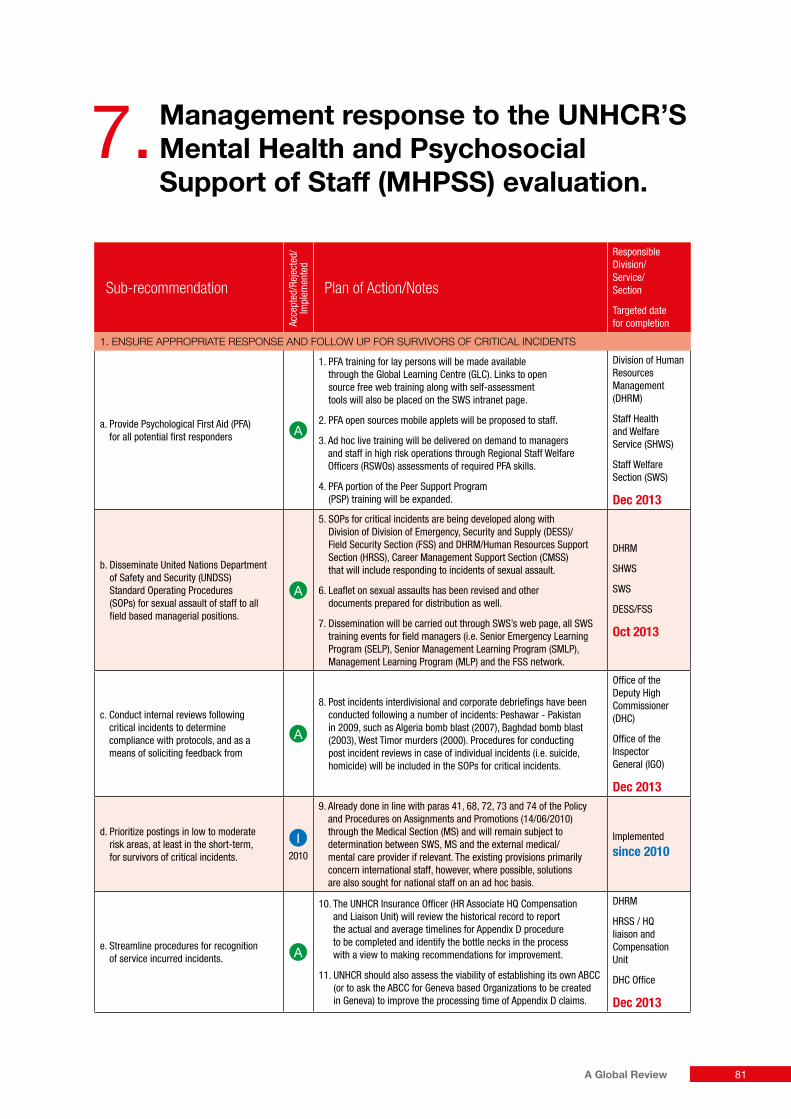
7. Management response to the UNHCR’S Mental Health and Psychosocial Support of Staff (MHPSS) evaluation.
Sub-recommendationAc
cept
ed/R
ejec
ted/
Im
plem
ente
dPlan of Action/Notes
Responsible Division/ Service/ Section
Targeted date for completion
1. ENSURE APPROPRIATE RESPONSE AND FOLLOW UP FOR SURVIVORS OF CRITICAL INCIDENTS
a. Provide Psychological First Aid (PFA) for all potential first responders
1. PFA training for lay persons will be made available through the Global Learning Centre (GLC). Links to open source free web training along with self-assessment tools will also be placed on the SWS intranet page.
2. PFA open sources mobile applets will be proposed to staff.
3. Ad hoc live training will be delivered on demand to managers and staff in high risk operations through Regional Staff Welfare Officers (RSWOs) assessments of required PFA skills.
4. PFA portion of the Peer Support Program (PSP) training will be expanded.
Division of Human Resources Management (DHRM)
Staff Health and Welfare Service (SHWS)
Staff Welfare Section (SWS)
Dec 2013
b. Disseminate United Nations Department of Safety and Security (UNDSS) Standard Operating Procedures (SOPs) for sexual assault of staff to all field based managerial positions.
5. SOPs for critical incidents are being developed along with Division of Division of Emergency, Security and Supply (DESS)/Field Security Section (FSS) and DHRM/Human Resources Support Section (HRSS), Career Management Support Section (CMSS) that will include responding to incidents of sexual assault.
6. Leaflet on sexual assaults has been revised and other documents prepared for distribution as well.
7. Dissemination will be carried out through SWS’s web page, all SWS training events for field managers (i.e. Senior Emergency Learning Program (SELP), Senior Management Learning Program (SMLP), Management Learning Program (MLP) and the FSS network.
DHRM
SHWS
SWS
DESS/FSS
Oct 2013
c. Conduct internal reviews following critical incidents to determine compliance with protocols, and as a means of soliciting feedback from
8. Post incidents interdivisional and corporate debriefings have been conducted following a number of incidents: Peshawar - Pakistan in 2009, such as Algeria bomb blast (2007), Baghdad bomb blast (2003), West Timor murders (2000). Procedures for conducting post incident reviews in case of individual incidents (i.e. suicide, homicide) will be included in the SOPs for critical incidents.
Office of the Deputy High Commissioner (DHC)
Office of the Inspector General (IGO)
Dec 2013
d. Prioritize postings in low to moderate risk areas, at least in the short-term, for survivors of critical incidents.
2010
9. Already done in line with paras 41, 68, 72, 73 and 74 of the Policy and Procedures on Assignments and Promotions (14/06/2010) through the Medical Section (MS) and will remain subject to determination between SWS, MS and the external medical/mental care provider if relevant. The existing provisions primarily concern international staff, however, where possible, solutions are also sought for national staff on an ad hoc basis.
Implemented
since 2010
e. Streamline procedures for recognition of service incurred incidents.
10. The UNHCR Insurance Officer (HR Associate HQ Compensation and Liaison Unit) will review the historical record to report the actual and average timelines for Appendix D procedure to be completed and identify the bottle necks in the process with a view to making recommendations for improvement.
11. UNHCR should also assess the viability of establishing its own ABCC (or to ask the ABCC for Geneva based Organizations to be created in Geneva) to improve the processing time of Appendix D claims.
DHRM
HRSS / HQ liaison and Compensation Unit
DHC Office
Dec 2013
81A Global Review

Sub-recommendation
Acce
pted
/Rej
ecte
d/
Impl
emen
ted
Plan of Action/Notes
Responsible Division/ Service/ Section
Targeted date for completion
2. INCREASE AVAILABILITY AND UTILIZATION OF FORMAL MENTAL HEALTH AND PSYCHOSOCIAL SUPPORT
a. Provide and promote the option for staff to utilize external mental health therapists remotely, e.g., Skype, telephone interviews.
1. Diversification of available treatment options for clients will be promoted through the establishment and regular update of regional directories of external service providers (already decided at the SHWS retreat 2012).
2. Access to the directories will be made available through SHWS and the relevant Service intranet webpages where clarifications on organizational liability and medical Insurance coverage will also be provided.
DHRM/SHWS/SWS
Dec 2013
b. Provide the option for staff to utilize local external mental health therapists and traditional healers or religious figures where these may be preferred options.
3. Refer to Plan of Action 2.a.1 above. This path has already been implemented in various operations for example in Syria, Lebanon, Jordan and Morocco. Referrals to mental health resources outside UNHCR (in or out of the UN) are made regularly.
4. While we can assess the quality of the mental health professional services, this would be difficult with regard to traditional healers. We can however get to know them and understand their importance and role in the society, and include reference to them in our conversations with clients.
DHRM/SHWS/SWS
Dec 2013
c. Disseminate information on what is covered by insurance for outside therapeutic support, and promote a diverse range of staff support options.
5. Refer to Plan of Action 2.a.2
DHRM/SHWS/SWS
Dec 2013
d. Invest in interactive website, including external confidential component, self-assessment tools, and online follow up resources such as Skype consultation with internal or external therapist of choice. Provide links to externally administered self-assessment tools such as: https://ecouch.anu.edu.au/welcome
6. A feasibility study will be undertaken with the Division of Information Systems and Telecommunications (DIST) who are the custodians of IT policy and strategy. Pending the longer-term corporate solution, the choice of existing links to self-assessment tools on the SWS Intranet will be expanded subject to technical feasibility and funding.
7. Establish a dual platform for iSurvived: one internal on the intranet and another external and independent to support their full functioning.
DIST/Intranet Team
DIST/Technical Authority
DHRM/SHWS/SWS
Dec 2013
e. Annually, or at minimum during end of assignment/periods of transition, provide an ‘opt out’ mental health and psychosocial wellness checkup.
8. An opt-out option will be included for the psychological preparation for staff who will be taking up assignments in to D&E duty stations. Participation rate will be monitored. Psychological de-briefing is being designed for the same categories of staff and it will also include an opt out option.
DHRM/SHWS/SWS
Dec 2013
f. Consider a brief mandatory mental health screen in the annual physical for those who “opt-out” of the more comprehensive evaluation. Use the annual physical as an opportunity to provide psycho-education about stress and coping and referral to external resources.
9. In the annual periodical medical examination, mental health assessment is already included by cross-matching staff member declaration, SL data and symptoms at consultation. When data prompt the need for counseling, treatment and/or referral they6 are already provided as a common practice. To increase the sensitivity of this procedure, self-assessment tools will be required to be used by candidates prior to consultation as soon as available on the SWS intranet web-page.
–
g. Put in place explicit means to ensure, and explain limits of, confidentiality, e.g. – written informed consent should be obtained for all staff receiving even brief services (including specifying who can and can’t be informed without additional express written permission from staff); informed consent should include limits of confidentiality such as risk of harm to self or others; staff in positions of authority should sign a confidentiality agreement; reports of critical incidents should at minimum, be de-identified before being distributed. Critical incident reports should have very restricted distribution even when victim’s details have been removed.
10. With the UN confidentiality guidelines for counselors being a guiding document, we will work on the implementation of these guidelines in UNHCR.
DHRM/SHWS/SWS
Sep 2013
82 UNHCR’S MENTAL HEALTH AND PSYCHOSOCIAL SUPPORT FOR STAFF

Sub-recommendation
Acce
pted
/Rej
ecte
d/
Impl
emen
ted
Plan of Action/Notes
Responsible Division/ Service/ Section
Targeted date for completion
3. ENCOURAGE INFORMAL SOCIAL SUPPORT AMONGST STAFF
a. Improve selection, accountability, and utilization of existing peer support personnel in operations deciding to retain this model.
1. UNHCR will keep the Peer Support Program (PSP) as over the years it has proven effective in its sentinel and support functions. The improvement of PSPs’ selection, accountability and utilization will be informed by quality control programs such as client satisfaction surveys (done periodically as a part of the global SWS survey on stress) and ad hoc reviews. Based on consultations with other UN organizations with similar programs in place and with external mental health professionals, we are aware that there is no single method of identifying and selecting potentially good PSPs. We will therefore continue to identify best practices and adjust our approaches to selection of peer support personnel.
DHRM
SHWS
SWS
Operational managers
Jul 2013
b. Channel formal, peer support resources such as training to more broad-based informal peer support groups and team building activities, including country or office-specific well-being initiatives.
2. References to the informal role of the PSP members are already significantly present in the PSP training courses and a number of the PSPs have been critical in the organization of social activities in their offices. Their role in organizing broad-based well-being activities will be more emphasized in revised PSPs Terms of References.
DHRM
SHWS
SWS
Oct 2013
c. Provide corporate support to ad-hoc critical incident survivor peer groups.
3. iSurvived is being launched next month and this has been supported actively by the SWS.
DHRM
SHWS
SWS
Jun 2013
d. Identify senior staff within the organization willing to speak frankly about their struggles with distress and burnout to act as role models.
4. Some Senior Managers have already expressed their willingness to speak in support of iSurvived.
DHRM
SHWS
SWS
Jun 2013
e. Provide mental health first aid training (MHFA) for all managers.
5. Blended training based on a combination of online tools available through the GLC and the SWS Web page and formal training given by the Regional Staff Welfare Officers will be provided to managers who will be identified in cooperation with the regional bureaux.
DHRM
SHWS
SWS
Jan 2014
f. Building on mandatory training on sexual harassment, provide advanced gender sensitivity training for all staff.
6. While recognizing and accepting the general value of this recommendation, the current actions that have been taken in the recent months by the Conflict Management Support Group (CMSG) include: a) update of the UNHCR policy on Discrimination, Harassment, Sexual Harassment and Abuse of Authority; and b) update of separate guidelines for managers and complainants on dealing with discrimination, harassment, sexual harassment and abuse of authorities that include specific tools for prevention or harassment in the workplace. The Ethics Office is a part of the Interagency Standing Committee (IASC) task force working on the Prevention of Sexual Exploitation and Abuse (PSEA). We recognize gender sensitivity as an issue that requires organization-wide action and an on-going engagement rather than a one-time training. We will continue to seek opportunities to enhance staff awareness of gender and harassment themes integrating them in all future training initiatives.
CMSG
Office of the HC
ETHICS
Jan 2014
g. Investigate peer based support models for alcohol and other forms of substance abuse and consider pilot initiatives to examine receptivity of staff.
7. SHWS is currently working on the policy on alcohol case management in the workplace. This document will certainly enable the managers, PSPs and colleagues in general to engage better in the initial alerting and subsequent follow up and monitoring phase.
DHRM
SHWS
SWS
Jan 2014
83A Global Review

Sub-recommendation
Acce
pted
/Rej
ecte
d/
Impl
emen
ted
Plan of Action/Notes
Responsible Division/ Service/ Section
Targeted date for completion
4. ENHANCE ACCOUNTABILITY OF STAFF WELFARE RELATED SERVICES THROUGH REGULAR RIGOROUS EVALUATION, CLEAR STAFF WELFARE POLICIES, AND ROLE DISTINCTION BETWEEN SECTIONS
a. Develop protocols for regular evaluation of staff distress levels and satisfaction with staff support services, e.g., online surveys; pre and post measures for specific programs; anonymous online evaluations for SWS mission visits, using indicators such as – “burnout” surveys, various forms of distress symptoms (note: many of these items can be pulled from the online staff survey Annex II)
1. Bi-annual surveys are being developed this year and as a joint venture with UNICEF to measure exposure to stressors, traumatic stress, burn-out, depression, anxiety, alcohol abuse, utilization of services and level of satisfaction.
2. All training activities, to the extent possible, will be subject to a 3 layer evaluation ( 1) client satisfaction; 2) knowledge retention; 3) behavioral changes) in line with the SHWS newly established criteria for formal evaluation of all SHWS training activities.
DHRM
SHWS
SWS
Dec 2013
b. Evaluate managers on staff welfare indicators such as staff perception of support (through anonymous means)
3. This recommendation has been on the agenda for a while and we will review it again in collaboration with the CMSG and Senior Management Consultative Committee (SMCC). It needs to be implemented in a context that will include conditions for an honest feedback and appropriate consequences (praise for good practices and imperative to change for bad practices. Support and example setting from senior management is required.
DHRMSHWSSWSDHRMGLCDHC Office
2014
c. Roll out UNHCR Staff Care Policy (follow next steps recommendations made by PeopleInAid for Duty of Care Project 2011).
4. While we agree with the spirit of the recommendation, we would prefer to pursue the development of a draft Occupational Health and Safety Policy in line with the JIU recommendation of 2011 and informed by World Health Organization (WHO), International Labour Organization (ILO) and Occupational Health and Safety Standards (OSHAS) 18001 standards. The Policy will encompass the requirements of the 5thprinciple of the UNHCR Code of Conduct and of the Occupational Health and Safety Policy in the UN System established from the High Level Committee on Management of the Chief Executive Board for Coordination (CEB /2010/HLCM/11).
DHRM
SHWS
Dec 2013
d. Clarify the roles of relevant services within DHRM - Staff Welfare Section, Medical, and Career Management Services.
5. Since its inception, SHWS has produced with a participatory method their Mission and Vision Statements. Within this framework the 3 Sections (MS, SWS and Staff Accommodation) will depict their corporate strategies highlighting areas in which synergies make the existence of one only Service more efficient and effective. A staff Welfare Strategy or Corporate Stress Policy to this effect is being drafted as part of the SWS work-plan for this year.
DHRM
SHWS
SWS
Dec 2013
with
rese
rvat
ion
e. Reallocate roles within SWS, with greater emphasis on case management, coordinator and referral to external (country-specific and remote web-based therapeutic) resources, capacity building, including support and replication of innovative country-specific pilot initiatives, and decreased emphasis on direct service provision.
In order to allow a re-allocation of roles within SWS a mapping of the different activities has to be carried out first; all SWS activities will be fully documented and recorded accurately as follows:
6. Direct services provisions will be recorded on MSRP platform with production of verifiable yearly statistics - this will include individual consultations or counseling sessions carried out from the duty station or while on missions –Informed consent to the use of the Section services and the terms of confidentiality applied thereto will be collected and electronically stored
7. Group Sessions and Trainings will be listed in the yearly final report of activities/SWO along with the relevant evaluation-
8. Psychological Preparation to Deployment to D-E DSs participation rate will be monitored every 6 months;
9. Psychological Debriefing on return from deployment to Emergency and/or D and E DSs will be carried out same way as soon as started;
10. Back-to-office mission reports will be reviewed and stored electronically on the Section common database and summarily included in the yearly report of activities;
11. PSPs’ report of activities will also be included along with services of any kind provided to other Agencies or to UN Common System Operations.
The foregoing will allow a better understanding of the actual volume of activities discharged from the SWS which have not been completely reflected in the MHPSS evaluation report (i.e. no mention is made in it of activities 7, 8, 10 and 11) while it has to be recognized that SWS should improve its way to accurately record, report and make visible its activities.
DHRM
SHWS
SWS
Jun 2013
84 UNHCR’S MENTAL HEALTH AND PSYCHOSOCIAL SUPPORT FOR STAFF
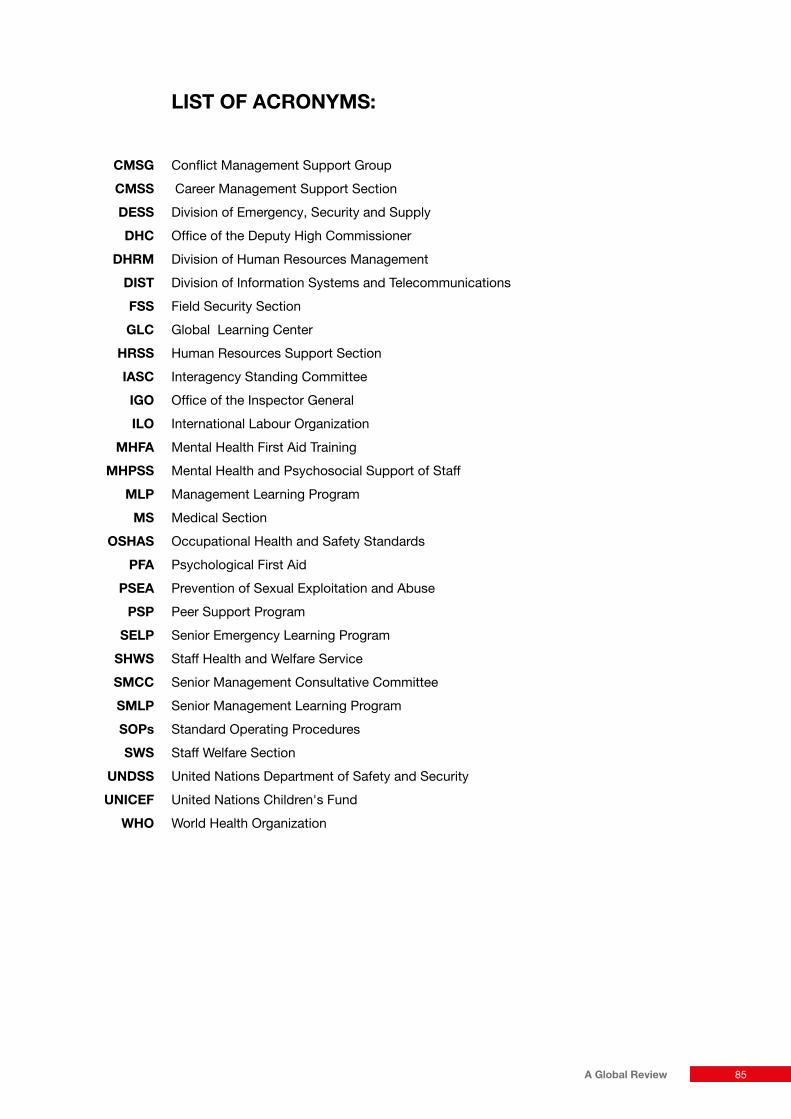
LIST OF ACRONYMS:
CMSG Conflict Management Support Group
CMSS Career Management Support Section
DESS Division of Emergency, Security and Supply
DHC Office of the Deputy High Commissioner
DHRM Division of Human Resources Management
DIST Division of Information Systems and Telecommunications
FSS Field Security Section
GLC Global Learning Center
HRSS Human Resources Support Section
IASC Interagency Standing Committee
IGO Office of the Inspector General
ILO International Labour Organization
MHFA Mental Health First Aid Training
MHPSS Mental Health and Psychosocial Support of Staff
MLP Management Learning Program
MS Medical Section
OSHAS Occupational Health and Safety Standards
PFA Psychological First Aid
PSEA Prevention of Sexual Exploitation and Abuse
PSP Peer Support Program
SELP Senior Emergency Learning Program
SHWS Staff Health and Welfare Service
SMCC Senior Management Consultative Committee
SMLP Senior Management Learning Program
SOPs Standard Operating Procedures
SWS Staff Welfare Section
UNDSS United Nations Department of Safety and Security
UNICEF United Nations Children's Fund
WHO World Health Organization
85A Global Review
8. References and Bibliography
Antares Foundation
Managingstressinhumanitarianworkers.Guidelinesforgoodpractice,Third edition. Netherlands: Antares Foundation, 2012.
Managingstressinhumanitarianworkers[Glossary],2009. From http://goo.gl/SHfuo
Managingstressinhumanitarianworkers.Guidelinesforgoodpractice,2006, Second edition. Netherlands: Antares Foundation.
Managingstressinhumanitarianworkers.Guidelinesforgoodpractice, 2004, First edition. Netherlands: Antares Foundation.
Managingstressinhumanitarianworkers:Asystemsapproachtoriskreduction[booklet], 2008. Netherlands: Antares Foundation.
Managingstressinhumanitarianworkers-GuidelinesforGoodPractice [Brochure]. From http://goo.gl/Or4w5
T. Barrett, J. Fox, J. Shriberg, K. Aden, W. Eich & A. Wolfe
Intervention,92,159-163,2011. The IASC Guidelines and the International Disaster Psychology Program at the University of Denver.
P. Bianchetiere
Resilienceofhumanitarianworkers,2006. From http://goo.gl/nyhgP
L. H. Bikos
First-yearadaptationoffemale,expatriatereligiousandhumanitarianaidworkers:amixedmethodsanalysis.Mental Health, Religion & Culture, 12, 7, 639-661, 2009.
V. Bowie, B. Fisher & C. Cooper
Workplaceviolence:Issues,trendsandstrategies,2005. Uffculme, UK: Willan Publishing.
V. K. Brabant
MainstreamingtheOrganisationalManagementofSafetyandSecurity,2001. A review of aid agency practices and a guide for management HPG Report 9. United Kingdom: HPG
B. E. Bride, M. R. Robinson, B. Yegidis & C. R. Figley
DevelopmentandvalidationoftheSecondaryTraumaticStressScale,2004. Research on Social Work Practice, 14, 27-35.
J. P. Brun n.d
Work-relatedstress:scientificevidence-baseofriskfactors,preventionandcosts[PowerPoint slides]. From http://goo.gl/HsfYJ
C. Campbell, D. Campbell, D. Krier, R. Kuehlthau, T. Hilmes & M. Stromberger
Reductioninburnoutmaybeabenefitforshort-termmedicalmissionvolunteers,2009. Mental Health, Religion, & Culture, 12, 7, 627-637.
B. Cardozo & P. Salama
Mental health of humanitarian aid workers in complex emergencies. In Y. Danieli Ed. Sharingthefrontlineandthebackhills:Peacekeepers,humanitarianaidworkersandthemediainthemidstofcrisis,2002pp.242-255. Amityville, NY: Baywood.
B. Cardozo, G. Crawford, C. Eriksson, J. Zhu, M. Sabi, A. Ager, D. Foy, L. Snider, W. Scholte, R. Kaiser, M. Olff, B. Rijnen & W. Simon2012
Psychologicaldistress,depression,anxiety,andburnoutamonginternationalhumanitarianaidworkers:Alongitudinalstudy.
86 UNHCR’S MENTAL HEALTH AND PSYCHOSOCIAL SUPPORT FOR STAFF

CARE 2009
CriticalIncidentProtocol:YourGuidetoManagingCriticalIncidents.From http://goo.gl/iT8M2
S. C. Carr, M. MacLachlan & A. Furnham
Humanitarianworkpsychology,2012. New York, NY: Palgrave-Macmillan.
Centre for Intercultural Learning Canadian Foreign Service Institute
Staffreintegrationfollowinghigh-riskmissions.Goodpracticesinsupportinginternationaldevelopmentandaidworkers.From http://goo.gl/wGC7u
Centre for Trauma, Resilience and Growth.Nottinghamshire Healthcare NHS Trust
CISMProgrammme2011,December 2012. From http://goo.gl/eqzSC
M. C. Creamer et al.
Guidelinesforpeersupportinhigh-riskorganizations:AninternationalconsensusstudyusingtheDelphimethod.Journal of Traumatic Stress, 25, 134-141, 2012.
P. Curling & K. B. Simmons 2010
JulyStressandstaffsupportstrategiesforinternationalaidworkinIntervention, 8, 2, pp. 93-105.
Danish Red Cross. 2012.
ICRCvolunteeradvocacyfolder,2012. Denmark: IFRC Pyschosocial Reference Centre
R. Deleon, T. Ditzler, P. Hastings 2009
Sustainablecommunitymentalhealth:psychologicalfirstaidinhumanitarianemergencies,2009. Journal of Human Security, 5, 2, 35.
E. Dunlop
Indicationsofprogress?AssessingtheuseofindicatorsinUNHCRoperations.NewIssuesinRefugeeResearch,July 2011.
K. Echavarr
RetentionofFieldStaff[Online Forum Comments], June 7, 2010. Retrieved from website.
H. Elsharkawi, H. Sandbladh, T. Aloudat, A. Girardau, I. Tjoflat & C. Brunnstrom
Preparinghumanitarianworkersfordisasterresponse:ARedCross/RedCrescentfieldtrainingmodel,March 2010. Humanitarian Exchange Magazine, 46. From http://goo.gl/NeA1v
Emergency Response Unit
PsychologicalSupportComponent.DelegateManuel[manual], 2010. Retrieved from website
C. B. Eriksson, J. P. Bjorck, L. C. Larson, S. M. Walling, G. Trice, J. Fawcett, A. D. Abernethy & D. W. Foy 2009
Socialsupport,organisationalsupport,andreligioussupportinrelationtoburnoutinhumanitarianaidworkers, 2009. Mental Health, Religion, and Culture, 12 7, 671-686.
C. B. Eriksson, H. Van de Kemp, R. Gorsuch, S. Hoke & D. Foy 2001
TraumaExposureandPTSDsymptomsininternationalreliefanddevelopmentpersonnel,2001. Journal of Traumatic Stress, 14, 1, 05-212.
C. B. Eriksson
Stressinhumanitarianaidworkers. Paper presented at Managing Stress in Humanitarian Aid Workers conference, September 26 2002, Antares Foundation, Amsterdam.
C. B. Eriksson, J. Bjorck & A. Abernethy 2003
Occupationalstress,traumaandadjustmentinexpatriatehumanitarianaidworkers.In J. Fawcett, 2003. Stress and Trauma Handbook, pp. 68- 100, Monrovia, CA: World Vision International.
87A Global Review

A. Filot & C. Uriarte 2008
ResilienceinMSFanditspersonnel,2008. African Health Sciences, 8, 44-45.
J. Fox, C. Welton-Mitchell & T. Barrett
InternationalDisasterPsychology:ConsiderationsforTraining.Chapter 6,Community Psychology 4 Volume Series, Praeger.
P. V. Gelder & R. V. D. Berkhof 2002
Psychosocialcareforhumanitarianaidworkers:TheMedecinsSansFrontieresHollamnexperience. In Y. Danieli Ed., 2002. The Medecins Sans Frontieres Holland Experience pp. 179-185. Amityville, NY: Baywood.
Global Learning Centre
SeptemberImpactEvaluationofthePSPandRWATrainingProgrammes, 2011.
A. Guterres
ClosingStatementbyMr.AntonioGuterres,UnitedNationsHighCommissionerforRefugees,attheFifty-eighthSessionoftheExecutiveCommitteeoftheHighCommissioner’sProgramme,October 5, 2007. HC Statements.
B. B. D. Haan
Providingsupportforredcrossvolunteersandotherhumanitarianworkersfollowingasecurityincidentoradisaster,30th June, 1997. International Review of the Red Cross, 318, 1-4.
M. B. Hamilton 2003
OnlineSurveyResponseRatesandTimes:BackgroundandGuidanceforIndustry.From: http://goo.gl/khKSp
Headington Institute http://www.headington-institute.org
Minimumoperatingstandardspsychosocialsupportforrelief&DevelopmentPersonnel[manual], 2005. From http://goo.gl/cy2gc
Health: Aiding workers
IRINAfrica,August 19, 2010. From http://goo.gl/X2oYK
A. Hearns & P. Deeny
Thevalueofsupportforaidworkersincomplexemergencies:Aphenomenologicalstudy,2007. Journal of Emergency Nursing Incorporating Disaster Management & Response, 5 2, 29-35.
J. T. Hodgson, J. R. Jones, S. D. Clarke, A. J. Blackburn, S. Webster, C. S. Huxtable & S. Wilkinson 2006
Workplacehealthandsafetysurveyprogramme:2005workerssurveyfirstfindingsreport, 2006. Caerphilly: Health and Safety Executive, HSE Information Services.
Institut Universitaire Kurt Bosch
MeasuringandReducingtheCostofconflictatWorkinUNHCR, March 2009.
Inter-Agency Standing Committee [IASC]
IASCguidelinesonmentalhealthandpsychosocialsupportinemergencysettings, 2007. Geneva: IASC.
InterHealth & People In Aid
ApproachestoStaffCareinInternationalNGOs,September 2009.
Kemp & Merkelback
PolicyPaper:CanYouGetSued? Geneva: Security Management Initiative, 2011.
V. Lionetti 2011
ImpactEvaluationofthePSPandtheRWATrainingPrograms, 2011. Global Learning Centre, UNHCR.
L. Lipsky, C. Burk
TraumaStewardship,AnEverydayGuidetoCaringforSelfWhileCaringforOthers, 2009. San Francisco.
88 UNHCR’S MENTAL HEALTH AND PSYCHOSOCIAL SUPPORT FOR STAFF
D. Loquercio, M. Hammersley & B. Emmens 2006
Understandingandaddressingstaffturnoverinhumanitarianagencies, HPN Report # 55, 2006. London: Humanitarian Practice Network Paper No 55, Humanitarian Practice Network.
S. A. Marotta
Voicesofhope:Acommentaryondislocationandrelation.In P. Dass-Brailsford Ed., 2010. CrisisandDisasterCounseling:LessonslearnedfromHurricaneKatrinaandotherdisasters.Thousand Oaks, CA: Sage Publishing.
C. Maslach & M. P. Leiter
TheTruthAboutBurnout:Howorganizationscausepersonalstressandwhattodoaboutit,1997. San Francisco, CA: Jossey-Bass.
M. McCall & P. Salama 1999
Educationanddebate.Selection,training,andsupportofreliefworkers:anoccupationalhealthissue, 1999. BMJ Group Journal, 318, 113-116.
A. C. McFarlane
Disabilityandaging,2004. In C. Barnes, C. Thomas, S. French & J. Swain Eds., DisablingBarriers,EnablingEnvironement.pp. 189-194. Thousand Oaks: Sage.
A. C. McFarlane & B. A. Van Der Kolk
Traumaanditschallengetosociety, 1996. In. B. A. Van Der Kolk, A. C. McFarlane & L. Weisaeth Eds., Traumaticstress:TheHeadingtonInstituteeffectsofoverwhelmingexperienceonmind,body,andsociety.pp. 24-46. New York, NY: Guilford Press.
L. McKay
Understandingandcopingwithtraumaticstress. Headington Institute. Online training modules. From http://goo.gl/wbWI9
Medecins Sans Frontiere
Psychosocialandmentalhealthinterventionsinareasofmassviolence,MedecinsSansFrontiereReport#2, 2005. From http://goo.gl/9nzT0
Medecins Sans Frontieres & Doctors Without Borders
Yourbenefits[Brochure], 2010.
MondayDevelopments, September 2008. Washington D.C.: InterAction.
S. A. Musa & A. A. R. M. Hamid 2008
PsychologicalproblemsamongaidworkersoperatinginDarfur, 2008. Social Behavior and Personality, 36 3, 407-416.
National Child Traumatic Stress Network
PsychologicalFirstAidFieldOperationsGuide, 2d ed., 2006. From http://goo.gl/Q72Qq
M. Neira n.d.
Healthyworkplaces:Amodelforaction[Powerpoint slides]. From http://goo.gl/fTUi6
S. Nilsson, M. Sjoberg, K. Kallenberg & G. Larsson
Moralstressininternationalhumanitarianaidandrescueoperations:Agroundedtheorystudy, 2011. Ethics & Behavior, 21, 1, 49-68.
Northern Territory Government Work Health Authority
Managingstressintheworkplace.NTWorkSafeapracticalguideformanagers, 2003. From http://goo.gl/FFbsm
K. Nowlan
StaffCare:AGlobalApproach, 2012. PeopleInAid and CiC Supporting Organizations, powerpoint slides.
People In Aid.
Codeofgoodpracticeinthemanagementandsupportofaidpersonnel,2003. London: Regents Wharf.
Promotinggoodpracticeinthemanagementandsupportofaidpersonnel,January 2007. United Kingdom: England and Wales.
Whatiswell-being,January 2007. People In Aid Newsletter, 1-8.
89A Global Review

B. Porter & B. Emmens 2009
ApproachestostaffcareininternationalNGOs, 2009. From http://goo.gl/YTxRQ
Qualtrics Survey Software https://www.qualtrics.com/why-survey-software
S. Rose, J. Bisson, R. Churchill & S. Wessely
Psychologicaldebriefingforpreventingpost-traumaticstressdisorderPTSD, 2009. The Cochrane Library, 1. doi: 10.1002/14651858.CD000560
A. Schafer, L. Snider & M. Van Ommeren 2010
Psychologicalfirstaidpilot:Haitiemergencyresponse,2010. Intervention, 8 3, 245 – 254.
N. K. Semmer
Recognitionandrespectorlackthereofaspredictorsofoccupationalhealthandwell-being[Powerpoint slides], 14 February, 2007. From http://goo.gl/Uw7fq
Shah, Garland & Katz
SecondaryTraumaticStress:PrevalenceinHumanitarianAidWorkersinIndia,2007. Traumatology. Vol. 13, No. 1. doi: 10.1177/1534765607299910
D. M. Smick 2007, January 10
Increasingriskstoaidworkers.Globalist Analysis, #, 1-6, January 10, 2007.
Sphere Project
HumanitarianCharterandMinimumStandardsinDisasterResponse,2011. Switzerland: Author.
Thecodeofconductfortheinternationalredcrossandredcrescentmovementandnon-governmentalorganisationsNGOsindisasterrelief, 2004. In The Sphere Project Ed. Humanitariancharterandminimumstandardsindisasterresponse.pp. 315-322. Switzerland: Author.
Staffreintegrationfollowinghigh-riskmissions:Goodpracticesinsupportinginternationaldevelopmentandaidworkers.n.d.From http://goo.gl/MmHAe
S. Stansfeld & B. Candy
Psychosocialworkenvironmentandmentalhealth-ameta-analyticreview. Scand J Work Environ Health. 2006; 32 6: 443–62.
A. Stoddard, A. Harmer & K. Haver
AidWorkerSecurityReport:Spotlightonsecurityfornationalaidworkers:Issuesandperspective.Humanitarian Outcomes, August 2011.
Supportto,andworkingconditionsfor,volunteers. Information sheet for Red Cross and Red Crescent National societies. n.d. Retrieved from website.
W. Towers
UNHCRGlobalstaffsurvey, PowerPoint presentation, 2011.
D. W. Turner
Qualitativeinterviewdesign:Apracticeguidefornoviceinvestigators2010. The Qualitative Report, 15 3, 754-760. From http://goo.gl/GQmZE
J. A. Uhernik & M. A. Husson
Psychologicalfirstaid:Anevidenceinformedapproachforacutedisaster, 2009.
Behavioralhealthresponse.In G. R. Walz, J. C. Bleuer & R. K. Yep Eds., Compellingcounselinginterventions:VISTAS2009, pp. 271-280. Alexandria, VA: American Counseling Association.
United Nations High Commissioner for Refugees
OfficeofOmbudsmanFinalReport,2010.
StaffStressandSecurity:AManagementChallengeforUNHCR,January 1, 1997.
GlobalReport2000:StaffWelfareUnit.
ManagingtheStressofHumanitarianEmergencies,July 2001.
Stress,Coping,andBurnoutinUNHCRStaff:APilotStudy, 2001.
90 UNHCR’S MENTAL HEALTH AND PSYCHOSOCIAL SUPPORT FOR STAFF

UNHCR’sPolicyonHarassment,SexualHarassment,andAbuseofAuthority, April 2005.
UNHCRStaffHandbook:CopingwithStress,2007 pp. 512-518.
Alcohol:ManageorAbstain, August 2009.
RegionalStaffWelfareOfficerPakistanP3publicad.,2010, September 22.
WorkLifeBalance:UNHCR’spoliciesandpractice,December 2010.
UNHCRWorldwideStats, 2010.
ChiefStaffWelfareSectionP5PublicAd., March 31, 2011.
CombatingRacism,RacialDiscrimination,XenophobiaandRelatedIntolerancethroughaStrategicApproach.Division of International Protection 2009, December.
ExecutiveCommittee,HumanResourcesManagement, 2002, May 30.
GlobalManagementAccountabilityFramework,May 2010, Country ARAs.
GlobalManagementAccountabilityFramework,May 2010, Headquarters ARAs.
GlobalManagementAccountabilityFramework,May 2010, Regional ARAs.
GlobalStaffSurvey2011.
UNHCR - Staff Welfare Section
ProposalsforaStressManagementStrategyatUNHCR, April 19, 1995.
ProposalsforaStressManagementStrategy:ProgressReport, April 1, 1996.
HeadquartersReport1999
JulyBriefingReport,2001.
BasicStressManagementforDifficultAssignments:NotesforStaffAssignedtoEmergencies.ManagingtheStressofHumanitarianEmergencies, 2001.
HQReport2001
BriefingPaper2001
TraumaticStressReactions:AnInformativeandEducativeGuidefortheSurvivorsofTraumaticEvents, 2001.
HQReport2002
AnnualReport2004
AnnualReport2005
HQReport2005
2006HeadquartersReport
2007HeadquartersReport
SupporttoUNHCRstaffaffectedbythesuicidebombattackinAlgierson11December2007, 2008, April 30,
2008HeadquartersReport
NovemberMissionStatement
DecemberReportontheSurveyontheImplementationoftheUNHCRMinimumStandardsonWorkingandLivingConditionsintheField,2009.
2009HeadquartersReport
2009Strategy
Coordinationofthefollow-upsupportforstaffdirectlyimpactedbyseriousviolence.Division of Human Resources Management 2011, February 10.
AugustPsychologicalpreparationforthenewlyrecruitedassignments–apilotproject,2011.
Managingstressinaresettlementoperation, 2011
1StressManagementStrategiesforSeniorLeadersinEmergencyOperations, 2012, January.
2013OperationsPlanNarrative,2012.
Discussionpaper:RotationPolicyandD&Ecapwaivers.
GuidelinesfortheD&Ecapinterview
NeedsAssessmentforUNHCRstaffmembersatHeadquarters
PeerSupportPersonnelProgramme
ProposedoutlinefortheServiceOrientationTrainingforDHRMstaff
Psychologicalpreparationforthenewlyrecruitedstaffforhardshipassignments–apilotproject:Sessionprotocols
PsychologicalpreparationforcolleaguesreassignedtoD&EcategorydutystationsDRAFTforSWteamdiscussion
91A Global Review

Psychosocialsupporttonationalstaffinhardshiplocations
RelaxationTechniquesforStressRelief
SWSSubmissionNarrative2012-13
SWSHQReport2008,pg. 2.
SWSHQReport,2006.
TakingCareofYourself:ABriefguideforUNHCRFieldworkers
UNHCRStaffWelfareSectionMonthlyIndicators
AReviewofUNHCR’sSecurityPolicyandPolicyImplementation.Steering Committee on Security Policy and Policy Implementation 2004, October.
SickLeavePolicy2012
United Nations World Food Programme WFP
ReportoftheJointInspectionUnitRelevanttotheWorkofWFP,ExecutiveBoarddocument061674, 2012. UNWFP.
J. A. Vergara & D. Gardner 2011
Stressorsandpsychologicalwell-beinginlocalhumanitarianworkersinColombia,2011. Journal of Managerial Psychology, 26, 6, 500-507.
G. Vogel, J. Stiebel & R. Vogel 2011
Psychologyinaction:Reentrytrauma:Theshockofreturninghome, 2011. Psychology International, 1, 1-6
N. Wiedemann & L. Norgaard 2012
Focus:Volunteersinemergencies, 2012. Coping with crisis, 1, 1-24.
B. Wigley
The state of UNHCR’s organizational culture, May 8, 2005. PDES, UNHCR.
Workinfo
Healthywork:Managingstressintheworkplace, 2003. Health and safety is good business. From http://goo.gl/fl88G
Additional relevant websites Antares Foundation http://antaresfoundation.org
Headington Institute http://www.headington-institute.org
Konterra Group http://www.konterragroup.net/client/ united-states-agency-for-international-development-usaid
PeopleInAid http: //www.peopleinaid.org/resources/casestudies.aspx
National Child Traumatic Stress Network http: //learn.nctsn.org/course/category.php?id=11
SalusWorld http: //salusworld.org/services/staff-welfare.php
USAID Staff Care http: //staffcare.usaid.gov
92 UNHCR’S MENTAL HEALTH AND PSYCHOSOCIAL SUPPORT FOR STAFF

Annex I.Antares Framework: UNHCR’s Indicator Level Scores
Principle Indicators (brief description) and UNHCR score
� Agency has a written and active policy to prevent or mitigate the effects of stress. (4/8)
� Written policy covers expected and unexpected circumstances. (0)
� Agency warns about the risks of humanitarian work. (1)
� Agency has a specific strategy for reducing risks for each individual project. (1)
� Agency routinely reviews policies and protocols. (0)
� Agency devises policies and practices that match needs of staff. (0)
� Agency regularly evaluates policies and practices. (0)
� Agency asks staff to comply with policy. (1)
� Agency encourages staff to hold agency to its commitment. (1)
� Agency systematically screens and /or assesses the current capacity of staff members to respond to and cope with the anticipated stressors of an assignment. (1/5)
� Agency has understanding of requirements for high risk assignments. (0)
� Prospective staff and staff seeking new assignments are screened as to the likelihood of adverse responses. (0)
� The results of such screenings are used to match staff to assignments. (0)
� Appropriately trained interviewers are used for screening and assessing. (1)
� The individual seeking assignment is held responsible for disclosing information that may be relevant to assessing risks. (0)
� Agency ensures that all employees have appropriate pre-assignment preparation and training in managing stress. (1/3)
� All staff has received information about recognizing and managing stressors of humanitarian work. (1)
� All staff have received updated briefing and training before a new assignment and when an assignment changes. (0)
� Supervisors and field managers are adequately trained and evaluated in stress management skills and capacities. (0)
� Agency ensures the monitoring of the response to stress of its staff on an ongoing basis. (1/4)
� Managers are appraising staff for signs of stress regularly. (0)
� Managers are monitoring staff for signs of stress after a critical incident. (0)
� Individual staff are monitoring and reporting signs of stress in themselves. (1)
� Agency has an explicit written policy that it will respond constructively (not punitively) to any revelations of stress. (0)
� Agency is providing training and support, on an ongoing basis, to help its staff deal with the daily stresses of humanitarian aid work. (1/3)
� Agency provides ongoing training and support for staff. (1)
� Organizational and management practices are reviewed with respect to their impact on staff stress, possibilities to mitigate stress and strengthening team cohesion. (0)
� Staff are encouraged to engage in good practices of selfcare and collegial support. (0)
� Agency provides staff with specific and culturally appropriate support in the wake of critical or traumatic incidents and other unusual and unexpected sources of severe stress. (2/4)
� All staff are provided with explicit guidelines as to the kinds of critical or potentially stressful incidents that must be reported to higher management. (1)
� All managers/ supervisors are trained in responses to traumatic incidents. (0)
� The agency has arranged for staff with specific training in psychological first aid to be available to consult with staff members after traumatic incidents. (.5)
� The agency has standing arrangements with local, regional or international specialists during a crisis period to provide culturally relevant trauma assistance. (.5)
� Agency provides practical, emotional and culturally appropriate support for staff at the end of an assignment or contract. This includes a personal stress review and an operational debriefing. (2/5)
� Agency has a program for assisting staff to prepare for the stresses involved in leaving a project and returning home (or taking on another assignment). (0)
� All staff members are offered an exit operational debriefing at the end of their assignment or contract. (0)
� All staff members have access to a personal stress assessment and review at the end of their assignment or on an annual basis. The assessment is conducted by someone who is not associated with human resources management within the agency. (0)
� Agency has arrangements to make psycho social services available for staff members in the wake of an evacuation or unexpected termination of a project or contract. (1)
� Agency has an explicit commitment to provide support to help employees make arrangements associated with relocation or unexpected termination. (1)
� The agency has clear written policies with respect to the ongoing support they will provide to staff members who have been adversely impacted by exposure to stress and trauma during their assignment. (0/2)
� Agency has a clear policy aimed at monitoring and supporting employees who have job stress related disabilities such as ‘burnout,’ depression, or PTSD. (0)
� Agency has developed policies for employees who are unable to continue working for the agency due to job-related stress or injury. This addresses issues such as salary and benefits and provision (or financing) of psychosocial support services. (0)
2 out of 8 principles 12 out of 34 = 35%
93A Global Review
Annex II.
UNHCR STAFF WELL-BEING SURVEYThis survey will be used to assist UNHCR in better understanding staff well-being. Staff working in humanitarian organizations often experience stressful situations. If not given adequate resources to manage stress, productivity can suffer. Feeling “burnt out” (exhausted as a result of longtime stress), some people choose to leave the organization. In the interest of retaining qualified staff and maintaining the integrity of UNHCR’s services, we would like to better understand how best to meet the mental health and psychosocial needs of UNHCR staff. Please take a moment to complete this important anonymous survey.
What is STAFF WELL-BEING?Staff well-being can be defined as the overall quality of experience and functioning at work - psychological, physical, and social.
Promoting staff well-being includes self-care and institutional responses to stress, tailored for humanitarian workers in particularly difficult and stressful environments.
The purpose of promoting staff well-being is to create a healthy and productive workforce (InterAction, 2008; InterHealth & PeopleInAid, 2009; Grant et al., 2007).
For more information on the purpose of this survey and a description of how your identity is protected please click here.
Section I: Satisfaction
1. Overall, how would you rate UNHCR’s efforts to promote staff well-being (to support staff and promote psychosocial and mental health)?
¨ Extremely satisfied
¨ Somewhat satisfied
¨ Slightly satisfied
¨ Neutral
¨ Slightly dissatisfied
¨ Somewhat dissatisfied
¨ Extremely dissatisfied
Section II: Existing Policies
2. Are you familiar with any UNHCR policies related to staff well-being that help staff or managers cope with stress?
¨ Very familiar
¨ Somewhat familiar
¨ Not familiar
94 UNHCR’S MENTAL HEALTH AND PSYCHOSOCIAL SUPPORT FOR STAFF

Section III: Stress and Coping
3. In the past few years what do you think is the greatest source of staff stress in UNHCR?
......................................................................................................................................................
......................................................................................................................................................
......................................................................................................................................................
4. Are any of the areas below a significant cause of stress for you currently? (select all that apply)
¨ Status of employment contract
¨ Feeling undervalued
¨ Feeling unable to contribute to decision making
¨ Workload
¨ Ability to achieve work goals and objectives
¨ Working hours
¨ Relationship with supervisor(s)
¨ Relationship with work colleagues
¨ Family concerns
¨ Financial concerns
¨ Health concerns
¨ Safety concerns
¨ Exposure to suffering of persons of concern
¨ Exposure to incidents when you were seriously injured or your life was threatened
¨ The political situation in the county where you are presently working
¨ Other (please specify)
......................................................................
5. What helps you most in keeping stress on a manageable level?
......................................................................................................................................................
......................................................................................................................................................
......................................................................................................................................................
6. Do you do any of the following to cope with stress? (select all that apply)
¨ I've been working more to try to take my mind off things.
¨ I've been using alcohol or other drugs to make myself feel better.
¨ I've been getting emotional support from others.
¨ I've given up on trying to deal with it.
¨ I've been taking action to try to make the situation better.
¨ I've been trying to see it in a different light, to make it seem more positive.
¨ I’ve been criticizing or blaming myself.
95A Global Review

¨ I've been making jokes about the situation, using humor.
¨ I've been doing something to think about it less, such as watching TV, reading, daydreaming, or sleeping.
¨ I've been trying to learn to live with it.
¨ I've been expressing my negative feelings, complaining, venting to get the frustration out.
¨ I've been trying to find comfort in my religion or spiritual beliefs (e.g. praying, meditating).
¨ I’ve been trying to get advice or help from other people about what to do.
¨ Other, please describe ..............................................................................................................
Section IV: Healthy Work Environments
7. Do you have an updated job description?
¨ Yes ¨ No
(7.a.) How accurately does it reflect your actual work? (question only shown if yes to above is checked)
¨ Very much
¨ Somewhat
¨ Not at all
8. Do you think the activities and objectives in your operation or work unit are well-defined?
¨ Yes ¨ No
9. Is the leadership structure in your operation or work unit clear?
¨ Yes ¨ No
10. Do you think the workload is divided equally among staff based on their jobs?
¨ Yes ¨ No
11. Do you frequently work overtime?
¨ Yes ¨ No
(11.a.) Are you compensated in some way (e.g. compensatory time off)? question only shown if yes checked for the above)
¨ Yes ¨ No
96 UNHCR’S MENTAL HEALTH AND PSYCHOSOCIAL SUPPORT FOR STAFF
12. Do you have regular staff/team meetings and briefings?
¨ Yes ¨ No
13. Do you feel included and informed in staff/team meetings and briefings?
¨ Yes ¨ No
14. Do international and national staff have a good working relationship?
¨ Yes ¨ No
15. What type of conflict is common in your operation or work unit?
......................................................................................................................................................
16. Have you participated in any teambuilding exercises (e.g. retreats, social activities, trust-building
or communication games) with other UNHCR staff in the past two years?
¨ Yes ¨ No
17. How might UNHCR promote team building and mutual respect amongst colleagues?
......................................................................................................................................................
18. Do members of senior management regularly visit country, S/FO operations,
or keep in touch in other ways?
¨ Yes ¨ No
Section V: Preparation and Ongoing Support
19. When you joined UNHCR did you receive a psychological screening (asking several questions
about your previous and current state of mental health)?
¨ Yes ¨ No ¨ I don’t recall
20. Have you ever received information about common stressors of humanitarian work, how to
recognize stress reactions, and/or how to cope with stress? (check all that apply)
¨ Yes, before my first assignment with UNHCR
¨ Yes, before I was posted to a C, D, or E duty station
¨ Yes, at some other time since joining UNHCR
¨ No, I have never received this type of information from UNHCR
97A Global Review

21. Do managers in your current location emphasize the importance of staff well-being?
¨ Yes, most emphasize staff well-being
¨ Yes, some emphasize staff well-being
¨ No, none emphasize staff well-being
22. If you are a manager what do you do to emphasize staff well-being? (skip if not applicable)
......................................................................................................................................................
......................................................................................................................................................
23. Have you ever looked at any of the well-being or stress management resources
on the UNHCR intranet?
¨ Yes ¨ No
(23.a.) Why not? (question only shown if no checked for above)
¨ I didn’t know about the materials
¨ I didn’t need the materials
¨ I didn’t think the materials would be useful
¨ Other ................................................................
(23.b.) Did you find the materials useful? (question only shown if yes checked for the above)
¨ Yes ¨ No
Section VI: Critical Incidents
24. Have you experienced an incident when you believed your life was in danger or you thought you
would be seriously injured?
¨ Yes ¨ No
25. Have you experienced an incident when you witnessed someone else being seriously injured,
killed, or threatened in a manner that led you to believe their life was in danger?
¨ Yes ¨ No
(25.a.) Did you receive any type of support immediately after the incident (within 24 hours)? (question only shown if yes to 24 or 25)
¨ Yes ¨ No
98 UNHCR’S MENTAL HEALTH AND PSYCHOSOCIAL SUPPORT FOR STAFF

(25. b.) From whom did you receive support? (check all that apply) (question only shown if yes to 24 or 25 )
¨ UNHCR peer support member
¨ UNHCR Staff Welfare Officer
¨ UNHCR Medical Officer
¨ UNHCR Administrator
¨ UNHCR manager
¨ Other UN staff, please specify (by position, not name)
¨ Staff from other (non-UN) agencies, please specify (by position, not name)
¨ Friends
¨ Family
¨ Others, please specify
......................................................................
(25.c.) What type of support did person(s) provide? (check all that apply) (question only shown if yes to 24 or 25)
¨ Spent time with you.
¨ Asked about your needs.
¨ Helped you to feel safe.
¨ Assisted you in calming down, and/or getting through feeling disoriented or overwhelmed.
¨ Assisted you with information, either giving you up to date information, or helping you to share information with others.
¨ Helped you to make practical arrangements as needed.
¨ Helped to connect you with social supports (friends, family, others).
¨ Provided information on normal psychological reactions you might experience.
¨ Provided examples of coping strategies.
¨ Linked you with support services for additional follow up (e.g. counseling).
¨ Encouraged you to describe in detail what happened (in individual or group setting).
¨ Other, please describe .........................................................
26. Were you treated differently after the incident by other UNHCR staff in some way that made you
uncomfortable? (question only shown if yes to 24 or 25)
¨ Yes ¨ No
27. Did a UNHCR Staff Welfare Officer follow up with you 1-3 months after the incident? (question only shown if yes to 24 or 25)
¨ Yes ¨ No
99A Global Review

28. When transitioning to a new job assignment and/or location has any UNHCR staff member (e.g. manager, Staff Welfare Officer, peer support member, Medical Officer) ever talked with you about your stress level and use of coping techniques? (question only shown if yes to 24 or 25)
¨ Yes ¨ No
¨ Not applicable, I have never changed job assignments or location
Section VII: Peer Support Members and Staff Welfare Officers
29. Have you ever approached a member of the peer support network for assistance?
¨ Yes ¨ No
(29.a.) Why not? (question only shown if yes to 29)
......................................................................................................................................................
(29.b.) Would you recommend other UNHCR staff contact a peer support network member to
assist in managing stress?
¨ Yes ¨ No
30. Have you ever contacted a Staff Welfare Officer in UNHCR?
¨ Yes ¨ No
(30.a.) Why not? (question only shown if no to 30)
......................................................................................................................................................
(30.b.) Would you recommend other UNHCR staff contact Staff Welfare Officer to assist in managing stress?
¨ Yes ¨ No
31. Would you prefer to have contact with someone who is not affiliated with UNHCR (e.g. private
counselor, someone from another agency)?
¨ Yes ¨ No
32. Comparing informal support (friends, colleagues) and UNHCR's institutional responses (Staff
Welfare Officers, peer support network members), how would you rate the effectiveness of each of the two support mechanisms?
¨ I find informal support (friends, colleagues) more useful than UNHCR’s responses.
¨ I find informal support (friends, colleagues) and UNHCR’s responses equally useful.
¨ I find UNHCR’s responses more useful than informal support (friends, colleagues).
¨ I find neither particularly useful.
100 UNHCR’S MENTAL HEALTH AND PSYCHOSOCIAL SUPPORT FOR STAFF

Section VIII: Hardship/ Insecure Settings
33. If you have ever worked in a C, D, or E duty station - does UNHCR make an effort to manage the
security risks facing international and national staff equally?
¨ Yes ¨ No
¨ Not applicable, I’ve never worked in a C, D, or E duty station
34. If you have ever worked in a C, D, or E duty station - are “entitlements” (e.g. R&R/ STO, annual
leave, hardship allowance/danger pay) being implemented?
¨ Yes ¨ No
¨ Not applicable, I’ve never worked in a C, D, or E duty station
The following questions should be answered by all respondents, regardless of the category of your duty station.
35. Are there opportunities for non-work related/leisure activities at your location?
¨ Yes ¨ No
36. Are you able to obtain adequate food and water (not only for drinking but also to engage in
washing in a manner consistent with your religion and culture)?
¨ Yes ¨ No
37. Do you have a minimally comfortable and safe place to live?
¨ Yes ¨ No
38. Do you think you have adequate training and equipment to deal with potential security
concerns?
¨ Yes ¨ No
Section IX: Substance Abuse
39. What percentage of UNHCR staff that you have worked with do you think drink alcohol to
excess or use substances to excess, in a manner that interferes with their work performance?
¨ 0% ¨ 10% ¨ 20% ¨ 30% ¨ 40% ¨ 50% ¨ 60% ¨ 70% ¨ 80% ¨ 90% ¨ 100%
40. Are you satisfied with the way UNHCR addresses substance abuse?
¨ Yes ¨ No
101A Global Review
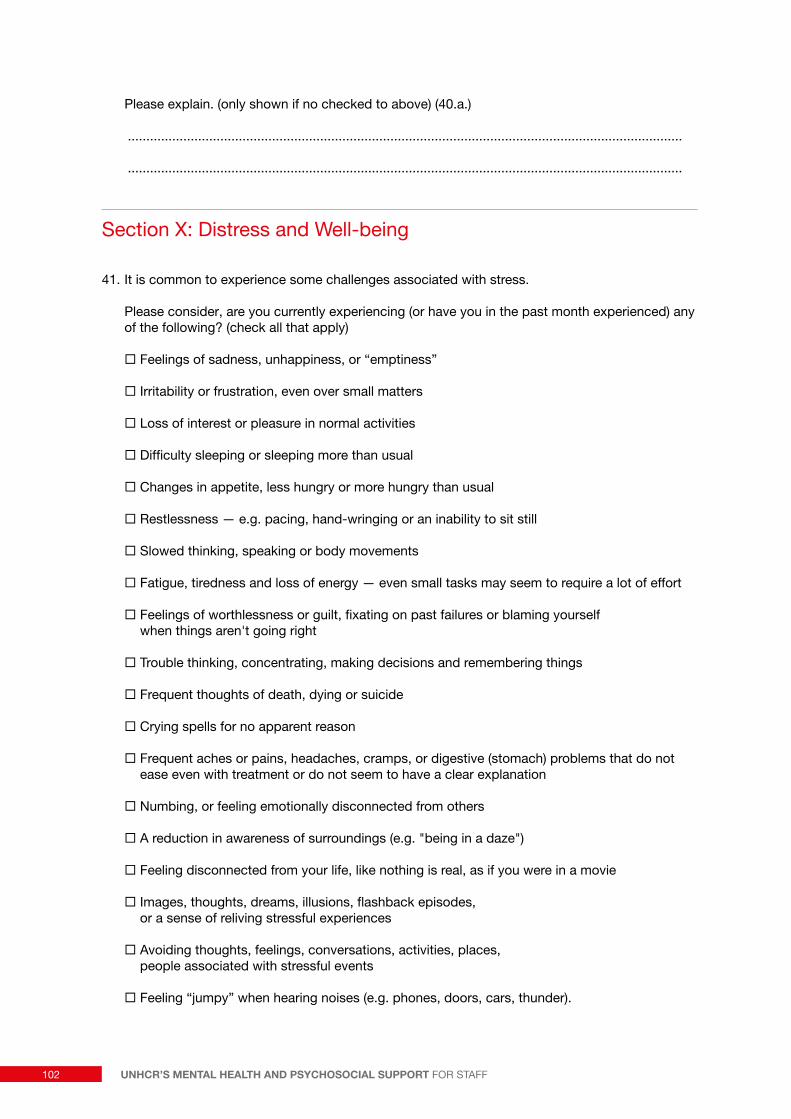
Please explain. (only shown if no checked to above) (40.a.)
......................................................................................................................................................
......................................................................................................................................................
Section X: Distress and Well-being
41. It is common to experience some challenges associated with stress.
Please consider, are you currently experiencing (or have you in the past month experienced) any of the following? (check all that apply)
¨ Feelings of sadness, unhappiness, or “emptiness”
¨ Irritability or frustration, even over small matters
¨ Loss of interest or pleasure in normal activities
¨ Difficulty sleeping or sleeping more than usual
¨ Changes in appetite, less hungry or more hungry than usual
¨ Restlessness — e.g. pacing, hand-wringing or an inability to sit still
¨ Slowed thinking, speaking or body movements
¨ Fatigue, tiredness and loss of energy — even small tasks may seem to require a lot of effort
¨ Feelings of worthlessness or guilt, fixating on past failures or blaming yourself when things aren't going right
¨ Trouble thinking, concentrating, making decisions and remembering things
¨ Frequent thoughts of death, dying or suicide
¨ Crying spells for no apparent reason
¨ Frequent aches or pains, headaches, cramps, or digestive (stomach) problems that do not ease even with treatment or do not seem to have a clear explanation
¨ Numbing, or feeling emotionally disconnected from others
¨ A reduction in awareness of surroundings (e.g. "being in a daze")
¨ Feeling disconnected from your life, like nothing is real, as if you were in a movie
¨ Images, thoughts, dreams, illusions, flashback episodes, or a sense of reliving stressful experiences
¨ Avoiding thoughts, feelings, conversations, activities, places, people associated with stressful events
¨ Feeling “jumpy” when hearing noises (e.g. phones, doors, cars, thunder).
102 UNHCR’S MENTAL HEALTH AND PSYCHOSOCIAL SUPPORT FOR STAFF

42. Are any of the items checked interfering with your ability to:
(42.a.) Do your job?
¨ Yes ¨ No ¨ not applicable, I did not check any items
(42.b.) Maintain relationships with your family, friends, or colleagues?
¨ Yes ¨ No ¨ not applicable, I did not check any items
43. Sometimes people report unexpected or surprising benefits associated with stress exposure.
In your case, have stressful experiences with UNHCR resulted in any of the following? (check all that apply)
¨ I changed my priorities about what is important in life.
¨ I have a greater appreciation for the value of my own life.
¨ I have a greater sense of closeness with others.
¨ I established a new path for my life.
¨ I know better that I can handle difficulties; I’m stronger than I thought I was.
¨ I have a stronger religious faith.
¨ I learned a how wonderful people are.
¨ I enjoy my work more and am performing better.
¨ Other ........................................................................
¨ Not applicable - I have not experienced any benefits associated with stress exposure.
44. Please respond to the following statement:
I can find something positive in even the most difficult situation.
¨ Never true
¨ Rarely true
¨ True about half the time
¨ Usually true
¨ Always true
45. Is there anything else about stress and well-being you think would be important for us to know?
......................................................................................................................................................
......................................................................................................................................................
......................................................................................................................................................
103A Global Review

Section XI: Demographic Information
We are asking for demographic information to better understand the needs of different groups (e.g. women compared to men). This information will not be associated directly with your responses to the previous survey questions. Your identity is protected, this questionnaire is anonymous.
A. Gender
¨ Female
¨ Male
¨ other
¨ prefer not to answer
B. Job Location
¨ HQ
¨ Africa
¨ Americas
¨ Asia
¨ Europe
¨ MENA
¨ SIBA (at home not working currently)
¨ Other .................................................
¨ prefer not to answer
C. Office Configuration
¨ HQ
¨ Regional Office
¨ Hub
¨ Country Office
¨ Sub-Office
¨ Field Office/Unit
¨ Liaison Office
¨ Other .................................................
¨ prefer not to answer
D. Job Category
¨ International Professional
¨ National Professional
¨ Field Service
¨ General Service
¨ UNV
¨ Consultant
¨ Contractors (UNOPS)
¨ Other .................................................
¨ prefer not to answer
104 UNHCR’S MENTAL HEALTH AND PSYCHOSOCIAL SUPPORT FOR STAFF

E. Job Sector
¨ Protection (includes Education, Field, Community Services)
¨ Programme (includes Livelihoods, Health, Shelter, Camp Management, Data Management)
¨ Admin (includes Finance, Budget, Project Control, Admin/Program, Office Support, Drivers)
¨ External Relations (includes Public Information, Resource Mobilization)
¨ Supply Chain (includes Procurement, Logistics, Contract s and Asset Management)
¨ Emergency Support (on temporary emergency support missions)
¨ Information Technology
¨ Representation and Executive Office
¨ Human resources (includes Personnel Administration, Learning, Performance and Career Management)
¨ Other ...........................................................................................................................................
¨ prefer not to answer
F. How many years have you worked for UNHCR?
¨ less than one year
¨ 1-5 years
¨ 6-10 years
¨ 11-15 years
¨ 16- 20 years
¨ more than 20 years
¨ prefer not to answer
G. How old are you?
¨ 20-30 years old
¨ 31-40 years old
¨ 41-50 years old
¨ 51-60 years old
¨ Over 60 years of age
¨ prefer not to answer
105A Global Review

Annex III.
DEMOGRAPHICS: Survey Respondents compared to UNHCR all staff
Variable Survey Respondents
All UNHCR staff
GENDER
Women 53% 37%
Men 47% 63%
JOB LOCATION
Africa 28% 45%
Asia 22% 18%
HQ 17% 12%
Europe 13% 8%
MENA 11% 13%
Americas 6% 4%
Other 1% -
SIBA (without current post) 1% -
OFFICE CONFIGURATION
Country Office 33% -
Headquarters* 19% 17%
Sub-office 18% -
Field Office/Unit 17% -
Regional Office 9% -
Other 2% -
Hub 1% -
Liaison Office 1% -
NA (Headquarters)
JOB CATEGORY
International Professional 42% 25%
General Service 34% 68%
National Professional 11% 7%
UNV 5% -
Field Service 3% 1%
Contractors (UNOPS) 3% -
Other 1% -
Consultant 1% -
Variable Survey Respondents
All UNHCR staff
JOB SECTOR
Protection 37% 25%
Admin 16% 42%
Programme 12% 21%
Other 8% -
Representation and Executive Office
8% 8%
Human Resources 6% -
Information Technology 6% -
External Relations 4% 4%
Supply Chain 3% -
Emergency Support 1% -
YEARS WORKING FOR UNHCR
Less than 1 year 7% -
1-5 years 29% -
6-10 years 22% -
11-15 years 15% -
16-20 years 15% -
More than 20 years 12% -
AGE
20-30 13% -
31-40 36% -
41-50 31% -
51-60 19% -
Over 60 years of age 1% -
MENA = Middle East North Africa;
SIBA = represents those on payroll without current assignment. Depending on the demographic question, between 3-12% of respondents chose not to answer the question; the totals above do not reflect this missing data.
*The job location and office configuration questions are slightly different (e.g. HQ extension office - Global Learning Center in Budapest).
106 UNHCR’S MENTAL HEALTH AND PSYCHOSOCIAL SUPPORT FOR STAFF

Annex IV.
Staff Welfare-related Website Examples
http://staffcare.usaid.gov
http://www.globalwellnesscenter.net
http://www.theresilientmind.org
http://aidsource.ning.com
Interactive websites: utilizing video links, humanitarian testimonials, blog posts, chat rooms, discussion forums, skype consultation, live trainings (pod casts), self-assessment tools, links to anonymous surveys.
http://www.humanitarian-psy.org
http://www.endrape.msu.edu
http://www.realwarriors.net
107A Global Review
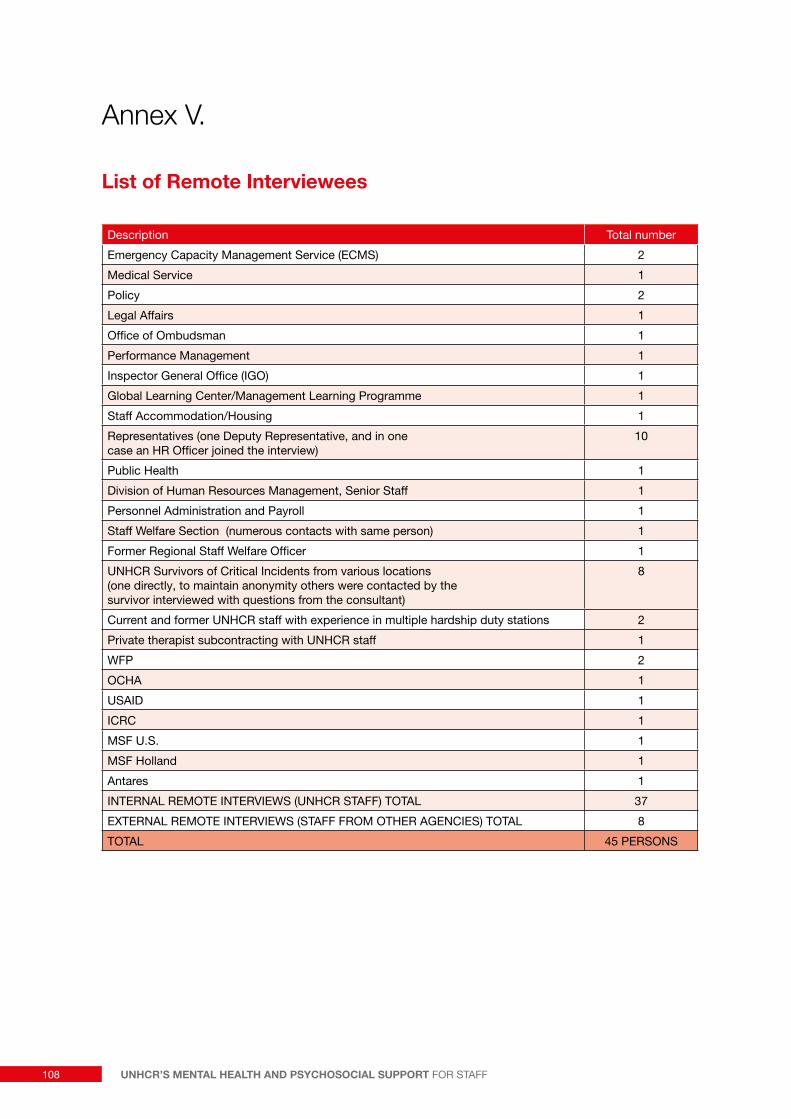
Annex V.
List of Remote Interviewees
Description Total number
Emergency Capacity Management Service (ECMS) 2
Medical Service 1
Policy 2
Legal Affairs 1
Office of Ombudsman 1
Performance Management 1
Inspector General Office (IGO) 1
Global Learning Center/Management Learning Programme 1
Staff Accommodation/Housing 1
Representatives (one Deputy Representative, and in one case an HR Officer joined the interview)
10
Public Health 1
Division of Human Resources Management, Senior Staff 1
Personnel Administration and Payroll 1
Staff Welfare Section (numerous contacts with same person) 1
Former Regional Staff Welfare Officer 1
UNHCR Survivors of Critical Incidents from various locations (one directly, to maintain anonymity others were contacted by the survivor interviewed with questions from the consultant)
8
Current and former UNHCR staff with experience in multiple hardship duty stations 2
Private therapist subcontracting with UNHCR staff 1
WFP 2
OCHA 1
USAID 1
ICRC 1
MSF U.S. 1
MSF Holland 1
Antares 1
INTERNAL REMOTE INTERVIEWS (UNHCR STAFF) TOTAL 37
EXTERNAL REMOTE INTERVIEWS (STAFF FROM OTHER AGENCIES) TOTAL 8
TOTAL 45 PERSONS
108 UNHCR’S MENTAL HEALTH AND PSYCHOSOCIAL SUPPORT FOR STAFF

Annex VI.
Chain of Evidence Supporting Recommendations
Conclusion: Response to critical incidents is inadequate, this appears to be particularly true to survivors of sexual assault. Critical incident survivors don’t consistently receive appropriate psychological care.
Examples of Data Source/ Supporting Evidence
è Online survey responses indicate high numbers of UNHCR staff are exposed to critical incidents.
è PFA is the recommended intervention for critical incidents. Stakeholder interviews and online responses indicate comprehensive PFA is not provided.
è Feedback from at least a few critical incident survivors indicates sexual assault SOPs are not being followed at the office-level.
è Feedback from critical incident survivors indicates there is no formal mechanism for feedback about adequacy of agency response in a given critical incident.
è Critical incident survivors indicate concerns about being able to work in high risk settings during a recovery period.
Recommendations 1: Ensure Appropriate Response and Follow up for Survivors of Critical Incidents
a. Provide Psychological First Aid (PFA) for first all potential first responders.
b. Disseminate UNDSS SOPs for sexual assault of staff.
c. Conduct internal reviews following critical incidents to determine compliance with protocols, and as a means of soliciting feedback from survivors.
d. Prioritize jobs in low to moderate risk areas. at least in the short-term, for survivors of critical incidents.
e. Streamline procedures for recognition of service incurred incidents.
109A Global Review
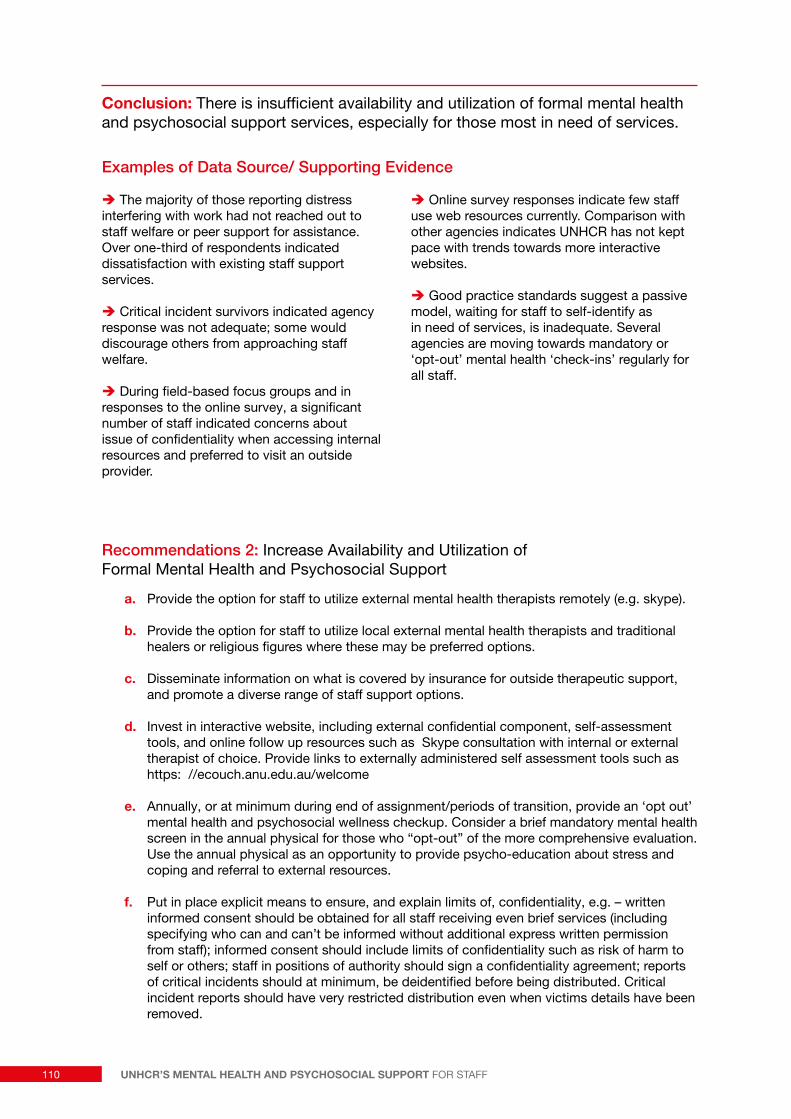
Conclusion: There is insufficient availability and utilization of formal mental health and psychosocial support services, especially for those most in need of services.
Examples of Data Source/ Supporting Evidence
è The majority of those reporting distress interfering with work had not reached out to staff welfare or peer support for assistance. Over one-third of respondents indicated dissatisfaction with existing staff support services.
è Critical incident survivors indicated agency response was not adequate; some would discourage others from approaching staff welfare.
è During field-based focus groups and in responses to the online survey, a significant number of staff indicated concerns about issue of confidentiality when accessing internal resources and preferred to visit an outside provider.
è Online survey responses indicate few staff use web resources currently. Comparison with other agencies indicates UNHCR has not kept pace with trends towards more interactive websites.
è Good practice standards suggest a passive model, waiting for staff to self-identify as in need of services, is inadequate. Several agencies are moving towards mandatory or ‘opt-out’ mental health ‘check-ins’ regularly for all staff.
Recommendations 2: Increase Availability and Utilization of Formal Mental Health and Psychosocial Support
a. Provide the option for staff to utilize external mental health therapists remotely (e.g. skype).
b. Provide the option for staff to utilize local external mental health therapists and traditional healers or religious figures where these may be preferred options.
c. Disseminate information on what is covered by insurance for outside therapeutic support, and promote a diverse range of staff support options.
d. Invest in interactive website, including external confidential component, self-assessment tools, and online follow up resources such as Skype consultation with internal or external therapist of choice. Provide links to externally administered self assessment tools such as https: //ecouch.anu.edu.au/welcome
e. Annually, or at minimum during end of assignment/periods of transition, provide an ‘opt out’ mental health and psychosocial wellness checkup. Consider a brief mandatory mental health screen in the annual physical for those who “opt-out” of the more comprehensive evaluation. Use the annual physical as an opportunity to provide psycho-education about stress and coping and referral to external resources.
f. Put in place explicit means to ensure, and explain limits of, confidentiality, e.g. – written informed consent should be obtained for all staff receiving even brief services (including specifying who can and can’t be informed without additional express written permission from staff); informed consent should include limits of confidentiality such as risk of harm to self or others; staff in positions of authority should sign a confidentiality agreement; reports of critical incidents should at minimum, be deidentified before being distributed. Critical incident reports should have very restricted distribution even when victims details have been removed.
110 UNHCR’S MENTAL HEALTH AND PSYCHOSOCIAL SUPPORT FOR STAFF
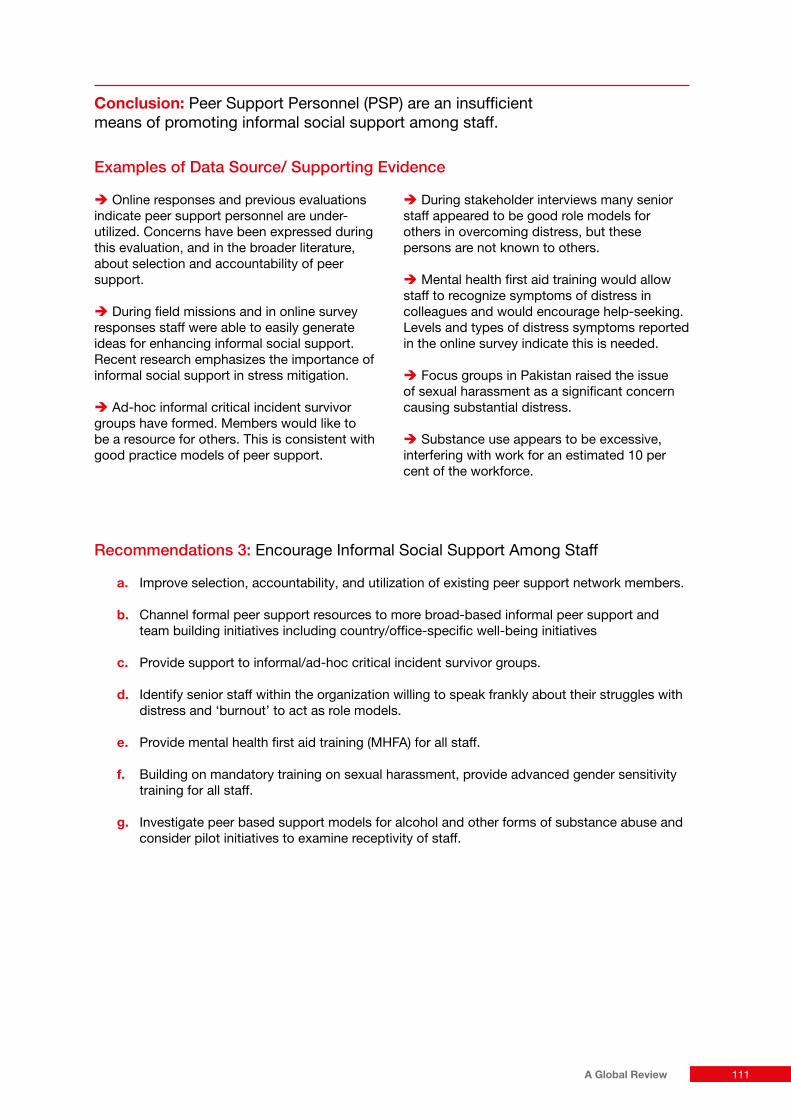
Conclusion: Peer Support Personnel (PSP) are an insufficient means of promoting informal social support among staff.
Examples of Data Source/ Supporting Evidence
è Online responses and previous evaluations indicate peer support personnel are under-utilized. Concerns have been expressed during this evaluation, and in the broader literature, about selection and accountability of peer support.
è During field missions and in online survey responses staff were able to easily generate ideas for enhancing informal social support. Recent research emphasizes the importance of informal social support in stress mitigation.
è Ad-hoc informal critical incident survivor groups have formed. Members would like to be a resource for others. This is consistent with good practice models of peer support.
è During stakeholder interviews many senior staff appeared to be good role models for others in overcoming distress, but these persons are not known to others.
è Mental health first aid training would allow staff to recognize symptoms of distress in colleagues and would encourage help-seeking. Levels and types of distress symptoms reported in the online survey indicate this is needed.
è Focus groups in Pakistan raised the issue of sexual harassment as a significant concern causing substantial distress.
è Substance use appears to be excessive, interfering with work for an estimated 10 per cent of the workforce.
Recommendations 3: Encourage Informal Social Support Among Staff
a. Improve selection, accountability, and utilization of existing peer support network members.
b. Channel formal peer support resources to more broad-based informal peer support and team building initiatives including country/office-specific well-being initiatives
c. Provide support to informal/ad-hoc critical incident survivor groups.
d. Identify senior staff within the organization willing to speak frankly about their struggles with distress and ‘burnout’ to act as role models.
e. Provide mental health first aid training (MHFA) for all staff.
f. Building on mandatory training on sexual harassment, provide advanced gender sensitivity training for all staff.
g. Investigate peer based support models for alcohol and other forms of substance abuse and consider pilot initiatives to examine receptivity of staff.
111A Global Review

Conclusion: There is a lack of accountability of staff welfare services. Regular rigorous evaluation, clear policies, and role distinction between sections are required.
Examples of Data Source/ Supporting Evidence
è UNHCR was not compliant with the majority of Antares ‘Good Practice’ Principles and associated indicators.
è Stakeholder interviews, field data, and online survey responses indicate there is a lack of management accountability for promoting (or undermining) staff well-being.
è Desk review and stakeholder interviews indicate a preliminary staff care policy was developed, but was never completed or rolled out.
è Stakeholder and critical incident survivor interviews indicated confusion regarding role distinction between staff welfare and medical.
Recommendations 4: Enhance Accountability of Staff Welfare Related Services through Regular Rigorous Evaluation, Clear Staff Welfare Policies, and Role Distinction between Sections.
a. Develop protocols for regular evaluation of staff distress levels and satisfaction with staff support services, e.g. online surveys; pre and post measures for specific programs; anonymous online evaluations for SWS mission visits, using indicators such as – “burnout” surveys, various forms of distress symptoms (note: many of these items can be pulled from the online staff survey Annex II).
b. Evaluate managers on staff welfare indicators such as staff perception of support (through anonymous means)
c. Roll out UNHCR Staff Care Policy (follow next steps recommendations made by PeopleInAid for Duty of Care Project 2011).
d. Clarify the roles of relevant services within DHRM - Staff Welfare Section, Medical, and Career Management Services.
e. Reallocate roles within SWS, with greater emphasis on case management, coordinator and referral to external (country-specific and remote web-based therapeutic) resources, capacity building, including support and replication of innovative country-specific pilot initiatives, and decreased emphasis on direct service provision.
112 UNHCR’S MENTAL HEALTH AND PSYCHOSOCIAL SUPPORT FOR STAFF
Annex VII.
Summary of Recommendations
� Ensure Appropriate Response and Follow up for Survivors of Critical Incidents
a. Provide Psychological First Aid (PFA) for all potential first responders.
b. Disseminate UNDSS Standard Operating Procedures (SOPs) for sexual assault of staff to all field based managerial positions.
c. Conduct internal reviews following critical incidents to determine compliance with protocols, and as a means of soliciting feedback from survivors.
d. Prioritize postings in low to moderate risk areas, at least in the short-term, for survivors of critical incidents.
e. Streamline procedures for recognition of service incurred incidents.
� Increase Availability and Utilization of Formal Mental Health and Psychosocial Support
a. Provide and promote the option for staff to utilize external mental health therapists remotely, e.g. Skype, telephone interviews.
b. Provide and promote the option for staff to utilize local external mental health therapists and traditional healers or religious figures where these may be preferred options.
c. Disseminate information on what is covered by UNSMIS for international staff and the Medical Insurance Plan (MIP) for national staff for outside therapeutic support, and promote a diverse range of staff support options within these coverage parameters.
d. Invest in an interactive website, including an external confidential component, with links to self-assessment tools such as https: //ecouch.anu.edu.au/welcome, and online follow up resources such as a Skype consultation with an internal or external therapist of choice.
e. Annually, or at a minimum during the end of an assignment or another transitional phase, provide a regularly scheduled mental health and psychosocial wellness checkup with the option for staff to decline at their own initiative: an “opt-out” model of compliance. Consider a brief mandatory mental health screen in the annual physical for those who “opt-out” of the more comprehensive evaluation. Use the annual physical as an opportunity to provide psycho-education about stress and coping and referral to external resources.
f. Put in place explicit means to both ensure, and explain limits of, confidentiality. Written informed consent should be obtained for all staff receiving even brief internal or external services. This should include specifying if anyone can be informed of session content without additional express written permission from staff and other limits of confidentiality such as risk of harm to self or others. Staff in positions of authority should sign a confidentiality agreement. Reports of critical incidents should at minimum, be de-identified before being distributed. Critical incident reports should have very restricted distribution even when victim details have been removed.
113A Global Review

� Encourage Informal Social Support Amongst Staff
a. Improve selection, accountability, and utilization of existing Peer Support Personnel in operations deciding to retain this model.
b. Channel formal, peer support resources such as training to more broad-based informal low-cost peer support groups and team building activities, including country or office-specific well-being initiatives.
c. Provide corporate managerial support to ad-hoc critical incident survivor peer groups.
d. Identify senior staff within the organization willing to speak frankly about their struggles with distress and burnout to act as role models.
e. Provide mental health first aid training (MHFA) for all managers.
f. Building on mandatory training on sexual harassment, provide advanced gender sensitivity training for all staff.
g. Investigate peer based support models for alcohol and other forms of substance abuse and consider pilot initiatives to examine receptivity of staff.
� Enhance Accountability of Staff Welfare Related Services through Regular Rigorous Evaluation, Clear Staff Welfare Policies, and Role Distinction between Sections
a. Develop protocols for regular evaluation of staff distress levels and satisfaction with staff support services, e.g. regular online surveys; anonymous online evaluations for SWS mission visits; pre and post measures for specific programs, using indicators such as – “burnout” and other distress symptoms (note: many of these items can be pulled from the online staff survey Annex II).
b. Evaluate managers on staff welfare indicators such as staff perception of support (through anonymous means).
c. Introduce a new UNHCR Staff Care Policy (follow next steps recommendations made by PeopleInAid for UNHCR Duty of Care Project 2011).
d. Clarify the roles of relevant services within DHRM – the Staff Welfare Section (SWS), Medical, and Career Management Services (CMS).
e. Reallocate roles in SWS, with greater emphasis on case management, coordination and referral to external (country-specific and remote web-based therapeutic) resources, capacity building, including support and replication of innovative country-specific pilot initiatives, and decreased emphasis on direct service provision.
114 UNHCR’S MENTAL HEALTH AND PSYCHOSOCIAL SUPPORT FOR STAFF


© United Nations High Commissioner for Refugees Policy Development & Evaluation Service Geneve, June 2013
Related Documents











