Anaesthetic Consideratio ns in preparations for the OR/OT Joachim Unger, MD Germany

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

Anaesthetic Consideratio
ns in preparations for the OR/OT
Joachim Unger, MD
Germany

-Can only concentrate on one patient-Acts as supportive psychotherapist for surgeons
Hates chaos
Characteristics of an
anesthesiologist
no conflict of interests


AirwayManagement-Respiratory Insuffency:
RR <6 / >29-GCS <9
-Hypoxia: Sat < 90%
-Hemodynamic Instability: BP <90

Choise of Induction
Hypnotics

Maintaining
SedationPrevention of
Awareness
No Pain
No Brain

Zeile 1 Zeile 2 Zeile 3 Zeile 40
2
4
6
8
10
12
Spalte 1Spalte 2Spalte 3
Effects of Muscle Relaxants
HyperkalemiaOxygen consuming
Long-term duration

Laryngoscopy #1
Laryngoscopy #2(+/- Bougie)
Laryngoscopy #3(Attending)
Laryngeal Mask Surgical Airway
ConfirmationCapnography
RSI

Video-Laryngoscopy superior
to direct Laryngoscopy?
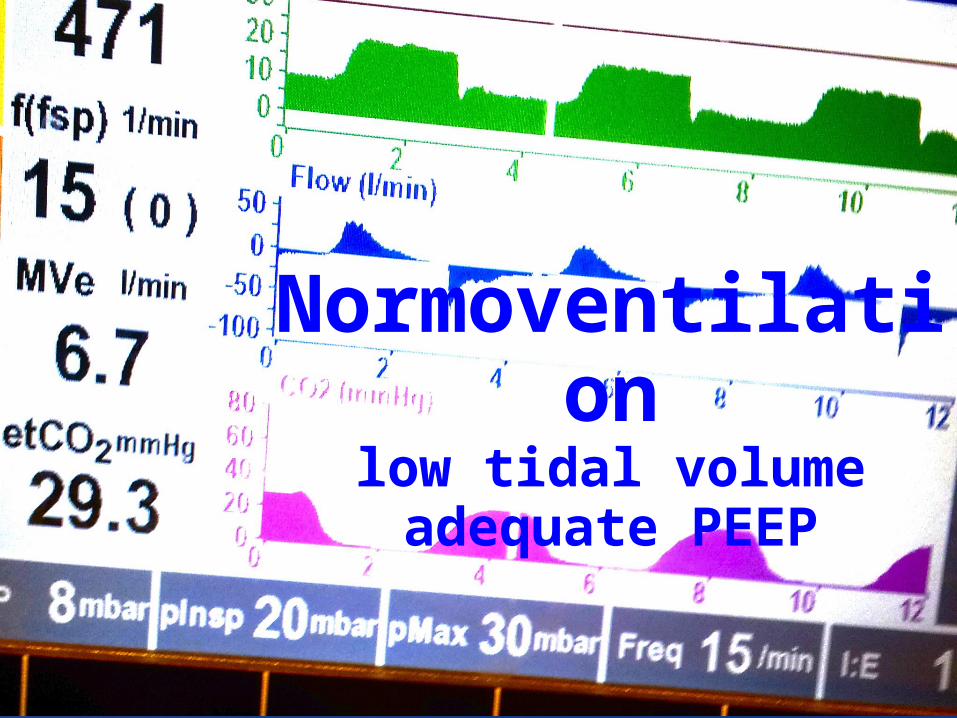
Normoventilationlow tidal volumeadequate PEEP

Damage Control
Resuscitation
Acidosis Hypocalcemia Hypothermia
Permissive Hypotentio
n

Establish venous
access
No fluid administration
in normotention

Second line: Intraosseal
access
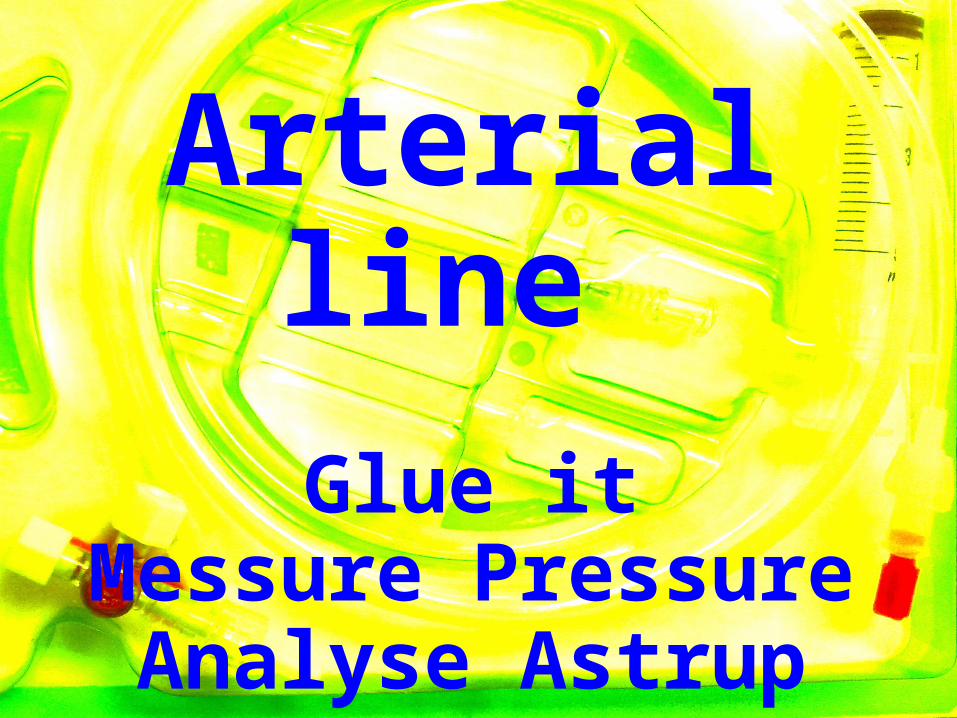
Arterial line Glue it
Messure PressureAnalyse Astrup

Lactate-free
Crystalloids
Starch is outRestrictiv
euse

Calcium and Tranexamic Acid
Avoid Hypocalcemia < 0,9
TXA: Early Administration 1g/10 min followed by 1g/8h

.
Transfusion Hematocrit 25-30

Ratio
RBC:FFP
1:1

Centralline
For massive Transfusion
Catecholamines can run initially peripherically

Temperature control
Warmedinfusion
Warmed blankets

Strategiesfor
rising ICPHyperventilation Mannitol
Hypertone NaCl 7,5%Normoxie
NormocapnieNormotonie
CCP > 50

Keep itSafe and Simple
(KISS)
References IStephens CT et al. The Success of Emergency Endotracheal Intubation in Trauma Patients: A 10-Year Experience at a Major Adult Trauma Referral Center. (Anesth Analg 2009;109:866–72)
Yeatts DJ et al. Effect of video laryngoscopy on trauma patient survival. J Trauma Acute Care Surg. 2013 Aug;75(2):212-9
Taha SK et al. Effect of suxamethonium vs rocuronium on onset of oxygen desaturation during apnoea following rapid sequence induction. Anaesthesia. 2010 Apr;65(4):358-61
Wagner CE et al. Etomidate Use and Postoperative Outcomes among Cardiac Surgery Patients. Anesthesiology 2014; 579-89
Wang X et al. Ketamine does not increase intracranial pressure compared with opioids. J Anesth 2014
Futier E et al. A trial of intraoperative low-tidal-volume ventilation in abdominal surgery. NEJM 2013
Errando CL et al. Awareness with recall during general anaesthesia: a prospective observational evaluation of 4001 patients. British Journal of Anaesthesia 101 (2): 178–85 (2008)
Turner J et al. (2000) A randomised controlled trial of prehospital intravenous fluid replacement therapy in serious trauma. Health Technol Assess 4:1-57
Kozek-Langenecker S (2007) Monitoring hemostasis in emergency medicine. Yearb Intensive Care Emerg Med 848-859

References IIShakur H et al. Effects of tranexamic acid on death, vascular occlusive events, and blood transfusion in trauma patients with significant haemorrhage (CRASH-2) Lancet 2010; 376:23-32
Simonova G1 et al. Cyanoacrylate tissue adhesives - effective securement technique for intravascular catheters: in vitro testing of safety and feasibility. Anaesth Intensive Care. 2012 May;40(3):460-6.
Wilkinson JN et al. Tissue adhesive as an alternative to sutures for securing central venous catheters. Anaesthesia. 2007 Sep;62(9):969-70.
Kwan I et al. (2003) Timing and volume of fluid administration for patients with bleeding. Cochrane Database Syst Rev
Bickell Wh et al. (1994) Immediate versus delayed fluid resuscitation for hypotensive patients with penetrating torso injuries. NEJM 331:1105-1109
Annane D1 et al. Effects of fluid resuscitation with colloids vs crystalloids on mortality in critically ill patients presenting with hypovolemic shock: the CRISTAL randomized trial. JAMA. 2013 Nov 6;310(17):1809-17.
John A. Myburgh et al. Hydroxyethyl Starch or Saline for Fluid Resuscitation in Intensive Care. NEJM 2012; 367:1901-1911Richard PD. Damage Control Anesthesia. International TraumaCare (ITACCS) Fall 2005
Perner A. Et al. Hydroxyethyl Starch 130/0.42 versus Ringer's Acetate in Severe Sepsis. NEJM 2012; 367:124-134
Brunkhorst FM et al. Intensive Insulin Therapy and Pentastarch Resuscitation in Severe Sepsis (VISEP) NEJM 2008;358:125-39
Related Documents











