UNDERSTANDING OSTEOPOROSIS Stephen L. Kates, MD Hansjӧrg Wyss Professor of Orthopaedic Surgery Department of Orthopedics and Rehabilitation Associate Director, Center for Musculoskeletal Research University of Rochester Medical Center THE AMERICAN GERIATRICS SOCIETY Geriatrics Health Professionals. Leading change. Improving care for older adults. AGS

UNDERSTANDING OSTEOPOROSIS Stephen L. Kates, MD Hansj ӧ rg Wyss Professor of Orthopaedic Surgery Department of Orthopedics and Rehabilitation Associate.
Dec 23, 2015
Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

UNDERSTANDING OSTEOPOROSIS
Stephen L. Kates, MDHansjӧrg Wyss Professor of Orthopaedic
SurgeryDepartment of Orthopedics and
RehabilitationAssociate Director, Center for
Musculoskeletal ResearchUniversity of Rochester Medical Center
THE AMERICAN GERIATRICS SOCIETY
Geriatrics Health Professionals.
Leading change. Improving care for older adults.
AGS

WHAT IS OSTEOPOROSIS?
• Skeletal disorder with: Compromised bone strength Increased risk of fractures Deterioration of microarchitecture
• Most common bone disease

Healthy vertebra
Osteoporotic vertebra
Slide 3

OSTEOPOROSIS
Normal bone Osteoporosis
Loss of critical bony interconnections
Thinner internal support
Slide 4

OSTEOPOROSIS OF THE HIP
Loss of critical bony trabeculae occurs with osteoporosis
Slide 5
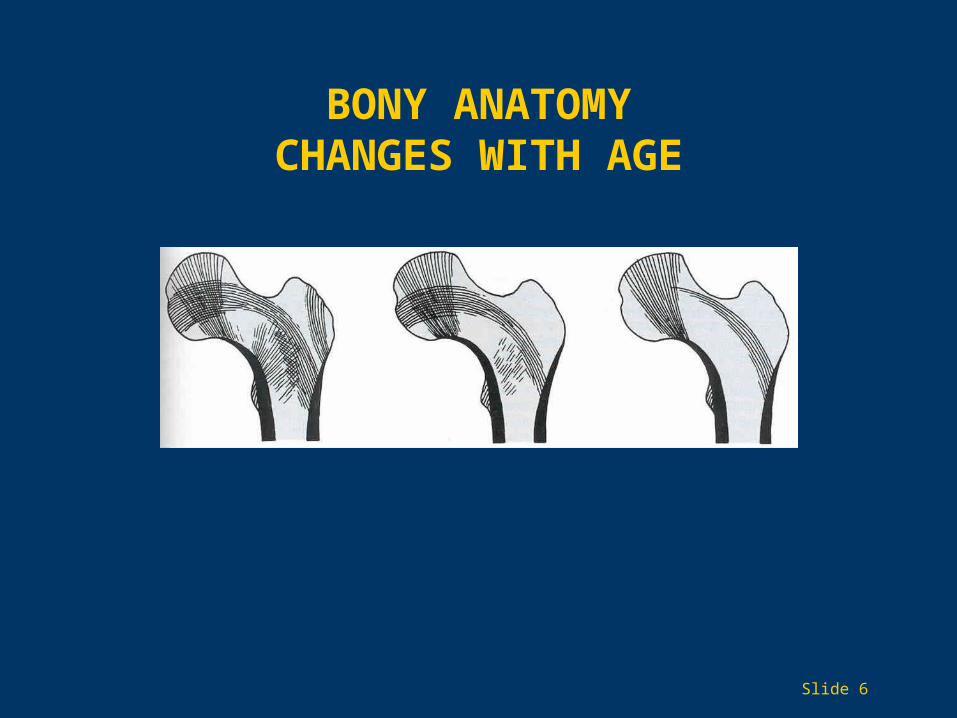
BONY ANATOMYCHANGES WITH AGE
Slide 6

WHAT ARE BONES MADE OF?
• Minerals bound to proteins
• Calcium
• Hydroxyapatite
• Organized collagen fibers
• Cells — osteocytes, osteoblasts, osteoclasts
Slide 7

BONE REMODELING
Slide 8
BONES CHANGE DURING LIFE
• Modeling as a child and adolescent
• Remodeling throughout life
• Peak bone mass reached in your 20s
• Remodeling allows bones to heal
• Resorption in later years
Slide 9

WHAT KEEPSNORMAL BONES HEALTHY?
• Genetic factors
• Moderate physical activity
• Calcium
• Vitamin D
• Hormones Parathyroid hormone Calcitonin Estrogen Testosterone
Slide 10
CAUSES OF OSTEOPOROSIS
• Primary
• Secondary
• Nutrition
• Lifestyle (Exercise, smoking, alcohol)
• Hormonal problems
• Age
• Medications (steroids, seizure meds)
Slide 11
FRAGILITY FRACTURE
• Caused by a fall from a standing height or less
• Osteoporosis is the cause
• 33%50% of women will develop a fragility fracture
• 15%33% of men get a fragility fracture
• Likelihood increases with age
Slide 12
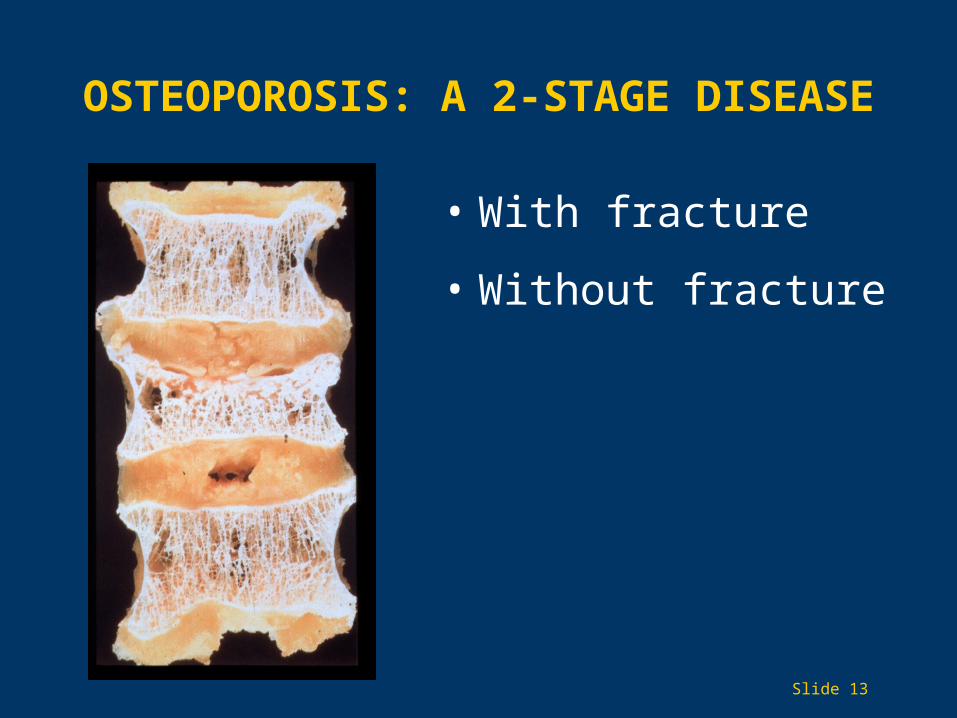
• With fracture
• Without fracture
OSTEOPOROSIS: A 2-STAGE DISEASE
Slide 13

HIP FRACTURELifetime Incidence in Women 1:6
Slide 14
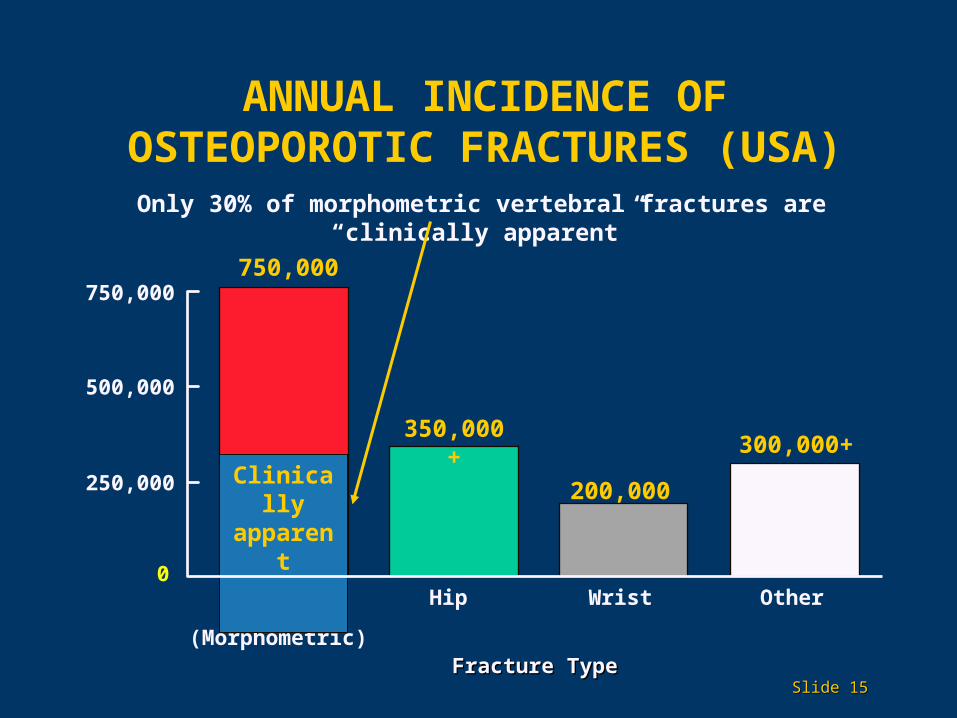
ANNUAL INCIDENCE OFOSTEOPOROTIC FRACTURES (USA)
Fracture TypeFracture Type
Hip
350,000+
Vertebral
(Morphometric)
750,000
300,000+
Wrist0
250,000
500,000
750,000
200,000
Other
Only 30% of morphometric vertebral fractures are “clinically apparent”
Clinically apparent
Slide Slide 1515

DIAGNOSIS OF OSTEOPOROSIS
• DEXA scan is best at present
• T score Compares density relative to peak bone mass
(normal healthy 25-year-old)Matched to sex and race
• Z score compares density to peers
Slide 16
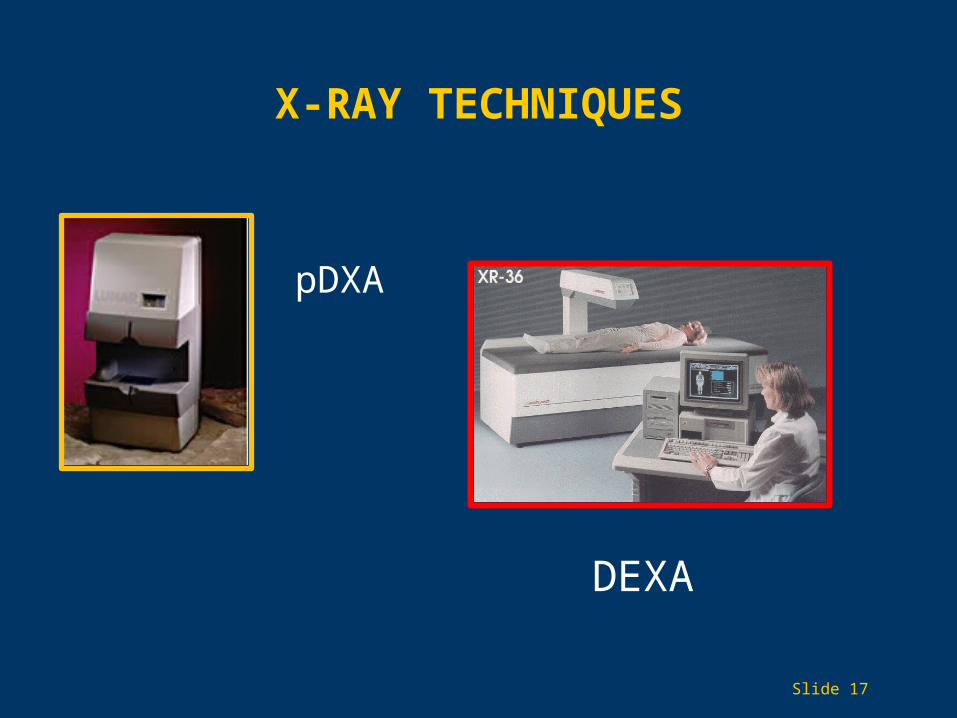
X-RAY TECHNIQUES
DEXA
pDXA
Slide 17

Slide Slide 1818
T scoreNormal > 1Osteopenia < 1 and > 2.5Osteoporosis 2.5Severe osteoporosis 2.5 with fracture
Mainly for spine and hip in women
WHO DEFINITIONS
WHO SHOULD BE TESTED?
• All women aged 65 and older regardless of risk factors
• Younger postmenopausal women with 1 or more risk factors (other than being white, postmenopausal, and female)
• Postmenopausal women who present with fractures (to confirm the diagnosis and determine disease severity)
Slide 19

CASES IN WHICH MEDICARE COVERS DEXA EVERY 2 YEARS
• Estrogen-deficient women at clinical risk of osteoporosis
• Individuals with vertebral abnormalities
• Individuals receiving, or planning to receive, long-term glucocorticoid (steroid) therapy
• Individuals with primary hyperparathyroidism
• Individuals being monitored to assess the response or efficacy of an approved osteoporosis drug therapy
Slide 20

WHAT ABOUT MEN?
• Fragility fracture
• Steroid use
• Forearm fracture
• Vertebral fracture
Slide 21

OSTEOPOROSIS IS TREATABLE
• Nutrition
• Exercise
• Lifestyle changes
• Medications
• Fall prevention
Slide 22

CALCIUM
• RequirementsYoung 1000 mg/day in 2 dosesOlder 1500 mg/day in 3 doses
• Calcium gluconate
• Calcium citrate
• Calcium carbonate
• Whatever you can tolerate
Slide 23

BODY WEIGHT
• Very low weight is a risk factor (<127 lb)
• Normal weight is best
• Obesity may predispose to falls
Slide 24
VITAMIN D3 (1 of 2)
• Deficiency is common with age
• Lack of sunlight
• Deficiency = osteomalacia
• Very common in nursing homes
• May cause fractured bones not to heal
Slide 25

VITAMIN D3 (2 of 2)
• Vitamin D3 — not D2 — is best
• Dose Young 400 units/day Older 600 to 800 units/day — maintenance If deficient, 50,000 units/day
• A blood test is needed to determine deficiency
• Sunlight helps — we have very little
• Essential for bone health!!!!!!
Slide 26

EXERCISE
• Weight-bearing exercise is best
• Low-impact exercise can help prevent falls
• Weight training
• Tai Chi
• Exercise helps other body systems too
• You have control over this!
• Helps to start young
Slide 27

FALL PREVENTION
• Medications can cause falls
• Poor lighting
• Throw rugs
• Fall-proofing the home
• Exercise, balance, and strength training
• Correct your vision
• Pets
Slide 28
CAUSES OF FALLS AT HOME
• Tripping
• Slipping
• Pets
• Ladders
• Stairs
• Poor lighting
Slide 29

LIFESTYLE
• Alcohol in moderation only
• Alcohol can cause osteoporosis
• Alcohol can cause falls
• Cigarette smoking causes osteoporosisMakes bones heal poorlySmoking cessation is the best plan
Slide 30

MEDICATIONS
• Many medications can hurt your bonesSteroids (prednisone)Seizure drugsElevated thyroid hormoneCancer drugs (Lupron)
• Avoid these if possible
• DEXA scans necessary with these
Slide 31

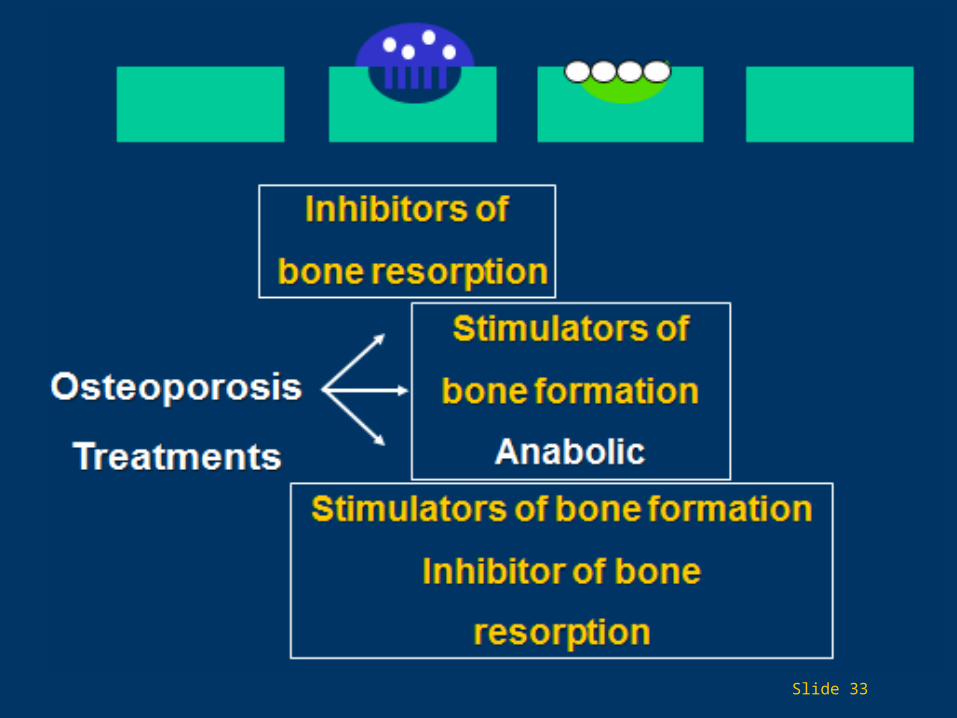
OSTEOPOROSIS MEDICATIONS
• Antiresorptive drugs
• Anabolic therapies
Slide 32
Slide 33
ANTI-RESORPTIVE THERAPIES: BISPHOSPHONATES
• Nonhormone compounds
• Bind to hydroxyapatite crystals in bone
• Inhibit the osteoclasts that resorb bone
• Cause osteoclasts to die prematurely
• Half-life 6 to 10 years in bone
• Can be taken by mouth or IV
Slide 34

ORAL BISPHOSPHONATES
• Alendronate (Fosamax)
• Risedronate (Actonel)
• Ibandronate (Boniva)
• IV bisphosphonates are used when oral medications are not tolerated
• Work for men and women
• Best treatment for steroid osteoporosis
Slide 35
Fra
ctu
re
Ris
k R
edu
ctio
n (
%)
Fra
ctu
re
Ris
k R
edu
ctio
n (
%)
Anysymptomatic
WristVertebral (radiographic)
Multiple vertebral
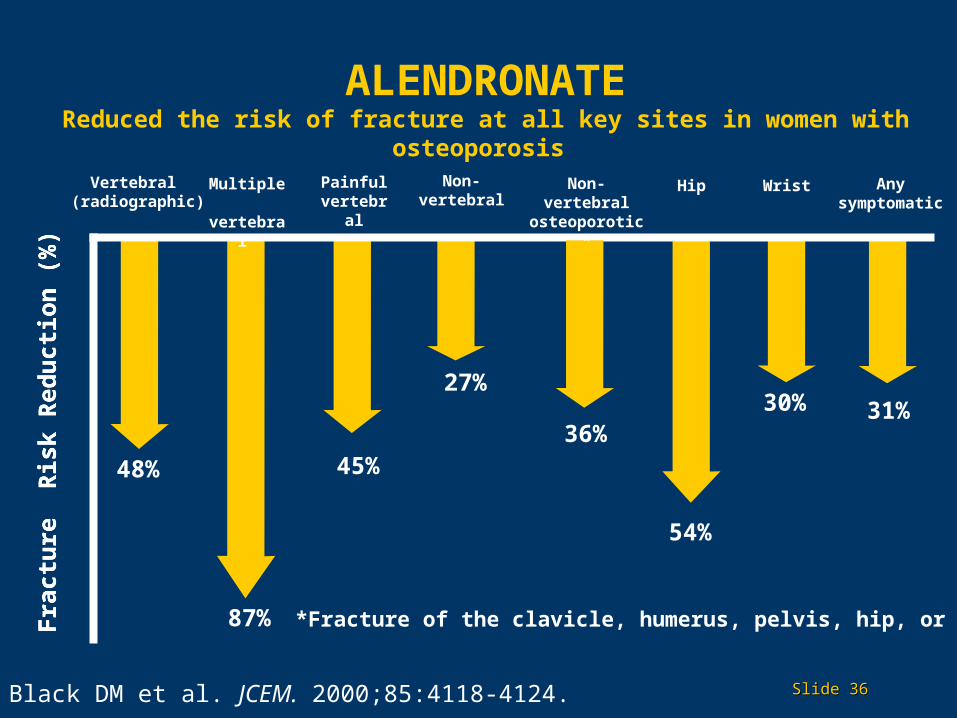
54%
27%
45%
87%
48%
30%
Non-vertebral
HipPainful vertebral
31%36%
Non-vertebral osteoporotic*
*Fracture of the clavicle, humerus, pelvis, hip, or leg
Black DM et al. JCEM. 2000;85:4118-4124. Slide Slide 3636
ALENDRONATEReduced the risk of fracture at all key sites in women with osteoporosis

BISPHOSPHONATES: PROBLEMS
• Reflux
• Must be upright for 1 hour
• Mostly GI symptoms
• Rare: osteonecrosis of jaw
• Long-term effects not known
Slide 37

ANTI-RESORPTIVE THERAPIES:SERMs
• Raloxifene and tamoxifen
• Bind to estrogen receptor
• Have a good effect on bone density
• For women only
• Should be used with calcium, vitamin D
• Reduce risk of breast cancer
• Increase risk of a blood clot
Slide 38
CALCITONIN
• Hormone that regulates calcium, bone
• Synthetic salmon calcitonin
• Decreases bone resorption
• Reduces pain from vertebral fractures
• Nasal spray or injection
Slide 39

TERIPARATIDE (FORTEO)(1 of 3)
• Synthetic hormone like human parathyroid hormone
• Builds bone mass
• Improves bone quality
• Increases the life span of osteoblasts
• Injection for 2 to 3 years
Slide 40
TERIPARATIDE (FORTEO)(2 of 3)
• FDA-approved for women with:High fracture riskMultiple fracturesFailure of other therapies
• FDA-approved for men with:Hypogonadal osteoporosisHigh fracture risk
Slide 41

TERIPARATIDE (FORTEO)(3 of 3)
• Contraindications• Previous radiation therapy• Paget’s disease• Young patients still growing
• Very expensive
Slide 42

Visit us at:
Facebook.com/AmericanGeriatricsSociety
Twitter.com/AmerGeriatrics
www.americangeriatrics.org
THANK YOU FOR YOUR TIME!
linkedin.com/company/american-geriatrics-society
Slide 43
Related Documents











