Umar Chaudhry+, Saba Hamid+, Umber Shafique+, Joan Maley+, Bruno Polliceni+, Henry Hoffmman* KNOWING WHAT, WHEN AND HOW TO INTERPRET: GUIDE TO IMAGING SALIVARY GLAND PATHOLOGY + Section of Neuroradiology, Department of Diagnostic Radiology, Univeristy of Iowa Hospitals and Clinics. * Department of Otolaryngology, University of Iowa Hospitals and Clinics. eEdE#: eEdE-127

Umar Chaudhry+, Saba Hamid+, Umber Shafique+, Joan Maley+, Bruno Polliceni+, Henry Hoffmman* KNOWING WHAT, WHEN AND HOW TO INTERPRET: GUIDE TO IMAGING.
Dec 28, 2015
Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

Umar Chaudhry+, Saba Hamid+, Umber Shafique+, Joan Maley+, Bruno Polliceni+, Henry Hoffmman*
KNOWING WHAT, WHEN AND HOW TO INTERPRET: GUIDE TO IMAGING SALIVARY
GLAND PATHOLOGY
+ Section of Neuroradiology, Department of Diagnostic Radiology, Univeristy of Iowa Hospitals and Clinics. * Department of Otolaryngology,University of Iowa Hospitals and Clinics.
eEdE#: eEdE-127

OUTLINE
• INTRODUCTION
• MODALITIES AVAILABLE
• INDIVIDUAL MODALITIES
• INDICATIONS
• PROTOCOL
• ADVANTAGES
• DISADVATAGES
• PICTORIAL EXAMPLES
• PEARLS
“ The years teach much which the days never knew ” Ralph Waldo Emerson

INTRODUCTION
• Salivary gland pathology is one the most variable amongst the organ system
• Wide variety of imaging modalities used
• It becomes confusing to determine the most optimum modality when encountered with a clinical scenario
• With era of cost effectiveness, ever increasing patient awareness, and extensive clinician interactions, the expectations from a radiologist have increased
• This presentation is intended to be a quick reference guide and refresher for various tools in our arsenal when dealing with such scenarios

MODALITIES
• Computed Tomography
• Magnetic resonance imaging
• Ultrasound
• Conventional Sialography
• Nuclear imaging

COMPUTED TOMOGRAPHY (CT)

INDICATIONS:
Optimal:
Occasional:
- Inflammatory pathologies, infection- Obstructive pathologies: stones
- CT sialography, ductal pathology- Masses- Post radiation

PROTOCOL- Multidetector CT (MDCT)- kVP 80-120 kVP- Dose reduction techniques:
- Thyroid bismuth shields- Automated dose reduction- Lower kV- Studies showed no significant diagnostic difference between 80 and
120 kV protocols - Inflammatory conditions, abscess usually IV contrast- Stones - Non contrast
ADVANTAGES
- Quick- Readily available- Gross anatomical detail of surrounding structuresextent of
inflammation- High sensitivity for Stones/calcifications- 3D reconstructions: CT Sialography
DISADVANTAGES
- Ionizing radiation- pregnant and children- Not ideal for tumors as higher detail from MRI- Perineural spread in malignancies is difficult- Poor ductal anatomical detail with standard CT

Inflammation of left parotid gland
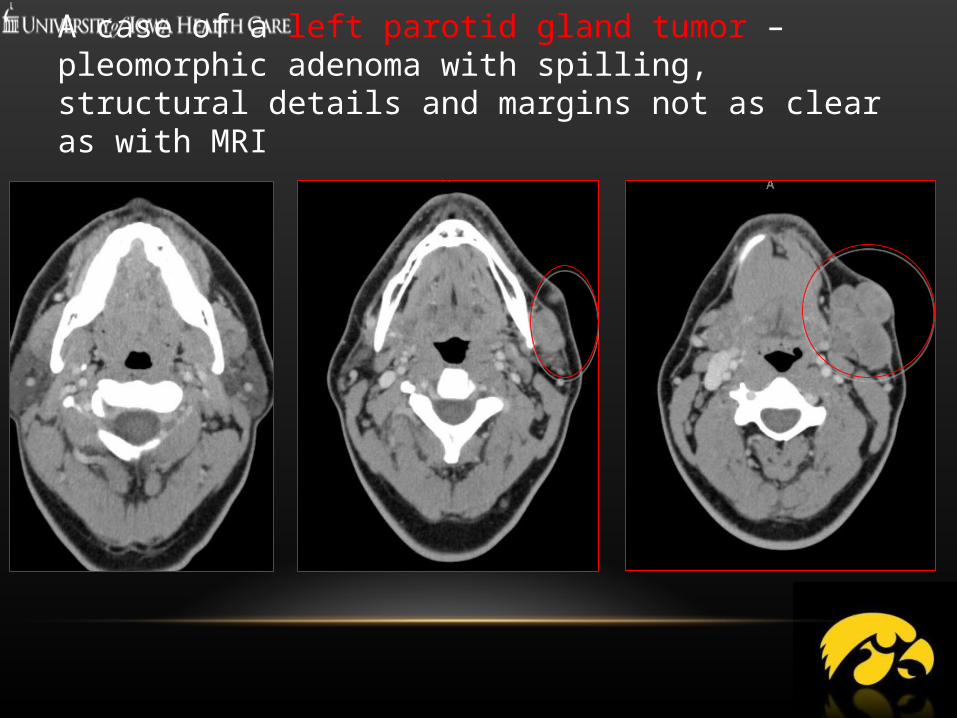
A case of a left parotid gland tumor – pleomorphic adenoma with spilling, structural details and margins not as clear as with MRI

RIGHT SUBMANDIBULAR GLAND DUCT STONE (RECTANGLE) WITH DILATED DUCT (CIRCLE)
PEARLS - CT
- Acute conditions in adult patients- Inflammation- Stones questioned- With radiation awareness, consider dose modulation

MAGNETIC RESONANCE IMAGING (MRI)

INDICATIONS
Salivary gland massesSystemic conditions, usually non acuteDuctal anatomy - Sialography

PROTOCOL
- For masses or major salivary glands, usually gadolinium based contrast
- Varies from one institution to the other - Our institution protocol
- 3 plane localizer - Coronal and axial T2- Axial T1- Diffusion- 3 plane post -contrast T1 images

EXAMPLE OF SCAN VOLUMES FOR PAROTID GLAND

MRI SIALOGRAPHY- Relies on heavily T2 weighted sequences and water property of saliva
- Side of abnormality and duct included in the scan volume for MR Sialography
- Protocol also varies from institution to institution
- 2D pulse sequences used traditionally - Projection and Maximum Intensity projections for Sialography
- 2D pulse sequence techniques to increase quality of images include
- Projection technique by using a microscopic coil improving the quality of the images obtained with larger coils
- Recently 3D pulse sequences utilized for more post processing options

ADVANTAGES
- No radiation- Non invasive- Excellent gland detail- Tumor characterization, using signal intensity, margins,
pattern of spread, diffusion coefficients- Facial nerve characterization in parotid lesions

DISADVANTAGES
- Time consuming - not ideal for acute settings- Expensive - Limited field of view - More susceptible to artifacts- Ductal detail needs careful optimization, otherwise may be
confounded by vessels etc.

PEARLS
- Non acute - Ideal for major salivary gland masses and systemic conditions such
as Sjogren characterization- Spread of malignancies- perineural tumor spread- New techniques such as dynamic contrast high potential - After optimization ductal details acquired non invasively
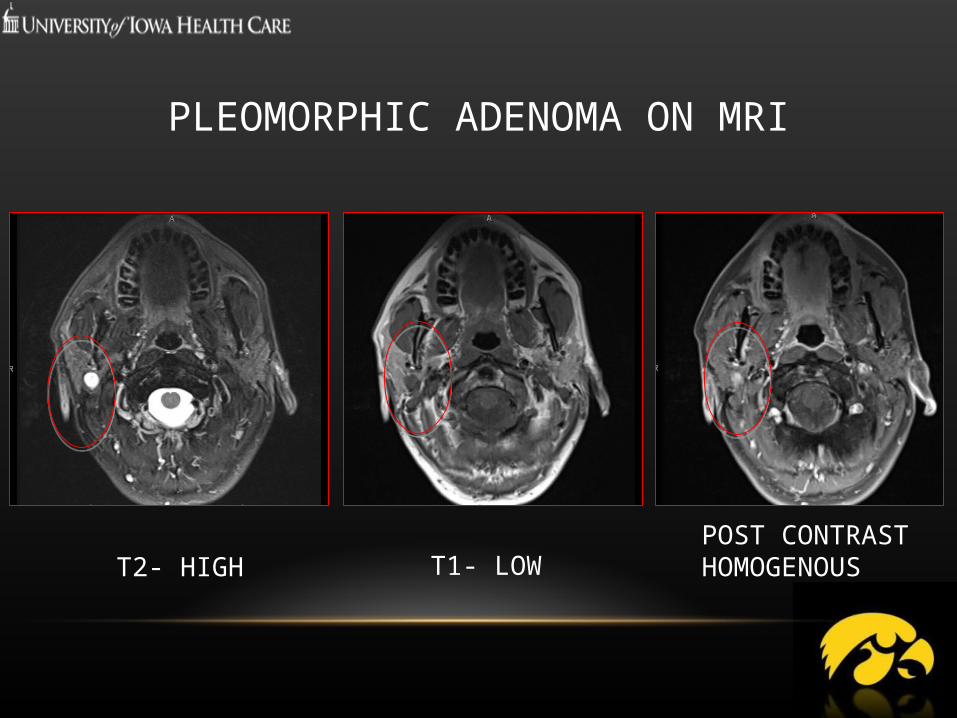
PLEOMORPHIC ADENOMA ON MRI
T1- LOWT2- HIGHPOST CONTRAST HOMOGENOUS

MALIGNANT PAROTID TUMOR WITH PERINEURAL TUMOR SPREAD (CIRCLE)

ULTRASOUND

INDICATIONS:
- Acute inflammations- Pediatric and pregnant population - Image guided procedures- Initial screening of major salivary gland mass
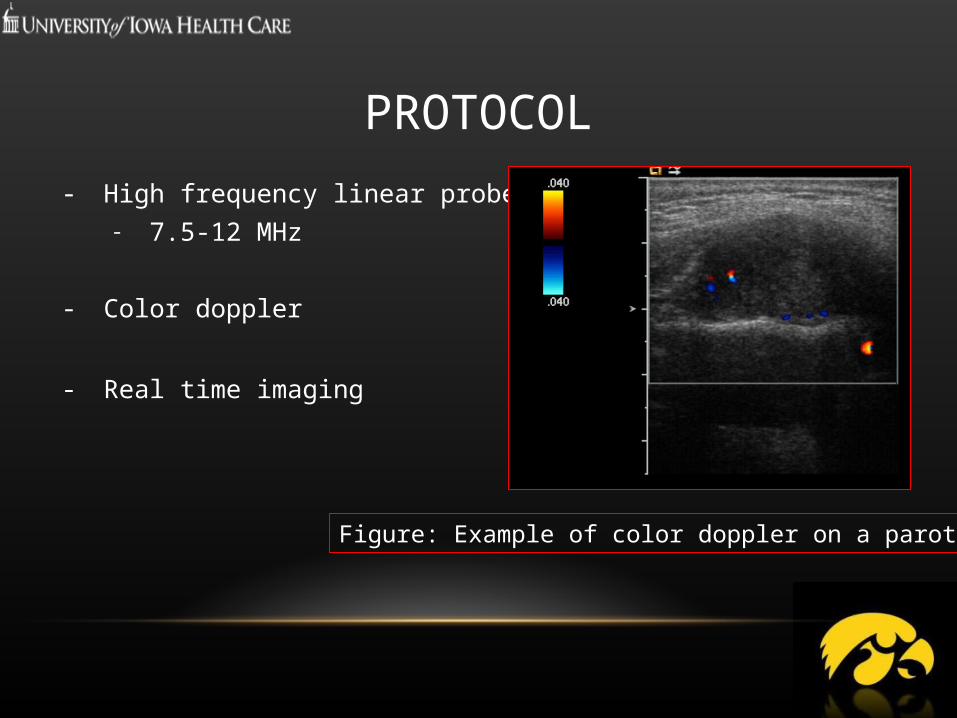
PROTOCOL
- High frequency linear probes- 7.5-12 MHz
- Color doppler
- Real time imaging
Figure: Example of color doppler on a parotid mass
ADVANTAGES
- No ionizing radiations- Quick- Real time imaging- image guided procedures- Less expensive and more readily available than MRI
DISADVANTAGES
- Operator dependence- Ducts especially Parotid duct not well seen unless largely
dilated- Limited field of view- Deeper pathologies such as
parapharyngeal space lesions and deep lobes of parotid glands not well see
- Less specific characterization of masses as compared to MRI
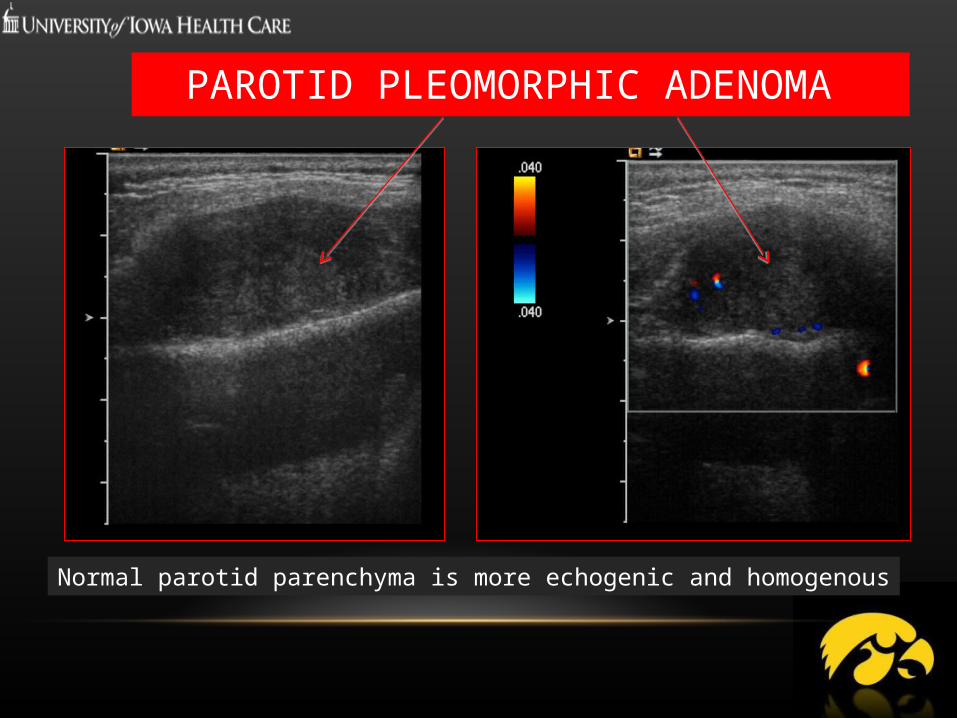
PAROTID PLEOMORPHIC ADENOMA
Normal parotid parenchyma is more echogenic and homogenous
PEARLS
- Children and pregnant patients- Initial screening for acute conditions such as infections- Image guided procedures- One of the most cost effective modalities in cross sectional imaging

CONVENTIONAL SIALOGRAPHY
INDICATIONS:
- Obstructive and ductal salivary gland pathology- Preoperative exam before sialendoscopy
PROTOCOL- Fluoroscopy- real time imaging- Usually Kv range close to 70 kV- Iodine based contrast directly instilled into major salivary gland ducts- Images in two planes- Ductal and glandular phase- Stimulation for glandular phase - Lime/candy
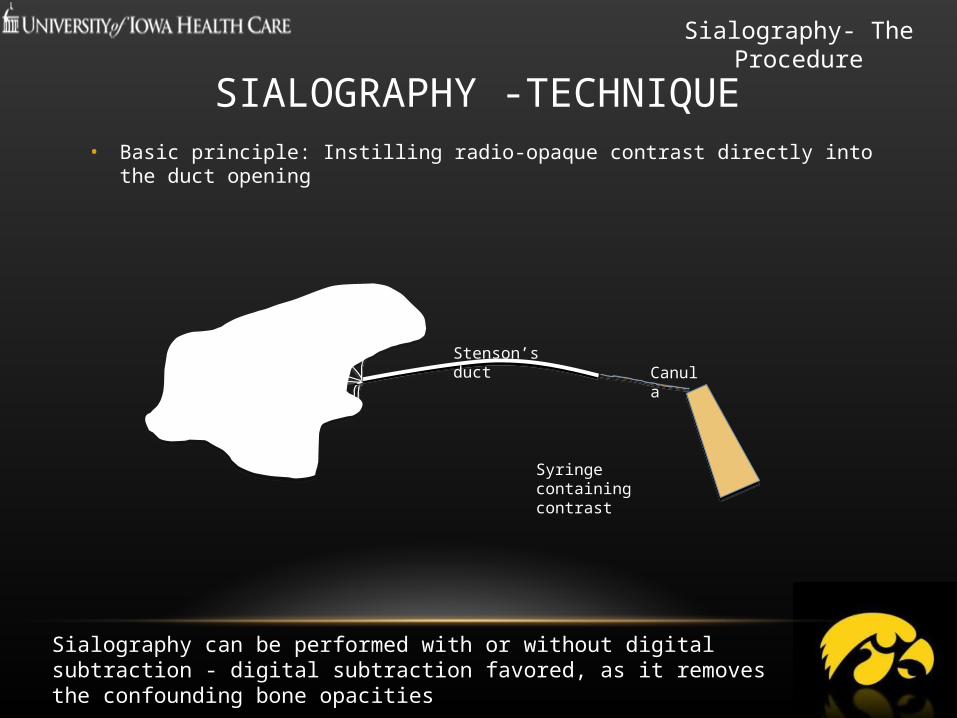
SIALOGRAPHY -TECHNIQUE• Basic principle: Instilling radio-opaque contrast directly into the duct opening
Sialography can be performed with or without digital subtraction - digital subtraction favored, as it removes the confounding bone opacities
Syringe containing contrast
CanulaStenson’s duct
Salivary Gland
Sialography- The Procedure
ADVANTAGES- Resurgence due to preoperative insight before minimally
invasive ENT procedures- Ductal resolution and detail superior to many other
modalities- Lower dose than CT sialography

DISADVANTAGES
- Invasive- Ionizing radiation- Expertize required
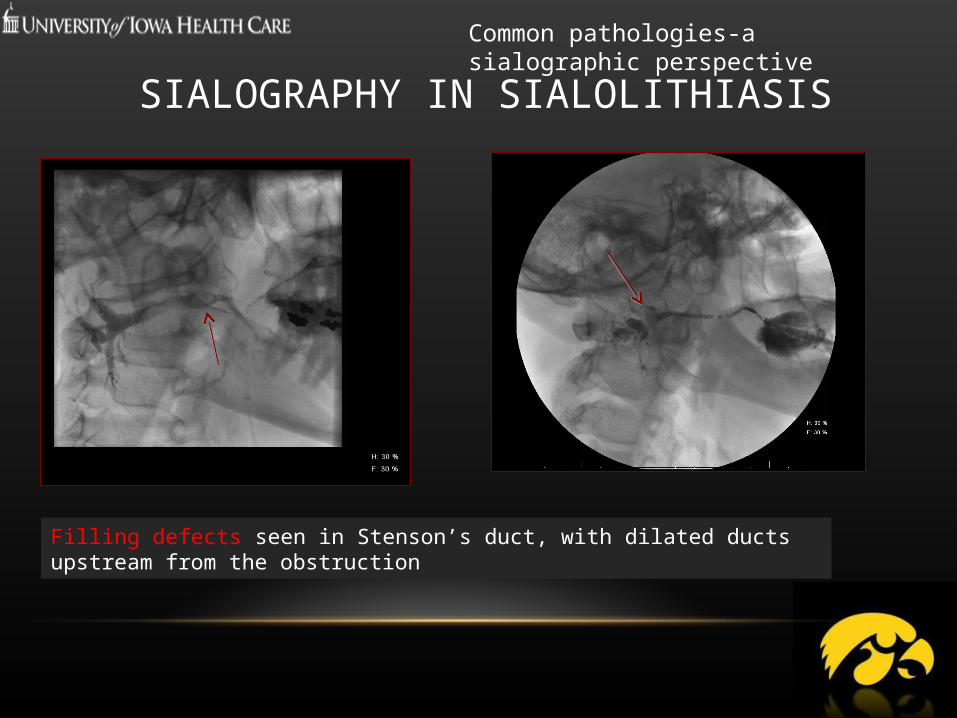
SIALOGRAPHY IN SIALOLITHIASIS
Filling defects seen in Stenson’s duct, with dilated ducts upstream from the obstruction
Common pathologies-a sialographic perspective

PEARLS
- Not to be overlooked and seeing a resurgence due to new minimally invasive techniques in ENT
- Ductal pathology well seen- Usually requires close collaboration with ENT

NUCLEAR MEDICINE

INDICATIONS:- Long term dysfunction/sialadenitis- Metastatic workup
PROTOCOL- Salivary scintigraphy
- Tc-99m Planar and SPECT imaging- Mainly for long term dysfunction after radioiodine
- PET- Fluoro-deoxy glucose for metastatic workup and distant lesions

ADVANTAGES
- Functional information - Distant metastatic lesions
DISADVANTAGES
- Non-specific for salivary gland tumors- Non acute pathologies only- Limited use- Cost and availabillity

PET-FDG SCAN IN METASTATIC SALIVARY GLAND TUMOR: NECK NODE AND RIGHT LUNG NODULE

PEARLS
- Overall limited role
- Chronic sialadenitis after radioactive iodine- Tc-99m scintigraphy
- FDG-PET is non specific, can be used for distant metastasis after tissue diagnosis
REFERENCES• Carotti M, Ciapetti A, Jousse-Joulin S, Salaffi F.Ultrasonography of the salivary glands: the role of grey-
scale and colour/power Doppler.Clin Exp Rheumatol. 2014 Jan-Feb;32(1 Suppl 80):S61-70. Epub 2014 Feb 17.
• Aghaghazvini L, Salahshour F, Yazdani N, Sharifian H, Kooraki S, Pakravan M, Shakiba M. Dynamic contrast-enhanced MRI for differentiation of major salivary glands neoplasms, a 3-T MRI study.Dentomaxillofac Radiol. 2015;44(2):20140166.
• Burke CJ, Thomas RH, Howlett D. Imaging the major salivary glands. Br J Oral Maxillofac Surg. 2011 Jun;49(4):261-9. Epub 2010 Apr 9.
• Harrison JD. Causes, natural history, and incidence of salivary stones and obstructions. Otolaryngol Clin North Am. 2009 Dec;42(6):927-47.
• Brown JE, Drage NA, Escudier MP, Wilson RF, McGurk M. Minimally invasive radiologically guided intervention for the treatment of salivary calculi. Cardiovasc Intervent Radiol. 2002 Sep-Oct;25(5):352-5. Epub 2002 Sep 18.

• Abdullah A, Rivas FF, Srinivasan A. Imaging of the salivary glands.Semin Roentgenol. 2013 Jan;48(1):65-74.
• Gonzalez-Beicos A, Nunez D. Imaging of acute head and neck infections.Radiol Clin North Am. 2012 Jan;50(1):73-83.
• Obinata K, Sato T, Ohmori K, Shindo M, Nakamura M. A comparison of diagnostic tools for Sjögren syndrome, with emphasis on sialography, histopathology, and ultrasonography. Oral Surg Oral Med Oral Pathol Oral Radiol Endod. 2010 Jan;109(1):129-34.
• Nahlieli O, Nakar LH, Nazarian Y, Turner MD. Sialoendoscopy: A new approach to salivary gland obstructive pathology. J Am Dent Assoc. 2006 Oct;137(10):1394-400.
• Mosier KM. Diagnostic radiographic imaging for salivary endoscopy. Otolaryngol Clin North Am. 2009 Dec;42(6):949-72.
REFERENCES

THANKS FOR WATCHING THE PRESENTATION
Visit us in Iowa – Go Hawkeyes!
Related Documents