Abstract Alzheimer’s disease (AD) is a major cause of dementia. Characteristic neuropathological features of AD include neurofibrillary tangles, senile plaques, amy- loid angiopathy and microvascular atrophy. The ultra- structure of the microvascular atrophy in AD and its pathogenetic significance have not been defined. This re- port presents an analysis of ultrastructural and morphome- tric features in the cerebral microvasculature of five brain biopsy specimens from AD patients. The cerebral mi- crovasculature normally constitutes the blood-brain bar- rier (BBB), characterized by interendothelial tight junc- tions, few pinocytotic vesicles and high mitochondrial content in endothelial cells. In the AD brain biopsy tissue analyzed in the present article, data for endothelial cells were expressed as percentage of cytoplasmic area occu- pied by the respective organelles. The values for vesicular content ranged from 0.49% to 1.17% and were inversely correlated with mitochondrial content, which ranged from 7.04% to 2.88%. These results indicate decreased mito- chondrial content and increased pinocytotic vesicles as compared to values obtained previously in endothelium from multiple sclerosis patients and in laboratory animals. Other findings such as accumulation of collagen in vascu- lar basement membranes and focal necrotic changes in en- dothelial cells are further indications of BBB disruption. These data, together with earlier reports, suggest that dys- function of the BBB is a characteristic feature of AD. Key words Basement membrane · Capillaries · Endothelium · Microvasculature · Mitochondria Introduction The microvasculature of the central nervous system (CNS) is highly specialized and has been shown to restrict the transit of macro-molecules between the blood and the CNS. This specialized CNS vasculature has been termed the blood-brain barrier (BBB) and functions to safeguard the homeostasis of the cerebral environment [4]. The main cellular component of the BBB, the endothelium, is characterized by the presence of interendothelial tight junctions with no fenestrations [5], paucity of pinocytotic vesicles [55], differential localization of enzymes between luminal and abluminal membranes [2], high mitochondr- ial content [48] and specialized glucose transporter sys- tems [22] among other features. Other components of the BBB include a well-defined basement membrane [64]; pericytes [38] and astrocyte foot processes surrounding the blood vessels [25]. Dysfunction of the BBB occurs in various pathological states in humans and in animal models. Changes in BBB permeability can be measured directly using in vivo neu- roimaging techniques [10, 32] or can be inferred through the ultrastructural analysis of changes in BBB features [11, 12, 14, 63]. In several studies of human subjects, changes in the ultrastructure of the BBB have been sub- stantiated by neuroimaging indications of a functional BBB disruption. Some of these include studies of patients with multiple sclerosis [6, 10, 13, 32], epilepsy [31, 47], and cerebral tumors [46, 56, 58]. These data suggest that neuropathological changes observed microscopically may correlate with impairment of BBB function, even when a mild increase in BBB permeability may not be detectable through neuroimaging techniques, as has also been con- cluded by others [36]. Using methods of ultrastructural morphometric analy- sis of BBB features, we have previously found that a de- crease in mitochondrial content and an increase in pinocy- totic vesicles in CNS endothelium correlate with edema formation and clinical signs in an animal model of multi- ple sclerosis [11, 14]. More recently, we have applied Luz Claudio Ultrastructural features of the blood-brain barrier in biopsy tissue from Alzheimer’s disease patients Acta Neuropathol (1996) 91 : 6–14 © Springer-Verlag 1996 Received: 12 June 1995 / Revised, accepted: 11 August 1995 REGULAR PAPER L. Claudio Division of Environmental and Occupational Medicine and Division of Neuropathology, Mount Sinai Medical Center, Box 1057, One Gustave L. Levy Place, New York, NY 10029, USA Fax: 1-212-996-0407

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript
Abstract Alzheimer’s disease (AD) is a major cause ofdementia. Characteristic neuropathological features ofAD include neurofibrillary tangles, senile plaques, amy-loid angiopathy and microvascular atrophy. The ultra-structure of the microvascular atrophy in AD and itspathogenetic significance have not been defined. This re-port presents an analysis of ultrastructural and morphome-tric features in the cerebral microvasculature of five brainbiopsy specimens from AD patients. The cerebral mi-crovasculature normally constitutes the blood-brain bar-rier (BBB), characterized by interendothelial tight junc-tions, few pinocytotic vesicles and high mitochondrialcontent in endothelial cells. In the AD brain biopsy tissueanalyzed in the present article, data for endothelial cellswere expressed as percentage of cytoplasmic area occu-pied by the respective organelles. The values for vesicularcontent ranged from 0.49% to 1.17% and were inverselycorrelated with mitochondrial content, which ranged from7.04% to 2.88%. These results indicate decreased mito-chondrial content and increased pinocytotic vesicles ascompared to values obtained previously in endotheliumfrom multiple sclerosis patients and in laboratory animals.Other findings such as accumulation of collagen in vascu-lar basement membranes and focal necrotic changes in en-dothelial cells are further indications of BBB disruption.These data, together with earlier reports, suggest that dys-function of the BBB is a characteristic feature of AD.
Key words Basement membrane · Capillaries · Endothelium · Microvasculature · Mitochondria
Introduction
The microvasculature of the central nervous system(CNS) is highly specialized and has been shown to restrictthe transit of macro-molecules between the blood and theCNS. This specialized CNS vasculature has been termedthe blood-brain barrier (BBB) and functions to safeguardthe homeostasis of the cerebral environment [4]. Themain cellular component of the BBB, the endothelium, ischaracterized by the presence of interendothelial tightjunctions with no fenestrations [5], paucity of pinocytoticvesicles [55], differential localization of enzymes betweenluminal and abluminal membranes [2], high mitochondr-ial content [48] and specialized glucose transporter sys-tems [22] among other features. Other components of theBBB include a well-defined basement membrane [64];pericytes [38] and astrocyte foot processes surroundingthe blood vessels [25].
Dysfunction of the BBB occurs in various pathologicalstates in humans and in animal models. Changes in BBBpermeability can be measured directly using in vivo neu-roimaging techniques [10, 32] or can be inferred throughthe ultrastructural analysis of changes in BBB features[11, 12, 14, 63]. In several studies of human subjects,changes in the ultrastructure of the BBB have been sub-stantiated by neuroimaging indications of a functionalBBB disruption. Some of these include studies of patientswith multiple sclerosis [6, 10, 13, 32], epilepsy [31, 47],and cerebral tumors [46, 56, 58]. These data suggest thatneuropathological changes observed microscopically maycorrelate with impairment of BBB function, even when amild increase in BBB permeability may not be detectablethrough neuroimaging techniques, as has also been con-cluded by others [36].
Using methods of ultrastructural morphometric analy-sis of BBB features, we have previously found that a de-crease in mitochondrial content and an increase in pinocy-totic vesicles in CNS endothelium correlate with edemaformation and clinical signs in an animal model of multi-ple sclerosis [11, 14]. More recently, we have applied
Luz Claudio
Ultrastructural features of the blood-brain barrier in biopsy tissue from Alzheimer’s disease patients
Acta Neuropathol (1996) 91 :6–14 © Springer-Verlag 1996
Received: 12 June 1995 / Revised, accepted: 11 August 1995
REGULAR PAPER
L. ClaudioDivision of Environmental and Occupational Medicine and Division of Neuropathology, Mount Sinai Medical Center, Box 1057, One Gustave L. Levy Place, New York, NY 10029, USAFax: 1-212-996-0407

these methods to study brain biopsy tissue from patientswith multiple sclerosis and found similar changes in thecontent of mitochondria and pinocytotic vesicles in capil-lary endothelial cells within chronic silent lesions [13]. Inthe present report, similar methods of analysis have beenapplied to study cerebrovascular changes in brain biopsytissues from patients with Alzheimer’s disease (AD).
AD and vascular dementia are the two primary causesof the clinical symptoms that constitute the dementiacomplex [33]. These two entities can be distinguishedthrough neuropathological examination, which in AD ischaracterized by the presence of three distinctive lesions:neurofibrillary tangles, senile plaques and cerebral amy-loid angiopathy. Another lesion that has long been ob-served in AD is the alteration of the microvasculature [1].However, the nature of these microvascular alterationshas not been defined, nor their pathogenetic significanceestablished.
In the study presented here, morphometric analysis ofmicrovascular features was performed in five brain biopsysamples obtained from patients with AD. The impossibil-ity of obtaining brain biopsy tissue from normal humansimpeded direct comparison with control samples. Never-theless, conclusions could be made that relate the presentresults to previous observations. The results, together withothers in the literature, suggest that subtle but significantindications of a BBB dysfunction are present in AD andmay be important in the pathogenesis of the disease.
Materials and methods
Biopsy procedure
CNS tissue was obtained at biopsy after approval by the Institu-tional Review Board and appropriate consent from the patients.Biopsies were cubes of tissue, 3–6 mm3, which were placed onsaline-soaked gauze within a sterile petri dish. Samples were im-mersed in cold 5% glutaraldehyde in phosphate buffer, pH 7.4. Af-ter 30 min, the tissue was cut into 1-mm slices, fixed for an addi-tional 1 h in glutaraldehyde, and postfixed in osmic acid for 1 h.The samples were dehydrated through a graded series of ethyl al-cohol, cleared in propylene oxide, and flat-embedded in epoxyresin. For electron microscopy, thin sections were cut from theepoxy blocks, placed on uncoated grids, stained with uranyl andlead salts, and carbon-coated prior to scanning in a JEOL JEM-100CX electron microscope.
All patients who underwent the biopsy procedure were diag-nosed clinically and neuropathologically as having AD in accor-dance with published diagnostic criteria [23, 34]. Of 12 biopsiesperformed, 5 were chosen by a clinical neuropathologist accordingto the following criteria: tissue preservation, similar sample area(cortical gray matter), degree of pathology and patient ages.
Visualization and quantitation
For quantitation of morphometric features, vessels with diametersof 10 µm or less (in the capillary range) were photographed sys-tematically in non-serial sections. First, the capillaries were pho-tographed at a magnification of × 3,000 and then non-overlappingphotographs were taken at × 20,000 to include all the visible en-dothelial cytoplasmic area. Analysis of relevant features was per-formed using a computer-assisted morphometric program (Jandel
Scientific Measurement System, Corte Madera, Calif.). A mini-mum of 40 vessels was analyzed from each patient. The number ofvessels analyzed to achieve statistical power in relation to samplesize was determined so that the square root of n would exceed thestandard deviation of the data [37]. Student’s paired t-test was usedto assess statistical significance.
Goniometer stage microscopy
To visualize the whole length of junctional clefts, grids wereplaced in an electron microscope equipped with a goniometer tiltstage (Hitachi, Japan). The grid was rotated so that the length ofthe junction would fall perpendicular to the tilt axis. Photographswere taken at various angles from the 0° axis.
Results
General characteristics
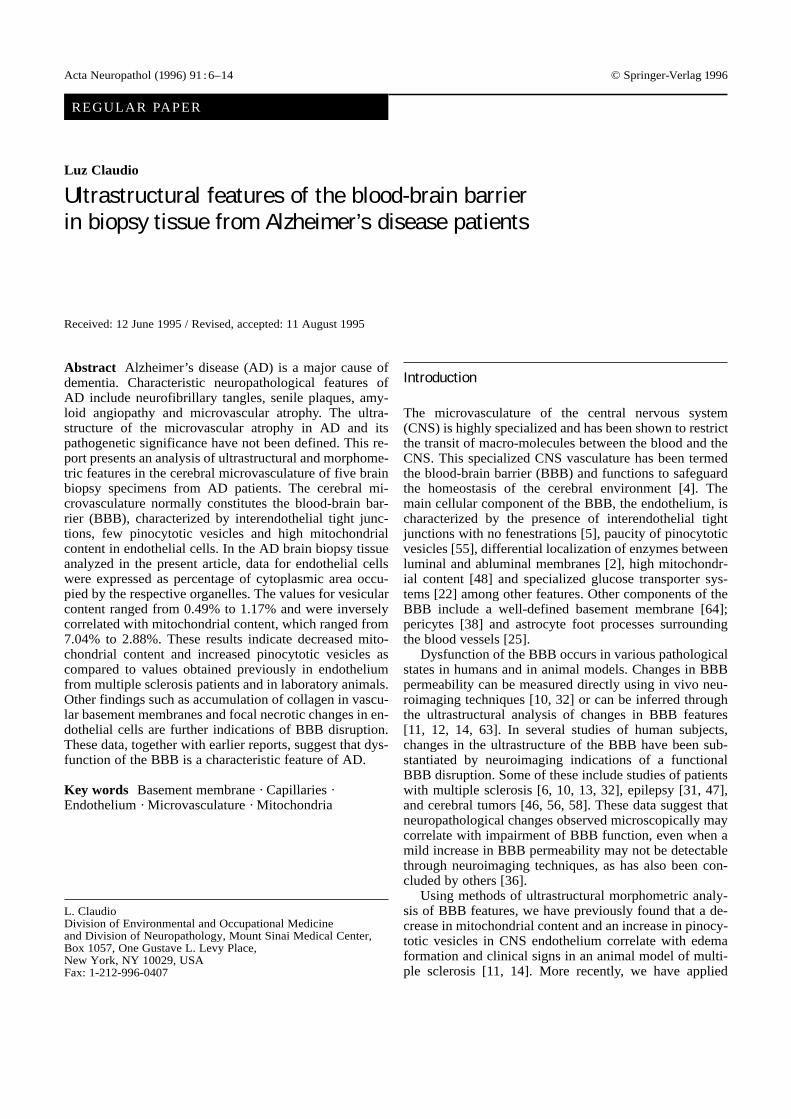
Excellent tissue preservation was obtained in these speci-mens as evidenced by the integrity of the tissueparenchyma and the lack of cellular vacuolization. Char-acteristic neuropathological features of AD, includingamyloid plaques and degenerating neurites are noted inFig.1. The mean lumen diameter of capillaries analyzedin this study was 7.29 ± 1.4 µm.
Structural characteristics of endothelial cells
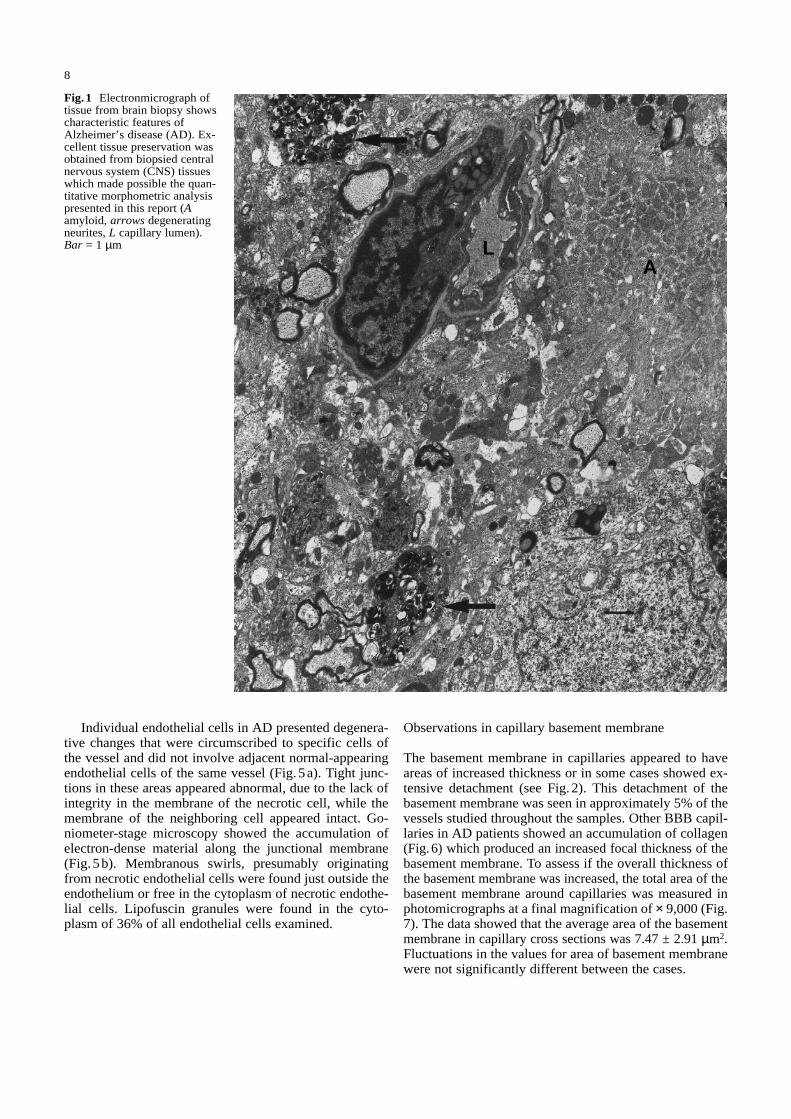
Photomicrographs were systematically obtained from en-dothelial cells at a magnification of × 20,000 and enlargedto × 60,000 for morphometric analysis. A representativeexample is shown in Fig.2 and the intracellular organellesmeasured are indicated. The data were calculated as thepercentage of endothelial cell cytoplasm occupied by therespective organelles. Pinocytotic vesicles measured anaverage of 72 ± 6.73 nm in diameter. In these patients, thepercentage of endothelial cell area occupied by pinocy-totic vesicles ranged from 0.49 ± 0.04% to 1.17 ± 0.1%with a mean of 0.76 ± 0.33% (Fig.3a). Mitochondrialcontent ranged from 7.04 ± 1.31% to 2.88 ± 0.39%. The mean for mitochondrial content was 5.48 ± 1.67%(Fig. 3b). An inverse correlation between vesicular andmitochondrial content in endothelial cells of CNS ca-pillaries was observed, with a correlation coefficient of–0.80.
Endothelial cell content of coated vesicles was as-sessed as a relative measure of receptor-mediated endocy-tosis in the same vessels. The percentage area of coatedvesicles had a mean of 0.08 ± 0.02% and did not vary sig-nificantly among the samples (Fig.4). The high variabilityof this measurement was due to the larger size of coatedvesicles (110 ± 9.81 µm in diameter), which makes a small difference in the number of coated vesiclesmore significant when expressed as percentage of cyto-plasmic area, as compared to pinocytotic vesicles.Tubules spanning the length of the endothelium were notobserved.
7
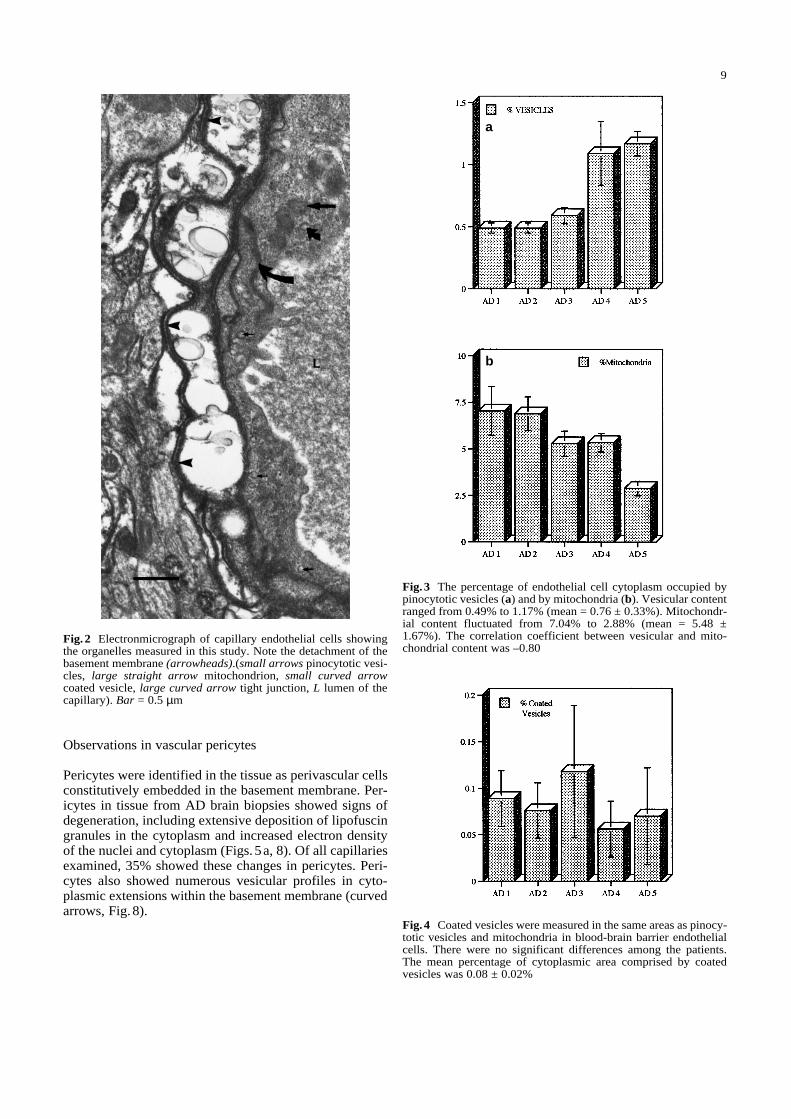
Individual endothelial cells in AD presented degenera-tive changes that were circumscribed to specific cells ofthe vessel and did not involve adjacent normal-appearingendothelial cells of the same vessel (Fig. 5a). Tight junc-tions in these areas appeared abnormal, due to the lack ofintegrity in the membrane of the necrotic cell, while themembrane of the neighboring cell appeared intact. Go-niometer-stage microscopy showed the accumulation ofelectron-dense material along the junctional membrane(Fig. 5b). Membranous swirls, presumably originatingfrom necrotic endothelial cells were found just outside theendothelium or free in the cytoplasm of necrotic endothe-lial cells. Lipofuscin granules were found in the cyto-plasm of 36% of all endothelial cells examined.
Observations in capillary basement membrane
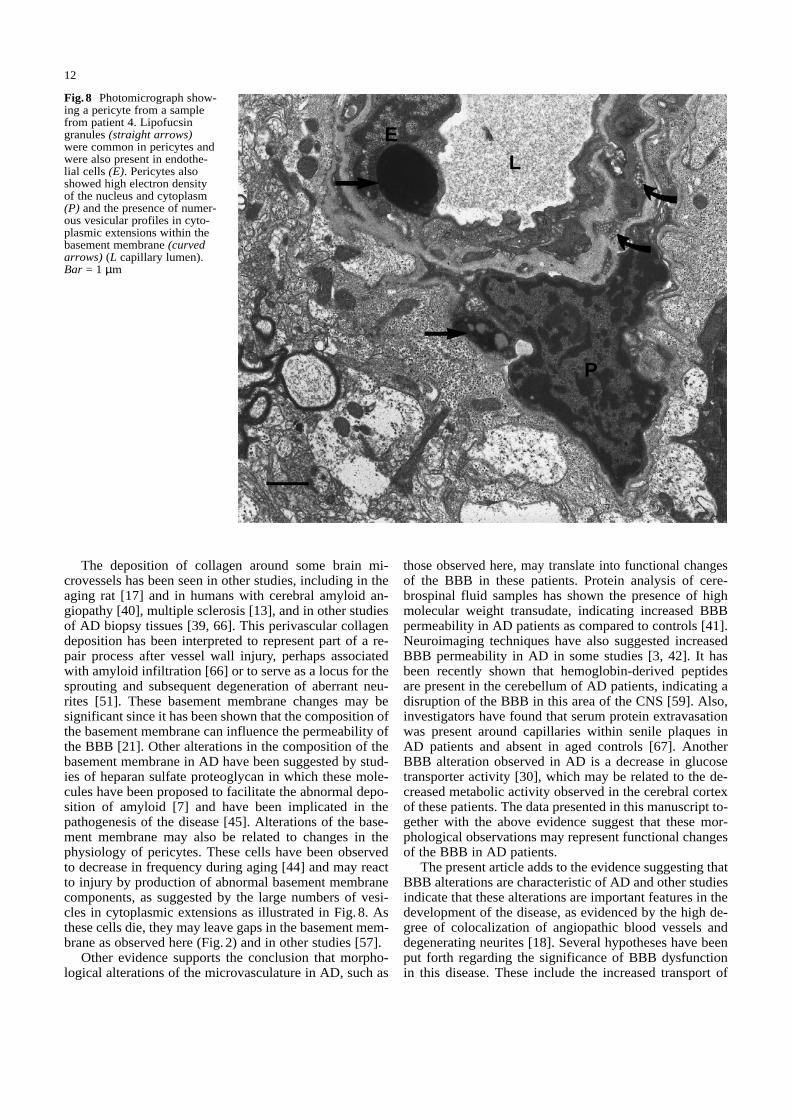
The basement membrane in capillaries appeared to haveareas of increased thickness or in some cases showed ex-tensive detachment (see Fig.2). This detachment of thebasement membrane was seen in approximately 5% of thevessels studied throughout the samples. Other BBB capil-laries in AD patients showed an accumulation of collagen(Fig.6) which produced an increased focal thickness of thebasement membrane. To assess if the overall thickness ofthe basement membrane was increased, the total area of thebasement membrane around capillaries was measured inphotomicrographs at a final magnification of × 9,000 (Fig.7). The data showed that the average area of the basementmembrane in capillary cross sections was 7.47 ± 2.91 µm2.Fluctuations in the values for area of basement membranewere not significantly different between the cases.
8
Fig.1 Electronmicrograph oftissue from brain biopsy showscharacteristic features ofAlzheimer’s disease (AD). Ex-cellent tissue preservation wasobtained from biopsied centralnervous system (CNS) tissueswhich made possible the quan-titative morphometric analysispresented in this report (Aamyloid, arrows degeneratingneurites, L capillary lumen).Bar = 1 µm L
A
Observations in vascular pericytes
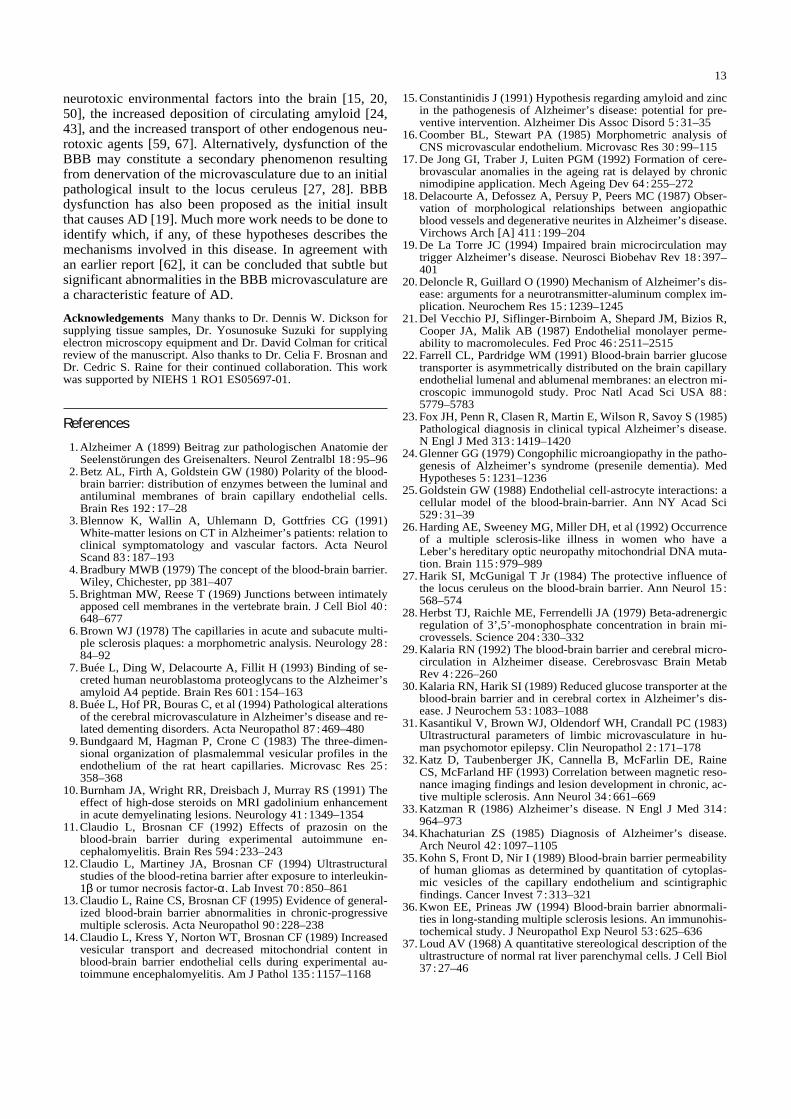
Pericytes were identified in the tissue as perivascular cellsconstitutively embedded in the basement membrane. Per-icytes in tissue from AD brain biopsies showed signs ofdegeneration, including extensive deposition of lipofuscingranules in the cytoplasm and increased electron densityof the nuclei and cytoplasm (Figs. 5a, 8). Of all capillariesexamined, 35% showed these changes in pericytes. Peri-cytes also showed numerous vesicular profiles in cyto-plasmic extensions within the basement membrane (curvedarrows, Fig. 8).
9
Fig.4 Coated vesicles were measured in the same areas as pinocy-totic vesicles and mitochondria in blood-brain barrier endothelialcells. There were no significant differences among the patients.The mean percentage of cytoplasmic area comprised by coatedvesicles was 0.08 ± 0.02%
Fig. 2 Electronmicrograph of capillary endothelial cells showingthe organelles measured in this study. Note the detachment of thebasement membrane (arrowheads).(small arrows pinocytotic vesi-cles, large straight arrow mitochondrion, small curved arrowcoated vesicle, large curved arrow tight junction, L lumen of thecapillary). Bar = 0.5 µm
Fig.3 The percentage of endothelial cell cytoplasm occupied bypinocytotic vesicles (a) and by mitochondria (b). Vesicular contentranged from 0.49% to 1.17% (mean = 0.76 ± 0.33%). Mitochondr-ial content fluctuated from 7.04% to 2.88% (mean = 5.48 ±1.67%). The correlation coefficient between vesicular and mito-chondrial content was –0.80
a
b
10
a
b
Fig.5a, b Focal degenerationof endothelial cells. a Somecapillary endothelial cellsshowed degenerative changesas evidenced by increased elec-tron density and vacuolation ofthe cytoplasm (arrows). Fre-quently, adjacent endothelialcells appeared normal (arrow-head). b An enlarged view ofthe area between two of thesecells shows the tight junctionbetween a normal-appearing(cell at left) and a degeneratedendothelial cell with membra-nous cellular debris present inthe cytoplasm and in the capil-lary lumen (arrowheads in b)and accumulation of electron-dense material along the junc-tional membrane (curved ar-row in b). Tilt angle = 10°.Bars a = 1 µm, b = 0.5 µm
Discussion
Many lines of evidence suggest that the cerebral mi-crovasculature is abnormal in AD. Some of the first stud-ies of AD noted the presence of atrophic vessels ([1], forreview see [29]). More recently, atrophic vessels that ap-peared tortuous and stenotic have also been observed inother dementia syndromes in addition to AD [8], but thenature and significance of this vascular atrophy have notbeen defined.
To address this topic, ultrastructural analysis of BBBfeatures in AD brain biopsies has been performed in thepresent report. The use of well-preserved biopsy samplesis necessary in this type of study where tissue integrity iscrucial; however, this presents a problem due to the lackof normal tissues for a controlled analysis [65]. To cir-
cumvent this problem, Stewart et al. [62] utilized “nor-mal-appearing” tissue obtained from patients undergoingprimary tumor removal as a control for a study of ADbrain biopsy tissues. However, in an earlier article theseauthors [60] had found that vessels in peritumoral braintissue “that were not immediately invested by tumor cellsalso showed some abnormalities”. Other observations ofmild increases in BBB permeability within apparentlynormal areas that do not produce enhancement withneuro-imaging techniques have also been reported byKwon and Prineas in multiple sclerosis autopsy material[36]. These reports, together with our earlier observations[11], indicate that increased BBB permeability can occurin the absence of gross tissue abnormalities. Therefore,utilization of apparently normal brain biopsy tissues ob-tained from patients with other neurological conditions ascontrol samples may not be representative of the BBB inits normal state.
Direct comparisons of morphometric values in humanswith those observed in animals may be useful but limitedby the possibility of interspecies variation and the diversemethodology used among investigators [61]. In the pre-sent study, pinocytotic vesicles measured an average of 72nm in diameter, within the range observed by Palade in1961 [49] and their frequency in the endothelium was in-versely correlated with mitochondrial content. This obser-vation parallels those made by others and by us in the rat[14, 48] and the rabbit [13].
The role of vesicular profiles in trans-endothelial trans-port has been controversial [9]. However, more recent ev-idence has shown that vesicles must fuse with the adven-titial plasma membrane for transport to occur, suggestingthat vesicular profiles travel across the cytoplasm [54].Those results, together with others [63], suggest that mor-phometric quantitation of pinocytotic vesicles is an appro-priate method for inferring the permeability of the BBB,since increased pinocytotic activity is one mechanism bywhich transport through the BBB can occur. Our conclu-sions are also consistent with the observation of largernumbers of vesicular profiles found in permeable en-dothelia than in “tight” endothelia in animals [16] and inhumans [35].
In agreement with the earlier report by Stewart et al.[62], mitochondrial content in endothelial cells was foundto be low in AD. This low mitochondrial content had aninverse relation with signs of increased vesicular transportin the present study. Regarding this observation, it is in-teresting to note that defects in mitochondrial functionhave been associated with multiple sclerosis-like illnessesin which the BBB is impaired [26, 53]. Decreases in themitochondrial content of cerebral endothelium have alsobeen observed in the aging monkey [44] and in mice withcerebral malaria [52] and indicated BBB dysfunction inboth studies. It has been suggested that BBB endotheliamay contain more mitochondria to maintain energy de-pendent systems such as the glucose transporter and theNa+, K+ pump [48]. A reduction in mitochondrial contentmay lower the endothelial cell capacity for normal barrierfunction, therefore allowing increased permeability.
11
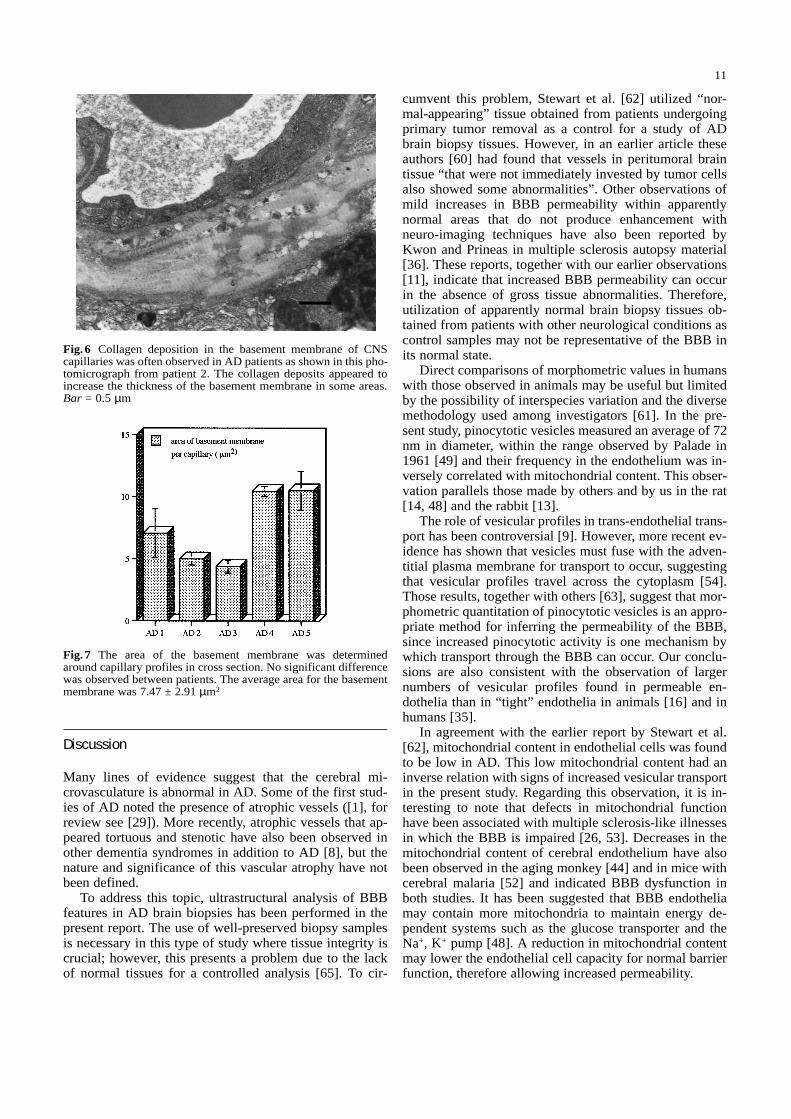
Fig. 6 Collagen deposition in the basement membrane of CNScapillaries was often observed in AD patients as shown in this pho-tomicrograph from patient 2. The collagen deposits appeared toincrease the thickness of the basement membrane in some areas.Bar = 0.5 µm
Fig. 7 The area of the basement membrane was determinedaround capillary profiles in cross section. No significant differencewas observed between patients. The average area for the basementmembrane was 7.47 ± 2.91 µm2
The deposition of collagen around some brain mi-crovessels has been seen in other studies, including in theaging rat [17] and in humans with cerebral amyloid an-giopathy [40], multiple sclerosis [13], and in other studiesof AD biopsy tissues [39, 66]. This perivascular collagendeposition has been interpreted to represent part of a re-pair process after vessel wall injury, perhaps associatedwith amyloid infiltration [66] or to serve as a locus for thesprouting and subsequent degeneration of aberrant neu-rites [51]. These basement membrane changes may besignificant since it has been shown that the composition ofthe basement membrane can influence the permeability ofthe BBB [21]. Other alterations in the composition of thebasement membrane in AD have been suggested by stud-ies of heparan sulfate proteoglycan in which these mole-cules have been proposed to facilitate the abnormal depo-sition of amyloid [7] and have been implicated in thepathogenesis of the disease [45]. Alterations of the base-ment membrane may also be related to changes in thephysiology of pericytes. These cells have been observedto decrease in frequency during aging [44] and may reactto injury by production of abnormal basement membranecomponents, as suggested by the large numbers of vesi-cles in cytoplasmic extensions as illustrated in Fig.8. Asthese cells die, they may leave gaps in the basement mem-brane as observed here (Fig. 2) and in other studies [57].
Other evidence supports the conclusion that morpho-logical alterations of the microvasculature in AD, such as
those observed here, may translate into functional changesof the BBB in these patients. Protein analysis of cere-brospinal fluid samples has shown the presence of highmolecular weight transudate, indicating increased BBBpermeability in AD patients as compared to controls [41].Neuroimaging techniques have also suggested increasedBBB permeability in AD in some studies [3, 42]. It hasbeen recently shown that hemoglobin-derived peptidesare present in the cerebellum of AD patients, indicating adisruption of the BBB in this area of the CNS [59]. Also,investigators have found that serum protein extravasationwas present around capillaries within senile plaques inAD patients and absent in aged controls [67]. AnotherBBB alteration observed in AD is a decrease in glucosetransporter activity [30], which may be related to the de-creased metabolic activity observed in the cerebral cortexof these patients. The data presented in this manuscript to-gether with the above evidence suggest that these mor-phological observations may represent functional changesof the BBB in AD patients.
The present article adds to the evidence suggesting thatBBB alterations are characteristic of AD and other studiesindicate that these alterations are important features in thedevelopment of the disease, as evidenced by the high de-gree of colocalization of angiopathic blood vessels anddegenerating neurites [18]. Several hypotheses have beenput forth regarding the significance of BBB dysfunctionin this disease. These include the increased transport of
12
Fig.8 Photomicrograph show-ing a pericyte from a samplefrom patient 4. Lipofucsingranules (straight arrows)were common in pericytes andwere also present in endothe-lial cells (E). Pericytes alsoshowed high electron densityof the nucleus and cytoplasm(P) and the presence of numer-ous vesicular profiles in cyto-plasmic extensions within thebasement membrane (curvedarrows) (L capillary lumen).Bar = 1 µm
L
P
E
neurotoxic environmental factors into the brain [15, 20,50], the increased deposition of circulating amyloid [24,43], and the increased transport of other endogenous neu-rotoxic agents [59, 67]. Alternatively, dysfunction of theBBB may constitute a secondary phenomenon resultingfrom denervation of the microvasculature due to an initialpathological insult to the locus ceruleus [27, 28]. BBBdysfunction has also been proposed as the initial insultthat causes AD [19]. Much more work needs to be done toidentify which, if any, of these hypotheses describes themechanisms involved in this disease. In agreement withan earlier report [62], it can be concluded that subtle butsignificant abnormalities in the BBB microvasculature area characteristic feature of AD.
Acknowledgements Many thanks to Dr. Dennis W. Dickson forsupplying tissue samples, Dr. Yosunosuke Suzuki for supplyingelectron microscopy equipment and Dr. David Colman for criticalreview of the manuscript. Also thanks to Dr. Celia F. Brosnan andDr. Cedric S. Raine for their continued collaboration. This workwas supported by NIEHS 1 RO1 ES05697-01.
References
1. Alzheimer A (1899) Beitrag zur pathologischen Anatomie derSeelenstörungen des Greisenalters. Neurol Zentralbl 18 :95–96
2. Betz AL, Firth A, Goldstein GW (1980) Polarity of the blood-brain barrier: distribution of enzymes between the luminal andantiluminal membranes of brain capillary endothelial cells.Brain Res 192 :17–28
3. Blennow K, Wallin A, Uhlemann D, Gottfries CG (1991)White-matter lesions on CT in Alzheimer’s patients: relation toclinical symptomatology and vascular factors. Acta NeurolScand 83 :187–193
4. Bradbury MWB (1979) The concept of the blood-brain barrier.Wiley, Chichester, pp 381–407
5. Brightman MW, Reese T (1969) Junctions between intimatelyapposed cell membranes in the vertebrate brain. J Cell Biol 40 :648–677
6. Brown WJ (1978) The capillaries in acute and subacute multi-ple sclerosis plaques: a morphometric analysis. Neurology 28 :84–92
7. Buée L, Ding W, Delacourte A, Fillit H (1993) Binding of se-creted human neuroblastoma proteoglycans to the Alzheimer’samyloid A4 peptide. Brain Res 601 :154–163
8. Buée L, Hof PR, Bouras C, et al (1994) Pathological alterationsof the cerebral microvasculature in Alzheimer’s disease and re-lated dementing disorders. Acta Neuropathol 87 :469–480
9. Bundgaard M, Hagman P, Crone C (1983) The three-dimen-sional organization of plasmalemmal vesicular profiles in theendothelium of the rat heart capillaries. Microvasc Res 25 :358–368
10. Burnham JA, Wright RR, Dreisbach J, Murray RS (1991) Theeffect of high-dose steroids on MRI gadolinium enhancementin acute demyelinating lesions. Neurology 41 :1349–1354
11. Claudio L, Brosnan CF (1992) Effects of prazosin on theblood-brain barrier during experimental autoimmune en-cephalomyelitis. Brain Res 594 :233–243
12. Claudio L, Martiney JA, Brosnan CF (1994) Ultrastructuralstudies of the blood-retina barrier after exposure to interleukin-1β or tumor necrosis factor-α. Lab Invest 70 :850–861
13. Claudio L, Raine CS, Brosnan CF (1995) Evidence of general-ized blood-brain barrier abnormalities in chronic-progressivemultiple sclerosis. Acta Neuropathol 90 :228–238
14. Claudio L, Kress Y, Norton WT, Brosnan CF (1989) Increasedvesicular transport and decreased mitochondrial content inblood-brain barrier endothelial cells during experimental au-toimmune encephalomyelitis. Am J Pathol 135 :1157–1168
15.Constantinidis J (1991) Hypothesis regarding amyloid and zincin the pathogenesis of Alzheimer’s disease: potential for pre-ventive intervention. Alzheimer Dis Assoc Disord 5 :31–35
16.Coomber BL, Stewart PA (1985) Morphometric analysis ofCNS microvascular endothelium. Microvasc Res 30 :99–115
17.De Jong GI, Traber J, Luiten PGM (1992) Formation of cere-brovascular anomalies in the ageing rat is delayed by chronicnimodipine application. Mech Ageing Dev 64 :255–272
18.Delacourte A, Defossez A, Persuy P, Peers MC (1987) Obser-vation of morphological relationships between angiopathicblood vessels and degenerative neurites in Alzheimer’s disease.Virchows Arch [A] 411 :199–204
19.De La Torre JC (1994) Impaired brain microcirculation maytrigger Alzheimer’s disease. Neurosci Biobehav Rev 18 :397– 401
20.Deloncle R, Guillard O (1990) Mechanism of Alzheimer’s dis-ease: arguments for a neurotransmitter-aluminum complex im-plication. Neurochem Res 15 :1239–1245
21.Del Vecchio PJ, Siflinger-Birnboim A, Shepard JM, Bizios R,Cooper JA, Malik AB (1987) Endothelial monolayer perme-ability to macromolecules. Fed Proc 46 :2511–2515
22.Farrell CL, Pardridge WM (1991) Blood-brain barrier glucosetransporter is asymmetrically distributed on the brain capillaryendothelial lumenal and ablumenal membranes: an electron mi-croscopic immunogold study. Proc Natl Acad Sci USA 88 :5779–5783
23.Fox JH, Penn R, Clasen R, Martin E, Wilson R, Savoy S (1985)Pathological diagnosis in clinical typical Alzheimer’s disease.N Engl J Med 313 :1419–1420
24.Glenner GG (1979) Congophilic microangiopathy in the patho-genesis of Alzheimer’s syndrome (presenile dementia). MedHypotheses 5 :1231–1236
25.Goldstein GW (1988) Endothelial cell-astrocyte interactions: acellular model of the blood-brain-barrier. Ann NY Acad Sci529 :31–39
26.Harding AE, Sweeney MG, Miller DH, et al (1992) Occurrenceof a multiple sclerosis-like illness in women who have aLeber’s hereditary optic neuropathy mitochondrial DNA muta-tion. Brain 115 :979–989
27.Harik SI, McGunigal T Jr (1984) The protective influence ofthe locus ceruleus on the blood-brain barrier. Ann Neurol 15 :568–574
28.Herbst TJ, Raichle ME, Ferrendelli JA (1979) Beta-adrenergicregulation of 3’,5’-monophosphate concentration in brain mi-crovessels. Science 204 :330–332
29.Kalaria RN (1992) The blood-brain barrier and cerebral micro-circulation in Alzheimer disease. Cerebrosvasc Brain MetabRev 4 :226–260
30.Kalaria RN, Harik SI (1989) Reduced glucose transporter at theblood-brain barrier and in cerebral cortex in Alzheimer’s dis-ease. J Neurochem 53 :1083–1088
31.Kasantikul V, Brown WJ, Oldendorf WH, Crandall PC (1983)Ultrastructural parameters of limbic microvasculature in hu-man psychomotor epilepsy. Clin Neuropathol 2 :171–178
32.Katz D, Taubenberger JK, Cannella B, McFarlin DE, RaineCS, McFarland HF (1993) Correlation between magnetic reso-nance imaging findings and lesion development in chronic, ac-tive multiple sclerosis. Ann Neurol 34 :661–669
33.Katzman R (1986) Alzheimer’s disease. N Engl J Med 314 :964–973
34.Khachaturian ZS (1985) Diagnosis of Alzheimer’s disease.Arch Neurol 42 :1097–1105
35.Kohn S, Front D, Nir I (1989) Blood-brain barrier permeabilityof human gliomas as determined by quantitation of cytoplas-mic vesicles of the capillary endothelium and scintigraphicfindings. Cancer Invest 7 :313–321
36.Kwon EE, Prineas JW (1994) Blood-brain barrier abnormali-ties in long-standing multiple sclerosis lesions. An immunohis-tochemical study. J Neuropathol Exp Neurol 53 :625–636
37.Loud AV (1968) A quantitative stereological description of theultrastructure of normal rat liver parenchymal cells. J Cell Biol37 :27–46
13
14
38.Majno G (1965) Ultrastructure of the vascular membrane. In:Hamilton WF, Dowie P (eds) Handbook of physiology, vol 3.American Physiological Society, Bethesda, pp 2293–2375
39.Mancardi GL, Perdelli F, Rivano C, Leonardi A, Gugiani O(1980) Thickening of the basement membrane of cortical cap-illaries in Alzheimer’s disease. Acta Neuropathol (Berl) 49 :79–83
40.Mandybur TI (1986) Cerebral amyloid angiopathy: the vascu-lar pathology and complications. J Neuropathol Exp Neurol 45 :79–90
41.Mattila KM, Pirttilä T, Blennow K, Wallin A, Viitanen M, FreyH (1994) Altered blood-brain barrier function in Alzheimer’sdisease? Acta Neurol Scand 89 :192–198
42.McGeer PL, Kamo H, Harrop R, et al (1986) Comparison ofPET, MRI, and CT with pathology in a proven case of Alz-heimer’s disease. Neurology 36 :1569–1574
43.Miyakawa T, Shimoji A, Kuramoto R, Higuchi Y (1982) Therelationship between senile plaques and cerebral blood vesselsin Alzheimer’s disease and senile dementia. Virchows Arch [B]40 :121–129
44.Mooradian AD (1988) Effect of aging on the blood-brain bar-rier. Neurobiol Aging 9 :31–39
45.Narindrasorasak S, Altman RA, Gonzalez-DeWhitt P, Green-berg, Kisilevsky R (1995) An interaction between basementmembrane and Alzheimer amyloid precursor proteins suggestsa role in the pathogenesis of Alzheimer’s disease. Lab Invest72 :272–283
46.Neuwelt EA, Frenkel EP (1989) The challenge of the blood-brain barrier. In: Neuwelt EA (ed) Implications of the blood-brain barrier and its manipulation, vol 1. Plenum Press, NewYork, pp 1–26
47.Oakley J, Ohemann GA, Ojeman LM, et al (1979) Identifyingepileptic foci on contrast-enhanced computerized tomographicscans. Arch Neurol 36 :669–671
48.Oldendorf WH, Cornford ME, Brown WJ (1977) The large ap-parent work capability of the blood-brain barrier: a study of themitochondrial content of capillary endothelial cells in brain andother tissues of the rat. Ann Neurol 1 :409–417
49.Palade GE (1961) Blood capillaries of the heart and other or-gans. Circulation 24 :368–384
50.Perl DP, Brody AR (1980) Alzheimer’s disease: X-ray spectro-metric evidence of aluminum accumulation in neurofibrillarytangle-bearing neurons. Science 208 :297–299
51.Perlmutter LS, Chang Chui H (1990) Microangiopathy, thevascular basement membrane and Alzheimer’s disease: a re-view. Brain Res Bull 24 :677–686
52.Polder TW, Eling WM, Kubat K, Jerusalem CR (1988) Histo-chemistry of cerebral lesions in mice infected with Plasmod-ium berghei. Trop Med Parasitol 39 :277–283
53.Powell BR, Kennaway NG, Rhead WJ, Reece CJ, BurlingameTG, Buist NRM (1990) Juvenile multiple sclerosis-likeepisodes associated with a defect of mitochondrial beta oxida-tion. Neurology 40 :487–491
54.Predescu D, Horvat R, Predescu S, Palade GE (1994) Transcy-tosis in the continuous endothelium of the myocardial mi-crovasculature is inhibited by N-ethylmaleimide. Proc NatlAcad Sci USA 91 :3014–3018
55.Reese TS, Karnovsky MJ (1967) Fine structural localization ofthe blood-brain barrier to exogenous peroxidase. J Cell Biol 34 :207–217
56.Sage MR, Turski PA, Levin A (1989) Central nervous systemimaging and the brain barriers. In: Neuwelt EA (ed) Implica-tions of the blood-brain barrier and its manipulation, vol 2.Plenum Press, New York, pp 1–51
57.Scheibel AB, Duong T (1988) On the possible relationship ofcortical microvascular pathology to blood brain barrier changesin Alzheimer’s disease. Neurobiol Aging 9 :41–42
58.Shibata S (1989) Ultrastructure of capillary walls in humanbrain tumors. Acta Neuropathol 78 :561–571
59.Slemmon JR, Hughes CM, Campbell GA, Flood DG (1994)Increased levels of hemoglobin-derived and other peptides inAlzheimer’s disease cerebellum. J Neurosci 14 :2225–2235
60.Stewart PA, Hayakawa K, Farrel CL, Del Maestro RF (1987)Quantitative study of microvessel ultrastructure in human peri-tumoral brain tissue. Evidence for a blood-brain defect. J Neu-rosurg 67 :697–705
61.Stewart PA, Magliocco M, Hayakawa K, et al (1987) A quan-titative analysis of blood-brain barrier ultrastructure in the ag-ing human. Microvasc Res 33 :270–282
62.Stewart PA, Hayakawa K, Akers M-A, Vinters HV (1992) Amorphometric study of the blood-brain barrier in Alzheimer’sdisease. Lab Invest 67 :734–742
63.Stewart PA, Hayakawa K, Farrell CL (1994) Quantitation ofblood-brain barrier ultrastructure. Microsc Res Tech 27 :516–527
64.Timpl R, Dziadek M (1986) Structure, development and mole-cular pathology of basement membrane. Int Rev Exp Pathol 29 :1–21
65.Torack RM (1979) Adult dementia: history, biopsy, pathology.Neurosurgery 4 :434–442
66.Vinters HV, Lenard Secor D, Read SL, et al (1994) Microvas-culature in brain biopsy specimens from patients with Alz-heimer’s disease: an immunohistochemical and ultrastructuralstudy. Ultrastruct Pathol 18 :333–348
67.Wisniewski HM, Kozlowski PB (1982) Evidence for blood-brain barrier changes in senile dementia of the Alzheimer type(SDAT). Ann NY Acad Sci 396 :119–129
Related Documents











