UKMI 38th Professional Development Seminar 2012 Poster collation 7. MiDatabank ADR reporting – One year on 8. Identification of hospital-specific quality signals (QSig) using documented enquiries to the drug information center (DIC) of the pharmacy. 9. Improving patient perception on the provision of medicines Information 10. Could analysis of Medicines Information enquiries help to determine whether there is a need for a screening tool for women of child bearing age in outpatient clinics? 11.Why do patients under the care of the Royal Eye Hospital contact the Medicines Helpline?

UKMI 38th Professional Development Seminar 2012 Poster ... · UKMI 38th Professional Development Seminar 2012 Poster collation ... [email protected] ... the medical unit
May 25, 2018
Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript
UKMI 38th Professional Development Seminar 2012
Poster collation
7. MiDatabank ADR reporting – One year on
8. Identification of hospital-specific quality signals (QSig) using
documented enquiries to the drug information center (DIC) of the
pharmacy.
9. Improving patient perception on the provision of medicines
Information
10. Could analysis of Medicines Information enquiries help to determine
whether there is a need for a screening tool for women of child
bearing age in outpatient clinics?
11.Why do patients under the care of the Royal Eye Hospital contact the
Medicines Helpline?
MiDatabank ADR reporting
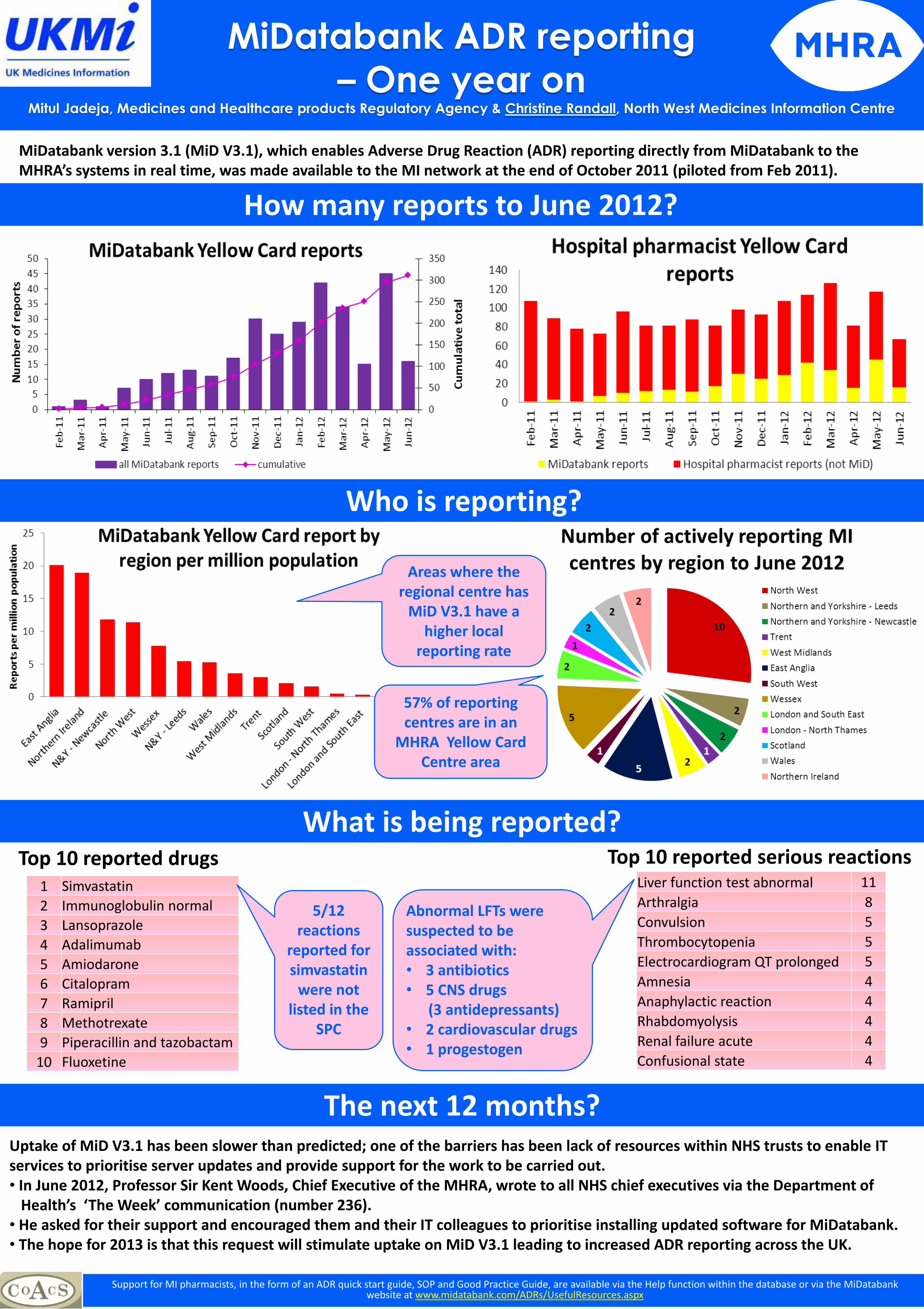
– One year on Mitul Jadeja, Medicines and Healthcare products Regulatory Agency & Christine Randall, North West Medicines Information Centre
MiDatabank version 3.1 (MiD V3.1), which enables Adverse Drug Reaction (ADR) reporting directly from MiDatabank to the MHRA’s systems in real time, was made available to the MI network at the end of October 2011 (piloted from Feb 2011).
Uptake of MiD V3.1 has been slower than predicted; one of the barriers has been lack of resources within NHS trusts to enable IT services to prioritise server updates and provide support for the work to be carried out. • In June 2012, Professor Sir Kent Woods, Chief Executive of the MHRA, wrote to all NHS chief executives via the Department of Health’s ‘The Week’ communication (number 236). • He asked for their support and encouraged them and their IT colleagues to prioritise installing updated software for MiDatabank. • The hope for 2013 is that this request will stimulate uptake on MiD V3.1 leading to increased ADR reporting across the UK.
How many reports to June 2012?
Who is reporting?
What is being reported? Top 10 reported drugs Top 10 reported serious reactions
1 Simvastatin
2 Immunoglobulin normal
3 Lansoprazole
4 Adalimumab
5 Amiodarone
6 Citalopram
7 Ramipril
8 Methotrexate
9 Piperacillin and tazobactam
10 Fluoxetine
Support for MI pharmacists, in the form of an ADR quick start guide, SOP and Good Practice Guide, are available via the Help function within the database or via the MiDatabank website at www.midatabank.com/ADRs/UsefulResources.aspx
5/12
reactions reported for simvastatin
were not listed in the
SPC
Liver function test abnormal 11
Arthralgia 8
Convulsion 5
Thrombocytopenia 5
Electrocardiogram QT prolonged 5
Amnesia 4
Anaphylactic reaction 4
Rhabdomyolysis 4
Renal failure acute 4
Confusional state 4
The next 12 months?
Abnormal LFTs were suspected to be associated with: • 3 antibiotics • 5 CNS drugs (3 antidepressants) • 2 cardiovascular drugs • 1 progestogen
57% of reporting centres are in an
MHRA Yellow Card Centre area
Areas where the regional centre has
MiD V3.1 have a higher local
reporting rate
CAMPUS GROSSHADERNCAMPUS GROSSHADERNCAMPUS GROSSHADERNCAMPUS GROSSHADERN
APOTHEKE APOTHEKE APOTHEKE APOTHEKE ---- ARZNEIMITTELINFORMATIONARZNEIMITTELINFORMATIONARZNEIMITTELINFORMATIONARZNEIMITTELINFORMATION
Table 5: Examples DIC Intranet Information Platform
excerpt of DIC intranet information platform
excerpt from intranet table: administration of oral medication excerpt from intranet table: administration of i.v. antiinfectives
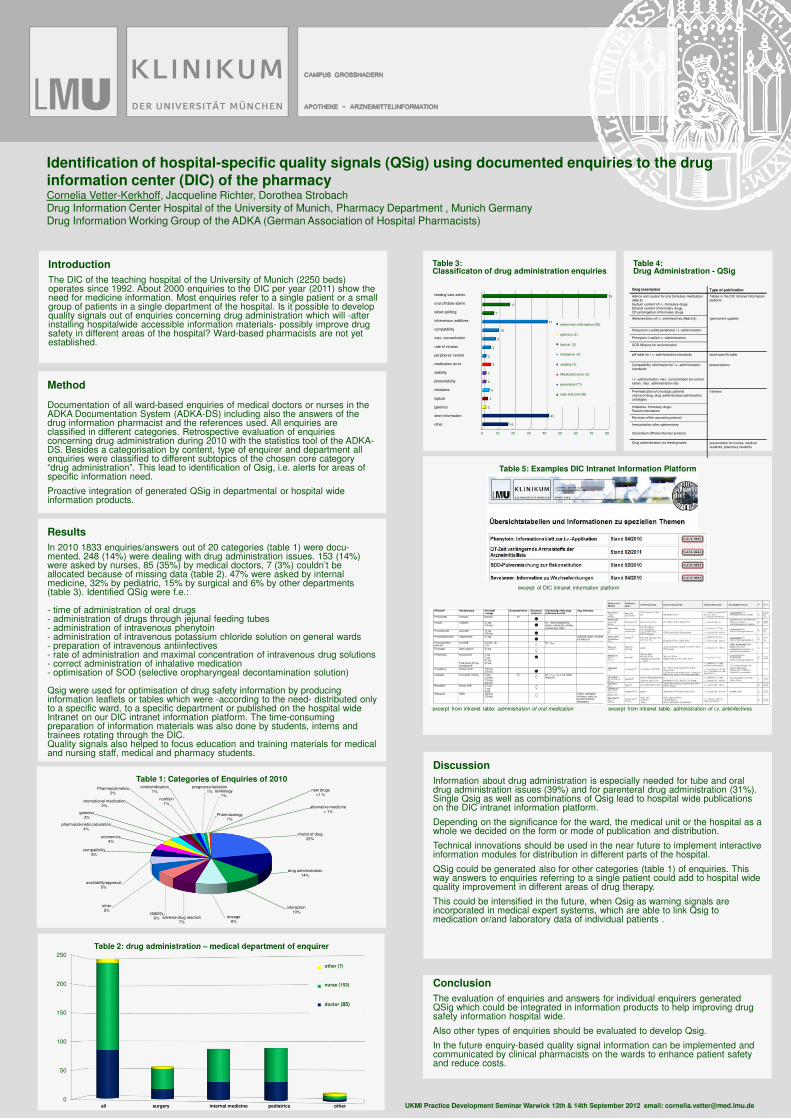
Method
Documentation of all ward-based enquiries of medical doctors or nurses in the ADKA Documentation System (ADKA-DS) including also the answers of the drug information pharmacist and the references used. All enquiries are classified in different categories. Retrospective evaluation of enquiries concerning drug administration during 2010 with the statistics tool of the ADKA-DS. Besides a categorisation by content, type of enquirer and department all enquiries were classified to different subtopics of the chosen core category “drug administration”. This lead to identification of Qsig, i.e. alerts for areas of specific information need.
Proactive integration of generated QSig in departmental or hospital wide information products.
Identification of hospital-specific quality signals (QSig) using documented enquiries to the drug information center (DIC) of the pharmacyCornelia Vetter-Kerkhoff, Jacqueline Richter, Dorothea Strobach Drug Information Center Hospital of the University of Munich, Pharmacy Department , Munich Germany Drug Information Working Group of the ADKA (German Association of Hospital Pharmacists)
UKMI Practice Development Seminar Warwick 13th & 14th September 2012 email: [email protected]
Results
In 2010 1833 enquiries/answers out of 20 categories (table 1) were docu-mented. 248 (14%) were dealing with drug administration issues. 153 (14%) were asked by nurses, 85 (35%) by medical doctors, 7 (3%) couldn’t be allocated because of missing data (table 2). 47% were asked by internal medicine, 32% by pediatric, 15% by surgical and 6% by other departments (table 3). Identified QSig were f.e.:
- time of administration of oral drugs- administration of drugs through jejunal feeding tubes- administration of intravenous phenytoin- administration of intravenous potassium chloride solution on general wards- preparation of intravenous antiinfectives- rate of administration and maximal concentration of intravenous drug solutions- correct administration of inhalative medication- optimisation of SOD (selective oropharyngeal decontamination solution)
Qsig were used for optimisation of drug safety information by producing information leaflets or tables which were -according to the need- distributed only to a specific ward, to a specific department or published on the hospital wide Intranet on our DIC intranet information platform. The time-consuming preparation of information materials was also done by students, interns and trainees rotating through the DIC.Quality signals also helped to focus education and training materials for medical and nursing staff, medical and pharmacy students.
Introduction
The DIC of the teaching hospital of the University of Munich (2250 beds) operates since 1992. About 2000 enquiries to the DIC per year (2011) show the need for medicine information. Most enquiries refer to a single patient or a small group of patients in a single department of the hospital. Is it possible to develop quality signals out of enquiries concerning drug administration which will -after installing hospitalwide accessible information materials- possibly improve drug safety in different areas of the hospital? Ward-based pharmacists are not yet established.
Discussion
Information about drug administration is especially needed for tube and oral drug administration issues (39%) and for parenteral drug administration (31%). Single Qsig as well as combinations of Qsig lead to hospital wide publicationson the DIC intranet information platform.
Depending on the significance for the ward, the medical unit or the hospital as a whole we decided on the form or mode of publication and distribution.
Technical innovations should be used in the near future to implement interactiveinformation modules for distribution in different parts of the hospital.
QSig could be generated also for other categories (table 1) of enquiries. This way answers to enquiries referring to a single patient could add to hospital widequality improvement in different areas of drug therapy.
This could be intensified in the future, when Qsig as warning signals areincorporated in medical expert systems, which are able to link Qsig to medication or/and laboratory data of individual patients .
Conclusion
The evaluation of enquiries and answers for individual enquirers generated QSig which could be integrated in information products to help improving drug safety information hospital wide.
Also other types of enquiries should be evaluated to develop Qsig.
In the future enquiry-based quality signal information can be implemented and communicated by clinical pharmacists on the wards to enhance patient safety and reduce costs.
Table 2: drug administration – medical department of enquirer
Table 1: Categories of Enquiries of 2010
Table 4: Drug Administration - QSig
Table 3: Classificaton of drug administration enquiries
0
50
100
150
200
250
Sonstige (7)
Pflege (153)
Arzt (85)
all surgery internal medicine pediatrics other
choice of drug22%
drug administration14%
interaction10%
dosage8%
adverse drug reaction7%
stability6%
other5%
availability/approval5%
compatibility5%
economics4%
pharmacokinetic calculation4%
galenics3%
international medication2%
Pharmacokinetics2%
nutrition1%
contraindication1%
pregnancy/lactation1% toxikology
1%
Pharmacology1%
new drugs<1 %
alternative medicine< 1%
0 10 20 30 40 50 60 70 80
16
42
2
3
4
2
2
5
2
5
8
10
41
7
17
79
Kurzinformation
Galenik
Topika
Inhalativa
Lichtschutz
Medikationsfehler/CIRS
peripher/zentral
Teilbarkeit
feeding tube admin.
oral off lable admin.
tablet splitting
intravenous additives
compatibility
max. concentration
rate of infusion
peripheral/ central
medication error
stability
photostability
inhalative
topical
galenics
short information
other
other/short information (58)
galenics (2)
topical (3)
Inhalative (4)
stability (4)
Medication error (5)
parenteral (71)
tube and oral (96)
Qsig (examples) Type of publication
Advice and caution for oral formulary medication(Abb.5)Sodium content of i.v.-formulary drugsEthanol content of formulary drugsQT-prolongation of formulary drugs
Tables in the DIC intranet informationplatform
Administration of i.v. antiinfectives (Abb.5,6) (permanent update)
Potassium: Leaflet peripheral i.v.-adminstration
Phenytoin: Leaflet i.v.-administration
SOD-Mixture for reconstitution
pH-table for i.v.-administration standards ward-specific table
Compatibility information for i.v.-administration standards
presentations
i.v.-administration, max. concentration for centrallumen, max. administration rate
Premedication of oncologic patientschoice of drug, drug administration optimisationstrategies
trainees
Inhalative formulary drugs: Patient information
Revision of the mucositis protocol
Immunisation after splenectomy
Clostridium difficile infection protocol
Drug administration via feeding tubes presentation for nurses, medicalstudents, pharmacy students
other (7)
nurse (153)
doctor (85)
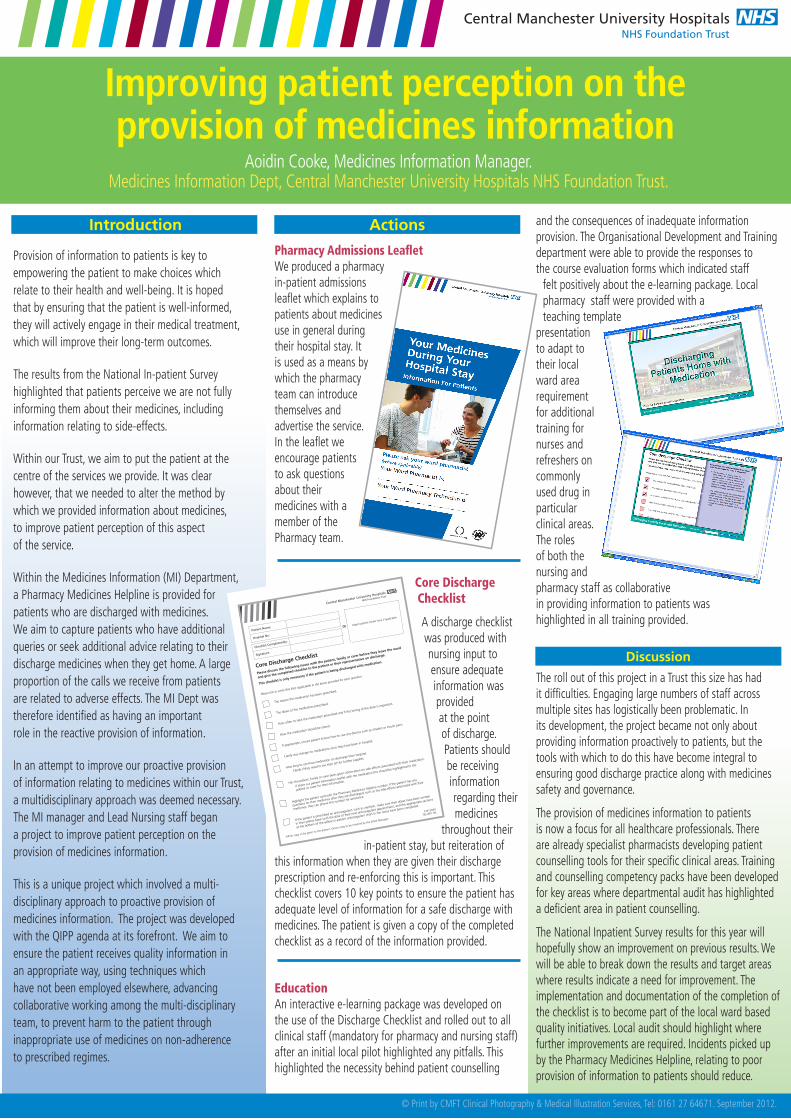
Central Manchester University HospitalsNHS Foundation Trust
Improving patient perception on the provision of medicines information
Aoidin Cooke, Medicines Information Manager. Medicines Information Dept, Central Manchester University Hospitals NHS Foundation Trust.
© Print by CMFT Clinical Photography & Medical Illustration Services, Tel: 0161 27 64671. September 2012.
Introduction
Provision of information to patients is key to empowering the patient to make choices which relate to their health and well-being. It is hoped that by ensuring that the patient is well-informed, they will actively engage in their medical treatment, which will improve their long-term outcomes.
The results from the National In-patient Survey highlighted that patients perceive we are not fully informing them about their medicines, including information relating to side-effects.
Within our Trust, we aim to put the patient at the centre of the services we provide. It was clear however, that we needed to alter the method by which we provided information about medicines, to improve patient perception of this aspect of the service.
Within the Medicines Information (MI) Department, a Pharmacy Medicines Helpline is provided for patients who are discharged with medicines. We aim to capture patients who have additional queries or seek additional advice relating to their discharge medicines when they get home. A large proportion of the calls we receive from patients are related to adverse effects. The MI Dept was therefore identified as having an important role in the reactive provision of information.
In an attempt to improve our proactive provision of information relating to medicines within our Trust, a multidisciplinary approach was deemed necessary. The MI manager and Lead Nursing staff began a project to improve patient perception on the provision of medicines information.
This is a unique project which involved a multi-disciplinary approach to proactive provision of medicines information. The project was developed with the QIPP agenda at its forefront. We aim to ensure the patient receives quality information in an appropriate way, using techniques which have not been employed elsewhere, advancing collaborative working among the multi-disciplinary team, to prevent harm to the patient through inappropriate use of medicines on non-adherence to prescribed regimes.
Actions
Pharmacy Admissions LeafletWe produced a pharmacy in-patient admissions leaflet which explains to patients about medicines use in general during their hospital stay. It is used as a means by which the pharmacy team can introduce themselves and advertise the service. In the leaflet we encourage patients to ask questions about their medicines with a member of the Pharmacy team.
Core Discharge Checklist
A discharge checklist was produced with nursing input to ensure adequate information was provided at the point of discharge. Patients should be receiving information regarding their medicines
throughout their in-patient stay, but reiteration of
this information when they are given their discharge prescription and re-enforcing this is important. This checklist covers 10 key points to ensure the patient has adequate level of information for a safe discharge with medicines. The patient is given a copy of the completed checklist as a record of the information provided.
EducationAn interactive e-learning package was developed on the use of the Discharge Checklist and rolled out to all clinical staff (mandatory for pharmacy and nursing staff) after an initial local pilot highlighted any pitfalls. This highlighted the necessity behind patient counselling
and the consequences of inadequate information provision. The Organisational Development and Training department were able to provide the responses to the course evaluation forms which indicated staff
felt positively about the e-learning package. Local pharmacy staff were provided with a teaching template
presentation to adapt to their local ward area requirement for additional training for nurses and refreshers on commonly used drug in particular clinical areas. The roles of both the nursing and pharmacy staff as collaborative in providing information to patients was highlighted in all training provided.
Discussion
The roll out of this project in a Trust this size has had it difficulties. Engaging large numbers of staff across multiple sites has logistically been problematic. In its development, the project became not only about providing information proactively to patients, but the tools with which to do this have become integral to ensuring good discharge practice along with medicines safety and governance.
The provision of medicines information to patients is now a focus for all healthcare professionals. There are already specialist pharmacists developing patient counselling tools for their specific clinical areas. Training and counselling competency packs have been developed for key areas where departmental audit has highlighted a deficient area in patient counselling.
The National Inpatient Survey results for this year will hopefully show an improvement on previous results. We will be able to break down the results and target areas where results indicate a need for improvement. The implementation and documentation of the completion of the checklist is to become part of the local ward based quality initiatives. Local audit should highlight where further improvements are required. Incidents picked up by the Pharmacy Medicines Helpline, relating to poor provision of information to patients should reduce.
Central Manchester University Hospitals
NHS Foundation Trust
Could analysis of Medicines Information enquiries help to
determine whether there is a need for a screening tool for
women of child bearing age in outpatient clinics?By Laura Smith, Pre-registration Pharmacist. Supervisor: Charlotte Hay, Medicines Information Pharmacist.
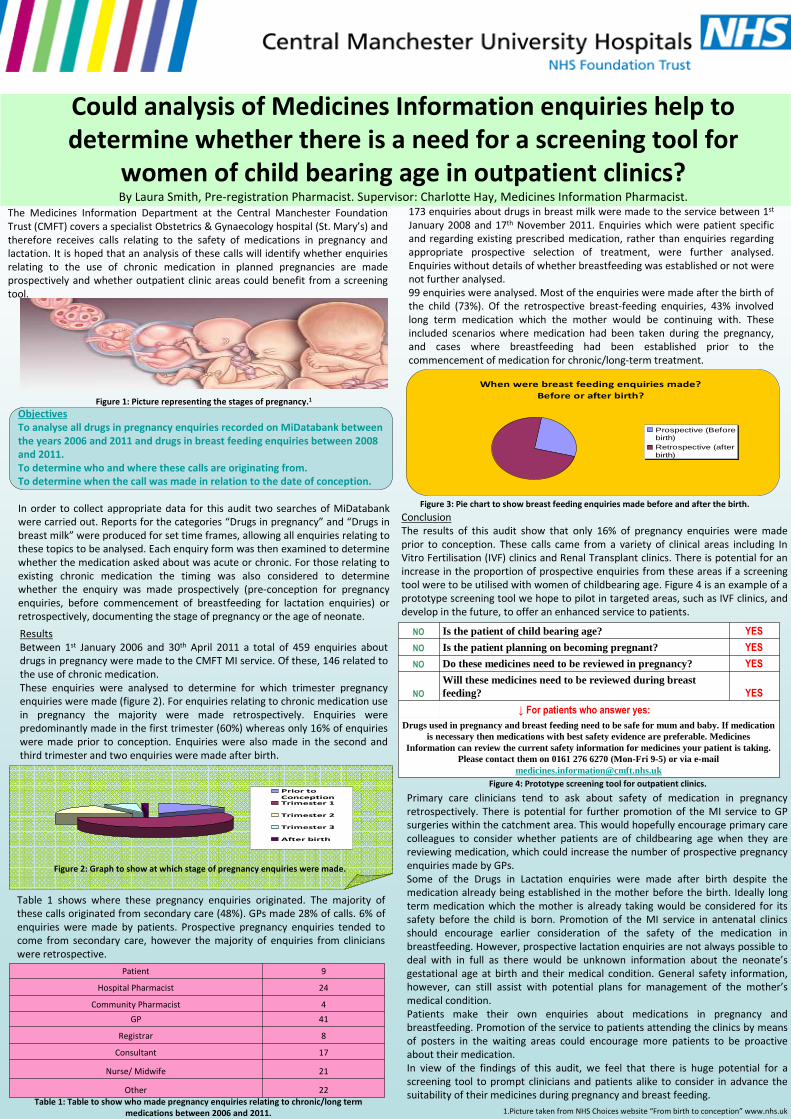
Results
Between 1st January 2006 and 30th April 2011 a total of 459 enquiries about
drugs in pregnancy were made to the CMFT MI service. Of these, 146 related to
the use of chronic medication.
These enquiries were analysed to determine for which trimester pregnancy
enquiries were made (figure 2). For enquiries relating to chronic medication use
in pregnancy the majority were made retrospectively. Enquiries were
predominantly made in the first trimester (60%) whereas only 16% of enquiries
were made prior to conception. Enquiries were also made in the second and
third trimester and two enquiries were made after birth.
173 enquiries about drugs in breast milk were made to the service between 1st
January 2008 and 17th November 2011. Enquiries which were patient specific
and regarding existing prescribed medication, rather than enquiries regarding
appropriate prospective selection of treatment, were further analysed.
Enquiries without details of whether breastfeeding was established or not were
not further analysed.
99 enquiries were analysed. Most of the enquiries were made after the birth of
the child (73%). Of the retrospective breast-feeding enquiries, 43% involved
long term medication which the mother would be continuing with. These
included scenarios where medication had been taken during the pregnancy,
and cases where breastfeeding had been established prior to the
commencement of medication for chronic/long-term treatment.
The Medicines Information Department at the Central Manchester Foundation
Trust (CMFT) covers a specialist Obstetrics & Gynaecology hospital (St. Mary’s) and
therefore receives calls relating to the safety of medications in pregnancy and
lactation. It is hoped that an analysis of these calls will identify whether enquiries
relating to the use of chronic medication in planned pregnancies are made
prospectively and whether outpatient clinic areas could benefit from a screening
tool.
Figure 1: Picture representing the stages of pregnancy.1
Objectives
To analyse all drugs in pregnancy enquiries recorded on MiDatabank between
the years 2006 and 2011 and drugs in breast feeding enquiries between 2008
and 2011.
To determine who and where these calls are originating from.
To determine when the call was made in relation to the date of conception.
In order to collect appropriate data for this audit two searches of MiDatabank
were carried out. Reports for the categories “Drugs in pregnancy” and “Drugs in
breast milk” were produced for set time frames, allowing all enquiries relating to
these topics to be analysed. Each enquiry form was then examined to determine
whether the medication asked about was acute or chronic. For those relating to
existing chronic medication the timing was also considered to determine
whether the enquiry was made prospectively (pre-conception for pregnancy
enquiries, before commencement of breastfeeding for lactation enquiries) or
retrospectively, documenting the stage of pregnancy or the age of neonate.
Conclusion
The results of this audit show that only 16% of pregnancy enquiries were made
prior to conception. These calls came from a variety of clinical areas including In
Vitro Fertilisation (IVF) clinics and Renal Transplant clinics. There is potential for an
increase in the proportion of prospective enquiries from these areas if a screening
tool were to be utilised with women of childbearing age. Figure 4 is an example of a
prototype screening tool we hope to pilot in targeted areas, such as IVF clinics, and
develop in the future, to offer an enhanced service to patients.
Drugs used in pregnancy and breast feeding need to be safe for mum and baby. If medication is necessary then medications with best safety evidence are preferable. Medicines
Information can review the current safety information for medicines your patient is taking. Please contact them on 0161 276 6270 (Mon-Fri 9-5) or via e-mail
↓ For patients who answer yes:
YES
Will these medicines need to be reviewed during breast feeding? NO
YESDo these medicines need to be reviewed in pregnancy? NO
YESIs the patient planning on becoming pregnant? NO
YESIs the patient of child bearing age?NO
Prior to
ConceptionTrimester 1
Trimester 2
Trimester 3
After birth
Figure 2: Graph to show at which stage of pregnancy enquiries were made.
Table 1: Table to show who made pregnancy enquiries relating to chronic/long term
medications between 2006 and 2011. 1.Picture taken from NHS Choices website “From birth to conception” www.nhs.uk
When were breast feeding enquiries made?
Before or after birth?
Prospective (Beforebirth)Retrospective (afterbirth)
Figure 3: Pie chart to show breast feeding enquiries made before and after the birth.
Figure 4: Prototype screening tool for outpatient clinics.
22Other
21Nurse/ Midwife
17Consultant
8Registrar
41GP
4Community Pharmacist
24Hospital Pharmacist
9Patient
Table 1 shows where these pregnancy enquiries originated. The majority of
these calls originated from secondary care (48%). GPs made 28% of calls. 6% of
enquiries were made by patients. Prospective pregnancy enquiries tended to
come from secondary care, however the majority of enquiries from clinicians
were retrospective.
Primary care clinicians tend to ask about safety of medication in pregnancy
retrospectively. There is potential for further promotion of the MI service to GP
surgeries within the catchment area. This would hopefully encourage primary care
colleagues to consider whether patients are of childbearing age when they are
reviewing medication, which could increase the number of prospective pregnancy
enquiries made by GPs.
Some of the Drugs in Lactation enquiries were made after birth despite the
medication already being established in the mother before the birth. Ideally long
term medication which the mother is already taking would be considered for its
safety before the child is born. Promotion of the MI service in antenatal clinics
should encourage earlier consideration of the safety of the medication in
breastfeeding. However, prospective lactation enquiries are not always possible to
deal with in full as there would be unknown information about the neonate’s
gestational age at birth and their medical condition. General safety information,
however, can still assist with potential plans for management of the mother’s
medical condition.
Patients make their own enquiries about medications in pregnancy and
breastfeeding. Promotion of the service to patients attending the clinics by means
of posters in the waiting areas could encourage more patients to be proactive
about their medication.
In view of the findings of this audit, we feel that there is huge potential for a
screening tool to prompt clinicians and patients alike to consider in advance the
suitability of their medicines during pregnancy and breast feeding.
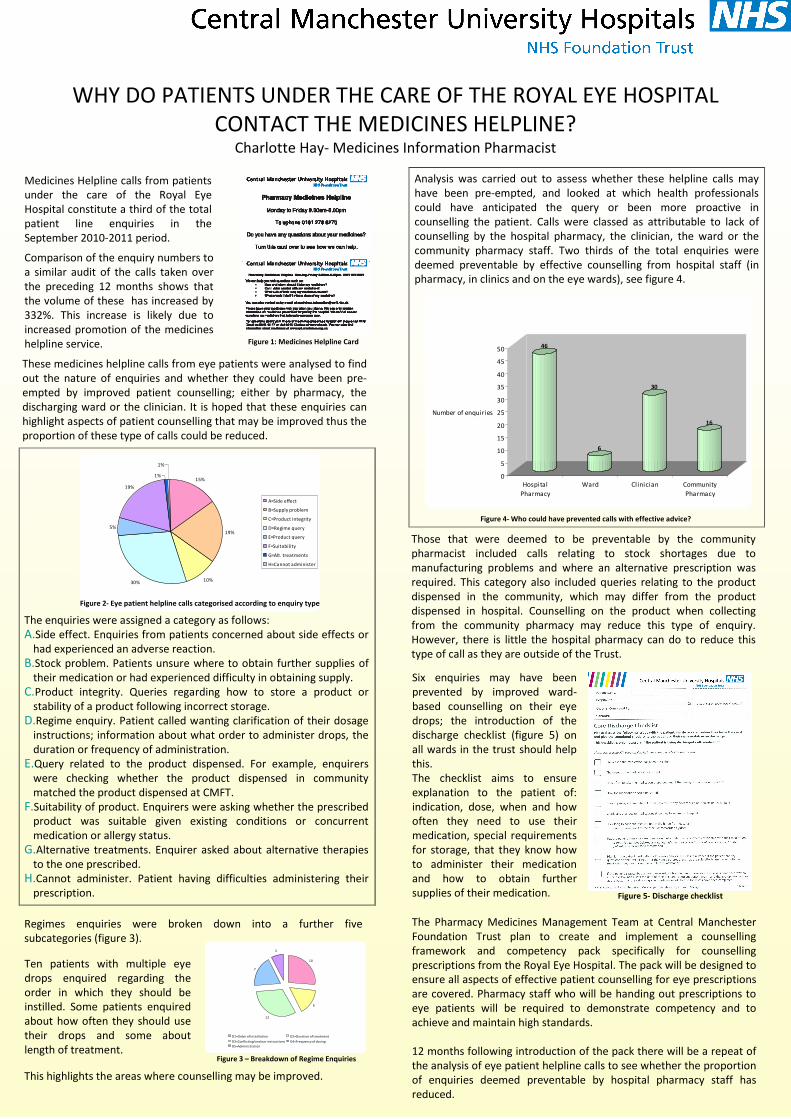
WHY DO PATIENTS UNDER THE CARE OF THE ROYAL EYE HOSPITAL
CONTACT THE MEDICINES HELPLINE?Charlotte Hay- Medicines Information Pharmacist
Medicines Helpline calls from patients
under the care of the Royal Eye
Hospital constitute a third of the total
patient line enquiries in the
September 2010-2011 period.
The enquiries were assigned a category as follows:
A.Side effect. Enquiries from patients concerned about side effects or
had experienced an adverse reaction.
B.Stock problem. Patients unsure where to obtain further supplies of
their medication or had experienced difficulty in obtaining supply.
C.Product integrity. Queries regarding how to store a product or
stability of a product following incorrect storage.
D.Regime enquiry. Patient called wanting clarification of their dosage
instructions; information about what order to administer drops, the
duration or frequency of administration.
E.Query related to the product dispensed. For example, enquirers
were checking whether the product dispensed in community
matched the product dispensed at CMFT.
F.Suitability of product. Enquirers were asking whether the prescribed
product was suitable given existing conditions or concurrent
medication or allergy status.
G.Alternative treatments. Enquirer asked about alternative therapies
to the one prescribed.
H.Cannot administer. Patient having difficulties administering their
prescription.
15%
19%
10%30%
5%
19%
1%
1%
A=Side effect
B=Supply problem
C=Product integrity
D=Regime query
E=Product query
F=Suitability
G=Alt. treatments
H=Cannot administer
Figure 2- Eye patient helpline calls categorised according to enquiry type
Analysis was carried out to assess whether these helpline calls may
have been pre-empted, and looked at which health professionals
could have anticipated the query or been more proactive in
counselling the patient. Calls were classed as attributable to lack of
counselling by the hospital pharmacy, the clinician, the ward or the
community pharmacy staff. Two thirds of the total enquiries were
deemed preventable by effective counselling from hospital staff (in
pharmacy, in clinics and on the eye wards), see figure 4.
Those that were deemed to be preventable by the community
pharmacist included calls relating to stock shortages due to
manufacturing problems and where an alternative prescription was
required. This category also included queries relating to the product
dispensed in the community, which may differ from the product
dispensed in hospital. Counselling on the product when collecting
from the community pharmacy may reduce this type of enquiry.
However, there is little the hospital pharmacy can do to reduce this
type of call as they are outside of the Trust.
The Pharmacy Medicines Management Team at Central Manchester
Foundation Trust plan to create and implement a counselling
framework and competency pack specifically for counselling
prescriptions from the Royal Eye Hospital. The pack will be designed to
ensure all aspects of effective patient counselling for eye prescriptions
are covered. Pharmacy staff who will be handing out prescriptions to
eye patients will be required to demonstrate competency and to
achieve and maintain high standards.
12 months following introduction of the pack there will be a repeat of
the analysis of eye patient helpline calls to see whether the proportion
of enquiries deemed preventable by hospital pharmacy staff has
reduced.
Figure 5- Discharge checklist
This highlights the areas where counselling may be improved.
These medicines helpline calls from eye patients were analysed to find
out the nature of enquiries and whether they could have been pre-
empted by improved patient counselling; either by pharmacy, the
discharging ward or the clinician. It is hoped that these enquiries can
highlight aspects of patient counselling that may be improved thus the
proportion of these type of calls could be reduced.
Comparison of the enquiry numbers to
a similar audit of the calls taken over
the preceding 12 months shows that
the volume of these has increased by
332%. This increase is likely due to
increased promotion of the medicines
helpline service. Figure 1: Medicines Helpline Card
Figure 3 – Breakdown of Regime Enquiries
Ten patients with multiple eye
drops enquired regarding the
order in which they should be
instilled. Some patients enquired
about how often they should use
their drops and some about
length of treatment.
Regimes enquiries were broken down into a further five
subcategories (figure 3).
46
6
30
16
0
5
10
15
20
25
30
35
40
45
50
Number of enquiries
Hospital
Pharmacy
Ward Clinician Community
Pharmacy
Figure 4- Who could have prevented calls with effective advice?
Six enquiries may have been
prevented by improved ward-
based counselling on their eye
drops; the introduction of the
discharge checklist (figure 5) on
all wards in the trust should help
this.
The checklist aims to ensure
explanation to the patient of:
indication, dose, when and how
often they need to use their
medication, special requirements
for storage, that they know how
to administer their medication
and how to obtain further
supplies of their medication.
10
6
12
7
3
D1=Order of installation D2=Duration of treatment
D3=Conflicting/unclear instructions D4=Frequency of dosing
D5=Administration
Related Documents











