U N I V E R S I T Ä T S M E D I Z I N B E R L I N Goal directed perioperative monitoring Univ.-Prof. Dr. Michael Sander Klinik für Anästhesiologie mit Schwerpunkt operative Intensivmedizin Campus Charité Mitte, Campus Virchow-Klinikum Charité - Universitätsmedizin Berlin

U N I V E R S I T Ä T S M E D I Z I N B E R L I N Goal directed perioperative monitoring Univ.-Prof. Dr. Michael Sander Klinik für Anästhesiologie mit.
Dec 17, 2015
Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

U N I V E R S I T Ä T S M E D I Z I N B E R L I N
Goal directed perioperative monitoring
Univ.-Prof. Dr. Michael Sander
Klinik für Anästhesiologie mit Schwerpunkt operative IntensivmedizinCampus Charité Mitte, Campus Virchow-Klinikum
Charité - Universitätsmedizin Berlin
Disclosure
Research grants or royalties for lectures:
Edwards Life Science Fresenius Medical The Medicines Company Pulsion Medical Systems

Educational objective
Goal-directed perioperative monitoring – Why?– Who?– What?
– How?
AGENDA Risks in the OR
Parameters– Blood pressure– Venous saturation– Dynamic parameters of circulation
Conclusion
4

Old people – a challenge for the futureJeanne Louise Calment * February, 21th 1875 in Arles, France; † August, 4th 1997
5
Old people – a challenge for the futureJeanne Louise Calment * February, 21th 1875 in Arles, France; † August, 4th 1997
6
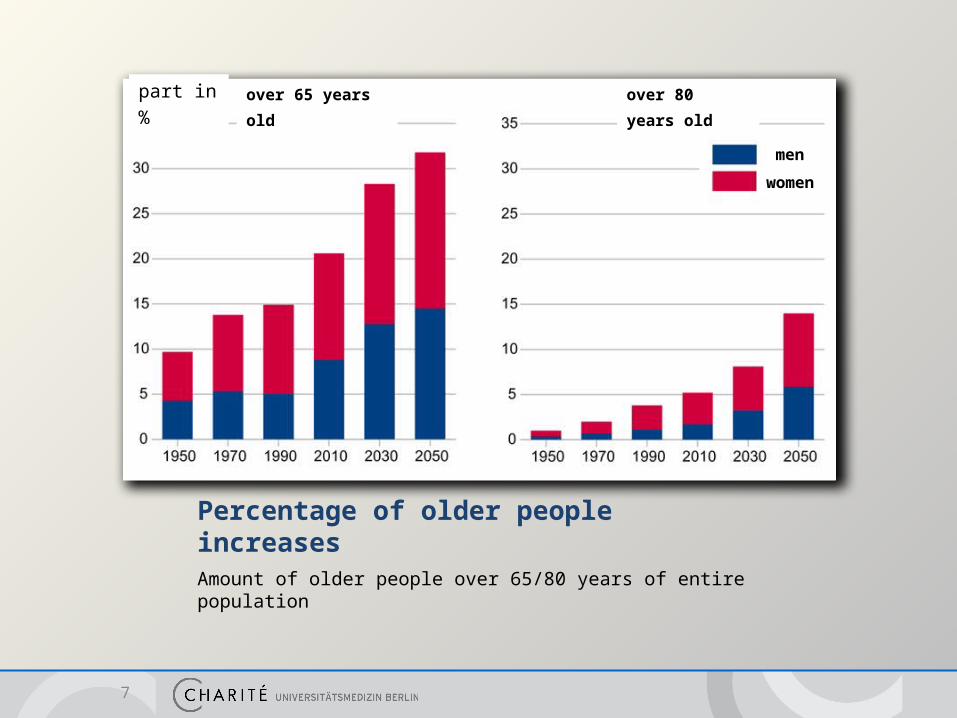
Percentage of older people increases Amount of older people over 65/80 years of entire population
7
part in % over 65 years old over 80 years old
men
women

Demographic change- a challenge for the future -
8 Siewert, U. et al. (2010). Deutsches Ärzteblatt international, 107(18), 328–334.
2005 2020
Mecklenburg-Vorpommern Number of cases Number of cases Change
Prevalence
- Hypertension 618,855 650,858 + 5.2 % (+32,003)
- Diabetes 117,919 141,125 + 19.7 % (+23,206)
- Myocardial infarction 40,976 51,549 + 25.8 % (+10,573)
- Stroke 31,322 79,053 + 16.3 % (+5,100)
Incidence
- Colon carcinoma 728 936 + 28.6 % (+208)
- Cancer (all) 8,612 10,388 + 20.6 % (+1,776)

European Surgical Outcome Study
Results– Inclusion of 46.539 patients– 1.855 patients died
(in-hospital mortality 4%)
Conclusion– Strategies to minimise risk
Methods– 7 day cohort study– Time of recruitment: 4.4.2011
to 11.4.2011– Multi center study (498
centers in Europe) Patients
– Inclusion of all „non cardiac-surgery“ patients (elective and not elective)
Primary endpoint– hospital mortality (maximum
follow-up 60 days)
9 Pearse, R. et al. (2012). Lancet, 380(9847), 1059–1065.
Improving our care“Now, here, you see, it takes all the running you can do to keep in the same place. If you want to get somewhere else, you must run at least twice as fast as that!”

Patient safety- risk reduction strategy -
11
Risks on patient side:• Age• Pre-existing conditions • Heart and circulation• Anaemia• Genetic• ...
Risk in surgery:• Type of surgery• Blood loss• Emergency vs. elective• ...
Structural risk:• Checklists• Monitoring• Education• Standardized paths for treatments• SOP
individualgoal-directed therapy
Sander, M. (2013) Perioperatives Risiko. DIVI Jahrbuch 2012/2013ISBN: 978-3-941468-84-9
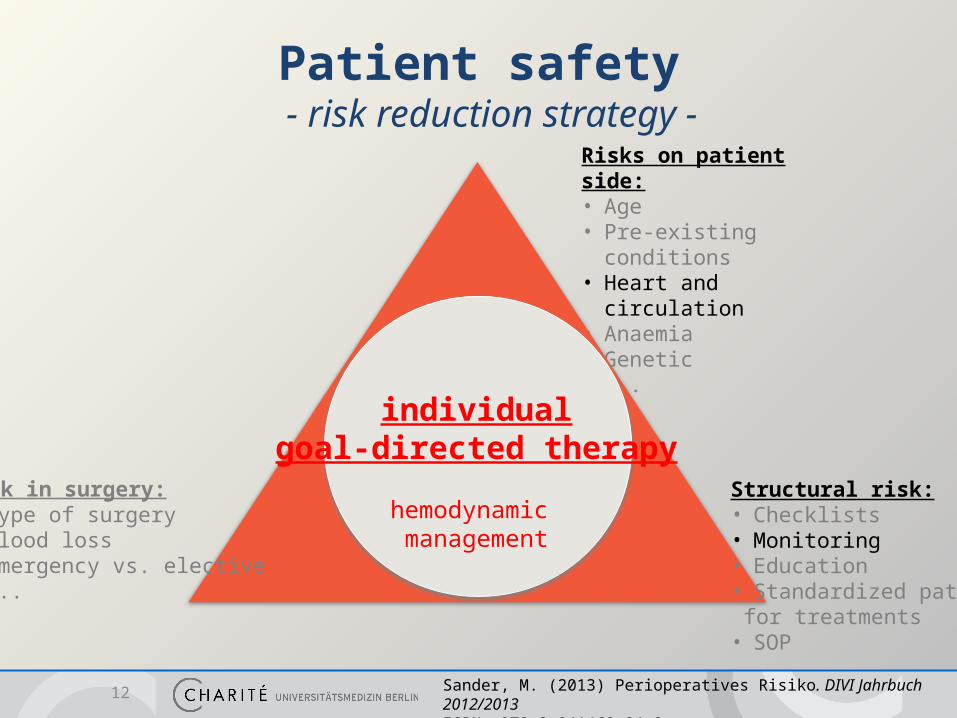
Patient safety- risk reduction strategy -
12
Risks on patient side:• Age• Pre-existing conditions • Heart and circulation• Anaemia• Genetic• ...
Risk in surgery:• Type of surgery• Blood loss• Emergency vs. elective• ...
Structural risk:• Checklists• Monitoring• Education• Standardized paths for treatments• SOP
individualgoal-directed therapy
hemodynamic management
Sander, M. (2013) Perioperatives Risiko. DIVI Jahrbuch 2012/2013ISBN: 978-3-941468-84-9

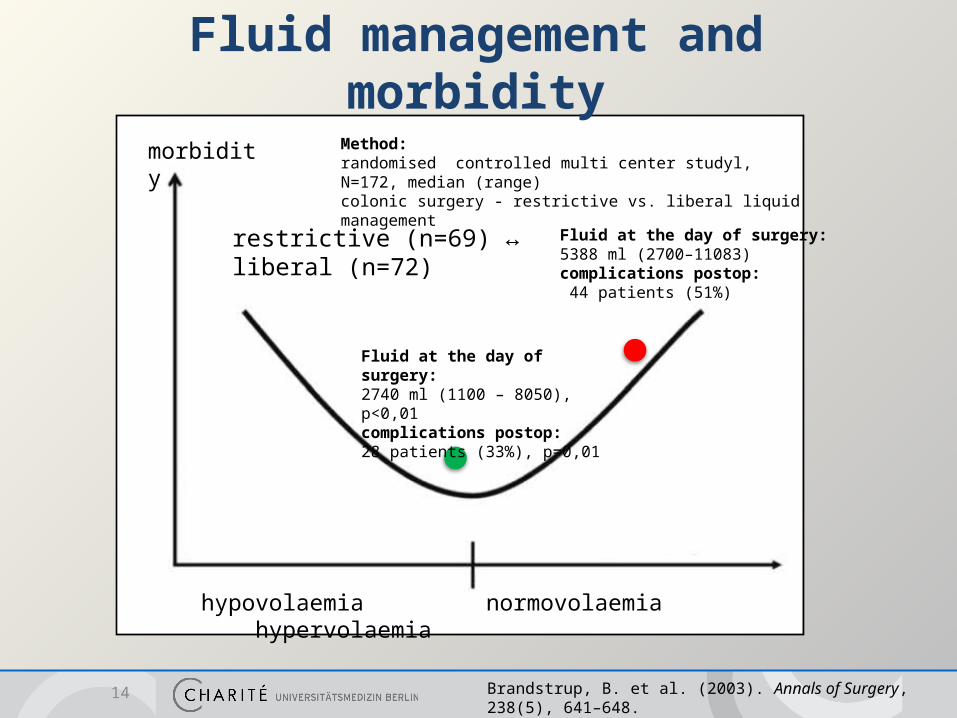
Fluid management and morbidity
morbidity
hypovolaemia normovolaemia hypervolaemia
Risks - Hypoperfusion- SIRS- Sepsis- MOV
Risks - Edema- Ileus- PONV- Pulmonary dysf.
Habicher, M., Sander, M. (2011). Journal of Cardiothoracic and Vascular Anesthesia, 25(6), 1141–1153.
13
morbidity
hypovolaemia normovolaemia hypervolaemia
Brandstrup, B. et al. (2003). Annals of Surgery, 238(5), 641–648.
Fluid at the day of surgery:2740 ml (1100 – 8050), p<0,01complications postop:28 patients (33%), p=0,01
Fluid at the day of surgery:5388 ml (2700–11083)complications postop: 44 patients (51%)
Method:randomised controlled multi center studyl, N=172, median (range) colonic surgery - restrictive vs. liberal liquid management
restrictive (n=69) ↔ liberal (n=72)
14
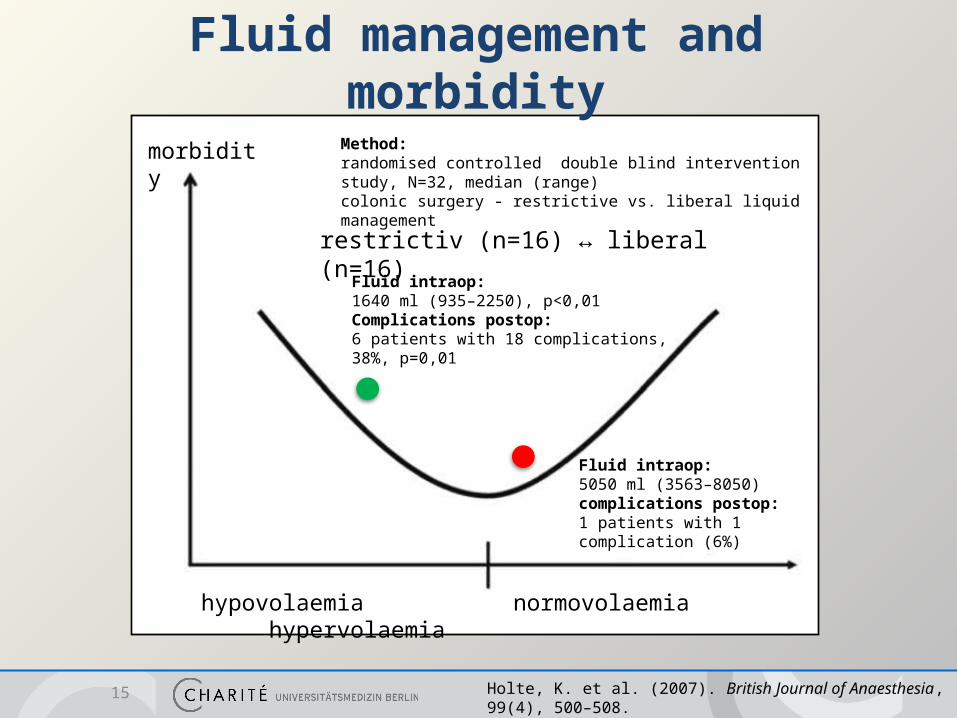
Fluid management and morbidity
morbidity
hypovolaemia normovolaemia hypervolaemia
Holte, K. et al. (2007). British Journal of Anaesthesia, 99(4), 500–508.
Fluid intraop:1640 ml (935–2250), p<0,01Complications postop:6 patients with 18 complications, 38%, p=0,01
Fluid intraop:5050 ml (3563–8050)complications postop:1 patients with 1 complication (6%)
Method:randomised controlled double blind intervention study, N=32, median (range) colonic surgery - restrictive vs. liberal liquid management
restrictiv (n=16) ↔ liberal (n=16)
15
Fluid management and morbidity

Individualized hemodynamic goal-directed therapy
morbidity
hypovolaemia normovolaemia hypervolaemia
individualized hemodynamic management
restrictive ↔ liberal
Habicher, M., Sander, M. (2011). Journal of Cardiothoracic and Vascular Anesthesia, 25(6), 1141–1153.
pre-existing conditionTyp of intervention
Preop loss of bloodPreop preload
Epidural anaesthesia...
16

Classics
17
Supranormal DO2
18 Shoemaker et al. Role of oxygen debt in the development of organ failure sepsis, and death in high-risk surgical patients. Chest (1992) vol. 102 (1) pp. 208-15
Adequate oxygen suply
consumption
supply
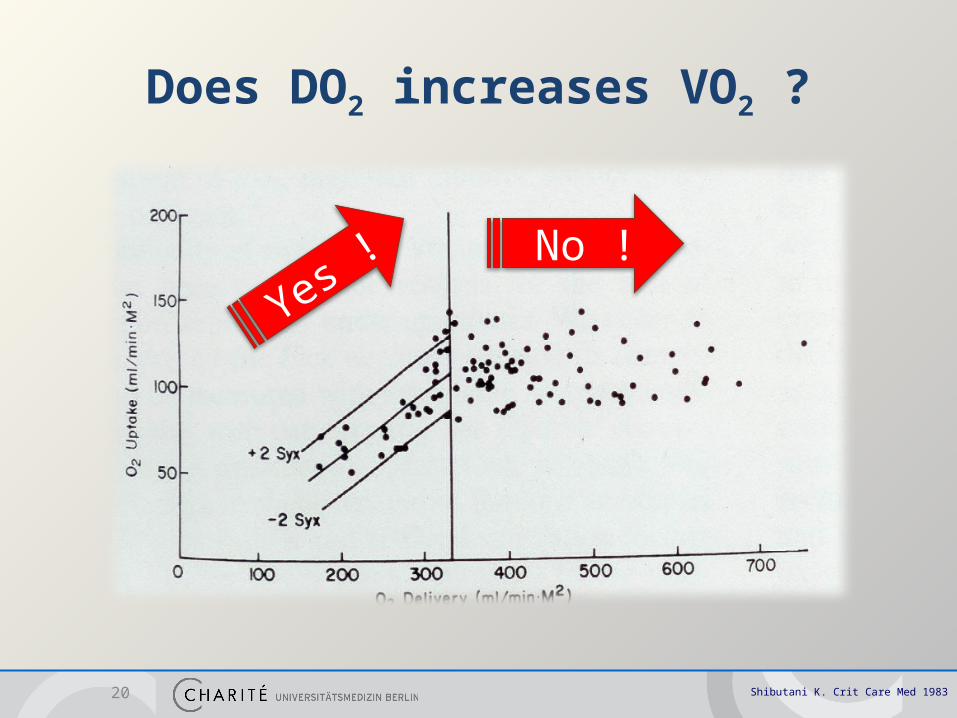
Does DO2 increases VO2 ?
20 Shibutani K. Crit Care Med 1983
Yes !No !
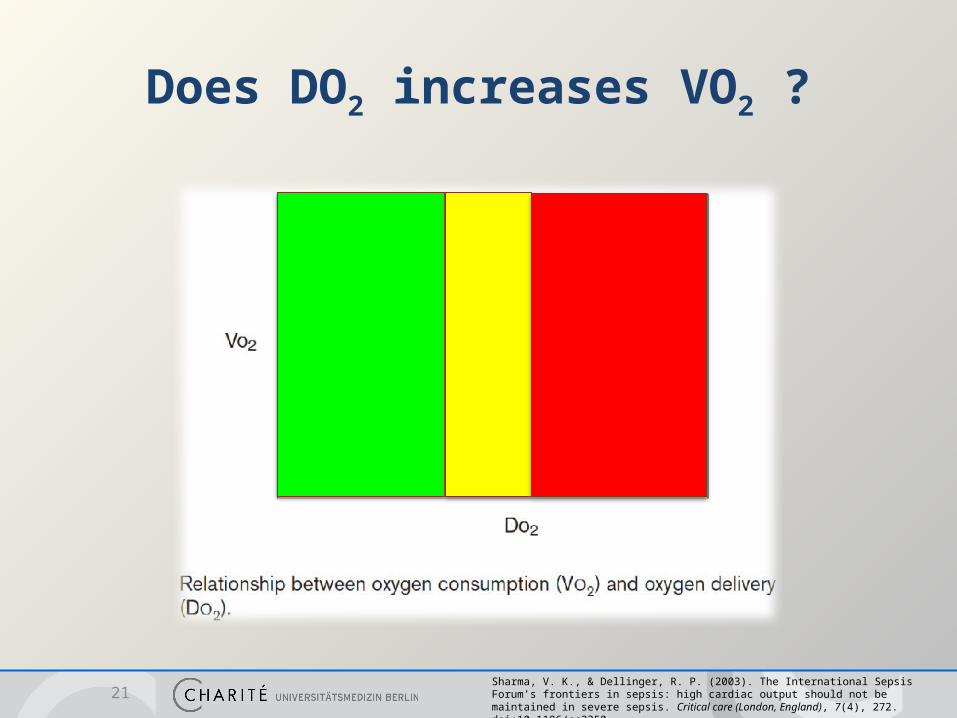
Does DO2 increases VO2 ?
21Sharma, V. K., & Dellinger, R. P. (2003). The International Sepsis Forum’s frontiers in sepsis: high cardiac output should not be maintained in severe sepsis. Critical care (London, England), 7(4), 272. doi:10.1186/cc2350

Oxygen supply: DO2 simplified fomula =
DO2 = CO X (Hgb X 1.34 X Sa02) X 10
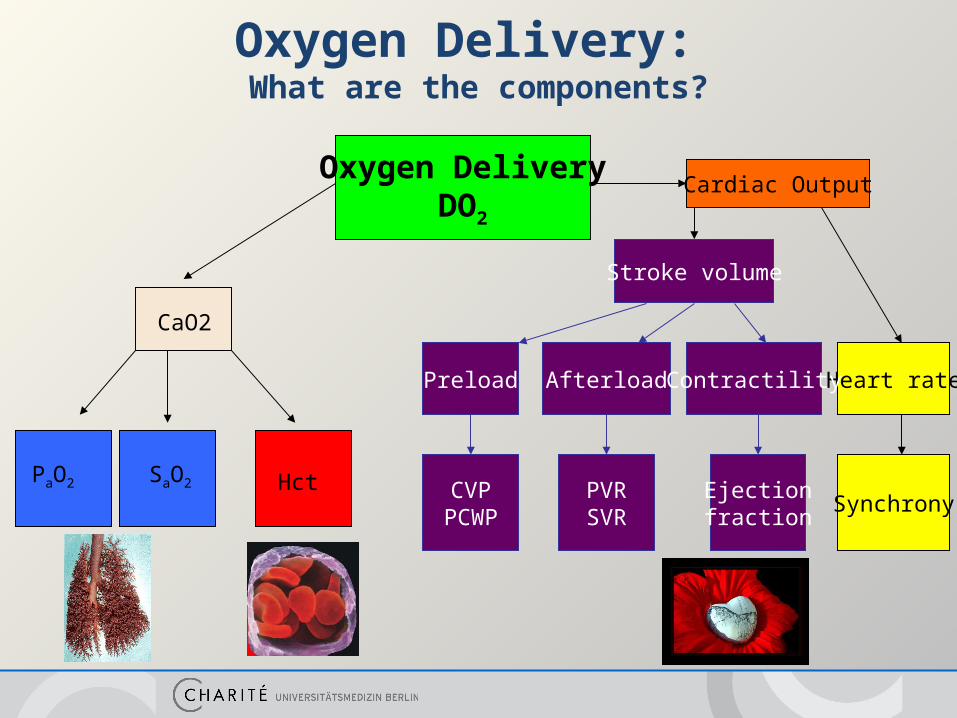
Oxygen Delivery: What are the components?
Oxygen DeliveryDO2
Cardiac Output
Heart rate
Stroke volume
CaO2
PaO2 SaO2 HctSynchrony
Preload Afterload Contractility
CVPPCWP
PVRSVR
Ejectionfraction
Implementation into practice?Monitoring of circulation:„It was fatal for the development of our understanding of circulation, that blood flow is relatively difficult to measure, whereas blood pressure is easily measured: This is the reason why the blood pressure meter has gained such a fascinating influence, although most organs do not need pressure, but blood flow.
Jarisch A. (1928). Deutsche Medizinische Wochenschrift
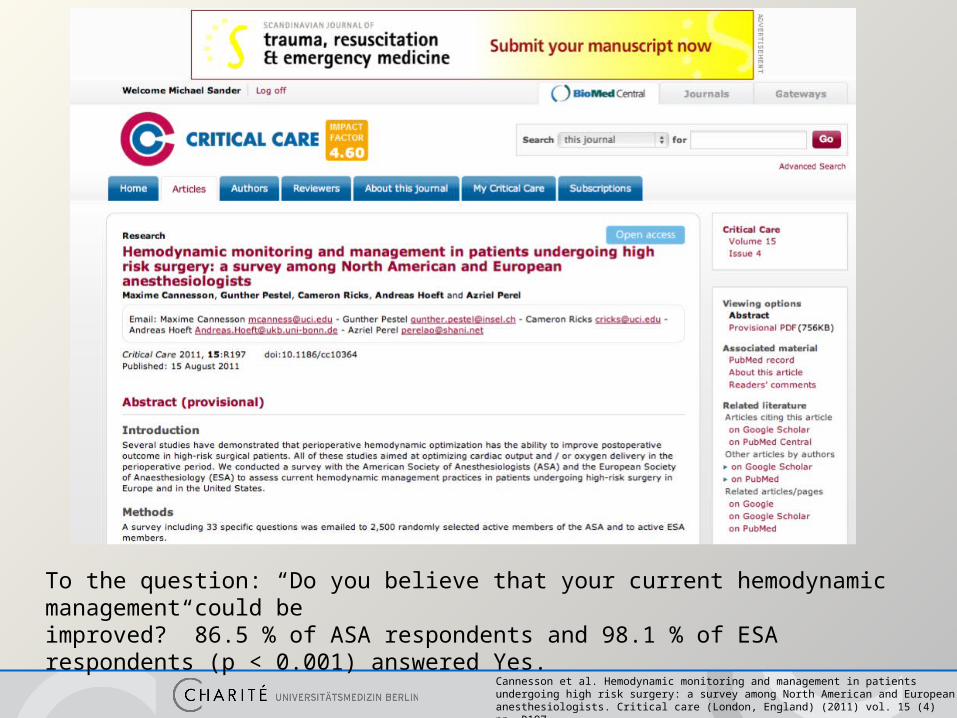
Cannesson et al. Hemodynamic monitoring and management in patients undergoing high risk surgery: a survey among North American and European anesthesiologists. Critical care (London, England) (2011) vol. 15 (4) pp. R197
To the question: “Do you believe that your current hemodynamic management could beimproved?” 86.5 % of ASA respondents and 98.1 % of ESA respondents (p < 0.001) answered Yes.

Cannesson et al. Hemodynamic monitoring and management in patients undergoing high risk surgery: a survey among North American and European anesthesiologists. Critical care (London, England) (2011) vol. 15 (4) pp. R197
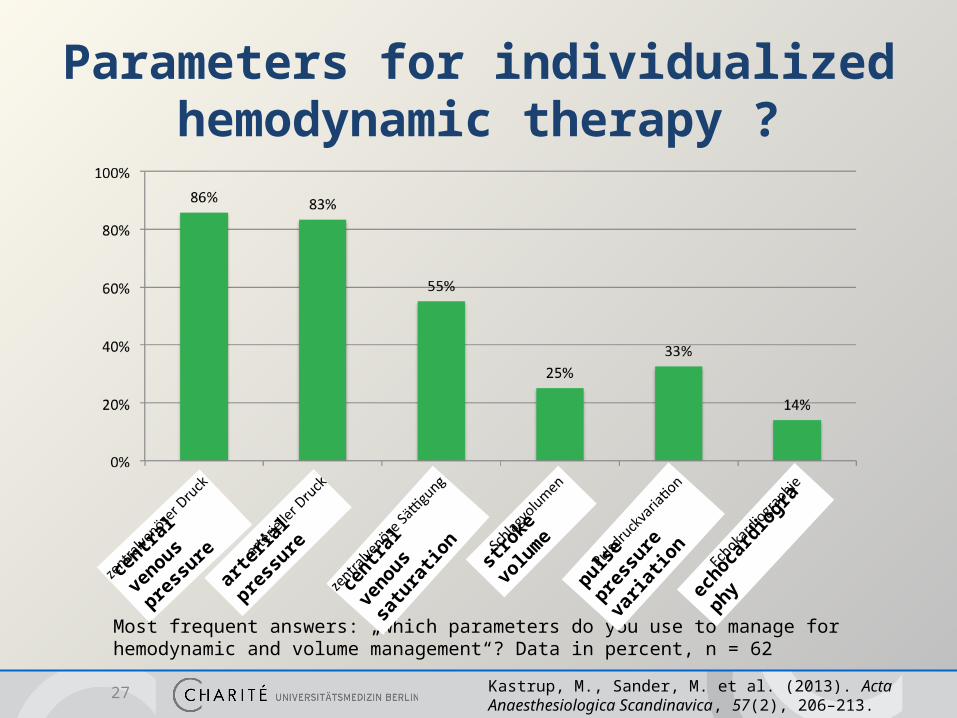
Parameters for individualized hemodynamic therapy ?
27 Kastrup, M., Sander, M. et al. (2013). Acta Anaesthesiologica Scandinavica, 57(2), 206–213.
Most frequent answers: „which parameters do you use to manage for hemodynamic and volume management“? Data in percent, n = 62
arteria
l pressu
re
centra
l venous
pressure
centra
l venous
satu
ration
stroke
volume
pulse pre
ssure
varia
tion
echoca
rdiogra
phy

PressureArterial pressure and central venous pressure for rmanagement of circulation therapy
28
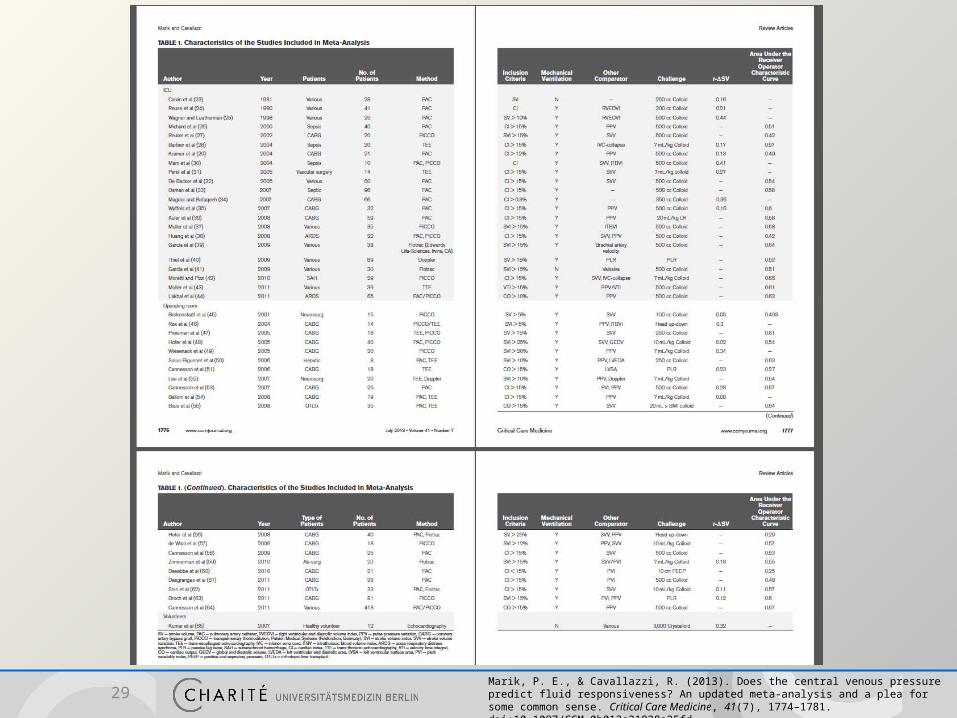
29Marik, P. E., & Cavallazzi, R. (2013). Does the central venous pressure predict fluid responsiveness? An updated meta-analysis and a plea for some common sense. Critical Care Medicine, 41(7), 1774–1781. doi:10.1097/CCM.0b013e31828a25fd
Does CVP predict fluid responsiveness?
An Updated Meta-Analysis and a Plea for Some Common Sense
There are no data to support the widespread prac- tice of using central venous pressure to guide fluid therapy. This approach to fluid resuscitation should be abandoned. (Crit Care Med 2013; 41:1774–1781)
30Marik, P. E., & Cavallazzi, R. (2013). Does the central venous pressure predict fluid responsiveness? An updated meta-analysis and a plea for some common sense. Critical Care Medicine, 41(7), 1774–1781. doi:10.1097/CCM.0b013e31828a25fd
venous saturation
31

HemoglobinHemoglobin
Physiology – Oxygen transport
Hemoglobin
Hemoglobin
Hemoglobin
Hemoglobin
Hemoglobin
Hemoglobin
Hemoglobin
Hemoglobin
Hemoglobin
Hemoglobin
Hemoglobin
Hemoglobin
Hemoglobin
Hemoglobin
Hemoglobin
O2
CO2CO2
Lung Tissue
O2
HemoglobinHemoglobin
O2
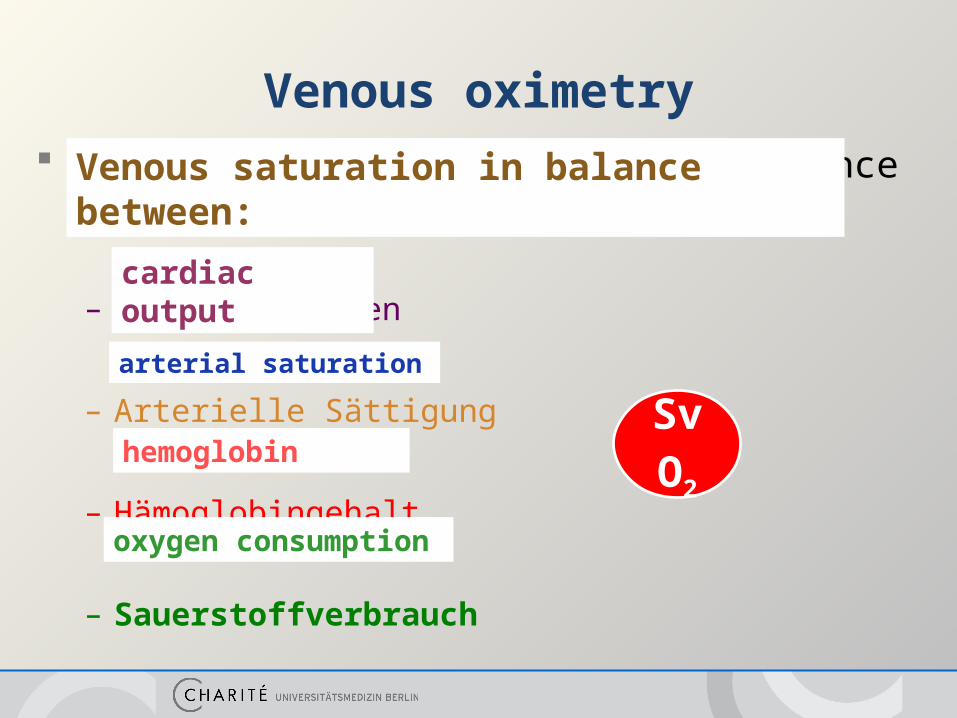
Venous oximetry Venöse Sättigungen zeigen die Balance zwischen:
– Herzzeitvolumen
– Arterielle Sättigung
– Hämoglobingehalt
– Sauerstoffverbrauch
SvO2
Venous saturation in balance between:
cardiac output
arterial saturation
hemoglobin
oxygen consumption
A low ScvO2 in the perioperative setting is associated with a higher risk of postoperative complications
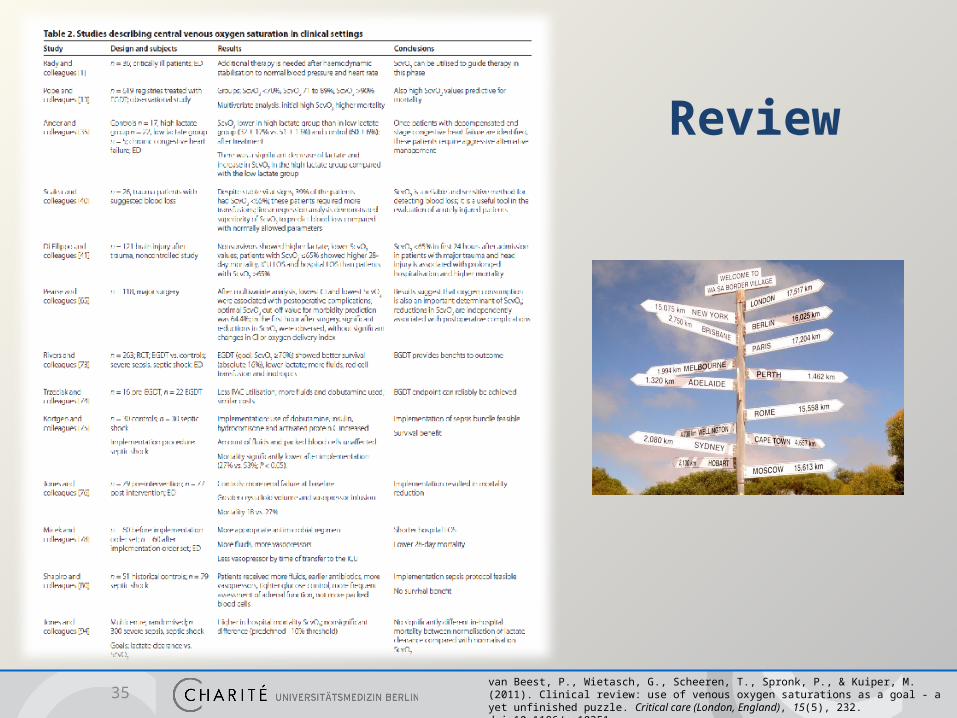
Review
35van Beest, P., Wietasch, G., Scheeren, T., Spronk, P., & Kuiper, M. (2011). Clinical review: use of venous oxygen saturations as a goal - a yet unfinished puzzle. Critical care (London, England), 15(5), 232. doi:10.1186/cc10351
Limitations
36
A low ScvO2 indicates that something is wrong, but not what is
wrong nor what needs to be done (fluids? inotropics?)
But,
If O2ER is reduced - especially in high risk surgery patients -
normal and high ScvO2 does not guarantee that perfusion is
adequate and that the patient has an ideal state of volume
Problems with interpretation of ScvO2
Hemoglobin
Hämoglobin
Pathophysiology of oxygen transport
Hemoglobin
Hemoglobin
Hemoglobin
Hemoglobin
Hemoglobin
Hemoglobin
Hemoglobin
Hemoglobin
Hemoglobin
Hemoglobin
Hemoglobin
Hemoglobin
Hemoglobin
Hemoglobin
Hämoglobin
O2
CO2CO2
Lung Tissue
O2
Hemoglobin
O2

Hemodynamic monitoring
39
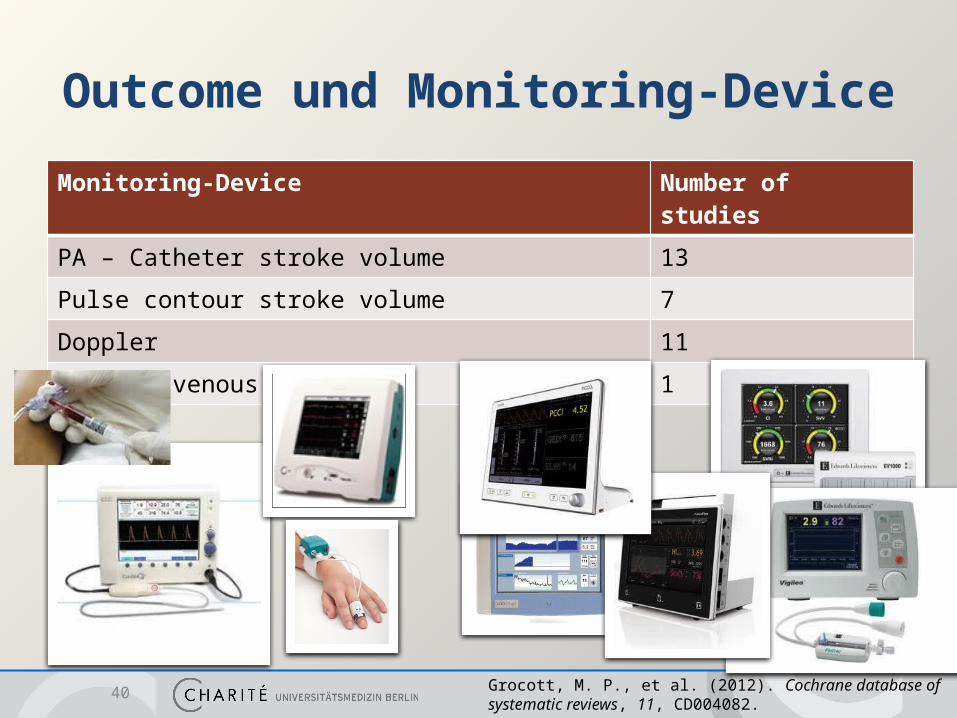
Outcome und Monitoring-Device
Monitoring-Device Number of studies
PA – Catheter stroke volume 13
Pulse contour stroke volume 7
Doppler 11
central venous saturation 1
40 Grocott, M. P., et al. (2012). Cochrane database of systematic reviews, 11, CD004082.
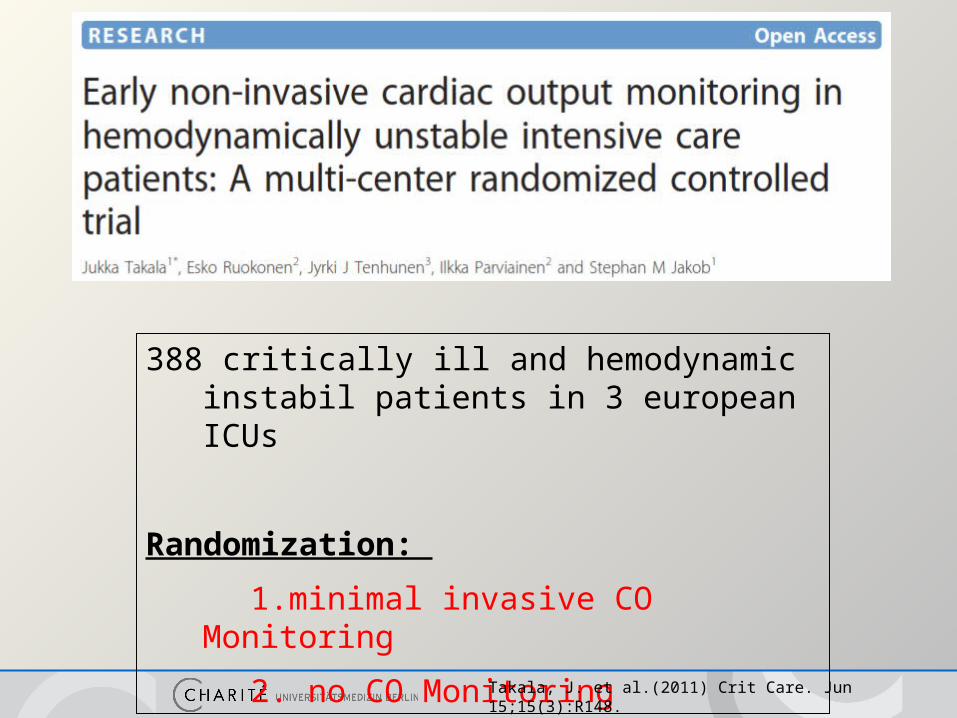
388 critically ill and hemodynamic instabil patients in 3 european ICUs
Randomization:
1.minimal invasive CO Monitoring
2. no CO Monitoring
Takala, J. et al.(2011) Crit Care. Jun 15;15(3):R148.
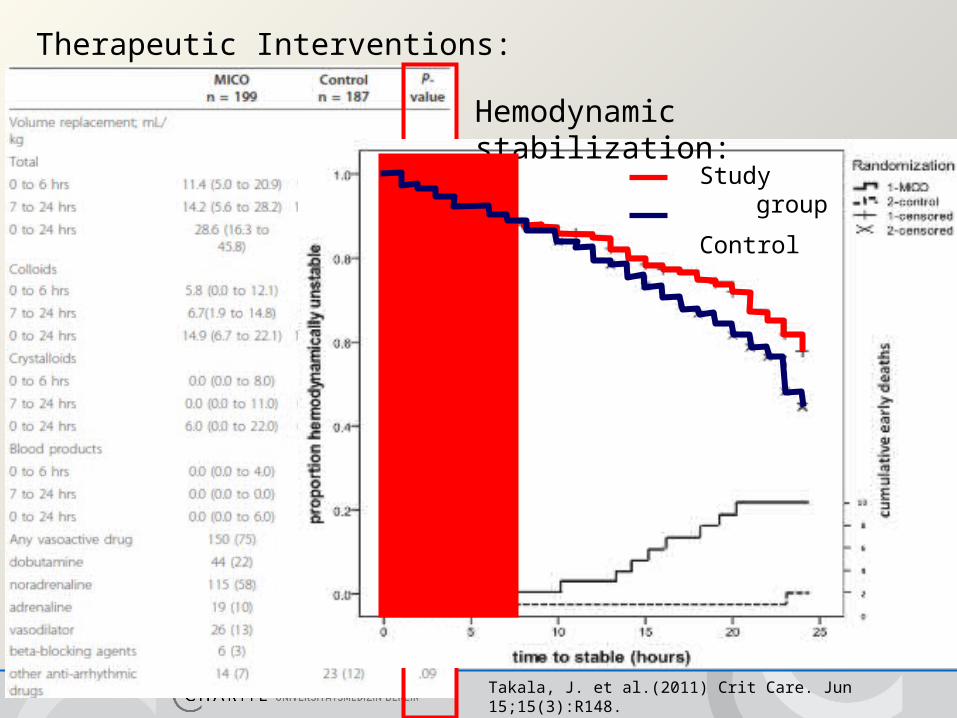
Therapeutic Interventions:
Hemodynamic stabilization:
Study group
Control
Takala, J. et al.(2011) Crit Care. Jun 15;15(3):R148.
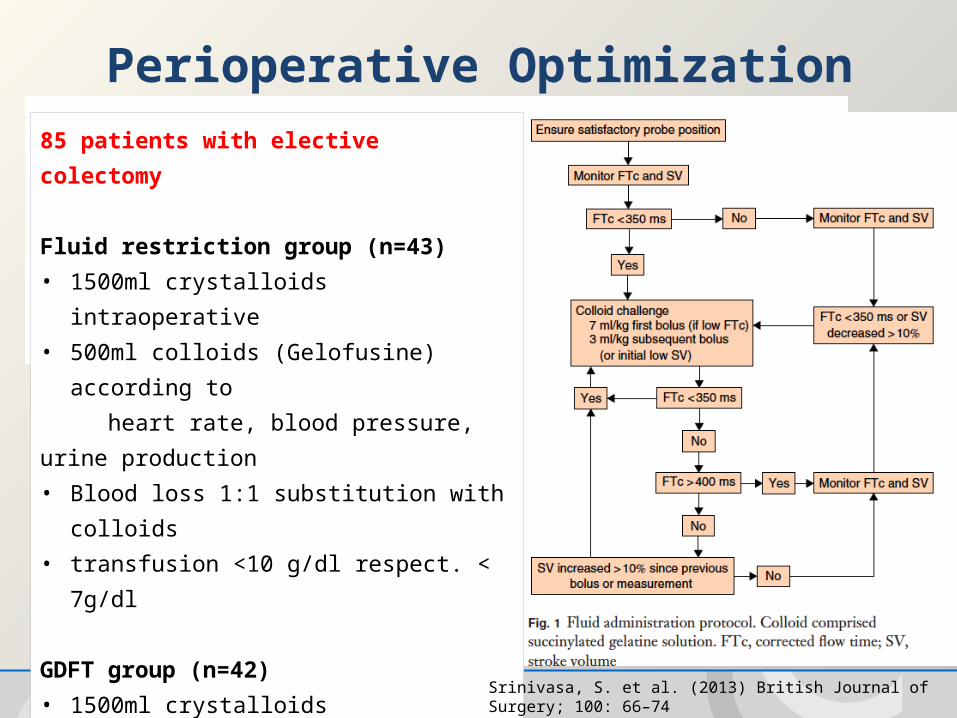
Perioperative Optimization85 patients with elective colectomy
Fluid restriction group (n=43)
• 1500ml crystalloids intraoperative
• 500ml colloids (Gelofusine) according to
heart rate, blood pressure, urine production
• Blood loss 1:1 substitution with colloids
• transfusion <10 g/dl respect. < 7g/dl
GDFT group (n=42)
• 1500ml crystalloids
• colloids according to flow chart
• Blood loss 1:1 substitution with colloids
• transfusion <10 g/dl respect. < 7g/dl
Srinivasa, S. et al. (2013) British Journal of Surgery; 100: 66–74

Perioperative Optimization
No difference in outcome
Srinivasa, S. et al. (2013) British Journal of Surgery; 100: 66–74

Most importantly, one must never forget that it is not the monitoring itself that can improve outcomes but the changes in therapy guided by the data obtained.
Vincent, J-L. et al. (2011) Critical Care 15:229.

Goal directed hemodynamic monitoring AND therapy
46
47

48Marik, P. et al. (2009). Critical Care Medicine, 37(9), 2642–2647.
Functional hemodynamics- stroke volume, PPV, SVV and TOE vs. CVP -
parameters Area under the curve (AUC) 95% - CI
pulse pressure variation 0,94 0,93 – 0,95
stroke volume variation 0,84 0,78 – 0,88
echocardiography (LVEDAI) 0,64 0,53 – 0,74
CVP 0,55 0,48 – 0,62
Stroke volume optimization and functional hemodynamic parameters are very suitable for individualized management of hemodynamic therapy.
methods:metaanalyse of 29 studies, N=685 patientsstatistics: ROC analyses (AUC; 95% - CI; increase SVI, CI)
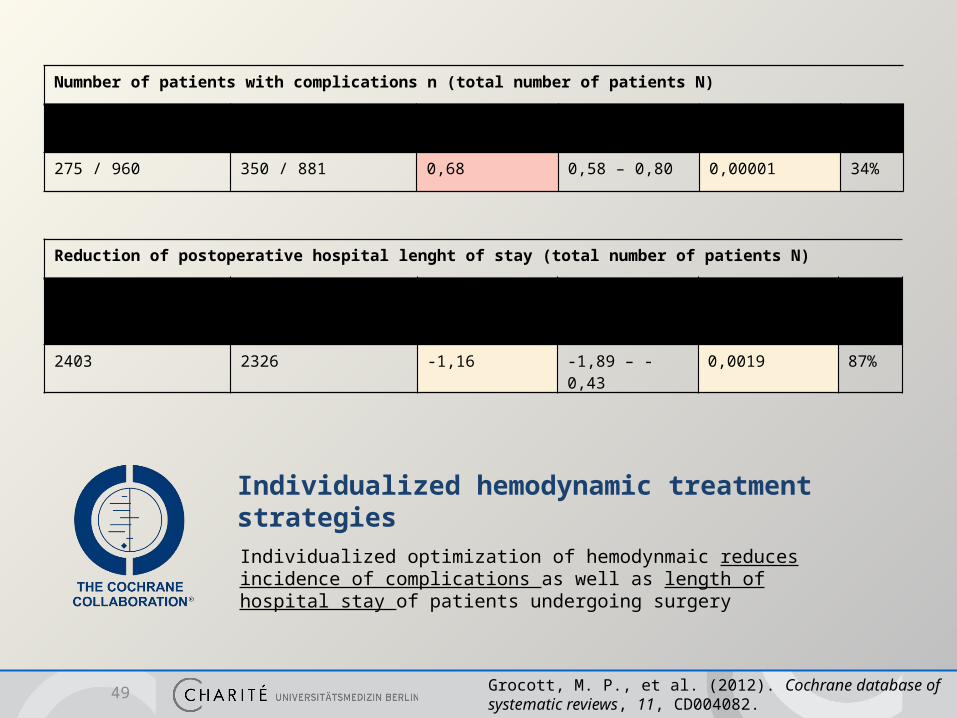
Individualized hemodynamic treatment strategiesIndividualized optimization of hemodynmaic reduces incidence of complications as well as length of hospital stay of patients undergoing surgery
49 Grocott, M. P., et al. (2012). Cochrane database of systematic reviews, 11, CD004082.
Numnber of patients with complications n (total number of patients N)
Protocol group(n/N)
Control group(n/N)
Risk Ratio 95% - CI p value I2
275 / 960 350 / 881 0,68 0,58 – 0,80 0,00001 34%
Reduction of postoperative hospital lenght of stay (total number of patients N)
Protocol group(N)
Control group(N)
Mean difference(d)
95% - CI p value I2
2403 2326 -1,16 -1,89 – -0,43 0,0019 87%
Conclusion Hemodynmic monitoring
– Alone does not change outcome
Individualized hemodynamic treatment strategies– Do have an impact on patient outcome– „One size does not fit all“ – Individualized approach for hemodynmamic management – Goals of treatment are not static parameters (MAP, CVP, ScvO2) – Goals of treament are functional parameters, i.e. stroke volume optimization, pulse pressure
variation and stroke volume variation
Perspective– International guidelines– Clinical implementation patient safety
50
Related Documents











