Dr. Muhammad Sajjad Sabir MBBS, DCH, MCPS, FCPS Assistant Professor of Paediatrics Pediatric Diabetes Mellitus

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript
Dr. Muhammad Sajjad SabirMBBS, DCH, MCPS, FCPS
Assistant Professor of Paediatrics
Pediatric Diabetes Mellitus
PEDIATRIC DIABETES MELLITUS
Juvenile diabetes mellitus is a chronic metabolic disorder resulting from absolute lack of insulin
Most pediatric patients have type 1 diabetes mellitus → lifetime dependence on exogenous insulin
Abnormal metabolism of carbohydrate , protein and fat
Characterized by hyperglycemia , glycosuria and tendency to ketoacidosis
CAUSES
Progressive loss of islet-cell functionInsulin resistanceIatrogenic - post pancreatic surgery

ETIOLOGY Idiopathic: 95% belong to this category Hereditary Multi-factorial inheritanceSecondary: Cushing syndrome Hyperpituitarism Surgical removal of pancreas

Type 1 - Insulin dependentInsulin dependent Most childhood diabetes Prone to ketosis
Type 2 - Non-Insulin dependent Usually Older children Obesity-related Positive family history Not prone to ketosis
Classification of DM according to Causes
CLASSIFICATION OF DM ACCORDING TO CAUSES
Type 3 - Other Specific Types Genetic defects in β-cell function( Maturity Onset
Diabetis of Young,MODY ) → responds to oral
hypoglycemic drugs Genetic defect in insulin action Infections - Congenital rubella Drugs - Corticosteroids Pancreatic exocrine insufficiency - Cystic fibrosis Genetic/Chromosomal disorders
Type 4 - Gestational Diabetes Mellitus(GDM)
Type 1- Diabetes Mellitus
T1DM

EPIDEMIOLOGY
UK- annual incidence 20 per 100,000 children
Incidence increasing in children < 5yr age Under 1 - Extremely rareMinor peak 4-6yrMajor peak 10-14yr
EPIDEMIOLOGY
No clear pattern of inheritanceIncreased risk if 1 member of family
affectedIdentical twin has 50% risk to develop DMIndividuals with HLA-DR3 and HLA-DR4
have increased risk
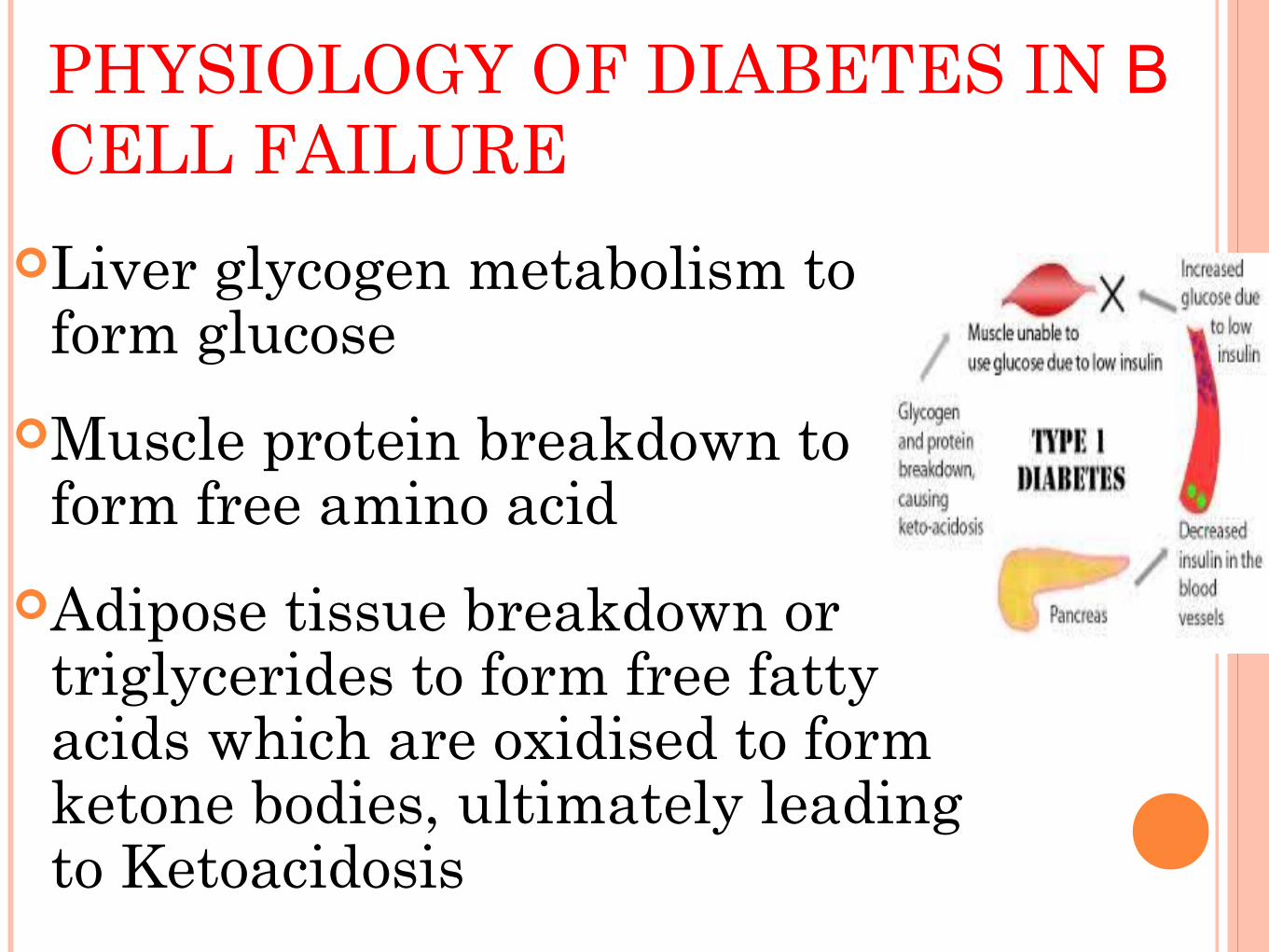
PHYSIOLOGY OF DIABETES IN Β CELL FAILURE
Liver glycogen metabolism to form glucose
Muscle protein breakdown to form free amino acid
Adipose tissue breakdown or triglycerides to form free fatty acids which are oxidised to form ketone bodies, ultimately leading to Ketoacidosis
Hypothyroidism affects 2-5% of children with diabetes
Addison disease
Celiac disease
Associated Autoimmune diseases
Natural history of T1DM T1DM involves some or all following stages:
1) Initiation of autoimmunity2) Preclinical autoimmunity with progressive loss of β-cells
3) Onset of clinical disease
4) Transient remission
5) Established disease
6) Development of complication
CLINICAL FEATURESAcute onsetUsually preceded by infection
PolyuriaPolyphagiaPolydypsiaWeight lossNocturiaDiabetic coma

The main symptoms of are secondary to osmotic diuresis and glycosuria
Insulin deficiency→ hyperglycemia →
glycosuria→ osmotic diuresis
→Polyuria → ↑thurst →Polydipsia
Pathophysiology of T1DM

Insulin deficiency→ lack of glucose utilization→ ↑ appetite→ Polyphagia
Insulin deficiency→ lack of glucose utilization→ ↑utilization of fats → DKA
Impaired protein synthesis → Weight loss
Pathophysiology of T1DM
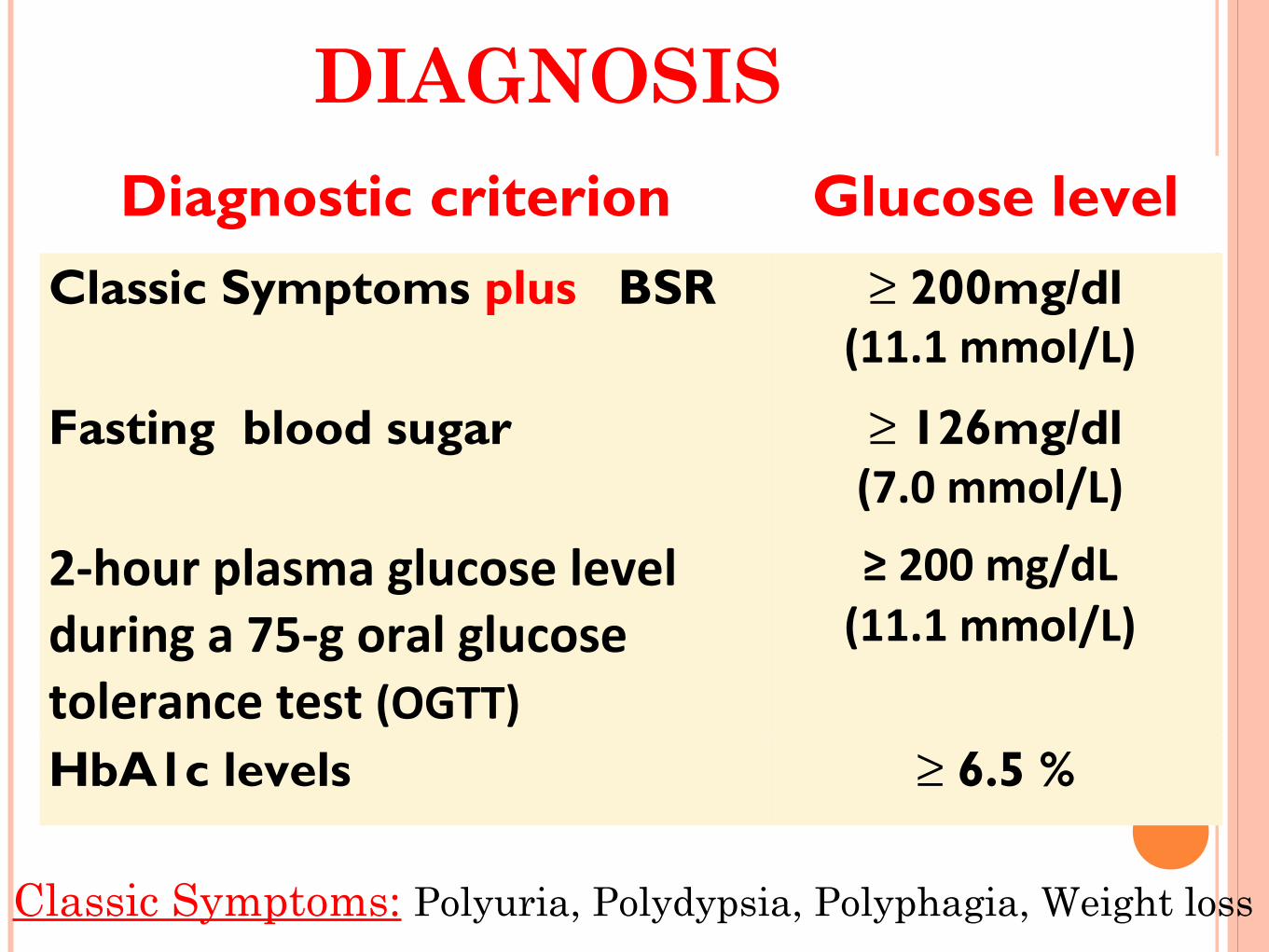
DIAGNOSIS
Classic Symptoms: Polyuria, Polydypsia, Polyphagia, Weight loss
Diagnostic criterion Glucose level
Classic Symptoms plus BSR ≥ 200mg/dl(11.1 mmol/L)
Fasting blood sugar ≥ 126mg/dl(7.0 mmol/L)
2-hour plasma glucose level during a 75-g oral glucose tolerance test (OGTT)
≥ 200 mg/dL (11.1 mmol/L)
HbA1c levels ≥ 6.5 %

• Type 2 diabetes mellitus
• MODY
• Psychogenic polydipsia
• Nephrogenic diabetes insipidus
• High-output renal failure
• Transient hyperglycemia with illness / stress
• Factitious illness (Münchhausen syndrome by
proxy)
Differential Diagnosis

INVESTIGATIONS1. Urine examination:• glucosuria• ketonuria2. Blood sugar levels ( ↑BSR, ↑ BSF )3.Serum electrolytes: Hyponatremia Hypokalemia Low chloride

4. Acid Base Balance: pH is low Bicarbonate base deficit low5. Blood examination: Hb and Hct ↑ due to dehydration ↑ TLC
Investigations

Management

Insulin Types 4 basic formulations Ultra-short acting insulin
Lispro aspart
Short acting insulin Regular Insulin Soluble Insulin
Intermediate acting insulin NPH (Neutral Protamine Hagedorn) Lente Ultralente
Long acting Insulin Glargine ultralente
INSULIN THERAPY
1. Insulin Replacement:
Insulin DOSE 0.75-1.0 U/kg S/C
(Range = 0.5 - 1.2 U/kg) Total daily dose divided into
NPH (2/3rd of total) Regular (1/3rd of total) 2/3rd of daily dose- before breakfast 1/3rd - evening

Insulin- available forms

Insulin - available forms

Insulin Inj sites

DIET Recent dietary recommendations• Carbohydrates
• Should provide 50-55% of daily energy intake; • no more than 10% of carbohydrates should be
from sucrose or other refined carbohydrates• Fat - Should provide 30-35% of daily energy intake• Protein - Should provide 10-15% of daily energy
intake
Important aspect of diabetes management
Real benefits for a child with diabetes
No form of exercise, including competitive sports, should be forbidden to the diabetic child
25 min aerobic exercise- encourage regular daily exercise
Exercise
Patient and Parent EducationEducation is a continuing process involving the child, family, and all members of the diabetes team Recognition and treat hypoglycemia How to mix insulin How to inject / change sites How to store insulin How to check BSR/urine tests Increase dose in acute illness Complications
BLOOD SUGAR MONITORING
4 readings (before meal, before snack and in middle of night 3:00 am)
2 readings (before breakfast , before dinner)
Good Control: Fasting and Preprandial BSR – 70-
150mg/dl Postprandial BSR – 180-200mg/dl 3:00 am Value – 65mg/dl
Home Monitoring
Blood Sugar Monitoring:
• By Glucometer
Urin dipstick:
• Glucsuria
• Ketonuria
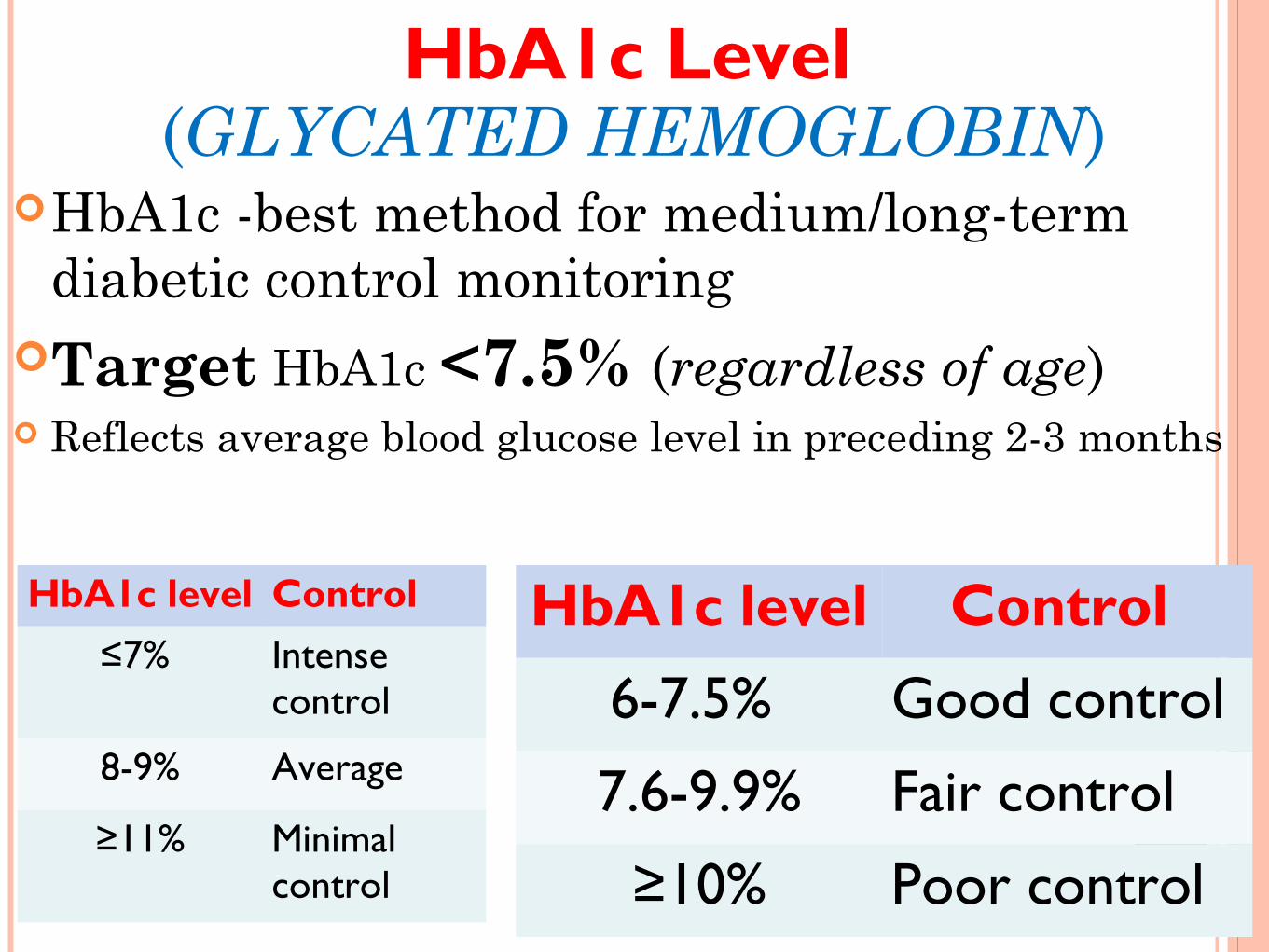
(GLYCATED HEMOGLOBIN)HbA1c -best method for medium/long-term
diabetic control monitoringTarget HbA1c <7.5% (regardless of age) Reflects average blood glucose level in preceding 2-3 months
HbA1c level Control
≤7% Intense control
8-9% Average
≥11% Minimal control
HbA1c level Control
6-7.5% Good control
7.6-9.9% Fair control
≥10% Poor control
HbA1c Level

FOLLOW UP:Monitor GrowthBlood pressureSchool progressDietary complianceHbA1c levelJoint mobilityFundus examinationThyroid function testCheck insulin site
•Injection -site hypertrophy•Retinopathy•Cataracts•Gastroparesis•Hypertension •Progressive renal failure•Early coronary artery disease•Peripheral vascular disease•Peripheral and autonomic neuropathy•Increased risk of infection
Complications:
COMPLICATIONS: Brittle Diabetes Mellitus:marked fluctuation in blood sugar
despite frequent adjustment of doses Diabetic Ketoacidosis Neuropathy Nephropathy Retinopathy and Blindness Hyperosmolar Diabetic Coma Lipoatrophy Growth Retardation and Emotional problem

HYPOGLYCEMIAMajor complicationBlood sugar level < 60mg/dlSign / Symptoms: Behavior changes ,
palpitation, pallor , diplopia , sweating ,nausea , vomiting , hunger, disorientation tremors, may progress to convulsion and coma
Treatment: lump of sugar, sweet drinkSevere hypoglycemia : Inj. Glucagon
DIABETIC KETOACIDOSIS
(DKA)
Hyperglycemia >300mg/dl
Ketonemia Plasma ketone >3mmol/l
Acidosis Bicarbonate<15meq/l
Ketonuria +ve
PRESENTATION OF DKA
Polyuria , Polydipsia , Weight lossAcutely ill patient with fruity smell
due to ketosisNausea , Vomiting , LethargyHyperventilation , DehydrationAbdominal PainDrowsiness or Coma
DKA INVESTIGATIONS
1. CBC2. ESR3. BSR4. Urine ketone5. Urine sugar
6. ABG’S
7. Urea ,Creatinine
8. Electrolyte
9. Blood C/S
10. Urine C/S
DKA MANAGEMENT1. ABC2. Correction of fluid and electrolyte3. Correction of metabolic acidosis4. Provision of adequate insulin to prevent ketosis and
decrease hyperglycemia5. Prevention and monitoring of complications6. Identification of precipitating factors7. Insulin regimen8. Teaching of sick days

DKA PROTOCOL1st hour : 10-20ml/kg iv bolus 0.9% NaCl or LR Insulin drip at 0.05 - 0.10 units/kg/hr (Regular insulin)
2nd hr until DKA resolution : 0.45% NaCl : plus continue insulin drip I.V Rate= 85ml/kg + maintenance - bolus 23 hr
Note(1) Initial IV bolus is considered part of total fluid allowed in 1st 24 hr(2) Maintenance (24 hr) = 100 mL/kg (for the 1st 10 kg) + 50 mL/kg (for the 2nd 10 kg) + 25 mL/kg (for all remaining kg)(3) Cerebral edema major cause of morbidity and mortality
DKA PROTOCOL 20 mEq/L KCL (20ml in each Lit fluid)Cerebral edema =1g/Kg Mannitol I.V push 5% glucose if blood sugar <250 mg/dl Shift to subcutaneous insulin
• BSR is 180-240mg/dl • Oral intake• No emesis • CO2 ≥16 mEq/L• normal electrolytes

D/D OF DIABETIC KETOACIDOSIS
1. Hyperosmolar Non Ketotic Coma2. Meningoencephalitis3. Salicylate Poisoning4. Gastroenteritis with Acidosis

SOMOGYI PHENOMENON
Due to ↑insulin dose in evening →Mid-night hypoglycemia → counter regulatory hormones → early morning ↑serum glucose (hyperglycemia)Management↓ evening insulin dose

DAWN PHENOMENON Simple decline in insulin levels (seen in many
children using NPH insulin at supper or bedtime)
→ early morning hyperglycemia Dawn phenomenon is due to overnight growth
hormone secretion and increased insulin clearance
Management↑ evening insulin dose

?
Related Documents











