Type 2 diabetes in children and youth Shokoufeh Bonakdaran, MD Assistant Professor of Endocrinology Mashhad University of Medical Sciences

Type 2 diabetes in children and youth Shokoufeh Bonakdaran, MD Assistant Professor of Endocrinology Mashhad University of Medical Sciences.
Dec 27, 2015
Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

Type 2 diabetes in children and youth
Shokoufeh Bonakdaran, MD
Assistant Professor of Endocrinology
Mashhad University of Medical Sciences
There has been a rise in type 2 diabetes mellitus (T2DM) in children and adolescents, which may be related to global obesity trends , an actual rise in incidence and an increased diagnostic recognition that this condition can occur in children
The global burden of T2DM continues to rise as the worldwide
prevalence of adult diabetes is projected to increase from 246 to 380 million people by 2025.
T2DM currently accounts for 15% to 87% of newly diagnosed American youth compared with only 3% in the 1990s

Health burden
The decreasing age at onset of T2DM
has serious public health implications, as future generations are burdened with micro- and macrovascular complications at the peak of their productive years

Risk factors:
overweight or at risk for overweight Most pediatric patients are in the midst of puberty. 90% have at least one first- or second degree relative
with T2DM
- female predominance - more common among racial minorities, especially American Indians) and Asian/Pacific Islanders . genetic loci associated with higher risk for polygenic forms of
T2DM:transcription factor 7-like 2 gene (TCF7L2)


normal FPG in 91.5% combination of higher levels of
BMIz(standard deviation score for age and gender, HOMA-IR, and family history suggests the greatest risk for T2D and targets them for further evaluation and intensive preventative management.



clinical presentation of T2DM in youth can range from mild asymptomatic hyperglycemia to severe ketoacidosis
About one-third of T2DM patients are diagnosed by routine laboratory screening rather than as a result of specific complaints. Such accidental’ diagnosis is rare in T1DM

42% of African-American patients with T2DM presented with ketonuria and 25% with DKA
insulin resistance combined with the deleterious effect of chronic hyperglycemia on insulin secretion and action (glucose toxicity’) results in relative insulin deficiency

HHS
there are currently 29 reported cases of adolescents with HHS, of whom 26 were
African- Americans and 22 were males As in adults, HHS in adolescents is
associated with significant mortality (12 of these 29 cases, 41.4%

Accelerator Hypothesis
Obesity driven insulin resistance accelerates beta cell apoptosis through glucotoxicity and lipotoxicity
stressed beta cell metabolically and immunologicaly upregulated and more vulnerable to immune injury and apoptosis
obesity and weight gain are at the core of β-cell stress leading to both T1DM and T2DM and predicts earlier presentation of all diabetes types in individuals with increased weight gain

a 10% increment in relative weight was associated with a 50% to 60% increase in the risk of T1DM before age 3 years and a 20% to 40% increase from age 3 to 10 years

Autoimmunity?
a significant proportion of physician-diagnosed T2DM youth show evidence of pancreatic autoimmunity at screening
The presence of autoantibodies in adults with clinically suspected T2DM who have positive antibodies is associated with a high risk of eventually becoming insulin dependent, a condition termed latent autoimmune diabetes
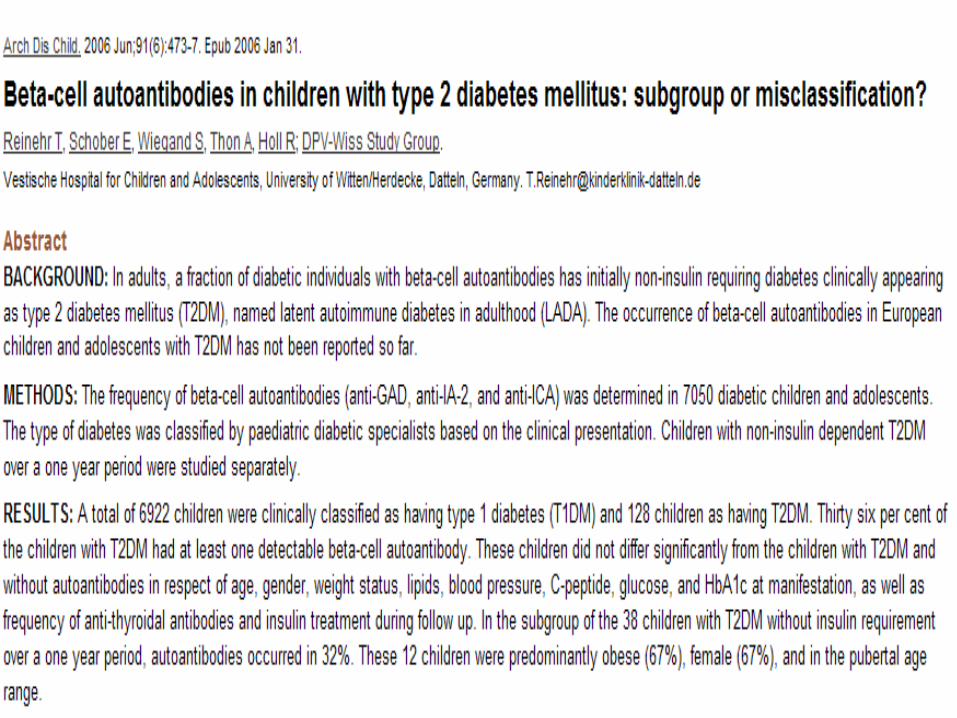

children did not differ significantly from the children with T2DM and without autoantibodies with respect to age, gender, overweight status, lipids, blood pressure, C-peptide, glucose, and hemoglobin A1c (HbA1c) at manifestation as well as frequency of anti-thyroidal antibodies and insulin treatment during follow-up. Because starting insulin treatment in patients with T1DM is critical, the diagnosis of T2DM should be made with caution and only when beta-cell autoantibodies are negative.

In TODAY study
autoantibody positive patients: - Were less likely to have a first degree relative with diabetes- had lower BMI - lower systolic and diastolic blood pressure- higher HDL- Lower TG- higher HbA1C- Lower fasting C-peptide
- obese seropositive diabetic youth are closer to T1DM than their seronegative T2DM

TREATMENT
initial approach to the treatment of T2DM generally focuses on improvement in insulin
sensitivity, either through modification of
lifestyle habits or through pharmacologic intervention.

Patients who are not critically ill but
have signs of dehydration, ketosis, severe
hyperglycemia, or HbA1c >8.5% require treatment with insulin
Despite the goal of withdrawing insulin therapy after its initial introduction, only 28% of patients
were able to come off insulin, and of those, 60%required reinitiation of insulin because of poor control

PHARMAOCOTHERAPY
metformin is the only U.S. Food and Drug Administration (FDA)-approved oral treatment for youth with type 2 diabetes
Medication be titrated to a maximum dose of 2,000 mg/day, divided twice daily, based on effectiveness and tolerance of side effects
once glycemic control fails, additional agents, and typically insulin, are considered
bedtime long-acting analog (glargine or detemir) at a dose of 0.3–0.4 units/kg/day. thiazolidinediones (TZDs) and insulin secretagogues are
not FDA approved glinides(repaglinide and nateglinide, short-acting insulin
secretagogues) and glucosidase inhibitors (acarbose), are available for adults but are not approved in pediatrics

But!
Surveys show that ;50% of youth were treated with secretagogues in 2000 and 28% in 2008, and 9% were treated with TZDs in 2000


glucagon-like peptide (GLP)-1
GLP1 : data in pediatrics is almost nonexistent. administration of single 2.5- and 5-microg doses of
exenatide were associated with dose-dependent increases in plasma exenatide concentrations and improved postprandial glucose concentrations compared with placebo
there are no study outcomes of liraglutide in adolescents with type 2 diabetes.
Currently, there are no data on the use of dipeptidyl peptidase-4 inhibitors in pediatrics

COMORBIDITIES ANDCOMPLICATIONS
49% of young people with diabetes had systolic hypertension( eight times higher than in type 1 diabetes)
Microalbuminuria was more prevalent in youth with type 2 diabetes (22.2%) compared with youth with type 1 diabetes (9.2%) AND the rate of progression of microalbuminuria seems to be more rapid in adolescents with type 2 diabetes
Dyslipidemia, a major comorbidity of obesity, is present in high rates in youth with type 2 diabetes, ranging from 18 to 61% at diagnosis

management of hypertension
blood pressure tables must be used for diagnosis of hypertension.
Hypertension in pediatrics (blood pressure >95% for age, sex, and height, especially in conjunction with albuminuria) should be treated aggressively
If tolerated, an ACE inhibitor should be used; otherwise, an angiotensin receptor blocker should be used

hyperlipidemia
goal of LDL <100 mg/dL, triglycerides <150 mg/Dl, and HDL >35 mg/dL
Treatment strategies include maximizing
Non pharmacologic interventions for LDL
of 100–129 mg/dL, considering medication
on the basis of presence of other risk factors for LDL of 130–159 mg/dL, and initiating medication for LDL >160 mg/dL
Statin therapy has been shown to be safe and effective in youth and should be the first pharmacologic intervention
If triglycerides are >1,000 mg/dL, treatment with fibric acid should be considered to reduce the risk of pancreatitis

Related Documents