Two Palliative Care Giants Dr Jennifer Vidrine ST4 Palliative Medicine

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

Two Palliative Care Giants
Dr Jennifer VidrineST4 Palliative Medicine

Overview
• A broad overview of palliative care in relation to general practice
• Pain• Case 1• BREAK• Nausea and Vomiting• Case 2 • Round Up

Palliative Care
• Recognised as distinct entity since 1980s• First modern hospice opened 1967• Based on concept of ‘Holistic’ care • Palliative care teams• Not just for patients with cancer

GPs and palliative care

• “GPs found looking after palliative care patients satisfactory and varied but burdensome”
• Found barriers on three levels:– Personal– Relational – Organisational

Challenges faced…• Personal– Knowledge symptom and symptom control– Technical procedures in pts who want to stay at
home (ie Catheter)– Small numbers of palliative care patients in a year– Emotional – Time constraints– Lack of psychological support in an autonomous
worker

• Relational– Communication• Between pts, carers, other HCPs
– ‘Territory’ (GP? SPCT? Hospital team?)
• Organisational– Bureaucracy– Obtaining medications (Controlled drugs, CSCI etc)– Need to organise care/social work review etc

They conclude
• Barriers exist• It is imperative to support GPs as the frontline
of service provision• Role of specialist palliative care teams in this
(both specialist knowledge and emotional support)


Common Symptoms
• Pain• Nausea and Vomiting• Shortness of Breath• Anxiety/Psychological Distress

Common Symptoms
• Pain• Nausea and Vomiting• Shortness of Breath• Anxiety/Psychological Distress

Pain

Nociceptive vs neuropathic pain

Nociceptive vs neuropathic pain

Neuropathic pain
• Disproportionate to stimulation of the nociceptor
• Leads to:– Hyperalgesia (exaggerated and prolonged pain response to a mildly painful stimulus)– Allodynia(Pain produced by a stimulus that is not normally painful, such as light
touch)– Spontaneous pain
• No protective function
• Pathological pain

Distinguishing the two…
• History History History• Thinking abut possible/likely aetiologies• What has the pain responded to thus far?

• Very often in palliative care it is a combination of both
• Requires combination treatments (Often one won’t cut it)
• Often requires some lateral thinking

WHO analgesic ladder


An approach…
• Patient specific• Tend to start with low dose strong opiate
(eg Oramorph 2.5-5mg PRN)• If possible also give regular paracetamol• Ask patient/relative to write down the
following:
Date Time Site Pain Pain score /10 before
What taken
Pain Score /10 after
Notes/Side effects
• Review in a couple of days.• Establish if opioid making ANY difference• Establish any side effects• Calculate what has been taken in last 24 hours
(ie 4 doses of 5mg=20mg)• Start BD preparation of long acting opiate• Explain need to continue with Breakthroughs
and ongoing monitoring.• Breakthrough is 1/6 total daily opioid dose
(except Alfentanil which is 1/10th)

Established on Morphine but still in pain?
• Would an adjunct help?Steroids (Dexamethasone)TCA (Amitriptyline)Anti-epileptics (Gabapentin/Pregabalin)
• Very often end up on combination

Evidence Base
• Amitriptiline-OD dosing, syrup available.
• Gabapentin- syrup available, TDS
• Pregabablin- ?more tolerable, BD, only tablets
• Valporate- OD, syrup available, RCT conflicting
• Clonazepam- Concurrent anxiolytic and muscle relaxant properties, SC
Anti-epileptic NNT
Carbmazepine 3.3
Gabapentin 3.5
Lamotrigine 4
Sodium valporate
2-2.5?

Other things to consider
• NSAIDs– If no contra-indications– Esp if inflamm element of pain– Useful in bone pain– Ibuprofen used most frequently– Ketorolac useful as can be used subcut (Generally
only for short spells/at end of life)• Bisphosphonates

Particular Challenges
• Episodic Pain• High anxiety element (Total pain)• Non-concordance
Consider referral/involvement SPCT

What might be offered…
MethadoneKetamineSpinal Lines (epidural/intrathecal line)Nerve BlocksCordotomy (Division of lateral spinothalamic
tracts in the spine)Involvement of clinical psychology

Case 1
• Break up into groups of 3-5• Look at the case and start to think about the
issues involved for 20 mins• Try to approach as holistically as possible• Feed back to group.

Comfort Break

Nausea &
Vomiting

Nausea & Vomiting-Background
• Extremely common in cancer patients• Deeply distressing• Vomiting generally tolerated better than
nausea
“Last night we went to a Chinese dinner at six and a French dinner at nine, and I can feel the shark’s fins navigating unhappily in the Burgundy”Peter Flemming, Letter from Yunnanfu, March 1938

Reality of the situation
• Often as/more challenging to treat than pain• Many patients have multifactorial N&V• Absorption of the very stuff we are giving
them to make them better• May well require more than one anti-emetic• Systematic/logical approach….
Questions to ask
• Nausea/vomiting predominant?• Timing?• What is vomited? (Consistency, volume, colour)• Feel better after vomiting?• Associated features?• Exacerbating/relieving factors• Are there are any probable causes? (eg
Constipation)

Identify specifically treated causes
• Constipation-Laxatives/PR intervention (Prevention)• Gastritis-Would PPI help?• Oropharyngeal Candida-Often difficult to treat• Hypercalcaemia-IV hydration +/- Bisphosphonate• Pain-Optimise analgesia• If drug induced how essential is drug?• Treat infection

• Think about non-drug measures• Select anti-emetic based on most likely cause• Basic principals:– Give regular antiemetics– Need to carefully assess risk of non-absorption
and consider alt routes (CSCI) early– If you are relatively sure about cause consider
maximising dose rather than switching (esp Metoclopramide)

Two ‘broad’ avenues..
1.Gastric-stasis2.Chemically mediated (central)

1. Gastric Stasis-presentation
• Early Satiety• Large volume vomits• Undigested food• Relief after vomiting• Hiccoughs/belching• Exacerbated by eating/medcations

1.Gastric stasis-causes
• Slowed gastric emptying• ‘Squashed stomach’ due to Hepatomegally• Ascites• Subacute obstruction (consider specialist
input)

1.Gastric Stasis-management
• Prokinetic eg Metoclopramide• Targets peripheral (and central) Dopamine (D2)
receptors.• Caution in young females• CAUTION IN PARKINSON’S DISEASE/SYNDROMES• Dose: 10-20mg tds/qds– CSCI 30-120mg/24 hours
• Domperidone (less side effects but limited routes)
• OBSERVE FOR INTESTINAL COLIC

Vomiting
Centre
ChemicalMedicationBiochemical
Toxins
GI tractObstruction
Gastric stasisIrritation/hepatic
VestibularMotion sickness
Local tumourMedication
Central Anxiety
PainCerebral mets
Raised ICP
DopamineSeretonin 3
Dopamine Seretonin
4Acetylcholine
Histamine
HistamineCTZMetoclopramide
Two ‘broad’ avenues..
1.Gastric-stasis2.Chemically mediated (central)

2.Central Causes-presentation
• Constant nausea• No/little relief after vomiting• May be able to identify cause• Other signs drug toxicity

Central-Causes
Drugs:OpiatesAntidepressantsAEDs
Electrolyte ImbalanceRenal FailureHypercalcaemia
SepsisAnxietyPainRaised Intracranial
PressureIschemic Bowel

2. Central Causes-Management
Cyclizine• Antihistaminic/Anticholinergic antiemetic acting
at AChM and H1 receptors• Acts centrally to help with vagally mediated
nausea.• Can give anticholinergic side effects• Dose: 25-50mg tds– CSCI: 150mg/24 hour
• Particularly useful if raised intracerebral pressure

Vomiting
Centre
ChemicalMedicationBiochemical
Toxins
GI tractObstruction
Gastric stasisIrritation/hepatic
VestibularMotion sickness
Local tumourMedication
Central Anxiety
PainCerebral mets
Raised ICP
DopamineSeretonin 3
Dopamine Seretonin
4Acetylcholine
Histamine
HistamineCTZ
Cyclizine

2. Central Causes-Management
Haloperidol• Useful for chemical induced nausea (inc
Drug induced) • Centrally acting anti-emetic acting at D2 receptor at the
CTZ• Contraindications• Dose: 1.5mg Nocte (0.5-1.5mg bd)– CSCI: 2.5-5mg/24 hours
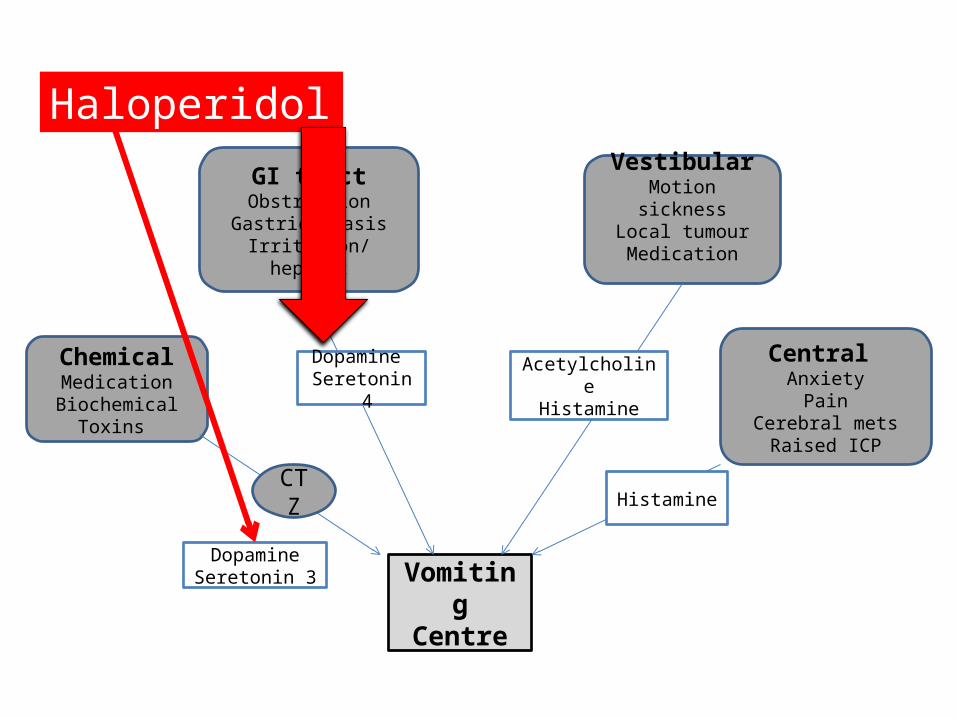
Vomiting
Centre
ChemicalMedicationBiochemical
Toxins
GI tractObstruction
Gastric stasisIrritation/hepatic
VestibularMotion sickness
Local tumourMedication
Central Anxiety
PainCerebral mets
Raised ICP
DopamineSeretonin 3
Dopamine Seretonin
4Acetylcholine
Histamine
HistamineCTZ
Haloperidol

If at first you don’t succeed
• Remember often multifactorial• Consider increasing dose• Consider combinations (that target diff
receptors)• Dex 4mg will often enhance affect anti-emetic
(unknown mech)• Levomepromazine

Vomiting
Centre
ChemicalMedicationBiochemical
Toxins
GI tractObstruction
Gastric stasisIrritation/hepatic
VestibularMotion sickness
Local tumourMedication
Central Anxiety
PainCerebral mets
Raised ICP
DopamineSeretonin 3
Dopamine Seretonin
4Acetylcholine
Histamine
HistamineCTZ
Levomepromazine
Chemotherapy Induced N&V
• Ondansetron often used• Best to time limit it’s use• Headaches • Constipation• Has a very specific role• Consider anticipatory n&v– Levomepromazine– Lorazapam
Case 2
• Break up into groups of 3-5• Look at the case and start to think about the
issues involved for 20 mins• Try to approach as holistically as possible• Feed back to group.

In summary
• A whistle stop tour of two pretty meaty subjects
• The importance of a thorough assessment in managing symptoms
• The importance of a systematic approach in managing them
• Make use of community SPCT/hospice advice lines if in doubt.

Any questions?

Watson, M. Lucas, C. Hoy, A. Wells, J (2010) The Oxford Handbook of palliative care. Oxford university press.
Twycross, R. Wilcock, A. Palliative care formulary 4th Edition (2012) Palliativedrugs.com
Groot, M. Vernooij-Dassen, M. Crul, B. Grol, R. (2005) General practitioners (GPs) and palliative care: percieved tasks and barriers in daily practice. J Pall Med. (19)111-118
Related Documents











