TVT(tension-free vaginal tape) TVT(tension-free vaginal tape) vs TOT(transobturator tape)- vs TOT(transobturator tape)- techniques for Female Stress techniques for Female Stress Urinary Incontinence Urinary Incontinence Eija Laurikainen Eija Laurikainen Department of Obstetrics and Department of Obstetrics and Gynecology, Turku University Gynecology, Turku University Central Hospital 23.9.-04 Central Hospital 23.9.-04

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript
TVT(tension-free vaginal tape) TVT(tension-free vaginal tape) vs TOT(transobturator tape)-vs TOT(transobturator tape)-techniques for Female Stress techniques for Female Stress
Urinary IncontinenceUrinary Incontinence
Eija LaurikainenEija Laurikainen
Department of Obstetrics and Department of Obstetrics and Gynecology, Turku University Gynecology, Turku University
Central Hospital 23.9.-04Central Hospital 23.9.-04
TOTTOToutside-in and inside-out outside-in and inside-out
techniquestechniques
Transobturator approach spares Transobturator approach spares retropubic spaceretropubic space
TVTTVT
• cure rates of approximately 87% ( Ulmsten 98, cure rates of approximately 87% ( Ulmsten 98, Olsson 99, Moran 2000, Nilsson 2001 and Nilsson Olsson 99, Moran 2000, Nilsson 2001 and Nilsson –03 IUGA 7 years follow-up)–03 IUGA 7 years follow-up)
• complications:complications:• perforation of the bladder 3.7-23%perforation of the bladder 3.7-23%• bleeding 0.8-3.3%bleeding 0.8-3.3%• voiding difficulty 1.5-17%voiding difficulty 1.5-17%• DE NOVO urge 2.5-25%DE NOVO urge 2.5-25%• some fatal peritonitis and fatal wounds of the large some fatal peritonitis and fatal wounds of the large
retroperitoneal vesselsretroperitoneal vessels

TVT and PU LigamentsTVT and PU Ligaments
• based on the integral based on the integral theory of stress theory of stress urinary incontinence, urinary incontinence, Ulmsten and Petros Ulmsten and Petros developed an developed an innovative technique innovative technique to compensate for the to compensate for the insufficiency of insufficiency of pubourethral pubourethral ligamentsligaments

The TOT Subfascial HammockThe TOT Subfascial Hammock
• restores anatomical restores anatomical pubourethral ligament pubourethral ligament support like the TVT support like the TVT Pubovaginal SlingPubovaginal Sling
TVT (dotted) TOT (solid)
TOTTOT & & NormalNormal PU LigamentPU Ligament
LA = Levator Ani U = Urethra V = Vagina
Why transobturator tape Why transobturator tape techniques?techniques?
• To reduce TVT complications; avoiding the To reduce TVT complications; avoiding the retropubic space reduces the risk of retropubic space reduces the risk of perforation of the bladder, bowel and major perforation of the bladder, bowel and major pelvic vesselspelvic vessels

Obturator AnatomyObturator Anatomy
Ischiopubic Ramus
IschiumPubic Symphysis
Obturator Obturator ForamenForamen
Obturator Canal
Ilium
Obturator canal
Urethra
SAFE ENTRY ZONE FOR NEEDLE INSERTION
Adductor longusinsertion
Obturator Nerve, Artery and Obturator Nerve, Artery and VeinVein
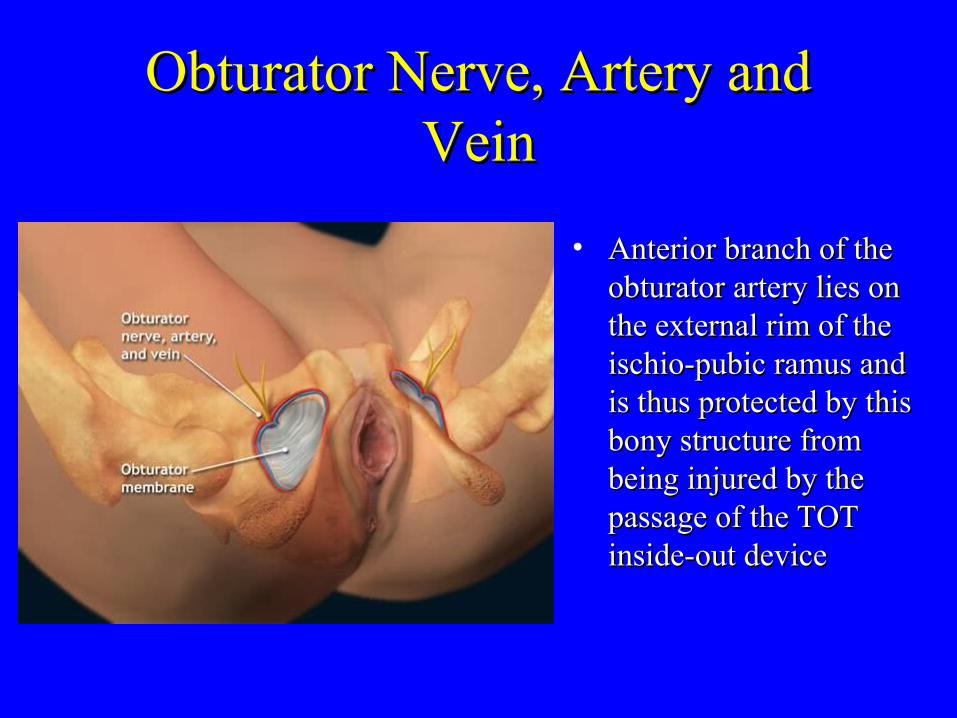
• Anterior branch of the Anterior branch of the obturator artery lies on obturator artery lies on the external rim of the the external rim of the ischio-pubic ramus and ischio-pubic ramus and is thus protected by this is thus protected by this bony structure from bony structure from being injured by the being injured by the passage of the TOT passage of the TOT inside-out deviceinside-out device
Femoral Nerve, Artery and VeinFemoral Nerve, Artery and Vein
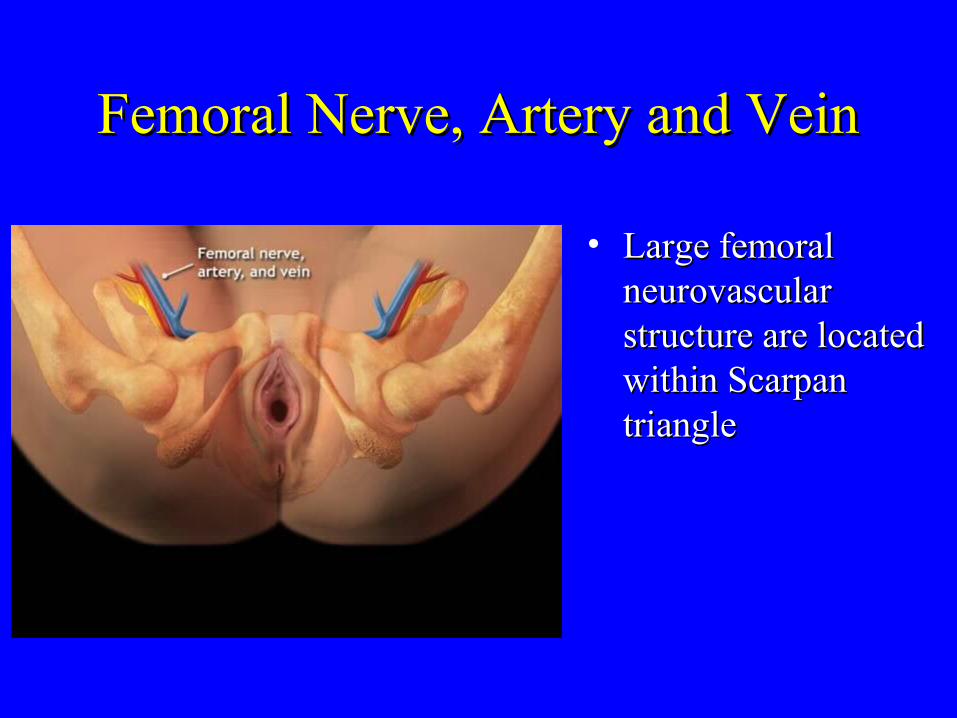
• Large femoral Large femoral neurovascular neurovascular structure are located structure are located within Scarpan within Scarpan triangletriangle

Outside-in Transobturator Approach Outside-in Transobturator Approach -developed by Dr Emmanuel -developed by Dr Emmanuel
Delorme 2001, FranceDelorme 2001, France
• Vaginal epithelium is Vaginal epithelium is dissected off dissected off underlying underlying periurethral fascia, periurethral fascia, dissect bilaterally to dissect bilaterally to the inferior pubic the inferior pubic ramusramus

Vaginal DissectionVaginal Dissection
Introduce fingertipIntroduce fingertip

Palpate Obturator Incision Palpate Obturator Incision PositionPosition
Identify internal edge Identify internal edge of obturator foramenof obturator foramen

Needle Path and Needle PlacementNeedle Path and Needle Placement
needle

Mesh Attachment and Needle Mesh Attachment and Needle RemovalRemoval

Inside-out Transobturator ApproachInside-out Transobturator Approach-developed by prof. Jean de Leval 2003, Belgium-developed by prof. Jean de Leval 2003, Belgium





Delorme et al.One year results of Delorme et al.One year results of TOT outside-in procedureTOT outside-in procedure
Prog.Urol.2003(4):656-659Prog.Urol.2003(4):656-659
• 32 pat.,mean age 6432 pat.,mean age 64
• urodynamics, 5 ISDurodynamics, 5 ISD
• 18 mixed inc.18 mixed inc.
• no prolapseno prolapse
• no intraop. complic.no intraop. complic.
• mean oper.time 15minmean oper.time 15min
• follow-up 17 monthsfollow-up 17 months
• 29/32 cured (90.6%)29/32 cured (90.6%)
• 3/32 improved (9.4%)3/32 improved (9.4%)
• 5/32 relative BOO5/32 relative BOO
• 1 ret.(4 weeks cathetr.)1 ret.(4 weeks cathetr.)
• 2 de NOVO URGE2 de NOVO URGE
• no erosionsno erosions
Costa et al.TOT( outside in)for Costa et al.TOT( outside in)for SUI:multicenter study, FranceSUI:multicenter study, France
• ICS 10/2003 FlorenceICS 10/2003 Florence• 7 centres, 165 patients7 centres, 165 patients• mean age 57 yearsmean age 57 years• 61% mixed incont.61% mixed incont.• urodynamics,5% ISDurodynamics,5% ISD• 15% recurrent inc.15% recurrent inc.• with or without associated with or without associated
prolapseprolapse• spinal (50), general (115)spinal (50), general (115)• follow-up 5 monthsfollow-up 5 months
• 1 bladder,2 urethral perf.1 bladder,2 urethral perf.
• 1 vaginal perforation1 vaginal perforation
• 5 pat. complained from 5 pat. complained from transient pain ( 13%)transient pain ( 13%)
• 4 (2.4%) post.op.ret.4 (2.4%) post.op.ret.
• 6 vaginal erosions 6 vaginal erosions
• 4% de NOVO URGE4% de NOVO URGE
• 1 urethral perf. later1 urethral perf. later
• cured 83%, failed 10%cured 83%, failed 10%
Jacquetin et al.Early Experience with Jacquetin et al.Early Experience with 120 Patients and TOT outside-in for 120 Patients and TOT outside-in for
Female SUI, 2004Female SUI, 2004
• 15 centers15 centers
• effectiveness obj./subj.effectiveness obj./subj.
• follow-up 3 monthsfollow-up 3 months
• operating time 20 minoperating time 20 min
• blood loss 32.4 mlblood loss 32.4 ml
• no hematomasno hematomas
• no perforationsno perforations
• 4 (3.3%) had surgical 4 (3.3%) had surgical revisions to release revisions to release sling tensionsling tension
• 4 (3.3%) urge sympt.4 (3.3%) urge sympt.
• 5 (4.2%) urinary inf.5 (4.2%) urinary inf.
• signif.impr. in QoLsignif.impr. in QoL
• cured: 2 (1.8%) cured: 2 (1.8%) recurrent incontinencerecurrent incontinence

de Leval New technique for de Leval New technique for treatment of SUI;TOT inside –treatment of SUI;TOT inside –
out.Eur Urol 2003:44(6):724-730out.Eur Urol 2003:44(6):724-730
• 107 patients107 patients
• mean age 62 yearsmean age 62 years
• urodynamics,74 SUIurodynamics,74 SUI
• spinal 82, general 24spinal 82, general 24
• 33 prolapse oper.33 prolapse oper.
• operating time 14 minoperating time 14 min
• no peroperat. complic.no peroperat. complic.
• 15.9% ( 17) pain in the 15.9% ( 17) pain in the thigh foldsthigh folds
• mean hospital stay 1.8 mean hospital stay 1.8 days(0.5-8)days(0.5-8)
• 3 ret.(2.8%), no 3 ret.(2.8%), no transectionstransections
• one vaginal erosionone vaginal erosion
• an abscess drainage at an abscess drainage at day 8day 8
• follow-up one monthfollow-up one month

Waltregny et al.Inside-out transobturator Waltregny et al.Inside-out transobturator vag. tape(TVT-O): short- term results of vag. tape(TVT-O): short- term results of
a prospect.study.ICS/IUGA 8/2004a prospect.study.ICS/IUGA 8/2004
• 53 patients53 patients• mean age 61 yearsmean age 61 years• urodynamics, 48 SUIurodynamics, 48 SUI• 6 ISD,12 concomitant 6 ISD,12 concomitant
prolapse operationsprolapse operations• 33 spinal, 20 general33 spinal, 20 general• follow-up over 6 follow-up over 6
months in all patientsmonths in all patients• 3 de NOVO URGE3 de NOVO URGE
• no vaginal, urethral or no vaginal, urethral or bladder perforationsbladder perforations
• no hematoma, vaginal no hematoma, vaginal or urethral erosion, or urethral erosion, fistula or tape reject.fistula or tape reject.
• pain in thigh regionpain in thigh region• 3 ret.,2 tape transect.3 ret.,2 tape transect.• cured:94.3%,1 improv.cured:94.3%,1 improv.• QoL: signif. improv.QoL: signif. improv.
Mellier et al.Suburethral tape via the Mellier et al.Suburethral tape via the obturator route: is the TOT a obturator route: is the TOT a
simplification of the TVT? Int simplification of the TVT? Int Urogynecol J (2004)15:227-232Urogynecol J (2004)15:227-232
• retrospect.,non-retrospect.,non-random.,non-concurr.random.,non-concurr.
• 99 TVT, 2/3 local99 TVT, 2/3 local
• 94 TOT, 2/3 spinal94 TOT, 2/3 spinal
• urodynam.,no prolapseurodynam.,no prolapse
• clinical evaluation at 6-8 clinical evaluation at 6-8 weeksweeks
• follow-up 30/13 months follow-up 30/13 months via telephonevia telephone
• TVT:bladder perf. TVT:bladder perf. 10%,vaginal 4%10%,vaginal 4%
• TOT:1 urethral perf.TOT:1 urethral perf.
• TVT 8 hemorrh.TOT 2TVT 8 hemorrh.TOT 2
• TVT 2 hematomasTVT 2 hematomas
• TOT 1 vaginal erosionTOT 1 vaginal erosion
• TVT de NOVO URGE TVT de NOVO URGE 3%,TOT 4%3%,TOT 4%
• cure:TVT 91%,TOT 95%cure:TVT 91%,TOT 95%

de Tayrac et al.A prospective de Tayrac et al.A prospective randomized trial comparing TVT and randomized trial comparing TVT and
TOT for SUI.Am J Obstet TOT for SUI.Am J Obstet Gynecol(2004)190, 602-608Gynecol(2004)190, 602-608
• TVT 31,TOT 30TVT 31,TOT 30
• 1-year outcome1-year outcome
• spinal or general anesth.spinal or general anesth.
• urodynamics, SUIurodynamics, SUI
• no prolapseno prolapse
• no cystoscopy, indigo no cystoscopy, indigo carmine i.v.(TOT)carmine i.v.(TOT)
• operating time:TVT 27 operating time:TVT 27 min and TOT 15 minmin and TOT 15 min
• bladder perf.: TVT 9.3%, bladder perf.: TVT 9.3%, TOT 0%TOT 0%
• urethral erosions:TVT 1, urethral erosions:TVT 1, TOT 0TOT 0
• no vaginal erosionsno vaginal erosions
• obturator hematoma: TVT 0, obturator hematoma: TVT 0, TOT 1TOT 1
• tape transection(ret.): TVT 0, tape transection(ret.): TVT 0, TOT 1TOT 1
• cure:TVT 84%,TOT 90%cure:TVT 84%,TOT 90%

Delmas et al.TOT(outside-in) in the Delmas et al.TOT(outside-in) in the treatment of Female SUI:Anatomical treatment of Female SUI:Anatomical
dangers.Eur Urol Suppl 2003;2(1):197dangers.Eur Urol Suppl 2003;2(1):197
• 10 female cadavers10 female cadavers
• when the tunneler is entered more when the tunneler is entered more anteriorly, there is a danger for a superior anteriorly, there is a danger for a superior passage and perforation of the anterior passage and perforation of the anterior aspect of the bladder ; when the tunneler is aspect of the bladder ; when the tunneler is entered more posteriorly, perforation of the entered more posteriorly, perforation of the vagina is possible as urethral perforationvagina is possible as urethral perforation

Transobturator techniqueTransobturator technique
• may eliminate vascular, bladder and bowel may eliminate vascular, bladder and bowel injuriesinjuries
• avoids retropubic scarringavoids retropubic scarring• may prove useful in patients with earlier may prove useful in patients with earlier
retropubic proceduresretropubic procedures• offers minimal blind perineal needle offers minimal blind perineal needle
passagepassage• may prove useful in obese patientsmay prove useful in obese patients

Transobturator techniqueTransobturator technique
• offers short-term efficacy similar to TVToffers short-term efficacy similar to TVT
• offers shortened procedure timeoffers shortened procedure time
• may prove useful in treatment failures?may prove useful in treatment failures?
• may eliminate the need for cystoscopy?may eliminate the need for cystoscopy?
• easy to learneasy to learn

With the transobturator technique the tape is With the transobturator technique the tape is inserted at a 45 angle to the vertical and inserted at a 45 angle to the vertical and horizontal planes. A narrower angle, such horizontal planes. A narrower angle, such as that which occurs with the TVT, can as that which occurs with the TVT, can contribute to difficult micturition? TOT: contribute to difficult micturition? TOT: fewer voiding difficulties, urinary retention fewer voiding difficulties, urinary retention and urge symptoms?and urge symptoms?

ConclusionConclusion
• The U-shaped placement of the TVT-tape The U-shaped placement of the TVT-tape can contribute to long-term efficacy?can contribute to long-term efficacy?
• Prospective, randomized study between Prospective, randomized study between tension-free vaginal tape and a new tension-free vaginal tape and a new transobturator procedure is needed with transobturator procedure is needed with longer follow-up times.longer follow-up times.
Related Documents