Research Article Turning Disaster into an Opportunity for Quality Improvement in Essential Intrapartum and Newborn Care Services in the Philippines: Pre- to Posttraining Assessments M. S. Castillo, 1 M. A. Corsino, 2,3 A. P. Calibo, 4 W. Zeck, 1,5 D. S. Capili, 2 L. C. Andrade, 6 K. A. Reyes, 2,7 R. C. Alfonso, 2 M. B. Ponferrada, 1 and M. A. Silvestre 2 1 UNICEF Philippines, 1200 Makati, Philippines 2 Kalusugan ng Mag-Ina, Inc. (Health of Mother and Child), 1103 Quezon City, Philippines 3 Remedios T. Romualdez Medical Foundation (RTRMF), College of Medicine, 6500 Tacloban, Philippines 4 Department of Health Disease Prevention and Control Bureau, 1003 Manila, Philippines 5 Department of Obstetrics and Gynaecology, Medical University of Graz, 8010 Graz, Austria 6 Department of Health Regional Health Office 8 (Eastern Visayas), Palo, 6501 Leyte, Philippines 7 Alliance for Improving Health Outcomes Inc., 1104 Quezon City, Philippines Correspondence should be addressed to M. S. Castillo; [email protected] Received 30 October 2015; Revised 9 March 2016; Accepted 20 April 2016 Academic Editor: Ying-Ru Lo Copyright © 2016 M. S. Castillo et al. is is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited. Background. On 8 November 2013, supertyphoon Haiyan made landfall in the Philippines, severely disrupting health service delivery. Reestablishment of essential services for birthing mothers and their newborns became high priority. Methodology. Following a baseline assessment, an Essential Intrapartum and Newborn Care (EINC) training package was implemented and posttraining assessments (1 and 3 months aſter training) were undertaken. Results. Baseline assessments ( = 56 facilities) revealed gaps in provider’s skill and shortage of life-saving commodities. Facilities lacked newborn bags/masks (9%), towels (6%), and magnesium sulfate (39%). Service providers lacked skills in partograph use (54%), antenatal steroid (44%) use, and breastfeeding initiation (50%). At 3 months aſter training ( = 51 facilities), dramatic increases in correct partograph use (to 92%), antenatal steroid use (to 98%), breastfeeding initiation (to 86%), kangaroo mother care (to 94%), availability of magnesium sulfate (to 94%), and bag/masks (to 88%) were documented. Gaps persisted for skills in assisted vaginal delivery and removal of placental fragments. Conclusion. Health services were severely disrupted aſter supertyphoon Haiyan. Our study demonstrates that essential birthing services and quality improvements to strengthen local health systems can be restored in a timely manner even in immediate postdisaster settings. 1. Introduction Supertyphoon Haiyan made landfall in the Philippines on November 8, 2013, with most of the damages sustained in the central part of the country. 14.1 million people were affected, mostly in Eastern Visayas (Region 8), followed by Central Visayas (Region 7) and Western Visayas (Region 6) [1]. Immediate response efforts for vast areas ravaged by Haiyan were extremely difficult, due to breakdown of transportation and communication infrastructure, and consisted largely of provision of food and water, infant and child feeding, and triage and treatment for traumatic injuries and acute medical illnesses [2, 3]. Demand for health services surged as complete devastation of health infrastructure, logistics, and human resources rendered the local health system unable to respond. National and local government and interagency assessments immediately aſter the typhoon identified the reestablishment of health services for mothers and children, particularly primary and secondary care for obstetric emer- gencies, as a priority. e Emergency Health Cluster led by the Department of Health (DOH) (co-led by the World Health Organization, WHO) provided recommendations Hindawi Publishing Corporation BioMed Research International Volume 2016, Article ID 6264249, 9 pages http://dx.doi.org/10.1155/2016/6264249

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

Research ArticleTurning Disaster into an Opportunity for Quality Improvementin Essential Intrapartum and Newborn CareServices in the Philippines Pre- to Posttraining Assessments
M S Castillo1 M A Corsino23 A P Calibo4 W Zeck15 D S Capili2 L C Andrade6
K A Reyes27 R C Alfonso2 M B Ponferrada1 and M A Silvestre2
1UNICEF Philippines 1200 Makati Philippines2Kalusugan ng Mag-Ina Inc (Health of Mother and Child) 1103 Quezon City Philippines3Remedios T Romualdez Medical Foundation (RTRMF) College of Medicine 6500 Tacloban Philippines4Department of Health Disease Prevention and Control Bureau 1003 Manila Philippines5Department of Obstetrics and Gynaecology Medical University of Graz 8010 Graz Austria6Department of Health Regional Health Office 8 (Eastern Visayas) Palo 6501 Leyte Philippines7Alliance for Improving Health Outcomes Inc 1104 Quezon City Philippines
Correspondence should be addressed to M S Castillo mscastillouniceforg
Received 30 October 2015 Revised 9 March 2016 Accepted 20 April 2016
Academic Editor Ying-Ru Lo
Copyright copy 2016 M S Castillo et al This is an open access article distributed under the Creative Commons Attribution Licensewhich permits unrestricted use distribution and reproduction in any medium provided the original work is properly cited
Background On 8 November 2013 supertyphoon Haiyan made landfall in the Philippines severely disrupting health servicedelivery Reestablishment of essential services for birthing mothers and their newborns became high priority MethodologyFollowing a baseline assessment an Essential Intrapartum and Newborn Care (EINC) training package was implemented andposttraining assessments (1 and 3 months after training) were undertaken Results Baseline assessments (119899 = 56 facilities) revealedgaps in providerrsquos skill and shortage of life-saving commodities Facilities lacked newborn bagsmasks (9) towels (6) andmagnesium sulfate (39) Service providers lacked skills in partograph use (54) antenatal steroid (44) use and breastfeedinginitiation (50) At 3 months after training (119899 = 51 facilities) dramatic increases in correct partograph use (to 92) antenatalsteroid use (to 98) breastfeeding initiation (to 86) kangaroo mother care (to 94) availability of magnesium sulfate (to94) and bagmasks (to 88) were documented Gaps persisted for skills in assisted vaginal delivery and removal of placentalfragments Conclusion Health services were severely disrupted after supertyphoon Haiyan Our study demonstrates that essentialbirthing services and quality improvements to strengthen local health systems can be restored in a timelymanner even in immediatepostdisaster settings
1 Introduction
Supertyphoon Haiyan made landfall in the Philippines onNovember 8 2013 with most of the damages sustained in thecentral part of the country 141 million people were affectedmostly in Eastern Visayas (Region 8) followed by CentralVisayas (Region 7) and Western Visayas (Region 6) [1]Immediate response efforts for vast areas ravaged by Haiyanwere extremely difficult due to breakdown of transportationand communication infrastructure and consisted largelyof provision of food and water infant and child feeding
and triage and treatment for traumatic injuries and acutemedical illnesses [2 3] Demand for health services surged ascomplete devastation of health infrastructure logistics andhuman resources rendered the local health system unableto respond National and local government and interagencyassessments immediately after the typhoon identified thereestablishment of health services for mothers and childrenparticularly primary and secondary care for obstetric emer-gencies as a priority The Emergency Health Cluster ledby the Department of Health (DOH) (co-led by the WorldHealth Organization WHO) provided recommendations
Hindawi Publishing CorporationBioMed Research InternationalVolume 2016 Article ID 6264249 9 pageshttpdxdoiorg10115520166264249
2 BioMed Research International
and supported appropriate humanitarian responses Amongthe WHO endorsed interventions for saving the lives ofmothers and children is the so-called Essential Intrapartumand Newborn Care (EINC) a package of cost-effective time-bound interventions [4] In the Philippines EINC (popularlyknown as ldquoUnang Yakaprdquo or the First Embrace) is imple-mented and mainstreamed in practice protocols or tools [5]following quality improvement principles [6] The develop-ment of this standardized protocol was triggered by datafrom observational assessments in 51 government hospitalsin the Philippines revealing that practices in the immediatenewborn care period were undermining thermoregulationand breastfeeding initiation of newborns [7]The importanceof providing quality care forwomenduring labor and deliveryand implementation of safe practices for their newborns toensure their best outcomes became paramount [8] Prior totyphoon Haiyan implementation of the EINC Protocol wasbeing undertaken only in selected government hospitals andprimary level facilities (rural health units and district hospi-tals) Inequity and systembarriers to bring implementation toscale persisted despite national health policies being in place[9] Neonatal mortality rate (NMR) reported in the NationalDemographic and Health Survey (NDHS 2013) [10] was 13per 1000 live births nationally and 15 18 and 10 per 1000live births in Western Central and Eastern Visayas regionsrespectively
When a 72 magnitude earthquake jolted the provinceof Bohol in the Visayas region one month prior to typhoonHaiyan WHO supported the rapid building of health workercapacity for maternalnewborn care in a postdisaster settingEINC training packages were updated to incorporate newWHO guidelines on basic newborn resuscitation and post-natal care of mothers and newborns including magnesiumsulfate administration to address gaps in care After a pilotimplementation in Bohol province the trainingmoduleswiththe expanded content were endorsed byWHO for utilizationin postdisaster areas where similar needs existed
The aim of this intervention was to support the reestab-lishment of health care services for birthingmothers and theirnewborns in the areas affected by typhoon Haiyan guided byquality improvement principles Specific objectives were to
(1) conduct EINC training of trainers (TOT) and qualityassurance (QA) workshops in target areas withinEastern Central and Western Visayas regions toaddress gaps identified in the baseline assessment
(2) and undertake rapid assessments of EINC servicesusing a standard tool at baseline and at 1 and 3monthsafter the training
2 Materials and Methods
Based on a multistage vulnerability analysis UNICEF andpartners identified forty (40) prioritymunicipalities along thepath of typhoon Haiyan where the humanitarian responsewould be intensified during the period from February toSeptember 2014
This multistage vulnerability analysis entailed severalstages in the first stage an initial list of 120 areas (cities
and municipalities) was constituted based on preliminarydata from the Philippines National Disaster Risk Reduc-tion and Management Council (NDRRMC) and UnitedNations Office for the Coordination of Humanitarian Affairs(OCHA) Criteria used were (a) areas with 95 and aboveaffected population (b) areas given typhoon signal number4 and (c) areas with highest potential for storm surgeTyphoon storm signal number 4 signifies a very intensetyphoon with winds of more than 185 kph speed [11] Inthe second stage official data such as detailed populationpre- and post-Haiyan poverty incidence and local data wereincorporated In the third stage convergence of UNICEFinterventions in the sectors of health nutrition educationchild protection and water sanitation and hygiene (WASH)were analyzed to find the ldquobestrdquo model for prioritizationof areas In the fourth and final stage the 40 prioritymunicipalities were identified based on cumulative affectedpopulation that would yield optimal coverage in relation toUN strategic response plan targets developed with the Philip-pine government These were in Eastern Visayas (Region8) in the province of LeytemdashTacloban City Palo TanauanDulag Burauen Dagami La Paz Julita Tabontabon Cari-gara Jaro San Miguel Alangalang Pastrana Mayorga andMacArthur in the provinces of Eastern andWestern SamarmdashGuiuan Salcedo Hernani Mercedes Balangiga GiporlosLawaan Quinapondan Balangkayan Borongan City andMarabut Those included in Western Visayas (Region 6)were in the province of CapizmdashPontevedra Pilar PresidentRoxas Maayon Ivisan Panay Panitan and Jamindan inthe province of IloilomdashConcepcion Sara and Estancia InCentral Visayas (Region 7) Bantayan and Daanbantayanmunicipalities in the province of Cebu were included Tech-nical experts from a local nongovernmental organization(NGO Kalusugan ng Mag-Ina or ldquoHealth of Mother andChildrdquo) were engaged to roll out the EINC implementationand quality improvement capacity buildingtraining activitiesin priority municipalities from February to September 2014In 2011 the same NGO provided the technical assistance inthe pilot implementation of EINC in the Eastern VisayasRegional Medical Center in Leyte and the subsequent train-ing of trainers and quality assurance workshop cascaded bythe Region 8 Health Office for all Eastern Visayas provincesin 2012
The methodology to facilitate the capacity building ofhealth workers in the forty (40) priority municipalities con-sisted of a training of trainers and cascade quality assurance(QA) workshops with rapid assessment before the trainingand at one and three months posttraining (see Figure 1)
Using the ldquoNewborn Services Rapid Health FacilityAssessmentrdquo tool that was developed by the InteragencyNewborn Indicators Technical Working Group as a template[12] rapid facility assessments were done at baseline (beforetraining) and at one month and three months after train-ing Technical experts acting as external assessors used theidentical tool to conduct pre- and posttraining assessmentsduring facility visits External assessors performed ocularsurveys of the access and quality of the labor-delivery andpostpartum environments equipment supplies and patientpathways Information was collected through interviews of
BioMed Research International 3
Baseline assessment
EINC training of
trainers (TOT)
Training via EINC QA workshops
1-monthposttrainingassessments
3-monthposttrainingassessments
Figure 1 Flow of assessments and interventions
health workers and mothers supplemented by review ofrecords Whenever possible deliveries were observed
In the priority municipalities primary level health facili-ties with the highest number of deliveries were intentionallyselected Based on usual patient traffic the biggest districthospital or rural health unit (RHU) and its correspondingbusiest lying-in clinic were selected subject to the limitedaccessibility of facilities after typhoon Haiyan In consider-ation of service delivery networks and referral flows withinand across municipalities assessments covered additionalmunicipalities beyond the 40 priority areas
The tool was used to assess facility-based delivery andnewborn care service capacity in primary and referral levelfacilities Gaps in newborn care health services were sys-tematically identified using tracer indicators Findings wereutilized to describe capacity to address three main causesof newborn deaths asphyxia prematurity and infectionDeterminants were classified as (a) service availability (b)equipment and supplies and (c) service standards
21 EINC Training of Trainers Updated EINC training mod-ules contained brief didactic sessions on basic topics Essen-tial Intrapartum and Newborn Care breastfeeding supportkangaroo mother care Infant and Young Child Feeding inEmergencies (IYCF-E) partograph use and the recentWHOrecommendations on basic newborn resuscitation correctadministration of magnesium sulfate and postnatal care ofmothers and newborns Skills sessions consisted of ldquocoachingsessionsrdquo with demonstrationreturn demonstrations usingmanikins and delivery kits Workshops culminated withaction planning sessions on effective mainstreaming of EINCin their practice These planning sessions allowed the partic-ipants to voice out their concerns and their apprehensionsand discuss among themselves ways to contextualize thesechallenges and address them
Training of trainers (TOT) workshops were conductedin the three regions Selection of trainees was strategic toinclude senior health care workers with aptitude to becometrainers in their respective service delivery networks (roughlycorresponding to geopolitical Interlocal Health Zones orILHZs) Representation of involved ILHZs was ensured asmuch as possible to create a pool of trainers to cascadethe training locally Local trainers were further chosen fromthis pool based on their performance during the TOT
Participants included thirty (30) trainees each from LeyteEastern and Western Samar Capiz Iloilo and Cebu
22 Cascade EINC Quality Assurance Workshops The tech-nical experts supervised and mentored the new local trainersas they implemented their own cascade quality assurance(QA) workshops In each of the areas two QA workshopsof 30 participants each were conducted targeting a totalof 300 capacitated skilled birth attendants QA workshopmodules for service providers were delivered over 6 half-daysessions Pre- to postworkshop acquisition of knowledge wasmeasured through 15 item multiple choice question writtenquizzes and acquisition of skills in the classroom assessmentsthrough performance checklists
23 Statistical Analysis Epi Info 6 was used for dataanalysis Categorical variables at baseline 1-month and 3-month after training presented as proportions () werecompared using Fisherrsquos exact and 1205942 tests with significanceset at 119901 lt 005
3 Results and Discussion
External experts supported the rehabilitation of EINC healthservices in 40 priority municipalities in Eastern Central andWesternVisayas severely devastated byHaiyan (See Figure 2)
As part of the service delivery networks additional areasadjacent to the priority municipalities were included namelyfour (4)municipalities and one city (Abuyog andOrmoc Cityin Leyte Basey in Western Samar and Barotac Viejo andBalasan in Iloilo) The grand total of 45 local governmentunits (LGUs) thus included three (3) cities (in Leyte) andforty-two (42) municipalities (see Figure 3)
31 Baseline Assessments (Table 1) Baseline rapid assess-ments were done at 16 weeks after landfall in Eastern Visayas(Leyte and Eastern and Western Samar) 20 weeks afterlandfall in Western Visayas (Iloilo and Capiz) and 22 weeksafter landfall in Central Visayas (Cebu) A total of 56 healthfacilities were assessed at baseline Assessments revealed sig-nificant disruption in obstetric and newborn health servicesin Eastern Visayas and much less significant disruption inCentral and Western Visayas
4 BioMed Research International
Figure 2 Path of typhoon Haiyan through central Philippines [15]
At baseline health facilities assessed ranged from ruralhealth units (RHU 39) first level referral hospitals (15community district and city hospitals) and in addition2 provincial hospitals with birthing services After typhoonHaiyan the physical devastation in Eastern Visayas causedthe most serious interruptions in EINC delivery Immediateresponse services were provided primarily through contri-butions from international partners in tents and makeshiftfacilities The lack of availability of 247 delivery servicesrevealed the importance of improved referral mechanismsthat could bring mothers experiencing complications duringor after birth to a higher level facility if neededThese findingsdiffered from the assessment of Central and Western Visayasmunicipalities where facilities mostly sustained partial dam-age with no interruption of birthing services
Apart from damage to infrastructure commodities werein serious shortage or absent with stock-outs of life-savingdrugs (eg oxytocin magnesium sulfate and dexametha-sone) Health human resources suffered serious setbacksnot only due to substantial loss of lives among health careproviders but also due to lack of training and technicalcapacity (in basic newborn resuscitation care of the low birthweight kangaroo mother care breastfeeding and Infant andYoung Child Feeding in Emergencies (IYCF-E)) In facilitieswhere health workers had participated in a previous 11-dayBasic Emergency Obstetric and Newborn Care (BEmONC)training low self-efficacy ratings especially in partographuse magnesium sulfate administration and newborn resus-citation rates were noted Very few facilities experiencedsupervisory visits in the previous 6 months None performedroutine postnatal care services Documentation of practiceswas weak Finally not all facilities conducted regular mater-nal and newborn death reviews
Table 1 Number of facilities assessed at pretraining (baseline) andat 1 month and 3 months posttraining by region and by province
RegionprovinceFacility level
Rural healthunit
First levelhospital
Provincialhospital
Eastern VisayasLeyteBaseline 15 4 11 month 16 5 13 months 12 4 1
SamarBaseline 11 4 11 month 11 4 13 months 10 4 0
Western VisayasCapizBaseline 3 3 01 month 3 3 03 months 3 3 0
IloiloBaseline 8 2 01 month 8 2 03 months 8 2 0
Central VisayasCebuBaseline 2 2 01 month 2 2 03 months 2 2 0
Progress in EINC implementation and quality improvement from baselineassessments through 1- and 3-month posttraining assessments
32 EINC Training of Trainers (TOT) Out of 150 candidatetrainers who were invited 112 (75) attended the trainingThese were maternal and child health workers holding strate-gic positions (provincial level program managers hospitalspecialists municipal health officers public health nursesandmidwife supervisors) A total of five (5) training of trainer(TOT) workshops of 3 daysrsquo duration each were conductedone each for the provinces of Leyte Eastern and WesternSamar Iloilo Capiz and Cebu
33 Cascade EINC QA Workshops As part of the trainingrequirement each TOT candidate trainer participated in atleast one of a total of ten (10) cascade QA workshops fortheir colleagues with supportive supervision and technicaloversight from expert trainers A total of 281 out of 300targeted skilled birth attendants (937) were further trained
Thus a total of 393 health workers completed EINCworkshops over this period 281 completed their participationin 3-day QA workshops and 112 attended the five TOT work-shops Consistent improvements in posttraining assessmentquizzes and performance checklists for both the TOT andQAworkshop participants were noted
BioMed Research International 5
Bukidnon
Sulu Sea
LeyteIloilo
Cebu
Samar
Bohol
Capiz
Negros Occidental
Albay
Masbate
Antique
Negros Oriental
Aklan
Eastern Samar
Sorsogon
Northern Samar
Agusan del Sur
Agusan del Norte
Misamis Oriental
QuezonCamarines Sur
Marinduque
Biliran
Romblon
Southern Leyte
Surigao del Norte
Guimaras
Dinagat Islands
Zamboanga del Norte
SiquijorSurigao del Sur
Misamis Occidental
Camiguin
Catanduanes
Bohol Sea
Philippine Sea
Sibuyan Sea
Visayan Sea
Samar Sea
Leyte Gulf
Ragay Gulf
Surigao Strait
Tayabas Bay
Map shows PhilippinesUNICEF Haiyan programmeareas and typhoon Haiyanpath
Disclaimer the boundaries and names shown and the designations used in this map do not imply official endorsement or acceptance by the United Nations
0 10 20 30 405(Kilometers)
Data source UNICEFDate of data source 14 Dec 2014Map sources NE COD GADMMap production date 06 March 2016Feedback jbacaluniceforg
ScaleProgramme areas
HaiyanTyphoon Haiyan path
VIII
VIIVI
Capiz
IloiloVI IloiloVI IloiloVIVI
CapizVICapizVICapizVICapizVICapizVICapizVICapizVICapizVICapizVI
Iloilo
CebuVII CebuVII Cebu
Eastern SamarVIII Eastern SamarVIII Eastern SamarVIII Eastern SamarVIII Eastern SamarVIII Eastern SamarVIII Eastern SamarVIII Eastern SamarVIII Eastern SamarVIIIVIII
Eastern Samar
Samar
LeyteVIII LeyteVIII LeyteVIII LeyteVIII LeyteVIII LeyteVIII LeyteVIII LeyteVIII LeyteVIII LeyteVIII LeyteVIII LeyteVIII LeyteVIII LeyteVIII LeyteVIII LeyteVIII LeyteVIII LeyteVIII LeyteVIII LeyteVIII LeyteVIII
IvisanJamindanMa-AyonPanayPanitanPilarPontevedraPresident RoxasRoxas CityTapazCarlesConcepcionEstanciaSaraBantayanCebu CityDaanbantayanBalangigaBalangkayanBorongan CityGiporlosGuiuanHernaniLawaanMercedesQuinapondanSalcedoAlangalangBurauenCarigaraDagamiDulagIsabelJaroJulitaKanangaLa PazMacarthurMatag-ObMayorgaMeridaPaloPastranaSan MiguelTabontabonTacloban CityTanauanVillabaMarabut
998400Region 4B
998400Region 4A
998400Region 5
998400Region 8
998400Region 6
998400Region 7
998400Region 9
998400Region 10
998400Region Caraga
1 cm = 16km
Region Province Municipilaty
Philippines UNICEF Haiyan programme areas
N
Figure 3 40 priority municipalities listed in orange box and shaded in map
6 BioMed Research International
96 98 98 98
16 22
17 96 98
94
0 10()
20 30 40 50 60 70 80 90 100
Service availability indicators at baseline and at 1- and 3-month posttraining assessment in Eastern Western and
Central Visayas Philippines 2013
3-month PTA 1-month PTA Baseline
Kangaroo mother carelowastAntenatal steroidslowast
Neonatal resuscitationlowast
Manual removal of retained products after deliveryManual placental removal
Assisted vaginal deliveryParenteral magnesium sulfatelowast
Parenteral oxytocinlowast
Parenteral antibioticslowast247 skilled birth attendancelowast
lowastIndicates significant change from baseline to 3-month PTA p lt 005
Figure 4 Proportion of facilities assessed providing various services at pretraining (baseline) and at 1 and 3 months posttraining assessment(PTA) Eastern Western and Central Visayas post-Haiyan
34 Posttraining Assessments (Table 1) At 1 month and 3months after training field visits to 58 and 51 facilities respec-tively were carried out The facilities that completed the 3assessments were thirty-five (35) rural health units (RHUs)15 primary level hospitals (13 district 1 city and 1 communityhospitals) and one (1) provincial hospital These field visitsrevealed that uptake of EINC knowledge and skills was trans-lated to significant changes in daily practice Posttrainingassessment visits revealed good evidence of changes in thephysical environments in the labordelivery and postpartumareas and implementation of many of the EINC practices
However apart from the overall improvement someposttraining gaps were identified (1) not allowing a com-panion of choice (2) nonadministration of birth dosesof BCG vaccine (3) unavailability of nevirapine therapy(4) unavailability of protocols or guidelines for IntegratedManagement of Pregnancy and Childbirth (IMPAC) referralof sick newborns Comprehensive Emergency Obstetric andNewborn Care (CEmONC) and preterm labormanagement(5) absence of soap and hand disinfectants in postnatal areas
35 Service Availability (Figure 4) In Eastern Visayas theworst hit region baseline assessment revealed that 27 of 36facilities were providing birthing services At 1 month aftertraining 32 of 38 assessed birthing facilities were providinground-the-clockdaily (247) skilled birth attendance (SBA)At 3 months 30 of 31 birthing facilities were providing 247SBA InWesternVisayas 16 of 16 facilities were able to sustaindelivery services at baseline and 1 month assessments Onefacility suspended its delivery services to undergo renova-tions at the 3-month assessment All of the 15 other facilitieswere providing 247 SBA In Central Visayas all 4 facilitiesassessed were providing 247 SBA at baseline 1-monthand 3-month assessments Over the period from baselineassessment to 3 months after training there were significantimprovements in self-reported availability of services such as
neonatal resuscitation kangaroomother care administrationof parenteral oxytocin antibiotics antenatal steroids andmagnesium sulfate In contrast persistent gaps remainedfor assisted vaginal delivery manual placental removal andmanual removal of retained products after delivery In Figures4ndash6 the proportion of facilities () at end line (3months aftertraining) is labeled
36 Equipment and Supplies (Figure 5) Over the period frombaseline assessment to 3 months after training (20-week 19-week and 14-week periods for Eastern Western and Cen-tral Visayas resp) there were significant improvements inavailability of life-saving drugs (ie oxytocin) and equipment(ie for resuscitation) most notably for Eastern and CentralVisayas For Western Visayas some improvements were seenin the facilities but the limited availability of equipmentconstrained the appropriate delivery of services Not all life-saving drugs were available in all facilities especially antibi-otics and steroids
Though there was significant improvement persistentgaps remained for antenatal steroids injectable gentamicinand magnesium sulfate supplies Towels for drying werestill being provided by families instead of by facilitiesNevirapine for prevention of mother-to-child transmissionof HIV remained unavailable across all regions MultidoseBCG vaccines were available but considered ldquoinsufficientrdquo byhealth workers Many facilities had moved their weighingscales from their delivery areas to their maternity careareas for deferred weighing until after the first breastfeedas recommended in EINC protocols Protocols for IMPACsick newborn carereferral preterm labor management andCEmONCmanuals remain unavailable
37 Service Standards (Figure 6) In addition to parametersincluded in the Newborn Care Services Rapid AssessmentTool selected parameters relevant to the Philippines EINC
BioMed Research International 7
69 88
86 96
84 4
73 2
57 98
71
0 10 20 30 40 50()
60 70 80 90 100
Equipment and supplies availability at baseline and at 1- month and 3-month posttraining assessment in Eastern
Western and Central Visayas Philippines 2013
3-month PTA 1-month PTA Baseline
Magnesium sulfateInjectable uterotoniclowast
CorticosteroidsPMTCT drugslowast
Injectable gentamicinTowels for drying
Soap or hand disinfectantInfant scalelowast
lowastResuscitation tableNewborn bag and masklowast
Up-to-date delivery register
lowastIndicates significant change from baseline to 3-month PTA p lt 005
Figure 5 Proportion of facilities assessed to have various equipment and supplies at pretraining (baseline) and at 1 and 3months posttrainingassessment (PTA) Eastern Western and Central Visayas post-Haiyan
87 58
96 84
0 98 98
86 80
84 82
92 76
70 72
70
0 10 20 30 40 50()
60 70 80 90 100
Service standards indicators at baseline and at 1-month and 3-month posttrainingassessment in Eastern Western and Central Visayas Philippines 2013
Companion of choiceAllowed to eatdrink
Selective episiotomyperineal supportAMTSLlowast
Partograph filled out correctlylowast
Immediatethorough dryingSkin-to-skin contact
Properly timed cord clampingNonseparation and initiation of Breastfeeding
Eye carelowast
Vitamin Klowast
BCG birth doseHepatitis B birth dose
Wall clock in delivery arealowast
Room thermometer in delivery arealowast
Size 0 or preterm masklowast
3-month PTA 1-month PTA Baseline
lowastIndicates significant change from baseline to3-month PTA p lt 005
Figure 6 Proportion of facilities assessed to be implementing various service standards at pretraining (baseline) and at 1 and 3 monthsposttraining assessment (PTA) Eastern Western and Central Visayas post-Haiyan
8 BioMed Research International
Protocol and Basic Emergency Obstetric and Newborn Care(BEmONC) services standards were assessed through inter-views of health service providers
Significant improvements in service standards usingtracer indicators were noted across all regions over the periodfrom pretraining assessment to the 3 months posttrainingassessment Most notable were performance of the EINCldquocore stepsrdquo in immediate newborn care proper WHOpartograph use and availability of size 0 face masks forresuscitation of preterms which improved from 0 to 100at 3 months posttraining assessment
Quality labor and delivery for mothers (companion ofchoice allowing mothers to eatdrink semiupright deliverybed perineal support and restrictive episiotomy and activemanagement of the third stage of labor) and quality post-partum care (monitoring vital signs uterine massage andpostpartum visit within first week and then within fourthto sixth weeks after discharge) were carried out Facilitiesreported performance of the ldquocore stepsrdquo of immediatenewborn care (immediate and thorough drying skin-to-skincontact properly timed cord clamping and nonseparation ofnewborn from mother for early breastfeeding) and routinenewborn care (eye care physical examination and vitamin Kadministration) Postpartumwomen interviewed in the facil-ities verified the consistency of applying the EINC protocol
A persistent gap in EINC standard practice was the birthdose of BCG vaccine Ninety-six percent of facilities were notadministering this birth dose as recommended by nationalguidelines citing that using the available multidose vials foronly a few patients at each time constitutes ldquowastagerdquo Thisreflects the common practice of deferring the BCG vaccina-tion to the first-postnatal visit in the Philippines Number ofroom thermometers and wall clocks had increased in somefacilities
UnlikeWestern Visayas the 4 facilities in Central Visayashad newborn resuscitator bags and masks available priorto the EINC intervention With the intervention howeverhealth workers reported increased confidence in their newlyacquired resuscitation skills Wall clocks were present indelivery areas in all 4 facilities assessed from baseline to endline Room thermometers absent at baseline in all facilitieswere available in all 4 facilities and end line
Across the 3 regions significant improvements in servicestandards were documented In 2008 coverage of early skin-to-skin contact (SSC) was documented at 96 in deliveryassessments in 51 government hospitals [7] After governmentefforts at EINC scale-up SSC coverage was at 64 bymaternal report in 2013 [10] In this study SSC was at84 in primary level facilities postdisaster by health workerreport Before Haiyan barriers to EINC implementation thatis absence of enabling physical and policy environmentsnoncompliance by specialists and other ldquoexpertsrdquo unfamiliarwith the updated EINC practices had been diminished butnot eliminated The devastation brought by Haiyan disman-tled the systems that enabled EINC practice Neverthelessover a 3-month period an intervention of training andposttraining assessments was able to restore and for someEINC practices even exceed pre-Haiyan coverage rates
The high coverage rates for EINC indicators at baselinesuggests that previous scale-up efforts in EINC and othercross-cutting areas increased the potential for resilienceThis complemented assistance offered by other humanitarianactors (eg infrastructure rehabilitation and provision ofsupplies and equipment) turning this into an opportunity toldquobuild back betterrdquo However the contribution of pre-Haiyancapacity building efforts to this rapid restoration and furtherimprovement of EINC services requires further evaluationWe postulate that if capacity building efforts have establishedenabling environments under normal circumstances rehabil-itation could be achieved in similarly brief time periodsThuscapacity building for EINC may potentially be considered asan important disaster preparedness measure
Aiming to improve the sustainability of this interventionthe external experts provided close supportive supervisionduring the cascade training sessions and the two posttrainingassessments Our experience reveals that both performanceand environments have improved creating an enabling envi-ronment for EINC practices There were still aspects thatrequired improvement that could be reinforced by the localhealth officials during supervisory visits However this can bea challenge in areas where regular supervision visits are raredue to difficulties in geographic access or security constraints
Government support was provided through so-calledInterlocal Health Zones (ILHZs) utilizing existing referralnetworks often with rural health units (RHUs) and districthospitals as the focal point Trainers were capacitated asILHZ groups for subsequent roll-out through a skills transfermethodology This approach had its limitation though astrained health care providers from one ILHZ in generalcould not be tapped to train health care workers of anotherILHZ
In the aftermath of the disaster several developmentand recovery activities resulted in competing schedules(eg water sanitation and hygiene (WASH) vaccine coldchain implementation etc) making it difficult to scheduletraining dates Often competing capacity building activitiesand the local rehabilitation efforts involved the same setof (limited) local manpower Consequently mobilizing localstaffs to implement their trainersrsquo knowledge in cascade QAworkshops proved difficult Another constraint posed thehealth human resource availability after the disaster sincemany health care workers were victims themselves
The postdisaster setting likewise presented more chal-lenges in conducting capacity building interventions In somegeographic areas communication and road infrastructurecontinued to be unusable making it difficult for healthworkers to attend trainings or gather local data This post-disaster scenario constrained us to ldquopre- to postinterventionassessmentrdquo and its inherent methodologic limitations
This study was also limited by the fact that not all facilitieswho participated in baseline assessment were included inthe posttraining assessment Thus this study could benefitfrom another evaluation after a longer interval posttrain-ing to assess newborn outcome indicators sustainability ofimprovements and further analysis on possible contributoryeffects of other sectoral interventions (eg WASH) and
BioMed Research International 9
partner efforts in the areas The contribution of predisastercapacity building to the results could not be studied
4 Conclusions
This intervention filled the service gaps identified immedi-ately after a large scale natural disaster and helped to reestab-lish and improve the delivery of health services in affectedareas Where baseline indices were worse because of theimmediate effects of the typhoon (ie Eastern Visayas) themagnitude of improvement across most assessed parameterswas more significant However there were other parameterswhere gaps persist despite intensive efforts and othermethodsand systemic interventions need to be explored address thesedeficiencies
Our study demonstrates that quick important qualityimprovements can bemade in a timelymanner across a rangeof health facilities andwith differing cadres of health workerseven in immediate postdisaster settings Capacity building ofhealth workers and strengthening of the local health systemto deliver quality care before during and in the aftermath ofa major disaster are among the preconditions for a resilienthealth system [13] Building the evidence base linking thesequality improvement efforts in EINC and basic newbornresuscitation with impact on newborn and maternal healthoutcomes postdisaster is imperative [14]
Disclosure
Any opinions stated by UNICEF affiliates are those of theauthors and not of UNICEF
Competing Interests
The authors declare no competing interests regarding thepublication of this paper
Acknowledgments
Funding support was provided by UNICEF The authorswould like to thank our colleagues in the Department ofHealth Regional Health Offices of Eastern Central andWestern Visayas (especially Drs Corazon Sabulao and AlmaBernardo) the Provincial Health Offices of Capiz CebuIloilo Leyte and Eastern and Western Samar (especiallyDrs Samuel Delfin Cynthia Genosolango Grace Trabadoand Marian Isiderio) Dr Nabila Zaka (UNICEF) and theInternational Medical Corps
References
[1] October 2015 httplibrarypcwgovphsitesdefaultfiles14011120SDR20Yolanda20Philippnes20finalpdf
[2] ldquoResponding toTyphoonHaiyanrdquoTheLancet vol 382 no 9907article 1769 2013
[3] R C Alfonso D S Capili K A Reyes F Tatad-To and M ASilvestre ldquoContributing to the Infant and Young Child Feedingin Emergencies (IYCF-E) response in the Philippines A local
NGOperspectiverdquo 2015 httpwwwennonlinenetfex50iycf-philippines
[4] WHO Philippines ldquoEssential Intrapartum and Newborn Care(EINC) Evidence-based Standard Practicesrdquo 2016 httpwwwwprowhointphilippinesareasmaternal child nutritionnew-born mother careeinc protocolsen
[5] WHO WPRO ldquoEarly Essential Newborn Care First EmbraceClinical Practice Pocket Guiderdquo 2014 httpiriswprowhointbitstreamhandle106651107989789290616856 engpdfjsessi-onid=B789B68B6D8BF8BB2C7F99F09E698AE1sequence=3
[6] H Obara and H Sobel ldquoQuality maternal and newborn care toensure a healthy start for every newborn in the World HealthOrganization Western Pacific Regionrdquo BJOG An InternationalJournal of Obstetrics andGynaecology vol 121 pp 154ndash159 2014
[7] H L Sobel M A A Silvestre J B V Mantaring III Y EOliveros and S Nyunt-U ldquoImmediate newborn care practicesdelay thermoregulation and breastfeeding initiationrdquo Acta Pae-diatrica International Journal of Paediatrics vol 100 no 8 pp1127ndash1133 2011
[8] Z A Bhutta J K Das R Bahl et al ldquoEvery newborn canavailable interventions end preventable deaths in mothersnewborn babies and stillbirths and at what costrdquo The Lancetvol 384 no 9940 pp 347ndash370 2014
[9] E Duysburgh B Kerstens M Diaz et al ldquoNewborn care inIndonesia Lao Peoplersquos Democratic Republic and the Philip-pines a comprehensive needs assessmentrdquo BMC Pediatrics vol14 no 1 article 46 2014
[10] Philippine Statistics Authority (PSA) and ICF InternationalPhilippines National Demographic and Health Survey 2013Philippine Statistics Authority (PSA) Manila Philippines ICFInternational Rockville Md USA 2014
[11] Philippine Public StormSignals 2015 httpdrrmregion4adostgovphknowledge-management-center7Philippine-public-storm-signalshtml
[12] Healthy Newborn Network (HNN) Inter-agency NewbornIndicators Technical Working Group 2012 Newborn ServicesRapid Health Facility Assessment tool 2016 httpwwwheal-thynewbornnetworkorgresourcenewborn-services-rapid-health-facility-assessment
[13] M E Kruk M Myers S T Varpilah and B T Dahn ldquoWhat isa resilient health system Lessons from Ebolardquo The Lancet vol385 no 9980 pp 1910ndash1912 2015
[14] C Enweronu-Laryea K E Dickson S G Moxon et al ldquoBasicnewborn care and neonatal resuscitation a multi-countryanalysis of health system bottlenecks and potential solutionsrdquoBMCPregnancy and Childbirth vol 15 supplement 2 article 542015
[15] United Nations Office for the Coordination of HumanitarianAffairs (UN-OCHA) ldquoTyphoon HaiyanmdashHumanitarian Snap-shotrdquo Philippines (as of Nov 12 2013) Data Sources DSWDDROMICReport Nov 12 2013 NDRRMC Situation Report 14OCHO Situation Report 5 and UNDAC Reports

2 BioMed Research International
and supported appropriate humanitarian responses Amongthe WHO endorsed interventions for saving the lives ofmothers and children is the so-called Essential Intrapartumand Newborn Care (EINC) a package of cost-effective time-bound interventions [4] In the Philippines EINC (popularlyknown as ldquoUnang Yakaprdquo or the First Embrace) is imple-mented and mainstreamed in practice protocols or tools [5]following quality improvement principles [6] The develop-ment of this standardized protocol was triggered by datafrom observational assessments in 51 government hospitalsin the Philippines revealing that practices in the immediatenewborn care period were undermining thermoregulationand breastfeeding initiation of newborns [7]The importanceof providing quality care forwomenduring labor and deliveryand implementation of safe practices for their newborns toensure their best outcomes became paramount [8] Prior totyphoon Haiyan implementation of the EINC Protocol wasbeing undertaken only in selected government hospitals andprimary level facilities (rural health units and district hospi-tals) Inequity and systembarriers to bring implementation toscale persisted despite national health policies being in place[9] Neonatal mortality rate (NMR) reported in the NationalDemographic and Health Survey (NDHS 2013) [10] was 13per 1000 live births nationally and 15 18 and 10 per 1000live births in Western Central and Eastern Visayas regionsrespectively
When a 72 magnitude earthquake jolted the provinceof Bohol in the Visayas region one month prior to typhoonHaiyan WHO supported the rapid building of health workercapacity for maternalnewborn care in a postdisaster settingEINC training packages were updated to incorporate newWHO guidelines on basic newborn resuscitation and post-natal care of mothers and newborns including magnesiumsulfate administration to address gaps in care After a pilotimplementation in Bohol province the trainingmoduleswiththe expanded content were endorsed byWHO for utilizationin postdisaster areas where similar needs existed
The aim of this intervention was to support the reestab-lishment of health care services for birthingmothers and theirnewborns in the areas affected by typhoon Haiyan guided byquality improvement principles Specific objectives were to
(1) conduct EINC training of trainers (TOT) and qualityassurance (QA) workshops in target areas withinEastern Central and Western Visayas regions toaddress gaps identified in the baseline assessment
(2) and undertake rapid assessments of EINC servicesusing a standard tool at baseline and at 1 and 3monthsafter the training
2 Materials and Methods
Based on a multistage vulnerability analysis UNICEF andpartners identified forty (40) prioritymunicipalities along thepath of typhoon Haiyan where the humanitarian responsewould be intensified during the period from February toSeptember 2014
This multistage vulnerability analysis entailed severalstages in the first stage an initial list of 120 areas (cities
and municipalities) was constituted based on preliminarydata from the Philippines National Disaster Risk Reduc-tion and Management Council (NDRRMC) and UnitedNations Office for the Coordination of Humanitarian Affairs(OCHA) Criteria used were (a) areas with 95 and aboveaffected population (b) areas given typhoon signal number4 and (c) areas with highest potential for storm surgeTyphoon storm signal number 4 signifies a very intensetyphoon with winds of more than 185 kph speed [11] Inthe second stage official data such as detailed populationpre- and post-Haiyan poverty incidence and local data wereincorporated In the third stage convergence of UNICEFinterventions in the sectors of health nutrition educationchild protection and water sanitation and hygiene (WASH)were analyzed to find the ldquobestrdquo model for prioritizationof areas In the fourth and final stage the 40 prioritymunicipalities were identified based on cumulative affectedpopulation that would yield optimal coverage in relation toUN strategic response plan targets developed with the Philip-pine government These were in Eastern Visayas (Region8) in the province of LeytemdashTacloban City Palo TanauanDulag Burauen Dagami La Paz Julita Tabontabon Cari-gara Jaro San Miguel Alangalang Pastrana Mayorga andMacArthur in the provinces of Eastern andWestern SamarmdashGuiuan Salcedo Hernani Mercedes Balangiga GiporlosLawaan Quinapondan Balangkayan Borongan City andMarabut Those included in Western Visayas (Region 6)were in the province of CapizmdashPontevedra Pilar PresidentRoxas Maayon Ivisan Panay Panitan and Jamindan inthe province of IloilomdashConcepcion Sara and Estancia InCentral Visayas (Region 7) Bantayan and Daanbantayanmunicipalities in the province of Cebu were included Tech-nical experts from a local nongovernmental organization(NGO Kalusugan ng Mag-Ina or ldquoHealth of Mother andChildrdquo) were engaged to roll out the EINC implementationand quality improvement capacity buildingtraining activitiesin priority municipalities from February to September 2014In 2011 the same NGO provided the technical assistance inthe pilot implementation of EINC in the Eastern VisayasRegional Medical Center in Leyte and the subsequent train-ing of trainers and quality assurance workshop cascaded bythe Region 8 Health Office for all Eastern Visayas provincesin 2012
The methodology to facilitate the capacity building ofhealth workers in the forty (40) priority municipalities con-sisted of a training of trainers and cascade quality assurance(QA) workshops with rapid assessment before the trainingand at one and three months posttraining (see Figure 1)
Using the ldquoNewborn Services Rapid Health FacilityAssessmentrdquo tool that was developed by the InteragencyNewborn Indicators Technical Working Group as a template[12] rapid facility assessments were done at baseline (beforetraining) and at one month and three months after train-ing Technical experts acting as external assessors used theidentical tool to conduct pre- and posttraining assessmentsduring facility visits External assessors performed ocularsurveys of the access and quality of the labor-delivery andpostpartum environments equipment supplies and patientpathways Information was collected through interviews of
BioMed Research International 3
Baseline assessment
EINC training of
trainers (TOT)
Training via EINC QA workshops
1-monthposttrainingassessments
3-monthposttrainingassessments
Figure 1 Flow of assessments and interventions
health workers and mothers supplemented by review ofrecords Whenever possible deliveries were observed
In the priority municipalities primary level health facili-ties with the highest number of deliveries were intentionallyselected Based on usual patient traffic the biggest districthospital or rural health unit (RHU) and its correspondingbusiest lying-in clinic were selected subject to the limitedaccessibility of facilities after typhoon Haiyan In consider-ation of service delivery networks and referral flows withinand across municipalities assessments covered additionalmunicipalities beyond the 40 priority areas
The tool was used to assess facility-based delivery andnewborn care service capacity in primary and referral levelfacilities Gaps in newborn care health services were sys-tematically identified using tracer indicators Findings wereutilized to describe capacity to address three main causesof newborn deaths asphyxia prematurity and infectionDeterminants were classified as (a) service availability (b)equipment and supplies and (c) service standards
21 EINC Training of Trainers Updated EINC training mod-ules contained brief didactic sessions on basic topics Essen-tial Intrapartum and Newborn Care breastfeeding supportkangaroo mother care Infant and Young Child Feeding inEmergencies (IYCF-E) partograph use and the recentWHOrecommendations on basic newborn resuscitation correctadministration of magnesium sulfate and postnatal care ofmothers and newborns Skills sessions consisted of ldquocoachingsessionsrdquo with demonstrationreturn demonstrations usingmanikins and delivery kits Workshops culminated withaction planning sessions on effective mainstreaming of EINCin their practice These planning sessions allowed the partic-ipants to voice out their concerns and their apprehensionsand discuss among themselves ways to contextualize thesechallenges and address them
Training of trainers (TOT) workshops were conductedin the three regions Selection of trainees was strategic toinclude senior health care workers with aptitude to becometrainers in their respective service delivery networks (roughlycorresponding to geopolitical Interlocal Health Zones orILHZs) Representation of involved ILHZs was ensured asmuch as possible to create a pool of trainers to cascadethe training locally Local trainers were further chosen fromthis pool based on their performance during the TOT
Participants included thirty (30) trainees each from LeyteEastern and Western Samar Capiz Iloilo and Cebu
22 Cascade EINC Quality Assurance Workshops The tech-nical experts supervised and mentored the new local trainersas they implemented their own cascade quality assurance(QA) workshops In each of the areas two QA workshopsof 30 participants each were conducted targeting a totalof 300 capacitated skilled birth attendants QA workshopmodules for service providers were delivered over 6 half-daysessions Pre- to postworkshop acquisition of knowledge wasmeasured through 15 item multiple choice question writtenquizzes and acquisition of skills in the classroom assessmentsthrough performance checklists
23 Statistical Analysis Epi Info 6 was used for dataanalysis Categorical variables at baseline 1-month and 3-month after training presented as proportions () werecompared using Fisherrsquos exact and 1205942 tests with significanceset at 119901 lt 005
3 Results and Discussion
External experts supported the rehabilitation of EINC healthservices in 40 priority municipalities in Eastern Central andWesternVisayas severely devastated byHaiyan (See Figure 2)
As part of the service delivery networks additional areasadjacent to the priority municipalities were included namelyfour (4)municipalities and one city (Abuyog andOrmoc Cityin Leyte Basey in Western Samar and Barotac Viejo andBalasan in Iloilo) The grand total of 45 local governmentunits (LGUs) thus included three (3) cities (in Leyte) andforty-two (42) municipalities (see Figure 3)
31 Baseline Assessments (Table 1) Baseline rapid assess-ments were done at 16 weeks after landfall in Eastern Visayas(Leyte and Eastern and Western Samar) 20 weeks afterlandfall in Western Visayas (Iloilo and Capiz) and 22 weeksafter landfall in Central Visayas (Cebu) A total of 56 healthfacilities were assessed at baseline Assessments revealed sig-nificant disruption in obstetric and newborn health servicesin Eastern Visayas and much less significant disruption inCentral and Western Visayas
4 BioMed Research International
Figure 2 Path of typhoon Haiyan through central Philippines [15]
At baseline health facilities assessed ranged from ruralhealth units (RHU 39) first level referral hospitals (15community district and city hospitals) and in addition2 provincial hospitals with birthing services After typhoonHaiyan the physical devastation in Eastern Visayas causedthe most serious interruptions in EINC delivery Immediateresponse services were provided primarily through contri-butions from international partners in tents and makeshiftfacilities The lack of availability of 247 delivery servicesrevealed the importance of improved referral mechanismsthat could bring mothers experiencing complications duringor after birth to a higher level facility if neededThese findingsdiffered from the assessment of Central and Western Visayasmunicipalities where facilities mostly sustained partial dam-age with no interruption of birthing services
Apart from damage to infrastructure commodities werein serious shortage or absent with stock-outs of life-savingdrugs (eg oxytocin magnesium sulfate and dexametha-sone) Health human resources suffered serious setbacksnot only due to substantial loss of lives among health careproviders but also due to lack of training and technicalcapacity (in basic newborn resuscitation care of the low birthweight kangaroo mother care breastfeeding and Infant andYoung Child Feeding in Emergencies (IYCF-E)) In facilitieswhere health workers had participated in a previous 11-dayBasic Emergency Obstetric and Newborn Care (BEmONC)training low self-efficacy ratings especially in partographuse magnesium sulfate administration and newborn resus-citation rates were noted Very few facilities experiencedsupervisory visits in the previous 6 months None performedroutine postnatal care services Documentation of practiceswas weak Finally not all facilities conducted regular mater-nal and newborn death reviews
Table 1 Number of facilities assessed at pretraining (baseline) andat 1 month and 3 months posttraining by region and by province
RegionprovinceFacility level
Rural healthunit
First levelhospital
Provincialhospital
Eastern VisayasLeyteBaseline 15 4 11 month 16 5 13 months 12 4 1
SamarBaseline 11 4 11 month 11 4 13 months 10 4 0
Western VisayasCapizBaseline 3 3 01 month 3 3 03 months 3 3 0
IloiloBaseline 8 2 01 month 8 2 03 months 8 2 0
Central VisayasCebuBaseline 2 2 01 month 2 2 03 months 2 2 0
Progress in EINC implementation and quality improvement from baselineassessments through 1- and 3-month posttraining assessments
32 EINC Training of Trainers (TOT) Out of 150 candidatetrainers who were invited 112 (75) attended the trainingThese were maternal and child health workers holding strate-gic positions (provincial level program managers hospitalspecialists municipal health officers public health nursesandmidwife supervisors) A total of five (5) training of trainer(TOT) workshops of 3 daysrsquo duration each were conductedone each for the provinces of Leyte Eastern and WesternSamar Iloilo Capiz and Cebu
33 Cascade EINC QA Workshops As part of the trainingrequirement each TOT candidate trainer participated in atleast one of a total of ten (10) cascade QA workshops fortheir colleagues with supportive supervision and technicaloversight from expert trainers A total of 281 out of 300targeted skilled birth attendants (937) were further trained
Thus a total of 393 health workers completed EINCworkshops over this period 281 completed their participationin 3-day QA workshops and 112 attended the five TOT work-shops Consistent improvements in posttraining assessmentquizzes and performance checklists for both the TOT andQAworkshop participants were noted
BioMed Research International 5
Bukidnon
Sulu Sea
LeyteIloilo
Cebu
Samar
Bohol
Capiz
Negros Occidental
Albay
Masbate
Antique
Negros Oriental
Aklan
Eastern Samar
Sorsogon
Northern Samar
Agusan del Sur
Agusan del Norte
Misamis Oriental
QuezonCamarines Sur
Marinduque
Biliran
Romblon
Southern Leyte
Surigao del Norte
Guimaras
Dinagat Islands
Zamboanga del Norte
SiquijorSurigao del Sur
Misamis Occidental
Camiguin
Catanduanes
Bohol Sea
Philippine Sea
Sibuyan Sea
Visayan Sea
Samar Sea
Leyte Gulf
Ragay Gulf
Surigao Strait
Tayabas Bay
Map shows PhilippinesUNICEF Haiyan programmeareas and typhoon Haiyanpath
Disclaimer the boundaries and names shown and the designations used in this map do not imply official endorsement or acceptance by the United Nations
0 10 20 30 405(Kilometers)
Data source UNICEFDate of data source 14 Dec 2014Map sources NE COD GADMMap production date 06 March 2016Feedback jbacaluniceforg
ScaleProgramme areas
HaiyanTyphoon Haiyan path
VIII
VIIVI
Capiz
IloiloVI IloiloVI IloiloVIVI
CapizVICapizVICapizVICapizVICapizVICapizVICapizVICapizVICapizVI
Iloilo
CebuVII CebuVII Cebu
Eastern SamarVIII Eastern SamarVIII Eastern SamarVIII Eastern SamarVIII Eastern SamarVIII Eastern SamarVIII Eastern SamarVIII Eastern SamarVIII Eastern SamarVIIIVIII
Eastern Samar
Samar
LeyteVIII LeyteVIII LeyteVIII LeyteVIII LeyteVIII LeyteVIII LeyteVIII LeyteVIII LeyteVIII LeyteVIII LeyteVIII LeyteVIII LeyteVIII LeyteVIII LeyteVIII LeyteVIII LeyteVIII LeyteVIII LeyteVIII LeyteVIII LeyteVIII
IvisanJamindanMa-AyonPanayPanitanPilarPontevedraPresident RoxasRoxas CityTapazCarlesConcepcionEstanciaSaraBantayanCebu CityDaanbantayanBalangigaBalangkayanBorongan CityGiporlosGuiuanHernaniLawaanMercedesQuinapondanSalcedoAlangalangBurauenCarigaraDagamiDulagIsabelJaroJulitaKanangaLa PazMacarthurMatag-ObMayorgaMeridaPaloPastranaSan MiguelTabontabonTacloban CityTanauanVillabaMarabut
998400Region 4B
998400Region 4A
998400Region 5
998400Region 8
998400Region 6
998400Region 7
998400Region 9
998400Region 10
998400Region Caraga
1 cm = 16km
Region Province Municipilaty
Philippines UNICEF Haiyan programme areas
N
Figure 3 40 priority municipalities listed in orange box and shaded in map
6 BioMed Research International
96 98 98 98
16 22
17 96 98
94
0 10()
20 30 40 50 60 70 80 90 100
Service availability indicators at baseline and at 1- and 3-month posttraining assessment in Eastern Western and
Central Visayas Philippines 2013
3-month PTA 1-month PTA Baseline
Kangaroo mother carelowastAntenatal steroidslowast
Neonatal resuscitationlowast
Manual removal of retained products after deliveryManual placental removal
Assisted vaginal deliveryParenteral magnesium sulfatelowast
Parenteral oxytocinlowast
Parenteral antibioticslowast247 skilled birth attendancelowast
lowastIndicates significant change from baseline to 3-month PTA p lt 005
Figure 4 Proportion of facilities assessed providing various services at pretraining (baseline) and at 1 and 3 months posttraining assessment(PTA) Eastern Western and Central Visayas post-Haiyan
34 Posttraining Assessments (Table 1) At 1 month and 3months after training field visits to 58 and 51 facilities respec-tively were carried out The facilities that completed the 3assessments were thirty-five (35) rural health units (RHUs)15 primary level hospitals (13 district 1 city and 1 communityhospitals) and one (1) provincial hospital These field visitsrevealed that uptake of EINC knowledge and skills was trans-lated to significant changes in daily practice Posttrainingassessment visits revealed good evidence of changes in thephysical environments in the labordelivery and postpartumareas and implementation of many of the EINC practices
However apart from the overall improvement someposttraining gaps were identified (1) not allowing a com-panion of choice (2) nonadministration of birth dosesof BCG vaccine (3) unavailability of nevirapine therapy(4) unavailability of protocols or guidelines for IntegratedManagement of Pregnancy and Childbirth (IMPAC) referralof sick newborns Comprehensive Emergency Obstetric andNewborn Care (CEmONC) and preterm labormanagement(5) absence of soap and hand disinfectants in postnatal areas
35 Service Availability (Figure 4) In Eastern Visayas theworst hit region baseline assessment revealed that 27 of 36facilities were providing birthing services At 1 month aftertraining 32 of 38 assessed birthing facilities were providinground-the-clockdaily (247) skilled birth attendance (SBA)At 3 months 30 of 31 birthing facilities were providing 247SBA InWesternVisayas 16 of 16 facilities were able to sustaindelivery services at baseline and 1 month assessments Onefacility suspended its delivery services to undergo renova-tions at the 3-month assessment All of the 15 other facilitieswere providing 247 SBA In Central Visayas all 4 facilitiesassessed were providing 247 SBA at baseline 1-monthand 3-month assessments Over the period from baselineassessment to 3 months after training there were significantimprovements in self-reported availability of services such as
neonatal resuscitation kangaroomother care administrationof parenteral oxytocin antibiotics antenatal steroids andmagnesium sulfate In contrast persistent gaps remainedfor assisted vaginal delivery manual placental removal andmanual removal of retained products after delivery In Figures4ndash6 the proportion of facilities () at end line (3months aftertraining) is labeled
36 Equipment and Supplies (Figure 5) Over the period frombaseline assessment to 3 months after training (20-week 19-week and 14-week periods for Eastern Western and Cen-tral Visayas resp) there were significant improvements inavailability of life-saving drugs (ie oxytocin) and equipment(ie for resuscitation) most notably for Eastern and CentralVisayas For Western Visayas some improvements were seenin the facilities but the limited availability of equipmentconstrained the appropriate delivery of services Not all life-saving drugs were available in all facilities especially antibi-otics and steroids
Though there was significant improvement persistentgaps remained for antenatal steroids injectable gentamicinand magnesium sulfate supplies Towels for drying werestill being provided by families instead of by facilitiesNevirapine for prevention of mother-to-child transmissionof HIV remained unavailable across all regions MultidoseBCG vaccines were available but considered ldquoinsufficientrdquo byhealth workers Many facilities had moved their weighingscales from their delivery areas to their maternity careareas for deferred weighing until after the first breastfeedas recommended in EINC protocols Protocols for IMPACsick newborn carereferral preterm labor management andCEmONCmanuals remain unavailable
37 Service Standards (Figure 6) In addition to parametersincluded in the Newborn Care Services Rapid AssessmentTool selected parameters relevant to the Philippines EINC
BioMed Research International 7
69 88
86 96
84 4
73 2
57 98
71
0 10 20 30 40 50()
60 70 80 90 100
Equipment and supplies availability at baseline and at 1- month and 3-month posttraining assessment in Eastern
Western and Central Visayas Philippines 2013
3-month PTA 1-month PTA Baseline
Magnesium sulfateInjectable uterotoniclowast
CorticosteroidsPMTCT drugslowast
Injectable gentamicinTowels for drying
Soap or hand disinfectantInfant scalelowast
lowastResuscitation tableNewborn bag and masklowast
Up-to-date delivery register
lowastIndicates significant change from baseline to 3-month PTA p lt 005
Figure 5 Proportion of facilities assessed to have various equipment and supplies at pretraining (baseline) and at 1 and 3months posttrainingassessment (PTA) Eastern Western and Central Visayas post-Haiyan
87 58
96 84
0 98 98
86 80
84 82
92 76
70 72
70
0 10 20 30 40 50()
60 70 80 90 100
Service standards indicators at baseline and at 1-month and 3-month posttrainingassessment in Eastern Western and Central Visayas Philippines 2013
Companion of choiceAllowed to eatdrink
Selective episiotomyperineal supportAMTSLlowast
Partograph filled out correctlylowast
Immediatethorough dryingSkin-to-skin contact
Properly timed cord clampingNonseparation and initiation of Breastfeeding
Eye carelowast
Vitamin Klowast
BCG birth doseHepatitis B birth dose
Wall clock in delivery arealowast
Room thermometer in delivery arealowast
Size 0 or preterm masklowast
3-month PTA 1-month PTA Baseline
lowastIndicates significant change from baseline to3-month PTA p lt 005
Figure 6 Proportion of facilities assessed to be implementing various service standards at pretraining (baseline) and at 1 and 3 monthsposttraining assessment (PTA) Eastern Western and Central Visayas post-Haiyan
8 BioMed Research International
Protocol and Basic Emergency Obstetric and Newborn Care(BEmONC) services standards were assessed through inter-views of health service providers
Significant improvements in service standards usingtracer indicators were noted across all regions over the periodfrom pretraining assessment to the 3 months posttrainingassessment Most notable were performance of the EINCldquocore stepsrdquo in immediate newborn care proper WHOpartograph use and availability of size 0 face masks forresuscitation of preterms which improved from 0 to 100at 3 months posttraining assessment
Quality labor and delivery for mothers (companion ofchoice allowing mothers to eatdrink semiupright deliverybed perineal support and restrictive episiotomy and activemanagement of the third stage of labor) and quality post-partum care (monitoring vital signs uterine massage andpostpartum visit within first week and then within fourthto sixth weeks after discharge) were carried out Facilitiesreported performance of the ldquocore stepsrdquo of immediatenewborn care (immediate and thorough drying skin-to-skincontact properly timed cord clamping and nonseparation ofnewborn from mother for early breastfeeding) and routinenewborn care (eye care physical examination and vitamin Kadministration) Postpartumwomen interviewed in the facil-ities verified the consistency of applying the EINC protocol
A persistent gap in EINC standard practice was the birthdose of BCG vaccine Ninety-six percent of facilities were notadministering this birth dose as recommended by nationalguidelines citing that using the available multidose vials foronly a few patients at each time constitutes ldquowastagerdquo Thisreflects the common practice of deferring the BCG vaccina-tion to the first-postnatal visit in the Philippines Number ofroom thermometers and wall clocks had increased in somefacilities
UnlikeWestern Visayas the 4 facilities in Central Visayashad newborn resuscitator bags and masks available priorto the EINC intervention With the intervention howeverhealth workers reported increased confidence in their newlyacquired resuscitation skills Wall clocks were present indelivery areas in all 4 facilities assessed from baseline to endline Room thermometers absent at baseline in all facilitieswere available in all 4 facilities and end line
Across the 3 regions significant improvements in servicestandards were documented In 2008 coverage of early skin-to-skin contact (SSC) was documented at 96 in deliveryassessments in 51 government hospitals [7] After governmentefforts at EINC scale-up SSC coverage was at 64 bymaternal report in 2013 [10] In this study SSC was at84 in primary level facilities postdisaster by health workerreport Before Haiyan barriers to EINC implementation thatis absence of enabling physical and policy environmentsnoncompliance by specialists and other ldquoexpertsrdquo unfamiliarwith the updated EINC practices had been diminished butnot eliminated The devastation brought by Haiyan disman-tled the systems that enabled EINC practice Neverthelessover a 3-month period an intervention of training andposttraining assessments was able to restore and for someEINC practices even exceed pre-Haiyan coverage rates
The high coverage rates for EINC indicators at baselinesuggests that previous scale-up efforts in EINC and othercross-cutting areas increased the potential for resilienceThis complemented assistance offered by other humanitarianactors (eg infrastructure rehabilitation and provision ofsupplies and equipment) turning this into an opportunity toldquobuild back betterrdquo However the contribution of pre-Haiyancapacity building efforts to this rapid restoration and furtherimprovement of EINC services requires further evaluationWe postulate that if capacity building efforts have establishedenabling environments under normal circumstances rehabil-itation could be achieved in similarly brief time periodsThuscapacity building for EINC may potentially be considered asan important disaster preparedness measure
Aiming to improve the sustainability of this interventionthe external experts provided close supportive supervisionduring the cascade training sessions and the two posttrainingassessments Our experience reveals that both performanceand environments have improved creating an enabling envi-ronment for EINC practices There were still aspects thatrequired improvement that could be reinforced by the localhealth officials during supervisory visits However this can bea challenge in areas where regular supervision visits are raredue to difficulties in geographic access or security constraints
Government support was provided through so-calledInterlocal Health Zones (ILHZs) utilizing existing referralnetworks often with rural health units (RHUs) and districthospitals as the focal point Trainers were capacitated asILHZ groups for subsequent roll-out through a skills transfermethodology This approach had its limitation though astrained health care providers from one ILHZ in generalcould not be tapped to train health care workers of anotherILHZ
In the aftermath of the disaster several developmentand recovery activities resulted in competing schedules(eg water sanitation and hygiene (WASH) vaccine coldchain implementation etc) making it difficult to scheduletraining dates Often competing capacity building activitiesand the local rehabilitation efforts involved the same setof (limited) local manpower Consequently mobilizing localstaffs to implement their trainersrsquo knowledge in cascade QAworkshops proved difficult Another constraint posed thehealth human resource availability after the disaster sincemany health care workers were victims themselves
The postdisaster setting likewise presented more chal-lenges in conducting capacity building interventions In somegeographic areas communication and road infrastructurecontinued to be unusable making it difficult for healthworkers to attend trainings or gather local data This post-disaster scenario constrained us to ldquopre- to postinterventionassessmentrdquo and its inherent methodologic limitations
This study was also limited by the fact that not all facilitieswho participated in baseline assessment were included inthe posttraining assessment Thus this study could benefitfrom another evaluation after a longer interval posttrain-ing to assess newborn outcome indicators sustainability ofimprovements and further analysis on possible contributoryeffects of other sectoral interventions (eg WASH) and
BioMed Research International 9
partner efforts in the areas The contribution of predisastercapacity building to the results could not be studied
4 Conclusions
This intervention filled the service gaps identified immedi-ately after a large scale natural disaster and helped to reestab-lish and improve the delivery of health services in affectedareas Where baseline indices were worse because of theimmediate effects of the typhoon (ie Eastern Visayas) themagnitude of improvement across most assessed parameterswas more significant However there were other parameterswhere gaps persist despite intensive efforts and othermethodsand systemic interventions need to be explored address thesedeficiencies
Our study demonstrates that quick important qualityimprovements can bemade in a timelymanner across a rangeof health facilities andwith differing cadres of health workerseven in immediate postdisaster settings Capacity building ofhealth workers and strengthening of the local health systemto deliver quality care before during and in the aftermath ofa major disaster are among the preconditions for a resilienthealth system [13] Building the evidence base linking thesequality improvement efforts in EINC and basic newbornresuscitation with impact on newborn and maternal healthoutcomes postdisaster is imperative [14]
Disclosure
Any opinions stated by UNICEF affiliates are those of theauthors and not of UNICEF
Competing Interests
The authors declare no competing interests regarding thepublication of this paper
Acknowledgments
Funding support was provided by UNICEF The authorswould like to thank our colleagues in the Department ofHealth Regional Health Offices of Eastern Central andWestern Visayas (especially Drs Corazon Sabulao and AlmaBernardo) the Provincial Health Offices of Capiz CebuIloilo Leyte and Eastern and Western Samar (especiallyDrs Samuel Delfin Cynthia Genosolango Grace Trabadoand Marian Isiderio) Dr Nabila Zaka (UNICEF) and theInternational Medical Corps
References
[1] October 2015 httplibrarypcwgovphsitesdefaultfiles14011120SDR20Yolanda20Philippnes20finalpdf
[2] ldquoResponding toTyphoonHaiyanrdquoTheLancet vol 382 no 9907article 1769 2013
[3] R C Alfonso D S Capili K A Reyes F Tatad-To and M ASilvestre ldquoContributing to the Infant and Young Child Feedingin Emergencies (IYCF-E) response in the Philippines A local
NGOperspectiverdquo 2015 httpwwwennonlinenetfex50iycf-philippines
[4] WHO Philippines ldquoEssential Intrapartum and Newborn Care(EINC) Evidence-based Standard Practicesrdquo 2016 httpwwwwprowhointphilippinesareasmaternal child nutritionnew-born mother careeinc protocolsen
[5] WHO WPRO ldquoEarly Essential Newborn Care First EmbraceClinical Practice Pocket Guiderdquo 2014 httpiriswprowhointbitstreamhandle106651107989789290616856 engpdfjsessi-onid=B789B68B6D8BF8BB2C7F99F09E698AE1sequence=3
[6] H Obara and H Sobel ldquoQuality maternal and newborn care toensure a healthy start for every newborn in the World HealthOrganization Western Pacific Regionrdquo BJOG An InternationalJournal of Obstetrics andGynaecology vol 121 pp 154ndash159 2014
[7] H L Sobel M A A Silvestre J B V Mantaring III Y EOliveros and S Nyunt-U ldquoImmediate newborn care practicesdelay thermoregulation and breastfeeding initiationrdquo Acta Pae-diatrica International Journal of Paediatrics vol 100 no 8 pp1127ndash1133 2011
[8] Z A Bhutta J K Das R Bahl et al ldquoEvery newborn canavailable interventions end preventable deaths in mothersnewborn babies and stillbirths and at what costrdquo The Lancetvol 384 no 9940 pp 347ndash370 2014
[9] E Duysburgh B Kerstens M Diaz et al ldquoNewborn care inIndonesia Lao Peoplersquos Democratic Republic and the Philip-pines a comprehensive needs assessmentrdquo BMC Pediatrics vol14 no 1 article 46 2014
[10] Philippine Statistics Authority (PSA) and ICF InternationalPhilippines National Demographic and Health Survey 2013Philippine Statistics Authority (PSA) Manila Philippines ICFInternational Rockville Md USA 2014
[11] Philippine Public StormSignals 2015 httpdrrmregion4adostgovphknowledge-management-center7Philippine-public-storm-signalshtml
[12] Healthy Newborn Network (HNN) Inter-agency NewbornIndicators Technical Working Group 2012 Newborn ServicesRapid Health Facility Assessment tool 2016 httpwwwheal-thynewbornnetworkorgresourcenewborn-services-rapid-health-facility-assessment
[13] M E Kruk M Myers S T Varpilah and B T Dahn ldquoWhat isa resilient health system Lessons from Ebolardquo The Lancet vol385 no 9980 pp 1910ndash1912 2015
[14] C Enweronu-Laryea K E Dickson S G Moxon et al ldquoBasicnewborn care and neonatal resuscitation a multi-countryanalysis of health system bottlenecks and potential solutionsrdquoBMCPregnancy and Childbirth vol 15 supplement 2 article 542015
[15] United Nations Office for the Coordination of HumanitarianAffairs (UN-OCHA) ldquoTyphoon HaiyanmdashHumanitarian Snap-shotrdquo Philippines (as of Nov 12 2013) Data Sources DSWDDROMICReport Nov 12 2013 NDRRMC Situation Report 14OCHO Situation Report 5 and UNDAC Reports

BioMed Research International 3
Baseline assessment
EINC training of
trainers (TOT)
Training via EINC QA workshops
1-monthposttrainingassessments
3-monthposttrainingassessments
Figure 1 Flow of assessments and interventions
health workers and mothers supplemented by review ofrecords Whenever possible deliveries were observed
In the priority municipalities primary level health facili-ties with the highest number of deliveries were intentionallyselected Based on usual patient traffic the biggest districthospital or rural health unit (RHU) and its correspondingbusiest lying-in clinic were selected subject to the limitedaccessibility of facilities after typhoon Haiyan In consider-ation of service delivery networks and referral flows withinand across municipalities assessments covered additionalmunicipalities beyond the 40 priority areas
The tool was used to assess facility-based delivery andnewborn care service capacity in primary and referral levelfacilities Gaps in newborn care health services were sys-tematically identified using tracer indicators Findings wereutilized to describe capacity to address three main causesof newborn deaths asphyxia prematurity and infectionDeterminants were classified as (a) service availability (b)equipment and supplies and (c) service standards
21 EINC Training of Trainers Updated EINC training mod-ules contained brief didactic sessions on basic topics Essen-tial Intrapartum and Newborn Care breastfeeding supportkangaroo mother care Infant and Young Child Feeding inEmergencies (IYCF-E) partograph use and the recentWHOrecommendations on basic newborn resuscitation correctadministration of magnesium sulfate and postnatal care ofmothers and newborns Skills sessions consisted of ldquocoachingsessionsrdquo with demonstrationreturn demonstrations usingmanikins and delivery kits Workshops culminated withaction planning sessions on effective mainstreaming of EINCin their practice These planning sessions allowed the partic-ipants to voice out their concerns and their apprehensionsand discuss among themselves ways to contextualize thesechallenges and address them
Training of trainers (TOT) workshops were conductedin the three regions Selection of trainees was strategic toinclude senior health care workers with aptitude to becometrainers in their respective service delivery networks (roughlycorresponding to geopolitical Interlocal Health Zones orILHZs) Representation of involved ILHZs was ensured asmuch as possible to create a pool of trainers to cascadethe training locally Local trainers were further chosen fromthis pool based on their performance during the TOT
Participants included thirty (30) trainees each from LeyteEastern and Western Samar Capiz Iloilo and Cebu
22 Cascade EINC Quality Assurance Workshops The tech-nical experts supervised and mentored the new local trainersas they implemented their own cascade quality assurance(QA) workshops In each of the areas two QA workshopsof 30 participants each were conducted targeting a totalof 300 capacitated skilled birth attendants QA workshopmodules for service providers were delivered over 6 half-daysessions Pre- to postworkshop acquisition of knowledge wasmeasured through 15 item multiple choice question writtenquizzes and acquisition of skills in the classroom assessmentsthrough performance checklists
23 Statistical Analysis Epi Info 6 was used for dataanalysis Categorical variables at baseline 1-month and 3-month after training presented as proportions () werecompared using Fisherrsquos exact and 1205942 tests with significanceset at 119901 lt 005
3 Results and Discussion
External experts supported the rehabilitation of EINC healthservices in 40 priority municipalities in Eastern Central andWesternVisayas severely devastated byHaiyan (See Figure 2)
As part of the service delivery networks additional areasadjacent to the priority municipalities were included namelyfour (4)municipalities and one city (Abuyog andOrmoc Cityin Leyte Basey in Western Samar and Barotac Viejo andBalasan in Iloilo) The grand total of 45 local governmentunits (LGUs) thus included three (3) cities (in Leyte) andforty-two (42) municipalities (see Figure 3)
31 Baseline Assessments (Table 1) Baseline rapid assess-ments were done at 16 weeks after landfall in Eastern Visayas(Leyte and Eastern and Western Samar) 20 weeks afterlandfall in Western Visayas (Iloilo and Capiz) and 22 weeksafter landfall in Central Visayas (Cebu) A total of 56 healthfacilities were assessed at baseline Assessments revealed sig-nificant disruption in obstetric and newborn health servicesin Eastern Visayas and much less significant disruption inCentral and Western Visayas
4 BioMed Research International
Figure 2 Path of typhoon Haiyan through central Philippines [15]
At baseline health facilities assessed ranged from ruralhealth units (RHU 39) first level referral hospitals (15community district and city hospitals) and in addition2 provincial hospitals with birthing services After typhoonHaiyan the physical devastation in Eastern Visayas causedthe most serious interruptions in EINC delivery Immediateresponse services were provided primarily through contri-butions from international partners in tents and makeshiftfacilities The lack of availability of 247 delivery servicesrevealed the importance of improved referral mechanismsthat could bring mothers experiencing complications duringor after birth to a higher level facility if neededThese findingsdiffered from the assessment of Central and Western Visayasmunicipalities where facilities mostly sustained partial dam-age with no interruption of birthing services
Apart from damage to infrastructure commodities werein serious shortage or absent with stock-outs of life-savingdrugs (eg oxytocin magnesium sulfate and dexametha-sone) Health human resources suffered serious setbacksnot only due to substantial loss of lives among health careproviders but also due to lack of training and technicalcapacity (in basic newborn resuscitation care of the low birthweight kangaroo mother care breastfeeding and Infant andYoung Child Feeding in Emergencies (IYCF-E)) In facilitieswhere health workers had participated in a previous 11-dayBasic Emergency Obstetric and Newborn Care (BEmONC)training low self-efficacy ratings especially in partographuse magnesium sulfate administration and newborn resus-citation rates were noted Very few facilities experiencedsupervisory visits in the previous 6 months None performedroutine postnatal care services Documentation of practiceswas weak Finally not all facilities conducted regular mater-nal and newborn death reviews
Table 1 Number of facilities assessed at pretraining (baseline) andat 1 month and 3 months posttraining by region and by province
RegionprovinceFacility level
Rural healthunit
First levelhospital
Provincialhospital
Eastern VisayasLeyteBaseline 15 4 11 month 16 5 13 months 12 4 1
SamarBaseline 11 4 11 month 11 4 13 months 10 4 0
Western VisayasCapizBaseline 3 3 01 month 3 3 03 months 3 3 0
IloiloBaseline 8 2 01 month 8 2 03 months 8 2 0
Central VisayasCebuBaseline 2 2 01 month 2 2 03 months 2 2 0
Progress in EINC implementation and quality improvement from baselineassessments through 1- and 3-month posttraining assessments
32 EINC Training of Trainers (TOT) Out of 150 candidatetrainers who were invited 112 (75) attended the trainingThese were maternal and child health workers holding strate-gic positions (provincial level program managers hospitalspecialists municipal health officers public health nursesandmidwife supervisors) A total of five (5) training of trainer(TOT) workshops of 3 daysrsquo duration each were conductedone each for the provinces of Leyte Eastern and WesternSamar Iloilo Capiz and Cebu
33 Cascade EINC QA Workshops As part of the trainingrequirement each TOT candidate trainer participated in atleast one of a total of ten (10) cascade QA workshops fortheir colleagues with supportive supervision and technicaloversight from expert trainers A total of 281 out of 300targeted skilled birth attendants (937) were further trained
Thus a total of 393 health workers completed EINCworkshops over this period 281 completed their participationin 3-day QA workshops and 112 attended the five TOT work-shops Consistent improvements in posttraining assessmentquizzes and performance checklists for both the TOT andQAworkshop participants were noted
BioMed Research International 5
Bukidnon
Sulu Sea
LeyteIloilo
Cebu
Samar
Bohol
Capiz
Negros Occidental
Albay
Masbate
Antique
Negros Oriental
Aklan
Eastern Samar
Sorsogon
Northern Samar
Agusan del Sur
Agusan del Norte
Misamis Oriental
QuezonCamarines Sur
Marinduque
Biliran
Romblon
Southern Leyte
Surigao del Norte
Guimaras
Dinagat Islands
Zamboanga del Norte
SiquijorSurigao del Sur
Misamis Occidental
Camiguin
Catanduanes
Bohol Sea
Philippine Sea
Sibuyan Sea
Visayan Sea
Samar Sea
Leyte Gulf
Ragay Gulf
Surigao Strait
Tayabas Bay
Map shows PhilippinesUNICEF Haiyan programmeareas and typhoon Haiyanpath
Disclaimer the boundaries and names shown and the designations used in this map do not imply official endorsement or acceptance by the United Nations
0 10 20 30 405(Kilometers)
Data source UNICEFDate of data source 14 Dec 2014Map sources NE COD GADMMap production date 06 March 2016Feedback jbacaluniceforg
ScaleProgramme areas
HaiyanTyphoon Haiyan path
VIII
VIIVI
Capiz
IloiloVI IloiloVI IloiloVIVI
CapizVICapizVICapizVICapizVICapizVICapizVICapizVICapizVICapizVI
Iloilo
CebuVII CebuVII Cebu
Eastern SamarVIII Eastern SamarVIII Eastern SamarVIII Eastern SamarVIII Eastern SamarVIII Eastern SamarVIII Eastern SamarVIII Eastern SamarVIII Eastern SamarVIIIVIII
Eastern Samar
Samar
LeyteVIII LeyteVIII LeyteVIII LeyteVIII LeyteVIII LeyteVIII LeyteVIII LeyteVIII LeyteVIII LeyteVIII LeyteVIII LeyteVIII LeyteVIII LeyteVIII LeyteVIII LeyteVIII LeyteVIII LeyteVIII LeyteVIII LeyteVIII LeyteVIII
IvisanJamindanMa-AyonPanayPanitanPilarPontevedraPresident RoxasRoxas CityTapazCarlesConcepcionEstanciaSaraBantayanCebu CityDaanbantayanBalangigaBalangkayanBorongan CityGiporlosGuiuanHernaniLawaanMercedesQuinapondanSalcedoAlangalangBurauenCarigaraDagamiDulagIsabelJaroJulitaKanangaLa PazMacarthurMatag-ObMayorgaMeridaPaloPastranaSan MiguelTabontabonTacloban CityTanauanVillabaMarabut
998400Region 4B
998400Region 4A
998400Region 5
998400Region 8
998400Region 6
998400Region 7
998400Region 9
998400Region 10
998400Region Caraga
1 cm = 16km
Region Province Municipilaty
Philippines UNICEF Haiyan programme areas
N
Figure 3 40 priority municipalities listed in orange box and shaded in map
6 BioMed Research International
96 98 98 98
16 22
17 96 98
94
0 10()
20 30 40 50 60 70 80 90 100
Service availability indicators at baseline and at 1- and 3-month posttraining assessment in Eastern Western and
Central Visayas Philippines 2013
3-month PTA 1-month PTA Baseline
Kangaroo mother carelowastAntenatal steroidslowast
Neonatal resuscitationlowast
Manual removal of retained products after deliveryManual placental removal
Assisted vaginal deliveryParenteral magnesium sulfatelowast
Parenteral oxytocinlowast
Parenteral antibioticslowast247 skilled birth attendancelowast
lowastIndicates significant change from baseline to 3-month PTA p lt 005
Figure 4 Proportion of facilities assessed providing various services at pretraining (baseline) and at 1 and 3 months posttraining assessment(PTA) Eastern Western and Central Visayas post-Haiyan
34 Posttraining Assessments (Table 1) At 1 month and 3months after training field visits to 58 and 51 facilities respec-tively were carried out The facilities that completed the 3assessments were thirty-five (35) rural health units (RHUs)15 primary level hospitals (13 district 1 city and 1 communityhospitals) and one (1) provincial hospital These field visitsrevealed that uptake of EINC knowledge and skills was trans-lated to significant changes in daily practice Posttrainingassessment visits revealed good evidence of changes in thephysical environments in the labordelivery and postpartumareas and implementation of many of the EINC practices
However apart from the overall improvement someposttraining gaps were identified (1) not allowing a com-panion of choice (2) nonadministration of birth dosesof BCG vaccine (3) unavailability of nevirapine therapy(4) unavailability of protocols or guidelines for IntegratedManagement of Pregnancy and Childbirth (IMPAC) referralof sick newborns Comprehensive Emergency Obstetric andNewborn Care (CEmONC) and preterm labormanagement(5) absence of soap and hand disinfectants in postnatal areas
35 Service Availability (Figure 4) In Eastern Visayas theworst hit region baseline assessment revealed that 27 of 36facilities were providing birthing services At 1 month aftertraining 32 of 38 assessed birthing facilities were providinground-the-clockdaily (247) skilled birth attendance (SBA)At 3 months 30 of 31 birthing facilities were providing 247SBA InWesternVisayas 16 of 16 facilities were able to sustaindelivery services at baseline and 1 month assessments Onefacility suspended its delivery services to undergo renova-tions at the 3-month assessment All of the 15 other facilitieswere providing 247 SBA In Central Visayas all 4 facilitiesassessed were providing 247 SBA at baseline 1-monthand 3-month assessments Over the period from baselineassessment to 3 months after training there were significantimprovements in self-reported availability of services such as
neonatal resuscitation kangaroomother care administrationof parenteral oxytocin antibiotics antenatal steroids andmagnesium sulfate In contrast persistent gaps remainedfor assisted vaginal delivery manual placental removal andmanual removal of retained products after delivery In Figures4ndash6 the proportion of facilities () at end line (3months aftertraining) is labeled
36 Equipment and Supplies (Figure 5) Over the period frombaseline assessment to 3 months after training (20-week 19-week and 14-week periods for Eastern Western and Cen-tral Visayas resp) there were significant improvements inavailability of life-saving drugs (ie oxytocin) and equipment(ie for resuscitation) most notably for Eastern and CentralVisayas For Western Visayas some improvements were seenin the facilities but the limited availability of equipmentconstrained the appropriate delivery of services Not all life-saving drugs were available in all facilities especially antibi-otics and steroids
Though there was significant improvement persistentgaps remained for antenatal steroids injectable gentamicinand magnesium sulfate supplies Towels for drying werestill being provided by families instead of by facilitiesNevirapine for prevention of mother-to-child transmissionof HIV remained unavailable across all regions MultidoseBCG vaccines were available but considered ldquoinsufficientrdquo byhealth workers Many facilities had moved their weighingscales from their delivery areas to their maternity careareas for deferred weighing until after the first breastfeedas recommended in EINC protocols Protocols for IMPACsick newborn carereferral preterm labor management andCEmONCmanuals remain unavailable
37 Service Standards (Figure 6) In addition to parametersincluded in the Newborn Care Services Rapid AssessmentTool selected parameters relevant to the Philippines EINC
BioMed Research International 7
69 88
86 96
84 4
73 2
57 98
71
0 10 20 30 40 50()
60 70 80 90 100
Equipment and supplies availability at baseline and at 1- month and 3-month posttraining assessment in Eastern
Western and Central Visayas Philippines 2013
3-month PTA 1-month PTA Baseline
Magnesium sulfateInjectable uterotoniclowast
CorticosteroidsPMTCT drugslowast
Injectable gentamicinTowels for drying
Soap or hand disinfectantInfant scalelowast
lowastResuscitation tableNewborn bag and masklowast
Up-to-date delivery register
lowastIndicates significant change from baseline to 3-month PTA p lt 005
Figure 5 Proportion of facilities assessed to have various equipment and supplies at pretraining (baseline) and at 1 and 3months posttrainingassessment (PTA) Eastern Western and Central Visayas post-Haiyan
87 58
96 84
0 98 98
86 80
84 82
92 76
70 72
70
0 10 20 30 40 50()
60 70 80 90 100
Service standards indicators at baseline and at 1-month and 3-month posttrainingassessment in Eastern Western and Central Visayas Philippines 2013
Companion of choiceAllowed to eatdrink
Selective episiotomyperineal supportAMTSLlowast
Partograph filled out correctlylowast
Immediatethorough dryingSkin-to-skin contact
Properly timed cord clampingNonseparation and initiation of Breastfeeding
Eye carelowast
Vitamin Klowast
BCG birth doseHepatitis B birth dose
Wall clock in delivery arealowast
Room thermometer in delivery arealowast
Size 0 or preterm masklowast
3-month PTA 1-month PTA Baseline
lowastIndicates significant change from baseline to3-month PTA p lt 005
Figure 6 Proportion of facilities assessed to be implementing various service standards at pretraining (baseline) and at 1 and 3 monthsposttraining assessment (PTA) Eastern Western and Central Visayas post-Haiyan
8 BioMed Research International
Protocol and Basic Emergency Obstetric and Newborn Care(BEmONC) services standards were assessed through inter-views of health service providers
Significant improvements in service standards usingtracer indicators were noted across all regions over the periodfrom pretraining assessment to the 3 months posttrainingassessment Most notable were performance of the EINCldquocore stepsrdquo in immediate newborn care proper WHOpartograph use and availability of size 0 face masks forresuscitation of preterms which improved from 0 to 100at 3 months posttraining assessment
Quality labor and delivery for mothers (companion ofchoice allowing mothers to eatdrink semiupright deliverybed perineal support and restrictive episiotomy and activemanagement of the third stage of labor) and quality post-partum care (monitoring vital signs uterine massage andpostpartum visit within first week and then within fourthto sixth weeks after discharge) were carried out Facilitiesreported performance of the ldquocore stepsrdquo of immediatenewborn care (immediate and thorough drying skin-to-skincontact properly timed cord clamping and nonseparation ofnewborn from mother for early breastfeeding) and routinenewborn care (eye care physical examination and vitamin Kadministration) Postpartumwomen interviewed in the facil-ities verified the consistency of applying the EINC protocol
A persistent gap in EINC standard practice was the birthdose of BCG vaccine Ninety-six percent of facilities were notadministering this birth dose as recommended by nationalguidelines citing that using the available multidose vials foronly a few patients at each time constitutes ldquowastagerdquo Thisreflects the common practice of deferring the BCG vaccina-tion to the first-postnatal visit in the Philippines Number ofroom thermometers and wall clocks had increased in somefacilities
UnlikeWestern Visayas the 4 facilities in Central Visayashad newborn resuscitator bags and masks available priorto the EINC intervention With the intervention howeverhealth workers reported increased confidence in their newlyacquired resuscitation skills Wall clocks were present indelivery areas in all 4 facilities assessed from baseline to endline Room thermometers absent at baseline in all facilitieswere available in all 4 facilities and end line
Across the 3 regions significant improvements in servicestandards were documented In 2008 coverage of early skin-to-skin contact (SSC) was documented at 96 in deliveryassessments in 51 government hospitals [7] After governmentefforts at EINC scale-up SSC coverage was at 64 bymaternal report in 2013 [10] In this study SSC was at84 in primary level facilities postdisaster by health workerreport Before Haiyan barriers to EINC implementation thatis absence of enabling physical and policy environmentsnoncompliance by specialists and other ldquoexpertsrdquo unfamiliarwith the updated EINC practices had been diminished butnot eliminated The devastation brought by Haiyan disman-tled the systems that enabled EINC practice Neverthelessover a 3-month period an intervention of training andposttraining assessments was able to restore and for someEINC practices even exceed pre-Haiyan coverage rates
The high coverage rates for EINC indicators at baselinesuggests that previous scale-up efforts in EINC and othercross-cutting areas increased the potential for resilienceThis complemented assistance offered by other humanitarianactors (eg infrastructure rehabilitation and provision ofsupplies and equipment) turning this into an opportunity toldquobuild back betterrdquo However the contribution of pre-Haiyancapacity building efforts to this rapid restoration and furtherimprovement of EINC services requires further evaluationWe postulate that if capacity building efforts have establishedenabling environments under normal circumstances rehabil-itation could be achieved in similarly brief time periodsThuscapacity building for EINC may potentially be considered asan important disaster preparedness measure
Aiming to improve the sustainability of this interventionthe external experts provided close supportive supervisionduring the cascade training sessions and the two posttrainingassessments Our experience reveals that both performanceand environments have improved creating an enabling envi-ronment for EINC practices There were still aspects thatrequired improvement that could be reinforced by the localhealth officials during supervisory visits However this can bea challenge in areas where regular supervision visits are raredue to difficulties in geographic access or security constraints
Government support was provided through so-calledInterlocal Health Zones (ILHZs) utilizing existing referralnetworks often with rural health units (RHUs) and districthospitals as the focal point Trainers were capacitated asILHZ groups for subsequent roll-out through a skills transfermethodology This approach had its limitation though astrained health care providers from one ILHZ in generalcould not be tapped to train health care workers of anotherILHZ
In the aftermath of the disaster several developmentand recovery activities resulted in competing schedules(eg water sanitation and hygiene (WASH) vaccine coldchain implementation etc) making it difficult to scheduletraining dates Often competing capacity building activitiesand the local rehabilitation efforts involved the same setof (limited) local manpower Consequently mobilizing localstaffs to implement their trainersrsquo knowledge in cascade QAworkshops proved difficult Another constraint posed thehealth human resource availability after the disaster sincemany health care workers were victims themselves
The postdisaster setting likewise presented more chal-lenges in conducting capacity building interventions In somegeographic areas communication and road infrastructurecontinued to be unusable making it difficult for healthworkers to attend trainings or gather local data This post-disaster scenario constrained us to ldquopre- to postinterventionassessmentrdquo and its inherent methodologic limitations
This study was also limited by the fact that not all facilitieswho participated in baseline assessment were included inthe posttraining assessment Thus this study could benefitfrom another evaluation after a longer interval posttrain-ing to assess newborn outcome indicators sustainability ofimprovements and further analysis on possible contributoryeffects of other sectoral interventions (eg WASH) and
BioMed Research International 9
partner efforts in the areas The contribution of predisastercapacity building to the results could not be studied
4 Conclusions
This intervention filled the service gaps identified immedi-ately after a large scale natural disaster and helped to reestab-lish and improve the delivery of health services in affectedareas Where baseline indices were worse because of theimmediate effects of the typhoon (ie Eastern Visayas) themagnitude of improvement across most assessed parameterswas more significant However there were other parameterswhere gaps persist despite intensive efforts and othermethodsand systemic interventions need to be explored address thesedeficiencies
Our study demonstrates that quick important qualityimprovements can bemade in a timelymanner across a rangeof health facilities andwith differing cadres of health workerseven in immediate postdisaster settings Capacity building ofhealth workers and strengthening of the local health systemto deliver quality care before during and in the aftermath ofa major disaster are among the preconditions for a resilienthealth system [13] Building the evidence base linking thesequality improvement efforts in EINC and basic newbornresuscitation with impact on newborn and maternal healthoutcomes postdisaster is imperative [14]
Disclosure
Any opinions stated by UNICEF affiliates are those of theauthors and not of UNICEF
Competing Interests
The authors declare no competing interests regarding thepublication of this paper
Acknowledgments
Funding support was provided by UNICEF The authorswould like to thank our colleagues in the Department ofHealth Regional Health Offices of Eastern Central andWestern Visayas (especially Drs Corazon Sabulao and AlmaBernardo) the Provincial Health Offices of Capiz CebuIloilo Leyte and Eastern and Western Samar (especiallyDrs Samuel Delfin Cynthia Genosolango Grace Trabadoand Marian Isiderio) Dr Nabila Zaka (UNICEF) and theInternational Medical Corps
References
[1] October 2015 httplibrarypcwgovphsitesdefaultfiles14011120SDR20Yolanda20Philippnes20finalpdf
[2] ldquoResponding toTyphoonHaiyanrdquoTheLancet vol 382 no 9907article 1769 2013
[3] R C Alfonso D S Capili K A Reyes F Tatad-To and M ASilvestre ldquoContributing to the Infant and Young Child Feedingin Emergencies (IYCF-E) response in the Philippines A local
NGOperspectiverdquo 2015 httpwwwennonlinenetfex50iycf-philippines
[4] WHO Philippines ldquoEssential Intrapartum and Newborn Care(EINC) Evidence-based Standard Practicesrdquo 2016 httpwwwwprowhointphilippinesareasmaternal child nutritionnew-born mother careeinc protocolsen
[5] WHO WPRO ldquoEarly Essential Newborn Care First EmbraceClinical Practice Pocket Guiderdquo 2014 httpiriswprowhointbitstreamhandle106651107989789290616856 engpdfjsessi-onid=B789B68B6D8BF8BB2C7F99F09E698AE1sequence=3
[6] H Obara and H Sobel ldquoQuality maternal and newborn care toensure a healthy start for every newborn in the World HealthOrganization Western Pacific Regionrdquo BJOG An InternationalJournal of Obstetrics andGynaecology vol 121 pp 154ndash159 2014
[7] H L Sobel M A A Silvestre J B V Mantaring III Y EOliveros and S Nyunt-U ldquoImmediate newborn care practicesdelay thermoregulation and breastfeeding initiationrdquo Acta Pae-diatrica International Journal of Paediatrics vol 100 no 8 pp1127ndash1133 2011
[8] Z A Bhutta J K Das R Bahl et al ldquoEvery newborn canavailable interventions end preventable deaths in mothersnewborn babies and stillbirths and at what costrdquo The Lancetvol 384 no 9940 pp 347ndash370 2014
[9] E Duysburgh B Kerstens M Diaz et al ldquoNewborn care inIndonesia Lao Peoplersquos Democratic Republic and the Philip-pines a comprehensive needs assessmentrdquo BMC Pediatrics vol14 no 1 article 46 2014
[10] Philippine Statistics Authority (PSA) and ICF InternationalPhilippines National Demographic and Health Survey 2013Philippine Statistics Authority (PSA) Manila Philippines ICFInternational Rockville Md USA 2014
[11] Philippine Public StormSignals 2015 httpdrrmregion4adostgovphknowledge-management-center7Philippine-public-storm-signalshtml
[12] Healthy Newborn Network (HNN) Inter-agency NewbornIndicators Technical Working Group 2012 Newborn ServicesRapid Health Facility Assessment tool 2016 httpwwwheal-thynewbornnetworkorgresourcenewborn-services-rapid-health-facility-assessment
[13] M E Kruk M Myers S T Varpilah and B T Dahn ldquoWhat isa resilient health system Lessons from Ebolardquo The Lancet vol385 no 9980 pp 1910ndash1912 2015
[14] C Enweronu-Laryea K E Dickson S G Moxon et al ldquoBasicnewborn care and neonatal resuscitation a multi-countryanalysis of health system bottlenecks and potential solutionsrdquoBMCPregnancy and Childbirth vol 15 supplement 2 article 542015
[15] United Nations Office for the Coordination of HumanitarianAffairs (UN-OCHA) ldquoTyphoon HaiyanmdashHumanitarian Snap-shotrdquo Philippines (as of Nov 12 2013) Data Sources DSWDDROMICReport Nov 12 2013 NDRRMC Situation Report 14OCHO Situation Report 5 and UNDAC Reports

4 BioMed Research International
Figure 2 Path of typhoon Haiyan through central Philippines [15]
At baseline health facilities assessed ranged from ruralhealth units (RHU 39) first level referral hospitals (15community district and city hospitals) and in addition2 provincial hospitals with birthing services After typhoonHaiyan the physical devastation in Eastern Visayas causedthe most serious interruptions in EINC delivery Immediateresponse services were provided primarily through contri-butions from international partners in tents and makeshiftfacilities The lack of availability of 247 delivery servicesrevealed the importance of improved referral mechanismsthat could bring mothers experiencing complications duringor after birth to a higher level facility if neededThese findingsdiffered from the assessment of Central and Western Visayasmunicipalities where facilities mostly sustained partial dam-age with no interruption of birthing services
Apart from damage to infrastructure commodities werein serious shortage or absent with stock-outs of life-savingdrugs (eg oxytocin magnesium sulfate and dexametha-sone) Health human resources suffered serious setbacksnot only due to substantial loss of lives among health careproviders but also due to lack of training and technicalcapacity (in basic newborn resuscitation care of the low birthweight kangaroo mother care breastfeeding and Infant andYoung Child Feeding in Emergencies (IYCF-E)) In facilitieswhere health workers had participated in a previous 11-dayBasic Emergency Obstetric and Newborn Care (BEmONC)training low self-efficacy ratings especially in partographuse magnesium sulfate administration and newborn resus-citation rates were noted Very few facilities experiencedsupervisory visits in the previous 6 months None performedroutine postnatal care services Documentation of practiceswas weak Finally not all facilities conducted regular mater-nal and newborn death reviews
Table 1 Number of facilities assessed at pretraining (baseline) andat 1 month and 3 months posttraining by region and by province
RegionprovinceFacility level
Rural healthunit
First levelhospital
Provincialhospital
Eastern VisayasLeyteBaseline 15 4 11 month 16 5 13 months 12 4 1
SamarBaseline 11 4 11 month 11 4 13 months 10 4 0
Western VisayasCapizBaseline 3 3 01 month 3 3 03 months 3 3 0
IloiloBaseline 8 2 01 month 8 2 03 months 8 2 0
Central VisayasCebuBaseline 2 2 01 month 2 2 03 months 2 2 0
Progress in EINC implementation and quality improvement from baselineassessments through 1- and 3-month posttraining assessments
32 EINC Training of Trainers (TOT) Out of 150 candidatetrainers who were invited 112 (75) attended the trainingThese were maternal and child health workers holding strate-gic positions (provincial level program managers hospitalspecialists municipal health officers public health nursesandmidwife supervisors) A total of five (5) training of trainer(TOT) workshops of 3 daysrsquo duration each were conductedone each for the provinces of Leyte Eastern and WesternSamar Iloilo Capiz and Cebu
33 Cascade EINC QA Workshops As part of the trainingrequirement each TOT candidate trainer participated in atleast one of a total of ten (10) cascade QA workshops fortheir colleagues with supportive supervision and technicaloversight from expert trainers A total of 281 out of 300targeted skilled birth attendants (937) were further trained
Thus a total of 393 health workers completed EINCworkshops over this period 281 completed their participationin 3-day QA workshops and 112 attended the five TOT work-shops Consistent improvements in posttraining assessmentquizzes and performance checklists for both the TOT andQAworkshop participants were noted
BioMed Research International 5
Bukidnon
Sulu Sea
LeyteIloilo
Cebu
Samar
Bohol
Capiz
Negros Occidental
Albay
Masbate
Antique
Negros Oriental
Aklan
Eastern Samar
Sorsogon
Northern Samar
Agusan del Sur
Agusan del Norte
Misamis Oriental
QuezonCamarines Sur
Marinduque
Biliran
Romblon
Southern Leyte
Surigao del Norte
Guimaras
Dinagat Islands
Zamboanga del Norte
SiquijorSurigao del Sur
Misamis Occidental
Camiguin
Catanduanes
Bohol Sea
Philippine Sea
Sibuyan Sea
Visayan Sea
Samar Sea
Leyte Gulf
Ragay Gulf
Surigao Strait
Tayabas Bay
Map shows PhilippinesUNICEF Haiyan programmeareas and typhoon Haiyanpath
Disclaimer the boundaries and names shown and the designations used in this map do not imply official endorsement or acceptance by the United Nations
0 10 20 30 405(Kilometers)
Data source UNICEFDate of data source 14 Dec 2014Map sources NE COD GADMMap production date 06 March 2016Feedback jbacaluniceforg
ScaleProgramme areas
HaiyanTyphoon Haiyan path
VIII
VIIVI
Capiz
IloiloVI IloiloVI IloiloVIVI
CapizVICapizVICapizVICapizVICapizVICapizVICapizVICapizVICapizVI
Iloilo
CebuVII CebuVII Cebu
Eastern SamarVIII Eastern SamarVIII Eastern SamarVIII Eastern SamarVIII Eastern SamarVIII Eastern SamarVIII Eastern SamarVIII Eastern SamarVIII Eastern SamarVIIIVIII
Eastern Samar
Samar
LeyteVIII LeyteVIII LeyteVIII LeyteVIII LeyteVIII LeyteVIII LeyteVIII LeyteVIII LeyteVIII LeyteVIII LeyteVIII LeyteVIII LeyteVIII LeyteVIII LeyteVIII LeyteVIII LeyteVIII LeyteVIII LeyteVIII LeyteVIII LeyteVIII
IvisanJamindanMa-AyonPanayPanitanPilarPontevedraPresident RoxasRoxas CityTapazCarlesConcepcionEstanciaSaraBantayanCebu CityDaanbantayanBalangigaBalangkayanBorongan CityGiporlosGuiuanHernaniLawaanMercedesQuinapondanSalcedoAlangalangBurauenCarigaraDagamiDulagIsabelJaroJulitaKanangaLa PazMacarthurMatag-ObMayorgaMeridaPaloPastranaSan MiguelTabontabonTacloban CityTanauanVillabaMarabut
998400Region 4B
998400Region 4A
998400Region 5
998400Region 8
998400Region 6
998400Region 7
998400Region 9
998400Region 10
998400Region Caraga
1 cm = 16km
Region Province Municipilaty
Philippines UNICEF Haiyan programme areas
N
Figure 3 40 priority municipalities listed in orange box and shaded in map
6 BioMed Research International
96 98 98 98
16 22
17 96 98
94
0 10()
20 30 40 50 60 70 80 90 100
Service availability indicators at baseline and at 1- and 3-month posttraining assessment in Eastern Western and
Central Visayas Philippines 2013
3-month PTA 1-month PTA Baseline
Kangaroo mother carelowastAntenatal steroidslowast
Neonatal resuscitationlowast
Manual removal of retained products after deliveryManual placental removal
Assisted vaginal deliveryParenteral magnesium sulfatelowast
Parenteral oxytocinlowast
Parenteral antibioticslowast247 skilled birth attendancelowast
lowastIndicates significant change from baseline to 3-month PTA p lt 005
Figure 4 Proportion of facilities assessed providing various services at pretraining (baseline) and at 1 and 3 months posttraining assessment(PTA) Eastern Western and Central Visayas post-Haiyan
34 Posttraining Assessments (Table 1) At 1 month and 3months after training field visits to 58 and 51 facilities respec-tively were carried out The facilities that completed the 3assessments were thirty-five (35) rural health units (RHUs)15 primary level hospitals (13 district 1 city and 1 communityhospitals) and one (1) provincial hospital These field visitsrevealed that uptake of EINC knowledge and skills was trans-lated to significant changes in daily practice Posttrainingassessment visits revealed good evidence of changes in thephysical environments in the labordelivery and postpartumareas and implementation of many of the EINC practices
However apart from the overall improvement someposttraining gaps were identified (1) not allowing a com-panion of choice (2) nonadministration of birth dosesof BCG vaccine (3) unavailability of nevirapine therapy(4) unavailability of protocols or guidelines for IntegratedManagement of Pregnancy and Childbirth (IMPAC) referralof sick newborns Comprehensive Emergency Obstetric andNewborn Care (CEmONC) and preterm labormanagement(5) absence of soap and hand disinfectants in postnatal areas
35 Service Availability (Figure 4) In Eastern Visayas theworst hit region baseline assessment revealed that 27 of 36facilities were providing birthing services At 1 month aftertraining 32 of 38 assessed birthing facilities were providinground-the-clockdaily (247) skilled birth attendance (SBA)At 3 months 30 of 31 birthing facilities were providing 247SBA InWesternVisayas 16 of 16 facilities were able to sustaindelivery services at baseline and 1 month assessments Onefacility suspended its delivery services to undergo renova-tions at the 3-month assessment All of the 15 other facilitieswere providing 247 SBA In Central Visayas all 4 facilitiesassessed were providing 247 SBA at baseline 1-monthand 3-month assessments Over the period from baselineassessment to 3 months after training there were significantimprovements in self-reported availability of services such as
neonatal resuscitation kangaroomother care administrationof parenteral oxytocin antibiotics antenatal steroids andmagnesium sulfate In contrast persistent gaps remainedfor assisted vaginal delivery manual placental removal andmanual removal of retained products after delivery In Figures4ndash6 the proportion of facilities () at end line (3months aftertraining) is labeled
36 Equipment and Supplies (Figure 5) Over the period frombaseline assessment to 3 months after training (20-week 19-week and 14-week periods for Eastern Western and Cen-tral Visayas resp) there were significant improvements inavailability of life-saving drugs (ie oxytocin) and equipment(ie for resuscitation) most notably for Eastern and CentralVisayas For Western Visayas some improvements were seenin the facilities but the limited availability of equipmentconstrained the appropriate delivery of services Not all life-saving drugs were available in all facilities especially antibi-otics and steroids
Though there was significant improvement persistentgaps remained for antenatal steroids injectable gentamicinand magnesium sulfate supplies Towels for drying werestill being provided by families instead of by facilitiesNevirapine for prevention of mother-to-child transmissionof HIV remained unavailable across all regions MultidoseBCG vaccines were available but considered ldquoinsufficientrdquo byhealth workers Many facilities had moved their weighingscales from their delivery areas to their maternity careareas for deferred weighing until after the first breastfeedas recommended in EINC protocols Protocols for IMPACsick newborn carereferral preterm labor management andCEmONCmanuals remain unavailable
37 Service Standards (Figure 6) In addition to parametersincluded in the Newborn Care Services Rapid AssessmentTool selected parameters relevant to the Philippines EINC
BioMed Research International 7
69 88
86 96
84 4
73 2
57 98
71
0 10 20 30 40 50()
60 70 80 90 100
Equipment and supplies availability at baseline and at 1- month and 3-month posttraining assessment in Eastern
Western and Central Visayas Philippines 2013
3-month PTA 1-month PTA Baseline
Magnesium sulfateInjectable uterotoniclowast
CorticosteroidsPMTCT drugslowast
Injectable gentamicinTowels for drying
Soap or hand disinfectantInfant scalelowast
lowastResuscitation tableNewborn bag and masklowast
Up-to-date delivery register
lowastIndicates significant change from baseline to 3-month PTA p lt 005
Figure 5 Proportion of facilities assessed to have various equipment and supplies at pretraining (baseline) and at 1 and 3months posttrainingassessment (PTA) Eastern Western and Central Visayas post-Haiyan
87 58
96 84
0 98 98
86 80
84 82
92 76
70 72
70
0 10 20 30 40 50()
60 70 80 90 100
Service standards indicators at baseline and at 1-month and 3-month posttrainingassessment in Eastern Western and Central Visayas Philippines 2013
Companion of choiceAllowed to eatdrink
Selective episiotomyperineal supportAMTSLlowast
Partograph filled out correctlylowast
Immediatethorough dryingSkin-to-skin contact
Properly timed cord clampingNonseparation and initiation of Breastfeeding
Eye carelowast
Vitamin Klowast
BCG birth doseHepatitis B birth dose
Wall clock in delivery arealowast
Room thermometer in delivery arealowast
Size 0 or preterm masklowast
3-month PTA 1-month PTA Baseline
lowastIndicates significant change from baseline to3-month PTA p lt 005
Figure 6 Proportion of facilities assessed to be implementing various service standards at pretraining (baseline) and at 1 and 3 monthsposttraining assessment (PTA) Eastern Western and Central Visayas post-Haiyan
8 BioMed Research International
Protocol and Basic Emergency Obstetric and Newborn Care(BEmONC) services standards were assessed through inter-views of health service providers
Significant improvements in service standards usingtracer indicators were noted across all regions over the periodfrom pretraining assessment to the 3 months posttrainingassessment Most notable were performance of the EINCldquocore stepsrdquo in immediate newborn care proper WHOpartograph use and availability of size 0 face masks forresuscitation of preterms which improved from 0 to 100at 3 months posttraining assessment
Quality labor and delivery for mothers (companion ofchoice allowing mothers to eatdrink semiupright deliverybed perineal support and restrictive episiotomy and activemanagement of the third stage of labor) and quality post-partum care (monitoring vital signs uterine massage andpostpartum visit within first week and then within fourthto sixth weeks after discharge) were carried out Facilitiesreported performance of the ldquocore stepsrdquo of immediatenewborn care (immediate and thorough drying skin-to-skincontact properly timed cord clamping and nonseparation ofnewborn from mother for early breastfeeding) and routinenewborn care (eye care physical examination and vitamin Kadministration) Postpartumwomen interviewed in the facil-ities verified the consistency of applying the EINC protocol
A persistent gap in EINC standard practice was the birthdose of BCG vaccine Ninety-six percent of facilities were notadministering this birth dose as recommended by nationalguidelines citing that using the available multidose vials foronly a few patients at each time constitutes ldquowastagerdquo Thisreflects the common practice of deferring the BCG vaccina-tion to the first-postnatal visit in the Philippines Number ofroom thermometers and wall clocks had increased in somefacilities
UnlikeWestern Visayas the 4 facilities in Central Visayashad newborn resuscitator bags and masks available priorto the EINC intervention With the intervention howeverhealth workers reported increased confidence in their newlyacquired resuscitation skills Wall clocks were present indelivery areas in all 4 facilities assessed from baseline to endline Room thermometers absent at baseline in all facilitieswere available in all 4 facilities and end line
Across the 3 regions significant improvements in servicestandards were documented In 2008 coverage of early skin-to-skin contact (SSC) was documented at 96 in deliveryassessments in 51 government hospitals [7] After governmentefforts at EINC scale-up SSC coverage was at 64 bymaternal report in 2013 [10] In this study SSC was at84 in primary level facilities postdisaster by health workerreport Before Haiyan barriers to EINC implementation thatis absence of enabling physical and policy environmentsnoncompliance by specialists and other ldquoexpertsrdquo unfamiliarwith the updated EINC practices had been diminished butnot eliminated The devastation brought by Haiyan disman-tled the systems that enabled EINC practice Neverthelessover a 3-month period an intervention of training andposttraining assessments was able to restore and for someEINC practices even exceed pre-Haiyan coverage rates
The high coverage rates for EINC indicators at baselinesuggests that previous scale-up efforts in EINC and othercross-cutting areas increased the potential for resilienceThis complemented assistance offered by other humanitarianactors (eg infrastructure rehabilitation and provision ofsupplies and equipment) turning this into an opportunity toldquobuild back betterrdquo However the contribution of pre-Haiyancapacity building efforts to this rapid restoration and furtherimprovement of EINC services requires further evaluationWe postulate that if capacity building efforts have establishedenabling environments under normal circumstances rehabil-itation could be achieved in similarly brief time periodsThuscapacity building for EINC may potentially be considered asan important disaster preparedness measure
Aiming to improve the sustainability of this interventionthe external experts provided close supportive supervisionduring the cascade training sessions and the two posttrainingassessments Our experience reveals that both performanceand environments have improved creating an enabling envi-ronment for EINC practices There were still aspects thatrequired improvement that could be reinforced by the localhealth officials during supervisory visits However this can bea challenge in areas where regular supervision visits are raredue to difficulties in geographic access or security constraints
Government support was provided through so-calledInterlocal Health Zones (ILHZs) utilizing existing referralnetworks often with rural health units (RHUs) and districthospitals as the focal point Trainers were capacitated asILHZ groups for subsequent roll-out through a skills transfermethodology This approach had its limitation though astrained health care providers from one ILHZ in generalcould not be tapped to train health care workers of anotherILHZ
In the aftermath of the disaster several developmentand recovery activities resulted in competing schedules(eg water sanitation and hygiene (WASH) vaccine coldchain implementation etc) making it difficult to scheduletraining dates Often competing capacity building activitiesand the local rehabilitation efforts involved the same setof (limited) local manpower Consequently mobilizing localstaffs to implement their trainersrsquo knowledge in cascade QAworkshops proved difficult Another constraint posed thehealth human resource availability after the disaster sincemany health care workers were victims themselves
The postdisaster setting likewise presented more chal-lenges in conducting capacity building interventions In somegeographic areas communication and road infrastructurecontinued to be unusable making it difficult for healthworkers to attend trainings or gather local data This post-disaster scenario constrained us to ldquopre- to postinterventionassessmentrdquo and its inherent methodologic limitations
This study was also limited by the fact that not all facilitieswho participated in baseline assessment were included inthe posttraining assessment Thus this study could benefitfrom another evaluation after a longer interval posttrain-ing to assess newborn outcome indicators sustainability ofimprovements and further analysis on possible contributoryeffects of other sectoral interventions (eg WASH) and
BioMed Research International 9
partner efforts in the areas The contribution of predisastercapacity building to the results could not be studied
4 Conclusions
This intervention filled the service gaps identified immedi-ately after a large scale natural disaster and helped to reestab-lish and improve the delivery of health services in affectedareas Where baseline indices were worse because of theimmediate effects of the typhoon (ie Eastern Visayas) themagnitude of improvement across most assessed parameterswas more significant However there were other parameterswhere gaps persist despite intensive efforts and othermethodsand systemic interventions need to be explored address thesedeficiencies
Our study demonstrates that quick important qualityimprovements can bemade in a timelymanner across a rangeof health facilities andwith differing cadres of health workerseven in immediate postdisaster settings Capacity building ofhealth workers and strengthening of the local health systemto deliver quality care before during and in the aftermath ofa major disaster are among the preconditions for a resilienthealth system [13] Building the evidence base linking thesequality improvement efforts in EINC and basic newbornresuscitation with impact on newborn and maternal healthoutcomes postdisaster is imperative [14]
Disclosure
Any opinions stated by UNICEF affiliates are those of theauthors and not of UNICEF
Competing Interests
The authors declare no competing interests regarding thepublication of this paper
Acknowledgments
Funding support was provided by UNICEF The authorswould like to thank our colleagues in the Department ofHealth Regional Health Offices of Eastern Central andWestern Visayas (especially Drs Corazon Sabulao and AlmaBernardo) the Provincial Health Offices of Capiz CebuIloilo Leyte and Eastern and Western Samar (especiallyDrs Samuel Delfin Cynthia Genosolango Grace Trabadoand Marian Isiderio) Dr Nabila Zaka (UNICEF) and theInternational Medical Corps
References
[1] October 2015 httplibrarypcwgovphsitesdefaultfiles14011120SDR20Yolanda20Philippnes20finalpdf
[2] ldquoResponding toTyphoonHaiyanrdquoTheLancet vol 382 no 9907article 1769 2013
[3] R C Alfonso D S Capili K A Reyes F Tatad-To and M ASilvestre ldquoContributing to the Infant and Young Child Feedingin Emergencies (IYCF-E) response in the Philippines A local
NGOperspectiverdquo 2015 httpwwwennonlinenetfex50iycf-philippines
[4] WHO Philippines ldquoEssential Intrapartum and Newborn Care(EINC) Evidence-based Standard Practicesrdquo 2016 httpwwwwprowhointphilippinesareasmaternal child nutritionnew-born mother careeinc protocolsen
[5] WHO WPRO ldquoEarly Essential Newborn Care First EmbraceClinical Practice Pocket Guiderdquo 2014 httpiriswprowhointbitstreamhandle106651107989789290616856 engpdfjsessi-onid=B789B68B6D8BF8BB2C7F99F09E698AE1sequence=3
[6] H Obara and H Sobel ldquoQuality maternal and newborn care toensure a healthy start for every newborn in the World HealthOrganization Western Pacific Regionrdquo BJOG An InternationalJournal of Obstetrics andGynaecology vol 121 pp 154ndash159 2014
[7] H L Sobel M A A Silvestre J B V Mantaring III Y EOliveros and S Nyunt-U ldquoImmediate newborn care practicesdelay thermoregulation and breastfeeding initiationrdquo Acta Pae-diatrica International Journal of Paediatrics vol 100 no 8 pp1127ndash1133 2011
[8] Z A Bhutta J K Das R Bahl et al ldquoEvery newborn canavailable interventions end preventable deaths in mothersnewborn babies and stillbirths and at what costrdquo The Lancetvol 384 no 9940 pp 347ndash370 2014
[9] E Duysburgh B Kerstens M Diaz et al ldquoNewborn care inIndonesia Lao Peoplersquos Democratic Republic and the Philip-pines a comprehensive needs assessmentrdquo BMC Pediatrics vol14 no 1 article 46 2014
[10] Philippine Statistics Authority (PSA) and ICF InternationalPhilippines National Demographic and Health Survey 2013Philippine Statistics Authority (PSA) Manila Philippines ICFInternational Rockville Md USA 2014
[11] Philippine Public StormSignals 2015 httpdrrmregion4adostgovphknowledge-management-center7Philippine-public-storm-signalshtml
[12] Healthy Newborn Network (HNN) Inter-agency NewbornIndicators Technical Working Group 2012 Newborn ServicesRapid Health Facility Assessment tool 2016 httpwwwheal-thynewbornnetworkorgresourcenewborn-services-rapid-health-facility-assessment
[13] M E Kruk M Myers S T Varpilah and B T Dahn ldquoWhat isa resilient health system Lessons from Ebolardquo The Lancet vol385 no 9980 pp 1910ndash1912 2015
[14] C Enweronu-Laryea K E Dickson S G Moxon et al ldquoBasicnewborn care and neonatal resuscitation a multi-countryanalysis of health system bottlenecks and potential solutionsrdquoBMCPregnancy and Childbirth vol 15 supplement 2 article 542015
[15] United Nations Office for the Coordination of HumanitarianAffairs (UN-OCHA) ldquoTyphoon HaiyanmdashHumanitarian Snap-shotrdquo Philippines (as of Nov 12 2013) Data Sources DSWDDROMICReport Nov 12 2013 NDRRMC Situation Report 14OCHO Situation Report 5 and UNDAC Reports
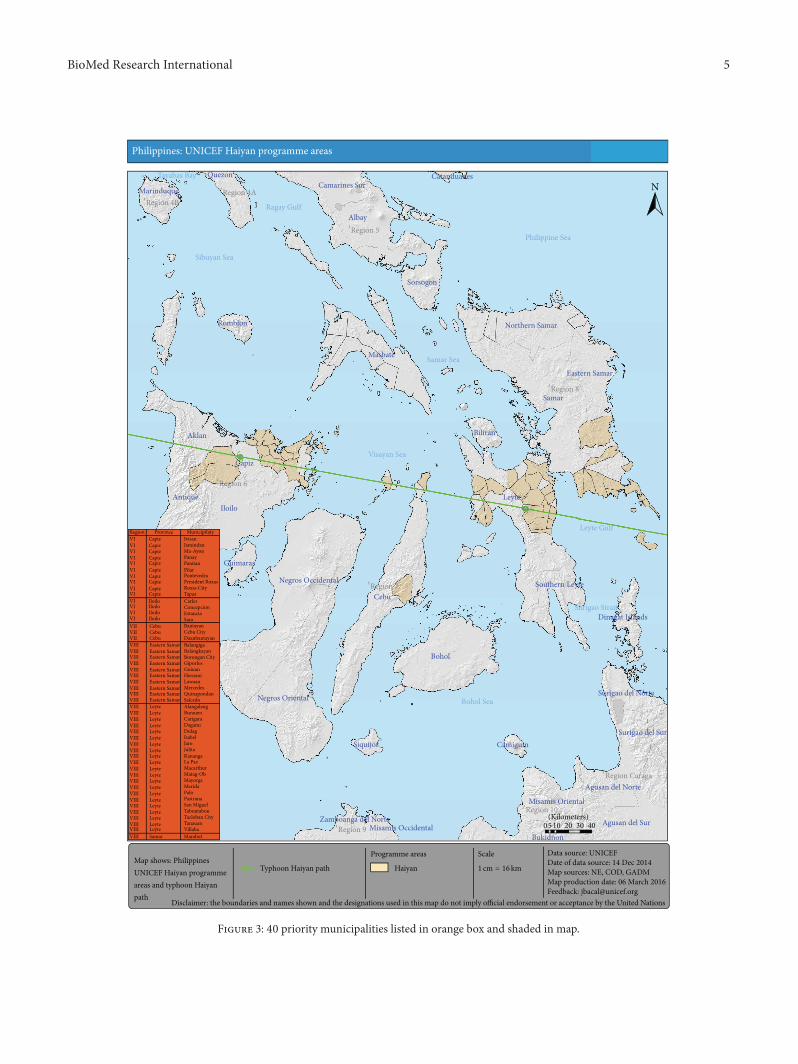
BioMed Research International 5
Bukidnon
Sulu Sea
LeyteIloilo
Cebu
Samar
Bohol
Capiz
Negros Occidental
Albay
Masbate
Antique
Negros Oriental
Aklan
Eastern Samar
Sorsogon
Northern Samar
Agusan del Sur
Agusan del Norte
Misamis Oriental
QuezonCamarines Sur
Marinduque
Biliran
Romblon
Southern Leyte
Surigao del Norte
Guimaras
Dinagat Islands
Zamboanga del Norte
SiquijorSurigao del Sur
Misamis Occidental
Camiguin
Catanduanes
Bohol Sea
Philippine Sea
Sibuyan Sea
Visayan Sea
Samar Sea
Leyte Gulf
Ragay Gulf
Surigao Strait
Tayabas Bay
Map shows PhilippinesUNICEF Haiyan programmeareas and typhoon Haiyanpath
Disclaimer the boundaries and names shown and the designations used in this map do not imply official endorsement or acceptance by the United Nations
0 10 20 30 405(Kilometers)
Data source UNICEFDate of data source 14 Dec 2014Map sources NE COD GADMMap production date 06 March 2016Feedback jbacaluniceforg
ScaleProgramme areas
HaiyanTyphoon Haiyan path
VIII
VIIVI
Capiz
IloiloVI IloiloVI IloiloVIVI
CapizVICapizVICapizVICapizVICapizVICapizVICapizVICapizVICapizVI
Iloilo
CebuVII CebuVII Cebu
Eastern SamarVIII Eastern SamarVIII Eastern SamarVIII Eastern SamarVIII Eastern SamarVIII Eastern SamarVIII Eastern SamarVIII Eastern SamarVIII Eastern SamarVIIIVIII
Eastern Samar
Samar
LeyteVIII LeyteVIII LeyteVIII LeyteVIII LeyteVIII LeyteVIII LeyteVIII LeyteVIII LeyteVIII LeyteVIII LeyteVIII LeyteVIII LeyteVIII LeyteVIII LeyteVIII LeyteVIII LeyteVIII LeyteVIII LeyteVIII LeyteVIII LeyteVIII
IvisanJamindanMa-AyonPanayPanitanPilarPontevedraPresident RoxasRoxas CityTapazCarlesConcepcionEstanciaSaraBantayanCebu CityDaanbantayanBalangigaBalangkayanBorongan CityGiporlosGuiuanHernaniLawaanMercedesQuinapondanSalcedoAlangalangBurauenCarigaraDagamiDulagIsabelJaroJulitaKanangaLa PazMacarthurMatag-ObMayorgaMeridaPaloPastranaSan MiguelTabontabonTacloban CityTanauanVillabaMarabut
998400Region 4B
998400Region 4A
998400Region 5
998400Region 8
998400Region 6
998400Region 7
998400Region 9
998400Region 10
998400Region Caraga
1 cm = 16km
Region Province Municipilaty
Philippines UNICEF Haiyan programme areas
N
Figure 3 40 priority municipalities listed in orange box and shaded in map
6 BioMed Research International
96 98 98 98
16 22
17 96 98
94
0 10()
20 30 40 50 60 70 80 90 100
Service availability indicators at baseline and at 1- and 3-month posttraining assessment in Eastern Western and
Central Visayas Philippines 2013
3-month PTA 1-month PTA Baseline
Kangaroo mother carelowastAntenatal steroidslowast
Neonatal resuscitationlowast
Manual removal of retained products after deliveryManual placental removal
Assisted vaginal deliveryParenteral magnesium sulfatelowast
Parenteral oxytocinlowast
Parenteral antibioticslowast247 skilled birth attendancelowast
lowastIndicates significant change from baseline to 3-month PTA p lt 005
Figure 4 Proportion of facilities assessed providing various services at pretraining (baseline) and at 1 and 3 months posttraining assessment(PTA) Eastern Western and Central Visayas post-Haiyan
34 Posttraining Assessments (Table 1) At 1 month and 3months after training field visits to 58 and 51 facilities respec-tively were carried out The facilities that completed the 3assessments were thirty-five (35) rural health units (RHUs)15 primary level hospitals (13 district 1 city and 1 communityhospitals) and one (1) provincial hospital These field visitsrevealed that uptake of EINC knowledge and skills was trans-lated to significant changes in daily practice Posttrainingassessment visits revealed good evidence of changes in thephysical environments in the labordelivery and postpartumareas and implementation of many of the EINC practices
However apart from the overall improvement someposttraining gaps were identified (1) not allowing a com-panion of choice (2) nonadministration of birth dosesof BCG vaccine (3) unavailability of nevirapine therapy(4) unavailability of protocols or guidelines for IntegratedManagement of Pregnancy and Childbirth (IMPAC) referralof sick newborns Comprehensive Emergency Obstetric andNewborn Care (CEmONC) and preterm labormanagement(5) absence of soap and hand disinfectants in postnatal areas
35 Service Availability (Figure 4) In Eastern Visayas theworst hit region baseline assessment revealed that 27 of 36facilities were providing birthing services At 1 month aftertraining 32 of 38 assessed birthing facilities were providinground-the-clockdaily (247) skilled birth attendance (SBA)At 3 months 30 of 31 birthing facilities were providing 247SBA InWesternVisayas 16 of 16 facilities were able to sustaindelivery services at baseline and 1 month assessments Onefacility suspended its delivery services to undergo renova-tions at the 3-month assessment All of the 15 other facilitieswere providing 247 SBA In Central Visayas all 4 facilitiesassessed were providing 247 SBA at baseline 1-monthand 3-month assessments Over the period from baselineassessment to 3 months after training there were significantimprovements in self-reported availability of services such as
neonatal resuscitation kangaroomother care administrationof parenteral oxytocin antibiotics antenatal steroids andmagnesium sulfate In contrast persistent gaps remainedfor assisted vaginal delivery manual placental removal andmanual removal of retained products after delivery In Figures4ndash6 the proportion of facilities () at end line (3months aftertraining) is labeled
36 Equipment and Supplies (Figure 5) Over the period frombaseline assessment to 3 months after training (20-week 19-week and 14-week periods for Eastern Western and Cen-tral Visayas resp) there were significant improvements inavailability of life-saving drugs (ie oxytocin) and equipment(ie for resuscitation) most notably for Eastern and CentralVisayas For Western Visayas some improvements were seenin the facilities but the limited availability of equipmentconstrained the appropriate delivery of services Not all life-saving drugs were available in all facilities especially antibi-otics and steroids
Though there was significant improvement persistentgaps remained for antenatal steroids injectable gentamicinand magnesium sulfate supplies Towels for drying werestill being provided by families instead of by facilitiesNevirapine for prevention of mother-to-child transmissionof HIV remained unavailable across all regions MultidoseBCG vaccines were available but considered ldquoinsufficientrdquo byhealth workers Many facilities had moved their weighingscales from their delivery areas to their maternity careareas for deferred weighing until after the first breastfeedas recommended in EINC protocols Protocols for IMPACsick newborn carereferral preterm labor management andCEmONCmanuals remain unavailable
37 Service Standards (Figure 6) In addition to parametersincluded in the Newborn Care Services Rapid AssessmentTool selected parameters relevant to the Philippines EINC
BioMed Research International 7
69 88
86 96
84 4
73 2
57 98
71
0 10 20 30 40 50()
60 70 80 90 100
Equipment and supplies availability at baseline and at 1- month and 3-month posttraining assessment in Eastern
Western and Central Visayas Philippines 2013
3-month PTA 1-month PTA Baseline
Magnesium sulfateInjectable uterotoniclowast
CorticosteroidsPMTCT drugslowast
Injectable gentamicinTowels for drying
Soap or hand disinfectantInfant scalelowast
lowastResuscitation tableNewborn bag and masklowast
Up-to-date delivery register
lowastIndicates significant change from baseline to 3-month PTA p lt 005
Figure 5 Proportion of facilities assessed to have various equipment and supplies at pretraining (baseline) and at 1 and 3months posttrainingassessment (PTA) Eastern Western and Central Visayas post-Haiyan
87 58
96 84
0 98 98
86 80
84 82
92 76
70 72
70
0 10 20 30 40 50()
60 70 80 90 100
Service standards indicators at baseline and at 1-month and 3-month posttrainingassessment in Eastern Western and Central Visayas Philippines 2013
Companion of choiceAllowed to eatdrink
Selective episiotomyperineal supportAMTSLlowast
Partograph filled out correctlylowast
Immediatethorough dryingSkin-to-skin contact
Properly timed cord clampingNonseparation and initiation of Breastfeeding
Eye carelowast
Vitamin Klowast
BCG birth doseHepatitis B birth dose
Wall clock in delivery arealowast
Room thermometer in delivery arealowast
Size 0 or preterm masklowast
3-month PTA 1-month PTA Baseline
lowastIndicates significant change from baseline to3-month PTA p lt 005
Figure 6 Proportion of facilities assessed to be implementing various service standards at pretraining (baseline) and at 1 and 3 monthsposttraining assessment (PTA) Eastern Western and Central Visayas post-Haiyan
8 BioMed Research International
Protocol and Basic Emergency Obstetric and Newborn Care(BEmONC) services standards were assessed through inter-views of health service providers
Significant improvements in service standards usingtracer indicators were noted across all regions over the periodfrom pretraining assessment to the 3 months posttrainingassessment Most notable were performance of the EINCldquocore stepsrdquo in immediate newborn care proper WHOpartograph use and availability of size 0 face masks forresuscitation of preterms which improved from 0 to 100at 3 months posttraining assessment
Quality labor and delivery for mothers (companion ofchoice allowing mothers to eatdrink semiupright deliverybed perineal support and restrictive episiotomy and activemanagement of the third stage of labor) and quality post-partum care (monitoring vital signs uterine massage andpostpartum visit within first week and then within fourthto sixth weeks after discharge) were carried out Facilitiesreported performance of the ldquocore stepsrdquo of immediatenewborn care (immediate and thorough drying skin-to-skincontact properly timed cord clamping and nonseparation ofnewborn from mother for early breastfeeding) and routinenewborn care (eye care physical examination and vitamin Kadministration) Postpartumwomen interviewed in the facil-ities verified the consistency of applying the EINC protocol
A persistent gap in EINC standard practice was the birthdose of BCG vaccine Ninety-six percent of facilities were notadministering this birth dose as recommended by nationalguidelines citing that using the available multidose vials foronly a few patients at each time constitutes ldquowastagerdquo Thisreflects the common practice of deferring the BCG vaccina-tion to the first-postnatal visit in the Philippines Number ofroom thermometers and wall clocks had increased in somefacilities
UnlikeWestern Visayas the 4 facilities in Central Visayashad newborn resuscitator bags and masks available priorto the EINC intervention With the intervention howeverhealth workers reported increased confidence in their newlyacquired resuscitation skills Wall clocks were present indelivery areas in all 4 facilities assessed from baseline to endline Room thermometers absent at baseline in all facilitieswere available in all 4 facilities and end line
Across the 3 regions significant improvements in servicestandards were documented In 2008 coverage of early skin-to-skin contact (SSC) was documented at 96 in deliveryassessments in 51 government hospitals [7] After governmentefforts at EINC scale-up SSC coverage was at 64 bymaternal report in 2013 [10] In this study SSC was at84 in primary level facilities postdisaster by health workerreport Before Haiyan barriers to EINC implementation thatis absence of enabling physical and policy environmentsnoncompliance by specialists and other ldquoexpertsrdquo unfamiliarwith the updated EINC practices had been diminished butnot eliminated The devastation brought by Haiyan disman-tled the systems that enabled EINC practice Neverthelessover a 3-month period an intervention of training andposttraining assessments was able to restore and for someEINC practices even exceed pre-Haiyan coverage rates
The high coverage rates for EINC indicators at baselinesuggests that previous scale-up efforts in EINC and othercross-cutting areas increased the potential for resilienceThis complemented assistance offered by other humanitarianactors (eg infrastructure rehabilitation and provision ofsupplies and equipment) turning this into an opportunity toldquobuild back betterrdquo However the contribution of pre-Haiyancapacity building efforts to this rapid restoration and furtherimprovement of EINC services requires further evaluationWe postulate that if capacity building efforts have establishedenabling environments under normal circumstances rehabil-itation could be achieved in similarly brief time periodsThuscapacity building for EINC may potentially be considered asan important disaster preparedness measure
Aiming to improve the sustainability of this interventionthe external experts provided close supportive supervisionduring the cascade training sessions and the two posttrainingassessments Our experience reveals that both performanceand environments have improved creating an enabling envi-ronment for EINC practices There were still aspects thatrequired improvement that could be reinforced by the localhealth officials during supervisory visits However this can bea challenge in areas where regular supervision visits are raredue to difficulties in geographic access or security constraints
Government support was provided through so-calledInterlocal Health Zones (ILHZs) utilizing existing referralnetworks often with rural health units (RHUs) and districthospitals as the focal point Trainers were capacitated asILHZ groups for subsequent roll-out through a skills transfermethodology This approach had its limitation though astrained health care providers from one ILHZ in generalcould not be tapped to train health care workers of anotherILHZ
In the aftermath of the disaster several developmentand recovery activities resulted in competing schedules(eg water sanitation and hygiene (WASH) vaccine coldchain implementation etc) making it difficult to scheduletraining dates Often competing capacity building activitiesand the local rehabilitation efforts involved the same setof (limited) local manpower Consequently mobilizing localstaffs to implement their trainersrsquo knowledge in cascade QAworkshops proved difficult Another constraint posed thehealth human resource availability after the disaster sincemany health care workers were victims themselves
The postdisaster setting likewise presented more chal-lenges in conducting capacity building interventions In somegeographic areas communication and road infrastructurecontinued to be unusable making it difficult for healthworkers to attend trainings or gather local data This post-disaster scenario constrained us to ldquopre- to postinterventionassessmentrdquo and its inherent methodologic limitations
This study was also limited by the fact that not all facilitieswho participated in baseline assessment were included inthe posttraining assessment Thus this study could benefitfrom another evaluation after a longer interval posttrain-ing to assess newborn outcome indicators sustainability ofimprovements and further analysis on possible contributoryeffects of other sectoral interventions (eg WASH) and
BioMed Research International 9
partner efforts in the areas The contribution of predisastercapacity building to the results could not be studied
4 Conclusions
This intervention filled the service gaps identified immedi-ately after a large scale natural disaster and helped to reestab-lish and improve the delivery of health services in affectedareas Where baseline indices were worse because of theimmediate effects of the typhoon (ie Eastern Visayas) themagnitude of improvement across most assessed parameterswas more significant However there were other parameterswhere gaps persist despite intensive efforts and othermethodsand systemic interventions need to be explored address thesedeficiencies
Our study demonstrates that quick important qualityimprovements can bemade in a timelymanner across a rangeof health facilities andwith differing cadres of health workerseven in immediate postdisaster settings Capacity building ofhealth workers and strengthening of the local health systemto deliver quality care before during and in the aftermath ofa major disaster are among the preconditions for a resilienthealth system [13] Building the evidence base linking thesequality improvement efforts in EINC and basic newbornresuscitation with impact on newborn and maternal healthoutcomes postdisaster is imperative [14]
Disclosure
Any opinions stated by UNICEF affiliates are those of theauthors and not of UNICEF
Competing Interests
The authors declare no competing interests regarding thepublication of this paper
Acknowledgments
Funding support was provided by UNICEF The authorswould like to thank our colleagues in the Department ofHealth Regional Health Offices of Eastern Central andWestern Visayas (especially Drs Corazon Sabulao and AlmaBernardo) the Provincial Health Offices of Capiz CebuIloilo Leyte and Eastern and Western Samar (especiallyDrs Samuel Delfin Cynthia Genosolango Grace Trabadoand Marian Isiderio) Dr Nabila Zaka (UNICEF) and theInternational Medical Corps
References
[1] October 2015 httplibrarypcwgovphsitesdefaultfiles14011120SDR20Yolanda20Philippnes20finalpdf
[2] ldquoResponding toTyphoonHaiyanrdquoTheLancet vol 382 no 9907article 1769 2013
[3] R C Alfonso D S Capili K A Reyes F Tatad-To and M ASilvestre ldquoContributing to the Infant and Young Child Feedingin Emergencies (IYCF-E) response in the Philippines A local
NGOperspectiverdquo 2015 httpwwwennonlinenetfex50iycf-philippines
[4] WHO Philippines ldquoEssential Intrapartum and Newborn Care(EINC) Evidence-based Standard Practicesrdquo 2016 httpwwwwprowhointphilippinesareasmaternal child nutritionnew-born mother careeinc protocolsen
[5] WHO WPRO ldquoEarly Essential Newborn Care First EmbraceClinical Practice Pocket Guiderdquo 2014 httpiriswprowhointbitstreamhandle106651107989789290616856 engpdfjsessi-onid=B789B68B6D8BF8BB2C7F99F09E698AE1sequence=3
[6] H Obara and H Sobel ldquoQuality maternal and newborn care toensure a healthy start for every newborn in the World HealthOrganization Western Pacific Regionrdquo BJOG An InternationalJournal of Obstetrics andGynaecology vol 121 pp 154ndash159 2014
[7] H L Sobel M A A Silvestre J B V Mantaring III Y EOliveros and S Nyunt-U ldquoImmediate newborn care practicesdelay thermoregulation and breastfeeding initiationrdquo Acta Pae-diatrica International Journal of Paediatrics vol 100 no 8 pp1127ndash1133 2011
[8] Z A Bhutta J K Das R Bahl et al ldquoEvery newborn canavailable interventions end preventable deaths in mothersnewborn babies and stillbirths and at what costrdquo The Lancetvol 384 no 9940 pp 347ndash370 2014
[9] E Duysburgh B Kerstens M Diaz et al ldquoNewborn care inIndonesia Lao Peoplersquos Democratic Republic and the Philip-pines a comprehensive needs assessmentrdquo BMC Pediatrics vol14 no 1 article 46 2014
[10] Philippine Statistics Authority (PSA) and ICF InternationalPhilippines National Demographic and Health Survey 2013Philippine Statistics Authority (PSA) Manila Philippines ICFInternational Rockville Md USA 2014
[11] Philippine Public StormSignals 2015 httpdrrmregion4adostgovphknowledge-management-center7Philippine-public-storm-signalshtml
[12] Healthy Newborn Network (HNN) Inter-agency NewbornIndicators Technical Working Group 2012 Newborn ServicesRapid Health Facility Assessment tool 2016 httpwwwheal-thynewbornnetworkorgresourcenewborn-services-rapid-health-facility-assessment
[13] M E Kruk M Myers S T Varpilah and B T Dahn ldquoWhat isa resilient health system Lessons from Ebolardquo The Lancet vol385 no 9980 pp 1910ndash1912 2015
[14] C Enweronu-Laryea K E Dickson S G Moxon et al ldquoBasicnewborn care and neonatal resuscitation a multi-countryanalysis of health system bottlenecks and potential solutionsrdquoBMCPregnancy and Childbirth vol 15 supplement 2 article 542015
[15] United Nations Office for the Coordination of HumanitarianAffairs (UN-OCHA) ldquoTyphoon HaiyanmdashHumanitarian Snap-shotrdquo Philippines (as of Nov 12 2013) Data Sources DSWDDROMICReport Nov 12 2013 NDRRMC Situation Report 14OCHO Situation Report 5 and UNDAC Reports

6 BioMed Research International
96 98 98 98
16 22
17 96 98
94
0 10()
20 30 40 50 60 70 80 90 100
Service availability indicators at baseline and at 1- and 3-month posttraining assessment in Eastern Western and
Central Visayas Philippines 2013
3-month PTA 1-month PTA Baseline
Kangaroo mother carelowastAntenatal steroidslowast
Neonatal resuscitationlowast
Manual removal of retained products after deliveryManual placental removal
Assisted vaginal deliveryParenteral magnesium sulfatelowast
Parenteral oxytocinlowast
Parenteral antibioticslowast247 skilled birth attendancelowast
lowastIndicates significant change from baseline to 3-month PTA p lt 005
Figure 4 Proportion of facilities assessed providing various services at pretraining (baseline) and at 1 and 3 months posttraining assessment(PTA) Eastern Western and Central Visayas post-Haiyan
34 Posttraining Assessments (Table 1) At 1 month and 3months after training field visits to 58 and 51 facilities respec-tively were carried out The facilities that completed the 3assessments were thirty-five (35) rural health units (RHUs)15 primary level hospitals (13 district 1 city and 1 communityhospitals) and one (1) provincial hospital These field visitsrevealed that uptake of EINC knowledge and skills was trans-lated to significant changes in daily practice Posttrainingassessment visits revealed good evidence of changes in thephysical environments in the labordelivery and postpartumareas and implementation of many of the EINC practices
However apart from the overall improvement someposttraining gaps were identified (1) not allowing a com-panion of choice (2) nonadministration of birth dosesof BCG vaccine (3) unavailability of nevirapine therapy(4) unavailability of protocols or guidelines for IntegratedManagement of Pregnancy and Childbirth (IMPAC) referralof sick newborns Comprehensive Emergency Obstetric andNewborn Care (CEmONC) and preterm labormanagement(5) absence of soap and hand disinfectants in postnatal areas
35 Service Availability (Figure 4) In Eastern Visayas theworst hit region baseline assessment revealed that 27 of 36facilities were providing birthing services At 1 month aftertraining 32 of 38 assessed birthing facilities were providinground-the-clockdaily (247) skilled birth attendance (SBA)At 3 months 30 of 31 birthing facilities were providing 247SBA InWesternVisayas 16 of 16 facilities were able to sustaindelivery services at baseline and 1 month assessments Onefacility suspended its delivery services to undergo renova-tions at the 3-month assessment All of the 15 other facilitieswere providing 247 SBA In Central Visayas all 4 facilitiesassessed were providing 247 SBA at baseline 1-monthand 3-month assessments Over the period from baselineassessment to 3 months after training there were significantimprovements in self-reported availability of services such as
neonatal resuscitation kangaroomother care administrationof parenteral oxytocin antibiotics antenatal steroids andmagnesium sulfate In contrast persistent gaps remainedfor assisted vaginal delivery manual placental removal andmanual removal of retained products after delivery In Figures4ndash6 the proportion of facilities () at end line (3months aftertraining) is labeled
36 Equipment and Supplies (Figure 5) Over the period frombaseline assessment to 3 months after training (20-week 19-week and 14-week periods for Eastern Western and Cen-tral Visayas resp) there were significant improvements inavailability of life-saving drugs (ie oxytocin) and equipment(ie for resuscitation) most notably for Eastern and CentralVisayas For Western Visayas some improvements were seenin the facilities but the limited availability of equipmentconstrained the appropriate delivery of services Not all life-saving drugs were available in all facilities especially antibi-otics and steroids
Though there was significant improvement persistentgaps remained for antenatal steroids injectable gentamicinand magnesium sulfate supplies Towels for drying werestill being provided by families instead of by facilitiesNevirapine for prevention of mother-to-child transmissionof HIV remained unavailable across all regions MultidoseBCG vaccines were available but considered ldquoinsufficientrdquo byhealth workers Many facilities had moved their weighingscales from their delivery areas to their maternity careareas for deferred weighing until after the first breastfeedas recommended in EINC protocols Protocols for IMPACsick newborn carereferral preterm labor management andCEmONCmanuals remain unavailable
37 Service Standards (Figure 6) In addition to parametersincluded in the Newborn Care Services Rapid AssessmentTool selected parameters relevant to the Philippines EINC
BioMed Research International 7
69 88
86 96
84 4
73 2
57 98
71
0 10 20 30 40 50()
60 70 80 90 100
Equipment and supplies availability at baseline and at 1- month and 3-month posttraining assessment in Eastern
Western and Central Visayas Philippines 2013
3-month PTA 1-month PTA Baseline
Magnesium sulfateInjectable uterotoniclowast
CorticosteroidsPMTCT drugslowast
Injectable gentamicinTowels for drying
Soap or hand disinfectantInfant scalelowast
lowastResuscitation tableNewborn bag and masklowast
Up-to-date delivery register
lowastIndicates significant change from baseline to 3-month PTA p lt 005
Figure 5 Proportion of facilities assessed to have various equipment and supplies at pretraining (baseline) and at 1 and 3months posttrainingassessment (PTA) Eastern Western and Central Visayas post-Haiyan
87 58
96 84
0 98 98
86 80
84 82
92 76
70 72
70
0 10 20 30 40 50()
60 70 80 90 100
Service standards indicators at baseline and at 1-month and 3-month posttrainingassessment in Eastern Western and Central Visayas Philippines 2013
Companion of choiceAllowed to eatdrink
Selective episiotomyperineal supportAMTSLlowast
Partograph filled out correctlylowast
Immediatethorough dryingSkin-to-skin contact
Properly timed cord clampingNonseparation and initiation of Breastfeeding
Eye carelowast
Vitamin Klowast
BCG birth doseHepatitis B birth dose
Wall clock in delivery arealowast
Room thermometer in delivery arealowast
Size 0 or preterm masklowast
3-month PTA 1-month PTA Baseline
lowastIndicates significant change from baseline to3-month PTA p lt 005
Figure 6 Proportion of facilities assessed to be implementing various service standards at pretraining (baseline) and at 1 and 3 monthsposttraining assessment (PTA) Eastern Western and Central Visayas post-Haiyan
8 BioMed Research International
Protocol and Basic Emergency Obstetric and Newborn Care(BEmONC) services standards were assessed through inter-views of health service providers
Significant improvements in service standards usingtracer indicators were noted across all regions over the periodfrom pretraining assessment to the 3 months posttrainingassessment Most notable were performance of the EINCldquocore stepsrdquo in immediate newborn care proper WHOpartograph use and availability of size 0 face masks forresuscitation of preterms which improved from 0 to 100at 3 months posttraining assessment
Quality labor and delivery for mothers (companion ofchoice allowing mothers to eatdrink semiupright deliverybed perineal support and restrictive episiotomy and activemanagement of the third stage of labor) and quality post-partum care (monitoring vital signs uterine massage andpostpartum visit within first week and then within fourthto sixth weeks after discharge) were carried out Facilitiesreported performance of the ldquocore stepsrdquo of immediatenewborn care (immediate and thorough drying skin-to-skincontact properly timed cord clamping and nonseparation ofnewborn from mother for early breastfeeding) and routinenewborn care (eye care physical examination and vitamin Kadministration) Postpartumwomen interviewed in the facil-ities verified the consistency of applying the EINC protocol
A persistent gap in EINC standard practice was the birthdose of BCG vaccine Ninety-six percent of facilities were notadministering this birth dose as recommended by nationalguidelines citing that using the available multidose vials foronly a few patients at each time constitutes ldquowastagerdquo Thisreflects the common practice of deferring the BCG vaccina-tion to the first-postnatal visit in the Philippines Number ofroom thermometers and wall clocks had increased in somefacilities
UnlikeWestern Visayas the 4 facilities in Central Visayashad newborn resuscitator bags and masks available priorto the EINC intervention With the intervention howeverhealth workers reported increased confidence in their newlyacquired resuscitation skills Wall clocks were present indelivery areas in all 4 facilities assessed from baseline to endline Room thermometers absent at baseline in all facilitieswere available in all 4 facilities and end line
Across the 3 regions significant improvements in servicestandards were documented In 2008 coverage of early skin-to-skin contact (SSC) was documented at 96 in deliveryassessments in 51 government hospitals [7] After governmentefforts at EINC scale-up SSC coverage was at 64 bymaternal report in 2013 [10] In this study SSC was at84 in primary level facilities postdisaster by health workerreport Before Haiyan barriers to EINC implementation thatis absence of enabling physical and policy environmentsnoncompliance by specialists and other ldquoexpertsrdquo unfamiliarwith the updated EINC practices had been diminished butnot eliminated The devastation brought by Haiyan disman-tled the systems that enabled EINC practice Neverthelessover a 3-month period an intervention of training andposttraining assessments was able to restore and for someEINC practices even exceed pre-Haiyan coverage rates
The high coverage rates for EINC indicators at baselinesuggests that previous scale-up efforts in EINC and othercross-cutting areas increased the potential for resilienceThis complemented assistance offered by other humanitarianactors (eg infrastructure rehabilitation and provision ofsupplies and equipment) turning this into an opportunity toldquobuild back betterrdquo However the contribution of pre-Haiyancapacity building efforts to this rapid restoration and furtherimprovement of EINC services requires further evaluationWe postulate that if capacity building efforts have establishedenabling environments under normal circumstances rehabil-itation could be achieved in similarly brief time periodsThuscapacity building for EINC may potentially be considered asan important disaster preparedness measure
Aiming to improve the sustainability of this interventionthe external experts provided close supportive supervisionduring the cascade training sessions and the two posttrainingassessments Our experience reveals that both performanceand environments have improved creating an enabling envi-ronment for EINC practices There were still aspects thatrequired improvement that could be reinforced by the localhealth officials during supervisory visits However this can bea challenge in areas where regular supervision visits are raredue to difficulties in geographic access or security constraints
Government support was provided through so-calledInterlocal Health Zones (ILHZs) utilizing existing referralnetworks often with rural health units (RHUs) and districthospitals as the focal point Trainers were capacitated asILHZ groups for subsequent roll-out through a skills transfermethodology This approach had its limitation though astrained health care providers from one ILHZ in generalcould not be tapped to train health care workers of anotherILHZ
In the aftermath of the disaster several developmentand recovery activities resulted in competing schedules(eg water sanitation and hygiene (WASH) vaccine coldchain implementation etc) making it difficult to scheduletraining dates Often competing capacity building activitiesand the local rehabilitation efforts involved the same setof (limited) local manpower Consequently mobilizing localstaffs to implement their trainersrsquo knowledge in cascade QAworkshops proved difficult Another constraint posed thehealth human resource availability after the disaster sincemany health care workers were victims themselves
The postdisaster setting likewise presented more chal-lenges in conducting capacity building interventions In somegeographic areas communication and road infrastructurecontinued to be unusable making it difficult for healthworkers to attend trainings or gather local data This post-disaster scenario constrained us to ldquopre- to postinterventionassessmentrdquo and its inherent methodologic limitations
This study was also limited by the fact that not all facilitieswho participated in baseline assessment were included inthe posttraining assessment Thus this study could benefitfrom another evaluation after a longer interval posttrain-ing to assess newborn outcome indicators sustainability ofimprovements and further analysis on possible contributoryeffects of other sectoral interventions (eg WASH) and
BioMed Research International 9
partner efforts in the areas The contribution of predisastercapacity building to the results could not be studied
4 Conclusions
This intervention filled the service gaps identified immedi-ately after a large scale natural disaster and helped to reestab-lish and improve the delivery of health services in affectedareas Where baseline indices were worse because of theimmediate effects of the typhoon (ie Eastern Visayas) themagnitude of improvement across most assessed parameterswas more significant However there were other parameterswhere gaps persist despite intensive efforts and othermethodsand systemic interventions need to be explored address thesedeficiencies
Our study demonstrates that quick important qualityimprovements can bemade in a timelymanner across a rangeof health facilities andwith differing cadres of health workerseven in immediate postdisaster settings Capacity building ofhealth workers and strengthening of the local health systemto deliver quality care before during and in the aftermath ofa major disaster are among the preconditions for a resilienthealth system [13] Building the evidence base linking thesequality improvement efforts in EINC and basic newbornresuscitation with impact on newborn and maternal healthoutcomes postdisaster is imperative [14]
Disclosure
Any opinions stated by UNICEF affiliates are those of theauthors and not of UNICEF
Competing Interests
The authors declare no competing interests regarding thepublication of this paper
Acknowledgments
Funding support was provided by UNICEF The authorswould like to thank our colleagues in the Department ofHealth Regional Health Offices of Eastern Central andWestern Visayas (especially Drs Corazon Sabulao and AlmaBernardo) the Provincial Health Offices of Capiz CebuIloilo Leyte and Eastern and Western Samar (especiallyDrs Samuel Delfin Cynthia Genosolango Grace Trabadoand Marian Isiderio) Dr Nabila Zaka (UNICEF) and theInternational Medical Corps
References
[1] October 2015 httplibrarypcwgovphsitesdefaultfiles14011120SDR20Yolanda20Philippnes20finalpdf
[2] ldquoResponding toTyphoonHaiyanrdquoTheLancet vol 382 no 9907article 1769 2013
[3] R C Alfonso D S Capili K A Reyes F Tatad-To and M ASilvestre ldquoContributing to the Infant and Young Child Feedingin Emergencies (IYCF-E) response in the Philippines A local
NGOperspectiverdquo 2015 httpwwwennonlinenetfex50iycf-philippines
[4] WHO Philippines ldquoEssential Intrapartum and Newborn Care(EINC) Evidence-based Standard Practicesrdquo 2016 httpwwwwprowhointphilippinesareasmaternal child nutritionnew-born mother careeinc protocolsen
[5] WHO WPRO ldquoEarly Essential Newborn Care First EmbraceClinical Practice Pocket Guiderdquo 2014 httpiriswprowhointbitstreamhandle106651107989789290616856 engpdfjsessi-onid=B789B68B6D8BF8BB2C7F99F09E698AE1sequence=3
[6] H Obara and H Sobel ldquoQuality maternal and newborn care toensure a healthy start for every newborn in the World HealthOrganization Western Pacific Regionrdquo BJOG An InternationalJournal of Obstetrics andGynaecology vol 121 pp 154ndash159 2014
[7] H L Sobel M A A Silvestre J B V Mantaring III Y EOliveros and S Nyunt-U ldquoImmediate newborn care practicesdelay thermoregulation and breastfeeding initiationrdquo Acta Pae-diatrica International Journal of Paediatrics vol 100 no 8 pp1127ndash1133 2011
[8] Z A Bhutta J K Das R Bahl et al ldquoEvery newborn canavailable interventions end preventable deaths in mothersnewborn babies and stillbirths and at what costrdquo The Lancetvol 384 no 9940 pp 347ndash370 2014
[9] E Duysburgh B Kerstens M Diaz et al ldquoNewborn care inIndonesia Lao Peoplersquos Democratic Republic and the Philip-pines a comprehensive needs assessmentrdquo BMC Pediatrics vol14 no 1 article 46 2014
[10] Philippine Statistics Authority (PSA) and ICF InternationalPhilippines National Demographic and Health Survey 2013Philippine Statistics Authority (PSA) Manila Philippines ICFInternational Rockville Md USA 2014
[11] Philippine Public StormSignals 2015 httpdrrmregion4adostgovphknowledge-management-center7Philippine-public-storm-signalshtml
[12] Healthy Newborn Network (HNN) Inter-agency NewbornIndicators Technical Working Group 2012 Newborn ServicesRapid Health Facility Assessment tool 2016 httpwwwheal-thynewbornnetworkorgresourcenewborn-services-rapid-health-facility-assessment
[13] M E Kruk M Myers S T Varpilah and B T Dahn ldquoWhat isa resilient health system Lessons from Ebolardquo The Lancet vol385 no 9980 pp 1910ndash1912 2015
[14] C Enweronu-Laryea K E Dickson S G Moxon et al ldquoBasicnewborn care and neonatal resuscitation a multi-countryanalysis of health system bottlenecks and potential solutionsrdquoBMCPregnancy and Childbirth vol 15 supplement 2 article 542015
[15] United Nations Office for the Coordination of HumanitarianAffairs (UN-OCHA) ldquoTyphoon HaiyanmdashHumanitarian Snap-shotrdquo Philippines (as of Nov 12 2013) Data Sources DSWDDROMICReport Nov 12 2013 NDRRMC Situation Report 14OCHO Situation Report 5 and UNDAC Reports

BioMed Research International 7
69 88
86 96
84 4
73 2
57 98
71
0 10 20 30 40 50()
60 70 80 90 100
Equipment and supplies availability at baseline and at 1- month and 3-month posttraining assessment in Eastern
Western and Central Visayas Philippines 2013
3-month PTA 1-month PTA Baseline
Magnesium sulfateInjectable uterotoniclowast
CorticosteroidsPMTCT drugslowast
Injectable gentamicinTowels for drying
Soap or hand disinfectantInfant scalelowast
lowastResuscitation tableNewborn bag and masklowast
Up-to-date delivery register
lowastIndicates significant change from baseline to 3-month PTA p lt 005
Figure 5 Proportion of facilities assessed to have various equipment and supplies at pretraining (baseline) and at 1 and 3months posttrainingassessment (PTA) Eastern Western and Central Visayas post-Haiyan
87 58
96 84
0 98 98
86 80
84 82
92 76
70 72
70
0 10 20 30 40 50()
60 70 80 90 100
Service standards indicators at baseline and at 1-month and 3-month posttrainingassessment in Eastern Western and Central Visayas Philippines 2013
Companion of choiceAllowed to eatdrink
Selective episiotomyperineal supportAMTSLlowast
Partograph filled out correctlylowast
Immediatethorough dryingSkin-to-skin contact
Properly timed cord clampingNonseparation and initiation of Breastfeeding
Eye carelowast
Vitamin Klowast
BCG birth doseHepatitis B birth dose
Wall clock in delivery arealowast
Room thermometer in delivery arealowast
Size 0 or preterm masklowast
3-month PTA 1-month PTA Baseline
lowastIndicates significant change from baseline to3-month PTA p lt 005
Figure 6 Proportion of facilities assessed to be implementing various service standards at pretraining (baseline) and at 1 and 3 monthsposttraining assessment (PTA) Eastern Western and Central Visayas post-Haiyan
8 BioMed Research International
Protocol and Basic Emergency Obstetric and Newborn Care(BEmONC) services standards were assessed through inter-views of health service providers
Significant improvements in service standards usingtracer indicators were noted across all regions over the periodfrom pretraining assessment to the 3 months posttrainingassessment Most notable were performance of the EINCldquocore stepsrdquo in immediate newborn care proper WHOpartograph use and availability of size 0 face masks forresuscitation of preterms which improved from 0 to 100at 3 months posttraining assessment
Quality labor and delivery for mothers (companion ofchoice allowing mothers to eatdrink semiupright deliverybed perineal support and restrictive episiotomy and activemanagement of the third stage of labor) and quality post-partum care (monitoring vital signs uterine massage andpostpartum visit within first week and then within fourthto sixth weeks after discharge) were carried out Facilitiesreported performance of the ldquocore stepsrdquo of immediatenewborn care (immediate and thorough drying skin-to-skincontact properly timed cord clamping and nonseparation ofnewborn from mother for early breastfeeding) and routinenewborn care (eye care physical examination and vitamin Kadministration) Postpartumwomen interviewed in the facil-ities verified the consistency of applying the EINC protocol
A persistent gap in EINC standard practice was the birthdose of BCG vaccine Ninety-six percent of facilities were notadministering this birth dose as recommended by nationalguidelines citing that using the available multidose vials foronly a few patients at each time constitutes ldquowastagerdquo Thisreflects the common practice of deferring the BCG vaccina-tion to the first-postnatal visit in the Philippines Number ofroom thermometers and wall clocks had increased in somefacilities
UnlikeWestern Visayas the 4 facilities in Central Visayashad newborn resuscitator bags and masks available priorto the EINC intervention With the intervention howeverhealth workers reported increased confidence in their newlyacquired resuscitation skills Wall clocks were present indelivery areas in all 4 facilities assessed from baseline to endline Room thermometers absent at baseline in all facilitieswere available in all 4 facilities and end line
Across the 3 regions significant improvements in servicestandards were documented In 2008 coverage of early skin-to-skin contact (SSC) was documented at 96 in deliveryassessments in 51 government hospitals [7] After governmentefforts at EINC scale-up SSC coverage was at 64 bymaternal report in 2013 [10] In this study SSC was at84 in primary level facilities postdisaster by health workerreport Before Haiyan barriers to EINC implementation thatis absence of enabling physical and policy environmentsnoncompliance by specialists and other ldquoexpertsrdquo unfamiliarwith the updated EINC practices had been diminished butnot eliminated The devastation brought by Haiyan disman-tled the systems that enabled EINC practice Neverthelessover a 3-month period an intervention of training andposttraining assessments was able to restore and for someEINC practices even exceed pre-Haiyan coverage rates
The high coverage rates for EINC indicators at baselinesuggests that previous scale-up efforts in EINC and othercross-cutting areas increased the potential for resilienceThis complemented assistance offered by other humanitarianactors (eg infrastructure rehabilitation and provision ofsupplies and equipment) turning this into an opportunity toldquobuild back betterrdquo However the contribution of pre-Haiyancapacity building efforts to this rapid restoration and furtherimprovement of EINC services requires further evaluationWe postulate that if capacity building efforts have establishedenabling environments under normal circumstances rehabil-itation could be achieved in similarly brief time periodsThuscapacity building for EINC may potentially be considered asan important disaster preparedness measure
Aiming to improve the sustainability of this interventionthe external experts provided close supportive supervisionduring the cascade training sessions and the two posttrainingassessments Our experience reveals that both performanceand environments have improved creating an enabling envi-ronment for EINC practices There were still aspects thatrequired improvement that could be reinforced by the localhealth officials during supervisory visits However this can bea challenge in areas where regular supervision visits are raredue to difficulties in geographic access or security constraints
Government support was provided through so-calledInterlocal Health Zones (ILHZs) utilizing existing referralnetworks often with rural health units (RHUs) and districthospitals as the focal point Trainers were capacitated asILHZ groups for subsequent roll-out through a skills transfermethodology This approach had its limitation though astrained health care providers from one ILHZ in generalcould not be tapped to train health care workers of anotherILHZ
In the aftermath of the disaster several developmentand recovery activities resulted in competing schedules(eg water sanitation and hygiene (WASH) vaccine coldchain implementation etc) making it difficult to scheduletraining dates Often competing capacity building activitiesand the local rehabilitation efforts involved the same setof (limited) local manpower Consequently mobilizing localstaffs to implement their trainersrsquo knowledge in cascade QAworkshops proved difficult Another constraint posed thehealth human resource availability after the disaster sincemany health care workers were victims themselves
The postdisaster setting likewise presented more chal-lenges in conducting capacity building interventions In somegeographic areas communication and road infrastructurecontinued to be unusable making it difficult for healthworkers to attend trainings or gather local data This post-disaster scenario constrained us to ldquopre- to postinterventionassessmentrdquo and its inherent methodologic limitations
This study was also limited by the fact that not all facilitieswho participated in baseline assessment were included inthe posttraining assessment Thus this study could benefitfrom another evaluation after a longer interval posttrain-ing to assess newborn outcome indicators sustainability ofimprovements and further analysis on possible contributoryeffects of other sectoral interventions (eg WASH) and
BioMed Research International 9
partner efforts in the areas The contribution of predisastercapacity building to the results could not be studied
4 Conclusions
This intervention filled the service gaps identified immedi-ately after a large scale natural disaster and helped to reestab-lish and improve the delivery of health services in affectedareas Where baseline indices were worse because of theimmediate effects of the typhoon (ie Eastern Visayas) themagnitude of improvement across most assessed parameterswas more significant However there were other parameterswhere gaps persist despite intensive efforts and othermethodsand systemic interventions need to be explored address thesedeficiencies
Our study demonstrates that quick important qualityimprovements can bemade in a timelymanner across a rangeof health facilities andwith differing cadres of health workerseven in immediate postdisaster settings Capacity building ofhealth workers and strengthening of the local health systemto deliver quality care before during and in the aftermath ofa major disaster are among the preconditions for a resilienthealth system [13] Building the evidence base linking thesequality improvement efforts in EINC and basic newbornresuscitation with impact on newborn and maternal healthoutcomes postdisaster is imperative [14]
Disclosure
Any opinions stated by UNICEF affiliates are those of theauthors and not of UNICEF
Competing Interests
The authors declare no competing interests regarding thepublication of this paper
Acknowledgments
Funding support was provided by UNICEF The authorswould like to thank our colleagues in the Department ofHealth Regional Health Offices of Eastern Central andWestern Visayas (especially Drs Corazon Sabulao and AlmaBernardo) the Provincial Health Offices of Capiz CebuIloilo Leyte and Eastern and Western Samar (especiallyDrs Samuel Delfin Cynthia Genosolango Grace Trabadoand Marian Isiderio) Dr Nabila Zaka (UNICEF) and theInternational Medical Corps
References
[1] October 2015 httplibrarypcwgovphsitesdefaultfiles14011120SDR20Yolanda20Philippnes20finalpdf
[2] ldquoResponding toTyphoonHaiyanrdquoTheLancet vol 382 no 9907article 1769 2013
[3] R C Alfonso D S Capili K A Reyes F Tatad-To and M ASilvestre ldquoContributing to the Infant and Young Child Feedingin Emergencies (IYCF-E) response in the Philippines A local
NGOperspectiverdquo 2015 httpwwwennonlinenetfex50iycf-philippines
[4] WHO Philippines ldquoEssential Intrapartum and Newborn Care(EINC) Evidence-based Standard Practicesrdquo 2016 httpwwwwprowhointphilippinesareasmaternal child nutritionnew-born mother careeinc protocolsen
[5] WHO WPRO ldquoEarly Essential Newborn Care First EmbraceClinical Practice Pocket Guiderdquo 2014 httpiriswprowhointbitstreamhandle106651107989789290616856 engpdfjsessi-onid=B789B68B6D8BF8BB2C7F99F09E698AE1sequence=3
[6] H Obara and H Sobel ldquoQuality maternal and newborn care toensure a healthy start for every newborn in the World HealthOrganization Western Pacific Regionrdquo BJOG An InternationalJournal of Obstetrics andGynaecology vol 121 pp 154ndash159 2014
[7] H L Sobel M A A Silvestre J B V Mantaring III Y EOliveros and S Nyunt-U ldquoImmediate newborn care practicesdelay thermoregulation and breastfeeding initiationrdquo Acta Pae-diatrica International Journal of Paediatrics vol 100 no 8 pp1127ndash1133 2011
[8] Z A Bhutta J K Das R Bahl et al ldquoEvery newborn canavailable interventions end preventable deaths in mothersnewborn babies and stillbirths and at what costrdquo The Lancetvol 384 no 9940 pp 347ndash370 2014
[9] E Duysburgh B Kerstens M Diaz et al ldquoNewborn care inIndonesia Lao Peoplersquos Democratic Republic and the Philip-pines a comprehensive needs assessmentrdquo BMC Pediatrics vol14 no 1 article 46 2014
[10] Philippine Statistics Authority (PSA) and ICF InternationalPhilippines National Demographic and Health Survey 2013Philippine Statistics Authority (PSA) Manila Philippines ICFInternational Rockville Md USA 2014
[11] Philippine Public StormSignals 2015 httpdrrmregion4adostgovphknowledge-management-center7Philippine-public-storm-signalshtml
[12] Healthy Newborn Network (HNN) Inter-agency NewbornIndicators Technical Working Group 2012 Newborn ServicesRapid Health Facility Assessment tool 2016 httpwwwheal-thynewbornnetworkorgresourcenewborn-services-rapid-health-facility-assessment
[13] M E Kruk M Myers S T Varpilah and B T Dahn ldquoWhat isa resilient health system Lessons from Ebolardquo The Lancet vol385 no 9980 pp 1910ndash1912 2015
[14] C Enweronu-Laryea K E Dickson S G Moxon et al ldquoBasicnewborn care and neonatal resuscitation a multi-countryanalysis of health system bottlenecks and potential solutionsrdquoBMCPregnancy and Childbirth vol 15 supplement 2 article 542015
[15] United Nations Office for the Coordination of HumanitarianAffairs (UN-OCHA) ldquoTyphoon HaiyanmdashHumanitarian Snap-shotrdquo Philippines (as of Nov 12 2013) Data Sources DSWDDROMICReport Nov 12 2013 NDRRMC Situation Report 14OCHO Situation Report 5 and UNDAC Reports

8 BioMed Research International
Protocol and Basic Emergency Obstetric and Newborn Care(BEmONC) services standards were assessed through inter-views of health service providers
Significant improvements in service standards usingtracer indicators were noted across all regions over the periodfrom pretraining assessment to the 3 months posttrainingassessment Most notable were performance of the EINCldquocore stepsrdquo in immediate newborn care proper WHOpartograph use and availability of size 0 face masks forresuscitation of preterms which improved from 0 to 100at 3 months posttraining assessment
Quality labor and delivery for mothers (companion ofchoice allowing mothers to eatdrink semiupright deliverybed perineal support and restrictive episiotomy and activemanagement of the third stage of labor) and quality post-partum care (monitoring vital signs uterine massage andpostpartum visit within first week and then within fourthto sixth weeks after discharge) were carried out Facilitiesreported performance of the ldquocore stepsrdquo of immediatenewborn care (immediate and thorough drying skin-to-skincontact properly timed cord clamping and nonseparation ofnewborn from mother for early breastfeeding) and routinenewborn care (eye care physical examination and vitamin Kadministration) Postpartumwomen interviewed in the facil-ities verified the consistency of applying the EINC protocol
A persistent gap in EINC standard practice was the birthdose of BCG vaccine Ninety-six percent of facilities were notadministering this birth dose as recommended by nationalguidelines citing that using the available multidose vials foronly a few patients at each time constitutes ldquowastagerdquo Thisreflects the common practice of deferring the BCG vaccina-tion to the first-postnatal visit in the Philippines Number ofroom thermometers and wall clocks had increased in somefacilities
UnlikeWestern Visayas the 4 facilities in Central Visayashad newborn resuscitator bags and masks available priorto the EINC intervention With the intervention howeverhealth workers reported increased confidence in their newlyacquired resuscitation skills Wall clocks were present indelivery areas in all 4 facilities assessed from baseline to endline Room thermometers absent at baseline in all facilitieswere available in all 4 facilities and end line
Across the 3 regions significant improvements in servicestandards were documented In 2008 coverage of early skin-to-skin contact (SSC) was documented at 96 in deliveryassessments in 51 government hospitals [7] After governmentefforts at EINC scale-up SSC coverage was at 64 bymaternal report in 2013 [10] In this study SSC was at84 in primary level facilities postdisaster by health workerreport Before Haiyan barriers to EINC implementation thatis absence of enabling physical and policy environmentsnoncompliance by specialists and other ldquoexpertsrdquo unfamiliarwith the updated EINC practices had been diminished butnot eliminated The devastation brought by Haiyan disman-tled the systems that enabled EINC practice Neverthelessover a 3-month period an intervention of training andposttraining assessments was able to restore and for someEINC practices even exceed pre-Haiyan coverage rates
The high coverage rates for EINC indicators at baselinesuggests that previous scale-up efforts in EINC and othercross-cutting areas increased the potential for resilienceThis complemented assistance offered by other humanitarianactors (eg infrastructure rehabilitation and provision ofsupplies and equipment) turning this into an opportunity toldquobuild back betterrdquo However the contribution of pre-Haiyancapacity building efforts to this rapid restoration and furtherimprovement of EINC services requires further evaluationWe postulate that if capacity building efforts have establishedenabling environments under normal circumstances rehabil-itation could be achieved in similarly brief time periodsThuscapacity building for EINC may potentially be considered asan important disaster preparedness measure
Aiming to improve the sustainability of this interventionthe external experts provided close supportive supervisionduring the cascade training sessions and the two posttrainingassessments Our experience reveals that both performanceand environments have improved creating an enabling envi-ronment for EINC practices There were still aspects thatrequired improvement that could be reinforced by the localhealth officials during supervisory visits However this can bea challenge in areas where regular supervision visits are raredue to difficulties in geographic access or security constraints
Government support was provided through so-calledInterlocal Health Zones (ILHZs) utilizing existing referralnetworks often with rural health units (RHUs) and districthospitals as the focal point Trainers were capacitated asILHZ groups for subsequent roll-out through a skills transfermethodology This approach had its limitation though astrained health care providers from one ILHZ in generalcould not be tapped to train health care workers of anotherILHZ
In the aftermath of the disaster several developmentand recovery activities resulted in competing schedules(eg water sanitation and hygiene (WASH) vaccine coldchain implementation etc) making it difficult to scheduletraining dates Often competing capacity building activitiesand the local rehabilitation efforts involved the same setof (limited) local manpower Consequently mobilizing localstaffs to implement their trainersrsquo knowledge in cascade QAworkshops proved difficult Another constraint posed thehealth human resource availability after the disaster sincemany health care workers were victims themselves
The postdisaster setting likewise presented more chal-lenges in conducting capacity building interventions In somegeographic areas communication and road infrastructurecontinued to be unusable making it difficult for healthworkers to attend trainings or gather local data This post-disaster scenario constrained us to ldquopre- to postinterventionassessmentrdquo and its inherent methodologic limitations
This study was also limited by the fact that not all facilitieswho participated in baseline assessment were included inthe posttraining assessment Thus this study could benefitfrom another evaluation after a longer interval posttrain-ing to assess newborn outcome indicators sustainability ofimprovements and further analysis on possible contributoryeffects of other sectoral interventions (eg WASH) and
BioMed Research International 9
partner efforts in the areas The contribution of predisastercapacity building to the results could not be studied
4 Conclusions
This intervention filled the service gaps identified immedi-ately after a large scale natural disaster and helped to reestab-lish and improve the delivery of health services in affectedareas Where baseline indices were worse because of theimmediate effects of the typhoon (ie Eastern Visayas) themagnitude of improvement across most assessed parameterswas more significant However there were other parameterswhere gaps persist despite intensive efforts and othermethodsand systemic interventions need to be explored address thesedeficiencies
Our study demonstrates that quick important qualityimprovements can bemade in a timelymanner across a rangeof health facilities andwith differing cadres of health workerseven in immediate postdisaster settings Capacity building ofhealth workers and strengthening of the local health systemto deliver quality care before during and in the aftermath ofa major disaster are among the preconditions for a resilienthealth system [13] Building the evidence base linking thesequality improvement efforts in EINC and basic newbornresuscitation with impact on newborn and maternal healthoutcomes postdisaster is imperative [14]
Disclosure
Any opinions stated by UNICEF affiliates are those of theauthors and not of UNICEF
Competing Interests
The authors declare no competing interests regarding thepublication of this paper
Acknowledgments
Funding support was provided by UNICEF The authorswould like to thank our colleagues in the Department ofHealth Regional Health Offices of Eastern Central andWestern Visayas (especially Drs Corazon Sabulao and AlmaBernardo) the Provincial Health Offices of Capiz CebuIloilo Leyte and Eastern and Western Samar (especiallyDrs Samuel Delfin Cynthia Genosolango Grace Trabadoand Marian Isiderio) Dr Nabila Zaka (UNICEF) and theInternational Medical Corps
References
[1] October 2015 httplibrarypcwgovphsitesdefaultfiles14011120SDR20Yolanda20Philippnes20finalpdf
[2] ldquoResponding toTyphoonHaiyanrdquoTheLancet vol 382 no 9907article 1769 2013
[3] R C Alfonso D S Capili K A Reyes F Tatad-To and M ASilvestre ldquoContributing to the Infant and Young Child Feedingin Emergencies (IYCF-E) response in the Philippines A local
NGOperspectiverdquo 2015 httpwwwennonlinenetfex50iycf-philippines
[4] WHO Philippines ldquoEssential Intrapartum and Newborn Care(EINC) Evidence-based Standard Practicesrdquo 2016 httpwwwwprowhointphilippinesareasmaternal child nutritionnew-born mother careeinc protocolsen
[5] WHO WPRO ldquoEarly Essential Newborn Care First EmbraceClinical Practice Pocket Guiderdquo 2014 httpiriswprowhointbitstreamhandle106651107989789290616856 engpdfjsessi-onid=B789B68B6D8BF8BB2C7F99F09E698AE1sequence=3
[6] H Obara and H Sobel ldquoQuality maternal and newborn care toensure a healthy start for every newborn in the World HealthOrganization Western Pacific Regionrdquo BJOG An InternationalJournal of Obstetrics andGynaecology vol 121 pp 154ndash159 2014
[7] H L Sobel M A A Silvestre J B V Mantaring III Y EOliveros and S Nyunt-U ldquoImmediate newborn care practicesdelay thermoregulation and breastfeeding initiationrdquo Acta Pae-diatrica International Journal of Paediatrics vol 100 no 8 pp1127ndash1133 2011
[8] Z A Bhutta J K Das R Bahl et al ldquoEvery newborn canavailable interventions end preventable deaths in mothersnewborn babies and stillbirths and at what costrdquo The Lancetvol 384 no 9940 pp 347ndash370 2014
[9] E Duysburgh B Kerstens M Diaz et al ldquoNewborn care inIndonesia Lao Peoplersquos Democratic Republic and the Philip-pines a comprehensive needs assessmentrdquo BMC Pediatrics vol14 no 1 article 46 2014
[10] Philippine Statistics Authority (PSA) and ICF InternationalPhilippines National Demographic and Health Survey 2013Philippine Statistics Authority (PSA) Manila Philippines ICFInternational Rockville Md USA 2014
[11] Philippine Public StormSignals 2015 httpdrrmregion4adostgovphknowledge-management-center7Philippine-public-storm-signalshtml
[12] Healthy Newborn Network (HNN) Inter-agency NewbornIndicators Technical Working Group 2012 Newborn ServicesRapid Health Facility Assessment tool 2016 httpwwwheal-thynewbornnetworkorgresourcenewborn-services-rapid-health-facility-assessment
[13] M E Kruk M Myers S T Varpilah and B T Dahn ldquoWhat isa resilient health system Lessons from Ebolardquo The Lancet vol385 no 9980 pp 1910ndash1912 2015
[14] C Enweronu-Laryea K E Dickson S G Moxon et al ldquoBasicnewborn care and neonatal resuscitation a multi-countryanalysis of health system bottlenecks and potential solutionsrdquoBMCPregnancy and Childbirth vol 15 supplement 2 article 542015
[15] United Nations Office for the Coordination of HumanitarianAffairs (UN-OCHA) ldquoTyphoon HaiyanmdashHumanitarian Snap-shotrdquo Philippines (as of Nov 12 2013) Data Sources DSWDDROMICReport Nov 12 2013 NDRRMC Situation Report 14OCHO Situation Report 5 and UNDAC Reports

BioMed Research International 9
partner efforts in the areas The contribution of predisastercapacity building to the results could not be studied
4 Conclusions
This intervention filled the service gaps identified immedi-ately after a large scale natural disaster and helped to reestab-lish and improve the delivery of health services in affectedareas Where baseline indices were worse because of theimmediate effects of the typhoon (ie Eastern Visayas) themagnitude of improvement across most assessed parameterswas more significant However there were other parameterswhere gaps persist despite intensive efforts and othermethodsand systemic interventions need to be explored address thesedeficiencies
Our study demonstrates that quick important qualityimprovements can bemade in a timelymanner across a rangeof health facilities andwith differing cadres of health workerseven in immediate postdisaster settings Capacity building ofhealth workers and strengthening of the local health systemto deliver quality care before during and in the aftermath ofa major disaster are among the preconditions for a resilienthealth system [13] Building the evidence base linking thesequality improvement efforts in EINC and basic newbornresuscitation with impact on newborn and maternal healthoutcomes postdisaster is imperative [14]
Disclosure
Any opinions stated by UNICEF affiliates are those of theauthors and not of UNICEF
Competing Interests
The authors declare no competing interests regarding thepublication of this paper
Acknowledgments
Funding support was provided by UNICEF The authorswould like to thank our colleagues in the Department ofHealth Regional Health Offices of Eastern Central andWestern Visayas (especially Drs Corazon Sabulao and AlmaBernardo) the Provincial Health Offices of Capiz CebuIloilo Leyte and Eastern and Western Samar (especiallyDrs Samuel Delfin Cynthia Genosolango Grace Trabadoand Marian Isiderio) Dr Nabila Zaka (UNICEF) and theInternational Medical Corps
References
[1] October 2015 httplibrarypcwgovphsitesdefaultfiles14011120SDR20Yolanda20Philippnes20finalpdf
[2] ldquoResponding toTyphoonHaiyanrdquoTheLancet vol 382 no 9907article 1769 2013
[3] R C Alfonso D S Capili K A Reyes F Tatad-To and M ASilvestre ldquoContributing to the Infant and Young Child Feedingin Emergencies (IYCF-E) response in the Philippines A local
NGOperspectiverdquo 2015 httpwwwennonlinenetfex50iycf-philippines
[4] WHO Philippines ldquoEssential Intrapartum and Newborn Care(EINC) Evidence-based Standard Practicesrdquo 2016 httpwwwwprowhointphilippinesareasmaternal child nutritionnew-born mother careeinc protocolsen
[5] WHO WPRO ldquoEarly Essential Newborn Care First EmbraceClinical Practice Pocket Guiderdquo 2014 httpiriswprowhointbitstreamhandle106651107989789290616856 engpdfjsessi-onid=B789B68B6D8BF8BB2C7F99F09E698AE1sequence=3
[6] H Obara and H Sobel ldquoQuality maternal and newborn care toensure a healthy start for every newborn in the World HealthOrganization Western Pacific Regionrdquo BJOG An InternationalJournal of Obstetrics andGynaecology vol 121 pp 154ndash159 2014
[7] H L Sobel M A A Silvestre J B V Mantaring III Y EOliveros and S Nyunt-U ldquoImmediate newborn care practicesdelay thermoregulation and breastfeeding initiationrdquo Acta Pae-diatrica International Journal of Paediatrics vol 100 no 8 pp1127ndash1133 2011
[8] Z A Bhutta J K Das R Bahl et al ldquoEvery newborn canavailable interventions end preventable deaths in mothersnewborn babies and stillbirths and at what costrdquo The Lancetvol 384 no 9940 pp 347ndash370 2014
[9] E Duysburgh B Kerstens M Diaz et al ldquoNewborn care inIndonesia Lao Peoplersquos Democratic Republic and the Philip-pines a comprehensive needs assessmentrdquo BMC Pediatrics vol14 no 1 article 46 2014
[10] Philippine Statistics Authority (PSA) and ICF InternationalPhilippines National Demographic and Health Survey 2013Philippine Statistics Authority (PSA) Manila Philippines ICFInternational Rockville Md USA 2014
[11] Philippine Public StormSignals 2015 httpdrrmregion4adostgovphknowledge-management-center7Philippine-public-storm-signalshtml
[12] Healthy Newborn Network (HNN) Inter-agency NewbornIndicators Technical Working Group 2012 Newborn ServicesRapid Health Facility Assessment tool 2016 httpwwwheal-thynewbornnetworkorgresourcenewborn-services-rapid-health-facility-assessment
[13] M E Kruk M Myers S T Varpilah and B T Dahn ldquoWhat isa resilient health system Lessons from Ebolardquo The Lancet vol385 no 9980 pp 1910ndash1912 2015
[14] C Enweronu-Laryea K E Dickson S G Moxon et al ldquoBasicnewborn care and neonatal resuscitation a multi-countryanalysis of health system bottlenecks and potential solutionsrdquoBMCPregnancy and Childbirth vol 15 supplement 2 article 542015
[15] United Nations Office for the Coordination of HumanitarianAffairs (UN-OCHA) ldquoTyphoon HaiyanmdashHumanitarian Snap-shotrdquo Philippines (as of Nov 12 2013) Data Sources DSWDDROMICReport Nov 12 2013 NDRRMC Situation Report 14OCHO Situation Report 5 and UNDAC Reports
Related Documents











