TRUST BOARD PART 1 Schedule Tuesday, 27 Nov 2018 8:30 AM — 10:00 AM GMT Venue BOARDROOM Organiser Claire Coles Agenda 1. AGENDA 1 11~18 Part 1.doc 2 2. 312/18 WELCOME FROM THE CHAIRMAN AND APOLOGIES FOR ABSENCE 4 3. 313/18 DECLARATION OF INTERESTS OR AMENDMENTS TO THE REGISTER OF INTEREESTS 5 4. 314/18 MINUTES OF THE LAST MEETING 6 10 Draft Public Minutes 6 November 2018 V2.doc 7 5. 315/18 MATTERS ARISING FROM THE MINUTES - ACTIONS ARISING REPORT 16 10 Matters Arising Report for October Public Board.doc 17 6. 316/18 CHIEF EXECUTIVE REPORT AND INTEGRATED PERFORMANCE REPORT 21 316~18_IPR for Board - November 2018 Meeting.doc 22 316~18_IPR - October 2018.pdf 24 316~16_M7 Finance Report cover sheet.doc 50 316~18_NEW BOARD FINANCE REPORT Oct 2018 M7 (Final).ppt 51 316~18_CEO Report November 2018 Board.docx 64

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

TRUST BOARD PART 1Schedule Tuesday, 27 Nov 2018 8:30 AM — 10:00 AM GMT
Venue BOARDROOM
Organiser Claire Coles
Agenda
1. AGENDA 1
11~18 Part 1.doc 2
2. 312/18 WELCOME FROM THE CHAIRMAN AND APOLOGIES FORABSENCE
4
3. 313/18 DECLARATION OF INTERESTS OR AMENDMENTS TO THEREGISTER OF INTEREESTS
5
4. 314/18 MINUTES OF THE LAST MEETING 6
10 Draft Public Minutes 6 November 2018 V2.doc 7
5. 315/18 MATTERS ARISING FROM THE MINUTES - ACTIONS ARISINGREPORT
16
10 Matters Arising Report for October Public Board.doc 17
6. 316/18 CHIEF EXECUTIVE REPORT AND INTEGRATED PERFORMANCEREPORT
21
316~18_IPR for Board - November 2018 Meeting.doc 22 316~18_IPR - October 2018.pdf 24 316~16_M7 Finance Report cover sheet.doc 50 316~18_NEW BOARD FINANCE REPORT Oct 2018 M7 (Final).ppt 51 316~18_CEO Report November 2018 Board.docx 64

7. 317/18 QUALITY COMMITTEE 84
317~18_Report from the Quality Committee_Nov 2018.doc 85
8. 318/18 FINANCE AND RESOURCES COMMITTEEAppendix A - to follow
87
318~18_Report from the Finance and Resources Committee_Nov2018.doc
88
318~18 FRC report - App A.docx 91
9. 319/18 RISK AND AUDIT COMMITTEE 93
319_18_Report from Risk and Audit Committee Nov 2018 (updated).doc 94
10. 320/18 BOARD ASSURANCE FRAMEWORK 97
320~18_BAF Risks cover sheet.doc 98 320~18_BAF Updated Nov 2018 reported to Board.pdf 100
11. 321/18 NURSING ESTABLISHMENT 101
321~18_Nursing Est Review Nov 18 front sheet.doc 102 321~18_Nursing Establishment Review Oct 2018 V2.docx 103
12. 322/18 TRUST STRATEGIES- Communications Strategy- Marketing Strategy- Risk Management Strategy
118
322~18_i_Board Cover Sheet_Communications Strategy.doc 119 322~18_i_Communications Strategy 2018-2021.pdf 121 322~18_ii_marketing strategy cover sheet.doc 138 322~18_ii_Marketing strategy draft 1.7.pdf 139 322~18_iii_Public Template_2018_Part 1_Caring Together.doc 173 322~18_iii_Strategy RM.docx 175

13. 323/18 CQC UNANNOUNCED VISIT REPORTS 187
323~18_CQC unnannouced CWAMH Visit Report COVER SHEET.docx 188
14. 324/18 SOUTH YORKSHIRE AND BASSETLAW ICS: MOU 199
324~18_ICS MOU Cover sheet.doc 200 324~18_SYB_MOU_FINAL (3) national signed by Andrew Cash no
confidential.pdf201
15. 326/18 ICS - MONTH 6 FINANCE POSITION 234
326~18 Cover sheet for ICS Month 6 Finance Position.doc 235 326~18_Financial reporting Month 6 ESG v4 JC.docx 237
16. 327/18 ANY OTHER BUSINESS 245
17. 328/18 IDENTIFICATION OF KEY RISKS, SUCCESSES, DECISIONSMADE TO BE ESCALATED / SHARED FROM THE MEETING
246
18. 329/18 DATE OF NEXT PUBLIC MEETING: Tuesday 18 December 2018,08:30 Boardroom
247

1. AGENDA

Meeting of the Board of Directors held on 27 November 2018 at 08:30hrs – 13:00hrs
The Boardroom
PART ONE
1.1 BOARD BUSINESS
312/18 WELCOME FROM THE CHAIRMAN AND APOLOGIES FOR ABSENCE:
313/18 DECLARATION OF INTERESTS OR AMENDMENTS TO THE REGISTER OF INTERESTS
314/18 MINUTES OF THE LAST MEETING The Board is asked to approve the minutes of the Board meeting held on 6 November 2018
To approve
315/18 MATTERS ARISING FROM THE MINUTES - ACTIONS ARISING REPORT To note
1.3 QUALITY, PERFORMANCE & RESOURCES (TO BE TAKEN AT 08:35)
316/18 CHIEF EXECUTIVE REPORT AND INTEGRATED PERFORMANCE REPORT, Mr J Somers, Chief Executive The Board is asked to note the briefing which provides context and updates the Board on key activities during the last month and presents an overview of performance within the Trust.
To note
1.4 GOVERNANCE (TO BE TAKEN AT 08:55)
317/18 QUALITY COMMITTEE, Ms P Mitchell, NED, Chair of the Quality Committee The Board is asked to note any key issues arising from the Quality Committee held 19 November 2018.
To note
318/18 FINANCE AND RESOURCES COMMITTEE, Mr A Baker, NED, Chair of the Finance and Resources Committee The Board is asked to note any key issues arising from the Finance and Resources Committee held 21 November 2018
To note
319/18 RISK AND AUDIT COMMITTEE, Mr J Cowling, NED, Chair of the Risk and Audit Committee The Board is asked to note any key issues arising from the Risk and Audit Committee held 14 November 2018
To note
1.5 REPORTS FOR BOARD CONSIDERATION (TO BE TAKEN AT 09:10)
320/18 BOARD ASSURANCE FRAMEWORK, Mr M Kane, Associate Director of Corporate Affairs The Board is asked to review the Board Assurance Framework following discussion at the November Risk and Audit Committee.
To note & gain assurance
321/18 NURSING ESTABLISHMENT, Ms S Shearer, Director of Nursing and Quality
The Board is asked to review the report and recommendations, as considered by the November Quality Committee.
To note & gain assurance
322/18 TRUST STRATEGIES, Introduced by Mr J Somers, Chief Executive Communications Strategy: Recommended by Finance and Resources Committee
Mr S Ned, Director of HR and OD Marketing Strategy: Recommended by Finance and Resources Committee
Ms R Brown, Director of Strategy and Operations and Mr S Ned, Director of HR and OD Risk Management Strategy: Recommended by Risk and Audit Committee
Mrs S Shearer, Director of Nursing and Quality
The Board is asked to approve updated Trust Strategies, which have been reviewed and recommended for approval by the relevant Board Committee.
To Approve
323/18 CQC UNANNOUNCED VISIT REPORTS, Ms S Shearer, Director of Nursing and Quality
The Board is asked to note the report and the actions plans that are in place. To note & gain
assurance
1.6 STRATEGIC ISSUES (TO BE TAKEN 09:40)
324/18 SOUTH YORKSHIRE AND BASSETLAW ICS: MEMORANDUM OF UNDERSTANDING, Mr J Somers, Chief Executive The Board is asked to approve the Memorandum of Understanding.
To Approve
AGENDA
TRUST BOARD PART 1 1. AGENDA Page 2 of 247

326/18 ICS – MONTH 6 FINANCE POSITION, Mr M Smith, Chief Finance Officer The Board is asked to note the ICS Month 6 finance report, to ensure the Trust continues to be kept updated, and agree any actions required.
To Note
1.7 CLOSING MATTERS (TO BE TAKEN AT 10:00)
327/18 ANY OTHER BUSINESS Action as appropriate
328/18 IDENTIFICATION OF KEY RISKS, SUCCESSES, DECISIONS MADE TO BE ESCALATED / SHARED FROM THE MEETING
Action as appropriate
329/18 DATE OF NEXT PUBLIC MEETING: Tuesday 18 December 2018, 08:30hrs in the Boardroom.
Action as appropriate
Resolution: To exclude the press and public from the meeting at this point on the grounds that publicity of the matters being reviewed would be prejudicial to public interest, by reason of the confidential
nature of business. The press and public are requested to leave at this point.
TRUST BOARD PART 1 1. AGENDA Page 3 of 247

2. 312/18 WELCOME FROM THECHAIRMAN AND APOLOGIES FORABSENCE

3. 313/18 DECLARATION OFINTERESTS OR AMENDMENTS TO THEREGISTER OF INTEREESTS

4. 314/18 MINUTES OF THE LASTMEETING

1
277/18 – 295/18
Minutes of the Meeting of the Board of Directors - Part One
on Tuesday 6 November 2018 at 08.30hrs
The Boardroom
In the Chair: Ms S Jones Chair Present: Mr A Baker Non-executive Director Ms R Brown Director of Strategy and Operations Mr J Cowling Non-executive Director Mr S Green Non-executive Director Mr P Lauener Non-executive Director Mr S Ned Director of Human Resources and Organisational Development / Deputy CE Dr J Perring Medical Director Ms S Shearer Director of Nursing and Quality Mr M Smith Chief Finance Officer Mr J Somers Chief Executive
Apologies: Ms P Mitchell Non-executive Director In attendance: Ms D Bedford CQC Mrs C Coles Minute Taker Ms J Dentith Interim – Corporate Affairs Professor P Dimitri (item 281/18) Director of Research and Innovation Jane Giniver Deputy Director ACP Ms E Hopkinson (items 288/18 & 291/18) Head of Learning and Organisational Development Mr M Kane Associate Director of Corporate Affairs Designate (Observing) One member of staff One member of the public
TRUST BOARD PART 1 4. 314/18 MINUTES OF THE LAST ... Page 7 of 247

2
Action 277/18 WELCOME FROM THE CHAIRMAN AND APOLOGIES FOR ABSENCE Ms Jones, Chair, welcomed Board Members and noted the apologies as above.
278/18 DECLARATION OF INTERESTS OR AMENDMENTS TO THE REGISTER OF INTERESTS Mr Kane was welcomed to the meeting as an observer, and would be commencing employment with the Trust from 12 November 2018, in the role of Associate Director of Corporate Affairs.
279/18 MINUTES OF THE LAST MEETING The draft minutes of the meeting held on 26 September 2018 were approved as an accurate record of the meeting with amendments made to: 242/19 Chief Executive Report and Integrated Performance Report “Discharge summaries continued to remain below the 100 per cent target. The Quality Committee would receive a quarterly follow up report following a recent deep dive into the issue at its October meeting. The Director of Strategy and Operations would investigate why a suggested pilot of no discharge without a discharge summary had not been taken forward over the summer …” 249/19 Patient Story “The Board welcomed a parent and patient’s sister to the meeting to share a patient story.”
280/18 MATTERS ARISING The Board noted the updates on the actions arising report. 247/18 iii) Quarterly Report from the Guardian of Safe Working Hours It was confirmed to the Board that a meeting had taken place to agree resolution of the concerns. Technical issues relating to system log ins had been actioned. The Quality Committee had been asked to oversee resolution of the concerns. 248/18 iv) Annual Report from the Responsible Officer: Revalidation The Medical Director had received assurance from the HR department that appropriate checks were completed. The concern raised relating to outstanding identity checks was due to the timing in receiving DBS clearance. 249/18 vii) Patient Story The Medical Director had met with the patient’s Consultant to ensure the patient received the right access to services. The Medical Director had also written to Consultants to ensure that patients over 18 years transitioning to adult services had access to services and level of care. The Quality Committee had oversight of issues relating to patients over 18 who were transitioning. 208/18 Finance and Resources Committee Director of HR and OD confirmed that the new Finance and Resources Committee agenda cycle was providing greater focus on people. The work plan had recently been reviewed and Committee would continue to receive routine HR items as part of the work plan. 242/18 Chief Executive Report and Integrated Performance Report The Medical Director informed the Board that meetings with Leeds and Hull were taking
Action closed Action closed Action closed Action closed
Action
TRUST BOARD PART 1 4. 314/18 MINUTES OF THE LAST ... Page 8 of 247

3
place, this was an ongoing piece of work. Progress updates would be built into the Integrated Performance Report therefore this action would be closed. 242/18 Chief Executive Report and Integrated Performance Report The Director of Strategy and Operations informed the Board that a pilot for discharge summaries had been discussed at Quality Committee following a deep dive of this area. A discussion had taken place with the Medical Director and it was agreed it was essential to ensure that staffing and governance arrangements were in place before a pilot could be undertaken, and also agreed that this should not be undertaken over the winter period. This position would be reviewed following further discussion at Quality Committee. This action would be closed, and an update provided by the Quality Committee as appropriate. Performance against discharge summaries would continue through the intergrated performance report. 249/18 vi) Patient Story The Medical Director provided assurance that a review of complex patients with learning disabilities formed part of a piece of work by the Mortality Review Group. A baseline audit against national learning disabilities guidelines was also taking place. This was an ongoing piece of work, therefore the action would be closed. 249/18 ix) Patient Story The Director of Nursing and Quality reported on work taking place with specialist nurses, and two way communications would be picked up through those conversations. The Director of Nursing and Quality also reported that a patient story had been filmed for the December Board, and Board members were offered the opportunity to be involved in the filming of future stories. The report and additional verbal updates were noted.
closed Action closed Action closed Action closed
281/18 RESEARCH AND INNOVATION ANNUAL REPORT 2017/18 Professor Dimitri presented highlights from the annual report. Key points from the presentation were made / highlighted: i) The Trust had recruited 1271 participants to the National Institute of Health
Research (NIHR) portfolio research projects, this was 134 per cent of the total recruitment target for the year, exceeding other trusts within the region. It was positive to see the level of interest within the Trust and reflected the increase in studies and high number of commercial trials being undertaken. The Trust generated £208k income within 2017/18 for commercial trials.
ii) The positive progress of the Centre of Child Health and Technology was noted. It was agreed that a progress update on the programme would be presented to the Finance and Resources Committee at a future meeting. The challenge to identifying full funding of the programme was noted, and that options to identify funding were being explored.
iii) The proposal to bring Children’s Clinical Research Facility in-house was noted, following sharing of the facility with medical day care. This would provide opportunity to focus on mental health, as well as explore interest from industry.
iv) The challenges going forward were noted in relation to workforce flexibility and capacity to support the growth in a number of studies, and ways to financially do this were being explored.
v) Whilst the research culture within the Trust was positive it was acknowledged that this was across clusters of professionals, however other areas were now developing research groups. The Board supported an opt out model, and strengthening of the message that the Trust was an active research organisation. Consideration would
TRUST BOARD PART 1 4. 314/18 MINUTES OF THE LAST ... Page 9 of 247

4
be given to having a research focused quarterly clinical summit, as there was clear interest from across the Trust.
vi) It was important to have joined up working arrangements with partners across the ACP in supporting a city wide strategy, and to support city wide bids to bring in funding opportunities to the city as one unit within Sheffield.
Professor Dimitri was thanked for his presentation.
282/18 CHIEF EXECUTIVE REPORT AND INTEGRATED PERFORMANCE REPORT The Chief Executive provided an overview of key issues, highlighting key points from supporting papers appended for information and invited Executive Directors to outline key successes or issues currently affecting the Trust.
The Trust had met all its NHS Improvement targets and key performance indicators, with overall performance of the Trust reported as good. Referral to Treatment 18 week waits was an area of focus due to concerns on how close it was to the target to understand from a local perspective.
The Board positively noted that no patients had been cancelled on the day.
The Did Not Attend rate was reported higher against target, this was a concern due to the amount of work currently happening around the new terminology and campaign for Was Not Brought. This data would be reviewed.
Friends and Family Test performance had exceeded the target, and Board noted the positive increase that 90 per cent of staff would recommend the Trust as place to work. Response rates were improving month on month due to a number of proactive interventions to increase rates driven by the Care Experience Group. The sustained improvement was good.
The high number of incidents was due to a back log of incidents due for review within Datix. This was an improving position however focus on reducing the back log would be maintained.
Plans were in place to update out of date policies and clinical guidelines. These were being tracked on a weekly basis. It was unclear how the number of out of date policies compared to the number of policies in place within the Trust, however Board was assured that some policies required minor changes and remained procedurally compliant.
Sickness absence rates were reported above target at 4.07 per cent against a target of 4 per cent. This was due to ward sickness and number of vacancies, this position was being reviewed. The Board noted that this rate was above other regional trusts rates.
The Trust reported its month 6 financial position was slightly ahead of plan, and that the cash position was healthy. The forecast outturn position was on plan at quarter 2, however the risk in the profile from month 7 to month 12 was highlighted to the Board. Key Updates
The Trust had received the Provider Information Request (PIR) from the Care Quality Commission (CQC) and focus was on preparations for inspection, and the team were working towards submission of the PIR by the 22 November deadline.
The Board noted involvement in the recent ACP workshop. Discussions focussed on governance, and aligning statutory and non-statutory functions. It was important to ensure the Trust was represented within the ACP. The workshop had agreed to focus on a small number of priority areas as a City. The
TRUST BOARD PART 1 4. 314/18 MINUTES OF THE LAST ... Page 10 of 247

5
Board recognised the importance of citywide partner organisations aligning in to a Sheffield strategy from a city perspective, to create a “Sheffield” brand.
The Board noted the positive report and key additional verbal updates.
283/18 QUALITY COMMITTEE Mr Lauener, Non-executive Director noted, on behalf of Ms Mitchell Chair of the Quality Committee, the key issues arising from the Quality Committee meeting on 15 October 2018 as outlined in the supporting summary report. The following points were made / emphasised: i) The report reflected the significant work of the Committee and volume of papers on
the agenda which required scrutiny. The volume of papers and depth of discussion at Committee meetings was noted, this would be reviewed as part of a review of organisational decision-making processes.
ii) A deep dive of CWAMH Division provided assurance that issues highlighted at the Becton site were being addressed, and that improvements were being made to accommodation and security. A further update would be provided to the November meeting in the Committee’s continuing oversight of these issues and monitoring of implementation going forward.
The report and additional update was noted.
284/18 FINANCE AND RESOURCES COMMITTEE Mr Baker, Chair of the Finance and Resources Committee, presented key issues arising from the meeting on 24 October 2018 as outlined in the supporting summary. The following was noted: i) The reflection of volume of papers, and concern that any deferring of papers
impacted on future meetings, and ensuring appropriate time to discuss items. ii) The risk in the phased profile of the financial plan was highlighted as a concern.
Delivery of the transformation and recovery programme was key, and maintaining the pace was important.
iii) The Board noted a Was Not Brought report with 10,000 missed appointments year to date. The cost of each missed appointment was between £130-150 per appointment. An appropriate plan and campaign would develop to reduce the number.
The report and additional update was noted.
285/18 WINTER RESILIENCE PLAN The Director of Strategy and Operations, and Director of Nursing and Quality outlined actions in the winter resilience plan to ensure the hospital remained safe over the winter. The following was noted:
i) The report provided assurance to the Board that the Trust was prepared for winter, building on previous years and plans for coming winter outlined.
ii) No additional non-recurrent monies were available for 2018/19. The Trust was encouraged to consider writing to the Clinical Commissioning Group outlining actions happening and additional actions that would be undertaken with support from them.
iii) Risks related to operational issues around staffing, due to a potential influx of activity. Implementation of huddles and an escalation process put in place in 2017/18 had worked well and these would be built on. Clinical operations group was tracking operational issues and overseeing the plan.
iv) Flu vaccinations programme was reported at 43 per cent, and staff that had not
TRUST BOARD PART 1 4. 314/18 MINUTES OF THE LAST ... Page 11 of 247

6
received their flu vaccination were being targeted within divisions. It was unclear how this figure compared to the 2017/18 position at the same point in the year, as it had been made mandatory nationally. The Board supported the 2017/18 decision to make this requirement mandatory for this and future years.
v) The Board noted the ambulance handover target. The delay in time taken to handover a child was due to complex cases and data issues tracking. Work was being taken forward with Yorkshire Ambulance Service to align electronic systems in the aspiration to achieve the 15 minute handover target.
The report and additional update was noted.
286/18 SHADOW BOARD DEVELOPMENT PROGRAMME
The Head of Learning and Organisational Development presented the report for information. The following was noted: i) The programme had met all the criteria, which had been funded through Health
Education England. Three participants on the programme had now successfully taken up more senior roles, and participants were keen to offer insight into Board papers as directed by Board.
ii) Whilst mentorship had been light touch, the Board was thanked for their commitment to support the programme, which was appreciated by participants and all involved in the programme. Mentor meetings had been flexible and were felt to be productive, and also gave Non-executive Directors additional insight into the organisation.
iii) Whilst there was no formal programme continuing with existing participants they had committed to have a network, and aspired to continue discussions.
iv) Next steps would be to run a programme for next management tier, potentially a Shadow TEG, and run another shadow board in the future.
v) The Director of Strategy and Operations would discuss how Associate Director development overlapped with the shadow programme in relation to identifying potential future leaders.
The Board noted the report.
287/18 EMERGENCY PLANNING STATEMENT OF COMPLIANCE The Director of Nursing and Quality presented the report. Key points were highlighted: i) The Trust had self-assessed against revised NHS core standards for Emergency
Planning, Resilience and Response. Following discussion with the Local Health Resilience Partnership the Trust had declared non-compliance. This was due to changes in the core standards and having a vacancy for the Emergency Planning Officer. The Emergency Planning Officer was now in post and was progressing actions within the improvement programme to address outstanding core standards to achieve 76 per cent compliance by the end of January 2019.
ii) The Risk and Audit Committee had sought assurance on progress against actions to address compliance and progress would be reviewed quarterly by the Committee.
The Board noted the report.
288/18 SPOTLIGHT PRESENTATION – LOOKED AFTER CHILDREN The Designated Doctor, Looked After Children gave a presentation outlining the work of the Looked After Children Team. The following was highlighted to the Board: i) The team was achieving 70 per cent completion of initial health assessments within
20 days. The delay was due to the completion of health assessments across health boundaries, and related to consent, and the impact of other agencies
TRUST BOARD PART 1 4. 314/18 MINUTES OF THE LAST ... Page 12 of 247

7
priorities causing delays.
ii) A presentation had been provided to the Safeguarding Board following a deep dive to understand the reasons for not achieving the target. The team had met with partners to speed up processes and standardise KPIs. Following this deep dive the target was now achieving 90 – 95 per cent rates.
iii) It was highlighted that Level 4 knowledge and training was required by Board, this would be included in the Board’s annual safeguarding training. Training would also be incorporated into the Trust’s safeguarding training programme to ensure all staff had knowledge, with higher level of knowledge for key specialist staff. The Head of Learning and Development would reflect this in the training programme.
iv) The service was now a more holistic service, with improved efficiency to allow the team flexibility to support other areas of service. Their future aspiration was to be a centre of excellence.
v) There was currently a two tier system for looked after children, once adopted children moved back into the general system. Project Aspire would have impact an on children on the edge of care, this system would go live from January.
vi) Looked after children’s teams were meeting regionally to look more strategically at cross boundary working and across specialty pathways.
vii) The Board noted the change in having a designated doctor which sat within the Clinical Commissioning Group and named doctor role which sat within the Trust to ensure there were no conflicts. This was a key change to take forward. The Medical Director would pick this up.
viii) Board members were invited to undertake back to the floor visits to the service.
The report presentation was noted and Dr Pearson thanked for her presentation.
MD
289/18 DELIVERING “CARING TOGETHER”: QUARTER 2 PERFORMANCE AGAINST CORPORATE OBJECTIVES 2018/19 The Director of Strategy and Operations presented the quarter two report. The following was noted: i) Quarter two progress update was noted, with four areas identified where progress
had been slower than anticipated. These were reported to Board as ongoing areas of focus, and ratings would be refreshed.
ii) The rating of financial plan delivery would be refreshed to amber following discussion at the mid-year review point. Divisional performance and quality meetings would review individual divisional positions.
iii) Work on ward accreditation had been paused to allow the implementation of quality improvement work and consideration of alternative models, with mock CQC inspections and Executive visits to services increased as part of the quality improvement programme. A quality strategy was being developed with divisions which was expected to be in place by February. Progress of the objective would be updated to reflect this change.
iv) Recruitment was taking place to vacancies in the finance department, which would increase finance support to divisions. The department was prioritising actions to develop reports for divisions. The Board was assured that divisions received activity information for them to review. These packs had significantly improved engagement and enabled divisions to make decisions.
v) Director of Strategy and Operations would advise how performance against the Trust’s objectives and within certain areas would be communicated to the Trust to help drive up performance. It was suggested that relevant sections of performance
DSO
TRUST BOARD PART 1 4. 314/18 MINUTES OF THE LAST ... Page 13 of 247

8
should be considered by Committees before being reviewed by Board. The Board noted the report and good progress.
290/18 PRESENTATION OF THE PEOPLE STRATEGY The Director of HR and OD presented the strategy. Key points were highlighted: i) The Board recognised that a high quality workforce was key to achieving its
strategic aims. The strategy provided a broad strategic framework to achieve these strategic aims and objectives.
ii) The draft strategy had been scrutinised by committees, who supported the key themes identified.
iii) The next steps would be to develop each chapter. Whilst the key themes was not a priority list the Board considered that development of the health and wellbeing and staff engagement chapters were current priorities, and these were interlinked to the culture and behaviour strategy.
iv) The aspiration to achieve 100 per cent PDR and mandatory training compliance was recognised, and Board supported sustaining rates at 90 per cent, with consideration given to how 100 per cent could be achieved. Clinical and nursing staff engagement was key to achieving 100 per cent compliance as the Trust’s largest workforce.
v) The Board supported developing a front facing staff focussed version around the key themes. Whilst a review of the gender pay gap had been undertaken earlier in the year this would be referenced within the chapters. Consideration would be given to whether there was a role for the shadow board in the next phase of work to develop a cohesive plan and identify timelines for the final strategy.
vi) The strategy would be developed through Committee support, and prioritisation of chapters considered. The completed strategy would be taken to February Finance and Resources Committee and February Board.
The strategy was approved.
DHROD Planner
291/18 PRESENTATION OF THE CULTURE AND BEHAVIOUR STRATEGY The Head of Learning and Organisational Development presented the strategy for information. The following was noted: i) Comments received through consultation had been incorporated into the final draft.
The four areas identified to create the culture within the organisation to reinforce the Trust values were endorsed.
ii) Slight amendments would be made to some of the wording within section 3. iii) The Board supported setting qualitative measures to be able to track progress,
embeddedness and culture change as well as ensuring consistent working across the Trust as a multi-site organisation, recognising the challenge to create the desired culture across a number of sites.
iv) Further action was required to understand how behaviours linked to the Trust values with consideration given to workplace accreditation programmes, and the academic theory behind these.
v) The timelines for the final strategy would be identified. The final chapters developed and programme of activity needed to help achieve this culture within all aspects of the organisation would be taken to the December Finance and Resources Committee, and brought back to the February Board.
The strategy was approved.
Planner
TRUST BOARD PART 1 4. 314/18 MINUTES OF THE LAST ... Page 14 of 247

9
292/18 SOUTH YORKSHIRE AND BASSETLAW: HOSPITAL SERVICES REVIEW: STRATEGIC OUTLINE CASE The Chief Executive presented the report. The following was noted: i) The report had been through due process and reviewed in detail at the September
Board Part 2. The report was noted.
293/18 ANY OTHER BUSINESS
None.
2942/18 IDENTIFICATION OF KEY RISKS, SUCCESSES, DECISIONS MADE TO BE ESCALATED/ SHARED FROM THE MEETING
No items were discussed.
295/18 DATE OF THE NEXT PUBLIC MEETING Tuesday 27 November 2018, 08:30hrs in the Boardroom.
TRUST BOARD PART 1 4. 314/18 MINUTES OF THE LAST ... Page 15 of 247

5. 315/18 MATTERS ARISING FROMTHE MINUTES - ACTIONS ARISINGREPORT

Actions Arising Report – updated following 6 November 2018 Board Meeting held in Public
Action ref:
Date Action raised
Action Action with
Target date to
complete Progress / evidence that
completed
137/18 Hospital Project Board: Operationalisation of the Hospital Wing
23/05/18
Mr Green, would raise the concerns with the Safer Roads Policing Team in relation to a crossing on Clarkson Road.
SG AD
Comms
June Nov 2018
Concerns raised verbally with the Safer Roads Policy Team. The Trust should continue to make representations to Sheffield City Council.
Update provided under agenda item 205/18. Action transferred to AD Communications. Action Carried Forward. Update provided under agenda item 241/18. Communications plan to be brought to the November meeting.
288/18 vii) Spotlight Presentation – Looked After Children
06/11/18
The change to the Designated doctor and Named doctor roles was a key change to take forward. The Medical Director would pick this up.
MD TBC
Completed Actions updated following 6 November Board Meeting held in Public
Action ref:
Date Action raised
Action Action with
Target date to
complete Progress / evidence that
completed
208/18 Finance and Resources Committee
31/07/18
Reflections from the new agenda cycle would be reported back to a future Board meeting.
DHROD Oct 2018
Action Closed. Minute Ref: 280/18
214/18 Freedom To Speak Up – Board Self-Evaluation Tool
31/07/18
Board agreed to consider the self-evaluation tool and discuss their views at the September Board meeting, with a self-evaluation undertaken at the October meeting.
FTSU Sept 2018
The self-evaluation would be undertaken outside of the meeting and reported to the November meeting. Action Closed.
242/18 Chief Executive Report and Integrated Performance Report
25/09/18
Board requested a more balanced summary be presented as part of future reports, which highlighted not only the areas for improvement, but also those areas where the Trust was performing well.
DSO Oct 2018
Action Closed. Minute Ref 282/18.
242/18 Chief Executive Report and Integrated Performance
25/09/18 DNQ to update the bullet point within the report relating to C.Difficile to provide more explicit
DNQ Oct 2018
Action Closed. Minute Ref 282/18.
TRUST BOARD PART 1 5. 315/18 MATTERS ARISING FRO... Page 17 of 247

Report assurance to the Board.
242/18 Chief Executive Report and Integrated Performance Report
25/09/18
Board members to provide comments on People Strategy and OD Strategy as part of the consultation.
DHROD Oct 2018
Action Closed. Minute Ref 290/18 and 291/18.
242/18 Chief Executive Report and Integrated Performance Report
25/09/18
Board to receive an update on discharge summaries following discussion at QC.
QC Chair Nov 2018
Action Closed. Minute Ref: 280/18.
242/18 Chief Executive Report and Integrated Performance Report
25/09/18
Staff wellbeing initiatives would be re-publicised to help improve responses in the staff survey, and update provided would be reflected within the dashboard.
DHROD Oct 2018
Update provided as part of the communications to staff on this year’s staff survey. Action Closed.
242/18 Chief Executive Report and Integrated Performance Report
25/09/18
CFO to provide a detailed financial report from month 6, for the Board’s continuing oversight of the financial position.
CFO Oct 2018
Action Closed. Minute Ref 282/18.
247/18 iii) Quarterly Report from the Guardian of Safe Working Hours
25/09/18
Report to provide assurance on how junior doctor hours exception reporting links to the risk of gaps in junior doctor rotas, and any potential impact on patient safety. This would be reported to October Board, to provide reassurance the Guardian was provided with assurance that allocation of log ins was in progress.
GSW/ DHROD
Oct 2018
Action Closed. Minute Ref: 280/18
248/18 iv) Annual Report from the Responsible Officer: Revalidation
25/09/18
MD to review the position in relation to outstanding identity checks and report back to the Board.
MD Oct 2018
Action Closed. Minute Ref: 280/18
249/18 vii) Patient Story 25/09/18
MD to follow up with the patient’s Consultant to ensure the patient received the right access to services and level of care in the future.
MD Oct 2018
Action Closed. Minute Ref: 280/18
242/18 Chief Executive Report and Integrated Performance Report
25/09/18
MD would keep the Board apprised of progress in relation to joint work between the Trust and Leeds and Hull in regard to one or two test sites for
MD Oct 2018
Action Closed. Minute Ref: 280/18
TRUST BOARD PART 1 5. 315/18 MATTERS ARISING FRO... Page 18 of 247

some services.
242/18 Chief Executive Report and Integrated Performance Report
25/09/18
DSO to investigate why a suggested pilot of an electronic solution for discharge summaries had not been taken forward, it was understood this was due to the impact on bed flow but further clarification would be provided.
DSO Oct 2018
Action Closed. Minute Ref: 280/18
249/18 vi) Patient Story 25/09/18
MD to investigate the transition of patients with learning difficulties from a legal perspective, in line with the policy.
MD Oct 2018
Action Closed. Minute Ref: 280/18
249/18 ix) Patient Story 25/09/18
DNQ to investigate how patients and families contacted specialist nurse teams and transition teams to ensure there is two way communication for telephone follow up appointments.
DNQ Oct 2018
Action Closed. Minute Ref: 280/18
Actions Scheduled updated following 6 November 2018 Board Meeting held in Public
Action ref:
Date Action raised
Action Action with
Target date to
complete Progress / evidence that
completed
146/18 Aseptic Suite Business Case
23/05/18
A proposal would be brought back a future meeting to consider further, in protecting the Trust from extra costs. An application to the Integrated Care System for any additional capital could be considered.
CFO TBC Completed. Included within prioritised ICS submission.
146/18 Aseptic Suite Business Case
23/05/18
The suite would take up to 18 months to build, and the final business case with final build costs would be brought back to a future Board.
CFO TBC
Finalised design out to tender week commencing 10 September 2018. Tenders are expected back by 5 October 2018.
179/18 v) Well Led Self Assessment 26/06/18
Consideration to be given to a timely Well Led reassessment.
CEO TBC Well Led on September agenda. Date for re-assessment to be agreed.
214/18 Freedom To Speak Up – Board Self-Evaluation Tool
31/07/18 The Board to undertake a self-evaluation at the October meeting.
Chair Oct Nov 2018
This item has been deferred to the November meeting due to a full agenda at the October meeting. Item deferred to December.
TRUST BOARD PART 1 5. 315/18 MATTERS ARISING FRO... Page 19 of 247

233/18 Patient Story 31/07/18
A Board member(s) would be included within the new process / future plans to film patient stories for reporting to Board, as well as for training use.
DNQ Dec 2018
289/18 v) Delivering – “Caring Together”: Quarter 2 Performance Against Corporate Objectives 2018/19
06/11/18
DSO to advise how performance against the Trust’s objectives would be communicated to the Trust to drive up performance. And how relevant sections should be considered by Committees before being reviewed by Board.
DSO Dec 2018
Meeting with communications team and ADs planned to agree plan for cascade of progress with Trust objectives. Meeting with new AD corporate affairs tba to agree process with sub committees. Update to be provided to Board Dec 2018 meeting.
290/18 v) Presentation of the People Strategy
06/11/18
A front facing staff focussed version around the key themes would be developed. Reference to the gender pay gap would be referenced within the chapters. Consideration would be given to a potential role for the shadow board in the next phase of work to develop a cohesive plan and identify timelines for the final strategy.
DHROD Feb 2019
290/18 vi) Presentation of the People Strategy
06/11/18
The strategy would be developed through Committee support, and prioritisation of chapters considered. The completed strategy would be taken to February FRC and February Board.
DHROD Feb 2019
291/18 v) Presentation of the Culture and Behaviour Strategy
06/11/18
The timelines for the final strategy to be identified. The final chapters and programme of activity needed to help achieve this culture within all aspects of the organisation to be developed and taken to the December FRC, and February Board.
DHROD Feb 2019
TRUST BOARD PART 1 5. 315/18 MATTERS ARISING FRO... Page 20 of 247

6. 316/18 CHIEF EXECUTIVE REPORTAND INTEGRATED PERFORMANCEREPORT

REPORT TO THE TRUST BOARD OF DIRECTORS’ MEETING (PART 1) HELD ON 27 NOVEMBER 2018
Chief Executive’s Report and Trust-Wide Integrated Performance Report
Trust Aims Supported by this Paper
Provide high quality patient experience and outcomes Employ motivated and compassionate staff Lead improvements in paediatric care Build clinical and financial sustainability Discover new ways of improving child health through research, innovation and technology
Links to Board Assurance Framework
Failure to effectively deliver healthcare impacts on the safety and quality of patient experience,
regulatory compliance and loss of confidence of the wider community. Risk that we do not maintain financial stability due to failure to deliver the financial plan resulting in
requirements for additional CIPs or reduction in level and standard of services. Failure to ensure that the Trust has a motivated, suitably trained and engaged workforce impacts on
operational performance, transformational change and achievement of strategic objectives. Failure to ensure that the Trust recruits staff in the right numbers and with the appropriate breadth of
skills and competencies to deliver high quality services now and in the future. Risk that insufficient leadership capacity and capability prevents necessary transformational change. Risk to clinical service viability due to failure to meet nationally defined standards or unfavourable
changes to the commissioning of services. Failure to engage effectively with partner organisations and the local community threatens the ability of
the Trust to deliver its strategic ambition. Failure to engage with our clinicians prevents the development / implementation of an effective clinical
strategy that responds to the needs of patients and other health and social care partners. Failure to ensure that the required IT infrastructure and strategy is in place to deliver clinical services
and support clinical strategy and transformation impacts on the Trust's ability to deliver services, improve quality and transform services.
Capacity constraints impact on our ability to deliver planned activity and manage demand impacting on operational efficiency, service quality and financial performance.
Purpose of the Paper To present to the Trust Board an integrated overview of performance within the Trust. This provides a summarised description of the Trust’s most recent performance against key national and local performance indicators at the end of October 2018.
Summary of Key Points The Integrated Performance Report (including quality, activity, workforce and performance) including a high level dashboard is structured around the organisation’s five strategic aims. Comments are welcome on this report to ensure that it can be developed to maximise its usefulness.
TRUST BOARD PART 1 6. 316/18 CHIEF EXECUTIVE REP... Page 22 of 247

It is recommended to: Note the current performance against the Trust’s strategic and corporate objectives. Note the actions being taken to address performance areas.
All data relates to October 2018 unless otherwise specified (e.g. cancer KPI’s and sickness absence which are reported one month in arrears). Key Achievements The Trust achieved 100% on all Cancer standards throughout September 2018. The Trust has continued to achieve the ED Waiting Time standard, with 97% of patients being seen
within four hours. The Trust achieved the 92% target for patients on an incomplete pathway within 18-weeks. This is an
improving position on the previous month and the target was also achieved at Divisional level. The Trust achieved the Diagnostic standard, with 99% of patients receiving their procedure within six
weeks of referral. For the sixth consecutive month, there were no patients whose admission was cancelled on the day for
non-clinical reasons which subsequently did not have their procedure booked within 28 days. The patient Friends and Family response rate during October exceeded the Trust target for the second
consecutive month. Outpatient clinic utilisation improved for the second consecutive month. Areas for Improvement 81 Policies are currently out of date. Divisions are required to review and update these as a high
priority. Sickness absence is higher than the Trust’s target limit of 4%. Both PDR and Mandatory Training compliance remained below target (75% and 85% respectively).
Trust Board Action Required The Board is asked to note the briefing which provides context and updates the Board on key activities during the last month and presents an overview of performance within the Trust.
Author: Mr C Radford Deputy Director of Strategy and Operations
TO NOTE
Executive Sponsor: Ms R Brown Executive Director of Strategy and Operations
TRUST BOARD PART 1 6. 316/18 CHIEF EXECUTIVE REP... Page 23 of 247

Integrated Performance Report
Reporting Period: October 2018
TRUST BOARD PART 1 6. 316/18 CHIEF EXECUTIVE REPORT AND IN... Page 24 of 247

Contents 2
Section Title Page Number
1.1 Executive Summary 3
1.2 Executive Summary – Continued 4
2.0 High Level Dashboard 5
3.0 Legal & Governance KPIs 6
4.0 Friends & Family KPIs 7
5.0 Safety & Patient Experience Indicators 8
6.0 Discharge Summaries 9
7.0 Workforce - Sickness Absence & Training KPIs 10
8.0 Accident & Emergency and Ambulance Handovers 11
9.0 Referral to Treatment (18 Weeks) 12
10.0 Diagnostics (DM01) & Long Stay Inpatients 13
11.0 CAMHS Waiting Times 14
12.0 Cancer Waits 15
13.0 eReferrals Appointment Slot Issues 16
14.0 Outpatient Clinic WNB (Was Not Brought – Previously DNA) 17
15.0 Outpatient Review List 18
16.0 Outpatient Clinic & Theatres Utilisation 19
17.0 Activity v Plan: Outpatients and Inpatients 20
18.1 Finance – Agency Spend & Cash Balance 21
18.2 Finance – Income and Expenditure & CIP 22
19.0 20.0
CQUIN Integrated Care System Dashboard
23 24
TRUST BOARD PART 1 6. 316/18 CHIEF EXECUTIVE REPORT AND IN... Page 25 of 247

1.1 Executive Summary 3
Provide high quality patient experience and outcomes:
• There were no C.Diff, MRSA , MSSA Bacteraemia cases during October and no never events. • There was one serious incident during October. A clinical review has taken place and a report has been provided to the CCG. • The number of incidents reported during October increased. This is however, likely due to better reporting processes following the implementation of Datix. • The number of investigations pending review continues to reduce as the backlog from Datix is addressed. • The percentage of complaints responded to within the deadline improved during October. A review of complaint handling processes is ongoing. • There are currently 50 clinical guidelines and 81 policies currently out of date (9.3% and 44.3% respectively). • The patient Friends and Family response rate during October exceeded the Trust target for the second consecutive month following ongoing work to increase
engagement from service users and their families. • Progress to achieve the target for discharge summaries continues to be below target. A pilot to improve and change processes is being considered.
Empower motivated and compassionate staff:
• Sickness absence was 4.24% during September (target reported one month in arrears). This is a 0.27% increase on the previous month, but subject to further validation.
• PDR compliance was 75% during October (15% below target). • Mandatory Training compliance remained static at 85% during October (5% below target).
Lead improvements in paediatric care:
• The elective workstream of the ACP has agreed to work within the Trust on the ‘Was Not Brought’ campaign to be launched in the new year. • A further meeting between Leeds and SCH clinical teams on the provision of oncology and haematology services occurred in month to continue to build on working
relations between the two Trusts.
TRUST BOARD PART 1 6. 316/18 CHIEF EXECUTIVE REPORT AND IN... Page 26 of 247

1.2 Executive Summary – Continued 4
Build clinical and financial sustainability:
• The four-hour ED standard continued to be achieved at 96.54% throughout October against the 95% national target. • The percentage of ambulance handovers within thirty minutes continued to be achieved at 100%. • The percentage of patients on an 18-week RTT incomplete pathway was achieved at Trust-level at 93.39% against the national standard of 92%. The standard was
also achieved at Divisional level. • There continued to be no patients waiting more than 52 weeks for treatment. • During the month 23 patients had their operation cancelled on the day for non-clinical reasons. All of these were subsequently admitted within 28-days. • The diagnostic target was achieved with 99.50% of patients waiting less than six weeks for their test against the national target of 99%. • All national cancer targets continued to be achieved at 100% for the month of September (note, reporting is always one month in arrears). • Outpatient clinic utilisation increased during October for the second consecutive month across both first and follow-up appointments. • Outpatient Was Not Brought (previously DNA) rates were higher than target across both first and follow-up. This is however, an improving trend over the last two
months. • Freedom of Information backlog clearance started in September. The backlog is expected to be complete by the end of quarter three. New requests are now being
acknowledged within three days of receipt and processed within the twenty-day deadline, subject to the timely information provided by departments. • Of the five waiting time standards relating to mental health, four of these were achieved. Waiting times for CAMHS has been highlighted within recent CQC reports
and a review of waiting time, lists and process is underway. This will be joint work with commissioners to enable any revisions to be included in next year’s contract
Discover new ways of improving child health:
• A total of 22 Audits / Service Evaluations were initiated during the month of October. • There are currently 14 active Microsystem Improvement Projects ongoing within the Trust. • Health Education England have recently confirmed 100% funding for a future leader fellow (Doctor ST3+/ Band 6 Nurse/AHP level) for 1 year to work on Enhanced
Recovery within Well Prepared Programme
TRUST BOARD PART 1 6. 316/18 CHIEF EXECUTIVE REPORT AND IN... Page 27 of 247

2.0 High Level Dashboard 5
Organisational Aim Indicator Target Target Aim Mar-18 Apr-18 May-18 Jun-18 Jul-18 Aug-18 Sep-18 Oct-18 Nov-18 Dec-18 Jan-19 Feb-19 Mar-19
Number of Incidents Reported N/A N/A 527 586 490 515 537 393 321 439
Number of Serious Incidents Reported 0 Below 1 0 2 1 0 4 1 1
Number of Never Events Reported 0 Below 0 0 0 1 0 1 0 0
Number of Incidents Pending Investigation that are Overdue 0 Below 527 382
Number of Actions Outstanding from Serious Incident/Never Event Action Plans N/A N/A 13 7 10 23
Number of Complaints Received N/A N/A 16 20 12 25 17 19 29 20
Complaints Responded Within Deadline N/A N/A 9 7 6 13 4 2 4 7
Percentage of Complaints Responded Within Deadline 100.00% Above 35.00% 35.29% 81.25% 14.29% 15.38% 30.77% 36.84%
Number of Claims/Inquests Registered N/A N/A 4 0 0 6
Number of Freedom to Speak Up Concerns Raised N/A N/A 1 3 15 6 9 2 6 5
Response Rate in the Friends and Family Test 7.57% Above 3.09% 4.02% 2.81% 4.87% 6.00% 6.62% 8.11% 9.27%
Percentage of Recommendations in the Friends and Family Test 92.10% Above 85.14% 85.36% 85.15% 83.07% 79.06% 82.27% 83.84% 83.38%
Percentage of staff who recommend this organisation to friends / family if they needed care or treatment N/A N/A 89.08% - - 89.00% - - 89.93% - - - - -
Number of C.Diff Cases 2 Below 0 1 2 0 1 1 0 0
Number of MRSA Cases 0 Below 0 0 0 0 0 0 0 0
Number of MSSA Bacteraemia Cases N/A N/A 1 1 1 0 1 1 2 0
Number of Clinical Guidelines Out of Date 0 Below 35 45 44 43 45 52 45 50
Number of Policies Out of Date 0 Below 82 81
Number of patients with an inpatient length of stay over 30 days (Acute & Tier 4 CAMHS) N/A N/A 36 36 42 33 34 35 28 36
Percentage of Discharge Summaries Complete (inc CAMHS Brief) 100.00% Above 80.10% 75.59% 76.59% 73.90% 76.78% 80.00% 72.52% 69.84%
Percentage of Discharge Summaries Completed Within 24 Hours of Discharge Date (inc CAMHS Brief) 100.00% Above 75.37% 69.76% 71.59% 69.72% 69.59% 74.52% 68.60% 67.34%
Percentage of Full Discharge Summaries Complete (CAMHS only) 100.00% Above 62.50% 75.00% 100.00% 100.00% 100.00% 100.00% 100.00% 100.00%
Percentage of Full Discharge Summaries Complete Within 2 weeks (CAMHS only) 100.00% Above 25.00% 37.50% 100.00% 33.33% 66.67% 27.27% 66.67% 33.33%
Outpatient Appointment Letters Sent Within 10 Days N/A N/A
Outpatient Letter Typing Turnaround N/A N/A
Sickness Absence (percentage of time lost) 4.00% Below 3.97% 3.74% 3.16% 3.38% 3.93% 3.97% 4.24%
PDR Compliance 90.00% Above 82.00% 80.00% 79.00% 75.00% 76.00% 76.00% 76.00% 75.00%
Mandatory Training Compliance 90.00% Above 88.00% 88.00% 87.00% 85.00% 85.00% 86.00% 85.00% 85.00%
Retention of Staff N/A N/A - - - 88.50% 88.39% 88.05% 88.73% 88.75%
Number of Excellence Reports Submitted N/A N/A - - - - 27 28 25 24
Staff engagement as measured by the Staff Survey (Organisation Average) N/A N/A 3.82 - - - - - - - - - - -
Percentage Increase in staff feeling valued as measured by the Staff Survey N/A N/A - - - - - - - - - - -
Percentage of staff who recommend this organisation to friends / family as a place to work N/A N/A 60.82% - - 63.00% - - 62.70% - - - - -
A&E 4+ Hour Waits 95.00% Above 97.31% 97.70% 98.47% 98.35% 98.56% 98.60% 96.63% 96.54%
Percentage of Ambulance Handovers Within 30 Minutes 100.00% Above 99.25% 100.00% 100.00% 100.00% 100.00% 100.00% 100.00% 100.00%
18 Weeks RTT (Referral to Treatment) Time - Incomplete 92.00% Above 93.01% 93.81% 93.86% 93.37% 93.07% 92.67% 92.03% 93.39%
18 Weeks RTT (Referral to Treatment) Number of Patients Waiting 52+ Weeks - Incomplete 0 Below 0 0 0 0 0 0 0 0
Diagnostic Waits (DM01) Within 6 Weeks 99.00% Above 99.52% 99.75% 99.67% 99.42% 99.68% 99.58% 99.48% 99.50%
CAMHS Tier 3 Waiting Times (Wait to 1st Appt) - 18 Weeks 92.00% Above 96.31% 97.05% 97.36% 99.35% 97.85% 96.15% 99.39% 96.67%
CAMHS Tier 3 Waiting Times (Wait to 2nd Appt) - 18 Weeks 92.00% Above 59.64% 54.94% 55.94% 57.64% 62.12% 61.42% 65.69% 65.37%
Eating Disorder Routine Patients - 28 Days (Incomplete) 92.00% Above 80.00% 50.00% 100.00% 100.00% 100.00% 33.33% 100.00% 100.00%
Eating Disorder Urgent Patients - 7 Days (Incomplete) 92.00% Above N/A N/A N/A N/A N/A N/A N/A N/A
Early Intervention for Psychosis (EIP) - 14 Days (Incomplete) 92.00% Above N/A N/A N/A N/A N/A N/A 100.00% 100.00%
2 Week Wait from GP Referral to 1st Outpatient Appointment (All Cancers) 93.00% Above 100.00% 100.00% 100.00% 100.00% 100.00% 100.00% 100.00%
31 Day Wait from Diagnosis to 1st Definitive Treatment (All Cancers) 96.00% Above 100.00% 100.00% 100.00% 100.00% 100.00% 100.00% 100.00%
31 Day Wait for Subsequent Treatment where Treatment is Surgery 94.00% Above 100.00% 100.00% 100.00% 100.00% 100.00% 100.00% N/A
31 Day Wait for Subsequent Treatment where Treatment is an Anti-Cancer Drug Regime 98.00% Above 100.00% 100.00% 100.00% 100.00% 100.00% 100.00% 100.00%
Cancelled Elective Operations (on the day for non-clinical reasons by the hospital) - Patients Not Offered TCI Within 28 Days 0 Below 4 1 0 0 0 0 0 0
Number of Urgent Operations Cancelled for the 2nd or More Time 0 Below 0 0 0 0 0 0 1 0
Mixed Sex Accommodation Breaches (patients over 16 years) 0 Below 0 0 0 0 0 0 0 0
eReferral Utilisation (Percentage booked through eReferrals) N/A N/A 56.69% 72.84% 93.57% 97.49% 97.51% 96.71% 96.10% 100.00%
eReferral Appointment Slot Issues per eRS Booking (ASI Ratio) N/A N/A 0.20 0.06 0.12 0.15 0.18 0.13 0.24 0.17
WNB (Was Not Brought - previously DNA) Rate (New) 9.00% Below 9.45% 11.14% 10.43% 9.71% 12.14% 12.34% 11.28% 9.45%
WNB (Was Not Brought - previously DNA) Rate (Follow Up) 11.00% Below 12.43% 12.68% 13.23% 11.80% 12.85% 13.12% 12.17% 11.47%
Outpatient Clinic Utilisation - Acute 80.00% Above 74.45% 78.69% 78.02% 80.22% 76.97% 76.52% 78.55% 79.97%
Theatres Utilisation 85.00% Above 86.54% 83.49% 85.24% 85.36% 83.16% 87.35% 83.50% 84.79%
Contract - % Variance from Plan - A&E 0.00% Above -12.24% -5.82% 2.78% 4.47% 5.72% -5.94% 1.36% 2.71%
Contract - % Variance from Plan - Oupatient Attendances 0.00% Above -10.61% -3.22% 8.33% 2.99% 1.07% -15.66% 4.74% -1.24%
Contract - % Variance from Plan - Elective Inpatient Spells 0.00% Above -24.03% -7.72% 4.92% 0.36% -9.02% -8.96% -1.43% -17.28%
Contract - % Variance from Plan - Non-Elective Inpatient Spells 0.00% Above -9.72% -13.29% -18.47% -12.52% -18.19% -14.98% -6.71% -2.60%
Agency spend (£'000) N/A N/A 416 129 111 189 145 126 142
Income & Expenditure in month position (against control total) £'000 ((surplus)/deficit)) N/A N/A 1242 -209 -59 -202 -92 559 -90
Income & Expenditure cumulative position (against control total) £'000 ((surplus)/deficit)) N/A N/A 434 -209 -268 -470 -562 -3 -93
£ Delivery of CIP (£'000) N/A N/A 680 0 92 129 300 640 358
Percentage Delivery of CIP (against YTD profiled plan) 100.00% Above 56.60% 0.00% 40.26% 39.15% 80.12% 146.48% 81.98%
Cash Balance (£'000) N/A N/A 20955 17765 16188 15402 17711 17419 16493
Number of FOIs outstanding at the end of the month that are overdue 0 Below - 0 41 83 88 92 93 100
Percentage of FOIs outstanding at the end of the month that are overdue 0.00% Below - 0.00% 47.13% 70.34% 67.69% 74.80% 80.17% 86.21%
Number of Active Microsystem Projects N/A N/A 0 0 0 0 0 0 0 14
Increase in clinical research N/A N/A
Audits / Service Evaluations Inititated N/A N/A 23 28 32 33 22 13 19 22
Key:
Green Achievement - performance is in line with the identified target
Red Non-achievement - performance is below the required standard
Metrics highlighted in grey denote that data is intended for inclusion at a future date 0 Data has been provided, with zero actual, therefore performance is 0.
RAG Data Notes
Blank data Data is not available/has not been provided yet.
N/A Data has been provided, the denominator is zero, therefore percentage cannot be calculated.
Discover new ways of
improving child health
through research
Empower motivated
and compassionate
staff
Provide high quality
patient experience and
outcomes
Build clinical and
financial sustainability
TRUST BOARD PART 1 6. 316/18 CHIEF EXECUTIVE REPORT AND IN... Page 28 of 247

Incidents
Note: Managers have 21 days following the incident being reported to complete investigations. The figures shown in the chart above are the amount of incidents pending investigation that are classed as overdue at the end of the reporting period.
Lead: Sally Shearer Timescale: Monthly
Key Issues: • The overall amount of incidents pending investigation which are overdue is reducing
due to targeted work within the divisions. • During October there have been two new claims and four new inquests. • One serious incident occurred during October. A clinical review has taken place and a
report provided to commissioners.
Key Actions: • Surgery and Critical Care are reviewing outstanding actions from serious incidents at
the Division’s Quality Meeting in November. • Details of out of date policies and guidelines is provided to Divisions on a monthly
basis for review and action at the Divisional Quality Meetings.
3.0 Legal & Governance KPIs
Complaints
Policies & Guidelines
6
Apr-18 May-18 Jun-18 Jul-18 Aug-18 Sep-18 Oct-18 Nov-18 Dec-18 Jan-19 Feb-19 Mar-19Number of Incidents Reported 586 490 515 537 393 321 439 Of which are… No of Serious Incidents 0 2 1 0 4 1 1 Of which are… Never Events 0 0 1 0 1 0 0
Apr May Jun Jul Aug Sep Oct Nov Dec Jan Feb Mar
Trust Total 0 0 0 0 0 527 382 0 0 0 0 0
Target 0 0 0 0 0 0 0 0 0 0 0 0
Previous Year 0 0 0 0 0 0 0 0 0 0 0 0
0
100
200
300
400
500
600
Number of Incidents Pending Investigation that are Overdue - 2018/19
Apr-18 May-18 Jun-18 Jul-18 Aug-18 Sep-18 Oct-18 Nov-18 Dec-18 Jan-19 Feb-19 Mar-19
Number of Clinical Guidelines Out of Date 45 44 43 45 52 45 50
Number of Policies Out of Date 82 81
Apr May Jun Jul Aug Sep Oct Nov Dec Jan Feb Mar
Trust Total 35.0% 35.3% 81.3% 14.3% 15.4% 30.8% 36.8%
Target 100% 100% 100% 100% 100% 100% 100% 100% 100% 100% 100% 100%
Previous Year
0.00%
10.00%
20.00%
30.00%
40.00%
50.00%
60.00%
70.00%
80.00%
90.00%
100.00%
Percentage of Complaints Responded Within Deadline - 2018/19
Apr May Jun Jul Aug Sep Oct Nov Dec Jan Feb Mar
% of Clinical Guidelines Out of Date 8.8% 8.4% 8.2% 8.7% 9.8% 8.4% 9.3%
% of Policies Out of Date 44.3% 44.3%
Target 0% 0% 0% 0% 0% 0% 0% 0% 0% 0% 0% 0%
0.00%
5.00%
10.00%
15.00%
20.00%
25.00%
30.00%
35.00%
40.00%
45.00%
50.00%
Percentage of Clinical Guidelines and Policies Out of Date - 2018/19
TRUST BOARD PART 1 6. 316/18 CHIEF EXECUTIVE REPORT AND IN... Page 29 of 247

Friends & Family Test – Response Rate
Note: the target line shown above is based on the national average for the previous financial year.
Lead: Sally Shearer Timescale: Monthly
Key Issues: • The patient Friends and Family response rate during October exceeded the
Trust target for the second consecutive month. • All areas across the Trust have seen an increase in responses. This is due to
ongoing work to engage with service users and families through the use of cards, bedhead TV system and staff promoting FFT as a method to feedback.
Key Actions: • The Trust continues to work on a set of actions to improve uptake across all
areas with outpatients as a priority. • The Friends and Family Netcall module has continued to see an increase in
response rates within ED during October.
4.0 Friends & Family KPIs
Friends & Family Test – Percentage Recommended
Note: the target line shown above is based on the national average for the previous financial year.
Staff Friends & Family Test – Q2 2018/19
The table below shows the latest quarterly information for the staff friends & family return: Notes: 1. Staff FFT data is reported on a quarterly basis. 2. Percentages for Recommended and Not Recommended may not equal 100%. This is due to neutral responses being selected (these include ‘Neither likely nor unlikely’ and ‘Don't know’).
7
Apr May Jun Jul Aug Sep Oct Nov Dec Jan Feb Mar
Current Year 85.4% 85.2% 83.1% 79.1% 82.3% 83.8% 83.4%
Previous Year 94.1% 96.9% 94.7% 94.5% 88.2% 90.4% 87.9% 90.8% 86.3% 87.0% 87.9% 85.1%
Target 92.1% 92.1% 92.1% 92.1% 92.1% 92.1% 92.1% 92.1% 92.1% 92.1% 92.1% 92.1%
0.0%
10.0%
20.0%
30.0%
40.0%
50.0%
60.0%
70.0%
80.0%
90.0%
100.0%
Percentage Recommended
Apr May Jun Jul Aug Sep Oct Nov Dec Jan Feb Mar
Current Year 4.0% 2.8% 4.9% 6.0% 6.6% 8.1% 9.3%
Previous Year 2.2% 1.3% 2.0% 1.9% 2.1% 1.8% 2.0% 2.3% 2.1% 2.0% 3.6% 3.1%
Target 7.6% 7.6% 7.6% 7.6% 7.6% 7.6% 7.6% 7.6% 7.6% 7.6% 7.6% 7.6%
0.0%
1.0%
2.0%
3.0%
4.0%
5.0%
6.0%
7.0%
8.0%
9.0%
10.0%
Response Rate
RecommendNot
RecommendRecommend
Not
Recommend
How likely are you to recommend this organisation to friends and
family if they needed care or treatment991 25 90% 2%
How likely are you to recommend this organisation to friends and
family as a place to work691 175 63% 16%
Volume %
TRUST BOARD PART 1 6. 316/18 CHIEF EXECUTIVE REPORT AND IN... Page 30 of 247

Patient Experience – Mixed Sex Accommodation
Lead: Sally Shearer Timescale: Monthly
Key Issues: N/A
Key Actions: N/A
Patient Experience – Cancelled Operations
Lead: Ruth Brown Timescale: Monthly
Key Issues: • There were 23 elective operations
cancelled on the day for non-clinical reasons during October.
• All of these were subsequently accommodated within the 28-day standard.
Key Actions: N/A
Patient Safety – Infection Control
Note: Number of C.Diff Cases Per Month are trust attributable cases where there has been a lapse in care and the target of 2 is for the whole year.
Lead: Sally Shearer Timescale: Monthly
Key Issues: • There were no Infection Control issues experienced during October.
Key Actions: N/A
5.0 Safety & Patient Experience Indicators 8
Area Indicator Data Period Target Aim Actual YTD Last 6 Months Trend
Cancelled Operations
Cancelled Elective Operations (on the day for non-
clinical reasons by the hospital) - Patients Not
Offered TCI Within 28 Days
October 0 Below 0 1Area Indicator Data Period Target Aim Actual YTD Last 6 Months Trend
C.Difficile Infection Number of C.Diff Cases October 2 Below 0 5
MRSA Bacteraemia Number of MRSA Cases October 0 Below 0 0
MRSA Screening High Risk Elective Patients - Percentage Screened October 100.00% Above 100.00% 100.00%
MSSA Bacteraemia Number of MSSA Bacteraemia Cases October N/A N/A 0 6
Mixed Sex
Accommodaton Breaches
Mixed Sex Accommodation Breaches (patients
over 16 years)October 0 Below 0 0
Area Indicator Data Period Target Aim Actual YTD Last 6 Months Trend
TRUST BOARD PART 1 6. 316/18 CHIEF EXECUTIVE REPORT AND IN... Page 31 of 247

Acute & Brief CWAMH Discharge Summaries (completed within 24 hours)
Note: data reported prior to September 2018 for discharge summaries did not take into
account the "Ready to Send" field. A discharge summary is not sent until this field is set to
"Yes", therefore the discharge summary process is not complete until this has happened. This
has now been factored in so there may be a drop in performance shown in the above chart if
comparing back to previous reports (prior to September 2018).
Lead: Ruth Brown Timescale: Monthly
Key Issues: • The completion of discharge summaries remains below target and deteriorated during
September.
Key Actions: • Divisions have action plans in place to address discharge summary completion. • A data cleansing exercise is currently underway. • A junior doctor has been allocated within Medicine to lead on discharge summaries. • Standard templates are currently being developed to enable discharge summaries to
be completed more quickly and easily. • IT are reviewing links from the Bluespier system to pre-populate discharge summaries
as much as possible. • The Medical Director has sent a communication highlighting the importance of
sustaining discharge summaries across the trust.
CWAMH Discharge Summaries – Full (completed within 2 Weeks)
Note: data reported prior to September 2018 for discharge summaries did not take into
account the "Ready to Send" field. A discharge summary is not sent until this field is set to
"Yes", therefore the discharge summary process is not complete until this has happened. This
has now been factored in so there may be a drop in performance shown in the above chart if
comparing back to previous reports (prior to September 2018).
6.0 Discharge Summaries 9
Apr May Jun Jul Aug Sep Oct Nov Dec Jan Feb Mar
Completed 75.6% 76.6% 73.9% 76.8% 80.0% 72.5% 69.8% 0.0% 0.0% 0.0% 0.0% 0.0%
Completed Within 24 Hrs 69.8% 71.6% 69.7% 69.6% 74.5% 68.6% 67.3% 0.0% 0.0% 0.0% 0.0% 0.0%
Prev Yr - Completed 80.3% 82.5% 76.9% 78.0% 80.5% 79.4% 77.6% 83.2% 83.1% 80.9% 81.6% 80.1%
Prev Yr - Completed Within 24 Hrs 70.5% 75.4% 73.3% 72.8% 76.7% 73.7% 72.3% 76.7% 74.0% 76.0% 74.1% 75.4%
Target 100% 100% 100% 100% 100% 100% 100% 100% 100% 100% 100% 100%
0.0%
20.0%
40.0%
60.0%
80.0%
100.0%
Trust Total
Percentage of Discharge Summaries Completed (and within 24 Hours of Discharge Date) - 2018/19
Apr May Jun Jul Aug Sep Oct Nov Dec Jan Feb Mar
Completed 75.0% 100.0% 100.0% 100.0% 100.0% 100.0% 100.0% 0.0% 0.0% 0.0% 0.0% 0.0%
Completed Within 2 Wks 37.5% 100.0% 33.3% 66.7% 27.3% 66.7% 33.3% 0.0% 0.0% 0.0% 0.0% 0.0%
Prev Yr - Completed 100.0% 100.0% 100.0% 100.0% 100.0% 100.0% 100.0% 100.0% 100.0% 100.0% 100.0% 62.5%
Prev Yr - Completed Within 2 Wks 14.3% 0.0% 0.0% 11.1% 0.0% 12.5% 0.0% 50.0% 50.0% 33.3% 50.0% 25.0%
Target 100% 100% 100% 100% 100% 100% 100% 100% 100% 100% 100% 100%
0.0%
20.0%
40.0%
60.0%
80.0%
100.0%
CWAMH
Percentage of Full Discharge Summaries Completed (and within 2 weeks of Discharge Date) - 2018/19
Lead: Ruth Brown Timescale: Monthly
Key Issues: • The completion rate for discharge summaries within the CWAMH Division remained at
100% for the sixth consecutive month. • Completion within two weeks deteriorated, however, the overall patient numbers are
low which therefore has a higher impact as a percentage.
Key Actions: N/A
TRUST BOARD PART 1 6. 316/18 CHIEF EXECUTIVE REPORT AND IN... Page 32 of 247

Sickness Absence Levels – All Staff (% of Time Lost)
Please note: Sickness reporting runs a month in arrears.
Lead: Steve Ned Timescale: Monthly
Key Issues:
• Sickness absence in terms of time lost during September was 4.24% which is a 0.27% increase on the previous month.
• PDR compliance during October was 75% against the 90% Trust target. • Mandatory training compliance during October remained static on the
previous month at 85%.
Key Actions:
• Workforce KPIs continue to be monitored as part of the Monthly Performance and Quality Review Meetings for clinical divisions and these will be extended to corporate areas shortly.
7.0 Workforce - Sickness Absence & Training KPIs
PDR Compliance – All Staff
Mandatory Training Compliance – All Staff
10
Apr May Jun Jul Aug Sep Oct Nov Dec Jan Feb Mar
Trust Total 3.74% 3.16% 3.38% 3.93% 3.97% 4.24%
Target 4.00% 4.00% 4.00% 4.00% 4.00% 4.00% 4.00% 4.00% 4.00% 4.00% 4.00% 4.00%
Previous Year 4.68% 4.92% 4.85% 4.80% 4.75% 4.59% 5.18% 4.65% 4.80% 4.73% 4.21% 3.97%
0.00%
1.00%
2.00%
3.00%
4.00%
5.00%
6.00%
Sickness Absence - 2018/19
Apr May Jun Jul Aug Sep Oct Nov Dec Jan Feb Mar
Trust Total 80.00% 79.00% 75.00% 76.00% 76.00% 76.00% 75.00%
Target 90.00% 90.00% 90.00% 90.00% 90.00% 90.00% 90.00% 90.00% 90.00% 90.00% 90.00% 90.00%
Previous Year 71.00% 67.00% 67.00% 69.00% 71.00% 75.00% 79.00% 80.00% 80.00% 79.00% 77.00% 82.00%
0.00%
10.00%
20.00%
30.00%
40.00%
50.00%
60.00%
70.00%
80.00%
90.00%
100.00%
PDR Compliance - 2018/19
Apr May Jun Jul Aug Sep Oct Nov Dec Jan Feb Mar
Trust Total 88.00% 87.00% 85.00% 85.00% 86.00% 85.00% 85.00%
Target 90.00% 90.00% 90.00% 90.00% 90.00% 90.00% 90.00% 90.00% 90.00% 90.00% 90.00% 90.00%
Previous Year 85.00% 85.00% 84.00% 85.00% 86.00% 86.00% 86.00% 87.00% 88.00% 88.00% 88.00% 88.00%
0.00%
10.00%
20.00%
30.00%
40.00%
50.00%
60.00%
70.00%
80.00%
90.00%
100.00%
Mandatory Training Compliance - 2018/19
TRUST BOARD PART 1 6. 316/18 CHIEF EXECUTIVE REPORT AND IN... Page 33 of 247

Activity Performance - A&E Attendances
A&E Quality Indicators & Ambulance Handovers
8.0 Accident & Emergency and Ambulance Handovers
A&E 4 Hour Waits (95% of Patients Seen & Discharged/Admitted Within 4 Hours)
Lead: Ruth Brown Timescale: Monthly
Key Issues: • Performance within ED continues to exceed the national standard of 95% of
patients being seen and discharged or admitted within four hours. • ED Unplanned re-admission rates remain higher than the national target of 5%
(this is for both adults and children). However, audits indicate that this is not as a result of poor patient outcomes.
Key Actions: N/A
11
75.00%
80.00%
85.00%
90.00%
95.00%
100.00%
Ap
r
Ma
y
Jun
Jul
Au
g
Sep
Oct
No
v
De
c
Jan
Feb
Ma
r
A&E 4 Hour Waits Performance2018/19
% Waiting under 4 Hours Target Previous Year
Area Indicator Data Period Target Aim Actual YTD Last 6 Months Trend
A&E 4+ Hour Waits October 95% Above 96.54% 97.81%
A&E Time to Initial Assessment for Patients
Arriving by Ambulance (95th Percentile)October 00:15:00 Below 00:13:00 00:12:00
A&E Median Time to Treatment October 01:00:00 Below 00:38:00 00:35:00
A&E Unplanned Reattendance Rate October 5% Below 8.16% 8.16%
A&E Left Without Being Seen October 5% Below 0.98% 1.14%
Percentage of Ambulance Handovers Within 15
MinutesOctober 100% Above 100.00% 97.48%
Percentage of Ambulance Handovers Within 30
MinutesOctober 100% Above 100.00% 100.00%
Number of Ambulance Handover Times Between
30 & 60 MinutesOctober 0 Below 0 0
Number of Ambulance Handover Times Over 60
MinutesOctober 0 Below 0 0
Accident and
Emergency
Ambulatory
0
1000
2000
3000
4000
5000
6000
Ap
r-1
8
Ma
y-1
8
Jun
-18
Jul-
18
Au
g-1
8
Sep
-18
Oct
-18
No
v-1
8
De
c-18
Jan
-19
Feb
-19
Ma
r-19
Act
ivit
y
Apr-18 May-18 Jun-18 Jul-18 Aug-18 Sep-18 Oct-18 Nov-18 Dec-18 Jan-19 Feb-19 Mar-19
Actual 4477 5095 4960 4927 3363 4567 5206 0 0 0 0 0
Plan 4754 4957 4748 4660 3575 4506 5069 0 0 0 0 0
Previous Year 4546 4983 4728 4790 3617 4610 5409 0 0 0 0 0
Variance From Plan -5.8% 2.8% 4.5% 5.7% -5.9% 1.4% 2.7% 0.0% 0.0% 0.0% 0.0% 0.0%
A&E Attendances
TRUST BOARD PART 1 6. 316/18 CHIEF EXECUTIVE REPORT AND IN... Page 34 of 247

9.0 Referral to Treatment (18 Weeks)
RTT Incomplete Performance (92% of Patients Waiting Under 18 Weeks For Treatment)
Lead: Ruth Brown Timescale: Monthly
Key Issues: • Overall Trust performance continued to remain above the 92% target during
October. • The standard was also achieved at Divisional level. • There are no patients on an incomplete pathway exceeding 52 weeks.
Key Actions: • Long-wait patients continue to be reviewed, discussed and actively managed
at weekly Divisional PTL Meetings. • Additional meetings are being held to undertake a more comprehensive
review of specific services which are currently not achieving the standard.
RTT Incomplete Performance by Division
Number of Patients On Incomplete Pathways Over 52 Weeks
Underperforming Specialties Ranked by Margin (Volume)
12
Month Apr-18 May-18 Jun-18 Jul-18 Aug-18 Sep-18 Oct-18 Nov-18 Dec-18 Jan-19 Feb-19 Mar-19
52+ Weeks 0 0 0 0 0 0 0
Month Apr-18 May-18 Jun-18 Jul-18 Aug-18 Sep-18 Oct-18 Nov-18 Dec-18 Jan-19 Feb-19 Mar-19
MED 95.20% 94.82% 94.19% 93.68% 93.50% 92.58% 94.03%
S&CC 92.37% 92.76% 92.28% 92.17% 91.45% 90.83% 92.21%
PDG 94.49% 94.71% 94.99% 94.48% 94.35% 94.58% 95.44%
Trust Total 93.81% 93.86% 93.37% 93.07% 92.67% 92.03% 93.39%
86.00%
88.00%
90.00%
92.00%
94.00%
96.00%
98.00%
100.00%
Oct
-17
No
v-1
7
Dec
-17
Jan-
18
Feb
-18
Mar
-18
Ap
r-18
May
-18
Jun
-18
Jul-
18
Au
g-18
Sep
-18
Oct
-18
Trust Total Incomplete Performance October 2017 - October 2018
Trust Total MEDicine S&CC PDG Target
Division Local Specialty Performance %Excess Breaches (over
the 8% allowance)
MEDicine Neuro-Disability 80.38% 49
Surgery & Critical Care Paediatric Dentistry 71.67% 25
MEDicine Sleep Clinic 85.95% 12
MEDicine Respiratory 89.24% 5
Surgery & Critical Care Trauma & Orthopaedics 91.54% 4
Surgery & Critical Care Pain Clinic 88.73% 3
Surgery & Critical Care Plastic Surgery 90.24% 3
Surgery & Critical Care Ophthalmology 91.54% 2
Surgery & Critical Care Exodontia 91.20% 1
Surgery & Critical Care OMFS 91.94% 1
Surgery & Critical Care Scoliosis 91.86% 1
TRUST BOARD PART 1 6. 316/18 CHIEF EXECUTIVE REPORT AND IN... Page 35 of 247

Long Stay Inpatients (Number of Acute and CAMHS Inpatients with Length of Stay of 30+ Days (as at the end of the month))
Lead: Jeff Perring Timescale: Monthly
Key Issues: • Work is currently being undertaken to further understand Length of Stay
across the Trust, with a particular focus on patients over 30 days. This work is likely to be on-going until the end of the year.
Key Actions: • Length of Stay information is now routinely circulated to bed-holding Divisions
to ensure that a co-ordinating consultant is in place, along with a care plan and estimated date of discharge (where possible).
10.0 Diagnostics (DM01) & Long Stay Inpatients 13
Diagnostic (DM01) Waiters (99% of Patients Waiting Under 6 Weeks For Diagnostic Test)
Lead: Ruth Brown Timescale: Monthly
Key Issues: • The Trust continues to achieve the Diagnostic standard. • The standard was achieved at Divisional-level with the exception of Surgery
and Critical Care Medicine who had one breach due to capacity issues and the servicing of diagnostic equipment.
Key Actions: • The standard will continue to be closely monitored with action being taken to
address any themes as and when they arise.
Apr May Jun Jul Aug Sep Oct Nov Dec Jan Feb Mar
Current Year 36 42 33 34 35 28 36
Previous Year 36 39 39 33 30 26 27 23 22 32 38 36
0
5
10
15
20
25
30
35
40
45
Long Stay Inpatients (30+ Days)
80.00%
82.00%
84.00%
86.00%
88.00%
90.00%
92.00%
94.00%
96.00%
98.00%
100.00%
Oct
-17
No
v-1
7
Dec
-17
Jan-
18
Feb
-18
Mar
-18
Ap
r-18
May
-18
Jun
-18
Jul-
18
Au
g-18
Sep
-18
Oct
-18
Trust Total DM01 Performance
October 2017 - October 2018
Trust Total MEDicine S&CC PDG Target
Oct-17 Nov-17 Dec-17 Jan-18 Feb-18 Mar-18 Apr-18 May-18 Jun-18 Jul-18 Aug-18 Sep-18 Oct-18
MED 98.71% 99.67% 98.30% 97.95% 99.29% 99.50% 99.50% 99.27% 99.11% 99.33% 99.15% 98.82% 99.20%
S&CC 100.00% 96.30% 91.11% 82.86% 96.30% 94.74% 100.00% 100.00% 98.51% 100.00% 100.00% 100.00% 95.24%
PDG 100.00% 100.00% 100.00% 100.00% 100.00% 99.75% 100.00% 100.00% 100.00% 100.00% 100.00% 100.00% 100.00%
Trust 99.36% 99.68% 98.58% 98.16% 99.48% 99.52% 99.75% 99.67% 99.42% 99.68% 99.58% 99.48% 99.50%
TRUST BOARD PART 1 6. 316/18 CHIEF EXECUTIVE REPORT AND IN... Page 36 of 247

CAMHS ED (Eating Disorder) and EIP (Early Intervention for Psychosis) Incomplete Performance (92% of Patients Waiting Under 18 Weeks)
Data notes: due to the small number of patients on ED / EIP pathways, individual cases can have a large impact on the percentage performance.
Lead: Ruth Brown Timescale: Monthly
Key Issues: • Incomplete performance for both
ED routine and EIP were achieved at 100% during October.
Key Actions: N/A
CAMHS Tier 3 Incomplete Performance (92% of Patients Waiting Under 18 Weeks)
Lead: Ruth Brown Timescale: Monthly
Key Issues: • Wait to first appointment continues to exceed the 92% target. • Wait to second appointment is now included within the IPR for transparency.
The wait to second appointment is also calculated from the date the referral was received.
Key Actions: • A deep dive of waiting list and times is underway to review processes and
identify an action plan to meet the regulation received from the CQC 2018 visit
11.0 CAMHS Waiting Times 14
0.00%
10.00%
20.00%
30.00%
40.00%
50.00%
60.00%
70.00%
80.00%
90.00%
100.00%
Oct-17 Nov-17 Dec-17 Jan-18 Feb-18 Mar-18 Apr-18 May-18 Jun-18 Jul-18 Aug-18 Sep-18 Oct-18
Wait to 1st Appt 98.21% 98.99% 99.71% 97.03% 95.90% 96.31% 97.05% 97.36% 99.35% 97.85% 96.15% 99.39% 96.67%
Wait to 2nd Appt 65.19% 60.48% 62.57% 61.96% 61.15% 59.64% 54.94% 55.94% 57.64% 62.12% 61.42% 65.69% 65.37%
Target 92.00% 92.00% 92.00% 92.00% 92.00% 92.00% 92.00% 92.00% 92.00% 92.00% 92.00% 92.00% 92.00%
CAMHS Tier 3 Incomplete Performance
October 2017 - October 2018
0.00%
10.00%
20.00%
30.00%
40.00%
50.00%
60.00%
70.00%
80.00%
90.00%
100.00%
CAMHS ED & EIP Incomplete Performance
October 2017 - October 2018
ED Routine
ED Urgent
EIP
Target
Oct-17 Nov-17 Dec-17 Jan-18 Feb-18 Mar-18 Apr-18 May-18 Jun-18 Jul-18 Aug-18 Sep-18 Oct-18
ED Routine (< 28 Days) 5 4 4 5 0 4 1 4 2 3 1 1 5
ED Routine (Total) 5 4 5 6 0 5 2 4 2 3 3 1 5
ED Routine 100.00% 100.00% 80.00% 83.33% N/A 80.00% 50.00% 100.00% 100.00% 100.00% 33.33% 100.00% 100.00%
ED Urgent (< 7 Days) 0 0 0 0 0 0 0 0 0 0 0 0 0
ED Urgent (Total) 0 0 0 0 0 0 0 0 0 0 0 0 0
ED Urgent N/A N/A N/A N/A N/A N/A N/A N/A N/A N/A N/A N/A N/A
EIP (< 14 Days) 0 0 0 0 0 0 0 0 0 0 0 2 1
EIP (Total) 0 0 0 0 0 0 0 0 0 0 0 2 1
EIP N/A N/A N/A N/A N/A N/A N/A N/A N/A N/A N/A 100.00% 100.00%
Incomplete Pathways
TRUST BOARD PART 1 6. 316/18 CHIEF EXECUTIVE REPORT AND IN... Page 37 of 247

12.0 Cancer Waits 15
Cancer Waits – 2 Week & 31 Day Waits
Note: Cancer data is reported a month in arrears.
Lead: Ruth Brown Timescale: Monthly (month in arrears)
Key Issues and Actions: All cancer standards continue to be achieved at 100%
Apr May Jun Jul Aug Sep Oct Nov Dec Jan Feb Mar
Previous year 100.00%100.00%100.00%100.00%100.00%100.00%100.00%100.00%100.00%100.00%100.00%100.00%
Current year 100.00%100.00%100.00%100.00%100.00%100.00%
Target 93.00% 93.00% 93.00% 93.00% 93.00% 93.00% 93.00% 93.00% 93.00% 93.00% 93.00% 93.00%
50.00%
55.00%
60.00%
65.00%
70.00%
75.00%
80.00%
85.00%
90.00%
95.00%
100.00%
2 Week Wait from GP Referral to 1st Outpatient Appointment (All Cancers)
Apr May Jun Jul Aug Sep Oct Nov Dec Jan Feb Mar
Previous year 100.00% 100.00%100.00% 100.00% 100.00%100.00% 100.00% 100.00%100.00% 100.00% 100.00%100.00%
Current year 100.00% 100.00%100.00% 100.00% 100.00%100.00%
Target 96.00% 96.00% 96.00% 96.00% 96.00% 96.00% 96.00% 96.00% 96.00% 96.00% 96.00% 96.00%
50.00%
55.00%
60.00%
65.00%
70.00%
75.00%
80.00%
85.00%
90.00%
95.00%
100.00%
31 Day Wait from Diagnosis to 1st Definitive Treatment (All Cancers)
Apr May Jun Jul Aug Sep Oct Nov Dec Jan Feb Mar
Previous year 100.00%100.00% 100.00%100.00% 100.00% 100.00%100.00%
Current year 100.00%100.00%100.00%100.00%100.00% 0.00%
Target 94.00% 94.00% 94.00% 94.00% 94.00% 94.00% 94.00% 94.00% 94.00% 94.00% 94.00% 94.00%
50.00%
55.00%
60.00%
65.00%
70.00%
75.00%
80.00%
85.00%
90.00%
95.00%
100.00%
31 Day Wait for Subsequent Treatment where Treatment is Surgery
Apr May Jun Jul Aug Sep Oct Nov Dec Jan Feb Mar
Previous year 100.00% 100.00%100.00% 100.00% 100.00%100.00% 100.00% 100.00% 100.00% 100.00%100.00%
Current year 100.00% 100.00%100.00% 100.00% 100.00%100.00%
Target 98.00% 98.00% 98.00% 98.00% 98.00% 98.00% 98.00% 98.00% 98.00% 98.00% 98.00% 98.00%
50.00%
55.00%
60.00%
65.00%
70.00%
75.00%
80.00%
85.00%
90.00%
95.00%
100.00%
31 Day Wait for Subsequent Treatment where Treatment is an Anti-Cancer Drug Regime
TRUST BOARD PART 1 6. 316/18 CHIEF EXECUTIVE REPORT AND IN... Page 38 of 247

eRS Appointment Slot Issue (ASI) Ratio Comparison
The graph below shows the ASI ratio for the current financial year, previous financial year, with a comparison against the agreed trajectory target and to the national average for the current year. Notes: 1. The Appointment Slot Issue (ASI) Ratio is calculated as the Total ASIs/Total Bookings
for the stated time period 2. National ASI data for October 2018 was not yet published at the time of reporting.
Lead: Ruth Brown Timescale: Monthly
Key Issues: • The number of ASIs reduced throughout October in comparison to the
previous month.
Key Actions: N/A
eRS Appointment Slot Issues (ASIs)
The table below shows the Appointment Slot Issues encountered in the current reporting month by Division.
13.0 eReferrals Appointment Slot Issues 16
Apr May Jun Jul Aug Sep Oct Nov Dec Jan Feb Mar
Current Year 0.06 0.12 0.15 0.18 0.13 0.24 0.17
Previous Year 0.50 0.63 0.57 0.35 0.30 0.24 0.39 0.24 0.25 0.11 0.15 0.20
Current Year National Average 0.20 0.22 0.23 0.22 0.20 0.19
0.00
0.10
0.20
0.30
0.40
0.50
0.60
0.70
eReferrals Appointment Slot Issue Ratio
Division Local SpecialtyAppointment
Slot Issues (ASIs)Total Bookings
Appointment
Slot Issues (ASI)
Ratio
MEDicine Allergy 161 0.00
Clinical Haematology 8 5 1.60
Continence Service 47 74 0.64
Dermatology 48 144 0.33
Endocrinology 1 24 0.04
Hepatology 2 0.04
Immunology 17 12 0.04
Lipid 2 0.04
Metabolic Bone Disease 1 0.04
Paediatric Nephrology 7 4 1.75
Paediatric Neurology 4 91 0.04
Paediatrics 35 359 0.10
Respiratory 48 0.00
Rheumatology 31 0.00
Sleep Clinic 14 0.00
MEDicine Total 170 969 0.18
Surgery & Critical Care ENT 241 0.00
Fracture 1 0.00
Neurosurgery 4 1 4.00
Ophthalmology 21 130 0.16
Paediatric Surgery 80 254 0.31
Pain Clinic 3 10 0.30
Plastic Surgery 45 0.00
Scoliosis 28 0.00
Trauma and Orthopaedics 67 302 0.22
Surgery & Critical Care Total 175 1012 0.17
Grand Total 345 1981 0.17
Notes:
1. The Appointment Slot Issue (ASI) Ratio i s ca lculated as the Tota l ASIs/Tota l Bookings for the s tated time period
2. Where there are ASIs but zero bookings within a service, the ratio wi l l be displayed as - and highl ighted in red
Appointment Slot Issue Ratio > 1 (meaning there are more ASIs than appointments booked)
Appointment Slots Issue Ratio > 0 and < 1
eReferrals Appointment Slot Issue (ASI) Ratio - October 2018
RAG Rating Key:
No Appointment Slot Issues
TRUST BOARD PART 1 6. 316/18 CHIEF EXECUTIVE REPORT AND IN... Page 39 of 247

Outpatient Clinic WNB – Follow-up Appointments
14.0 Outpatient Clinic WNB (Was Not Brought – Previously DNA) 17
Outpatient Clinic WNB – New Appointments
Lead: Ruth Brown Timescale: Monthly
Key Issues:
• Was Not Brought rates for first outpatient attendances improved throughout October.
Key Actions: • Was Not Brought rates are continuing to be reviewed as part of the
Modernising Outpatients Programme.
Lead: Ruth Brown Timescale: Monthly
Key Issues: • Was Not Brought rates for follow-up outpatient attendances improved throughout
October.
Key Actions: • Was Not Brought rates are continuing to be reviewed as part of the
Modernising Outpatients Programme.
Apr May Jun Jul Aug Sep Oct Nov Dec Jan Feb Mar
Current Year 11.1% 10.4% 9.7% 12.1% 12.3% 11.3% 9.5% 0.0% 0.0% 0.0% 0.0% 0.0%
Previous Year 10.9% 11.1% 10.9% 10.0% 11.0% 10.6% 9.0% 9.8% 11.0% 11.0% 10.6% 9.3%
Target 9.0% 9.0% 9.0% 9.0% 9.0% 9.0% 9.0% 9.0% 9.0% 9.0% 9.0% 9.0%
0.0%
2.0%
4.0%
6.0%
8.0%
10.0%
12.0%
14.0%
Trust Total Outpatient WNB Rate (%) - New Appointments
Apr May Jun Jul Aug Sep Oct Nov Dec Jan Feb Mar
Current Year 12.7% 13.2% 11.8% 12.9% 13.1% 12.2% 11.5% 0.0% 0.0% 0.0% 0.0% 0.0%
Previous Year 13.5% 13.9% 14.0% 13.3% 13.4% 13.6% 12.8% 11.3% 14.9% 13.2% 12.3% 12.3%
Target 11.0% 11.0% 11.0% 11.0% 11.0% 11.0% 11.0% 11.0% 11.0% 11.0% 11.0% 11.0%
0.0%
2.0%
4.0%
6.0%
8.0%
10.0%
12.0%
14.0%
16.0%
Trust Total Outpatient WNB Rate (%) - Follow-up Appointments
TRUST BOARD PART 1 6. 316/18 CHIEF EXECUTIVE REPORT AND IN... Page 40 of 247

Specialties ranked by % of patients on the review list who are overdue (Latest Snapshot: 31/10/2018)
Outpatient Review List (Patients waiting past their review date)
Note: the figure shown in the grey box on the chart denotes the longest waiter in weeks at the point the snapshot was taken.
Lead: Ruth Brown Timescale: Monthly
Key Issues: • The Trust continues to have significant overdue review lists in a number of
areas.
Key Actions: • Work is on-going in relation to patients who attend the satellite clinics across
the region and being able to manage these more robustly.
15.0 Outpatient Review List 18
140 144 149 144 148 1530
500
1000
1500
2000
2500
3000
3500
4000
4500
May-18 Jun-18 Jul-18 Aug-18 Sep-18 Oct-18
Outpatient Review List - Overdue Patients by Due DateMay 2018 – October 2018
0-3 Months 3-6 Months 6+ Months
Division Local Specialty % Overdue Total OverdueLongest Wait
(Weeks)
Surgery & Critical Care PSU Peripheral Clinic 54.67% 474 153
MEDicine Neuro-Disability 39.62% 1265 52
Surgery & Critical Care Ophthalmology 30.69% 410 52
MEDicine Metabolics 27.81% 42 25
MEDicine Sleep Clinic 24.31% 44 19
MEDicine Immunology 22.95% 95 21
MEDicine Rheumatology 20.00% 42 19
MEDicine Dermatology 19.89% 149 19
MEDicine Neurofibromatosis 18.31% 13 11
MEDicine Cystic Fibrosis 16.67% 6 5
MEDicine Lipid 16.50% 17 22
MEDicine Paediatric Nephrology 15.59% 53 9
MEDicine Phenylketonuria 14.81% 4 0
MEDicine Epilepsy Nurse Clinic 12.33% 9 1
MEDicine Allergy 11.89% 301 21
Surgery & Critical Care Limb Reconstruction 11.29% 14 13
MEDicine Continence Service 10.84% 49 13
Surgery & Critical Care Paediatric Surgery 10.54% 116 66
MEDicine Gastroenterology 8.92% 111 3
MEDicine Endocrinology 8.84% 73 33
Surgery & Critical Care Orthoptic 8.75% 75 33
Surgery & Critical Care ENT 8.64% 109 34
MEDicine Paediatric Neurology 8.63% 82 24
Surgery & Critical Care Scoliosis 8.06% 47 10
Surgery & Critical Care Trauma and Orthopaedics 7.48% 151 28
Surgery & Critical Care Pain Clinic 7.38% 22 2
MEDicine Respiratory 6.70% 57 6
Surgery & Critical Care Refraction 5.80% 38 24
MEDicine TB 4.00% 1 0
MEDicine Clinical Haematology 3.70% 1 5
MEDicine Paediatrics 3.45% 15 2
MEDicine Hearing Services - Audiology 3.16% 37 17
MEDicine Cardiology 1.77% 13 4
MEDicine Home Oximetry Test 1.75% 1 0
MEDicine Paediatric Dietetics 1.69% 1 13
Surgery & Critical Care Neurosurgery 1.42% 4 5
MEDicine Metabolic Bone Disease 1.23% 3 7
TRUST BOARD PART 1 6. 316/18 CHIEF EXECUTIVE REPORT AND IN... Page 41 of 247

Theatres Utilisation
The data is calculated based on elective lists only and excludes Audit and Bank Holiday Lists, and any MRI lists or external theatre activity. Where a list is scheduled to run all day, these are counted as 2 sessions. Theatre Utilisation shows the percentage of time used in theatre (touch time) of the total planned theatre time. Touch Time has been calculated using the minutes between Enter Anaesthetic Room and Enter Recovery. This is in line with the national methodology used by NHSI and Four Eyes. Planned Theatre Time has been calculated by counting all day lists as 420 mins and AM/PM lists as 210 mins.
Lead: Ruth Brown Timescale: Monthly
Key Issues: • Theatre utilisation increased on the previous month.
Key Actions: • Work is being undertaken to determine utilisation targets at specialty level.
16.0 Outpatient Clinic & Theatres Utilisation 19
Outpatient Clinic Utilisation
The data and graph below show the utilisation rates for outpatient clinics at trust level. Notes: Utilisation rate is calculated by the following method: Total Attends / Total Slots. Missing Attendance Indicator refers to where it has not yet been recorded on the system whether the patient attended or not.
Lead: Ruth Brown Timescale: Monthly
Key Issues: • Changes to improve clinic utilisation were implemented during October which
imported all vacant, first-appointment slots within the following two weeks into the Clinic Utilisation Netcall data for automated slot-filling.
• Carved-out slots that can be released are now opened for booking at two weeks.
Key Actions: • Clinic utilisation is continuing to be reviewed as part of the Modernising Outpatients
Programme.
Apr May Jun Jul Aug Sep Oct Nov Dec Jan Feb MarCumulative
Position
Attends 78.69% 78.02% 80.22% 76.97% 76.52% 78.55% 79.97% 78.45%
Was Not Brought (WNB) 12.34% 12.59% 11.38% 12.50% 13.12% 12.29% 11.43% 12.21%
Patient Cancellations - On the Day 2.05% 1.65% 1.67% 2.02% 1.70% 1.87% 1.85% 1.83%
Patient Cancellations - 24 - 72 Hours Notice 0.95% 1.06% 0.86% 0.95% 0.81% 1.08% 0.96% 0.95%
Missing Attendance Indicator 0.00% 0.00% 0.00% 0.00% 0.00% 0.00% 0.00% 0.00%
Vacant (Patient Cancellations <72 Hours Notice)0.69% 0.86% 0.74% 0.99% 1.06% 0.86% 0.73% 0.84%
Vacant Slots 5.28% 5.83% 5.14% 6.58% 6.80% 5.36% 5.06% 5.71%
Current Year Utilisation (%) 78.69% 78.02% 80.22% 76.97% 76.52% 78.55% 79.97% 78.45%
Target Utilisation (%) 80% 80% 80% 80% 80% 80% 80% 80% 80% 80% 80% 80% 80%
Previous Year Utilisation (%) 76.6% 76.5% 77.6% 77.3% 76.2% 75.9% 75.8% 77.8% 73.6% 75.9% 75.1% 74.5% 76.1%
Trust Total
0.00%
10.00%
20.00%
30.00%
40.00%
50.00%
60.00%
70.00%
80.00%
90.00%
100.00%
0%
10%
20%
30%
40%
50%
60%
70%
80%
90%
100%
Apr May Jun Jul Aug Sep Oct Nov Dec Jan Feb Mar
Attends Was Not Brought (WNB) Patient Cancellations - On the Day
Patient Cancellations - 24 - 72 Hours Notice Missing Attendance Indicator Previous Year Utilisation (%)
Apr May Jun Jul Aug Sep Oct Nov Dec Jan Feb Mar
Current Year 83.5% 85.2% 85.4% 83.2% 87.3% 83.5% 84.8%
Previous Year 86.2% 85.9% 83.1% 82.1% 83.2% 82.2% 88.2% 83.8% 78.6% 82.5% 80.0% 82.4%
Target 85% 85% 85% 85% 85% 85% 85% 85% 85% 85% 85% 85%
40.0%
50.0%
60.0%
70.0%
80.0%
90.0%
100.0%
Theatre Utilisation
TRUST BOARD PART 1 6. 316/18 CHIEF EXECUTIVE REPORT AND IN... Page 42 of 247

Activity Performance – Outpatient Attendances (1st & FUp)
Lead: Ruth Brown Timescale: Monthly
Key Issues: • Outpatient attendances and non-elective inpatient activity was slightly below plan
at the end of October. • Elective inpatient and daycase activity saw the biggest under-performance during
October.
Key Actions: • Activity plans are currently being reviewed by the Divisions.
17.0 Activity v Plan: Outpatients and Inpatients
Activity Performance - Elective Inpatients (IP & DC)
Activity Performance – Non-Elective Inpatients
20
0
500
1000
1500
2000
2500
Ap
r-1
8
Ma
y-1
8
Jun
-18
Jul-
18
Au
g-1
8
Sep
-18
Oct
-18
No
v-1
8
De
c-18
Jan
-19
Feb
-19
Ma
r-19
Act
ivit
y
Apr-18 May-18 Jun-18 Jul-18 Aug-18 Sep-18 Oct-18 Nov-18 Dec-18 Jan-19 Feb-19 Mar-19
Actual 1409 1682 1609 1528 1529 1505 1635 0 0 0 0 0
Plan 1527 1603 1603 1680 1680 1527 1977 0 0 0 0 0
Previous Year 1461 1580 1691 1419 1532 1487 1638 0 0 0 0 0
Variance From Plan -7.7% 4.9% 0.4% -9.0% -9.0% -1.4% -17.3% 0.0% 0.0% 0.0% 0.0% 0.0%
Elective Inpatients (IP & DC)
0
100
200
300
400
500
600
700
Ap
r-1
8
Ma
y-1
8
Jun
-18
Jul-
18
Au
g-1
8
Sep
-18
Oct
-18
No
v-1
8
De
c-18
Jan
-19
Feb
-19
Ma
r-19
Act
ivit
y
Apr-18 May-18 Jun-18 Jul-18 Aug-18 Sep-18 Oct-18 Nov-18 Dec-18 Jan-19 Feb-19 Mar-19
Actual 471 471 472 454 418 522 586 0 0 0 0 0
Plan 543 578 540 555 492 560 602 0 0 0 0 0
Previous Year 548 587 563 589 487 568 642 0 0 0 0 0
Variance From Plan -13.3% -18.5% -12.5% -18.2% -15.0% -6.7% -2.6% 0.0% 0.0% 0.0% 0.0% 0.0%
Non-Elective Inpatients
0
5000
10000
15000
20000
Ap
r-1
8
Ma
y-1
8
Jun
-18
Jul-
18
Au
g-1
8
Sep
-18
Oct
-18
No
v-1
8
De
c-18
Jan
-19
Feb
-19
Ma
r-19
Act
ivit
y
Apr-18 May-18 Jun-18 Jul-18 Aug-18 Sep-18 Oct-18 Nov-18 Dec-18 Jan-19 Feb-19 Mar-19
Actual 14193 16744 15833 16256 13394 15336 17443 0 0 0 0 0
Plan 14658 15453 15364 16081 15874 14642 17661 0 0 0 0 0
Previous Year 12697 15992 15475 15047 13097 15317 15866 0 0 0 0 0
Variance From Plan -3.2% 8.4% 3.0% 1.1% -15.6% 4.7% -1.2% 0.0% 0.0% 0.0% 0.0% 0.0%
Outpatient Attendances (1st & FUp)
TRUST BOARD PART 1 6. 316/18 CHIEF EXECUTIVE REPORT AND IN... Page 43 of 247

Cash Balance (£'000)
Please note: reporting may run a month in arrears.
Lead: Mark Smith Timescale: Monthly
Key Issues:
• The Trust is currently c£460k ahead of the planned cash balance of £16.083m.
Key Actions: • A rolling 12 month cash flow is being agreed by Cash committee and will part of the
detailed Board report. • Refined Capital expenditure profile to be incorporated into Cash Flow Projection.
Agency Spend (£'000)
Please note: reporting may run a month in arrears.
Lead: Mark Smith Timescale: Monthly
Key Issues: • The Trust has been issued with a agency expenditure ceiling by NHS Improvement of
£3,441k for 2018/19, pro-rated evenly throughout the year. This equates to circa 3% of the pay bill.
• The external agency spend is currently tracking below the control target year to date, with a spend of £1.083m against a target of £1.689m.
Key Actions: • CWAMH are now using NHSP for their MH nursing requests. • Expedite recruitment timetable and challenge of existing hard to fill posts (alternative
skill mix/post types) through the VCP process • October 2018 sees the commencement of direct engagement of Agency Medical
staffing.
18.1 Finance – Agency Spend & Cash Balance 21
Apr May Jun Jul Aug Sep Oct Nov Dec Jan Feb Mar
Trust Total 129 240 429 574 700 842 1083 0 0 0 0 0
Target 241 483 724 965 1207 1448 1689 1930 2172 2413 2654 2896
Previous Year 156 317 553 791 1079 1301 1542 1869 2138 2153 2414 2830
0
500
1000
1500
2000
2500
3000
3500
Agency Spend (£'000) - 2018/19
Cumulative Position
Apr May Jun Jul Aug Sep Oct Nov Dec Jan Feb Mar
Trust Total 17,765 16,188 15,402 17,711 17,419 16,493 16,501
Target 21,771 20,280 18,386 18,568 16,778 15,144 16,038 16,804 17,501 18,126 18,490 18,863
Previous Year 30,770 28,447 29,357 29,715 27,903 24,396 21,870 19,721 19,557 21,691 21,870 20,955
0
5000
10000
15000
20000
25000
30000
35000
Cash Balance (£'000) - 2018/19
TRUST BOARD PART 1 6. 316/18 CHIEF EXECUTIVE REPORT AND IN... Page 44 of 247

Cost Improvement Programme (£ Delivery (£’000) and Percentage Delivery (against YTD profiles plan))
Please note: reporting may run a month in arrears.
Lead: Mark Smith Timescale: Monthly
Key Issues: • Current CIP performance is £981k behind plan for 7 months of the financial year
2018-19. • Significant year to date Divisional variances against plan are: Medicine - £455k behind plan PDG - £79k ahead of plan SCC – £299k behind plan CWAMH - £83k behind plan
Key Actions: • Phasing of CIP saving plan significantly increased in October 18 (additional £440k from
September value) and therefore a significant in month deficit (£465k)is seen as only the delivery of existing schemes continued.
• Actions to recover this are being worked up as part of the Trust wide recovery plan/actions.
Income & Expenditure position (against control total) £'000 ((surplus)/deficit))
Please note: reporting may run a month in arrears.
Lead: Mark Smith Timescale: Monthly
Key Issues: • Current performance against control total at period 7 (October 18) is £423k behind
(deficit) of the YTD control total. • Within this YTD Trust wide performance there are significant variances to Divisional
planned budgeted positions. • Key variances after 7 months are Medicine £2.59m deficit and SCC £1.4m surplus. • CIP performance is currently behind plan by £981k (Key variances/issues identified on
corresponding slide).
Key Actions: • Performance against Divisional Forecast outturns positions to be highlighted at
Performance reviews. • Recovery/stretch plans to be confirmed with actions – Divisional Performance reviews.
18.2 Finance – Income and Expenditure & CIP 22
Apr May Jun Jul Aug Sep Oct Nov Dec Jan Feb Mar
Trust Total (Cumulative) -210 -268 -472 -564 -7 -97 423 0 0 0 0 0
Previous Year (Cumulative) -452 164 78 -410 -255 -58 -259 -515 -198 -949 -808 434
Plan/Control Total (Cumulative) 0 0 0 0 0 0 0 0 0 0 0 0
-1200
-1000
-800
-600
-400
-200
0
200
400
600
Income & Expenditure (against control total) £'000 ((surplus)/deficit)) - 2018/19Cumulative Position
Apr May Jun Jul Aug Sep Oct Nov Dec Jan Feb Mar
£ Delivery (£'000) 0 92 221 521 1161 1519 1933 0 0 0 0 0
Percentage Delivered 0.0% 20.1% 28.1% 44.8% 72.6% 74.6% 66.3% 0.0% 0.0% 0.0% 0.0% 0.0%
Target £ Delivery (£'000) 229 459 788 1161 1598 2035 2914 3793 4722 5679 6636 8600
Previous Year £ Delivery 203 421 699 1013 1313 1583 1849 2308 2683 2937 3281 3961
0.0%
20.0%
40.0%
60.0%
80.0%
100.0%
0100020003000400050006000700080009000
10000
Cost Improvement Programme - 2018/19
Cumulative Position
TRUST BOARD PART 1 6. 316/18 CHIEF EXECUTIVE REPORT AND IN... Page 45 of 247

19.0 CQUIN 23
Action Required:Hospital Medicines Optimisation
CCG-2d - Antibiotic
Q1 Q2 Q3 Q4 - - - - -
CCG-6 - Advice and Guidance
Jude Stone Transition to new way of processing risked not hitting the 2 day turn around in Q2
Plans in place to roll out and increase robustness of process.
- -54,105 - - -54,105
- -54,105 - - -54,105
- - - - -
- - - - -
CCG-1a - Staff Health & W: Staff Survey
Jane Clawson *Survey only taken once leaving no time to change or continue to improve.*No plan has yet been developed to deliver the changes needed this year to better support achieving the CQUIN. The longer this is left the less time there is to make an impact.
Escalation through Corporate Planning. Confirmed no further monies to be given to support this CQUIN. Evidence of action in the organisation but still an unknown end position.
- - - -120,233 -120,233
CCG-2d - Antibiotic Sarah Thompson Multi-faceted approach leading to behaviour change required.Ward rounds need to be more targeted and to be financially secured.Lack of pharmacy input.
Strategy developed and now being implemented.Ward round funding being secured through the directorates. Targets for 2 indicators have been successfully re-negotiated with CCG. Full impact to be assessed before January 2019. CQUIN funding supporting additional clinical support and new pharmacy role.
- - - -60,117 -60,117
- - - -240,466 -240,466 - -54,105 - -240,466 -294,571
Total Projected Finance Risk, £
CWAMHs Total
SRO RAG
Status
Risks Mitigating Actions Projected Finance Risk, £
Success Stories:This CQUIN is developing and both the implentation of the strategy, including ward rounds and re-negotiating targets has been successful. However there is a longer term risk to this initiative as a % is funded via CQUINs monies which needs to be continued in 19/20.
PDG Total
Only CQUIN Schemes RAG rated Amber or Red are shown below. Forecast financial loss shown by quarter.
Division CQUIN
MEDicine
MEDicine Total
SCC Total
Negotiations with NHSE around how this is to be applied in Paediatric settings have been succesfull.
TOTAL VALUE of CQUIN for 18/19: £3,297,779
Total for all CQUINs
The project is on track to being delivered on time and within budget. Full year financial forecast is 100%.
There are problems but they are under control. Each milestone within the project has been RAG rated. Amber milestones which are pass/fail are forecast 100% financial achievement. Those with partial payment are forecast 50% financial achievement.There are major issues for which there is currently no resolution. Full year financial forecast reduced to £0.
Trust Wide CCG-1 - Staff Health & Wellbeing
CCG-2 - Reducing Impact of serious infections (Sepsis and Antimicrobial resistance)
Trust Wide Total
TRUST BOARD PART 1 6. 316/18 CHIEF EXECUTIVE REPORT AND IN... Page 46 of 247

Contents 24
Integrated Care System Dashboard
October (August 2018 data)
TRUST BOARD PART 1 6. 316/18 CHIEF EXECUTIVE REPORT AND IN... Page 47 of 247

TRUST BOARD PART 1 6. 316/18 CHIEF EXECUTIVE REPORT AND IN... Page 48 of 247

TRUST BOARD PART 1 6. 316/18 CHIEF EXECUTIVE REPORT AND IN... Page 49 of 247

REPORT TO THE TRUST BOARD OF DIRECTORS’ MEETING (PART 1) HELD ON 27 NOVEMBER 2018
MONTH 7 HEADLINE FINANCE REPORT
Trust aims supported by this paper
Build clinical and financial sustainability
Link to Board Assurance Framework
Risk that we do not maintain financial stability due to failure to deliver our financial plan or the negative impact of movement to a system-wide financial planning regime, resulting in requirements for additional CIPs or reduction in level and standard of services.
Failure to manage the Trust’s cash position would result in the Trust not being able to satisfy its obligations in respect of pay and non-pay costs.
Purpose of the paper
To present to the Trust Board of Directors the financial position of the Trust for the 7 months ending 31st October 2018.
Summary of key points
The Trust did not achieve the control total target for the period April – October 2018 by £423k, representing a downturn in month of £520k. Cumulatively the Trust is £423k behind plan with a reported deficit of £4.97m compared to a plan of £4.55m deficit excluding PSF (previously STF). The Trust’s control total deficit for the year is £1,613k.
Delivery of CIPs to date is £1.933m against a phased plan of £2.916m representing a shortfall of £983k.This element of the Trust’s financial plan remains the most significant risk in terms of delivery
The Trust’s cash position is £0.7m ahead of plan with Capital expenditure £5.6m behind Capital programme planned spend year to date
Board Action required The Board is asked to note the reported position ending 31st October 2018 along with the Divisional split of the Trust position. To also note current CIP shortfall and CIP FOT.
Author: Mr S Alexander, Head of Financial Management FOR ASSURANCE
Executive Sponsor: Mr M Smith, Director of Finance
TRUST BOARD PART 1 6. 316/18 CHIEF EXECUTIVE REP... Page 50 of 247

KEY MEASURES Narrative
Plan Actual Var Plan Actual Var Plan Actual Var
£m £m £m £m £m £m £m £m £m
I&E: Surplus/(Defict) Control total basis 0.67 0.15 (0.52) (4.55) (4.97) (0.42) 0.00
Agency expenditure (NHSI Ceiling= Plan) 0.29 0.16 0.13 2.01 0.89 1.11 0.00
CIP 0.88 0.41 (0.47) 2.91 1.93 (0.98) 0.00
Cash balance 16.04 16.50 0.46 0.00
Income (16.80) (16.57) (0.23) (110.13) (108.94) (1.19) 0.00
Plan Actual Var Plan Actual Var Plan Actual Var
£m £m £m £m £m £m £m £m £m
Income: Contracted (14.875) (14.508) (0.367) (96.770) (94.832) (1.938)
Income: Other (inc PSF) (1.925) (2.061) 0.136 (13.360) (14.110) 0.750
Total income (16.800) (16.569) (0.231) (110.130) (108.942) (1.188)
Pay 11.266 11.498 (0.232) 79.613 79.421 0.192
Non Pay 3.660 4.188 (0.528) 26.194 27.507 (1.313)
Total Expenditure 14.926 15.686 (0.760) 105.807 106.928 (1.121)
EBITDA (1.874) (0.883) 0.991 (4.323) (2.014) 2.309
Non operating expenditure 2.796 1.436 (1.360) 1.612 (0.894) (2.506)
Surplus/(Defict) 0.922 0.553 (0.369) (2.711) (2.908) (0.197)
Less:items excluded form control total (0.256) (0.407) (0.151) (1.836) (2.062) (0.226)
Surplus/(Deficit) Control total basis 0.666 0.146 (0.52) (4.547) (4.970) (0.42)
KEY MEASURES
INCOME AND EXPENDITURE SUMMARY (Control total)
M7 YTD (October 2018) Forecast 18/19
M7 YTD (October 2018) Forecast 18/19
FINANCE REPORT TO THE TRUST EXECUTIVE GROUP 21st November 20187 Months to 31st October 2018
1
Summary Activity Income Expenditure CIP Agency Cash Run Rate Divisional
Key issues:
•For the year to date, the Trust is in a £423k deficit position against the control total .
In month the Trusts recorded a £0.146m surplus against a planned control total surplus position of £0.666m resulting in a £520k deficit against plan.
•The year to date Trust position of £423k deficit is made up of:
Key message:
Within the £0.423m deficit position the following items/risks are excluded with no provision in the position:£0.312m ICS profile adjustment£0.1m of risk for NHSE contract (Sapphire lodge)£0.2m of risk for CQUIN non achievement
Plan ActualVariance
(deficit)/surplus
Plan ActualVariance
(deficit)/surplus
Medicine (1.82) (1.62) (0.20) (10.48) (7.89) (2.59)
SCC (1.47) (0.74) (0.72) (5.42) (6.82) 1.41
CWAMH (0.20) (0.11) (0.09) (1.57) (1.49) (0.08)
PDG 0.46 0.52 (0.05) 4.20 4.16 0.04
Finance 0.43 0.43 (0.01) 3.14 3.23 (0.09)
HR 0.23 0.22 0.01 1.59 1.61 (0.02)
Non Clinical 0.62 0.76 (0.15) 4.36 4.76 (0.39)
Research 0.02 0.01 0.00 0.12 0.11 0.00
Clinical support 0.75 0.70 0.05 5.04 4.87 0.17
M7 18-19 £'000 M7 YTD 18-19 £'000
Divisional position versus plan 2018/19
£m
(0.861) Income deficit (£1.188m inc CIP)
Outpatients £732k behind plan
Accident and Emergency £184k ahead of plan
Drugs and Devices £438k behind plan
R&D income £166k ahead of plan
0.848 Pay surplus (£0.192 surplus inc CIP)
Nursing vacancies/cap planning £1.76m surplus
Agency staff spend £0.894m (£1.349m Inc. NHSP)
Admin vacancies £527k surplus
Balancing Cap planning surplus
(1.313) Non Pay deficit
Lab equipment and materials £527k above plan
BMT £99k above plan
IT hardware/software £35k above plan
Bought in Services (NHS) £133k above plan
(0.983) CIP (£0.983m included in above values)
2.51 Contingency
£0.57m Central CIP
£1.94m contingency
(0.226) Control total adj.
(0.42) Control total surplus/(deficit)
TRUST BOARD PART 1 6. 316/18 CHIEF EXECUTIVE REPORT AND IN... Page 51 of 247

FINANCE REPORT TO THE TRUST EXECUTIVE GROUP 21st November 20187 Months to 31st October 2018
2
Summary Activity Income Expenditure CIP Agency Cash Run Rate Divisional
SLAM ACTIVITY (actual/£) SLAM ACTIVITY (actual/£) Narrative
Key issues:
• Medical activity is circa £1.2m below plan YTD (exc. Drugs and devices). Main areas of underperformance are :
Outpatients £732k behind plan - £50k deficit in October. (improved clinic utilisation in month 7 –80%)
Elective (inc. Day case) activity is £597k behind plan. Bone marrow transplant is £406k behind year to date plan
Accident and Emergency is £184k ahead of plan ytd resulting from an additional 327 children seen versus the plan based on last years performance.
Key actions:
•Modernising Outpatient programme /Medicine division tasked by the Recovery and Transformation to scope additional patients on lists numbers. Update at November Divisional Performance meeting .
• BMT variation of patients explained at previous Performance review. Forecast is assuming similar current levels.
Owner:
Modernising Outpatient programme
All Divisions (Performance review meeting)
£0
£2,000,000
£4,000,000
£6,000,000
£8,000,000
£10,000,000
£12,000,000
£14,000,000
£16,000,000
Apr-17 Jun-17 Aug-17 Oct-17 Dec-17 Feb-18 Apr-18 Jun-18 Aug-18 Oct-18
Act
ivit
y £
SLAM Income - 2018-19 (excluding drugs and devices)
£ Price Plan £ Price Actual
Commissioner Price Plan Price Actual Variance
Collaborative 32,179,054 31,997,722 (181,333)
Devolved Admin 126,577 70,434 (56,143)
Non Contract Account 616,995 793,211 176,215
NHSE 58,553,944 59,010,598 456,655
Overseas Visitors 31,729 23,860 (7,869)
Other 9,757 6,903 (2,854)
Internal (Non Commissioned) 1,874,152 - (1,874,152)
Private Patient 51,177 30,560 (20,617)
Grand Total 93,443,384 91,934,232 (1,509,151)
Total Income performance by Commissioner YTD at M7:
TRUST BOARD PART 1 6. 316/18 CHIEF EXECUTIVE REPORT AND IN... Page 52 of 247

SLAM ACTIVITY SLAM ACTIVITY Narrative
FINANCE REPORT TO THE TRUST EXECUTIVE GROUP 21st November 20187 Months to 31st October 2018
3
Summary Activity Income Expenditure CIP Agency Cash Run Rate Divisional
-
5,000
10,000
15,000
20,000
25,000
30,000
35,000
Apr-17 Jun-17 Aug-17 Oct-17 Dec-17 Feb-18 Apr-18 Jun-18 Aug-18 Oct-18
Apr-17
May-17
Jun-17
Jul-17
Aug-17
Sep-17
Oct-17
Nov-17
Dec-17
Jan-18
Feb-18
Mar-18
Apr-18
May-18
Jun-18
Jul-18
Aug-18
Sep-18
Oct-18
AE 4,54 4,98 4,72 4,79 3,61 4,61 5,40 5,33 4,96 4,53 4,61 4,83 4,47 5,09 4,96 4,92 3,36 4,56 5,20
DC 1,07 1,18 1,25 1,03 1,16 1,07 1,23 1,17 941 1,20 1,08 1,05 1,03 1,21 1,17 1,12 1,11 1,09 1,17
EL 498 400 472 411 389 438 427 452 380 420 546 454 392 590 638 436 479 441 456
NEL 716 745 762 862 949 1,16 740 680 731 607 894 917 501 1,07 792 589 512 773 773
OP 13,1 16,7 16,2 15,9 13,6 16,4 16,8 18,6 14,2 17,3 14,9 15,8 15,4 18,1 17,0 17,5 14,7 16,0 18,6
Other 5,75 5,79 6,11 5,68 5,81 5,43 5,93 6,34 5,18 6,35 5,93 6,04 5,93 5,77 5,92 5,72 5,75 5,11 6,34
Grand Total 25,7 29,8 29,5 28,7 25,6 29,2 30,6 32,6 26,4 30,4 28,0 29,1 27,7 31,8 30,5 30,4 25,9 28,0 32,5
Activity by POD 2017/18/19 (excluding Drugs and devices)Key issues:
•Outpatients saw an increase of 16% attendances in October compared to September (12% increase on the YTD average).
•Accident and Emergency attendances are currently tracking marginally behind attendances for the same period in 2017/18 (0.003%).
Key actions:
• Modernising outpatient programme continuation of “Was not Brought” (WNB)campaign across the city and ICS highlighting levels of children not being brought to clinic appointments. WNB Summit in January 19
• Additional patients per clinic calculation to be brought to performance review.
Owner:
Modernising Outpatient programme
Medicine Division (Performance review meeting)
TRUST BOARD PART 1 6. 316/18 CHIEF EXECUTIVE REPORT AND IN... Page 53 of 247

FINANCE REPORT TO THE TRUST EXECUTIVE GROUP 21st November 20187 Months to 31st October 2018
4
Summary Activity Income Expenditure CIP Agency Cash Run Rate Divisional
Key issues:
•Pay costs are £192k favourable compared to the NHSI plan.
•Removing unmet CIP targets this is £0.848m favourable. The capacity funding set aside has not been fully utilised by divisions to deliver the activity as services explore alternative delivery models to improve efficiency.
•Key Divisional Pay variances:SCC £1.043m surplus (£1.227m removing CIP)£1.1m Nursing vacancies and Cap planning
•In addition, planned developments assumed to commence at the start of the year (i.e. investment in ward nursing establishment -as shown in the Nursing staff graph opposite) has been delayed due to recruitment resulting in the YTD surplus. This along with current vacancies accounts for a large proportion of the Nursing and Medical variance.
Key actions:
• Divisions to confirm accurate nursing hours owed as per Eroster and actions to be followed.
Owner:• All Divisions to review and inform
Transformation and Recovery board.
TRUST BOARD PART 1 6. 316/18 CHIEF EXECUTIVE REPORT AND IN... Page 54 of 247

Plan Actual Var Plan Actual Var
£m £m £m £m £m £m
Drugs/Blood 1.05 1.17 (0.13) 6.87 6.69 0.18
IT Software/Hardware 0.18 0.12 0.07 1.27 1.30 (0.03)
Medical/Laboratory equipment 0.66 0.80 (0.14) 4.07 4.69 (0.62)
Services from NHS organisations 0.50 0.53 (0.04) 3.48 3.62 (0.13)
Services from Non NHS organisations 0.13 0.10 0.03 1.01 1.02 (0.01)
Other 1.152 1.467 (0.32) 9.494 10.193667 (0.70)
Total (Surplus/(Deficit)) 3.67 4.19 (0.52) 26.19 27.51 (1.31)
EXPENDITURE (Non Pay)
M7 YTD (Oct 2018)
0
0.5
1
1.5
2
2.5
3
3.5
4
4.5
5
Oct-17 Nov-17 Dec-17 Jan-18 Feb-18 Mar-18 Apr-18 May-18 Jun-18 Jul-18 Aug-18 Sep-18 Oct-18
Trust: Non Pay expenditure
Plan
Actual
FINANCE REPORT TO THE TRUST EXECUTIVE GROUP 21st November 20187 Months to 31st October 2018
5
Summary Activity Income Expenditure CIP Agency Cash Run Rate Divisional
Key issues:
Non pay expenditure is £1.313m above plan year to October 2018 as a result of:
•Lab equipment and materials £620k above plan, the majority of this is offset by additional income from activity over and above that planned at the beginning of the financial year.
•Services from other NHS organisations £133k – SLA values (Maintenance contracts, patient testing)
•Work services £102k, associated with the relocation •of corporate departments to the Moorfoot building and repair/maintenance of CAMH properties
•Bone marrow transplant costs £99k due to activity levels which as previously reported experience a lag in funding based on the child discharge date.
Key actions:
• Continued grip and control procurement measures remain in place. Owner:Simon Alexander (Head of Financial Management)
•Business travel group first meeting November 18 to ascertain actions/savings from staff/business travel.Owner:CMM/Workforce work streams
TRUST BOARD PART 1 6. 316/18 CHIEF EXECUTIVE REPORT AND IN... Page 55 of 247

Plan Actual Var Actual Plan Var
Division breakdown £'000 £'000 £'000 Workstream breakdown £'000 £'000 £'000
CLINICAL SUPPORT 38 21 (17) 7 Day Services 0 0 0
CWAMH 217 135 (81) ACP 0 0 0
FINANCE 89 95 6 Careful Money Management 996 1,036 (40)
MEDICINE 604 146 (458) Enablers 264 116 148
PDG 303 378 76 ICS 0 0 0
RESEARCH 6 - (6) Improving Flow 44 43 1
SCC 581 280 (301) Modernising Outpatients 0 0 0
NON CLINICAL SUPPORT 127 205 77 Service Development 212 150 62
HR 15 - (15) Well prepared surgery 0 0 0
CENTRAL 935 672 (263) Workforce 418 1,848 (1,430)
Other (277) 277
TOTAL 2,916 1,933 (983) TOTAL 1,933 2,916 (983)
CIP
YTD (OCT 2018) YTD (Oct 2018)
£-
£1,000
£2,000
£3,000
£4,000
£5,000
£6,000
£7,000
£8,000
£9,000
£10,000
Ap
r-1
8
Ma
y-1
8
Jun
-18
Jul-
18
Au
g-1
8
Sep
-18
Oct
-18
No
v-1
8
De
c-18
Jan
-19
Feb
-19
Ma
r-19
2018-19 CIP Performance ('000)
Cumulative target
Monthly actual
Monthly target
Cumulative actual
FINANCE REPORT TO THE TRUST EXECUTIVE GROUP 21st November 20187 Months to 31st October 2018
6
Summary Activity Income Expenditure CIP Agency Cash Run Rate Divisional
Key issues:
•Delivery of the £8.6m efficiency plans at month6 is £1,933k compared to a profiled plan of £2,916k (66%). The work stream that is significantly behind plan in terms of finance at this stage is Workforce – this has been well documented.
•Under YTD CIP delivery resulting in £983k deficit partially offset by pay vacancies and unspent capacity planning funding.
• This element of the Trust’s financial plan remains the most significant risk in terms of delivery.
Key actions:
•Modernising Outpatients work stream, as apart of the Trust recovery plan, to bring plan of adding additional patients per clinic.
Owner: Medicine Division
TRUST BOARD PART 1 6. 316/18 CHIEF EXECUTIVE REPORT AND IN... Page 56 of 247

FINANCE REPORT TO THE TRUST EXECUTIVE GROUP 21st November 20187 Months to 31st October 2018
7
Summary Activity Income Expenditure CIP Agency Cash Run Rate Divisional
Key issues:
•The Recovery and transformation board oversee productivity and efficiency schemes which contribute to the CIP target of the Trust and improve financial performance but do not contribute to the CIP target.
•Modernising outpatients work stream has schemes which have generated an additional; £340k of efficiency to the Trust. This results from increased the levels of clinic utilisation to 80% in October 2018 against a baseline of 76% in 2017/18.
Key actions:
• Under delivery of the CIP target is the Trust greatest financial risk Recovery plans for the Trust current FOT value incorporate all recovery actions and schemes .
Owner:
• All Divisions
Divisional CIP FOT 2018-19
£ Divisional Target £ Divisional FOT
Medicine 1,677,000 181,140
SCC 1,613,000 491,070
CWAMH 602,000 617,480
PDG 840,000 721,600
Finance 248,000 147,500
HR 43,000 -
Non-Clinical Support 353,000 460,000
Research 18,000 -
Clinical Support 106,000 104,040
Central 682,696
Total 5,500,000 3,405,526 (2,094,474)
Key issues (FOT):
• Current Divisional forecast outturn of CIP shows a deficit of c£2m against the Divisional plan of £5.5m
Division Workstream2 Sum of Oct Sum of YTD Total
CSUP Careful Money Management 4 4
Workforce 18 18
CSUP Total 21 21
CWAMH Careful Money Management 18 123
Enablers -
Service Development 2 12
Workforce -
CWAMH Total 20 135
Estates Enablers 35 35
Estates Total 35 35
Finance Careful Money Management 8 60
Finance Total 8 60
IM&T Enablers 21 107
IM&T Total 21 107
MEDicine Careful Money Management 59
Enablers 2 14
Workforce 20 73
MEDicine Total 22 146
Non-Clinical Workforce 5 99
Non-Clinical Total 5 99
PDG Careful Money Management 3 8
Improving Flow 7 44
Service Development 36 194
Workforce 21 133
PDG Total 67 379
S&CC Careful Money Management 25 72
Enablers 108
Service Development 1 6
Workforce 12 94
S&CC Total 37 281
Trust wide Careful Money Management 96 96
Trust wide Total 96 96
Central Careful Money Management 81 576
Central Total 81 576
Grand Total 414 1,934
Divisional CIP by workstream (M7 and YTD)
TRUST BOARD PART 1 6. 316/18 CHIEF EXECUTIVE REPORT AND IN... Page 57 of 247

FINANCE REPORT TO THE TRUST EXECUTIVE GROUP 21st November 20187 Months to 31st October 2018
8
Summary Activity Income Expenditure CIP Agency Cash Run Rate Forecast Divisional
AGENCYEXPENDITURE AGENCYEXPENDITURE-Narrative
Key issues:
• Agency spend for the year to date is £894k (exc. NHSP) which is a significant improvement compared to 2017/18 run rate.
•Agency admin and clerical has decreased considerably in 2018-19 due to the conclusion of the admin review and subsequent substantive recruitment.
•The NHSI Trust ceiling is £3.441m with a ytd value of £2.007m. The Trust is currently tracking well within this requested ceiling with a ytd expense of £.894m.
Key actions:
•Implementation of direct engagement with current Medical agency staff commenced in October 2018 (VAT savings built into FOT).
•Mental health nurses (Agency) now being sourced through NHSP.
Owner:
• CWAMH Division to confirm any financial impact of NHSP being used for MH nursing.
Expenditure to dateDivision Total Pay Spend £ Substantive/NHSP Pay £ Agency Spend YTD £ NHSI Target YTD £ NHSI Target £
MEDICINE £22,562,959.47 £22,329,590.69 £233,368.78 £583,824.50 £1,000,842.00SURGERY & CRITICAL CARE £18,680,749.51 £18,567,994.00 £112,755.51 £520,617.42 £892,487.00COMMUNITY SERVICES & WAMH
£13,710,452.74 £13,339,080.59 £371,372.15 £353,210.08 £605,503.00
DIAGNOSTICS & PHARMACY £8,662,573.18 £8,660,361.98 £2,211.20 £223,273.17 £382,754.00FINANCE £1,010,869.52 £951,587.79 £59,281.73 £25,424.58 £43,585.00HUMAN RESOURCES £3,762,613.89 £3,762,613.89 £0.00 £96,269.25 £165,033.00CLINICAL SUPPORT £3,031,657.78 £2,971,386.71 £60,271.07 £71,487.50 £122,550.00NON CLINICAL SUPPORT £3,337,688.48 £3,282,176.01 £55,512.47 £119,548.92 £204,941.00RESEARCH INNOVATION & PROJECTS
£640,481.19 £640,481.19 £0.00 £13,594.58 £23,305.00
Total £75,400,045.76 £74,505,272.85 £894,772.91 £2,007,250.00 £3,441,000.00
TRUST BOARD PART 1 6. 316/18 CHIEF EXECUTIVE REPORT AND IN... Page 58 of 247

FINANCE REPORT TO THE TRUST EXECUTIVE GROUP 21st November 20187 Months to 31st October 2018
9
Summary Activity Income Expenditure CIP Agency Cash Run Rate Divisional
CASHBALANCE CASHBALANCE-Narrative
Cash Flow Summary (M07) £'mCash balance b/f 16,493Surplus/(Deficit) 553(Increase)/Decrease in receivables (335)Increase/(Decrease) in creditors 1,125Other movements (1,333)Cash balance c/f 16,501
Key issues:
• Closing cash balance is ahead of the NHSI submitted plan by £0.7m.
• Projected year end cash balance is £3m behind NHSI plan
• Downside cash balance is £9m behind NHSI plan and represents £6m identified risk against the forecasted year end cash position
• Downside risk consists of ICS support (£0.8m), non-qualification for Provider Sustainability Funding (£2.2m), (£2m) forecast deficit position, (£1m) non-cash balance sheet release in recovery plan.
• Capital expenditure £5.6m behind Capital programme planned spend year to date. Forecasted expenditure has been revised to circa £10m
Key actions:
• Cash Committee to continue to closely monitor cash position – identifying risks and strategies to mitigate cash balance risk
• Refined Capital expenditure profile to be worked through and incorporated into Cash Flow projection
• Cash metrics re: creditor / debtor days to be added to report
Owner:
Financial Accountant
TRUST BOARD PART 1 6. 316/18 CHIEF EXECUTIVE REPORT AND IN... Page 59 of 247
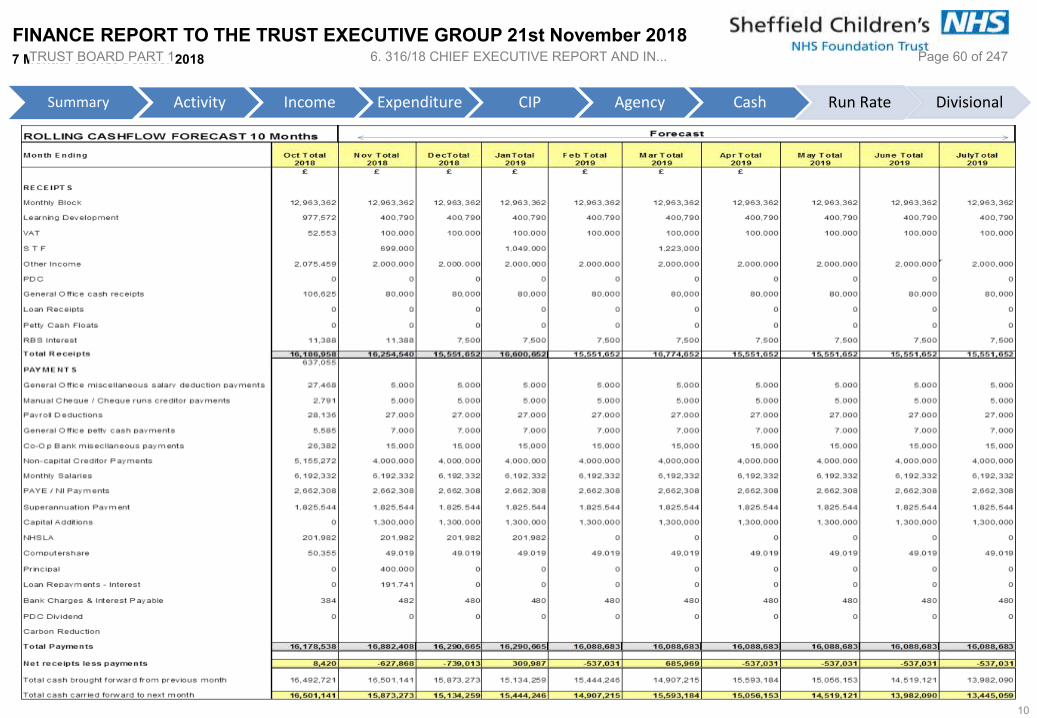
FINANCE REPORT TO THE TRUST EXECUTIVE GROUP 21st November 20187 Months to 31st October 2018
10
Summary Activity Income Expenditure CIP Agency Cash Run Rate Divisional
TRUST BOARD PART 1 6. 316/18 CHIEF EXECUTIVE REPORT AND IN... Page 60 of 247

FINANCE REPORT TO THE TRUST EXECUTIVE GROUP 21st November 20187 Months to 31st October 2018
11
Summary Activity Income Expenditure CIP Agency Cash Run Rate Divisional
NHS Apr-18 May-18 Jun-18 Jul-18 Aug-18 Sep-18 Oct-18Within Terms 3,870 1,321 2,401 3,037 3,688 2,659 1,668 Over Term 31-90 Days 429 1,072 500 639 416 677 724 Over Term 91-150 Days 304 352 284 518 498 762 514 Above 151 Days 509 494 513 579 609 651 1,331 Total 5,112 3,239 3,698 4,773 5,211 4,749 4,237
Non NHSWithin Terms 1,618 1,095 748 739 651 513 662 Over Term 31-90 Days 180 451 323 90 59 188 53 Over Term 91-150 Days 174 195 124 345 297 316 93 Above 151 Days 279 268 373 361 365 391 754 Total 2,251 2,009 1,568 1,535 1,372 1,408 1,562
Sales Ledger Debt Balances Month on Month £'000
Key issues:
• PDG Division currently holding highest value of outstanding debt on invoices raised at close of period, predominantly related to Genetics test income
• PDG debt stands at £2m at October 18 which is a £0.1m improvement on the prior period. £0.6m is currently within term leaving £1.4m outside of term, of which £0.2m is older than 1 year+
Key actions:
• Principal Accountant pro-actively working with Finance and labs teams to identify issues and establish best course of action to both reduce levels of debt beyond payment terms and improve processes internally to reduce risk of bad debt accumulation going forward
• A strategy incorporating a number of measures to tackle debt currently being formulated. Principal Accountant issuing update to PDG performance review
• Definitive debtors in distress funding list to be drawn up to identify those Trusts who pose a payment risk
• Director of Finance to follow-up letters already issued to poor paying Trusts with DoF to DoF conversation
Owner:
Financial Accountant
TRUST BOARD PART 1 6. 316/18 CHIEF EXECUTIVE REPORT AND IN... Page 61 of 247

RUN RATE
FINANCE REPORT TO THE TRUST EXECUTIVE GROUP 21st November 20187 Months to 31st October 2018
12
Summary Activity Income Expenditure CIP Agency Cash Run Rate Divisional
Monthly Actuals Oct-17 Nov-17 Dec-17 Jan-18 Feb-18 Mar-18 Apr-18 May-18 Jun-18 Jul-18 Aug-18 Sep-18 Oct-18
SLAM income (exc Drugs/Blood) 13,140,061 13,491,848 12,796,977 12,523,252 13,019,152 14,522,531 11,721,534 12,937,079 12,793,636 12,942,375 12,324,840 12,273,608 13,477,514 Drugs/Blood income 774,130 788,621 758,775 932,622 591,494 785,959 787,552 782,568 715,676 858,897 722,003 721,098 924,792 Non SLAM income 74,447 84,517 42,456 46,008 48,603 51,827 105,161 45,621 183,048 60,597 89,569 84,404 106,467 Other
Clinical income 13,988,638 14,364,986 13,598,208 13,501,882 13,659,249 15,360,317 12,614,247 13,765,268 13,692,360 13,861,869 13,136,412 13,079,110 14,508,773
Non clinical income 2,103,459 1,991,324 2,081,776 2,253,751 1,824,333 3,308,667 1,964,062 2,061,061 2,167,720 2,213,104 2,003,425 1,836,322 2,061,778
Total income 16,092,097 16,356,310 15,679,984 15,755,633 15,483,582 18,668,984 14,578,309 15,826,329 15,860,080 16,074,973 15,139,837 14,915,432 16,570,551
Pay 11,042,457 11,063,297 11,078,115 10,812,771 11,053,216 11,612,784 10,952,592 11,399,483 11,380,471 11,280,917 11,498,259 11,411,196 11,498,228 Non-Pay (exc Reserves, Drugs & Blood)
3,012,963 2,987,117 2,621,266 3,175,540 2,644,982 3,094,878 2,662,310 2,703,701 3,133,598 3,164,276 3,071,306 2,621,413 3,015,951
Drugs/Blood costs 859,900 1,043,608 997,144 1,208,664 819,277 1,570,396 950,846 1,159,851 850,089 1,146,939 1,022,966 880,535 1,172,863 Interest 194,296 195,537 196,785 175,744 214,810 (186,235) 206,052 288,981 117,274 211,710 203,972 215,470 196,744 Depreciation 374,208 374,208 374,208 374,208 374,208 365,482 413,502 421,341 422,888 423,299 436,922 439,672 439,971
Total expenditure 15,483,824 15,663,767 15,267,518 15,746,927 15,106,493 16,457,305 15,185,302 15,973,357 15,904,320 16,227,141 16,233,425 15,568,286 16,323,757
'Operational' Surplus/(Deficit) 608,273 692,543 412,466 8,706 377,089 2,211,679 (606,993) (147,028) (44,240) (152,168) (1,093,588) (652,854) 246,794
Non pay reserves 16,000 34,833 (21,333) - (193,250) 11,250 63,000 325,333 381,667 6,667 6,667 6,667 (305,833)
Reported Surplus/(Deficit) 592,273 657,710 433,799 8,706 570,339 2,200,429 (669,993) (472,361) (425,907) (158,835) (1,100,255) (659,521) 552,628
TRUST BOARD PART 1 6. 316/18 CHIEF EXECUTIVE REPORT AND IN... Page 62 of 247

FINANCE REPORT TO THE TRUST EXECUTIVE GROUP 21st November 20187 Months to 31st October 2018
13
Summary Activity Income Expenditure CIP Agency Cash Run Rate Divisional
Key issues:
Medicine Divisional position is £2.589m (pre int. recharges) deficit driven by income underperformance (OP £753k behind plan YTD) and pay pressures (Mat leave, Jnr medic rota gaps) and CIP under delivery
Key actions:Recovery plan to be actioned by MEDicine division with OP calculations to be bought to Performance review meeting detailing OP additional patients.
Owner:Medicine Division
Key issues:
SCC Divisional position is £1.363m surplus (pre int. recharges) driven by income over performance and Capacity planning surplus on unspent projects yet to start. October saw a £724k deterioration in the YTD position due to increased CIP target and an increased contracted income target. CIP delivery and contracted actuals remained at previous months performance levels.
Key actions:Forecast out turn position to be confirmed following October performance. Recover plan update at Performance review meeting in November.
Owner:SCC Division
Plan Actual
Variance
Deficit)/
Surplus
Plan Actual
Variance
Deficit)/
Surplus
Plan Actual
Variance
Deficit)/
Surplus
Plan Actual
Variance
Deficit)/
Surplus
£m £m £m £m £m £m £m £m £m £m £m £m
Income: Contracted (40.176) (38.444) (1.732) Income: Contracted (31.734) (31.879) 0.145 Income: Contracted 0.000 0.000 0.000 Income: Contracted 0.000 0.000 0.000
Income: Other (1.662) (1.788) 0.126 Income: Other (1.268) (1.166) (0.102) Income: Other (0.450) (0.406) (0.044) Income: Other (0.327) (0.285) (0.042)
Total income (41.838) (40.232) (1.606) Total income (33.002) (33.045) 0.043 Total income (0.450) (0.406) (0.044) Total income (0.327) (0.285) (0.042)
Pay 22.927 23.537 (0.610) Pay 21.977 20.934 1.043 Pay 3.245 3.117 0.128 Pay 1.131 1.010 0.121
Non Pay 8.433 8.806 (0.373) Non Pay 5.608 5.288 0.320 Non Pay 2.242 2.156 0.086 Non Pay 2.340 2.507 (0.167)
Total Expenditure 31.360 32.343 (0.983) Total Expenditure 27.585 26.222 1.363 Total Expenditure 5.487 5.273 0.214 Total Expenditure 3.471 3.517 (0.046)
EBITDA (10.478) (7.889) (2.589) EBITDA (3.947) (6.074) 1.406 EBITDA 5.037 4.867 0.170 EBITDA 3.144 3.232 (0.088)
Internal recharges 5.316 5.092 0.224 Internal recharges 1.697 1.735 (0.038) Internal recharges 0.000 0.000 0.000 Internal recharges 0.000 0.000 0.000
Total position post Int. recharges(5.162) (2.797) (2.365) Total position post Int. recharges(2.250) (4.339) 1.368 Total position post Int. recharges5.037 4.867 0.170 Total position post Int. recharges3.144 3.232 (0.088)
Plan Actual
Variance
Deficit)/
Surplus
Plan Actual
Variance
Deficit)/
Surplus
Plan Actual
Variance
Deficit)/
Surplus
Plan Actual
Variance
Deficit)/
Surplus
£m £m £m £m £m £m £m £m £m £m £m £m
Income: Contracted (15.696) (15.676) (0.020) Income: Contracted (4.917) (4.917) 0.000 Income: Contracted 0.000 0.000 0.000 Income: Contracted (0.366) (0.366) 0.000
Income: Other (0.485) (0.621) 0.136 Income: Other (4.404) (4.812) 0.408 Income: Other (2.881) (3.063) 0.182 Income: Other (0.031) (0.020) (0.011)
Total income (16.181) (16.297) 0.116 Total income (9.321) (9.729) 0.408 Total income (2.881) (3.063) 0.182 Total income (0.397) (0.386) (0.011)
Pay 13.813 13.904 (0.091) Pay 9.168 8.946 0.222 Pay 3.721 3.793 (0.072) Pay 3.322 3.419 (0.097)
Non Pay 0.801 0.906 (0.105) Non Pay 4.351 4.944 (0.593) Non Pay 0.748 0.877 (0.129) Non Pay 1.439 1.722 (0.283)
Total Expenditure 14.614 14.810 (0.196) Total Expenditure 13.519 13.890 (0.371) Total Expenditure 4.469 4.670 (0.201) Total Expenditure 4.761 5.141 (0.380)
EBITDA (1.567) (1.487) (0.080) EBITDA 4.198 4.161 0.037 EBITDA 1.588 1.607 (0.019) EBITDA 4.364 4.755 (0.391)
Internal recharges (1.048) (1.048) 0.000 Internal recharges (5.964) (5.780) (0.184) Internal recharges 0.000 0.000 0.000 Internal recharges 0.000 0.000 0.000
Total position post Int. recharges(2.615) (2.535) (0.080) Total position post Int. recharges(1.766) (1.619) (0.147) Total position post Int. recharges1.588 1.607 (0.019) Total position post Int. recharges4.364 4.755 (0.391)
Plan Actual
Variance
Deficit)/
Surplus
£m £m £m
Income: Contracted 0.000 0.000 0.000
Income: Other (0.570) (0.811) 0.241
Total income (0.570) (0.811) 0.241
Pay 0.472 0.657 (0.185)
Non Pay 0.213 0.268 (0.055)
Total Expenditure 0.685 0.925 (0.240)
EBITDA 0.115 0.114 0.001
Internal recharges 0.000 0.000 0.000
Total position post Int. recharges0.115 0.114 0.001
YTD (October 2018)
MEDicine SCC
YTD (October 2018)
Clinical support
YTD (October 2018)
Finance
YTD (October 2018)
HR Non Clinical
YTD (October 2018) YTD (October 2018)
R&I
YTD (October 2018)
CWAMH
YTD (October 2018)
PDG
YTD (October 2018)
TRUST BOARD PART 1 6. 316/18 CHIEF EXECUTIVE REPORT AND IN... Page 63 of 247

Chief Executive’s Report – November 2018 1. Integrated Performance Report
The Integrated Performance Report for October 2018 is attached. This includes an Executive Summary of Trust wide performance against the five strategic aims. Each Director will report key highlights of the report for TEG to note or consider. This month’s report also includes the Integrated Care System dashboard for October (August 2018 data). 2. Care Quality Commission (CQC) Update
The Trust received the Provider Information Request (PIR) on 1 November with a deadline to be completed by Thursday 22 November 2018. Data requests have been completed from a wide range of departments across the Trust which were signed off by an Executive Director and the PIR successfully submitted. The information will be reviewed by the CQC over the coming weeks and we will move into a Well Led Inspection and unannounced visits. A communication plan is in place to ensure all staff are kept up to date on progress. In the meantime all staff are encouraged to prepare their ‘Glimpses of Brilliance’ to ensure we are showing the inspectors all the amazing work underway across the whole Trust. 3. Sheffield SEND Local Area Inspection
Inspectors from OFSTED and the CQC have visited Sheffield this week to conduct an inspection of the Local Area’s effectiveness in identifying and meeting the needs of children and young people who have special educational needs and/or disabilities (SEND). They have conducted 20 focus groups and visited 12 settings. They have met with children, young people, parents and carers as well as providers and professionals from across Education, Health and Care. They investigated three areas:
the effectiveness of the local area in identifying children and young people who have special educational needs and/or disabilities
the effectiveness of the local area in assessing and meeting the needs of children and young people who have special educational needs and/or disabilities
the effectiveness of the local area in improving outcomes for children and young people who have special educational needs and/or disabilities
It has been a tough and rigorous process which will help us to continue to drive our future improvement for children and young people with SEND and we are grateful to inspectors for their feedback. We would like to thank all the children, young people and their families, as well as professionals from across Education, Health and Care in the Local Area for their contributions to the inspection. As with all inspections the outcome is confidential until the report is published. We expect this to be in late December or early January 2019.
4. Accountable Care Partnership (ACP) The Sheffield ACP Programme Director report is attached at appendix A for information.
TRUST BOARD PART 1 6. 316/18 CHIEF EXECUTIVE REP... Page 64 of 247

5. Integrated Care System (ICS) The CEO Report for the ICS in South Yorkshire and Bassetlaw is attached at appendix B for information. This includes forthcoming ICS meeting dates. Hospital Services Review - Clinical workshops continue to refine models and CEO level workshops are taking place to discuss options for the hosted network development. A review of the ICS governance is also underway with all Chairs and Chief Executives.
6. 2019 Clinical Summit – Reminder to save the date Building on the success this this year’s summit, we have agreed to hold larger annual events. Next year’s will be held on Thursday 26th September 2019 – SAVE THE DATE! We are giving notice of the date now to enable clinical services and rota’s to be planned accordingly.
TRUST BOARD PART 1 6. 316/18 CHIEF EXECUTIVE REP... Page 65 of 247

ACP Programme Director Report This brief report will fall into three sections: Strategic, Delivery and Development
1. Strategic National/Regional
A Place Response for Sheffield has been submitted for the NHS Long Term Plan consultation. All partners were involved in its development and it is attached as Appendix 1.
On 20 September 2018, The King’s Fund published “A Year of Integrated Care Systems: Reviewing the Journey so Far”. In population terms, Sheffield is comparative to many of the ten vanguard ICS footprints. Hence there is significant applicable learning for place development as well as at ICS level. A summary of recommendations from the report is provided below:
A group of Sheffield leaders attended the first of four days of the King’s Fund ICS Learning Network on 4 October 2018. The network brings together ICS/ACP/STP groups alongside sharing evidence from international case studies of integrated care systems.
Sheffield Children’s NHS Foundation Trust
Sheffield Clinical Commissioning Group Sheffield Health and Social Care NHS Foundation Trust
Sheffield Teaching Hospitals NHS Foundation Trust
Recommendations for local systems Invest in building collaborative relationships at all levels of the system – this can only be
done locally and takes time and commitment. Promote and value system leadership – ICS leadership should be developed with a continuing
emphasis on collective and distributed leadership, ensuring leaders have dedicated time to fulfil their roles.
Integrate at different levels of the system, building up from places and neighbourhoods in line with the principle of subsidiarity, ICSs should set the overall vision, provide leadership across the system and undertake functions that are best performed at scale.
Draw on the skills and leadership of frontline staff – staff should be front and centre of plans to redesign services, with clinical leadership at the fore.
Build governance in an evolutionary way to support delivery – this should be iterative and locally led, ensuring that it does not conflict with accountabilities of statutory organisations.
Develop system-wide capabilities to gather, share and act on public insights – ICSs must take active steps to listen to and work with the public on an ongoing basis, and to bring together dispersed insight and feedback data from across the system.
Develop active strategies to facilitate wider adoption of new care models – this requires an active approach centred around peer-to-peer learning and networks.
Build robust evaluation into the ICS programme that supports learning and improvement and measures progress – metrics should reflect the breadth of ICSs’ priorities, and recognise that much of the impact will emerge in the long term.
Look beyond the health and care system to improve population health – this requires deeper local authority involvement and closer working with the voluntary and community sector, independent sector organisations and communities (see Figure below).
https://www.kingsfund.org.uk/publications/year-integrated-care-systems
Appendix A
TRUST BOARD PART 1 6. 316/18 CHIEF EXECUTIVE REP... Page 66 of 247

NHS England has launched a consultation on the contracting arrangements for Integrated Care Providers (ICPs) link
o Sheffield colleagues attended events in Leeds and at Sheffield CCG and a summary was considered at October EDG.
Refreshed Place Plan At EDG on 9 October, the Communications work stream set out their overall
Communication Plan for the ACP. Staff, stakeholders and the public will be involved in a set of deliberative workshops to widen the reach of discussion on the ACP and key priorities for health and care in Sheffield. This will feed into a refresh of ‘Shaping Sheffield: the Plan’. Dates have been identified for the workshops in January/February 2019. The dates for the events are:
7th January: 13:30-16:30, Mayfield Suite, Fulwood 11th January: 9:00-12:00, Children’s Hospital Lecture Theatre 28th January: 9:00-12:00, St Mary’s Church 29th January: Medical Education Centre, Northern General Hospital 31st January: 9 – 12:00, Circle, Town Centre
This will be brought together with the work taking place on developing a Children’s blueprint for Sheffield, working on a similar timescale.
The intention is that these workshops will bring together staff from across the health system, and therefore a “cross section” of staff from individual partner organisations will be invited. The refreshed plan as a whole will be positioned in the context of the wider Health and Well-Being Strategy.
Strategy Leads from across the city will support the leadership and design of these events. The Strategy Directors have emphasised the importance of ensuring the core priorities of the plan are fed into partner business planning processes to ensure our system aspirations are tied in with organisational plans and become “real”.
It is intended the draft ACP – Shaping Sheffield plan will be produced by the end of March. During December – February it will also be important there is opportunity for executive and Board teams to feed in to ensure this is a genuinely owned plan by all partners.
2. Delivery i. CQC Local System Review
A full quarterly progress report against the CQC plan was considered by the ACP Board on 31 October 2018. Good progress has been made in some areas, but there are key risks around the delivery of the DTOC position and delivering on the ambitions of new care models, to be achieved by end of March 2019 through a new integrated commissioning model. EDG requested an update from each organisation by 21 September 2018 on internal partner governance arrangements. All partners have also confirmed they will release the necessary internal resource (time and people, not necessarily money) to enable the actions they are leading on/involved with to deliver. Executive leads from each organisation have been identified. A cross-system Steering Group comprising the Executive Leads above will meet on a 6 weekly basis to oversee the overall CQC plan. This will feed into Executive Delivery Group and, subsequently, to the ACP Board. Health and Well-Being Board have requested regular
TRUST BOARD PART 1 6. 316/18 CHIEF EXECUTIVE REP... Page 67 of 247

updates and SCC Scrutiny and Oversight Committee have indicated their intention to call this in for scrutiny on a 6 monthly basis. Individual aspects of the plan are receiving very close attention – for example the CEO led meetings with Chief Operating Officers on Why Not Home Why Not Today work.
ii. Overview of Programmes The Programme Director is reviewing overall ACP architecture in line with the CEO Away Day decision, in conjunction with work stream teams. Summary of Programmes – Highlights
Significant activity is now taking place across most ACP workstreams. There are considerable links between all of the programmes, and the overall strategy and vision needs to be developed, with the solid delivery plan underneath. There are three stands to this:
Developing the coherent strategy: This will be a key focus of ACP work from now until the end of the financial year resulting in the “Refreshed Place Plan” alluded to in Section 1.
Developing credible underpinning delivery plans: whilst considerable progress is being made here there are workstreams which need further help to increase pace and the strength of their approach. The workstreams are all at different stages but good progress has been made since the last ACP Board meeting.
Increasingly we need to be redirecting resource across ACP partners to this agenda in order to move this system work at greater pace.
A framework paper will be developed to help guide how we move into a coherent strategy and set of delivery plans, and this will frame consultation with partner organisations. Core Workstreams The Elective work stream has refreshed its focus and had held successful system wide
events on skin and cardiology with positive priorities to pursue. ENT and Gastroenterology are next priorities. There is an effective system leadership team working together on this and good progress is being made.
As part of the Urgent and Emergent Care Work Stream, two clinical ACP workshops between CCG and STHFT have taken place on “Developing Improved Services for Patients at Risk of Unplanned Hospital Admission”. A headline vision is developing, with a 3rd meeting planned for November. There is an in principle commitment from both organisations to a new supporting contractual framework. A cross-organisational team attended the recent NHS England Large Scale Change Masterclasses with a focus on this project.
The Children’s Work Stream are looking to streamline reporting and mobilise clinical and leadership capacity to progress the work. They are developing a refreshed “blueprint” for children’s care by April 2019.
Long Term Conditions held a refresh workshop on Friday 28 September, to re-clarify shape and priorities. A discussion with the primary care work stream needs to take place to ensure a joined up approach and in order avoid duplication. A high level programme vision and objectives document will be brought together to provide direction for the programme.
The importance of effective neighbourhood development is a key theme in many programmes, and a joined up system approach that draws together current system work is essential. Following the September workshop, a second workshop with Local Authority colleagues, with greater input from children’s and SCC colleagues took place on Friday
TRUST BOARD PART 1 6. 316/18 CHIEF EXECUTIVE REP... Page 68 of 247

26th October. From this we need to strengthen the system wide approach to neighbourhood development as part of our “system approach”.
Mental Health and Learning Disabilities work stream secured agreement from ACP Executive Delivery Group to think differently about ‘transitions’ issues in Sheffield (in the context of young person mental health). This has historically been an issue both nationally and locally in Sheffield and despite many attempts to resolve this, problems continue to occur. Taking an “organisational agnostic” system wide approach has been agreed, with a set of more radical options discussed by EDG. It was agreed initial whole system discussions would take place to reach a new vision for an all age service, commencing in December. All partners will be involved in this work and this has been a persistent theme raised by staff around the system to the Programme Director and the MH & LD work stream.
MH & LD are planning a programme workshop stock-take in December 2018 and considering how this takes an all-age focus. The workshop will review progress and plan key next steps for the next stage of the programme.
The ACP Board on 31 October also considered next steps relating to urgent primary care, following the CCG consultation between September 2017 and January 2018, which sought public input into the proposals to reconfigure minor illness and minor injury in Sheffield. Since the consultation, analysis was undertaken of the consultation feedback and a final report and recommendations were brought to the CCG Primary Care Commissioning Committee in September 2018. It was agreed that the approach and proposals would be reconsidered and options would be developed. Following that meeting the CCG team have started to re-evaluate the drivers and root causes for change to be able to clearly identify strategic objectives in improving urgent primary care and plan to continue this with partners and the public. The CCG team have noted that the drivers and root causes impact the whole health and care system. Therefore it was proposed and agreed at ACP Board on 31 October that:
o Strategic oversight will take place through the ACP work streams and Executive Delivery Group to ensure a joined up “system” approach. Further discussions will take place at EDG to work through the mechanics of this.
Enabling Workstreams Positive progress is being made for the delivery of a Sheffield Care Record and
improved Patient Flow. A workshop with CIO leads from Sheffield place partners was completed in October that supported the overall approach and identified priority actions to resolve. Formal initiation of the project is targeted for end October-18, with a Delivery Group meeting in November-18 for the first time. Work is ongoing across Sheffield, Barnsley place and the ICS to finalise an MoU for the delivery of Care Records and Patient flow in Sheffield and Barnsley (Linked by NHS England Business Case and same supplier in use). Target date for signature of the MoU is 1 November. Further communications and engagement activities are required to raise awareness and engage patients and professionals appropriately in the delivery of a Sheffield Care Record. The communications/engagement approach is in development and being based on exemplars such as Rotherham Health Record and the Leeds Care Record, as is the IG/Data Sharing approaches. Alignment between a Sheffield Care Record and the emerging work on Continuing Access to Care is being progressed.
The population analytics pilot commences on 1st September. This will provide good learning for the longer term requirements for the future. Sheffield ACP is linking into ICS work on this topic, alongside considering how the population analytics work and digital workstream need to collaborate. Both will be underpinning foundations of developing integrated care, learning from international case studies.
TRUST BOARD PART 1 6. 316/18 CHIEF EXECUTIVE REP... Page 69 of 247

The Pharmacy Work Stream is making good progress, with a clear focused set of priorities on medicines management, maximising the contribution of pharmacy within primary care and developing shared care. Improved digital inter-operability, matching prescribing pharmacist to system demand and developing community pharmacy provision are key foundations. The team will have crystallised the vision & headline programme plan by November 2018 when they will report back to EDG.
The Workforce programme is working on four priorities, with varying degrees of progress. The 12 week planning rapid planning cycle for an Older People’s workforce strategy commenced with support from GE Finnamore. This is a core part of the CQC Action Plan. A discussion regarding potential integration of the workforce and OD programme is taking place. In conjunction with the primary care workstream, the work on developing a primary care workforce strategy is commencing, with good learning from the GE Finnamore approach. Two bids have been submitted to Health Education England to bid for non-recurrent year end funds for the North region linked to this work.
A set of specific proposals on system development work, developed by the organisational development work stream were agreed by EDG on 9 October. Specifically these were:
o Leadership Development (with the Sheffield Liminal Leadership Programme to run twice yearly, with next course, from early 2019)
o Centres of Excellence (with each partner opening up one “exemplar” developmental activity to all partners)
o Microsystems Coaching Academy (with a commitment from VCSE and SCC to explore microsystem coaching capability to ensure a common QI language across the city)
o Identifying support for the ACP Board and Executive Delivery Group (to further develop system leadership skills within our most senior leaders, as individuals and as a team)
o Providing a bespoke OD offer to priority ACP delivery objectives (with neighbourhood development and person centred care two initial priorities).
The OD group will now start planning delivery, with commitment from all partners at EDG to provide resource to help deliver this.
Healthwatch have been appointed as the ACP VCSE partner on public and service user voice and will mobilise in November. Laura Cook from Healthwatch will work into the ACP team on this agenda from 12 November 2018. This contract will last for 12 months, with the funding source being ACP team pay slippage in 2018/19. This will provide a great opportunity to build the public and service user voice to the strategic and operational development of the ACP, alongside focusing on priorities, such as Older People’s experience (as captured by the CQC Local System Review).
iii. Cross-Cutting Risks A set of key themes around programme risks are taken from the highlight reports:
Risk Mitigation
Workforce Development – identified as top risk within Primary care work stream, and within pharmacy programme. Programme resourcing for the Workforce Programme is raised as a key risk.
Essential to have the 2 day a week ICS funded appointment in place. Post will be re-advertised.
TRUST BOARD PART 1 6. 316/18 CHIEF EXECUTIVE REP... Page 70 of 247

UEC have raised the risk of operational pressures impeding transformation work.
Review of links between transformation and performance aspects of workstream taking place
MH & LD, Primary Care work streams alongside other groups around the system have raised the importance of a robust system approach and leadership to neighbourhood development. It is identified as a key risk area by two work streams.
This requires greater system focus and is an identified priority by the CEOs. An initial ACP meeting took place 3 September to explore this, a second workshop planned for 26 October. A refreshed approach will be proposed thereafter.
Some programmes need still to develop greater clarity of focus and direction. The Long Term Conditions Programme in particular is identified by the Programme Director as a particular risk at this time.
Good initial stock-take in October – LTC programme now needs to define this programme and ensure a more robust approach.
Project/ programme management support to help drive programmes forward identified as risk in a number of programmes (primary care, workforce, LTC, elective, finance & payment reform) Mitigation outlined, but we need to start re-shaping some of our collective resource in line with ACP priorities in order to accelerate the system wide work
LTC: Support from Programme Director to crystallise shape of programme & prioritise
Primary Care: Deputy Director to provide support before dedicated project manager commences in post
Workforce Programme: Deputy ACP Director to support, ICS programme lead to be re-advertised.
Elective: cross system team in place – team need to find sustainable capacity following one colleague’s departure in December.
Payment Reform: dedicated system finance post to be advertised in October
Sheffield Care Record: Due to the commercial route to market being via a Barnsley Hospital Trust contract and a need for an MoU across Sheffield and Barnsley, there is a risk that this will delay deployment in Sheffield. Due to the need to establish a Sheffield Care Record alongside existing systems that professionals use, there is a risk that professionals will not adopt/use an integrated care record.
Full discussion on Sheffield Care Record planned at EDG in December 2018 to lift profile of work across all executive leads and ensure the programme team are supported to make rapid progress.
TRUST BOARD PART 1 6. 316/18 CHIEF EXECUTIVE REP... Page 71 of 247

3. Other Updates
i. Governance It was agreed on 31 October at ACP Board that an independent chair of the Sheffield
ACP should be appointed. This is to address the criticism from the CQC in the Local System Review that Sheffield had the same chairs for both the Health and Well-Being Board and the Accountable Care Partnership Board. Both are chaired by the CCG Chair and the Cabinet Member for Health and Social Care. The CQC saw the Health and Well-Being Board as accountable for the Local System Review and stated the HWB should be holding the ACP accountable for the delivery of the LSR Action Plan. They felt this responsibility was difficult to execute effectively due to both bodies have the same chairs. A series of options were considered by HWB and ACP Board in October and the conclusion was that an independent chair will be advertised.
Following legal advice, improved protocols for managing conflicts of interest will be issued during November to all workstreams.
It has been agreed that the governance for the Sheffield Outcomes Fund will fall within the Accountable Care Programme. Individual business cases are already aligned with individual workstreams.
ii. System Metrics As the overall population analytics work progresses EDG requires some system metrics
to determine whether progress is being made. Sandie Buchan (Head of PMO, CCG) has led this approach and developed an initial draft. This links to the wider Population Health work. This will report back to EDG in December 2018.
iii. ACP Team Recruitment Jane Ginniver commenced as Deputy ACP Programme Director for Development on 17
September.
Kathryn Robertshaw was appointed to the ACP Programme Deputy Director - Delivery on 1 October and will commence in post on 7 January 2019.
The ACP Finance post will be interviewed for on 5 November and the 1 year workforce ICS/and ACP responsibilities will be re-advertised shortly.
Conclusions and Recommendations The SCH Board is asked to note the above report. Paper prepared by: Rebecca Joyce, ACP Programme Director On behalf of: Kevan Taylor, CEO Chair of the Executive Delivery Group and
John Somers, CEO of SCH Date: 1 November 2018
TRUST BOARD PART 1 6. 316/18 CHIEF EXECUTIVE REP... Page 72 of 247

APPENDIX 1 [email protected]' NHS England Long Term Plan Engagement Team Skipton House 80 London Road London SE1 6LH To NHS England Long Term Plan Engagement Team Long Term Plan for the NHS: Consultation - NHS ENGLAND PUBLICATIONS GATEWAY REFERENCE: 08415 Sheffield Place Response Thank you for the opportunity to comment on the long term plan for the NHS. I am writing on behalf of the Sheffield Accountable Care Partnership comprising seven partners:
Primary Care Sheffield (our GP Federation)
Sheffield City Council
Sheffield Children’s NHS Foundation Trust
Sheffield Clinical Commissioning Group
Sheffield Health and Social Care Trust
Sheffield Teaching Hospitals NHS Foundation Trust
Voluntary Action Sheffield (the umbrella membership organisations for our Voluntary and Community Sector)
On behalf of the partnership I will respond to your three over-arching questions. Partner organisations across Sheffield have responded to some of the more specific chapters of the consultation.
1) What are the core values that should underpin a long term plan for the NHS? i. The factors that contribute to people’s health and wellbeing are multiple, complex
and intricately entwined; the majority are beyond the reach of traditional NHS services. The NHS needs to work in partnership with all interested partners, to ensure a whole pathway and population approach is taken. This includes public health, housing, social care, the voluntary sector and other partners that contribute to the wider determinants of health. We need to further shift our focus from treatment to keeping people well and focus on some of the key public health challenges – smoking, obesity and increasing physical activity.
ii. We need to change the current emphasis and political/ media debate and reorient our system to improving health & wellbeing from birth. This includes embedding the value of a whole family integrated working approach throughout the NHS.
iii. We need to commit to enabling an all age approach to care – for example in mental health. Transition between child and adult organisations remains a challenge locally and nationally across physical and mental health services. This value of more seamless “all age” care should underpin our approach – and mechanisms be developed to support this shift.
TRUST BOARD PART 1 6. 316/18 CHIEF EXECUTIVE REP... Page 73 of 247

iv. We need to embed a population approach through our NHS. This needs to be
accompanied by acceleration towards integrated commissioning and delivery, with supporting policy and legislation to aid this direction of travel. Rather than being an end in itself structural integration should follow transformation and increased integration in ways of working.
v. As a core value, we need much more explicit acknowledgment of the absolute inter-dependence between health and social care, with a policy environment that shifts us towards integrated delivery. Current policy and relative funding constraints between NHS and local government provide a context which gets in the way of providing joined up, best value care for the vulnerable populations receiving this care.
vi. We need to explicitly value the importance of the voluntary and community sector as a strategic and operational partner in our approach to care.
vii. We need to embed an outcomes focus as a key value within our approach, moving away from performance and financial system based more on activity based inputs and outputs.
viii. We need to be explicit about a core value of valuing our staff –and the social value of those that protect the most vulnerable in society – who “touch our lives at times of basic need where care and compassion are what matter most”.
ix. We also need to develop a culture across the NHS and Social Care that genuinely sees the relationship with its people/ citizens as one of equals, underpinned by a real commitment to co-production. This needs to build on pockets of good practice that exist within the statutory sector, but deliver a more cultural shift learning perhaps from the voluntary and community sector.
x. Collaboration and integration as key values needs to be supported by a policy environment that moves away from fragmentation and competition and helps build improving health and wellbeing into every area of local and national government policy to underpin our stated ambition towards integration and a greater prevention orientation. This should include health and well-being considerations being fully embedded in:
How we plan and design our towns
How we educate our children
Enable an environment that is conducive to good health
A wider societal culture that promotes good health xi. Finally, genuinely holistic, person centred care needs to be at the heart of our values
– with an expectation of care that reaches across organisations, and mental and physical health. This will require significant training and development of our workforce and an organisational and policy environment that helps provide the conditions for this shift. This needs to be in a set of values that explicitly aims to build the resilience of communities, families, societies to improve our collective health and well-being.
2) What examples of good services or ways of working that are taking place locally should be spread across the country?
A number of good practice examples of integrated working, or developments that more broadly support strategic and operational system wide development at place level are provided below.
TRUST BOARD PART 1 6. 316/18 CHIEF EXECUTIVE REP... Page 74 of 247

i. Our mental health trust Sheffield Health and Social Care NHS FT is significantly less dependent on inpatient care to support people with complex needs or experiencing a crisis and can share learning about intensive community focussed care, step up, down and crisis beds services delivered in partnership with the third sector. This long term strategic focus on delivering socially inclusive support and keeping people at home has involved long term commitment to developing innovative intensive workforce models and services to provide intense support to individuals in the community. This has improved experience and outcomes for service users, many of whom used to be cared for many miles from their homes and families, outside of Sheffield. The Sheffield system has a low bed base, low admission rate, below average lengths of stay, has almost eradicated out of town locked rehabilitation care, made significant investments in community services and also saved the health economy millions by repatriating patients from private residential providers and providing support in the community.
ii. We have developed pooled budgets and commissioning arrangements across Sheffield CCG and Sheffield Council for mental health. This involves a risk and benefit share agreement that includes Sheffield Health and Social Care NHS FT as our main mental health provider. This arrangement ensures all parties are inextricably connected both in terms of budgetary shares and how each respective budget is spent. This has moved to collective accountability and responsibility and “shared issues” across the system. For example, this has enabled us to simply split section 117 costs on a 50:50 basis meaning assessments are now focused on quality and outcomes not on who should pay for each element of care. Examples of genuine collaborative working include a city wide approach to perinatal, liaison and primary care mental health services.
iii. Our musculoskeletal care model is based on an integrated model of care underpinned by an outcomes based contract. Sheffield CCG and Sheffield Teaching Hospitals have moved away from Payment by Results, based on a transformed model of care, with an integrated virtual triage, enabling patient to be directed to the right service on receipt of referral. The model was co-designed with patients, carers and local patient groups, alongside staff from across community, primary secondary, independent and voluntary sector. Access to secondary care services has significantly improved through the changes, alongside genuinely integrated working across departments and sectors, to ensure patients get to the right place, first time. A patient reported outcomes framework and virtual care record, “My Pathway” has been implemented, which partners in the system intend to roll out to other models of care.
iv. Our single GP Federation for Sheffield (Primary Care Sheffield) is at the forefront of national primary care development. All practices that can are shareholders. This offers a significant strategic opportunity for Sheffield as a city to develop both GP practice and primary care more widely – and we look forward to sharing learning over the coming years.
v. We have made good progress in Sheffield on developing data sharing arrangements across the Local Authority and the NHS on a retrospective basis for analysis. This enables more whole system analysis, through our CCG and public health team.
vi. We have some good examples of collaborative working with the VCS sector including the WHO exemplar Age Better programme and Dance to Health. However, we have acknowledged the need as a place to develop a stronger strategic relationship with our VCSE partners and this is an ambition of our place arrangements.
vii. Our Sheffield Outcomes Fund approach, supported by central government with funds of £80 million over five years, offers an opportunity to test out the value of Social Investment Bonds as a means to pump prime public sector innovation and new
TRUST BOARD PART 1 6. 316/18 CHIEF EXECUTIVE REP... Page 75 of 247

outcomes based payment mechanisms. This offers innovation in investment and contracting for some of the most challenging areas facing both local and national government, such as mental health and homelessness. Sheffield would be interested in working with partners in central government to take the learning from the Sheffield Outcomes Fund and apply it to a major challenge facing the public sector, such as adult social care. Expanding the scale of this work, with the aim of identifying solutions in such an area, which would be of national interest, would be a natural progression. This would require the relevant central government departments/organisations to work alongside the public sector in Sheffield, and to contribute resources and funding to address the identified challenge. This would provide an opportunity both to draw on the lessons from the Sheffield Outcomes Fund, and work on a much larger scale than has been possible under the Fund. Such a piece of work could incorporate elements funded through SIBs and other funding options, and also could be an opportunity to use other innovative commissioning tools such as Innovation Partnerships.
viii. Expanding Improving Access to Psychological Therapies (IAPT) services to include a focus on people with long term conditions and persistent physical symptoms is a national programme of work set out in the ‘Five Year Forward View for Mental Health’ (Mental Health Task Force, 2016) Sheffield IAPT is a wave 2 site for IAPT-LTC expansion, and city’s new ‘Health and Wellbeing Service’ (HWS) commenced in October 2017. Commissioned by Sheffield Clinical Commissioning Group (CCG), the HWS service is working in partnership with the CCG, primary and secondary care, city council and community partners to deliver an ambitious and transformational service across ten conditional pathways:
Pain/Musculoskeletal (including Low Back Pain & Sciatica)
Respiratory (including COPD, Asthma)
Cardiovascular Disease (CVD) (including non-cardiac chest pain)
Diabetes (Type 1 and 2)
Cancer (following successful treatment)
Irritable Bowel Syndrome
CFS/ME/Fatigue
Generic Long-term Conditions (including Dermatology)
Persistent physical symptoms (or Medically Unexplained Symptoms)
Health Anxiety NHS-E have developed a case study about the low back pain course jointly delivered by colleagues in HWS and ‘Physioworks’ (Sheffield’s community physiotherapy MSK service) https://www.england.nhs.uk/mental-health/case-studies/chronic-pain-and-low-back-pain-pathway-at-sheffield-improving-access-to-psychological-therapies-iapt-service/ Considerable engagement and development work has been undertaken, to support full integration within all ten medical pathways. New health and wellbeing courses and individual support are available across the city.
3) What do you think are the barriers to improving care and health outcomes for NHS patients?
i. Despite recent investment in mental health care, the percentage of the wider NHS budget that is spent on mental health compared to the level of mortality and morbidity
TRUST BOARD PART 1 6. 316/18 CHIEF EXECUTIVE REP... Page 76 of 247

attributable to mental ill health remains very low. Challenges are compounded by the fact that there are long standing gaps in key strategic areas, in particular primary care mental health and a broader approach to emotional wellbeing for children and young people.
ii. Social care funding needs to be increased in line with health care funding and care systems need to be encouraged – either through policy or structural change – to ensure the local pound is spent in the best way – beyond what Better Care Funds were able to achieve. Otherwise investment in the NHS could be undermined is social care cannot meet resultant demand.
iii. We need to be honest and realistic about other areas of public sector reform and their implications for health – for example changes to benefit payments, and wider reductions in local government funding.
iv. We need longer term, cross-party planning at national level to plan and deliver long term improvements for health and well-being. We need to be supported to invest in and develop preventative services that address the wider determinants of health – even when results will not be seen for several years. This might include the development of bespoke housing solutions, investing in green space, encouraging our townscapes to focus on active travel, developing sustainable employment, investing in school based well-being and increasing early years investment.
v. The challenge of shifting our resource profile to provide more resources for prevention cannot be under-estimated. There is also a wide acknowledgement in Sheffield of the challenge of achieving this in the current regulatory and performance context given the importance of maintaining sustainability of all partners in an inter-dependent system. We need to develop a programme of provider payment reform that will better enable the aims of the integrated systems at place level to be met, and incentivise more outcome focused, preventative, population-based models of care.
a. The need for a shared financial strategy, aligned to population need is crucial if we want to achieve the stated ambition of integration.
vi. In this context, it is hard to underplay the critical importance of upfront transformation investment from central government. We note the around £500 million transformation fund that Greater Manchester received as part of their devolution arrangements. We would welcome additional transformation funding to enable the significant transformation programme we have planned.
a. We need to acknowledge the particular risk to sustainability faced by our secondary care providers in this context, and “double running” money will be essential to maintain business as usual and statutory and NHS Plan commitments to be met, as our system develops greater prevention orientation over the long term. It is vitally important this transformation funding reaches “places” when operating within larger footprint Integrated Care Systems such as South Yorkshire and Bassetlaw.
b. We often discuss the 80:20 rule of thumb between Place led transformation and South Yorkshire and Bassetlaw ICS level transformation, and need to be sure transformation investment reflects this split (and is directed in this way from NHS England). In central policy announcements we would welcome more emphasis on “places” within Integrated Care Systems, given the differences in size of ICSs (and therefore the varying profile/ significance of “place”) across the 10 frontrunner Integrated Care Systems.
vii. A lack of inter-operability between IT systems across providers and clinicians across health and care organisations is a major barrier to enabling integrated working across organisations and teams. Our frontline staff across the whole system, frequently raise
TRUST BOARD PART 1 6. 316/18 CHIEF EXECUTIVE REP... Page 77 of 247

this as an issue which gets in the way of providing the best, holistic care to the individual across primary care, secondary care, social care and other areas of public service delivery. This lack of inter-operability also causes significant duplication and inefficient work practice. Whilst some progress is being made within individual care economies, this remains a major barrier. Information sharing governance also gets in the way of better, integrated delivery and planning.
viii. Workforce planning, nationally, regionally and locally has historically been poor in the NHS and has led to significant workforce challenges, alongside a slowness to adapt agile, workforce planning processes. We need more expertise nationally to guide workforce planning for the long term, focusing on workforce supply and workforce innovation – to help shape new roles for our changing care models of the future. This will need a cross-sector focus (for example across social care and the NHS as well as within the NHS).
ix. The policy and regulatory environment at times appears confused. We await the developing merger of NHS England and NHS Improvement, and anticipate a regulatory and national policy context that clarifies the role with Integrated Care Systems. There is often considerable confusion for local leaders, and increasing challenges of delivering the organisational day job, alongside system roles, and different or duplicated messages from Integrated Care Systems, local Places and national bodies.
x. Local Consideration needs to be given to future architecture, system support and development. As part of this agenda there will be a shift in roles and responsibilities – and this is starting to be discussed locally. For example, specifically, what will be the future governance around a greater role for primary care and community, if this plays a much broader role in the future? We are interested to understand what help will be given by NHS England to develop systems on this journey of maturity.
xi. Procurement legislation is currently trailing the direction of health and care policy and gets in the way of developing integrated ways of working. We want to benefit from local providers’ relevant service experience, knowledge about the local context, and the cohorts we are targeting; and to benefit from this while proposals are being developed. We often want to develop care models for the long term, locally owned and locally designed and driven, but procurement rules currently get in the way of this integration rules and distract leadership attention to governance rather than transformation. However, the policy landscape is moving faster than the legal or commercial landscape here and it has, at times, felt unclear how to progress the work ‘safely’ in commercial, procurement and contracting terms.
xii. Further work on estates nationally would also help the changing context. Developing new approaches to where and how people access health and care services recognising there may be an increasing role for virtual, digital enabled access will be important. We would welcome further policy thinking and development in this area from NHS England.
xiii. There are also challenges for smaller providers, particularly in the voluntary and community sector. It is a more complicated process to engage in for voluntary sector providers and there is a strong sense that this is much harder for smaller local groups to do, potentially skewing the process towards bigger players.
I hope this response is helpful. Please do not hesitate to contact me if you have any queries. Yours Sincerely
TRUST BOARD PART 1 6. 316/18 CHIEF EXECUTIVE REP... Page 78 of 247

Rebecca Joyce Sheffield Accountable Care Partnership Programme Director cc. Sheffield Executive Delivery Group, ACP Paul Buckley, Deputy Director of Strategy and Planning, STHFT Yvonne Elliot, Deputy CEO, Primary Care Sheffield Maddy Desforges, Chief Executive of Voluntary Action Sheffield Anne Gibbs, Director of Strategy and Planning, STHFT Fiona Goudie, Clinical Director - Strategic Partnerships, SHSC Steven Haigh, Director, PCS James Henderson, Director of Policy & Performance, SCC Brian Hughes, Director of Commissioning, SCCG Jason Rowlands, Director of Strategy and Planning, SHSC Eleanor Rutter, Consultant in Public Health, SCC Mark Tuckett, Assistant Director of Public Sector Reform, SCC Nick Wilkinson, Clinical Lead & Consultant Clinical Psychologist, SHSC
TRUST BOARD PART 1 6. 316/18 CHIEF EXECUTIVE REP... Page 79 of 247

Integrated Care System CEO Report
SOUTH YORKSHIRE AND BASSETLAW SHADOW INTEGRATED CARE SYSTEM
9 November 2018
1. Purpose
This monthly paper from the ICS CEO provides an:
Update on the work of the ICS CEO over the last month Update on a number of key priorities not covered elsewhere on the agenda
2. Report – November 2018 2.1 ICS Performance Scorecard
The attached scorecards show our collective position at August 2018 as compared with other areas in the North of England and also the other ICSs. We continue to make good progress on our NHS Constitution commitments to our populations, though in line with other systems in England, we have seen our collective A&E performance dip. We have seen an improvement in our 31 day cancer standard (moving from 95.3% in July to 96% in August) but our 62 day cancer standard remains red (we are again reporting 82.9%) and we have also moved to red on diagnostics within 6 weeks. Teams across our organisations are working extremely hard to align our collective position, with remedial actions in place. This month’s scorecard also includes the ICS financial position, which is £3.4m ahead of plan (excluding Provider Sustainability Funding(PSF)) for the half year. This has secured £2m of the £5.7m of PSF linked to system financial performance. The place-based conversations to understand the good practice happening in Place and explore issues or areas where additional support would be helpful are now underway. Doncaster has volunteered to pilot the approach, which will enable a review and iteration of the process for future conversations in other places. The approach focuses on understanding the aspirations for local systems, the key issues, so that we can build on what is working well and bring about improvements through local support and mutual accountability. 2.2 ICS ways of working/governance review The first phase of engagement with our senior leaders in local authorities, CCGs and
Trusts, together with other partners and collaborations, on the current and potential future models for ways of working/governance is now complete.
The discussions set out refreshed partnership governance arrangements and ways
of working which reflected and built on:
The learning from the past two years
Appendix B TRUST BOARD PART 1 6. 316/18 CHIEF EXECUTIVE REP... Page 80 of 247

Our strong partnership history both in each place and across South Yorkshire and Bassetlaw
And the confidence there is in South Yorkshire and Bassetlaw, nationally, which has been recognized through significant investment coming into the region and each of our places, increased autonomy for NHS organisations and support as one of the first new system partnerships
Each conversation with senior leaders has built on the ‘strawman’ and explored how health and care partners within the system can re-set the context for working together. All partners agree that this means having the right forums for the right business and which ensure all partners continue to work within their current statutory duties.
The next phase of engagement will go back round all the senior leaders groups with the refreshed approach. It is anticipated that the new arrangements will start in April 2019.
2.3 Long Term Plan listening events ICS colleagues were invited to attend one of the two Long Term Plan events led by
Chief Executive of NHS England, Simon Stevens and Chief Executive of NHS Improvement, Ian Dalton last month.
As NHS England and NHS Improvement were keen to discuss the emerging plans to
help inform the final stages of the plan’s development. Key themes from the session included prevention, mental health, strengthening primary care networks and integration as the direction of travel.
Each ICS/STP will be expected to respond to the Long Term Plan with a five -year
strategic plan for the whole system. 2.4 Launch of the South Yorkshire and Bassetlaw QUIT Programme
The South Yorkshire and Bassetlaw QUIT programme is an innovative systematic intervention for people who are tobacco dependent, based on current best practice and research. It builds on learning from Canada and London, where similar hospital-based programmes had a significant impact on not only health outcomes, but also on short and medium term hospital re-admissions. Hospitals in SY&B see a large proportion of our population as patients each year, many of whom are admitted for at least several days. It is estimated that 25% of hospital patients are current smokers. Their admission period is a unique opportunity during which they could be supported to make one of the single most effective changes possible to improve their long-term health.
We recognise that working together at system level we will have a consistent approach and a clarity of message that can add real value. All our hospitals have appointed senior executive sponsors and are signed up to delivering the programme.
The launch takes place on Wednesday November 7th at St Mary’s Conference Centre in Sheffield. The system-wide commitment to the programme puts SYB alongside the fore- runners in taking tobacco dependency seriously, and is predicted to bring significant health and financial gains to the local system within a relatively short time period.
TRUST BOARD PART 1 6. 316/18 CHIEF EXECUTIVE REP... Page 81 of 247

3. Recommendation
The Collaborative Partnership Board is asked to note and discuss the update and Chief Executives and Accountable Officers are asked to share the paper with their individual Boards, Governing Bodies and Committees.
Date 2 November 2018
TRUST BOARD PART 1 6. 316/18 CHIEF EXECUTIVE REP... Page 82 of 247

ICS meetings in November Monday 5th CCG accountable officers: Oak House 1.30-3.30pm Acute Federation (committees in common): 722 1-5pm Tuesday 6th ICS Senior Executive Team: 722 9am-12pm Thursday 8th Elective and Diagnostics Steering Board: Barnsley Hospital 2-4pm Friday 9th Collaborative Partnership Board: 722 9.30am-11.30am Tuesday 13th Mental Health and Learning Disabilities Programme Board: Sovereign House 3.30-4.30pm Wednesday 14th ICS Directors of Finance: Sovereign House 1-4pm Friday 16th System Efficiency Board: Don Valley House 9-11am Monday 19th Urgent and Emergency Care Steering Board: 722 10.30am-12.30pm Tuesday 20th Executive Steering Group: 722 10am-12pm Discovery Workshop: The Source 1-5pm Tuesday 27th ICS Senior Executive Team: 722 9am-12pm Mental Health and Learning Disabilities Workshop: Sovereign House 1-5pm Wednesday 28th Joint Committee CCGs: 722 3.30-5.30pm Thursday 29th Elective and Diagnostic Executive Steering Group: 722 2-4pm Friday 30th Hospital Services Review Hosted Networks 3: 722 2-5pm
TRUST BOARD PART 1 6. 316/18 CHIEF EXECUTIVE REP... Page 83 of 247

7. 317/18 QUALITY COMMITTEE

REPORT TO THE TRUST BOARD OF DIRECTORS’ MEETING (PART 1) HELD ON 27 NOVEMBER 2018
REPORT FROM THE QUALITY COMMITTEE
Trust aims supported by this paper
Provide high quality patient experience and outcomes Empower motivated and compassionate staff Lead improvements in paediatric care
Link to Board Assurance Framework
Failure to effectively deliver healthcare impacts on the safety and quality of patient experience, regulatory compliance and loss of confidence of the wider community
Purpose of the paper To present to the Trust Board of Directors the key issues arising from the 19 November 2018 Quality Committee. Summary of key points All reports are available for members of the Board to view on Convene.
The following reports were noted by the Quality Committee for information/assurance; Annual Report from the Child Death Overview Panel Presentation on Outpatient Department Improvements Quarterly Safeguarding Report Quarterly Report from the Director of Infection Prevention and Control Resuscitation Committee Annual Report Report from the Guardian of Safe Working Hours Quarterly Report from the Accountable Officer for Controlled Drugs Update from the Recovery and Transformation Board Discharge Summaries – Position Statement Clinician Accountability for Safeguarding: Action Plan NHS Plan: New Learning Disabilities Standards Report on Transition Plans for Patients Over 18 CQC unannounced Visit Reports Update on Progress on Transition in Surgery and Critical Care Division Monthly Clinical Quality Dashboard Update on Serious Incidents Nursing Establishment Committee Oversight of Delivery of the Board’s Well-Led Action Plan
Verbal updates were noted by the Quality Committee on the below items for information/assurance; Quality Impact Assessments CQC Action Plan Update
From the Committee’s consideration of agenda items presented for discussion it was agreed that the following would be reported to the Trust Board:
Quarterly Safeguarding Report As part of the quarterly report the committee received a progress update to provide assurance that safeguarding was discussed at multidisciplinary team meetings. Whilst there had been progress
TRUST BOARD PART 1 7. 317/18 QUALITY COMMITTEE Page 85 of 247

within some teams to embed discussions within team meetings, the level of compliance across the Trust was unclear. This would be followed up to ensure discussions happened within team meetings. The committee also raised concern on the lack of progress to backfill capacity support currently provided by the Trust as part of health support to the Sheffield safeguarding hub, noting that this continued to impact on the Trust’s achievement of its key performance indicators. Progress of the business case would be followed up with the partner organisation. Report from the Guardian of Safe Working Hours The committee received assurance on progress to resolve concerns highlighted to Trust Board. HR Manager support was now in place to support the Guardian to receive the correct information, and trainee’s access to exception reporting software had been resolved. This would be highlighted to Board for their assurance that concerns had been resolved. Discharge Summaries – Position Statement The committee discussed actions to improve compliance which currently fluctuated around 80 per cent against a target of 100 per cent for completion of discharge summaries within 24 hours. Whilst the committee supported a move towards no discharge summary no discharge to improve rates it recognised the practicalities of doing this and impact this would have on flow of patients at the current time. Completion of discharge summaries was important from a quality of care perspective. Further work was needed on processes to reduce duplication and ensure that electronic systems aligned which would improve rates. This would remain an area of continuing focus. Report on Transition Plans for Patients Over 18 The committee received an update on the issue of live transition plans for patients over 18. Whilst these patients had valid reasons for continuing to receive care by the Trust within their care pathway, and services had transition plans, the issue related to not having a central database for these patients, and committee emphasised the importance of evidencing that plans were in place for valid reasons. The committee acknowledged progress to date however there was still more to do, and a gap analysis would be undertaken. An update on progress to establish a central database would be brought to the December meeting.
The following items were approved by the Committee;
Resuscitation Policy Limitation of Treatment Agreements Policy CP1513 Patient / Parent / Carer HDU Support Workers Only - Administration of Medication Policy Private Patients Policy Trust Safeguarding Committee Terms of Reference Care Experience Board Terms of Reference
Board Action required The Trust Board is asked to note the items for escalation from the meeting held on 19 November 2018.
Author: Ms P Mitchell, Non-Executive Director – Chair of the Quality Committee TO NOTE
TRUST BOARD PART 1 7. 317/18 QUALITY COMMITTEE Page 86 of 247

8. 318/18 FINANCE AND RESOURCESCOMMITTEEAppendix A - to follow

REPORT TO THE TRUST BOARD OF DIRECTORS’ MEETING (PART 1) HELD ON 27 NOVEMBER 2018
REPORT FROM THE FINANCE AND RESOURCES COMMITTEE
Trust aims supported by this paper
Empower motivated and compassionate staff Build clinical and financial sustainability
Link to Board Assurance Framework
Risk that we do not maintain financial stability due to failure to deliver our financial plan or the negative impact of movement to a system-wide financial planning regime, resulting in requirements for additional CIPs or reduction in level and standard of services.
Failure to ensure that the Trust has a motivated, suitably trained and engaged workforce impacts on operational performance, transformational change and achievement of strategic objectives.
Failure to ensure that the Trust recruits staff in the right numbers and with the appropriate breadth of skills and competencies to deliver high quality services now and in the future.
Risk that insufficient leadership capacity and capability prevents necessary transformational change Failure to ensure that the required IT infrastructure and strategy is in place to deliver clinical services
and support clinical strategy and transformation impacts on the Trust's ability to deliver services, improve quality and transform services.
Failure to develop our leadership, management and governance arrangements to ensure delivery of sustainable high quality person-centred care, support learning and innovation, and promote an open and fair culture prevents the Trust from demonstrating it is a Well Led organisation
Operational capacity constraints and failure to deliver transformation impact on our ability to deliver planned activity and manage demand impacting on operational efficiency, service quality and financial performance.
Failure to manage the Trust’s cash position would result in the Trust not being able to satisfy its obligations in respect of pay and non-pay costs.
Purpose of the paper
To present to the Trust Board of Directors the key issues arising from the 21 November 2018 meeting of the Finance and Resources Committee.
Summary of key points
The following routine reports were noted by the Finance and Resources Committee for information/assurance:
o Month 7 Integrated Performance Report o Update from the Recovery and Transformation Board o Month 7 Headline Finance Report, Including Escalations from Cash Management Committee
and Project Board o Update on Financial Planning 2019/20 o Committee Oversight of Delivery of the Board’s Well-Led Action Plan
From the Committee’s consideration of agenda items presented for discussion it was agreed that the following would be reported to the Trust Board:
TRUST BOARD PART 1 8. 318/18 FINANCE AND RESOUR... Page 88 of 247

Month 7 Integrated Performance Report The committee noted the trust had met all its local and national key performance indicators, this position had been reported to NHS Improvement at their recent quarterly review meeting. The committee received a summary of activity to achieve the Trust’s strategic aims. The committee would consider how waiting times to first appointment within CAMHS fitted within RTT 18 week wait rules at a future meeting. This issue had been highlighted by the recent unannounced CQC inspection, and was a national issue within CAHMS services which was causing confusion. The Trust was supported by commissioners in relation to how its performance was measured, however further investigation of the regulations nationally would be undertaken before bringing back to a future meeting. The number of outstanding clinical guidelines and policies continued to be tracked, these were being systematically worked through. The committee requested identification of an end date in place. The committee supported the quality committee monitoring progress of this indictor. Recovery and Transformation Programme The committee received an update on workstream activity in particular relating to service improvements. The programme was progressing however risks to the financial delivery of the programmes remained for the second half of the year. The committee welcomed medicine and surgery and critical care now moving to a weekly governance review with executives given the ongoing challenges in each division, and to identify actions to improve their financial position. The committee noted realistic planning of activity for 2019/20 was essential. Month 7 Headline Finance Report The committee noted the reported position had fallen slightly behind plan, with concern in relation to the November position. A mitigations plan was in place however risks remained. Update on Financial Planning 2019/20 The committee noted the key dates of the national timetable. These are shown in Appendix A. Flexible Endoscope and Stacker Systems in Theatres The committee recommended approval of the business case to Trust Board and following discussion supported the recommendation to lease equipment. The committee also recognised the 18/19 capital budget should reduce by the exact same amount if the lease model was agreed, and would recommend this option to the Board for approval. Private Patients Scoping Exercise and Outline Proposed 5 Year Strategy (2019/24) The committee received a report following a recent scoping exercise and outline of a proposed strategy. The steering group would be reformed to appraise options available to the Trust, and to ensure that no NHS patients would be displaced should the strategy be progressed. The terms of reference of the reformed steering group and any ‘red lines’ for the strategy would be brought back to the January meeting. A plan and framework would be developed and brought back to a future meeting for further consideration, and the committee noted the importance of linking the private patient strategy with the communications and marketing strategies. Marketing and Communications Strategies The strategies were interlinked; both were endorsed by the committee for approval by Trust Board as part of their annual review. Next phase plans would be brought back to the committee. Internal Estates Capital Projects Scheme delivery The committee was assured that the Trust had the internal capabilities to successfully deliver major capital projects within the estates department, following a restructure and strengthening of the team to support a number of capital project schemes currently in development. There were no actions for the Finance and Resources Committee to accept on the cross working actions arising report.
The following item was approved by the Committee on behalf of the Board; Raising Concerns Policy
Board Action required
TRUST BOARD PART 1 8. 318/18 FINANCE AND RESOUR... Page 89 of 247

The Trust Board is asked to note any key issues arising from the Finance and Resources Committee held on 21 November 2018.
Author: Mr A Baker, Non-Executive Director (Chair of Finance and Resources Committee) TO NOTE
TRUST BOARD PART 1 8. 318/18 FINANCE AND RESOUR... Page 90 of 247

APPENDIX A
1. Key Actions Next Month
Business cases to Business Planning Committee – 23 November Finance at ADs meeting to discuss and agree key planning principles – 27 November First cut high level efficiency plans to PMO – 30 November Share activity plans with commissioners – 30 November Capacity funding requests to Corporate Planning Team – 5 December Divisional cost pressure submissions to Finance – 7 December December TEG paper update on key planning elements - 12 November
TRUST BOARD PART 1 8. 318/18 FINANCE AND RESOUR... Page 91 of 247

TRUST BOARD PART 1 8. 318/18 FINANCE AND RESOUR... Page 92 of 247

9. 319/18 RISK AND AUDIT COMMITTEE

REPORT TO THE TRUST BOARD OF DIRECTORS’ MEETING (PART 1) HELD ON 27 NOVEMBER 2018
REPORT FROM THE RISK AND AUDIT COMMITTEE
Trust aims supported by this paper
This paper supports the delivery of all the Trust’s aims through ensuring that the Trust is well governed.
Link to Board Assurance Framework
Failure to effectively deliver healthcare impacts on the safety and quality of patient experience, regulatory compliance and loss of confidence of the wider community
Purpose of the paper
To present to the Trust Board of Directors the key issues arising from the 14 November 2018 Risk and Audit Committee.
Summary of key points
All reports are available for members of the Board to view on Convene.
The following reports were noted by the Risk and Audit Committee for information / assurance:
Exception Report – Risk Register
Serious Incident Reports and Root Cause Analysis Investigations – Action Plan Update
Quarterly Report on Unresolved Claims
Minutes of the 23 July and 19 September 2018 Finance and Resources Committee
Minutes of the 16 July and 17 September 2018 Quality Committee
Routine review of Board Assurance Framework to Inform Presentation to Board
Quarterly Monitoring of Emergency Planning, Resilience and Response Compliance – Action Plan
Local Counter Fraud Specialist Progress Report
Internal Audit Progress Report
Quarterly Report on Unresolved Claims
Review of Board Standing Orders, Standing Financial Instructions and Scheme of Delegation
Financial Reporting
Risk Management Strategy
External Audit Technical Update
TRUST BOARD PART 1 9. 319/18 RISK AND AUDIT COMMI... Page 94 of 247

It was agreed that the following points from review of these reports would be highlighted to the Trust Board:
Risk register – The committee reviewed the risk register, and a small number of long term risks were reviewed in detail. These would be picked up with divisions and the Executive Risk Management Committee to receive assurance on the continued management of these risks. The risk register would also be aligned to the Board Assurance Framework.
Serious Incident Report – The committee reviewed the report. To provide assurance to the committee that actions were being progressed each division would review outstanding serious incidents at their December performance and quality meetings before reporting back to the committee. If progress continues to be slow the committee will consider revising the escalation process to get the assurance that incidents are being actioned. The committee will continue to monitor progress on a regular basis.
Well Led action plan – The committee reviewed each action allocated for its oversight, there was good correlation of evidence to show progress. The next steps would be to ensure there were action plans in place following identification of any gaps. The committee recognised, as part of the next stage, it was important to understand well led from a service perspective.
Emergency Planning and Resilience Response compliance – The Trust had self-assessed against revised NHS core standards for Emergency Planning, Resilience and Response, and had declared non-compliance, due to changes in the core standards and having a vacant the Emergency Planning Officer post. The committee had sought assurance on progress against actions to address compliance, and noted the Emergency Planning Officer was now in post and was progressing actions to achieve compliance. Progress would be reviewed quarterly by the committee with the expectation that the majority of the issues would be dealt with by end January 2019.
Review of Board Assurance Framework (BAF) – The committee noted the overview of the BAF, and a verbal update would be provided to Board following the committee’s recommendations to update a number of areas, capture discussions by the committee within the review of BAF 5 and BAF 7 and mitigations in place. The BAF would also be updated to reflect scores against the Care Quality Commission key lines of enquiry in respect of quality and review of how quality sat within the BAF especially reflecting findings from recent CQC visits. In particular The Director of Nursing was considering the BAF areas and scores relating to CWAHMs (Becton and the Community teams).
Internal Audit Progress Report – Completion of follow up actions was reported at 58 per cent. Outstanding follow up actions had been reviewed by divisional performance and quality review meetings and this position was improving. Internal audit stressed the importance of completing follow up actions as it is one of factors taken into account in forming their overall opinion (needs to be >75%). The committee supported escalation of the issue to ensure the importance of completing follow up actions was recognised by divisions.
Quarterly report on unresolved claims – The committee considered the report noting a number of unresolved claims were historic, and requested that a report providing detail of high value claims were brought to the next meeting to provide background, how they linked to serious incidents and lessons learned reports, to provide a better understanding of the claims.
Review of board standing orders, standing financial instructions and scheme of delegation – A current review of the constitution, standing orders, standing financial instructions and scheme of delegation was taking place. The committee supported proposed changes to tender limits to align with partners across Sheffield; these would be incorporated into the review.
Financial reporting – The committee noted clarity would be given in relation to the authority to sign off single tender waivers within the review of the scheme of delegation and standing financial instructions. The committee also noted updates against two entries on the gifts and hospitality report; these had been considered and staff advised to decline the gifts in line with Trust policy.
Risk Management Strategy – The strategy was considered and the committee recommended approval by the Board, subject to a number of minor amendments and strengthening of the wording within the training chapter. The committee recognised the importance of the Board being able to describe the risk management process and how it fitted with the BAF, and a flow chart would be developed.
External Audit Technical Update – The committee noted 2019/20 planning discussions had commenced and that planning guidance would be brought to the January meeting.
TRUST BOARD PART 1 9. 319/18 RISK AND AUDIT COMMI... Page 95 of 247

The following were presented to the Committee for discussion:
Discussion on Key Strategic Risk – BAF 7 and BAF 5
o BAF (7) "Failure to engage effectively with partner organisations and the local community threatens the ability of the Trust to deliver its strategic ambition."
o BAF (5 “Risk that insufficient leadership capacity and capability prevents necessary transformational change to deliver efficient, high quality services.”
Key points from discussion to be noted / further discussed by the Board include:
BAF 7 – Following a detailed discussion of the risk and mitigations in place. The current rating of the risk was supported. A strategic discussion was required at Trust Board level to be clear on the strategic ambition of the trust as a provider of paediatric healthcare across the ACP and implications. The CEO will identify a number of key areas to be considered.
BAF 5 - A full review of the risk had been undertaken by the Chief Executive. The committee recommended re-rating the current risk as likelihood 4, and recognised that the risk was being managed however there was still further work required to achieve the target rating of likelihood score 2. A further strategic discussion would take place with Trust Board, which would consider capability and capacity within the organisation, stepping up of performance and avoiding duplication of resources. Cost probably needs to be incurred (~£750K / £1m pa) to attain results and consideration needed whether redeploy certain resources, recruit or bring in expertise to help (Capacity Vs Capability). These discussions and mitigations would be captured within the next review of the BAF.
The Risk and Audit Committee accepted the cross working actions arising report: The Finance and Resources Committee would continue to track progress of the NHS Improvement financial governance action plan as part of the Committee’s oversight of the recovery and transformation programme.
Board Action required The Trust Board is asked to note the items for escalation from the meeting held on 14 November 2018.
Author: Mr J Cowling, Non-Executive Director - Chair of the Risk and Audit Committee TO NOTE
TRUST BOARD PART 1 9. 319/18 RISK AND AUDIT COMMI... Page 96 of 247

10. 320/18 BOARD ASSURANCEFRAMEWORK

REPORT TO THE TRUST BOARD OF DIRECTORS’ MEETING (PART 1) HELD ON 27 NOVEMBER 2018
BOARD ASSURANCE FRAMEWORK QUARTER 2 REVIEW
Trust aims supported by this paper
The paper supports the achievement of all Trust aims by ensuring that the Trust is well governed.
Link to Board Assurance Framework
The paper contributes to the development of the Board Assurance Framework.
Purpose of the paper
The paper provides the Board of Directors with assurance that key, high level risks agreed by the Board relating to the delivery of the Trust’s strategic objectives are being managed appropriately. Summary of key points The Board Assurance Framework (BAF) has been reviewed by Executive colleagues and changes are highlighted in the document in blue. Alignment is demonstrated between entries on the risk register and the 12 high-level risks identified on the BAF. A review of risk register entries with the Trust Risk Manager has identified all risks with a score of 12+ that have a direct link with achievement of the Trust’s strategic objectives. A Standard Operating Procedure (SOP) has been produced which details the process adopted to ensure that the BAF is updated ensuring that the document continues to be a helpful tool to Committee and Board members as part of the broader corporate governance framework. It has also been agreed that the review process for the BAF will be strengthened. This will include scrutiny of the relevant sections of the BAF at the Finance and Resource Committee and the Quality Committee on a quarterly basis with a review of the full BAF at Executive Briefing, Risk and Audit Committee and Board on a quarterly basis. The Audit and Risk Committee meeting on 14 November carried out a deep dive of two BAF risks which the Chief Executive presented:
- BAF 5 – Risk that insufficient leadership capacity and capability prevents necessary transformational change.
- BAF 7 – Failure to engage effectively with partner organisations and the local community threatens the ability of the Trust to deliver its strategic ambition.
Further work is required to map over the additional controls and assurances given in the presentations and identified during the meeting. This will be undertaken as part of the next executive review. The Committee recommended a change to the current rating of BAF 5, increasing the likelihood from 3 to 4 in view of the need for embedding of additional corporate resource following approval of recent investment. Board is asked to agree the change to the rating. At the Executive Briefing meeting on 11 October 2018 the Executive Directors conducted a high level risk review of the BAF. Executives reviewed the top three risks on the BAF to establish if these accurately reflected the key risks to the organisation in relation to delivery of the Trust’s strategic objectives. Recognising that the Trust’s top three BAF risks focus on financial viability, cash and leadership further work will be undertaken during the next executive review to ensure that risks to quality are fully covered off and given sufficient prominence.
TRUST BOARD PART 1 10. 320/18 BOARD ASSURANCE ... Page 98 of 247

Board Action required The Board is asked to:
(1) Note the Board Assurance Framework following discussion at the most recent Risk and Audit Committee.
(2) Agree to change BAF 5’s rating to C=5, L=4 = 20.
Author: Mr M Kane, Associate Director Corporate Affairs TO NOTE
Executive Sponsor: Mr J Somers, Chief Executive
TRUST BOARD PART 1 10. 320/18 BOARD ASSURANCE ... Page 99 of 247

Sheffield Children's NHS Foundation Trust Board Assurance Framework last updated - Nov 2018
BOARD ASSURANCE FRAMEWORK
2018/19 Issue 1.0
BAF RISKSNo. of
Independent Assurances
Inherent R
isk
Inherent R
isk Effectiveness of Controls
Target
Risk
Current R
isk No. of Trust Assurances
BAF (1) DNQ Failure to effectively deliver healthcare impacts on the safety and quality of patient experience, regulatory compliance and loss of confidence of the wider community. 16 8 12 25
%
98
BAF (2) CFORisk that we do not maintain financial stability due to failure to deliver our financial plan or the negative impact of movement to a system-wide financial planning regime, resulting in requirements for additional CIPs or reduction in level and standard of quality of our services.
20 16 20 17%
40
BAF (3) DHR Failure to ensure that the Trust has a motivated, suitably trained and engaged workforce impacts on operational performance, transformational change and achievement of strategic objectives. 20 10 15 12
%
34
BAF (4) DHR Failure to ensure that the Trust recruits staff in the right numbers and with the appropriate breadth of skills and competencies to deliver high quality services now and in the future. 16 6 12 9
%
27
BAF (5) CEO Risk that insufficient leadership capacity and capability prevents necessary transformational change to deliver efficient, high quality services. 20 10 15 9
%
20
BAF (6) DSO Risk to clinical service viability due to failure to meet nationally defined standards or changes to the commissioning and / or configuration of services. 16 12 16 4 11
BAF (7) CEO Failure to engage effectively with partner organisations and the local community threatens the ability of the Trust to deliver its strategic ambition. 12 8 8 14 22
BAF (8) MDFailure to engage with our clinicans prevents the development / implementation of an effective clinical strategy to deliver high quality services that responds to the needs of patients and other health / social care partners and prevents us from capitalising on the use of research, innovation and technology.
15 4 12 7%
32
BAF (9) DSOFailure to ensure that the required IT infrastructure and strategy is in place to safeguard patient safety, deliver clinical services and support clinical strategy and transformation impacts on the Trust's ability to improve quality and transform services.
16 10 15 10%
20
BAF (10) CEOFailure to develop our leadership, management and governance arrangements to ensure delivery of sustainable high quality person-centred care, support learning and innovation, and promote an open and fair culture prevents the Trust from demonstrating that it is a 'Well Led' organisation.
12 6 12 16%
41
BAF (11) DSO Operational constraints and failure to deliver transformation impact on our ability to deliver planned activity and manage demand impacting on operational efficiency, service quality and financial performance. 16 9 12 5
%
14
BAF (12) CFO Failure to maintain the Trust's cash position would result in the Trust not being able to satisfy its obligations in respect of pay and non-pay costs. 20 12 20 3 11
% one or more sources of assurance - limited or none# BAF (10) controls are collated into Well Led action plan
BAF RISKSNo. of
Independent Assurances
Inherent R
isk
Inherent R
isk Effectiveness of Controls
Target
Risk
Current R
isk
27 11 0
6 11 1
11 3 0
5 9 0
6 11 0
2 5 1
16 5 0
19 1 0
5 7 0
0 1# 0
88 4 0
5 0 0
Board Assurance Framework 1
TRUST BOARD PART 1 10. 320/18 BOARD ASSURANCE FRAMEWORK Page 100 of 247

11. 321/18 NURSING ESTABLISHMENT

REPORT TO THE TRUST BOARD OF DIRECTORS’ MEETING (PART 1) HELD ON 27 NOVEMBER 2018
Nursing Establishment Review
Trust aims supported by this paper
Provide high quality patient experience and outcomes Empower motivated and compassionate staff
Link to Board Assurance Framework Failure to effectively deliver healthcare impacts on the safety and quality of patient experience,
regulatory compliance and loss of confidence of the wider community Failure to ensure that the Trust has a motivated, suitably trained and engaged workforce impacts on
operational performance, transformational change and achievement of strategic objectives. Failure to ensure that the Trust recruits staff in the right numbers and with the appropriate breadth of
skills and competencies to deliver high quality services now and in the future. Risk that insufficient leadership capacity and capability prevents necessary transformational change Risk to clinical service viability due to failure to meet nationally defined standards or unfavourable
changes to the commissioning of services Failure to develop our leadership, management and governance arrangements to ensure delivery of
sustainable high quality person-centred care, support learning and innovation, and promote an open and fair culture prevents the Trust from demonstrating it is a Well Led organisation
Purpose of the paper To present to the Trust Board of Directors the Nursing Establishment report for 2018. Summary of key points
The current, budgeted nursing establishment is sufficient to deliver safe and quality care The introduction of e-Roster and safe care acuity module is providing consistent information about
staff levels versus the acuity of patients
A number of new initiatives have an unknown or limited known impact in future therefore close monitoring through the recommendations proposed is essential.
Action required
The Board is asked to review the report and recommendations, as considered by the November Quality Committee.
Author: Mrs C E Harness Deputy Director of Nursing FOR ASSURANCE
Executive Sponsor: Mrs S Shearer Director of Nursing and Quality
TRUST BOARD PART 1 11. 321/18 NURSING Page 102 of 247

1
Sheffield Children’s NHS Foundation Trust
Nursing Establishment Review of Clinical Inpatient Wards October 2018
Introduction The National Quality Board (NQB) produced guidance on the assurance of safe staffing levels in 2016 in response to recommendations from the Francis report. The document ‘How to ensure the right people, with the right skills, are in the right place at the right time – A guide to nursing, midwifery and care staffing and capability’ clearly outlined the responsibilities of NHS Trust Boards in assuring safe staffing levels. Many other documents produced at this time outlined the correlation between deficiencies in nurse workforce numbers and adverse standards of patient care In June 2018 the NQB released the document ‘Safe, Sustainable and Productive Staffing’ an improvement resource for children and young people’s inpatient wards in acute hospitals. The aim of the document is to provide a systematic approach to identifying the organisational, managerial and ward factors that support safe staffing. The document identifies 6 key elements which should be considered under any review, they are:-
feedback from service users what is important to them and how well their needs are met
a systematic and evidence based approach to number and skill mix required use of valid acuity tools exercise professional judgement benchmarking with peers taking account of national guidelines
The last establishment review was undertaken in June 2017 with 11 recommendations. Of the recommendations made the bed manager team was strengthened to minimise the use of ward managers at weekend. Electronic rostering and the safe care patient acuity tool has been introduced on the acute in patient wards, with mental health developing its own acuity tool based on available evidence. Becton expenditure has been monitored and all bank and agency is now captured through eRostering. Senior nurse meetings monitor vacancies and sickness across all nursing areas. In addition ward 6 (formally M3) and ward 5 (formally S2) have had full establishment reviews in light of increasing patient acuity and evidence staff levels were insufficient to deliver appropriate care, both areas have had an increase in registered and non-registered staff. Following the move of 3 wards to the new building information is available on the impact on staff levels The purpose of this paper is to:-
Review current establishments against demand using a retrospective review of the previous year
Assess establishments using the safe care patient acuity data Make recommendations as a result of the review outcomes
This review will take into account the four lodges at Becton, the four remaining inpatient wards on the acute side, the Emergency Department, Paediatric Critical Care Unit and the Neonatal Surgical Unit. Wards 5 and 6 will be considered as required following full review earlier in the year.
TRUST BOARD PART 1 11. 321/18 NURSING Page 103 of 247

2
The review will use a variety of information to inform the paper including current establishments, bed occupancy rates for 2017/18, acuity data taken from Safe Care within the eRoster system, nationally recognised patient to staff ratios and observational feedback from the ward and department managers. Ward and lodge information In April 2018 wards 1, 2 and 3 moved into new ward areas with a substantial increase in the ratio of cubicle to open bay beds and an increase in footprint of the overall size of the ward
Old ward in square
metres New ward in square
metres S1 450 1 2000 S3 503.06 2 and burns 1159.92 Burns 100 X M2 690.75 3 2000 The table below describes the ward number of beds and current budgeted establishments Ward/department Beds Band
2 Band 3
Band 5
Band 6
Band 7 Band 8a
Total
Ward 1 24 2 5.57 18.05 8.5 1.6 0 35.72 Ward 2 & burns 22 1 8.71 26.5 10.13 2.6 0 48.94 Ward 3 24 4.53 2 20.94 8 1.6 0 36.77 Ward 4 20 3.64 3.23 18.27 5 1.6 0 31.54 Ward 4* 24 - - - - - 0 NSU 11 0 1.78 17.63 12.04 5.28*** 0 36.73 ICU/HDU 10/9 0 6.4 50 28.5 11.5 1 96.4 ED/AAU 14
AAU 2 5.8 28.7 11.71 8.2 1 56.41
MDC 8 0 1 3.4 0.8 0.8 0 6 *potential increase to 24 beds when ward moves from current location to new area with larger footprint The striking factor in comparing the 4 medical and surgical wards is the higher number of bands 3, 5, 6 and 7 on ward 2 and burns. This is as a result of the combining of the wards when moved into the new building. However caution is required when interpreting and comparing the figures. As part of the national Burns standards at least 1 nurse on each shift is required to be a holder of a specialist burns qualification. Currently there are a limited number of staff who hold this and plans are in place to increase the number but this will take a period of approximately 18 -24 months. It should also be noted that as well as the 4 commissioned burns beds the service can have up to 12 burns dressings each day which require a separate nurse to review and manage care. These patients are currently seen within the ward area but once moved to the OPD as planned in the reconfiguration of services they will be completely separate to ward staff numbers. The band 7 figure reflects the ward and department managers and educator hours. The ward managers are supernumerary. However there is a point of caution in that they already fill short term gaps on rotas and therefore there is an element of cost saving when bank is not used.
TRUST BOARD PART 1 11. 321/18 NURSING Page 104 of 247

3
There may be capacity to reduce ward manager supernumerary time in future, however the Trust is about to enter the first winter in the new build, with the aforementioned increase in footprint and increased cubicle capacity which currently remains untested. Additionally, the Trust has strengthened medication administration procedures following a review of nationally accepted practice and an external review of CQC readiness by KPMG. From December 2018 all medications are to be double checked by Registered Nurses and measures have been put into place to ensure that medication cupboards are only accessed by Registered Nurses. This will have increased Registered Nurse workload on wards and departments. PCCU and ED have band 8a lead nurses with responsibility for the wider management of the whole service and less of the day to day operational management which is undertaken by band 7 nurses. Whilst not part of this overall review, following the previously agreed investment earlier in the year, ward 6 has a band 8a lead nurse but no band 7 operational nurses and as such is an outlier with its structure. The impacts of operational issues are therefore dealt with by the lead nurse which does impact on their ability to take a wider strategic view of this specialised commissioned service. Bed occupancy 2017/18 This figure is as calculated at midnight by the number of patients occupying a bed throughout the organisation. Caution is required when reviewing the figures as the length of stay for children is often very short and the through put on 1 bed could be 2 or occasionally 3 patients in a 24 hour period. The figure however will only represent 1 patient in the bed at midnight thus masking the actual activity undertaken in a 24 hour period. The figures provide an overview of the peaks and troughs experienced throughout the year. 2017/18 is comparable to 2016/17 over the acute site wards and departments but within the mental health lodges shows some significant variation. This can be accounted for in 2017/18 by the patient population and the impact their acuity had on being able to admit to full capacity. 2017/2018 % Occupancy
April May June July Aug Sept Oct Nov Dec Jan Feb Mar
M1 (4) 77 67 64 73 64 67 72 74 69 64 78 66 M2(3) 76 74 78 74 61 78 81 85 78 81 84 68 M3 (6) 76 71 76 77 62 71 87 73 74 77 86 76 S1 (1) 79 68 68 62 64 84 79 75 72 71 81 76 S2 (5) 95 95 89 80 92 98 96 82 70 77 82 93 S3 (2) 69 63 66 59 64 72 75 72 61 62 82 62 Burns 63 64 61 57 43 51 45 72 44 52 33 32 ICU 74 75 63 67 56 57 57 67 61 55 77 62 HDU 32 32 35 24 24 33 45 55 55 65 58 52 NSU 85 82 83 89 87 87 85 77 70 70 67 77 All Wards 74 69 69 67 63 72 75 74 68 69 77 68
TRUST BOARD PART 1 11. 321/18 NURSING Page 105 of 247

4
Registered to unregistered ratio September 2018 Patient to nurse ratios are recommended according to guidance issued by the professional bodies including the RCN (2013), PICS standards (2015) BAPM standards (2010) Burns standards (2012) Time to move on (2014) They state that for ward based care a ratio of 1 nurse to 4 patients if they are aged 2 years or older, under 2 years the ratio is 1:3 For critical care areas the ratio is widely accepted as Level 3 critical care 1:1 Level 2 critical care as 1:2 Level 3 critical care as 1:3 This standard relates to a standard level of care delivery which will need to be increased if additional factors occur, such as tracheostomy care, safeguarding issues, mental health or learning disability are identified as an unmet need. As well as ratios of nurses per patient there are recommendations for the ratio of registered and unregistered staff within wards and departments. For general wards this is 70% registered to 30% unregistered For critical care areas this is 85% registered to 15% unregistered with an establishment of 7.01WTE nurses per bed for level 3 care. This includes a 25% uplift to cover sick, study and maternity leave. In addition critical care, neonatal care, and burns care require a level of qualified in speciality nurses per shift and per patient numbers depending on acuity. Another significant but challenging area to measure is the care provided by parents. Family centred care can have a positive and a negative impact on nurse staffing levels. Physical and emotional support is given to patients by families, but equally families themselves can require a lot of attention and support whilst their child is hospitalised.
Ward Unregistered WTE
Registered WTE
Total staff Unregistered %
Registered %
1 7.57 28.15 35.72 21 79 2 and Burns
9.71 39.23 48.94 20 80
3 6.53 30.24 36.77 18 82 4 6.67 24.87 31.54 21 79 NSU 1.78 34.95 36.73 3 97 PCCU 6.4 90 96.4 7 93 ED/AAU 7.8 48.61 56.41 14 86 MDC 1 5 6 17 83 Table showing Registered: Non registered staffing ratios. Ward 5 and Ward 6 is excluded from this review as separate establishment reviews were approved in February and May 2018. The reviews are included in Appendix 1 Sickness and maternity leave data The Trust target for sickness absence is 4% and the uplift for maternity leave is 1% As detailed below for the 6 month period from 1st April 2108 information taken from the eRostering system shows a significant number of wards experienced levels of
TRUST BOARD PART 1 11. 321/18 NURSING Page 106 of 247

5
absence up to 4 times higher than the Trust target. This has a substantial impact on the ability to maintain safe staffing levels on a day to day basis. Maternity leave is consistently above the 1% allowance. This is built into the uplift given. As temporary maternity leave cover contracts are unattractive the Trust mitigates this issue by over recruiting staff during recruitment drives. Sickness Apr May June July August September Ward 1 3.12% 5.03% 2.49% 7.91% 6.55% 2.77% Ward 2 & Burns 6.81% 6.42% 6.86% 9.48% 8.46% 10.17%
Ward 3 2.76% 2.32% 3.49% 5.06% 4.31% 7.37% Ward 4 5.14% 2.48% 0.30% 3.37% 5.26% 5.03% Ward 5 4.51% 9.05% 10.30% 7.64% 5.17% 4.25% Ward 6 4.03% 4.00% 13.08% 17.97% 16.40% 12.10% NSU 3.59% 1.43% 1.81% 2.21% 3.46% 3.40% ED 2.70% 1.90% 0.70% 1.60% 3.80% 5.10% PCCU 7.20% 5.50% 6.10% 6.10% 9.50% 6.70% MDC 6.30% 3.00% 11.10% 7.00% 0.20% 1.00% MAT Leave Apr May June July August September Ward 1 6.80% 7.10% 6.30% 7.20% 6.60% 6.10% Ward 2 & Burns 2.20% 4.30% 3.90% 4.70% 8.60% 4.70%
Ward 3 6.50% 6.00% 5.40% 5.40% 3.60% 3.50% Ward 4 10.40% 8.80% 5.50% 1.80% 2.70% 4.50% Ward 5 7.80% 8.60% 7.10% 10.60% 10.80% 9.90% Ward 6 5.90% 7.00% 8.80% 7.40% 4.20% 5.50% NSU 13.30% 14.10% 12.40% 10.70% 9.60% 8.00% ED 7.30% 6.60% 3.70% 4.50% 3.60% 4.70% PCCU 6.50% 6.90% 4.70% 4.80% 3.20% 2.60% NB There was no maternity leave for MDC over the 6 month period. Acuity data for 6/12 from 1/4/18 to 30/9/18 Safe Care was introduced on wards 1-6 and NSU as part of the Allocate health roster suite of tools. This tracks patient acuity over a 24 hour period through information provided by ward staff at 4 set time points, using the modified Shelford group paediatric acuity assessment tool. It should be noted that not all wards commenced safe care from 1/4/18 which will account for some gaps in the data. The following graphs show the spread of patients from 1st April 2018 to 30th September 2018. Not all wards commenced at the same time and there are gaps when insufficient or no data has been submitted. These are typically displayed as zero points on the graphs or very low scores followed by a significant increase. As this collection has been in place for 6 months or less it is too early to use as a tool for assessing any trends in patient types but does provide an overview of the acuity patients accessing services. With 1 years data the organisation will have a better understanding of season related trends and other influences to inform future establishment reviews.
TRUST BOARD PART 1 11. 321/18 NURSING Page 107 of 247
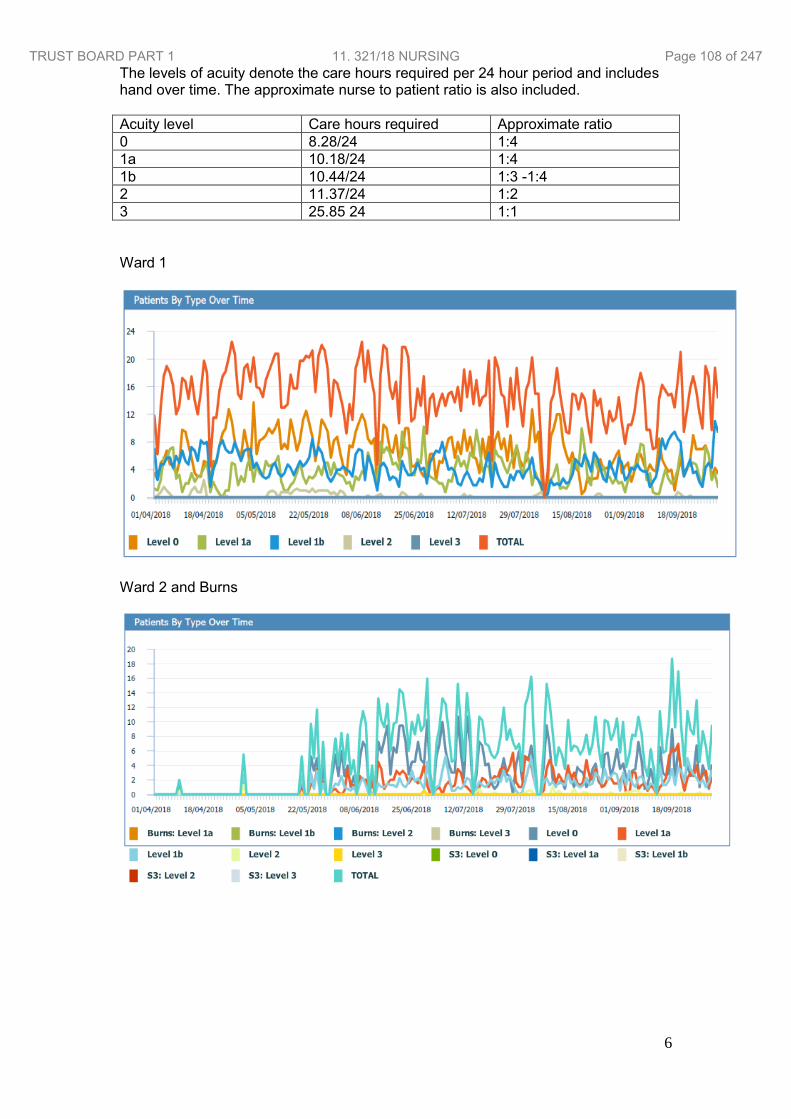
6
The levels of acuity denote the care hours required per 24 hour period and includes hand over time. The approximate nurse to patient ratio is also included. Acuity level Care hours required Approximate ratio 0 8.28/24 1:4 1a 10.18/24 1:4 1b 10.44/24 1:3 -1:4 2 11.37/24 1:2 3 25.85 24 1:1 Ward 1
Ward 2 and Burns
TRUST BOARD PART 1 11. 321/18 NURSING Page 108 of 247

7
Ward 3
Ward 4
Ward 5
TRUST BOARD PART 1 11. 321/18 NURSING Page 109 of 247

8
Ward 6
NSU
Rostered demand and required care versus average bed occupancy As a Health Roster module, Safe Care is able to correlate nurse staffing levels against patient acuity data. The following graphs show the correlation between the rostered staff, patient acuity and the average bed occupancy. A significant point to note is that all wards with the exception of ward 5, show correct staffing levels when average occupancy is between 70% - 80%. With the exception of NSU, most wards reflect 70-80% as a midnight bed occupancy. Daytime variation is managed on a shift by shift basis by the site management team. The introduction of the eRoster system has produced transparency for annual leave allocation, shift allocation of substantive staff, the use of bank workers, and the number of unused hours available each month of the substantive workforce. Detailed work is being undertaken to understand the context of the figures in each are. The
TRUST BOARD PART 1 11. 321/18 NURSING Page 110 of 247

9
challenge required back to managers is to ensure that shifts are filled as per rostering policy. There may be the potential for more flexible use of the work force once more information is available, showing acuity trends across a week, month and season. Ward 1
Ward 2 and Burns
TRUST BOARD PART 1 11. 321/18 NURSING Page 111 of 247

10
Ward 3
Ward 4
TRUST BOARD PART 1 11. 321/18 NURSING Page 112 of 247

11
Ward 5
Ward 6
The graphs show a variance between positive and negative figures throughout the reporting period. This can be attributed to the number of inpatients during the day and the changes in their acuity over the 24 hour period. There appears to be a correlation between bed occupancy and the establishment available related to the acuity of the patients. I.E. when occupancy is high, staff levels show as insufficient to meet the demand and vice versa. The acuity is factored into the variance graph points.
TRUST BOARD PART 1 11. 321/18 NURSING Page 113 of 247

12
Incidents and Complaints A measure related to safe staffing levels is the number of recorded incidents and the context within which they occurred. Medication errors, specifically delayed medications can be an indicator of staffing problems. In the 6 month period from 1st April 2018 to 30th September 2018 there was one recorded delay directly related to staff workload. On review there was no impact on the patient’s physical health but the potential for increased stress for the patient and family was high. There are minimal complaints made about insufficient nurses on duty to provide care. Comments are made however about how busy staff appear to be. In the year April 2017 to March 2018 there were a total of 4 serious incidents where patient observation was noted to be suboptimal. It was not identified as a root cause in any of the cases but it was noted as contributory factor in the investigations. None of the reports identify staff levels as being insufficient however patient acuity was not being measured using the safe care module and therefore information would have been less accurate. Over the same period there were 29 occasions whereby staffing levels were reported as insufficient for the patient work load. There were 2 main themes, that of raised patient acuity and short term late notice sickness. In all cases mitigations were put in place to maintain patient safety. Since the introduction of Datix on the 1st March 2018 the number of incidents related to delayed or missing observations was 6. All incidents were investigated and reported as part of the learning process to minimise future risk of reoccurrence. Friends and family test information Positive feedback from patients and their families is an important indicator of how well a ward or department is performing. Safe staffing is a key component of a patient experience. Over the 6 months from April 2018 the total of unlikely and extremely unlikely to recommend care responses on Friends and Family Test data was between 4% and 6%. Less than 1% of the reasons given for this response related to nurses and nursing. The overwhelming patient and family response regarding nursing was positive. Examples of comments received include:- All staff on every ward are absolutely amazing and go out of their way to help in any way they can. Thank you all The nurses/HCAs/housekeeper are fabulous and amazing! The care from you all has made our stay a pleasant one with lots of support to help us at a difficult time Very good - thank you for helping and supporting me Staff excellent. They took care of my grandson and my daughter. Thank you. Friendly, helpful staff. Good communication with us regarding our child's care
TRUST BOARD PART 1 11. 321/18 NURSING Page 114 of 247

13
New workforce models The development of the Trainee Nursing Associate role will commence in January 2019. Eight current support workers will commence this training. Once qualified, they will have the skills and knowledge to be able to accept a patient workload over seen by the registered nurse. This will include medication administration. There is a cost pressure of 0.4 WTE x 8 for the duration of the course allowing for study days and off site experience which has been agreed by the Trust Executive Group. This workforce will be banded at Band 4 once training is completed. They will replace band 5 Registered Nurses. Further work is required to decide how far this workforce is grown. Ward and department manager feedback The level of professional judgement used to assess what is a safe level of staffing in any situation alongside the factual evidence is essential and is recognised in the National Quality Board 2018 guidance. Ward managers report that if all staff were in post and present as rostered, establishments are sufficient to provide safe quality care. Their feeling is that high levels of maternity leave alongside the unpredictability of sickness absence make shift fill challenging.
0%10%20%30%40%50%60%70%80%90%
100%
ExtremelyLikely
Likely Neither Unlikely ExtremelyUnlikely
Don't Know
Friends & Family Test Results - Quarter 1 2018/19
Apr
May
Jun
0%10%20%30%40%50%60%70%80%90%
100%
ExtremelyLikely
Likely Neither Unlikely ExtremelyUnlikely
Don't Know
Friends & Family Test Results - Quarter 2 2018/19
Jul
Aug
Sep
TRUST BOARD PART 1 11. 321/18 NURSING Page 115 of 247

14
Wards 1, 2 and 3 all report concern over staff welfare and their visibility to patients and their families due to the increase in size of the wards. Ward managers have raised concern over the introduction of the two registered nurse check for all drugs from 3rd December 2018. Whilst they fully understand the safety reasons behind the introduction and support it they are concerned over potential delays in other care delivered. The MDC manager raised concern that a variety of factors impact on their ability to accurately calculate the numbers of MDC staff required on any one day as the service is used by specialist nurses for specific work which impacts on space. The comparison with other children’s hospital services for medical day care does show the organisation is below staff numbers found in these organisations. Staff continue to be moved across acute wards to ensure safe staffing on every shift Heads of Nursing and Matron feed back The Heads of Nursing and matrons have reviewed findings and will work on the recommendations to provide information for future reviews. Conclusion Over the last year a significant amount of work has been undertaken in implementing and embedding the eRoster and safe care acuity module. The data these systems are now providing need to be reviewed when years’ worth of information is available looking for themes and trends in particular seasonal variations. The Trust does over recruit to cover sickness and maternity leave however this does not have a major impact as other staff leave and some change their minds and do not join the Trust. The impact this is having on the delivery of safe patient care, should continue to be monitored and escalated by both the ward managers and Heads of Nursing. The winter season and the move to the new wards and the introduction of changes in practice such as two nurse checking of all drugs, are unknown quantities in terms of their impact on staff to deliver safe, quality care. The Trust will need to review them in quarter 1 2019 or earlier if issues are highlighted. Overall the Trust has sufficient nurses within the budgeted establishments to deliver safe, quality care. However the challenges of sickness absence, maternity leave and changes in environment and practices mean that over the following months the recommendations below must be undertaken to confirm or refute this fact. Recommendations
Check and challenge meetings to be held 1-2 monthly between ward/department managers, divisional management and eRoster manager to question rostering practices
Use of a rolling advertisement as well as the targeted advert for the twice yearly newly qualifying students.
In April 2019 review of the ratio of registered to unregistered staff with a view to increasing the support worker team utilising the Calderdale framework service review process.
Future work on the role of nursing associates within the organisation must continue with plans for further cohorts to be employed and utilised across the organisation once qualified
MDC to continue the work started on understanding patient types, length of stay, care required and the correlation with staff required.
TRUST BOARD PART 1 11. 321/18 NURSING Page 116 of 247

15
Ward 4 review if the bed base increase to 24 from 20. Potential need for increase in bands 3 and 6 when compared to other 24 bedded wards.
Review ward 2 and burns in April to see if staffing can be reduced/realigned with other wards
Commence work looking at recording red flags to highlight and escalate staffing challenges and their impact on the delivery of safe patient care.
Employment of a band 7 sister/charge nurse for ward 6 to support the Lead nurse role and provide daily operational leadership. This will allow the lead nurse to undertake the wider Trust and Regional responsibilities associated with the role and be consistent with other lead nurse posts within the trust e.g, Paediatric Critical care
Costs
Band 7 ward manager is required for the oncology and haematology services. Midpoint costs for a band 7 nurse with on costs but no unsocial hour’s payments are £46,470 per annum. The division of Medicine have an overall budget of £14.2m for nursing which has a forecast underspend of approximately £900K by year end which would support the introduction of this role. However this is offset by a predicted over spend across all substantive posts and the associated agency costs of £0.8m. This would result in a cost pressure for the division.
References National quality Board (2016) How to ensure the right people, with the right skills, are in the right place at the right time – A guide to nursing, midwifery and care staffing and capability’ National quality Board (2018) Safe, sustainable and productive staffing. An improvement resource for children and young people’s inpatient wards in acute hospitals Royal College of Nursing (2013) Defining staffing levels for children and young people’s services National Burns care standards (2013) PICS (2105) Quality standards for the care of critically ill children BAPM (2010) Service standards for hospitals providing neonatal care RCPCH (2014) High dependency care for children – time to move on
TRUST BOARD PART 1 11. 321/18 NURSING Page 117 of 247

12. 322/18 TRUST STRATEGIES- Communications Strategy- Marketing Strategy- Risk Management Strategy

REPORT TO THE TRUST BOARD OF DIRECTORS’ MEETING
(PART 1) HELD ON 27 NOVEMBER 2018
COMMUNICATIONS STRATEGY 2018 - 2021
Trust aims supported by this paper
Provide high quality patient experience and outcomes Empower motivated and compassionate staff Lead improvements in paediatric care Build clinical and financial sustainability Discover new ways of improving child health through research, innovation and technology
Link to Board Assurance Framework Failure to effectively deliver healthcare impacts on the safety and quality of patient experience,
regulatory compliance and loss of confidence of the wider community Risk that we do not maintain financial stability due to failure to deliver our financial plan or the
negative impact of movement to a system-wide financial planning regime, resulting in requirements for additional CIPs or reduction in level and standard of services.
Failure to ensure that the Trust has a motivated, suitably trained and engaged workforce impacts on operational performance, transformational change and achievement of strategic objectives.
Failure to ensure that the Trust recruits staff in the right numbers and with the appropriate breadth of skills and competencies to deliver high quality services now and in the future.
Risk that insufficient leadership capacity and capability prevents necessary transformational change Risk to clinical service viability due to failure to meet nationally defined standards or unfavourable
changes to the commissioning of services Failure to engage effectively with partner organisations and the local community threatens the
ability of the Trust to deliver its strategic ambition Failure to engage with our clinicians prevents the development / implementation of an effective
clinical strategy that responds to the needs of patients and other health and social care partners and prevents us from capitalising on the use of research, innovation and technology
Failure to ensure that the required IT infrastructure and strategy is in place to deliver clinical services and support clinical strategy and transformation impacts on the Trust's ability to deliver services, improve quality and transform services.
Failure to develop our leadership, management and governance arrangements to ensure delivery of sustainable high quality person-centred care, support learning and innovation, and promote an open and fair culture prevents the Trust from demonstrating it is a Well Led organisation
Operational capacity constraints and failure to deliver transformation impact on our ability to deliver planned activity and manage demand impacting on operational efficiency, service quality and financial performance.
Failure to manage the Trust’s cash position would result in the Trust not being able to satisfy its obligations in respect of pay and non-pay costs.
Purpose of the paper To present to Board with the draft Communications Strategy for approval. Summary of key points
TRUST BOARD PART 1 12. 322/18 TRUST STRATEGIES - ... Page 119 of 247

Effective communication is key to the success of any organisation. Whether it is communication with
children, young people, parents, carers, staff, potential employees, referrers, regulators or our partner organisations, a good flow of information is vital.
This strategy sets out the Communications priorities over the next three years, in order to effectively support the organisation’s aims and objectives in a coordinated way.
Care was taken at each stage to ensure that the objectives of the Communications Strategy directly support the objectives within the Trust’s overall strategy.
To develop this plan, previous activity has been analysed, the current progress assessed, previous requests from staff and patients have been considered, Board member comments noted and discussions have taken place with members of the Executive Team. In addition, early drafts of this strategy’s key objectives have been shared with the Trust Executive Group (TEG) and feedback taken on board.
The proposed areas of work allow the Trust to build on the progress the Trust has made over the last four years, through the implementation of the previous strategy.
The strategy includes three core objectives – profile raising, staff engagement and communications,
and supporting recruitment
Objective 1 Profile Raising – To further develop the regional, national, international reputation of Sheffield Children’s as a specialist provider
Objective 2 Internal Communications and Engagement – To give staff a greater sense of
belonging and involvement with the Trust, by developing a shared staff engagement approach and continuing to strengthen internal communications.
Objective 3 Recruitment – To support the recruitment of the best possible staff through
comprehensive and engaging recruitment materials, and bespoke support for hard-to-recruit roles
The actions that will be taken to support each of these objectives are listed within the strategy.
Each year there will also be a small number of agreed projects and campaigns. Each will have its own dedicated communications plan. In year 1 these are identified as:
o Transformation (whole programme) o Modernising Outpatients o Theatres Well Prepared o CQC inspection
In addition to planned activity, the team will continue to manage reputational issues as they arise.
Progress reports will be provided to TEG on a monthly basis, and to Finance and Resources every
six months. Finance and Resources Committee Action required
To approve this strategy as the direction for communications activity over the next three years.
Author: Lea Fountain, Associate Director of Communications FOR APPROVAL
Executive Sponsor: Steven Ned, Director of HR and OD
TRUST BOARD PART 1 12. 322/18 TRUST STRATEGIES - ... Page 120 of 247

1 – Introduction 2 2 – Looking back at 2014-2018 2
2.1. Overview 2 2.2. Internal communications 3 2.3. Corporate identity 4 2.4. Strategic approach 6 2.5. Priority campaigns 8 2.6. Unplanned communications
3 - Objectives 2019-2021 9 3.1. Objective 1 - Profile raising 9
3.2. Objective 2 - Internal Communications and Engagement 10 3.3. Objective 3 – Recruitment 12 3.4. Year 1 projects 13
4 – Key messages 13 5 – Audiences 14 6 – Channels 14 7 – Measures 15 8 – Risks 15
Caring Together Communications Strategy 2018-2021
TRUST BOARD PART 1 12. 322/18 TRUST STRATEGIES - ... Page 121 of 247

Effective communication is key to the success of any organisation. Whether it is communication with children, young people, parents, carers, staff, potential employees, referrers, regulators or our partner organisations, a good flow of information is vital. This strategy sets out the key areas of focus for Communications over the next three years, in order to effectively support the organisation’s aims and objectives. To develop this plan, previous activity has been analysed, the current progress assessed, previous requests from staff and patients have been considered and discussions have taken place with members of the Executive Team. In addition, early drafts of this strategy’s key objectives have been shared with the Trust Executive Group (TEG) and feedback taken on board. Care was taken at each stage to ensure that the objectives of this strategy directly support the objectives within the Trust’s overall strategy. While this Communications Strategy won’t prevent unplanned urgent matters – which will be prioritised as required – it allows a coordinated, sustained and results-driven approach, targeted specifically to the areas the Trust has identified as of primary importance for its current work and future plans.
Supporting Trust Aims and Objectives
In pursuit of a shared vision “to provide a healthier future for children and young people”, the objectives of Sheffield Children’s NHS Foundation Trust are as follows.
Provide high quality patient experience and outcomes Empower motivated and compassionate staff Lead improvements in paediatric care Build clinical and financial sustainability Discover new ways to improve children's health
2.1. Overview
Sheffield Children’s last Communications Strategy was developed in 2014. It included a range of objectives all of which contributed to delivering the same over-arching goal: building a structured and effective communications service. As well as achieving the objectives set out in the strategy with measurable results during implementation, this work
1. Introduction
2. Looking back at 2014-2018
TRUST BOARD PART 1 12. 322/18 TRUST STRATEGIES - ... Page 122 of 247

has created a stable base which will provide many benefits as we look to develop further over the course of the next strategy. The 2014 strategy had three core strands: improving our internal communications, ensuring a clearer corporate identity and developing a more strategic approach – both more strategic in the way the communications function operates and ensuring communications activity is more closely aligned to the strategic objectives of the Trust as a whole. Strong progress has been made in all three areas, as reported in more detail below.
2.2. Internal communications
Staff communication plays a vital role in the effectiveness of any organisation. Staff need to understand the objectives of an organisation if they are to support their delivery on a daily basis. They need to understand new developments, whether structural changes or implementation of new ways of working. They need to be engaged with numerous projects, from having their flu jab, to coming up with money saving ideas, to completing their PDR. They need opportunities to feedback to senior leadership with their views and ideas. They also need to be equipped with the right information to help them be ambassadors for the Trust, whether at home in the community or out at professional events. Significant progress has been made to strengthen our internal communication approach including:
Developing a new intranet that’s easier to use and includes tools to make the working life of staff simpler
Developing a regular schedule of face-to-face Open Meetings which is published months in advance and includes a range of locations and times to suit all staff
Restricting access to “everyone on email” to reduce the bombardment of information, saving staff time and making it easier for them to find the information they do need
Developing new email groups to help target information to the right place, either by location or professional group
Introducing the new Weekly Digest, to bring together the core information each week into a single place
Introducing a new fortnightly newsletter about learning and development called “The More You Know” to highlight educational opportunities, provide mandatory training reminders and highlight the importance of PDRs
Evolving the newsletter New Wing News into Building Our Care, providing a suitable way of highlighting improvements and developments being made in the Trust, not just those linked to physical construction work
TRUST BOARD PART 1 12. 322/18 TRUST STRATEGIES - ... Page 123 of 247

Working with the Illingworth Library to convert frequent sporadic messages into a weekly newsletter highlighting the support and tools available to clinicians and promoting evidence-based practice
Developing a clear schedule of publications, to better manage the flow of information
Coordinating the organisation of the Star Awards, developing a bigger and better event to celebrate the achievements of staff and significantly increasing the number of nominations each year
Trialling Cascade, a new team briefing system Improving access to our annual reporting through the development of infographics
and live coverage of members meetings via social media This work has proved effective in improving staff sense of feeling informed, as the staff communications survey demonstrated at the end of 2016. This found that:
Staff felt more informed about what is happening in the Trust. 24% said they felt well informed, an increase of 2% on 2013, while 67% felt reasonably informed. Only 9% felt uninformed, down from 11% in 2013
More staff find communications useful and interesting. 56.1% of staff always found communications useful or interesting, compared to 20% three years earlier. A further 40.2% said things were useful or interesting some of the time
Other successes include:
Hundreds of staff have attending open meetings every quarter Strong read rates for core publications 5206 bookings for courses have been made by staff via the intranet 5590 online PDR declarations have been made by staff More than 100 staff submitted transformational ideas The introduction of a clinic booking tool was awarded the Star Award for “Service
Improvement of the Year 2018” Despite this success, there is still much more that can be done to improve internal communication and engagement, so this will remain a priority area for the course of this new strategy. Priorities will include non-digital communication (including print and face-to-face), particularly for clinical groups, and more support for managers to help them communicate effectively with their teams.
2.3. Corporate identity
In 2014, there was a lack of clarity in the Trust’s corporate identity. Visually, there was no consistency and many materials were developed without professional input. There was also confusion with the naming for our specialist hospital – which was sometimes called Sheffield Children’s Hospital and sometimes called The Children’s Hospital, Sheffield.
TRUST BOARD PART 1 12. 322/18 TRUST STRATEGIES - ... Page 124 of 247

The Trust had a good reputation within the local area, but was less known further afield. Where it was known, it tended to be for the compassion of staff, but less known as an organisation with world-class expertise. Over the last four years the Communications Team has:
Developed a clear and simple new visual identity, including a colour palette and guide to implementation
Used the new identity for all centrally produced materials Relaunched the website in line with the new identity. The content of the site was
also significantly redeveloped and restructured to make it more user friendly, guided by feedback from young people, parents and staff
Developed templates to support staff to create materials that are clear and in line with brand, such as the template research poster developed in coordination with the research team
Created a consistent tone of voice for social media channels, whilst also ensuring high quality and engaging content
Developed a regular stream of case studies and features about the specialist care offered by Sheffield Children’s – ranging from the expertise shown in lifesaving surgeries to the stories of the care and compassion shown by staff
Developed improved links with regional television companies and several national production companies, helping get the stories of Sheffield Children’s broadcast more widely
Strengthened links with The Children’s Hospital Charity to ensure a more coordinated approach. This included agreeing consistent name and brand rules
Supported services with the development of materials to support a range of projects – such as conference promotional materials for the Healthy Minds programme, training materials for the Neurodisability training course and display materials about children’s services for an Accountable Care Partnership (ACP) event
Supported services with management of reputational issues, to protect the reputation of the Trust whilst also ensuring actions are honest and compassionate, in line with Trust values
Results of this work include:
Extensive positive media coverage including articles in national and international publications including the Huffington Post, The Sun, The Daily Mail, Mail on Sunday, the Telegraph, the Guardian, the Independent, The i, The Daily Express, The Mirror and The Times, appearances on national programmes including BBC Breakfast, ITV News and The One Show, a lead role in the popular Channel 4 series Secret Life of 4 and 5 Year Olds and the BBC children’s series Operation Ouch, interviews and features on national radio including Radio 4 and LBC, and as well as numerous articles, features and other content in specialist publications (such as the Nursing
TRUST BOARD PART 1 12. 322/18 TRUST STRATEGIES - ... Page 125 of 247

Times, HSJ, Children and Young People Now), magazines, regional publications and on television
A growing following on social media, with some content seen by hundreds of thousands of people. Over the course of the strategy period follower numbers on Twitter increased by 87% and Facebook likes increased by 22% – despite an ever more challenging Facebook algorithm. The most popular post reached more than a million people
By working with families interested in giving feedback, boosted the Trust’s rating on Facebook from 3.5 to 4.8 out of 5 and on NHS Choices from 3 to 4
By optimising website content and making information easier to find, there have been 1.8million visits to the website, where people have viewed 4.9million pages, an increase of 140% and 75% respectively compared to the four years before the strategy was in place.
Services have reported increases in calls about referrals as a result of communications activity
Thousands of people have been recruited for research studies through new research leaflets, poster templates, social media and work with partner organisations. Some studies have reached more than 10k people on social media, others have directed more than 1k people to the Trust’s research page. The most successful promotion – a research study into slings and baby carriers – directly resulted in 1,473 people taking part and completing the study.
There are still some areas of service-produced information that do not use the identity, and this will be worked on over the course of the next strategy. The work of the last four years has significantly increased the profile of the Trust’s specialist services. However there is potential to grow this much further over the next strategy period. The relationships that have been developed with media and the production companies will prove incredibly helpful as we take these next steps. The additional resource within the team to support video making will also support the Trust to become a stronger broadcaster in its own right. More work will also be put into building reputation with other clinical professionals, to increase referrals and boost recruitment.
2.4. Strategic approach
Before 2014, the communications service was predominantly reactive. Media releases were sent to local media outlets with no specific objective beyond securing coverage. Campaigns and messages were sent out by request, rather than based on a coordinated plan or any particular reference to the Trust’s overarching strategy. Publications were issued, but timing varied and no clear description of purpose sat behind them – a vagueness which sometimes came across in the content. Over the last four years the Communications Team has:
TRUST BOARD PART 1 12. 322/18 TRUST STRATEGIES - ... Page 126 of 247

Developed the Communications Strategy, which was directly linked to the Trust’s strategic priorities
Developed a full Emergency Communications Plan, including recruiting and training volunteer communications support officers to support in crisis situations
Refreshed action plans on a regular basis to reflect changing priorities and new challenges, in coordination with the Executive Team and Trust Executive Group (TEG)
Developed an annual programme of campaigns, agreed each year by TEG Worked with partner organisations to ensure a more coordinated approach –
including partner charities, local health organisations, Sheffield City Council, the Sheffield universities and regulators
Supported the development of the Trust Strategy in 2018, including helping organise opportunities for staff to contribute to the process, helping to develop phrasing in the strategy to ensure it was reflective of the feedback from staff and meaningful to colleagues whatever their role and developing its visual identity
Provided detailed reports on activity to TEG every month, reporting activity directly against the agreed objectives. Extensive reports also provided to Board via the Finance and Resources Committee every six months
Acted as a coordinator for numerous Trust projects, including closure of the Emergency Dept doors (with the associated replacement of close to 200 signs), the Bus Boost scheme (which has seen more than 100 staff get free travel to work, and is now offered to all new starters), patient entertainment (securing a free Sky contract saving £9k per year and a DVD library from Disney, with perpetual screening rights, with the DVDs alone worth £5K) and sponsorship (securing £5,5k to support the Star Awards and £500 to support the Clinical Summit)
Coordinating official visits, including MPs, the regional Mayor, the Deputy Prime Minister, the Secretary of State for Health, sports personalities, children’s TV stars, a rapper and Disney characters. An Official Visits Policy was developed to support this work, which includes ensuring safeguarding and infection control processes are followed, appropriate senior leadership is involved and schedules are coordinated with staff in clinical areas (often via play staff)
This work has meant there is now a strong clarity of purpose for the Communications Team. This has helped to prioritise the work of most significance to the Trust and ensure far greater impact for key projects. It has also given clear ways for TEG members and others to measure the effectiveness of the team and to evaluate progress against pre-agreed goals. The work of the team was recognised in professional circles. In 2017 the team was given a silver award by the Chartered Institute of Public Relations (CIPR)’s Yorkshire and Lincolnshire branch for In-house Team of the Year, in recognition of the enormous strategic impact made by the small team at Sheffield Children’s.
TRUST BOARD PART 1 12. 322/18 TRUST STRATEGIES - ... Page 127 of 247

2.5. Priority campaigns 2014-18
Each year the Trust Executive Group agreed its three core campaign areas for the year ahead. For most of these areas, the campaign approach was highly successful. Clear measurable results were achieved, particularly by the plans supporting the New Wing, Research, Mandatory Training and PDRs. For example, the Mandatory Training and PDRs campaign supported the Trust in raising compliance rates to reach their target. The research campaign resulted in a big increase in recruitment of volunteers. The new wing campaign helped ensure a smooth transition to the new wards (despite new ways of working as well as new locations) brought a sense of celebration for staff and patients, whilst also securing exclusive coverage on prime time television. The plan to support CAMHS was less successful due to confidentiality issues within the service, however while not delivered exactly as detailed at the start, a range of activity was still carried out to support this important area of the Trust’s work.
2.6. Unplanned communications
In communications, there will always be a level of unexpected activity. Within the time of the previous strategy, this included a range of crisis communications and reputational management support for issues such as:
• Serious Incidents • Inquests • Absconsions • Junior doctor’s strikes • Hospital cladding removal • Data losses • Severe weather • NED resignation • Gas explosions adjacent to the acute site • Cyber attack and loss of access
While this work was dictated by events outside of the Trust’s control, other communications tasks arose during each year as the Trust responded to emerging needs, partner projects and regulatory requirements. Mid-year campaigns worked on by the Communications Team included:
TRUST BOARD PART 1 12. 322/18 TRUST STRATEGIES - ... Page 128 of 247

• Sepsis • Care Quality Commission (CQC) • General Data Protection Regulation (GDPR) • The Yorkshire and Humber Genomic Medicine Centre (GMC) • IT A Day In The Life • Closure plan of the Emergency Dept doors
The Communications Team worked hard to reprioritise projects as new ones arose and no significant project was left without support. However the Communications Team will be working hard to support teams in their advance planning for the years ahead, as the more planned approach is still preferable wherever possible in order to ensure the very best outcomes.
The three core objectives of this strategy over its three year term are: 1. Profile raising – To further develop the regional, national, international reputation of Sheffield Children’s as a specialist provider 2. Internal Communications and Engagement – To give staff a greater sense of belonging and involvement with the Trust, by developing a shared staff engagement approach and continuing to strengthen internal communications. 3. Recruitment – To support the recruitment of the best possible staff through comprehensive and engaging recruitment materials, and bespoke support for hard-to-recruit roles More detail on the plans to support each of these objectives can be found below.
3.1. Objective 1 - Profile raising
Supporting Trust objectives:
Empower motivated and compassionate staff Lead improvements in paediatric care Build clinical and financial sustainability
Sheffield Children’s has a good reputation. Within Sheffield and surrounding areas it is known as a caring place, and through the work of recent years, many people are beginning to have an understanding that it also carries out a range of specialist work.
3. Objectives 2019 – 2021
TRUST BOARD PART 1 12. 322/18 TRUST STRATEGIES - ... Page 129 of 247

Outside of the Sheffield City Region, the Trust is less well known. While in recent years the Trust has gained a significant amount of national exposure, building a strong reputation on a national scale can only take place with significant investment of time and energy – not just from communications professionals, but also from the people behind the story. To deliver this objective, the Communications Team will be:
Working with clinicians to ensure more articles in professional publications/journals Supporting teams to enhance their presence at professional conferences Supporting successful services with award applications Increasing the amount of regional, national and international media, showcasing
specialist services with a compassionate approach Continuing to increase social media presence and engagement rate Extensive development of our YouTube offer, with instructional videos for both
parents and professionals Continued development of the Trust website to make it a go-to place for specialist
information about the care of children – increasing content like case studies, videos and signposting to self-care resources
Developing our identity as a digital leader. The Communications Team will develop a Digital Strategy which will explore how we can be involved in the development of more digital tools, involve more families in that development process, and work more closely with other digital providers, including our university partners, NHS Digital and the private sector
Developing and delivering a plan for external stakeholder engagement, including our partners across the Accountable Care Partnership (ACP), the Integrated Care System (ICS), GPs, referring clinicians, national commissioners and regulators.
The support of patients and their families will play a big role in the success of this objective, as they are key to showing the human impact of our work. In addition, clinicians will be vital. Some may not see the value of sharing their work or be too humble to want to shout about their achievements. To combat these issues, the Communications Team will be working with clinical teams to help explain the value of communicating, develop trusting relationships and find ways of showcasing services and advancements in a way that clinicians feel comfortable with. However time is also likely to be a factor, so consideration will need to be given to how this will be incorporated into clinical roles.
3.2. Objective 2 - Internal Communications and Engagement
Supporting Trust objectives:
• Provide high quality patient experience and outcomes • Empower motivated and compassionate staff
TRUST BOARD PART 1 12. 322/18 TRUST STRATEGIES - ... Page 130 of 247

• Lead improvements in paediatric care Sheffield Children’s has a solid base of internal communications channels which are now well established and well rated. From the internal communications side, digital communications are strong and the Open Meetings provide a regular opportunity for face-to-face sessions with the Executive Team. However it is recognised there is a communications gap for people who do not use computers regularly. This is a particular concern for clinical staff. Printed materials work well for specific campaigns, but are not currently used routinely. This will be explored further. An initial trial of a ward communications folder is under way and the results of this will help inform the options moving forward. Communication must also take place at multiple levels of an organisation – central production and distribution of all information is neither practical nor desirable. Informal feedback from managers is that many feel poorly equipped to communicate effectively with their staff, both in terms of skills or knowing the right things to communicate. These are both areas where further support can be provided, equipping managers with the skills and information they need for this crucial role. In terms of staff engagement, there are projects which touch on this as part of other work by Communications, HR, Learning and Organisational Development and Transformation. However none of these projects have the specific aim of improving engagement – engagement is either a means to an end or a side benefit. Staff survey results suggest this needs to change; that Sheffield Children’s needs to actively work on this area. To deliver this objective, the Communications Team will:
Develop and deliver an Internal Communications and Engagement Strategy Develop an alternative communications method (likely to be paper-based) to
support staff who are not regularly using computers Relaunch the team briefing system, including a more developed process to ensure
this is effectively utilised across the Trust Provide tools and guidance to support managers in their communication with teams Explore and develop staff engagement opportunities, including the potential for
face-to-face events and use of intranet discussion forums Consult with staff from various staff groups and locations to ensure new channels
and activities developed within the strategy meet their needs Further develop the intranet to ensure it is as user-friendly as possible and has tools
which make it easier for staff to do their jobs Boost the staff benefits proportion of the intranet and share these benefits regularly
through other channels Explore the potential for communication and engagement through mobile devices
TRUST BOARD PART 1 12. 322/18 TRUST STRATEGIES - ... Page 131 of 247

Work in partnership on plans with HR and Learning and Development leads, to ensure an approach which meets the needs of all services and which takes advantage of existing channels, such as Trust Induction
3.3. Objective 3 - Recruitment
Supporting Trust objectives:
Provide high quality patient experience and outcomes Empower motivated and compassionate staff Lead improvements in paediatric care Build clinical and financial sustainability
Work through the “profile raising” objective will play as big role in supporting this objective. The stories celebrating great staff through the “Internal communications and engagement” objective will also support this objective, as it will show Sheffield Children’s as a place with great staff and also as an employer that appreciates the people who work for it. However a range of additional actions are planned to specifically help with recruitment. This includes:
Working with HR to create a template job ad, to improve the attractiveness of all roles advertised by the Trust
Improving web information available to potential recruits. This will include providing more in-depth information about Sheffield Children’s as a place to work, Sheffield as a place to live and the various ways the Trust will support and develop new recruits
More targeted information for in-demand roles, such as digital information packs about nursing careers at Sheffield Children’s
Working with HR to support the “First Day Ready” project, which will include improving the information provided to recruits after their informal offer and through their induction process
Personalised support for managers writing job ads for hard-to-fill roles, particularly where an initial recruitment search has proved unsuccessful
Further development of LinkedIn as a Trust communications platform, as a broadcast channel, amplifying messages by working with well-connected employees and answering common questions posed by jobseekers
Working with HR to explore the potential of the Glassdoor site as a way to showcase Sheffield Children’s as a great employer
Coordinating general reputational activity with recruitment needs. For example, if the Trust is looking to recruit researchers, then that month’s Twitter takeover by a staff member could be by a member of the research team
TRUST BOARD PART 1 12. 322/18 TRUST STRATEGIES - ... Page 132 of 247

3.4. Year 1 projects
In common with the previous strategy, the intention is to agree a small number of additional projects each year for progression, which may fall outside of the scope of the strategy objectives, but which are still of high priority for the Trust. The Year 1 additional projects will be:
Transformation (whole programme) Supporting Provide, Empower, Lead, Build and Discover
Modernising Outpatients Supporting Provide, Empower, Lead, Build and Discover
Theatres Well Prepared Supporting Provide, Empower, Lead, Build and Discover
CQC inspection Supporting Provide and Empower
All of these projects will involve a combination of external and internal communication. The activity will be set out in a dedicated communications plan for each project. The CQC Communications Plan is already in place and delivery is underway. A draft Transformation Communications Plan has been developed and is awaiting sign off. Plans have yet to be developed for Modernising Outpatients or Theatres Well Prepared. However a campaign plan has been developed to support the reduction of Was Not Brought (WNBs) numbers – a key issue for Outpatients - and materials are being created for this ready for a public launch in early 2019.
Different strands of the strategy will have different messages, as the audiences and purposes can vary significantly. However it is important to have a core set of key messages that apply to all of our communications. These are identified as: 1. Sheffield Children’s is a world-class specialist Trust, bringing together mental and physical health services to provide a healthier future for children and young people 2. Sheffield Children’s has amazing staff who not only have clinical expertise, but also demonstrate care and compassion to children and their families every day 3. Through research, innovation and scientific development, Sheffield Children’s is leading the way in improving diagnosis, treatment and quality of life for children and young people worldwide
4. Key messages
TRUST BOARD PART 1 12. 322/18 TRUST STRATEGIES - ... Page 133 of 247

The audiences will vary according to the specific project or objective. Across the whole range of activity covered by this strategy, audiences will include:
Clinical staff Non-clinical staff Patients Potential patients Parents/carers of patients Parents/carers of potential patients GPs Other referrers Healthcare professionals (not currently employed by the Trust) Integrated Care System (ICS) partner organisations Commissioners Regulators General public Media
Internal
Open Meetings Staff noticeboards Team briefings Intranet Weekly Digest Spotlight newsletter Transition newsletter Chief Executive’s blog Medical Director’s blog PC desktop notifications New face-to-face staff engagement sessions New staff app Communications Champions All staff emails Targeted mailing lists (including by staff group and staff location)
5. Audiences
6. Channels
TRUST BOARD PART 1 12. 322/18 TRUST STRATEGIES - ... Page 134 of 247

External Social media Media Trust website New GP newsletter Care Experience newsletter Digital screens External signage Appointment letters
For external audiences, we also have many opportunities to work with partners and utilise their channels – this would include channels managed by other Trust’s, primary care groups, professional bodies, parent support groups, charitable organisations and condition specific groups.
Staff survey Internal Communications Survey Recruitment – quality and quantity of applications Number of professional conferences attended Number of articles in professional publications/journals Amount of regional, national and international media coverage Stakeholder satisfaction with Trust communication (tested via survey) Referrals to pre-agreed services Website analytics Social media evaluation Impacts on service delivery and other “real world” outcomes
Reports based on this information will continue to be prepared for Trust Executive Group (TEG) on a monthly basis and for Finance and Resources Committee twice a year.
Risk Mitigation
Clinicians not given sufficient time in working hours to support projects
Communications Team to minimise requirement on staff, only taking clinician time where required
7. Measures
8. Risks
TRUST BOARD PART 1 12. 322/18 TRUST STRATEGIES - ... Page 135 of 247

Wide range of clinical staff involved, to avoid overburden on individuals or teams Raised as part of Trust Strategy development work, and being considered in job planning
Clinicians too humble or do not see the benefit of sharing their work
Greater presence of Communications Team members around the Trust, developing relationships and trust Work with clinical teams to share the importance of celebrating good work Greater recognition of staff work internally and externally, so that sharing stories becomes normalised Training provided to help staff develop skills to share their stories with the media and at events Communications Team support in developing case studies and award submissions – so staff feel the Trust is showcasing their work, rather than the staff member/team having to do this alone
Large scale reputational issue – damaging profile and/or absorbing staff time
Realistic planning, which accounts for some of the “known unknowns” Focusing on profile raising, to lessen the impact of reputational issues Close working with Trust leadership to ensure early communications involvement, to ensure correct communications approach at the start
Additional objectives/requests not in line with the achievement of this strategy
Communications objectives in this strategy developed with the support of Trust leadership (to TEG level) Continuing to work with divisions so Communications understands developing service needs, and to highlight the importance of advance notice
Continued growth of external projects Monitoring requirements as they develop
TRUST BOARD PART 1 12. 322/18 TRUST STRATEGIES - ... Page 136 of 247

requiring communications support (eg Accountable Care Partnership, Integrated Care System, Children’s Partnership Board, SheffieldChildren’s@, TITCH, National Institute for Children’s Sport and Exercise Medicine (NICSEM), Centre for Child Health Technology)
Reviewing priorities should any of these projects ramp up significantly Close working with partner organisations
TRUST BOARD PART 1 12. 322/18 TRUST STRATEGIES - ... Page 137 of 247
REPORT TO THE TRUST BOARD OF DIRECTORS’ MEETING (PART 1) HELD ON 2018
Marketing Strategy
Trust aims supported by this paper
Provide high quality patient experience and outcomes Empower motivated and compassionate staff Lead improvements in paediatric care Build clinical and financial sustainability
Link to Board Assurance Framework
Failure to ensure that the Trust recruits staff in the right numbers and with the appropriate breadth of skills and competencies to deliver high quality services now and in the future.
Failure to engage effectively with partner organisations and the local community threatens the ability of the Trust to deliver its strategic ambition
Operational capacity constraints and failure to deliver transformation impact on our ability to deliver planned activity and manage demand impacting on operational efficiency, service quality and financial performance.
Purpose of the paper
To present to the Trust Board of Directors the Sheffield Children’s marketing strategy, which outlines our marketing positioning based upon our strengths, current market forces and the audiences we need to connect with.
Summary of key points
Our overall marketing position, including our brand Suggested future approach to marketing, including strategy, positioning and marketing mix
Recommendations for promotion, product development and private patients
Board Action required The Committee is asked to approve the updated strategy which has been reviewed and recommended for approval by the Finance and Resources Committee.
Author: Mr G Critchley, Senior Digital Communications Officer
TO APPROVE Executive Sponsor:
Mr S Ned, Deputy Chief Executive and Director of HR Ms R Brown, Director of Strategy and Operations
TRUST BOARD PART 1 12. 322/18 TRUST STRATEGIES - ... Page 138 of 247

1. Executive Summary 1
1.1. Strategic/Operational challenge 1
1.2. Recommendations 1
2. Introduction 3
3. Aims and objectives 4
3.1. Trust Aims and Objectives 4
3.2. Marketing Strategy Objectives 4
3.3. Measures 4
4. Our Approach 5
4.1. Research and Best Practice in Marketing 5
4.2. How we have reached conclusions 5
5. Strategic elements 7
5.1. Our Brand 7
5.2. Product strategy 10
5.3. Market positioning 13
5.4. Audience segmentation 16
5.5. Marketing Mix 26
6. Resources 31
7. Recommendations 31
7.1. Focus on training 31
7.2. Promote our Trust and strengthen our hand 32
7.3. Market and product development 32
7.4. Promote private care and desirable referrals 32
Sheffield Children’s Marketing strategy
TRUST BOARD PART 1 12. 322/18 TRUST STRATEGIES - ... Page 139 of 247

1 of 34
This marketing strategy has been created to achieve consistency and impact in the
ways the Trust engages in marketing in all forms.
It examines the current state of the context in which the Trust operates and explores
our marketing positioning based upon our strengths, current market forces and the
audiences we need to connect with.
The strategy clarifies our brand, its elements and values, as well as key marketing
messages. Further into the document, a product strategy is proposed and key
messages stratified based upon segmented target audiences.
1.1. Strategic/Operational challenge
This strategy recognises that a key part of our most valuable marketing collateral is
the expertise of our specialist staff. In turn, effective promotion and involvement of
these staff is central to achieving marketing goals. These staff, therefore, need to be
sure that, in word and in action, spending time engaging in marketing activity is a
priority for them and the Trust. This necessitates a strategic decision with an
operational impact: how much ‘marketing’ time to set aside for clinicians as part of
their job, when they will not be fulfilling clinical activity. This is the decisive challenge
to be overcome regarding the achievement of the aims set out in this marketing
strategy.
1.2. Recommendations
Actionable recommendations of the strategy are made on the final page. These
discuss how to make progress towards developing our training offer, strengthening
our market position, and take advantage of developing markets, such as private
patients, innovation and intellectual property registration, and investigative work via
MRI.
Training
▪ Develop wider suite of sessions based on needs of market/most inappropriate
referrals
▪ Make costing and invoicing, and surrounding processes e.g. booking easier
▪ Create promotional collateral
1. Executive Summary
TRUST BOARD PART 1 12. 322/18 TRUST STRATEGIES - ... Page 140 of 247

2 of 34
▪ Develop thought leadership in our trainers through research and attendance at
conferences, including seminars and mini workshops
Central brand and general offer
▪ Celebrate our successes
▪ Emphasise our brand values
▪ Advocate on behalf of children and young people
▪ Promotion of paediatric healthcare as a career, with resource packages, advertising
campaigns and visits with schools/colleges
▪ Centre of excellence emphasis/development
▪ Promotion of clinicians via website and conferences
▪ Thought leadership via blogs, presentations and research
Development areas
▪ Investigation via MRIs, evaluation and expansion if appropriate
▪ Research, innovation and intellectual property of products
Paying patients
▪ Emphasise our points of difference
▪ Select appropriate services for private referrals – strategic decision required
▪ Build relationships with providers of ancillary services such as transport and
accommodation to provide a seamless and high quality experience of care for
family and patient
▪ Create promotional materials about private patient experience including travel,
accommodation etc.
▪ Reduce barriers to access
▪ Target overlap areas for referrals
▪ Place case studies with condition specific support networks
TRUST BOARD PART 1 12. 322/18 TRUST STRATEGIES - ... Page 141 of 247

3 of 34
This marketing strategy outlines how Sheffield Children’s NHS Foundation Trust will
communicate and engage with members of the public and healthcare professionals
about its services and how to access them.
Target audiences:
General public
Families with young children
Parents of children with a health condition
Parents of children with a health condition considering treatment outside of their
CCG
Other providers
Healthcare professionals
Third sector organisations
The primary objective of this strategy is to understand how we can effectively engage
and communicate with our target audiences about SCH and how people can use our
services.
With the development of Integrated Care Systems, of which Sheffield Children’s is an
active regional partner, new models of commissioning and provision of care are
being explored. Whereas providers may previously have competed to attract
additional activity, the new approach promotes organisations working together to
develop and protect quality services across regions.
Within this work is a focus on transformation of the way specialised services are
delivered. As a specialist provider of paediatric services, Sheffield Children’s is
presented with unique opportunities and challenges.
2. Introduction
TRUST BOARD PART 1 12. 322/18 TRUST STRATEGIES - ... Page 142 of 247

4 of 34
3.1. Trust Aims and Objectives
In pursuit of a shared vision “to provide a healthier future for children and young
people”, the objectives of Sheffield Children’s NHS Foundation Trust are as follows.
Provide high quality patient experience and outcomes Empower motivated and compassionate staff Lead improvements in paediatric care Build clinical and financial sustainability Discover new ways to improve children's health
3.2. Marketing Strategy Objectives
The objectives of this marketing strategy are as follows:
To increase the awareness of the high quality services provided by Sheffield
Children’s
To increase the understanding of the options available for referral
To encourage pro-active choosing of Sheffield Children’s as a location for care
To emphasise the added value provided by Sheffield Children’s
To use marketing to optimise the potential provided for income generation
To achieve these objectives we will:
Promote services provided by Sheffield Children’s
Promote and provide training by our experts
Educate referrers and families about the referral process
Take advantage of opportunities to highlight our unique selling points
Work with departments internally to ensure our marketing is responsive to the
needs and capacity of the organisation
Encourage and facilitate staff with specialised expertise to research and present at
conferences, take up national advisory positions
3.3. Measures
3. Aims and objectives
TRUST BOARD PART 1 12. 322/18 TRUST STRATEGIES - ... Page 143 of 247

5 of 34
We will measure success against these objectives by:
Increase in number of referral enquiries
Increase in number of enquires converted to referrals
Change in brand and key message awareness and understanding survey of public
and patients
Increase in number of training enquiries
Increase in training enquiries converted to course attendance
Any increase in revenue from private patient activity
Number of staff on advisory boards
Number of staff presenting at conferences
Staff feeling confident and supported in taking on promotional activity
4.1. Research and Best Practice in Marketing
A secondary research review in conjunction with the primary research detailed above
has given us examples of industry best practice to use in our strategic
recommendations.
In addition to this, a variety of marketing best practice models have been used
throughout the report. These models have been adapted to make them applicable to
our sector.
4.2. How we have reached conclusions
Our approach to our marketing strategy is an iterative process whereby each phase
informs the next.
This approach can be described as follows:
1. All of our activities will originate from understanding our customers and our
products.
2. We will use this understanding to segment ‘key audience groups’. These are
4. Our Approach
TRUST BOARD PART 1 12. 322/18 TRUST STRATEGIES - ... Page 144 of 247

6 of 34
groups of individuals who share similar behaviours and characteristics.
3. We will also develop a product strategy to ensure we are communicating
about our preferred services.
4. We will then use this understanding to identify the key audience groups that
will have an interest in those services.
5. Once we have identified these groups we will seek to identify the key
messages which would be of most interest to them.
6. We then use this information to develop a marketing mix that ensures that
materials highlight the benefits of Sheffield Children’s and encourages the
audience to consider using our services.
7. This marketing mix will then be developed to that particular key audience
group to influence how they view Sheffield Children’s and their interaction
with us.
8. The effectiveness of the marketing mix will then be evaluated and the
outcomes will inform future activities.
Our activities will therefore be planned to target marketing activities around a series
of Key Target Audiences. To identify these Key Target Audiences, we will need to
adopt an appropriate segmentation approach.
TRUST BOARD PART 1 12. 322/18 TRUST STRATEGIES - ... Page 145 of 247

7 of 34
5.1. Our Brand
We want to ensure that all our products, services and materials are recognisable to
our customers. Our brand should therefore be consistently used across all of the
above, as well as in our marketing.
Brand name
Sheffield Children’s NHS Foundation Trust (or Sheffield Children’s) is the overarching name for the services provided at Sheffield Children’s Hospital and at other sites across the city. It encompasses acute, elective, community and mental wellbeing care. Referencing our location sites us geographically and appeals to local pride as well as the national profile Sheffield has built as being friendly and well connected. “Children’s” is important to mark us out as a paediatric specialist. Having NHS in our name is an important factor which uses the excellent international brand recognition of the NHS while aligning us with a historical commitment to compassionate care. Brand position
To achieve effective engagement with our target audiences we need a solid brand position that reflects the values we hold and their benefits for families. Our brand position will therefore be: Sheffield Children’s NHS Foundation Trust is a trusted provider of high quality care, where everything we do is specialised for children and young people. We are home to some of the world’s leading experts in children’s health, with excellent facilities and constant innovation through research which allows us to keep ensuring that children are getting the best care. We understand the needs of families and are known for our compassionate and friendly approach. Logo
Our logo helps us build brand recognition and awareness. It is important that this is
applied consistently across all materials that we produce.
At present there is scope to develop this logo to include an iconic visual identifier,
without changing the layout of the text and NHS lozenge. This will require working
with an agency to create a unique and meaningful icon which represents our brand
5. Strategic elements
TRUST BOARD PART 1 12. 322/18 TRUST STRATEGIES - ... Page 146 of 247

8 of 34
values and separates us from other providers across a range of applications. This
would likely involve a one-off a six month process at a cost of around £10-20k.
There are also a number of instances where a historic use of the original Theo Bear
mascot is taken as a proxy logo for Sheffield Children’s. This potential confusion in
brand recognition is a threat to consistent brand application which jeopardises
awareness and understanding of our brand values.
Brand values
Our brand values incorporate the following elements:
Excellence – Clinical high quality, positive patient experience, leadership in general
and specialist clinical knowledge, leading in research and innovation.
Child-focused – whole experience of care is specialised for children and young
people, with an understanding and provision for the needs of families.
Friendly – care is delivered with compassion and kindness, with friendly staff who
get to know patients and families as individuals, and the little details most important
to them.
Trusted – safe, high quality, reliable, well led.
Northern/Regional – serving a wide area, well connected, accessible.
Key messages
Our key messages will vary depending on the target audience, especially between
the public, overseas patients, and influencers. These key messages have been
developed to ensure our brand values are communicated clearly and our unique
selling points highlighted with the aim of helping to achieve marketing goals.
For the public:
Sheffield Children’s is a specialist provider of high quality care for children and
young people
Everything at Sheffield Children’s is centred around children and young people
Sheffield Children’s understands the needs of children and their families
Sheffield Children’s is home to trusted experts and world class specialists
Sheffield Children’s serves families across the UK
Sheffield Children’s is known for the friendliness and compassion of its staff
Sheffield Children’s manages services that treat children holistically, providing
TRUST BOARD PART 1 12. 322/18 TRUST STRATEGIES - ... Page 147 of 247

9 of 34
acute care, community care and CAMHS
Families can choose to be referred for specialist care at Sheffield Children’s,
regardless of where they are from
We use our clinical expertise, high tech equipment and innovative research give
children in our care the best possible chance
For stakeholders:
Sheffield Children’s understands the needs of children and their families and is well
placed to advise on service provision
Sheffield Children’s is well led and has a history of sound management
Sheffield Children’s is a safe pair of hands, trusted by the public
Sheffield Children’s is home to trusted experts and world class specialists
TRUST BOARD PART 1 12. 322/18 TRUST STRATEGIES - ... Page 148 of 247

10 of 34
Market penetration
Product development
Market development Diversification
5.2. Product strategy
Three separate product streams:
Investigation Category: Diversification
MRI scans for clinical negligence cases
Key audience: Solicitors
Competitive advantage/USP: 3T scanner, Paediatric specialty, we are only
employers of paed. anaesthetists in area.
Healthcare Category: Protect/Build market penetration, product development
Three separate strands:
- Recommissioned services
- Referrals on NHS
- Private patients
We need to protect and strengthen current relationships with healthcare
commissioners and referrers, using these relationships to maintain the marketing of
Existing market New market
Exis
tin
g p
rod
uct
N
ew p
rod
uct
TRUST BOARD PART 1 12. 322/18 TRUST STRATEGIES - ... Page 149 of 247

11 of 34
existing products and therefore a recommission of current services.
We should also encourage current partnerships within regional working groups such
as the Integrated Care System by feeding back to them stories of success elsewhere
in our Trust. This further strengthens the position of the Trust as leaders in paediatric
care. While the Trust would like to see a growth in private patient activity, the main
emphasis of market penetration building should be put on recommissioned services
including specialised services and referrals on the NHS. Key audiences for this are
the public and other healthcare professionals. To protect this market it is essential to
ensure the expertise and sustainability of our specialties.
To build our core business, there should be encouragement of referrers, such as
GPs and local hospitals to refer preferred specialist cases to Sheffield Children’s.
Meanwhile parents of children with health conditions applicable to our preferred
specialisms could be encouraged to request referral from their doctor. Working with
condition-specific support networks and by direct promotion would be the best way to
reach these parents.
We should also look to build the reputation of our clinicians to raise the awareness of
the innovation and skillsets available at Sheffield Children’s. This can be achieved
through thought leadership, conference presentation, panel appearances and
research publications.
Action:
- investigate competitive advantage outside of specialism e.g. waiting
times/environment/food etc.
- ensure parity and depth of information for consultants and their publications on
the Trust website
Training Category: Market Development
In support of the strategic aim to lead improvements in paediatric care, the Trust
should pursue the development of its training offer as a marketing goal. With the
development of a ‘Sheffield Children’s @‘ model, where the essential elements of
TRUST BOARD PART 1 12. 322/18 TRUST STRATEGIES - ... Page 150 of 247

12 of 34
care central to the Trust are provided in novel satellite locations, training by Sheffield
Children’s staff becomes a necessary part of setup and ongoing quality assurance. In
addition to training in preparation for ‘franchised care’, training could also be provided
to GPs, school workers, and doctors who have not had paediatric rotation. Our
CAMHS and neurodisability teams also have a wealth of knowledge to offer training
to parents and support workers who care for children with ADHD, epilepsy and other
relevant conditions.
By providing training of this sort, Sheffield Children’s is fulfilling regional and citywide
aims by equipping and empowering others in the region to provide better care to
children and young people which should increase consistency of the quality of
available care as well as help to reduce referrals to secondary care.
TRUST BOARD PART 1 12. 322/18 TRUST STRATEGIES - ... Page 151 of 247

13 of 34
Industry competition
Supplier power
Threat of new entry
Buyer power
Threat of substitution
5.3. Market positioning
Five Forces of Competition Model
Threat of new entries to market While theoretically we provide healthcare as a public service within a protected marketplace, there have been increasing numbers of examples where private healthcare providers such as Virgin Care, Circle and Ramsay Health have won contracts for services traditionally provided by the NHS. Equally, commissioners have been spending more on private providers, with 7.6% of budget being given to private providers in 2015/161, up from 4.4% in 2009/102. This increase is roughly 0.5% each year. However, most of the increase in spending is on non-acute services such as GP/out of hours, pharmacy, and diagnostics. The rate of spending on acute services has 1 Department of Health accounts: https://www.gov.uk/government/uploads/system/uploads/attachment_data/file/539602/DH_Annual_Report_Web.pdf#page=44 2 http://www.bbc.co.uk/news/health-30397329,
Threat of new entry
- Time and cost of entry - Specialist knowledge - Economies of scale - Cost advantages - Technology protection - Government policy
Rivalry determinants
- Industry growth - Intermittent capacity issues - Quality differences - Customer loyalty - Switching costs - Brand strength
Determinants of supplier power
- Number of suppliers - Size of suppliers - Uniqueness of service - Ability to substitute - Cost of changing
Determinants of buyer power
- Number of customers - Demand - Difference between competitors - Price sensitivity - Ability to substitute - Cost of changing
Determinants of substitution threat
- Substitute performance - Cost of change
TRUST BOARD PART 1 12. 322/18 TRUST STRATEGIES - ... Page 152 of 247

14 of 34
slowed, and there has been evidence of the negative impact on quality where a private sector provider was awarded management of an NHS hospital. To date there have been very few new entries in the provider of specialist paediatric services. Rating: Low/medium pressure Bargaining power of buyers In this instance, buyers are twofold – our commissioners and our families/service users. Commissioners have the ability to dictate terms and costs. While there are a number of commissioners with whom we work, they often take different or contradictory positions. Joint negotiation of commissioners, such as the regional partnerships recently formed will give increased power to these buyers as well as uniformity in commissioning. Families who use our services generally do not have much power. They are referred based on condition or location, and there is not yet a particularly strong culture of choosing providers. Rating: High pressure Bargaining power of suppliers Our suppliers fall into two groups: Material providers and staff. Costs of materials and resources are generally increasing, with Brexit approaching and a weak pound this situation looks to continue as suppliers pass on higher costs to us. In some cases we use products where a wide range of suppliers are available, and can therefore choose cheaper alternatives. However, due to the specialist nature of some of our services, there are some instances in which specialist equipment is only available from a small range of suppliers. It is also true that we cannot ignore the associated risk of the impact on quality which switching to cheaper suppliers could entail. Staff are a key supplier of our services. Many are members of a union and therefore have the potential to increase their bargaining power. Many negotiations over supply of work and wages happen at a national level, but we have some local autonomy to increase the engagement and positive sentiment of our staff. Engaged staff are central to the delivery of quality services. Communications with unions and staff should remain open to avoid strike action or similar consequences and increase engagement. Rating: Medium pressure Threat of substitutes Substitutes in the acute sector are very rare. In fact, the only area where most people are tempted to attempt substitutes are low-level injuries or conditions which would not be appropriate for acute care.
TRUST BOARD PART 1 12. 322/18 TRUST STRATEGIES - ... Page 153 of 247

15 of 34
Rating: Low pressure Competitive rivalry Rivalry in our sub-sector of this industry (paediatric health and wellbeing) is relatively low. Competitors are located in areas where we do not regularly compete for the loyalties of customers. Quality is roughly comparable, while specialisms and niche offers differ between suppliers, but customers are referred. More could be done to explore this quid pro quo arrangement. We also benefit from a strong brand and good reputation. The development of a larger Leeds Children’s Hospital, while still at a fundraising stage, would represent an increase in competition and at this point differentiation would need to be effectively managed to ensure significant specialist activity was not lost through commissioning arrangements or individual referrals.
Rating: Low pressure Overall rating: Low-medium pressure
Competitive Advantage As the competitiveness of the market is low-medium, it is crucial that Sheffield Children’s builds a reputation of trust and reliability, positioning itself wisely to leverage current relationships with suppliers and referrers through strong and consistent internal marketing and positioning itself with the public as having unique value. It will do this by adopting a mixed mode positioning strategy of differentiation. Differentiation Sheffield Children’s will differentiate itself from the competition on the basis of the following elements. Product characteristics
- We are unique in the position of offering specialised paediatric acute and
community care
- We are unique in the geographical area we serve
Pseudo physical characteristics
- Intangible values of compassion, friendliness, and a child focussed
approach
- Tangible values of quality of care, continuity/consistency of care
Benefits
- The clinical outcomes for our patients
TRUST BOARD PART 1 12. 322/18 TRUST STRATEGIES - ... Page 154 of 247

16 of 34
- The transformational impact these outcomes have on the life of a young
patient
Product/user approach
- Maintaining and building our reputation as a centre of excellence in the
mind of three key audiences: Senior clinicians, Referrers, and condition-
specific support organisations
Cultural symbol approach
- We must leverage and build upon the reputation we hold as a well-loved
institution in Yorkshire to embed and communicate our brand values
5.4. Audience segmentation
Our marketing activities and key messages will be segmented depending on our
audience type. The main split will be between the general public, public sector
stakeholders, and condition specific support groups.
It is important that we understand that our target audience will be accessible through
different types of marketing depending on who they are. When choosing
communication channels, age and socio-economic class are significant factors when
considering which communications channels are the best to utilise to make sure we
maximize our reach. We will ensure that we use a variety of these mediums to
ensure we are engaging with as many people in the most impactful ways possible.
The following are our key customer groups:
Audience 1 - The general public It is important Sheffield Children’s maintains its strong reputation and promotes its
brand values to the general public, many of whom could become or have influential
contact with our key audiences. Public opinion will also affect the decision making of
commissioners and political figures.
Generally the public we target can be geographically separated into the following
areas: Sheffield, South Yorkshire, Yorkshire, Humber and North Derbyshire,
peripheral/overlap regions where families are equidistant from specialists (e.g.
Nottingham/Leicester), and United Kingdom. Most of our general marketing will be
TRUST BOARD PART 1 12. 322/18 TRUST STRATEGIES - ... Page 155 of 247

17 of 34
targeted at the first three areas with targeted messages going to overlap regions and
national audiences.
1a – The public with children 0 – 18 years old Parents and carers are an important audience as they are most likely to use our
services. They have a key role in choosing where they are referred as well as
influencing other parents and carers, especially if they have an experience of care at
Sheffield Children’s.
1b – Parents/carers of children with chronic/long term condition and young people/adults who could directly benefit from our services 1c - Parents overseas
2 - Public stakeholders
- Other provider Trusts - Health professionals/academics around country - Commissioners - GPs - Influencers in councils/political parties
TRUST BOARD PART 1 12. 322/18 TRUST STRATEGIES - ... Page 156 of 247

18 of 34
Segment Characteristics Attractiveness Strengths we have to offer
Messages Channel
The general public
Aware of Sheffield
Children’s
Proud of NHS
Positive feeling about
specialist children’s Trust
Emotional value via
historic connections to city
and personal / family
illness
Awareness of our key
messages can help
achieve appropriate
access of care
Many are potential
patients or parents of
potential patients
Maintaining positive
public image important
for our brand and long
term survival
Can exert pressure on
political influencers and
commissioners
Regional coverage
General paediatrics
care delivered with
compassion and child-
centred manner
All key messages for public Social media, local and national media
TRUST BOARD PART 1 12. 322/18 TRUST STRATEGIES - Communications St... Page 157 of 247

19 of 34
Segment Characteristics Attractiveness Strengths we have to offer
Messages Channel
Parents or carers of children with chronic/long term condition
All will have experience of
paediatric care
Some may be personally
familiar with Sheffield
Children’s
Value the impact of
specialisms and specialist
care
Potentially willing to switch
providers based on
expertise
Often closely linked in
condition specific support
groups
Messages spread well
among this group
Many of our specialisms
relate directly to them
They can influence
others via
recommendation
Specialisms and
excellence of
outcomes
Research and
innovation
Sheffield Children’s understands
the needs of children and their
families
Sheffield Children’s is home to
trusted experts and world class
specialists
Sheffield Children’s serves families
across the UK
Families can choose to be referred
for specialist care at Sheffield
Children’s, regardless of where they
are from
We use our clinical expertise, high
tech equipment and innovative
research give children in our care
the best possible chance
Social media, national media, condition – specific support news
TRUST BOARD PART 1 12. 322/18 TRUST STRATEGIES - Communications St... Page 158 of 247

20 of 34
Segment Characteristics Attractiveness Strengths we have to offer
Messages Channel
Parents / clinicians overseas
Potentially willing to switch
providers based on
expertise
Value clinical reputation
and technological
innovation
Value second opinions
Will also consider the
reputation of
Sheffield/Yorkshire itself
when making
considerations
Will have different
expectations of experience
re. delays, consultant
communication,
accommodation
Can provide income for
the Trust
Can build our reputation
overseas
Can widen our
recruitment pool
World class technology
Specialty range
aligned with global
need
Relatively accessible
via road, rail and air
Adequate city
infrastructure
Comfortable
accommodation (apart
from S2, where many
referrals could land)
Well connected
clinicians
Multi-lingual clinicians
Families can choose to be referred
for specialist care at Sheffield
Children’s, regardless of where they
are from
We use our clinical expertise, high
tech equipment and innovative
research give children in our care
the best possible chance
Sheffield Children’s is home to
trusted experts and world class
specialists
Social media, web content, overseas advertising, via embassies, in overseas medical journals
TRUST BOARD PART 1 12. 322/18 TRUST STRATEGIES - Communications St... Page 159 of 247

21 of 34
Segment Characteristics Attractiveness Strengths we have to offer
Messages Channel
Other paediatric specialist providers
Spaced geographically far
as to not compete directly
Can often compete for staff
and nationally
recommissioned services
Competing for
overseas/private patients
Potentially willing to share
resources / training /
recruitment burden
Generally larger and more
advanced in terms of
research, activity and
facilities
Opportunity to learn
from peer organisations
Chance to collaborate
and save funds and
duplication
Strengthen our hand in
national commissioning
negotiations
Unique specialisms
Research approaches
Local experience
CAMHS and
community care offer
is unique
Historic organisation
Access to the further
north
Sheffield Children’s is well placed to
advise on service provision thanks
to their paediatric specialisms and
understanding of the needs of
children and their families
Sheffield Children’s is home to
trusted experts and world class
specialists
Sheffield Children’s manages
services that treat children
holistically, providing acute care,
community care and CAMHS
Direct comms National media Conferences
TRUST BOARD PART 1 12. 322/18 TRUST STRATEGIES - Communications St... Page 160 of 247

22 of 34
Segment Characteristics Attractiveness Strengths we have to offer
Messages Channel
Other non-paediatric specialist providers
Short on genuine
paediatric expertise
Potentially unaware of
knowledge gaps
Larger/more influential but
also impacted by higher
demand and financial
pressure
Looking to expand (in
some cases)
Opportunity to improve
transition
Opportunity to partner
with larger
organisations
Opportunity to build our
reputation
Opportunity to provide
training
Opportunity to deliver
services with paediatric
element
Opportunity to align
ourselves alongside a
stronger partner during
commissioning
challenges
Paediatric expertise
and specialisms
Suite of training (to
develop)
Research base
Good reputation
Well-loved local
treasure
Sheffield Children’s is home to
trusted experts and world class
specialists
Sheffield Children’s is well placed to
advise on service provision thanks
to their paediatric specialisms and
understanding of the needs of
children and their families
Sheffield Children’s is well led and
has a history of sound management
Professional publications, local media, national media, conferences
TRUST BOARD PART 1 12. 322/18 TRUST STRATEGIES - Communications St... Page 161 of 247

23 of 34
Segment Characteristics Attractiveness Strengths we have to offer
Messages Channel
Health professionals and academics
Value paediatric expertise
Open to collaboration
Value research and
innovation
Reachable via networking
Respect personal
reputation as well as
organisational reputation
Potential employees
Opportunity to
collaborate
Opportunity to provide
training
Opportunity to increase
our reputation as
influencers
Employment
opportunities
Research growth and
opportunities for
collaboration
Access to rare disease
patients
Sheffield Children’s is home to
trusted experts and world class
specialists
Conferences, journal publications, NHS publications, national media
Commissioners Open to influence
politically and via
partnership
Value stability
Care about measurables
Value financial prudence
Need to feel in control
Opportunity to maintain
and grow our service
offer
Opportunity to lead
negotiations involving
paediatrics
History of prudence
and strong leadership
Genuine concern for
children and families
Expertise and
experience in full
range of service
delivery
Sheffield Children’s is well placed to
advise on service provision thanks
to their paediatric specialisms and
understanding of the needs of
children and their families
Sheffield Children’s is well led and
has a history of sound management
Sheffield Children’s is a safe pair of
hands, trusted by the public across
a range of provisions
We are is home to trusted experts
and world class specialists
Direct, local media, social media, NHS publications, conferences
TRUST BOARD PART 1 12. 322/18 TRUST STRATEGIES - Communications St... Page 162 of 247

24 of 34
Segment Characteristics Attractiveness Strengths we have to offer
Messages Channel
GPs Short on genuine
paediatric expertise
Potentially unaware of
knowledge gaps
Open to collaboration in
some cases
Opportunity to provide
training
Opportunity to increase
referrals
Opportunity to reduce
inappropriate or
emergency admissions
Paediatric specialisms
Training suite (to
develop)
Range of services
open for referral
Sheffield Children’s is well placed to
advise on service provision thanks
to their paediatric specialisms and
understanding of the needs of
children and their families
Sheffield Children’s is home to
trusted experts and world class
specialists
Direct messaging via CCG newsletter, professional publications
Political influencers
Value stability
Value and understand our
reputation as local treasure
Influenced by public mood
Apprehensive of making
unpopular decisions
Include organisations such
as councils as well as
individuals such as MPs
Aware of PR angles
Good allies to have
during commissioning
negotiations
Able to exert pressure
on national and local
commissioners
Opportunity to build
network and influence
relationship
Good reputation
Leadership
unencumbered by
organisational or
personal scandal
Association with
children
Positive narratives
involving outcomes
Advocacy expertise (to
develop)
PR understanding
Sheffield Children’s is well led and
has a history of sound management
Sheffield Children’s is a safe pair of
hands, trusted by the public across
a range of provisions
Direct, via local and regional media
TRUST BOARD PART 1 12. 322/18 TRUST STRATEGIES - Communications St... Page 163 of 247

25 of 34
Infl
uen
ce
Interest
NHSI
CQC
STH
NHS England
SCC
LA Leaders
MAST Media/Press Healthcare Specific
National MPs Council scrutiny
committee
Charity
SHSCT
Local councils
Universities
General public
Trust membership
Faith groups
National Institute of Health Research
DGH Other children’s hospitals
“Working Together” groups
Schools
National Press/media (general)
Local media
General public
Patient groups and parent/carer groups
Other provider organisations (their lead clinicians)
Voluntary sector
Young People
ODN’s Maternity & Children SCN
Professional organisations e.g. RCPCH
Parents Patients & families
Local councillors
Local authority children’s leads
Local MPs Sheffield CCG
Staff
Board
Council of Governors
Local/ regional Trusts/Hospitals
Other Trusts
Working Together providers
Our local universities
GPs
Sheffield Health and Social Care Trust
Patients & Parents of. Chronic & Complex patients
Regional leadership e.g. City region Mayor
Sheffield audience Regional audience National audience
TRUST BOARD PART 1 12. 322/18 TRUST STRATEGIES - Communications St... Page 164 of 247

26 of 34
Demand Supply
Resilience Profit /
strategic benefit
5.5. Marketing Mix
Product
Our product portfolio outlines the products we currently offer, with recommendations
of where we can develop our product in line with our product development strategy.
This analysis of our marketable products and preferred specialisms uses a balance
of four factors to choose the most optimal products for the Trust to offer on a wider
basis.
Demand The desire for services we offer – the strength of this demand considered alongside
the size of the customer base demanding the service. As an example, rare disease
testing has a strong demand due to the seriousness of a given disease, but a
comparatively small customer base in that these diseases are by their nature, rare.
Supply The ability of other providers to meet
the demands of a customer base.
We may benefit from a geographical
advantage, where surrounding
providers do not offer the same
services as us, or a technical
advantage, where the skills of our staff
uniquely position us to meet demand.
Resilience The ability of the Trust to increase its provision of services to meet demand if a
service is marketed, without impacting negatively on activity.
Profit and/or strategic benefit Some procedures or treatments are relatively well rewarded, but total cost of
aftercare, or associated risk of overstay impacts on profitability. Equally, in areas
where a profit is negligible, we may gain a strategic benefit. This could be by
TRUST BOARD PART 1 12. 322/18 TRUST STRATEGIES - ... Page 165 of 247

27 of 34
reducing emergency admissions, or patenting a product that can be used by other
providers.
Product outline
What we offer is more than just a physical product. In addition to the ‘Core Product’
and ‘Tangible Product’ we also offer extra elements to the product that give added
value to what we offer. These elements are the parts of the product that will give
Sheffield Children’s a competitive advantage over other providers. Therefore, in
addition to the product portfolio outlined above, we will also continue to
develop the augmented product to ensure that our customers feel they are getting
value for the costs associated with coming to Sheffield Children’s.
Augmented product
Tangible product
Clinical services Buildings
Marketing materials
Patient information
Website
Phone / switchboard
service
Opportunities e.g. Burns
Camp, Do it For You
Training and conference
presentations
Vehicles
Staff
Branding
A beloved institution
Active research and innovation
In Yorkshire
On the doorstep of the Peak
District
Sense of communal ownership
through the charity
Press releases
Social media updates
Compassion
Staff attitude
Child-centred atmosphere
Case studies / testimonials Reputation Partnerships
with other organisations
Sheffield city
infrastructure
Core product
Sheffield Children’s NHS
Foundation Trust
TRUST BOARD PART 1 12. 322/18 TRUST STRATEGIES - ... Page 166 of 247

Sheffield Children's
Diagnostic services
SDGS
Radiology
X-Ray 3T MRI Fluoroscopy
Clinical chemistry
Pharmacy
Haematology
Histopathology
Community services
Health Visitors
Looked After Children
School Nursing
Speech and Language
Child Health
CAMHS
Community Psychology
Tier 4 Psychology
Learning Disability and Mental Health
Youth Offending Team
Becton Lodges
Section 136
Acute care (see sub-portfolio)
Training
Product portfolio
Sheffield Children’s offers a range of products.
Highlighted in orange are services which have the potential,
based upon criteria in the product assessment matrix, to be
developed and/or marketed further.
TRUST BOARD PART 1 12. 322/18 TRUST STRATEGIES - ... Page 167 of 247

29 of 34
Acute care
Medicine
Allergy
Cystic Fibrosis
Dermatology
Diabetes
Dietetics
Physiotherapy & Occuptional
Therapy Gastro and Hepatology
Hearing and Speech
Immunology
Metabolic
Metabolic Bone
Oncology & Haematology
Neurology
Respiratory
Sleep Service Rheumatology
Emergency care Critical care Surgery
Burns
ENT
PSU
Neurosurgery
Opthalmology
Orthopaedic
PLRS Spinal
Urology
TRUST BOARD PART 1 12. 322/18 TRUST STRATEGIES - ... Page 168 of 247

30 of 34
Price
The price of our products, to NHS patients, is nothing. There may be additional costs
that families incur as a result of receiving hospital care, such as accommodation,
food and parking. Most of the time, these costs are not comparable from one provider
to another and are seen as inevitable, until they become so high that they are
potentially prohibitive (e.g. regular hotel accommodation/parking in London).
For private patients, we must assess the comparative pricing of procedures from
other providers and use the advantages (e.g. economies of scale) we have to price
competitively. This does not mean we should look to provide our services marginally
cheaper than another provider, but that we should not put a price high without good
reason. Nor should we devalue the excellence of our clinical services by pricing at
the low end of the scale.
For both public and private patients, value becomes the most important issue when
assessing costs. The quality of care received makes the impact of any incidental
costs negligible. Within this assessment of value, our augmented product (see page
29) becomes particularly important, especially for private patients. The patient
experience, which encompasses surroundings, nearby facilities, quality of food,
customer service and additional child-centred adaptations, has a strong bearing on
the perception of value, and can negatively affect the overall evaluation despite the
quality of the care received.
With a maintained emphasis on high quality care and excellent patient experience,
estimations of good value will remain in our favour and associated costs viewed as
incidental.
We should also explore the incentives which we are able to offer to increase desired
referrals. This could involve partnerships with providers of travel or accommodation.
These incentives should not look to mitigate trivial costs (e.g. a free coffee or
discounted parking) but serve to reduce barriers and provide a desirable additional
value.
TRUST BOARD PART 1 12. 322/18 TRUST STRATEGIES - ... Page 169 of 247

31 of 34
People
Our staff are our biggest brand ambassadors, and the key to ensuring the success of
the organisation and its strategy. Without a well-trained, dedicated team, the
successful implementation of this strategy is limited.
Stakeholders play an important role in influencing their respective networks and re-
emphasising our brand values through sharing our messages.
Delivery of this strategy will require investment in resources, staff time to manage,
and accounting for activity lost due to clinician involvement in marketing activities. In
many cases, these costs are offset by the benefits felt by a stronger brand and wider
recognition, which can include increased opportunity to build clinical activity,
improved quality of candidates at recruitment. Investing in marketing also brings
smaller less measurable advantage that the Trust and its staff will be able to take
benefit from in a range of settings.
• Staff cost for marketing coordinator/manager = Band 5/6 (£24k to £32k p/a
FTE)
• Collateral cost for print and design = Annual budget - £200-1000 per job for
standard work, £10k to 20k for brand refresh
• Clinician time for promotional work and/or delivering training = within job plan,
additional PAs as identified in growth areas, plus loss in income from clinical
work undelivered
• Ad space buying & content marketing = £10k /year minimum
• Research/surveying time to measure impact = £5k
7.1. Focus on training
Develop wider suite of sessions based on needs of market/most inappropriate
referrals
6. Resources
7. Recommendations
TRUST BOARD PART 1 12. 322/18 TRUST STRATEGIES - ... Page 170 of 247

32 of 34
Reduce barriers to entry
Make costing and invoicing, and surrounding processes e.g. booking easier
Develop training packages designed to facilitate and encourage high quality care in
a ‘Sheffield Children’s @’ model.
Create promotional collateral
Thought leadership by trainers via blogs, attendance at conferences and
campaigns
7.2. Promote our Trust and strengthen our hand
Celebrate our successes
Emphasise our brand values
Advocate on behalf of children and young people
Promotion of paediatric healthcare as a career, with resource packages, advertising
campaigns and visits with schools/colleges
Centre of excellence emphasis/development
Promotion of clinicians via website and conferences
Thought leadership via blogs, presentations and research
Conduct pre and post surveys to measure awareness and understanding of our
brand, brand values and key messages
7.3. Market and product development Investigation via MRIs, evaluation and expansion if appropriate
Research, innovation and intellectual property of products
7.4. Promote private care and desirable referrals
Emphasise our points of difference
Select appropriate services for private referrals – strategic decision required
Build relationships with providers of ancillary services such as transport and
accommodation to provide a seamless and high quality experience of care
Create promotional materials about private patient experience including travel,
accommodation etc.
Reduce barriers to access
TRUST BOARD PART 1 12. 322/18 TRUST STRATEGIES - ... Page 171 of 247

33 of 34
Standardise private patient liaison communication, payment processes
Foster links with embassies
Explore relationship with GOSH to share network
Target overlap areas for referrals
Place case studies with condition specific support networks
TRUST BOARD PART 1 12. 322/18 TRUST STRATEGIES - ... Page 172 of 247

REPORT TO THE TRUST BOARD OF DIRECTORS’ MEETING (PART 1) HELD ON 27 NOVEMBER 2018
RISK MANAGEMENT STRATEGY
Trust aims supported by this paper
Provide high quality patient experience and outcomes Lead improvements in paediatric care Build clinical and financial sustainability Discover new ways of improving child health through research, innovation and technology
Link to Board Assurance Framework
Failure to effectively deliver healthcare impacts on the safety and quality of patient experience, regulatory compliance and loss of confidence of the wider community
Failure to ensure that the Trust recruits staff in the right numbers and with the appropriate breadth of skills and competencies to deliver high quality services now and in the future.
Risk to clinical service viability due to failure to meet nationally defined standards or unfavourable changes to the commissioning of services
Failure to engage effectively with partner organisations and the local community threatens the ability of the Trust to deliver its strategic ambition.
Failure to develop our leadership, management and governance arrangements to ensure delivery of sustainable high quality person-centred care, support learning and innovation, and promote an open and fair culture prevents the Trust from demonstrating it is a Well Led organisation
Operational capacity constraints and failure to deliver transformation impact on our ability to deliver planned activity and manage demand impacting on operational efficiency, service quality and financial performance.
Purpose of the paper
To present to the Trust Board of Directors the Risk Management Strategy.
Summary of key points The Risk Management Strategy sets out a clear strategy for the Trust’s vision in relation to the management of risk, detailing the system and processes in place and highlighting roles and responsibilities. It has been produced in line with the Trust’s Corporate objectives in mind. The main aim of the strategy is to have a robust and well embedded risk management system which ensures that all risks are managed in line with the Board’s risk appetite which in turn will ensure Trust’s risks in relation to the delivery of services and care to patients are minimised, that the wellbeing of patients, staff and visitors is optimised and that the assets, business systems and income of the Trust are protected.
In order to do this the following objectives have been set:
Ensure Datix is embedded with the Trust not only within the Clinical Divisions but within the Corporate and Non Clinical Divisions
Embed Risk Management at all levels of the organisation to create a safety culture and lead and
TRUST BOARD PART 1 12. 322/18 TRUST STRATEGIES - ... Page 173 of 247

support staff to promote reporting.
Strengthen the read across of risks between Committees of the Board to ensure relevant Committees have sight of their relevant Risks and assurance is provided to the Board.
Develop a pro-active reporting culture to ensure the Trust is horizon scanning and not simply responding in a reactive way to risk management.
Develop processes for identifying themes and trends within incidents, complaints, claims, audit, service evaluations and patient feedback to enable dynamic risk controls by learning lessons and effecting change from these. Thereby reducing risk, improving patient safety and supporting the quality strategy.
Ensure all staff have the requisite knowledge, skills and information to consider risks within the Trust including risks relating to emergency planning and resilience.
Link Corporate and Clinical Governance to enable robust management of risks across the Trust
The strategy has been approved by the Risk and Audit Committee. Board Action required The Board is asked to approve the Risk Management Strategy, which has been reviewed by the Risk and Audit Committee and recommended for approval.
Author: Ms M Whittle, Head of Legal and Governance FOR APPROVAL
Executive Sponsor: Mrs S Shearer, Director of Nursing and Quality
TRUST BOARD PART 1 12. 322/18 TRUST STRATEGIES - ... Page 174 of 247

Ref No:
Sheffield Children’s NHS Foundation Trust
Risk Management Strategy
TRUST BOARD PART 1 12. 322/18 TRUST STRATEGIES - ... Page 175 of 247

Contents
1. PURPOSE 3
2. INTRODUCTION 3
3. DEFINITISONS 3
4. RISK APPETITE STATEMENT 4
5. VISIONAND AIMS 5
6. OBJECTIVES 5
7. RISK MANAGEMENT PROCESS 6
8. GOVERNACNE STRUCTURE 8
9. REPORTING 9
10. ROLES AND RESPONSIBILITIES 10
11. RISK CATEGORIES 10
12. TRAINING 11
13. REVIEW 11
14. REGULATORY FRAMEWORK AND REFERENCES 11
TRUST BOARD PART 1 12. 322/18 TRUST STRATEGIES - ... Page 176 of 247

1. PURPOSE The purpose of this document is to set out a clear strategy for the Trust’s vision in relation to the management of risk, detailing the system and processes in place and highlighting roles and responsibilities.
2. INTRODUCTION
Risk is an inherent part of the delivery of healthcare. It is integral to our approach to quality improvement and good governance, being a central part of strategic and operational management. Risk management includes identifying and assessing risks and responding to them. This risk management strategy outlines the Trust’s approach to risk management throughout the organisation.
The Risk Management Strategy is aligned with the Sheffield Children’s NHS Foundation Trust Corporate Strategy, The Quality Strategy and the Board’s Risk Appetite. It supports our progress towards achieving our aspirational goals set against the Well Led Framework, reducing risk to patients and staff and supporting sustainability of the organisation.
The strategy applies to all Trust staff, who are expected to take an active lead to ensure that risk management is a fundamental part of their operational area. All staff should recognise risk management as everyone’s business and staff should proactively identify risks, incidents, near misses and areas for improvement. There should be an open and supportive management culture. Managers at all levels are expected to make risk management a fundamental part of their approach to clinical and corporate governance. Patients and service users views, using patient feedback and experience should be utilised to promote effective management of risk as an opportunity for learning and improving the quality of services. Emergency Planning and Resilience risks should also be considered as part of an overall approach to risk management.
The Trust encourages an open culture that requires all Trust employees, contractors and third parties working within the Trust to operate within the systems and structures set out in relevant policies.
Considered risk taking is encouraged, together with experimentation and innovation within authorised and defined limits. The priority is to reduce those risks that impact on safety, and reduce our financial, operational and reputational risks.
Effective risk management ensures; there is a safe environment for staff, patients, visitors and members of the public; that there is best clinical care for patients; that we maximise resources available for patient care; our reputation is protected; we have effective partnership arrangements; and that services are commissioned and delivered to a high standard.
3. DEFINITIONS
TRUST BOARD PART 1 12. 322/18 TRUST STRATEGIES - ... Page 177 of 247

BAF – Board Assurance Framework
HAZARD – Something which has the potential to cause harm.
RISK – the chance of something happening, or a hazard being realised, that will have an adverse impact on the achievement of the Trust’s objectives and the delivery of high quality care. It is measured in terms of consequence and likelihood.
RISK MANAGEMENT – pro-active identification, classification and control of events and activities to which the Trust is exposed.
RISK APPETITE - is defined as ‘the amount and type of risk that an organisation is prepared to seek, accept or tolerate. The acceptable level of risk an organisation is prepared to take will vary from one organisation to another and will be indicative of the operating environment of the organisation.’
4. RISK APPETITE STATEMENT The risk appetite statement defines the Board’s appetite for each risk identified to the achievement of strategic objectives for the financial year in question. It will be refreshed and updated every year.
Risks throughout the organisation should be managed within the risk appetite, or where this is exceeded, action taken to reduce the risk. In order to facilitate this managers should use the risk appetite statement but should also refer to the Risk Matrix Appendix ….
The risk appetite statement and risk matrix will be communicated to relevant staff involved in the management of risks. In order to use the risk matrix it should always be read as the likelihood being 5. This should then be multiplied by the consequence, which should be identified by the matrix. This would then give a score. On the right hand side fo the matrix there is the indication of what score for each element would be acceptable and what would be classed as being suboptimal. The Trust will accept scores in the tolerable column, they will accept scores in the discomfort column as long as we are happy with the mitigations in place, and there would have to be very good reasons why a risk in the suboptimal column is being accepted. Clear mitigations and reasoning behind suboptimal risks will need to be given.
The current risk appetite is set out below under 9 different headings. This statement should be read in conjunction with the Risk Matrix from which the risk appetite statement is formulated:
Financial/ Value for Money – The Trust is prepared to invest for return and minimise the possibility of financial loss by managing risks to a tolerable level. Value and benefits considered, not just the cheapest price. Resources are allocated in order to capitalise on opportunities.
Compliance/ Regulatory – The Trust is willing to take some risk where challenge would be problematic but that we are likely to win that challenge and the gain of taking the risk would outweigh the adverse consequences.
TRUST BOARD PART 1 12. 322/18 TRUST STRATEGIES - ... Page 178 of 247

Innovation – The Trust is willing to challenge current working practices and pursue innovation. New technologies should be viewed in terms of key enablers of operational delivery. The Trust is willing to devolve authority here to management by trust rather than tight control.
Quality/ Patient Related Outcomes – The Trust has a preference for safe activities that have a low degree of inherent risks. The Trust will consider similar activities to elsewhere where they have not breached compliance to clinical standards and professional practice.
Patient Safety - The Trust has a preference for very safe activities that have a low degree of inherent risk. The Trust would consider similar activities to elsewhere where they have not resulted in adverse outcomes.
Reputation – The Trust has a tolerance for risks in this area limited to events where there is little chance of any significant repercussions for the organisation should there be failure. Mitigation should be in place for any undue interest.
Workforce/ Staff Engagement – The Trust is willing to take risks in relation to workforce and staff engagements that will offer potential high benefits to staff, patients and the organisation.
Performance – The Trust has a low degree of inherent risk in relation to compliance with performance standards (internal or external) where there is limited chance of adverse consequences to patient outcomes.
Partnerships – The Trust is willing to accept partnerships with management control, with Board oversight if these are strategic. There will be acceptance of some devolved decisions.
5 VISION AND AIMS The Trust vision is ‘to provide a healthier future for children and young people.’
AIM
Corporate aims –
Provide high quality patient experiences and outcomes
Empower motivated and compassionate staff
Lead improvements in paediatric care
Build clinical and financial sustainability
Discover new ways to improve children’s health
Risk Management Aim –
To have a robust and well embedded risk management system which ensures that all risks are managed in line with the Board’s risk appetite which in turn will ensure Trust’s risks in relation to the delivery of services and care to patients are minimised, that the wellbeing of
TRUST BOARD PART 1 12. 322/18 TRUST STRATEGIES - ... Page 179 of 247

patients, staff and visitors is optimised and that the assets, business systems and income of the Trust are protected.
6 OBJECTIVES Ensure Datix is embedded with the Trust not only within the Clinical Divisions but within the Corporate and Non Clinical Divisions
Embed Risk Management at all levels of the organisation to create a safety culture and lead and support staff to promote reporting.
Strengthen the read across of risks between Committees of the Board to ensure relevant Committees have sight of their relevant Risks and assurance is provided to the Board.
Develop a pro active reporting culture to ensure the Trust is horizon scanning and not simply responding in a reactive way to risk management.
Develop processes for identifying themes and trends within incidents, complaints, claims, audit, service evaluations and patient feedback to enable dynamic risk controls by learning lessons and effecting change from these. Thereby reducing risk, improving patient safety and supporting the quality strategy.
Ensure all staff have the requisite knowledge, skills and information to consider risks within the Trust including risks relating to emergency planning and resilience.
Link Corporate and Clinical Governance to enable robust management of risks across the Trust
7 RISK MANAGEMENT PROCESS
The Trust have a structured approach to risk management. Risks are identified, assessed and controlled and if appropriate, escalated or de-escalated through the governance mechanisms of the Trust. The Trust should work to identify not only current risks but also complete horizon scanning to be aware of risks that are likely to emerge in the future.
Adequate Risk Management by the Legal and Governance Department will identify themes and trends that run though risks, incidents, complaints, claims, inquests and audits in order to ensure there is appropriate organisational and Divisional learning and to ensure that the Trust engage in relevant patient safety initiatives.
Risk Management
Please refer to the Trusts Guidance on Assessing Risk Policy for the full information on how risks should be assessed and recorded. This strategy provides a brief overview of the process.
The following should be kept in mind when risk assessing.
RISK – is described as something that may happen and could prevent us from meeting its objectives. i.e risk of failure to maintain safe staffing levels.
TRUST BOARD PART 1 12. 322/18 TRUST STRATEGIES - ... Page 180 of 247

CAUSE – is the problem or issue that ‘could’ cause the risk to happen.i.e high sickness rate, difficulties in recruiting staff, inability to release staff for mandatory training.
EFFECT – is the result of something that will happen if we do nothing about the risk i.e. staff not receiving compulsory training in resus or blood safety
IMPACT – is the wider impact of the risk on the objectives if we do nothing i.e. increased safety risk to patients.
When identifying a risk the following steps should be undertaken:
Step 1 – Identify the hazard arising from the task or activity.
Step 2 – Decide who may be harmed (Trust or reputation/ Staff/ Service users/ Visitor/ Contractors/ Finances)
Step 3 – Consider current control measures and precautions to prevent the hazard from materialising.
Step 4 – Assess risk for categorisation (likelihood of occurrence and consequence, severity if they were to occur)
Step 5 – Identify other control measures which can be introduced to reduce the level of risk.
Step 6 – Record and review the assessment periodically.
When considering the Key controls – the actions put in place as preventative measures to lessen or reduce the likelihood or consequence of the risk happening and the severity if it does. You must ensure that each control (or action where a gap in control has been identified) has an owner (i.e. named individual) and a target completion date. Key controls must describe the practical steps that need to be taken to manage and control the risk.
Not all risks can be dealt with in the same way. The 5 T’s provide an easy list of options available to anyone considering how to manage risk:
Tolerate – the likelihood and consequence of a particular risk happening is accepted.
Treat – work is carried out to reduce the likelihood or consequence of the risk
Transfer – shifting the responsibility or burden for loss to another party e.g the risk is insured against or sub-contracted to another party.
Terminate – an informed decision not to become involved in a risk situation
Take the opportunity – actively taking advantage, regarding the uncertainty as an opportunity to benefit.
Good governance and risk management practice requires that a formalised risk assessment is carried out by a competent person to determine the significant risks associated with the provision of Trust services.
ALL risks should be entered into Datix and placed on the appropriate Corporate of Divisional Risk Register. Each risk should then have an action plan associated with the risk.
TRUST BOARD PART 1 12. 322/18 TRUST STRATEGIES - ... Page 181 of 247

Identifying Themes and Trends On a regular basis the Legal & Governance Department will review data from Risks, Incidents, Complaints, Claims, Inquests and Audits to obtain trend information. This will be analysed and fed back to the relevant Divisions/ Departments/ Groups and Committees to ensure that the Trust is fully aware of trends and to enable patient safety initiatives to be devised. The Legal & Governance Department will assist the Trust in identifying relevant actions, initiatives, controls or monitoring for relevant trends in order to support the Corporate aims. 8 GOVERNANCE STRUCTURE The Governance structure identifies the relevant committees and their relationship to the Board. Specific responsibilities in relation to this strategy, for the management of risk and assurance on its effectiveness are monitored by the following committees
Board – Receives reports from RAC and QC. They reviews risks of 20 and above for Board assurance and have sight of the BAF. The Board sets the risk appetite statement every year. Risk management of the Board is underpinned by a number of interlocking systems of control: The Board reviews risk principally through the following three related mechanisms:
BAF – sets out the strategic objectives, identifies risks in relation to each strategic objective along with the controls in place and assurances available on their operation. BAF can be used to drive the Board agenda.
Corporate risk register – is a high level operational risk register used as a tool for managing risks an monitoring actions and plans against them. Used correctly it demonstrates that an effective risk management approach is in operation within the Trust.
Annual Governance Statement – signed by the Chief Executive as the Accountable Officer and sets out the organisational approach to internal control. This is produced at the year end (following regular reviews of the internal control environment during the year) and scrutinised as part of the Annual Accounts process and brought to the Board with the Accounts
Finance and Resources Committee – Provide the Board of Directors with assurance concerning the development and delivery of the Trust’s Annual Business Plan.
Risk and Audit Committee (RAC)– Provides the Board of Directors with a means of independent and objective review of financial and corporate governance, assurance processes and risk management across the whole of the Trust’s activities both generally and in support of the annual governance statement.
Quality Committee (QC)– Obtains assurance that high standards of care are provided by the Trust and ,in particular, that adequate and appropriate clinical governance structures, processes and controls are in place throughout the Trust.
Executive Risk Management Committee – develops the risk management objectives and the trust board approve them as part of the ratification of this strategy
TRUST BOARD PART 1 12. 322/18 TRUST STRATEGIES - ... Page 182 of 247

The RAC and QC exist to provide assurance of the robustness of risk processes and to support the Board of Directors
Each Division and Corporate area will have a Quality Meeting where risk is discussed including the risk register, actions and any required escalation. Managed risks are monitored solely at these meetings.
9 REPORTING
Board of Directors
Quality CommitteeRisk and Audit
CommitteeFinance and Resurces
CommitteeBoard nominations and
remuneration CommitteeCommittee in Common
Trust Executive Group
Quality Committee
•Clinical Audit and Effectiveness Committee
•Drugs and Theraputics Committee
•Child Deah Overview Panel
•Mortality Review Group
•Infection Control Committee
•Point of Care Testing (POCT)
•Resuscitation Committee
•Trust Safeguardin Committee
•Mental Health Act Committee
•Education Board
•Care Experience Board
•Nursing Quality Board
Risk and Audit Committee
•Quality Committee
•Finance and Resource Committee
•Executive Risk Management Committee
Finance and Resources Committee
•Recovery and Transformation Board
•IM&T Strategy Board
•Information Governance Committee
•Hospital Development Project Board
•Sustainable Development Working Group
•Cash Managmeent Committee
Risk Rating Type of Risk Recorded as Review periods
TRUST BOARD PART 1 12. 322/18 TRUST STRATEGIES - ... Page 183 of 247

Risks are reported to the Divisional Quality Meetings, ERMC, QC, RAC and the Board . The chart above shows what is expected for the systematic review of risk based on their risk score. This risk score is taken from the risk matrix and applied to the Risk Appetite Statement.
10 ROLES AND RESPONSIBILITIES Chief Executive and Executive Directors Executive Directors are Executive Action Owners for risks graded 20 or above. Executive Directors should be aware of all risks 20 and above and be assured that these are being managed appropriately with adequate controls. They should also be assured that risks under 20 are being managed appropriately by the relevant Committees and Divisions. They should apply the Risk Appetite Statement to all risks. The Chief Executive is ultimately responsible for the Risks and should be assured that there is an adequate process for managing these. He should also make sure the Risk Appetite Statement is reviewed yearly to ensure it is relevant for the current board members. Non Executive Directors Non Executive Directors are expected to challenge risks and controls in place during the relevant Committee Meetings on order to make sure they themselves and they collectively as part of the Board are assured Risks are being adequately managed. They should apply the Risk Appetite Statement to all risks. Legal and Governance Department The Legal and Governance Department will assists Divisions, Executives and Non Executives in their roles. They will provide support and advice on the risk assessment process and how to apply the scoring systems and risk appetite statement. Legal and Governance will have oversight of all risks on the risk registers and will ensure these are regularly updated and managed as per the policy. Risks that are not managed appropriately will be escalated at Committees.
20-25 Risk Register BAF, Corporate or Divisional Monthly
12-16 Risk Register Corporate or Divisional 3 monthly
8-10 Managed / Risk Register* Divisional* or Department Internal 6 monthly
1-6 Managed Department Internal 12 monthly
TRUST BOARD PART 1 12. 322/18 TRUST STRATEGIES - ... Page 184 of 247

Associate Director of Corporate Affairs The Associate Director of Corporate Affairs is responsible for maintaining the BAF and will regularly meet with the Legal & Governance Department to discuss the relevant risks on the BAF. 11 RISK CATEGORIES
Likelihood
Consequence 1 2 3 4 5
Rare Unlikely Possible Likely Almost Certain
5 Catastrophic
5 10 15 20 25
4 Major 4 8 12 16 20
3 Moderate 3 6 9 12 15
2 Minor 2 4 6 8 10
1 Negligible 1 2 3 4 5
12 TRAINING Knowledge of how to manage risk is essential to the successful embedding and maintenance of effective risk management.
The Executive and Non Executive Director’s will receive board risk awareness training annually.
Trust senior managers will receive general risk awareness training, including risk assessment training, risk register training, and management of risk every 3 years via e-learning.
All new staff will receive risk awareness training and understanding the roles of risk management in the organisation at induction.
Existing staff will receive ad hoc bespoke training as required/ requested. This could either be face to face or e-learning, depending on the requirement.
Staff involved in risk management will receive individually addressed training according to their individual needs.
TRUST BOARD PART 1 12. 322/18 TRUST STRATEGIES - ... Page 185 of 247

13 REVIEW Risk Management strategy will be reviewed every 3 years at least. This will be reviewed by the Risk and Audit Committee and Executive Risk Management Committee 14 REGULATORY FRAMEWORK AND REFERENCES CQC Registration Regulations 2009 (Part4)
NHS Improvement’s Single Oversight Framework
Health and Safety Executive
Annual Governance Statement
NHS England’s Risk Management Policy and Process Guide 2015
Department of Health, Best Practice in Managing Risk, guidance on risk assessment and management in mental health 2007
TRUST BOARD PART 1 12. 322/18 TRUST STRATEGIES - ... Page 186 of 247

13. 323/18 CQC UNANNOUNCED VISITREPORTS

1
REPORT TO THE TRUST BOARD OF DIRECTORS’ MEETING (PART 1) HELD ON 27 NOVEMBER 2018
CQC UNANNOUNCED VISIT REPORTS
Trust aims supported by this paper
Provide high quality patient experience and outcomes Empower motivated and compassionate staff Lead improvements in paediatric care Build clinical and financial sustainability Discover new ways of improving child health through research, innovation and technology
Link to Board Assurance Framework
Failure to effectively deliver healthcare impacts on the safety and quality of patient experience, regulatory compliance and loss of confidence of the wider community
Failure to engage with our clinicians prevents the development / implementation of an effective clinical strategy that responds to the needs of patients and other health and social care partners and prevents us from capitalising on the use of research, innovation and technology
Failure to develop our leadership, management and governance arrangements to ensure delivery of sustainable high quality person-centred care, support learning and innovation, and promote an open and fair culture prevents the Trust from demonstrating it is a Well Led organisation
Operational capacity constraints and failure to deliver transformation impact on our ability to deliver planned activity and manage demand impacting on operational efficiency, service quality and financial performance.
Purpose of the paper
To present to the Trust Board if Directors details of the unannounced CQC Inspections of Community and Inpatient CAMHS Services that took place on 14th and 15th August 2018.
Summary of key points
Whilst considerable progress has been made in many areas across the CAMHS service it is evident that regulatory breaches remain in place and further improvement work and monitoring is required.
Action required
The Board is asked to note the report and the actions plans that are in place.
Author: FOR ASSURANCE
Executive Sponsor: Mrs S Shearer, Director of Nursing & Quality
TRUST BOARD PART 1 13. 323/18 CQC UNANNOUNCED V... Page 188 of 247

2
TRUST BOARD PART 1 13. 323/18 CQC UNANNOUNCED V... Page 189 of 247

3
UNANNOUNCED CQC INSPECTIONS OF COMMUNITY AND INPATIENT CAMHS
AUGUST 2018
1. Introduction
An unannounced inspection of both community (Tier 3) and inpatient (Tier 4) Child and Adolescent Mental Health Services (CAMHS) was undertaken on the 14th and 15th August.
The inspection was conducted in response to concerns received by the CQC about the safety, leadership and culture of the services. The inspection was conducted sooner than the planned CQC inspection that the Trust is expecting before the end of the financial year. The inspection was targeted to review the safe, responsive and well led domains for the community service, and the safe and well led domains of the inpatient service.
The CQC conducted the inspections by visiting the premises at Beighton, Becton and Centenary House, attending a handover and a meeting, reviewing care records, talking to frontline and managerial staff, patients and parents and by reviewing documents submitted during and after the inspection.
The CQC last inspected the services in June 2016 and rated services at that time as ‘Requires Improvement’. The CQC have not altered their rating following this inspection.
2. Specialist community mental health services for children and young people 2.1 Positive feedback Positive feedback in relation to approachable and visible leadership was received. The CQC acknowledged that since the last inspection the Section 136 suite and STAR team had ben established and that the datix incident system had been implemented. The team noted the improvement in the standard of the treatment rooms and that patient tracking systems had been implemented following the screening of referrals and job planning to help address waiting lists. Patients and families reported that staff were very understanding, polite and respectful and that they were very satisfied with treatment received. Patients and families also commented on the long waits some of them had experienced in accessing that treatment. 2.2 CQC recommendations The CQC noted breach of the following regulations :
Regulation 12 Safe care and treatment Half of the patient risk assessments contained brief or basic information. Only 1 out of 22 patient records contained a crisis plan
TRUST BOARD PART 1 13. 323/18 CQC UNANNOUNCED V... Page 190 of 247

4
Assessments in relation to the management and mitigation of environmental risks had improved since 2016, but some were not enacted by staff. For example there were some unsupervised young people in the building.
Regulation 17 Good governance There are significant waiting lists for assessment and treatment within the service. The key performance indicators (KPI) did not accurately assess service performance. (This relates to an agreed KPI with the CCG that the service will measure Referral to Assessment instead of Referral to Treatment. Whilst this is an agreed KPI, the service does have a large number of patients waiting for subsequent treatment) The risk register had not been reviewed Business Continuity Plans had not been updated A fire risk assessment had been renewed but a copy of the report was not available on site. Procedures for raising the alarm in relation to lone working in Centenary House were not robust.
Regulation 18 Staffing Staff had not received all the required mandatory training. Eight out of the 26 training elements had less than 75% compliance .
These regulations were breached in 2016 although the reasons for the breaches are not consistently the same. 2.3 The breaches have converted into the following MUSTS and SHOULDS Action the provider MUST take to improve
1. The trust must ensure that all staff receive mandatory training. 2. The trust must ensure that an effective system is in place to manage the waiting list.
Where waiting time exceeds 18 weeks, there must be an effective system to identify this as a risk and an effective plan to resolve this.
3. The trust must review the key performance indicators for the services to ensure these assess performance accurately.
4. The trust must ensure that risk registers are reviewed regularly. 5. The trust must consider standard use of crisis plans. 6. The trust must ensure that risk assessments are comprehensive and detailed with
the relevant information. 7. The trust must ensure that the identified mitigation and management techniques for
ligature anchor points are followed by staff.
Action the provider SHOULD take to improve
8. The trust should ensure that where ligature cutters are in place these are accessible quickly if required.
TRUST BOARD PART 1 13. 323/18 CQC UNANNOUNCED V... Page 191 of 247

5
Summary of finding 2.4 Actions taken
The CWAMHS division are reviewing their security and risk assessment processes in readiness for submission of the action plan to the CQC by the deadline of 14 November 2018. The work required to address the waiting list, which was also reflected in the 2016 CQC report is also under review. The fire risk assessment (and accompanying required actions) was obtained and actioned on the day of the inspection.
3. Child and Adolescent Mental Health Wards 3.1 Positive findings The CQC praised infection control and cleanliness procedures across the site and stated that staff at all levels of the service had the right skills and experience to perform their duties. They noted the ongoing challenges on one of the lodges but acknowledged that leaders had flagged these concerns and put an action plan in place. The lodge concerned also received mixed feedback from patients and families on how friendly and respectful staff were. There were also some concerns on this lodge that it could be noisy and unsettled, although staff appeared to manage that well. Across the other lodges feedback was more positive in relation to cleanliness, adequate staffing and friendly and approachable staff . Concerns were raised about the length of time taken to address estates issues. 3.2 CQC recommendations The CQC noted the following regulatory breaches:
Regulation 12 Safe care and treatment
Staff were not clearly managing and mitigating ligature risks. Rooms designated as requiring staff supervision were left unlocked. Communal areas contained a number of risk items and these areas were left unsupervised. Staff did not keep appropriate records of medication. Prescription cards were incomplete and were not completed consistently.
Regulation 13 safeguarding service users from abuse and improper treatment
Staff had not responded to an allegation of abuse appropriately. This meant that staff did not understand how to protect patients from abuse and work with other agencies to do so. Staff had implemented restrictions which were not individualised to each patient’s presenting risks. It was not clear how the service was identifying and reviewing potential blanket restrictions.
TRUST BOARD PART 1 13. 323/18 CQC UNANNOUNCED V... Page 192 of 247

6
Regulation 17 Good governance
The trust had implemented guidance which meant that staff were not consistently reporting incidents of restraint. Incidents of restraint to support patients receiving nasogastric feeding were not consistently reported using the trust’s electronic incident reporting system. This meant that the trust’s data submission on the use of restraint did not fully reflect the number of restraints on each lodge. Systems were not operating effectively to identify areas of concern in relation to the safety of the lodges.
Regulation 18 Staffing
Not all staff had completed mandatory training. Average compliance was below the trust target. Compliance rates for training in approved restraint techniques was significantly below the trust target Managers did not consistently make sure staff were competent for their roles. Staff supervision and appraisal rates were below the trust’s compliance target.
The CQC noted comparable breaches in 2016 but did not review all regulatory breaches from that inspection. 3.3 The breaches have converted into the following MUSTS and SHOULDS Action the provider MUST take to improve
1. The trust must ensure that staff report all incidents using the trust’s incident reporting system.
2. The trust must ensure that systems are put in place to ensure that staff receive feedback and learn from incidents.
3. The trust must ensure that managers and staff in the service understand their individual responsibilities to respond to concerns about potential abuse when providing care and treatment, including investigating concerns.
4. The trust must ensure that staff manage ligature risks in line with ligature risk assessments.
5. The trust must ensure that blanket restrictions are reviewed and ensure that all restrictions are individually risk assessed.
6. The trust must ensure patients have access to a nurse call system in the event of an emergency.
7. The trust must ensure that staff complete prescription cards appropriately and consistently and that cards are effectively audited.
8. The trust must ensure that staff receive appropriate support, training, professional development, supervision and appraisal as is necessary to enable them to carry out the duties they are employed to perform.
9. The trust must ensure that systems and processes operate effectively to enable them to assess, monitor and improve the quality and safety of the service provided.
Action the provider SHOULD take to improve
10. The trust should ensure that staff update risk assessments following every patient incident and that this is recorded consistently.
11. The trust should ensure that staff update risk assessments during risk assessment reviews and designate where there had been no changes in risk.
TRUST BOARD PART 1 13. 323/18 CQC UNANNOUNCED V... Page 193 of 247

7
12. The trust should ensure that all staff know and understand the duty of candour. 13. The trust should ensure that all staff understand whistleblowing procedures, including
the role of the Freedom to Speak Up Guardian, and are encouraged to raise concerns.
14. The trust should ensure action plans improve lodge environments to reduce ligature risks are completed.
15. The trust should ensure trust-wide policies which are overdue for review are reviewed and updated in line with best practice
4. Actions taken
The CWAMH division has appointed a temporary quality improvement manager to ensure that a comprehensive action planning process is in place. The community action plan was submitted on 13th November 2018 and the inpatient action plan is under development and will be submitted to the CQC on 19th November 2018. It should be noted that the CQC required action plan template is narrative in nature and therefore now needs to be transposed into a template the Trust can monitor. Action (3) related to a safeguarding allegation. This was addressed immediately by the Director of Nursing. Since the incident Becton staff have received training from the Local Authority Designated Officer (LADO) and daily safeguarding huddles put into place. The signed off actions for the community service include: Risk assessments:
The service will review and update all current risk assessments, prioritising higher risk young people, to reflect their current and known risks.
The audit criteria for the ‘monthly peer case note audit’ of Community CAMHS will be reviewed. The case note audit will recommence from the end of February 2019. An annual corporate audit of case notes will also take place in November 2018 and each year thereafter, following new audit criteria.
The quality of risk assessment completion will be measured monthly using a quality dashboard.
A nominated/named lead will be accountable in each team for undertaking the audit and ensuring shortfalls are rectified. The Modern Matron and Community CAMHS clinical lead will oversee these audits.
The service, in partnership with the inpatient CAMHS services, is reviewing nationally available patient risk assessment tools. This may provide a more robust standardised risk assessment form.
Crisis plans:
A cascade reminder in relation to appropriate recording of crisis plans will be sent to staff to remind about completion of crisis plans. The reminder will also be given verbally at all huddles and team meetings.
The service will work to produce a care planning model within the Carenote electronic application which includes crisis plans. This work will be shared with all staff through huddles and team meetings.
TRUST BOARD PART 1 13. 323/18 CQC UNANNOUNCED V... Page 194 of 247

8
The service will review the Trust’s current casenote audit standards, to ensure CAMHS best practice /standards are included, eg. a crisis plan.
These actions will ensure that all patient records include a crisis plan and that staff
are aware of the improved process. Management techniques for ligature:
The Centenary House Access Standard Operating Procedure (SOP) outlines management and mitigation plans when a young person visits the building and poses such risks. The SOP will be revised to reflect a request from other non-CAMHS services, who share accommodation space, to ensure practice is standardised and in line for their service risk assessments.The amended SOP will be sent to all staff in November 2018, by way of an update and will also be discussed at each team huddle and team meeting during this period.
An audit will be undertaken to establish if staff who use the Centenary House
accommodation are aware of and following the amended SOP. Audit to be completed by April 2019.
The case note audit standards will be reviewed to ensure that any known ligature
risks are documented within the risk assessment, which would subsequently direct them to follow the access SOP.
Waiting times: • Referral to first appointment
The service has an agreement with the local CCG that the longest wait from referral to first appointment is 18 weeks. The service is achieving 92% against this target and the current average wait is circa. eight weeks. The service has an average KPI compliance 98% annually. These waits are monitored through the Patient Tracker meetings with any potential breaches identified, the reasons why, noting actions required. Any changes to this practice will be incorporated in the KPI discussion with commissioners (see point 3). Appointments are agreed with family/patient as the service noted that if appointments are booked too early, the young people and families may have a change in circumstances, which can result in a WNB (Was Not Brought). The projected capacity needed for first appointments are matched in clinical job plans. Further discussions are taking place with the local CCG under a sustainability project. This plan will be reviewed together in January 2019 with to a view any changes are reflected in next year’s contract.
• First appointment to treatment
Over the past 9 months the service has had an action plan in place which included addressing first appointment to treatment times waits. The following actions are required
The service will revise job plans The service will implement an ‘up to six session’ treatment plan. (This will offer a follow-up appointment from assessment in a timely manner, avoids people waiting on a specific treatment pathway if not required and will ensure young people who are waiting for treatment are on the correct pathway and seen faster).
TRUST BOARD PART 1 13. 323/18 CQC UNANNOUNCED V... Page 195 of 247

9
Monitoring the effect/improvement through fortnightly Patient Tracker meetings. KPIs The service will revisit targets with local commissioners to ensure that the relevant performance indicators are being measured locally and in conjunction with the national benchmarking data. This links to the sustainability work programme. Risk register:
• The service will review its risk register at the Divisional Risk and Quality meeting (DRT/DQT) as per Trust policy.
Business Continuity Plan:
• The service will update the Community CAMHS business continuity plan, ensuring that it is captured in the annual corporate review cycle. This will clearly differentiate Community CAMHS from in-patient CAMHS.
Raising alert at Centenary:
• A review of the alert system will be undertaken at Centenary House. The service will work with Estates and the Landlord to install an appropriate panic alarm system.
Fire risk assessment:
• The business support team have already reviewed the fire risk assessment with oversight from the Trusts Fire Officer and Community CAMHS Service Manager, creating an action plan.
Mandatory training
• The service will review the mandatory training compliance on a monthly basis at the Community CAMHS Strategy and Performance meeting and escalate any concerns around accessing training or cancelled training sessions and review compliance by subject and teams. The service will work with L&D team to provide additional and E-learning access sessions.The service will ensure that all staff have protected time to undertake mandatory training. Additional mandatory sessions are being planned and will commence from February 2019 for staff to access so as to increase opportunities to access.
The actions for the inpatient lodges (currently in draft) include: Ligatures:
The service will review lodge ligature risk assessments to ensure that mitigating factors are appropriate in light of ongoing removal of ligatures points. This will include ensuring that the lodges have wireless electronic game controllers to further mitigate any risks. Where this is not possible the service will ensure that all electronic games equipment cables are boxed.
The service will ensure that the management of ligature points policy is reviewed to ensure it is in line with the reducing restrictive practices policy.
The service will inform staff of the outcome of the above reviews, once they are completed through team meetings via lodge managers.
The service will ensure that individual ligature risk are documented and assessed in
TRUST BOARD PART 1 13. 323/18 CQC UNANNOUNCED V... Page 196 of 247

10
patient records and therefore levels of staff observation and patient supervision are individualised according to known and currently risks. This includes access to rooms which are reviewed as part of the reducing restrictive practices/blanket rules work.
Medications:
• The service will include audit a pharmacy check section in to the monthly clinical practice (patient records) to include the following areas, identified by CQC in 2016 and 2018 Medications with reduced expiry dates when opened include date opened Drug chart allergy information consistent with care plan Record of 'leave' medicines being returned No abbreviations used Patient photographs present Kardex numbered Medication start dates documented
The service will introduce a new formatted drug kardex and carry out an audit of the new kardex, within a month of them being in place. The Head of Nursing for CAMHS and Trust’s Chief Pharmacist will meet with the service pharmacists to confirm audit frequency, in line with requirements. The Trust Pharmacy department will undertake a review of medicines management provision to in patient CAMHS facilities. Safeguarding: The service will increase staff awareness via an email circulation from the CAMHS
Head of Nursing to remind Becton staff of the escalation process in relation to reporting potential safeguarding issues.
The service will invite the Local Authority Dedicated Officer (LADO) to facilitate a update/training safeguarding session at Becton Centre for staff.
The service will ensure that Safeguarding escalation flow chart will be made available as an easy aid for staff on each lodge
The service will commence individual lodge and site ‘safety huddles’, where safeguarding incidents will be discussed as a standing agenda item.
Blanket Restrictions:
• The service will implement a revised Reducing Restrictive Intervention strategy and delivery plan which incorporates blanket restrictions.
• The service will carry out a staff survey in relation to establishing current knowledge and confidence around practice including restrictive interventions and blanket restrictions. The results of the survey will inform the training needs of the staff group.
• The service will developed a restrictive intervention / blanket restriction assessment and register, which will outline the current practice across a range of domains, which will identify restrictions that are in place, the rationale, mitigation and review timelines to ensure the service minimises restrictions and ensure patient safety
• NG Feeding recording:
TRUST BOARD PART 1 13. 323/18 CQC UNANNOUNCED V... Page 197 of 247

11
• The service will meet with legal and governance department to establish an agreed method of recording restraints whilst NG feeding in process. An action plan will developed to reflect planned changes in practice. National benchmark on other services practice e.g. Coburn centre (ELFT) and Newcastle CAMHS services to reflect best practice.
Systems operating effectively:
• The service will trend datix incidents and share learning at the CWAMH Quality Assurance fortnightly meeting. This learning will then be shared at Lodge team meetings, at which “Shared Learning from Incidents” will be a standing item on the agendas. Lodge team meeting will reflect the recording and sharing of lessons learnt
The service will undertake a review to look at options around the installation of a
nurse call system. An email has been sent to the QNIC discussion group to find out what national best practice is.
Training: A collaborative review of training to be undertaken with the division and learning and development team to ensure that staff can access training so that to meet mandatory training compliance. This will ensure:
Training compliance will be monitored at individuals Personal Development Reviews. There will be an aim to complete all PDRs by Quarter 3.
Extra provision of Conflict resolution training The service will ensure dedicated administrative resource in place to oversee
specific training recording and compliance/provision for CAMHS staff.
Supervision: Process to be put in place that records staff uptake of clinical supervision aiming to attain 90% per quarter.
5. Conclusion Considerable progress has been made in many areas across the CAMHS service. The hard work of the division should be recognised and acknowledged, particularly against considerable operational challenges. However, from a regulatory perspective it is evident that breaches remain in place and further improvement work, support and monitoring is required. The CQC did not re rate the services on this occasion. Given the continuation of regulatory breaches, some of which are consistent with those seen in 2016, increased focus in this area needs to be maintained in order to protect and improve on the current rating for the two services of ‘Requires Improvement’.
TRUST BOARD PART 1 13. 323/18 CQC UNANNOUNCED V... Page 198 of 247

14. 324/18 SOUTH YORKSHIRE ANDBASSETLAW ICS: MOU

REPORT TO THE TRUST BOARD OF DIRECTORS’ MEETING (PART 1) HELD ON 27 NOVEMBER 2018
SOUTH YORKSHIRE AND BASSETLAW ICS:
MEMORANDUM OF UNDERSTANDING
Trust aims supported by this paper
Provide high quality patient experience and outcomes Empower motivated and compassionate staff Lead improvements in paediatric care Build clinical and financial sustainability Discover new ways of improving child health through research, innovation and technology
Link to Board Assurance Framework
Failure to engage effectively with partner organisations and the local community threatens the ability of the Trust to deliver its strategic ambition
Purpose of the paper
To present to the Trust Board of Directors the final Memorandum of Understanding for South Yorkshire and Bassetlaw Integrated Care System (ICS) for 2018/19.
Summary of key points
The final version of the Memorandum of Understanding for South Yorkshire and Bassetlaw ICS for 2018/19 has been developed in negotiation with NHS England and NHS Improvement. The Level 2 go live date was 1 October 2018. The Memorandum of Understanding for 2018 builds on the Memorandum of Understanding signed by the SYB ICS Chief Executive on behalf of the system last year. It covers:
The national NHS priorities and deliverables (the NHS Constitution standards) The financial framework (all governing bodies and boards previously agreed the
framework) The ICS priority areas (also previously agreed)
The one area within the MOU yet to be finalised is the revised operating model and governance arrangements for 18/19, which is currently being worked through, both as part of a wider system governance review and with NHS England / NHS Improvement regional colleagues to ensure the ICS is empowered and enabled to deliver its responsibilities as a level 2 ICS. This will be taken forward through a process of enabled due diligence.
Board Action required The Board is asked to approve the Memorandum of Understanding.
Author: Mr W Cleary-Gray, Chief Operating Officer, South Yorkshire and Bassetlaw ICS TO APPROVE
Executive Sponsor: Mr J Somers, Chief Executive
TRUST BOARD PART 1 14. 324/18 SOUTH YORKSHIRE AN... Page 200 of 247
1
Memorandum of understanding for Integrated Care Systems
Dear Andrew,
We are writing to confirm South Yorkshire and Bassetlaw’s status as an Integrated
Care System (ICS), subject to collective agreement of all the leaders in your system,
and to describe the terms of this relationship with the national leadership bodies.
In order to enable the further development of the ICS approach in 2018/19, this
document sets out the national expectations of ICSs, the freedoms and flexibilities
that these systems will gain in return and how we will work to support system
leaders and their teams.
1. Objectives
ICSs are systems in which NHS commissioners providers, NHS England and NHS
Improvement, working closely with GP networks, local authorities and other
partners, agree to take shared responsibility (in ways that are consistent with their
individual legal obligations) for how they use their collective resources to improve
quality of care and health outcomes. They are expected to make faster progress
than other health systems in transforming the way care is delivered, to the benefit
of the population they serve.
ICSs will:
• re-design and integrate clinical and care pathways to better meet the needs of the local population, incorporating use of prevention and self-care where appropriate;
• develop population health management approaches that facilitate
the integration of services focused, in the first instance, on populations that are most at risk of developing acute illness and hospitalisation;
• work with key system partners and stakeholders including patients and residents and their democratic representatives, health and care staff, local government and the voluntary sector;
• take collective responsibility for managing financial and operational performance, quality of care (including patient/user experience) and health and care outcomes;
• implement new methods of payment that support integration of services and population health management approaches, whilst enabling delivery of a shared system control total;
TRUST BOARD PART 1 14. 324/18 SOUTH YORKSHIRE AN... Page 201 of 247

2
• create more robust cross-organisational arrangements to tackle the systemic
challenges that the health and care system is facing;
• act as a leadership cohort, demonstrating what can be achieved with strong local
leadership, operating with increased freedoms and flexibilities; and
• commit to developing and disseminating learning, together with the national
bodies, so that other systems can develop ICSs.
2. National NHS priorities and deliverables
The NHS guidance for refreshing 2018/19 plans confirmed the priorities set out in Next
Steps on the Five Year Forward View. These include to:
improve investment in, access to and the quality of mental health services as defined in Implementing the Five Year Forward View for Mental Health and the planning round refresh;
promote better prevention and earlier diagnosis of cancer, as well as increasing access to innovative and timely treatments that improve survival, quality of life and
patient experience;
stabilise general practice, ensuring measures are in place to maximise GP retention
and recruitment, and support the development of primary care networks that
improve access and share assets and workforce. In time these networks will
collaborate to expand the range of services available in the community, including
proactive services aimed at keeping people well and/or prevent acute
deterioration;
redesign and strengthen the urgent and emergency care system through successful
implementation of the UEC transformation programme. This includes delivering
national operational standards, the 2018/19 ambitions on “Reducing long stays in
hospital - to reduce patient harm and bed occupancy” and urgent and emergency
mental health care for people of all ages;
transform the treatment, care and support available to people of all ages with a learning disability, autism or both so that they can lead longer, happier, healthier lives in homes not hospitals; and
continue to make maternity services in England safer and more personal through the implementation of the Better Births guidance.
The national deliverables that underpin these priorities are set out in Annex 1 of this
document for ease of reference.
We are also expecting ICSs to go further than other systems in driving improvement
across the clinical priority areas including:
reaching 100% coverage of self-identified primary care networks (PCNs) by the
end of 2018/19. We expect PCNs to be: functionally sharing assets and
workforce and consistently delivering care through integrated teams to high risk
TRUST BOARD PART 1 14. 324/18 SOUTH YORKSHIRE AN... Page 202 of 247

3
groups; making use of data to understand their populations, identifying variation
in resource use and outcomes, and guiding clinical decision making; acting as a
core partner in system decision making. We will work with each ICS over the
summer to agree the level of primary care network maturity that systems expect
to achieve by March 2019, and that would represent a step change in the delivery
of integrated primary care during 2018-19. We will also co-produce with ICSs
appropriate measures to assess progress and impact, aligned with the national
Primary Care Network Programme;
enhancing resilience of systems before next winter, for example by improving system-level working across urgent and emergency care and improving resilience in care homes through implementation of the Enhanced Health in Care Homes framework;
working in partnership with the National Mental Health Team to develop and implement actions to improve system-level working across all local partners for Mental Health delivery in 2018/19, and work towards a system-wide mental health investment strategy, and credible mental health workforce plan for 2019/20;
working through, and as an active member of your Cancer Alliance, and in partnership with the National Cancer Programme, to implement the National Cancer Taskforce’s recommendations1.
1 http://www.cancerresearchuk.org/sites/default/files/achieving_world-class_cancer_outcomes_-
_a_strategy_for_england_2015-2020.pdf
TRUST BOARD PART 1 14. 324/18 SOUTH YORKSHIRE AN... Page 203 of 247

4
3. Integrating care
In addition to making progress on these core priorities, ICSs will lead the way in
integrating health and care services at the population and person level, including in the
following ways.
Analysing patterns of need, health and care utilisation, cost and other metrics
by population segment. These analyses should help ICSs identify population
groups that should receive proactive care with the objective of preventing
illness or hospitalisation and reducing inequalities. Nationally we will work
with ICSs to design a mechanism that can provide a common and consistent
source of data to support benchmarking, peer learning and improvement.
Using these analyses to redesign care with a view to providing proactive
services to at-risk population groups and coordinating different services for
them. We will support ICSs with practical learning derived from the new care
models programme as well as other models used internationally.
As population analytical methods will initially be snapshots, ICSs will
increasingly need to build the digital infrastructure that allows for real-time
analyses, patient ‘tracking’ and actionable insight. We will provide ICSs with
advice on interoperability, information governance and, where necessary and
appropriate investment.
With support from the national team, ICSs will be required to make significant
progress from baseline assessment towards full maturity of the three
population health management capabilities and develop a system-wide plan
setting out locally determined population health priorities.
TRUST BOARD PART 1 14. 324/18 SOUTH YORKSHIRE AN... Page 204 of 247

5
4. Local priorities and deliverables
As well as delivering the priorities outlined in our system operating plan, the ICS
leadership commits to take responsibility for developing a shared system strategy and
plan to oversee transformation delivery in the following high priority deliverables in
2018/19:
Summary:
The next stage of building and strengthening primary care networks
Building capacity and capability for population health management
Implementing the next stage of the hospital services review and
corresponding SYB out of hospital strategy
Implementing a system efficiency approach together with governance arrangements and efficiency boards.
ICS Function Priority Area Actions
Strategy, Planning and Transformation
Governance arrangements Build on existing partnership arrangements to establish robust arrangements for level 2 ICS governance which are inclusive and transparent.
Review of governance arrangements for ICS at level 2 moving to level 3 by 2019/20
Including the future role of provider Committees in Common, and the Joint Committee of CCGs
Develop and implement Accountable Care Partnership (ACP) Integration Agreement within the ICS and each of its five Places
SYB ICS strategy 2018/19 – 2019/20 Refresh SYB system plan
Refresh STP plan to create strategy todeliver level 3 ICS by April 2019
Working with each of the five places,develop Out of Hospital/ Shift leftstrategy in parallel with HospitalServices Review next stage
Patient and public involvement
Undertake Hospital Services Reviewcommunications / engagement/consultation in line with StrategicOutline Case and Outline BusinessCase process
Strengthening capacity and capability
Develop Human ResourcesFramework for ICS
Provider development
Hospital Services Review – next stage
Successful implementation of next stage of the Hospital Services Review (HSR)
Agree collective response to the HSR. Develop Strategic Outline Case and
OBC (following the national assuranceprocess)
Develop Pre-Consultation BusinessCase / Decision Making Business Case
Meet change assurance process Procurement arrangements with
ACPs
TRUST BOARD PART 1 14. 324/18 SOUTH YORKSHIRE AN... Page 205 of 247

6
Population health and primary care
Integrated primary care networks Take forward development of primary care at scale and integrated primary care networks
Support ACPs to deliver nationalrequirements
Develop ICS out-of-hospital model Develop SYB population health plan
for 2019/20
Population health management Building and strengthening population health management capability in each place and across the system
Develop population health capacity and capability in partnership, with each of the five ACPs making good progress towards being a middle range system by 2019/20
For each of the five ACPs, enable all local care networks to achieve a level of maturity that ensures consistent coverage of new models of integrated primary care underpinned by population health management
Adopt integrated ways of working within the five localities that bring together local networks, including community services, with secondary care redesign – to support whole place-based care
Finance, contracting, capital and estates
Finance Building on finance strategy and making best use of resources
Develop financial strategy, governanceand mechanisms underpinned by thenational financial framework for ICSsand aligned with system-wideprovider /commissioner finance andefficiency plans and payment reform
Estates and capital planning Strengthening capital and planning capability and capacity
Develop estates strategy and capitalplans to support systemtransformation
Review capacity and capability andrequirements for 2018/19 andbeyond
Contracting Establishing system approach to contracting
Implement ‘system commissioning’lead contracting models and new(outcomes based) paymentmechanisms
Develop outcomes-based contracts(i.e. alliance, ICP contract model) toincentivise quality of care andpopulation health management
System efficiency Establishing a system approach to improving efficiency
Implement SYB ICS Efficiency Board tooversee system efficiency programme
Implement priorities for 2018/19 anddevelop priorities for 2019/20
Integrated assurance and improvement
Single assurance framework
Establishing a mutual accountability model and integrated assurance approach
Work with the regions and centralsponsor to establish how the ICS willbe enabled to have a shared oversightrole
Develop and implement mutualaccountability model building on
TRUST BOARD PART 1 14. 324/18 SOUTH YORKSHIRE AN... Page 206 of 247

7
existing work and approaches Deliver integrated ICS System
Operational Plan Develop 2019/20 system plan and
priorities via the local planning roundwith the five Places
TRUST BOARD PART 1 14. 324/18 SOUTH YORKSHIRE AN... Page 207 of 247

8
5. Transformation funding
ICSs have been given transformation funding delegated to a host CCG on behalf of an ICS
to support the implementation of integrated care and the local priorities set out above.
This transformation funding package is set out in Annex 2. We will also be taking steps
where possible to increase the flexibility of transformation funding streams dedicated
to specific priorities from 2019/20 and beyond.
Financial governance arrangements
Definitive allocations are subject to NHS England and NHS Improvement approval for
ICSs to go live. Prior to the release of any of the additional devolved funding included in
this package each ICS will need to demonstrate:
Governance and accountability arrangements so it is clear how decisions are made and who is accountable for delivering value for money from the expenditure.
A value based allocation process for determining the use of the funding.
Arrangements for oversight and reporting of expenditure and tracking of benefits realisation.
TRUST BOARD PART 1 14. 324/18 SOUTH YORKSHIRE AN... Page 208 of 247

9
6. Managing collective resources
i) System improvement plan
You have committed to operating as a live ICS and as such, you are required to work within your system improvement plan as detailed below. You have been given the flexibility, on a net neutral basis, and in agreement with NHS England and NHS Improvement, to vary individual control totals during the planning process and to agree in-year offsets of financial over-performance in one organisation against financial under-performance in another.
ii) Incentive scheme
You have selected the 50% partial PSF/CSF Option as set out in NHS England and NHS Improvement’s letter of 15 May 2018.
The tables in Annex 3 set out the organisation control totals, system control total and Provider Sustainability Funding allocations for your system. They also set out the quarterly phasing of the Provider Sustainability Funding by type for each organisation, which will reflect the incentive scheme you have chosen.
As you have agreed a system improvement plan, Annex 3 also shows the calculation of the starting point for your system improvement plan and the level of performance at which you will begin to ‘earn back’ lost PSF.
The calculation for the amount of PSF to be earned-back is below.
The maximum amount of PSF that can be earned-back will be capped at the
lost PSF from the ICS's share of the £650m, which in SYB's case is £2,363,000.
Earned-back PSF will be paid at the financial year-end based on full year
financial performance.
Trust Finance PSF is linked to the delivery of individual control totals and
System PSF is linked to the delivery of the system improvement plan.
Trust A&E PSF is linked to delivery of A&E performance at acute trust level, or
where the acute trust does not achieve - at A&E Delivery Board level, provided
the trust has met its individual control total, subject to any agreed net-neutral
changes or in-year offsets between organisations. For trusts without an A&E,
the PSF associated with this element (30% of the total) will be paid based on
individual control total performance (as is the case for non-ICSs) and is shown
under Trust Finance PSF.
TRUST BOARD PART 1 14. 324/18 SOUTH YORKSHIRE AN... Page 209 of 247

10
Where the quarterly system improvement plan value as per Table 4 is not
achieved, the ICS will lose System PSF (finance) at a rate of £1.50 per £1 of
system underperformance compared to the system improvement plan value.
This will be lost pro rata in each trust up to the maximum System PSF
(finance) available in that quarter (as per Table 2), unless an alternative
distribution is agreed between the ICS and NHSE/I, prior to the quarter end.
Any lost System PSF can be recovered in later quarters if the system recovers
its cumulative position to achieve its system improvement plan value.
Similarly, lost Trust PSF (finance) can also be recovered in later quarters if the
trust achieves its cumulative individual control total. However, lost Trust PSF
(A&E) cannot be recovered.
Where the ICS earns its System PSF (finance) allocation in one quarter, but
then goes off-plan in subsequent quarters the funds it has previously received
will not be clawed back.
System PSF (finance), Trust PSF (finance) and Trust PSF (A&E) will be paid
quarterly and phased in the same way as for non-ICSs in line with the
applicable PSF/STF guidance.
iii) Single system operating plan
In the 2018/19 planning round, you set out a single system operating plan that aligns the activity and financial plans of CCGs and providers. We expect you to collaborate to manage income and expenditure as a system openly across commissioners and providers, working together to ensure you live within your agreed system improvement plan value during 2018/19.
iv) Capital and estates
As for STPs, you developed a system-wide estates and capital plan for submission in July. We asked that this should include sufficient focus on out-
of-hospital schemes. This STP capital process is the main channel for access to strategic capital in 2018/19.
TRUST BOARD PART 1 14. 324/18 SOUTH YORKSHIRE AN... Page 210 of 247

11
7. Oversight
We will progressively look to systems to manage and improve their own performance,
as well as transforming services to ensure they are clinically and financially sustainable.
We will develop an oversight model that empowers your system to take a shared or
leading role in decisions about oversight of trusts and CCGs, supported as necessary by
NHS England and NHS Improvement, and with a commitment to minimising the
administrative burden placed upon systems.
Regional teams will agree with ICSs how this oversight model will operate, taking into
account the maturity of system working, including governance and financial
management. This will include:
establishing a single governance forum, (led and hosted by the ICS, but with
input from regional teams) to review both system performance and the
performance of individual providers and CCGs.
agreeing an accountability framework setting out how oversight will work in
practice.
agreeing a work programme and timetable which identifies specific and tangible
changes that will be made to the relationship between NHS England, NHS
Improvement, the ICS and local trusts and CCGs.
General principles
In order to support system working and as the oversight model develops, all parties
agree to work by the following principles:
The ICS will interact with a single regional director, acting on behalf of both NHS
Improvement and NHS England. We are working towards having fully integrated
regional teams, as part of our wider plans for joint working.
Where underperformance is identified, the ICS will generally be responsible in
the first instance for working with local organisations to address the issue,
supported by regional teams of NHS England and NHS Improvement. Any NHS
England or NHS Improvement intervention required will, wherever possible, be
identified in consultation with and agreed with the ICS.
Any regulatory decisions e.g. to put a trust or CCG into special measures, will, as
now, be made by NHS England and NHS Improvement, but wherever possible in
consultation with and taking into account the views of the ICS.
NHS England/NHS Improvement will not generally engage with individual
providers or CCGs without the knowledge of the system and an invitation to
participate in the discussion.
National programmes will, wherever possible, work through and with the ICS to
ensure that challenge and support is in line with the needs of the system. Where
TRUST BOARD PART 1 14. 324/18 SOUTH YORKSHIRE AN... Page 211 of 247

12
there are national support offers focussed on systems, these offers will be agreed
with the ICS.
NHS England/Improvement will minimise ad hoc data and information requests.
Where additional data or information is sought, the ICS will be consulted before
the request is issued. Where additional data or information is being sought from
CCGs or trusts, we will, wherever possible, agree whether the request should
come from NHS England/NHS Improvement or the ICS.
These principles support a single route of communication, seek to enable the
system to focus on improving and transforming quality and efficiency of care and
reduce duplication of effort across our organisations. They also start a change in
the way the system operates which starts to enable resources to be utilised
differently both locally and in the regions.
establish a governance mechanism, in discussion with the regions and the national
team, to support this process
agree the principles and terms of reference which will guide the Enabled Due
Diligence process.
commit to defining through the accountability agreement:
‒ How the ICS will relate to a single regional director
‒ Which functional accountabilities and responsibilities will empower the
ICS
‒ The identification of any active interventions and their status
‒ How the ICS will be enabled through a single integrated assurance and
improvement delivery team
‒ How the ICS will be enabled to be assured once, as a system, for delivery
of the NHS Constitution, mandate and quality and financial performance
‒ How the ICS gives wider assurance to the system
‒ How the ICS is enabled though data and systems
‒ How the ICS is enabled through access to improvement capacity from NHS
England and NHS Improvement team
SYB, during its shadow phase, has started to test ways of working which start to model
the new assurance framework.
Specific additional agreements made between the region and the ICS
In addition to abiding by the above general principles, the regional team and the ICS also commit to the following specific actions:
Agreeing that the ICS will not create an additional layer for organisations or the system
A process of Enabled Due Diligence, together with the Regions (NHS England and NHS Improvement) and dedicated senior sponsor from the national team to:
TRUST BOARD PART 1 14. 324/18 SOUTH YORKSHIRE AN... Page 212 of 247

13
We commit to continue to build on this over the next year and as part of our due
diligence process would aim to strengthen and add clarity what we have begun to test:
Integrated Assurance
The SYB ICS through the ICS Chief Executive lead will interact with the single regional
director. The ICS lead will be supported by an integrated regional team from NHS
England and NHS Improvement.
Within the ICS, the ambition is for the assurance system to be led by a single integrated
team and Director. The Director will be responsible for the conduct of the NHS England
and NHS Improvement regulatory and assurance functions within South Yorkshire &
Bassetlaw, and will report to the ICS lead.
SYB ICS will have flexibility in how the process of assurance is delivered, locally. NHS
England and NHS Improvement will be supportive of any SYB assurance process which
does not conflict with national frameworks but encourages improved outcomes and
improved system management; operational and financial.
SYB will be assured once, as a system, for delivery of the NHS Constitution, mandate,
and quality as set out in its Single Operating Plan (April 2018).
The draft SYB ICS Single Assurance Framework sets out how the ICS plans to carry out
its assurance process.
There will be a separate assurance process for financial performance, linked to the
system control total and described in section 6.
The ICS leader will advise NHS England on the annual assessment of each individual
SYB CCG, against the Improvement & Assessment Framework. NHS England will retain
responsibility for the publication of the CCG annual assessment.
Regional Oversight
If SYB ICS performance is outside of a set of agreed triggers described, it will set out for
the regional team its proposal for improvement including:
Improvement plan
Monitoring of the standard at increased frequency
Any requirement for improvement support from the integrated regional team
If SYB ICS performance is outside of the agreed thresholds, then NHS England and / or
NHS Improvement retain the right to intervene in the system or individual organisation,
with the support of the ICS.
If SYB ICS wishes NHS England or NHS Improvement to exercise their wider powers of
intervention, the ICS will provide reasons and evidence to the Regional Director.
TRUST BOARD PART 1 14. 324/18 SOUTH YORKSHIRE AN... Page 213 of 247

14
An agreed suite of performance reports will be made available by NHS England and NHS
Improvement to SYB ICS, including on-line access to the relevant databases. This will
be under-pinned by a data sharing agreement.
The ICS will have access to improvement capacity from the NHS England clinical
networks and the NHSI improvement team.
Planning
On an annual basis, NHS organisations are required to develop an Annual Operating
Plan. For organisations and places within SYB, the assurance of these plans will be the
responsibility of the ICS.
The ICS will submit a single operating plan in line with national planning guidance and
the ICS strategy. This will be an integrated plan between providers and commissioners
based on “place” as the unit of planning.
The single operating plan will include specialised services and NHS England’s other
direct commissioning responsibilities in SYB.
The integrated assurance team will provide advice on the aggregate achievement
expected at SYB ICS level to contribute to the NHS plan as a whole.
TRUST BOARD PART 1 14. 324/18 SOUTH YORKSHIRE AN... Page 214 of 247

15
8. National support
NHS Improvement and NHS England will continue to support ICSs. We will:
Facilitate learning between systems including convening a regular ICS leads
development day. We will also continue to convene learning groups on specific topics
such as primary care development, population health and communications and
engagement. In addition, in 2018/19 we intend to start convening other professional
groups such as ICS programme directors.
Dedicate a senior ‘sponsor’ from the national team to support the ICS working with the
regional team to help source national expertise and help coordinate and control the
demands placed on local systems. This sponsor will also be able to provide hands-on
help in solving problems or removing barriers that inhibit ICS development.
Provide bespoke support to leadership teams drawing on the King’s Fund, NHS
Confederation and others. In addition to re-procuring leadership support similar to that
which we provided last year, we will expand our development offer in 2018/19 to
provide, for example, clinical leadership teams with a facilitated programme that builds
on Surrey Heartland’s Clinical Academy and Frimley’s 2020 programme.
Mobilise teams with specific expertise or tasked with solving common problems faced by
ICSs and other systems. For example, we already have teams assisting many systems
with the rollout of primary care networks. In 2018/19, we will provide hands-on
expertise around population health management approaches, engagement and
communication, and system financial management, resources and staff in our clinical
networks and improvement support from NHS Improvement. Other workstreams will
be developed in consultation with ICS leaders.
Continue to develop national strategy and policy with ICSs. The ICS community provides
an invaluable source of expertise on which we will draw in developing policy, for
instance on national financial architecture and incentives, the operating model for
integrated regional teams, and how national bodies should oversee and support
systems as they mature.
Promote a collaborative and open approach, working with the ICS community to
collectively solve problems and set future direction for the NHS. We commit to
communicating openly with you, providing support where we can and doing so at a
pace that supports the development of ICSs.
TRUST BOARD PART 1 14. 324/18 SOUTH YORKSHIRE AN... Page 215 of 247

16
Andrew Cash confirms collective agreement of South Yorkshire and Bassetlaw system
leaders
Matthew Swindells on behalf of NHS England and Kathy McLean on behalf of NHS
Improvement
TRUST BOARD PART 1 14. 324/18 SOUTH YORKSHIRE AN... Page 216 of 247

17
Annex 1: 2018/19 Deliverables
Reminder of 2018/19 deliverables – drawn from ‘Next Steps on the NHS Five Year Forward View’ published in March 2017
The NHS already has two-year priorities, set out in last year’s Planning Guidance and the March 2017 publication of the Next Steps on the NHS Five Year Forward View. This Annex confirms these deliverables for 2018/19.
For national targets we will, where appropriate, provide disaggregated STP and CCG-level improvement targets and templates to ensure plans are completed on a consistent basis.
1. Mental Health
Overall Goals for 2017-2019 We published Implementing the Mental Health Forward View in July 2016 to set out clear deliverables for putting the recommendations of the independent Mental Health Taskforce Report into action by 2020/21. The publication of Stepping Forward to 2020/215 in July 2017 provides a roadmap to increase the mental health workforce needed to deliver this. Making parity a reality will take time, but this a major step on the journey towards providing equal status for mental and physical health. These ambitions are underpinned by significant additional funding for mental health care, which should not be used to supplant existing spend or balance reductions elsewhere. Progress in 2017/18 • On track to ensure an extra 35,000 children and young
people are able to access services this year.• 70 new or extended community eating disorder services
funded and commissioned.• 81 new beds for Children and Adolescent Mental Health
Services (Tier 4) and at least another 50 beds will open by
Deliverables for 2018/19 Additional funding has now been built into CCG 2018/19 allocations to support the expansion of services outlined in this planning guidance and the specific trajectories set for 2018/19 to deliver the Five Year Forward View for Mental Health. Progress to be made against all deliverables in the Next Steps on the NHS Five Year Forward View and the Implementing the Mental
5 Stepping Forward to 2020/21: Mental Health Workforce Plan for England (Health Education England).
TRUST BOARD PART 1 14. 324/18 SOUTH YORKSHIRE AND BASSETLAW IC... Page 217 of 247
18
end of March 2018. • Expanded specialist perinatal care with over 5,000
additional women accessing these services between April and December 2017. Contracts awarded for four new Mother and Baby Units.
• Continued to meet the waiting time standard for early intervention in psychosis.
• Physical health checks and interventions for patients with severe mental illness in secondary care, with 60% of people in inpatient settings and 42% in community mental health teams receiving this to date.
• Health Education England (HEE) expects to provide over 600 training places for Improving Access to Psychological Therapies (IAPT) practitioners. At least 800 practitioners in primary care settings by March 2018.
• 10 mental health new care models up and running and an additional 7 go live by April 2018.
• CCGs have continued to meet the dementia diagnosis standard, which was at 68.3% by December 2017.
• Seven Global Digital Exemplar Mental Health Trusts, funded to identify trusts which they will partner with as ‘fast followers’.
Health Forward View in 2018/19 with all CCGs and STPs required to: • Each CCG must meet the Mental Health Investment
Standard (MHIS) by which their 2018/19 investment in mental health rises at a faster rate than their overall programme funding. CCGs’ auditors will be required to validate their 2018/19 year-end position on meeting the MHIS.
• Ensure that an additional 49,000 children and young people receive treatment from NHS-commissioned community services (32% above the 2014/15 baseline) nationally, towards the 2020/21 objective of an additional 70,000 additional children and young people. Ensure evidence of local progress to transform children and young people’s mental health services is published in refreshed joint agency Local Transformation Plans aligned to STPs.
• Make further progress towards delivering the 2020/21 waiting time standards for children and young people’s eating disorder services of 95% of patient receiving first definitive treatment within four weeks for routine cases and within one week for urgent cases.
• Deliver against regional implementation plans to ensure that by 2020/21, inpatient stays for children and young people will only take place where clinically appropriate, will have the minimum possible length of stay, and will be as close to home as possible to avoid inappropriate out of area placements, within a context of 150-180 additional beds.
• Continue to increase access to specialist perinatal mental health services, ensuring that an additional 9,000 women access specialist perinatal mental health services and boost bed numbers in the 19 units that will be open by the end of 2018/19 so that overall capacity is increased by 49%.
TRUST BOARD PART 1 14. 324/18 SOUTH YORKSHIRE AND BASSETLAW IC... Page 218 of 247

19
• Continue to improve access to psychology therapies (IAPT) services with, maintaining the increase of 60,000 people accessing treatment achieved in 2017/18 and increase by a further 140,000 delivering a national access rate of 19% for people with common mental health conditions. Do so by supporting HEE’s commissioning of 1,000 replacement practitioners and a further 1,000 trainees to expand services. This will release 1,500 mental health therapists to work in primary care. Approximately two-thirds of the increase to psychological therapies should be in new integrated services focused on people with co-morbid long term physical health conditions and/or medically unexplained symptoms, delivered in primary care. Continue to ensure that access, waiting time and recovery standards are met.
• Continue to work towards the 2020/21 ambition of all acute hospitals having mental health crisis and liaison services that can meet the specific needs of people of all ages including children and young people and older adults; and deliver Core 24 mental health liaison standards for adults in 50% of acute hospitals subject to hospitals being able to successfully recruit.
• Ensure that 53% of patients requiring early intervention for psychosis receive NICE concordant care within two weeks.
• Support delivery of STP-level plans to reduce all inappropriate adult acute out of area placements by 2020/21, including increasing investment for Crisis Resolution Home Treatment Teams (CRHTTs) to meet the ambition of all areas providing CRHTTs resourced to operate in line with recognised best practice by 2020/21. Review all patients who are placed out of area to ensure that have appropriate packages of care.
TRUST BOARD PART 1 14. 324/18 SOUTH YORKSHIRE AND BASSETLAW IC... Page 219 of 247

20
• Deliver annual physical health checks and interventions, in line with guidance, to at least 280,000 people with a severe mental health illness.
• Provide a 25% increase nationally on 2017/18 baseline in access to Individual Placement and Support services.
• Maintain the dementia diagnosis rate of two thirds (66.7%) of prevalence and improve post diagnostic care.
• Deliver their contribution to the mental health workforce expansion as set out in the HEE workforce plan, supported by STP-level plans. At national level, this should also specifically include an increase of 1,500 mental health therapists in primary care in 2018/19 and an expansion in the capacity and capability of the children and young people’s workforce building towards 1,700 new staff and 3,400 existing staff trained to deliver evidence based interventions by 2020/21.
• Deliver against multi-agency suicide prevention plans, working towards a national 10% reduction in suicide rate by 2020/21.
• Deliver liaison and diversion services to 83% of the population.
• Ensure all commissioned activity is recorded and reported through the Mental Health Services Dataset.
2. Cancer
Overall Goals for 2017-2019 Advance delivery of the National Cancer Strategy to promote better prevention and earlier diagnosis and deliver innovative and timely treatments to improve survival, quality of life and patient experience by 2020/21.
TRUST BOARD PART 1 14. 324/18 SOUTH YORKSHIRE AND BASSETLAW IC... Page 220 of 247

21
Progress in 2017/18 • Cancer survival at its highest ever with latest figures
showing that one-year cancer survival is up by over 2,000 people a year.
• 95.1% of people seen by a specialist within two weeks of an urgent GP referral for suspected cancer, with 5.1% more patients being seen in the 12 months to November 2017 than in the previous 12 months.
• Ten multidisciplinary rapid diagnostic and assessment centres in place across the country by March 2018, supporting patients with complex symptoms through to diagnosis.
• We are on track to deliver the largest radiotherapy upgrade programme in 15 years modern radiotherapy have now funded 26 new machines in 21 trusts in 2017/18.
• Half of the country’s Cancer Alliances have begun to roll out personalised follow-up after cancer treatment.
• Added 22 more drugs to the Cancer Drugs Fund, which have benefitted nearly 7,500 more patients, taking the total since the reformed CDF launched in July 2016 to 15,700 patients having benefited from 52 drugs treating 81 different cancers.
Deliverables for 2018/19 • Ensure all eight waiting time standards for cancer are met,
including the 62 day referral-to-treatment cancer standard. The ‘10 high impact actions’ for meeting the 62 day standard should be implemented in all trusts, with oversight and coordination by Cancer Alliances. The release of cancer transformation funding in 2018/19 will continue to be linked to delivery of the 62 day cancer standard.
• Support the implementation of the new radiotherapy service specification, ensuring that the latest technologies, including the new and upgraded machines being funded through the £130 million Radiotherapy Modernisation Fund, are available for all patients across the country.
• Ensure implementation of the nationally agreed rapid assessment and diagnostic pathways for lung, prostate and colorectal cancers, ensuring that patients get timely access to the latest diagnosis and treatment. Accelerating the adoption of these innovations helps meet the 62 days standard ahead of the introduction of the 28 day Faster Diagnosis Standard in April 2020.
• Progress towards the 2020/21 ambition for 62% of cancer patients to be diagnosed at stage 1 or 2, and reduce the proportion of cancers diagnosed following an emergency admission.
• Support the rollout of FIT in the bowel cancer screening programme during 2018/19 in line with the agreed national timescales following PHE’s procurement of new FIT kit, ensuring that at least 10% of all bowel cancers diagnosed through the screening programme are detected at an early stage, increasing to 12% in 2019/20.
• Participate in pilot programmes offering low dose CT scanning based on an assessment of lung cancer risk in
TRUST BOARD PART 1 14. 324/18 SOUTH YORKSHIRE AND BASSETLAW IC... Page 221 of 247

22
CCGs with lowest lung cancer survival rates. • Progress towards the 2020/21 ambition for all breast cancer
patients to move to a stratified follow-up pathway after treatment. Around two-thirds of patients should be on a supported self-management pathway, freeing up clinical capacity to see new patients and those with the most complex needs. All Cancer Alliances should have in place clinically agreed protocols for stratifying breast cancer patients and a system for remote monitoring by the end of 2018/19.
• Ensure implementation of the new cancer waiting times system in April 2018 and begin data collection in preparation for the introduction of the new 28 day Faster Diagnosis standard by 2020.
3. Primary Care
Overall Goals for 2017-2019 Stabilise general practice today and support the transformation of primary care and for tomorrow, by delivering General Practice Forward View and Next Steps on the NHS Five Year Forward View.
Progress in 2017/18 • 52% of the country now benefitting from extended access
including appointments on evenings and weekends, beating the target of 40% for 2017/18.
• Primary care workforce: o Over 770 additional GP trainees started specialist
training since 2015 baseline (3,157 in total in 2017/18);
o Begun GP international recruitment, with the first 100 GPs being recruited;
Deliverables for 2018/19 Progress against all Next Steps on the NHS Five Year Forward View and General Practice Forward View commitments. This includes all CCGs: • Providing extended access to GP services, including at
evenings and weekends, for 100% of their population by 1 October 2018. This must include ensuring access is available during peak times of demand, including bank holidays and across the Easter, Christmas and New Year periods.
• Delivering their contribution to the workforce commitment
TRUST BOARD PART 1 14. 324/18 SOUTH YORKSHIRE AND BASSETLAW IC... Page 222 of 247

23
o Launched the GP Retention Scheme; o Recruitment of an additional 505 clinical pharmacists,
in addition to the 494 already in post. • Investment in general practice continues to increase on
track to deliver the pledged additional £2.4 billion by 2021. • CCGs investing in line with expectations set out in the
2017/18 NHS’s Planning Guidance, for additional primary care transformation investment (£3/head) over two years.
• Invested in upgrading primary care facilities, with 844 schemes completed and a further 868 schemes in development.
to have an extra 5,000 doctors and 5,000 other staff working in primary care. CCGs will work with their local NHS England teams to agree their individual contribution and wider workforce planning targets for 2018/19. At national aggregate level we are expecting the following for 2018/19:
o CCGs to recruit and retain their share of additional doctors via all available national and local initiatives;
o 600 additional doctors recruited from overseas to work in general practice;
o 500 additional clinical pharmacists recruited to work in general practice (CCGs whose bids have been successful will be expected to contribute to this increase);
o An increase in physician associates, contributing to the target of an additional 1000 to be trained by March 2020 (supported by HEE);
o Deliver increase to 1,500 mental health therapists working in primary care.
• Investing the balance of the £3/head investment for general practice transformation support.
• Actively encourage every practice to be part of a local primary care network, so that there is complete geographically contiguous population coverage of primary care networks as far as possible by the end of 2018/19, serving populations of at least 30,000 to 50,000.
• Investing in upgrading primary care facilities, ensuring completion of the pipeline of Estates and Technology Transformation schemes, and that the schemes are delivered within the timescales set out for each project.
• Ensuring that 75% of 2018/19 sustainability and resilience funding allocated is spent by December 2018, with 100% of the allocation spent by March 2019.
TRUST BOARD PART 1 14. 324/18 SOUTH YORKSHIRE AND BASSETLAW IC... Page 223 of 247

24
• Ensuring every practice implements at least two of the high impact ‘time to care’ actions.
• In all practices, delivering primary care provider development initiatives for which CCGs will receive delegated budgets, including online consultations.
• Where primary care commissioning has been delegated, providing assurance that statutory primary medical services functions are being discharged effectively.
• Lead CCGs expected to commission, with support from NHS England Regional Independent Care Sector Programme Management Offices, medicines optimisation for care home residents with the deployment of 180 pharmacists and 60 pharmacy technician posts funded by the Pharmacy Integration Fund for two years.
4. Urgent and Emergency Care
Overall Goals for 2017-2019 Redesign and strengthen the urgent and emergency care system to ensure that patients receive the right care in the right place, first time.
Progress in 2017/18 • More patients able to speak to a clinician about their urgent
and emergency care needs when calling NHS 111 – 40% of answered calls now receive clinical input, up from 22% last year.
• Piloted and evaluated NHS 111 Online in a number of areas, with 27% of the population now able to access urgent and emergency care advice through this online portal.
Deliverables for 2018/19 • Ensure that aggregate performance against the four-hour
A&E standard is at or above 90% in September 2018, that the majority of providers are achieving the 95% standard for the month of March 2019. Also Trusts are expected to improve on their performance each quarter compared to their performance in the same quarter the prior year in order to qualify for STF payments.
TRUST BOARD PART 1 14. 324/18 SOUTH YORKSHIRE AND BASSETLAW IC... Page 224 of 247
25
• 110 Urgent Treatment Centres (UTCs) designated according to the revised standard specification.
• Ambulance Response Programme implemented in all English mainland ambulance trusts.
• 105 Trusts received capital funding of £96.7 million to implement front-door clinical streaming. Over 90% of Trusts now have this in place.
• 1,491 beds have been freed up as a result of reducing delayed transfers of care (DTOC).
• £30 million awarded to 74 areas to increase number of acute hospitals meeting the ‘Core 24’ standard for 24/7 mental health liaison teams.
• 97% of A&Es, 98% of the initial cohort of UTCs and 96% of e-prescribing pharmacies now have access to primary care records through either summary care records or local record sharing portals.
• Implementation of the NHS 111 Online service to 100% of the population by December 2018.
• Access to enhanced NHS 111 services to 100% of the population, with more than half of callers to NHS 111 receiving clinical input during their call. Every part of the country should be covered by an integrated urgent care Clinical Assessment Service (IUC CAS), bringing together 111 and GP out of hours service provision. This will include direct booking from NHS 111 to other urgent care services.
• By March 2019, CCGs should ensure technology is enabled and then ensure that direct booking from IUC CAS into local GP systems is delivered wherever technology allows.
• Designate remaining UTCs in 2018/19 to meet the new standards and operate as part of an integrated approach to urgent and primary care.
• Work with local Ambulance Trusts to ensure that the new ambulance response time standards that were introduced in 2017/18 are met by September 2018. Handovers between ambulances and hospital A&Es should not exceed 30 minutes.
• Deliver a safe reduction in ambulance conveyance to emergency departments.
• Continue to make progress on reducing delayed transfers of care (DTOC), reducing DTOC delayed days to around 4,000 during 2018/19, with the reduction to be split equally between health and social care.
• Continue to improve patient flow inside hospitals through implementing the “Improving Patient Flow” guidance6. Focus specifically on reducing inappropriate length of stay for admissions, including specific attention on ‘stranded’ and
6
https://improvement.nhs.uk/resources/good-practice-guide-focus-on-improving-patient-flow/
TRUST BOARD PART 1 14. 324/18 SOUTH YORKSHIRE AND BASSETLAW IC... Page 225 of 247

26
‘super stranded’ patients who have been in hospital for over 7 days and over 21 days respectively.
• Continue to work towards the 2020/21 deliverable of all acute hospitals having mental health crisis and liaison services that can meet the specific needs of people of all ages including children and young people and older adults; and deliver Core 24 mental health liaison standards for adults in 50% of acute hospitals, subject to hospitals being able to successfully recruit.
• Ensure that fewer than 15% of NHS continuing healthcare full assessments take place in an acute setting.
• Continue to progress implementation of the Emergency Care Data Set in all A&Es (Type 1 and Type 2 by June 2018; and Type 3 by the end of 2018/19).
• Increase the number of patients who have consented to share their additional information through the extended summary care record to 15% and improve the functionality of e-SCR by December 2018.
• Implement a proprietary appointment booking system at particular GP practices, 50% of integrated urgent care services and 50% of UTCs by May 2018, supported by improved technology and clear appointment booking standards issued by December 2018.
• Continue to rollout the seven-day services four priority clinical standards to five specialist services (major trauma, heart attack, paediatric intensive care, vascular and stroke) and the seven-day services four priority clinical standards in hospitals to 50% of the population.
TRUST BOARD PART 1 14. 324/18 SOUTH YORKSHIRE AND BASSETLAW IC... Page 226 of 247

27
5. Transforming Care for People with Learning Disabilities
Overall Goals for 2017-2019 Our goal is to transform the treatment, care and support available to people of all ages with a learning disability, autism or both so that they can lead longer, happier, healthier lives in homes not hospitals.
Progress in 2017/18 • 22% increase in the number of annual health checks
delivered by GPs to improve access to community alternatives to hospital and tackle premature mortality.
• New and expanded community teams to support people with a learning disability at risk of admission to hospital, backed by £10 million transformation funding.
• 6% reduction in inappropriate hospitalisation of people with a learning disability, autism or both, between March and November 2017, totalling a 14% reduction since March 2015. In addition, over 100 people previously in hospital for 5 years or more were discharged between March and November 2017.
• Tackling premature mortality by beginning to systematically review and learn from deaths of patients with learning disabilities by March 2018.
Deliverables for 2018/19 All Transforming Care Partnerships (TCPs), CCGs and STPs are expected to: • Continue to reduce inappropriate hospitalisation of people
with a learning disability, autism or both, so that the number in hospital reduces at a national aggregate level by 35% to 50% from March 2015 by March 2019. As part of achieving that reduction we expect CCGs and TCPs to place a particular emphasis on making a substantial reduction in the number of long-stay (5 year+ inpatients).
• Continue to improve access to healthcare for people with a learning disability, so that the number of people receiving an annual health check from their GP is 64% higher than in 2016/17. CCGs should achieve this by both increasing the number of people with a learning disability recorded on the GP Learning Disability Register, and by improving the proportion of people on that register receiving a health check.
• Make further investment in community teams to avoid hospitalisation, including through use of the £10 million transformation fund.
• Ensure more children with a learning disability, autism or both get a community Care, Education and Treatment Review (CETR) to consider other options before they are admitted to hospital, such that 75% of under 18s admitted to hospital have either had a pre-admission CETR or a CETR immediately post admission.
TRUST BOARD PART 1 14. 324/18 SOUTH YORKSHIRE AND BASSETLAW IC... Page 227 of 247

28
• Continue the work on tackling premature mortality by supporting the review of deaths of patients with learning disabilities, as outlined in the National Quality Board 2017 guidance.
6. Maternity
Overall Goals for 2017-2019 Continue to make maternity services in England safer and more personal through the implementation of the Better Births.
Progress in 2017/18 • Continuing the year on year safety improvements to
maternity services including, since 2010, a 16% reduction in stillbirths, 10% reduction in neonatal mortality and 20% reduction in maternal deaths.
• Seven maternity ‘early adopters’ established covering 125,000 births a year to implement specific elements of Better Births and service improvements. Pilots of continuity of carer established to over 3,000 women.
• 44 Local Maternity Systems established bringing together commissioners, providers and service users to lead and deliver transformation of maternity services in every part of the country.
• We will exceed the planned goal of 2,000 more women receiving specialist perinatal care in 2017/18, with over 5,000 additional women accessing these services between April and December 2017. Four new mother and baby units also funded.
Deliverables for 2018/19 • Deliver improvements in safety towards the 2020 ambition to
reduce stillbirths, neonatal deaths, maternal death and brain injuries by 20% and by 50% in 2025, including full implementation of the Saving Babies Lives Care Bundle by March 2019.
• Increase the number of women receiving continuity of the person caring for them during pregnancy, birth and postnatally, so that by March 2019, 20% of women booking receive continuity.
• Continue to increase access to specialist perinatal mental health services, ensuring that an additional 9,000 women access specialist perinatal mental health services and boost bed numbers in the 19 units that will be open by the end of 2018/19 so that overall capacity is increased by 49%.
• By June 2018, agree trajectories to improve the safety, choice and personalisation of maternity.
TRUST BOARD PART 1 14. 324/18 SOUTH YORKSHIRE AND BASSETLAW IC... Page 228 of 247

29
N.B. This is not a comprehensive list of ‘Next Steps’ deliverables for 2018/19, simply an ‘aide memoire’ covering these service improvement areas. CCGs and STPs should also continue to work to reduce inequalities in access to services and in people’s experiences of care.
TRUST BOARD PART 1 14. 324/18 SOUTH YORKSHIRE AND BASSETLAW IC... Page 229 of 247

30
Annex 2: Transformation Funding Package
South Yorkshire and Bassetlaw 2.73% Share of all weighted patients
INDICATIVE FIGURES (£m's)
ICS Transformation Funding 2018/19 Requirements/notes
1. Committed programme transformation funds
General Practice Forward View
- Access 7.53 Delivery of GPFV Access requirements
- Training Care Navigators 0.26 Funded from core Primary Care allocations for 2018/19 only
- Online Consultations 0.52 Funded from core Primary Care allocations for 2018/19 only
- Practice Resilience 0.21 Based on a Fair share % per registered patient applied as per the Primary Care team guidance
- Clinical Pharmacists 2 0.39 Delivery of GPFV requirements
- ETTF 1.17 Capital and revenue funds
Other Programmes
Mental Health 1.01 Tied to delivery of mental health requirements on IPS, Suicide, Perinatal, Liaison and CYP
Diabetes 1.89 Diabetes Next Steps FYFV objectives
Cancer 3.07 Indicative value for the ICS (from Cancer Alliance funds) to deliver the Cancer strategy
Maternity 0.76 Maternity Next Steps FYFV objectives
UEC 0.43 Indicative figures to be confirmed by the UEC team
STP infrastructure 0.28 STP infrastructure support - only applicable to ICS areas co-terminus with STPs
Sub Total 17.54
2. Uncommitted funds
Uncommitted Funds 6.94Released on acceptance of governance information and subject to acceptance of the incentive option.
Used to deliver national priorities
£1 per head population notionally allocated to primary care network development.
TOTAL 24.47
TRUST BOARD PART 1 14. 324/18 SOUTH YORKSHIRE AND BASSETLAW IC... Page 230 of 247

31
Annex 3: System improvement plan agreement
South Yorkshire and Bassetlaw (SYB)
50% partial
Table 1: Organisation control total, system control total and Provider Sustainability Funding allocations
Org Name Included in SCT
Control
Total
(excl.
PSF)
(£000s)
PSF
Allocation
(£1.8bn)
(£000s)
PSF
Allocation
(£650m)
(£000s)
Total PSF
Allocation
(£000s)
NHS Barnsley CCG 100% (600) - - -
NHS Bassetlaw CCG 100% (700) - - -
NHS Doncaster CCG 100% (700) - - -
NHS Rotherham CCG 100% (3,000) - - -
NHS Sheffield CCG 100% 0 - - -
CCG Subtotal (5,000) 0 0 0
Barnsley Hospital NHS Foundation Trust 100% (17,002) 5,880 2,389 8,269
Doncaster and Bassetlaw Teaching Hospitals NHS Foundation Trust 100% (22,853) 11,547 4,691 16,238
Rotherham Doncaster and South Humber NHS Foundation Trust 100% 668 987 401 1,388
Sheffield Children's NHS Foundation Trust 100% (1,613) 2,485 1,010 3,495
Sheffield Health and Social Care NHS Foundation Trust 100% 405 780 317 1,097
Sheffield Teaching Hospitals NHS Foundation Trust 100% (20,999) 18,562 7,541 26,103
The Rotherham NHS Foundation Trust 100% 2,919 5,817 2,363 8,180
Provider Subtotal (58,475) 46,058 18,712 64,770
System Total (63,475) 46,058 18,712 64,770
TRUST BOARD PART 1 14. 324/18 SOUTH YORKSHIRE AN... Page 231 of 247

32
Table 2: Quarterly phasing of the control total (excl. PSF) and Provider Sustainability Funding by type for organisations that accepted their CT
Org NameQ1
(£000s)
Q2
(£000s)
Q3
(£000s)
Q4
(£000s)
2018/19
Total
(£000s)
Barnsley Hospital NHS Foundation Trust CT (4,860) (4,839) (3,340) (3,963) (17,002)
Trust A&E PSF 372 496 744 868 2,481
Trust Finance PSF 743 990 1,486 1,733 4,952
System PSF 125 167 251 293 836
Total PSF 1,240 1,654 2,481 2,894 8,269
Doncaster and Bassetlaw Teaching Hospitals NHS Foundation Trust CT (8,670) (8,959) (4,500) (724) (22,853)
Trust A&E PSF 731 974 1,461 1,705 4,871
Trust Finance PSF 1,459 1,945 2,917 3,404 9,725
System PSF 246 328 493 575 1,642
Total PSF 2,436 3,248 4,871 5,683 16,238
Rotherham Doncaster and South Humber NHS Foundation Trust CT 178 174 170 146 668
Trust Finance PSF 187 250 374 437 1,248
System PSF 21 28 42 49 140
Total PSF 208 278 416 486 1,388
Sheffield Children's NHS Foundation Trust CT (2,780) (2,433) 1,525 2,075 (1,613)
Trust A&E PSF 157 210 315 367 1,049
Trust Finance PSF 314 419 628 733 2,093
System PSF 53 71 106 124 354
Total PSF 524 699 1,049 1,223 3,495
Sheffield Health and Social Care NHS Foundation Trust CT 104 102 102 98 405
Trust Finance PSF 148 197 296 345 986
System PSF 17 22 33 39 111
Total PSF 165 219 329 384 1,097
Sheffield Teaching Hospitals NHS Foundation Trust CT (8,693) (4,277) (5,339) (2,690) (20,999)
Trust A&E PSF 1,175 1,566 2,349 2,741 7,831
Trust Finance PSF 2,345 3,127 4,690 5,471 15,633
System PSF 396 528 792 924 2,639
Total PSF 3,915 5,221 7,831 9,136 26,103
TRUST BOARD PART 1 14. 324/18 SOUTH YORKSHIRE AN... Page 232 of 247

33
Table 3: Quarterly phasing of the control total and draft plan for CT non-acceptors (excl. PSF)
The Rotherham NHS Foundation Trust CT 120 811 1,300 688 2,919
Draft plan (6,300) (4,935) (4,974) (4,858) (21,067)
Total PSF** N/A N/A N/A N/A 8,180
Table 4: System improvement plan starting point (excl. PSF)
Org Name CT Acceptor
Starting
Point for
System
Improve
ment
Plan
£000s
Source
NHS Barnsley CCG Y (600) Final CT
NHS Bassetlaw CCG Y (700) Final CT
NHS Doncaster CCG Y (700) Final CT
NHS Rotherham CCG Y (3,000) Final CT
NHS Sheffield CCG Y 0 Final CT
CCG Subtotal (5,000)
Barnsley Hospital NHS Foundation Trust Y (17,002) Final CT
Doncaster and Bassetlaw Teaching Hospitals NHS Foundation Trust Y (22,853) Final CT
Rotherham Doncaster and South Humber NHS Foundation Trust Y 668 Final CT
Sheffield Children's NHS Foundation Trust Y (1,613) Final CT
Sheffield Health and Social Care NHS Foundation Trust Y 405 Final CT
Sheffield Teaching Hospitals NHS Foundation Trust Y (20,999) Final CT
The Rotherham NHS Foundation Trust N (21,067) Draft plan
Provider Subtotal (82,461)
System Total (87,461)
** CT non-acceptors will not have PSF paid quarterly, but the system may ‘earn back’ some of this PSF at the end of the year.
Details of the earn back calculation are included within NHS Improvement’s letter of 15 May 2018 and Section 6 ii) of the MoU.
TRUST BOARD PART 1 14. 324/18 SOUTH YORKSHIRE AN... Page 233 of 247

15. 326/18 ICS - MONTH 6 FINANCEPOSITION

REPORT TO THE TRUST BOARD OF DIRECTORS’ MEETING (PART 1) HELD ON 27 NOVEMBER 2018
MONTH 6 INTEGRATED CARE SYSTEM REPORT
Trust aims supported by this paper
Build clinical and financial sustainability
Link to Board Assurance Framework
Risk that we do not maintain financial stability due to failure to deliver our financial plan or the negative impact of movement to a system-wide financial planning regime, resulting in requirements for additional CIPs or reduction in level and standard of services.
Failure to manage the Trust’s cash position would result in the Trust not being able to satisfy its obligations in respect of pay and non-pay costs.
Failure to engage effectively with partner organisations and the local community threatens the ability of the Trust to deliver its strategic ambition.
Purpose of the paper
To present to the Trust Board of Directors the updated position.
Summary of key points
The ICS System Improvement Plan Value is measured before PSF. Both the year to date and forecast position before PSF are showing favourable variances. However, there is a need to improve the current run rate in order to deliver the system improvement plan value. Current forecast is £3.5m better than plan (previous month £0.8m).
Year to date reported position is a favourable variance against plan of £3.4m excluding PSF; all organisations are currently forecasting break even or better against plan before PSF. RDASH have declared an improved forecast of £2.1m to benefit from the NHSI incentive scheme.
Sheffield Teaching Hospitals has not achieved its A&E PSF in Q2 as performance is less than Q2 in 2017/18 resulting in an adverse PSF variance f £2.7m, £1.6m for Q2.
CIP and QIPP schemes are forecast behind plan, QIPP schemes are slightly ahead year to date, CIP schemes are behind. There is a need to ensure that a strong focus remains on CIP and QIPP delivery.
Key ICS financial risks are:
o Plan Alignment Gap: There is a £15.6m plan alignment gap between commissioners and provider within the Doncaster and Bassetlaw and Sheffield systems.
o CIP / QIPP Delivery Gap: There is a £29.2m stretch on CIP/QIPP delivery compared to 2017-18 outturn.
TRUST BOARD PART 1 15. 326/18 ICS - MONTH 6 FINANC... Page 235 of 247

o CIP / QIPP Phasing: CIP plans are phased 67% in the last six months and QIPP plans are phased 55% in the last six months.
Board Action required The Board is asked to note the reported position at Month 6 and the risks to achievement of the system.
Author: Jeremy Cook, ICS Director of Finance FOR NOTING
Executive Sponsor: Mr M Smith, Director of Finance
TRUST BOARD PART 1 15. 326/18 ICS - MONTH 6 FINANC... Page 236 of 247

Page 1 of 8
FINANCE UPDATE
SOUTH YORKSHIRE AND BASSETLAW INTEGRATED CARE SYSTEM EXECUTIVE STEERING GROUP
November 2018
Author(s) Jeremy Cook, ICS Director of Finance
Sponsor Will Cleary-Gray, ICS Chief Operating Officer
The report is for approval OR noting
Noting
Links to the STP (please tick)
Reduce inequalities
Join up health and care
Invest and grow primary and community care
Treat the whole person, mental and physical
Standardise acute hospital care
Simplify urgent and emergency care
Develop our workforce
Use the best technology
Create financial sustainability
Work with patients and the public to do this
Are there any resource implications (including Financial, Staffing etc)?
There is a risk of loss of System PSF if the system does not meet its quarterly phased system improvement
plan value up to an annual cap of £5.7m. The M6 position shows that Q2 system PSF has been secured with
a £3.3m favourable variance on plan. This means, as Q1 & Q2 is confirmed, that £2.2m of the £5.7m
system PSF is secure. The residual risk for the remainder of the year is £3.5m.
Summary of key issues
Key messages
1. The ICS System Improvement Plan Value is measured before PSF. Both the year-to-date and forecast positions before PSF are showing favourable variances. However, there is a need to improve the current run-rate in order to deliver the system improvement plan value. Current forecast is £3.5m better than plan (previous month £0.8m).
2. Year to date reported position is a favourable variance against plan of £3.4m excluding PSF; all organisations are currently forecasting break even or better against plan before PSF. RDASH have declared an improved forecast of £2.1m to benefit from the NHSI incentive scheme.
3. Sheffield Teaching Hospitals has not achieved its A&E PSF in Q2 as performance is less than Q2 in 2017/18 resulting in an adverse PSF variance of £2.7m, £1.6m for Q2.
TRUST BOARD PART 1 15. 326/18 ICS - MONTH 6 FINANC... Page 237 of 247

Page 2 of 8
4. CIP & QIPP schemes are forecast behind plan, QIPP schemes are slightly ahead year-to-date, CIP schemes are behind. There is a need to ensure that a strong focus remains on CIP and QIPP delivery
5. Key ICS financial risks are: o Plan Alignment Gap: There is a £15.6m plan alignment gap between commissioners and
provider within the Doncaster & Bassetlaw and Sheffield systems; o CIP / QIPP delivery gap: There is a £29.2m stretch on CIP/QIPP delivery compared to 2017-
18 out-turn; o CIP / QIPP phasing: CIP plans are phased 67% in the last six months and QIPP plans are
phased 55% in the last six months.
Recommendations
The Board is asked to note the position at Month 6 and the risks to achievement of the system improvement plan.
TRUST BOARD PART 1 15. 326/18 ICS - MONTH 6 FINANC... Page 238 of 247

Page 3 of 8
South Yorkshire and Bassetlaw ICS Finance Report Month 6 – September 2018
Financial reporting
1. Performance against System Improvement Plan:
2. The year to date reported position (before PSF) across the ICS is a favourable variance against plan of £3.5m (£2.3m at Month 5); all organisations are currently forecasting break even or better against plan before PSF, but are reporting to their boards a range of risks and challenges to be managed in year if this position is to be delivered, particularly in the light of CIP/QIPP slippage.
3. The YTD actual position excluding PSF represents 65% of plan for the first five months (6/12=50%), meaning expenditure needs to be slowed to pull it back to the planned deficit system improvement plan (£81.5m). This is reflective of the phasing of efficiencies being back-ended in the second half of the year. There is a need to improve the current run-rate in order to deliver the system improvement plan value; forecast position based on current run rate is £105.5m compared to plan of £81.5m.
TRUST BOARD PART 1 15. 326/18 ICS - MONTH 6 FINANC... Page 239 of 247

Page 4 of 8
4. System Performance including PSF :
5. Sheffield Teaching Hospitals has reported non-achievement of PSF in Q1 and Q2 as A&E performance in
Q1 and Q2 18/19 was worse than in 17/18. This has adversely impacted both YTD variance and forecast variance for that organisation. It does not impact on achievement of the System Improvement Plan value or achievement of organisational PSF linked to financial performance or system PSF.
TRUST BOARD PART 1 15. 326/18 ICS - MONTH 6 FINANC... Page 240 of 247

Page 5 of 8
Efficiency
6. Efficiency Plan analysis is provided below:
7. Based on the information reported to NHSE/NHSI, efficiency plans are YTD £0.8m behind plan overall (£1.8m behind at Month 5). The improvement being mainly due to a move from adverse to favourable of £0.9m for DBH, a £0.7m increase in over delivery on Rotherham CCG and a favourable move for Barnsley FT. QIPP overall is £0.1m ahead of plan Year to date. Forecast for QIPP at year end is £1.3m adverse against plan.
8. CIP and QIPP schemes are forecasting a shortfall of £2.8m against plan (£2.7m at Month 5). This is due to Sheffield CCG forecasting an under achievement of £2.6m against plan (£2m last month) reflecting the CCG position reported to Governing Body in October. In addition to the under achievement for Sheffield Children’s of £1.6m full year forecast as reported last month.
9. CCGs are required to submit monthly monitoring returns to NHSE before full contract monitoring and prescribing data is available, which means the return is based on estimates using prior month data. This can mean revised positions are reported to CCG Governing Bodies when a full data set is available for the relevant month.
TRUST BOARD PART 1 15. 326/18 ICS - MONTH 6 FINANC... Page 241 of 247

Page 6 of 8
10. CIP underperformance of £2.6m at Sheffield Teaching Hospitals is primarily due to unidentified CIPs
and underperformance of individual schemes. This is currently forecast to recover by the year end.
11. Sheffield Children’s Hospital is currently showing an under performance of CIP of £0.6m and is forecasting an under performance of £1.6m by year end. This is the main element of a forecast shortfall of £1.5m for CIP for the system.
12. Delivery of efficiency plans represents the single largest financial risk to the system in 2018/19. In line with the proposed financial framework, forecast positions are planned to be managed initially by organisations and then by places before system-escalation.
13. The next System Efficiency Board meeting is scheduled for 16 November 2018 and the agenda will look to further explore the transformation opportunities outlined in the GIRFT/Model Hospital and Right Care joint assessments alongside the identified workstream opportunities across pathways and variation, business strategy, workforce and digital.
Risks
Background
14. Information on downside risks and mitigating actions were requested from provider and commissioner organisations based on Month 5 data. This identified two of the four places with the highest level of risk as Sheffield and Doncaster & Bassetlaw. This does not underestimate the challenges in the Barnsley and Rotherham places to deliver their financial plans.
15. It was therefore agreed that ICS finance meet with the two places and the following organisations that declared unmitigated risk. These were :
Doncaster & Bassetlaw Teaching Hospitals NHS FT (DBTH)
Sheffield Teaching Hospitals NHS FT (STH)
Sheffield Children’s Hospital NHS FT (SCH)
Sheffield CCG (SCCG)
Sheffield place
16. Further work has been undertaken to refine the gross risk against achievement of plan for the Sheffield place which currently stands at £8.7m although further work is currently being undertaken at SCH to ensure all risks have been captured. Further mitigating actions have been identified, including the retention of £750k of transformation funding for SCH, which potentially would bring the place to an in year balanced position. However there are significant risks which need to be managed and monitored closely.
17. There is some in year alignment risk between SCCG and STH and SCH but these are not material and
are likely to be resolved through ongoing contract discussions. There are alignment issues with STH and SCH and Specialised Commissioning although the risk primarily rests with Specialised Commissioning which is out-with the assessment of the systems financial performance. Discussions are ongoing to quantify the level of misalignment and further actions.
18. Sheffield City Council is currently overspent and they are reviewing their plans to look at the scope to
mitigate risk. This could have implications for NHS organisations.
TRUST BOARD PART 1 15. 326/18 ICS - MONTH 6 FINANC... Page 242 of 247

Page 7 of 8
Doncaster and Bassetlaw place 19. DBTH took a paper to its Financial Oversight Committee on the Month 6 forecast position which
identified the following
Best case £1.8m favourable to plan ex PSF Most realistic (£2.9m) adverse to plan ex PSF Worst case (£13.2m) adverse to plan ex PSF
20. The most realistic assumption assumes that the Trust will receive an adjustment of £3m to its control total due to the decision by NHSE/I to put a hold nationally on the implementation of the Wholly Owned Subsidiary schemes unless they had already been approved by Trust Boards. The Trust has requested that its control total be adjusted to reflect this.
21. Work is ongoing to establish the level of any forecast plan alignment risks between DBTH and
22. RDASH has submitted a revised plan that is £2m better than its control total and Doncaster CCG and Bassetlaw CCG are showing no unmitigated risk. Therefore the Doncaster and Bassetlaw place, based on DBTH most realistic outcome, identifies £0.9m unmitigated risk ((£2.9m) + £2m).
23. The risks will continue to be monitored on a monthly basis by the ICS.
Other risks
24. Risks identified by providers and commissioners, referred to in 14 above reflect that provider CIP plans are back-end loaded with 67% planned for the second half of the year. Therefore achievement becomes more stretching as the year progresses. CCG plans are more evenly distributed with 55% in the second half of the year.
25. Q1 and Q2 System PSF (£2.2m of £5.7m) is now secured given overall delivery of the pre-PSF financial position. STH did not achieve A&E PSF for Q1 or Q2.
26. There remains a residual System-PSF risk for all providers of £3.5m (£5.7m available less Q1 & Q2 delivery) if the system does not achieve the phased quarterly system improvement value. This will become more difficult to achieve in later quarters due to the phasing of efficiency plans.
Financial reporting
27. Financial reporting will continue to be developed to ensure that it is fit for purpose as an ICS and that partners have sufficient detail to understand the risks within organisational plans in order that mitigating action can be undertaken at organisation, place and system as required.
28. The ICS has approval from the 7 provider organisations to access monthly financial returns to NHSI.
This will allow further granularity of CIP performance to be identified. In addition, the ICS has commenced conversations with NHSI regarding a “data-sharing-agreement” which should identify any further data which could usefully be utilised at ICS level.
29. The dates for the Finance and Activity Committee have now been agreed on a monthly basis from November to March and nominations have been received from:
TRUST BOARD PART 1 15. 326/18 ICS - MONTH 6 FINANC... Page 243 of 247

Page 8 of 8
Julia Newton, CCG CFO representation
Steve Hackett, Mental Health Trust representative
Jon Sargeant – Acute Trust representative
30. The meetings have been scheduled to ensure that finance and activity data can be discussed as soon as possible after month end reports to NHSE/I are concluded
Jeremy Cook Director of Finance South Yorkshire & Bassetlaw ICS 9 November 2018
TRUST BOARD PART 1 15. 326/18 ICS - MONTH 6 FINANC... Page 244 of 247

16. 327/18 ANY OTHER BUSINESS

17. 328/18 IDENTIFICATION OF KEYRISKS, SUCCESSES, DECISIONSMADE TO BE ESCALATED / SHAREDFROM THE MEETING

18. 329/18 DATE OF NEXT PUBLICMEETING: Tuesday 18 December 2018,08:30 Boardroom
Related Documents