Tropisetron for Treating Established Postoperative Nausea and Vomiting: A Randomized, Double-Blind, Placebo- Controlled Study Eli Alon, MD*, Eric Buchser, MDt, Eduardo Herrera, MDS, Frank Christiaens, MDS, Christian De Pauw, MD/I, Linda Ritter, MST, Frank Hulstaert, MD, MS#, and Vito Grimaudo, MD** Anesthesiology Departments of *Zurich University Hospital, tMorges Hospital, SFribourg Cantonal Hospital, Switzerland, SBrussels Akademisch Ziekenhuis VUB, IlEek Heilig Hartkliniek, IInternational Institute for Drug Development, Brussels, #Sandoz Pharma Ltd Brussels, Belgium, and **Sandoz-Wander Pharma Ltd, Berne, Switzerland Tropisetron can prevent postoperative nausea and vomiting (PONV) at doses smaller than those used to control chemotherapy-induced nausea and vomiting. In this placebo-controlled study, the efficacy and toler- ability of three different doses of tropisetron were com- pared for the treatment of established PONV after sur- gical procedures in general anesthesia. Of 1513 patients who satisfied inclusion criteria, 314 experiencing PONV during the first 2 h after recovery from anesthe- sia were treated with one of three different doses of tro- pisetron (0.5,2, or 5 mg) or placebo, administered IV as a single dose. Patients were then observed during 24 h for efficacy and tolerability. All three doses of tropise- tron were significantly better than placebo in control- ling emetic episodes and in reducing the need for rescue treatment. There were no significant differences among the three doses. However, in the subgroup of patients who had previous PONV, and in those randomized for nausea alone, the 2-mg and 5-mg doses controlled emetic episodes better than the 0.5-mg dose. All studied doses of tropisetron were well tolerated and did not affect vital signs. We conclude that a single IV adminis- tration of tropiestron significantly reduces the recur- rence of emetic episodes in patients with established PONV after elective surgery with general anesthesia. Its optimal dose seems to be 2 mg. Implications: Three hundred-fourteen patients suffering from postopera- tive nausea and vomiting received different IV doses of a new antiemetic drug, tropisetron, to determine the lowest effective dose. We found that a single IV admin- istration of tropisetron significantly reduced postoper- ative nausea and vomiting after elective surgery with general anesthesia. (Anesth Analg 1998;86:617-23) T ropisetron, a highly potent and selective antagonist of serotonin type 3 receptors (5-HT,), has proven to be effective and well tolerated against nausea and vomiting induced by chemotherapy and radiotherapy (1). It is also effective and well tolerated in the prevention of postoperative nausea and vomiting (PONV). Its opti- mal dose was found to be 2 mg (2-4). This study was designed to investigate the efficacy and tolerability of three different doses of tropisetron for the treatment of established PONV in patients after elective surgery. This study was funded by Sandoz Pharma Ltd. The results were presented in part at the fourth annual congress of the European Society of Anaesthesiologists, London, June l-5, 1996. Accepted for publication November 19, 1997. Address correspondence and reprint request to Eli Alon, MD, Department of Anesthesiology, Ospedale Civico, 6903 Lugano, Switzerland. 01998 by the International Anesthesia Research Society 0003.2999/98/$5.00 Methods This was a multicenter, prospective, randomized, double-blind, placebo-controlled, parallel-group trial comparing the efficacy and tolerability of three differ- ent doses of tropisetron for treating established PONV. The protocol was approved by the ethics com- mittee at each study center. Eligible patients were ASA physical status I and II, 18-75 yr old, experiencing nausea lasting 210 min and/or emesis (vomiting or retching) within 2 h after recovery from general anesthesia. Patients who had vomited or had received antiemetics during the 24 h before surgery were excluded. Patients were also ex- cluded if they had a history of alcohol or drug abuse, or if they were known to have hypersensitivity reac- tions. Pregnant or lactating women were also ex- cluded, except for those in whom early termination of the pregnancy was part of the operation. Anesth Analg 1998;86:617-23 617

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript
Tropisetron for Treating Established Postoperative Nausea and Vomiting: A Randomized, Double-Blind, Placebo- Controlled Study
Eli Alon, MD*, Eric Buchser, MDt, Eduardo Herrera, MDS, Frank Christiaens, MDS,
Christian De Pauw, MD/I, Linda Ritter, MST, Frank Hulstaert, MD, MS#, and Vito Grimaudo, MD**
Anesthesiology Departments of *Zurich University Hospital, tMorges Hospital, SFribourg Cantonal Hospital, Switzerland, SBrussels Akademisch Ziekenhuis VUB, IlEek Heilig Hartkliniek, IInternational Institute for Drug Development, Brussels, #Sandoz Pharma Ltd Brussels, Belgium, and **Sandoz-Wander Pharma Ltd, Berne, Switzerland
Tropisetron can prevent postoperative nausea and vomiting (PONV) at doses smaller than those used to control chemotherapy-induced nausea and vomiting. In this placebo-controlled study, the efficacy and toler- ability of three different doses of tropisetron were com- pared for the treatment of established PONV after sur- gical procedures in general anesthesia. Of 1513 patients who satisfied inclusion criteria, 314 experiencing PONV during the first 2 h after recovery from anesthe- sia were treated with one of three different doses of tro- pisetron (0.5,2, or 5 mg) or placebo, administered IV as a single dose. Patients were then observed during 24 h for efficacy and tolerability. All three doses of tropise- tron were significantly better than placebo in control- ling emetic episodes and in reducing the need for rescue treatment. There were no significant differences among the three doses. However, in the subgroup of patients
who had previous PONV, and in those randomized for nausea alone, the 2-mg and 5-mg doses controlled emetic episodes better than the 0.5-mg dose. All studied doses of tropisetron were well tolerated and did not affect vital signs. We conclude that a single IV adminis- tration of tropiestron significantly reduces the recur- rence of emetic episodes in patients with established PONV after elective surgery with general anesthesia. Its optimal dose seems to be 2 mg. Implications: Three hundred-fourteen patients suffering from postopera- tive nausea and vomiting received different IV doses of a new antiemetic drug, tropisetron, to determine the lowest effective dose. We found that a single IV admin- istration of tropisetron significantly reduced postoper- ative nausea and vomiting after elective surgery with general anesthesia.
(Anesth Analg 1998;86:617-23)
T ropisetron, a highly potent and selective antagonist
of serotonin type 3 receptors (5-HT,), has proven to be effective and well tolerated against nausea and
vomiting induced by chemotherapy and radiotherapy (1). It is also effective and well tolerated in the prevention of postoperative nausea and vomiting (PONV). Its opti- mal dose was found to be 2 mg (2-4). This study was designed to investigate the efficacy and tolerability of three different doses of tropisetron for the treatment of established PONV in patients after elective surgery.
This study was funded by Sandoz Pharma Ltd. The results were presented in part at the fourth annual congress
of the European Society of Anaesthesiologists, London, June l-5, 1996.
Accepted for publication November 19, 1997. Address correspondence and reprint request to Eli Alon, MD,
Department of Anesthesiology, Ospedale Civico, 6903 Lugano, Switzerland.
01998 by the International Anesthesia Research Society 0003.2999/98/$5.00
Methods This was a multicenter, prospective, randomized, double-blind, placebo-controlled, parallel-group trial comparing the efficacy and tolerability of three differ- ent doses of tropisetron for treating established PONV. The protocol was approved by the ethics com- mittee at each study center.
Eligible patients were ASA physical status I and II, 18-75 yr old, experiencing nausea lasting 210 min and/or emesis (vomiting or retching) within 2 h after recovery from general anesthesia. Patients who had vomited or had received antiemetics during the 24 h before surgery were excluded. Patients were also ex- cluded if they had a history of alcohol or drug abuse, or if they were known to have hypersensitivity reac- tions. Pregnant or lactating women were also ex- cluded, except for those in whom early termination of the pregnancy was part of the operation.
Anesth Analg 1998;86:617-23 617

618 ALON ET AL. TROPISETRON FOR TREATMENT OF ESTABLISHED PONV
ANESTH ANALG 1998;86:617-23
After giving written, informed consent, patients meeting entry requirements were randomly assigned to receive an antiemetic treatment consisting of one of three different doses of tropisetron (0.5,2, or 5 mg) or placebo administered IV in 1 min. The randomization list was composed of balanced blocks of 12: 3~ tropi- setron 0.5 mg/0.5 mL, 3X tropisetron 2 mg/2 mL, 3X tropisetron 5 mg/5 mL, 1X placebo 0.5 mL, IX pla- cebo 2 mL, and IX placebo 5 mL. Blinding was guar- anteed by presentation of the study medication in identical glass ampules containing either 5 mg/5 mL of tropisetron or 5 mL of placebo. Depending on the instructions on the leaflet in the sealed study medica- tion box, 0.5, 2, or 5 mL of solution was drawn from the blind study ampoule into a 5-mL syringe and diluted with saline to a total volume of 5 mL. This was performed by a third person (a nurse) not participat- ing in the study in any other way.
Patients were then observed for assessment of effi- cacy and tolerability during 24 h after study drug administration. They could be given rescue antiemet- its at the discretion of the physician in case of anti- emetic treatment failure (severe nausea persisting more than 30 min after study drug administration, nausea and/or emesis occurring or recurring more than twice), or at their request. Baseline information included demographic data, physical status, and pa- tient medical history, with special attention paid to previous motion sickness and/or PONV. These data were, however, recorded for the purpose of explor- atory analysis.
For the purpose of exploratory analysis, the obser- vation period was divided into two assessment peri- ods: the first 4 h and the last 20 h. The occurrence of emetic episodes, the occurrence and severity of nau- sea, and the use of rescue antiemetics were recorded separately for these two periods. For the purpose of data collection, no distinction was made between vomiting and retching. Patients were also asked to assess the overall control of PONV during the 24-h period after study drug administration by using a 4-point scale: 1= excellent, 2 = good, 3 = satisfactory, and 4=unsatisfactory.
The criteria of tolerability and safety were the re- ported nature, severity, and frequency of adverse events in each treatment group during the 24-h obser- vation period and the recording of vital signs (blood pressure and heart rate) before and 1, 5, and 60 min after study drug administration. Oxygen saturation (Sao,) and sedation scores (l=awake, 2=asleep re- sponding to verbal command, 3 = asleep responding to physical stimulation, and 4=not arousable) were as- sessed before and 1, 5, and 60 min after study drug administration.
The primary efficacy variable was the proportion of patients with complete response for vomiting during the 24-h period after the administration of the study
drug. Complete response for vomiting was defined as the absence of emetic episodes (vomiting or retching) regardless of whether rescue treatment was given. A minimal sample size of 260 patients (in four groups of 65 patients) was selected to detect a 100% increase in response rate (patients with no further emetic epi- sodes) from an estimate of 25% with placebo to 50% with the optimal dose of tropisetron at a 5% signifi- cance level with 80% power. The differences in pro- portions among treatment groups were tested by us- ing 2 tests without continuity correction. A global test of all treatment groups versus placebo was followed by pairwise tests comparing placebo with each dose of tropisetron. A closed-test procedure (5) was used to ensure that the nominal level of significance was kept at 0.05. All tests were two-sided.
Further exploratory analyses of possible prognostic factors were performed using logistic regression mod- els. The following factors were considered: treatment group (each dose compared with placebo), center (each center compared with the others), sex, age (con- tinuous), weight (continuous), history of previous PONV (yes/no), history of motion sickness (yes/no), type of surgery (abdominal, nonabdominal), duration of anesthesia (continuous), use of postoperative opi- oids (yes/no), placement of a nasogastric tube (yes/ no), reason for randomization (emetic episodes or nausea alone), and use of rescue treatment for nausea before first emetic episode (yes/no). The odds ratio and 95% confidence intervals were calculated for all the variables in the final model, both unadjusted and adjusted for the other factors.
Secondary efficacy variables were the proportion of patients with complete response for nausea (absence of nausea) regardless of rescue treatment received, and the proportion of patients who remained without rescue treatment for nausea or vomiting during the 24-h period. Formal statistical tests were performed on secondary parameters, but such tests were reported with the caveat that their significance level must be adjusted to account for multiple testing.
Results A total of 1513 inpatients satisfying eligibility criteria were observed for the occurrence of PONV. Of these, 316 (21%) experienced PONV within the first 2 h after recovery from general anesthesia and were random- ized into the study. Two randomized patients with- drew their consent before receiving the study medica- tion; thus, 314 patients received study medication. There were no patients withdrawn after receiving the study medication. Five patients had protocol viola- tions-two in the 0.5-mg tropisetron group, two in the 5-mg tropisetron group, and one in the placebo group. Because only 5 patients among the 314 treated had

ANESTH ANALG ALON ET AL. 619 1998;86:617-23 TROPISETRON FOR TREATMENT OF ESTABLISHED PONV
Table 1. Baseline Demographics, Background Characteristics, and Prognostic Factor for Postoperative Nausea and Vomiting
Gender Female Male
Age (Median; yr) (Range; yr)
Weight (median; kg) Height (median; cm) Race (Caucasian) ASA physical status
I II
Coexisting medical conditions History of motion sickness Previous surgery
If previous PONV yes, Anesthesia
(Median; min) (Range; min)
Nasogastric tube
Placebo (I? = 77)
71 (92%) 6 (8%)
40 16-75
64.0 163 70 (91%)
51 (66%) 26 (34%) 65 (84%)
3 (4%) 60 (78%) 17 (28%)
117 20435
31 (40%)
0.5 mg (n = 77)
71 (92%) 6 (8%)
44 18-75
65.0 165 74 (96%)
48 (62%) 29 (38%) 69 (90%)
0 (0%) 54 (70%) 17 (31%)
125 25-330
30 (39%)
Tropisetron
2mg (n = 80)
76 (95%) 4 (5%)
41 18-76
65.0 163
78 (98%)
55 (69%) 25 (31%) 69 (86%)
1 (1%) 62 (78%) 19 (31%)
121 30-345
34 (43%)
5% (n = 80)
71 (89%) 9 (11%)
42 19-72
64.5 164
78 (98%)
51 (64%) 29 (36%) 72 (90%)
3 (4%) 62 (78%) 18 (29%)
120 20480
29 (36%)
All patients (n = 314)
289 (92%) 25 (8%)
42 16-76
65.0 164 300 (96%)
205 (65%) 109 (35%) 275 (88%)
7 (2%) 238 (76%)
71 (30%)
120 20480
124 (39%)
PONV = postoperative nausea and vomiting.
protocol deviations, the analyses were performed only on the intent to treat population (n = 314), which also corresponds to the safety population. Of these 314 patients, 77 were randomized to the placebo group and 77,80, and 80 were randomized to the 0.5-, 2-, and 5-mg tropisetron groups, respectively.
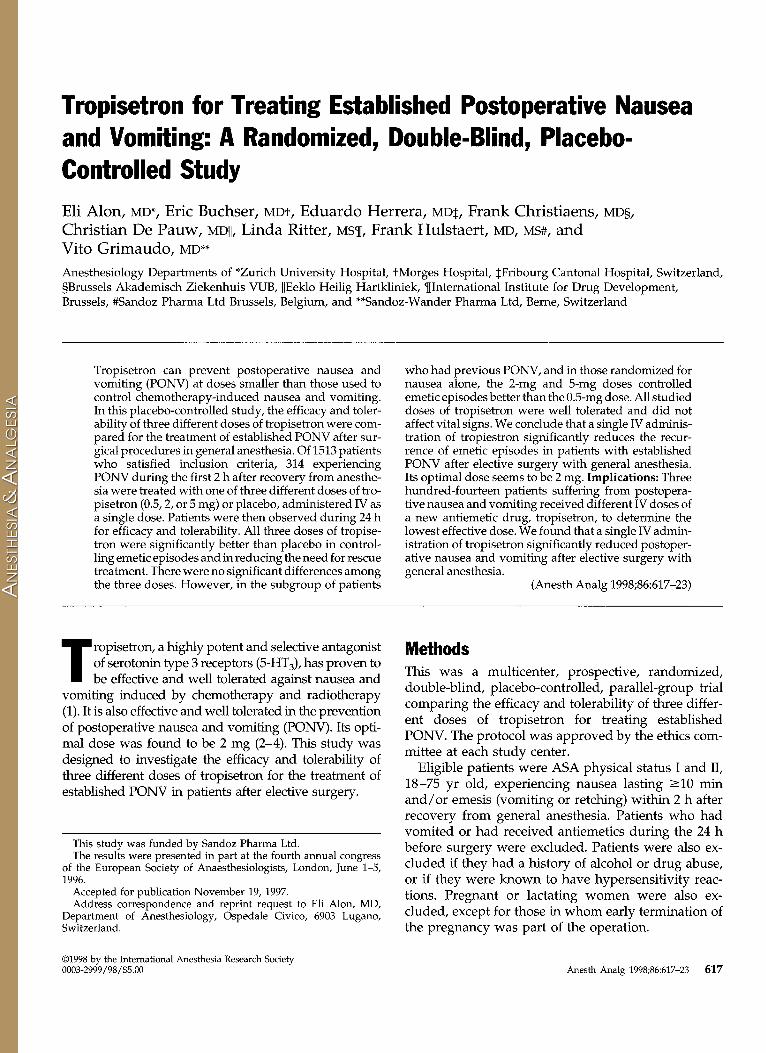
Most patients had coexisting medical conditions at baseline in the urogenital body system (54%), fol- lowed by digestive (17%); cardiovascular (15%); endo- crine, metabolic, and nutritional (12%); and musculo- skeletal (12%). The most commonly observed ab- normalities in the physical examination at entry, well balanced over the treatment groups, were obesity in 9% and abdominal pain in 8% of patients (Tables 1 and 2).
The drugs and techniques used for premeditation and for induction, maintenance, and reversal of anes- thesia were similar among groups. Figures for patients receiving propofol, narcotics, or volatile anesthetics are shown in Table 2. All patients received either 0.5, 2, or 5 mg tropisetron or placebo IV within a median time of 40 min (range 3-180 min) after recovery. This median time was comparable among the treatment groups.
The use of nonopioid as well as opioid analgesics after recovery from anesthesia before receiving the study medication was similar among the treatment groups.
Overall, 64% of patients were randomized because of emetic episodes with or without nausea (38% and
26%, respectively) whereas 36% were randomized be- cause of nausea alone. Slightly more patients in the 2- and 5-mg groups were randomized because of nausea alone (31% in the placebo and 32%, 40%, and 39% in the 0.5-, 2-, and 5-mg tropisetron groups, respectively).
More than half of the patients (64%) received non- opioid analgesic treatment in the 24 h after receiving study medication. Most of these patients received paracetamol or propacetamol (72%). Many patients received opioid analgesic treatment in this time period (55%). Overall, 15% of the patients (10% in the placebo and 15%, 17%, and 16% in the 0.5-, 2-, and 5-mg tropisetron groups, respectively) received rescue anti- emetics for nausea alone. These factors were all bal- anced among treatment groups.
The results for the primary and secondary variables are summarized in Table 3. All three doses of tropise- tron resulted in a significant improvement, compared with placebo, in controlling emetic episodes-the 2- and 5-mg doses provided a doubling of the response rate compared with placebo. All three doses of tropi- setron were also significantly better than placebo for reducing the need of rescue treatment. For the variable “absence of nausea,” all three doses of tropisetron were numerically better than placebo, but the differ- ences were not statistically significant. However, if patients included for nausea (with or without emesis) were analyzed separately in an exploratory manner (230 patients in total: 55 in the placebo and 54,61, and 60 in the 0.5-, 2-, and 5-mg groups, respectively), the
620 ALON ET AL. ANESTH ANALG TROPISETRON FOR TREATMENT OF ESTABLISHED PONV 1998;86:617-23
Table 2. Type of Surgery and Main Anesthetics
Placebo (n = 77)
0.5 mg (n = 77)
Tropisetron
2mg (n = 80)
5 mg (n = 80)
All patients
(n = 314)
Abdominal surgery Laparoscopy Vaginal Other abdominal Hernioplasty
Nonabdominal surgery ENT Thyroparathyroidectomy Eye Gynecological Breast surgery Varicose veins Major orthopedic Minor orthopedic Other
IV drug Fentanyl Propofol
Volatile agent Nitrous oxide
Data are expressed as n (%).
Emesis 04h O-24 h 04 and 4-24 h
Nausea 04h 4-24 h
Severe nausea 04h 4-24 h
Rescue antiemetics 04h 4-24 h
Absence of emetic episodes
Absence of nausea
Absence of rescue antiemetics
45 (58) 23 (30)
5 (6) 15 (19) 2 (3)
32 (42) l(l) 2 (3) 0 (0)
13 (17) 4 (5) 2 (3) 5 (6) 0 (0) 5 (6)
48 (62) 23 (30)
62 (81)
42 (55) 22 (29) 8 (10)
11 (14) 10)
35 (45) 1 (1) 2 (3) 2 (3)
13 (17) 5 (6) 2 (3) 4 (5) 3 (4) 3 (4)
46 (60) 26 (34)
67 (87)
51 (64) 24 (30)
5 (6) 19 (24)
3 (4) 29 (36)
3 (4) 0 (0) cl (0) 9 01) 6 (8) 5 (6) 2 (3) 3 (4) 10)
52 (65) 25 (31)
63 (79)
44 (55) 21 (26)
7 (9) 15 (19)
1 (1) 36 (45)
3 (4) 2 (3) 1 (1)
12 (15) 8 (10) 2 (3) 5 (6) l(l) 2 (3)
51 (64) 30 (38)
67 (84)
182 (58) 90 (29) 25 (8) 60 (19)
7 (2) 132 (42)
8 (3) 6 (2) 3 (1)
47 (15) 23 (7) 11 (4) 16 (5)
7 (2) ll(4)
197 (63) 104 (33)
259 (82)
Table 3. Primary and Secondary Efficacy Variables during the 24-H Period, Results of Exploratory Analysis, and the Use of Rescue Antiemetics in the Subperiods of O-4 H and 4-24 H
Placebo (n = 77)
22 (29%)
26 (34%)
25 (32%)
42 (55%) 31 (40%) 18 (23%)
42 (55%) 28 (36%)
17 (40%) 13 (46%)
38 (49%) 30 (39%)
0.5 mg (i-l = 77)
40 (52%) 0.003*
(0.003) 33 (43%)
0.25* (0.25)
42 (55%) 0.006*
(0.006)
23 (30%) 28 (36%) 14 (18%)
32 (42%) 27 (35%)
4 (13%) 8 (30%)
19 (25%) 28 (36%)
Tropisetron
2% (n = 80)
46 (58%) 0.001*
(0.001) 36 (45%)
0.15* (0.15)
44 (55%) 0.004*
(0.004)
19 (24%) 24 (30%)
9 (11%)
35 (44%) 29 (36%)
8 (23%) 5 (17%)
23 (29%) 24 (30%)
5 mg (n = 80)
48 (60%) 0.001*
(0.001) 37 (46%)
0.11* (0.11)
45 (56%) 0.003*
(0.003)
21 (26%) 21 (26%) 10 (12%)
35 (44%) 27 (34%)
6 (17%) 10 (37%)
27 (34%) 23 (29%)
All patients (n = 314)
156 (50%)
132 (42%)
156 (50%)
105 (33%) 104 (33%) 51 (16%)
144 (46%) 111 (35%)
35 (24%) 36 (32%)
107 (34%) 105 (33%)
* P value (,$ test) for comparison with placebo (adjusted P value).
ANESTH ANALG ALON ET AL. 621 1998;86:617-23 TROI’ISETRON FOR TREATMENT OF ESTABLISHED PONV
Table 4. Absence of Emetic Episodes by Prognostic Factors
Placebo (n = 77)
0.5 mg (n = 77)
Tropisetron
2mg (n = 80)
5mg (n = 80)
Sex Female Male
History of PONV Yes No
Type of Surgery Abdominal Nonabdominal
Duration of anesthesia <2 h z2h
Postoperative opioids Yes No
Nasogastric tube after study drug Yes No
Reason for randomisation Emetic episodes Nausea alone
Rescue treatment before first emetic episode Yes No
21 (30) 1 (17)
3 (18) 19 (32)
12 (27) 10 (31)
12 (29) 10 (28)
12 (23) 10 (40)
1Gv 21 (29)
16 (30) 6 (25)
8 (100) 14 (20)
38 (54) 2 (33)
4 (24) 36 (60)
24 (57) 16 (46)
21 (58) 19 (46)
24 (52) 16 (52)
2 (40) 38 (53)
24 (46) 16 (64)
10 (83) 30 (46)
43 (57) 3 (75)
9 (47) 37 (61)
31 (61) 15 (52)
23 (66) 23 (51)
27 (54) 19 (63)
3 (43) 43 (59)
20 (42) 26 (81)
10 (71) 36 (55)
43 (61) 5 (56)
10 (56) 38 (61)
25 (57) 23 (64)
25 (68) 23 (53)
25 (50) 23 (77)
l(33) 47 (61)
25 (51) 23 (74)
9 (69) 39 (58)
Data are expressed as n (“Q. PONV = postoperative nausea and vomiting.
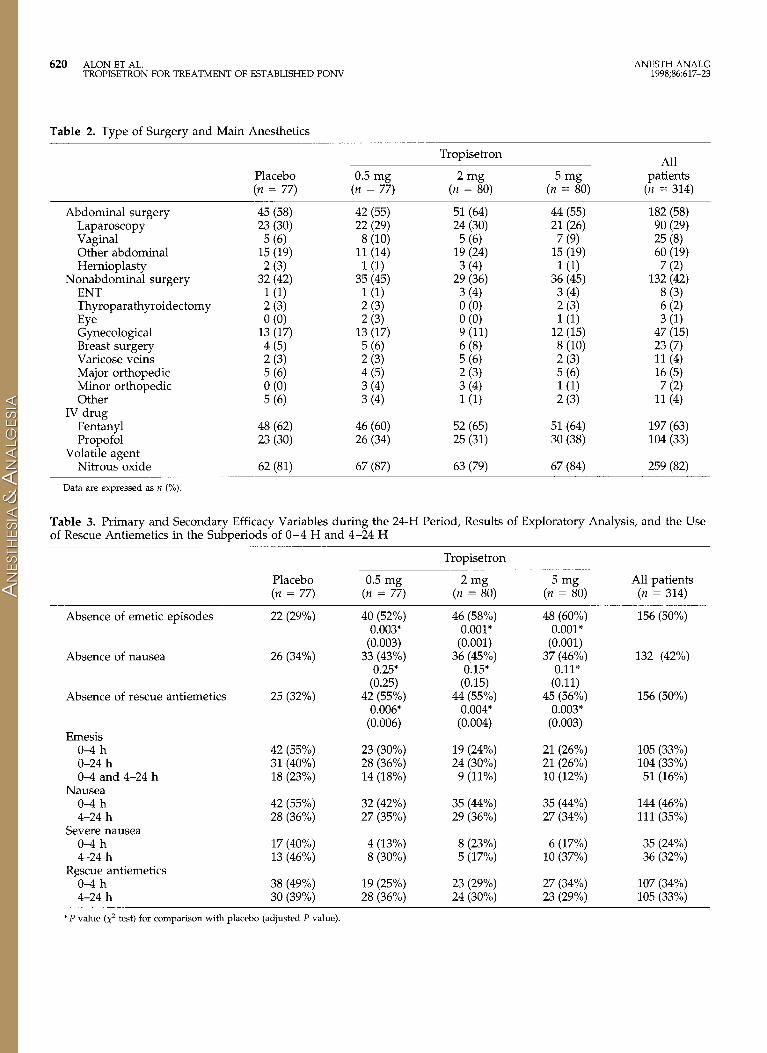
reduction in nausea for the 2- and 5-mg doses com- pared with placebo was statistically significant (P < 0.05). Results of exploratory analysis are also included in Table 3.
The primary end point was also tabulated by sub- group for the prognostic factors listed earlier (Table 4). Using logistic models on the probability of having an emetic episode during the 24-h period after receiving the study medication, the factors of treatment, age, history of PONV, duration of anesthesia, postopera- tive opioid use, reason for randomization, and use of antiemetics before first emetic episode were all signif- icant in the univariate models. All of these except for duration of anesthesia remained significant in the final model. The results for the variables in the final model are shown in Table 5.
Patients were asked to score their overall control of emesis and nausea. The median score was 3 (satisfac- tory) in the placebo group and 2 (good) in each of the three treatment groups.
There were no differences among groups in the evolution of vital signs, Sao,, and sedation scores re- corded before and 1, 5, and 60 min after the study drug administration. There were few adverse events reported in this study, which are summarized in Table 6. All adverse events, except headache, were generally mild or moderate in severity. Severe headache was
Table 5. Results of the Logistic Models of Prognostic Factors on Absence of Emetic Episodes
Adjusted Unadjusted model model OR
OR (95% CI) (95% CI)
Treatment group’ 0.5 mg 0.37 (0.19,0.72) 0.32 (0.15,0.67)
2% 0.30 (0.15,0.57) 0.28 (0.13,0.58) 5mg 0.27 (0.14,0.52) 0.25 (0.12,0.51)
Other factors Rescue treatment 0.22 (0.10,0.46) 0.22 (0.10,0.49)
for nausea Age (increase of 1.31 (1.11,1.54) 1.33 (1.11,1.61)
10 yr) Emesis as reason 2.38 (1.48,3.83) 2.68 (1.55,4.65)
for entry Postoperative use 1.77 (1.11,2.81) 2.08 (1.21,3.55)
of opioids Previous PONV 1.99 (1.15,3.43) 2.15 (1.16,3.97)
OR = odds ratio, CI = confidence intervals, PONV = postoperative nausea and vomiting.
a Odds ratios compared with placebo.
reported once each in the placebo, 0.5-mg, and 2-mg tropisetron groups, and three times in the 5-mg tropi- setron group. Most adverse events were not consid- ered by the investigators to be related to the study medication. The only exceptions were abdominal

622 ALON ET AL. ANESTH ANALG TROPISETRON FOR TREATMENT OF ESTABLISHED PONV 1998;86:617-23
Table 6. Adverse Events by Treatment Group
Abdominal pain Allergy Coughing Abdominal cramp Dizziness Fever Headache Hiccup Hypertension Itching abdomen and back Dry mouth Paraesthesia Shivering Sore throat Patients with at least one
adverse event
Placebo (n = 77)
0 (0) 1 (1) 0 (0) 0 (0) 0 (0) l(l) 9 (12) 0 (0) 0 (0) 0 (0) 0 (0) 0 (0) 10) 0 (0)
11 (14)
0.5 mg (n = 77)
0 (0) 0 (0) 0 (0) 1 (1) 1 (1) 0 (0) 2 (3) 0 (0) 1 (1) 0 (0) 0 0 0 (0) 10) 0 (0) 6 (8)
Tropisetron
2mg (n = 80)
0 (0) 0 (0) 0 (0) 0 (0) l(l) 0 (0) 8 (10) 0 (0) l(l) l(l) 0 (0) 0 (0) 0 (0) 2 (3)
12 (15)
5 mg (n = 80)
1 (1) 0 0 10) 0 (0) 0 (0) 0 (0)
13 (16) 1 (1) 0 (0) 0 (0) 1 (1) 1 (1) 0 (0) 0 (0)
17 (21)
All patients
(n = 314)
1 (0) l(O) 10 l(O) 2 (1) l(O)
32 (10) 1 (0) 2 (1) 1 (0) 10 160 2 (1) 2 (1)
46 (15)
Data are presented as n (%).
cramp, dizziness, and headache. The latter was con- sidered possibly related for five patients in the placebo and for one, four, and eight patients in the 0.5-, 2-, and 5-mg groups, respectively, and considered probably related for one placebo and one tropisetron 5 mg patient. There were no serious adverse events.
Discussion The aim of this study was to determine the optimal effective dose of Iv tropisetron in the treatment of established nausea and vomiting after general anes- thesia and to evaluate its tolerability.
All three doses of tropisetron resulted in a signifi- cant improvement, compared with placebo, in control- ling emetic episodes in the 24-hour period after study drug administration, with the 2-mg and the 5-mg doses providing the highest efficacy. For the 2- and 5-mg doses, this constitutes a 100% increase in the response rate compared with placebo, which corre- sponds exactly to the hypothesis used for the sample size calculation. This improvement is at least the same as has been reported with ondansetron (6). Compared with placebo, patients who received tropisetron were more satisfied with their treatment. Dose-comparative studies in the prevention and treatment of PONV have been,published or ondansetron (6-8) and also for granisetron (9). As was the case for ondansetron and granisetron, and for tropisetron itself in the prevention of PONV (4), the minimal dose of tropisetron found to be effective in this study was smaller than the dose used for cancer chemotherapy-induced nausea and vomiting.
The number of patients with emesis in the first 4 hours after study drug was comparable to that in the
20-hour period from the 5th to the 24th hour. Whereas in the first 4 hours, the three doses of tropisetron reduced PONV in a more or less similar way, the efficacy in the 4-24 hour period seemed to be re- stricted to the larger doses. Thus, the 2- and 5-mg doses seem to confer longer protection compared with the 0.5-mg dose.
The advantage of tropisetron was striking in pa- tients with a history of PONV and was restricted to the 2- and 5-mg doses. The advantage of tropisetron was also important in patients receiving postoperative opi- oids. The most striking advantage of tropisetron was in the patients randomized because of nausea alone, and especially for the 2- and 5-mg doses. The odds ratios in the final logistic regression model suggested a weak dose-response relationship, which remained after adjustment for the other prognostic factors that could possibly have influenced the results.
In accordance with the recommendations published by Korttila (lo), the study was designed as a prospec- tive, randomized, double-blind, placebo-controlled, and parallel-group comparison of the three doses of tropisetron. The 5-mg dose was chosen as the largest dose because it is the recommended dose for the con- trol of chemotherapy-induced emesis; the 2-mg dose was chosen because it is suboptimal for the control of chemotherapy-induced emesis and, hence, expected to be in the effective dose range for PONV; and the 0.5-mg dose was chosen because it was expected to be suboptimal for the control of PONV.
The 21% overall incidence of PONV corresponds to that reported in the literature (11-13). The incidence of PONV per center ranged from 0% to 54% (median 22%). This large variability is probably due to the large variability of total screened patients among centers

ANESTH ANALG ALON ET AL. 623 1998;86:617-23 TROPISETRON FOR TREATMENT OF ESTABLISHED PONV
(range 9-305) and to the different surgery depart- ments used to recruit patients among centers. Most of the treated patients were women, and the incidence of PONV in men was lower than that in women.
Two points particular to the design of this study were the inclusion of nausea alone as sufficient reason for randomization and the administration of rescue treatment for nausea. No limitations were given for the use of opioid analgesics or for the use of a naso- gastric tube in the postoperative period. Slightly more patients in the 2- and 5-mg groups were randomized because of nausea alone, whereas the use of rescue treatment for nausea and the use of postoperative opioids as well as a nasogastric tube were balanced among the groups. These four factors were considered prognostic for the primary efficacy variable. The re- sults of logistic regression models confirm that the observed reduction in the proportion of patients who continued to suffer from PONV due to treatment is still significant, even after adjusting for other impor- tant prognostic factors.
As reported for ondansetron (8), our data suggest that the effect of 5-HT, antagonists on vomiting might be more pronounced than the effect on nausea, which is not necessarily a low-level stimulation of the vom- iting reflex.
The safety and tolerability profile suggests that from a clinical point of view, there are no major drug-drug interactions between tropisetron and the various con- comitant medications given before, during, and after surgery.
In conclusion, tropisetron administered to treat es- tablished PONV significantly reduced the recurrence of vomiting and need for rescue antiemetics. It also reduced the recurrence or persistence of nausea, but this reduction was significant only in the subgroup of patients included for nausea. The advantage of tropi- setron was consistent with overall results in all patient categories. Reviewing all the efficacy and safety data, from a clinical point of view, it is clear that the 2-mg dose of tropisetron offers some advantage compared with the 0.5-mg dose, whereas the 5-mg dose does not offer additional advantages compared with the 2-mg dose. The optimal dose seems to be 2 mg, and a single dose of up to 5 mg, administered as a slow IV injec- tion, is well tolerated. Future studies should also con- sider the pharmacoeconomic implications of these findings.
We thank the following investigators and coinvestigators: J.-P. Gardaz, MD, D. Thorin, MD, D. Schwander, MD, D. Morel, MD, C. E. Klopfenstein, MD, D. Fevrier, MD, M. Stotz, MD, P. Frey, MD, S. Gligorijevic, MD, I’. Gtinter, MD, R. Bloch, cand med, R. Tomasetti, MD, I’. Baele, MD, V. Capouet, MD, M. Vercauteren, MD, A. d’Hollander, MD, G. Rolly, MD, and S. Castellanelli, MD. We also are indebted to K. de Bruijn, MD, PhD, and G. Varrassi, MD, for critical scientific review. We thank R. Bayer, Y.
Delafontaine, Ch. Boller, R. Erne, G. Fedrigo, and I. De Kerpel, MSc, for data monitoring; J. Montandon for data monitoring and as GCP officer; and I’. Baes for data management.
References 1. de Bruijn KM. The development of tropisetron in its clinical
perspective. Ann Oncol 1993;4(Suppl 3):19-23. 2. Zomers PJW, Langenberg CJM, de Bruijn KM. Tropisetron for
postoperative nausea and vomiting in patients after gynaceo- logical surgery. Br J Anaesth 1993;71:667-80.
3. Alon E, Kocian R, Nett PC, et al. Tropisetron for the prevention of postoperative nausea and vomiting in women undergoing gynecologic surgery. Anesth Analg 1996;82:338-41.
4. Capouet V, De Pauw C, Vernet B, et al. Single dose iv. tropise- tron in the prevention of postoperative nausea and vomiting after gynaecological surgery. Br J Anaesth 1996;76:54-60.
5. Budde M, Bauer I’. Multiple test procedures in clinical dose finding studies. J Am Stat Assoc 1989;84:792-6.
6. Claybon L. Single dose intravenous ondansetron for the 24-hour treatment of postoperative nausea and vomiting. Anaesthesia 1994;49(Suppl):24-9.
7. McKenzie R, Kovac A, O’Connor T, et al. Comparison of on- dansetron versus placebo to prevent postoperative nausea and vomiting in women undergoing ambulatory gynecologic sur- gery. Anesthesiology 1993;78:21-8.
8. Pearman MH. Single dose intravenous ondansetron in the pre- vention of postoperative nausea and vomiting. Anaesthesia 1994;49(Suppl)Sll-5.
9. Fuji Y, Tanaka H, Toyooka H. Optimal anti-emetic dose of granisetron for preventing postoperative nausea and vomiting. Can J Anaesth 1994;41:794-7.
10. Korttila K. The study of postoperative nausea and vomiting. Br J Anaesth 1992;69(Suppl 1):2OS-3s.
11. Palazzo MGA, Strunin L. Anaesthesia and emesis. I. Etiology. Can Anaesth Sot J 1984;31:178-87.
12. Palazzo MGA, Strunin L. Anaesthesia and emesis. II. Prevention and management. Can Anaesth Sot J 1984;31:407-15.
13. Watcha MF, White PF. Postoperative nausea and vomiting: its etiology, treatment and prevention. Anesthesiology 1992;77: 162-84.
Related Documents