Trigeminal Autonomic Trigeminal Autonomic Cephalalgias Cephalalgias Manjit S Matharu Manjit S Matharu Headache Group, Institute of Neurology Headache Group, Institute of Neurology & & The National Hospital for Neurology and The National Hospital for Neurology and Neurosurgery Neurosurgery London London UK UK Third Biennial Hull-BASH Headache Meeting 23 rd January 2009

Trigeminal Autonomic Cephalalgias Manjit S Matharu Headache Group, Institute of Neurology & The National Hospital for Neurology and Neurosurgery LondonUK.
Dec 15, 2015
Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript
Trigeminal Autonomic CephalalgiasTrigeminal Autonomic Cephalalgias
Manjit S MatharuManjit S Matharu
Headache Group, Institute of Neurology &Headache Group, Institute of Neurology &The National Hospital for Neurology and NeurosurgeryThe National Hospital for Neurology and Neurosurgery
London London UKUK
Third Biennial Hull-BASH Headache Meeting 23rd January 2009
Trigeminal Autonomic CephalgiasTrigeminal Autonomic CephalgiasTrigeminal Autonomic CephalgiasTrigeminal Autonomic Cephalgias
• Unilateral head pain, Unilateral head pain, predominantly Vpredominantly V11
• Very severe / excruciatingVery severe / excruciating
• Cranial autonomic symptomsCranial autonomic symptoms– Parasympathetic Parasympathetic – Sympathetic Sympathetic
• Attack frequency and duration Attack frequency and duration differsdiffers
• Treatment responses differTreatment responses differ
• Unilateral head pain, Unilateral head pain, predominantly Vpredominantly V11
• Very severe / excruciatingVery severe / excruciating
• Cranial autonomic symptomsCranial autonomic symptoms– Parasympathetic Parasympathetic – Sympathetic Sympathetic
• Attack frequency and duration Attack frequency and duration differsdiffers
• Treatment responses differTreatment responses differ
• Cluster HeadacheCluster Headache
• Paroxysmal HemicraniaParoxysmal Hemicrania
• SUNCT (Short-lasting SUNCT (Short-lasting Unilateral Neuralgiform Unilateral Neuralgiform headache with Conjunctival headache with Conjunctival injection and Tearing)injection and Tearing)
• Cluster HeadacheCluster Headache
• Paroxysmal HemicraniaParoxysmal Hemicrania
• SUNCT (Short-lasting SUNCT (Short-lasting Unilateral Neuralgiform Unilateral Neuralgiform headache with Conjunctival headache with Conjunctival injection and Tearing)injection and Tearing)
Paroxysmal HemicraniaParoxysmal Hemicrania IHS CLASSIFICATION CRITERIAIHS CLASSIFICATION CRITERIA
Paroxysmal HemicraniaParoxysmal Hemicrania IHS CLASSIFICATION CRITERIAIHS CLASSIFICATION CRITERIA
• Severe Severe
• Unilateral Unilateral
• Orbital, supraorbital or temporal Orbital, supraorbital or temporal painpain
• 2-30 minutes duration2-30 minutes duration
• >5 attacks daily at least 50% of >5 attacks daily at least 50% of the timethe time
• Associated symptoms:Associated symptoms:-Conjunctival injection-Conjunctival injection-Lacrimation-Lacrimation-Ptosis-Ptosis-Miosis-Miosis-Eyelid oedema-Eyelid oedema-Nasal congestion-Nasal congestion-Rhinorrhea-Rhinorrhea-Forehead and facial -Forehead and facial
sweatingsweating
• Stopped completely by Stopped completely by indomethacinindomethacin
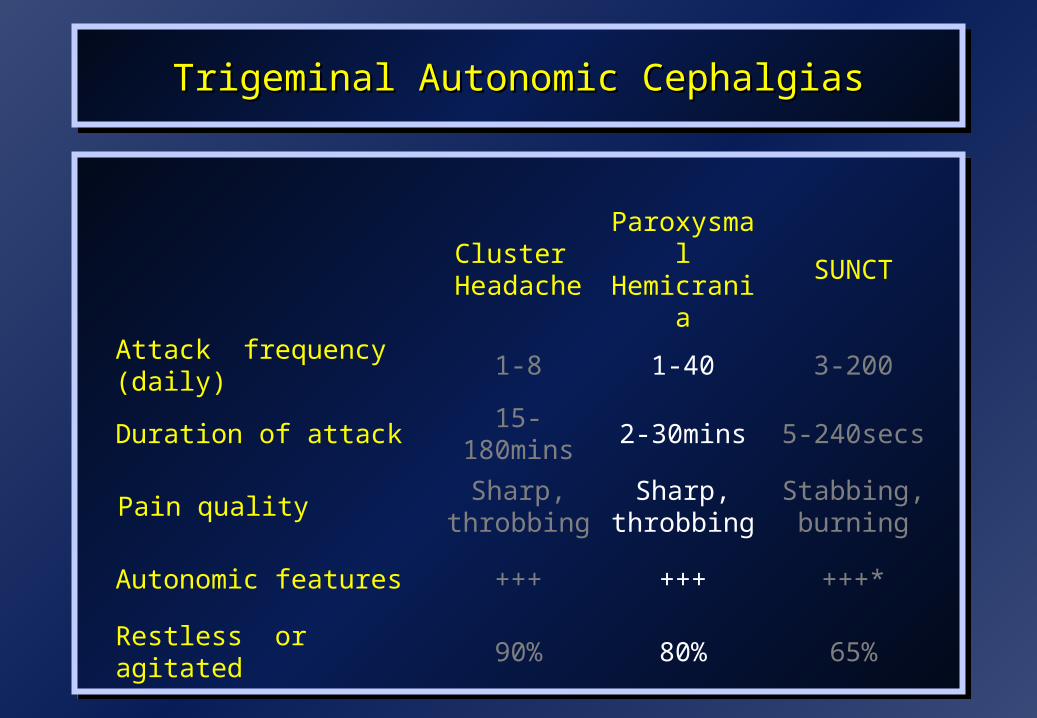
Trigeminal Autonomic CephalgiasTrigeminal Autonomic CephalgiasTrigeminal Autonomic CephalgiasTrigeminal Autonomic Cephalgias
Cluster
HeadacheParoxysmal Hemicrania
SUNCT
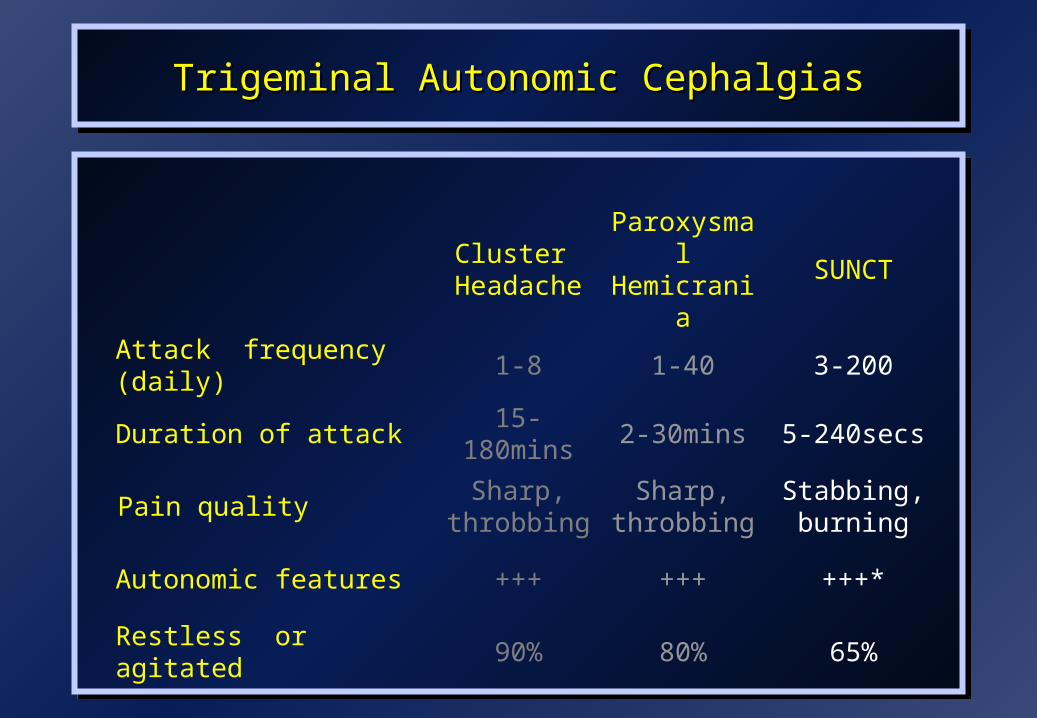
Attack frequency (daily) 1-8 1-40 3-200
Duration of attack 15-180mins 2-30mins 5-240secs
Pain qualitySharp,
throbbingSharp,
throbbingStabbing, burning
Autonomic features +++ +++ +++*
Restless or agitated 90% 80% 65%

Trigeminal Autonomic CephalgiasTrigeminal Autonomic CephalgiasTrigeminal Autonomic CephalgiasTrigeminal Autonomic Cephalgias
Cluster Cluster
HeadacheHeadacheParoxysmal Paroxysmal HemicraniaHemicrania
SUNCTSUNCT
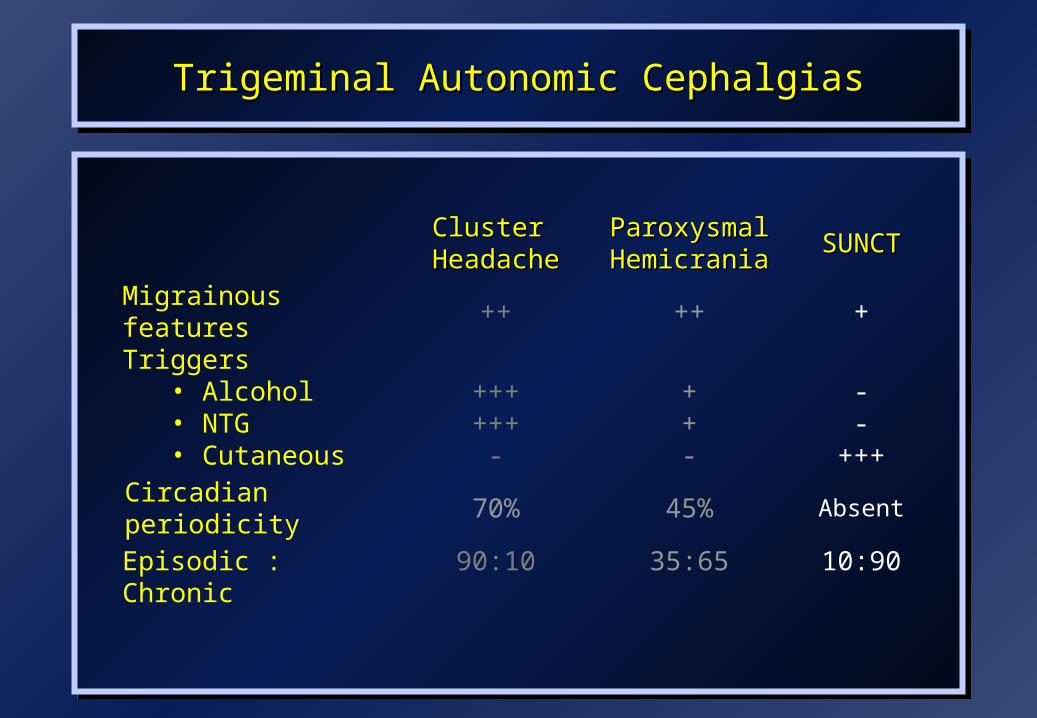
Migrainous features ++ ++ +
Triggers• Alcohol• NTG• Cutaneous
++++++
-
++-
--
+++
Circadian periodicity 70% 45% Absent
Episodic : Chronic 90:10 35:65 10:90
Trigeminal Autonomic CephalgiasTrigeminal Autonomic CephalgiasTrigeminal Autonomic CephalgiasTrigeminal Autonomic Cephalgias
Cluster
HeadacheParoxysmal Hemicrania
SUNCT
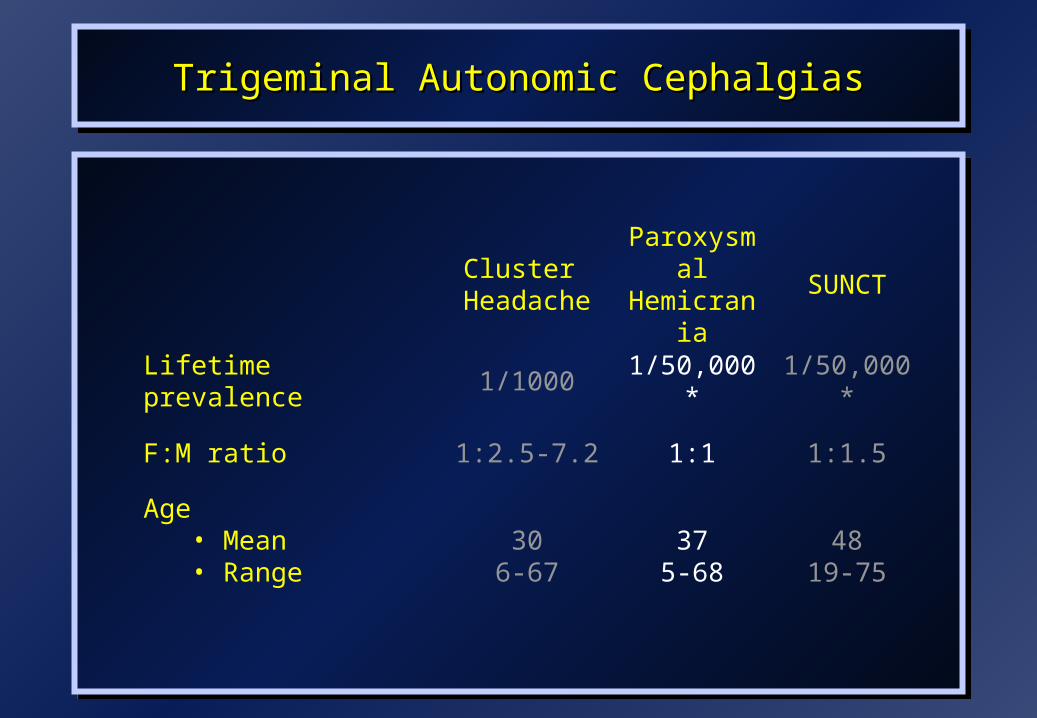
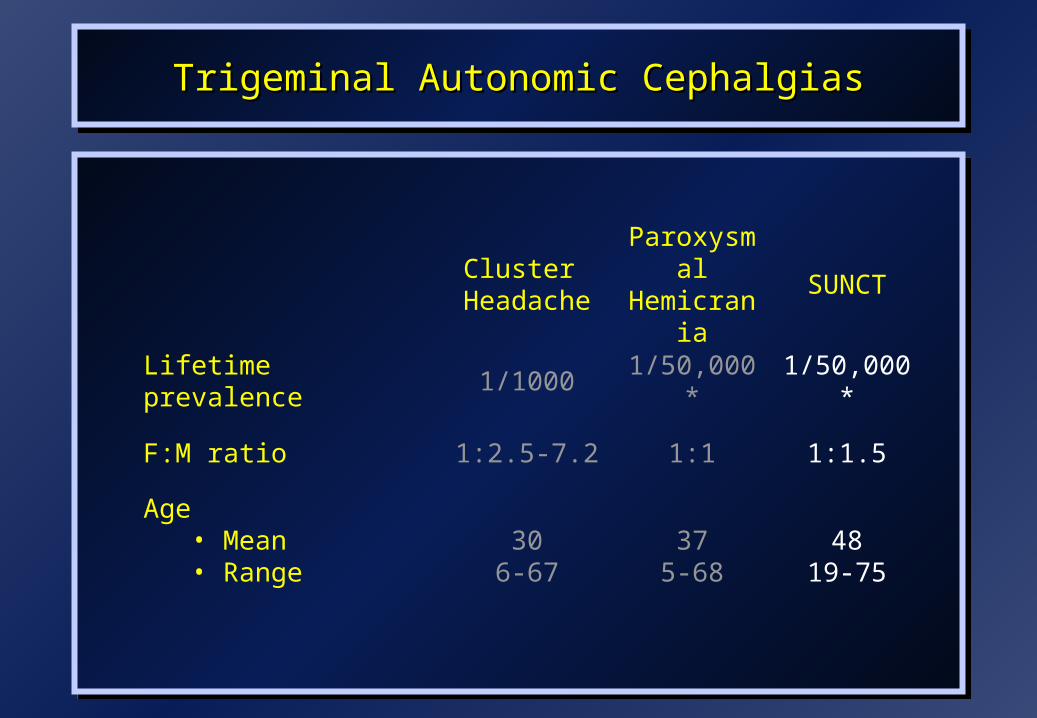
Lifetime prevalence 1/1000 1/50,000* 1/50,000*
F:M ratio 1:2.5-7.2 1:1 1:1.5
Age• Mean• Range
306-67
375-68
4819-75
Paroxysmal HemicraniaParoxysmal HemicraniaDIFFERENTIAL DIAGNOSISDIFFERENTIAL DIAGNOSIS
Paroxysmal HemicraniaParoxysmal HemicraniaDIFFERENTIAL DIAGNOSISDIFFERENTIAL DIAGNOSIS
• Symptomatic Paroxysmal HemicraniaSymptomatic Paroxysmal Hemicrania
• Cluster headacheCluster headache
• SUNCT syndrome SUNCT syndrome
• Hemicrania continuaHemicrania continua
• Symptomatic Paroxysmal HemicraniaSymptomatic Paroxysmal Hemicrania
• Cluster headacheCluster headache
• SUNCT syndrome SUNCT syndrome
• Hemicrania continuaHemicrania continua

Symptomatic Paroxysmal HemicraniaSymptomatic Paroxysmal HemicraniaSymptomatic Paroxysmal HemicraniaSymptomatic Paroxysmal Hemicrania
VascularVascularICA aneurysmICA aneurysm
Subclavian artery dilatationSubclavian artery dilatation
Parietal AVMParietal AVM
MCA StrokeMCA Stroke
Occipital infarctionOccipital infarction
Inflammatory or InfectionInflammatory or InfectionCollagen vascular diseaseCollagen vascular disease
Ophthalmic herpes zosterOphthalmic herpes zoster
IatrogenicIatrogenicSurgical sympathectomySurgical sympathectomy
TumoursTumoursPituitary tumoursPituitary tumours
Frontal tumourFrontal tumour
Tuber cinereum hamartomaTuber cinereum hamartoma
Sella turcica gangliocytomaSella turcica gangliocytoma
Cavernous sinus meningiomaCavernous sinus meningioma
Multiple parotid ca. MetastasisMultiple parotid ca. Metastasis
Non-Hodgkin’s lymphomaNon-Hodgkin’s lymphoma
Pancoast syndromePancoast syndrome
MiscellaneousMiscellaneousEssential thrombocythaemiaEssential thrombocythaemia
Intracranial hypertensionIntracranial hypertension
Maxillary cystMaxillary cyst
Trigeminal Autonomic CephalgiasPituitary and TACs
Trigeminal Autonomic CephalgiasPituitary and TACs
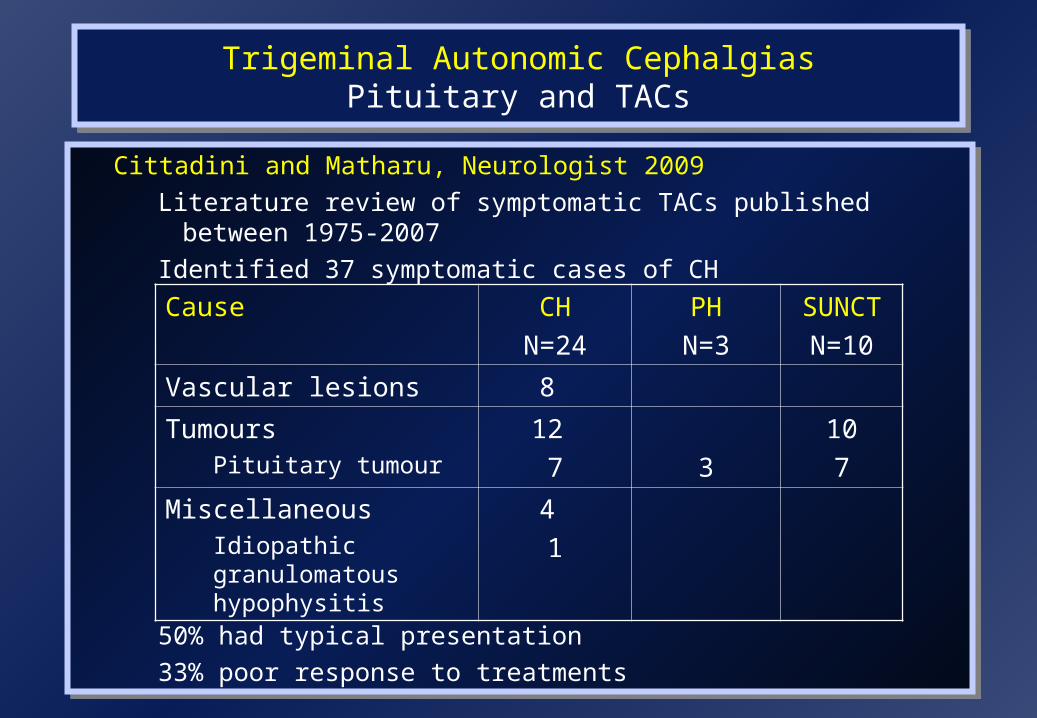
Cittadini and Matharu, Neurologist 2009
Literature review of symptomatic TACs published between 1975-2007
Identified 37 symptomatic cases of CH
50% had typical presentation
33% poor response to treatments
Cittadini and Matharu, Neurologist 2009
Literature review of symptomatic TACs published between 1975-2007
Identified 37 symptomatic cases of CH
50% had typical presentation
33% poor response to treatments
Cause CH
N=24
PH
N=3
SUNCT
N=10
Vascular lesions 8
TumoursPituitary tumour
12
7 3
10
7
MiscellaneousIdiopathic granulomatous hypophysitis
4
1
Trigeminal Autonomic Cephalgias Pituitary and TACs
Trigeminal Autonomic Cephalgias Pituitary and TACs
Levy et al, Brain 2005• 84 pituitary tumour patients with headaches studied• 9% had TACs• Functioning adenomas more likely to cause TACs• Investigate all TAC patients for pituitary tumours?
• Prevalence of pituitary tumours in TACs is unknown• 1 in 10 of the population have an incidental pituitary micro-
adenoma (< 1cm diameter) on routine MRI • 1 in 500 have a macro-adenoma
Levy et al, Brain 2005• 84 pituitary tumour patients with headaches studied• 9% had TACs• Functioning adenomas more likely to cause TACs• Investigate all TAC patients for pituitary tumours?
• Prevalence of pituitary tumours in TACs is unknown• 1 in 10 of the population have an incidental pituitary micro-
adenoma (< 1cm diameter) on routine MRI • 1 in 500 have a macro-adenoma

Trigeminal Autonomic Cephalgias Pituitary and TACs
Trigeminal Autonomic Cephalgias Pituitary and TACs
• Difficult to draw up definitive guidelines from retrospective reviews
• Pituitary imaging should be performed in:– Atypical phenotype/abnormal examination
– Treatment resistant cases
• Do typical cases require neuroimaging? – Increases likelihood of identifying incidental lesion
• Implication of data on pituitary lesions?– Need prospective community based study in CH patients
– Carefully elicit symptoms related to pituitary disease in all TAC patients but only perform MRI scans of the pituitary and a basal pituitary hormone profile in:
• patients with atypical features (including pituitary related symptoms)
• abnormal examination
• poor response to appropriate treatments.
• Difficult to draw up definitive guidelines from retrospective reviews
• Pituitary imaging should be performed in:– Atypical phenotype/abnormal examination
– Treatment resistant cases
• Do typical cases require neuroimaging? – Increases likelihood of identifying incidental lesion
• Implication of data on pituitary lesions?– Need prospective community based study in CH patients
– Carefully elicit symptoms related to pituitary disease in all TAC patients but only perform MRI scans of the pituitary and a basal pituitary hormone profile in:
• patients with atypical features (including pituitary related symptoms)
• abnormal examination
• poor response to appropriate treatments.
Paroxysmal HemicraniaParoxysmal HemicraniaDIFFERENTIAL DIAGNOSISDIFFERENTIAL DIAGNOSIS
Paroxysmal HemicraniaParoxysmal HemicraniaDIFFERENTIAL DIAGNOSISDIFFERENTIAL DIAGNOSIS
• Symptomatic Paroxysmal HemicraniaSymptomatic Paroxysmal Hemicrania
• Cluster headacheCluster headache
• SUNCT syndrome SUNCT syndrome
• Hemicrania continuaHemicrania continua
• Symptomatic Paroxysmal HemicraniaSymptomatic Paroxysmal Hemicrania
• Cluster headacheCluster headache
• SUNCT syndrome SUNCT syndrome
• Hemicrania continuaHemicrania continua

Cluster Headache Vs Paroxysmal HemicraniaCluster Headache Vs Paroxysmal HemicraniaCluster Headache Vs Paroxysmal HemicraniaCluster Headache Vs Paroxysmal Hemicrania
Trial of Indomethacin if:Trial of Indomethacin if:
1.1. Attack frequency Attack frequency >> 5 daily 5 daily
2.2. Attack duration Attack duration << 30 minutes 30 minutes
3.3. Chronic subtypesChronic subtypes
FeatureFeature CHCH PHPH
Gender (M:F)Gender (M:F) 2.5-7:12.5-7:1 1:11:1
Duration (min)Duration (min) 15 - 18015 - 180 2 – 302 – 30
Frequency (attacks/day)Frequency (attacks/day) 1- 81- 8 1 - 401 - 40
IndomethacinIndomethacin -- ++

Paroxysmal HemicraniaParoxysmal HemicraniaDIFFERENTIAL DIAGNOSISDIFFERENTIAL DIAGNOSIS
Paroxysmal HemicraniaParoxysmal HemicraniaDIFFERENTIAL DIAGNOSISDIFFERENTIAL DIAGNOSIS
• Symptomatic Paroxysmal HemicraniaSymptomatic Paroxysmal Hemicrania
• Cluster headacheCluster headache
• Hemicrania continuaHemicrania continua
• SUNCT syndromeSUNCT syndrome
• Symptomatic Paroxysmal HemicraniaSymptomatic Paroxysmal Hemicrania
• Cluster headacheCluster headache
• Hemicrania continuaHemicrania continua
• SUNCT syndromeSUNCT syndrome
Hemicrania ContinuaHemicrania ContinuaHemicrania ContinuaHemicrania Continua
• Unilateral headacheUnilateral headache
• Forehead, temple, orbit and occiputForehead, temple, orbit and occiput
• Continuous, moderate painContinuous, moderate pain
• Exacerbations:Exacerbations:
– lasting from 20 min to several days lasting from 20 min to several days
– accompanied by autonomic and migrainous featuresaccompanied by autonomic and migrainous features
– occur in 75%occur in 75%
• Lack of precipitating factorsLack of precipitating factors
• Complete response to indomethacinComplete response to indomethacin
• Unilateral headacheUnilateral headache
• Forehead, temple, orbit and occiputForehead, temple, orbit and occiput
• Continuous, moderate painContinuous, moderate pain
• Exacerbations:Exacerbations:
– lasting from 20 min to several days lasting from 20 min to several days
– accompanied by autonomic and migrainous featuresaccompanied by autonomic and migrainous features
– occur in 75%occur in 75%
• Lack of precipitating factorsLack of precipitating factors
• Complete response to indomethacinComplete response to indomethacin
Paroxysmal Hemicrania Paroxysmal Hemicrania TREATMENTSTREATMENTS
Paroxysmal Hemicrania Paroxysmal Hemicrania TREATMENTSTREATMENTS
N=77
Indomethacin:Indomethacin:
• Oral Indomethacin trialOral Indomethacin trial
– 25mgs tds25mgs tds
– 50mgs tds50mgs tds
– If high index of suspicion: 75mgs tds If high index of suspicion: 75mgs tds
– Lower doses for 3 days; maximum dose Lower doses for 3 days; maximum dose for for 7 days7 days
• Indotest (Intramuscular indomethacin)Indotest (Intramuscular indomethacin)
Indomethacin:Indomethacin:
• Oral Indomethacin trialOral Indomethacin trial
– 25mgs tds25mgs tds
– 50mgs tds50mgs tds
– If high index of suspicion: 75mgs tds If high index of suspicion: 75mgs tds
– Lower doses for 3 days; maximum dose Lower doses for 3 days; maximum dose for for 7 days7 days
• Indotest (Intramuscular indomethacin)Indotest (Intramuscular indomethacin)
Paroxysmal Hemicrania Paroxysmal Hemicrania INDOTESTINDOTEST
Paroxysmal Hemicrania Paroxysmal Hemicrania INDOTESTINDOTEST
N=77
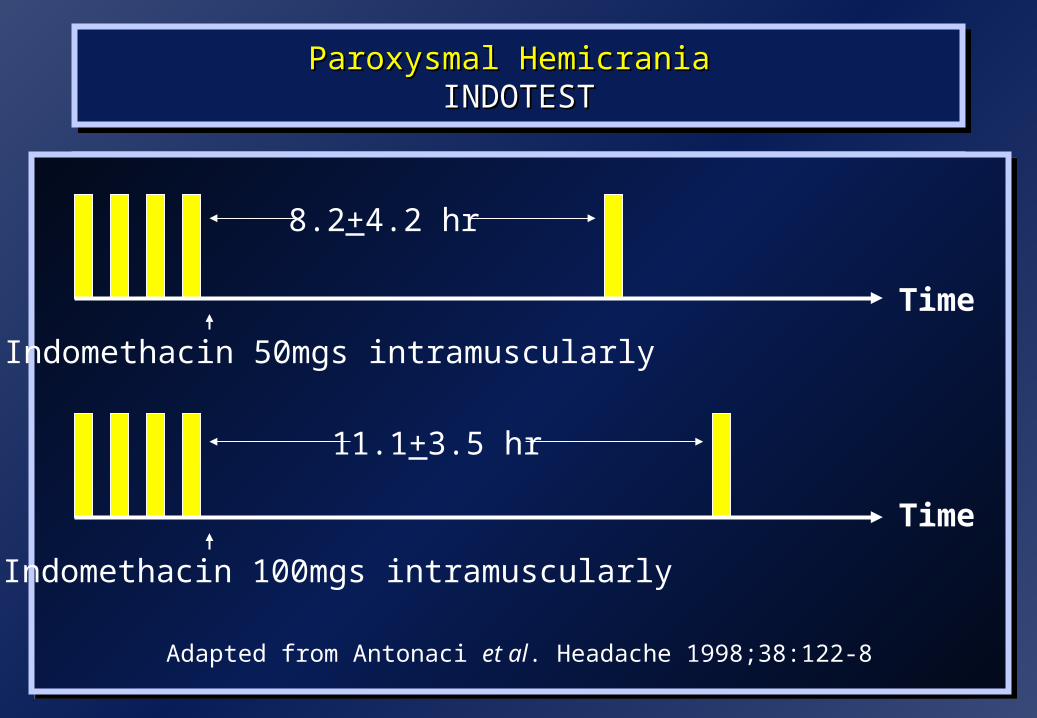
Time
Indomethacin 50mgs intramuscularly
8.2+4.2 hr
Indomethacin 100mgs intramuscularly
11.1+3.5 hr
Time
Adapted from Antonaci et al. Headache 1998;38:122-8
Paroxysmal Hemicrania Paroxysmal Hemicrania TREATMENTSTREATMENTS
Paroxysmal Hemicrania Paroxysmal Hemicrania TREATMENTSTREATMENTS
N=77
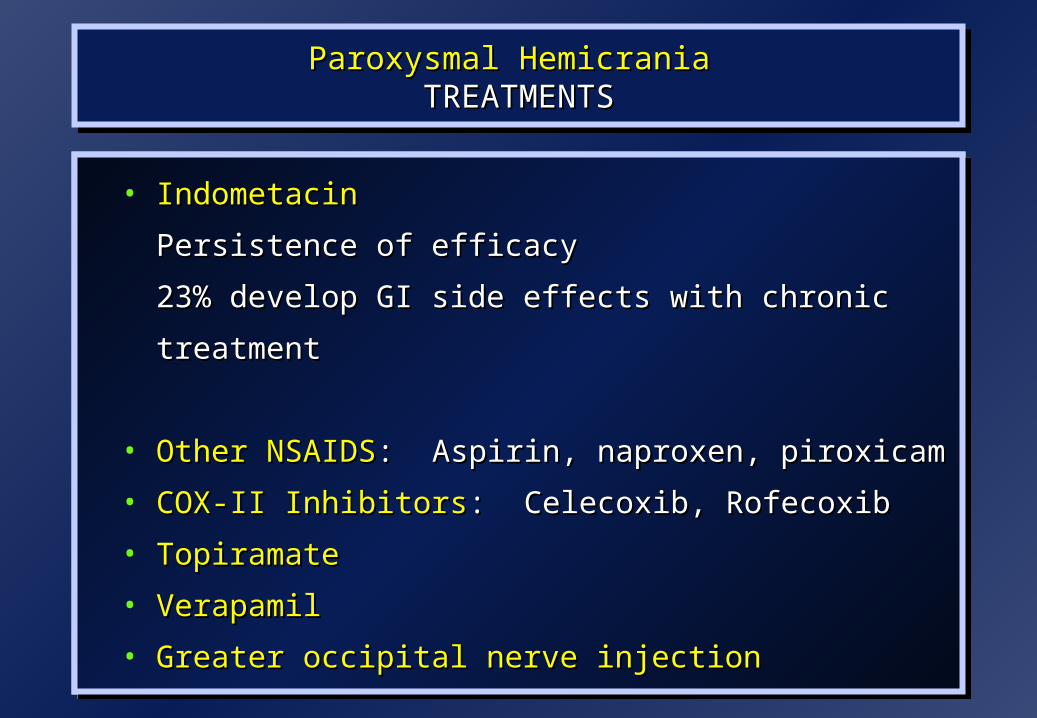
• IndometacinIndometacin
Persistence of efficacyPersistence of efficacy
23% develop GI side effects with chronic treatment23% develop GI side effects with chronic treatment
• Other NSAIDSOther NSAIDS: : Aspirin, naproxen, piroxicamAspirin, naproxen, piroxicam
• COX-II InhibitorsCOX-II Inhibitors: : Celecoxib, RofecoxibCelecoxib, Rofecoxib
• TopiramateTopiramate
• VerapamilVerapamil
• Greater occipital nerve injectionGreater occipital nerve injection
• IndometacinIndometacin
Persistence of efficacyPersistence of efficacy
23% develop GI side effects with chronic treatment23% develop GI side effects with chronic treatment
• Other NSAIDSOther NSAIDS: : Aspirin, naproxen, piroxicamAspirin, naproxen, piroxicam
• COX-II InhibitorsCOX-II Inhibitors: : Celecoxib, RofecoxibCelecoxib, Rofecoxib
• TopiramateTopiramate
• VerapamilVerapamil
• Greater occipital nerve injectionGreater occipital nerve injection

SUNCT SUNCT SUNCT SUNCT
SShort-lasting hort-lasting
UUnilateral nilateral
NNeuralgiform attacks with euralgiform attacks with
CConjunctival injection and onjunctival injection and
TTearingearing

SUNCT SUNCT IHS CLASSIFICATION CRITERIAIHS CLASSIFICATION CRITERIA
SUNCT SUNCT IHS CLASSIFICATION CRITERIAIHS CLASSIFICATION CRITERIA
• Unilateral orbital, supraorbital or temporal painUnilateral orbital, supraorbital or temporal pain
• Stabbing or pulsating painStabbing or pulsating pain
• 10-240 seconds duration10-240 seconds duration
• Attack frequency from 3-200/dayAttack frequency from 3-200/day
• Pain is accompanied by conjunctival injection and lacrimationPain is accompanied by conjunctival injection and lacrimation
• Unilateral orbital, supraorbital or temporal painUnilateral orbital, supraorbital or temporal pain
• Stabbing or pulsating painStabbing or pulsating pain
• 10-240 seconds duration10-240 seconds duration
• Attack frequency from 3-200/dayAttack frequency from 3-200/day
• Pain is accompanied by conjunctival injection and lacrimationPain is accompanied by conjunctival injection and lacrimation
Trigeminal Autonomic CephalgiasTrigeminal Autonomic CephalgiasTrigeminal Autonomic CephalgiasTrigeminal Autonomic Cephalgias
Cluster
HeadacheParoxysmal Hemicrania
SUNCT
Attack frequency (daily) 1-8 1-40 3-200
Duration of attack 15-180mins 2-30mins 5-240secs
Pain qualitySharp,
throbbingSharp,
throbbingStabbing, burning
Autonomic features +++ +++ +++*
Restless or agitated 90% 80% 65%
Trigeminal Autonomic CephalgiasTrigeminal Autonomic CephalgiasTrigeminal Autonomic CephalgiasTrigeminal Autonomic Cephalgias
Cluster Cluster
HeadacheHeadacheParoxysmal Paroxysmal HemicraniaHemicrania
SUNCTSUNCT
Migrainous features ++ ++ +
Triggers• Alcohol• NTG• Cutaneous
++++++
-
++-
--
+++
Circadian periodicity 70% 45% Absent
Episodic : Chronic 90:10 35:65 10:90
Trigeminal Autonomic CephalgiasTrigeminal Autonomic CephalgiasTrigeminal Autonomic CephalgiasTrigeminal Autonomic Cephalgias
Cluster
HeadacheParoxysmal Hemicrania
SUNCT
Lifetime prevalence 1/1000 1/50,000* 1/50,000*
F:M ratio 1:2.5-7.2 1:1 1:1.5
Age• Mean• Range
306-67
375-68
4819-75
SUNCT SUNCT DIFFERENTIAL DIAGNOSISDIFFERENTIAL DIAGNOSIS
SUNCT SUNCT DIFFERENTIAL DIAGNOSISDIFFERENTIAL DIAGNOSIS
• Secondary causesSecondary causes
– Posterior fossa pathologyPosterior fossa pathology
– Pituitary tumoursPituitary tumours
• Trigeminal neuralgiaTrigeminal neuralgia
• Primary stabbing headachePrimary stabbing headache
• Paroxysmal hemicraniaParoxysmal hemicrania

SUNCT Vs Trigeminal NeuralgiaSUNCT Vs Trigeminal NeuralgiaSUNCT Vs Trigeminal NeuralgiaSUNCT Vs Trigeminal Neuralgia
FeatureFeature SUNCTSUNCT TNTN
Gender (M:F)Gender (M:F) 1.5:11.5:1 1:21:2
Site of painSite of pain VV11 VV2/32/3
Duration (secs)Duration (secs) 5-2405-240 <5<5
Autonomic featuresAutonomic features ProminentProminent SparseSparse
Refractory periodRefractory period AbsentAbsent PresentPresent
Trigeminal Vascular loopTrigeminal Vascular loop 7%7% 47-90%47-90%

SUNCT SUNCT DIFFERENTIAL DIAGNOSISDIFFERENTIAL DIAGNOSIS
SUNCT SUNCT DIFFERENTIAL DIAGNOSISDIFFERENTIAL DIAGNOSIS
• Stabbing or jabbing painStabbing or jabbing pain• Ophthalmic trigeminal Ophthalmic trigeminal
distributiondistribution• Last a few seconds (rarely Last a few seconds (rarely
up to 1 minute)up to 1 minute)• Occurs at irregular Occurs at irregular
intervalsintervals
• Site of pain varies from Site of pain varies from
attack to attackattack to attack• Spontaneous attacks onlySpontaneous attacks only• Autonomic features Autonomic features
absentabsent• Attacks subside with Attacks subside with
indomethacinindomethacin
Primary Stabbing HeadachePrimary Stabbing Headache
SUNCT SUNCT INVESTIGATIONSINVESTIGATIONS
SUNCT SUNCT INVESTIGATIONSINVESTIGATIONS
MRI (including pituitary views)MRI (including pituitary views)
Pituitary hormone profilePituitary hormone profile
Trial of indomethacinTrial of indomethacin
SUNCT SUNCT TREATMENTSTREATMENTS
SUNCT SUNCT TREATMENTSTREATMENTS
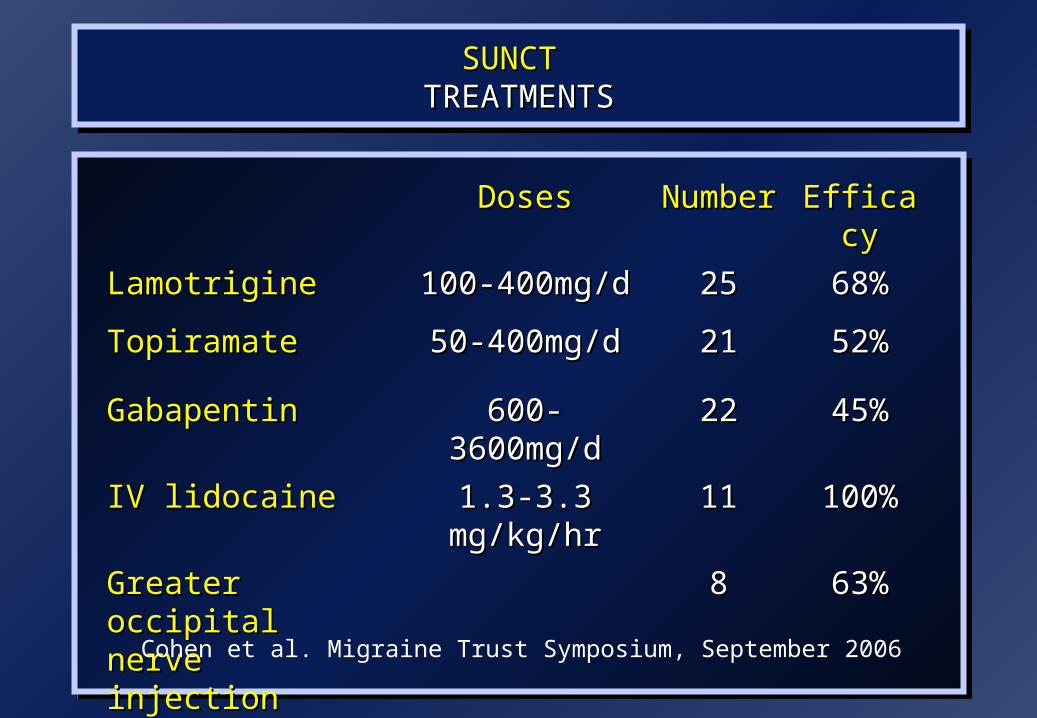
DosesDoses NumberNumber EfficacyEfficacy
LamotrigineLamotrigine 100-400mg/d100-400mg/d 2525 68%68%
TopiramateTopiramate 50-400mg/d50-400mg/d 2121 52%52%
GabapentinGabapentin 600-3600mg/d600-3600mg/d 2222 45%45%
IV lidocaineIV lidocaine 1.3-3.3 mg/kg/hr1.3-3.3 mg/kg/hr 1111 100%100%
Greater occipital Greater occipital nerve injectionnerve injection
88 63%63%
Cohen et al. Migraine Trust Symposium, September 2006
SUNCT SUNCT TREATMENTSTREATMENTS
SUNCT SUNCT TREATMENTSTREATMENTS
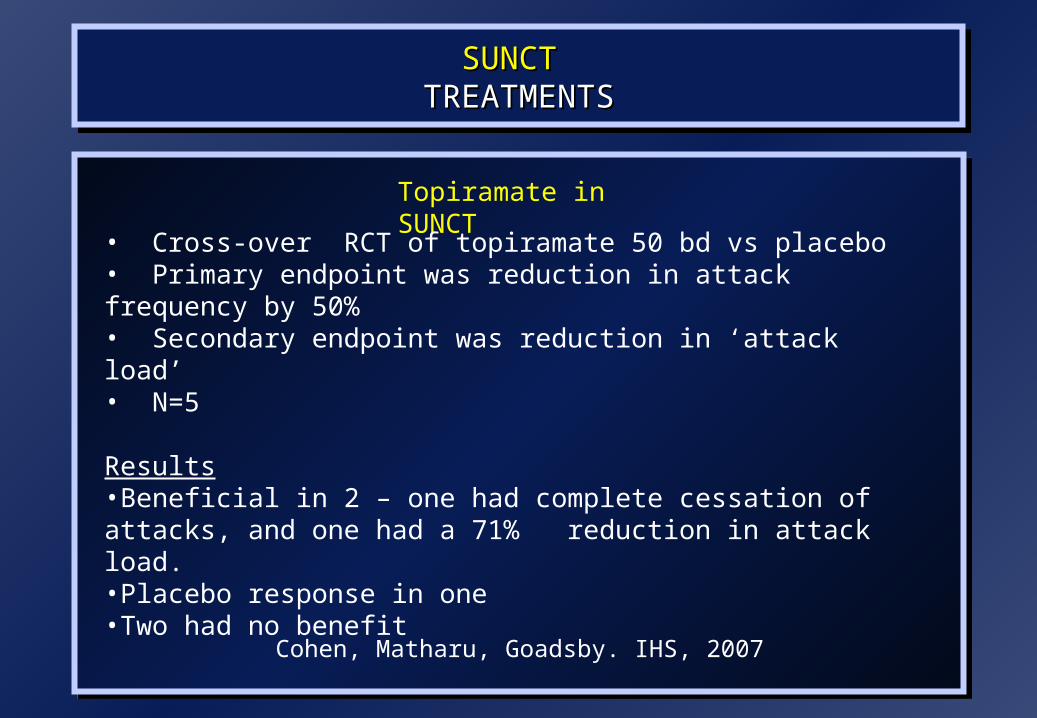
Cohen, Matharu, Goadsby. IHS, 2007
Topiramate in SUNCT
• Cross-over RCT of topiramate 50 bd vs placebo• Primary endpoint was reduction in attack frequency by 50% • Secondary endpoint was reduction in ‘attack load’ • N=5
Results•Beneficial in 2 – one had complete cessation of attacks, and one had a 71% reduction in attack load. •Placebo response in one•Two had no benefit

SUNCT SUNCT TREATMENTSTREATMENTS
SUNCT SUNCT TREATMENTSTREATMENTS
Hypothalamic StimulatorHypothalamic Stimulator
Leone M, Leone M, Ann NeurolAnn Neurol 2005. 2005.

Trigeminal Autonomic Cephalgias Trigeminal Autonomic Cephalgias PATHOPHYSIOLOGYPATHOPHYSIOLOGY
Trigeminal Autonomic Cephalgias Trigeminal Autonomic Cephalgias PATHOPHYSIOLOGYPATHOPHYSIOLOGY
Cluster HeadachePET Study
May et al, Lancet 1998
Ipsilateral hypothalamic activation in CH
Trigeminal Autonomic Cephalgias Trigeminal Autonomic Cephalgias PATHOPHYSIOLOGYPATHOPHYSIOLOGY
Trigeminal Autonomic Cephalgias Trigeminal Autonomic Cephalgias PATHOPHYSIOLOGYPATHOPHYSIOLOGY
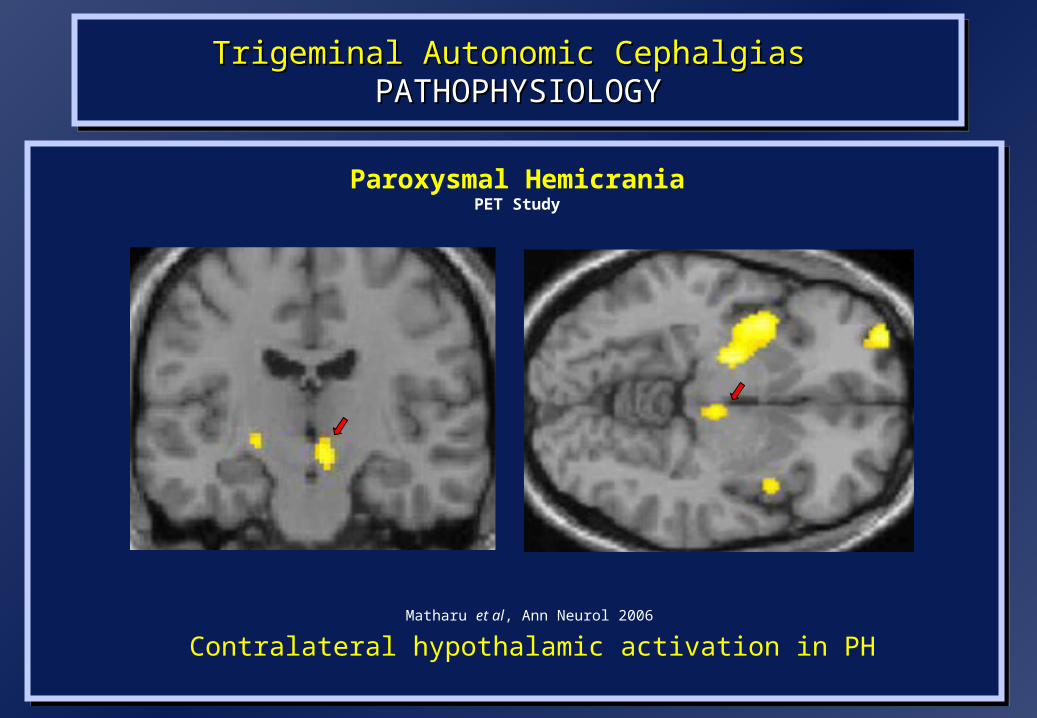
Paroxysmal HemicraniaPET Study
Matharu et al, Ann Neurol 2006
Contralateral hypothalamic activation in PH

Trigeminal Autonomic Cephalgias Trigeminal Autonomic Cephalgias PATHOPHYSIOLOGYPATHOPHYSIOLOGY
Trigeminal Autonomic Cephalgias Trigeminal Autonomic Cephalgias PATHOPHYSIOLOGYPATHOPHYSIOLOGY
SUNCTfMRI Studies
May et al, Ann Neurol 1999 Cohen et al, Cephalalgia 2004Sprenger et al, Pain 2005
Hypothalamic activation in SUNCT

Functional Neuroimaging of Primary HeadachesHeadache Phase
Functional Neuroimaging of Primary HeadachesHeadache Phase
Episodic and Chronic MigraineEpisodic and Chronic MigraineEpisodic and Chronic MigraineEpisodic and Chronic Migraine
Spontaneous Episodic Migraine
Weiller et al, Nature 1995
Spontaneous Episodic Migraine
Afridi et al, Arch Neurol 2005
Chronic Migraine
Matharu et al, Brain 2004
Specific dorsal rostral pontine activation in migraine
Trigeminal Autonomic Cephalgias Trigeminal Autonomic Cephalgias PATHOPHYSIOLOGYPATHOPHYSIOLOGY
Trigeminal Autonomic Cephalgias Trigeminal Autonomic Cephalgias PATHOPHYSIOLOGYPATHOPHYSIOLOGY
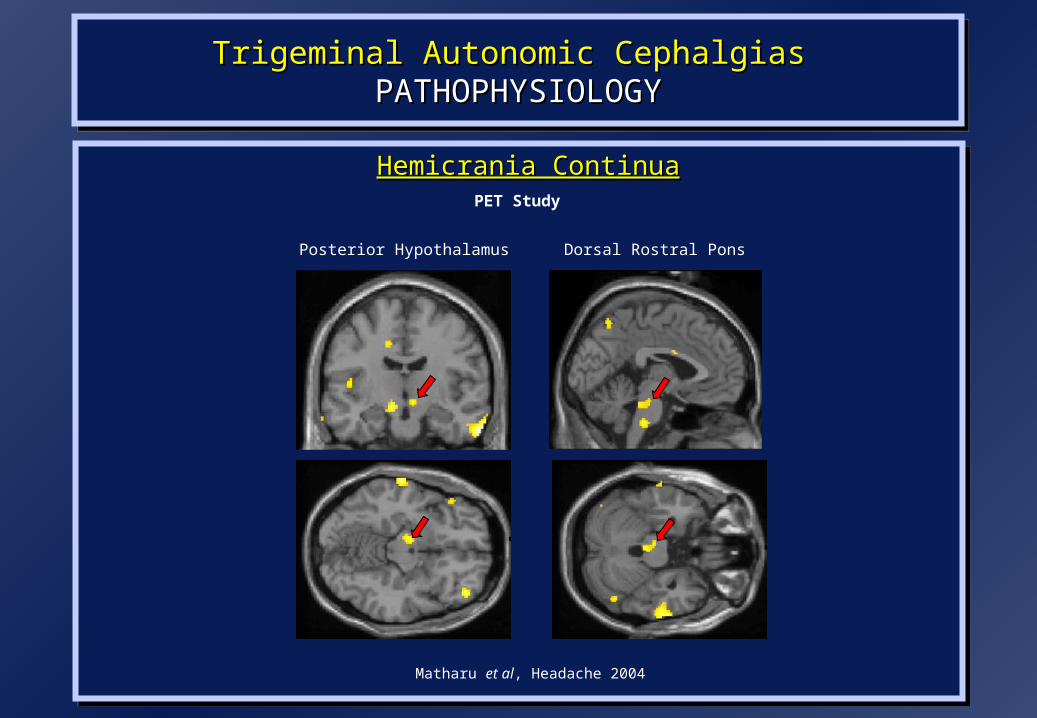
Hemicrania ContinuaHemicrania ContinuaHemicrania ContinuaHemicrania ContinuaPET Study
Matharu et al, Headache 2004
Posterior Hypothalamus Dorsal Rostral Pons
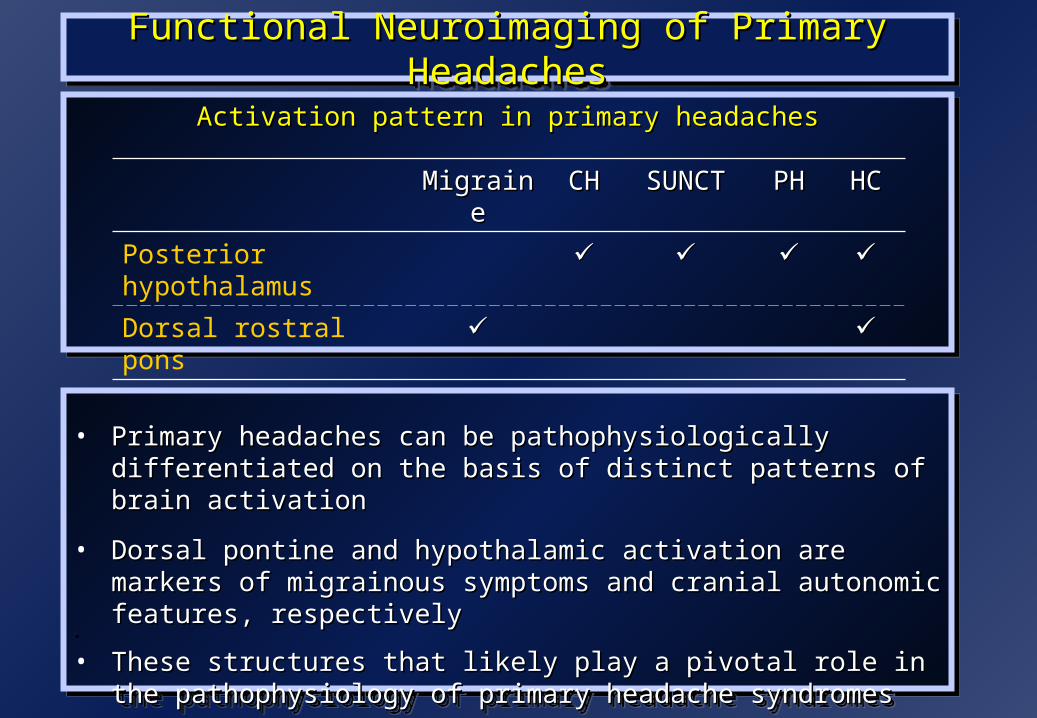
• Primary headaches can be pathophysiologically differentiated on the basis of Primary headaches can be pathophysiologically differentiated on the basis of distinct patterns of brain activationdistinct patterns of brain activation
• Dorsal pontine and hypothalamic activation are markers of migrainous Dorsal pontine and hypothalamic activation are markers of migrainous symptoms and cranial autonomic features, respectivelysymptoms and cranial autonomic features, respectively
•
• These structures that likely play a pivotal role in the pathophysiology of These structures that likely play a pivotal role in the pathophysiology of primary headache syndromesprimary headache syndromes
• Primary headaches can be pathophysiologically differentiated on the basis of Primary headaches can be pathophysiologically differentiated on the basis of distinct patterns of brain activationdistinct patterns of brain activation
• Dorsal pontine and hypothalamic activation are markers of migrainous Dorsal pontine and hypothalamic activation are markers of migrainous symptoms and cranial autonomic features, respectivelysymptoms and cranial autonomic features, respectively
•
• These structures that likely play a pivotal role in the pathophysiology of These structures that likely play a pivotal role in the pathophysiology of primary headache syndromesprimary headache syndromes
Activation pattern in primary headachesActivation pattern in primary headachesActivation pattern in primary headachesActivation pattern in primary headaches
Functional Neuroimaging of Primary HeadachesFunctional Neuroimaging of Primary HeadachesFunctional Neuroimaging of Primary HeadachesFunctional Neuroimaging of Primary Headaches
MigraineMigraine CHCH SUNCTSUNCT PHPH HCHC
Posterior hypothalamus
Dorsal rostral pons
““Pain is a more Pain is a more terrible lord of terrible lord of mankind than mankind than even death itself” even death itself”
Albert SchweitzerAlbert Schweitzer
““Pain is a more Pain is a more terrible lord of terrible lord of mankind than mankind than even death itself” even death itself”
Albert SchweitzerAlbert Schweitzer
Related Documents
![Medulloblastoma: [Print] - eMedicine Neurology · emedicine.medscape.com eMedicine Specialties > Neurology > Pediatric Neurology Medulloblastoma George I Jallo, MD, Associate Professor](https://static.cupdf.com/doc/110x72/5d472c3c88c993527c8b60e5/medulloblastoma-print-emedicine-neurology-emedicinemedscapecom-emedicine.jpg)










