Trends in Donor Cell Source NMDP Presentation October 2016 Operated by the National Marrow Donor Program ®

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript
Trends in Donor Cell Source
NMDP PresentationOctober 2016
Operated by the National Marrow Donor Program®
Welcome to Minneapolis!
NMDP Mission Statement
We save lives through cellular therapy
Our focus is on patients for whom cellular therapy is the best hope for their diseases and often is
the only therapy available with an intent to cure.
NMDP Vision Statement
Successfully serve all patients in need of cellular therapy
NMDP is committed to removing barriers to cell therapy so that patients regardless of their ethnicity and
economic status have access.
– Be the Match/NMDP is the best-in-class cellular therapy registry that provides the most comprehensive array of cellular therapy products and services and listing of donors and cord bloods easily accessed through our proprietary algorithm
– Through the CIBMTR, we will continue to lead the field in conducting cellular therapy research that improves outcomes and is rapidly adopted by the field
– Foster a sustainable organization that has the resources to continuously invest in and improve our organization
NMDP Strategic Objectives
Conclusions • Few patients lack an acceptable donor• All donors (8/8, 7/8 adult, haplo, cord)
produce outcomes that, if not identical, are in same range– Maximum differences in survival, compared to
8/8 adult donor, are in the range of 10%-15%• Donor availability cannot fully account for
differences in access to HCT in diverse ethnic and racial groups

There’s new hope for blood cancers, and it comes from umbilical cords
• Washington Post Article of Sept 4th, 2016– Story of Jesse Quinn
• Cord Blood Expansion• Haploidentical
Transplants
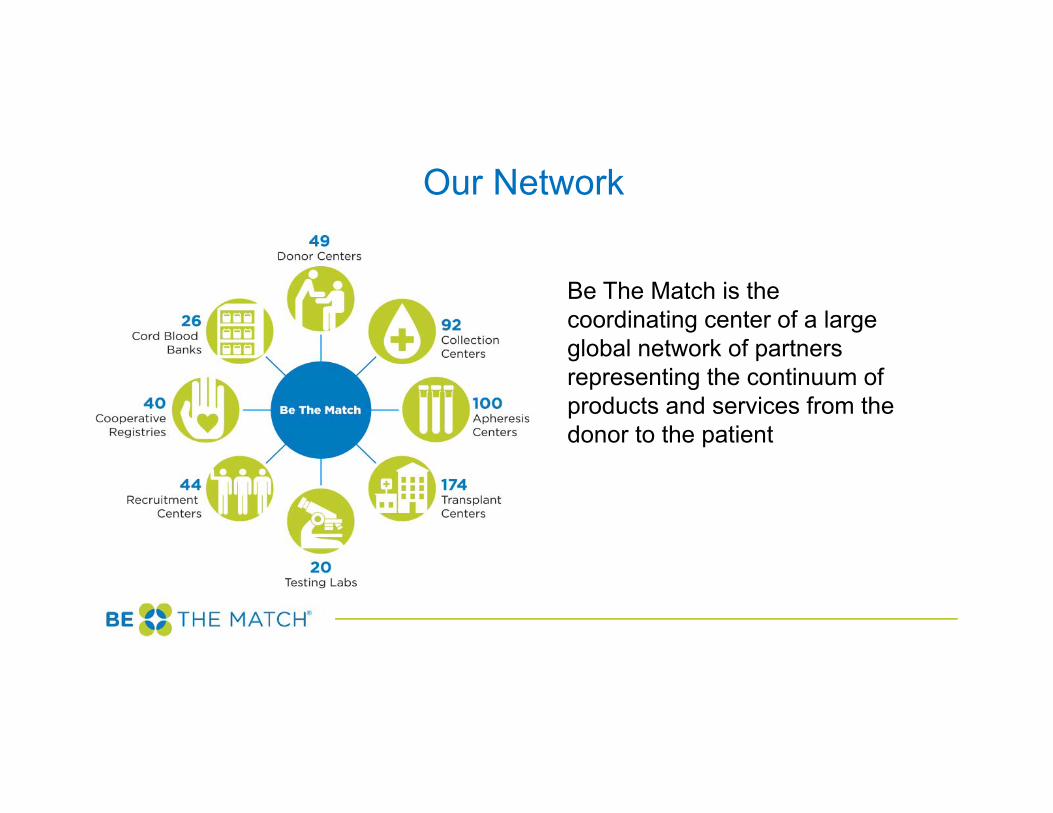
Our Network
Be The Match is the coordinating center of a large global network of partners representing the continuum of products and services from the donor to the patient
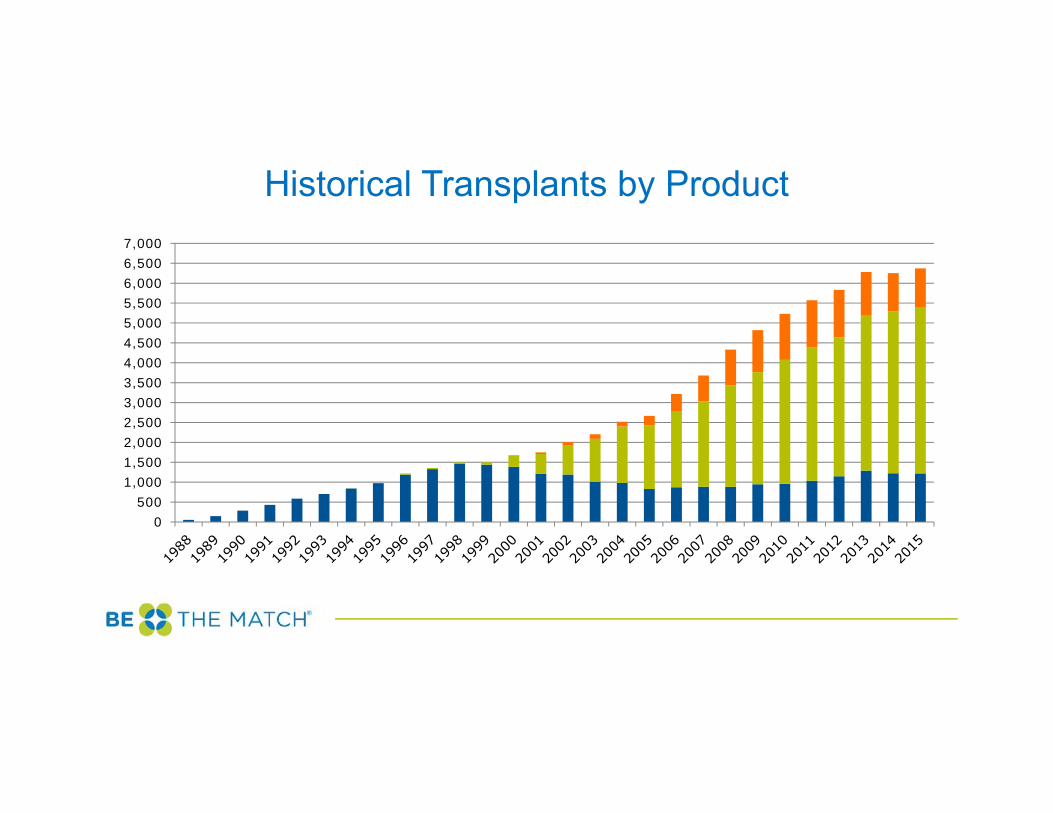
Historical Transplants by Product
0500
1,0001,5002,0002,5003,0003,5004,0004,5005,0005,5006,0006,5007,000
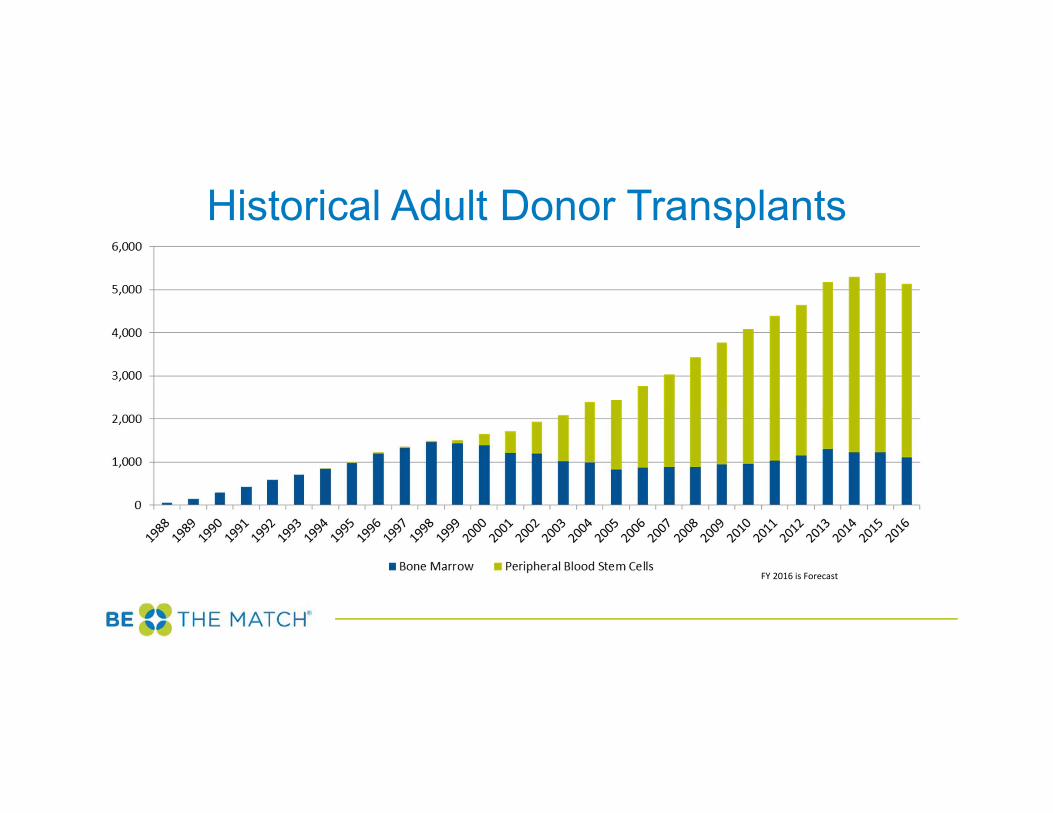
Historical Adult Donor Transplants
FY 2016 is Forecast
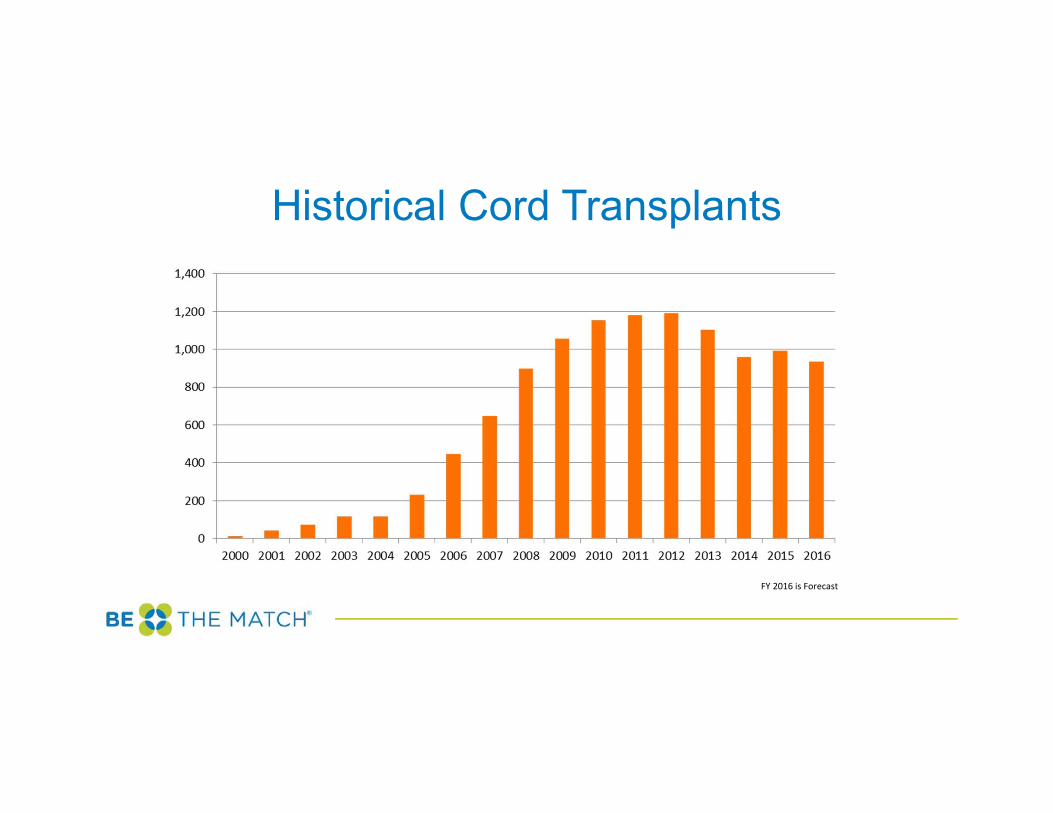
Historical Cord Transplants
FY 2016 is Forecast
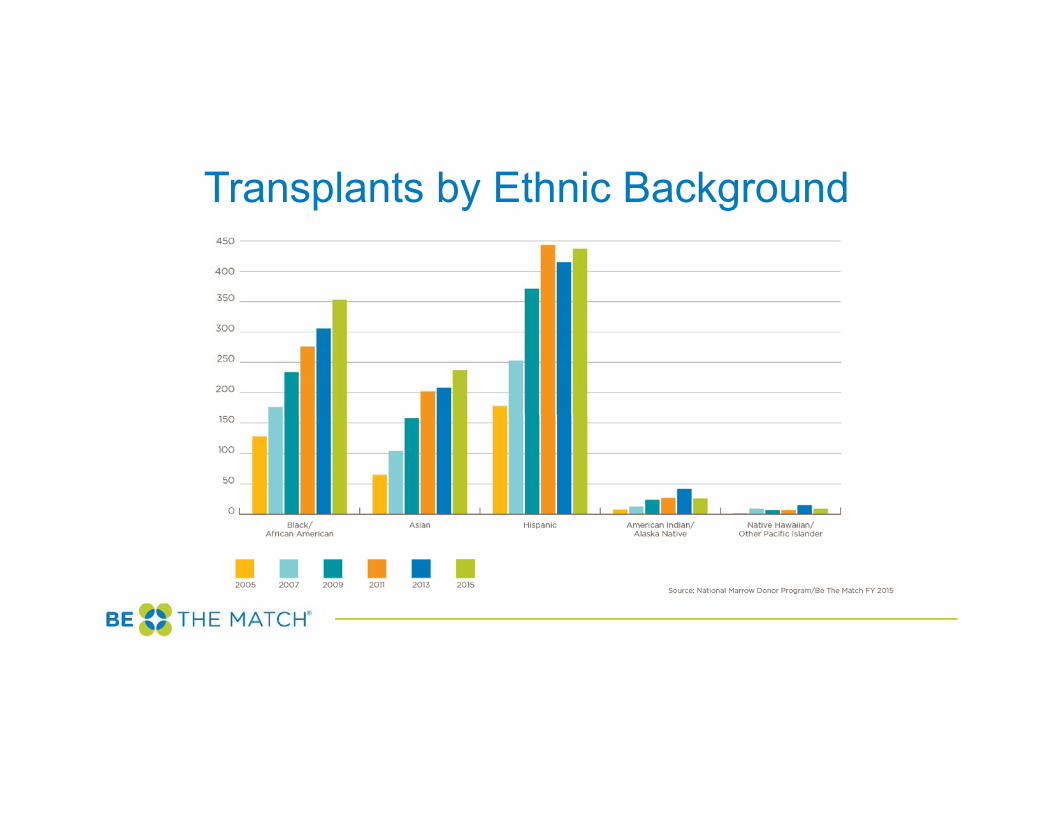
Transplants by Ethnic Background
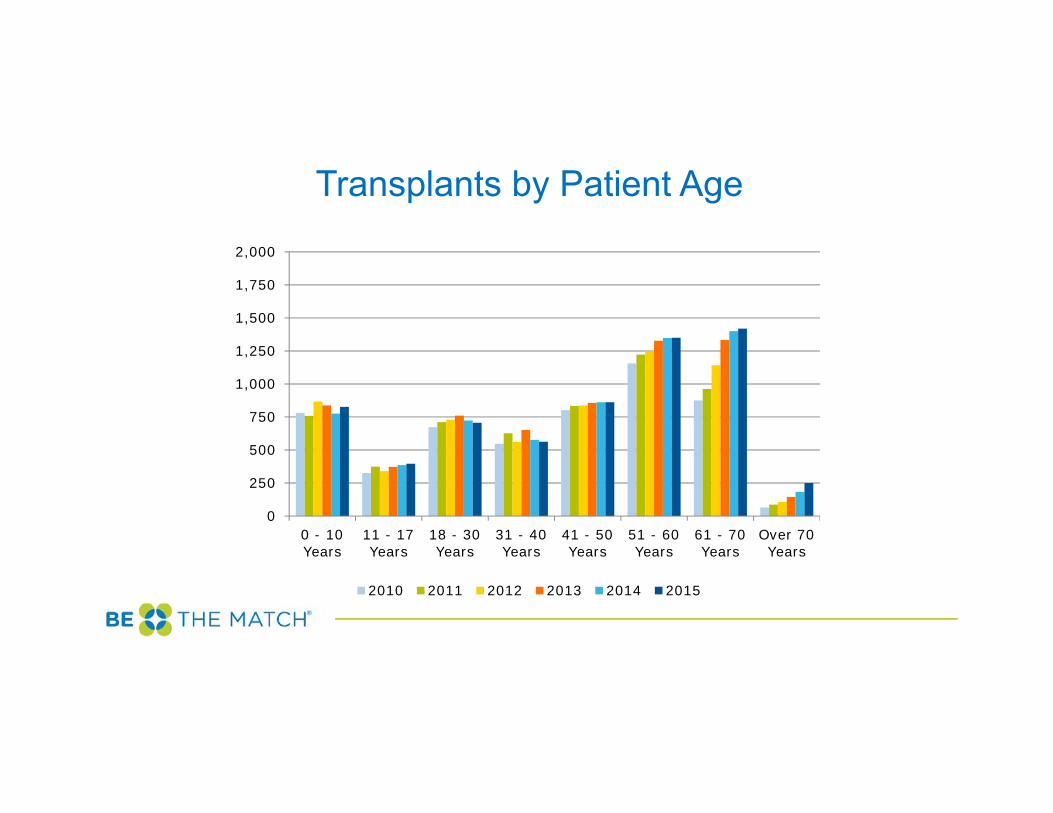
Transplants by Patient Age
0
250
500
750
1,000
1,250
1,500
1,750
2,000
0 - 10Years
11 - 17Years
18 - 30Years
31 - 40Years
41 - 50Years
51 - 60Years
61 - 70Years
Over 70Years
2010 2011 2012 2013 2014 2015
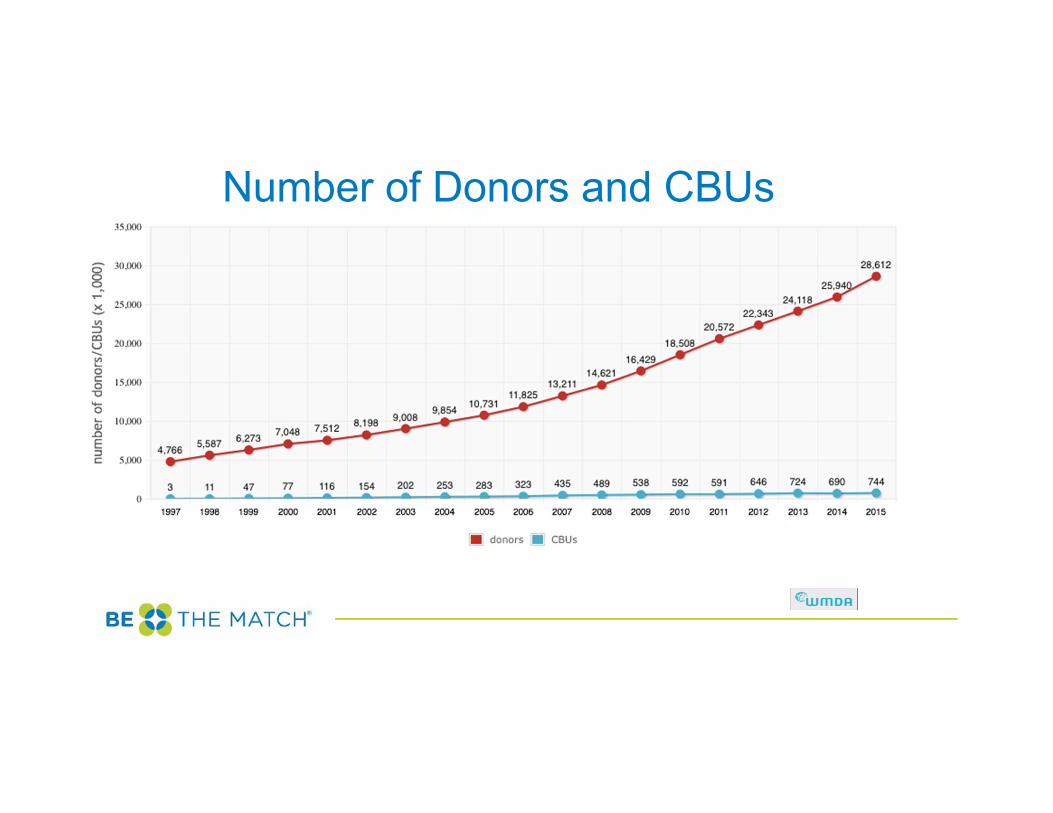
Number of Donors and CBUs
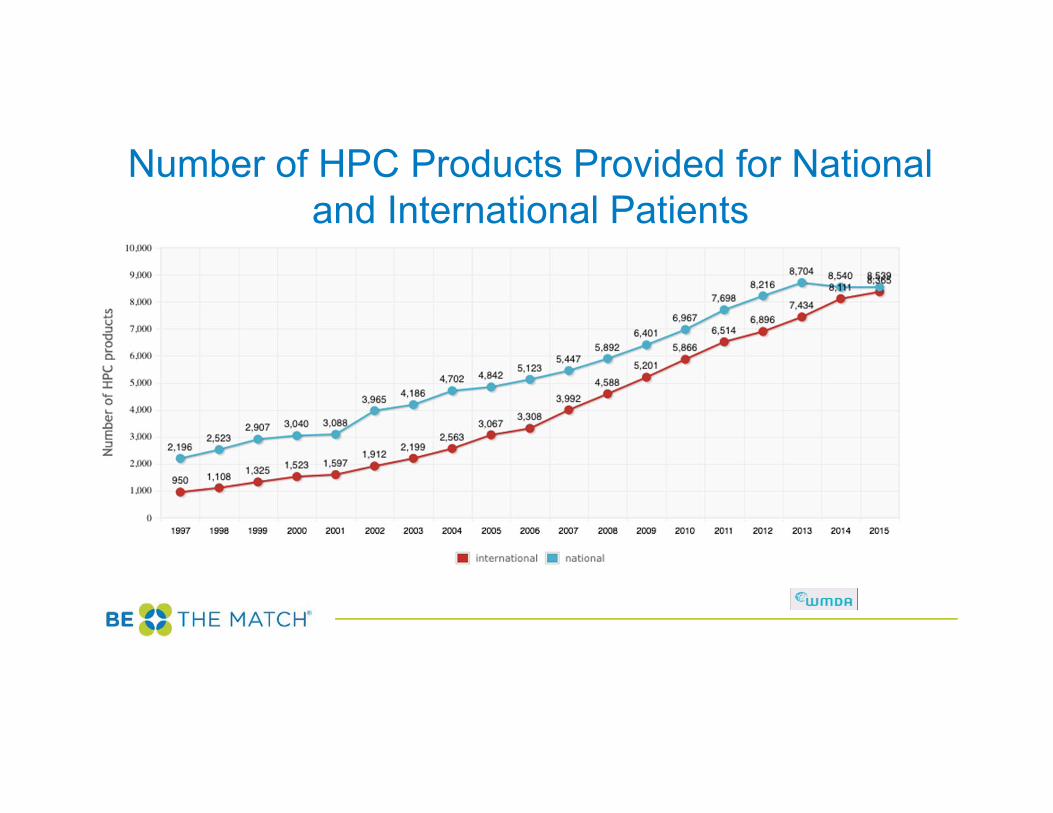
Number of HPC Products Provided for National and International Patients
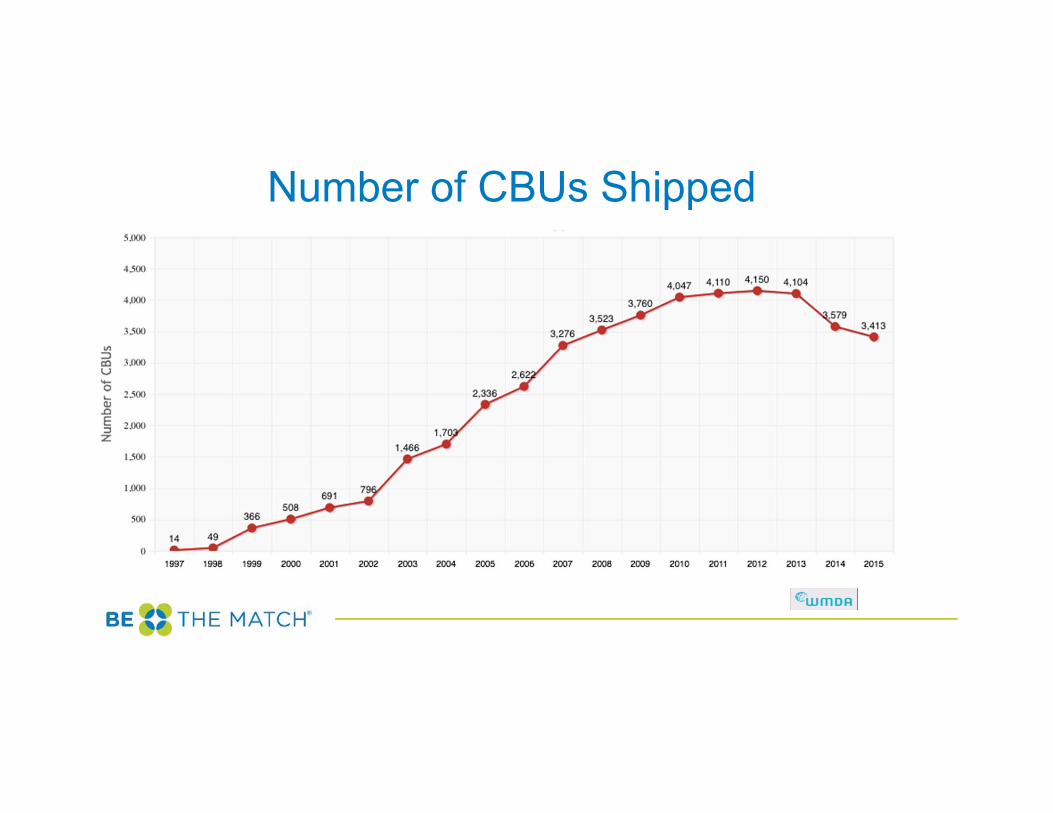
Number of CBUs Shipped
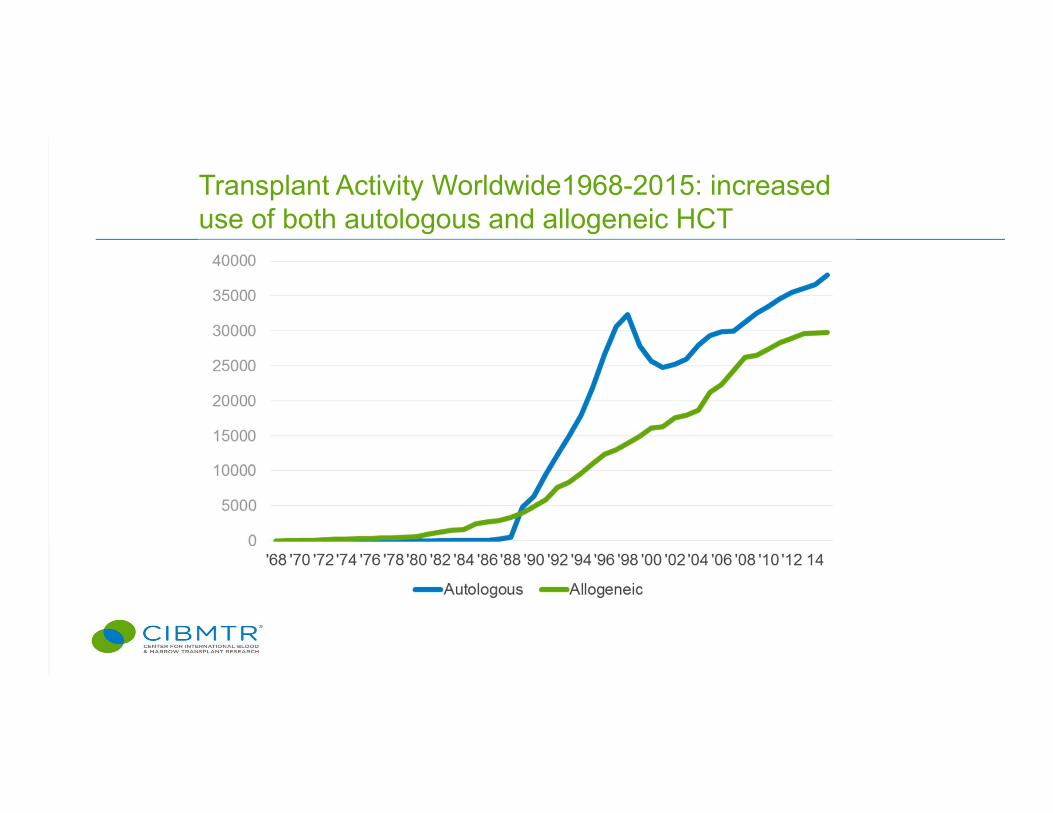
Transplant Activity Worldwide1968-2015: increased use of both autologous and allogeneic HCT
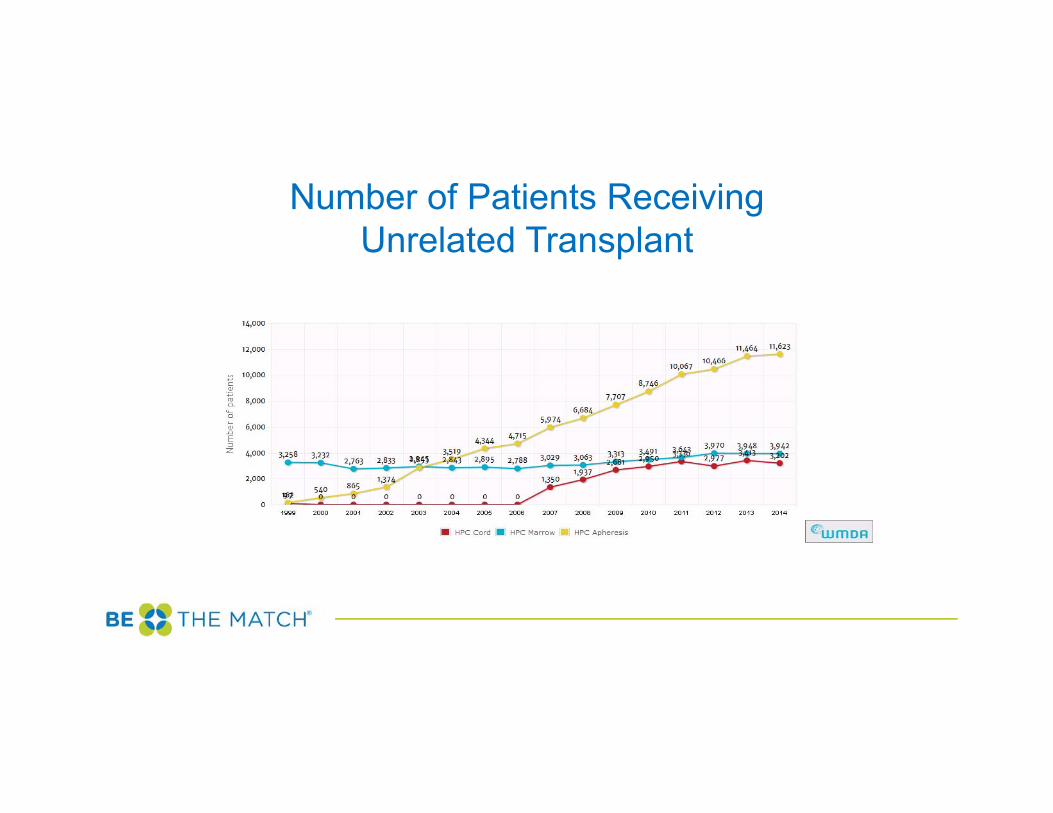
Number of Patients Receiving Unrelated Transplant
Volunteer Donors
• NMDP has on file – 13.5 million adult donors – 225,000 cord blood units
• Total Global Supply– 28 million donors– 744,000 cord blood units
International Activity
• Last year, NMDP provided donors for patients in 37 countries
• U.S. patients received donors from 42 countries• NMDP provides research samples and
repository services for international partners
Non-match Barriers to Transplant
• Increasingly important as adult donor and cord blood registries grow
• Non-match barriers to access and care have a profound effect on our ability to make transplant therapies accessible to all
• Language, literacy, finances, insurance, geography, lack of knowledge, predisposition by general Hematologists and Oncologists towards non-transplant therapies all have an impact
Trends in Graft Sources for Allogeneic Hematopoietic Stem Cell Transplantation (HCT): Everyone Has a Donor
Mary M. Horowitz, MD, MSCIBMTR, Medical College of WisconsinSeptember, 2016
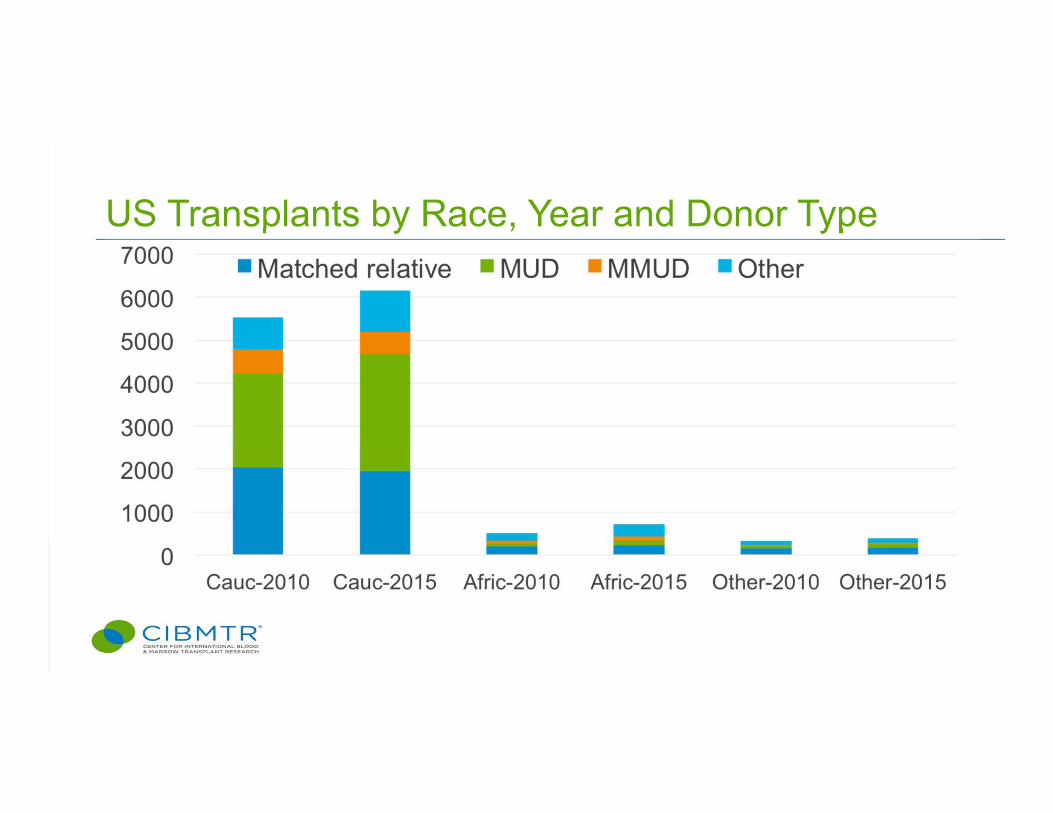
US Transplants by Race, Year and Donor Type
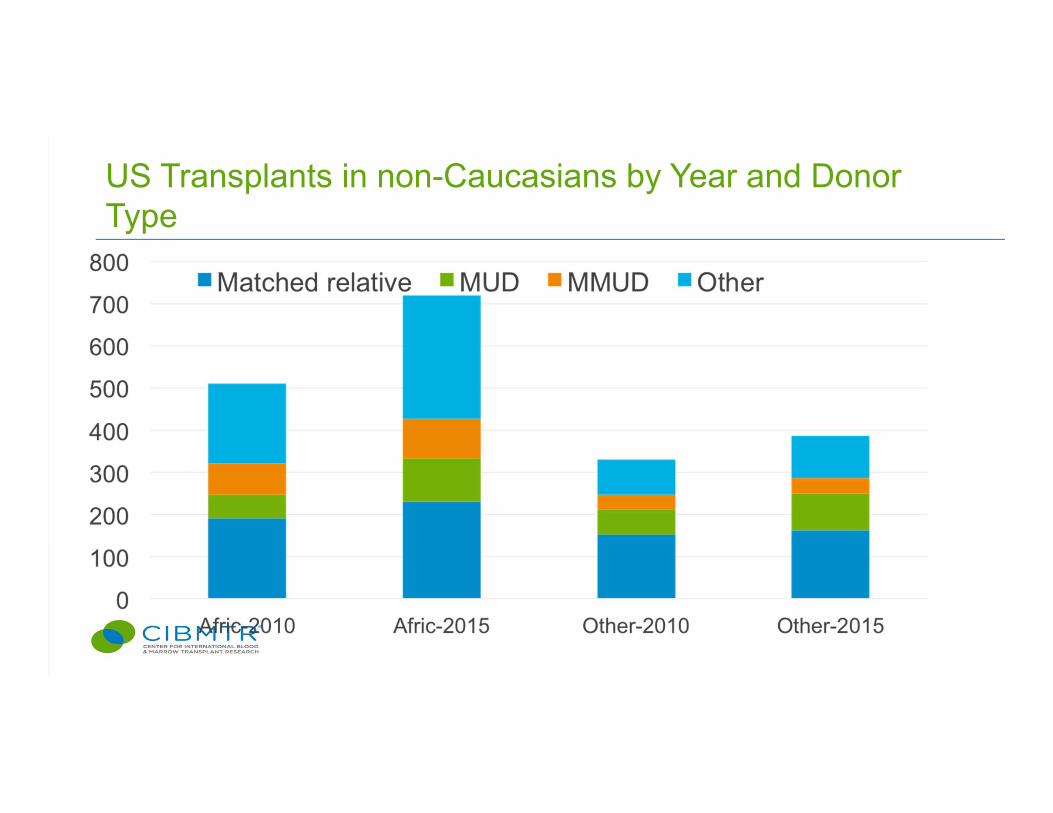
US Transplants in non-Caucasians by Year and Donor Type
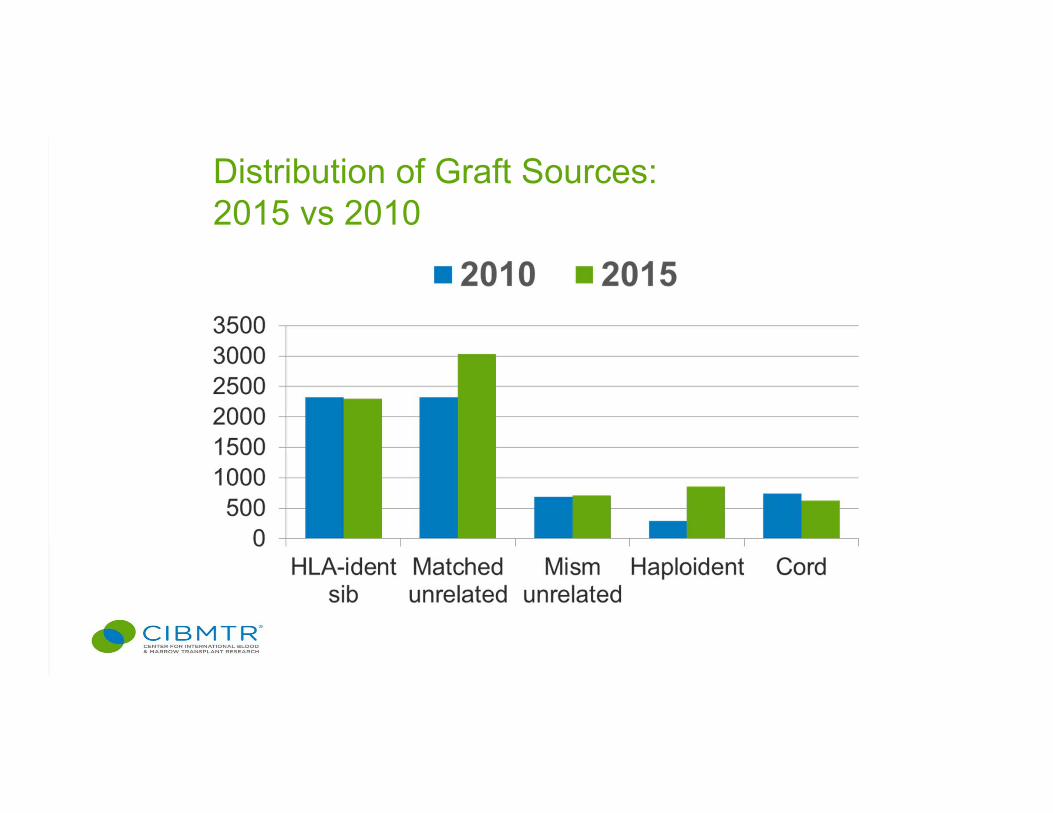
Distribution of Graft Sources: 2015 vs 2010
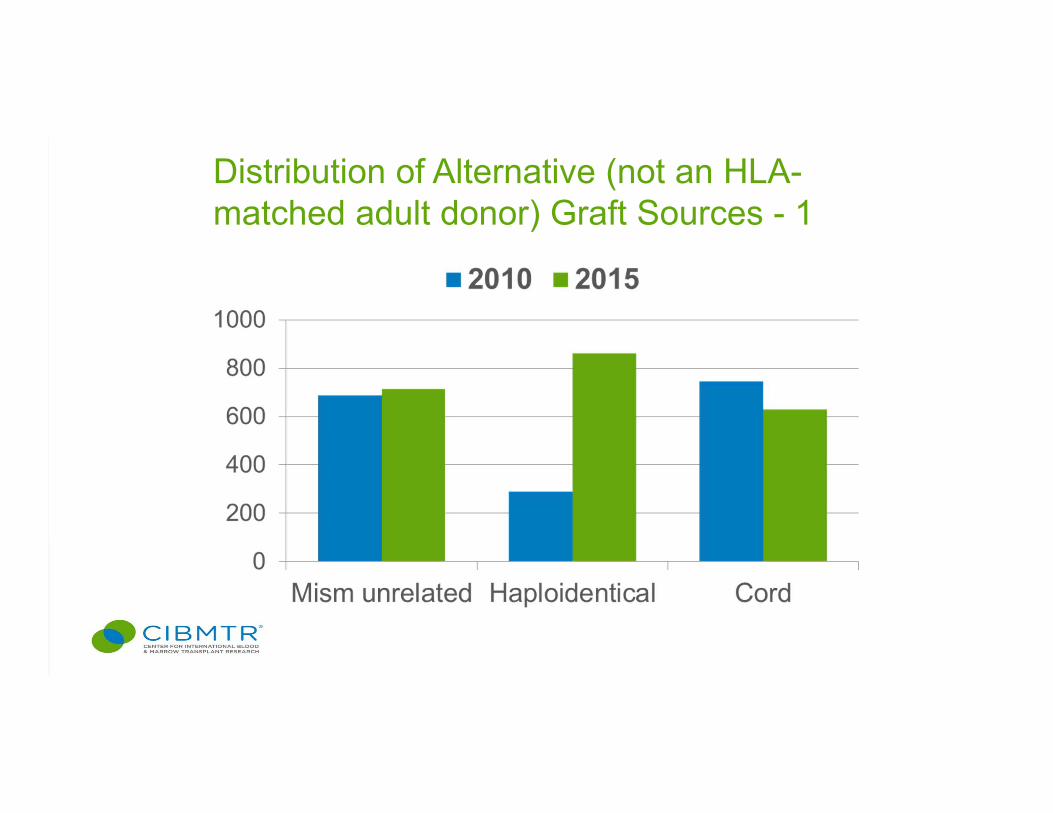
Distribution of Alternative (not an HLA-matched adult donor) Graft Sources - 1
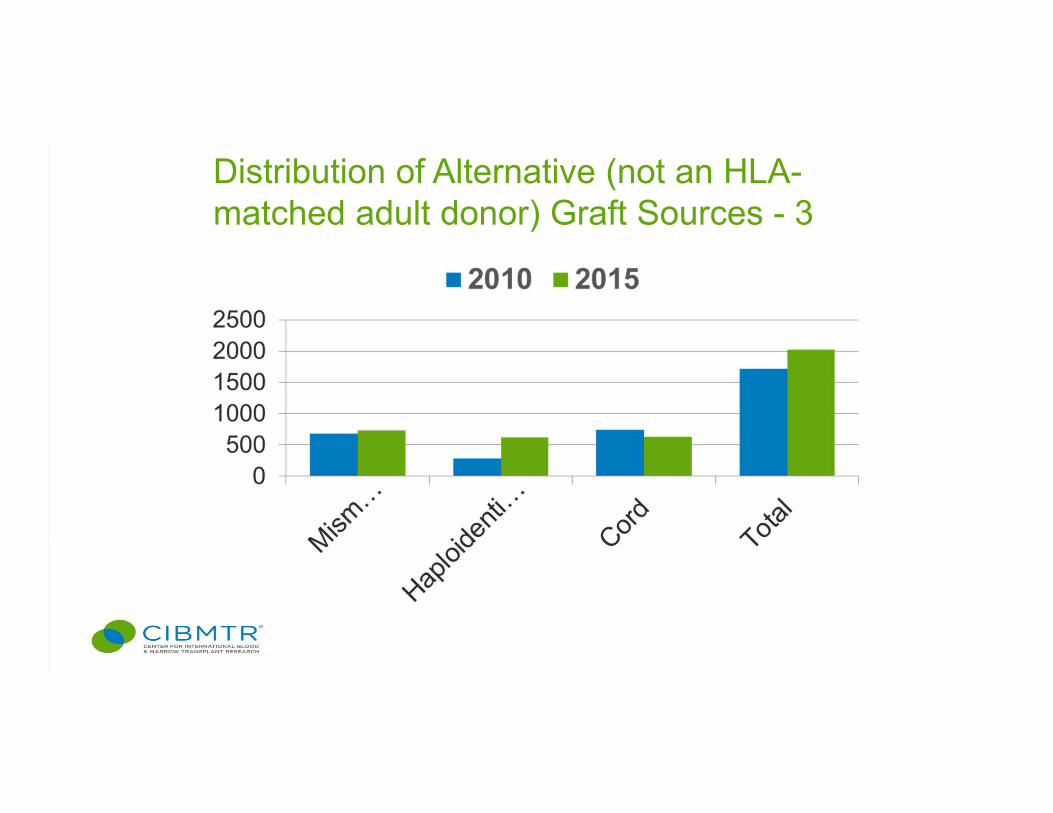
Distribution of Alternative (not an HLA-matched adult donor) Graft Sources - 3
Reasons for Increased Use• Better outcomes
• Expanding Indications: MDS, follicular
lymphoma, myeloma
• Expanding Age Range: up to 75 for both
autos and allos
• Expanding Donor Availability and Sources
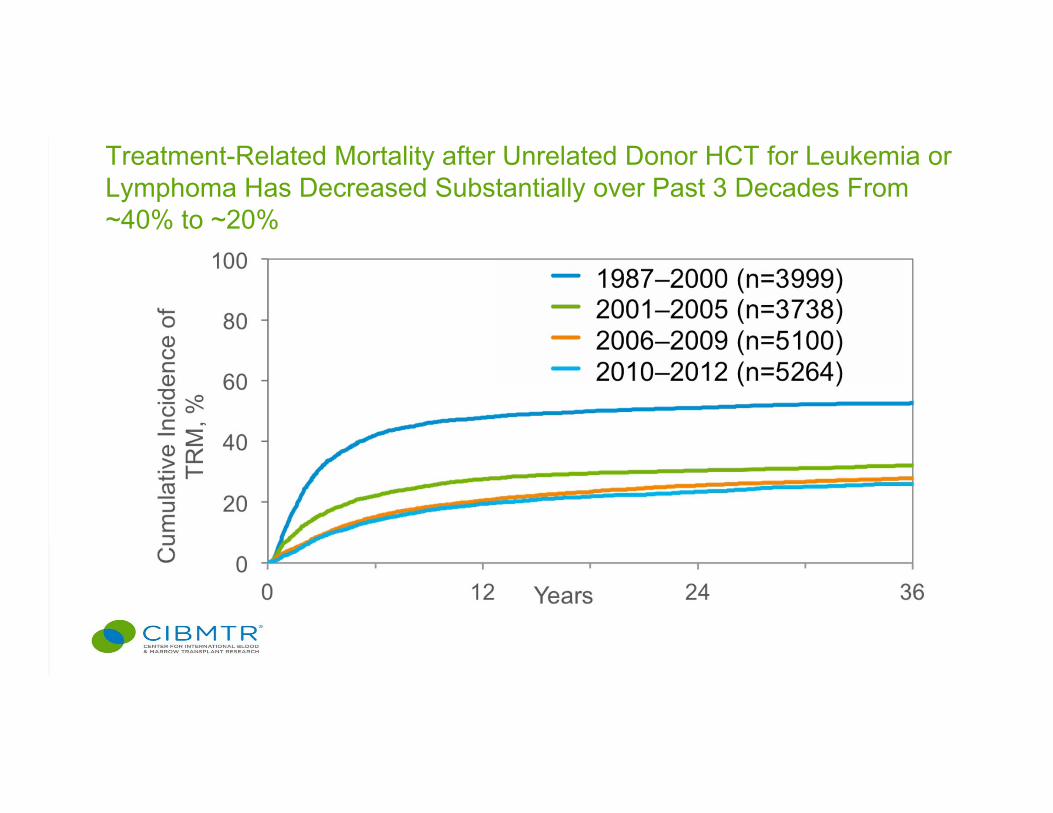
Treatment-Related Mortality after Unrelated Donor HCT for Leukemia or Lymphoma Has Decreased Substantially over Past 3 Decades From ~40% to ~20%
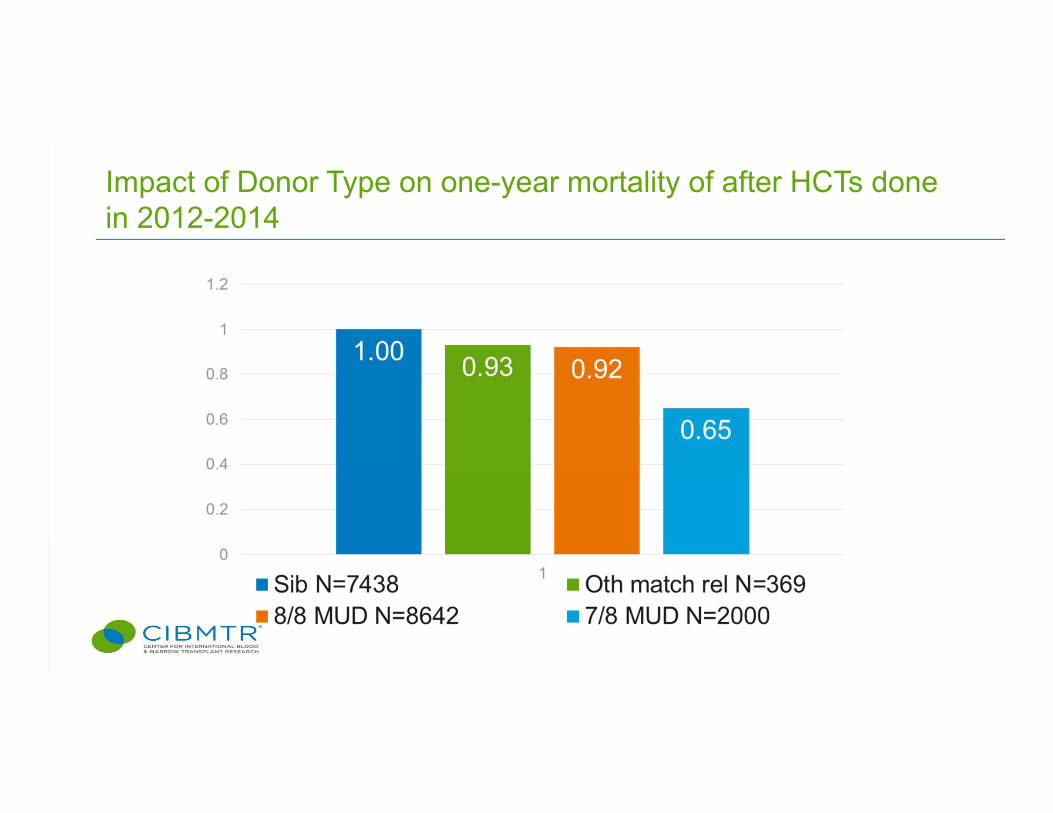
Impact of Donor Type on one-year mortality of after HCTs done in 2012-2014
Other HLA/Donor Characteristics Associated with Outcome• Low-expression HLA alleles (DQ, DP, DRB3,4,5)
– Permissive versus non-permissive DP mismatches– Multiple mismatches
• Donor age – age >46 about equivalent to a single locus mismatch
• Non-HLA genomics – KIR Phenotype• Others – CMV, sex-match, ABO-match
Donor Availability • HLA-matched relative 25-30%• Unrelated donor 40-90%
– Optimally selected* 10-60%*HLA-matched, permissive DP mismatch, age <30, (ABO, CMV, sex)
Umbilical Cord BloodAdvantages: Immediately available (important for
patients with rapidly progressive diseases) No risk to donor Allows more HLA-mismatch with lower
risk of GVHD
Cord Blood Transplantation• Multiple studies from individual centers,
Eurocord, the NYBC, EBMT and CIBMTR document that Umbilical Cord Blood cells – Can establish durable hematopoiesis– Have potent graft-versus-tumor effects– Can lead to successful transplant outcomes in a
variety of malignant and non-malignant diseases in adults and children
• Outcomes of UCB transplants have improved over time
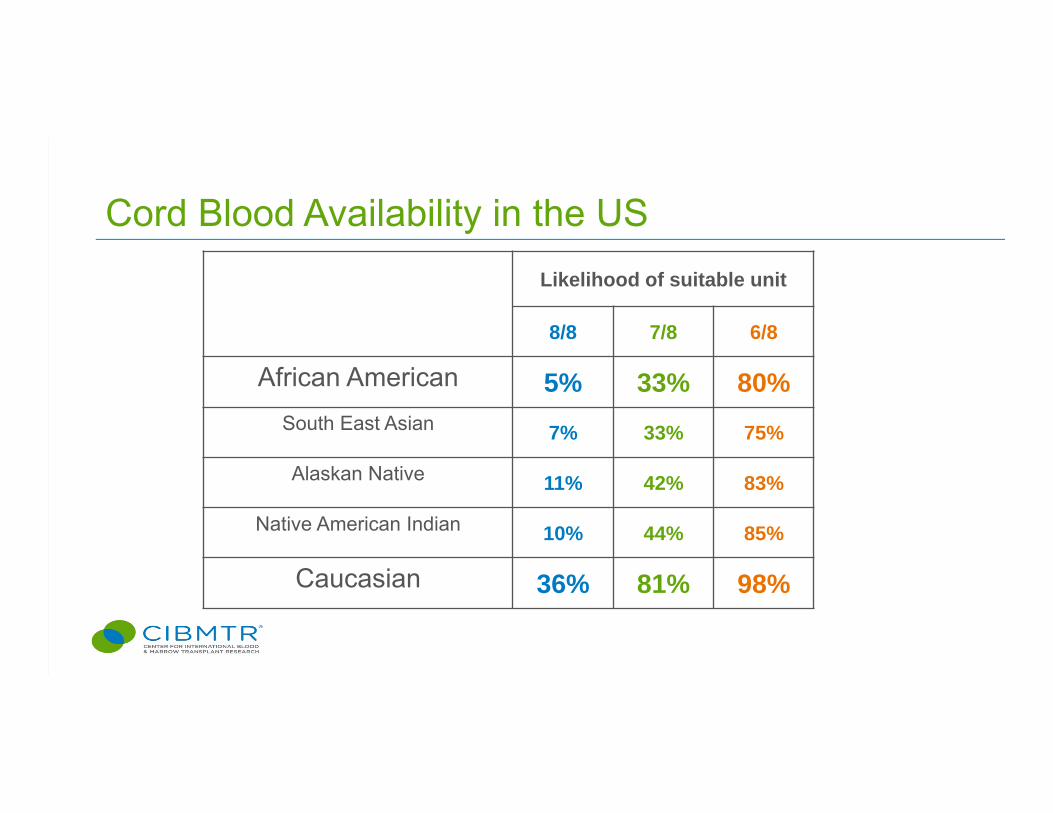
Cord Blood Availability in the USLikelihood of suitable unit
8/8 7/8 6/8
African American 5% 33% 80%South East Asian 7% 33% 75%
Alaskan Native 11% 42% 83%
Native American Indian 10% 44% 85%
Caucasian 36% 81% 98%
Limitations of Cord Blood Use• Major limitation to Cord Blood Transplantation is the small number
of cells in each unit– Slow hematopoietic recovery– Slow immune recovery– Graft failure– No second donation
• Strategies:– Selection of large units– Double cord transplantation (expensive)– Expansion and homing techniques (in development, often requires two
units)
The “New” Alternative – Haploidentical• Europe: haplo-transplants using T-depleted
peripheral blood grafts long used for a small but important proportion of transplants
• China: intensive immune suppression allows successful haplo-transplantation
• US: very few haplo-transplants until last 6 years– No approved CD34 selection or T-depletion device– Hopkins approach using post-transplant
cyclophosphamide increased interest– Technically simple, costs similar to HLA-identical sib
transplantation
BMT CTN 0603 and 0604: Parallel Single Arm Studies of Haploand CB Transplants • Age ≤ 70• Diseases
– Leukemia: high risk, in remission– Lymphoma
• Hodgkin, mantle cell, or large cell: chemosensitive relapse, not eligible for autologous SCT
• Follicular or marginal zone: multiply relapsed• Adequate organ function, performance score >60%• N=50 in each trial• Primary endpoint: 6-month survival
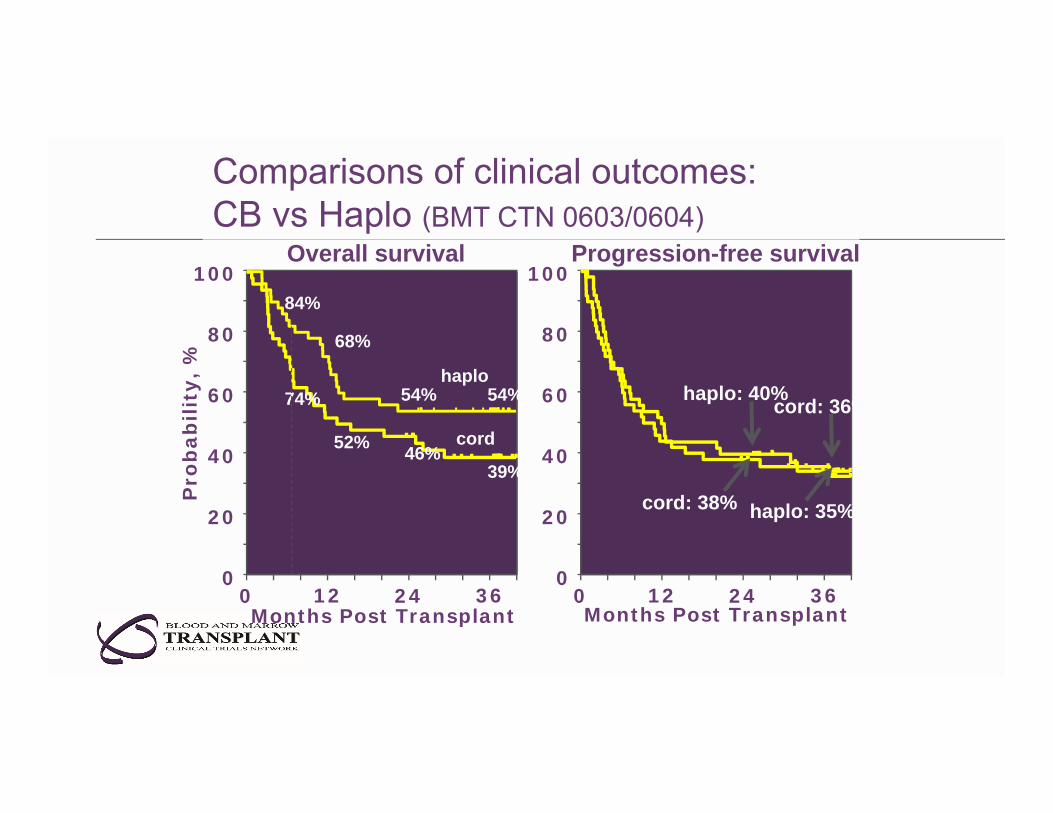
Comparisons of clinical outcomes:CB vs Haplo (BMT CTN 0603/0604)
Months Post Transplant
Pro
bab
ility
, %
100
0
20
40
60
80
0 2412 36
68%
54% 54%
52% 46%39%
84%
74%haplo
cord
100
0
20
40
60
80
Months Post Transplant0 2412 36
haplo: 35%
cord: 36%
cord: 38%
haplo: 40%
Overall survival Progression-free survival
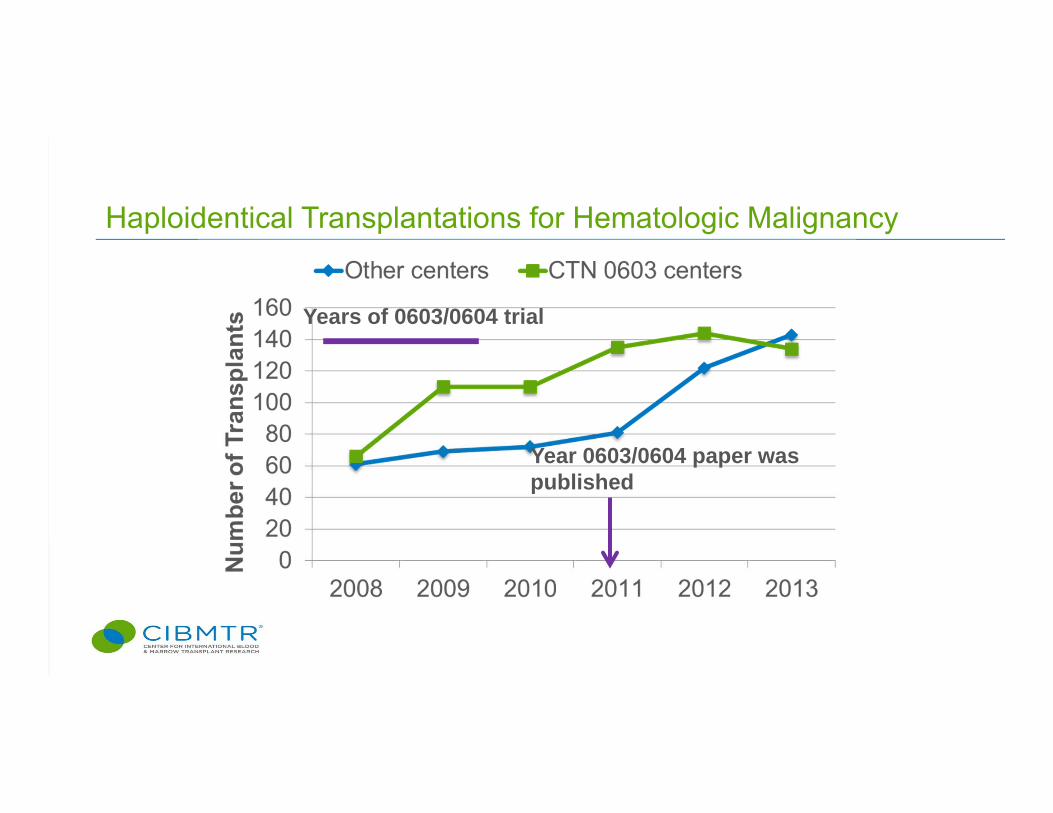
Haploidentical Transplantations for Hematologic Malignancy
Year 0603/0604 paper was published
Years of 0603/0604 trial
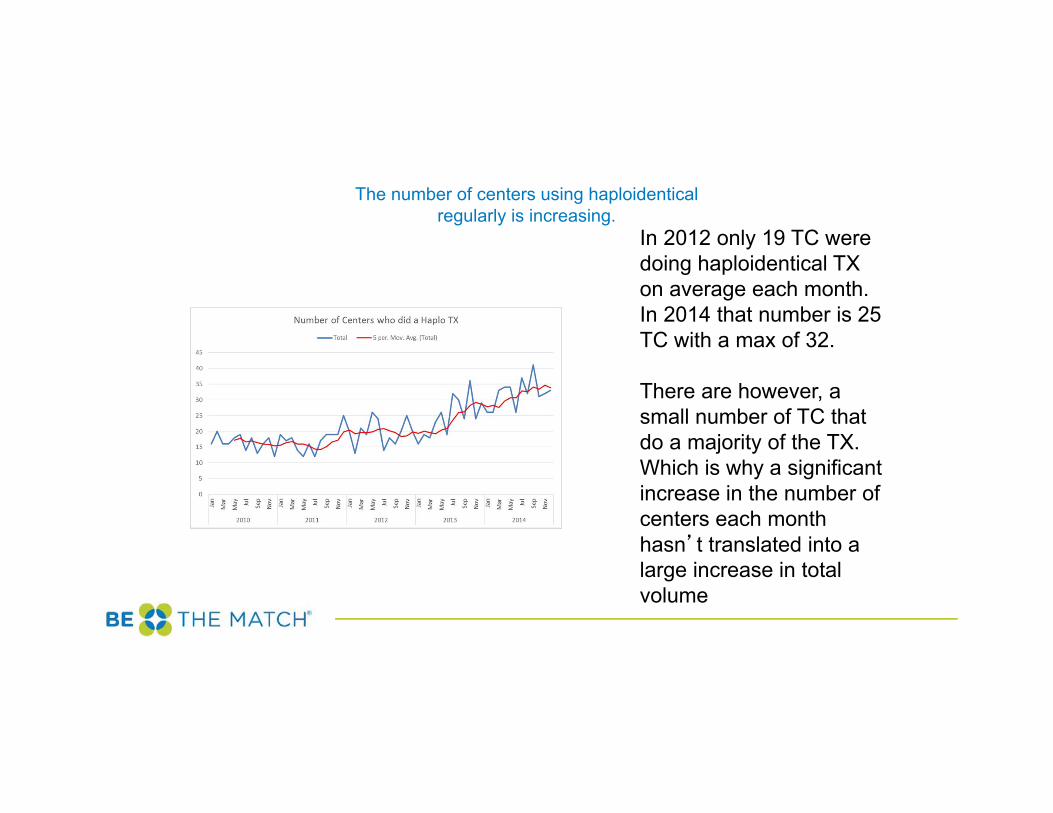
The number of centers using haploidenticalregularly is increasing.
In 2012 only 19 TC were doing haploidentical TX on average each month.In 2014 that number is 25 TC with a max of 32.
There are however, a small number of TC that do a majority of the TX. Which is why a significant increase in the number of centers each month hasn’t translated into a large increase in total volume
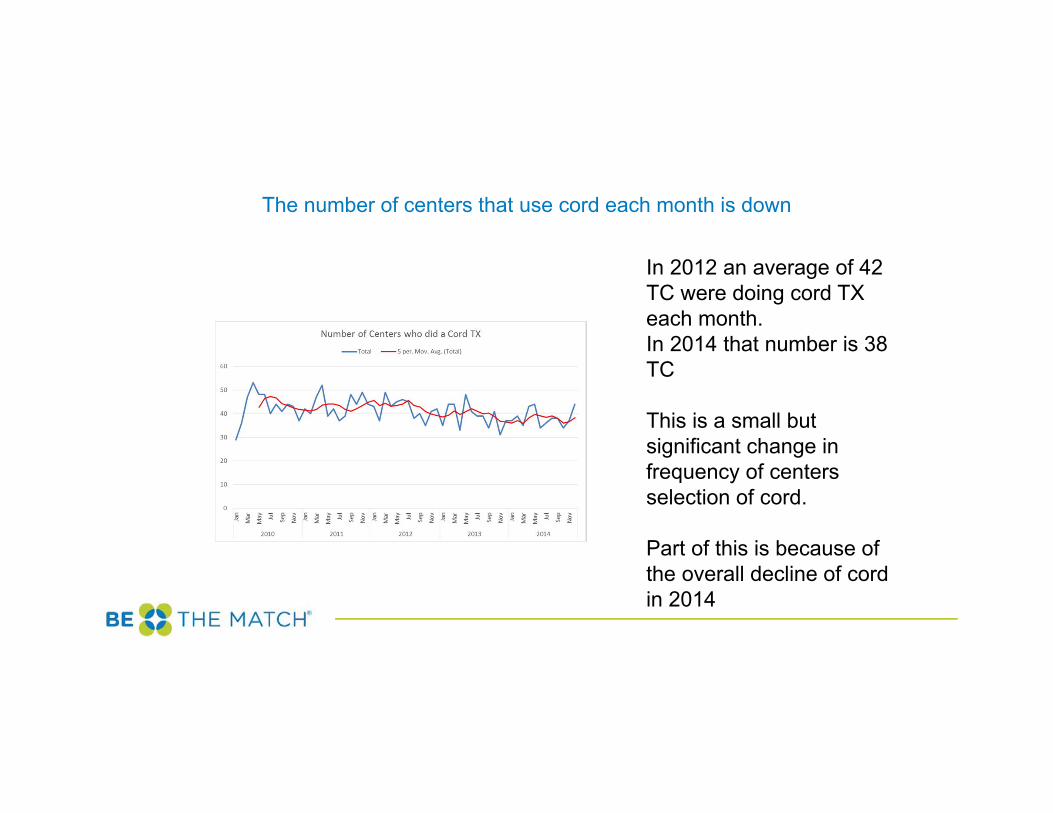
The number of centers that use cord each month is down
In 2012 an average of 42 TC were doing cord TX each month.In 2014 that number is 38 TC
This is a small but significant change in frequency of centers selection of cord.
Part of this is because of the overall decline of cord in 2014
BMT CTN 1101: Randomized Comparison of Haplo and Double Cord HCT• Primary: 2 year Progression-free survival• Secondary: Engraftment, hematopoietic recovery, GVHD,
TRM, relapse/progression, infections, hospitalizations, health-related quality of life
• Planned ancillary studies:• Immune reconstitution• Cost effectiveness• 267 of 410 patients accrued to date
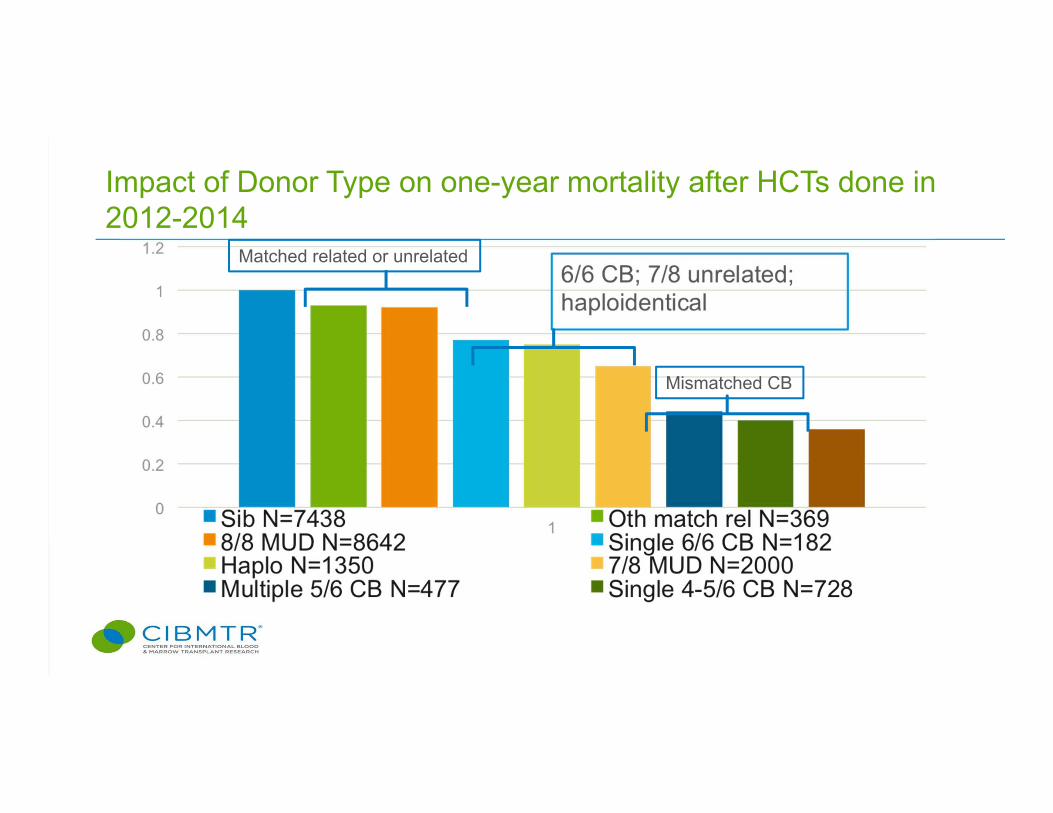
Impact of Donor Type on one-year mortality after HCTs done in 2012-2014
Matched related or unrelated
Mismatched CB
What Do We Know About Haplos with Post-txCyclophosphamide?• Haploidentical HCT can be performed with low GVHD and low
early TRM and acceptable 2-3 year overall mortality, when used with postCy
• Haploidentical HCT is increasingly used, predominantly for adult patients who do not have an HLA-matched adult donor –and some who do
Some Unknowns About Haplos with Post-tx Cyclophosphamide
• Long-term control of malignancy• Engraftment in non-malignant diseases• Optimal graft type (PB or BM) or conditioning
regimen• Suitability of Older Donors
– More graft failure– Clonal hematopoiesis more common with older
donors – uncertain significance
Some Other Important Unknowns About Post-txCyclophosphamide
• Roles in HLA-mismatched unrelated donor transplantation
• Role in HLA-matched related and unrelated donor transplantation
• Viral immunity• Are the same donor and recipient risk factors
important for TRM, relapse and survival
US National Trials Addressing Some of These Issues• BMT CTN 1101: Haplo vs Cord with reduced
intensity conditioning• BMT CTN 1203: PostCy as GVHD prophylaxis with
matched donors and reduced intensity conditioning• BMT CTN 1301: PostCy as GVHD prophylaxis with
matched donors and myeloablative conditioning• BMT CTN 1502: Haplo with PostCy and UCB for
aplastic anemia • BMT CTN 1507: Haplo with PostCy in Sickle Cell
Disease• RCI BMT MMUD: PostCy as GVHD prophylaxis with
multiply mismatched unrelated donors
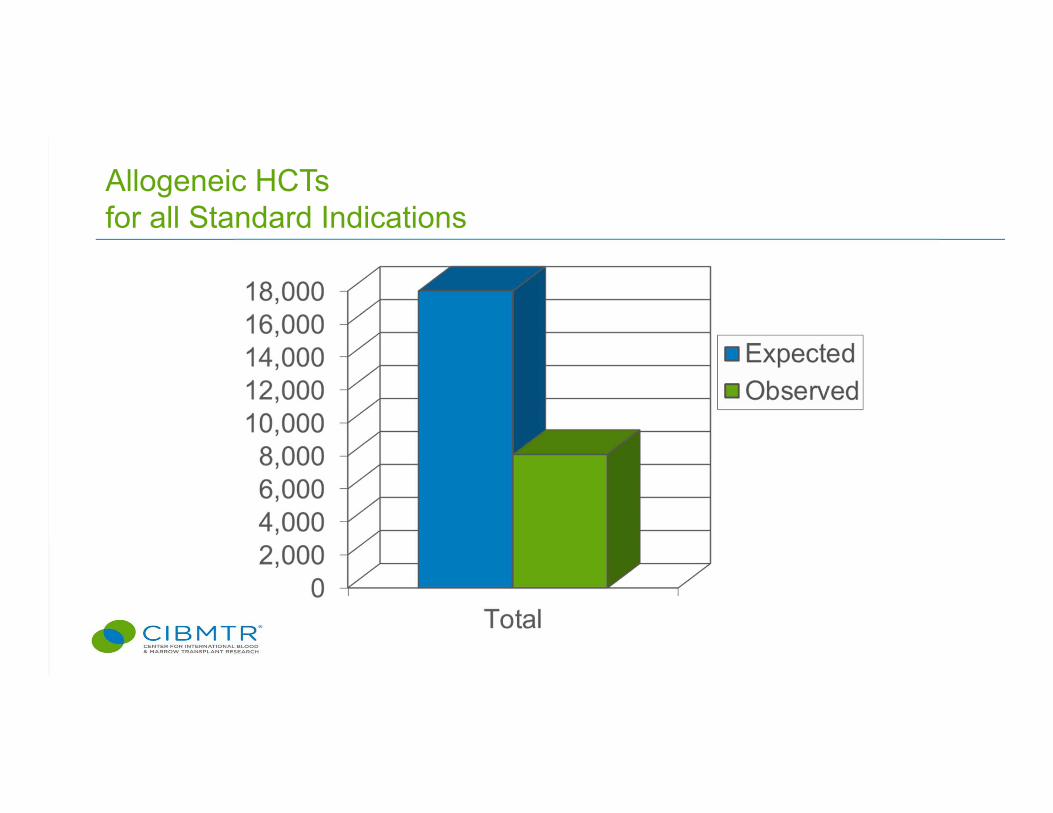
Allogeneic HCTs for all Standard Indications
NMDP View
• Nearly all patients have a donor• Biggest barriers are access, disease state and co-
morbidity• Outcomes can continue to improve with all cell sources• More studies needed to sort out best alternative
transplant therapy based on diagnosis, age, TC experience and interest, etc.
Operated by the National Marrow Donor Program®
NMDP/CIBMTR Approach
• Promote studies through the BMT CTN and RCIBMT• Focus on recruiting young, diverse, committed donors• Encourage collection of large CBUs• Provide donor management and collection services for
related transplants• Extend need-based free HLA testing of related donors
Operated by the National Marrow Donor Program®
Thank you!
Questions?
Operated by the National Marrow Donor Program®
Related Documents











