Trends in Abdominal Obesity Among US Children and Adolescents WHAT’S KNOWN ON THIS SUBJECT: Previous studies showed that prevalence of abdominal obesity among US children and adolescents increased significantly between 1988–1994 and 2003– 2004. However, little is known about recent time trends in abdominal obesity since 2003–2004. WHAT THIS STUDY ADDS: In 2011–2012, 17.95% of children and adolescents aged 2 to 18 years were abdominally obese defined by waist circumference. The prevalence of abdominal obesity leveled off among US children and adolescents from 2003–2004 to 2011–2012. abstract OBJECTIVES: Previous studies showed that prevalence of abdominal obesity among US children and adolescents increased significantly between 1988–1994 and 2003–2004. However, little is known about recent time trends in abdominal obesity since 2003–2004.This study was to provide recent updated national estimates of childhood abdom- inal obesity and examine the trends in childhood abdominal obesity from 2003 to 2012. METHODS: Data were from the National Health and Nutrition Examina- tion Survey (NHANES) conducted during 5 time periods (2003–2004, 2005–2006, 2007–2008, 2009–2010, and 2011–2012). A total of 16 601 US children and adolescents aged 2 to 18 years were included. Abdom- inal obesity is defined as a waist circumference (WC) $ gender- and age-specific 90th percentile based on data from NHANES III (1988–1994) and a waist-to-height (WHtR) $0.5, respectively. RESULTS: In 2011–2012, 17.95% of children and adolescents aged 2 to 18 years were abdominally obese defined by WC, and 32.93% of those aged 6 to 18 years were abdominally obese defined by WHtR. Mean WC and WHtR and prevalence of abdominal obesity kept stable between 2003–2004 and 2011–2012, independently of gender, age, and race/ ethnicity. However, there was a significant decrease in abdominal obesity among children aged 2 to 5 years. CONCLUSIONS: The prevalence of abdominal obesity leveled off among US children and adolescents from 2003–2004 to 2011–2012. Pediatrics 2014;134:e334–e339 AUTHORS: Bo Xi, MD, a Jie Mi, MD, b Min Zhao, MD, c Tao Zhang, MD, a Cunxian Jia, MD, a Jiajia Li, MD, d Tao Zeng, MD, e and Lyn M. Steffen, PhD, f on behalf of Public Health Youth Collaborative and Innovative Study Group of Shandong University (PHYCISG-SDU) a Departments of Epidemiology and Health Statistics, c Nutrition and Food Hygiene, d Social Medicine and Health Service Management, and e Toxicology, School of Public Health, Shandong University, Jinan, China; b Department of Epidemiology, Capital Institute of Pediatrics, Beijing, China; and f Division of Epidemiology and Community Health, School of Public Health, University of Minnesota, Minneapolis, Minnesota KEY WORDS abdominal obesity, waist circumference, waist-to-height ratio, children ABBREVIATIONS CI—confidence interval CVD—cardiovascular disease NHANES—National Health and Nutrition Examination Survey OR—odds ratio WC—waist circumference WHtR—waist-to-height ratio Drs Xi, Mi and Steffen conceptualized and designed the study and drafted the initial manuscript; Drs Zhao and Zhang carried out the initial analyses and reviewed and revised the manuscript; Drs Jia, Li, and Zeng designed the data collection instruments, coordinated data collection, and critically reviewed the manuscript; and all authors approved the final manuscript as submitted and agree to be accountable for all aspects of the work. www.pediatrics.org/cgi/doi/10.1542/peds.2014-0970 doi:10.1542/peds.2014-0970 Accepted for publication May 20, 2014 Jie Mi, MD, Department of Epidemiology, Capital Institute of Pediatrics, 2 Ya Bao Road, Beijing, 100020 China. E-mail: [email protected] PEDIATRICS (ISSN Numbers: Print, 0031-4005; Online, 1098-4275). Copyright © 2014 by the American Academy of Pediatrics FINANCIAL DISCLOSURE: The authors have indicated they have no financial relationships relevant to this article to disclose. FUNDING: This study was supported by the Scientific Research Organization Construction Project of Shandong University (grant 21320074615021). POTENTIAL CONFLICT OF INTEREST: The authors have indicated they have no potential conflicts of interest to disclose. e334 XI et al at Tulane Univ on March 23, 2015 pediatrics.aappublications.org Downloaded from

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

Trends in Abdominal Obesity Among US Children andAdolescents
WHAT’S KNOWN ON THIS SUBJECT: Previous studies showed thatprevalence of abdominal obesity among US children andadolescents increased significantly between 1988–1994 and 2003–2004. However, little is known about recent time trends inabdominal obesity since 2003–2004.
WHAT THIS STUDY ADDS: In 2011–2012, 17.95% of children andadolescents aged 2 to 18 years were abdominally obese definedby waist circumference. The prevalence of abdominal obesityleveled off among US children and adolescents from 2003–2004 to2011–2012.
abstractOBJECTIVES: Previous studies showed that prevalence of abdominalobesity among US children and adolescents increased significantlybetween 1988–1994 and 2003–2004. However, little is known aboutrecent time trends in abdominal obesity since 2003–2004.This studywas to provide recent updated national estimates of childhood abdom-inal obesity and examine the trends in childhood abdominal obesityfrom 2003 to 2012.
METHODS: Data were from the National Health and Nutrition Examina-tion Survey (NHANES) conducted during 5 time periods (2003–2004,2005–2006, 2007–2008, 2009–2010, and 2011–2012). A total of 16 601US children and adolescents aged 2 to 18 years were included. Abdom-inal obesity is defined as a waist circumference (WC) $ gender- andage-specific 90th percentile based on data from NHANES III (1988–1994)and a waist-to-height (WHtR) $0.5, respectively.
RESULTS: In 2011–2012, 17.95% of children and adolescents aged 2 to18 years were abdominally obese defined by WC, and 32.93% of thoseaged 6 to 18 years were abdominally obese defined by WHtR. Mean WCand WHtR and prevalence of abdominal obesity kept stable between2003–2004 and 2011–2012, independently of gender, age, and race/ethnicity. However, there was a significant decrease in abdominalobesity among children aged 2 to 5 years.
CONCLUSIONS: The prevalence of abdominal obesity leveled off amongUS children and adolescents from 2003–2004 to 2011–2012. Pediatrics2014;134:e334–e339
AUTHORS: Bo Xi, MD,a Jie Mi, MD,b Min Zhao, MD,c TaoZhang, MD,a Cunxian Jia, MD,a Jiajia Li, MD,d Tao Zeng, MD,e
and Lyn M. Steffen, PhD,f on behalf of Public Health YouthCollaborative and Innovative Study Group of ShandongUniversity (PHYCISG-SDU)aDepartments of Epidemiology and Health Statistics, cNutritionand Food Hygiene, dSocial Medicine and Health ServiceManagement, and eToxicology, School of Public Health, ShandongUniversity, Jinan, China; bDepartment of Epidemiology, CapitalInstitute of Pediatrics, Beijing, China; and fDivision ofEpidemiology and Community Health, School of Public Health,University of Minnesota, Minneapolis, Minnesota
KEY WORDSabdominal obesity, waist circumference, waist-to-height ratio,children
ABBREVIATIONSCI—confidence intervalCVD—cardiovascular diseaseNHANES—National Health and Nutrition Examination SurveyOR—odds ratioWC—waist circumferenceWHtR—waist-to-height ratio
Drs Xi, Mi and Steffen conceptualized and designed the studyand drafted the initial manuscript; Drs Zhao and Zhang carriedout the initial analyses and reviewed and revised themanuscript; Drs Jia, Li, and Zeng designed the data collectioninstruments, coordinated data collection, and critically reviewedthe manuscript; and all authors approved the final manuscriptas submitted and agree to be accountable for all aspects of thework.
www.pediatrics.org/cgi/doi/10.1542/peds.2014-0970
doi:10.1542/peds.2014-0970
Accepted for publication May 20, 2014
Jie Mi, MD, Department of Epidemiology, Capital Institute ofPediatrics, 2 Ya Bao Road, Beijing, 100020 China. E-mail:[email protected]
PEDIATRICS (ISSN Numbers: Print, 0031-4005; Online, 1098-4275).
Copyright © 2014 by the American Academy of Pediatrics
FINANCIAL DISCLOSURE: The authors have indicated they haveno financial relationships relevant to this article to disclose.
FUNDING: This study was supported by the Scientific ResearchOrganization Construction Project of Shandong University (grant21320074615021).
POTENTIAL CONFLICT OF INTEREST: The authors have indicatedthey have no potential conflicts of interest to disclose.
e334 XI et al at Tulane Univ on March 23, 2015pediatrics.aappublications.orgDownloaded from

Childhood obesity is a serious publichealth problem worldwide, includingin the United States.1 BMI is the mostwidely recognized surrogate of obesity,but it does not provide informationabout the distribution of body fat.2 An-thropometric measures such as waistcircumference (WC) and waist-to-heightratio (WHtR), used for defining abdominalobesity, are better than BMI for predictingrisk for hypertension, type 2 diabetes,metabolic syndrome, cardiovascular dis-ease (CVD), and all-cause mortality.3,4 Im-portantly, the US National Institutes ofHealth recommends screening of WC forhealth risk, especially in overweight orobese adults (BMI$25.0 kg/m2).5
To prevent and control an epidemic ofobesity, it is necessary to monitor sec-ular trends in obesity through pop-ulation surveillance. Abdominal obesityamong US children and adolescents in-creaseddramatically from1988–1994 to1999–2004 according to the NationalHealth and Nutrition Examination Sur-vey (NHANES) III and the continuousNHANES 1999–2004.6 However, it is un-clear whether abdominal obesity hascontinued to increase since 2004.
Using the most recent national datafrom NHANES since 2004, we examinedthe secular trends of WC, WHtR, andabdominal obesity among children andadolescents aged 2 to 18 years in theUnited States.
METHODS
Design and Subjects
The NHANES population is a complex,multistage probability sample of UScivilian, non-institutionalized adultsand children; details have been de-scribed elsewhere.1 The NHANES since1999 has been conducted annually bythe National Center for Health Statis-tics of the Centers for Disease Controland Prevention. A questionnaire wasadministered during the home in-terview, and physical measurementsincluding weight, height, and WC were
measured at the mobile examinationcenter. Written informed consent wasobtained from parents and/or childrenaged 2 to 18 years. The NHANES wasapproved by the National Center forHealth Statistics Ethics Review Board.
Measurements and Definitions
Height, weight, and WC were obtainedusing standardized protocols and cali-brated equipment.1,6 Height was mea-sured to the nearest 0.1 cm withoutshoes using a portable stadiometer.1
WC was measured by using a steelmeasuring tape to the nearest 0.1 cm atthe high point of the iliac crest at mini-mal respiration when the participantwas in a standing position.6 Abdominalobesity is defined as WC equal to orabove the gender- and age-specific 90thpercentile based on data from NHANES III(1988–1994).7 In addition, a WHtR $0.5defined abdominal obesity for youth aged6 to 18 years, because this cutoff mayoverestimate the prevalence of abdomi-nal obesity in children aged 2 to 5 years.8
Statistical Analysis
Differences in distributions of gender,age, and race/ethnicity between 5 cyclesurveys were tested by using a x2 test.Time trends in mean WC and WHtR andprevalence of abdominal obesity from2003–2004 to 2011–2012 were exam-ined by usingmultiple linear regression
or logistical regression model, respec-tively, with consideration of age, gender,and race/ethnicity, when applicable.Multiple logistical regression analysiswas also used to assess the effect ofsurvey years, age, gender, and race/ethnicity on risk for abdominal obesity.P , .05 was considered statisticallysignificant. Statistical analysis wasperformed by using SPSS version 13.0(SPSS, Inc, Chicago, IL).
RESULTS
Characteristics of the StudyPopulation
Table 1 shows the characteristics ofstudy population between 5 surveyperiods (2003–2004, 2005–2006, 2007–2008, 2009–2010, and 2011–2012). Thedistribution of gender was homoge-neous between 5 periods (P. .05) butthere were significant differences inthe proportions of age- and race/ethnicgroups (both P , .001).
Trends in Mean WC and WHtRAmong US Children andAdolescents
Mean WC and WHtR remained stableamong US children and adolescents from2003–2004 to 2011–2012 for each surveyand by age, gender, and race/ethnicgroup, except for non-Hispanic blacks,whose WCmarginally increased (Table 2).
TABLE 1 Characteristics of US Children and Adolescents Aged 2 to 18 Years, NHANES 2003–2004 to2011–2012
2003–2004 2005–2006 2007–2008 2009–2010 2011–2012 P value
All, n 3595 3849 3005 3104 3048Age group, %2 to 5 y 21.6 23.5 27.1 26.7 26.2 0.436 to 11 y 26.5 28.5 39.0 37.5 40.512 to 18 y 51.8 48.0 33.9 35.8 33.4
Gender, %Boys 50.3 50.1 52.1 51.6 51.0 ,0.001Girls 49.7 49.9 47.9 48.4 49.0
Race/ethnicity, %Non-Hispanic white 27.3 26.6 31.7 33.1 21.8 ,0.001Non-Hispanic black 34.7 31.0 25.2 19.6 30.0Mexican American 29.7 33.3 25.6 28.3 19.5Other race 8.2 9.2 17.5 19.1 28.7
ARTICLE
PEDIATRICS Volume 134, Number 2, August 2014 e335 at Tulane Univ on March 23, 2015pediatrics.aappublications.orgDownloaded from

Trends in Prevalence of AbdominalObesity Among US Children andAdolescents
In 2011–2012, 17.95% of children andadolescents aged 2 to 18 years wereabdominally obese (defined by WC);32.93% of those aged 6 to 18 years wereabdominally obese (defined by WHtR).Compared with 2003–2004, the preva-lence of abdominal obesity in 2011–2012, as defined byWC andWHtR, did notchange in the total population or by age,gender, and race/ethnic group, exceptfor children aged 2 to 5 years (Table 3).
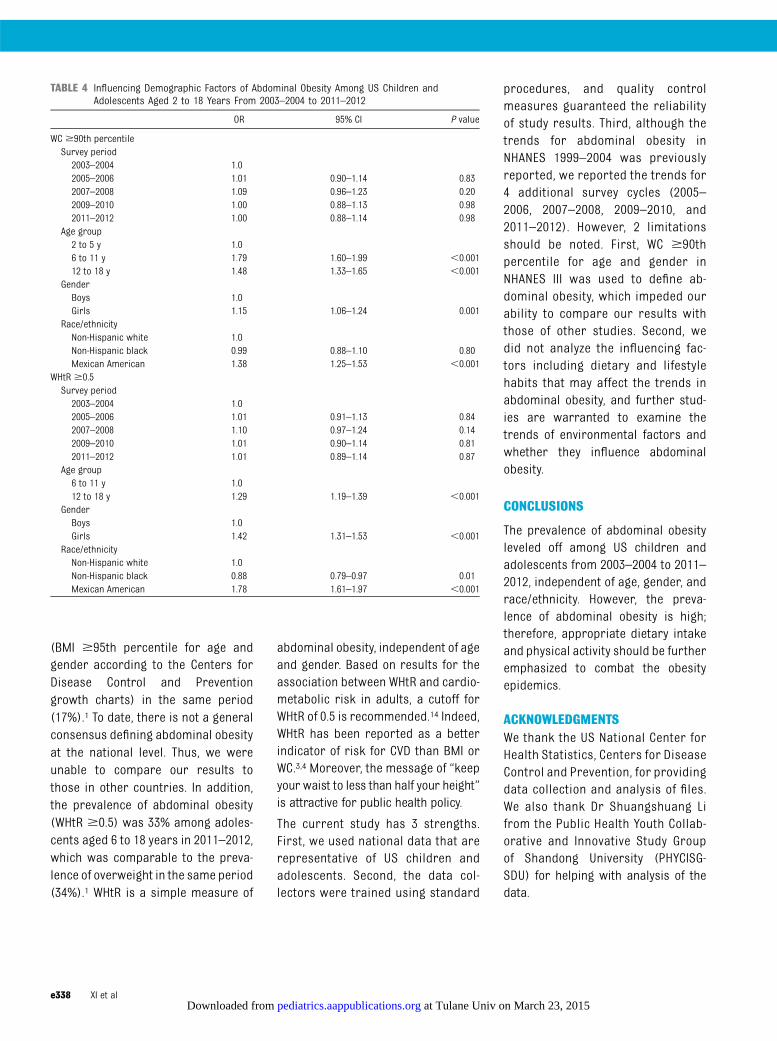
Influence of Demographic Factorson Abdominal Obesity Among USChildren and Adolescents
As shown in Table 4, compared withchildren aged 2 to 5 years, those aged
6 to 11 years (odds ratio [OR], 1.79; 95%confidence interval [CI], 1.60–1.99) and12 to 18 years (OR, 1.48; 95% CI, 1.33–1.65) were more likely to be abdomi-nally obese defined by WC. In addition,girls (boys as referent: OR, 1.15; 95% CI,1.06–1.24) andMexican American (non-Hispanic white as referent: OR, 1.38;95% CI, 1.25–1.53) were more likely tohave abdominal obesity. Similar resultswere found when using WHtR $0.5 todefine abdominal obesity (Table 4).
DISCUSSION
In the current study, trends in meanWC and WHtR and the prevalence ofabdominal obesity remained stableamong US children and adolescentsfrom 2003–2004 to 2011–2012, whichis consistent with the level trends in
obesity (defined by BMI) from 2003–2004 to 2011–2012 in this young pop-ulation.1 Our findings have importantpublic health implications, because ab-dominal obesity is a better indicator ofmany chronic diseases such as hyper-tension, diabetes, CVD, and death thangeneral obesity. Although the preva-lence of abdominal obesity leveled offover the past nine years among USchildren and adolescents, it is stillhigh, being nearly 18% (defined by WC)in participants aged 2 to 18 years and33% (defined by WHtR) in those aged 6to 18 years, suggesting an urgent needfor lifestyle modifications to lowerabdominal obesity.
The stable trends in mean WC andWHtR and prevalence of abdominalobesity were consistent in each age,
TABLE 2 Trends in Mean WC (SE) and WHtR (SE) Among US Children and Adolescents Aged 2 to 18 Years, NHANES 2003–2004 to 2011–2012
2003–2004 2005–2006 2007–2008 2009–2010 2011–2012 AbsoluteIncrease
P forTrend
Mean SE Mean SE Mean SE Mean SE Mean SE
WC, cmAll 68.15 0.19 68.15 0.18 68.25 0.21 68.22 0.21 68.43 0.21 0.28 0.33Age group2 to 5 y 51.58 0.17 51.07 0.16 51.17 0.17 51.26 0.16 51.05 0.17 20.53 0.136 to 11 y 65.73 0.35 64.82 0.33 64.93 0.31 64.72 0.32 65.48 0.31 20.25 0.7112 to 18 y 80.42 0.33 81.21 0.33 81.22 0.45 81.32 0.43 81.18 0.45 0.76 0.13
GenderBoys 68.13 0.27 67.98 0.26 68.26 0.29 68.14 0.29 68.62 0.29 0.49 0.21Girls 68.18 0.27 68.32 0.26 68.25 0.30 68.30 0.29 68.22 0.30 0.04 0.94
Race/ethnicityNon-Hispanic
white68.45 0.35 67.57 0.34 68.31 0.35 67.57 0.34 68.65 0.42 0.20 0.98
Non-Hispanicblack
67.94 0.35 67.48 0.36 67.91 0.45 68.96 0.50 68.64 0.41 0.70 0.04
Mexican American 69.10 0.36 70.48 0.33 69.59 0.42 69.60 0.39 70.16 0.48 1.06 0.82WHtRAll 0.492 0.001 0.493 0.001 0.493 0.001 0.492 0.001 0.493 0.001 0.001 0.13Age group2 to 5 y 0.509 0.001 0.506 0.001 0.507 0.001 0.508 0.001 0.505 0.001 20.004 0.146 to 11 y 0.486 0.002 0.481 0.002 0.483 0.002 0.480 0.002 0.485 0.002 20.001 0.9212 to 18 y 0.488 0.002 0.494 0.002 0.494 0.003 0.493 0.002 0.494 0.003 0.006 0.05
GenderBoys 0.485 0.002 0.485 0.002 0.487 0.002 0.486 0.002 0.487 0.002 0.002 0.42Girls 0.500 0.002 0.502 0.002 0.499 0.002 0.499 0.002 0.499 0.002 20.001 0.42
Race/ethnicityNon-Hispanic
white0.494 0.002 0.489 0.002 0.493 0.002 0.487 0.002 0.492 0.003 20.002 0.21
Non-Hispanicblack
0.480 0.002 0.479 0.002 0.479 0.003 0.485 0.003 0.484 0.003 0.004 0.10
Mexican American 0.505 0.002 0.514 0.002 0.509 0.003 0.508 0.002 0.509 0.003 0.004 0.76
Time trends in mean WC and WHtR from 2003–2004 to 2011–2012 were examined by using multiple linear regression model, with adjustment for age, gender, and race/ethnicity, whenapplicable.
e336 XI et al at Tulane Univ on March 23, 2015pediatrics.aappublications.orgDownloaded from
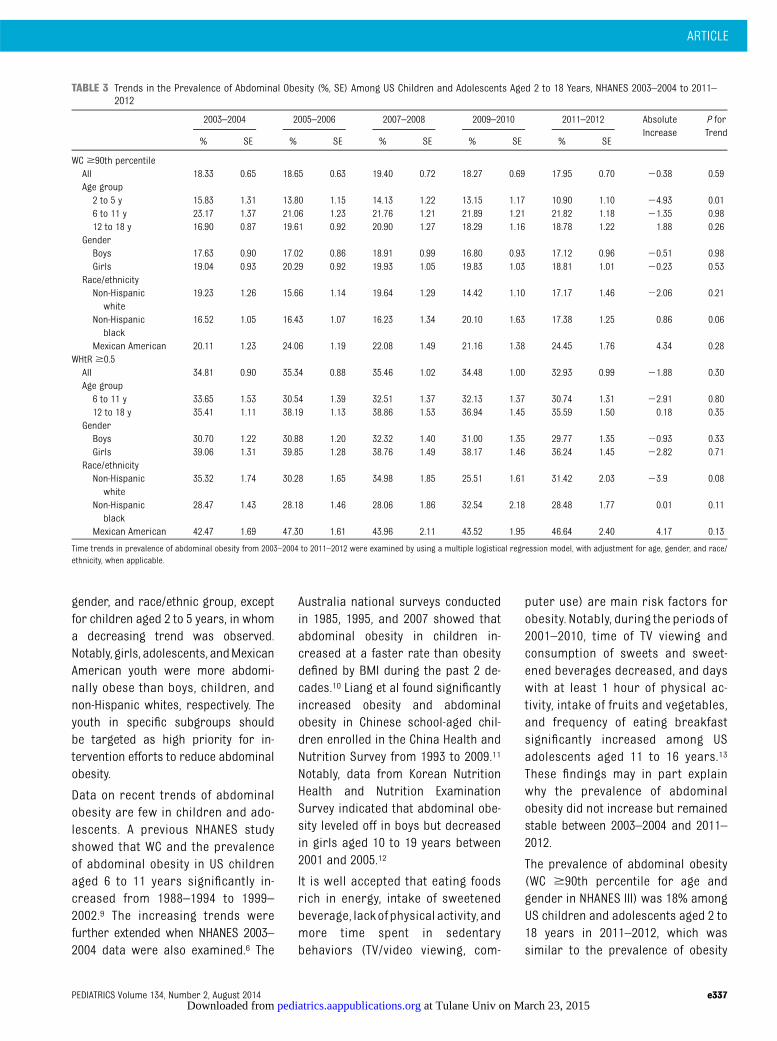
gender, and race/ethnic group, exceptfor children aged 2 to 5 years, in whoma decreasing trend was observed.Notably, girls, adolescents, andMexicanAmerican youth were more abdomi-nally obese than boys, children, andnon-Hispanic whites, respectively. Theyouth in specific subgroups shouldbe targeted as high priority for in-tervention efforts to reduce abdominalobesity.
Data on recent trends of abdominalobesity are few in children and ado-lescents. A previous NHANES studyshowed that WC and the prevalenceof abdominal obesity in US childrenaged 6 to 11 years significantly in-creased from 1988–1994 to 1999–2002.9 The increasing trends werefurther extended when NHANES 2003–2004 data were also examined.6 The
Australia national surveys conductedin 1985, 1995, and 2007 showed thatabdominal obesity in children in-creased at a faster rate than obesitydefined by BMI during the past 2 de-cades.10 Liang et al found significantlyincreased obesity and abdominalobesity in Chinese school-aged chil-dren enrolled in the China Health andNutrition Survey from 1993 to 2009.11
Notably, data from Korean NutritionHealth and Nutrition ExaminationSurvey indicated that abdominal obe-sity leveled off in boys but decreasedin girls aged 10 to 19 years between2001 and 2005.12
It is well accepted that eating foodsrich in energy, intake of sweetenedbeverage, lack of physical activity, andmore time spent in sedentarybehaviors (TV/video viewing, com-
puter use) are main risk factors forobesity. Notably, during the periods of2001–2010, time of TV viewing andconsumption of sweets and sweet-ened beverages decreased, and dayswith at least 1 hour of physical ac-tivity, intake of fruits and vegetables,and frequency of eating breakfastsignificantly increased among USadolescents aged 11 to 16 years.13
These findings may in part explainwhy the prevalence of abdominalobesity did not increase but remainedstable between 2003–2004 and 2011–2012.
The prevalence of abdominal obesity(WC $90th percentile for age andgender in NHANES III) was 18% amongUS children and adolescents aged 2 to18 years in 2011–2012, which wassimilar to the prevalence of obesity
TABLE 3 Trends in the Prevalence of Abdominal Obesity (%, SE) Among US Children and Adolescents Aged 2 to 18 Years, NHANES 2003–2004 to 2011–2012
2003–2004 2005–2006 2007–2008 2009–2010 2011–2012 AbsoluteIncrease
P forTrend
% SE % SE % SE % SE % SE
WC $90th percentileAll 18.33 0.65 18.65 0.63 19.40 0.72 18.27 0.69 17.95 0.70 20.38 0.59Age group2 to 5 y 15.83 1.31 13.80 1.15 14.13 1.22 13.15 1.17 10.90 1.10 24.93 0.016 to 11 y 23.17 1.37 21.06 1.23 21.76 1.21 21.89 1.21 21.82 1.18 21.35 0.9812 to 18 y 16.90 0.87 19.61 0.92 20.90 1.27 18.29 1.16 18.78 1.22 1.88 0.26
GenderBoys 17.63 0.90 17.02 0.86 18.91 0.99 16.80 0.93 17.12 0.96 20.51 0.98Girls 19.04 0.93 20.29 0.92 19.93 1.05 19.83 1.03 18.81 1.01 20.23 0.53
Race/ethnicityNon-Hispanic
white19.23 1.26 15.66 1.14 19.64 1.29 14.42 1.10 17.17 1.46 22.06 0.21
Non-Hispanicblack
16.52 1.05 16.43 1.07 16.23 1.34 20.10 1.63 17.38 1.25 0.86 0.06
Mexican American 20.11 1.23 24.06 1.19 22.08 1.49 21.16 1.38 24.45 1.76 4.34 0.28WHtR $0.5All 34.81 0.90 35.34 0.88 35.46 1.02 34.48 1.00 32.93 0.99 21.88 0.30Age group6 to 11 y 33.65 1.53 30.54 1.39 32.51 1.37 32.13 1.37 30.74 1.31 22.91 0.8012 to 18 y 35.41 1.11 38.19 1.13 38.86 1.53 36.94 1.45 35.59 1.50 0.18 0.35
GenderBoys 30.70 1.22 30.88 1.20 32.32 1.40 31.00 1.35 29.77 1.35 20.93 0.33Girls 39.06 1.31 39.85 1.28 38.76 1.49 38.17 1.46 36.24 1.45 22.82 0.71
Race/ethnicityNon-Hispanic
white35.32 1.74 30.28 1.65 34.98 1.85 25.51 1.61 31.42 2.03 23.9 0.08
Non-Hispanicblack
28.47 1.43 28.18 1.46 28.06 1.86 32.54 2.18 28.48 1.77 0.01 0.11
Mexican American 42.47 1.69 47.30 1.61 43.96 2.11 43.52 1.95 46.64 2.40 4.17 0.13
Time trends in prevalence of abdominal obesity from 2003–2004 to 2011–2012 were examined by using a multiple logistical regression model, with adjustment for age, gender, and race/ethnicity, when applicable.
ARTICLE
PEDIATRICS Volume 134, Number 2, August 2014 e337 at Tulane Univ on March 23, 2015pediatrics.aappublications.orgDownloaded from
(BMI $95th percentile for age andgender according to the Centers forDisease Control and Preventiongrowth charts) in the same period(17%).1 To date, there is not a generalconsensus defining abdominal obesityat the national level. Thus, we wereunable to compare our results tothose in other countries. In addition,the prevalence of abdominal obesity(WHtR $0.5) was 33% among adoles-cents aged 6 to 18 years in 2011–2012,which was comparable to the preva-lence of overweight in the same period(34%).1 WHtR is a simple measure of
abdominal obesity, independent of ageand gender. Based on results for theassociation between WHtR and cardio-metabolic risk in adults, a cutoff forWHtR of 0.5 is recommended.14 Indeed,WHtR has been reported as a betterindicator of risk for CVD than BMI orWC.3,4 Moreover, the message of “keepyour waist to less than half your height”is attractive for public health policy.
The current study has 3 strengths.First, we used national data that arerepresentative of US children andadolescents. Second, the data col-lectors were trained using standard
procedures, and quality controlmeasures guaranteed the reliabilityof study results. Third, although thetrends for abdominal obesity inNHANES 1999–2004 was previouslyreported, we reported the trends for4 additional survey cycles (2005–2006, 2007–2008, 2009–2010, and2011–2012). However, 2 limitationsshould be noted. First, WC $90thpercentile for age and gender inNHANES III was used to define ab-dominal obesity, which impeded ourability to compare our results withthose of other studies. Second, wedid not analyze the influencing fac-tors including dietary and lifestylehabits that may affect the trends inabdominal obesity, and further stud-ies are warranted to examine thetrends of environmental factors andwhether they influence abdominalobesity.
CONCLUSIONS
The prevalence of abdominal obesityleveled off among US children andadolescents from 2003–2004 to 2011–2012, independent of age, gender, andrace/ethnicity. However, the preva-lence of abdominal obesity is high;therefore, appropriate dietary intakeand physical activity should be furtheremphasized to combat the obesityepidemics.
ACKNOWLEDGMENTSWe thank the US National Center forHealth Statistics, Centers for DiseaseControl and Prevention, for providingdata collection and analysis of files.We also thank Dr Shuangshuang Lifrom the Public Health Youth Collab-orative and Innovative Study Groupof Shandong University (PHYCISG-SDU) for helping with analysis of thedata.
TABLE 4 Influencing Demographic Factors of Abdominal Obesity Among US Children andAdolescents Aged 2 to 18 Years From 2003–2004 to 2011–2012
OR 95% CI P value
WC $90th percentileSurvey period2003–2004 1.02005–2006 1.01 0.90–1.14 0.832007–2008 1.09 0.96–1.23 0.202009–2010 1.00 0.88–1.13 0.982011–2012 1.00 0.88–1.14 0.98
Age group2 to 5 y 1.06 to 11 y 1.79 1.60–1.99 ,0.00112 to 18 y 1.48 1.33–1.65 ,0.001
GenderBoys 1.0Girls 1.15 1.06–1.24 0.001
Race/ethnicityNon-Hispanic white 1.0Non-Hispanic black 0.99 0.88–1.10 0.80Mexican American 1.38 1.25–1.53 ,0.001
WHtR $0.5Survey period2003–2004 1.02005–2006 1.01 0.91–1.13 0.842007–2008 1.10 0.97–1.24 0.142009–2010 1.01 0.90–1.14 0.812011–2012 1.01 0.89–1.14 0.87
Age group6 to 11 y 1.012 to 18 y 1.29 1.19–1.39 ,0.001
GenderBoys 1.0Girls 1.42 1.31–1.53 ,0.001
Race/ethnicityNon-Hispanic white 1.0Non-Hispanic black 0.88 0.79–0.97 0.01Mexican American 1.78 1.61–1.97 ,0.001
e338 XI et al at Tulane Univ on March 23, 2015pediatrics.aappublications.orgDownloaded from

REFERENCES
1. Ogden CL, Carroll MD, Kit BK, Flegal KM.Prevalence of childhood and adult obesityin the United States, 2011-2012. JAMA. 2014;311(8):806–814
2. Janssen I, Shields M, Craig CL, TremblayMS. Prevalence and secular changes inabdominal obesity in Canadian adolescentsand adults, 1981 to 2007-2009. Obes Rev.2011;12(6):397–405
3. Czernichow S, Kengne AP, Stamatakis E,Hamer M, Batty GD. Body mass index, waistcircumference and waist-hip ratio: which isthe better discriminator of cardiovasculardisease mortality risk?: evidence from anindividual-participant meta-analysis of 82864 participants from nine cohort studies.Obes Rev. 2011;12(9):680–687
4. Ashwell M, Gunn P, Gibson S. Waist-to-height ratio is a better screening toolthan waist circumference and BMI foradult cardiometabolic risk factors: sys-tematic review and meta-analysis. ObesRev. 2012;13(3):275–286
5. Clinical guidelines on the identification,evaluation, and treatment of overweight
and obesity in adults: executive summary.Expert Panel on the Identification, Evalua-tion, and Treatment of Overweight inAdults. Am J Clin Nutr. 1998;68(4):899–917
6. Li C, Ford ES, Mokdad AH, Cook S. Recenttrends in waist circumference and waist-height ratio among US children and ado-lescents. Pediatrics. 2006;118(5). Availableat: www.pediatrics.org/cgi/content/full/118/5/e1390
7. Fernández JR, Redden DT, Pietrobelli A,Allison DB. Waist circumference percentilesin nationally representative samples ofAfrican-American, European-American, andMexican-American children and adoles-cents. J Pediatr. 2004;145(4):439–444
8. McCarthy HD, Ashwell M. A study of centralfatness using waist-to-height ratios in UKchildren and adolescents over two decadessupports the simple message—‘keep yourwaist circumference to less than half yourheight’. Int J Obes (Lond). 2006;30(6):988–992
9. Okosun IS, Boltri JM, Eriksen MP, HepburnVA. Trends in abdominal obesity in young
people: United States 1988-2002. Ethn Dis.2006;16(2):338–344
10. Garnett SP, Baur LA, Cowell CT. The preva-lence of increased central adiposity inAustralian school children 1985 to 2007.Obes Rev. 2011;12(11):887–896
11. Liang YJ, Xi B, Song AQ, Liu JX, Mi J. Trendsin general and abdominal obesity amongChinese children and adolescents 1993–2009. Pediatr Obes. 2012;7(5):355–364
12. Song Y, Park MJ, Paik HY, Joung H. Seculartrends in dietary patterns and obesity-related risk factors in Korean adolescentsaged 10-19 years. Int J Obes (Lond). 2010;34(1):48–56
13. Iannotti RJ, Wang J. Trends in physical ac-tivity, sedentary behavior, diet, and BMIamong US adolescents, 2001-2009. Pediat-rics. 2013;132(4):606–614
14. Browning LM, Hsieh SD, Ashwell M. A sys-tematic review of waist-to-height ratio asa screening tool for the prediction of car-diovascular disease and diabetes: 0·5 couldbe a suitable global boundary value. NutrRes Rev. 2010;23(2):247–269
ARTICLE
PEDIATRICS Volume 134, Number 2, August 2014 e339 at Tulane Univ on March 23, 2015pediatrics.aappublications.orgDownloaded from

DOI: 10.1542/peds.2014-0970; originally published online July 21, 2014;Pediatrics
SteffenBo Xi, Jie Mi, Min Zhao, Tao Zhang, Cunxian Jia, Jiajia Li, Tao Zeng and Lyn M.
Trends in Abdominal Obesity Among US Children and Adolescents
ServicesUpdated Information &
/peds.2014-0970http://pediatrics.aappublications.org/content/early/2014/07/16including high resolution figures, can be found at:
Supplementary Material
8/peds.2014-0970.DC1.htmlhttp://pediatrics.aappublications.org/content/suppl/2014/10/2Supplementary material can be found at:
Permissions & Licensing
tmlhttp://pediatrics.aappublications.org/site/misc/Permissions.xhtables) or in its entirety can be found online at: Information about reproducing this article in parts (figures,
Reprints http://pediatrics.aappublications.org/site/misc/reprints.xhtml
Information about ordering reprints can be found online:
rights reserved. Print ISSN: 0031-4005. Online ISSN: 1098-4275.Grove Village, Illinois, 60007. Copyright © 2014 by the American Academy of Pediatrics. All and trademarked by the American Academy of Pediatrics, 141 Northwest Point Boulevard, Elkpublication, it has been published continuously since 1948. PEDIATRICS is owned, published, PEDIATRICS is the official journal of the American Academy of Pediatrics. A monthly
at Tulane Univ on March 23, 2015pediatrics.aappublications.orgDownloaded from

DOI: 10.1542/peds.2014-0970; originally published online July 21, 2014;Pediatrics
SteffenBo Xi, Jie Mi, Min Zhao, Tao Zhang, Cunxian Jia, Jiajia Li, Tao Zeng and Lyn M.
Trends in Abdominal Obesity Among US Children and Adolescents
http://pediatrics.aappublications.org/content/early/2014/07/16/peds.2014-0970
located on the World Wide Web at: The online version of this article, along with updated information and services, is
of Pediatrics. All rights reserved. Print ISSN: 0031-4005. Online ISSN: 1098-4275.Boulevard, Elk Grove Village, Illinois, 60007. Copyright © 2014 by the American Academy published, and trademarked by the American Academy of Pediatrics, 141 Northwest Pointpublication, it has been published continuously since 1948. PEDIATRICS is owned, PEDIATRICS is the official journal of the American Academy of Pediatrics. A monthly
at Tulane Univ on March 23, 2015pediatrics.aappublications.orgDownloaded from
Related Documents











