J.biosoc.Sci, (2006) 38, 221–237, 2005 Cambridge University Press doi:10.1017/S0021932005007108 First published online 25 January 2005 TREATMENT-SEEKING PRACTICES FOR MALARIA IN PREGNANCY AMONG RURAL WOMEN IN MUKONO DISTRICT, UGANDA ANTHONY K. MBONYE*, STELLA NEEMA† PASCAL MAGNUSSEN‡ *Ministry of Health, Kampala, Uganda, †Makerere University, Kampala, Uganda and ‡Danish Bilharziasis Laboratory, Charlottenlund, Denmark Summary. Understanding treatment-seeking practices for malaria in preg- nancy is necessary in designing effective programmes to address the high malaria morbidity in pregnancy. This study assessed women’s perceptions on malaria in pregnancy, recognition of early signs of pregnancy and of malaria, and the cultural context in which treatment seeking takes place in Mukono District. Focus group discussions (FGD) and key informant interviews were conducted among pregnant women, non-pregnant women, adolescents and men. The results showed that malaria, locally known as omusujja, was perceived as the most common cause of ill health among pregnant women. Although malaria commonly presents with fever, some pregnant women feel hot in the womb with or without signs of fever and this illness, locally known as nabuguma, may lead to progressive weakness and occasionally to miscar- riage and few respondents associated it with malaria. Primigravidae, adoles- cents and men were not considered at risk of omusujja or nabuguma. Similarly anaemia and low birth weight were not associated with malaria; in fact paleness was described as a normal sign of pregnancy. There are cultural and social pressures on married women to get pregnant and this forces them to conceal symptoms like feeling feverishness, backache, nausea, general weak- ness, loss of appetite and vomiting until they are sure these are due to pregnancy. Most women, however, could not differentiate symptoms of malaria from those of early pregnancy. There is a belief that omusujja is a normal sign of pregnancy and this is coupled with a strong cultural practice of using herbs and clays as a first resort to treat pregnancy ailments including malaria. The cultural beliefs and practices regarding delivery of twin and first births, coupled with the high cost of care, prevent women from delivering and using other services at health units. Introduction Pregnant women in sub-Saharan Africa experience mortality mainly from preventable diseases like malaria (WHO, 1991). Malaria in pregnancy is currently recognized as 221

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript
J.biosoc.Sci, (2006) 38, 221–237, � 2005 Cambridge University Pressdoi:10.1017/S0021932005007108 First published online 25 January 2005
TREATMENT-SEEKING PRACTICES FORMALARIA IN PREGNANCY AMONG RURALWOMEN IN MUKONO DISTRICT, UGANDA
ANTHONY K. MBONYE*, STELLA NEEMA† PASCAL MAGNUSSEN‡
*Ministry of Health, Kampala, Uganda, †Makerere University, Kampala, Uganda and‡Danish Bilharziasis Laboratory, Charlottenlund, Denmark
Summary. Understanding treatment-seeking practices for malaria in preg-nancy is necessary in designing effective programmes to address the highmalaria morbidity in pregnancy. This study assessed women’s perceptions onmalaria in pregnancy, recognition of early signs of pregnancy and of malaria,and the cultural context in which treatment seeking takes place in MukonoDistrict. Focus group discussions (FGD) and key informant interviews wereconducted among pregnant women, non-pregnant women, adolescents andmen. The results showed that malaria, locally known as omusujja, wasperceived as the most common cause of ill health among pregnant women.Although malaria commonly presents with fever, some pregnant women feelhot in the womb with or without signs of fever and this illness, locally knownas nabuguma, may lead to progressive weakness and occasionally to miscar-riage and few respondents associated it with malaria. Primigravidae, adoles-cents and men were not considered at risk of omusujja or nabuguma. Similarlyanaemia and low birth weight were not associated with malaria; in factpaleness was described as a normal sign of pregnancy. There are cultural andsocial pressures on married women to get pregnant and this forces them toconceal symptoms like feeling feverishness, backache, nausea, general weak-ness, loss of appetite and vomiting until they are sure these are due topregnancy. Most women, however, could not differentiate symptoms ofmalaria from those of early pregnancy. There is a belief that omusujja is anormal sign of pregnancy and this is coupled with a strong cultural practiceof using herbs and clays as a first resort to treat pregnancy ailments includingmalaria. The cultural beliefs and practices regarding delivery of twin and firstbirths, coupled with the high cost of care, prevent women from delivering andusing other services at health units.
Introduction
Pregnant women in sub-Saharan Africa experience mortality mainly from preventablediseases like malaria (WHO, 1991). Malaria in pregnancy is currently recognized as
221

one of the major contributors to maternal morbidity in malaria-endemic areas (WHO,1993). During pregnancy, especially among primigravidae and secundigravidae,women are at increased risk of malaria parasitaemia and consequently anaemia andlow birth weight (McCorwick, 1985; Steketee et al., 1996; Bloland et al., 1996;Slutsker et al., 1996).
The clinical presentation of malaria is important for treatment-seeking practices.For example, in endemic areas clinical malaria commonly presents as a febrile illnesswith parasitaemia. The infection can, however, present as an asymptomatic parasi-taemia or severe malaria (anaemia and neurological syndromes) with high mortality(White & Breman, 2001). Some patients with Plasmodium falciparum malaria presentwith non-specific signs and symptoms resulting in misdiagnosis and poor treatment(Nathwani et al., 1992).
In Uganda, where most areas are malaria endemic and pregnant women presentwith asymptomatic parasitaemia and laboratory services are inadequate, intermittentpreventive treatment (IPT) is the most appropriate public health intervention.Accordingly, Uganda’s policy recommends two doses of sulfadoxine-pyrimethamineto be given during the second and third trimester of pregnancy to women of allparities attending antenatal care at health units (Ministry of Health, 2001).
Despite the available evidence on the epidemiology of malaria in pregnancy andtools for treatment and prevention, few studies have documented treatment-seekingpractices among pregnant women (Kengeya-Kayondo et al., 1994; Ndyomugyenyiet al., 1999). One study conducted in Masaka, Uganda, reported that fever locallyknown as omusujja posed a threat to adults and children. Omusujja was believed tocause miscarriages, vomiting, general weakness, a lot of heat in the stomach andfeeling cold in the body (Kengeya-Kayondo et al., 1994). Other studies (Agyepong,1992; Mwenesi, 1995; Ruebush et al., 1995; McCombie, 1996; Nyamongo, 2001) havedocumented treatment-seeking practices for malaria in adults and in children andshown that multiple treatment options exist. The first option is self-treatment withtablets bought over-the-counter. These studies highlight the importance of people’sperceptions about malaria, its symptoms and available treatment options.
Understanding people’s perceptions on malaria and the factors that influence theseperceptions is central to mounting successful malaria prevention interventions (Ahorluet al., 1997). In fact, people in different societies hold a variety of beliefs about thecause and transmission of malaria that vary according to cultural, educational andsocial economic factors with direct consequences for both preventive and treatment-seeking behaviour. Health treatment-seeking behaviour has been found to beinfluenced by other factors like access and attitudes to health workers (Heggenhougenet al., 2003). Attention to these factors is critical to public health for three reasons.First, beliefs that differ from scientific explanations about the cause and transmissionof malaria may lead to inaction. Secondly, people hold various views, oftencontradictory, about malaria at the same time; and thirdly, fevers and symptoms likeconvulsions may not be associated with malaria and this could have severeconsequences (Heggenhougen et al., 2003).
Research on treatment seeking for malaria in pregnancy is important in findingways of promoting timely and effective treatment for malaria. Previous authors haveunderlined the importance of malaria in pregnancy and identified this as a priority
222 A. K. Mbonye, S. Neema and P. Magnussen
area for research if maternal mortality and morbidity is to be reduced (D’Alessandro,1999; Menendez, 1999).
In this study the pattern of treatment seeking for malaria among pregnant womenwas explored and emphasis was placed on pregnant women’s perceptions of malaria,how women differentiate symptoms of malaria from those of pregnancy, and thecultural context in which treatment seeking for malaria takes place. The treatment-seeking pattern for malaria in pregnancy is conceptualized using the Health BeliefModel, developed by Becker (1974). In the model, two main factors influence thelikelihood that a person will adopt a recommended preventive action. First, a personmust feel susceptible and threatened by the disease with perceived serious conse-quences. Secondly, the person must believe that the benefits of practising preventionoutweigh the perceived barriers to the preventive action. In addition, the modelsuggests that health-related evaluations are triggered by environmental cues. Themodel therefore identifies four constructs: perceived susceptibility, perceived severity,perceived benefits and perceived barriers. The selection of this model to analyse thetreatment-seeking pattern for malaria in pregnancy in this study is based on itsprevious use to predict a number of health-related behaviours like engaging in exercise(Langie, 1977), child vaccination (Bennet & Smith, 1992) and compliance withrecommended medical regimens (Bradley & Kegeles, 1987). In addition, the modelconstructs have been found to have a high correlation with health-related behaviours(Janz & Becker, 1984).
Methods
The study was conducted in Mukono District in central Uganda where 88% of thepopulation is rural consisting of peasants who depend on subsistence agriculture forfood and as a source of income. The district is bordered by Lake Victoria and peopleliving on the lake shores engage mainly in fishing activities. The district is mainlyinhabited by Baganda people, the largest tribe in Uganda, and other small immigranttribes of Basoga, Badama, Bagisu, Basamya, Banyarwanda, Jaluos, Lugbar andBalulu. This district was specifically selected for the study because most areas arehyper-endemic for malaria while those areas near the shores of Lake Victoria areholo-endemic.
Data collection took place from November 2002 to January 2003 after the rainyseason when the population was experiencing intense malaria transmission.
The study design was exploratory using qualitative methods including focus groupdiscussions (FGD) and key informant interviews (KII). The following thematic areaswere explored: perceptions on malaria in pregnancy, recognition of symptoms ofmalaria and perceptions on seriousness of malaria in pregnancy, cultural aspectsinfluencing treatment and prevention of malaria in pregnancy and treatment-seekingpractices for malaria in pregnancy.
Study participants were selected from five sub-counties of the district taking intoconsideration age, education, socioeconomic status and marital status. Focus groupdiscussions were held separately with pregnant and non-pregnant women aged 20–49years, adolescent girls (both out of school and those in school) aged 10–19 years andmen aged 20–50 years. All respondents spoke the local dialect fluently. Key informant
Treatment-seeking practices for malaria 223
interviews targeted opinion leaders (e.g. local council officials, elderly midwives,retired women teachers, owners of drug shops), traditional birth attendants (TBAs)and pregnant and non-pregnant women. A total of 40 KIIs and 10 FGDs wereconducted in which 90 respondents participated. Fifteen of them were adolescents, 36were women and 39 were men. Most participants were married except for adolescents.Most respondents had attained primary education while few had secondary education.Sixty-three per cent of the respondents were engaged in peasant agriculture and 16%were engaged in petty trade.
Tape-recorded FGDs were transcribed in Luganda by two research assistants.Later the transcripts were translated into English. To avoid loss of data, duringanalysis frequent comparisons were made between the transcripts in Luganda and theEnglish version and relevant sections of tapes listened to in order to get appropriatequotes.
Data were initially coded separately for the Luganda and the English versions ofthe transcripts and thematic areas obtained. Data were manually analysed andpresented along these themes. The FGDs with different groups were analysed alongthe major themes on which data were collected and analysis followed the fourconstructs of the Health Belief Model (Becker, 1974). Quotes that best explain thecontext of malaria in pregnancy along these constructs were identified and arepresented here. Because there were no major differences noted among responses fromthe FGDs and KIIs, the data are presented together.
It was necessary to validate data obtained from FGDs using KIIs since both toolswere exploring the same thematic areas. Where possible data were compared withdata from other studies, especially the Uganda Demographic and Health survey(Uganda Bureau of Statistics, 2001), which contains the most recent data on healthand disease.
Results
Local perceptions on malaria in pregnancy
Data were obtained on perceptions about malaria in pregnancy and commonhealth problems experienced by pregnant women. Respondents were asked whatcommon illnesses pregnant women experience. The local terms for illnesses wereelicited spontaneously and recorded during the interviews. Omusujja, the local termfor any febrile illness, was cited as the most common illness among pregnant women.This was followed by kabotongo, a local term for syphilis. Cough, lack of blood(anaemia), common cold, backache, diarrhoea, joint pains, dizziness, swelling of legsand general weakness were mentioned in that order. Most respondents stated thatamong the sexually transmitted diseases, locally known as endwadde z’ubukaba,kabotongo (syphilis) was the most common. Respondents said that it is hard to finda woman who visits a clinic without complaining of kabotongo. Other sexuallytransmitted diseases mentioned but which were uncommon included vaginal itchingand gonorrhoea. HIV/AIDS, locally known as silimu, was mentioned in two FGDs atNajjembe and Buikwe sub-counties and the respondents said that pregnant women getworse when they get HIV/AIDS.
224 A. K. Mbonye, S. Neema and P. Magnussen
Respondents were asked to name other common illnesses and health problemsaffecting pregnant women. Most respondents mentioned ‘lack of blood’ (anaemia).However, this was attributed to poor nutrition and few respondents associated thiscondition with malaria. Poor nutrition was cited in all FGDs as a big problem forpregnant women because they thought that they needed to eat more frequently in asituation where food is not easily available. Poor nutrition was linked to thecarelessness of husbands who do not buy food for their wives but prefer to spend themoney on alcohol.
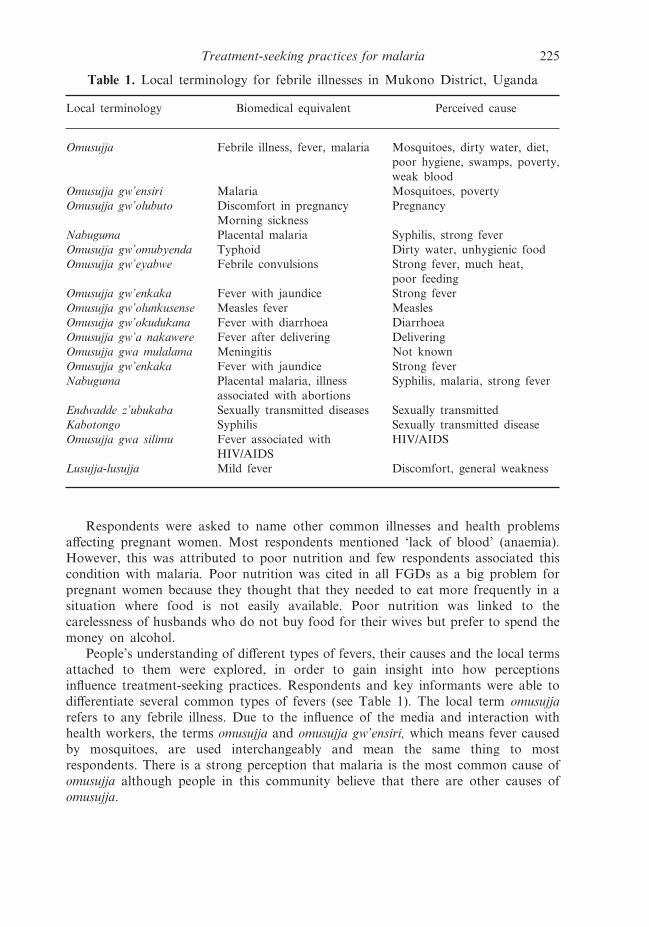
People’s understanding of different types of fevers, their causes and the local termsattached to them were explored, in order to gain insight into how perceptionsinfluence treatment-seeking practices. Respondents and key informants were able todifferentiate several common types of fevers (see Table 1). The local term omusujjarefers to any febrile illness. Due to the influence of the media and interaction withhealth workers, the terms omusujja and omusujja gw’ensiri, which means fever causedby mosquitoes, are used interchangeably and mean the same thing to mostrespondents. There is a strong perception that malaria is the most common cause ofomusujja although people in this community believe that there are other causes ofomusujja.
Table 1. Local terminology for febrile illnesses in Mukono District, Uganda
Local terminology Biomedical equivalent Perceived cause
Omusujja Febrile illness, fever, malaria Mosquitoes, dirty water, diet,poor hygiene, swamps, poverty,weak blood
Omusujja gw’ensiri Malaria Mosquitoes, povertyOmusujja gw’olubuto Discomfort in pregnancy Pregnancy
Morning sicknessNabuguma Placental malaria Syphilis, strong feverOmusujja gw’omubyenda Typhoid Dirty water, unhygienic foodOmusujja gw’eyabwe Febrile convulsions Strong fever, much heat,
poor feedingOmusujja gw’enkaka Fever with jaundice Strong feverOmusujja gw’olunkusense Measles fever MeaslesOmusujja gw’okudukana Fever with diarrhoea DiarrhoeaOmusujja gw’a nakawere Fever after delivering DeliveringOmusujja gwa mulalama Meningitis Not knownOmusujja gw’enkaka Fever with jaundice Strong feverNabuguma Placental malaria, illness
associated with abortionsSyphilis, malaria, strong fever
Endwadde z’ubukaba Sexually transmitted diseases Sexually transmittedKabotongo Syphilis Sexually transmitted diseaseOmusujja gwa silimu Fever associated with
HIV/AIDSHIV/AIDS
Lusujja-lusujja Mild fever Discomfort, general weakness
Treatment-seeking practices for malaria 225
Other types of fevers include omusujja gw’omubyenda, which is fever associatedwith abdominal pain, headache and diarrhoea. The description of this fever isequivalent to what is known as typhoid in biomedical terms. Fever for measles, locallyknown as olunkusense, fever for HIV, locally known as omusujja gwa silimu, andYellow Fever were mentioned. In fact depending on the level of education the termsmalaria, typhoid and measles have been adopted as local terms for fevers.
All female respondents in FGDs said that pregnancy is associated with a ‘feverish’discomfort and this is locally known as omusujja gw’olubuto, which means ‘fever ofpregnancy’. This fever is common and perceived as a normal condition in earlypregnancy but also occasionally experienced in late pregnancy. This fever ischaracterized by feeling weak and loosing appetite with occasional vomiting. This isequivalent to morning sickness in biomedical terms. Another type of illness describedwas nabuguma which respondents associated with abortions. Women who get thiscondition were said to feel hot in the womb with no obvious sign of fever, butprogressively become weak. This illness was not associated with malaria but morewith syphilis.
Respondents were asked which people were most vulnerable to malaria andwhether malaria was considered a serious problem for pregnant women. Respondentsagreed that children and pregnant women were at most risk of malaria. InKimenyedde and Buikwe sub-counties, people described how malaria attacks youngbabies, children and old people. Women respondents said that children and pregnantwomen were at risk of malaria because they eat poorly and have no money to buynutritious foods to keep them healthy. It was narrated how a pregnant woman mayspend a whole day without eating anything yet she carries the burden of pregnancyand in addition she has to carry out her usual household chores.
Pregnant women are especially at risk of mosquito bites and hence malariabecause there is a low usage of bed nets. This was mainly attributed to the chemicalsused to treat nets, which were considered harmful to the pregnant woman, andespecially the fetus. These chemicals were considered to be strong since they could killmosquitoes instantly. The strength that kills mosquitoes was perceived to be harmfulto children. It was also the opinion of many respondents that pregnant women couldnot afford the cost of bed nets. The fear of chemicals and the unaffordability of bednets are summarized in the expressions below:
Pregnant women are at risk of malaria because they do not sleep under mosquito nets. We fearwe may die fast because of the effect of the chemicals put in the nets. (Pregnant woman aged 27years)
Most pregnant women can’t afford mosquito nets, others refuse to use them claiming the nets aretreated with chemicals that may affect their pregnancies. (Adolescent aged 14 years)
Children were also considered a vulnerable group because they do not coverthemselves properly at night and mosquitoes bite them. Similarly, it was noted bymost respondents that children stay outside for long hours playing in bushes andclimbing trees looking for mangos and this behaviour puts them at risk of mosquitobites.
Men were believed not to be at risk of malaria because their blood was believedto be strong so when they have malaria they do not become as weak as women and
226 A. K. Mbonye, S. Neema and P. Magnussen

children. Pregnant women were thought to be weak because they do not have enoughblood since this is shared with the fetus in the womb. In addition to the poor dietearlier mentioned, this was considered another cause of lack of blood among pregnantwomen. Surprisingly, adolescent girls did not consider themselves at risk of malariaeven when pregnant and this was supported by adult respondents who also did notconsider adolescents and primigravidae to be at special risk for malaria in pregnancy.In this study primigravidae were not considered at special risk compared with otherpregnant women. This is because the effects of severe anaemia and low birth weightexperienced by primigravidae are not well understood and related to malaria inpregnancy in this community.
The adverse effects of malaria in pregnancy
Respondents knew that omusujja gw’ensiri (fever caused by mosquitoes) presentsin two forms. One is a mild type with headache, joint pains, nausea, loss of appetite,low grade fever, feeling lazy, heart palpitations and sour mouth. This condition islocally known as lusujja-lusujja. The severe type of malaria presents with very hightemperature, rigors, shivering, miscarriages, mental confusion, excessive vomiting andeyes turning yellow. Malaria presenting with yellow eyes is locally termed omusujjagw’enkaka. Malaria presenting with convulsions is termed omusujja gw’eyabwe. Severemalaria commonly presents with convulsions in children. The convulsions are locallyknown as okwesika, and considered a danger sign and most people are rushed tohealth units while few people with convulsions are taken to traditional healers. A typeof fever locally known as omusujja gw’a nakawere was associated with women whohad just delivered. This fever was considered normal for women who have justdelivered. This could be dangerous because biomedically fever during the six weeksafter delivery (peuperium) is dangerous and mainly caused by pelvic infections. Thisis one of the leading causes of maternal mortality in Uganda (Mbonye, 2001).
Respondents associated severe malaria with miscarriages although few of themassociated it with stillbirths. Stillbirths were perceived to be commonly caused bykabotongo (syphilis). Similarly, few respondents associated nabuguma with malariainfection because the illness presents commonly with no sign of fever. Wheninformants were asked if they knew that pregnant women may have malaria withoutpresenting any symptoms of fever, backache or vomiting, their response was that thisis not possible. When asked if they have ever heard that pregnant women should betreated for malaria even when they are not sick, most respondents stated that theyhad not heard of this before. They did not think that a person can have malaria andfail to know that he/she is sick. It was therefore apparent that malaria in pregnancy,which often presents as an asymptomatic parasitaemia, was not known by manypeople in this community. However, a few pregnant women shared their experiencesof how they had been pregnant and without any sign of illness, suddenly startedbleeding and subsequently had miscarriages. One woman respondent narrated herexperience as follows:
I went through a bad situation, I was four months pregnant, when I woke up, I was bleeding andI had a miscarriage. I was not sick before and never felt anything like a high temperature orvomiting. (Woman aged 20 years at Najjembe)
Treatment-seeking practices for malaria 227
The study investigated how easy it was to differentiate the signs of malaria fromthose of early pregnancy. Many of the informants drew similarities between symptomsof early pregnancy and mild malaria infection such as vomiting, nausea, loss ofappetite, backache and general weakness. It was noted that the way malaria inpregnancy presents confuses both the pregnant woman and the family. When malariaattacks a pregnant woman, signs like vomiting and general weakness become intenseand the pregnant woman is supposed to notice this change and take action. This iscomplicated by the fact that fever, nauseas and vomiting are signs of early pregnancyand in this community this is known as omusujja gw’olubuto, which means ‘normalfever of pregnancy’, as expressed below:
It depends on the time when the omusujja (fever) comes. Shortly after our marriage my wife feltfeverish and they called it omusujja omulungi (translated as good fever) because this was a signthat my wife had conceived. (Male teacher aged 20 years)
Biomedical explanatory models of malaria in pregnancy show that malaria leadsto abortion, stillbirth, low birth weight and other complications. To test knowledgeon dangers of malaria in pregnancy, respondents were asked if they associated theseconditions with malaria. Most respondents thought the commonest causes ofabortions were omusujja gw’ensiri, nabuguma and kabotongo (syphilis). Respondentsnoted that although abortion was common among adolescents, this was not due tomalaria but a deliberate effort by adolescents to do away with an unwantedpregnancy. No respondents mentioned omusujja (fever) or nabuguma as one of thecauses of abortion among adolescents. This is because in this community the termadolescent refers to young people who are not married. Those who are married arenot regarded as adolescents. Given the understanding of the term adolescent bypeople in this community, it is possible that married adolescents get abortionsassociated with omusujja and nabuguma. This is an area that needs further inquiry.
Most respondents did not associate malaria with low birth weight. They thoughtthat low birth weight was due to a poor diet described as lacking in terms ofnutritious foods like meat, eggs, fish, milk, rice and steamed bananas. Otherrespondents attributed low birth weight to drinking alcohol, while a few othersattributed it to the frequent disease burden experienced by pregnant women, whichincluded syphilis, malaria and HIV in that order (see Table 2). A few respondentsthought that tightening belts while pregnant causes low birth weight because the childdoes not move freely in the womb. The tightening of belts is in this communityassociated with the culture of concealing pregnancies. Tightening belts is thought tosqueeze the fetus and lead to low birth weight. Low birth weight was also attributedto domestic violence. Some husbands were known to beat their wives frequently andthis was thought to lead to psychological torture and poor health of the pregnantwoman. This poor health was believed to be a cause of low birth weight. Domesticviolence was noted in all the FGDs and the key informant interviews conducted inthis community as a serious problem. In addition to this, negligence of husbands wasmentioned as a serious problem to the health of pregnant women.
The commonest causes of anaemia (lack of blood) in pregnancy mentioned werepoor nutrition, followed by frequent diseases and sickness (see Table 2). Fewrespondents linked anaemia to malaria while others thought it was because of not
228 A. K. Mbonye, S. Neema and P. Magnussen
using herb baths during pregnancy. Most respondents knew that a common sign oflack of blood was general body weakness. Even with probing, few respondentsmentioned paleness as a sign of lack of blood. Most respondents thought that beingpale was a normal sign of pregnancy rather than a sign of lack of blood. In adiscussion with pregnant women at Nyenga, this was mentioned as one of thosecommon signs people look for in identifying a pregnancy. The expression belowsummarizes the respondent’s awareness on this topic:
When a pregnant woman’s eyes become whitish and the skin lightens this is recognized as a signof pregnancy. (Female aged 35 years)
In half of the FGDs conducted, premature births were attributed to omusujjagw’ensiri (fever caused by mosquitoes), followed by kabotongo (syphilis) andnabuguma (see Table 2). Few respondents thought that drinking alcohol causedpremature births while some mentioned modern drugs like Fansidar and quinine ascauses of premature births. Premature births were also associated with earthquakes,tremors, domestic violence and thunderstorms.
Culture and malaria in pregnancy
These findings indicate that in this community pregnancy outside marriage isregarded as a sign of promiscuity, degrades the family moral aptitudes and is seen asa shame to the family. This society also attaches great importance and esteem to awoman who gets married and becomes pregnant shortly afterwards. There is strongpressure from the husband, in-laws and the community for a woman to conceive.Therefore, when a woman experiences the first signs of pregnancy like amenorrhoea,nausea and discomfort, she waits until some time passes in order to confirm thatindeed she is pregnant. It is when a woman is sure of the pregnancy that she tells theanxious family. This is an interesting finding that shows that some women may findit difficult to differentiate signs of pregnancy and those of a febrile illness like malaria.Thus they wait until they can confirm to the anxious family and friends that it ispregnancy and not any other disease symptom. The social pressure equally exerted onsex outside marriage, especially among adolescents, drives them into fear when they
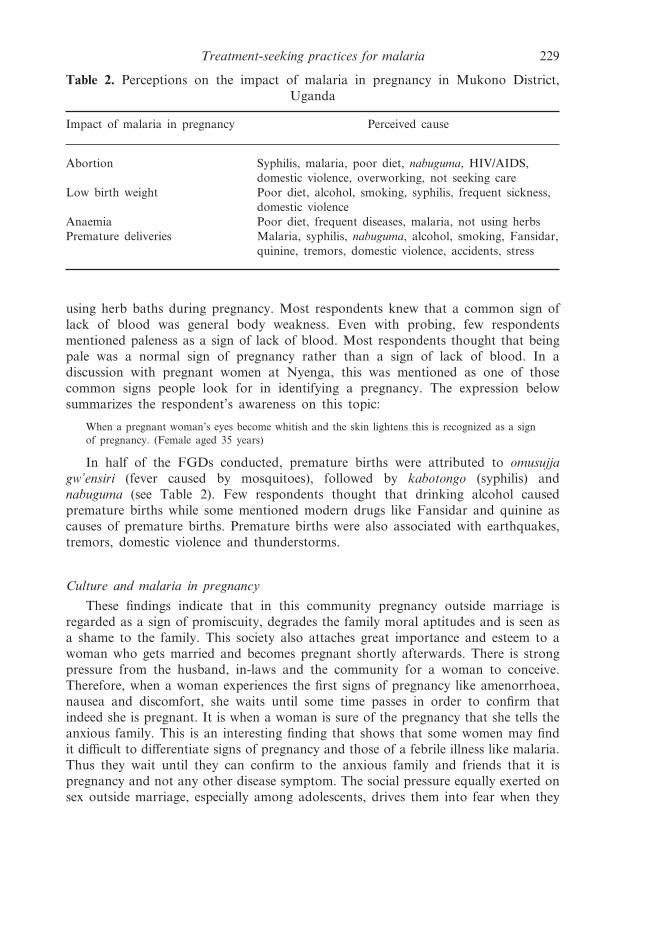
Table 2. Perceptions on the impact of malaria in pregnancy in Mukono District,Uganda
Impact of malaria in pregnancy Perceived cause
Abortion Syphilis, malaria, poor diet, nabuguma, HIV/AIDS,domestic violence, overworking, not seeking care
Low birth weight Poor diet, alcohol, smoking, syphilis, frequent sickness,domestic violence
Anaemia Poor diet, frequent diseases, malaria, not using herbsPremature deliveries Malaria, syphilis, nabuguma, alcohol, smoking, Fansidar,
quinine, tremors, domestic violence, accidents, stress
Treatment-seeking practices for malaria 229

become pregnant and the next immediate action is to seek an abortion by whatevermeans. In discussions with adolescents, they explained how pregnancy causes them alot of problems. They said that most often communicating with their parents isdifficult and some parents chase them away from home. This drives them to doanything to end the pregnancy. It was noted that some adolescents use herbs and avariety of modern drugs, while others may visit witch doctors in search of an abortionrather than seek care at health units.
There is a widespread cultural practice of using herbs and clays during pregnancy.Some people believe that when a woman has a twin pregnancy she is supposed to useherbs exclusively because modern medicines may affect the twins and prevent themfrom coming out of the womb or they may even die. There are rituals performed ontwin deliveries which involve mixing the umbilical cord with herbs. When womendeliver in health units they are not able to perform these rituals and this inhibits themfrom delivering at health units. Similarly, there are some people who believe that afirst-born is not supposed to be delivered in a health unit because in health units theumbilical cord and the placenta are thrown away yet they are supposed to be keptand rituals carried out before they are disposed of. Culturally it is a widespreadpractice for pregnant women to deliver at home rather than a health unit. In thiscommunity, it is common to use herbs to treat omusujja during pregnancy. Thispractice is so deeply rooted that even educated women use herbs believing that theymake pregnant women become stronger and prevent various ailments. Some peoplein this community do not believe that modern drugs can cure malaria, their argumentbeing that a long time ago people used to use herbs and they could cure a variety ofdiseases including malaria.
This study assessed how decisions are made where to seek treatment and whomakes the decisions. Female respondents narrated how husbands were the decision-makers on where to go for treatment. The main reason given was that husbandscontrol financial resources and female respondents felt that men make choices forthem sometimes against their own preferred choice. The following expressionsummarizes the feelings of most women in FGDs:
It is the husbands who decide whether to stay at home or to go to health units, because they arethe ones who have the money. Sometimes you as a woman you may wish to go to a health unitbut this cannot happen. (Female respondent aged 40 years at Kimenyedde)
Respondents emphasized that it should be the woman herself who decides whereto go for treatment, because she is the one who experiences the sickness, yet mostwomen do not have money, so they resort to using herbs. One of the reasons whymen refuse to allow their wives to go to health units was the fear that male healthworkers may make sexual advances to their wives or help them to abort.
Treatment-seeking practices for malaria in pregnancy
Respondents were asked what services they usually get from health units. Womensaid that they visit health units at least once during a pregnancy to check if the babyis healthy, to be checked for diseases like kabotongo, to receive immunization againsttetanus, to be checked for anaemia, and to seek treatment when they are sick. From
230 A. K. Mbonye, S. Neema and P. Magnussen
the discussions it was clear that routine visits for check-ups and treatment for mildailments were not a common practice. Women also said they wanted to get maternitycards because if they did not have one and came to deliver at a health unit they fearedthey would be abused and chased away.
Although most women usually go to the health units at least once to attendantenatal care, few deliver at health units. The commonly cited reasons for notdelivering at health units are the long distance pregnant women have to walk tohealth units, negligence of husbands, the easy accessibility to TBAs, the poor qualityof care at health units and the cultural beliefs and practices earlier mentioned. Seekingcare at health units was associated with cost of transport to and from the health unitsand the cost of food and drinks. At the health units, patients are required to buyitems like gloves, cotton wool and sometimes they are given prescriptions to buydrugs which are not in stock at the health units. All these factors generally lead tolow utilization of services at health units for treatment and prevention services suchas IPT for malaria prevention. In fact in all the FGDs conducted, few women saidthat they had gone to health units for malaria prevention.
The treatment-seeking practices for malaria in pregnancy were explored. In thiscommunity, it was found that omusujja in pregnancy is commonly treated with herbslike omululuza (Vernonia amygdalina) ebombo (Mormodica foetidicia), nalongo (Justicaspecies), omwetango (Chenopodium opulifolium) and emumbwa (a clay rich in oxyto-cics). Other herbs used in pregnancy include namirembe, nakayi, lukaka andakabombo. It was acknowledged that most women including the educated ones use theherbs to treat omusujja and the herbs are believed to be effective, as expressed in thequotes below:
Ha! Do you think all women go to health units? Do you think the women who do not go tohealth units die? Most pregnant women use herbs and feel fine; those who do not feel fine useother forms of treatment. (Female aged 29 years at Ngogwe)
Here in the village most women use emumbwa (clay with oxytocic agents). (Female respondentaged 35 years at Kimenyedde)
It was observed that in some families women are given instructions not to usemodern medicine in combination with local medicines since these local medicines arebelieved to contain everything they need.
It was noted that pregnant women make assessments before they make a choicefor treating an ailment. First choice is to use herbs to see whether the illness willimprove. For a few respondents cost was a key determinant for choice of treatmentof malaria in pregnancy. It was said that the main reason pregnant women resort toherbs is because of the high cost of accessing services at health units. Although mostpregnant women with fever use herbs as a first resort, it is common for some to useboth herbs and tablets purchased over the counter from drug shops, ordinary shopsand private clinics. People purchase drugs for certain ailments and then they keepsome drugs for future disease episodes. Commonly mentioned drugs includedparacetamol and chloroquine. Some women do not take anything and wait to see howthe symptoms develop before a decision is taken (see Table 3).
Respondents argued that although the use of herbs is a long-term practice passedover many generations, with the introduction of medical care, herbs are mainly used
Treatment-seeking practices for malaria 231

by the poor women who cannot afford the costs involved in seeking modern care.When herbs do not bring any relief and the symptoms persist or get worse, the secondchoice of treatment is to purchase drugs from nearby drug shops and clinics. At thispoint, depending on the availability of money, consultations with health workers inprivate clinics and drug shops begin. If care from nearby drug shops and clinics fails,then people switch to health centres and hospitals. Most respondents said thatpatients can be referred from one health unit to another depending on the seriousnessof the disease and the persistence of the symptoms; for instance a patient can bereferred to health units that have laboratory facilities and are able to carry out blood,stool and urine examinations.
This study assessed the sources of information about treatment and it was foundthat pregnant women first seek advice from close friends as these will not reveal thepregnancy to other people and will also advise on treatment choices for the illness.Some pregnant women may first seek advice from their mothers-in-law if a goodrelationship exists between them. A few women, mainly the educated ones, talk totheir husbands as a first resort. Some pregnant women talk to neighbours,grandparents and older experienced women because of their knowledge on herbs andother remedies. A few respondents mentioned that there are some pregnant womenwho first seek advice and care from clinics and health units and this was determinedby their financial status and the level of education. It was also noted that adolescentsprefer to seek care from private clinics and drug shops as they expressed a fear thathealth workers at government health units would not keep secrets about adolescents’illnesses and parents would get to know what their children are suffering from. It wasfurther noted that some women do not seek advice from anybody and keep theirdiscomfort to themselves until they either get relieved or the condition has progressedto a point where it attracts the attention of the husband, family members or friends.
Discussion
This study has given insight into the treatment-seeking pattern for malaria inpregnancy among rural women and the factors influencing this pattern. The majority
Table 3. Treatment practices for malaria in pregnancy in Mukono District, Uganda
Care Current practice
Self-treatmentWith local herbs Most common practiceCombination of herbs and modern drugs Quite common
Purchasing pills from drug shops and clinics(drugs commonly purchased: aspirin,paracetamol and chloroquine)
Second resort for most women when herbsfail; few women do this as first resort
Visiting health units and hospitals (mainlyto seek effective treatment and laboratoryservices to investigate cause of fever)
Last resort for most women who get sick
232 A. K. Mbonye, S. Neema and P. Magnussen
of pregnant women in this rural area who get fever resort to self-treatment with herbsas the first option. They switch to drugs purchased over-the-counter when symptomspersist. This practice leads to a delay in seeking care for malaria in pregnancy athealth units, which are used as a last resort in the treatment hierarchy. In additionto highlighting this pattern, these findings indicate that key factors that determinetreatment seeking for malaria in pregnancy are: the failure to distinguish signs of earlypregnancy and those of malaria like vomiting, backache, nausea, loss of appetite andgeneral weakness; low risk perception for malaria among adolescents, primigravidaeand men; the culture of using herbs in pregnancy with strong beliefs attached totheir effectiveness; cost implications of seeking care at health units, culturalbeliefs and practices associated with delivery of twin and first births and uncaringhusbands.
A recent review on treatment-seeking behaviour for malaria has documented arange of treatment behaviours and associated factors (Heggenhougen et al., 2003). Alarge variation in treatment seeking has been noted with resort to self-treatmentranging from 4% to 87% while exclusive use of traditional healers and herbalmedicines is rare and limited to remote areas (McCombie, 1996). Further to this, ina Kenyan study, it was found that self-treatment was extremely common and 60% offebrile illnesses were treated at home with herbal remedies or medicines purchased atlocal shops (Ruebush et al., 1995). Studies in Kenya and Zambia have also noted thatmost patients start with self-treatment at home as they wait for progression ofsymptoms (Baume et al., 2000; Nyamongo, 2001). A multi-country study also foundthat self-treatment in rural areas was the rule rather that the exception (Foster, 1995).An earlier study conducted in Uganda found a similar pattern where people resortedto herbs first before seeking formal care (Kengeya-Kayondo et al., 1994). In Somalia,a similar pattern of resort was documented (Abyan & Osman, 1993). The presentstudy has not only highlighted the treatment-seeking pattern for malaria in pregnancyamong rural women and shown that herbs are used as a first resort, but furtheridentified factors associated with this pattern, especially the cultural beliefs andpractices.
The finding that malaria is not associated with anaemia and low birth weight isimportant in two ways: first it affects treatment seeking as earlier indicated andsecondly it is important in designing health education messages that could beimportant in malaria prevention by highlighting the dangers of malaria, especially inpregnancy. ‘Lack of blood’ was associated with poor nutrition and sharing blood withthe fetus. This aspect could also be used in health education messages to highlight theeffects of maternal malaria on the mother and to emphasize the consequences ofplacental malaria for the fetus.
The perception that adolescents, primigravidae and men are not at risk of malariais probably because malaria is not associated with anaemia and low birth weight,which most affect this vulnerable group. This perception plays an important role fortreatment-seeking practices for malaria in pregnancy in this community. For exampleadolescents were not seeking care at health units and men were found not to care fortheir young wives when they were sick with malaria. This perception is a challenge tothe malaria prevention programme in Uganda where early marriages are common andthe adolescent pregnancy rate is high (32%) (Uganda Bureau of Statistics, 2001).
Treatment-seeking practices for malaria 233

There is therefore a need to target men and adolescents, especially those who aremarried, to explain the risk malaria poses to them.
It was also found that malaria in this community is referred to using two localterminologies: omusujja (fever) and omusujja gw’ensiri (fever caused by mosquitoes).Yet these terminologies refer to different disease categories. A study in Bagamoyo,Tanzania, assessed local terminology for malaria and obtained similar findingsregarding the term homa (fever), used to mean any illness including those with nosymptoms of fever, and homa ya malaria (malaria), a term used by health workers torefer to malaria (Winch et al., 1996). Local terminologies for malaria have also beendocumented elsewhere (Agyepong, 1992; Helitzer-Allen et al., 1993) and are useful indesigning health education messages on malaria treatment and prevention. Sincecurrent malaria prevention and treatment messages in Uganda use the two termsinterchangeably to refer to malaria, it is important to use the term omusujja gw’ensiri(fever caused by mosquitoes) in promoting malaria treatment and preventionpractices. This study has not been able to differentiate the treatment-seeking patternsamong people who commonly use the term omusujja and omusujja gw’ensiri. This isan area that needs further inquiry.
The importance of costs of accessing care at health units noted in this study hasalso been documented elsewhere as a significant factor determining treatment-seekingpractices (Beckerleg, 1994; Amuyunzu, 1998; Nyamongo, 2001). These studies haveshown that pregnant women make an assessment of several factors including costsbefore a treatment choice is made. The cost assessment involved in selecting treatmentchoices by pregnant women has implications for the gender roles in families. Itappears that most women do not make decisions on treatment care where money isinvolved. It is the husbands who make such decisions because they control financialresources. Similar findings have been documented in Kenya where men’s decisions inseeking care for sick children were found to be critical (Mwenesi, 1995). It is thereforenecessary to target men in malaria prevention in pregnancy and to improve incomesof women through small-scale income-generating projects. Since women themselvesthink that their husbands should play an important role in malaria prevention and insupporting their wives in many other roles, it is important to find out the barrierswomen meet in discussing with their husbands issues concerning health care of theirfamilies.
Using the Health Belief Model the treatment-seeking hierarchy for malaria inpregnancy was analysed. The findings show that pregnant women are perceived to besusceptible to malaria with severe consequences like abortion and stillbirths. Thisstudy has, however, shown that pregnant women do not perceive the benefit ofeffective treatment and prevention of malaria in pregnancy; rather they rely onself-treatment with herbs and they seek care at health units as a last resort.The perceived barriers to effective treatment of malaria in pregnancy consist ofcultural practices and pressures, uncaring husbands, perception that omusujja isnormal in pregnancy, low-risk perception for malaria among adolescents andprimigravidae, lack of knowledge on severe consequences of malaria like anaemia andlow birth weight, failure to differentiate signs of malaria from those of earlypregnancy, poor quality of care and high costs of accessing care at health units. Thesefindings present opportunities for designing a health promotion package that
234 A. K. Mbonye, S. Neema and P. Magnussen
addresses the perceived barriers to effective treatment and prevention of malaria inpregnancy.
Acknowledgments
The authors sincerely acknowledge the contribution of all the respondents who spenttime in answering questions and participating in the discussions. The following peopleare also acknowledged: the District Director of Health Services Mukono District, andthe District Nursing Officer and Mr Steven Kalake for their support during fieldwork.They also thank the two research assistants, Jolly Nammudu and Charity Wamala,who participated in data collection and later transcribed them. They are grateful toMs Harriet Birungi of the Population Council, Nairobi, for her valuable commentson the manuscript. This study was funded by the Gates Malaria Partnership atLondon School of Hygiene and Tropical Medicine, London University, and theDanish Bilharzias Laboratory, Denmark, in collaboration with the Ministry of HealthUganda.
References
Abyan, I. M. & Osman, A. A. (1993) Social and Behavioural Factors Affecting Malaria inSomalia. TDR Social and Economics Research Project Reports No. 11, pp. 1–28. WHO,Geneva.
Agyepong, I. A. (1992) Malaria: ethno medical perceptions and practice in an Adange farmingcommunity and implications for control. Social Science and Medicine 35(2), 131–137.
Ahorlu, C. K. (1997) Malaria related beliefs and behaviour in Southern Ghana: implications fortreatment, prevention and control. Tropical Medicine and International Health 2, 488–499.
Amuyunzu, M. K. (1998) Willing the spirits to reveal themselves: rural Kenyans mothers’responsibility to restore their children’s health. Medical Anthropology Quarterly 12(4),490–502.
Baume, C., Helitzer, D. & Kachur, S. P. (2000) Patterns of care for childhood malaria inZambia. Social Science and Medicine 51(10), 1491–1503.
Becker, M. H. (1974) The Health Belief Model and personal health Behaviour. HealthEducation Monographs 2(4).
Beckerleg, S. (1994) Medical pluralism and Islam in Swahili communities in Kenya. MedicalAnthropology Quarterly 8(3), 299–313.
Bennet, P. & Smith, C. (1992) Parent’s attitude and social influences on childhood vaccination.Health Education Research, Theory and Practice 7, 341–348.
Bradley, C. B. & Kegeles, S. M. (1987) The use of diabetics-specific perceived control andhealth beliefs measures to predict treatment choice and efficacy in a feasibility study ofcontinuous subcutaneous insulin infusion pumps. Psychology and Health 1, 133–146.
Bloland, B., Slutsker, L., Steketee, R. W., Wirima, J. J., Heymann, D. L. & Breman, J. G.(1996) Rates and risk factors for mortality during the first two years of life in rural Malawi.American Journal of Tropical Medicine and Hygiene (supplement), 82–86.
D’Alessandro, U. (1999) A rational approach to malaria control in pregnancy in sub-SaharanAfrica: the need for a link between scientific research and public health interventions. Annalsof Tropical Medicine and Parasitology 93 (supplement 1), S75–77.
Foster, S. (1995) Treatment of malaria outside the formal health services. Journal of TropicalMedicine and Hygiene 98, 29–34.
Treatment-seeking practices for malaria 235
Heggenhougen, H. K., Hackenthal, V. & Vivek, P. (2003) The Behaviour and Social Aspects ofMalaria Control: An Introduction and Annotated Biography. Special Program for Research &Training in Tropical Diseases (TDR).
Helitzer-Allen, D. L., Kendall, C. & Wirima, J. J. (1993) The role of ethnographic research inmalaria control: an example for Malawi. Research in Sociology and Health Care 10, 269.
Janz, N. & Becker, M. H. (1984) The Health Belief Model: a decade later. Health EducationQuarterly 11, 1–47.
Kengeya-Kayondo, J., Seeley, J. A., Kajura-Beganja, E., Kabunga, E., Mubiru, E., Sembaja, F.& Mulder, D.W. (1994) Recognition, treatment seeking behaviour and perception of cause ofmalaria among rural women in Uganda. Acta Tropica 58(3–4), 267–273.
Langie, J. K. (1977) Social networks, health beliefs and preventive health behaviour. Journal ofHealth and Social Behaviour 18, 244–260.
McCombie, S. C. (1996) Treatment seeking for malaria: a review of recent research. SocialScience and Medicine 43(6), 933–945.
McCorwick, M. (1985) The contribution of low birth weight to infant and childhood morbidity.New England Journal of Medicine 321, 82–90.
Mbonye, A. K. (2001) Risk factors associated with maternal deaths in health units in Uganda.African Journal of Reproductive Health 5(3), 47–53.
Menendez, C. (1999) Priority areas for current research on malaria in pregnancy. Annals ofTropical Medicine and Parasitology 93 (supplement 1), S71–74.
Ministry of Health Uganda (2001) HIV/AIDS Surveillance Report. Ministry of Health,Kampala, Uganda.
Mwenesi, H. A., Harpharm, T. T. & Snow, R. W. (1995) Child malaria treatment practicesamong mothers in Kenya. Social Science and Medicine 40(9), 1271–1277.
Nathwani, D., Curie, P. F., Douglas, G. J., Green, S. T. & Smith, N. C. (1992) Plasmodiumfalciparum malaria in pregnancy. British Journal of Obstetrics and Gynaecology 99, 118–121.
Ndyomugyenyi, R., Neema, S. & Magnussen, P. (1999) The use formal and informal services forantenatal care and malaria treatment in rural Uganda. Health Policy and Planning 13,94–104.
Nyamongo, I. K. (2001) Health care seeking behaviour of malaria patients in a Kenyan ruralcommunity. Social Science and Medicine 42, 1–10.
Ruebush, T. K., Kern, M. K., Campbell, C. C. & Oloo, A. J. (1995) Self-treatment of malariain a rural area of Western Kenya. Bulletin of the World Health Organization 73(2), 229–236.
Slutsker, L., Bloland, P., Steketee, R. W., Wirima, J. J., Heymann, D. L. & Breman, J. G.(1996) Infant and second year mortality in rural Malawi; causes and descriptive epidemiol-ogy. American Journal of Tropical Medicine and Hygiene (supplement), 77–81.
Steketee, R., Wirima, J. J., Hightower, A. W., Slutsker, L., Heyman, D. L. & Breman, J. G.(1996) The effect of malaria and malaria prevention in pregnancy on offspring birth weight,prematurity and intrauterine growth retardation in rural Malawi. American Journal ofTropical Medicine and Hygiene 55 (supplement), 33–41.
Uganda Bureau of Statistics (2001) The Uganda Demographic and Health Survey. UgandaBureau of Statistics, Entebbe, Uganda.
White, N. J. & Breman, J. G. (2001) Malaria and Babesiosis caused by red blood cell parasites.In Braunwald, E., Fauci, A. S., Kasper, D. L., Hauser, S. L., Longo, D. L., Jameson, J. L.& Harrison, S. (eds) Principles of Internal Medicine. Fifth edition. Mc-Graw-Hill, New York,pp. 1203–1213.
WHO (1991) Maternal Mortality: A Global Factbook. WHO Division of Family Health,Geneva, Switzerland, pp. 1170–1172.
236 A. K. Mbonye, S. Neema and P. Magnussen
WHO (1993) Implementation of the Global Malaria Control Strategy – Report of a WHO StudyGroup on the Implementation of the Global Action for Malaria Control 1993–2000. WHOTechnical Report Series 839. World Health Organization, Geneva, Switzerland.
Winch, P. J., Makemba, A. M., Kamazima, S. R., Lurie, M., Lwihura, G. K., Premji, J. N.,Minjas, J. N. & Shiff, C. J. (1996) Local terminology for febrile illnesses in Bagamoyodistrict, Tanzania and its impact on the design of a community-based malaria controlprogramme. Social Science and Medicine 42(7), 1057–1067.
Treatment-seeking practices for malaria 237
Related Documents











