PLEASE SCROLL DOWN FOR ARTICLE This article was downloaded by: [Brewerton, Timothy D.] On: 24 February 2011 Access details: Access Details: [subscription number 933991266] Publisher Routledge Informa Ltd Registered in England and Wales Registered Number: 1072954 Registered office: Mortimer House, 37- 41 Mortimer Street, London W1T 3JH, UK Eating Disorders Publication details, including instructions for authors and subscription information: http://www.informaworld.com/smpp/title~content=t713666342 Treatment Results of Anorexia Nervosa and Bulimia Nervosa in a Residential Treatment Program Timothy D. Brewerton a ; Carolyn Costin b a Department of Psychiatry & Behavioral Sciences, Medical University of South Carolina, Charleston, South Carolina, USA b Monte Nido & Affiliates, Malibu, California, USA Online publication date: 24 February 2011 To cite this Article Brewerton, Timothy D. and Costin, Carolyn(2011) 'Treatment Results of Anorexia Nervosa and Bulimia Nervosa in a Residential Treatment Program', Eating Disorders, 19: 2, 117 — 131 To link to this Article: DOI: 10.1080/10640266.2011.551629 URL: http://dx.doi.org/10.1080/10640266.2011.551629 Full terms and conditions of use: http://www.informaworld.com/terms-and-conditions-of-access.pdf This article may be used for research, teaching and private study purposes. Any substantial or systematic reproduction, re-distribution, re-selling, loan or sub-licensing, systematic supply or distribution in any form to anyone is expressly forbidden. The publisher does not give any warranty express or implied or make any representation that the contents will be complete or accurate or up to date. The accuracy of any instructions, formulae and drug doses should be independently verified with primary sources. The publisher shall not be liable for any loss, actions, claims, proceedings, demand or costs or damages whatsoever or howsoever caused arising directly or indirectly in connection with or arising out of the use of this material.

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

PLEASE SCROLL DOWN FOR ARTICLE
This article was downloaded by: [Brewerton, Timothy D.]On: 24 February 2011Access details: Access Details: [subscription number 933991266]Publisher RoutledgeInforma Ltd Registered in England and Wales Registered Number: 1072954 Registered office: Mortimer House, 37-41 Mortimer Street, London W1T 3JH, UK
Eating DisordersPublication details, including instructions for authors and subscription information:http://www.informaworld.com/smpp/title~content=t713666342
Treatment Results of Anorexia Nervosa and Bulimia Nervosa in aResidential Treatment ProgramTimothy D. Brewertona; Carolyn Costinb
a Department of Psychiatry & Behavioral Sciences, Medical University of South Carolina, Charleston,South Carolina, USA b Monte Nido & Affiliates, Malibu, California, USA
Online publication date: 24 February 2011
To cite this Article Brewerton, Timothy D. and Costin, Carolyn(2011) 'Treatment Results of Anorexia Nervosa andBulimia Nervosa in a Residential Treatment Program', Eating Disorders, 19: 2, 117 — 131To link to this Article: DOI: 10.1080/10640266.2011.551629URL: http://dx.doi.org/10.1080/10640266.2011.551629
Full terms and conditions of use: http://www.informaworld.com/terms-and-conditions-of-access.pdf
This article may be used for research, teaching and private study purposes. Any substantial orsystematic reproduction, re-distribution, re-selling, loan or sub-licensing, systematic supply ordistribution in any form to anyone is expressly forbidden.
The publisher does not give any warranty express or implied or make any representation that the contentswill be complete or accurate or up to date. The accuracy of any instructions, formulae and drug dosesshould be independently verified with primary sources. The publisher shall not be liable for any loss,actions, claims, proceedings, demand or costs or damages whatsoever or howsoever caused arising directlyor indirectly in connection with or arising out of the use of this material.
Eating Disorders, 19:117–131, 2011Copyright © Taylor & Francis Group, LLCISSN: 1064-0266 print/1532-530X onlineDOI: 10.1080/10640266.2011.551629
Treatment Results of Anorexia Nervosaand Bulimia Nervosa in a Residential
Treatment Program
TIMOTHY D. BREWERTONDepartment of Psychiatry & Behavioral Sciences, Medical University of South Carolina,
Charleston, South Carolina, USA
CAROLYN COSTINMonte Nido & Affiliates, Malibu, California, USA
Data on the effectiveness of residential treatment for patients withanorexia nervosa (AN) and bulimia nervosa (BN) are limited.We analyzed patient survey results at admission and dischargefrom Monte Nido Residential Treatment Program. Of 287 consec-utive admissions, 80% (231) “graduated” (completed ≥ 30 days oftreatment), and of these (all of whom gave consent), only patientswith AN (N = 120) or BN (N = 95) were included (215 of 231,93%) in this study. Analyses included a comparison of admissionvs. discharge variables (paired t-tests) for each diagnosis. At eachassessment, graduates completed the Eating Disorders Inventory-2(EDI-2), the Beck Depression Inventory (BDI), and a structuredeating disorder assessment questionnaire. For patients with AN,there were statistically significant improvements in mean BMI. Inaddition, for both AN and BN patients, there were statisticallysignificant improvements in BDI scores, all 11 EDI-2 subscales,and frequencies of bingeing, vomiting, laxative abuse, chew-ing and spitting, stimulant abuse, and restricting behavior. Thegreat majority of patients completing treatment showed significantimprovement at discharge from intensive residential treatment.
Address correspondence to Timothy D. Brewerton, M.D., D.F.A.P.A., F.A.E.D., 216 ScottStreet, Mt. Pleasant, SC 29464, USA. E-mail: [email protected]
117
Downloaded By: [Brewerton, Timothy D.] At: 16:16 24 February 2011

118 T. D. Brewerton and C. Costin
INTRODUCTION
Several studies report short-term improvements from inpatient treatment ofindividuals with anorexia nervosa (AN) and bulimia nervosa (BN) (Andersen,1986; Andersen, Bowers, & Evans, 1997; Andersen, Morse & Santmyer, 1985;Bowers, Andersen, & Evans, 2004; Garner, Garfinkel & Irvine, 1986; Vandereycken, 1985). However, there are very few published studies of theresults of treatment of patients who have been treated in residential treat-ment programs (RTCs). RTCs offer the advantage of a long-term, structured,and intensive treatment locale outside of the sterile environment of a hospitalsetting, generally at lower cost. Bean et al. (2008) reported positive short-term outcomes in 107 patients (72 females and 35 males) with AN treatedat the residential program at Rogers Memorial Hospital. The only report onthe short-term treatment of BN in a RTC was by Gleaves et al. (1993), whoreported on the effectiveness of residential treatment on a consecutive groupof 497 patients with BN. All measured subscales of the Eating DisordersInventory (EDI; Garner, Olmsted, & Polivy, 1983) significantly improvedbetween admission and discharge, although the authors did not measurebinge and purge frequency at discharge. Lowe et al. (2003) reported sig-nificant improvements in depression and eating disorder symptomatologyfollowing residential treatment of 472 patients (279 with AN, 193 with BN).According to the third edition of the Practice Guidelines for the Treatmentof Eating Disorders of the American Psychiatric Association (2006), RTCs areappropriate for patients who are medically stable to the extent that intra-venous fluids, nasogastric tube feedings, or multiple daily laboratory testsare not needed. In addition, patients appropriate for RTC manifest poor-to-fair motivation and are preoccupied with intrusive repetitive thoughts atleast 4–6 hours a day. However, they generally are cooperative with highlystructured treatment, have failed outpatient interventions, and need supervi-sion at all meals or they will restrict eating, binge and/or purge. They canask for and use support from others and utilize cognitive and behavioralskills to inhibit purging (APA 2006; LaVia et al., 1998). In addition, an RTCis a good treatment option when: a) patients have severe family conflict ordysfunction, or the absence of family support, such that the patient is unableto receive structured treatment in home; b) the patient lives alone withoutan adequate support system and/or c) treatment program is too distant forpatient to participate from home.
The other major eating disorder practice guidelines that are available,those of the National Institute of Clinical Excellence (NICE) (2004), have noreference to the use of RTCs given the lack of data.
Downloaded By: [Brewerton, Timothy D.] At: 16:16 24 February 2011

Anorexia Nervosa and Bulimia Nervosa in Residential Treatment 119
METHODS
Design and Hypothesis
This study involved a prospective cohort in design and planning of mea-sures. Our hypothesis was that patients who stayed at least 30 days intreatment (graduates) would show significant improvements in all measuresof ED and depressive symptomatology. A cutoff of 30 days was used a prioribecause it was considered the minimal time period necessary for complet-ing the program and effecting change and because it was a pre-designatedadmission requirement for all patients.
Subjects
We analyzed results from a survey of respondents before and after complet-ing at least 30 days or more of treatment at Monte Nido Residential TreatmentProgram in Malibu, CA. Of 287 consecutive admissions, 80% (231) were eli-gible for inclusion in the study, including 120 with AN, 95 with BN, and 16with EDNOS. All of these patients received at least 30 days or more of treat-ment and are referred to as “graduates.” The 20% of admissions who werenot eligible left treatment before 30 days and did not complete dischargesurvey measures. These patients are referred to as “non-graduates.” Becauseof the low sample size of the EDNOS group, only those graduates with ANand BN were analyzed for the purposes of this study. The analyses includeda comparison of admission vs. discharge (DC) assessment variables for eachdiagnosis.
The demographic and clinical characteristics of the graduates and thenon-graduates are shown in tables 1 and 2 for AN and BN, respectively.The age range of the graduates with AN was 17 to 55 years, while thatof the BN graduates was 22 to 57 years. It is important to note that thiswas largely a treatment refractory group, with 90% of patients with AN and93% of patients with BN failing prior outpatient, inpatient, and/or residentialtreatment.
Intervention
Individuals in this study received treatment for an eating disorder at MonteNido, a 24-hour residential care facility operated in a six bed homelikeenvironment. The treatment philosophy and the protocols used were devel-oped by one of the authors (CC), drawing from evidenced based researchand extensive clinical experience in both inpatient and outpatient settings.
Downloaded By: [Brewerton, Timothy D.] At: 16:16 24 February 2011

120 T. D. Brewerton and C. Costin
A comprehensive description of the program can be found in the first edi-tion of The Eating Disorder Sourcebook (Costin, 1996). An overview of theprogram components and program goals are provided below.
Weight restoration or stabilization is a primary treatment goal forpatients with AN. In addition, interventions for patients focus on the con-trol or reversal of weight and food phobias, and the development of trustin their bodies and the recovery process. Contrary to the rigid protocols ofother treatment protocols, patients with AN might be allowed periods ofweight gain balanced with periods of weight maintenance, allowing for thepsychological component of recovery to keep pace with weight restoration.Additionally, patients are initially allowed to abstain from eating certain fearfoods. Increasing the variety of food and the calories consumed may bealternated thereby allowing patients to focus on one aspect of recovery ata time. Clinically, patients report that this process forms a foundation forbetter tolerance and maintenance of weight gain during treatment, and mostnotably for the continuation of weight restoration post discharge.
A specific goal in the treatment of patients with BN is attaining absti-nence from any bingeing or purging behavior. Cognitive behavioral therapy(CBT) and dialectical behavior therapy (DBT) are used to assist patientswith their thought patterns and the emotional dysregulation that contributesto these behaviors. Through psychotherapy and by utilizing a level systemof decreased monitoring (observation after meals, staff supervision in thekitchen, etc.) along with increased exposure and responsibility, individualsare taught how, and are given the opportunity to replace, unhealthy behav-iors with healthy ones. The program and staff teach patients to reach out topeople rather than their behaviors to get their needs met.
Distinctive components of the Monte Nido program that are notableinclude:
● Range of therapeutic interventions. Each week, every patient receivedindividual psychotherapy three times with their assigned therapist, oneindividual session with the clinical director, one–two individual sessionswith a dietitian, a session with the psychiatrist, a session with the med-ical physician, two group sessions with an exercise trainer, and severalforms of group therapy, including Body & Soul group, Food & Feelingsgroup, Primary Process group, Nutrition group, Spirituality group, LifeSkills group, Goals group, Special Topics group, Meditation group, andYoga.
● Use of recovered staff in the treatment team. Recovered staff membersopenly serve as role models. Patients have consistently reported thatspeaking with someone who is recovered is a crucial factor in theirrecovery (Garrett, 1997; 1998; Redenbach & Lawler, 2003).
● Patients have hands-on experiences with food that simulates real life.Throughout the time frame of the study, patients utilized a kitchen andmade their own food.
Downloaded By: [Brewerton, Timothy D.] At: 16:16 24 February 2011

Anorexia Nervosa and Bulimia Nervosa in Residential Treatment 121
The home like environment with 6 patients can easily simulate lifebefore and after treatment. Staff and patients eat the same food and sittogether around a small dining room table. This is also a unique feature fora few reasons: a) many treatment programs are so large that patients haveto eat their food from a cafeteria setting; b) some treatment programs havestaff attending meals but not eating with the patients; c) at other treatmentprograms, the staff members at meals are not necessarily the same therapistsdoing the individual sessions.
A graduated level system allows for patients to gradually get increasedresponsibilities for taking care of their own nourishment. With help fromthe staff, eventually patients learn to portion, shop for, prepare, and cooktheir own snacks and then meals. Once each week, the higher-level patientsorganize for, shop, prepare, and cook a meal for the rest of the patients. Allof these experiences require certain skill sets that are important for successfultransition to after care and for long-term recovery. These experiences arenot available in larger programs using institutionalized kitchens and diningrooms.
● Level system. The level system provides structure for the entire treatmentprocess. Patients collaborate with their therapist and the treatment teamby means of a weekly contract with goals in a variety of treatmentcategories, e.g., nutrition, exercise, cognitive, behavioral, relationship,family, medical, and discharge. Patients must successfully complete whatis expected on each level to progress to the next level with its associatedresponsibilities and privileges.
● Medication management. All patients meet weekly with the programpsychiatrist for medication evaluation and management. Evaluation forpossible use of medication is based on available practice guidelines(American Psychiatric Association, 2006) and in some cases results fromquantitative electroencephalographic (EEG) analysis (Bares et al., 2007;2008; Hunter, Cook & Leuchter, 2007; Leuchter et al., 2009a; 2009b).
Assessment
At each assessment, graduates completed the Eating Disorders Inventory-2 (EDI-2) (Garner, 1991; Garner, Olmsted, & Polivy, 1983), the BeckDepression Inventory (BDI) (Beck, Steer, & Brown 1996), and a structuredeating disorder assessment questionnaire developed for outcome assessmentof eating disorder behaviors. Possible responses for each behavior were asfollows: 0) Not at all; 1) Once a month or less; 2) A few times a month;3) At least once a week; 4) At least twice a week; 5) Daily; 6) More thanonce a day.
All graduates gave written informed consent for their responses tobe used for both clinical and research purposes. To protect the client’s
Downloaded By: [Brewerton, Timothy D.] At: 16:16 24 February 2011

122 T. D. Brewerton and C. Costin
confidentiality and anonymity, each respondent was identified with acomputer-generated number.
The mean duration of treatment was 96.0 ± 53.8 days for the ANsubjects and 78.9 ± 49.1 days for the BN subjects.
Classification of Outcomes
Outcomes of AN were classified as per Morgan and Russell (1975) as “good,”“intermediate,” and “poor.” A “good” outcome was defined by the return ofnormal weight (BMI ≥ 18.0) and normal menstrual function. “Intermediate”outcome or partial recovery was indicated by either weight restoration(BMI ≥ 18.0) or resumption of normal menstrual function. “Poor” outcomewas indicated by the absence of both. For BN, a “good” outcome wasdefined by the complete cessation of binge eating and purging behaviors.An “intermediate” outcome or partial recovery was defined by at least a 50%reduction in binge eating and purging, and a “poor” outcome was definedby the failure to meet either of the above goals.
Statistics
Means are presented with standard deviations (SD). Comparisons of para-metric independent samples were completed using analyses of variance(ANOVA) and for nonparametric independent samples Kruskal-Wallis testswere used. Related parametric data were analyzed using paired t-tests,and related nonparametric data were analyzed using Wilcoxon SignedRanks Tests. Post-hoc Bonferroni corrections were made for multiplecomparisons.
RESULTS
Baseline Group Comparisons
We compared Monte Nido graduates with AN and BN on a number of demo-graphic and clinical variables by diagnosis, and these results are shown inTable 1. Significant differences between the groups were found in lengthof stay (AN > BN), number of past hospitalizations (AN > BN), admissionand discharge BMI (BN > AN), and bulimia subscale scores of the EDI-2(BN > AN).
We also compared graduates with non-graduates on the same set ofdemographic and clinical variables, and these results are shown in Table 2for the AN group and Table 3 for the BN group. Discharge assessmentsurveys were only completed by a small minority of non-graduates and aretherefore not presented.
Downloaded By: [Brewerton, Timothy D.] At: 16:16 24 February 2011

Anorexia Nervosa and Bulimia Nervosa in Residential Treatment 123
TABLE 1 Demographic and Baseline Clinical Characteristics of Study Graduates With ANand BN (Mean ± SD). Uncorrected p-Values are Provided, and When Appropriate, Correctedp-Values are Given in Parentheses
AN graduates BN graduates p-value
Sample size (N ) 120 95Age (years) 31.4 ± 8.3 29.8 ± 8.0 .016 (.3 corrected)Length of illness (years) 8.4 ± 6.2 8.5 ± 7.5Length of stay (days) 97.6 ± 65.2 72.1 ± 45.1 0.0001 (∗0.0019 corrected)Admit BMI 15.9 ± 1.8 20.8 ± 3.4 0.0001 (∗0.0019 corrected)Discharge BMI 18.2 ± 1.4 21.6 ± 4.0 0.0001 (∗0.0019 corrected)Admit BDI 28.9 ± 11.8 28.9 ± 12.6 .64Discharge BDI 12.6 ± 9.4 10.6 ± 9.0 .34# Past hospitalizations 1.7 ± 1.8 0.8 ± 1.4 .001 (∗.019 corrected)Drive for thinness (EDI-2) 14.1 ± 6.1 15.2 ± 5.1 .22Bulimia (EDI-2) 4.2 ± 5.2 11.4 ± 5.7 .001 (∗.019 corrected)Body dissatisfaction (EDI-2) 15.2 ± 8.0 18.2 ± 8.2 .003 (.057 corrected)Ineffectiveness (EDI-2) 13.0 ± 8.0 14.2 ± 8.1 .86Perfectionism (EDI-2) 9.2 ± 4.6 9.6 ± 4.7 .75Interpersonal distrust (EDI-2) 6.5 ± 4.4 6.1 ± 4.4 .5Interoceptive awareness (EDI-2) 11.0 ± 6.5 13.2 ± 7.2 .09Maturity fears (EDI-2) 6.0 ± 5.4 6.1 ± 5.8 .61Asceticism (EDI-2) 9.5 ± 5.5 9.1 ± 4.9 .64Impulse regulation (EDI-2) 5.7 ± 5.4 7.5 ± 5.8 .023 (.44 corrected)Social insecurity (EDI-2) 9.0 ± 4.7 9.4 ± 4.8 .91
Note. ∗ = Significance at the p ≤ .05 level (corrected).
TABLE 2 Demographic and Baseline Clinical Characteristics of Study Graduates and Non-Graduates With AN (Mean ± SD). Uncorrected p-Values are Provided, and When Appropriate,Corrected p-Values are Given in Parentheses
Graduates Non-graduates p-value (unpaired t-test)
Sample size (N ) 120 46Age (years) 31.4 ± 8.3 41.2 ± 11.3 .001 (∗.019 corrected)Length of illness (years) 8.4 ± 6.2 13.8 ± 7.5 .002 (∗.038 corrected)Length of stay (days) 97.6 ± 65.2 15.6 ± 9.3 .001 (∗.019 corrected)Admit BMI 15.9 ± 1.8 15.6 ± 1.7 .6Discharge BMI 17.8 ± 1.5 16.2 ± 1.8 .001 (∗.019 corrected)Admit BDI 28.9 ± 11.8 27.4 ± 15.0 .69Discharge BDI 12.6 ± 9.4 8.1 ± 11.5 .07 (>.7 corrected)# Past hospitalizations 1.7 ± 1.8 0.6 ± 1.0 .004 (.078 corrected)Drive for thinness (EDI-2) 14.1 ± 6.1 13.6 ± 7.8 .82Bulimia (EDI-2) 4.2 ± 5.2 2.9 ± 3.6 .37Body dissatisfaction (EDI-2) 15.2 ± 8.0 13.4 ± 8.9 .46Ineffectiveness (EDI-2) 13.0 ± 8.0 13.0 ± 8.0 .69Perfectionism (EDI-2) 9.2 ± 4.6 10.2 ± 5.4 .48Interpersonal distrust (EDI-2) 6.5 ± 4.4 5.7 ± 5.3 .57Interoceptive awareness (EDI-2) 11.0 ± 6.5 11.5 ± 8.9 .81Maturity fears (EDI-2) 6.0 ± 5.4 6.2 ± 6.8 .9Asceticism (EDI-2) 9.5 ± 5.5 8.2 ± 4.1 .44Impulse regulation (EDI-2) 5.7 ± 5.4 4.8 ± 4.0 .56Social insecurity (EDI-2) 9.0 ± 4.7 8.6 ± 5.4 .76
Note. ∗ = Significance at the p ≤ .05 level (corrected).
Downloaded By: [Brewerton, Timothy D.] At: 16:16 24 February 2011

124 T. D. Brewerton and C. Costin
TABLE 3 Demographic and Baseline Clinical Characteristics of Study Graduates and Non-Graduates With BN (Mean ± SD). Uncorrected p-Values are Provided, and When Appropriate,Corrected p-Values are Given in Parentheses
Graduates Non-graduates p-value (unpaired t-test)
Sample size (N ) 95 54Age (years) 29.8 ± 8.0 32.1 ± 7.0 .28Length of illness (years) 8.7 ± 7.5 9.4 ± 7.5 .75Length of stay (days) 72.1 ± 45.1 21.4 ± 8.6 0.0001 (∗0.0019 corrected)Admit BMI 20.8 ± 3.4 20.4 ± 2.1 .61Discharge BMI 21.4 ± 3.6 20.8 ± 1.9 .49Admit BDI 28.9 ± 12.5 23.1 ± 14.3 .17Discharge BDI 10.6 ± 9.0 11.6 ± 6.6 .76# Past hospitalizations 0.8 ± 1.4 0.6 ± 1.6 .03 (.57 corrected)Drive for thinness (EDI-2) 13.7 ± 6.3 15.3 ± 5.1 .36Bulimia (EDI-2) 11.4 ± 5.7 11.1 ± 5.9 .87Body dissatisfaction (EDI-2) 18.1 ± 8.2 18.2 ± 7.4 .98Ineffectiveness (EDI-2) 14.1 ± 8.1 10.5 ± 7.2 .12Perfectionism (EDI-2) 9.2 ± 4.6 9.6 ± 4.7 .16Interpersonal distrust (EDI-2) 6.1 ± 4.2 5.5 ± 4.6 .66Interoceptive awareness (EDI-2) 13.2 ± 7.2 10.4 ± 6.2 .18Maturity fears (EDI-2) 6.1 ± 5.8 3.9 ± 3.0 .15Asceticism (EDI-2) 9.1 ± 4.9 8.5 ± 3.1 .61Impulse regulation (EDI-2) 7.5 ± 5.8 6.0 ± 6.0 .39Social insecurity (EDI-2) 9.4 ± 4.8 7.7 ± 4.4 .23
Note. ∗ = Significance at the p ≤ .05 level (corrected).
For those with a diagnosis of AN, statistically significant differencesbetween the groups were only found for age (non-graduates > grad-uates), length of stay (graduates > non-graduates), duration of illness(non-graduates > graduates), and number of hospitalizations (graduates >
non-graduates; see Table 2). Graduates endorsed significantly more fre-quent restricting behavior (3.6 ± 2.5 v. 1.5 ± 1.5) and significantly lessfrequent enema abuse (1.5 ± 1.5 v. 2.9 ± 2.4) than non-graduates (p < .01,Mann-Whitney U test). There were no significant differences in any of theadmission EDI-2 subscale scores, admission and discharge BDI scores, andself-reported frequencies of bingeing, vomiting, chewing and spitting, lax-ative abuse, diuretic abuse, ipecac abuse, stimulant abuse, and compulsiveexercise.
For those with a diagnosis of BN, statistically significant differencesbetween the groups were found for length of stay (graduates > non-graduates; see Table 3). In addition, there was a significant differencebetween the 2 groups that remained after post-hoc corrections for frequen-cies of stimulant abuse (graduates > non-graduates, 1.95 ± 1.7 v. 0.86 ± 1.6,p < .01, Mann-Whitney U test). The two groups did not significantly differin age, length of illness, mean number of past hospitalizations, mean admitand discharge BMI’s, mean admit and discharge BDI’s, mean EDI subscale
Downloaded By: [Brewerton, Timothy D.] At: 16:16 24 February 2011

Anorexia Nervosa and Bulimia Nervosa in Residential Treatment 125
scores, and mean self-reported frequencies of bingeing, vomiting, chew-ing and spitting, laxative abuse, diuretic abuse, ipecac abuse, enema abuse,restricting behavior, and compulsive exercise.
Clinical Outcome: AN
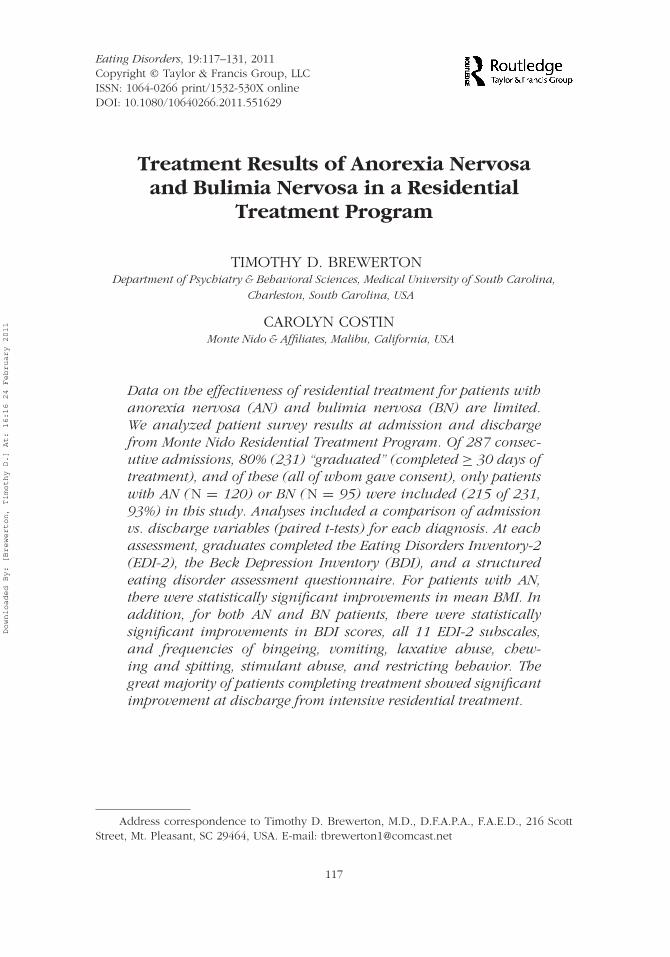
In the AN group, there was a statistically significant increase in mean BMIfrom 15.9 ± 1.7 to 18.2 ± 1.4 (p < .0001, paired t-test) following treatment.In addition, 11 of 11 EDI-2 subscales significantly increased from admissionto discharge (see Figure 1). Frequencies of bingeing, vomiting, chewing andspitting, laxative abuse, compulsive exercising, stimulant abuse, and restrict-ing behavior were all significantly reduced at the time of discharge (p ≤ .05,Wilcoxon Signed Rank Tests, see Figure 2). There were no significant dif-ferences between admission and discharge frequencies for diuretic abuse,ipecac abuse, and enema abuse, largely due to low base rates of and/orlarge variations in the frequencies of these behaviors in the AN group. MeanBDI scores significantly improved from admission (28.3 ± 12.1) to discharge(14.2 ± 9.5, p < .0001, paired t-test).
16
∗∗
∗
∗
∗
∗ ∗
∗∗∗
∗
14
12
10
8
6
4
2
0
Drive
for th
innes
s
Bulim
ia
Body d
issat
isfac
tion
Inef
fectiv
enes
s
Perfec
tionis
m
Inte
rper
sona
l dist
rust
Inte
roce
ptive
awar
enes
s
Mat
urity
fear
s
Ascet
icism
Impu
lse re
gulat
ion
Social
inse
curit
y
AN @ AdmissionAN @ Discharge
FIGURE 1 EDI-2 subscale scores in respondents with anorexia nervosa (AN) at admissionand discharge. Significant differences between admission and discharge scores are indicatedby an asterisk (∗), p < .05, paired t-test following post-hoc Bonferroni corrections.
Downloaded By: [Brewerton, Timothy D.] At: 16:16 24 February 2011
126 T. D. Brewerton and C. Costin
3.5
An @ Admission
An @ Discharge
3
∗ ∗
∗ ∗
∗
∗
∗
2.5
2
1.5
1
0.5
0
Binge
frequ
ency
Vom
iting
frequ
ency
Laxa
tive
frequ
ency
Diuret
ic fre
quen
cy
Ipec
ac fr
eque
ncy
Enem
a fre
quen
cy
Excer
cise
frequ
ency
Chewing
freq
uenc
y
Stimula
nt fr
eque
ncy
Restri
cting
freq
uenc
y
FIGURE 2 Frequency of eating disordered behaviors in respondents with anorexia nervosa(AN) at admission and discharge follow-up. Possible responses for each behavior were: 0) Notat all; 1) Once a month or less; 2) A few times a month; 3) At least once a week; 4) At leasttwice a week; 5) Daily; 6) More than once a day. Significant differences between admissionand discharge scores are indicated by an asterisk (∗), p < .05, Wilcoxon Signed Ranks Testfollowing post-hoc corrections for number of comparisons.
At the time of discharge 39% of AN graduates achieved weight recov-ery (BMI ≥ 18); in addition, 18% had a good outcome (BMI ≥ 18 ANDresumption of normal menses), 56% an intermediate outcome (BMI ≥ 18 ORresumption of normal menses) and 25% a poor outcome (neither restorationof weight nor menses). None of the graduates treated for AN were obese(BMI > 30) or overweight (BMI between 20 and 25) at the time of discharge.
Clinical Outcome: BN
In the BN group, there was no statistically significant change in mean BMIbetween admission (20.8 ± 3.6) and discharge (21.6 ± 4.0; NS, pairedt-test). All 11 of 11 EDI-2 subscales significantly improved from admissionto discharge (p < .01, Bonferroni corrected paired t-tests; see Figure 3).Frequencies of bingeing, vomiting, laxative abuse, diuretic abuse, chewingand spitting, compulsive exercising, stimulant abuse, and restricting behavior
Downloaded By: [Brewerton, Timothy D.] At: 16:16 24 February 2011

Anorexia Nervosa and Bulimia Nervosa in Residential Treatment 127
20
∗
∗∗
∗
∗ ∗
∗
∗
∗
∗
∗18
16
14
12
10
8
6
BN @ AdmissionBN @ Discharge
4
2
0
Drive
for th
innes
s
Bulim
ia
Body d
issat
isfac
tion
Inef
fectiv
enes
s
Perfec
tionis
m
Inte
rper
sona
l dist
rust
Inte
roce
ptive
awar
enes
s
Mat
urity
fear
s
Ascet
icism
Impu
lse re
gulat
ion
Social
inse
curit
y
∗∗∗∗
∗∗∗
∗
∗∗ ∗
∗∗∗∗
∗
∗
∗
∗
FIGURE 3 EDI-2 subscale scores in respondents with bulimia nervosa (BN) at admission anddischarge. Significant differences between admission and discharge scores are indicated byan asterisk (∗), p < .05, paired t-test following post-hoc Bonferroni corrections.
were all significantly reduced at the time of discharge (p < .01, WilcoxonSigned Rank Tests, see Figure 4). However, there were no significant dif-ferences between admission and discharge frequencies for diuretic abuse,ipecac abuse, and enema abuse, in large part due to low base rates of andsubstantial variations in the frequencies of these behaviors. Mean BDI scoressignificantly improved from admission (26.8 ± 12.2) to discharge (9.8 ± 8.6,p < .001, paired t-test).
At discharge 84% of BN graduates reported a good outcome (100%cessation of their binge, purge, and other compensatory behaviors), 11% anintermediate outcome (≥ 50% reduction in both) and 5% a poor outcome(< 50% reduction).
In terms of weight one of the graduates (1.6%) treated for BN was obese(BMI > 30) and 8 (6.6%) were overweight (BMI between 25 and 30) at thetimes of both admission and discharge.
DISCUSSION
The great majority of patients showed significant improvement at dischargeafter intensive residential care. Specifically, 74% of patients with AN and 95%
Downloaded By: [Brewerton, Timothy D.] At: 16:16 24 February 2011

128 T. D. Brewerton and C. Costin
5
∗
∗
∗ ∗
∗
∗
∗
4.5
4
3.5
3
2.5
2
1.5
1
0.5
0
BN @ Admission
BN @ Discharge
∗
∗
∗ ∗
∗
∗
∗
Binge
frequ
ency
Vom
iting
frequ
ency
Laxa
tive
frequ
ency
Diuret
ic fre
quen
cy
Ipec
ac fr
eque
ncy
Enem
a fre
quen
cy
Excer
cise
frequ
ency
Chewing
freq
uenc
y
Stimula
nt fr
eque
ncy
Restri
cting
freq
uenc
y
FIGURE 4 Frequency of eating disordered behaviors in respondents with bulimia nervosa(BN) at admission and discharge. Possible responses for each behavior were: 0) Not at all;1) Once a month or less; 2) A few times a month; 3) At least once a week; 4) At leasttwice a week; 5) Daily; 6) More than once a day. Significant differences between admissionand discharge scores are indicated by an asterisk (∗), p < .05, Wilcoxon Signed Rank Testfollowing post-hoc corrections for number of comparisons.
of patients with BN achieved a good or intermediate outcome by discharge.Residential treatment using this particular treatment philosophy may be aneffective and less costly alternative to inpatient treatment (Costin, 2007).Although our results are compelling, there are a number of limitations to thisstudy, the greatest of which is that it lacks a control or comparison group.This makes it impossible to definitely conclude that residential treatmentwas the cause of these patients’ improvement. However, it is very unlikelythat our patients would have improved to the extent that they did on theirown. Over 90% had been “treatment refractory” in that they had failed prioroutpatient, inpatient and/or residential programs.
Secondly, our results do not bear directly upon the question of whetherthe program’s treatment philosophy has anything to do with the patientimprovements reported. The methods of this study did not allow foran analysis of the “active ingredients” which may have contributed toimprovements.
Downloaded By: [Brewerton, Timothy D.] At: 16:16 24 February 2011

Anorexia Nervosa and Bulimia Nervosa in Residential Treatment 129
Thirdly, not all of the patients who were admitted into the programwere studied at discharge. Although approximately 20% of patients admittedto Monte Nido chose to leave or were asked to leave before completing30 days of treatment, which was for a variety of reasons, e.g., lack of readi-ness, insurance denial, financial difficulties, and rule breaking, there werevery few significant differences in baseline demographic or clinical variablesbetween the graduates and the non-graduates. For the AN group, the gradu-ates were significantly younger than the non-graduates. They had also beenill for a significantly shorter period of time but had a higher rate of past hos-pitalizations than the non-graduates. The graduates with AN also endorsedmore frequent restricting behaviors and less frequent enema abuse than thenon-graduates. It appears that patients with enema abuse find it harder totolerate the constraints of residential care and are more likely to leave treat-ment prematurely. Otherwise, there were no significant differences in any ofthe baseline EDI-2 subscale scores, BDI scores, or self-reported frequenciesof bingeing, vomiting, chewing and spitting, exercising, or abuse of laxa-tives, diuretics, ipecac or stimulants. For the BN group, the two groups werealso very similar in terms of clinical and demographic variables. The onlydifference was a greater mean frequency of stimulant abuse in the gradu-ates compared to the non-graduates. Overall, these findings suggest that thegraduates were just as sick as or sicker than the non-graduates.
Lastly, we do not report any follow-up data in this article, so it isunknown at this time whether the improvements reported in this sam-ple have any long-lasting therapeutic effects. However, we plan to analyzeresults of assessment surveys following long-term follow-up after dischargeto investigate the extent to which patients maintain their recovery. In addi-tion, we plan to explore the role of a number of possible positive andnegative prognostic factors, including comorbid diagnoses, age of onset,duration of illness, length of stay, and attendance at our transitional treat-ment program. In addition, once our sample sizes expand, we intend toanalyze the effects of residential treatment on patients with eating disordernot otherwise specified (EDNOS), as our current sample size was too smalland diverse to show meaningful statistical results.
REFERENCES
American Psychiatric Association (2006). Treatment of patients with eating disorders,third edition. American Journal of Psychiatry, 163(7 Suppl), 4–54.
Andersen, A. E. (1986). Inpatient and outpatient treatment of anorexia nervosa. InK. D. Brownell & J. P. Foreyt (Eds.), Handbook of eating disorders: Physiology,psychology, and treatment of obesity, anorexia and bulimia. New York, NY:Basic Books.
Downloaded By: [Brewerton, Timothy D.] At: 16:16 24 February 2011

130 T. D. Brewerton and C. Costin
Andersen, A. E., Bowers, W. A., & Evans, K. K. (1997). Inpatient treatment ofanorexia nervosa. In D. M. Garner & P. E. Garfinkel (Eds.), Handbook oftreatment for eating disorders (2nd ed., pp. 327–353). New York, NY: Guilford.
Andersen, A. E., Morse, C., & Santmyer, K. (1985). Inpatient treatment of anorexianervosa. In D. M. Garner DM & P. E. Garfinkel (Eds.), Handbook of psy-chotherapy for anorexia nervosa and bulimia (pp. 311–343). New York, NY:Guilford.
Bares, M., Brunovsky, M., Kopecek, M., Novak, T., Stopkova, P., Kozeny, J., . . .Hoschl, C. (2008). Early reduction in prefrontal theta QEEG cordance valuepredicts response to venlafaxine treatment in patients with resistant depres-sive disorder. European Psychiatry: The Journal of the Association of EuropeanPsychiatrists, 23, 350–355.
Bares, M., Brunovsky, M., Kopecek, M., Stopkova, P., Novak, T., Kozeny, J., &Hoschl, C. (2007). Changes in QEEG prefrontal cordance as a predictor ofresponse to antidepressants in patients with treatment resistant depressivedisorder: A pilot study. Journal of Psychiatric Research, 41, 319–325.
Bean, P., Welk, R., Hallinan, P., Cornella-Carlson, T., Weisensel, N., & Weltzin, T.(2008). The effects of a multidisciplinary approach to treatment in the recoveryof males and females diagnosed with anorexia nervosa in the presence andabsence of co-morbid obsessive compulsive disorders. Journal of Groups inAddiction & Recovery, 3, 305–321.
Beck, A. T., Steer, R. A., & Brown, G. K. (1996). The Beck Depression Inventorymanual (2n ed.). San Antonio, TX: Psychological Corporation Harcourt Brace& Company.
Bowers, W., Andersen, A., & Evans, K. (2004). Management of eating disorders:Inpatient and partial hospital programs. In T. D. Brewerton (Ed.), Clinical hand-book of eating disorders: An integrated approach (pp. 349–376). New York, NY:Marcel Dekker.
Costin, C. (1996). The eating disorders source book: A comprehensive guide to thecauses, treatments, and prevention of eating disorders (1st ed.). Los Angeles,CA: Lowell House.
Costin, C. (2007). The eating disorders source book: A comprehensive guide to thecauses, treatments, and prevention of eating disorders (3rd ed.). New York,NY: McGraw-Hill.
Garner, D. M. (1991). Eating Disorder Inventory-2 professional manual. Odessa, FL:Psychological Assessment Resources.
Garner, D. M., Garfinkel, P. E., & Irvine, M. J. (1986). Integration and sequencing oftreatment approaches for eating disorders. Psychotherapy and Psychosomatics,46 , 67–75.
Garner, D. M., Olmsted, M. P. & Polivy, J. (1983). Development and validation of amultidimensional eating disorders inventory for anorexia nervosa and bulimia.International Journal of Eating Disorders, 2, 15–34.
Garrett, C. J. (1997). Sociological perspectives on recovery from anorexia nervosa.International Journal of Eating Disorders, 21, 261–272.
Garrett, C. J. (1998). Beyond anorexia: Narrative, spirituality and recovery.Cambridge, UK: Cambridge University Press.
Downloaded By: [Brewerton, Timothy D.] At: 16:16 24 February 2011

Anorexia Nervosa and Bulimia Nervosa in Residential Treatment 131
Gleaves, D. H., Post, G. K., Eberenz, K. P., & Davis, W. N. (1993). A report of 497women hospitalized for treatment of bulimia nervosa. Eating Disorders: TheJournal of Treatment and Prevention, 1, 134–146.
Hunter, A. M., Cook, I. A., & Leuchter, A. F. (2007). The promise of the quantitativeelectroencephalogram as a predictor of antidepressant treatment outcomes inmajor depressive disorder. Psychiatric Clinics of North America, 30, 105–124.
LaVia, M., Kaye, W. H., Andersen, A., Bowers, W., Brandt, H. A., Brewerton, T. D.,. . . Zucker, M. L. (1998, November). Anorexia nervosa: Criteria for levels ofcare. Paper presented at the Annual Meeting of the Eating Disorders ResearchSociety, Cambridge, MA.
Leuchter, A. F., Cook, I. A., Gilmer, W. S., Marangell, L. B., Burgoyne, K. S., Howland,R. H., . . . Greenwald, S. (2009a). Effectiveness of a quantitative electroen-cephalographic biomarker for predicting differential response or remission withescitalopram and bupropion in major depressive disorder. Psychiatry Research,169, 132–138.
Leuchter, A. F., Cook, I. A., Marangell, L. B., Gilmer, W. S., Burgoyne, K. S., Howland,R. H., . . . Greenwald, S. (2009b). Comparative effectiveness of biomarkers andclinical indicators for predicting outcomes of SSRI treatment in Major DepressiveDisorder: Results of the BRITE-MD study. Psychiatry Research, 169, 124–131.
Lowe, M. R., Davis, W. N., Annunziato, R. A., & Lucks, D. L. (2003). Inpatienttreatment for eating disorders: Outcome at discharge and 3-month follow-up.Eating Behaviors, 4, 385–397.
National Collaborating Centre for Mental Health. (2004). Eating disorders: Coreinterventions in the treatment and management of anorexia nervosa, bulimianervosa and related eating disorders. In National clinical practice guidelinenumber CG9, National Institute for Clinical Excellence (NICE) (pp. 1–35).Leicester, UK: The British Psychological Society and Gaskell.
Redenbach, J., & Lawler, J. (2003). Recovery from disordered eating: What historiesreveal. Contemporary Nurse, 15, 148–156.
Vandereycken, W. (1985). Inpatient treatment of anorexia nervosa: Some researchguided changes. Journal of Psychiatric Research, 19, 413–422.
Downloaded By: [Brewerton, Timothy D.] At: 16:16 24 February 2011
Related Documents