Treatment Resistant Treatment Resistant Pediatric BD Pediatric BD Elham Shirazi M.D. Board of General Psychiatry Board of Child & Adolescent Psychiatry

Treatment Resistant Pediatric BD Elham Shirazi M.D. Board of General Psychiatry Board of Child & Adolescent Psychiatry.
Jan 14, 2016
Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

Treatment Resistant Treatment Resistant Pediatric BDPediatric BD
Elham Shirazi M.D.
Board of General Psychiatry
Board of Child & Adolescent Psychiatry

Pediatric BD:
Less adequate treatment response
More prolonged & treatment-refractory course
More relapse rates
More recurrent & intractable
More episodes over the course of a year
Reduced interepisode recovery
Factors associated with nonresponse:
1. Misdiagnosis
2. Poor adherence to treatment
3. Comorbid psychiatric and medical conditions
4. Ongoing exposure to negative events (family conflict, abuse)
5. Quality of treatment

Consider whether symptoms persist as a result of:
Inadequate response to treatment
Or as an expected response to inadequate treatment

Step 1
Discontinue potentially destabilizing agents:
Antidepressants
Can promote mania, mixed states, or rapid cycling in children/ adolescents with BD
Can increase the frequency & severity of mood symptoms
(Russel E. Scheffer, 2011)
Stimulants
Can be problematic in patients at risk for BD disorder.
Try to discontinue stimulants while stabilizing patients’ mood symptoms
Once the patient’s mood symptoms are controlled on a mood stabilizer regimen
Using stimulants for comorbid ADHD did not affect relapse rate
(Russel E. Scheffer, 2011)
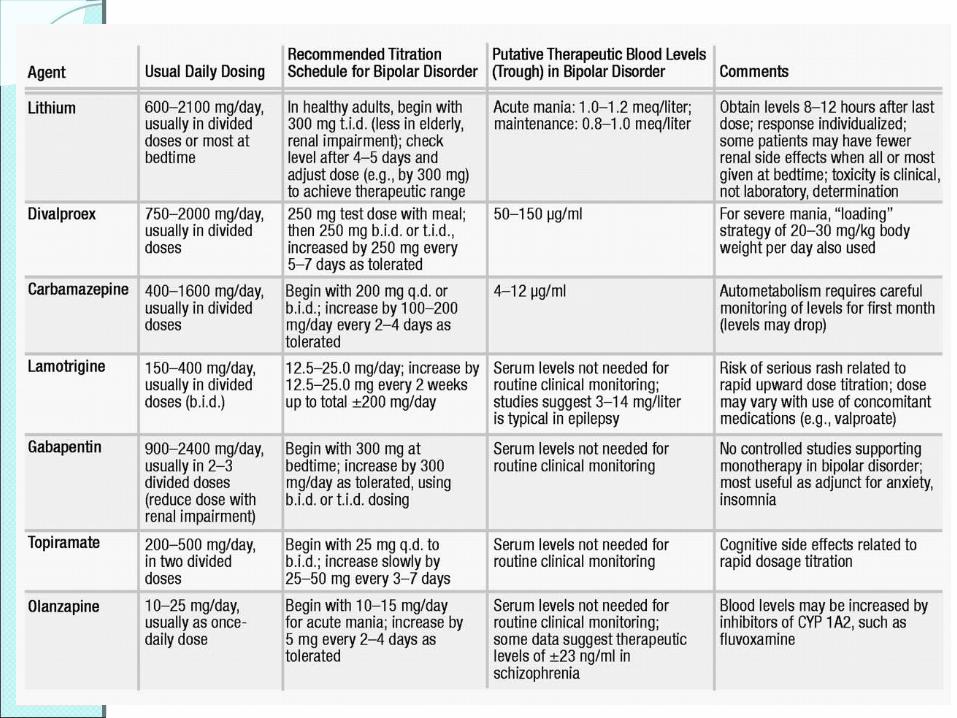
Step 2 Optimize the antimanic agents the patient is currently
receiving:
Serum Li levels between 0.8–1.2 mEq/dl
VPA levels between 80–120 mEq/dl
Risperidone up to 4 mg/day
Olanzapine up to 20 mg/day
Quetiapine up to 800 mg/day
Now lack of adequate response after a 4-week trial is a “true” treatment failure.
(Russel E. Scheffer, 2011)

If there is no improvement on a treatment after several months, don’t continue that treatment
Use combinations other than the one that hasn’t worked
For partial or nonresponders to monotherapy:
Combination of 2 mood stabilizers
Or of a mood stabilizer with an atypical antipsychotic is indicated
Medication combinations are additive both in:
Effectiveness
& in side effects

If remission is achieved on a particular regimen, it should be continued as long as possible
At least until the child/adolescent has navigated his most important develpmental, academic, & social milestones.
Majority of subjects relapse after the switch to monotherapy
A child stabilized on 2 medications needs to be maintained as such since the relapse rate on one drug is high.
Even in most treatment responsive youth with PBD, it is common to need 2 mood stabilizers
Lithium alone has not been successful in this age group as a maintenance medication.

BD + ADHD?
In cases where clinicians can not decide between mania & ADHD:
If the child becomes more irritable or aggressive with ADHD treatment
Use an atypical antipsychotic or a mood stabilizer
Followed by retrying the ADHD treatment
Keep in mind that “rebound”
the apparent return of worse ADHD symptoms at the end of the day
Has no diagnostic implications
& sometimes subsides over time
(Carlson 2003)

First-line medication for BP depression:
Lamotrigine
Lithium
Valproate
Atypical antipsychotics
For partial or non-responders combine with:
Another atypical antipsychotics
SSRIs
Bupropion
DMDD + ADHD + ODD
Comorbid DBD predict a poorer response to treatment.
(Masi 2004, State 2004)
A treatment algorithm for ADHD & aggression might be a reasonable course of action (Carlson 2007)
Antimanic medications have efficacy as antiaggression medication.
Clozapine:
Is reserved for the most treatment-resistant cases
Because of its side-effect profile.
TMS or augmentation with omega-3 fatty acids are yet to be evaluated for treatment of BP depression in youth.
ECT:
May be indicated for adolescents with severe & most treatment resistant disorders
Considered for adolescents with well-characterized BDI who have:
Severe episodes of mania or depression
Are nonresponsive
Or unable to take standard medication therapies.

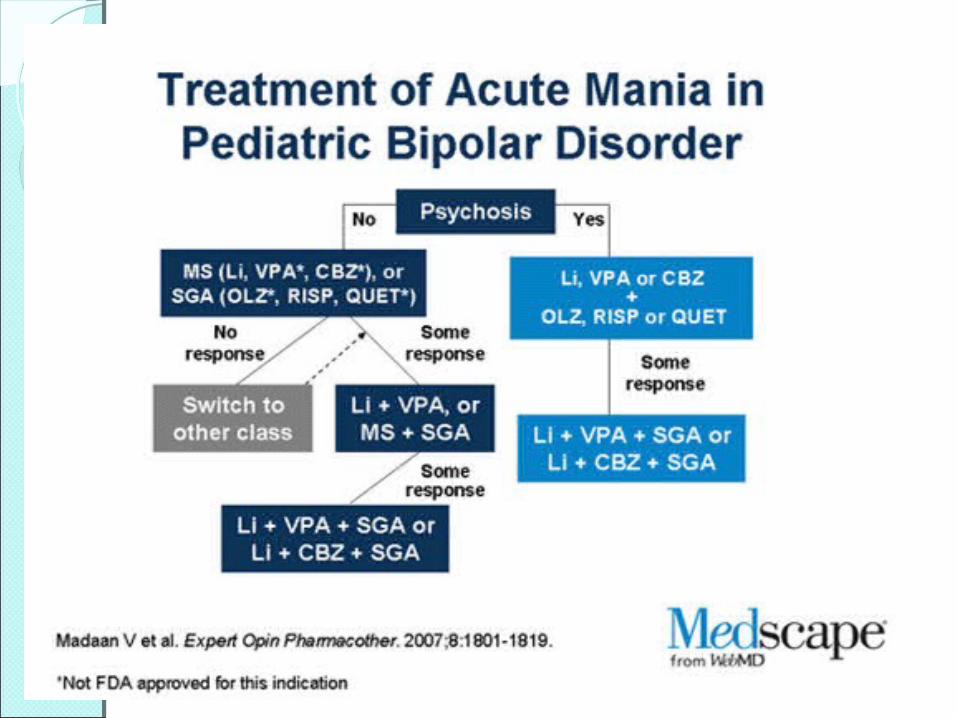
For subjects who do not respond to the initial monotherapy:
Treat with one of the other mood stabilizers
Or an atypical antipsychotic not previously tried
For subjects with a partial response to monotherapy:
Combination of 2 mood stabilizers
Or of a mood stabilizer with an atypical antipsychotic is indicated

Even in most treatment responsive youth with PBD, it is common to need 2 mood stabilizers
& a stimulant to treat ADHD symptoms.
The clinical course of PBD includes many affective & behavioral bumps.
If you attempt to treat all of these bumps it results in excessive polypharmacy.
(Russel E. Scheffer, 2011)
Also discontinue GABA-ergic agents
Gabapentin, Tiagabine, Levetiracetam, Pregabalin
GABA-ergic agents frequently cause disinhibition in children
Are not effective in treating manic symptoms
(Russel E. Scheffer, 2011)

Step 3
Use a limited number of mood stabilizers (one or two)
Nonconventional & empirically unsupported medications (e.g., oxcarbazepine) are discontinued
& replaced with a first-line treatment agent (e.g., Li, VPA, risperidone, olanzapine, or quetiapine)
(Russel E. Scheffer, 2011)
Related Documents











