Treatment of Pediatric Airway Disorders: Beyond Tracheostomy Meredith N. Merz, M.D. Nationwide Children’s Hospital Department of Pediatric Otolaryngology April 6, 2011

Treatment of Pediatric Airway Disorders: Beyond Tracheostomy
Dec 31, 2015
Treatment of Pediatric Airway Disorders: Beyond Tracheostomy. Meredith N. Merz, M.D. Nationwide Children’s Hospital Department of Pediatric Otolaryngology April 6, 2011. Objectives. 1. Identify the most common causes of stridor in the pediatric population. - PowerPoint PPT Presentation
Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

Treatment of Pediatric Airway Disorders: Beyond TracheostomyMeredith N. Merz, M.D.Nationwide Children’s HospitalDepartment of Pediatric OtolaryngologyApril 6, 2011

Objectives
1. Identify the most common causes of stridor in the pediatric population.
2. Discuss diagnostic techniques in a child with stridor.3. Understand the pathogenesis of acquired subglottic stenosis and the difference between congenital and acquired stenosis.
4. Discuss treatment options for the most common airway disorders in children.

Laryngeal Function
• Three Main Functions:Three Main Functions:1. Acts as an airway from pharynx 1. Acts as an airway from pharynx into trachea and lungsinto trachea and lungs
2. Instrument of phonation2. Instrument of phonation3. Protects the lower airways3. Protects the lower airways
• Closure of glottis during swallowingClosure of glottis during swallowing• Epiglottis folds posteriorly over Epiglottis folds posteriorly over glottisglottis
• CoughCough

Infant Larynx
• Larynx is more rostralLarynx is more rostral• Epiglottis apposes the soft palateEpiglottis apposes the soft palate• Hyoid bone is impacted on thyroid cartilageHyoid bone is impacted on thyroid cartilage• Vocal cords are oriented transverselyVocal cords are oriented transversely• Epiglottis is short and curled in on itselfEpiglottis is short and curled in on itself• Arytenoids are anteriorly oriented and involve half Arytenoids are anteriorly oriented and involve half the length of the vocal foldsthe length of the vocal folds

Infant Larynx
Bosma JF. Anatomy of the Infant Head. Baltimore, Johns Hopkins University Press, 1986, pp 366-367.

Stridor
• Harsh sound caused by turbulent airflowHarsh sound caused by turbulent airflow• Implies Implies partialpartial airway obstruction airway obstruction• Location of lesion determines character of stridorLocation of lesion determines character of stridor
o SupraglotticSupraglottico ExtrathoracicExtrathoracico IntrathoracicIntrathoracic

Physics Review…
• Poiseuille’s LawPoiseuille’s LawQ = [Q = [ππdd44 (P1-P2)] / 128 (P1-P2)] / 128νν
Flow within a system is related to the radius of the tube to the Flow within a system is related to the radius of the tube to the fourth powerfourth power
Resistance is related to the inverse of the radius to the fourth Resistance is related to the inverse of the radius to the fourth powerpower
• Bernouilli’s Law:Bernouilli’s Law:W = PAvW = PAv
As velocity increases through a constant area the pressure on the As velocity increases through a constant area the pressure on the wall of the lumen decreaseswall of the lumen decreases
A region of anatomic narrowing is predisposed to collapse further A region of anatomic narrowing is predisposed to collapse further with increased turbulent airflowwith increased turbulent airflow

Effect of Airway Narrowing

Localizing Stridor
• Supraglottic obstructionSupraglottic obstructiono With inspiration the loosely supported supraglottic structures collapse. With inspiration the loosely supported supraglottic structures collapse. Increased turbulence causes increased constriction Increased turbulence causes increased constriction
o Stridor is inspiratory and high pitchedStridor is inspiratory and high pitched• Extrathoracic obstructionExtrathoracic obstruction
o Airway is affected equally by inspiration and expirationAirway is affected equally by inspiration and expirationo Stridor is biphasic, often accompanied by increased work of breathingStridor is biphasic, often accompanied by increased work of breathing
• Intrathoracic obstructionIntrathoracic obstructiono Relative positive pressures of expiratory forces narrow the airway Relative positive pressures of expiratory forces narrow the airway lumen, resulting in increased constrictionlumen, resulting in increased constriction
o Stridor is expiratory and “musical”; WheezeStridor is expiratory and “musical”; Wheeze

Airway Evaluation- History
• Age at onsetAge at onset• Onset: acute, chronic, progressiveOnset: acute, chronic, progressive• Prior respiratory problemsPrior respiratory problems• Birth historyBirth history• Prior intubationPrior intubation• GERD symptomsGERD symptoms• Wheezing episodesWheezing episodes• Feeding problems:Feeding problems:
o FTT, weight gainFTT, weight gain• Choking episodesChoking episodes• Aggravating factorsAggravating factors

Airway Evaluation- Initial Examination
• InspectionInspectiono General appearance and position, color, retractions, level of General appearance and position, color, retractions, level of consciousnessconsciousness
• AuscultationAuscultationo Mouth/Nose, Neck and ChestMouth/Nose, Neck and Chest
• RepositioningRepositioningo Prone/Supine, lateral, jaw thrustProne/Supine, lateral, jaw thrust
• Is there acute distress?Is there acute distress?o Nasal flaringNasal flaringo TachypneaTachypneao CyanosisCyanosiso RetractionsRetractionso Tripod positionTripod position
Flexible Nasopharyngoscopy
• Gold Standard for Gold Standard for office evaluationoffice evaluation
• Assess nares/ choanaeAssess nares/ choanae• Assess adenoid and Assess adenoid and lingual tonsillingual tonsil
• Assess laryngeal Assess laryngeal structuresstructures
• Assess TVC mobilityAssess TVC mobility• Drawback:Drawback:
Poor for assessing Poor for assessing subglottic structuressubglottic structures

Radiologic Evaluation
• Plain films have limited utilityPlain films have limited utilityo PA/ Lateral NeckPA/ Lateral Neck
• Airway FluoroscopyAirway Fluoroscopyo Evaluate the dynamics of Evaluate the dynamics of respirationrespiration
• Inspiratory/ Expiratory CT ScanInspiratory/ Expiratory CT Scan

Rigid Laryngoscopy and Bronchoscopy
• Indications:Indications:o To establish diagnosis or evaluate for synchronous lesions To establish diagnosis or evaluate for synchronous lesions (after flexible exam)(after flexible exam)
o Severe or progressive stridorSevere or progressive stridoro Cyanosis or apnea concernsCyanosis or apnea concernso Radiologic abnormalitiesRadiologic abnormalitieso Parental or physician anxietyParental or physician anxietyo Foreign body evaluationForeign body evaluation

Rigid Laryngosocpy
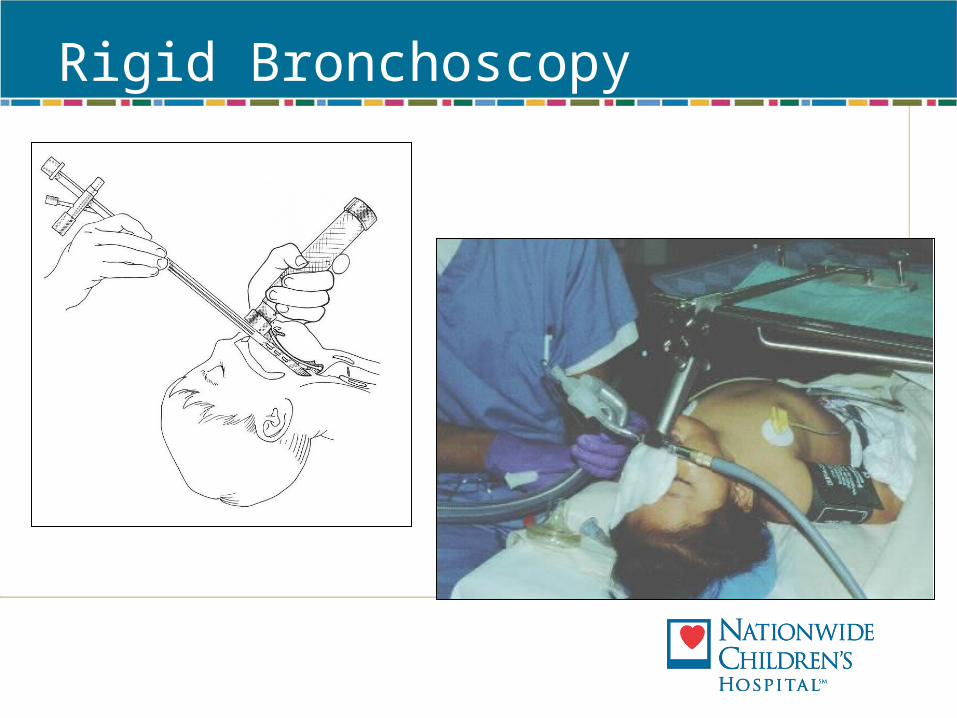
Rigid Bronchoscopy

Congenital Disorders of the Larynx
• LaryngomalaciaLaryngomalacia 60%60%• Congenital subglottic stenosisCongenital subglottic stenosis 16%16%• Vocal cord paralysisVocal cord paralysis 13%13%• All Others:All Others: 7%7%
o Congenital laryngeal webCongenital laryngeal webo Laryngocele and Saccular cystLaryngocele and Saccular cysto Laryngeal/ Laryngotrachealesophogeal CleftLaryngeal/ Laryngotrachealesophogeal Clefto Vascular lesionsVascular lesions
Holinger, LD. Etiology of Stridor in the Newborn, Infant, and Child. Annals of ORL, 1980; 89: 397-400.

Laryngomalacia
• Most common cause of stridor in infantsMost common cause of stridor in infants• PresentationPresentation
o Staccato/ Coarse inspiratory stridorStaccato/ Coarse inspiratory stridoro Worse with exertion, feeding, cryingWorse with exertion, feeding, cryingo Noisy breathing generally begins at about 2-4 weeks of ageNoisy breathing generally begins at about 2-4 weeks of age
• Office EvaluationOffice Evaluationo Character of stridorCharacter of stridoro Positional changesPositional changeso Flexible nasopharyngoscopyFlexible nasopharyngoscopy

Laryngomalacia
• Endoscopic appearanceEndoscopic appearanceo Omega epiglottisOmega epiglottiso Foreshortenend aryepiglottic foldsForeshortenend aryepiglottic foldso Cuneiform and corniculate prolapseCuneiform and corniculate prolapse

Laryngomalacia Classification
Kay DJ, Goldsmith AJ. Laryngomalacia: A Classification System and Surgical Treatment Strategy. Ear Nose Throat J. 2006 May;85(5):328-31, 336.
Type I Type II Type III
Type IV Type V

Laryngomalacia
• Vast majority are Vast majority are mildmild• Parental reassurance & educationParental reassurance & education
o Transient worsening, gradual improvementTransient worsening, gradual improvemento Weight gain issuesWeight gain issueso GERD issues- Consider GERD treatment if there is evidence GERD issues- Consider GERD treatment if there is evidence on endoscopyon endoscopy
Severe Laryngomalacia
• Respiratory difficultyRespiratory difficultyo Apnea/ Cyanosis/ ALTEApnea/ Cyanosis/ ALTE
• Feeding difficultyFeeding difficulty• Failure to thriveFailure to thrive• Uncontrolled GERDUncontrolled GERD• Sleep apneaSleep apnea• CNS abnormalitiesCNS abnormalities

Severe LaryngomalaciaSurgical Treatment
• Supraglottoplasty- Aryepiglottic fold division +/- Excision of corniculate cartilages
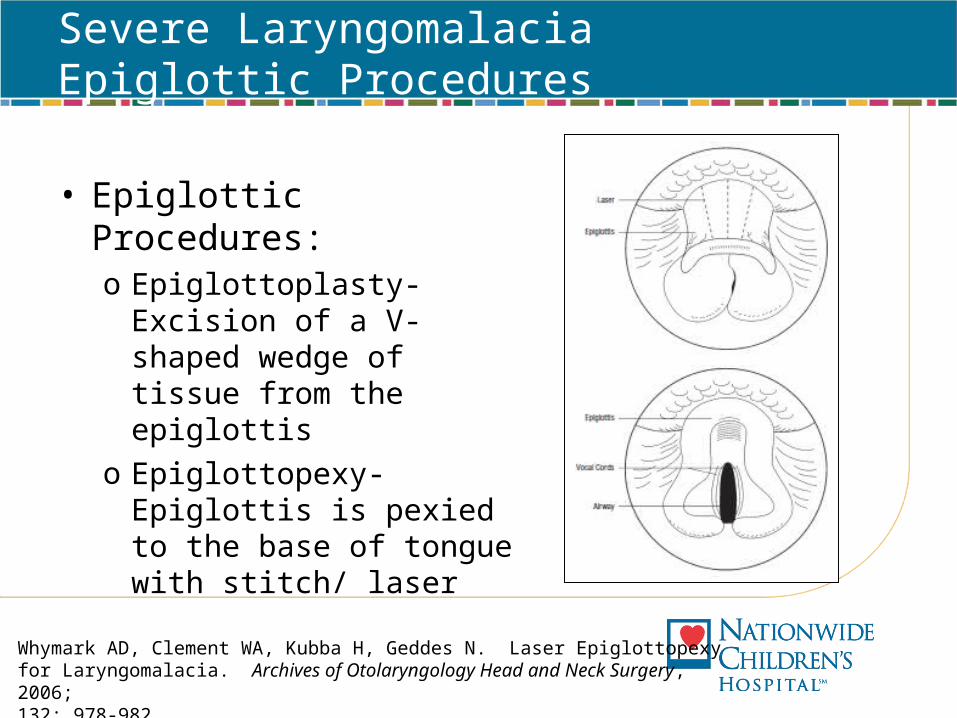
Severe LaryngomalaciaEpiglottic Procedures
• Epiglottic Procedures:o Epiglottoplasty- Excision of a V-shaped wedge of tissue from the epiglottis
o Epiglottopexy- Epiglottis is pexied to the base of tongue with stitch/ laser
Whymark AD, Clement WA, Kubba H, Geddes N. Laser Epiglottopexy for Laryngomalacia. Archives of Otolaryngology Head and Neck Surgery, 2006; 132: 978-982.

Vocal Cord Paralysis
• Bilateral: Airway issues, Bilateral: Airway issues, Aspiration issuesAspiration issueso Expectant (can take years Expectant (can take years to resolve)to resolve)o Close monitoring of OClose monitoring of O22 sat, sat, apnea, weight gainapnea, weight gaino TracheotomyTracheotomyo Posterior laryngeal Posterior laryngeal expansionexpansiono Botox (for spastic paralysis)Botox (for spastic paralysis)o CordotomyCordotomyo ArytenoidectomyArytenoidectomyo Re-innervation proceduresRe-innervation procedures
• Unilateral: Voice Issues, Unilateral: Voice Issues, Aspiration IssuesAspiration Issueso ObservationObservationo Vocal Cord InjectionVocal Cord Injectiono ThyroplastyThyroplasty
Related Documents









![Management of Pediatric Tracheostomy - · PDF fileManagement of Pediatric Tracheostomy ... dressing care – Surgical ... ppt-Dr.Mehta-Pediatric tracheostomy [Compatibility Mode] Author:](https://static.cupdf.com/doc/110x72/5a724bb37f8b9ab6538d5678/management-of-pediatric-tracheostomy-aocoohnswwwaocoohnsorgwp-contentuploads2014095794adpdf.jpg)

