PLEASE SCROLL DOWN FOR ARTICLE This article was downloaded by: [Canadian Research Knowledge Network] On: 10 October 2009 Access details: Access Details: [subscription number 783016864] Publisher Routledge Informa Ltd Registered in England and Wales Registered Number: 1072954 Registered office: Mortimer House, 37-41 Mortimer Street, London W1T 3JH, UK Cognitive Behaviour Therapy Publication details, including instructions for authors and subscription information: http://www.informaworld.com/smpp/title~content=t713926011 Treatment of Panic Disorder with Agoraphobia: Randomized Placebo- Controlled Trial of Four Psychosocial Treatments Combined with Imipramine or Placebo André Marchand ab ; Marie-France Coutu c ; Gilles Dupuis ad ; Richard Fleet ae ; François Borgeat b ; Christo Todorov b ; Nicole Mainguy b a Psychology Department, University of Quebec in Montreal, Montreal, Quebec b Fernand Seguin Resarch Center, Louis-H. Lafontaine Hospital, Montreal, Quebec c Université de Sherbrooke, Sherbrooke, Quebec d Montreal Heart Institute, Montreal, Quebec e Anxiety Disorder Clinic, Sacré-Coeur Hospital, Montreal, Quebec, Canada Online Publication Date: 01 September 2008 To cite this Article Marchand, André, Coutu, Marie-France, Dupuis, Gilles, Fleet, Richard, Borgeat, François, Todorov, Christo and Mainguy, Nicole(2008)'Treatment of Panic Disorder with Agoraphobia: Randomized Placebo-Controlled Trial of Four Psychosocial Treatments Combined with Imipramine or Placebo',Cognitive Behaviour Therapy,37:3,146 — 159 To link to this Article: DOI: 10.1080/16506070701743120 URL: http://dx.doi.org/10.1080/16506070701743120 Full terms and conditions of use: http://www.informaworld.com/terms-and-conditions-of-access.pdf This article may be used for research, teaching and private study purposes. Any substantial or systematic reproduction, re-distribution, re-selling, loan or sub-licensing, systematic supply or distribution in any form to anyone is expressly forbidden. The publisher does not give any warranty express or implied or make any representation that the contents will be complete or accurate or up to date. The accuracy of any instructions, formulae and drug doses should be independently verified with primary sources. The publisher shall not be liable for any loss, actions, claims, proceedings, demand or costs or damages whatsoever or howsoever caused arising directly or indirectly in connection with or arising out of the use of this material.

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

PLEASE SCROLL DOWN FOR ARTICLE
This article was downloaded by: [Canadian Research Knowledge Network]On: 10 October 2009Access details: Access Details: [subscription number 783016864]Publisher RoutledgeInforma Ltd Registered in England and Wales Registered Number: 1072954 Registered office: Mortimer House,37-41 Mortimer Street, London W1T 3JH, UK
Cognitive Behaviour TherapyPublication details, including instructions for authors and subscription information:http://www.informaworld.com/smpp/title~content=t713926011
Treatment of Panic Disorder with Agoraphobia: Randomized Placebo-Controlled Trial of Four Psychosocial Treatments Combined with Imipramine orPlaceboAndré Marchand ab; Marie-France Coutu c; Gilles Dupuis ad; Richard Fleet ae; François Borgeat b; ChristoTodorov b; Nicole Mainguy b
a Psychology Department, University of Quebec in Montreal, Montreal, Quebec b Fernand Seguin ResarchCenter, Louis-H. Lafontaine Hospital, Montreal, Quebec c Université de Sherbrooke, Sherbrooke, Quebec d
Montreal Heart Institute, Montreal, Quebec e Anxiety Disorder Clinic, Sacré-Coeur Hospital, Montreal,Quebec, Canada
Online Publication Date: 01 September 2008
To cite this Article Marchand, André, Coutu, Marie-France, Dupuis, Gilles, Fleet, Richard, Borgeat, François, Todorov, Christo andMainguy, Nicole(2008)'Treatment of Panic Disorder with Agoraphobia: Randomized Placebo-Controlled Trial of Four PsychosocialTreatments Combined with Imipramine or Placebo',Cognitive Behaviour Therapy,37:3,146 — 159
To link to this Article: DOI: 10.1080/16506070701743120
URL: http://dx.doi.org/10.1080/16506070701743120
Full terms and conditions of use: http://www.informaworld.com/terms-and-conditions-of-access.pdf
This article may be used for research, teaching and private study purposes. Any substantial orsystematic reproduction, re-distribution, re-selling, loan or sub-licensing, systematic supply ordistribution in any form to anyone is expressly forbidden.
The publisher does not give any warranty express or implied or make any representation that the contentswill be complete or accurate or up to date. The accuracy of any instructions, formulae and drug dosesshould be independently verified with primary sources. The publisher shall not be liable for any loss,actions, claims, proceedings, demand or costs or damages whatsoever or howsoever caused arising directlyor indirectly in connection with or arising out of the use of this material.

Treatment of Panic Disorder with Agoraphobia:Randomized Placebo-Controlled Trial of Four
Psychosocial Treatments Combined with Imipramine orPlacebo
Andre Marchand1,2, Marie-France Coutu3, Gilles Dupuis1,4, Richard Fleet1,5,Francois Borgeat2, Christo Todorov2 and Nicole Mainguy2
1Psychology Department, University of Quebec in Montreal, Montreal, Quebec; 2FernandSeguin Resarch Center, Louis-H. Lafontaine Hospital, Montreal, Quebec; 3Universite de
Sherbrooke, Sherbrooke, Quebec; 4Montreal Heart Institute, Montreal, Quebec; and5Anxiety Disorder Clinic, Sacre-Coeur Hospital, Montreal, Quebec, Canada
Abstract. Few randomized controlled trials have included panic disorder patients with moderate tosevere agoraphobia. Therefore, this population was studied using pharmacotherapy as well aspsychotherapy. At the time of the study, imipramine was widely used as a pharmacologicaltreatment. Also, current practice guidelines for patients with panic disorder find selective serotoninreuptake inhibitors and tricyclic antidepressants roughly comparable in terms of efficacy. Therefore,the main objective of this study is to compare four psychosocial treatments—cognitive and graded invivo exposure treatments, graded in vivo exposure, cognitive treatment, and supportive therapy—toevaluate the benefits of combining cognitive therapy with exposure in vivo. These treatments werecombined with imipramine or placebo for a total of eight experimental conditions. Participantspresented moderate to severe agoraphobia. The method involved a randomized, double-blind,placebo-controlled trial with 137 participants who completed a 14-session protocol involving thetreatments just mentioned. Measures were taken at baseline and posttreatment and at 3-, 6-, and 12-month follow-up. All treatment conditions were statistically and clinically effective in reducing self-reported panic–agoraphobia symptoms over the 1-year follow-up. No statistical differences wereobserved between imipramine and placebo conditions. This study found that all treatment modalitieshelped reduce panic and agoraphobic symptomatology over a 1-year follow-up period. Thesesurprising results support the need to document the relations among the various components of anintervention. This would make it possible to assess the relative efficacy of the treatment componentsrather than of the intervention as a whole. Key words: panic disorder; agoraphobia; adult; combinedmodality therapy; imipramine; graded exposure; cognitive therapy; follow-up study; treatment outcome.
Received 8 November, 2006; Accepted 10 October, 2007
Correspondence address: Andre Marchand, PhD, Universite du Quebec a Montreal, Departement dePsychologie, C.P. 8888, Succ. Centre-Ville, Montreal, Quebec H3C 3P8, Canada. Tel: +514 987 3000,ext. 8439. Fax: +514 987 7953. E-mail: [email protected]
Panic disorder (PD) and panic disorder withagoraphobia (PDA) are among the mostcommon and disabling anxiety disorders.Lifetime prevalence rates are 4.7% in thegeneral population (Kessler et al., 2005).Significantly higher rates, ranging from 8%to 60%, have been reported in various medical
settings, where patients primarily seek carebecause their panic symptoms mimic those ofa long list of cardiovascular, gastrointestinal,and neurological disorders (Zaubler & Katon,1996). Unfortunately, PD often goes unrecog-nized by nonpsychiatric physicians, anduntreated patients suffer chronically (Fleet
# 2008 Taylor & Francis ISSN 1650-6073DOI 10.1080/16506070701743120
Cognitive Behaviour Therapy Vol 37, No 3, pp. 146–159, 2008
Downloaded By: [Canadian Research Knowledge Network] At: 17:21 10 October 2009

et al., 1996). On average, patients have sufferedfrom their disorder for approximately a decadebefore receiving treatment in a mental healthsetting (Swinson & Koch, 1990). When PD isfinally suspected and patients are referred fortreatment in mental health clinics, their PDhas, in most cases, been complicated bymoderate to severe agoraphobic avoidance aswell as other Axis I and Axis II disorders(Brown & Barlow, 1992).
Effective treatments exist for PD patientswith no to mild agoraphobic avoidance(Barlow, Groman, Shear, & Woods, 2000;White & Barlow, 2002). Surprisingly, fewrandomized controlled trials (RCTs) haveevaluated these treatments for patients withmoderate to severe agoraphobia, which ispresumably a more representative sample ofthe psychiatric clinic population (Swinson,Cox, Kerr, Kuch, & Fergus, 1992). The fewRCTs that have included PD patients withmoderate to severe agoraphobia (Cottrauxet al., 1995; de Beurs, van Balkom, Lange,Koele, & van Dyck, 1995; Loerch et al., 1999;L. K. Michelson, Marchione, Greenwald,Testa, & Marchione, 1996; Oehrberg et al.,1995; Wardle et al., 1994; Williams & Falbo,1996) suggest that the level of agoraphobicavoidance is inversely related to the outcomeof the treatment (de Beurs et al., 1995; L. K.Michelson et al., 1996; Wardle et al., 1994;Williams & Falbo, 1996). In these studies,severe agoraphobic patients showed lessimprovement at posttreatment comparedwith mild agoraphobic patients. However,findings revealed improvement in PD patientswith moderate to severe agoraphobia whencognitive–behavioural treatment (CBT) isoffered with medication (American PsychiatricAssociation, 1998; Cottraux et al., 1995;Loerch et al., 1999; Oehrberg et al., 1995).Nonetheless, after reviewing RCTs based onCBT and PD, the American PsychiatricAssociation Work Group on Panic Disorder(American Psychiatric Association, 1998)suggested the need for further study of thespecific use of CBT interventions and theirefficacy.
During the 1980s and early 1990s, researchon combined treatment focused on the bene-fits of tricyclic antidepressants such as imi-pramine (Marchand & Boivin, 1999).Imipramine is used to decrease the intensityand frequency of panic attacks as well as to
lower anticipatory anxiety and comorbiddepression (American Psychiatric Associ-ation, 1998). In fact, studies showed specificand clinically significant differences in panicand agoraphobia symptoms when comparedwith the benefits of placebo treatments. Thesestudies also revealed a dose-dependentresponse (Mavissakalian & Perel, 1995). ByWeek 4, medium- and high-dose patients hadsignificantly improved in terms of dyspnea,choking, and fear (pv0.001) compared withthe placebo and low-dose groups. Chest pain,dizziness, fainting, and trembling symptomshad also significantly improved (p50.005)compared with the placebo and low-dosegroups (Mavissakalian, 1996). Imipraminehas also demonstrated a high degree ofprophylactic effectiveness (Mavissakalian &Perel, 1999). Of the 56 patients who were inremission and who consented to be randomlyassigned to either placebo or maintenancetreatment, only 1 (of 29 [3%]) in the main-tenance treatment group relapsed after 1 yearcompared with 10 (37%) in the placebo group(Mavissakalian & Perel, 1999). These resultsare comparable to the relapse rate (3%) foundwith fluoxetine (D. Michelson et al., 1999). Inpatients who discontinued paroxetine, theobserved relapse rate was higher than 30%,which is still comparable to that of theplacebo group (D. Michelson et al., 1999).In fact, the practice guidelines for the treat-ment of patients with panic disorder findselective serotonin reuptake inhibitors (SSRIs)and tricyclic antidepressants roughly compar-able in terms of efficacy. Rather, adverseeffects and patient preference seem to beguiding the choice of medication (AmericanPsychiatric Association, 1998). A meta-analysis corroborates these findings (Sturpe& Weissman, 2002). In fact, the differencebetween SSRIs and imipramine has not beenclearly established (Sturpe & Weissman,2002). Brokaw (2002), for example, couldnot support the hypothesis that SSRIs aremore effective and tolerable than tricyclicantidepressants.
Patients seeking care in psychiatric settingsare more likely to receive treatments thatintegrate medication and psychotherapy.Unfortunately, RCTs studying moderate tosevere PDA were found to exclude depressionas a comorbid condition, thus limiting thepossibility of generalizing the findings to a
VOL 37, NO 3, 2008 Combined modality therapy for panic disorder 147
Downloaded By: [Canadian Research Knowledge Network] At: 17:21 10 October 2009

more typical agoraphobic population. Themain objective of this study is, therefore, notto demonstrate medication efficacy, becausethat has been well established, but to increaseexternal validity in a more typical population.Consequently, it focuses on a populationsuffering from moderate to severe PDA withcomorbid depression and receiving medica-tion as well as psychotherapy. Imipraminewas chosen for the pharmacotherapy becauseit was still widely used as a pharmacologicaltreatment when this study was conducted. Tocontrol for medication responsiveness, pillplacebo groups were included in the design(Klein, 1996a, 1996b).
The main objective of this study was tocompare four psychosocial treatments inorder to evaluate the benefits of combiningcognitive therapy with exposure in vivo. Thesetreatments were combined with imipramine orplacebo for a total of eight experimentalconditions in a double-blind randomized trial.Psychosocial treatments were (a) cognitiveand graded in vivo exposure treatments, (b)graded in vivo exposure, (c) cognitive treat-ment, and (d) supportive therapy (nonpre-scriptive intervention). Participants presentedmoderate to severe agoraphobia. We hypothe-sized that participants receiving CBT andimipramine would reveal greater improvementover the 1-year follow-up compared withthose receiving supportive therapy and pla-cebo. The latter constitutes the control condi-tion. At the time this protocol was developed,there was little empirical evidence to supportthe efficacy of nonprescriptive forms oftherapy for PDA. We also hypothesized thatparticipants receiving CBT would improvemore than those receiving cognitive or beha-vioural treatment alone over the 1-yearfollow-up. This should help to shed somelight on whether specific cognitive or beha-vioural interventions with moderate to severeagoraphobic individuals are more importantor if their combination is still essential.
MethodParticipantsVolunteers were recruited, from 1992 to 1994,through media advertisements and referrals toa behaviour therapy unit of a psychiatrichospital in Montreal, where the study wasconducted. All men and women, ages 18 to 55
years, who met the Diagnostic and StatisticalManual of Mental Disorders (third edition,revised [DSM–III–R]; American PsychiatricAssociation, 1987) criteria for PDA and whorated the severity of their panic attacks (0–7)at greater than 3 were candidates for inclusionin the study. They were not admitted to thestudy if any of the following criteria werepresent: (a) other diagnoses that were thoughtto be more severe than the PDA diagnosis, (b)current involvement in psychotherapy, (c)alcohol or substance abuse within the pre-vious 6 months, (d) psychotic symptoms, or(e) evidence of organic impairment. In addi-tion, participants had to agree to withdrawfrom their medication (only the study medica-tion/placebo was permitted as well as smalldoses of oxazepam [15 mg] limited to 20 pills/month). The withdrawal period was 4 weeks,and participants were stabilized for 6 weeksbefore beginning the psychotherapy.
A total of 1,599 persons responded to theadvertisements or were referred to the study.Of these, 1,500 were screened by telephone,leaving less than 30% of potential partici-pants. Consequently, 445 potential partici-pants underwent a psychiatric and physicalexamination. Of these participants, only 228met the inclusion criteria and were interviewedusing the Anxiety Disorders InterviewSchedule–Revised (ADIS-R; (DiNardo &Barlow, 1985). Licensed psychologists specifi-cally trained in administering the ADIS-Rconducted the interviews. A second psychol-ogist, who was unaware of the diagnosis madeby the first psychologists, examined 20% ofthe patients’ files to determine the diagnosisfrom ADIS-R. From this sample, interraterreliability (k50.64) was calculated for axisdiagnoses between the two evaluators. Akappa value of .64 is a sufficiently highinterrater coefficient if we take into accountthat studies using structured interviews foranxiety disorders like the ADIS-R havereported similar kappa values for the evalua-tion of PD (about .69). Landis and Koch(1977) have suggested that a kappa valuebetween .60 and .70 can be considered a goodinterrater agreement level. Moreover, a con-sensus between the ADIS-R and psychiatristdiagnosis of PDA had to be reached in orderto include the participant in the study.Following the ADIS-R, 41 potential partici-pants did not meet inclusion criteria, primarily
148 Marchand et al. COGNITIVE BEHAVIOUR THERAPY
Downloaded By: [Canadian Research Knowledge Network] At: 17:21 10 October 2009

because other ADIS-R diagnoses werethought to be more severe than the PDAdiagnosis. Thirty-three candidates declined toparticipate, mostly upon refusal to take thestudy medication or to progressively withdrawfrom their own medication. The final sampleconsisted of 154 Caucasian and French-speaking participants, from whom informedconsent approved by the hospital ethicscommittee was obtained after discussion ofthe trial. A flowchart of recruitment andrandomization is shown in Figure 1.
Randomization and blindingParticipants were randomized to one of theeight treatment conditions: cognitive therapy,graded in vivo exposure, plus imipramine(CT+GE+I); cognitive therapy, graded in vivoexposure, plus placebo (CT+GE+P); cognitivetherapy plus imipramine (CT+I); cognitivetherapy plus placebo (CT+P); graded in vivoexposure plus imipramine (GE+I); graded invivo exposure plus placebo (GE+P); suppor-tive therapy plus imipramine (ST+I); andsupportive therapy plus placebo (ST+P). The
Figure. 1. Flowchart of recruitment and participation.
VOL 37, NO 3, 2008 Combined modality therapy for panic disorder 149
Downloaded By: [Canadian Research Knowledge Network] At: 17:21 10 October 2009

randomization technique used a computerrandom number generator to select four largerandom blocks every 6 months. No interimanalysis or stopping rules were applied.
Participants were unaware of the medica-tion conditions. In each of the eight differenttreatment groups, therapists were not per-mitted to discuss with participants any treat-ment options or techniques other than thosethat were part of the program. If specificallyquestioned about other treatment strategies oroptions, therapists were advised to acknowl-edge the existence of other techniques butwere required to specify that there was noactual evidence indicating that one optionclearly outperformed another in terms ofefficacy for PDA. Therapists were also dis-couraged from naming and describing theseother techniques. Furthermore, all studypersonnel were unaware of the medicationassignments and research hypotheses for theduration of the study. The codes were revealedto the researchers only when the final scien-tific report was submitted to the grant agency.
MeasuresParticipants completed self-report measures ofpanic–agoraphobia symptoms, general anxi-ety, and depression at baseline, posttreatment,and 3-, 6-, and 12-month follow-up visits.Panic–agoraphobia symptomatology. Severalself-report questionnaires were used to assessthe panic–agoraphobia symptomatology. TheAgoraphobia Cognitions Questionnaire(ACQ) assesses the frequency of catastrophicthoughts concerning negative consequences ofexperiencing anxiety (fear of fear; Bouvard,Cottraux, & Talbot, 1998; Chambless,Caputo, Bright, & Gallagher, 1984;Stephenson, Marchand, & Lavallee, 1999).The French Canadian adaptation of the ACQpresented satisfactory psychometric propertiesthat were similar to those of the original ACQversion (Stephenson et al., 1999). The BodySensations Questionnaire (BSQ) is a self-reported questionnaire that assesses the fre-quency and level of patient fear of physicalsymptoms common in PDA (Chambless et al.,1984). The French Canadian adaptationpresents good psychometric properties(Stephenson, Marchand, & Lavallee, 1998).Both the ACQ and the BSQ were shown to beresponsive to treatment effect (Bouvard et al.,1998; Chambless et al., 1984). The Mobility
Inventory for Agoraphobia (MIA) is aself-report questionnaire that assesses agora-phobic avoidance while alone and whenaccompanied by someone (Chambless,Caputo, Jasin, Gracely, & Williams, 1985).One question also asks for the occurrence ofpanic attacks in the last 7 days. A definition ofa panic attack is also provided (Chamblesset al., 1985). The MIA showed very goodpsychometric properties in terms of its relia-bility, validity, and responsiveness (Chamblesset al., 1985; Stephenson, Marchand, &Lavallee, 1997). The ACQ, BSQ, and MIAare recommended by a group of leading panicinvestigators (Shear & Maser, 1994) as essen-tial instruments to be included in researchpertaining to PD.General anxiety. The State–Trait AnxietyInventory (STAI) was used to assess bothgeneral and situational anxiety (Spielberger,Gorsuch, & Luschene, 1970). The validatedFrench language questionnaire (Gauthier &Bouchard, 1993) revealed an internal consis-tency of .86 and .95 for the Trait and Statesubscales respectively and good test–retestreliability (Gauthier & Bouchard, 1993).These results are comparable to thoseobtained with the English version (Kabacoff,Segal, Hersen, & Van Hasselt, 1997).Depression. The Beck Depression Inventory(BDI) assesses cognitive and somatic symp-toms of depression (Beck, Ward, Mendelsohn,Mock, & Erbaugh, 1961). The review per-formed by Richter, Werner, Heerlein, Kraus,and Sauer (1998) confirmed good reliabilityand responsiveness. A validated French lan-guage version was used for this study(Gauthier, Morin, Theriault, & Lawson,1982).Severity of PDA symptoms. An adaptation ofthe Global Symptom Severity Scale (GSSS)(Mavissakalian, Michelson, Greenwald,Kornblith, & Greenwald, 1983) was used toassess participants’ improvement. Two inde-pendent evaluators who were unaware of thetreatment allocation performed the evalua-tions. Interrater reliability scores were calcu-lated and found to be satisfactory (k5.84).This scale was also used to identify the level ofseverity of each participant’s symptoms. Theseverity of symptoms is rated on a 7-pointscale, with 1 indicating that the patient has nosymptoms of PDA and functions normally(symptoms do not interfere with psychosocial
150 Marchand et al. COGNITIVE BEHAVIOUR THERAPY
Downloaded By: [Canadian Research Knowledge Network] At: 17:21 10 October 2009

functioning) and 7 suggesting that PDAsubstantially interferes with the participant’sroutine daily activities, leisure, and work.Again, because this study sought to recruitsufferers of moderate to severe PDA, onlyparticipants with a score of 3 or above wereeligible, suggesting that PDA interferes withthe participants’ leisure activities but not theirroutine daily activities and work.
TreatmentTreatment manuals were elaborated for eachtreatment modality, offering guidelines foreach session. All treatments were conducted insmall groups of eight to 10 participants.Groups met for 14 three-hour sessions over18 weeks (10 weekly sessions followed by foursessions every other week to increase patientautonomy). The first 30 min of each sessionwere devoted to the teaching of specifictechniques. In the following 60 min, theparticipants were divided into two smallsubgroups, where they reviewed their specificdifficulties in carrying out previous homeworkassignments. New homework tasks were alsoassigned during this period. The remaining90 min of the session were devoted totherapist-assisted practice with the newlylearned techniques. The therapists (N54) werelicensed psychologists (specifically trained inCBT) with an average of 9.2 years (SD55.5)of experience. Two therapists per groupadministered the treatments. Therapists werecounterbalanced across treatment conditions.Graded in vivo exposure (GE). Participantswho received GE therapy were given extensiveinformation on the mechanisms of fear devel-opment and the potential benefits of in vivoexposure therapy. Exposure sessions wereplanned according to the participants’ evalua-tion of their difficulty in going ahead with theactual exposure sessions. Participants wereencouraged to gradually increase the difficultyof the exposure across sessions. The in vivoexposure procedure and exercises prescribedwere based on each participant’s functionalanalysis and several published treatmentmanuals (see Marchand & Beaudry, 1984;Marchand & Letarte, 1993; Marks, 1987).Cognitive therapy (CT). This was based onprocedures outlined by Beck (1988), Clark(1988), and Meichenbaum (1977). Specifictechniques included education regarding therelationship between maladaptive thoughts
and anxiety, identification and monitoring ofpanic-related cognitions, exploration of auto-matic negative thoughts and false assumptions,generation of alternative explanations, reattri-bution, and decatastrophization. In addition,thought-stopping, attention-distraction, andself-verbalization techniques were also taught.Cognitive and behavioural treatment combined(CT+GE). This approach included both theGE and CT techniques described previously.In the present study, the cognitive therapymodality addressed core schemas and dys-functional beliefs via cognitive restructuringwithout interoceptive exposure. It should benoted that at the time this study wasconducted, panic-focused cognitive treatment(cognitive model of panic)/panic-controlledtraining`studies were in the initial stages ofdevelopment (Barlow & Cerny, 1988; Beck,Sokol, Clark, Berchick, & Wright, 1992;Clark, 1994).Supportive therapy (ST). This was based ontechniques detailed in Friedman (1989) andYalom (1970). Therapists provided informa-tion on PDA (without detailing the differentnonpharmacological techniques); offeredhope; used reflection, empathy, active listen-ing, and insight-seeking questions; andemphasized group cooperation and support.A similar intervention was compared with theCBT and imipramine treatment of a groupwith no to mild agoraphobia. A study did notfind supportive therapy to be an effectivetreatment for panic disorder compared withCBT and pharmacological therapy (Shear,Houck, Greeno, & Masters, 2001). Supportivetherapy was, therefore, chosen as the con-trolled modality. Compared with a wait-list orrelaxation-alone approach, supportive ther-apy can control for length of treatment andtime spent with a therapist.Pharmacotherapy. At the time of the study,imipramine was widely used as a pharmaco-logical treatment. Participants were alsorandomly assigned to either imipramine orplacebo (double-blind). All participants hadto undergo withdrawal from their previousmedication, which lasted 4 weeks. During thisperiod, participants met with the psychiatristevery week. Participants who took benzodia-zepine on a regular basis underwent with-drawal using flurazepam, with a Serax dose of15 mg as needed to encourage a smoothtransition. Pharmacotherapy was initiated
VOL 37, NO 3, 2008 Combined modality therapy for panic disorder 151
Downloaded By: [Canadian Research Knowledge Network] At: 17:21 10 October 2009

4 weeks before the onset of psychotherapy.Doses of the medication were graduallyincreased from 25 mg up to the highest dosetolerated by the patient or to a maximum doseof 200 mg/day. Psychiatrists attempted toreach the maximum dose of 200 mg.However, in one case, a subtherapeutic doseof 50 mg was accepted. On average, partici-pants received 150 mg/day (range: 125–200 mg). Participants were kept on the med-ication (at the maximum dose) until the lastpsychotherapy session. Thereafter, medicationwas gradually tapered.
Treatment IntegrityAll therapy sessions were audiotaped. Thirtypercent of the sessions were randomly selectedand rated by an independent evaluator, whowas unaware of the specific hypotheses of thestudy. The evaluator used a checklist oftechniques deemed both appropriate andinappropriate for each treatment condition.Examination of the treatment integrity datarevealed essentially no violations and morespecifically high treatment integrity (84%adhesion to the protocol).
Monitoring can enhance adherence (Burke& Dunbar-Jacob, 1995). Therefore, to max-imize medication adherence, participants wereinformed of the possibility of random biolo-gical medication screening tests being con-ducted during the study. Random testing wasinitially intended. However, it was not per-formed because during the experiment inves-tigators learned that it was not possible toefficiently monitor adherence to medicationthrough urine samples. Monitoring of pre-scription renewal was performed because themedication was obtained free at the hospitalpharmacy. All patients renewed their prescrip-tions regularly.
Data AnalysesFirst, a repeated measures analysis of variance(ANOVA) with a 4 (treatments)62 (medica-tion)62 (time) design with time as a repeatedfactor was performed to assess whether therewere differences in the decline in complaintsfrom pre- to posttest between the treat-ment conditions. Analysis of interactioneffects was also performed between time andmedication and time and treatments in orderto reveal possible differences in acute treat-ment response between medication and
placebo and between the four treatmentconditions. The hypothesis was that three-way interaction effects might indicate thatthe difference between psychosocial groupswas larger when combined with placebo thanwhen combined with medication. A subse-quent set of analyses compared posttest out-comes with the 12-month follow-up in a46264 design, testing the hypothesis thattreatments differ in terms of further improve-ment during the follow-up interval. Toreduce Type I error, a Bonferroni adjust-ment was used because of the number oftests performed. With four repeated measuresANOVAs per set of analyses, an alpha level of.0125 was used for all statistical tests.
Additionally, an end-state functioningindex of treatment response was calculated.This index quantifies treatment responsebased on six variables: ACQ, BSQ, STAI–State subscale, GSSS, MIA, and panic attacks(presence or absence) during the previousweek (based on the MIA). To calculate theend-state functioning index score, we beganby comparing patients’ scores on each of thefour self-report questionnaires (MIA, ACQ,BSQ, STAI–State) with a cutoff score,referred to as the C index (Jacobson &Truax, 1992), derived from nonclinical sam-ples and pretest scores taken from our clinicalsamples. In order for a participant to beconsidered functional at posttreatment andfollow-up, the score on the self-report ques-tionnaire had to be equal to or below the Cindex. The participant obtained 1 point on theend-state functioning index of treatmentresponse for every questionnaire yieldingscores below or equal to the C index. Inaddition, the participant earned 1 point if heor she had not had a panic attack and anotherpoint if his or her GSSS rating was below 3.Hence, the end-state functioning index oftreatment response or the global functioningindex scores ranged from 0 to 6. It wasarbitrarily established that scores of 4 andabove would indicate major improvement;scores of 2 and 3, moderate improvement; anda score of 1, minimal improvement.
ResultsDescriptive statisticsFrom the initial sample (N5154), 17 partici-pants did not complete the study (11%): two
152 Marchand et al. COGNITIVE BEHAVIOUR THERAPY
Downloaded By: [Canadian Research Knowledge Network] At: 17:21 10 October 2009
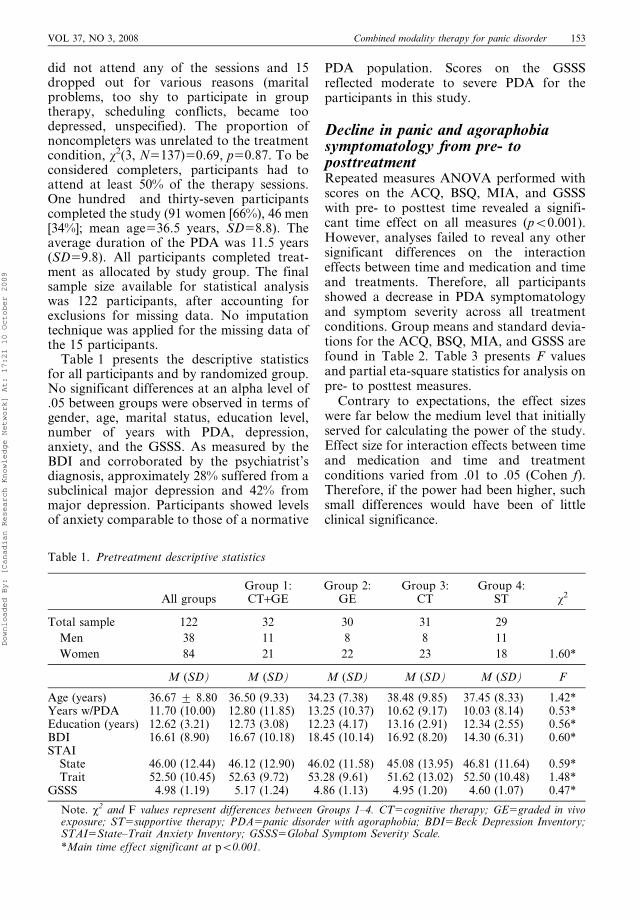
did not attend any of the sessions and 15dropped out for various reasons (maritalproblems, too shy to participate in grouptherapy, scheduling conflicts, became toodepressed, unspecified). The proportion ofnoncompleters was unrelated to the treatmentcondition, x2(3, N5137)50.69, p50.87. To beconsidered completers, participants had toattend at least 50% of the therapy sessions.One hundred and thirty-seven participantscompleted the study (91 women [66%), 46 men[34%]; mean age536.5 years, SD58.8). Theaverage duration of the PDA was 11.5 years(SD59.8). All participants completed treat-ment as allocated by study group. The finalsample size available for statistical analysiswas 122 participants, after accounting forexclusions for missing data. No imputationtechnique was applied for the missing data ofthe 15 participants.
Table 1 presents the descriptive statisticsfor all participants and by randomized group.No significant differences at an alpha level of.05 between groups were observed in terms ofgender, age, marital status, education level,number of years with PDA, depression,anxiety, and the GSSS. As measured by theBDI and corroborated by the psychiatrist’sdiagnosis, approximately 28% suffered from asubclinical major depression and 42% frommajor depression. Participants showed levelsof anxiety comparable to those of a normative
PDA population. Scores on the GSSSreflected moderate to severe PDA for theparticipants in this study.
Decline in panic and agoraphobiasymptomatology from pre- toposttreatmentRepeated measures ANOVA performed withscores on the ACQ, BSQ, MIA, and GSSSwith pre- to posttest time revealed a signifi-cant time effect on all measures (pv0.001).However, analyses failed to reveal any othersignificant differences on the interactioneffects between time and medication and timeand treatments. Therefore, all participantsshowed a decrease in PDA symptomatologyand symptom severity across all treatmentconditions. Group means and standard devia-tions for the ACQ, BSQ, MIA, and GSSS arefound in Table 2. Table 3 presents F valuesand partial eta-square statistics for analysis onpre- to posttest measures.
Contrary to expectations, the effect sizeswere far below the medium level that initiallyserved for calculating the power of the study.Effect size for interaction effects between timeand medication and time and treatmentconditions varied from .01 to .05 (Cohen f).Therefore, if the power had been higher, suchsmall differences would have been of littleclinical significance.
Table 1. Pretreatment descriptive statistics
All groupsGroup 1:CT+GE
Group 2:GE
Group 3:CT
Group 4:ST x2
Total sample 122 32 30 31 29
Men 38 11 8 8 11
Women 84 21 22 23 18 1.60*
M (SD) M (SD) M (SD) M (SD) M (SD) F
Age (years) 36.67 ¡ 8.80 36.50 (9.33) 34.23 (7.38) 38.48 (9.85) 37.45 (8.33) 1.42*Years w/PDA 11.70 (10.00) 12.80 (11.85) 13.25 (10.37) 10.62 (9.17) 10.03 (8.14) 0.53*Education (years) 12.62 (3.21) 12.73 (3.08) 12.23 (4.17) 13.16 (2.91) 12.34 (2.55) 0.56*BDI 16.61 (8.90) 16.67 (10.18) 18.45 (10.14) 16.92 (8.20) 14.30 (6.31) 0.60*STAI
State 46.00 (12.44) 46.12 (12.90) 46.02 (11.58) 45.08 (13.95) 46.81 (11.64) 0.59*Trait 52.50 (10.45) 52.63 (9.72) 53.28 (9.61) 51.62 (13.02) 52.50 (10.48) 1.48*
GSSS 4.98 (1.19) 5.17 (1.24) 4.86 (1.13) 4.95 (1.20) 4.60 (1.07) 0.47*
Note. x2 and F values represent differences between Groups 1–4. CT5cognitive therapy; GE5graded in vivoexposure; ST5supportive therapy; PDA5panic disorder with agoraphobia; BDI5Beck Depression Inventory;STAI5State–Trait Anxiety Inventory; GSSS5Global Symptom Severity Scale.*Main time effect significant at pv0.001.
VOL 37, NO 3, 2008 Combined modality therapy for panic disorder 153
Downloaded By: [Canadian Research Knowledge Network] At: 17:21 10 October 2009

Table 2. Group means of psychological distress measures
Measure/treatment
Baseline Post-tx
Follow-up
3 months 6 months 12 months
M SD M SD M SD M SD M SD
MIA–AloneCBT combined 3.17 0.83 1.89 0.83 1.79 0.75 1.74 0.72 1.89 0.92Graded exposure 3.81 0.90 2.49 1.29 2.35 1.29 2.24 1.26 2.41 1.27Cognitive 3.52 0.88 2.10 1.06 2.11 1.02 2.13 1.17 2.13 1.20Support 3.39 0.90 2.49 1.04 2.35 1.19 2.31 1.12 2.31 1.14Medication 3.40 0.91 2.13 1.02 2.04 1.05 1.98 1.04 2.09 1.10Placebo 3.56 0.89 2.38 1.15 2.28 1.13 2.25 1.15 2.30 1.18
BSQCBT combined 3.18 0.73 1.85 0.78 2.02 0.76 1.98 0.85 1.97 0.88Graded exposure 3.26 0.77 2.19 0.78 2.27 0.66 2.11 0.82 2.23 0.80Cognitive 3.06 0.82 2.11 0.63 2.30 0.73 2.18 0.67 2.13 0.65Support 3.21 0.72 2.52 0.79 2.43 0.78 2.53 0.71 2.32 0.90Medication 3.20 0.70 2.10 0.76 2.25 0.77 2.23 0.85 2.81 0.82Placebo 3.15 0.82 2.25 0.79 2.26 0.71 2.16 0.71 2.13 0.82
ACQCBT combined 2.59 0.54 1.85 0.70 1.85 0.70 1.71 0.60 1.78 0.72Graded exposure 2.68 0.65 1.76 0.48 1.78 0.49 1.79 0.59 1.75 0.59Cognitive 2.63 0.65 1.91 0.58 1.96 0.58 1.89 0.46 1.84 0.45Support 2.57 0.50 2.12 0.68 2.07 0.68 2.02 0.63 2.01 0.78Medication 2.67 0.56 1.89 0.67 1.91 0.67 1.86 0.64 1.86 0.70Placebo 2.56 0.60 1.93 0.57 1.92 0.57 1.84 0.50 1.83 0.59
GSSSCBT combined 5.17 1.24 2.78 1.52 2.89 1.53 2.39 1.33 2.39 1.38Graded exposure 4.86 1.13 3.04 1.40 2.73 1.45 2.91 1.31 3.18 1.44Cognitive 4.95 1.20 2.90 1.45 2.62 1.50 2.74 1.28 2.90 1.41Support 4.60 1.07 2.90 1.20 3.00 1.33 2.90 1.20 3.00 1.15Medication 4.70 1.20 2.56 1.23 2.49 1.09 2.40 1.01 2.54 1.21Placebo 5.20 1.06 3.40 1.48 3.17 1.76 3.17 1.49 3.33 1.49
Note. MIA–Alone5Mobility Inventory for Agoraphobia when alone; BSQ5Body Sensation Questionnaire;ACQ5Agoraphobia Cognition Questionnaire; GSSS5Global Symptom Severity Scale.*Main time effect significant at pv.001.
Table 3. F values and partial eta square statistics for analysis on pre- to posttest measures
Variable
MIA–Alone BSQ ACQ GSSS
F Partial g2 F Partial g2 F Partial g2 F Partial g2
Between subjectPsychologicalintervention (A)
1.50 .030 1.70 .042 1.08 .027 0.51 .013
Medication (B) 0.12 .001 1.79 .015 0.03 .000 2.66 .022AB 0.54 .014 0.42 .011 0.67 .017 0.40 .010
Within subjectTime (C) 221.58* .656 139.72* .546 142.56* .551 208.43* .639AC 1.11 .028 1.33 .033 1.84 .045 1.12 .028BC 0.92 .008 4.23* .035 3.05 .026 2.10 .017ABC 0.39 .010 1.36 .034 0.62 .016 0.54 .014
Note. MIA–Alone5Mobility Inventory for Agoraphobia when alone; BSQ5Body Sensation Questionnaire;ACQ5Agoraphobia Cognition Questionnaire; GSSS5Global Symptom Severity Scale.*Main time effect significant at pv0.001.
154 Marchand et al. COGNITIVE BEHAVIOUR THERAPY
Downloaded By: [Canadian Research Knowledge Network] At: 17:21 10 October 2009
Further improvement in panic andagoraphobia symptomatology fromposttreatment to 12-month follow-upRepeated measures of variance were per-formed on ACQ, BSQ, MIA, and GSSSscores between posttreatment and the 12-month follow-up. Analyses failed to revealany significant differences, including timeeffects. Group means and standard deviationsfor these measures are found in Table 2. Theseresults suggest a stabilization of PDA symp-tomatology and symptom severity during thefollow-up period across all treatment condi-tions, including imipramine and placebo.
Treatment responseAs measured using the MIA panic question,the proportion of participants who werepanic-free at posttreatment was as follows:90% GE (n528), 72% CT+GE (n523), 79%CT (n523), and 79% ST (n522). A chi-squareanalysis of these frequencies was nonsignifi-cant, x2(3, N5120)53.42, p50.33. At the 1-year follow-up, the proportion of participantswho were panic-free was as follows: 82% GE(n523), 79% CT+GE (n523), 59% CT(n516), and 63% ST (n517). A chi-squareanalysis of these frequencies was nonsignifi-cant, x2(3, N5111)55.33, p50.15.
End-state functioning index oftreatment responseCategorization of participants by treatmentresponse level indicated that at posttreatment64.5% of GE (n520), 58% of CT+GE (n519),68% of CT (n520), and 40% of ST (n511)participants showed major improvement,although the differences between groups didnot attain significance, x2(6, N5116)55.61,p50.46). However, 66.7% of participants onimipramine and 48.5% of those on placebodisplayed major improvements, a differencethat approached statistical significance, x2(2,N579)55.56, p50.06. At the 1-year follow-up, 71.4% of GE (n522), 58% of CT+GE(n519), 50% of CT (n515), and 59% of ST(n516) participants displayed major improve-ment from baseline. Differences betweenpsychotherapy groups did not attain signifi-cance at the 1-year follow-up as they did atposttreatment, x2(6, N5116)54.75, p50.57.However, 65.1% of participants on imipra-mine and 52.7% of those on placebo displayed
major improvement and a difference atfollow-up, x2(2, N579)56.31, p50.04.Finally, it is noteworthy that 90% of allparticipants continued to show eithermoderate or major improvement at 1-yearposttreatment.
Discussion
The main objective of this double-blindrandomized trial was to compare four psy-chosocial treatments given to moderate tosevere agoraphobia participants in order toevaluate the benefits of combining cognitivetherapy with exposure in vivo. These treat-ments were combined with imipramine orplacebo, for a total of eight experimentalconditions in a double-blind randomized trial.It was hypothesized that participants receivingany CBT treatments and imipramine wouldreveal greater improvement at the 1-yearfollow-up compared with participants receiv-ing supportive therapy and placebo. Resultsfailed to support the hypothesis. It was alsohypothesized that participants receiving CBTwould improve more than those receivingcognitive or behavioural treatment alone overthe 1-year follow-up. Results failed to supportthe hypothesis. The results of this studysuggest that all of the treatments tested wereboth statistically and clinically effective interms of self-reported panic–agoraphobiasymptomatology and the composite index oftreatment response at the 1-year follow-up.The end-state functioning index indicates thatroughly 90% of participants showed moderateor major improvement at posttreatment and 1year thereafter. Posttreatment and follow-upmeans on all of the self-report scales werewithin reported norms for these instru-ments. Analyses on self-report scales failedto reveal significant differences between imi-pramine and placebo; however, the end-statefunctioning index shows a trend at posttreat-ment for greater clinical improvement for theimipramine group (all psychotherapeuticgroups confounded) compared with the pla-cebo group (all psychotherapeutic groupsconfounded). This trend became significantat 1-year follow-up
The percentage of patients who improved isconsistent with findings in previous studiesusing CBT treatment (Craske & Barlow, 2001;Shear et al., 2001). Some studies have also
VOL 37, NO 3, 2008 Combined modality therapy for panic disorder 155
Downloaded By: [Canadian Research Knowledge Network] At: 17:21 10 October 2009
found differences between the results obtainedwith imipramine and placebo (Mavissakalian,1996; Mavissakalian & Perel, 1995). Findingsstrongly support CBT treatments (White &Barlow, 2002). Also, in mild to moderateagoraphobic patients, Shear et al. (2001) havefound CBT to be more effective than emotion-focused psychotherapy. However, in a pre-vious study with moderate to severe patients,emotion-focused psychotherapy, when com-pared with CBT, revealed no significantdifferences. The main limitation of this studywas that it used the number of panic attacksas the main outcome. Our study supportsthese findings and used other outcome vari-ables, thereby addressing this limitation.
One of the first points to question when nobetween-group differences are found is thepossibility of a Type II error, which erro-neously implies that there is no differencewhen, in fact, a difference does exist. Inestimating the required sample size for thisproject, we assumed a moderate effect size(Cohen f50.30) for treatments comparedwith the supportive therapy with placebo-controlled condition. However, the actualeffect size was smaller than anticipated. Inother words, the difference between what wehypothesized as being the effective treatments(CBT interventions with or without imipra-mine) and the supportive therapy with pla-cebo control was not as large as anticipated.Post hoc estimation of the required samplesize to detect such a small difference betweentreatments and control at an alpha level of .05at a power of 0.8 with Cohen’s formulasuggests that 63 participants per group (for atotal sample size of roughly 500) would berequired. However, this large number ofparticipants required to detect a small effectraises the question of the clinical significance.
We propose that the smaller actual effectsize is attributable to the fact that supportivetherapy with placebo was a more effectivetreatment-controlled condition than initiallyhypothesized. Hence, although the initiallycalculated sample size should have beenadequate, the fact that the controlled condi-tion was more effective than anticipatedcreated a problem in the resulting power.
On an exploratory basis, at follow-up,participants were asked for their view of theiroverall improvement and of the reasons forthis improvement. It was found that many
participants in the supportive therapy grouphad read a self-help book based on CBTprinciples (Marchand & Letarte, 1993). In thegroup setting, participants were found to beencouraging each other to expose themselvesto feared situations. The audiotaped sessions,in fact, confirmed that such exposure wasencouraged among participants. The thera-pists did not suggest any CBT interventionstrategies. The high treatment integrity ratingsindicate that the therapists respected theprotocol. However, they were asked to sup-port and encourage participants. Therefore,given that the issue of exposure was raised byparticipants, the therapists had to encouragetheir efforts. In fact, it would have beenunethical to ask participants to refrain fromexposure until the end of the study. It can,therefore, be hypothesized that the absence ofsignificant results among all treatment condi-tions may be due to the fact that there wasexposure to feared situations in all treatmentconditions.
Several limitations of this study need to beaddressed. First, the failure for imipramine tooutperform placebo is inconsistent with pre-vious studies, and thereby raises the questionof whether the pharmacotherapy was properlyadministered. We agree that this is a potentialexplanation; however, strategies for improv-ing adherence to medication were implemen-ted (e.g. medical management component:monitor adverse effects, clinical state, andthe patient’s physical/mental condition; max-imize compliance with the pharmacologicaltreatment protocol), and also the end-statefunctioning index shows a significant differ-ence at 1-year follow-up for greater clinicalimprovement for the imipramine group com-pared with placebo. Second, participants wereevaluated based on the ADIS-R, which bringssmall differences in the establishment of thediagnosis compared with the DSM–IV cri-teria. Participants who received more specifictherapy ingredients (techniques) in the com-bined cognitive and graded in vivo exposuregroups did not receive more effective therapythan participants in either the cognitive orgraded in vivo exposure group. All partici-pants received the same amount of therapytime; it is, however, possible that participantsin the cognitive and graded in vivo exposuregroups did not have enough time to master orbenefit from the effectiveness of either the
156 Marchand et al. COGNITIVE BEHAVIOUR THERAPY
Downloaded By: [Canadian Research Knowledge Network] At: 17:21 10 October 2009
cognitive or the graded in vivo exposurecomponent in contrast to the other condi-tions. This is an important issue to address,given that in clinical practice more flexibilityand therapy time may contribute to support-ing the widespread notion that combinedcognitive and behavioural techniques aremore effective than cognitive or graded invivo exposure used alone in treating PDA.Another limitation may be the overall designof this study, which does not enable us todraw direct conclusions concerning the indi-vidual efficacy of any of the treatmentconditions (psychotherapy or medication),because all treatments consisted of combinedpharmacological and psychological therapies.It may be argued that the addition ofpsychotherapy groups without medicationand vice versa would have clarified the relativeefficacy of drug and psychological treatmentsfor PDA. However, the purpose of this studywas to examine the combined efficacy oftreatments in order to reflect a clinical reality,which is that PD and PDA participants oftenreceive combined drug–psychotherapy treat-ments. This issue has rarely been addressed. Incontrast, studies that have compared drug-only with therapy-only groups have also beencriticized for their choice of design.
Conclusion
This study found that all treatment modalitieshelped reduce panic and agoraphobic symp-tomatology over a 1-year follow-up period.Also, the majority of participants (90%)showed moderate to major improvement upto the 1-year follow-up. Finally, these surpris-ing results support the need for a mixedmethod in order to set up a blueprint for theintervention by establishing the specific linksamong the objectives, activities, and expectedoutcomes and in order to state what theprogram is expected to do (Rossi, Lipsey, &Freeman, 2004). This is part of an evaluativeresearch approach (Weiss, 1997). This per-spective makes it possible to assess the relativeefficacy of the treatment components ratherthan of the intervention as a whole (Petrosino,2000). Also, the qualitative part of themixed method may help explain some of theresults obtained in the quantitative part ofthe study.
Acknowledgements
This research was supported by a jointprogram on mental health run by the Fondsde Recherche en Sante du Quebec and theConseil Quebecois de Recherche Social (GrantNo. 900763-104). The authors acknowledgethe contributions of Rock Morin, whoassisted in data collection and analysis, andKim Lavoie and Randolph Stephenson, whohelped edit this article.
ReferencesAmerican Psychiatric Association (1987).
Diagnostic and statistical manual of mentaldisorders (3rd ed., rev.). Washington, DC:American Psychological Association.
American Psychiatric Association (1998). Practiceguideline for the treatment of patients withpanic disorder. American Journal of Psychiatry,155(5, Suppl), 1–34.
Barlow, D. H., & Cerny, J. A. (1988). Psychologicaltreatment of panic. New York: Guilford Press.
Barlow, D. H., Groman, J. M., Shear, M. K., &Woods, S. C. (2000). Cognitive-behavioraltherapy, imipramine, or their combination forpanic disorder: A randomized controlled trial.Journal of American Psychiatry Association,283(19), 2519–2536.
Beck, A. T. (1988). Cognitive approaches topanic disorder: Theory and therapy. In S.Rachman & J. D. Maser (Eds), Panic:Psychological perspectives (pp. 90–107).Hillsdale, NJ: Erlbaum.
Beck, A. T., Sokol, L., Clark, D. A., Berchick, R.,& Wright, F. (1992). A crossover study offocused cognitive therapy for panic disorder.American Journal of Psychiatry, 149(6),778–783.
Beck, A. T., Ward, C. H., Mendelsohn, M., Mock,J., & Erbaugh, J. (1961). An inventory formeasuring depression. Archives of GeneralPsychiatry, 4, 53–63.
Bouvard, M., Cottraux, J., & Talbot, F. (1998).Cross-cultural validation of the AgoraphobicCognitions Questionnaire. Psychotherapy andPsychosomatics, 67, 249–253.
Brokaw, D. K. (2002). Are SSRIs and TCAsequally effective for the treatment of panicdisorder? Journal of Family Practice, 51(3), 279.
Brown, T. A., & Barlow, D. H. (1992).Comorbidity among anxiety disorders:Implications for treatment and DSM–IV.Journal of Consulting and Clinical Psychology,60, 835–844.
Burke, L. E., & Dunbar-Jacob, J. (1995).Adherence to medication, diet, and activityrecommendations: From assessment to main-tenance. Journal of Cardiovascular Nursing,9(2), 62–69.
Chambless, D. L., Caputo, G. C., Bright, P., &Gallagher, R. (1984). Assessment of ‘‘fear of
VOL 37, NO 3, 2008 Combined modality therapy for panic disorder 157
Downloaded By: [Canadian Research Knowledge Network] At: 17:21 10 October 2009
fear’’ in agoraphobics: The Body SensationsQuestionnaire and the Agoraphobic CognitionsQuestionnaire. Journal of Consulting andClinical Psychology, 52, 1090–1097.
Chambless, D. L., Caputo, G. C., Jasin, S. E.,Gracely, E. J., & Williams, C. (1985). TheMobility Inventory for Agoraphobia. BehaviourResearch and Therapy, 23(1), 35–44.
Clark, D. M. (1988). A cognitive model of panicattacks. In S. Rachman & J. D. Maser (Eds),Panic: Psychological perspectives (pp. 71–89).Hillsdale, NJ: Erlbaum.
Clark, D. M. (1994). Cognitive therapy for panicdisorder. In B. Wolfe & J. D. Maser (Eds),Treatment of panic disorder: A consensus devel-opment conference (pp. 53–72). Washington,DC: American Psychiatry Press.
Cottraux, J., Note, I. D., Cungi, C., Legeron, P.,Heim, F., & Chneiweiss, L., et al. (1995). Acontrolled study of cognitive behaviour therapywith buspirone or placebo in panic disorderwith agoraphobia. British Journal of Psychiatry,167(5), 635–641.
Craske, M. G., & Barlow, D. H. (2001). Panicdisorder and agoraphobia. In D. H. Barlow(Ed.), Clinical handbook of psychological dis-orders (3rd ed., pp. 1–59). New York: GuilfordPress.
De Beurs, E., van Balkom A., J., Lange, A., Koele,P., & van Dyck, R. (1995). Treatment of panicdisorder with agoraphobia: Comparison offluvoxamine, placebo, and psychological panicmanagement combined with exposure and ofexposure in vivo alone. American Journal ofPsychiatry, 152(5), 683–691.
DiNardo, P. A., & Barlow, D. H. (1985). AnxietyDisorders Interview Schedule—Revised (ADIS-R). Albany, NY: Phobia and AnxietyDisorders Clinic.
Fleet, R. P., Dupuis, G., Marchand, A., Burelle,D., Arsenault, A., & Beitman, B. D. (1996).Panic disorder in emergency department chestpain patients: Prevalence, comorbidity, suicidalideation, and physician recognition. AmericanJournal of Medicine, 101(4), 371–380.
Friedman, W. H. (1989). Practical group therapy.San Francisco: Jossey-Bass.
Gauthier, J. G., & Bouchard, S. (1993). Adaptationcanadienne–francaise de la forme revisee duState-Trait Anxiety Inventory de Spielberger[French–Canadian adaptation of the revisedState-Trait Anxiety Inventory fromSpielberger]. Revue Canadienne des Sciences duComportement, 25, 559–578.
Gauthier, J. G., Morin, C., Theriault, F., &Lawson, J. S. (1982). Adaptation francaised’une mesure d’auto-evaluation de l’intensitede la depression [French-language adaptationof a self-reported measure of depression]. RevueQuebecoise de Psychologie, 3, 13–27.
Jacobson, N. S., & Truax, P. (1992). Clinicalsignificance: A statistical approach to definingmeaningful change in psychotherapy research.In A. E. Kazdin (Ed.), Methodological issuesand strategies in clinical research (pp. 631–650).
Washington, DC: American PsychologicalAssociation.
Kabacoff, R. I., Segal, D. L., Hersen, M., & VanHasselt, V. B. (1997). Psychometric propertiesand diagnostic utility of the Beck AnxietyInventory and the State-Trait AnxietyInventory with older adult psychiatric out-patients. Journal of Anxiety Disorders, 11(1),33–47.
Kessler, R. C., Berglund, P., Demler, O., Jin, R.,Merikangas, K. R., & Walters, E. E. (2005).Lifetime prevalence and age-of-onset distribu-tions of DSM–IV disorders in the nationalcomorbidity survey replication. Archives ofGeneral Psychiatry, 26, 593–603.
Klein, D. F. (1996a). Discussion of ‘‘methodologi-cal controversies in the treatment of panicdisorder.’’ Behaviour Research and Therapy,34, 849–853.
Klein, D. F. (1996b). Preventing hung juries abouttherapy studies. Journal of Consulting andClinical Psychology, 64, 81–87.
Landis, J. R., & Koch, G. G. (1977). Themeasurement of observer agreement for cate-gorical data. Biometrics, 33, 159–174.
Loerch, B., Graf-Morgenstern, M., Hautzinger,M., Schlegel, S., Hain, C., & Sandmann, J., et al.(1999). Randomised placebo-controlled trial ofmoclobemide, cognitive-behavioural therapyand their combination in panic disorder withagoraphobia. British Journal of Psychiatry, 174,205–212.
Marchand, A., & Beaudry, M. (1984). Manueld’exercice pour les clients [Manual of exercisefor clients]. Unpublished manuscript.
Marchand, A., & Boivin, I. (1999). Le troublepanique [Panic disorder]. In R. Ladouceur, A.Marchand & J. M. Boisvert (Eds), Les troublesanxieux: Approche cognitive et comportementale[Anxiety disorders: Cognitive approach andcomportment]. Montreal, Quebec, Canada:Gaetan Morin.
Marchand, A., & Letarte, A. (1993). La peur d’avoirpeur: Guide de traitement de trouble paniqueavec agoraphobie [The fear of being afraid:Guide to the treatment of panic disorder withagoraphobia]. Montreal, Quebec, Canada:Stanke.
Marks, I. M. (1987). Fears, phobias, and rituals:Panic, anxiety, and their disorders. New York:Oxford University Press.
Mavissakalian, M. R. (1996). Phenomenology ofpanic attacks: Responsiveness of individualsymptoms to imipramine. Journal of ClinicalPsychopharmacology, 16(3), 233–237.
Mavissakalian, M. R., Michelson, L., Greenwald,D., Kornblith, S., & Greenwald, M. (1983).Cognitive-behavioral treatment of agorapho-bia: Paradoxical intention vs. self-statementtraining. Behaviour Research & Therapy, 21(1),75–86.
Mavissakalian, M. R., & Perel, J. M. (1995).Imipramine treatment of panic disorder withagoraphobia: Dose ranging and plasma level-response relationships. American Journal ofPsychiatry, 152(5), 673–682.
158 Marchand et al. COGNITIVE BEHAVIOUR THERAPY
Downloaded By: [Canadian Research Knowledge Network] At: 17:21 10 October 2009

Mavissakalian, M. R., & Perel, J. M. (1999). Long-term maintenance and discontinuation ofimipramine therapy in panic disorder withagoraphobia. Archives of General Psychiatry,56(9), 821–827.
Meichenbaum, D. (1977). Cognitive-behavior mod-ification: An integrative approach. New York:Plenum Press.
Michelson, D., Pollack, M., Lydiard, R. B.,Tamura, R., Tepner, R., & Tollefson, G.(1999). Continuing treatment of panic disorderafter acute response: Randomised, placebo-controlled trial with fluoxetine. TheFluoxetine Panic Disorder Study Group.British Journal of Psychiatry, 174, 213–218.
Michelson, L. K., Marchione, K. E., Greenwald,M., Testa, S., & Marchione, N. J. (1996). Acomparative outcome and follow-up investiga-tion of panic disorder with agoraphobia: Therelative and combined efficacy of cognitivetherapy, relaxation training, and therapist-assisted exposure. Journal of AnxietyDisorders, 10, 297–330.
Oehrberg, S., Christiansen, P. E., Behnke, K.,Borup, A. L., Severin, B., & Soegaard, J., et al.(1995). Paroxetine in the treatment of panicdisorder. A randomised, double-blind, placebo-controlled study. British Journal of Psychiatry,167(3), 374–379.
Petrosino, A. (2000). Answering the why questionin evaluation: The causal-model approach. TheCanadian Journal of Program Evaluation, 15(1),1–24.
Richter, P., Werner, J., Heerlein, A., Kraus, A., &Sauer, H. (1998). On the validity of the BeckDepression Inventory. Psychopathology, 31,160–168.
Rossi, P. H. (2004). Expressing and assessingprogram theory. In P. H. Rossi, M. W. Lipsey& H. E. Freeman (Eds), Evaluation: A systema-tic approach (7th ed., pp. 133–168). ThousandOaks, CA, USA: Sage.
Shear, M. K., Houck, P., Greeno, C., & Masters, S.(2001). Emotion-focused psychotherapy forpatients with panic disorder. American Journalof Psychiatry, 158(12), 1993–1998.
Shear, M. K., & Maser, J. D. (1994). Standardizedassessment for panic disorder research. Aconference report. Archives of GeneralPsychiatry, 51(5), 346–354.
Spielberger, C. D., Gorsuch, R. L., & Luschene, R. E.(1970). State-Trait Anxiety Inventory manual.Palo Alto, CA: Consulting Psychologists Press.
Stephenson, R., Marchand, A., & Lavallee, M.-C.(1997). Validation de l’inventaire de mobilite
pour l’agoraphobie aupres de la populationQuebecoise Francophone [Validation of theMobility Agoraphobia Inventory among theFrench-speaking population of Quebec].Science et Comportement, 26, 35–58.
Stephenson, R., Marchand, A., & Lavallee, M.-C.(1998). Validation du questionnaire des sensa-tions physiques aupres de la populationCanadienne–Francaise [Validation of theFrench–Canadian adaptation of the BodySensation Questionnaire]. Encephale, 24,415–425.
Stephenson, R., Marchand, A., & Lavallee, M. C.(1999). A Canadian French adaptation of theAgoraphobic Cognitions Questionnaire: Cross-cultural validation and gender differences.Scandinavian Journal of Behaviour Therapy,28(2), 58–69.
Sturpe, D. A., & Weissman, A. M. (2002). Whatare effective treatments for panic disorder?Journal of Family Practice, 51(9), 743.
Swinson, R. P., Cox, B. J., Kerr, S. A., Kuch, K., &Fergus, K. D. (1992). A survey of anxietydisorders clinics in Canadian hospitals.Canadian Journal of Psychiatry: RevueCanadienne de Psychiatrie, 37(3), 188–191.
Swinson, R. P., & Koch, K. (1990). Clinicalfeatures of panic and related disorders. In J.C. Ballenger (Ed.), Clinical aspects of panicdisorder (pp. 13–30). New York: Wiley-Liss.
Wardle, J., Hayward, P., Higgitt, A., Stabl, M.,Blizard, R., & Gray, J. (1994). Effects ofconcurrent diazepam treatment on the outcomeof exposure therapy in agoraphobia. BehaviourResearch and Therapy, 32(2), 203–215.
Weiss, C. H. (1997). How can theory-basedevaluation make greater headway? EvaluationReview, 21(4), 501–524.
White, K. S., & Barlow, D. H. (2002). Panicdisorder and agoraphobia. In D. H. Barlow(Ed.), Anxiety and its disorders: The nature andtreatment of anxiety and panic (2nd ed.,pp. 328–379). New York: Guilford Press.
Williams, S. L., & Falbo, J. (1996). Cognitive andperformance-based treatments for panic attacksin people with varying degrees of agoraphobicdisability. Behaviour Research and Therapy,34(3), 253–264.
Yalom, I. D. (1970). The theory and practice ofgroup psychotherapy. New York: Basics Books.
Zaubler, T. S., & Katon, W. (1996). Panic disorderand medical comorbidity: A review of themedical and psychiatric literature. Bulletin ofthe Menninger Clinic, 60(2, Suppl A), 12–38.
VOL 37, NO 3, 2008 Combined modality therapy for panic disorder 159
Downloaded By: [Canadian Research Knowledge Network] At: 17:21 10 October 2009
Related Documents