TREATMENT OF DEMENTIA

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

TREATMENT
OF
DEMENTIA

OUTLINE
Definition and Criteria
Classification of Dementia
Staging of Dementia
Classification Types and causes
of dementiaPathophysiology
Management of dementiaPHARMACOLOGIC
MANAGEMENT OF DEMENTIA Symptomatic Disease-modifying
treatments treatment of behavioral
disturbance
NON PHARMACOLOGIC MANAGEMENT OF DEMENTIA

Dementia
Term dementia in Latin means “devoid of the mind.”
It is defined as an acquired deterioration in cognitive abilities from a previ ously higher level of functioning that impairs the successful performance of activities of daily living.
In 2010, there are 3.7 million Indians with dementia and the total societal costs is about 14,700 crore(ALZHEIMER'S & RELATED DISORDERS SOCIETY OF INDIA ARDSI 2010)

DSM – IV Criteria for Dementia DSM-IV CriteriaMemory Impairment plus at least one of the following
APHASIA (Deterioration of Language function)
APRAXIA (inability to Execute Motor function)
AGNOSIA (inability to Recognise or Naming of Object)
Disturbance in executive functioning
with
• Impairment in occupational or social functioning• Represent a decline from a previous higher level of functioning

Mild cognitive impairment (MCI)Original Criteria
Memory complaint preferably qualified by an informant
Memory impairment for age
Preserved general cognitive function
Intact activities of daily living
Not dementedBy Peterson R, Negash S. CNS Spectr. vol 13 2008
Once the memory loss becomes noticeable to the patient and spouse and falls 1.5 standard deviations below normal on standardized memory tests, the term MCI is applied.
approximately 50% of patients with MCI (roughly 12% per year) will progress to AD over 4 years.
10% of persons >70 and 20–40% of individuals >85 have clinically identifiable memory loss. Harrison's 18 ed > Chapter 371. Dementia
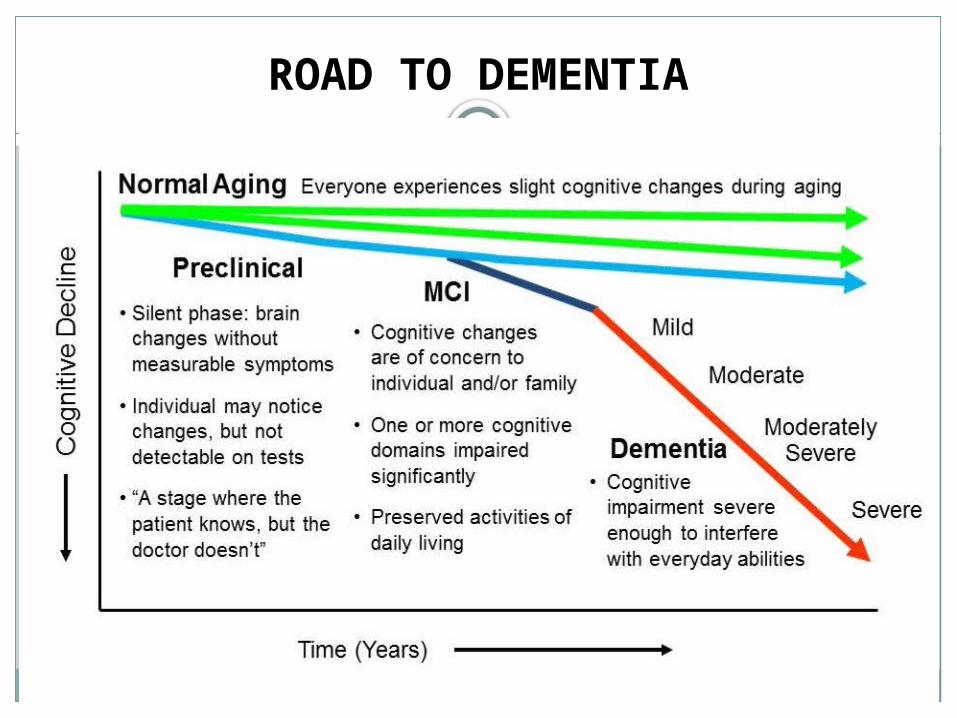
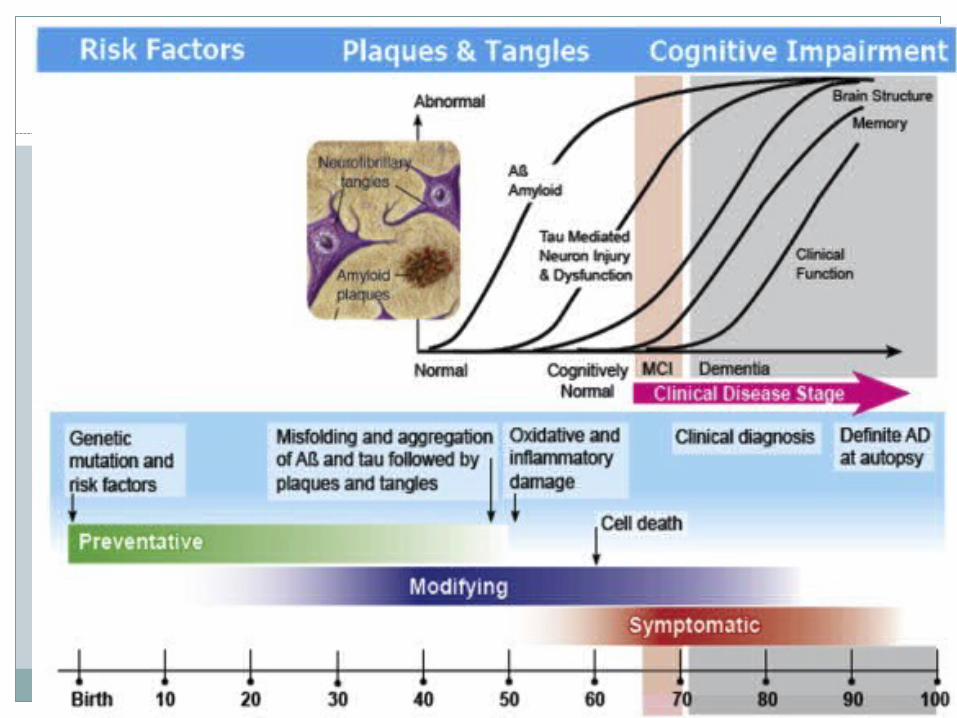
ROAD TO DEMENTIA

Staging of Dementias
MILD: difficulties with checkbook maintenance, complex meal preparations, complicated medication schedules
MODERATE: difficulties with simple food preparation, household or yard work. May need some assistance with self-care
SEVERE: Need considerable assistance with feeding, grooming and toileting
PROFOUND: Largely oblivious to surroundings, totally dependent
TERMINAL: Bed bound; require constant care
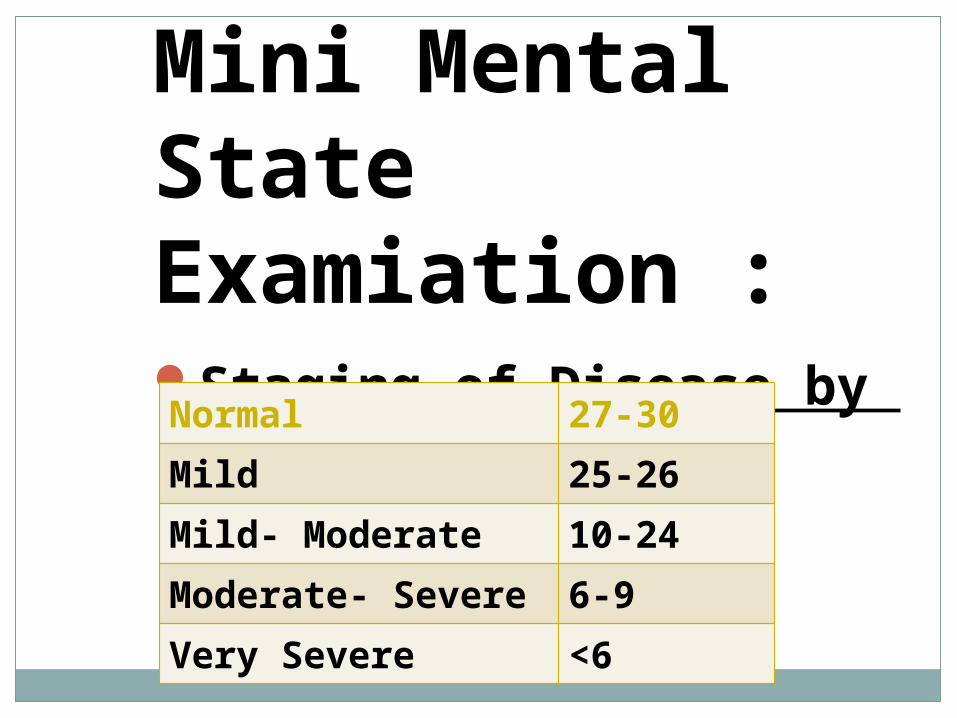
Mini Mental State Examiation :Staging of Disease by MMSENormal 27-30Mild 25-26Mild- Moderate 10-24Moderate- Severe 6-9Very Severe <6

MMSE

MMSE ‘norms’ by Age and Educational Level
Educational level
0-4y 5-8y 9-12y >12yAGE
18-24 23 28 29 30
35-39 23 27 29 30
50-54 22 27 29 30
70-74 21 26 28 29
80-84 19 25 26 28
Classification of Dementias
Primary versus secondary based on the pathophysiology leading to damaged brain tissue
Cortical versus sub-cortical depending on the cerebral location of the primary deficits
Reversible versus irreversible depending on treatment expectations
Early (before age 65) versus late onset

Causes of DementiaParkinsons diseaseHuntington’s disease
Primary Degenerative Dementia:•Alzheimer’s Disease
•Fronto temporal dementia
•Dementia with Lewy Body•Parkinsons disease•Huntington’s disease•Progressive supranuclear palsy•Corticobasal degeneration• ALS Parkinson's dementia complex of Guam•Multisystem atrophy

Secondary Dementia:
VITAMIN Deficiency
ENDOCRINE Chronic Infections
Vit B12/Folic acid
Hypothyroidism HIV
Thiamine B1 hyperthyroidism Neurosyphilis
Nicotinic acid (pellagra)
Cushing Syndrome PML, Prion Tuberculosis, fungal, and protozoal
Hypoparathyroidism
Whipple's disease
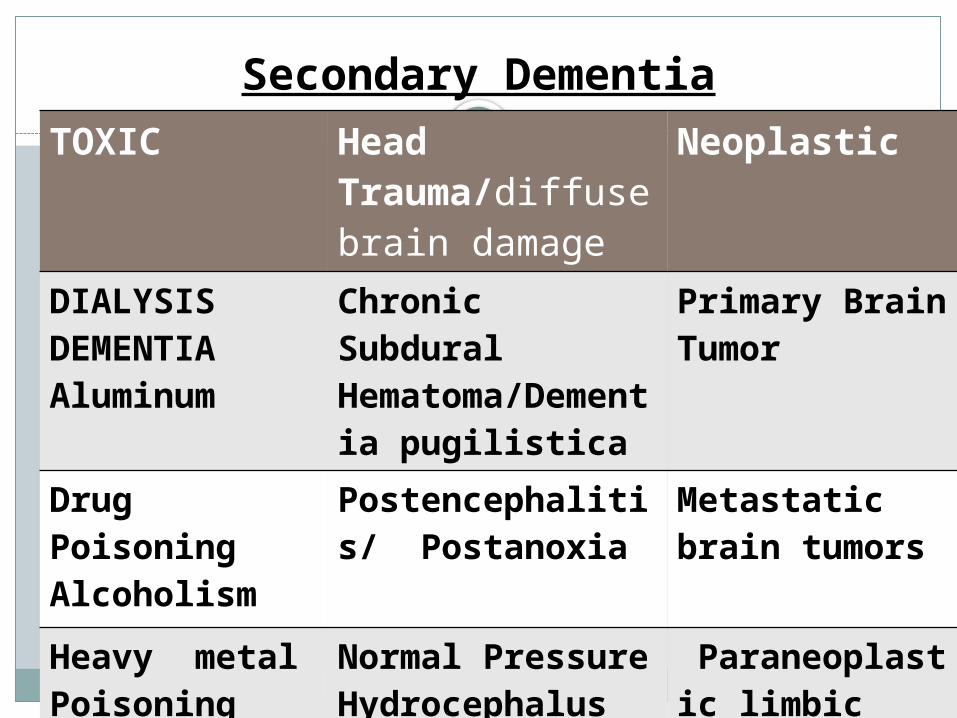
Secondary DementiaTOXIC Head
Trauma/diffuse brain damage
Neoplastic
DIALYSIS DEMENTIAAluminum
Chronic Subdural Hematoma/Dementia pugilistica
Primary Brain Tumor
Drug PoisoningAlcoholism
Postencephalitis/ Postanoxia
Metastatic brain tumors
Heavy metal PoisoningMercury,lead
Normal Pressure Hydrocephalus
Paraneoplastic limbic encephalitis
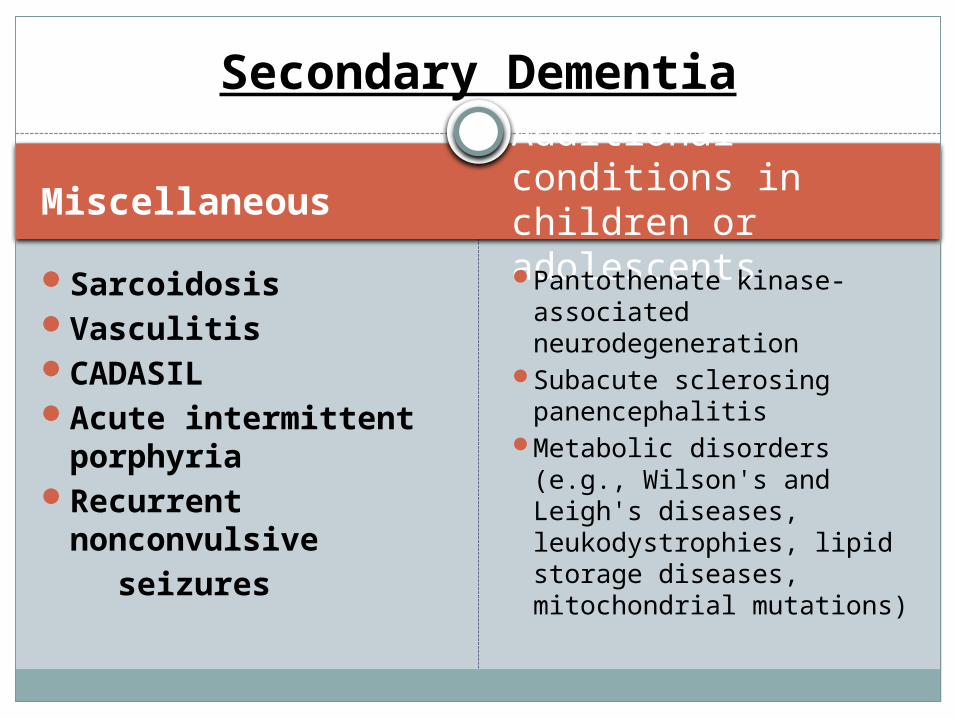
MiscellaneousAdditional conditions in children or adolescents
SarcoidosisVasculitisCADASILAcute intermittent
porphyriaRecurrent
nonconvulsive seizures
Pantothenate kinase-associated neurodegeneration
Subacute sclerosing panencephalitis
Metabolic disorders (e.g., Wilson's and Leigh's diseases, leukodystrophies, lipid storage diseases, mitochondrial mutations)
Secondary Dementia

70% of dementia is Alzheimer’s
10-15% is Vascular dementia
10-15% Lewy Body dementias
5-10% Others
Overall Situation:
USA DATA
Alzheimer’s disease
70 %
Vascular Dementia
15-20%
Lewy Body Dementia
10-15 %
Others 5 %
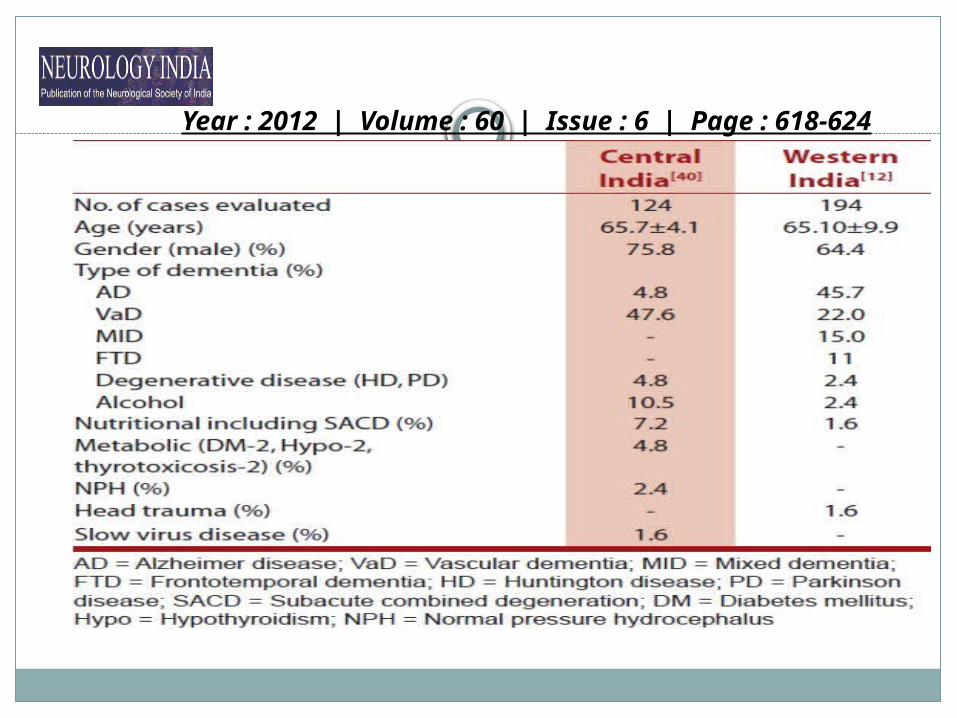
Year : 2012 | Volume : 60 | Issue : 6 | Page : 618-624

Types
CORTICAL SUBCORTICAL MIXED
Alzheimer’s Parkinson’s Vascular Dementia
Frontotemporal Dementia
Huntington’s disease
Lewy body dementia
CJD Normal pressure hydrocaphalus
Neurosyphilis
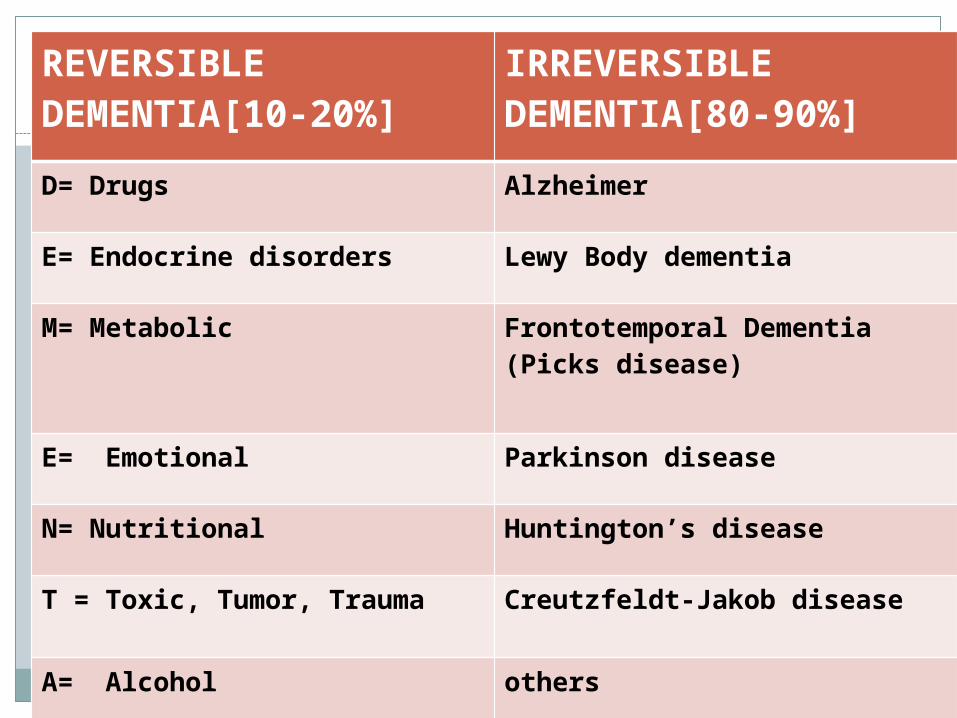
(REVERSIBLE DEMENTIA[10-20%]
IRREVERSIBLE DEMENTIA[80-90%]
D= Drugs Alzheimer
E= Endocrine disorders Lewy Body dementia
M= Metabolic Frontotemporal Dementia (Picks disease)
E= Emotional Parkinson disease
N= Nutritional Huntington’s disease
T = Toxic, Tumor, Trauma Creutzfeldt-Jakob disease
A= Alcohol others
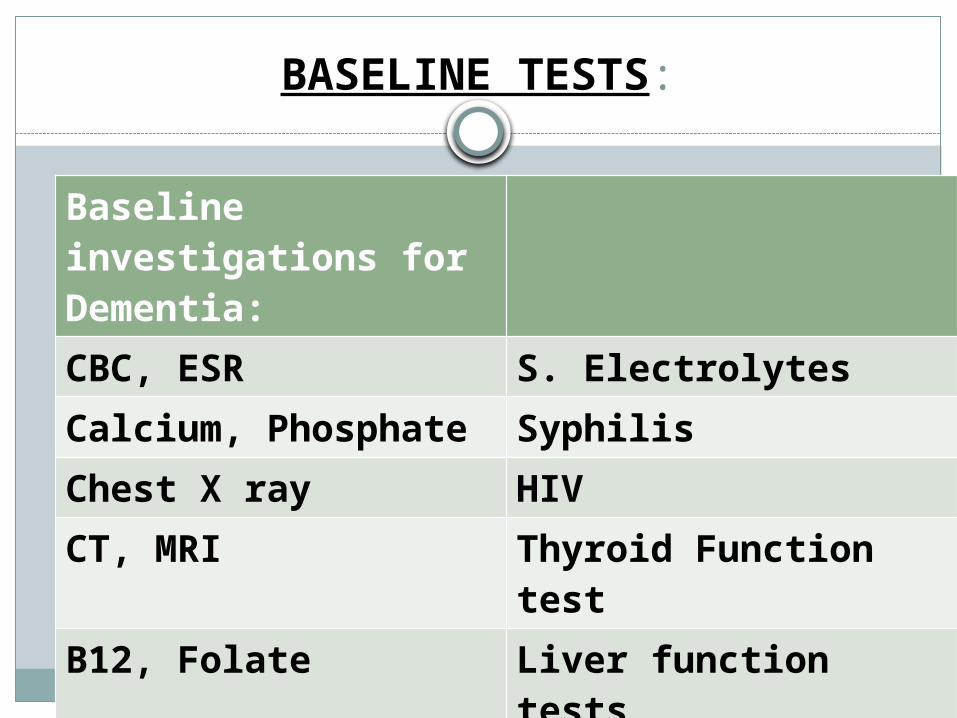
BASELINE TESTS:
Baseline investigations for Dementia:CBC, ESR S. Electrolytes
Calcium, Phosphate Syphilis
Chest X ray HIV
CT, MRI Thyroid Function test
B12, Folate Liver function tests
EEG, ECG Renal Function Tests


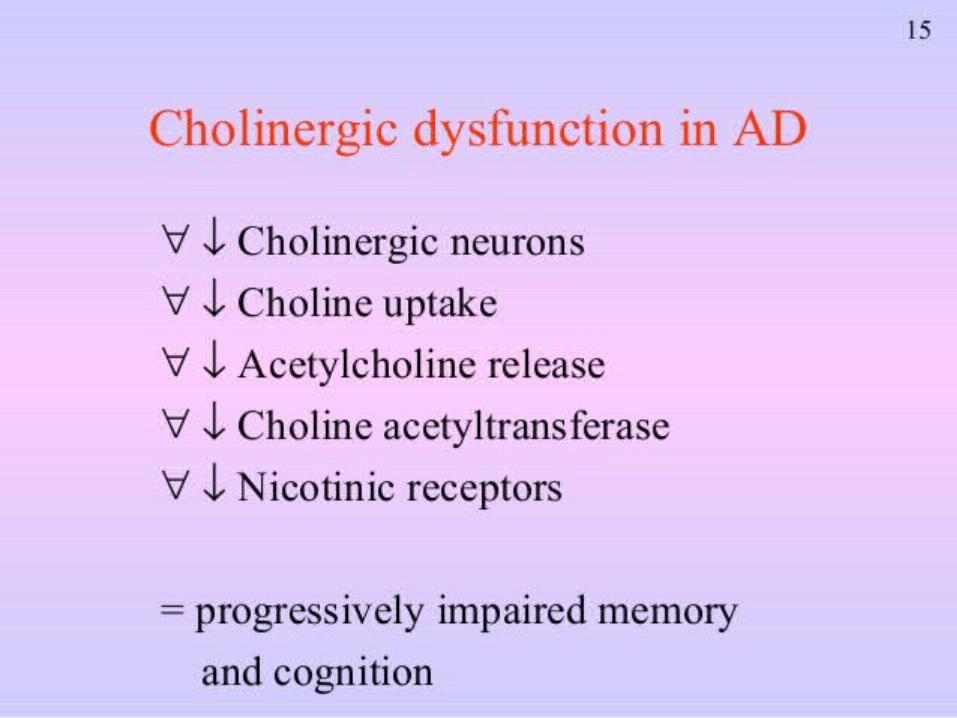
Cholinergic deficit– progressive loss of
cholinergic neurones
– progressive decrease in available ACh
– impairment in ADL, behaviour and cognition
Hippocampus
Cortex
N. basalis Meynert
Pathophysiology of AD (Biochemical)

Alzeimer’s Disease
Loss of cholinergic
neurons
Senile plaques & neurofibrillary
tangels
Glutamate transmission dysfunctiion
30% symptoms
70% Symptoms

Alzheimer’s Staging:
Management :Dementia
Reduce Cognitive Symptoms
Reduce Behaviour Symptoms
Slow disease progression
Delay the Onset of Disease

PHARMACOLOGIC MANAGEMENT OF DEMENTIA
Three broad categories of dementia pharmacotherapy:Symptomatic treatment of memory
disturbanceDisease-modifying treatmentsSymptomatic treatment of behavioral
disturbance

Symptomatic Treatment of AD
. The mainstay of symptomatic treatment of AD, so far, is the cholinergic treatment strategies and most widely used, till now, are the Cholinesterase (ChE) inhibitors.
. These agents •Reduce the metabolism of acetylcholine
•Prolonging its action at cholinergic synapses.

Cholinesterase inhibitors: two classes exist for the treatment of Dementia
Class Inhibit
Dual ChE inhibitors
– Rivastigmine Both AChE
– Tacrine and BuChE
Single ChE inhibitors
– Donepezil AChE
– Galantamine
Weinstock, 1999

FDA-approved drugs
Drug Target dose Approved for
year
Tacrine 40 mg/day Mild to moderate
1993
Donepezil 10 mg daily All stages 1996
Rivastigmine 6 mg twice daily or 9.5-
mg patch daily
All stages 2000
Galantamine target dose 24 mg daily, extended-
release
Mild to moderate
2001
Memantine 10 mg twice daily
Moderate to severe
2003

TACRINE
In 1993 first Drug approved for the treatment of Alzheimer's disease
marketed under the trade name Cognex. Tacrine was first synthesised by Adrie
Albert at the University of Sydney.Tacrine is a centrally
acting anticholinesterase and indirect cholinergic agonist (parasympathomimetic).

Tacrine Pharmacokinetis
Bioavailability 2.4–36% (oral)Protein binding 55%Metabolism Hepatic (CYP1A2)Half-life 2–4 hoursExcretion Renal

Initiation of Treatment Dose Titration
Cognex® is supplied as capsules of tacrine hydrochloride containing 10, 20, 30, and 40 mg of tacrine.
Cognex® brand of tacrine hydrochloride is 40 mg/day (10 mg QID).
This dose should be maintained for a minimum of 4 weeks with every other week monitoring of transaminase levels beginning 4 weeks after initiation of treatment.
Following 4 weeks dose to be increased to 80 mg/day (20 mg QID), providing there LFT is normal
Patients should be titrated to higher doses (120 and 160 mg/day, in divided doses on a QID schedule) at 4-week intervals on the basis of tolerance.
Tacrine dose

Very Common >10%Common 1-10% incidence
Increased LFTsHepatitisNauseaVomitingDiarrheaHeadacheDizziness
Indigestion,Belching Abdominal pain Myalgia Confusion Ataxia Insomnia Weight loss Constipation Somnolence Tremor Anxiety
Tacrine Adverse Effects

Tacrine Overdose
nausea, vomiting, salivation, sweating, bradycardia, hypotension, collapse,convulsions. Atropine is a popular treatment for overdose.

Studies found that it may have a small beneficial effect on cognition and other clinical measures
though study data was limited and the clinical relevance of these findings was unclear.
Tacrine has been discontinued due to hepatotoxicity

DONEPEZIL
In 1996, donepezil, a selective cholinesterase inhibitor, was approved for use in Alzheimer disease.
marketed under the trade name Aricept by its is a centrally acting reversible acetylcholinesterase inhibitor
devoid of peripheral cholinomimetic adverse effects.

Pharmacokinetics
Bioavailability 100 (%) not affected by the time of day or food intake
Protein binding 96%Half-life 70 hourspeak plasma concentration is reached in 3 to 5
hours. It is extensively metabolized by the hepatic
isoenzymes CYP2D6 and CYP3A4. minimally affected by hepatic or renal disease
and no dose adjustment is necessary for these conditions.

In mild to moderate A D Moderate to severe AD
Disease, a starting dose of 5 mg given once daily should be used.
a minimum of four to six weeks, an increase to 10 mg is recommended.
The usual dose is 5 to 10 mg once daily.
indicates the same regimen, but in a minimum of three months, a patient may receive a dose of 23 mg once daily.
The maximum daily dose is 23 mg once daily.
In the UK, the maximum licensed dose is 10 mg
Dosage

CONTRAINDICATIONS
ADVERSE EFFECTS
cardiac disease, cardiac conduction disturbances, chronic obstructive pulmonary disease, asthma, severe cardiac arrhythmias and sick sinus syndrome.
gastrointestinal disorders should use caution because nausea or vomiting may occur.
predisposition to seizures should be treated with caution.
Common side effects include bradycardia
cardiac conduction disturbances
nausea, diarrhea, anorexiaabdominal pain
vivid dreams and Several cases of mania induced by Donepezil have been reported
DONEPEZIL

Clinical Trials of Donepezil
Study (Rogers et al 1996).
Double-blind, placebo-controlled, 30-week, parallel study involving 450 patients with Alzheimer disease
ResultsSignificant
improvement on cognitive and clinical global assessments.
Study (Rogers and Friedhoff 1996).
Dose-ranging study on 161 patients with mild to moderate Alzheimerdisease who received donepezil 1, 3, or 5 mg, or placebo, daily for 12 weeks
ResultsPatients who received
donepezil 5 mg showed significant improvement in the Alzheimer Disease Assessment Scale Cognitive Subscale.


Clinical Trials of Donepezil
Study (Doody et al 2009)A 48-week, randomized,
placebo-controlled trial of donepezil for treatment of patients with mild cognitive impairment
ResultsDonepezil produced small
but significant improvement on the primary measure of cognition, but there was no change on the primary measure of global function
Study (Farlow et al 2011). A pivotal phase 3 study of
the safety and tolerability of increasing donepezil to 23 mg/d compared with continuing 10 mg/d
ResultsGood safety and
tolerability profile of donepezil 23 mg/d supports its favorable risk/benefit ratio in patients with moderate to severe Alzheimer disease.

Mechanism of Action PHARMACOKINETICS
Reversible acetylcholinesterase inhibitor that causes an increase in concentrations of acetylcholine, which in turn enhances cholinergic neurotransmission
Absorption Bioavailability: 36% (PO) Duration: 10 hr (PO); 24 hr (patch) Peak plasma time: 1 hr (PO); 8 hr
(patch)Distribution Protein bound: 40% Vd: 1.8-2.7 L/kgMetabolism Metabolized by cholinesteraseElimination Half-life: 1.5 hr (PO), 3 hr (patch) Total body clearance: 1.2-2.4 L/min Excretion: Urine (97%)
Rivastigmine (Rx) - Exelon

common UNCOMMON
Nausea (PO 47%; patch 21%) Vomiting (PO 31%; patch 6-
19%) Dizziness (PO 21%; patch 2-
7%) Diarrhea (PO 19%; patch 6-
10%) Headache (PO 17%; patch 3-
4%) Anorexia (PO 17%; patch 3-
9%) Abdominal pain (PO 13%;
patch 2-4%)
Decreased weight (3-8%)
Insomnia (PO 9%; patch 1-4%)
Anxiety (PO 5%; patch 3%)
Asthenia (PO 6%; patch 2-3%)
Vertigo (2%)Fatigue (2%)
Rivastigmine - Adverse effects

Rivastigmine Cautions
Renal impairmentHepatic impairmentSick sinus syndromeConduction abnormalities.H/O Asthma or COPDPregnancy .

Transdermal Patch Technology: Reservoir versus Matrix
Nitti VW, et al Urology. 2006;67:657–64
Drug contained in adhesive layer along with polymer
Smaller and thinner than reservoir patches
Reservoir
Matrix
Drug contained in separate layer, with a rate-controlling membrane
Matrix DiffusionControlled Patch
Release Liner
Drug + Polymer + Adhesive
Backing
Rate-ControlledReservoir/Membrane Patch
Dermal Layer
Backing
DrugReservoir
Release Liner Adhesive Layer
Exelon Transdermal 9.5 mg/24 h Patch

Where to Apply Exelon Patch
Apply to:Upper and lower backUpper armChest
The skin should be clean, dry and hairless before the patch is applied
Normal daily activities, such as bathing, are permitted
1Lefèvre G, et al. J Clin Pharmacol 2007;47:471–8.
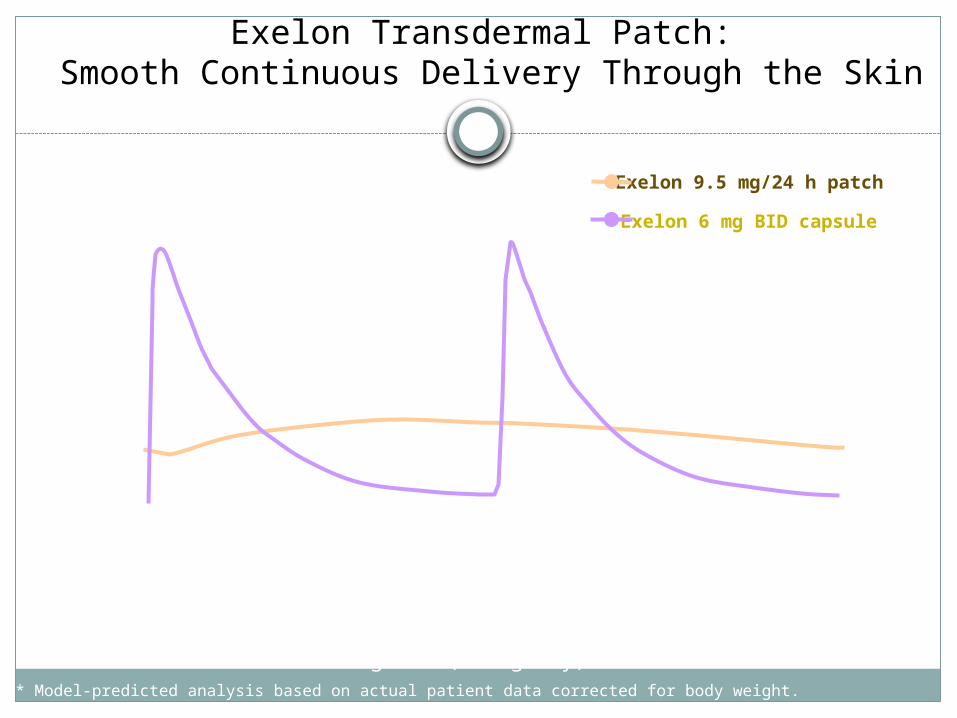
Exelon Transdermal Patch: Smooth Continuous Delivery Through the Skin
Exelon 6 mg BID capsule
Exelon 9.5 mg/24 h patch
Pla
sma
conc
entr
atio
n (n
g/m
L)
Exelon 9.5 mg/24 h patch delivered comparable average concentrations (AUC) to those provided by an oral dose of 6 mg BID (12 mg/day)*
* Model-predicted analysis based on actual patient data corrected for body weight.
0
5
10
15
20
25
0 6 12 18 24
Time (hours)

Starting transdermal ChEI therapy
Rivastigmine 4.6 mg/24 h
patch
Rivastigmine 9.5 mg/24 h
patch
Starting dose Target dose
4 weeks
One-step dose increase


Clinical trials Rivastigmine
Study (Burns et al 2004)
A retrospective analysis of pooled data from 3 randomized, placebo-controlled, double-blind, 6-month trials involving 2126 patients with Alzheimer disease suggests that rivastigmine 6 to 12 mg/day may benefit subjects with more severe disease as well as subjects with mild to moderate impairment
In an open-label, comparative study of rivastigmine with donepezil and galantamine, there were no statistically significant differences between the 3 drugs at 3 months (Aguglia et al 2004).
In a placebo-controlled study, rivastigmine was associated with moderate improvements in dementia associated with Parkinson disease but also with higher rates of nausea, vomiting, and tremor (Emre et al 2004).

Clinical trials Rivastigmine
Results of a 6-month, double-blind, randomized, placebo-controlled study of a transdermal patch in Alzheimer disease shows that the patch provides efficacy similar to the highest doses of capsules with a superior tolerability profile and may offer convenience important to many caregivers and patients (Winblad et al 2007).
A retrospective analysis of a large randomized, placebo-controlled trial of Alzheimer disease patients treated with transdermal rivastigmine or rivastigmine capsule compared to placebo showed greatest treatment effects in patients with more advanced dementia who received rivastigmine, and these were considered to be most likely due to greater decline in the patients treated with placebo (Farlow et al 2011).

Galantamine (Nivalin, Razadyne, Razadyne ER, Reminyl, Lycoremine)
It is an alkaloid that is obtained synthetically or from the bulbs and flowers of Galanthus caucasicus
(Caucasian snowdrop)Galantamine
hydrobromide was approved in 2001 by the FDA Indicated for the treatment of mild to moderate dementia IN Alzheimer's.
Galantamine-MOA
weak competitive and reversible cholinesterase inhibitor in all areas of the body.
It increases the concentration and thereby action of acetylcholine in certain parts of the brain.
It has shown activity in modulating the nicotinic cholinergic receptors on cholinergic neurons to increase acetylcholine release.
Pharmacokinetics DOSAGE
Bioavailability - 80 to 100%
Protein binding- 18%Metabolism-HepaticHalf-life-7 hoursExcretion -
Renal (95%, of which 32% unchanged), fecal (5%)
in twice-a-day tablets, in once-a-day extended-release capsules, and in oral solution.
The tablets come in 4 mg, 8 mg, and 12 mg forms.
The capsules come in 8 mg, 16 mg, and 24 mg forms.
Galantamine

Clinical Trials with Galantamine
Study (Raskind et al 2004). Patients with mild-to-
moderate Alzheimer disease who had been randomized to galantamine therapy in previous trials received open-label continuous galantamine therapy for up to 36 months(Raskind et al 2004).
Results Cognitive decline over 36
months with continuous galantamine treatment was substantially less than the predicted cognitive decline of untreated patients.
Study (Suh et al 2004) Prospective, randomized
multicenter, double-blind study of patients with mild-to-moderate Alzheimer disease: dose 8 mg/day, 16 mg/day, or 24 mg/day ).
Results All dose schedules were
well tolerated with significant improvements in all 3 treatment groups.

common Rare
Nausea, vomiting,Diarrhea, abdominal pain, upper abdominal pain, dyspepsia, stomach discomfort, abdominal discomfort
Bradycardia,First degree atrioventricular block, palpitations, sinus bradycardia, supraventricular extrasystoles, flushing, hypotension
Dizziness, headache, tremor, syncope, lethargy, somnolence
Blurred vision confusion decreased urination dizziness, faintness, or
lightheadedness dry mouth fainting fast, irregular, pounding, or
racing heartbeat or pulse feeling of warmth rapid breathing redness of the face, neck, arms,
and occasionally, upper chest sunken eyes,sweating, thirst
Galantamine-Adverse effects

Memantine
Memantine is the first in a novel class of Alzheimer's disease medications acting on the glutamatergic system by blocking NMDA receptor.
Memantine is approved by the U.S. F.D.A and the European Medicines Agency for treatment of moderate-to-severe Alzheimer's disease

Pharmacokinetic MOA
Bioavailability~100%
Metabolism-Hepatic (<10%)
Half-life- 60–100 hours
Excretion - Renal
Memantine is a low-affinity voltage dependent uncompetitive antagonist at glutamatergic NMDA receptors
non-competitive antagonist at the 5-HT3 receptor, this serotonergic activity in the treatment of Alzheimer's disease is unknown.
Memantine


Common Less common
confusion, dizziness, drowsiness,
headache, insomnia, agitation
hallucinations.
vomiting, anxiety, hypertonia cystitis, increased libidorareextrapyramidal side
effects(such as dystonic reactions etc.) may occur, in particular, in the younger population
Memantine -Adverse effects

Clinical trials Memantine The M-Best Study
The M-Best Study (Benefit and Efficacy in Severely demented patients during treatment with memantine) was a double-blind, placebo-controlled, phase III trial of memantine conducted in Sweden on care-dependent patients with severe dementia (Winblad and Poritis 1999).
The trial population consisted of 161 patients, 51% with vascular dementia and 49% with Alzheimer disease. Treated patients were given 10 mg memantine per day for 12 weeks, and evaluation was done using
Clinical Global Impression of Change by the physician and Behavioral Rating Scale for Geriatric Patients by the nursing staff.
The results supported the hypothesis that memantine treatment leads to functional improvement and reduces care dependence in severely demented patients.

The DOMINO-AD clinical trial
This study looked at 295 people with moderate to severe Alzheimer's disease
All of the study participants had been prescribed donepezil for at least three months, and had been taking a dose of 10mg for at least the six weeks prior to the trial. The trial lasted for 52 weeks.
Participants were divided into four different groups and were each given two drugs. These groups were:
donepezil and memantine donepezil and placebo
memantine placebo donepezil and
memantine placebo donepezil and placebo
memantine
Standardised Mini-Mental State Exam (SMMSE) and their abilities in daily life using the Bristol Activities of Daily Living Scale (BADLS).
All of these measures were taken at the start of the study, after six weeks, at 18 weeks, at 30 weeks and finally after 52 weeks.

The DOMINO-AD clinical trialRESULTS
There were benefits to cognitive function of taking donepezil (about 32% less cognitive decline than those on placebo).
Memantine also showed these benefits, although smaller (about 20% less decline than those on placebo).
Compared to placebo, memantine led to fewer behavioural symptoms developing, showing about 83% fewer symptoms.
The functional benefits of continuing donepezil showed about 23% less deterioration than those on placebo.
The functional benefits of memantine were about 11% less deterioration than those on placebo.
There were also small reductions in caregivers' psychological symptoms with either of the drugs, although these were not large enough to be measured reliably with statistics.
Combined treatment with both donepezil and memantine was not better than treatment with donepezil alone for any of the measures.
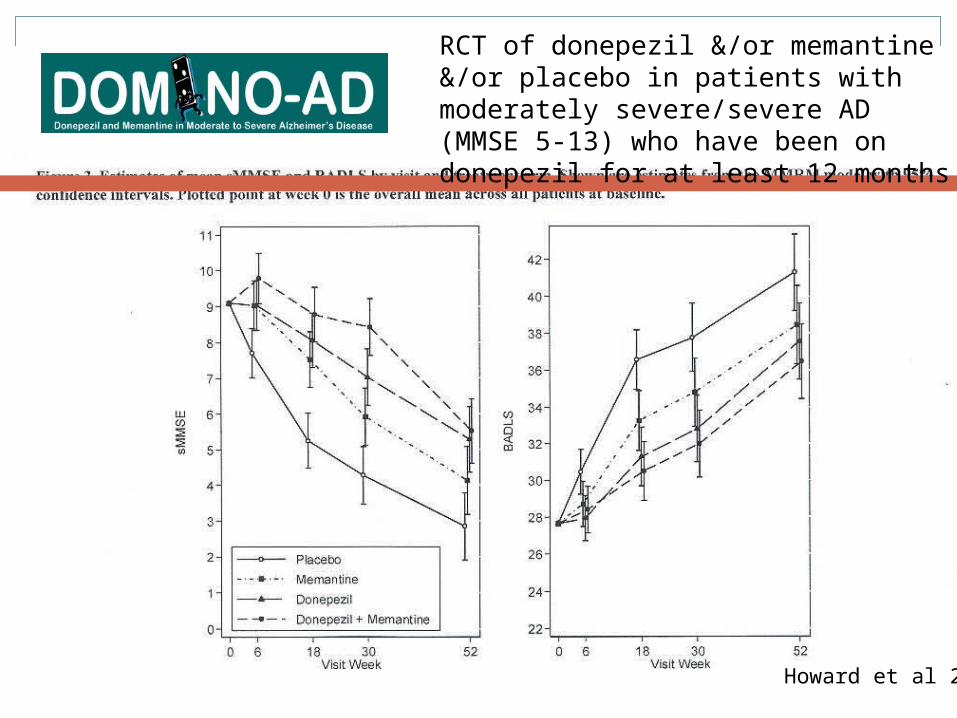
RCT of donepezil &/or memantine &/or placebo in patients with moderately severe/severe AD (MMSE 5-13) who have been on donepezil for at least 12 months
Howard et al 2012

RESULTS
DELAY OF PROGRESSION:
Duration
Memantine alone 2-3 yearsMemantine + Ch E inhibitors
5-6 years
Ch E Inhibitors alone 1.5 years


TREATMENT OPTIONS IN DEMENTIA
AD VaD FTD LBD
DONEPEZIL ChE Inhibitors
No ChE inhibitors
ChE inhibitors
RIVASTIGMIE HMG CoA SSRI SSRI
GALANTAMINE Stroke Prevent
Antipsychotics
Memantine
MEMANTINE Memantine Memantine Levodopa
SSRI Antipsychotic AvoidAntipsycho
tics

Disease-Modifying Agents
Proposed or unregulated drugs which require further studies
Selegeline
Vit-E
Oestrogen
Prednisolone
NSAIDs
Ginkgo biloba
Statins
IVIg
Glycogen syntehtase kinase 3 (GSK 3)
β-secretase inhibitors
γ-secretase inhibitors
α-secretase enhancers
Immunotherapy

Disease-Modifying Agents
Vitamin E Limits free-radical formation, oxidative stress and lipid
peroxidation Promotes survival of cultured neurons exposed to
beta amyloid Clinical trials have not be overwhelmingly convincing
Selegiline MAO-B inhibitor, increases brain catecholamines Also has antioxidant properties Clinical trials – alone and in combination with Vit.
E not effective

Disease-Modifying Agents
Anti-Inflammatory drugs Pathophysiological studies demonstrate a marked
inflammatory reaction induced by amyloid with microglial activation and cytokine release
Case-control studies of subjects taking NSAIDs regularly for arthritis demonstrate a reduced odds-ratio for developing AD
Recently developed NSAIDS currently in clinical trials of AD
Estrogen Body of preclinical evidence that estrogen enhances
cerebral blood flow, prevents atrophy of cholinergic neurons, reduces oxidative stress, and modulates the effects of nerve growth factors

Disease-Modifying Agents
Statins Direct association between amyloid processing and
cholesterol in the brain An indirect effect via decreasing the risk of stroke, since
even small vascular lesions worsen the severity of Alzheimer's disease
Ginkgo Biloba A single placebo-controlled trial with an extract of ginkgo
biloba showed a very modest improvement on cognitive testing
Only 50 percent of the treatment group completed the trial Use of ginkgo not recommended due to limited efficacy and
lack of regulation, including variability in the dosing and contents of herbal extracts

Disease-Modifying Agents
Idebenone Synthetic analogue to Co-Q10, known to have anti-
oxidant properties Controlled clinical trials have shown modest improvement
in cognitive function with highest doses Side effects including liver enzyme abnormalities (non-
serious) along with predominant G-I upsetNegative trials
Propentofylline (stimulates synthesis and release of NGF) Acetyl-L-carnitine (promotes ACh release, increases
acetyltransferase activity, has antioxidant properties)

The amyloid cascade hypothesis & drugs in clinical trials
Adapted from Biochem. Soc. Trans. (2005) 33, 553-558
Statins - promotes alpha secretase
Flurizan - modulates gamma secretase
Lilly - inhibits gamma secretase
Alzhemed - anti-fibrillar
Active and passive immunisation
?

Active and passive beta amyloid immunisation against AD
Vaccination against Aβ42 has proved highly efficacious in mouse models of AD, helping clear brain amyloid and preventing further amyloid accumulation.
In human trials, this approach led to life-threatening complications, including meningoencephalitis
modifications of the vaccine approach using passive immunization with monoclonal antibodies are currently being evaluated in phase 3 trials.

Bapineuzumab (anti-amyloid antibody)

Bapineuzumab (anti-amyloid antibody)
“I think the data are pretty clear from this trial that bapineuzumab is not effective for mild to moderate dementia, and the company was wise to stop the ongoing trials in that population,” said Salloway, who leads one of the trial sites.
Another antibody (solanezumab) also showed cognitive & functional benefit in mild AD.results awaited

Behavioral Problems in ADBehavioral Problems in AD depression (occurs in 20-40% - esp. AD
and VaD) psychosis (occurs in 30- 50%) - usually
see paranoid delusions (theft, infidelity) wandering/purposeless activity agitation/threatening behavior sleep disturbances delirium - minor insults can lead to major
decompensations

Depression and Alzheimer’s
Common early in the course of the illnessIncidence 40-50%Use SSRIs first; avoid anticholinergic
antidepressantsECT can be helpful but may temporarily
worsen cognitive symptoms

Treatment of Depression
Recognize that irritability and/or apathy /withdrawal may be indicative of depression
Allow patient choices and controlIdentify pleasurable activities (such as
singing old songs, pet therapy, etc.)Cognitive enhancers (e.g. Aricept) may help

Agitation
Non-aggressive verbal: complaining, constant requests for
attention, repetition of words, constant talk, screaming
physical: pacing, disrobing, stereotypies, trying to get to a different place
Aggressive Verbal: threats, name calling, obscenities Non-verbal: biting, scratching, spitting,
kicking, pushing, swinging fists

Medications for Agitation
Buspirone – Takes a while to workAntidepressants (SSRIs, Trazodone)Anticonvulsants (esp. valproate)Atypical Antipsychotics (stroke risk
concerning)Low dose narcotics?Estrogen?

Treatment of PsychosisTraditional antipsychotics
Low potency (chlorpromazine)– orthostasis, sedation, anticholinergic
High potency (haloperidol)– EPS/TD but otherwise well tolerated
New generations drugs (e.g. olanzapine, quetiapine, risperidone)- less EPS/TD but still see anticholinergic, BP and sedative effects

Treatment of Insomnia
Sleep hygiene (avoid caffeine, etc.)Treat causative psychiatric or medical
disordersPhsysiological remedies - melatonin, warm
milk, lavendar oilMedications - Benadryl, benzos, sedating
antidepressants or antipsychotics (all these drugs can make memory and confusion worse)
Light Therapy - to reset natural circadian rhythms for sleep

Use of Atypical Antipsychotics
Older, “typical” agents such as haloperidol and thioridazine (mellaril) associated with significant extrapyramidal symptoms
Theoretically combination of dopamine and serotonin effects of atypical agents allow treatment of positive and negative psychotic symptoms with less EPS
Risperidone
Evidence demonstrates efficacy in treatment of psychotic and behavior symptoms in patients with dementia
Exacerbates movement disorder in patients with Parkinson’s
Start .25/day, average daily dose 1-1.5mg/dayEPS in dose dependent manner (6mg/day)Insomnia, hypotension, weight gainElevation of prolactin levels

Olanzapine
Evidence that it is effective in AD patientsIncreases motor symptoms in PD patientsRecommended not to use with PDStart: 1.25-2.5/day, increase to 5/day (dosages of
10-15/day are not more effective!)More sedating than others (more anticholinergic
effects)Sedation, weight gain, orthostatic hypotension,
seizures, glucose intolerance
Quetiapine
Showing promise in patients with AD and PDDoes not exacerbate movement disorder of PD May be first line for PD patients with psychosis12.5 QHS, titrate every 3-5 daysSedation, HA, orthostatic hypotension?Cataract formation
Ziprasidone
New, clinical data lackingNon dose-dependent QT prolongation

Clozapine
Very effective in treating psychosis in PD patients
The most effective agent in treatment of drug induced psychosis in PD
Some efficacy with AD patientsStart: 6.5mg/dayAgranulocytosis, frequent monitoring limits
use

Caregiver Burden
Alzheimer’s caregivers spend an average of 69 to 100 hours per week providing care
Caregivers of patients suffering from dementia(compared to control subjects) reported: 46% more physician visits Over 70% more prescribed drugs More likely to be hospitalized
More than 50% of caregivers are at risk for clinical depression

Behavioral Strategy
Scheduled toileting, prompted voiding for incontinence.
Graded assistance, & positive reinforcement to increase functional independence
Music, esp. during meals, bathing
Walking , Light Exercise

Other Drugs in the Pipeline
Tau protein modulators (to prevent abnormal phosphorylated ‘tau’ protein
Bryostatin – drug that stimulates brain protein production. Reduces B-amyloid levels in mice, enhances memory and learning.
New generation NSAIDS (flubiprofen) – testing in humans looks promising
Immune enhancers (immunoglobulin)New vaccines and new anticholinesterases
(huperzine A)LADOSTIGIL-multimodal drug
Dementia and clinical trialsWhere next?
Disease modifying drugs need to start early Much of the damage been done by the time the patient presents with
dementiaWe need to consider new targets
Is amyloid the cause, or just a byproduct? What about tau? What about inflammation?
We need to have better outcome measures Current assessments do not always reflect outcomes that matter to
patients and families. We need more patients to enter clinical trials
Recruitment into dementia clinical trials is a fraction of the number entering cancer trials

Take Home Points
Cholinesterase Inhibitors are MODESTLY effective in treatment of mild to moderate AD
Cholinesterase Inhibitors are probably effective in more severe AD
No large difference in efficacy between agents, but Donepezil more easily titrated and tolerated
Evidence to support use of cholinesterase inhibitors for vascular and vascular/AD dementia
Memantine looks to be effective for more severe AD and vascular dementia, will likely be used in combination with cholinesterase inhibitors

Related Documents











