Treatment of Advanced Primary and Recurrent Diffuse Pigmented Villonodular Synovitis of the Knee by Kingsley R. Chin, Stephen J. Barr, Carl Winalski, David Zurakowski, and Gregory W. Brick J Bone Joint Surg Am Volume 84(12):2192-2202 December 1, 2002 ©2002 by The Journal of Bone and Joint Surgery, Inc.

Treatment of Advanced Primary and Recurrent Diffuse Pigmented Villonodular Synovitis of the Knee by Kingsley R. Chin, Stephen J. Barr, Carl Winalski, David.
Dec 28, 2015
Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript
Treatment of Advanced Primary and Recurrent Diffuse Pigmented Villonodular Synovitis of the Knee
by Kingsley R. Chin, Stephen J. Barr, Carl Winalski, David Zurakowski, and Gregory W. Brick
J Bone Joint Surg AmVolume 84(12):2192-2202
December 1, 2002
©2002 by The Journal of Bone and Joint Surgery, Inc.

Figs. 1-A through 1-I Posterior approach to the left knee.
Kingsley R. Chin et al. J Bone Joint Surg Am 2002;84:2192-2202
©2002 by The Journal of Bone and Joint Surgery, Inc.

The fibular head is identified, and the peroneal nerve is protected.
Kingsley R. Chin et al. J Bone Joint Surg Am 2002;84:2192-2202
©2002 by The Journal of Bone and Joint Surgery, Inc.

The lateral head of the gastrocnemius muscle and the lateral superior genicular artery are identified.
Kingsley R. Chin et al. J Bone Joint Surg Am 2002;84:2192-2202
©2002 by The Journal of Bone and Joint Surgery, Inc.

The posterolateral aspect of the capsule is exposed.
Kingsley R. Chin et al. J Bone Joint Surg Am 2002;84:2192-2202
©2002 by The Journal of Bone and Joint Surgery, Inc.

Dissection proceeds between the medial head of the gastrocnemius and the semimembranosus muscle.
Kingsley R. Chin et al. J Bone Joint Surg Am 2002;84:2192-2202
©2002 by The Journal of Bone and Joint Surgery, Inc.

The medial and lateral exposures are joined by blunt dissection beneath the midline structures containing the tibial nerve and the popliteal vessels.
Kingsley R. Chin et al. J Bone Joint Surg Am 2002;84:2192-2202
©2002 by The Journal of Bone and Joint Surgery, Inc.

A T incision is made in the lateral aspect of the capsule, over the lateral femoral condyle, and the incision is continued to the level of the popliteus tendon and the posterior horn of the lateral
meniscus.
Kingsley R. Chin et al. J Bone Joint Surg Am 2002;84:2192-2202
©2002 by The Journal of Bone and Joint Surgery, Inc.

All diffuse pigmented villonodular tissue is removed with careful dissection from the intercondylar region and laterally from the region of the popliteus sheath.
Kingsley R. Chin et al. J Bone Joint Surg Am 2002;84:2192-2202
©2002 by The Journal of Bone and Joint Surgery, Inc.
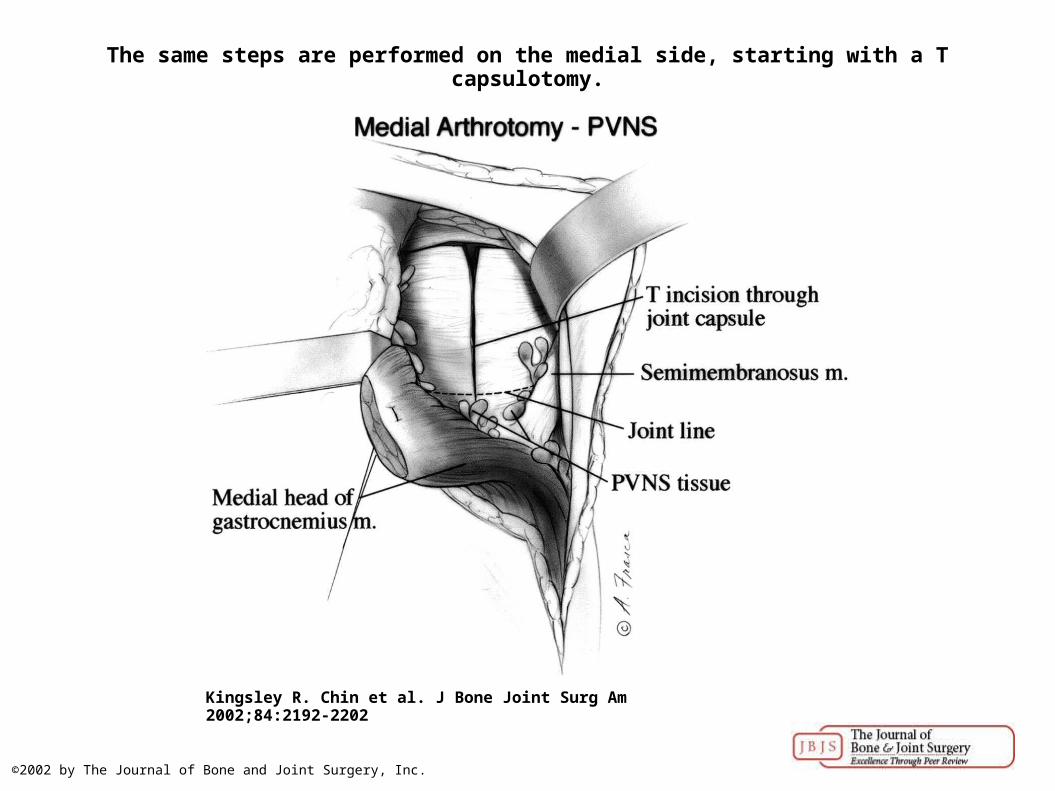
The same steps are performed on the medial side, starting with a T capsulotomy.
Kingsley R. Chin et al. J Bone Joint Surg Am 2002;84:2192-2202
©2002 by The Journal of Bone and Joint Surgery, Inc.

For the anterior approach to the knee, a standard anteromedial parapatellar incision is extended distal to the infrapatellar fat pad, passing lateral to the anterior horn of the medial meniscus.
Kingsley R. Chin et al. J Bone Joint Surg Am 2002;84:2192-2202
©2002 by The Journal of Bone and Joint Surgery, Inc.

Figs. 3-A through 3-D A twenty-two-year-old woman was referred with pain, swelling, and advanced pigmented villonodular synovitis of the left knee fifteen months after arthroscopic
synovectomy.
Kingsley R. Chin et al. J Bone Joint Surg Am 2002;84:2192-2202
©2002 by The Journal of Bone and Joint Surgery, Inc.

Figs. 3-C and 3-D Postoperative sagittal (Fig. 3-C) and coronal (Fig. 3-D) T1-weighted magnetic resonance images of the knee, showing complete removal of pigmented villonodular tissue from
the knee 7.5 years after combined posterior and anterior synovectom...
Kingsley R. Chin et al. J Bone Joint Surg Am 2002;84:2192-2202
©2002 by The Journal of Bone and Joint Surgery, Inc.
Related Documents











