1 PowerPoint Slides English Text Mandarin Chinese Translation Treatment Modalities: Drug Therapy, Part 2 VideoTranscript 2 Professional Oncology Education Treatment Modalities: Drug Therapy, Part 2 Time: 18:16 2 18:16 Jeffrey Bryan, Pharm.D. Clinical Pharmacy Specialist Pharmacy Clinical Programs The University of Texas MD Anderson Cancer Center MD Anderson Jeffrey Bryan, Pharm.D. Treatment Modalities: Treatment Modalities: Treatment Modalities: Treatment Modalities: Drug Therapy Part II Drug Therapy Part II Drug Therapy Part II Drug Therapy Part II Treatment Modalities: Treatment Modalities: Drug Therapy Drug Therapy – – Part II Part II Jeffrey Bryan, Pharm.D. Clinical Pharmacy Specialist Pharmacy Clinical Programs Hello, my name is Jeffrey Bryan. I am a Clinical Pharmacy Specialist with The University of Texas MD Anderson Cancer Center. I would like to welcome you to the second part of Treatment Modalities: Drug Therapy. Jeffrey Bryan MD Anderson

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

1
PowerPoint Slides English Text Mandarin Chinese Translation
Treatment Modalities: Drug Therapy, Part 2 VideoTranscript
治疗方法:药物疗法,第 2 部分 视频文本
Professional Oncology Education Treatment Modalities: Drug Therapy, Part 2 Time: 18:16
专业人员肿瘤教学讲座 治疗方法:药物疗法,第 2 部分 时间: 18:16
Jeffrey Bryan, Pharm.D. Clinical Pharmacy Specialist Pharmacy Clinical Programs The University of Texas MD Anderson Cancer Center
德克萨斯大学 MD Anderson 癌症中心 药学临床计划 临床药学专家
Jeffrey Bryan, Pharm.D.
Treatment Modalities: Treatment Modalities: Treatment Modalities: Treatment Modalities:
Drug Therapy Part IIDrug Therapy Part IIDrug Therapy Part IIDrug Therapy Part II
Treatment Modalities: Treatment Modalities:
Drug Therapy Drug Therapy –– Part II Part II
Jeffrey Bryan, Pharm.D.
Clinical Pharmacy Specialist
Pharmacy Clinical Programs
Hello, my name is Jeffrey Bryan. I am a Clinical Pharmacy Specialist with The University of Texas MD Anderson Cancer Center. I would like to welcome you to the second part of Treatment Modalities: Drug Therapy.
大家好,我叫 Jeffrey Bryan,是德克萨斯大学 MD
Anderson 癌症中心的临床药学专家。欢迎大家参加治疗方法:药物疗法第二部分的学习。

2
Treatment Modalities: Treatment Modalities: Treatment Modalities: Treatment Modalities:
Drug Therapy Part IIDrug Therapy Part IIDrug Therapy Part IIDrug Therapy Part II
ObjectivesObjectivesObjectivesObjectives
Upon completion of this lesson, participants will
be able to:
• Discuss the goals and roles of drug therapy
• Identify classifications of chemotherapy
• Differentiate between chemotherapy, hormone,
immune-based, and targeted therapy
• Identify common toxicities of drug treatment
Upon completion of this lesson, participants should be able to discuss the goals and roles of drug therapy; identify classifications of chemotherapy; differentiate between chemotherapy, hormone therapy, immune-based therapy, and targeted therapy; and identify some common toxicities associated with chemotherapeutic agents.
在完成本次课程之后,学员应该能够讨论药物疗法的目标和作用;识别化疗的分类;能区分化疗、荷尔蒙疗法、免疫疗法和靶向疗法;以及能够识别与化疗药剂相关的一些常见毒性反应。
Treatment Modalities: Treatment Modalities: Treatment Modalities: Treatment Modalities:
Drug Therapy Part IIDrug Therapy Part IIDrug Therapy Part IIDrug Therapy Part II
Immune-based Therapy and
Targeted Therapy
At first, we will start off with immune-based therapy, then discuss targeted therapy.
首先在一开始我们会谈谈免疫疗法,然后会讨论靶向疗法。

3
Treatment Modalities: Treatment Modalities: Treatment Modalities: Treatment Modalities:
Drug Therapy Part IIDrug Therapy Part IIDrug Therapy Part IIDrug Therapy Part II
ImmuneImmuneImmuneImmune----based Therapybased Therapybased Therapybased Therapy
• Treatment with agents from biologic sources
and/or agents able to affect biologic responses
• Stimulates host’s immune system to fight
against cancer
• A means to deliver systemic anticancer therapy
The idea of stimulating or augmenting the body’s own immune system to fight or prevent cancer led to the development of immune-based therapies. This is now referred to by many as the fourth cancer treatment modality. The idea is to use various cytokines and other biologic response modifiers, such as interferon, monoclonal antibodies, and vaccines, to stimulate the host immune system to attack the tumors.
开发免疫疗法的基本构想是刺激或增强机体自身对抗或预防癌症的免疫系统。现在许多人将免疫疗法称为第四种癌症治疗方法。其中的原理是使用各种细胞因子和其他生物反应调节剂,例如干扰素、单克隆抗体和疫苗,来刺激宿主免疫系统攻击肿瘤。
Treatment Modalities: Treatment Modalities: Treatment Modalities: Treatment Modalities:
Drug Therapy Part IIDrug Therapy Part IIDrug Therapy Part IIDrug Therapy Part IIImmuneImmuneImmuneImmune----based Therapy based Therapy based Therapy based Therapy ----Interferons/InterleukinsInterferons/InterleukinsInterferons/InterleukinsInterferons/Interleukins
• Cytokines - proteins that are normally produced in
the body in response to stress
• Act as chemical signals to:
– Directly slow tumor growth
– Slow angiogenesis (formation of new blood vessels)
– Stimulate cancer cells to produce antigens
– Stimulate immune system cells to attack cancer cells
• Interferon-alfa: CML, melanoma, lymphoma
• Interleukin-2 (IL-2): melanoma, renal cell
Interferons, interleukins are part of a family of cytokines and proteins that are normally produced in the body in response to stress or inflammation. Genetically-engineered interferon and interleukin have been shown to have anti-tumor effects in several malignancies. Although their toxicities differ from conventional chemotherapy, they are associated with a constellation of symptoms, such as fever, chills, myalgias, depression, and sometimes myelosuppression.
干扰素、白介素属于同一类细胞因子和蛋白质。在正常情况下机体会在出现压力或炎症时,产生这些细胞因子和蛋白质。基因工程干扰素和白介素已经显示出对数种恶性疾病具有抗肿瘤作用。其毒性与传统化疗有所不同,包括一系列症状,例如发烧、寒颤、肌痛、抑郁,有时会出现骨髓抑制。

4
Treatment Modalities: Treatment Modalities: Treatment Modalities: Treatment Modalities:
Drug Therapy Part IIDrug Therapy Part IIDrug Therapy Part IIDrug Therapy Part IIImmuneImmuneImmuneImmune----based Therapy based Therapy based Therapy based Therapy ----Monoclonal Antibodies (MoAb)Monoclonal Antibodies (MoAb)Monoclonal Antibodies (MoAb)Monoclonal Antibodies (MoAb)
• Developed to target specific proteins/antigens
involved in the development and progression
of cancer
• High specificity to tumor-specific targets
• Different toxicity profile from conventional
cytotoxic agents
• Synergy with chemotherapy agents
In recent years, a number of monoclonal antibodies have been developed for the treatment of patients with a variety of cancers. These agents target specific proteins or antigens that are expressed on tumor cells. Additionally, these agents can be given as a single agent or in combination with conventional chemotherapy without overlapping or increasing toxicity.
近年开发出了多种单克隆抗体,用于治疗各种癌症患者。这些药物以肿瘤细胞表达的特有蛋白质或抗原为靶的。此外,这些药剂可以单独用药,或者与传统化疗联合用药,只要毒性不会重叠或增强。
Treatment Modalities: Treatment Modalities: Treatment Modalities: Treatment Modalities:
Drug Therapy Part IIDrug Therapy Part IIDrug Therapy Part IIDrug Therapy Part II
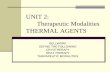
• Four Types of MoAbs
Murine (100% Murine)
Chimeric (30% Murine, 70% human)
Humanized (5% Murine, 95% human)
Human (100% human)
Monoclonal Antibodies (MoAbs)Monoclonal Antibodies (MoAbs)Monoclonal Antibodies (MoAbs)Monoclonal Antibodies (MoAbs)
Mouse
Human
(Murine = Mouse)
Monoclonal antibodies are synthesized from different sources. The majority of monoclonal antibodies are chimeric, meaning that they have a murine variable region fused to a human constant region or humanized, meaning they are predominantly of human origin.
单克隆抗体是不同来源的合成抗体。大多数单克隆抗体都是嵌合型,这是指这些抗体的鼠源可变区与人源恒定区相融合,或者被人源化,表示这些蛋白基本上是人源。

5
Treatment Modalities: Treatment Modalities: Treatment Modalities: Treatment Modalities:
Drug Therapy Part IIDrug Therapy Part IIDrug Therapy Part IIDrug Therapy Part IIMonoclonal Antibodies Monoclonal Antibodies Monoclonal Antibodies Monoclonal Antibodies ----Conjugated vs. UnconjugatedConjugated vs. UnconjugatedConjugated vs. UnconjugatedConjugated vs. Unconjugated
Additionally, monoclonal antibodies can be conjugated or unconjugated. Conjugated monoclonal antibodies have a toxin or a radionucleotide attached to the antibody that allows the toxin to be delivered to the tumor. Whereas unconjugated monoclonal antibodies rely on activating the host immune system, which in turn attacks the tumor.
此外,单克隆抗体可以是结合蛋白或非结合蛋白。结合型单克隆抗体在抗体上连附了某种毒素或放射性核素,以便将毒素运到肿瘤处。而非结合型单克隆抗体则是依靠激活宿主免疫系统,从而攻击肿瘤。
Treatment Modalities: Treatment Modalities: Treatment Modalities: Treatment Modalities:
Drug Therapy Part IIDrug Therapy Part IIDrug Therapy Part IIDrug Therapy Part IIImmuneImmuneImmuneImmune----based Therapy based Therapy based Therapy based Therapy ----Monoclonal AntibodiesMonoclonal AntibodiesMonoclonal AntibodiesMonoclonal Antibodies
This is a list of some of the FDA-approved monoclonal antibodies along with their main characteristics and indications. You can see that each monoclonal antibody has a very specific antigen it targets. For example, rituximab targets CD20 on B-cells and gemtuzumab target CD33 on myeloid cells.
这份表格列出了 FDA 批准的部分单克隆抗体及其主要特征和适应症。可以看到每种单克隆抗体都有特异性极强的靶的抗原。例如,利妥昔单抗的靶的是 B 细胞的 CD20,而吉妥单抗是针对髓系细胞的
CD33。

6
Treatment Modalities: Treatment Modalities: Treatment Modalities: Treatment Modalities:
Drug Therapy Part IIDrug Therapy Part IIDrug Therapy Part IIDrug Therapy Part II
Targeted TherapyTargeted TherapyTargeted TherapyTargeted Therapy
• Agents that specifically target cell processes that
are aberrant or more abundant in malignant cells
than normal cells
• Target cellular processes and signaling pathways
that affect:
– Cell growth and differentiation
– Angiogenesis (new blood vessel formation)
– Apoptosis (programmed cell death)
– Cell motility
We have discussed conventional chemotherapy, hormone therapy, and immune-based therapy. Now, I will spend some time discussing what is called targeted therapy and the implications on the treatment of cancer. A major limitation of current cytotoxic therapy is the lack of sensitivity on malignant cells. Chemotherapy can affect any cell that is rapidly dividing whether it be normal or malignant. As our knowledge of tumor biology increases, novel therapeutic strategies, such as targeted therapy have evolved. What is unique about targeted therapy [is] that it targets processes. Targeted therapy blocks growth of cancer cells by interfering with specific molecules, a process very different from conventional chemotherapy, hormone therapy, and immune-based therapy.
我们已经讨论了传统的化疗、荷尔蒙疗法和免疫疗法。现在我会花些时间讨论何谓靶向疗法及其治疗癌症的作用。目前细胞毒性疗法的主要局限性是缺乏对恶性细胞的敏感性。化疗会对快速分裂的所有细胞产生作用,无论是正常细胞还是恶性细胞都不能幸免。随着我们癌症生物学知识的不断增加,出现了新型的治疗策略,包括靶向疗法。靶向疗法的独特之处在于其靶向过程。靶向疗法通过干扰特定分子来阻断癌症的生长。这一过程与传统的化疗、荷尔蒙疗法和免疫疗法迥然不同。
Treatment Modalities: Treatment Modalities: Treatment Modalities: Treatment Modalities:
Drug Therapy Part IIDrug Therapy Part IIDrug Therapy Part IIDrug Therapy Part II
Targeted Therapy (continued)Targeted Therapy (continued)Targeted Therapy (continued)Targeted Therapy (continued)
• Systemic-like chemotherapy designed to target
cancer cells
• Optimal targets vary widely between cancers
• Effectiveness depends on the expression of
target antigen, receptor, or other molecules
• Different toxicity profile from conventional
cytotoxic agents
• Intravenous and oral formulations
Similar to conventional chemotherapy, targeted therapy is considered systemic therapy, but designed to affect predominantly cancer cells. For this reason, these drugs are associated with very different and sometimes less side effects. The effectiveness of these drugs often depends on the expression of the target antigen receptor and other molecules on the cancer cells. A benefit of targeted therapy is that they often come in oral formulations.
与传统化疗类似,靶向疗法也被认为是全身疗法,只是被设计成主要作用于癌细胞。因此,这些药物的相关副作用完全不同,而且有时候副作用较少。这些药物的效果常常取决于靶的抗原受体和癌细胞上其他分子的表达情况。靶向疗法的优点之一是其剂型常常是口服剂。

7
Treatment Modalities: Treatment Modalities: Treatment Modalities: Treatment Modalities:
Drug Therapy Part IIDrug Therapy Part IIDrug Therapy Part IIDrug Therapy Part II
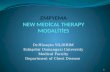
Targeted Therapy Targeted Therapy Targeted Therapy Targeted Therapy ---- Mechanism of ActionMechanism of ActionMechanism of ActionMechanism of Action
This diagram shows the different targets for drug therapy. You can see that outside of the cell, or on the cell surface, there are growth factors that bind to the receptors. The binding triggers a cascade of intracellular events involving many tyrosine kinases. This results in increasing cell growth, proliferation, and differentiation along with angiogenesis. By inhibiting one of these proteins, you can prevent the downstream effects.
这张图显示了药物疗法的不同靶的。可以看到,细胞外侧,也就是细胞表面,有生长因子与受体结合。这样的结合会触发涉及许多酪蛋白激酶的细胞内级联放大反应,造成细胞生长、繁殖和分化以及血管生成的增加。如果抑制其中一种蛋白质的活性,就可以防止出现这些下游作用。
Treatment Modalities: Treatment Modalities: Treatment Modalities: Treatment Modalities:
Drug Therapy Part IIDrug Therapy Part IIDrug Therapy Part IIDrug Therapy Part II
Targeted Therapy Targeted Therapy Targeted Therapy Targeted Therapy ---- Mechanism of ActionMechanism of ActionMechanism of ActionMechanism of Action
This is another depiction of the targets for some of our monoclonal antibodies and/or tyrosine kinase inhibitors. For instance, gemtuzumab targets the CD33. Gemtuzumab is complexed with a toxin called calicheamicin. Upon binding the CD33, the calicheamicin is engulfed by the cell, which causes ultimate cell death. On the bottom half of this picture, a lot of these monoclonal antibodies are used for solid tumors. But these target cell processes. And internally a lot of the tyrosine kinases such as imatinib and dasatinib target pathways that are responsible for cell differentiation and cell survival.
这张图示说明的是某些单克隆抗体和/或酪蛋白激酶抑制剂的靶的。例如,吉妥单抗的靶的是 CD33。吉妥单抗结合了名为加里刹霉素的一种毒素。与 CD33 结合后,加里刹霉素被细胞吞噬,最终造成细胞凋亡。在这张图下半部分的许多单克隆抗体用于治疗实体肿瘤。但这些单克隆抗体的靶的是细胞过程。诸如伊马替尼和达沙替尼等许多酪蛋白激酶抑制剂在细胞内部的靶的是负责细胞分化和细胞生存的路径。

8
Treatment Modalities: Treatment Modalities: Treatment Modalities: Treatment Modalities:
Drug Therapy Part IIDrug Therapy Part IIDrug Therapy Part IIDrug Therapy Part II
Targeted Therapy Targeted Therapy Targeted Therapy Targeted Therapy ---- Summary of AgentsSummary of AgentsSummary of AgentsSummary of Agents
Vascular endothelial growth factor = VEGF
Epidermal growth factor receptor = EGFRTyrosine kinase inhibitor = TKI
Platelet-derived growth factor receptor = PDGFR
This list lists --- this table lists many FDA-approved targeted therapies and summarizes their mechanisms of action, targets, and indications. For example, bevacizumab targets VGEF, which is the vascular endothelial growth factor. And cetuximab covers --- cetuximab binds to the epidermal growth factor receptor. And we get a whole list of tyrosine kinase inhibitors, which target the cell processes within the cell, for instance, imatinib, dasatinib and erlotinib.
这张表格列出了许多 FDA 批准的靶的疗法及其作用机制、靶的和适应症总结。例如,贝伐单抗的靶的是
VGEF,即血管内皮生长因子。妥昔单抗与表皮生长因子受体相结合。这里还有完整的酪蛋白激酶抑制剂列表,其靶的是细胞内的细胞过程。这些药物包括伊马替尼、达沙替尼和厄洛替尼。
Treatment Modalities: Treatment Modalities: Treatment Modalities: Treatment Modalities:
Drug Therapy Part IIDrug Therapy Part IIDrug Therapy Part IIDrug Therapy Part IIImmuneImmuneImmuneImmune----based and Targeted Therapy based and Targeted Therapy based and Targeted Therapy based and Targeted Therapy ----SummarySummarySummarySummary
• Blocks the growth of cancer cells by interfering with
specific targeted molecules needed for tumor growth
• Important role as monotherapy or in combination with
chemotherapy for the treatment of cancers
• Future of cancer drug development
In summary, immune-based therapy and targeted therapy blocks the growth of cancer cells by interfering with specific targeted molecules needed for tumor growth. These play an important role for monotherapy and in combination in chemotherapy for the treatment of cancers. And this is the future of cancer drug development.
总之,免疫疗法和靶向疗法通过干扰肿瘤生长必需的特定靶向分子,阻止癌细胞的生长。这些疗法在癌症的单药治疗和合并化疗治疗时起着重要作用,是癌症药物开发的未来。

9
Treatment Modalities: Treatment Modalities: Treatment Modalities: Treatment Modalities:
Drug Therapy Part IIDrug Therapy Part IIDrug Therapy Part IIDrug Therapy Part II
Dosing and Toxicity
Now we are going to switch gears a little bit and talk about dosing and toxicity.
现在让我们转而谈谈给药和毒性。
Treatment Modalities: Treatment Modalities: Treatment Modalities: Treatment Modalities:
Drug Therapy Part IIDrug Therapy Part IIDrug Therapy Part IIDrug Therapy Part II
Dosing StrategiesDosing StrategiesDosing StrategiesDosing Strategies
• Body Surface Area (BSA)
– BSA(m2) =
• Single Agent Chemotherapy
– Less toxicity to normal tissue BUT
less toxicity to cancer cells
– Palliative role
• Combination Chemotherapy
– Different mechanisms of action
– Greater cell kill
– Fewer resistant cell lines
height (cm) x weight (kg)
3600√
Conventional chemotherapy is generally dosed off of BSA, which is calculated off the height and weight of the patient. For instance, a dose of 20 mg/m
2 in
the BSA of a patient is 2, the dose will be 40 mg. Oftentimes, single-agent chemotherapy is used in the palliative role, but it is generally less toxic and less toxic to cancer cells, whereas chemotherapy given in combination capitalizes on different mechanisms of action of the chemotherapy for achieving greater cell kill and preventing resistant cell lines.
传统化疗一般是按照 BSA 确定剂量,而 BSA 是采用患者的身高和体重计算而得到的。例如,如果剂量为
20 mg/m2,而患者的 BSA 为 2,则剂量为 40 mg。单药化疗常常用于姑息性护理,毒性一般较小,对癌症细胞的毒性也较低;而合并用药的化疗则利用化疗的不同作用机制,达到更好的细胞杀灭效果,预防产生耐药细胞株。

10
Treatment Modalities: Treatment Modalities: Treatment Modalities: Treatment Modalities:
Drug Therapy Part IIDrug Therapy Part IIDrug Therapy Part IIDrug Therapy Part II
Dosing Strategies (continued)Dosing Strategies (continued)Dosing Strategies (continued)Dosing Strategies (continued)
• Dose Intensity - dose delivered over a specified
period of time (mg/m2/week)
– ⇑ dose intensity = ⇑ response rate
– Leukemias, lymphomas, breast, ovarian
• Dose Density - shortening the usual interval between
doses; designed to maximize the drug’s effects on
tumor growth kinetics
– May require growth factor support
Now that we are familiar with dosing chemotherapy, effecting --- effective dosing can be a factor limiting the ability of chemotherapy to achieve a cure. There are generally two types of dosing strategies: dose intensity and dose density. Dose intensity is the total amount of drug administered at one time or over a week, every 28 days for instance. There can be a positive relationship between dose intensity and response rate. However, there is also a correlation with increased toxicity with dose intense regimens. Dose density, on the other hand - you give the drug, give smaller doses of the drug more often, for instance, once a week or every two weeks.
现在我们已经了解有效给药可以成为化疗治愈效果的限制因素。一般有两种给药策略:剂量强度和剂量密度。剂量强度是特定时间内给予的药物总量,例如一次、一周之内或者每 28 天给予的量。剂量强度和疗效率可以有正相关关系。但是,剂量增加也会引起毒性增强。剂量密度则是指以更高的频率给予更少量的药物,例如每周一次或每两周一次。
Treatment Modalities: Treatment Modalities: Treatment Modalities: Treatment Modalities:
Drug Therapy Part IIDrug Therapy Part IIDrug Therapy Part IIDrug Therapy Part II
Common Drug Therapy ToxicitiesCommon Drug Therapy ToxicitiesCommon Drug Therapy ToxicitiesCommon Drug Therapy Toxicities
• Gastrointestinal toxicity
• Cardiotoxicity
• Neurotoxicity
• Hepatotoxicity
• Nephrotoxicity
• Dermatologic toxicity
• Myelotoxicity
The ideal chemotherapeutic medication will kill tumor cells and spare normal cells. Unfortunately, this is not the case when it comes to most --- most chemotherapy. Toxicities from chemotherapy can potentially affect any organ in the body and result in affecting both the patient’s quality of life and treatment outcomes. I will spend some time going over some of the toxicities of chemotherapy.
最理想的化疗药物需要杀灭肿瘤细胞,同时保留正常细胞。但是很遗憾,大多数化疗都并非如此。化疗产生的毒性可能影响机体的所有器官,从而累及患者的生活质量和治疗转归。我会花些时间讨论化疗的部分毒性。

11
Treatment Modalities: Treatment Modalities: Treatment Modalities: Treatment Modalities:
Drug Therapy Part IIDrug Therapy Part IIDrug Therapy Part IIDrug Therapy Part II
Drug Therapy ToxicityDrug Therapy ToxicityDrug Therapy ToxicityDrug Therapy Toxicity
• Factors that may influence treatment toxicity
– Dose of chemotherapy
• High dose vs. low dose
– Treatment schedule
• Weekly vs. biweekly vs. monthly
– Combination therapy
• Anthracycline with antimetabolite
– Patient specific factors
• Age, BSA, organ function, comorbidities,
response to prior therapies
– Method of administration
• Continuous vs. bolus
– Drug-drug and drug-herbal interactions
But, before we do this, there are many factors that influence treatment toxicity, for instance the dose of chemotherapy, the treatment schedule, whether the chemotherapy is given in combination or as a single agent, and patient-specific factors, such as age. Elderly patients have less --- are less tolerable of chemotherapy, oftentimes because they might have poor organ function or other comorbidities. Additionally, the method of administration, whether it is given continuous versus bolus, can affect the toxicity of the drug. And you have to consider other drugs and herbal products when giving chemotherapy as well.
但在此之前,有许多因素会影响治疗毒性,例如化疗的剂量、治疗时间表、化疗是作为合并治疗还是单药剂给予、以及患者特定因素,例如年龄。老年患者对化疗的耐受性较差,通常的原因是他们的器官功能可能不佳或者有其他并发病。此外,给药方法,是连续给药还是快速推注,也可影响药物的毒性。而且在给予化疗时还必须考虑其他药物和草药。
Treatment Modalities: Treatment Modalities: Treatment Modalities: Treatment Modalities:
Drug Therapy Part IIDrug Therapy Part IIDrug Therapy Part IIDrug Therapy Part II
Gastrointestinal ToxicityGastrointestinal ToxicityGastrointestinal ToxicityGastrointestinal Toxicity
• Nausea and vomiting
– Most common early manifestation of toxicity
– Mechanisms
• Stimulation of chemoreceptor zones
• Damage to gastrointestinal mucosa
• Alterations in taste and smell
• Five distinct clinical syndromes
– Acute: < 24 hours after chemotherapy
– Delayed: ≥ 24 hours after chemotherapy
– Breakthrough: Symptoms despite prophylaxis
– Refractory: Ineffective treatment
– Anticipatory: Symptoms prior to therapy
Nausea and vomiting are common side effects of chemotherapy and are feared by most patients. In the setting of chemotherapy, nausea and vomiting is medically known as chemotherapy-induced nausea and vomiting. It is often the first side effect of patients that --- it is often the first side effect patients experience. Nausea and vomiting can be characterized as acute, occurring within the first 24 hours of starting chemotherapy, or delayed nausea and vomiting occurs within 24 hours after chemotherapy. Breakthrough nausea and vomiting is that which occurs despite being on medication to preventive it. Refractory nausea and vomiting is that that does not respond at all to treatment. Finally, anticipatory nausea and vomiting is when a patient experiences symptoms prior to starting their next cycle of chemotherapy.
恶心和呕吐是化疗的常见副作用,令大多数患者畏惧。化疗时产生的恶心和呕吐在医学上被称为化疗引发的恶心和呕吐。这常常是患者最先出现的副作用。恶心和呕吐可以是急性,在开始化疗后 24 小时内出现;也可以是延迟性恶心和呕吐,化疗后 24 小时之后出现。突破性恶心和呕吐是接受预防药物之后仍然发生的恶心和呕吐。顽固性恶心和呕吐是对治疗没有任何反应的恶心和呕吐。最后,预期性恶心和呕吐是患者在开始下次化疗周期之前出现的症状。

12
Treatment Modalities: Treatment Modalities: Treatment Modalities: Treatment Modalities:
Drug Therapy Part IIDrug Therapy Part IIDrug Therapy Part IIDrug Therapy Part IIEmetogenic Potential of Commonly Emetogenic Potential of Commonly Emetogenic Potential of Commonly Emetogenic Potential of Commonly used Agents used Agents used Agents used Agents
NCCN v.1.2010 Antiemesis Practice Guidelineshttp://www.nccn.org/professionals/physician_gls/PDF/antiemesis.pdf
Interestingly, not all chemotherapeutic agents cause the same degree of nausea or vomiting. There are several classification systems that define emetogenicity of chemotherapy. And this helps us choose what kind of antiemesis regimen we will use. Although this table is not all inclusive, it shows examples of chemotherapeutic agents that are thought to be of high emetogenic risk and associated with minimal emetogenic risk. As you may have noticed, the emetogenic potential - some chemotherapy is dose --- dose-dependent.
值得关注的是,并不是所有化疗药剂都造成相同程度的恶心或呕吐。有数种分类系统来定义化疗的致呕性。这可以帮助我们选择使用的止吐疗法类型。尽管这份表格并不完整,但是它显示了被认为具有高致呕性以及致呕性轻微的化疗药剂实例。大家可能已经注意到,某些化疗的致呕作用具有剂量依赖性。
Treatment Modalities: Treatment Modalities: Treatment Modalities: Treatment Modalities:
Drug Therapy Part IIDrug Therapy Part IIDrug Therapy Part IIDrug Therapy Part II
Gastrointestinal ToxicityGastrointestinal ToxicityGastrointestinal ToxicityGastrointestinal Toxicity
• Mucositis
– Inflammatory reaction and ulcerative lesions
of mucosal surfaces
– Most commonly caused by methotrexate,
5-fluorouracil, vinca alkaloids
• Diarrhea
– Common adverse effect of irinotecan
• Constipation
– Common adverse effect of vincristine
And, if nausea and vomiting is not enough, certain agents also destroy the mucosal lining throughout the gastrointestinal tract. Tissue lining this gastrointestinal tract is usually rapidly dividing cells. Hence, these cells are susceptible to the actions of chemotherapy. Agents, such as methotrexate and 5-fluorouracil, can cause mucositis and inflammatory reactions of the mucosal lining. Irinotecan, used for the treatment of colon cancer, almost always causes diarrhea, whereas vincristine does the opposite, causes constipation.
除恶心和呕吐之外,某些药物还会破坏整个消化道的粘膜层。消化道的组织层通常是快速分裂细胞。因此,这些细胞容易受到化疗作用的影响。诸如甲氨蝶呤和 5-氟尿嘧啶等药剂可造成黏膜层出现黏膜炎和炎性反应。用于治疗结肠癌的伊立替康几乎总是会产生腹泻,而长春新碱的作用相反,会造成便秘。

13
Treatment Modalities: Treatment Modalities: Treatment Modalities: Treatment Modalities:
Drug Therapy Part IIDrug Therapy Part IIDrug Therapy Part IIDrug Therapy Part II
CardiotoxicityCardiotoxicityCardiotoxicityCardiotoxicity
• Rare but serious complication of cancer therapy
• Incidence and severity depends on agent, dose,
schedule, patient factors, and other treatments
• Cardiomyopathy
– Anthracyclines, interferon
• Ischemia
– Fluorouracil, sorafenib
• Arryhthmias
– Anthracyclines, arsenic, taxanes
• Hypertension
– Bevacizumab, sorafenib
A rare, but serious, complication with some chemotherapy agents is cardiotoxicity. Cardiotox --- Cardiotoxicity can manifest as cardiomyopathy, congestive heart failure, ischemia, arrhythmias, or hypertension. Anthracyclines are well recognized as the agents that cause cardiomyopathies and congestive heart failure when certain cumulative doses of the anthracycline have been reached.
某些化疗药剂的罕见但严重的并发症是心脏毒性。心脏毒性的表现可以是心肌病、充血性心脏衰竭、缺血、心律不齐或高血压。已经很清楚,当蒽环类药物的累积剂量达到特定水平时,会造成心肌病和充血性心脏衰竭。
Treatment Modalities: Treatment Modalities: Treatment Modalities: Treatment Modalities:
Drug Therapy Part IIDrug Therapy Part IIDrug Therapy Part IIDrug Therapy Part II
NeurotoxicityNeurotoxicityNeurotoxicityNeurotoxicity
• Cerebellar toxicity
– Ataxia, nystagmus, gait and coordination abnormalities
– High dose cytarabine (> 1 gm/m2)
• Encephalopathy
– Confusion, aphasia, headache
– Methotrexate, ifosfamide
• Arachnoiditis
– Headache, nausea/vomiting, fever, photophobia
– Intrathecal methotrexate and cytarabine
• Seizures
– Nelarabine
Neurotoxic effects of chemotherapy occur fairly frequently and are often reasons to limit the dose or delay therapy. Some agents cause both central and peripheral neurotoxicity. For example, high-dose cytarabine, ifosfamide, and nelarabine are commonly known for their central neurotoxic side effects.
化疗的神经毒性作用发生颇为频繁,而且常常是限制化疗剂量或延迟化疗的原因。某些药剂造成中枢神经和外周神经毒性。例如,高剂量氟达拉滨、异磷酰胺和奈拉滨通常被认为会引起中枢神经副作用。

14
Treatment Modalities: Treatment Modalities: Treatment Modalities: Treatment Modalities:
Drug Therapy Part IIDrug Therapy Part IIDrug Therapy Part IIDrug Therapy Part II
Neurotoxicity (continued)Neurotoxicity (continued)Neurotoxicity (continued)Neurotoxicity (continued)
• Peripheral neuropathy
– Manifest as stocking-glove like distribution,
pain, tingling
– Vinca Alkaloids
• Vincristine
– Platinum Analogs
• Cisplatin and oxaliplatin
– Taxanes
• Paclitaxel > Docetaxel
Chemotherapy can also induce peripheral neuropathy that is related to the cumulative dose and the type of drug used. The vinca alkaloids, the platinum analogs, and the taxanes are notorious for inducing peripheral neuropathy. The early signs and symptoms are pain or tingling in the hands and feet and sometimes loss of reflexes. And this is usually a reason for delaying or reducing the dose of the next cycle.
化疗还可引发与使用药物种类和累积剂量有关的外周神经病变。长春碱类药物、铂类似药物和紫杉类药物都有引发外周神经病变的恶名。早期体征和症状是手足疼痛或刺痛,有时反射会消失。而这通常是延迟或降低下个周期剂量的原因之一。
Treatment Modalities: Treatment Modalities: Treatment Modalities: Treatment Modalities:
Drug Therapy Part IIDrug Therapy Part IIDrug Therapy Part IIDrug Therapy Part II
Neurotoxicity (continued)Neurotoxicity (continued)Neurotoxicity (continued)Neurotoxicity (continued)
• Constipation, Bowel obstructions
– Vinca alkaloids, cisplatin
• Ocular Toxicity
– Chemical conjuctivitis
– High dose cytarabine
• Ototoxicity
– Loss of high frequency ranges,
acute tinnitus, chronic hearing loss
– Cisplatin
And some --- additional neurotoxic effects can involve the bowel system, the eyes, and the ears.
其他神经毒性作用可涉及肠道系统、眼和耳。

15
Treatment Modalities: Treatment Modalities: Treatment Modalities: Treatment Modalities:
Drug Therapy Part IIDrug Therapy Part IIDrug Therapy Part IIDrug Therapy Part II
HepatotoxicityHepatotoxicityHepatotoxicityHepatotoxicity
• Hepatotoxicity manifests in a variety of patterns
– Hepatocellular necrosis - acute toxicity
– Cholestasis - impaired flow of bile from liver to duodenum
– Steatosis - fatty liver
– Veno-occlusive disease (VOD) - injury to hepatic venous
endothelium
• Hepatocellular injury is generally reversible and nonfatal
• Many drugs require dose reduction or avoidance in the
setting of hepatic insufficiency
• Hepatotoxic agents include: vinca alkaloids, cytarabine,
methotrexate, clofarabine, gemtuzumab, imatinib,
L-asparaginase
Chemotherapy can also cause hepatotoxicity that can manifest as elevated liver function tests, cholestasis, and veno-occlusive disease, which is injury to the hepatic venous endothelium. Many of these drugs are cleared through the liver, hence, will require dose adjustment in the setting of hepatocellular injury or reduced liver function. I’ve provided a list of drugs that are typically hepatotoxic or hepatically-cleared agents. Some of them include vinca alkaloids, cytarabine, methotrexate, clofarabine, imatinib, and L-asparaginase.
化疗也可造成肝毒性。肝毒性可表现为肝功检查结果升高、胆汁滞留,以及疾病阻塞性疾病,即损伤肝静脉内皮细胞。这些药物很多都通过肝脏清除。因此,如果出现肝细胞损伤或肝功下降,则需要调整剂量。我在这里列出了通常具有肝毒性或在肝脏清除的一组药物。这些药物包括长春碱类药物、氟达拉滨、甲氨蝶呤、克罗拉滨、伊马替尼和 L-门冬酰胺酶。
Treatment Modalities: Treatment Modalities: Treatment Modalities: Treatment Modalities:
Drug Therapy Part IIDrug Therapy Part IIDrug Therapy Part IIDrug Therapy Part II
NephrotoxicityNephrotoxicityNephrotoxicityNephrotoxicity
• Chemotherapy can impair kidney function
• Impairment can range from asymptomatic elevations
of serum creatinine to renal failure requiring dialysis
– Methotrexate and cisplatin are well-known nephrotoxins
• Impaired renal function can increase systemic
toxicities
• Many drugs require dose reduction or avoidance in
the setting of renal insufficiency
– Cytarabine, methotrexate, cisplatin, carboplatin, etoposide
And you cannot forget about nephrotoxicity. Many of the chemotherapy agents are renally cleared through the kidneys. Two common agents are methotrexate and cisplatin. They are both renally eliminated and cause --- can cause renal insufficiency or renal failure. Impaired renal function can increase systemic toxicities. Hence many drugs require dose reduction or avoidance in the setting of renal insufficiency.
而且也不能忽略肾毒性。许多化疗药剂是通过肾脏清除。两种常见的药剂是甲氨蝶呤和顺铂。这两种药物都通过肾脏清除,均可造成肾功能不全或肾脏衰竭。肾功能受损可加重全身毒性。因此,许多药物都需要降低剂量或者避免用于肾功能不全的患者。

16
Treatment Modalities: Treatment Modalities: Treatment Modalities: Treatment Modalities:
Drug Therapy Part IIDrug Therapy Part IIDrug Therapy Part IIDrug Therapy Part II
Dermatologic ToxicityDermatologic ToxicityDermatologic ToxicityDermatologic Toxicity
It is not surprising that some of these medications cause problems with the skin. The good news is that many of these agents --- many of these problems are reversible. Hair loss is a common side effect of some of these agents. Extravasation occurs when the drug leaks through the tubing into the skin and causes skin necrosis. Occasionally, this may require surgical intervention. Interesting --- interestingly, some targeted therapies cause acne-like rash on the face, trunk, and extremities.
部分此类药物会造成皮肤问题,这一点是意料之中的。幸好大部分这类问题都可逆转。脱发是部分此类药物的常见副作用。药物外渗是指药物从给药管道漏出,进入皮肤,造成皮肤坏死。药物外渗有时需要采取外科干预措施。引人关注的是,部分靶向疗法会造成面部、躯干和四肢的粉刺样皮疹。
Treatment Modalities: Treatment Modalities: Treatment Modalities: Treatment Modalities:
Drug Therapy Part IIDrug Therapy Part IIDrug Therapy Part IIDrug Therapy Part II
MyelotoxicityMyelotoxicityMyelotoxicityMyelotoxicity
• Neutropenia
– Decrease in the number of circulating neutrophils
– Single most important predisposing factor to infection
• Anemia
– Decrease in hemoglobin or circulating erythrocytes
• Thrombocytopenia
– Decrease in the number of circulating platelets
Adverse effects on the bone marrow production called myelosuppression is a serious toxicity that can manifest as neutropenia, anemia, or thrombocytopenia. Myelosuppression is often dictated by the dose, schedule, and type of agent being used. Patient characteristics as well, the age, renal function, liver function, etc., can affect the dosing and the toxicity of these drugs. Neutropenia is a very serious side effect due to the risk of infection. Febrile neutropenia often requires hospitalization and IV antibiotics. Anemia is --- often causes fatigue and thrombocytopenia, increases your risk for bleeding. These complications can be thwarted by transfusions.
对骨髓生成细胞功能的不良作用被称为骨髓抑制。这是一种严重毒性反应,可以表现为嗜中性细胞减少、贫血或血小板减少。骨髓抑制常常受到剂量、用药时间表和用药种类的影响。而且患者的特点,例如年龄、肾功能、肝功能等,也会影响这些药物的给药和毒性。嗜中性细胞减少可能会引起感染,因此是非常严重的副作用。嗜中性细胞减少性发热常常需要住院治疗并静脉给予抗生素。贫血常常造成疲劳和血小板减少,增加出血的风险。这些并发症可以通过输血来缓解。

17
Treatment Modalities: Treatment Modalities: Treatment Modalities: Treatment Modalities:
Drug Therapy Part IIDrug Therapy Part IIDrug Therapy Part IIDrug Therapy Part II
Dosing and Toxicity SummaryDosing and Toxicity SummaryDosing and Toxicity SummaryDosing and Toxicity Summary
• Drug therapy can affect any organ system in
the body
• Factors that influence treatment toxicity may
include drug dose, organ function, age and method
of administration
• Monitoring and management of drug-induced toxicity
plays an important role in caring for cancer patients
So, in summary of dosing and toxicity, drugs can affect any organ system in the body. And factors that often influence treatment toxicity can include the drug, the drug dose, organ function, age, and method of administration. And monitoring and management of drug-induced toxicity requires a multidisciplinary approach.
对给药和毒性作一下总结。药物可影响机体的所有器官系统。常常影响治疗毒性的因素可包括药物种类、药物剂量、器官功能、年龄和给药方法。监控和管理药物引发毒性需要采取多学科手段。
Treatment Modalities: Treatment Modalities: Treatment Modalities: Treatment Modalities:
Drug Therapy Part IIDrug Therapy Part IIDrug Therapy Part IIDrug Therapy Part II
ConclusionsConclusionsConclusionsConclusions
• Drug therapy may be used for various goals in
cancer treatment depending on a patient’s disease
and prognosis
• Chemotherapy drugs are classified by mechanisms
of action and differ in cytotoxic mechanisms of action
• Newer immune-based and targeted therapies are
emerging and serve an important role in cancer
care
• Drug therapy may result in a wide variety
of side effects
In summary, the purpose of chemotherapy may vary depending on patient-specific factors, such as age, comorbidity, tumor stage, and type of malignancies. The mainstay of oncology therapy still involves cytotoxic agents that indiscriminately kill rapidly dividing cells. Novel therapies, such as immunotherapy and targeted therapy, targets tumor-specific molecules and processes while hopefully preserving normal tissue. Often targeted therapy is combined with conventional chemotherapy.
总而言之,化疗的目的可随患者的具体因素而改变,例如患者的年龄、并存病、肿瘤分期和恶性疾病的类型。肿瘤治疗的主流仍然是使用细胞毒性药剂不加区分地杀灭快速分裂细胞。诸如免疫疗法和靶向疗法的新型疗法以肿瘤特异性分子和过程为靶的,试图保留正常组织。靶向疗法通常与传统化疗合并使用。

18
Treatment Modalities: Treatment Modalities: Treatment Modalities: Treatment Modalities:
Drug Therapy Part IIDrug Therapy Part IIDrug Therapy Part IIDrug Therapy Part II
Cancer ResourcesCancer ResourcesCancer ResourcesCancer Resources
And lastly, I would like to leave you with this slide with a list of resources for additional cancer and chemotherapy information. I hope you have enjoyed this lecture and we welcome your feedback. Thank you.
最后,我想向大家提供一个可以获取癌症和化疗更多信息的资源列表。希望大家喜欢本次讲座,敬请提出反馈意见。谢谢。
Related Documents