CLINICIAN’S CORNER SPECIAL COMMUNICATION Treatment for Adult HIV Infection 2004 Recommendations of the International AIDS Society-USA Panel Patrick G. Yeni, MD Scott M. Hammer, MD Martin S. Hirsch, MD Michael S. Saag, MD Mauro Schechter, MD, PhD Charles C. J. Carpenter, MD Margaret A. Fischl, MD Jose M. Gatell, MD, PhD Brian G. Gazzard, MA, MD Donna M. Jacobsen, BS David A. Katzenstein, MD Julio S. G. Montaner, MD Douglas D. Richman, MD Robert T. Schooley, MD Melanie A. Thompson, MD Stefano Vella, MD Paul A. Volberding, MD T HE INTERNATIONAL AIDS SOCI- ety-USA panel last updated its guidelines for antiretroviral therapy in 2002. 1 Over the past 2 years, substantial new information has emerged influencing antiretroviral management. This includes the avail- ability of several new drugs that in- crease therapeutic options (ie, atazana- vir, emtricitabine, enfuvirtide, and fosamprenavir); the reporting of ma- jor randomized, multicenter trials that help define optimal initial regimens; an evolving understanding of the mechanisms and clinical significance of drug resistance, toxic effects, and interactions; and clinical trial results that address questions concerning strategic approaches to antiretroviral therapy (eg, structured treatment interruption). These updated guidelines reflect the international perspectives of the pan- elists and are designed to serve as a tool for clinicians in countries where re- sources are sufficient to provide rela- Author Affiliations and Financial Disclosures are listed at the end of the article. Corresponding Author: Patrick G. Yeni, MD, Ho ˆ pi- tal Bichat-Claude Bernard, 46 Rue Henri-Huchard, 75877 Paris Cedex 18, France (Patrick.Yeni@Bch .Ap-Hop-Paris.Fr). Context Substantial changes in the field of human immunodeficiency virus (HIV) treat- ment have occurred in the last 2 years, prompting revision of the guidelines for anti- retroviral management of adults with established HIV infection. Objective To update recommendations for physicians who provide HIV care regard- ing when to start antiretroviral therapy, what drugs to start with, when to change drug regimens, and what drug regimens to switch to after therapy fails. Data Sources Evidence was identified and reviewed by a 16-member noncompen- sated panel of physicians with expertise in HIV-related basic science and clinical re- search, antiretroviral therapy, and HIV patient care. The panel was designed to have broad US and international representation for areas with adequate access to antiret- roviral management. Study Selection Evidence considered included published basic science, clinical re- search, and epidemiological data (identified by experts in the field or extracted through MEDLINE searches using terms relevant to antiretroviral therapy) and abstracts from HIV-oriented scientific conferences between July 2002 and May 2004. Data Extraction Data were reviewed to identify any information that might change previous guidelines. Based on panel discussion, guidelines were drafted by a writing committee and discussed by the panel until consensus was reached. Data Synthesis Four antiretroviral drugs recently have been made available and have broadened the options for initial and subsequent regimens. New data allow more de- finitive recommendations for specific drugs or regimens to include or avoid, particu- larly with regard to initial therapy. Recommendations are rated according to 7 evi- dence categories, ranging from I (data from prospective randomized clinical trials) to VII (expert opinion of the panel). Conclusion Further insights into the roles of drug toxic effects, drug resistance, and pharmacological interactions have resulted in additional guidance for strategic ap- proaches to antiretroviral management. JAMA. 2004;292:251-265 www.jama.com For editorial comment see p 266. CME available online at www.jama.com ©2004 American Medical Association. All rights reserved. (Reprinted) JAMA, July 14, 2004—Vol 292, No. 2 251

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

CLINICIAN’S CORNERSPECIAL COMMUNICATION
Treatment for Adult HIV Infection2004 Recommendations of theInternational AIDS Society-USA PanelPatrick G. Yeni, MDScott M. Hammer, MDMartin S. Hirsch, MDMichael S. Saag, MDMauro Schechter, MD, PhDCharles C. J. Carpenter, MDMargaret A. Fischl, MDJose M. Gatell, MD, PhDBrian G. Gazzard, MA, MDDonna M. Jacobsen, BSDavid A. Katzenstein, MDJulio S. G. Montaner, MDDouglas D. Richman, MDRobert T. Schooley, MDMelanie A. Thompson, MDStefano Vella, MDPaul A. Volberding, MD
THE INTERNATIONAL AIDS SOCI-ety-USA panel last updated itsguidelines for antiretroviraltherapy in 2002.1 Over the past
2 years, substantial new information hasemerged influencing antiretroviralmanagement. This includes the avail-ability of several new drugs that in-crease therapeutic options (ie, atazana-vir, emtricitabine, enfuvirtide, andfosamprenavir); the reporting of ma-
jor randomized, multicenter trials thathelp define optimal initial regimens;an evolving understanding of themechanisms and clinical significanceof drug resistance, toxic effects, andinteractions; and clinical trial resultsthat address questions concerningstrategic approaches to antiretroviraltherapy (eg, structured treatmentinterruption).
These updated guidelines reflect theinternational perspectives of the pan-elists and are designed to serve as a toolfor clinicians in countries where re-sources are sufficient to provide rela-
Author Affiliations and Financial Disclosures are listedat the end of the article.Corresponding Author: Patrick G. Yeni, MD, Hopi-tal Bichat-Claude Bernard, 46 Rue Henri-Huchard,75877 Paris Cedex 18, France ([email protected]).
Context Substantial changes in the field of human immunodeficiency virus (HIV) treat-ment have occurred in the last 2 years, prompting revision of the guidelines for anti-retroviral management of adults with established HIV infection.
Objective To update recommendations for physicians who provide HIV care regard-ing when to start antiretroviral therapy, what drugs to start with, when to change drugregimens, and what drug regimens to switch to after therapy fails.
Data Sources Evidence was identified and reviewed by a 16-member noncompen-sated panel of physicians with expertise in HIV-related basic science and clinical re-search, antiretroviral therapy, and HIV patient care. The panel was designed to havebroad US and international representation for areas with adequate access to antiret-roviral management.
Study Selection Evidence considered included published basic science, clinical re-search, and epidemiological data (identified by experts in the field or extracted throughMEDLINE searches using terms relevant to antiretroviral therapy) and abstracts fromHIV-oriented scientific conferences between July 2002 and May 2004.
Data Extraction Data were reviewed to identify any information that might changeprevious guidelines. Based on panel discussion, guidelines were drafted by a writingcommittee and discussed by the panel until consensus was reached.
Data Synthesis Four antiretroviral drugs recently have been made available and havebroadened the options for initial and subsequent regimens. New data allow more de-finitive recommendations for specific drugs or regimens to include or avoid, particu-larly with regard to initial therapy. Recommendations are rated according to 7 evi-dence categories, ranging from I (data from prospective randomized clinical trials) toVII (expert opinion of the panel).
Conclusion Further insights into the roles of drug toxic effects, drug resistance, andpharmacological interactions have resulted in additional guidance for strategic ap-proaches to antiretroviral management.JAMA. 2004;292:251-265 www.jama.com
For editorial comment see p 266.
CME available online atwww.jama.com
©2004 American Medical Association. All rights reserved. (Reprinted) JAMA, July 14, 2004—Vol 292, No. 2 251

tively unrestricted choices of drugs anddiagnostic monitoring tools; the WorldHealth Organization has recently is-sued new guidelines for resource-limited settings.2 As with previous edi-tions, our updated guidelines center on4 major questions: when to start anti-retroviral therapy, what to start, whento change, and what to change to.
METHODSThe International AIDS Society-USA an-tiretroviral panel was convened in 1995to develop treatment guidelines foradults infected with human immuno-deficiency virus (HIV) in the devel-oped world.3 Panel members were se-lected by the International AIDSSociety-USA and include physicianswith expertise in basic science, clini-cal research, and HIV patient care andwere not compensated.
The panel continually monitorsmedical and scientific advances and up-dates its recommendations when newdata warrant a new report (approxi-mately every 2 years). It reconvened inlate 2003 to review new data that mightchange the 2002 recommendations.1
Panel members identified and criti-cally reviewed new data. A 5-memberwriting committee (P.G.Y., S.M.H.,M.S.H., M.S.S., and M.S.) was ap-pointed, which drafted the manu-script and made revisions based on sub-sequent panel meetings.
Published data and abstracts from se-lected scientific conferences (Confer-ences on Retroviruses and Opportu-nistic Infections; International AIDSSociety Conference on HIV Pathogen-
esis and Treatment; Interscience Con-ferences on Antimicrobial Agents andChemotherapy; Infectious Diseases So-ciety of America Conferences, and oth-ers) were considered. Reports from be-tween July 2002 and May 2004 werereviewed and data were extractedthrough MEDLINE searches usingterms relevant to antiretroviral therapy).Recommendations are made for anti-retroviral drugs approved in the UnitedStates as of mid 2004 for establishedHIV infection among adults.
Evidence strengths were rated accord-ing to type. We developed a rating scalefor the evidence that was adapted fromthe US Preventive Services Task Forceratings and modified to be relevant fortreatment of HIV (BOX).
Costs of specific medications andlaboratory monitoring have not beenconsidered in these recommenda-tions. However, costs are importantelements in therapeutic decision mak-ing. Recommendations herein weremade by full panel consensus. In eachsection, relevant data appearing sincethe last edition of the guidelines1 arepresented, followed by the panel’s rec-ommendations with the evidencestrength ratings indicated.
WHEN TO STARTANTIRETROVIRAL THERAPYRecent Data AddressingThis Question
Randomized clinical trials have demon-strated a survival benefit with the use ofantiretroviral therapy by patients withsevere immunodeficiency.1 For less se-verely compromised individuals (ie,
asymptomatic individuals with CD4 cellcounts �200/µL), there are no defini-tive data from prospective, random-ized controlled studies to determinewhen antiretroviral therapy is associ-ated with a survival benefit. In the ab-sence of such data, the decision to ini-tiate therapy should be made based onsurvival and disease progression infor-mation obtained from observationalstudies, the consequences of moderatedegrees of immune deficiency, and thelong-term safety of antiretroviral drugs.
Over the last 2 years, published re-sults of antiretroviral-treated cohortslargely support previous recommenda-tions. The largest study, which ana-lyzed data from 12574 patients, con-cluded that a prognosis could be bestpredicted by CD4 cell count and HIVRNA response after 6 months of treat-ment, independent of pretreatment val-ues.4,5 The HIV Outpatient Study ana-lyzed data from 1464 patients from 10clinics in the United States; after a me-dian of 4 years of follow-up, patientswith baseline CD4 cell counts be-tween 200/µL and 350/µL who startedantiretroviral therapy had lower mor-tality rates than those who waited un-til their CD4 cell count was below 200/µL.6 Another study reported outcomesof 1173 patients initiating therapy af-ter July 1, 1996, and receiving therapyfor at least 90 days.7 Those who initi-ated therapy with a CD4 cell count be-low 200/µL had a higher risk of dis-ease progression even if a durablevirological suppression was achieved.In a cohort of 1422 treatment-naive pa-tients in Canada (median follow-up, 40months), CD4 cell count was the bestpredictor of survival, but a baseline HIVRNA level higher than 100000 cop-ies/mL was independently associatedwith death.8 This group also studied acohort with pretreatment CD4 cellcounts between 200/µL and 350/µL.9
After a median follow-up of more than3 years, medication adherence (as es-timated by prescription refills) was thecritical determinant of survival. In astudy performed in 1132 women in-fected with HIV (median follow up, 3.9years), posttherapy CD4 cell counts
Box. Strength of Evidence Rating ScaleI. Prospective clinical trials (ie, properly randomized controlled trials) or data
from ancillary trials (pharmacological and drug interaction studies)A. PublishedB. Abstracts presented at scientific conferences
II. Cohort studiesIII. Observational studies (including meta-analyses)IV. Inferences from studies with similar drugs (or in similar settings)V. Extrapolations from pathogenesis studies
VI. Uncontrolled studies (eg, pilot studies, exploratory studies, etc)VII. Expert opinion (consensus of the panel in the absence of above evidence)
RECOMMENDATIONS FOR ADULT HIV
252 JAMA, July 14, 2004—Vol 292, No. 2 (Reprinted) ©2004 American Medical Association. All rights reserved.

(�200/µL vs �350/µL) and HIV RNAlevel (�10000 copies/mL vs �80 cop-ies/mL) predicted death and new AIDS-defining illness. Pretherapy values werenot predictive of clinical outcomes if ad-justed for values attained after therapyinitiation.10
Several potentially life-threateningconditions that may negatively affectsurvival, including tuberculosis andlymphomas, are common in individu-als with moderately advanced immu-nodeficiency (ie, CD4 cell count be-tween 200/µL and 350/µL).11,12 The useof antiretroviral therapy may decreasethe incidence of tuberculosis, and per-haps some other conditions, andthereby influence survival.
Arguing against earlier introduc-tion of antiretroviral therapy are con-cerns over the long-term safety oftherapy; toxic effects; potential cardio-vascular consequences; and the nega-tive impact of fat maldistribution onquality of life. In contrast, recent datahave demonstrated long-term safety ofsome drugs and regimens over oth-ers.13,14 Some treatment complications(eg, lipoatrophy)15 may be more fre-quent and severe when therapy is ini-tiated at lower CD4 cell counts.
Taken together, data from observa-tional cohorts indicating that antiret-roviral therapy may decrease the inci-dence of potentially life-threateningconditions, long-term safety data onsome regimens, and the availability ofnewer drugs that are safer and easier totake, argue for initiation of therapy be-fore HIV-related disease becomes clini-cally manifest whenever possible. How-ever, the fact that a high proportion ofpatients first present to care with ad-vanced HIV disease and CD4 cell countsbelow 200/µL16 emphasizes the need formore aggressive voluntary counselingand testing initiatives to identify pa-tients at earlier stages of disease.17
RecommendationsTherapy is recommended for all pa-tients with symptomatic HIV disease(evidence strength rating, IA; TABLE 1).1
The treatment of potentially life-threatening opportunistic diseases, or
conditions that require drugs that are dif-ficult to coadminister with antiretrovi-ral drugs (eg, tuberculosis or hepatitisC virus coinfection) or can lead to an im-mune reconstitution syndrome follow-ing the initial CD4 cell count increase,may take precedence over immediate ini-tiation of antiretroviral therapy (evi-dence strength rating, IV). There are suf-ficient data to continue to recommendantiretroviral treatment initiation be-fore CD4 cell counts reach 200/µL (evi-dence strength rating, II).1 Initiation oftherapy in patients with CD4 cell countsbelow 350/µL but above 200/µL needsto be individualized (evidence strengthrating, II). For example, low HIV RNAlevel, stable CD4 cell count (or one thatis declining slowly; eg, a loss of fewerthan 50/µL per year), and patient reluc-tance to start therapy, may be reasonsto defer therapy. Conversely, plasma HIVRNA levels above 100000 copies/mL ora CD4 cell count loss of more than100/µL per year may be reasons to ini-tiate therapy. Initiation of therapy is gen-erally not recommended for patientswith CD4 cell counts between 350/µLand 500/µL, but it may be considered incases with high plasma viral load or arapid decline in CD4 cell count (evi-dence strength rating, II).
CHOICE OF INITIAL REGIMENRecent Data AddressingThis Question
Within the past few years it has be-come clear that not all antiretroviralregimens are equivalent in potency or
toxicity. Initial regimens must still beindividualized,1 and the choice is in-fluenced by several factors including co-morbid conditions, the patient’s readi-ness to start therapy, and concomitantmedications, but it is now possible tosay that certain initial regimens are gen-erally preferable to others based on datafrom controlled clinical trials. Sincepublication of the last article, evalua-tions of regimens that contain non-nucleoside reverse transcriptase inhibi-tors (NNRTIs), protease inhibitors, andtriple-nucleoside (or nucleotide) re-verse transcriptase inhibitors (NR-TIs), and dual-NRTI backbones havebeen reported. Furthermore, severalmore convenient and tolerable formu-lations and fixed-dose combinations ofdrugs have become available. These for-mulations should improve adherenceand ultimately improve therapeutic suc-cess, but there are no data from clini-cal trials demonstrating improved out-come for most of these formulations.
NNRTI-Based Regimensand Dual NRTI BackbonesThe AIDS Clinical Trial Group 384study was a multicenter, randomized,partially double-blind trial in 980 par-ticipants enrolled in the United Statesand Italy (median follow up, 2.3years).13,14 A factorial design was usedto compare regimens and a compositeend point was used that included viralsuppression and toxicity. The combi-nation of zidovudine, lamivudine, andefavirenz was superior to the other
Table 1. Recommendations for Initiating Therapy in Treatment-Naive Individuals*
Disease Stage Recommendation Evidence Rating†
Symptomatic HIV disease Antiretroviral treatment IA
Asymptomatic HIV disease�200 CD4 cells/µL Antiretroviral treatment II
�200 CD4 cells/µL but�350 CD4 cells/µL
Antiretroviral treatment should beconsidered‡
II
�350 CD4 cells/µL but�500 CD4 cells/µL
Continued monitoring; counselingfor HIV transmission prevention§
II
�500 CD4 cells/µL Continued monitoring; counselingfor HIV transmission prevention
II
Abbreviation: HIV, human immunodeficiency virus.*Excludes pregnant women with specific regard to prevention of HIV transmission to the infant.†See Box for explanation of evidence ratings.‡The closer to 200 CD4 cells/µL, the stronger the recommendation for treatment, particularly if the plasma viral load is
high (�50 000-100 000 copies/mL) or if the CD4 cell count is declining rapidly (�100/µL per year).§Consider treatment for patients with high plasma viral load or with rapid decline of CD4 cell count.
RECOMMENDATIONS FOR ADULT HIV
©2004 American Medical Association. All rights reserved. (Reprinted) JAMA, July 14, 2004—Vol 292, No. 2 253

3-drug regimens studied (zidovudine,lamivudine, and nelfinavir; stavudine,didanosine, and nelfinavir; or stavu-dine, didanosine, and efavirenz)13 andwas similar to a 4-drug regimen con-sisting of nelfinavir and efavirenz witheither zidovudine and lamivudine orstavudine and didanosine. There wasno statistically significant differencein the duration of successful treat-ment between a single 4-drug regimenand 2 consecutive 3-drug regimens.14
The 4-drug regimen was associatedwith a longer time to first regimenfailure than the 3-drug regimensexcept for the combination of zidovu-dine, lamivudine, and efavirenz.
The NRTIs used in the 3- or 4-drugcombinations influenced toxicity risk,with higher incidences of peripheralneuropathy, pancreatitis, and hepaticenzyme abnormalities in regimens con-taining stavudine and didanosine.14
From this and earlier studies,18 it is clearthat a combination of zidovudine, la-mivudine, and efavirenz is a particu-larly useful initial regimen. However,the risk of virological resistance to la-mivudine and efavirenz is high if strictadherence to the regimen cannot bemaintained, given the low barrier to re-sistance with these 2 drugs.19,20
In the CNA30024 study, a combina-tion consisting of abacavir, lamivu-dine, and efavirenz was similar (non-inferior) to a combination consisting ofzidovudine, lamivudine, and efavi-renz in 649 patients receiving treat-ment for 48 weeks (HIV RNA level �50copies/mL in 70% and 69% of pa-tients, respectively).21 There was a largerCD4 cell count increase with abacavirthan with zidovudine. However, hy-persensitivity was reported in 9% of pa-tients taking abacavir. Gilead 903 wasa trial comparing stavudine and teno-fovir, each combined with lamivudineand efavirenz in 600 participants.22 Lev-els of HIV RNA suppression (�50 cop-ies/mL) and increases in CD4 cell countwere similar at 96 weeks. However,stavudine-treated participants had agreater risk of elevated fasting triglyc-eride and cholesterol levels and periph-eral neuropathy over 96 weeks.
Interim results from the FTC-301double-blind, placebo-controlled studyshowed that emtricitabine, a recently ap-proved NRTI, provided better viral sup-pression than stavudine when eachwas combined with didanosine andefavirenz in treatment-naive patients(TABLE 2).23 This led to a decision by anindependent data and safety monitor-ing board to discontinue the studyafter 24 weeks. The proportion of pa-tients with persistent HIV RNA suppres-sion below 50 copies/mL through week60 was 76% for the emtricitabine groupand 54% for the stavudine group (log-rank, P�.001). Patients receiving stavu-dine were more likely to experiencetreatment-limiting toxic effects and toprematurely discontinue therapy. Ofnote, there are fewer efficacy and safetydata for emtricitabine (which is similarto lamivudine) or tenofovir than for theother NRTIs.
TheNNRTInevirapinehasbeenevalu-ated in combination with 2 NRTIs. In 2relatively small controlled trials, nevira-pine was compared with a protease in-hibitor (indinavir in ATLANTIC24 andnelfinavir in COMBINE25). In theATLANTIC study, 55% of participantsin the nevirapine group and 44% in theindinavir group had HIV RNA levels be-low 50 copies/mL at 98 weeks.24 In theCOMBINE study, 75% of nevirapine and60% of nelfinavir participants had HIVRNA levels below 200 copies/mL at 12months (P=.06).25
In the 2NN study, nevirapine and efa-virenz were compared when each wascombined with stavudine and lamivu-dine.26 A total of 1216 participants wererandomized to receive 400 mg/d ofnevirapine; 200 mg of nevirapine twicedaily; 600 mg/d of efavirenz; or 400mg/d of nevirapine and 600 mg/d of efa-virenz. At 48 weeks, treatment failed in43.6% of participants in the group re-ceiving nevirapine once daily, 43.7% ofthe twice daily nevirapine group, 37.8%of efavirenz group, and 53.1% of thenevirapine and efavirenz group. A dif-ference between the nevirapine and efa-virenz groups of 10% at 48 weeks wasprespecified to be clinically meaning-ful. This magnitude of difference can-
not be ruled out based on the upperbound of the 95% confidence interval(CI). The mean proportions of pa-tients reaching an HIV RNA level be-low 50 copies/mL at 48 weeks were notdifferent among groups (70.0% for oncedaily nevirapine, 65.4% for twice dailynevirapine, 70.0% for efavirenz, and62.7% for the combination of nevira-pine and efavirenz). Adverse events orHIV progression caused treatment dis-continuation in 21.5% receiving nevira-pine twice daily, 15.8% receiving efa-virenz (P=.04), and 30.1% receivingnevirapine and efavirenz. More partici-pants in the nevirapine groups than inthe efavirenz group had grade 3 or 4clinical hepatotoxicity, but the differ-ences were statistically significant onlyin the twice daily nevirapine group(2.1% for twice daily nevirapine, 1.4%for once daily nevirapine, and 0.3% forefavirenz). Compared with efavirenz(4.5%), more patients taking nevira-pine either twice daily (8.3%) or oncedaily (13.6%) had grade 3 or 4 eleva-tions in liver function tests. Two deathswere attributed to nevirapine, one dueto hepatitis and another to Stevens-Johnson syndrome. Women (includ-ing pregnant women) who are takingnevirapine-containing regimens andwho have CD4 cell counts greater than250/µL are at a 12-fold greater risk ofhepatotoxicity.27 The highest risk forpotentially fatal hepatotoxicity is in thefirst 6 weeks of therapy.27 These re-sults underline the importance of care-ful monitoring of liver enzyme tests inpatients taking nevirapine (TABLE 3).
Protease Inhibitor-Based RegimensIn a double-blind, placebo-controlledtrial enrolling 653 adults, lopinavir/ritonavir and nelfinavir were com-pared when each was used in combi-nation with stavudine and lamivudine.28
The primary end points were HIV RNAlevel of less than 400 copies/mL at week24 and time to loss of virological re-sponse through week 48. All compari-sons favored lopinavir/ritonavir. Atweek 48, 75% of participants in thegroup taking lopinavir/ritonavir hadan HIV RNA level of less than 400
RECOMMENDATIONS FOR ADULT HIV
254 JAMA, July 14, 2004—Vol 292, No. 2 (Reprinted) ©2004 American Medical Association. All rights reserved.
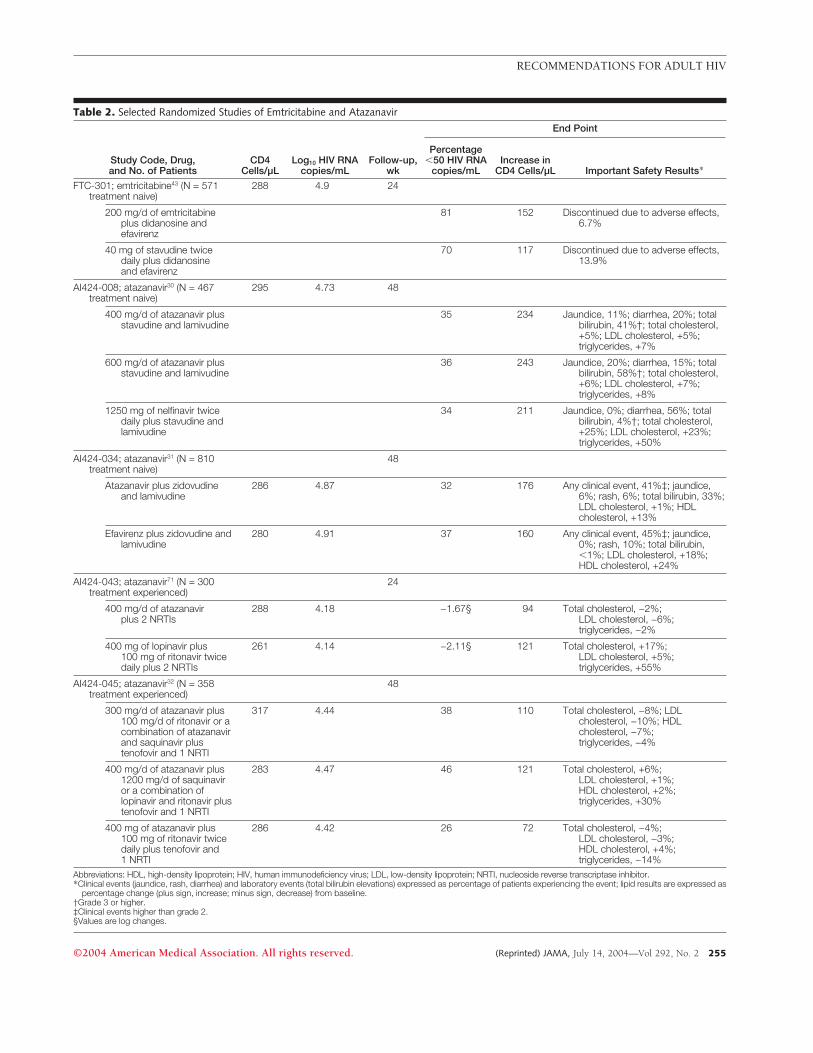
Table 2. Selected Randomized Studies of Emtricitabine and Atazanavir
Study Code, Drug,and No. of Patients
CD4Cells/µL
Log10 HIV RNAcopies/mL
Follow-up,wk
End Point
Percentage�50 HIV RNA
copies/mLIncrease in
CD4 Cells/µL Important Safety Results*
FTC-301; emtricitabine43 (N = 571treatment naive)
288 4.9 24
200 mg/d of emtricitabineplus didanosine andefavirenz
81 152 Discontinued due to adverse effects,6.7%
40 mg of stavudine twicedaily plus didanosineand efavirenz
70 117 Discontinued due to adverse effects,13.9%
AI424-008; atazanavir30 (N = 467treatment naive)
295 4.73 48
400 mg/d of atazanavir plusstavudine and lamivudine
35 234 Jaundice, 11%; diarrhea, 20%; totalbilirubin, 41%†; total cholesterol,+5%; LDL cholesterol, +5%;triglycerides, +7%
600 mg/d of atazanavir plusstavudine and lamivudine
36 243 Jaundice, 20%; diarrhea, 15%; totalbilirubin, 58%†; total cholesterol,+6%; LDL cholesterol, +7%;triglycerides, +8%
1250 mg of nelfinavir twicedaily plus stavudine andlamivudine
34 211 Jaundice, 0%; diarrhea, 56%; totalbilirubin, 4%†; total cholesterol,+25%; LDL cholesterol, +23%;triglycerides, +50%
AI424-034; atazanavir31 (N = 810treatment naive)
48
Atazanavir plus zidovudineand lamivudine
286 4.87 32 176 Any clinical event, 41%‡; jaundice,6%; rash, 6%; total bilirubin, 33%;LDL cholesterol, +1%; HDLcholesterol, +13%
Efavirenz plus zidovudine andlamivudine
280 4.91 37 160 Any clinical event, 45%‡; jaundice,0%; rash, 10%; total bilirubin,�1%; LDL cholesterol, +18%;HDL cholesterol, +24%
AI424-043; atazanavir71 (N = 300treatment experienced)
24
400 mg/d of atazanavirplus 2 NRTIs
288 4.18 −1.67§ 94 Total cholesterol, −2%;LDL cholesterol, −6%;triglycerides, −2%
400 mg of lopinavir plus100 mg of ritonavir twicedaily plus 2 NRTIs
261 4.14 −2.11§ 121 Total cholesterol, +17%;LDL cholesterol, +5%;triglycerides, +55%
AI424-045; atazanavir32 (N = 358treatment experienced)
48
300 mg/d of atazanavir plus100 mg/d of ritonavir or acombination of atazanavirand saquinavir plustenofovir and 1 NRTI
317 4.44 38 110 Total cholesterol, −8%; LDLcholesterol, −10%; HDLcholesterol, −7%;triglycerides, −4%
400 mg/d of atazanavir plus1200 mg/d of saquinaviror a combination oflopinavir and ritonavir plustenofovir and 1 NRTI
283 4.47 46 121 Total cholesterol, +6%;LDL cholesterol, +1%;HDL cholesterol, +2%;triglycerides, +30%
400 mg of atazanavir plus100 mg of ritonavir twicedaily plus tenofovir and1 NRTI
286 4.42 26 72 Total cholesterol, −4%;LDL cholesterol, −3%;HDL cholesterol, +4%;triglycerides, −14%
Abbreviations: HDL, high-density lipoprotein; HIV, human immunodeficiency virus; LDL, low-density lipoprotein; NRTI, nucleoside reverse transcriptase inhibitor.*Clinical events (jaundice, rash, diarrhea) and laboratory events (total bilirubin elevations) expressed as percentage of patients experiencing the event; lipid results are expressed as
percentage change (plus sign, increase; minus sign, decrease) from baseline.†Grade 3 or higher.‡Clinical events higher than grade 2.§Values are log changes.
RECOMMENDATIONS FOR ADULT HIV
©2004 American Medical Association. All rights reserved. (Reprinted) JAMA, July 14, 2004—Vol 292, No. 2 255

Table 3. Selected Randomized Studies of Enfuvirtide and Fosamprenavir
Study Code, Drug,and No. of Patients
CD4Cells/µL
Log10 HIV RNAcopies/mL
Follow-up,wk
End Point
Percentage�50 HIV RNA
copies/mLIncrease in
CD4 Cells/µL Important Safety Results*
TORO1; enfuvirtide61 (N = 501treatment experienced)
24 TORO1 and TORO2 pooleddata: 3.7% discontinuedenfuvirtide for injectionsite reactions;hypersensitivity, 1%;pneumonia, 5.6% inenfuvirtide group and0.6% in optimizedbackground group
Optimized background of 3-5antiretrovirals (history plusresistance testing)†
87 5.2 7.3 32
Optimized background plus90 mg of enfuvirtidesubcutaneously twice daily
75 5.2 19.6 76
TORO2; enfuvirtide60 (N = 512treatment experienced)
24 TORO1 and TORO2 pooleddata: 3.7% discontinuedenfuvirtide for injectionsite reactions;hypersensitivity, 1%;pneumonia, 5.6% inenfuvirtide group and0.6% in optimizedbackground group
Optimized background of 3-5antiretrovirals (history plusresistance testing)‡
101 5.1 5.3 38
Optimized background plus90 mg of enfuvirtidesubcutaneously twice daily
98 5.1 12.2 65
SOLO; fosamprenavir41 (N = 660treatment naive)
48
1400 mg/d of fosamprenavir plus200 mg/d of ritonavir plusabacavir and lamivudine
166§ 4.78 56 396 Diarrhea, 9%
1250 mg of nelfinavir twice dailyplus abacavir and lamivudine
177� 4.83 52 385 Diarrhea, 16%
NEAT; fosamprenavir72 (N = 251treatment naive)¶
48
1400 mg of fosamprenavir twicedaily plus abacavir pluslamivudine
211 4.82 55 201 Diarrhea, 5%
1250 mg of nelfinavir twice dailyplus abacavir plus lamivudine
213 4.85 41 216 Diarrhea, 18%
CONTEXT; fosamprenavir63† (N = 320treatment experienced)
263 4.14 24
700 mg of fosamprenavir plus100 mg of ritonavir twicedaily plus 2 optimized NRTIs
−1.48# 62 Clinical events � grade 2,35%; total cholesterol,0%; triglycerides, +8%
1400 mg of fosamprenavir plus200 mg of ritonavir once dailyplus 2 optimized NRTIs
−1.46# 72 Clinical events � grade 2,19%; total cholesterol,0%; triglycerides, +4%
400 mg of lopinavir plus 100 mgof ritonavir twice daily plus2 optimized NRTIs
−1.63# 63 Clinical events � grade 2,34%; total cholesterol,0%; triglycerides, +4%
Abbreviations: HDL, high-density lipoprotein; HIV, human immunodeficiency virus; LDL, low-density lipoprotein; NRTI, nucleoside reverse transcriptase inhibitor.*Clinical events are expressed as percentage of patients with event. Lipid results are expressed as percentage change (plus sign, increase) from baseline. Total cholesterol and
triglyceride events are of grade 3 or higher.†A total of 336 patients received 2 or fewer active drugs in optimized background (based on genotype).‡A total of 385 patients received 2 or fewer active drugs in optimized background (based on genotype).§Nineteen percent of the patients had a CD4 cell count of less than 50/µL.�Twenty-one percent of the patients had a CD4 cell count of less than 50/µL.¶Eighteen percent of the patients had a CD4 cell count of less than 50/µL.#Values are log changes.
RECOMMENDATIONS FOR ADULT HIV
256 JAMA, July 14, 2004—Vol 292, No. 2 (Reprinted) ©2004 American Medical Association. All rights reserved.

copies/mL compared with 63% in thenelfinavir group; similar differenceswere observed when the cutoff for HIVRNA level was below 50 copies/mL. Av-erage triglyceride increases were greaterin the group receiving lopinavir/ritonavir (125 mg/dL increase) than inthe group receiving nelfinavir (47mg/dL increase) (P�.001). Protease in-hibitor–resistance mutations were dem-onstrated in 33% of participants inwhom nelfinavir was failing and in noneof 37 patients in whom lopinavir/ritonavir was failing.
A twice daily regimen including1000 mg of saquinavir and 100 mg ofritonavir was compared with 800 mgof indinavir and 100 mg of ritonavirtwice daily in 306 participants (onlyone third of whom were treatmentnaive).29 Virological results at 48weeks were comparable (P=.84), butwhen treatment changes were consid-ered failures, the regimen withsaquinavir and ritonavir appeared bet-ter (P=.01) and was associated withfewer lipid level increases.
Atazanavir is a recently approvedonce daily protease inhibitor. Initialcomparative studies have shown some-what contradictory results (Table 2). Inthe AI424-008 study, atazanavir andnelfinavir had similar responses wheneach was combined with 2 NRTIs.30 Inthe AI424-034 study,31 atazanavir wascompared with efavirenz, each in com-bination with zidovudine and lamivu-dine. Virological results at week 48 werecomparable, although the responses inthe efavirenz group were below thoseseen in previous trials (eg, 37% receiv-ing efavirenz achieved a level of HIVRNA �50 copies/mL vs �70% in pre-vious studies). The rates of detectedplasma HIV RNA may have been over-estimated in AI424-034 because of tech-nical problems with sample process-ing. In both studies, lack of lipid levelchanges favored atazanavir.
Evaluations of atazanavir and low-dose ritonavir in initial regimens also areunder way. A preliminary study (AI424-045) in antiretroviral-experienced pa-tients (Table 2) suggests that the com-bination of atazanavir and ritonavir has
similar antiretroviral activity and fewerhyperlipidemic effects than other regi-mens containing ritonavir-boosted pro-tease inhibitors.32
Few studies have compared the regi-mens containing a boosted protease in-hibitor with regimens containing efavi-renz. The FOCUS trial compared aregimen including 1600 mg of saquina-vir and 100 mg of ritonavir with one in-cluding efavirenz in 152 individuals.33
The efavirenz group had better HIV RNAsuppression (71% reached a level of �50copies/mL compared with 51% in the sa-quinavir and ritonavir group) at 48weeks. The CLASS study34 compared thefollowing combinations: amprenavir andritonavir with abacavir and lamivu-dine; efavirenz and abacavir and lam-ivudine; and stavudine with abacavir andlamivudine. Preliminary results at 48weeks showed HIV RNA suppression(�50 copies/mL) superiority in the theefavirenz group (76%) compared withthe amprenavir and ritonavir group(59%) or the stavudine group (62%).
Triple NRTI-Based RegimensAIDS Clinical Trial Group 5095 is an1147-patient, ongoing, placebo-controlled, double-blind study de-signed to compare combinations of zi-dovudine, lamivudine, and abacavir;zidovudine, lamivudine, and efavi-renz; and zidovudine, lamivudine, aba-cavir, and efavirenz. A scheduled dataand safety monitoring board reviewfound differences between the 3-NRTIgroup and each of the other groups thatcrossed prespecified stopping bound-aries; the 3-NRTI group was discontin-ued.35 After a median follow-up of32 weeks, treatment failed in 21% ofthe 3-NRTI group and in 11% of thepooled efavirenz groups (regardless ofpretreatment HIV RNA level of�100000 copies/mL or HIV RNA levelof �100000 copies/mL).
The CLASS and ATLANTIC stud-ies24,34 also suggest that stavudine-based triple-NRTI regimens are less ef-fective than other regimens. InATLANTIC, stavudine and didano-sine were combined with nelfinavir,nevirapine, or lamivudine. Viral load re-
sponse in the 3-NRTI group was infe-rior to the other 2 groups at 96 weeks.24
Several recent trials were termi-nated early because of higher virologi-cal failure rates of 3-NRTI regimens, in-cluding those with tenofovir, abacavir,and lamivudine36,37 and tenofovir, di-danosine, and lamivudine.38 Themechanisms underlying these failuresare unclear, but emergence of the te-nofovir-associated K65R mutation wasobserved in a substantial number of par-ticipants. The combination of stavu-dine, didanosine, and abacavir is alsoan inferior initial regimen.39 It shouldbe noted that the virological failure ratesin these studies are higher than thoseseen previously with the combinationtherapy of zidovudine, lamivudine, andabacavir.40
Once Daily RegimensMany antiretroviral regimens are dosedtwice per day, but several drugs areadministered once per day. Theseinclude efavirenz, tenofovir, didano-sine, lamivudine, emtricitabine, stavu-dine extended release, atazanavir, andthe combination of amprenavir and low-dose ritonavir (or the combination offosamprenavir and low-dose ritonavirin protease inhibitor-naive patients41).Abacavir42 and nevirapine26 can also begiven once daily, but more hepatobili-ary toxicity occurred in the 2NN studywhen nevirapine was taken once dailythan when it was taken twice daily.26
However, few regimens in which alldrugs are given simultaneously havebeen evaluated in randomized studies,and, some once daily drugs cannot betaken simultaneously. In the FTC-301study,43 the once daily combination ofemtricitabine, didanosine, and efavi-renz was superior to the combinationof stavudine and didanosine taken twicedaily plus efavirenz taken once daily in571 treatment-naive patients for 24weeks. In the ZODIAC study,42 aba-cavir once daily was not inferior to aba-cavir twice daily when combined withlamivudine and efavirenz twice daily(plasma HIV RNA �50 copies/mL in66% and 68%, respectively) in 770patients at 48 weeks.
RECOMMENDATIONS FOR ADULT HIV
©2004 American Medical Association. All rights reserved. (Reprinted) JAMA, July 14, 2004—Vol 292, No. 2 257

RecommendationsA regimen containing an NNRTI is of-ten the regimen of choice for initial an-tiretroviral treatment when adherenceis expected to be good because of con-venience, superior virological suppres-sion, lower rates of toxic effects, andfewer interactions between drugs thanwith boosted protease inhibitor regi-mens (evidence strength rating, IA;TABLE 4). Of the NNRTIs available, theweight of available data favors efavi-renz (evidence strength rating, IA).Nevirapine is a reasonable option (evi-dence strength rating, IA); potential toxiceffects make it less satisfactory in somepatients (eg, those coinfected with hepa-titis C virus, those with elevated liver en-zymes, and women with �250 CD4
cells/µL) (evidence strength rating, IB).Efavirenz is contraindicated in womenwho are or wish to become pregnant be-cause of the potential teratogenicity (evi-dence strength rating, IA).44 Treatmentwith nevirapine during pregnancy mustbe monitored carefully for liver en-zyme elevations (evidence strength rat-ing, IB). Delavirdine is not generally rec-ommended for initial regimens becauseof insufficient data.
For initial regimens that include a pro-tease inhibitor, those that are ritonavirboosted are recommended because ofthe improvement in protease inhibitorpharmacokinetics and potency (evi-dence strength rating, IA). More data areavailable for lopinavir/ritonavir (evi-dence strength rating, IA)28 than for
some other recommended boosted pro-tease inhibitor components (eg, atazana-vir and low-dose ritonavir [evidencestrength rating, IV], indinavir and low-dose ritonavir, [evidence strength rat-ing, IB], or saquinavir and ritonavir [evi-dence strength rating, IA]), but it is notclear that lopinavir/ritonavir is the pre-ferred boosted protease inhibitor. Regi-mens containing lopinavir/ritonavir gen-erally produce durable responses amongthose who can tolerate ritonavir; viro-logical failure associated with the emer-gence of resistance is rare. Recommen-dations concerning the relative meritsof lopinavir/ritonavir compared withatazanavir and low dose ritonavir will de-pend on studies of the durability and po-tency of regimens containing atazana-vir and ritonavir. However, atazanaviris less likely to produce plasma lipid ab-normalities. The lower relative poten-cies of nelfinavir (evidence strength rat-ing, IA), unboosted atazanavir (evidencestrength rating, IB), and the combina-tion of fosamprenavir and low-dose rito-navir (evidence strength rating, IB) makethese drugs less attractive options for ini-tial regimens. Full-dose ritonavir as theonly protease inhibitor component is notgenerally recommended because of itstoxicity profile.
The recommended double NRTIbackbones in the initial regimen arezidovudine plus lamivudine or emtric-itabine; tenofovir plus lamivudine oremtricitabine; or emtricitabine plus di-danosine. Of note, emtricitabine plus di-danosine (or alternatively abacavir pluslamivudine) can be used with efavirenzwhen once daily regimens are neces-sary. Alternative dual NRTI regimens arelisted in Table 3. Combining stavudineand zidovudine is contraindicated; com-binations of stavudine and didanosine orcombinations with zalcitabine are notrecommended because of increased toxiceffects (evidence strength rating, IB).
Triple-NRTI regimens are no longerrecommended as initial therapy be-cause of insufficient antiretroviral po-tency compared with a regimen con-taining efavirenz (evidence strengthrating, IA). However, for patients re-quiring treatment with regimens that
Table 4. Recommended and Alternative Components for Initial Antiretroviral Regimens*
Regimen Evidence Rating†
Recommended Components
NNRTI componentEfavirenz IA
(Or nevirapine in selected patients)‡ IA
Protease inhibitor component§Lopinavir/ritonavir IA
Atazanavir with low dose ritonavir IV
Saquinavir with low dose ritonavir IA
Indinavir with low dose ritonavir IB
NRTI component�Zidovudine or tenofovir and lamivudine or emtricitabine
Didanosine and emtricitabine¶
Alternative Components
Protease inhibitor component§Fosamprenavir with low dose ritonavir IB
Atazanavir IB
Nelfinavir IA
NRTI componentAbacavir and lamivudine¶
Didanosine and lamivudine¶
Didanosine and tenofovir#
Stavudine and lamivudine¶
Zidovudine and abacavir
Special Circumstances Only
3-NRTI regimenZidovudine, lamivudine, and abacavir** IA, VII
Abbreviations: NRTI, nucleoside (or nucleotide) reverse transcriptase inhibitor; NNRTI, nonnucleoside reverse tran-scriptase inhibitor.
*Generally include a dual NRTI backbone with either an NNRTI or a ritonavir-boosted protease inhibitor. In specialcircumstances, a triple NRTI regimen (zidovudine, lamivudine and abacavir) may be an alternative regimen.
†See Box for explanation of ratings.‡See “Recommendations.”§Direct head-to-head comparative studies have not been performed to allow clear determination of the best protease
inhibitor.�Fewer long-term data are available for tenofovir and emtricitabine.¶Lamivudine and emtricitabine are considered interchangeable, but confirmatory data are lacking.#May be associated with more pancreatitis73 and more CD4 cell count declines.74 Also see Table 5.**A triple NRTI initial regimen may be necessary for selected patients.
RECOMMENDATIONS FOR ADULT HIV
258 JAMA, July 14, 2004—Vol 292, No. 2 (Reprinted) ©2004 American Medical Association. All rights reserved.

preclude use of NNRTIs or protease in-hibitors, a combination consisting of zi-dovudine, abacavir, and lamivudine maybe considered (evidence strength rat-ing, VII). In these special situations, closeHIV RNA level monitoring is manda-tory to identify early virological failure.The 3-NRTI regimens that should notbe used are: tenofovir, abacavir, and la-mivudine (evidence strength rating, IB);tenofovir, didanosine, and lamivudine(evidence strength rating, IB); and stavu-dine, didanosine, and abacavir (evi-dence strength rating, IB).
Initial 4-drug regimens (ritonavir atthe boosting dose is not considered anadditional antiretroviral drug) are notrecommended at this time (evidencestrength rating, IA). Experimental2-drug regimens (eg, a boosted prote-ase inhibitor and an NNRTI or a sec-
ond protease inhibitor) require furtherstudy before they can be safely recom-mended. Monotherapy consisting of aboosted protease inhibitor (eg, lopinavir/ritonavir alone) is not recommended(evidence strength rating, IV). Atten-tion to potential interactions betweendrugs among all drug components inregimens (first and subsequent ones) isimportant (TABLE 5), as is caution forthe use of combinations that have notbeen adequately tested in clinical trialsor pharmacokinetic evaluations.
WHEN TO CHANGE ANDWHAT TO CHANGE TORecent Data AddressingThese Questions
Changes to the initial antiretroviral regi-mens are common and most often re-lated to treatment-related toxic effects,
intolerance, inconvenience, or failure.Indeed, the median time of an initial regi-men is 1.6 years.16 The recommenda-tions for when to change a regimen andwhat to change to depend on the rea-son for changing therapy, whether it isin response to the first treatment or tomultiple treatment failure, and the avail-ability of active drugs to construct a po-tent regimen.
Toxicity, Intolerance,or InconvenienceSeveral studies have evaluated switch-ing the protease inhibitor componentof a regimen to an NNRTI in patientswith plasma HIV RNA levels belowdetection to reduce metabolic abnor-malities and fat maldistribution syn-dromes.45 In general, changing therapyis virologically safe in a patient harbor-
Table 5. Interactions Between Antiretroviral Drug Pairs Requiring Dosing Alteration or Avoidance*
Drug 1 Drug 2 Result Panel Suggestion
Zidovudine Stavudine Intracellular antagonism Do not combineStavudine Didanosine Toxicity (peripheral neuropathy, lactic
acidosis)Avoid, especially during pregnancy
Lamivudine Emtricitabine Similar drugs Do not combineTenofovir Enteric-coated didanosine Increased didanosine level75,76 Decrease didanosine to 250 mgTenofovir Atazanavir Increased tenofovir level, decreased
atazanavir levelAdd ritonavir boosting†
Delavirdine Amprenavir Increased amprenavir level77 Avoid, or decrease amprenavir doseDelavirdine Indinavir Increased indinavir level78 Avoid, or decrease indinavir dose‡Delavirdine Saquinavir Increased saquinavir level Decrease saquinavir doseEfavirenz Indinavir Decreased indinavir level79 Increase indinavir dose‡Efavirenz Lopinavir/ritonavir Decreased lopinavir level80,81 Increase lopinavir and ritonavir dose to
twice dailyEfavirenz Nevirapine Decreased efavirenz level82 Not recommendedEfavirenz Ritonavir Increased efavirenz and ritonavir levels83 Decrease ritonavir doseEfavirenz Amprenavir Decreased amprenavir level84,85 Add ritonavir boosting†Efavirenz Atazanavir Decreased atazanavir level Add ritonavir boosting†Efavirenz Saquinavir Decreased saquinavir level44 Add ritonavir boosting†Nevirapine Lopinavir/ritonavir Decreased lopinavir level86 Increase lopinavir and ritonavir dose to
twice dailyNevirapine Indinavir Decreased indinavir level87 Increase indinavir dose‡ or add ritonavir
boosting†Nevirapine Saquinavir Decreased saquinavir level Add ritonavir boosting†Nelfinavir Saquinavir Increased nelfinavir level88 Decrease saquinavir doseAtazanavir Indinavir Hyperbilirubinemia Do not combineFosamprenavir
or amprenavirLopinavir/ritonavir Decreased amprenavir
and lopinavir levelsAvoid unless doses can be adjusted
according to plasma concentrationsof amprenavir and lopinavir§
Fosamprenavir Amprenavir Similar drugs Do not combine
*Many antiretroviral drugs affect the level of a second agent in the class but not to a degree requiring dose changes or avoidance. There are many important interactions betweenantiretroviral agents and drugs in other classes, which are not summarized in this table. Certain groups of antiretroviral drugs affect resistance selection resulting in potentiallyadverse outcomes, but these are not included in this table.
†Dose of ritonavir in boost is not specified.‡Little or no data exist to define the exact dose adjustment required.§Data are conflicting. One study suggests no adjustment needed.
RECOMMENDATIONS FOR ADULT HIV
©2004 American Medical Association. All rights reserved. (Reprinted) JAMA, July 14, 2004—Vol 292, No. 2 259

ing no archived drug resistance muta-tions.46 Hyperlipidemia associated withprotease inhibitor use has improved af-ter changing therapy.45 Switching froma protease inhibitor to nevirapine pro-duced greater declines in cholesterollevels than did changing to efavirenz,and nevirapine was associated with sus-tained increases in levels of high-density lipoprotein cholesterol. Once afat maldistribution syndrome has oc-curred, switching the putatively offend-ing antiretroviral agents may halt fur-ther progression of the body shapechanges, but usually does not reversethe abnormality or does so slowly.45,47
Mitochondrial toxicity is the likelyunderlying mechanism responsible forthe lactic acidosis syndrome associ-ated with NRTIs, with the risk beingpresumptively related to the differen-tial inhibition of mitochondrial DNApolymerase � by NRTIs.48 Stavudine andthe combination of stavudine and di-danosine appear to pose the greatest riskamong NRTIs but lactic acidosis has oc-curred with zidovudine and other drugsin this class.48 Few studies have ad-dressed the consequences of switch-ing from a combination of 2 NRTIs anda protease inhibitor or an NNRTI to anNRTI-sparing regimen combining aprotease inhibitor and an NNRTI in pa-tients with HIV RNA plasma levels be-low detection. Preliminary data sug-gest that switching to a combination ofnevirapine, lopinavir/ritonavir49 or efa-virenz, saquinavir and low-dose rito-navir50 may be virologically safe.
Treatment FailureIncomplete adherence is the most fre-quent cause of first virological failure.1
The benefits of plasma HIV RNA sup-pression to less than 50 copies/mL ondurability of response and prevention ofemergence of resistance support usingthis cutoff as a strict definition of viro-logical failure.1 However, isolated epi-sodes of intermittent viremia, or blips(transient plasma HIV RNA levels �50copies/mL), do not predict subsequentvirological failure.51 In patients withmore advanced treatment failure and ahigh level of multidrug resistance in
whom a HIV RNA level below 50 cop-ies/mL cannot be achieved, the virologi-cal objective of the next regimen shiftsto reducing the HIV RNA level by at least0.5 log10 to 1 log10.52,53 Maintenance ofimmunological and clinical integritythen becomes the main objective.
A key to successful management ofantiretroviral treatment failure in whichdrug resistance is suspected or docu-mented is the ability to construct a regi-men that contains 3 active drugs; thenumber of active drugs in a regimencorrelates with subsequent virologicalsuccess.54 The challenge arises in try-ing to accomplish this given the in-creasing recognition of drug class cross-resistance that severely reduces options.
Treatment Interruptionsand Intermittent TherapyStudies are under way to evaluate struc-tured (or supervised) treatment inter-ruptions (STIs), which include inter-mittent therapy strategies in patientswith controlled virus replication whilereceiving drug therapy. The objectiveis to determine if several cycles of STIscan reduce the duration of exposure todrug therapy without compromising theCD4 cell count. A potential risk is theemergence of virus resistance to drugtherapy.55
In patients who had previously re-ceived treatment, STI has been pro-posed to allow “reversion” to wild-type virus. Three randomized trials haveshown no benefit to this approach56-58
and one has reported benefit.59 Differ-ences in baseline CD4 cell counts, useof multidrug therapy (ie, �6 drugs),and lengths of interruptions may ex-plain these differences.
New DrugsSince the previous guidelines, 3 newdrugs have become available for use intreatment failure.
Enfuvirtide. A subcutaneously ad-ministered HIV fusion inhibitor, enfu-virtide was evaluated in 2 large phase3 trials in patients with advancedHIV disease (median CD4 cell count,90/µL); in patients with multiple pre-vious and current treatment failures
(median, 12 prior antiretroviral drugs);and in patients with a median HIV RNAlevel of 130 000 copies/mL.60,61 Pa-tients were randomized to receive anoptimized background therapy with orwithout the addition of enfuvirtide. Af-ter 48 weeks, the enfuvirtide group hada significantly greater decrease in HIVRNA level (1.48 log10 reduction) thanthe optimized background only group(0.63 log10 reduction). With the excep-tion of frequent injection-site reac-tions, the drug was well tolerated.60,61
Bacterial pneumonia was more fre-quent with (6.6%) than without (0.6%)enfuvirtide, and hypersensitivity reac-tions were rare (�1%). In a secondaryanalysis of the combined TORO data-bases, 37.4% in the enfuvirtide groupand 16.2% in the optimized back-ground only group had plasma HIVRNA levels below 400 copies/mL at 24weeks (P�.001). Independent of en-fuvirtide use, the likelihood of viro-logical response was greater for pa-tients who had a baseline CD4 cellcount above 100/µL (odds ratio [OR],2.4; 95% CI, 1.6-3.5); baseline HIV RNAlevel below 100000 copies/mL (OR, 1.8;95% CI, 1.2-2.6); prior exposure tofewer than 10 antiretroviral drugs (OR,1.8; 95% CI, 1.2-2.6); and more than2 additional active antiretroviral drugsin their background regimen (OR, 2.8;95% CI, 2.0-4.0). Of note, in theseanalyses, 80% of patients who had all4 positive prognostic factors had HIVRNA levels below 400 copies/mL atweek 24.54
Atazanavir. A regimen containing300 mg/d of atazanavir and 100 mg/dof ritonavir provided viral load reduc-tion at 24 weeks comparable to lopi-navir/ritonavir in 1 study,32 whereas 400mg/d of atazanavir (unboosted) wasinferior to lopinavir/ritonavir.35 Of note,the combination of atazanavir andlow dose ritonavir was associatedwith less elevation of plasma lipid lev-els (particularly total cholesterol and tri-glycerides) than boosted proteaseinhibitor comparators in treatment-experienced patients.32 Tenofovir coad-ministration diminishes the oral bio-availability of atazanavir, and ritonavir
RECOMMENDATIONS FOR ADULT HIV
260 JAMA, July 14, 2004—Vol 292, No. 2 (Reprinted) ©2004 American Medical Association. All rights reserved.

boosting of atazanavir counteracts thisnegative drug interaction.62 Thus, whengiven to treatment-experienced patientsor when combined with tenofovir,atazanavir should only be used withritonavir boosting (evidence strengthrating, IB).
Fosamprenavir. A prodrug of am-prenavir, fosamprenavir has higherbioavailability and an improved formu-lation over the parent compound. Fos-amprenavir should be administered withlow-dose ritonavir (700 mg of fosam-prenavir and 100 mg of ritonavir twicedaily) (evidence strength rating, IB). Ina comparative study, fosamprenavir withlow-dose ritonavir taken twice daily hadsimilar activity and tolerability as lopi-navir/ritonavir.63
RecommendationsChanging Therapy Because of Toxic-ity, Intolerance, or Inconvenience. Ad-verse effects of antiretroviral drugs arenumerous, ranging from low-grade in-tolerance to life-threatening reac-tions. Low-grade and often transientsymptoms of high frequency that typi-cally occur early after initiation oftherapy (eg, zidovudine-related head-ache and nausea; efavirenz-related cen-tral nervous system adverse effects) canoften be mitigated through patient edu-cation. When symptoms associated witha particular agent do not resolve, orlaboratory toxicity develops (eg, zido-vudine-related anemia), single drugsubstitutions (eg, changing zidovu-dine to stavudine or changing efavi-renz to nevirapine) may be indicated(evidence strength rating, II).
When toxicity cannot be confi-dently attributed to a single drug andis severe enough to require temporarydiscontinuation of therapy, all agentsin the combination should be stopped(evidence strength rating, VII). If drugswith substantially different half lives arein the regimen(eg,NNRTIsandNRTIs),staggered discontinuation of the drugsshould be considered to avert the emer-gence of drug resistance (evidencestrength rating, V). For example, phar-macokinetic data indicate that NNRTIspersist and select for resistance after
drug discontinuation.19,64,65 Stoppingnevirapine or efavirenz 5 to 7 daysbefore stopping the NRTI componentshas been suggested. However, the effec-tiveness of this approach in avertingresistance in the clinical setting needsto be determined.66 Once the toxicityresolves, a new regimen can often beintroduced.67
Cycles of STIs in patients with con-trolled viremia simply to reduce long-term exposure to the drugs are notrecommended at this time, nor are in-termittent treatment approaches forinitial or failing regimens (evidencestrength rating, IB).
A difficult toxicity-management ques-tion is whether to change therapy in theface of metabolic abnormalities. Hyper-lipidemia associated with protease in-hibitors sometimes can be managed withdiet, exercise, and lipid-lowering agentsif the benefit of maintaining the particu-lar protease inhibitor is thought to out-weigh the risk of changing therapy.68
This situation commonly arises in thetreatment-experienced patient with adocumented drug-resistant virus inwhom a protease inhibitor-based regi-men has led to successful virological sup-pression. This contrasts to the clinicalcircumstance in which a patient withdrug-susceptible virus at baseline be-gins therapy with a protease inhibitor-based regimen and achieves virologicalsuppression, but in whom substantialhyperlipidemia develops. With the lat-ter, switching the protease inhibitor toan NNRTI is often virologically safe andleads to improving the lipid profile.
Fat maldistribution syndromes (in-cluding central fat accumulation andperipheral fat wasting) pose particularmanagement challenges because manydrugs from different classes are ofteninvolved. Given that stopping the re-sponsible drug(s) usually does not re-verse the abnormality or does so onlyslowly,68 close monitoring for the firstsigns of body fat changes and earlyswitching, if options exist, is recom-mended (evidence strength rating, VII).
Symptomatic lactic acidosis is a life-threatening condition for which imme-diate discontinuation of the antiretro-
viral regimen is indicated (evidencestrength rating, II). Following recov-ery, the safest course is to introduce anNRTI-sparing regimen, such as a rito-navir-boosted protease inhibitor withan NNRTI. However, lamivudine (andpresumably emtricitabine), abacavir,and tenofovir may sometimes be safelyreintroduced following full recoveryfrom this syndrome if benefit is thoughtto outweigh the risk (evidence strengthrating, V).48 Close monitoring is re-quired if this is attempted.
Changing Therapy Because of Treat-ment Failure. Treatment failure may bedefined clinically (HIV-related dis-ease progression), immunologically(declining CD4 cell count), or virologi-cally. Viral rebound should be con-firmed to ensure that it is not tran-sient (ie, a blip).
In individuals in whom the first regi-men fails and who were infected withdrug-susceptible virus, careful atten-tion to adherence is required (evidencestrength rating, VII). Supportive ques-tioning about adherence (eg, number ofmissed doses, reasons for the misseddoses, etc) may provide insight into thelikely success of the current regimen andcreate an opportunity for intervention.Assessment of subtle toxic effects as-cribed to the drugs is particularly im-portant in ensuring adequate adher-ence. If attempts at improving adherencefail and plasma HIV RNA levels are con-firmed to be higher than 500 cop-ies/mL up to 1000 copies/mL, resis-tance testing should be obtained(evidence strength rating, II). Full sus-ceptibility to all drugs in the regimensuggests an adherence problem. In thiscircumstance, the regimen does not needto be changed unless intolerance to orinconvenience of 1 or more compo-nents is at the root of the diminished ad-herence. If drug resistance is detected,altering the regimen is indicated (evi-dence strength rating, IA). The target forthe new therapy is the same as in thetreatment-naive patient—to suppress theplasma HIV RNA level below 50 cop-ies/mL (evidence strength rating, VII).
The management challenges increasesubstantially as subsequent regimen fail-
RECOMMENDATIONS FOR ADULT HIV
©2004 American Medical Association. All rights reserved. (Reprinted) JAMA, July 14, 2004—Vol 292, No. 2 261

ures cause further drug resistance andintolerance, and thereby limit theremaining antiretroviral options. Ifdurable undetectable levels of HIV RNAare deemed unachievable, the goal oftherapy shifts from preventing resis-tance (ie, maintaining �50 HIV RNAcopies/mL) to maintaining immuno-logical integrity and preventing clini-cal disease progression. Assumingadherence is optimized and overt clini-cal disease progression is not present,the following should be evaluated: (1)the antiretroviral drug options thatremain based on the results of drugresistance testing and treatment his-tory; (2) the plasma HIV RNA level; and(3) the CD4 cell count. If a new regi-men that contains at least 2 or 3 activedrugs can be constructed, strong con-sideration should be given to a changeso that further drug resistance compro-mising entire drug classes does notevolve (evidence strength rating, IA).If, however, such a regimen cannot beconstructed, changing therapy can bedeferred, unless the imminent risk ofan opportunistic disease is deemed high.
When resistance to and toxicity ofNRTIs or NNRTIs limits the availabil-ity of nonprotease inhibitor drugs, useof a double-boosted protease inhibitor(2 active protease inhibitors and low-dose ritonavir) has been proposed forstudy. Despite the frequent use in clini-cal practice, the paucity of data for mostmultiprotease inhibitor combinationsin terms of pharmacokinetic interac-tions, tolerance, or long-term adverseeffects warrants extreme caution. Forexample, coadministration of lopinavir/ritonavir with fosamprenavir causeslowered concentrations of both lopi-navir and fosamprenavir. This also il-lustrates the importance of having suf-ficient pharmacokinetic data to supportdosing in clinical practice and a pos-sible role for therapeutic drug levelmonitoring in patient management.There are, however, insufficient dataother than from pilot testing to recom-mend therapeutic drug monitoring atthis time.
Aspecialarea forconsiderationof regi-men change is in the type of discordant
response in which the HIV RNA level isbelow the limit of detection but the CD4cell count response is blunted. Currentmedications should be reviewed forpotential hematologic toxicity that alsomay be responsible for the blunted CD4cell response. Changing or intensifyingthe regimen has not been shown to haveaneffecton theCD4cell count response.The use of interleukin 2 in this settingremains a research question only. Therole of STIs for managing multiple fail-ure requiresmorestudy, andtheyarenotrecommended at this time.
Role of New Drugs in Treatment-Experienced Patients. The optimal timeto use enfuvirtide in treatment-experienced patients involves consid-ering its inconvenience, which is gen-erally acceptable in patients with alimited number of alternative options,and its high cost. Enfuvirtide is bestconsidered at the time of the second,third, or fourth failure, depending onthe number of active drugs that re-main as options (evidence strength rat-ing, IA). The cost and need for subcu-taneous administration often contributeto delayed use of this drug to a pointwhen outcome may be compromised bythe inability to combine it with otheractive drugs. If enfuvirtide is to be used,incremental, functional monotherapyshould be avoided whenever possible(evidence strength rating, IB). Amongpatients who have achieved an unde-tectable plasma HIV RNA level, thereis no evidence that enfuvirtide can bediscontinued without resulting in a vi-ral rebound.
Available data suggest that atazana-vir should be boosted with ritonavirwhen used in treatment-experiencedpatients (evidence strength rating, IV).The role of atazanavir in multiple treat-ment failure is unknown. Similarly, fos-amprenavir should be boosted andgiven twice daily, especially in the set-ting of multidrug-resistant virus. Theuse of either drug in this setting shouldbe guided by resistance testing results(evidence strength rating, IA).
Management of antiretroviral treat-ment failure and multidrug resistancemay also involve the use of investiga-
tional drugs through clinical trials. Phy-sicians specializing in the treatment ofHIV should remain cognizant of drugsin development that may become avail-able. These drugs may provide addi-tional options for constructing effec-tive regimens and may influence thetiming of a change in therapy.
Monitoring Antiretroviral Therapy.Clinical, CD4 cell count, and plasmaHIV RNA level monitoring remain toolsin assessing the need for and the re-sponse to therapy and recommenda-tions have not changed.1 Maximal ad-herence to the chosen regimen is crucialto the success of antiretroviral therapyand attention to adherence is re-quired.1 Routine drug resistance test-ing should be used in treatment-naiveand treatment-experienced persons asrecommended.69 Viral replicative ca-pacity, which can be impaired by drugresistance mutations, may in some pa-tients result in prolonged elevations ofCD4 cell counts in the setting of ap-parent virological failure. Althoughcommercially available, it is not yetknown if replicative capacity adds sub-stantial information to routine clini-cal and laboratory monitoring. Thera-peutic drug monitoring is performedfrequently in certain countries, but itsrole in clinical practice remains con-troversial. Experimental monitoring fortoxicity predilection, such as humanleukocyte antigen typing for abacavirhypersensitivity risk70 or mitochon-drial DNA quantitation for NRTI risks,requires further validation.
CONCLUSIONSAntiretroviral therapy remains a rap-idly evolving and challenging area ofHIV medicine. The field will continueto evolve with additional insights intopathogenesis and new drug develop-ment. With respect to the latter, newagents in existing drug classes (eg,D-D4FC, SPD-754, TMC-125, tiprana-vir, TMC-114) and in new drug classes(eg, CCR5 inhibitors, integrase inhibi-tors, maturation inhibitors) that havereached the clinical testing phase pro-vide hope that new options will be avail-able over the next few years.
RECOMMENDATIONS FOR ADULT HIV
262 JAMA, July 14, 2004—Vol 292, No. 2 (Reprinted) ©2004 American Medical Association. All rights reserved.

Clinicians and patients are con-fronted with the contrast of the increas-ingly complex individualization of treat-ment in the developed world and themassive antiretroviral implementationprograms that are planned or ongoingin the developing world. The prin-ciples of pathogenesis and treatmentlearned in both settings can ultimatelycontribute to improved care for all.
Author Affiliations: Department of Infectious Dis-eases, Hopital Bichat-Claude Bernard, X. Bichat Medi-cal School, Paris, France (Dr Yeni); Department of Medi-cine, Columbia University College of Physicians andSurgeons, New York, NY (Dr Hammer); Departmentof Immunology and Infectious Diseases, Harvard Medi-cal School, Boston, Mass (Dr Hirsch); Department ofMedicine, University of Alabama, Birmingham (Dr Saag);Department of Preventive Medicine, Universidade Fed-eral do Rio de Janeiro, Rio de Janeiro, Brasil (Dr Schech-ter); Department of Biomedicine, Brown UniversitySchool of Medicine, Providence, RI (Dr Carpenter); De-partment of Medicine, University of Miami School ofMedicine, Miami, Fla (Dr Fischl); Department of Medi-cine, University of Barcelona, Barcelona, Spain (Dr Ga-tell); Department of HIV Medicine, Chelsea and West-minster Hospital, London, England (Dr Gazzard);International AIDS Society-USA, San Francisco, Calif (MsJacobsen); Department of Medicine, Stanford Univer-sity Medical Center, Stanford, Calif (Dr Katzenstein);Department of Medicine, University of British Colum-bia, Vancouver (Dr Montaner); Departments of Pa-thology and Medicine, University of California and SanDiego VA Healthcare System, San Diego (Dr Rich-man); Department of Medicine, University of Colo-rado School of Medicine, Denver (Dr Schooley); AIDSResearch Consortium of Atlanta, Ga (Dr Thompson);Istituto Superiore di Sanita, Rome, Italy (Dr Vella); De-partment of Medicine, University of California and SanFrancisco Veterans Affairs Medical Center, San Fran-cisco (Dr Volberding).Financial Disclosures Dr Yeni has received researchgrants for site investigator from GlaxoSmithKline, Bris-tol-Myers Squibb, Boehringer Ingelheim, Roche,Tibotec/Virco, and Gilead. Dr Hammer has receivedresearch grants for site investigator from Roche,GlaxoSmithKline, and Merck. Dr Hirsch has receivedresearch support from Takeda. Dr Saag has receivedresearch support from Abbott Laboratories, Bristol-Myers Squibb, Gilead Sciences, GlaxoSmithKline, OrthoBiotech/Johnson & Johnson, Pfizer/Agouron, and Hoff-mann-LaRoche. Dr Fischl has received research grantsfrom Abbott Laboratories, Bristol-Myers Squibb, GileadSciences, GlaxoSmithKline, and Ortho Biotech. Dr Gaz-zard has received research grants from Abbott Labo-ratories, Boehringer Ingelheim, Pfizer, GlaxoSmithKline,Bristol-Myers Squibb, and Johnson & Johnson. Dr Mon-taner has received grants from Abbott Laboratories,Agouron Pharmaceuticals, Shire Biochemical, Boe-hringer Ingelheim, Bristol-Myers Squibb, DuPontPharma, Gilead Sciences, GlaxoSmithKline, Roche,Kucera Pharmaceutical, Merck Frosst Laboratories,Pharmacia & Upjohn, and Trimeris. Dr Schooley hasreceived grants from GlaxoSmithKline, Bristol-MyersSquibb, Merck, and Tibotec/Virco. Dr Thompson hasreceived grants from Abbott Laboratories, Agouron/Pfizer Pharmaceuticals, Boeringer Ingelheim, Bristol-Myers Squibb, Chiron Corporation, GlaxoSmithKline,Gilead Sciences, Merck Research Laboratories, Oxo-Chemie, Roche, Serono, Theratechnologies, TrianglePharmaceuticals, Trimeris, and VaxGen.
Dr Yeni has received honoraria for advisory posi-tions and lecture sponsorships from Abbott Labora-
tories, Bristol-Myers Squibb, Boehringer Ingelheim,Roche, Tibotec/Virco, and Merck Sharp and Dohme.Dr Saag has received honoraria for positions on thespeakers bureau for Abbott Laboratories, BoeringerIngelheim, Bristol-Myers Squibb, Gilead Sciences,GlaxoSmithKline, OrthoBiotech, Johnson & Johnson,Pfizer, Agouron, Roche, Schering-Plough, Shire Phar-maceutical, TherapyEdge, Tibotec/Virco, Trimeria, Ver-tex, and ViroLogic. Dr Schechter has received hono-raria from Abbott Laboratories, Bristol-Myers Squibb,GlaxoSmithKline, Merck, and Roche. Dr Fischl has re-ceived honoraria for continuing medical education pro-grams from GlaxoSmithKline. Dr Gatell has served inadvisory positions for Roche, Bristol-Myers Squibb,Merck Sharp and Dohme, GlaxoSmithKline, Gilead,Boehringer Ingelheim, Abbott Laboratories, Tibotec/Virco. Dr Gazzard has received lectureship fees fromAbbott Laboratories, Boehringer Ingelheim, Pfizer,GlaxoSmithKline, Bristol-Myers Squibb, and Johnson& Johnson. Dr Katzenstein has held advisory posi-tions at Boehringer Ingelheim, Bristol-Myers Squibb,Gilead Sciences, GlaxoSmithKline, Merck, ViroLogic,Visible Genetics, and the Doris Duke Charitable Trust.Dr Montaner has received honoraria for speaking fromAbbott Laboratories, Agouron Pharmaceuticals, ShireBiochemical, Boehringer Ingelheim, Bristol-MyersSquibb, DuPont Pharma, Gi lead Sc iences ,GlaxoSmithKline, Hoffmann-La Roche, Kucera Phar-maceutical, Merck Frosst Laboratories, Pharmacia &Upjohn, and Trimeris Inc. Dr Thompson has receivedhonoraria for lecture sponsorships and continuing medi-cal education from Abbott Laboratories, Agouron/Pfizer Pharmaceuticals, Boeringer Ingleheim, Bristol-Myers Squibb, GlaxoSmithKline, Gilead Sciences,Roche, Serono, Triangle Pharmaceuticals, and Trim-eris. Dr Vella has received lecture sponsorship for sat-ellite symposia and continuing medical education pro-grams from Merck, Agouron, Gilead, BoehringerIngelheim, and Roche. Dr Volberding has receivedhonoraria from Gilead, Bristol-Myers Squibb,GlaxoSmithKline, and Boehringer Ingelheim.
Dr Hammer has been a consultant for Bristol-Myers Squibb, GlaxoSmithKline, Merck, Shionogi,Pfizer, Boehringer Ingelheim, Shire, Gilead, and Tibotec/Virco. Dr Hirsch has been a consultant for ScheringPlough, GlaxoSmithKline, and Bristol-Myers Squibb.Dr Saag has been a consultant for Abbott Laborato-ries, Boeringer Ingelheim, Bristol-Myers Squibb, Gi-lead Sciences, GlaxoSmithKline, OrthoBiotech/Johnson & Johnson, Pfizer/Agouron, Roche, Schering-Plough, Shire Pharmaceutical, TherapyEdge, Tibotec/Virco, Trimeria, Vertex, and ViroLogic. Dr Schechterhas been a consultant for Abbott Laboratories, Bristol-Myers Squibb, GlaxoSmithKline, Merck, and Roche.Dr Fischl has served as an advisor for Agouron Phar-maceuticals and GlaxoSmithKline. Dr Richman has beena consultant for Abbott Laboratories, Bristol-MyersSquibb, Chiron, Gilead, GlaxoSmithKline, Merck, No-virio, Pfizer, Roche, Takeda, Triangle, and ViroLogic.Dr Schooley has been a consultant for Abbott Labo-ratories, Pfizer, Hoffmann-LaRoche, GlaxoSmithKline,Bristol-Myers Squibb, Merck, Vertex, ViroLogic, andTibotec/Virco. Dr Thompson has been a consultantfor Abbott Laboratories, Agouron/Pfizer Pharmaceu-ticals, GlaxoSmithKline, Gilead Sciences, Serono, andTriangle Pharmaceuticals. Dr Volberding has been aconsultant for Pfizer, Bristol-Myers Squibb, and Shire.
Dr Katzenstein holds a US patent for polymerasechain reaction assays monitoring antiviral therapy andmaking therapeutic decisions in the treatment of AIDS.Dr Montaner holds 2 US patents, one regarding useof nevirapine and another regarding pharmacologi-cal applications of mitochondrial DNA assays. Dr Mon-taner has 2 patent applications that are pending, oneregarding pharmacological applications of mitochon-drial DNA assays and another regarding sepsis.Author Contributions: Study concept and design: Yeni,Hammer, Hirsch, Saag, Schechter, Carpenter, Fischl,
Gatell, Jacobsen, Katzenstein, Montaner, Richman,Schooley, Vella, Volberding.Acquisition of data: Yeni, Hirsch, Jacobsen, Katzen-stein, Montaner, Vella, Volberding.Analysis and interpretation of data: Yeni, Hammer,Hirsch, Saag, Carpenter, Gatell, Gazzard, Montaner,Richman, Thompson, Volberding.Drafting of the manuscript: Yeni, Hammer, Hirsch,Saag, Schechter, Fischl, Gazzard, Jacobsen, Schooley,Volberding.Critical revision of the manuscript for important intel-lectual content: Yeni, Hammer, Hirsch, Saag, Schechter,Carpenter, Gatell, Katzenstein, Montaner, Richman,Schooley, Thompson, Vella, Volberding.Obtained funding: Hirsch, Jacobsen, Katzenstein,Montaner, Richman, Schooley, Vella, Volberding.Administrative, technical, or material support:Hammer, Hirsch, Schechter, Jacobsen, Katzenstein,Montaner, Richman, Schooley, Vella.Supervision: Yeni, Hammer, Hirsch, Carpenter, Gatell,Jacobsen, Katzenstein, Montaner, Richman, Schooley,Vella, Volberding.Funding/Support: This work was sponsored andfunded by the International AIDS Society-USA. No pri-vate sector or government funding contributed to thiseffort.Acknowledgment: We thank Mai Vu, PharmD, forcareful review of the information on interactions be-tween drugs and Michelle Tayag for administrative sup-port in preparing the manuscript.
REFERENCES
1. Yeni PG, Hammer SM, Carpenter CCJ, et al. An-tiretroviral treatment for adult HIV-1 infection in 2002:updated recommendations of the International AIDSSociety-USA panel. JAMA. 2002;288:222-235.2. World Health Organization Guidelines. Scaling upantiretroviral therapy in resource-limited settings:guidelines for a public health approach. June 2002.Available at: http://www.who.int/hiv/pub/prev_care/en/ScalingUp_E.pdf. Accessed November 13, 2003.3. Carpenter CCJ, Fischl MA, Hammer SM, et al. An-tiretroviral therapy for HIV infection in 1996: recom-mendations of an international panel. JAMA. 1996;276:146-154.4. Chene G, Sterne JA, May M, et al. Prognostic im-portance of initial response in HIV-1 infected pa-tients starting potent antiretroviral therapy: analysisof prospective studies. Lancet. 2003;362:679-686.5. Egger M, May M, Chene G, et al. Prognosis of HIV-1infected drug naive patients starting potent antiret-roviral therapy: a collaborative analysis of prospec-tive studies. Lancet. 2002;360:119-129.6. Palella FJ, Deloria-Knoll M, Chmiel JS, et al. Sur-vival benefit of initiating antiretroviral therapy in HIV-infected persons in different CD4+ cell strata. Ann In-tern Med. 2003;138:620-626.7. Sterling TR, Chaisson RE, Keruly J, Moore RD. Im-proved outcomes with earlier initiation of highly ac-tive antiretroviral therapy among human immunode-ficiency virus-infected patients who achieve durablevirologic suppression: longer follow-up of an obser-vational cohort study. J Infect Dis. 2003;188:1659-1665.8. Wood E, Hogg RS, Yip B, et al. Higher baseline lev-els of plasma human immunodeficiency virus type 1RNA are associated with increased mortality after ini-tiation of triple-drug antiretroviral therapy. J Infect Dis.2003;188:1421-1425.9. Wood E, Hogg RS, Yip B, Harr igan PR,O’Shaughnessy MV, Montaner JS. Effect of medica-tion adherence on survival of HIV-infected adults whostart highly active antiretroviral therapy when the CD4+cell count is 0.200 to 0.350 x 10(9) cells/L. Ann In-tern Med. 2003;139:810-816.10. Anastos K, Barron Y, Cohen MH, et al. The prog-nostic importance of changes in CD4+ cell count and
RECOMMENDATIONS FOR ADULT HIV
©2004 American Medical Association. All rights reserved. (Reprinted) JAMA, July 14, 2004—Vol 292, No. 2 263

HIV-1 RNA level in women after initiating highly ac-tive antiretroviral therapy. Ann Intern Med. 2004;140:256-264.11. de Pinho AM, Santoro-Lopes G, Harrold LR,Schechter M. Chemoprophylaxis for tuberculosis andsurvival of HIV-infected patients in Brazil. AIDS. 2001;15:2129-2135.12. Badri M, Wilson D, Wood R. Effect of highly ac-tive antiretroviral therapy on incidence of tuberculo-sis in South Africa: a cohort study. Lancet. 2002;359:2059-2064.13. Robbins GK, De Gruttola V, Shafer RW, et al. Com-parison of sequential three-drug regimens as initialtherapy for HIV-1 infection. N Engl J Med. 2003;349:2293-2303.14. Shafer RW, Smeaton LM, Robbins GK, et al. Com-parison of four-drug regimens and pairs of sequen-tial three-drug regimens as initial therapy for HIV-1infection. N Engl J Med. 2003;349:2304-2315.15. Lichtenstein KA, Delaney KM, Armon C, et al. In-cidence of and risk factors for lipoatrophy (abnormalfat loss) in ambulatory HIV-1-infected patients. J Ac-quir Immune Defic Syndr. 2003;32:48-56.16. Chen RY, Westfall AO, Mugavero MJ, et al. Du-ration of highly active antiretroviral therapy regi-mens. Clin Infect Dis. 2003;37:714-722.17. Centers for Disease Control and Prevention. In-corporating HIV prevention into the medical care ofpersons living with HIV: recommendations of the CDC,the Health Resources and Services Administration, theNational Institutes of Health, and the HIV MedicineAssociation of the Infectious Diseases Society ofAmerica. MMWR Recomm Rep. 2003;52(RR-12):1-24.18. Staszewski S, Morales-Ramirez J, Tashima KT, etal, for the Study 006 Team. Efavirenz plus zidovu-dine and lamivudine, efavirenz plus indinavir, and in-dinavir plus zidovudine and lamivudine in the treat-ment of HIV-1 infection in adults. N Engl J Med. 1999;341:1865-1873.19. Jourdain G, Ngo-Giang-Huong N, Tungyai P, etal. Exposure to intrapartum single-dose nevirapine andsubsequent maternal 6-month response to NNRTI-based regimens. In: 11th Conference on Retrovi-ruses and Opportunistic Infections; February 8-11,2004; San Francisco, Calif. Abstract 41LB.20. Mellors J, Palmer S, Nissley D, et al. Low-frequency NNRTI-resistant variants contribute to fail-ure of efavirenz-containing regimens. In: 11th Con-ference on Retroviruses and Opportunistic Infections;February 8-11, 2004; San Francisco, Calif. Abstract 39.21. DeJesus E, Herrera G, Teofilo E, et al. Efficacy andsafety of abacavir (ABC) versus zidovudine (ZDV) inantiretroviral therapy naive adults with HIV-1 infec-tion (Study CNA30024). In: 43rd Interscience Con-ference on Antimicrobial Agents and Chemotherapy;September 14-17, 2003; Chicago, Ill. Abstract H-446.22. Staszewski S, Gallant J, Pozniak A, et al. Efficacyand safety of tenofovir disoproxil fumarate (TDF) ver-sus stavudine (d4T) when used in combination withlamivudine (3TC) and efavirenz (EFV) in HIV-1 in-fected patients naive to antiretroviral therapy (ART):48-week interim results. In: 14th International AIDSConference; July 7-12, 2002; Barcelona, Spain. Ab-stract LbOr17.23. Cahn P, Raffi F, Saag M, et al. Virologic efficacyand patterns of resistance mutations in ART-naive pa-tients receiving combination therapy with once-dailyemtricitabine compared to twice-daily stavudine in arandomized, double-blind, multi-center clinical trial.In: 10th Conference on Retroviruses and Opportu-nistic Infections; 2004; Boston, Mass. Abstract 606.24. van Leeuwen R, Katlama C, Murphy RL, et al. Arandomized trial to study first-line combination therapywith or without a protease inhibitor in HIV-1-infected patients. AIDS. 2003;17:987-999.25. Podzamczer D, Ferrer E, Consiglio E, et al. A ran-domized clinical trial comparing nelfinavir or nevira-
pine associated to zidovudine/lamivudine in HIV-infected naive patients (the COMBINE Study). AntivirTher. 2002;7:81-90.26. Van Leth F, Phanuphak P, Ruxrungtham K, et al.Comparison of first-line antiretroviral therapy with regi-mens including nevirapine, efavirenz, or both drugs, plusstavudine and lamivudine: a randomised open-label trial,the 2NN Study. Lancet. 2004;363:1253-1263.27. Viramune [package insert]. Columbus, Ohio:Roxane Laboratories Inc; 2000.28. Walmsley S, Bernstein B, King M, et al. Lopinavir-ritonavir versus nelfinavir for the initial treatment ofHIV infection. N Engl J Med. 2002;346:2039-2046.29. Gerstoft J, Drake JW, Cahn P, et al. Final analysisof a randomised trial to evaluate safety and efficacyof indinavir/ritonavir versus saquinavir/ritonavir in adultHIV-1 infection: the MaxCmin1 Trial. In: 42nd Inter-science Conference on Antimicrobial Agents and Che-motherapy; September 27-30, 2002; San Diego, Calif.Abstract H-172.30. Murphy RL, Sanne I, Cahn P, et al. Dose-ranging, randomized, clinical trial of atazanavir withlamivudine and stavudine in antiretroviral-naive sub-jects: 48-week results. AIDS. 2003;17:2603-2614.31. Squires KE, Thiry A, Giordano M, for the AI424-034 International Study Team. Atazanavir (ATV) QDand efavirenz (EFV) QD with fixed-dose ZDV+3TC:comparison of antiviral efficacy and safety through wk24. In: 42nd Interscience Conference on Antimicro-bial Agents and Chemotherapy; September 27-30,2002; San Diego, Calif. Abstract AI424-034.32. DeJesus E, Grinsztejn B, Rodriguez C, et al. Effi-cacy and safety of atazanavir with ritonavir or sa-quinavir vs lopinavir/ritonavir in patients who have ex-perienced virologic failure on multiple HAART regimens:48 week results from BMS A1424-045. In: 11th Con-ference on Retroviruses and Opportunistic Infec-tions; February 8-11, 2004; San Francisco, Calif. Ab-stract 547.33. Montaner JSG, Saag MS, Barylski C, Siemon-Hryczyk P. FOCUS study: saquinavir QD regimen ver-sus efavirenz QD regimen 48 week analysis in HIV in-fected patients. In: 42nd Interscience Conference onAntimicrobial Agents and Chemotherapy; 2002; SanDiego, Calif. Abstract H-167.34. Bartlett JA, Johnson J, Herrera G, Sosa N, Rod-riguez AE, Shaefer MS. Abacavir/lamivudine (ABC/3TC) in combination with efavirenz (NNRTI), ampre-navir/ritonavir (PI) or stavudine (NRTI): ESS40001(CLASS) preliminary 48 week results. In: 14th Inter-national AIDS Conference; July 7-12, 2002; Barce-lona, Spain. Abstract TuOrB1189.35. Gulick RM, Ribaudo HJ, Shikuma CM, et al. Triple-nucleoside regimens versus efavirenz-containing regi-mens for the initial treatment of HIV-1 infection.N Engl J Med. 2004;350:1850-1861.36. Gallant JE, Rodriguez AE, Weinberg W, et al. Earlynon-response to tenofovir DF (TDF) + abacavir (ABC)and lamivudine (3TC) in a randomized trial com-pared to efavirenz (EFV) + ABC and 3TC: ESS30009.In: 43rd Interscience Conference on AntimicrobialAgents and Chemotherapy; September 14-17, 2003;Chicago, Ill. Abstract H-1772a.37. Landman R, Peytavin G, Descamps D, et al. Lowgenetic barrier to tesistance is a possible cause of earlyvirologic failures in once-daily regimen of abacavir, la-mivudine, and tenofovir: the tonus study. In: 11th Con-ference on Retroviruses and Opportunistic Infec-tions; February 8-11, 2004; San Francisco, Calif.Abstract 52.38. Jemsek J, Hutcherson P, Harper E. Poor virologicresponses and early emergence of resistance in treat-ment naive, HIV-infected patients receiving a once dailytriple nucleoside regimen of didanosine, lamivudine,and tenofovir DF. In: 11th Conference on Retrovi-ruses and Opportunistic Infections; February 8-11,2004; San Francisco, Calif. Abstract 51.39. Gerstoft J, Kirk O, Obel N, et al. Low efficacy and
high frequency of adverse events in a randomized trialof the triple nucleoside regimen abacavir, stavudineand didanosine. AIDS. 2003;17:2045-2052.40. Staszewski S, Keiser P, Montaner J, et al. Abacavir-lamivudine-zidovudine vs indinavir-lamivudine-zidovudine in antiretroviral-naive HIV-infected adults:a randomized equivalence trial. JAMA. 2001;285:1155-1163.41. Schurmann D, Gathe J, Sanne I, Wood R. Effi-cacy and safety of GW433908/ritonavir once daily intherapy-naive subjects, 48 week results: the SOLOstudy. In: 6th International Congress on Drug Therapyin HIV Infection. November 17-21, 2002; Glasgow,Scotland. Abstract PL14.4.42. Gazzard BG, De Jesus E, Cahn P, et al. Abacavir(ABC) once daily (OAD) plus lamivudine (3TC) OADin combination with efavirenz (EFV) OAD is well-tolerated and effective in the treatment of antiretro-viral therapy (ART) naive adults with HIV-1 infection(ZODIAC Study: CNA30021). In: 43rd InterscienceConference on Antimicrobial Agents and Chemo-therapy; September 14-17, 2003; Chicago, Ill. Ab-stract H-1722b.43. Saag MS, Cahn P, Raffi F. A randomized double-blind multicenter comparison of emtricitabine QD tostavudine BID. In: 42nd Interscience Conference onAntimicrobial Agents and Chemotherapy; Septem-ber 27-30, 2002; San Diego, Calif. Abstract LB-1.44. Sustiva [package insert]. Wilmington, Del: DuPontPharmaceuticals Inc; 2002.45. Saag MS, Powderly WG, Schambelan M, et al.Switching antiretroviral drugs for treatment of meta-bolic complications in HIV-1 infection: summary of se-lected trials. Top HIV Med. 2002;10:47-51.46. Martinez E, Arnaiz JA, Podzamczer D, et al. Sub-stitution of nevirapine, efavirenz, or abacavir for pro-tease inhibitors in patients with human immunodefi-ciency virus infection. N Engl J Med. 2003;349:1036-1046.47. Martin A, Smith DE, Carr A, et al. Reversibility oflipoatrophy in HIV-infected patients 2 years afterswitching from a thymidine analogue to abacavir: theMITOX extension study. AIDS. 2004;18:1029-1036.48. Cossarizza A, Moyle G. Antiretroviral nucleosideand nucleotide analogues and mitochondria. AIDS.2004;18:137-151.49. Negredo E, Bonjoch A, Sirera G, et al. NEKA study:NRTI-sparing regimen. In: 14th International AIDS Con-ference; July 7-12, 2002; Barcelona, Spain. AbstractLbPeB9021.50. Lopez-Cortes LF, Ruiz-Valderas R, Viciana P, etal. Once-daily saquinavir-sgc plus low-dose ritonavir(1200/100 mg) in combination with efavirenz: phar-macokinetics and efficacy in HIV-infected patients withprior antiretroviral therapy. J Acquir Immune DeficSyndr. 2003;32:240-242.51. Havlir DV, Bassett R, Levitan D, et al. Prevalenceand predictive value of intermittent viremia with com-bination HIV therapy. JAMA. 2001;286:171-179.52. Deeks SG, Wrin T, Liegler T, et al. Virologic andimmunologic consequences of discontinuing combi-nation antiretroviral-drug therapy in HIV-infected pa-tients with detectable viremia. N Engl J Med. 2001;344:472-480.53. Marschner IC, Collier AC, Coombs RW, et al.Use of changes in plasma levels of human immuno-deficiency virus type 1 RNA to assess clinical benefitto antiretroviral therapy. J Infect Dis. 1998;177:40-47.54. Montaner J. Analysis of virological response of en-fuvirtide in TORO: implications for patient manage-ment. In: 2nd International AIDS Society Conferenceon HIV Pathogenesis and Treatment; July 13-16, 2003;Paris, France. Abstract 116.55. Palmisano L, Giuliano M, Bucciardini R, et al. Emer-gence of resistance mutations during intermittentHAART: rate, predecting factors, and effect on viro-logic response. In: 11th Conference on Retroviruses
RECOMMENDATIONS FOR ADULT HIV
264 JAMA, July 14, 2004—Vol 292, No. 2 (Reprinted) ©2004 American Medical Association. All rights reserved.

and Opportunistic Infections; February 8-11, 2004;San Francisco, Calif. Abstract 552.56. Lawrence J, Mayers DL, Huppler Hullsiek K, et al.Structured treatment interruption in patients with mul-tidrug-resistant human immunodeficiency virus. N EnglJ Med. 2003;349:837-846.57. Ruiz L, Ribera E, Bonjoch A, et al. Role of struc-tured treatment interruption before a 5-drug salvageantiretroviral regimen: the Retrogene Study. J InfectDis. 2003;188:977-985.58. Benson C, Downey G, Havlir DV, et al. A 16-week treatment interruption does not improve the vi-rologic response to multidrug salvage therapy in treat-ment-experienced patients: 48-week results fromACTG A5086. In: 11th Conference on Retroviruses andOpportunistic Infections; February 8-11, 2004; SanFrancisco, Calif. Abstract 58.59. Katlama C, Dominguez S, Gourlain K, et al. Ben-efit of treatment interruption in HIV-infected patientswith multiple therapeutic failures: a randomized con-trolled trial (ANRS 097). AIDS. 2004;18:217-226.60. Lazzarin A, Clotet B, Cooper D. Efficacy of enfu-virtide in patients infected with drug-resistant HIV-1in Europe and Australia. N Engl J Med. 2003;348:2186-2195.61. Lalezari J, Henry K, O’Hearn M, et al. Enfu-virtide, an HIV-1 fusion inhibitor, for drug-resistantHIV infection in North and South America. N Engl JMed. 2003;348:2175-2185.62. Taburet AM, Piketty C, Gerard L, et al. Pharma-cokinetic parameters of atazanavir/ritonavir when com-bined to tenofovir in HIV infected patients with mul-tiple treatment failures: a sub-study of puzzle2-ANRS 107 trial. In: 10th Conference on Retrovirusesand Opportunistic Infections; February 10-14, 2003;Boston, Mass. Abstract 537.63. DeJesus E, LaMarca A, Sension M, Beltran C, YeniP. The context study: efficacy and safety ofGW433908/RTV in PI-experienced subjects with vi-rological failure (24 week results). In: 10th Confer-ence on Retroviruses and Opportunistic Infections; Feb-ruary 10-14, 2003; Boston, Mass. Abstract 178.64. Palmer S, Boltz V, Maldarelli F, et al. Emergenceand long-term persistence of NNRTI-resistant vari-ants in patients starting and stopping NNRTI-containing regimens. In: 11th Conference on Retro-viruses and Opportunistic Infections; February 8-11,2004; San Francisco, Calif. Abstract 37.65. Muro E, Droste J, Ter Hofstede H, Bosch M, Dol-mans W, Burger D. Nevirapine plasma concentra-tions are still detectable after more than 2 weeks inthe majority of women receiving single-dose NVP: im-plications for intervention studies. In: 11th Confer-ence on Retroviruses and Opportunistic Infections; Feb-ruary 8-11, 2004; San Francisco, Calif. Abstract 891.66. Lyons F, Coughlan S, Byrne C, et al. Emergenceof genotypic resistance in HIV-1-infected pregnantwomen taking HAART to reduce mother-to-child trans-mission of HIV-1. In: 11th Conference on Retrovi-
ruses and Opportunistic Infections; February 8-11,2004; San Francisco, Calif. Abstract 892.67. Taylor S, Allen S, Fidler S, et al. Stop study: afterdiscontinuation of efavirenz, plasma concentrationsmay persist for 2 weeks or longer. In: 11th Confer-ence on Retroviruses and Opportunistic Infections;February 8-11, 2004; San Francisco, Calif. Abstract131.68. Schambelan M, Benson CA, Carr A, et al. Man-agement of metabolic complications associatedwith antiretroviral therapy for HIV-1 infection: rec-ommendations of an International AIDS Society-USA Panel. J Acquir Immune Defic Syndr. 2002;31:257-275.69. Hirsch MS, Brun-Vezinet F, Clotet B, et al. Anti-retroviral drug resistance testing in adults infected withhuman immunodeficiency virus type I: 2003 recom-mendations of the International AIDS Society-USApanel. Clin Infect Dis. 2003;37:113-128.70. Mallal S, Nolan D, Witt C, et al. Association be-tween presence of HLA-B*5701, HLA-DR7, andHLA-DQ3 and hypersensitivity to HIV-1 reverse-transcriptase inhibitor abacavir. Lancet. 2002;359:727-732.71. Nieto-Cisneros L, Zala C, Fessel WJ, et al. Anti-viral efficacy, metabolic changes and safety of atazana-vir (ATV) versus lopinavir/ritonavir (LPV/RTV) in com-bination with 2 NRTIs in patients who have experiencedvirologic failure with prior PI-containing regimen(s):24-week results from BMS AI424-043. In: 2nd Inter-national AIDS Society Conference on HIV Pathogen-esis and Treatment; July 13-16, 2003; Paris, France.Abstract 117.72. Nadler J, Rodriguez-French A, Millard J, Wanna-maker P. The NEAT study: GW433908 efficacy andsafety in ART-naive subjects, final 48-week analysis.In: 10th Conference on Retroviruses and Opportu-nistic Infections; February 10-14, 2003; Boston, Mass.Abstract 177.73. Martinez E, Milinkovic A, de Lazzari E, et al. Pan-creatic toxicity associated with the co-administrationof didanosine and tenofovir in HIV-infected adults. Lan-cet. In press.74. Negredo E, Molto J, Burger D, et al. UnexpectedCD4 cell-count decline in patients receiving didano-sine- and tenofovir-based regimens despite undetect-able viral load. In: 11th Conference on Retrovirusesand Opportunistic Infections; February 8-11, 2004;San Francisco, Calif. Abstract 749.75. Viread [package insert]. Foster City, Calif: Gi-lead Sciences Inc; 2003.76. Kearney B, Flaherty J, Sayre J, et al. A multiple-dose, randomized, crossover, drug interaction studybetween tenofovir DF and lamivudine or didanosine.In: 1st International AIDS Society Conference on HIVPathogenesis and Treatment; July 8-11, 2001; Bue-nos Aires, Argentina. Abstract 337.77. Tran JQ, Petersen C, Garrett M, Hee B, Kerr BM.Pharmacokinetic interaction between amprenavir and
delavirdine: evidence of induced clearance by ampre-navir. Clin Pharmacol Ther. 2002;72:615-626.78. Ferry JJ, Herman BD, Carel BJ, Carlson GF, BattsD. Pharmacokinetic drug-drug interaction study ofdelavirdine and indinavir in healthy volunteers. J Ac-quir Def Syn Human Retrovir. 1998;18:252-259.79. Fiske WD, Mayers D, Wagner K, et al. Pharma-cokinetics of DMP 266 and indinavir multiple oral dosesin HIV-1 infected individuals. In: 4th Conference onRetroviruses and Opportunistic Infections; January 22-26, 1997; Washington, DC. Abstract 568.80. Bertz R, Hsu A, Lam W, et al. Pharmacokineticinteraction between lopinavir/ritonavir (ABT-378/r) andothers non-HIV drugs. AIDS. 2000;14(suppl 4):S100.81. Hsu A, Isaacson J, Brun S, et al. Pharmacokinetic-pharmacodynamic analysis of lopinavir-ritonavir in com-bination with efavirenz and two nucleoside reverse tran-scriptase inhibitors in extensively pretreated humanimmunodeficiency virus-infected patients. Antimi-crob Agents Chemother. 2003;47:350-359.82. Veldkamp AI, Hoetelmans RMW, Beijnen JH, etal. DONUT: the pharmacokinetics (PK) of the once dailynevirapine (NVP) and efavirenz (EFV) when used incombination. In: 7th Conference on Retroviruses andOpportunistic Infections; January 30-February 2, 2000;San Francisco, Calif. Abstract 80.83. Fiske W, Benedek IH, Joseph JL, et al. Pharma-cokinetics of efavirenz (EFV) and ritonavir (RIT) aftermultiple oral doses in healthy volunteers. In: 12th WorldAIDS Conference; June 28-July 3, 1998; Geneva, Swit-zerland. Abstract 42269.84. Falloon J, Piscitelli S, Vogel S, et al. Combinationtherapy with amprenavir, abacavir, and efavirenz inhuman immunodeficiency virus (HIV)-infected pa-tients failing a protease-inhibitor regimen: pharma-cokinetic drug interactions and antiviral activity. ClinInfect Dis. 2000;30:313-318.85. Department of Health and Human Services, HenryJ Kaiser Family Foundation. Guidelines for the use ofantiretroviral agents in HIV-infected adults and ado-lescents. Ann Intern Med. 1998;128:1079-1100.86. Degen O, Kurowski M, van Lunzen J, et al. Steadystate pharmacokinetics of lopinavir in combination withnevirapine or efavirenz. In: 14th International AIDSConference; July 7-12, 2002; Barcelona, Spain. Ab-stract TuPeB4573.87. Harris M, Durakovic C, Rae S, et al. Pilot studyof the safety, pharmacokinetics, immunological andantiviral effect of nevirapine, indinavir, and lamivu-dine among patients with advanced HIV disease whohad previously failed combination nucleoside therapy.J Infect Dis. 1998;177:1514-1520.88. Moyle G, Pozniak A, Opravil M, et al. The SPICEstudy: 48-week activity of combinations of saquina-vir soft gelatin and nelfinavir with and without nucleo-side analogues: study of Protease Inhibitor Combina-tions in Europe. J Acquir Immune Defic Syndr. 2000;23:128-137.
RECOMMENDATIONS FOR ADULT HIV
©2004 American Medical Association. All rights reserved. (Reprinted) JAMA, July 14, 2004—Vol 292, No. 2 265
Related Documents











