4 POSTGRADUATE MEDICAL JOURNAL January I953 additional hazard after the disease has been present for ten years. It is a radical concept which would connect the personality disorder with the malignant change, but such speculation, though idle, is of interest. K. GURLING. REFERENCES x. RICE-OXLEY, J. M., and TRUELOVE, S. (I950), Lancet, i, 663. 2. ANDRESEN, A. F. R. (1942), Am. J. Digest. Dis., 9, 9I. 3. MURRAY, C. D. (I930), J. Nerv. Ment. Dis., 72, 617. 4. MURRAY, C. D. (I930), Am. J. Med. Sci., I80, 239. 5. SULLIVAN, A. J. (I936), Am. J. Digest. Dis., 2, 65i. 6. DANIELS, G. E. (x942), New England J. Med., 226, 178. 7. WITTKOWER, E. (1938), Brit. Med. J., ii, I356. 8. GRACE, W. J., WOLF, S., and WOLFF, H. G. (195'), 'The Human Colon,' Heinneman, London. 9. LIUM, R. (1939), Am. J. Med. Sci., 197, 841. Io. LIUM, R. (1939), Arch. Int. Med., 63, 2I0. 11. FLEMING, A. B. (1922), Proc. Royal Soc., S.B., 306. 12. MEYER, K., and HAHNEL, E. (1946), J. biol. Chem., 163, 723. I3. SAMMONS, H. G. (I95I), Lancet, ii, 239. I4. PAULLEY, J. W. (1950), Gastroenterology, I6, 566. I5. HINTON, J. W., and SHARIHOFF, B. P., cited by Grace, Wolf and Wolff (8). i6. MORTON-GILL, A. (1944), Lancet, i, 536. I7. KIRSNER, J. B., and PALMER, W. L. (I95i), J. Ant. MVed. Ass., 147, 541. I8. HARDY, T. L., and BROOKE, B. (1952), 'Modern Trends in Gastroenterology,' edited by F. Avery Jones; Butter- worth, London. 19. LAHEY, F. H. (I950), Rev..Gastroenterology, 17, 723. 20. SLOAN, W. P., BARGEN, J. A., and CAGE, R. P., (I950) Gastroenterology, I6, 25. THE TREATMENT OF LUMBAR DISC-LESIONS By JAMES CYRIAX, M.D. Physician to the Department of Physical Medicine, St. Thomas's Hospital The discovery that the common cause of back- ache and sciatica is a disc-lesion has caught the medical profession largely unprepared. For centuries these symptoms had been considered a reason for instituting treatment by heat, massage and exercises. These methods have now lost their last shred of theoretical justification but are being replaced only very slowly by acceptable alterna- tives. Nevertheless, a number of simple measures exist, none a panacea, each with its due proportion of successes. Few patients cannot be relieved if conservative treatment is intelligently used, and it is for only a few of this remainder that surgery need be considered. Prophylaxis The direction in which a damaged disc tends to. move depends on the forces acting on it. During lordosis the inclination of the joint sur- faces (Fig. I) is such that the pressure of the body weight on the joint pushes the disc anteriorly. During kyphosis (Fig. 2) the tilt becomes reversed and the disc is pushed backwards. Hence it is only postures involving flexion that are apt to result in posterior displacement. The dura mater and the nerve roots lie posteriorly and are the sensitive structures that make the patient aware of disc-protrusion, the lumbar joints being in themselves all but insensitive. The important movement to avoid is stooping, especially when weight-lifting increases the compression force on the joint. Industrial medical officers should teach workers how to lift, using their knees rather than their backs (Fig. 3), should see to it that heavy objects are presented at a suitable height and .. .; '.' F · .1' ·jtf '7··, .·· ''.. . F I t;;!f': :r·;4i."' .P.1F ·! rlJ .·' ·, i :.C 5 ii ... t, ,, ,, ;." .. . ·:·. ::1. :r- .-·.. ;. .· r.··:··· .. t . 1.. ? · ·..5 i..r.:$:.C. I r It ·· r.-. :"' '. c 'f '" .·, .i·i?·rr !""l:r· ) 'd·' rE i:. I .·r 1 ;6·'.r·r 1. i ily.l :. I ·I /**; -t-· j. i : I I, 1 ·: i j··!·.:··! t; ?: I.... I ..i i. FIG. I.-Jomnt space in extension. Tracing of X-ray photograph of the fourth lumbar intervertebral joint in a normal subject, bending backwards. Note that the front of the joint space is i in. (I.2Z cm.) wide, but the back only 3/16 in. (0.5 cm.). In this position backward movement of the inter- vertebral disc is virtually impossible. copyright. on June 19, 2021 by guest. Protected by http://pmj.bmj.com/ Postgrad Med J: first published as 10.1136/pgmj.29.327.4 on 1 January 1953. Downloaded from

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript
-
4 POSTGRADUATE MEDICAL JOURNAL January I953
additional hazard after the disease has beenpresent for ten years.
It is a radical concept which would connect thepersonality disorder with the malignant change,but such speculation, though idle, is of interest.
K. GURLING.
REFERENCESx. RICE-OXLEY, J. M., and TRUELOVE, S. (I950), Lancet,
i, 663.2. ANDRESEN, A. F. R. (1942), Am. J. Digest. Dis., 9, 9I.3. MURRAY, C. D. (I930), J. Nerv. Ment. Dis., 72, 617.4. MURRAY, C. D. (I930), Am. J. Med. Sci., I80, 239.5. SULLIVAN, A. J. (I936), Am. J. Digest. Dis., 2, 65i.6. DANIELS, G. E. (x942), New England J. Med., 226, 178.
7. WITTKOWER, E. (1938), Brit. Med. J., ii, I356.8. GRACE, W. J., WOLF, S., and WOLFF, H. G. (195'),
'The Human Colon,' Heinneman, London.9. LIUM, R. (1939), Am. J. Med. Sci., 197, 841.
Io. LIUM, R. (1939), Arch. Int. Med., 63, 2I0.11. FLEMING, A. B. (1922), Proc. Royal Soc., S.B., 306.12. MEYER, K., and HAHNEL, E. (1946), J. biol. Chem., 163,
723.I3. SAMMONS, H. G. (I95I), Lancet, ii, 239.I4. PAULLEY, J. W. (1950), Gastroenterology, I6, 566.I5. HINTON, J. W., and SHARIHOFF, B. P., cited by Grace,
Wolf and Wolff (8).i6. MORTON-GILL, A. (1944), Lancet, i, 536.I7. KIRSNER, J. B., and PALMER, W. L. (I95i), J. Ant. MVed.
Ass., 147, 541.I8. HARDY, T. L., and BROOKE, B. (1952), 'Modern Trends
in Gastroenterology,' edited by F. Avery Jones; Butter-worth, London.
19. LAHEY, F. H. (I950), Rev..Gastroenterology, 17, 723.20. SLOAN, W. P., BARGEN, J. A., and CAGE, R. P., (I950)
Gastroenterology, I6, 25.
THE TREATMENT OF LUMBAR DISC-LESIONSBy JAMES CYRIAX, M.D.
Physician to the Department of Physical Medicine, St. Thomas's Hospital
The discovery that the common cause of back-ache and sciatica is a disc-lesion has caught themedical profession largely unprepared. Forcenturies these symptoms had been considered areason for instituting treatment by heat, massageand exercises. These methods have now lost theirlast shred of theoretical justification but are beingreplaced only very slowly by acceptable alterna-tives. Nevertheless, a number of simple measuresexist, none a panacea, each with its due proportionof successes. Few patients cannot be relieved ifconservative treatment is intelligently used, andit is for only a few of this remainder that surgeryneed be considered.
ProphylaxisThe direction in which a damaged disc tends
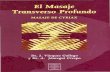
to. move depends on the forces acting on it.During lordosis the inclination of the joint sur-faces (Fig. I) is such that the pressure of thebody weight on the joint pushes the disc anteriorly.During kyphosis (Fig. 2) the tilt becomes reversedand the disc is pushed backwards. Hence it isonly postures involving flexion that are apt toresult in posterior displacement. The dura materand the nerve roots lie posteriorly and are thesensitive structures that make the patient awareof disc-protrusion, the lumbar joints being inthemselves all but insensitive. The importantmovement to avoid is stooping, especially when
weight-lifting increases the compression force onthe joint. Industrial medical officers should teachworkers how to lift, using their knees rather thantheir backs (Fig. 3), should see to it that heavyobjects are presented at a suitable height and
.. .; '.' F · .1' ·jtf'7··, .·· ''... F I
t;;!f'::r·;4i."'.P.1F·! rlJ.·'
·, i :.C 5ii... t, ,, ,,
;." ...·:·. ::1. :r- .-·.. ;. .· r.··:··· ..t . 1..? · ·..5 i..r.:$:.C. I rIt ·· r.-.:"' '. c'f '" .·, .i·i?·rr!""l:r·
)'d·' rE
i:.I.·r 1 ;6·'.r·r 1.i ily.l :. I·I /**; -t-·
j. i: I I, 1·:i j··!·.:··! t ;
?:I.... I ..i i.FIG. I.-Jomnt space in extension. Tracing of X-ray
photograph of the fourth lumbar intervertebraljoint in a normal subject, bending backwards.Note that the front of the joint space is i in.(I.2Z cm.) wide, but the back only 3/16 in. (0.5 cm.).In this position backward movement of the inter-vertebral disc is virtually impossible.
copyright. on June 19, 2021 by guest. P
rotected byhttp://pm
j.bmj.com
/P
ostgrad Med J: first published as 10.1136/pgm
j.29.327.4 on 1 January 1953. Dow
nloaded from
http://pmj.bmj.com/
-
January 1953 JAMES CYRIAX: The Treatment of Lumbar Disc-Lesions
I)'.P1.I.. ·4.. "':
-.--.; ;r·n··....*'.ii ".;- ,
.I·.t.· 'I,.1 · ··. : rC, ib.
: .··.C.fl.p. ··. :;
,,P(: i E.ci :1·O ii·..· 31·1 ''' 7'.·.·Y'$· :
···'' ' I·
:i. ''"' t·.·'- ··1;.·. :.. '*?4I:.;.rJC.3.FiP.?a'.·'
·i.1LLi9y ·r Ir 2··
i: ,
I .·.·....'·B·:··.
;··!''. '.···;.r.;·..l
FIG. 2.-Joint space in flexion. The same subject asin Fig. I bending forwards. The joint space isnow 5/I6 in. (o.8 cm.) wide behind, and i in.(o.6 cm.) in front.
attend to the design of chairs and car seats.Patients in bed should not be allowed to lie in' thenursing mother's position,' i.e. half-sitting withmany pillows behind the thorax and no supportfor the lumbar spine which droops into kyphosisall day. No wonder the posterior longitudinalligament finally stretches and the beginnings ofdisc-protrusion are laid down. The lithotomyposition and the flexion that some patients aremade to maintain during lumbar puncture areobvious offenders. Nurses require instruction onthese points and it should be explained to gymnastsgiving children postural training at school thatthe lordosis is not an unsightly curve requiringobliteration but the chief mechanical bar todisc-protrusion.Treatment
If something is out of place the most obviousapproach is to put it back again. This conceptgoverns the orthodox immediate treatment of mostfractures and of rupture with subluxation of themeniscus at the knee. When it comes to thespinal joints an extraordinary hiatus exists. Evenafter a doctor has arrived at a correct diagnosis heregards active measures to promote reduction as sounorthodox that he does not attempt them at all.This remarkable attitude has brought into being agroup of laymen-variously called bonesetters,osteopaths or chiropractors-who carry out to ourrecurrent discomfiture the simple spinal manipula-tions that we in general avoid. Lately we haveexplained away our neglect by dilating on thedangers of manipulating the spinal joints-to thegreat advantage of those laymen who, without
hi ii
rg
!Ul
III
FIG. 3.-A Canadian poster.
realizing it, have for years been reducing minorsubluxations of part of the intervertebral annulus.The first decision that has to be arrived at is
whether the displacement is likely or unlikely tobe reducible by manipulation. The reason for thetwo different responses to manipulation isanatomical. Displacements of the annulus (Fig.4) consist of hard material that moves' under thestresses of manipulation; protrusions of thenucleus 'usually do not for they have the con-sistency of wet sand (Fig. 5). Burns and Young(I945), analyzing cases coming to laminectomy,found that the primary lesion in 56 per cent. oftheir cases to be cartilaginous, and in 44 per cent.to be pulpy with an intact annulus. My impressionis that in patients not requiring laminectomy theproportion is more like one nuclear protrusion totwo annular. Thus the first major decision-whether or not manipulation should be attempted-rests on an evaluation of the symptoms 'andsigns differentiating a nuclear from an annularprotrusion. These are set.out overleaf.
Differentiation of Cartilaginous from PulpyProtrusionsHistory
This is often indicative. For example, a patient
copyright. on June 19, 2021 by guest. P
rotected byhttp://pm
j.bmj.com
/P
ostgrad Med J: first published as 10.1136/pgm
j.29.327.4 on 1 January 1953. Dow
nloaded from
http://pmj.bmj.com/
-
6 POSTGRADUATE MEDICAL JOURNAL January 1953nucleus pulposus
K annulus fibrosus
nerve roo.
d;dura matrs rl-or
longi'udinalW lijamenr
FIG. 4.-Cartilaginous protrusion causing lumbago. The annulusis cracked and hinged. Reduction by manipulation shouldbe simple.
bends forwards and feels some aching in his backwhich gets worse later in the day. Next morninghe finds himself unable to get out of bed becauseof severe lumbago. This history indicates a pro-trusion that has gradually increased in size--thatis, one-consisting of nuclear material. By contrast,the patient who is subject to attacks initiated by aclick in the back followe by agonizing lumbar painfixing him in flexion has clearly suffered an abruptcartilaginous displacement. Pulpy protrusions areuncommon in the elderly, hence manipulative re-duction should always be attempted for displace-ments, whether causing backache, gluteal pain orsciatica in patients over 6o years old.
Primary postero-lateral protrusions causingsciatica are irreducible by manipulation. This isindicated when a patient with a low lumbar disc-lesion states that his pain began in the calf or thighand does not reach the back. Naturally a centraldisplacement impinges first against the dura mater,causing backache before it sets up sciatica;primary postero-lateral protrusions never touchthe dura at all, hence premonitory backache isabsent,
Another type of history' characterizes the self-reducing pulpy disc-lesion; in such a casemanipulation is waste of time, achieving no morethan the patient achieves for himself by avoidingcompression. The patient wakes comfortable andas the'day goes on backache appears and becomesslowly more severe, especially if he stoops or lifts.A night's rest once more abolishes the pain;Naturallyj if the posterior bulge at the joint re-cedes spontaneously as soon as the stress on thejoint ends, only to recur when the joint is made tobear weight again, the reduction brought about bymanipulation is equally unstable and ephemeral.
Manipulation carried out at a time when no dis-placement is present is, of course, quite pointless.A similar history characterizes what I have
named the 'mushroom phenomenon' (Cyriax,1950). In an elderly patient, backache soon fol-lowed by bilateral sciatica comes on after about Iominutes' walking or standing and is abolished assoon as he rests. It is often mistaken for inter-mittent claudication. X-ray examination showsthat the joint space at, usually, the fifth lumbarlevel has disappeared, the disc substance beingdisplaced forwards and lying as a round ball be-tween two large osteophytes. Since nothingsensitive is touched, anterior protrusion proceedssilently, causing no symptoms until the disc hasbeen ground to pieces and the compression ofweight-bearing causes capsular bulging all the wayround the joint. The posterior component thenirritates both the dura mater and the nerve roots.This lesion does not respond to manipulation.A complaint of weakness of the bladder, saddle
anaesthesia, paraesthesiae in the scrotum or numb-ness of the labium shows that the fourth sacralroot is squeezed and provides an absolute contra-indication to manipulation. The significance ofreferred rectal, penile, or coccygeal pain is lessclear, but may also indicate a protrusion im-perilling the fourth sacral root. Since the im-portant danger of manipulation in an unsuitablecase is lasting urinary incontinence, I regard thistype of referred pain as contraindicating manipula-tion. Not having attempted it in such a case Inaturally cannot be sure to what extent thisapparent danger is real.SignsOf the physical signs the appearance of the
copyright. on June 19, 2021 by guest. P
rotected byhttp://pm
j.bmj.com
/P
ostgrad Med J: first published as 10.1136/pgm
j.29.327.4 on 1 January 1953. Dow
nloaded from
http://pmj.bmj.com/
-
January I953 JAMES CYRIAX: The Treatment of Lumbar Disc-Lesions 7
protrusion- dur& moar
verftbral body %r roo
neerve root
*IF (
FIG. 5.-Pulpy protrusion causing lumbago. The nucleus hasprotruded backwards, the annulus remaining intact (afterR. H. Young). Manipulation is unlikely to succeed; sus-tained traction or recumbency is effective.
patient's back is the most informative. Lateraldeformity of the lumbar spine when he is viewedstanding still, or apparent when he bends forwards,indicates a protrusion that has reached a size thatvisibly interferes with joint movement. Con-siderable lateral deviation therefore indicatesirreducibility. I have also found that reductionby manipulation is difficult, at times impossible, inpatients whose lumbar movements (other thanflexion) hurt in the thigh instead of the back orin whom the most painful movement is side-flexion towards the painful side.Marked neurological signs should be taken as
an indication of irreducibility, whether the lesionwas originally of cartilage or pulp. Displacementof a fragment of annulus may later be followed byextrusion of nuclear material along the line of thefracture. This leads to severe compression of thenerve root and proportionate interference withconduction. Thus weakness of more than onemuscle in the leg, combined with, say, loss ofankle jerk, cutaneous analgesia or much glutealwasting shows that this secondary effect hassupervened.A disc-lesion at the unstable joint resulting from
spondylolisthesis is treated in the same way as anordinary disc-lesion.
ManipulationThis is the treatment of choice; for it can be
immediately effective. It is carried out in allsuitable cases as soon as the diagnosis of anannular displacement is made.
General AnaesthesiaThis must be avoided, since it deprives the
manipulator of the patient's co-operation, so vitalto effective work. One manoeuvre is tried, where-upon the patient stands and by repeating the move-
ments previously found painful assesses the resulon his symptoms; the manipulator watches theeffect on his range of straight-leg raising, postureand lumbar mobility. If this manipulation hasdone good, it is repeated until no further benefitaccrues. The next is then performed and theresult noted again. In this way the manipulatorsees what results he is achieving and knows whatto do next, when to go on and when to stop.Anaesthesia denies him all this essential knowledgewith the result that it is not difficult to make thepatient, at least temporarily, worse. It is myexperience, too, that the muscular relaxation in-duced by general anaesthesia is not of muchadvantage, for displacements previously reducedunder anaesthesia have proved equally easy toreduce without, and failure without anaesthesialeads to failure with anaesthesia. It is not themanipulator or the patient's relaxation that is atfault but the type of protrusion. If it is large andpulpy no amount of manipulation has any chanceof success.
TechniqueThe patient lies prone on a firm couch 15 in.
(38 cm.) high and various manual pressures areapplied at the appropriate lumbar level. If thesefail, rotation strains should be tried. Thesemethods have been described and illustrated(Cyriax, 1950). This treatment may require twoor three repetitions and an adequate session maylast half an hour, hence it is my practice to delegatemuch of this work to physiotherapists trained-as all our students are-in these methods. Not alldoctors have time, inclination or a suitable couchfor carrying out such manoeuvres themselves;moreover these have in practice been found suitedto delegation.
C
copyright. on June 19, 2021 by guest. P
rotected byhttp://pm
j.bmj.com
/P
ostgrad Med J: first published as 10.1136/pgm
j.29.327.4 on 1 January 1953. Dow
nloaded from
http://pmj.bmj.com/
-
8 POSTGRADUATE MEDICAL JOURNAL yanuary I953
Sustained TractionBy this means a patient can, as it were, be put
to bed for several weeks in the course of a fewhours. Most pulpy protrusions should be treatedby immediate traction, carried out daily until re-duction is complete. They ooze out and are bythis means squeezed back into place again. Trac-tion has two effects: (i) Distraction of the vertebralbodies (Fig. 6). (2) Tautening of the posteriorcommon ligament which exerts contripetal force onthe nuclear protrusion and slowly pushes it back.The increased distance apart of the vertebralbodies not only enlarges the space into which theprotrusion can now return but creates suction.The couch is made of steel and has a pillar with
a hook on it at each end. One hook canr bemade to travel distally by rotating a wheel. Forpulpy lumbar herniations a band is applied roundthe patient's lower thorax and fixed to the upperhook, another about his pelvis passes to the lowerhook. Between ioo and zoo lb. traction is appliedfor half to one hour-as long as the patient cancomfortably stand it. In an emergency up to sixhours' continuous traction can be borne. Thephysiotherapist stays with the patient and adjuststhe tension, measured on a spring balance, asrequired. This balance is important, not only toenable accurate treatments to be given but it takesup slack should the belt slip slightly and preventsall traction being temporarily lost.
Contra-indicationsCartilaginous displacements should be manipu-
lated back into place. Elderly patients or thosewho have had thoracic operations may find thatthe band round the chest embarrasses respiration.Acute lumbago with twinges is unaffected or madeworse. A patient with sciatica due to a pulpyprotrusion of several months' standing is often inslight pain only, though the signs are marked.Traction may effect reduction, but a protrusionreduced may move again. By contrast if spon-taneous cure is awaited, though it often takes ayear from the onset of root pain, the tendency torecurrence is very slight. Hence there comes atime in the evolution of a pulpy protrusion when itis better policy to avoid even effective treatmentfor the sake of the long-term result.
Epidural Local AnaesthesiaThe injection for epidural analgesia is regarded
as difficult and dangerous by some authorities.During the last I2 years I have used this methodon unprepared out-patients more than Io,oootimes without ill effect, and have found it im-possible to introduce the needle properly in lessthan I per cent. of all cases. The patient can walk
*.X.:.
i:.· :.. ;·
FIG. 6.-Two radiographs have been superimposed, thesacra coinciding. One was taken before, the otherduring, traction.
home about half an hour after the injection isgiven. There are five main indications:
I. In acute lumbago the cause of the pain is acentral posterior protrusion impinging on the duramater (Cyriax, I945). If this membrane isanaesthetized by 50 ml. of o.5 per cent. procaine,introduced extrathecally via the sacral canal, theprotrusion presses on a membrane no longersensitive and all pain ceases for the duration of theanalgesia-that is, one to two hours. During thistime a patient can move freely, perform someessential work, or go home to bed. He can withadvantage lie on the couch for an hour in hyper-extension, thus initiating reduction. If this isdone he usually experiences a large measure oflasting relief.
2. Persistent lumbar or sciatic aching after re-duction of a prolapsed disc may prove trouble-some; it is apparently due to persistent localbruising of the dura mater. One or two epiduralinjections usually suffice to stop it.
3. Chronic backache, especially if it is moresevere at night than by day, associated with onlyslight articular signs at the lumbar spine can oftenbe lastingly abolished by one injection of epidurallocal analgesia.
copyright. on June 19, 2021 by guest. P
rotected byhttp://pm
j.bmj.com
/P
ostgrad Med J: first published as 10.1136/pgm
j.29.327.4 on 1 January 1953. Dow
nloaded from
http://pmj.bmj.com/
-
January 1953 JAMES CYRIAX: The Treatment of Lumbar Disc-Lesions 9
4. If a patient in whom spontaneous recoveryfrom sciatica is being awaited continues too longto suffer marked limitation of straight-leg raising,the nerve root can be painlessly mobilized by fullstraight-leg raising after the induction of anepidural block.
5. This is the treatment of choice in referredcoccygodynia.
Prolonged AnalgesiaThis is indicated in large irreducible protrusions
especially at the fourth lumbar level. The patientoften suffers little pain but has a gross lateraldeviation of the lumbar spine which may havepersisted unaltered for weeks or months.He lies supine in bed in his position of ease.
He is kept fully relaxed for four hours by a con-tinuous intravenous infusion of procaine solution.At the end of the third hour his position in bed isaltered to the reverse of that obtaining previously,so that the lumbar spine is held in lateral deviationin the opposite direction. Prolonged muscularrelaxation often results in reduction.
Rest in BedThis is the old-fashioned treatment for lumbago
and sciatica. It acts by avoiding the compressionof standing; the vertebral bodies finally move apartand reduction ensues. It is a most successfultreatment, but very slow. It is apt to fail only inthe elderly whose lumbar joints are so stiff as theresult of capsular contracture that they cannotmove adequately. In such patients a fragment ofannulus that weeks in bed have failed to shift canoften be reduced easily by manipulation.
Rest in bed is an admission of defeat and oftentakes weeks or months to become effective. It is,therefore, to be avoided as far as possible. If thereis nothing else for it, the patient must lie flat on afirm mattress, with a small pillow or a hot-waterbottle maintaining his lordosis. He must not getout of bed nor sit up or the relief from compressionat the joint is nullified. No sort of physiotherapyis called for and all exercises, even towards ex-tension lying prone, are contra-indicated, forcontraction of the sacrospinalis muscle squeezesthe joints together and extends the joints onlywhen this play has been taken up.
Awaiting Spontaneous CureBackache shows little tendency to spontaneous
cure; it may last, or recur, during a patient'swhole lifetime. Sciatica, however, nearly alwaysgets well of itself in about I2 months. The twoexceptions are: (a) after an unsuccesful laminec-tomy this does not happen and sciatica may thenpersist for years; and (b) after the age of 6o
spontaneous cure with the lapse of time isimprobable.Young patients with sciatica are often seen who
show clear signs of a nuclear protrusion at a lowerlumbar level of some months' standing. Thesymptoms amount to only an ache, the patientlooks cheerful and sleeps well. Examinationstanding shows a symmetrical lumbar spine withsome lateral deviation on attempted flexion.Straight-leg raising is 45° to 60° limited andslightly impaired conduction is noted, e.g. asluggish ankle-jerk and some weakness of theextensor hallucis muscle. As already mentioned,awaiting spontaneous recovery has a more per-manent result than such treatments as bring aboutreduction, for the protrusion becomes fixed in anew position from which it cannot becomedislodged.The tendency to lumbago often ceases spon-
taneously between the ages of 50 and 6o. As ageadvances the spinal joints stiffen and osteophytes,both cupping the disc and limiting articular move-ment, make their welcome appearance. Osteo-phyte formation at the lumbar spine is not apainful condition, on the contrary it is beneficial.It is the mechanism that prevents backache afteryears of wear and tear have damaged the disc.
LaminectomyThis is to be avoided as far as possible, but
operation should not be unreasonably withheld.In the best hands the results are not alwaysperfect; immediate cure may not be secured andeventual recurrence is regrettably frequent evenin patients who never go back to heavy work. Theintroduction of sustained traction in I950 reducedmy laminectomy rate for all disc-lesions fromI :40 to I :200. The five main indications are;
I. Gross lumbar deformity. A young patientshould not be left to recover spontaneously fromsciatica or, less often, backache causing markedpersistent lumbar deformity. Though he mayrecover as regards pain, the deformity remainspermanent.
2. Incipient drop foot. A patient who developsincreasingly pronounced weakness of the dorsi-flexor muscles of the foot must be warned so thathe must choose between laminectomy and thepossibility of a permanently weak foot. In suchcases pressure atrophy, doubtless from localischaemia, may result in complete insensitivity ofthe sheath of the affected nerve root. As a result,pain quickly ceases and straight-leg raising soonreaches full range at the same time as the palsybecomes complete. The patient, chiefly concernedwith his pain, is apt mistakenly to suppose that heis getting better, an error that the physician shares
copyright. on June 19, 2021 by guest. P
rotected byhttp://pm
j.bmj.com
/P
ostgrad Med J: first published as 10.1136/pgm
j.29.327.4 on 1 January 1953. Dow
nloaded from
http://pmj.bmj.com/
-
'POSTGRADUATE MEDICAL JOURNAL Yanuary I953
unless he examines again the power of the musclescontrolling the foot.
3. Intractable severe pain. Irreducible disc-lesions are caused by complete erosion of theposterior ligament with extrusion of part of theannulus into the neural canal. More rarely theend-plate becomes detached and buckles over onitself. No amount of conservative treatment canthen avail.The important point in such cases is to make
sure that the allegations of pain are borne out bythe physical signs. Patients with hysteria welcomeany operation the criterion of whose success restsalmost entirely on the patient's own statements.
4. Fourth sacral palsy. Weakness of thebladder, saddle anaesthesia, paraesthesiae inscrotum or labium call for immediate laminectomy.
5. Adherent root. If the symptoms warrant-they usually do not-the adhesions can be dividedat laminectomy.Arthrodesis
Arthrodesis is the operation of choice inspondylolisthesis causing sufficient local capsularpain or setting up traction on the relevant lumbarnerve roots with consequent bilateral sciatica. Itis the only effective treatment for anterior pro-trusion of the whole disc (mushroom phenomenon),and is well worth carrying out in patients under6o. It is also indicated in recurrence afterlaminectomy if conservative measures fail. Fre-quent crippling attacks of lumbago or sciaticaquickly recovering present a difficult problem.Laminectomy cures less than half of all suchcases. Arthrodr:sis is therefore to be preferred.Maintenance of ReductionExplanationThe mechanics of lumbar disc-protrusion must
be explained to the patient so that he understandswhy it is essential that he should maintain hislordosis at all times. The physiotherapist showshim how to stand, sit, lift and how to use hisknees instead of his lumbar joints for getting hishands close to the floor. Neurosis is prevented byemphasizing the purely mechanical nature of hisdisorder-the analogy with the knee is useful--and that it is not the precursor of arthritis likelyto spread to other parts of the body. It is not somuch that he cannot do this or that, he must doit in a different way. All exercises, especiallytowards trunk flexion, must be avoided. Theymaintain mobility and thus enable the movement
to take place that results in internal derangement.Active prone-lying trunk extension exercises areless harmful than the others, but are best avoidedsince the contraction of the sacrospinalis musclescompresses the joint. Press-ups, where by thetrunk is passively extended, are free from thisdefect.
SupportA Plaster Jacket
This is a method in great vogue at the moment,but I believe it is seldom worth the discomfort itentails. It is usually wrongly prescribed in thehope of achieving reduction rather than main-taining it. One untenable reason for immobiliza-tion in plaster has been expressed (Crisp, 1948)that rest in plaster allows the broken cartilage tounite. Intra-articular cartilage has no bloodsupply; therefore it cannot heal at a spinal jointany more than at the knee joint. Immobilizationachieves a spurious popularity when a patient, forwhom the proper treatment is to await spontaneouscure, is put in plaster until he is well. He does notknow that he would have recovered just as quicklywithout the added discomfort of the plaster jacket.A Perforated Plastic Jacket
This weighs a fifth as much as a plaster jacketand achieves a much greater degree of immobiliza-tion; for it can be tightened at will to any degree.It can be made in two days on a plaster cast takenfrom the patient. Hence it supersedes a plasterjacket from every point of view.A CorsetWhereas a plaster jacket cannot be worn for
longer than some months and thus cannot providelasting protection against recurrence, corsets, re-newed each year or two, can be worn indefinitely,thus affording permanent security. If the twosteels are accurately moulded to the lumbar curve,lordosis is maintained and the joints steadied.Moreover, if the patient bends too far forwards orsags as he sits, the front of the corset pressesunpleasantly against his lower ribs-a salutaryreminder.
BIBLIOGRAPHYBURNS, B. H., and YOUNG, R. H. (1945), ' Protrusion of Intra-
vertebral Disc,' Lancet, ii, 424.CRISP, E. J. (1948), 'Conservative Treatment of Lumbar Disc
Lesions,' Proc. Roy. Soc. Med., 26I.CYRIAX, J. (1945), ' Lumbago,' Lancet, ii, 426.CYRIAX, J. (1950),' Lumbar Disc Lesions,' Brit. med. j., ii, I434.CYRIAX, J. (i95o), 'Orthopaedic Medicine,' Vol. II, Cassell,
London.
copyright. on June 19, 2021 by guest. P
rotected byhttp://pm
j.bmj.com
/P
ostgrad Med J: first published as 10.1136/pgm
j.29.327.4 on 1 January 1953. Dow
nloaded from
http://pmj.bmj.com/
Related Documents







![[James H. Cyriax MD MRCP, P. J. Cyriax MCSP] Cyri(BookFi.org)](https://static.cupdf.com/doc/110x72/577cdc4d1a28ab9e78aa4571/james-h-cyriax-md-mrcp-p-j-cyriax-mcsp-cyribookfiorg.jpg)


