Turkish Neurosurgery 12: 50 - 54, 2002 Mirzai: Trnllllwtic Optic Neuropathy Blunt Caused by Report Neuropathy Trauma: Case Traumatic Optic Forehead Kiint Kafa Travmasini Takiben Travmatik Optik Noropati: Olgu Sunumu HASAN MiRZA!, EsiN FATMA ERKiN, CUMHUR TOSUN Celal Bayar University, Departments of Neurosurgery (HM, CT) and Ophthalmology (EFE), Manisa, Turkey Received: 01.11.2000 ¢::> Accepted: 25.11.2000 Abstract: A 28-year-old man sustained blunt forehead trauma in a traffic accident. He had a right orbital roof fracture and there was loss of vision in the right eye. At presentation, the visual acuity in the injured eye was light perception without projection, and there was a right afferent pupillary defect. There were no abnormalities on ophthalmoscopic examination. Computed tomography and magnetic resonance imaging demonstrated a fracture of the right orbital roof and showed that the optic nerve was intact. The patient was diagnosed with traumatic optic neuropathy, and was started on 1000 mg methylprednisolone therapy 18 hours after the trauma occurred. The vision in the traumatized eye improved to the level of 2/10 at 3 weeks after therapy, and remained at this level thereafter. Traumatic optic neuropathy associated with blunt forehead trauma and the various treatment strategies for this condition are discussed. Ozet: 28 ya~lllda erkek olgu trafik kazasl11da kiint kafa travmasma maruz kaldl. Sag gbzde gbrme kayblyla beraber sag orbita tavan frakturu yard!. 11k gbrme keskinligi projeksiyon olmakslZln l~lk hissi diizeyindeydi ve sag afferent pupil defekti mevcuttu. Oftalmoskobik muayene normaldi. Komputerize tomografi ve manyetik rezonans gbruntuleme sag orbita tavan fraktiirii oldugunu optik sinirin intakt oldugunu gbsterdi. Olguya travmatik optik nbropati te~hisi konuldu ve travmadan 18 saat soma 1000 mg metilprednizolon tedavisi ba~landl. Gorme keskinligi tedaviden sonraki 3. haftada 2/10 duzeyine ula~t1 ve bundan sonra stabil seyretti. Kiint aIm bolgesi travmaSl ile ili~kili travmatik optik noropati ve tedavi stratejileri tart1~lldl. Key words: blunt trauma, corticosteroid therapy, orbital fracture, traumatic optic neuropathy Anahtar kelimeler: Kunt travma, kortikosteroid tedavisi, orbita frakttiri.i, travmatik optik noropati INTRODUCTION Traumatic optic neuropathy is an uncommon but often devastating cause of permanent visual loss after blunt or penetrating injury. The most frequent form is indirect damage caused by a concussive blow to the head, especially to the forehead (11). Indirect traumatic optic neuropathy is defined as visual loss without clinical evidence of injury to the eye or optic nerve (15). The majority of victims are young males, and bicycle and motor vehicle accidents are the most common causes of damage (9,11,15). This case report 50

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript
Turkish Neurosurgery 12: 50 - 54, 2002 Mirzai: Trnllllwtic Optic Neuropathy
BluntCaused byReport
NeuropathyTrauma: Case
Traumatic OpticForehead
Kiint Kafa Travmasini Takiben Travmatik Optik Noropati: Olgu Sunumu
HASAN MiRZA!, EsiN FATMA ERKiN, CUMHUR TOSUN
Celal Bayar University, Departments of Neurosurgery (HM, CT) and Ophthalmology (EFE), Manisa, Turkey
Received: 01.11.2000 ¢::> Accepted: 25.11.2000
Abstract: A 28-year-old man sustained blunt foreheadtrauma in a traffic accident. He had a right orbital rooffracture and there was loss of vision in the right eye. Atpresentation, the visual acuity in the injured eye was lightperception without projection, and there was a rightafferent pupillary defect. There were no abnormalities onophthalmoscopic examination. Computed tomographyand magnetic resonance imaging demonstrated a fractureof the right orbital roof and showed that the optic nervewas intact. The patient was diagnosed with traumatic opticneuropathy, and was started on 1000 mgmethylprednisolone therapy 18 hours after the traumaoccurred. The vision in the traumatized eye improved tothe level of 2/10 at 3 weeks after therapy, and remained atthis level thereafter. Traumatic optic neuropathy associatedwith blunt forehead trauma and the various treatment
strategies for this condition are discussed.
Ozet: 28 ya~lllda erkek olgu trafik kazasl11da kiint kafatravmasma maruz kaldl. Sag gbzde gbrme kayblylaberaber sag orbita tavan frakturu yard!. 11k gbrmekeskinligi projeksiyon olmakslZln l~lk hissi diizeyindeydive sag afferent pupil defekti mevcuttu. Oftalmoskobikmuayene normaldi. Komputerize tomografi ve manyetikrezonans gbruntuleme sag orbita tavan fraktiiriioldugunu optik sinirin intakt oldugunu gbsterdi. Olguyatravmatik optik nbropati te~hisi konuldu ve travmadan18 saat soma 1000 mg metilprednizolon tedavisi ba~landl.Gorme keskinligi tedaviden sonraki 3. haftada 2/10duzeyine ula~t1 ve bundan sonra stabil seyretti. Kiint aImbolgesi travmaSl ile ili~kili travmatik optik noropati vetedavi stratejileri tart1~lldl.
Key words: blunt trauma, corticosteroid therapy, orbitalfracture, traumatic optic neuropathy
Anahtar kelimeler: Kunt travma, kortikosteroid tedavisi,orbita frakttiri.i, travmatik optik noropati
INTRODUCTION
Traumatic optic neuropathy is an uncommonbut often devastating cause of permanent visual lossafter blunt or penetrating injury. The most frequentform is indirect damage caused by a concussive blow
to the head, especially to the forehead (11). Indirecttraumatic optic neuropathy is defined as visual losswithout clinical evidence of injury to the eye or opticnerve (15). The majority of victims are young males,and bicycle and motor vehicle accidents are the mostcommon causes of damage (9,11,15).This case report
50
Turkish Neurosurgery 12: 50 - 54, 2001
discusses unilateral traumatic optic neuropathyassociated with forehead trauma.
CASE REPORT
A 28-year-old male sustained blunt foreheadtrauma in a traffic accident. He was admitted to our
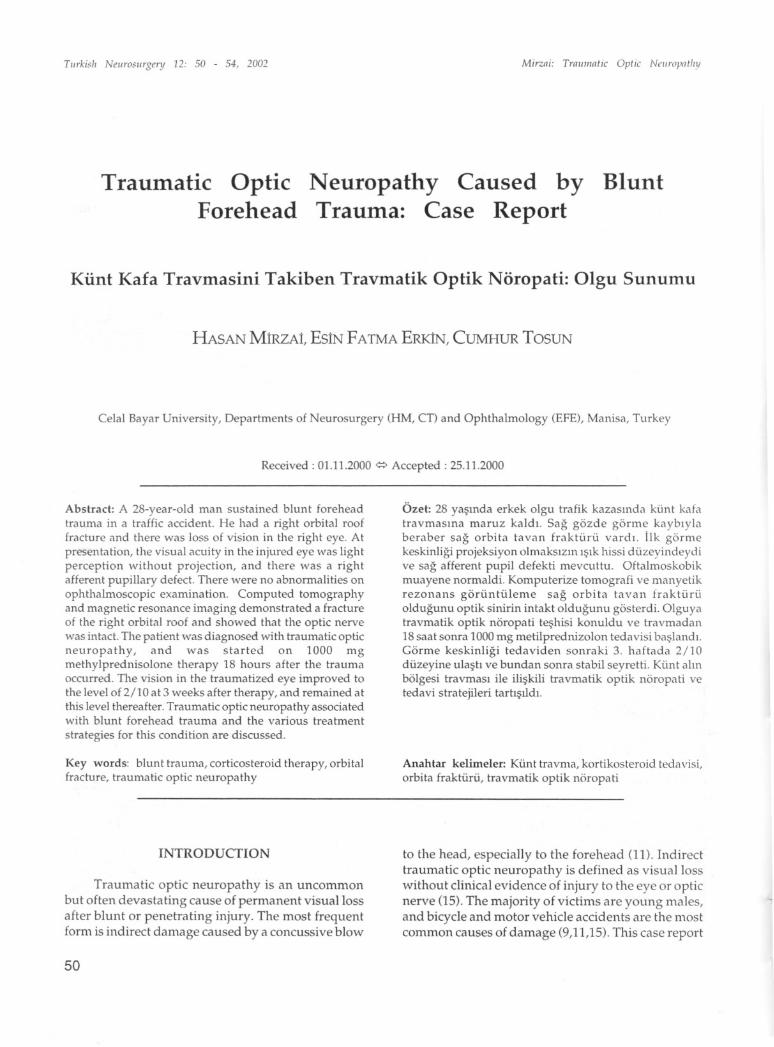
hospital several hours after the injury. Physical andneurological examinations revealed that the patientwas alert and had a Glasgow coma scale score of 15.His cranial nerve examination was unremarkable,apart from absence of the direct pupillary light reflexin the right eye, and of the indirect pupillary lightreflex in the left eye. Cranial and orbital computedtomography showed no significant cerebralpathology, but demonstrated a fracture of the roofof the right orbit and pneumoorbita. Also, the opticcanal was confirmed intact and no retrobulbar
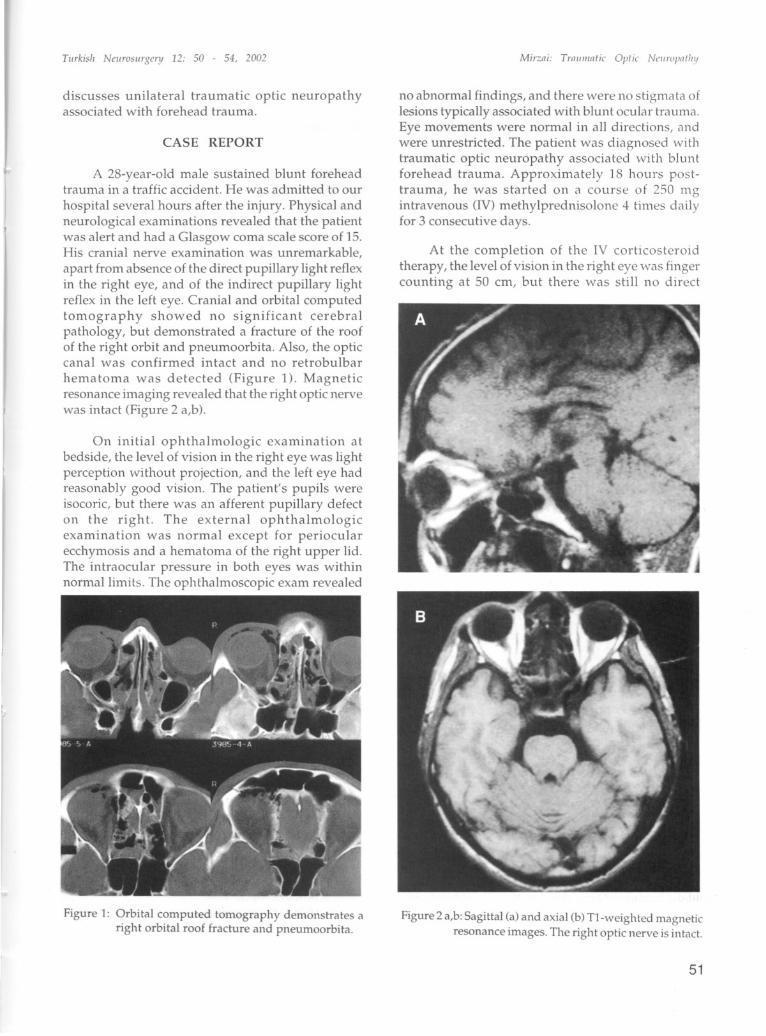
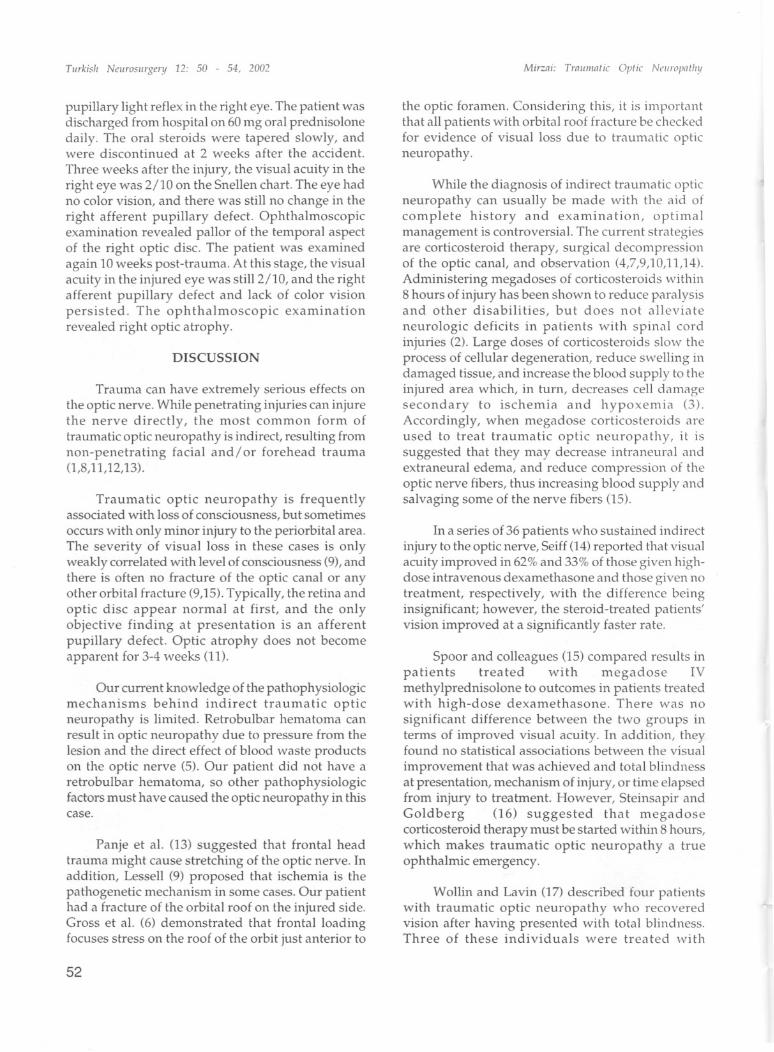
hematoma was detected (Figure 1). Magneticresonance imaging revealed that the right optic nervewas intact (Figure 2 a,b).
On initial ophthalmologic examination atbedside, the level of vision in the right eye was lightperception without projection, and the left eye hadreasonably good vision. The patient's pupils wereisocoric, but there was an afferent pupillary defecton the right. The external ophthalmologicexamination was normal except for periocularecchymosis and a hematoma of the right upper lid.The intraocular pressure in both eyes was withinnormal limits. The ophthalmoscopic exam revealed
Figure 1: Orbital computed tomography demonstrates aright orbital roof fracture and pneumoorbita.
Mir=ai: Traul/latic Optic Neuropathy
no abnormal findings, and there were no stigmata oflesions typically associated with blunt ocular trauma.Eye movements were normal in all directions, andwere unrestricted. The patient was diagnosed withtraumatic optic neuropathy associated with bluntforehead trauma. Approximately 18 hours posttrauma, he was started on a course of 250 mgintravenous (IV) methylprednisolone 4 times dailyfor 3 consecutive days.
At the completion of the IV corticosteroidtherapy, the level of vision in the right eye was fingercounting at 50 cm, but there was still no direct
Figure 2 a,b: Sagittal (a) and axial (b) Tl-weighted magneticresonance images. The right optic nerve is intact.
51
Turkish NeIlraslIrgery 12: 50 - 54, 2002
pupillary light reflex in the right eye. The patient wasdischarged from hospital on 60 mg oral prednisolonedaily. The oral steroids were tapered slowly, andwere discontinued at 2 weeks after the accident.Three weeks after the injury, the visual acuity in theright eye was 2/10 on the Snellen chart. The eye hadno color vision, and there was still no change in theright afferent pupillary defect. Ophthalmoscopicexamination revealed pallor of the temporal aspectof the right optic disc. The patient was examinedagain 10 weeks post-trauma. At this stage, the visualacuity in the injured eye was still 2/10, and the rightafferent pupillary defect and lack of color visionpersisted. The ophthalmoscopic examinationrevealed right optic atrophy.
DISCUSSION
Trauma can have extremely serious effects onthe optic nerve. While penetrating injuries can injurethe nerve directly, the most common form oftraumatic optic neuropathy is indirect, resulting fromnon-penetrating facial and / or forehead trauma0,8,11,12,13).
Traumatic optic neuropathy is frequentlyassociated with loss of consciousness, but sometimesoccurs with only minor injury to the periorbital area.The severity of visual loss in these cases is onlyweakly correlated with level of consciousness (9), andthere is often no fracture of the optic canal or anyother orbital fracture (9,15). Typically, the retina andoptic disc appear normal at first, and the onlyobjective finding at presentation is an afferentpupillary defect. Optic atrophy does not becomeapparent for 3-4 weeks (1).
Our current knowledge of the pathophysiologicmechanisms behind indirect traumatic opticneuropathy is limited. Retrobulbar hematoma canresult in optic neuropathy due to pressure from thelesion and the direct effect of blood waste productson the optic nerve (5). Our patient did not have aretrobulbar hematoma, so other pathophysiologicfactors must have caused the optic neuropathy in thiscase.
Panje et a!. (13) suggested that frontal headtrauma might cause stretching of the optic nerve. Inaddition, Lessell (9) proposed that ischemia is thepathogenetic mechanism in some cases. Our patienthad a fracture of the orbital roof on the injured side.Gross et a!. (6) demonstrated that frontal loadingfocuses stress on the roof of the orbit just anterior to
52
Mirzai: Trall/lliltic Optic Nellropathy
the optic foramen. Considering this, it is importantthat all patients with orbital roof fracture be checkedfor evidence of visual loss due to traumatic opticneuropathy.
While the diagnosis of indirect traumatic opticneuropathy can usually be made with the aid ofcomplete history and examination, optimalmanagement is controversial. The current strategiesare corticosteroid therapy, surgical decompressionof the optic canal, and observation (4,7,9,10,11,14).Administering megadoses of corticosteroids within8 hours of injury has been shown to reduce paralysisand other disabilities, but does not alleviateneurologic deficits in patients with spinal cordinjuries (2). Large doses of corticosteroids slow theprocess of cellular degeneration, reduce s\velling indamaged tissue, and increase the blood supply to theinjured area which, in turn, decreases cell damagesecondary to ischemia and hypoxemia (3).Accordingly, when megadose corticosteroids areused to treat traumatic optic neuropathy, it issuggested that they may decrease intraneural andextraneural edema, and reduce compression of theoptic nerve fibers, thus increasing blood supply andsalvaging some of the nerve fibers OS).
In a series of 36 patients who sustained indirectinjury to the optic nerve, Seiff (4) reported that visualacuity improved in 62% and 33% of those given highdose intravenous dexamethasone and those given notreatment, respectively, with the difference beinginsignificant; however, the steroid-treated patients'vision improved at a significantly faster rate.
Spoor and colleagues OS) compared results inpatients treated with megadose IVmethylprednisolone to outcomes in patients treatedwith high-dose dexamethasone. There was nosignificant difference between the two groups interms of improved visual acuity. In addition, theyfound no statistical associations between the visualimprovement that was achieved and total blindnessat presentation, mechanism of injury, or time elapsedfrom injury to treatment. However, Steinsapir andGoldberg (16) suggested that megadosecorticosteroid therapy must be started within 8 hours,which makes traumatic optic neuropathy a trueophthalmic emergency.
Wollin and Lavin (7) described four patientswith traumatic optic neuropathy who recoveredvision after having presented with total blindness.Three of these individuals were treated with

TlIrkish NellroslIrgery 12: 50 - 54, 2002
corticosteroids, and one improved spontaneously.The authors emphasized that even total blindnessdoes not rule out recovery of vision, and thattreatment should always be attempted (15).
Since the intracanalicular segment of the opticnerve is a common site of injury, surgicaldecompression of the optic canal may be a reasonabletreatment option (9). This can be accomplished byeither the transcranial or extracranial (transethmoidaland transsphenoidal) route. Joseph et a1.(7) reportedthat optic canal decompression through externalethmoidectomy combined with perioperativedexamethasone treatment yielded favorable resultsin 11 of 14 patients, including 3 of 5 who had no lightperception initially. Similarly, Levin and coauthors(0) reported favorable results in patients withindirect traumatic optic neuropathy who weretreated with transethmoidal decompression of theoptic canal in addition to perioperative steroids. Sincethe time elapsed from injury to surgery, initial visualacuity, and presence of an optic canal fracture didnot influence outcome, they recommended thattreatment be considered in patients with no lightperception, and in cases where there is a delaybetween injury and treatment. Mine et al. (2)compared the outcomes for 34 patients with indirectoptic neuropathy who were managed with andwithout surgical decompression. In the cases whereinitial visual acuity was hand movement or better,they found that vision improvement was significantlygreater when surgery was performed.
Cook and co-workers (4) performed metaanalysis on a large group of published cases oftraumatic optic neuropathy. They noted that recoveryof vision was significantly better in treated patientsthan in non-treated individuals. There was nosignificant difference in improvement amongpatients treated with corticosteroids alone, thosetreated with combined surgical decompression andcorticosteroids, and those treated with surgicaldecompression alone. The results also showed thatdegree of recovery was highly dependent on theseverity of initial injury. Further, they noted betterrecovery in cases where there was no orbital fracturethan in cases with these fractures, and better recoveryin cases where the fracture was anterior as opposedto posterior.
The International Optic Nerve Trauma Studyis a recently published comprehensive prospectivestudy on traumatic optic neuropathy. Thisinvestigation compared visual outcomes in 133
Mirzai: Trallmatic Optic Nmropalhy
traumatic optic neuropathy cases that were treatedwith either corticosteroids or optic canaldecompression surgery, or observed withouttreatment (11). The findings revealed no significantdifferences in outcome among the three groups. Theauthors also reported that dosage of corticosteroidtherapy, the timing of this treatment, and the timingof surgery were not associated with increasedprobability of visual improvement. On these bases,they concluded that neither steroids nordecompression surgery should be considered as apart of standard care for patients with traumatic opticneuropathy.
In the case described in this report, we usedmegadose methylprednisolone to treat opticneuropathy. There was no significant change in thepatient's condition initially, but markedimprovement in visual acuity occurred within 3weeks. Similarly, Seiff (4) noted that corticosteroidtreated patients may not begin to improve until 5days after treatment is started.
In conclusion, traumatic optic neuropathyassociated with blunt forehead trauma is a potentiallyvision-threatening process that requirescomprehensive clinical assessment and appropriateneuroimaging. The treatment options arecorticosteroid therapy, surgical decompression of theoptic canal, or observation alone. It seems clinicallyreasonable to decide whether to treat or to strictlyobserve on a case-by-case basis.
Correspondence: Do\. Dr. Esin ErkinMithatpa~a Cad. No: 144/935260 Karata~ iZMiRTel: 0-236-2349070Fax: 0-236-2370213
E-mail: [email protected]
REFERENCES
1. Anderson RL, Panje WR, Gross CE: Optic nerveblindness following blunt forehead trauma.Ophthalmology 89: 445455, 1982
2. Bracken MB, Shepard MJ, Collins WF, Holford TR,Young W, Baskin OS, Eisenberg HM, Flamm E, LeoSummers L, Maroon J, Marshall LF, Perot PL,
Peipmeier J, Sonntag VKH, Wagner FC, Wilberger JE,Winn HR: A randomised controlled trial of
methylprednisolone or naloxone in the treatment ofacute spinal cord injury. N Eng J Med 322: 1405, 1990
3. Braughler JM, Hall ED: Current applications of "highdose" steroid therapy for CNS injury. J Neurosurg 62:806, 1985
4. Cook MW, Levin LA, Joseph MP, Pinczower EF:
53

TIlrkish Nellrosurgery 12: 50 - 54, 2002
Traumatic optic neuropathy. A meta-analysis. ArchOtolaryngol Head Neck Surg 122: 389392, 1996
5. G6<;er AI, Udan F, HaClyakupoglu S, Tuna M,Bagdatoglu IS, Cetinalp E, Aksoy K: The effect ofimmediate decompression on the optic nerve inretrobulbar hematoma. Neurosurg Rev 19: 169173, 1996
6. Gross C, DeKockJ, Panje W, Hershkowitz N, NewmanJ: Evidence for orbital deformation that may contributeto monocular blindness following minor frontal headtrauma. J Neurosurg 55: 963966, 1981
7. Joseph MP, Lessell S, Rizzo J, Momose KJ: Extracranialoptic nerve decompression for traumatic opticneuropathy. Arch Ophthalmoll08: 10911093, 1990
8. Kline LB, Morawetz RB, Swaid SN: Indirect injury ofthe optic nerve. Neurosurgery 14: 756764, 1984
9. Lessell S: Indirect optic nerve trauma. ArchOphthalmoll07: 382386, 1989
10. Levin LA, Joseph MP, Rizzo JF 3rd, Lessell S: Opticcanal decompression in indirect optic nerve trauma.Ophthalmology 101: 566569, 1994
11. Levin LA, Beck RW, Joseph MP, Seiff S, Kraker R: The
Mir::ni: Trawuntie Optic NCIlroJ'atll!!
International Optic Nerve Trauma Study Group.Ophthalmology 106: 12681277,1999
12. Mine S, Yamakami I, Yamaura A, Hanawa K, lkejiriM, Miz Adachi-Usami E: Outcome of traumatic opticneuropathy. Comparison between surgical andnonsurgical treatment. Acta Neurochir (Wien) 141:2730, 1999
13. Panje WR, Gross CE, Anderson RL: Sudden blindnessfollowing facial trauma. Otolaryngol Head Neck Surg89: 941948, 1981
14. Seiff SR: High-dose corticosteroids for the treatment ofvision loss due to indirect injury to the optic nerve.Ophthalmic Surg 21: 389395, 1990
15. Spoor TC, Hartel WC, Lensink DB, Wilkinson MJ:Treatment of traumatic optic neuropathy withcorticosteroids. Am J Ophthalmol 110: 665669, 1990
16. Steinsapir KD, Goldberg RA: Traumatic opticneuropathy. Surv Ophthalmol 38: 487518, 1994
17. Wollin MJ, Lavin PJM: Spontaneous visual recoveryfrom traumatic optic neuropathy after blunt headinjury. Am J Ophthalmoll09: 430, 1990
PRI~L 'r:c ~1'DA· TE T r .•
1'.1< \I, (Al'lTIJ.
Q \' Af T ... ,vr,ITA.
Andreas Vesalius (1519-1564),presented the relation of the skull deformations and thesutures in his book: De Humani Corporis Fabrica. Basel, Opporinus, 1543.
Several early and original descriptions of craniosynostosis was described and illustrated by him.
54
Related Documents











