Trauma Case Ext. Boonphiphop Boonpheng Ext. Pataramon

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript
Trauma Case
Ext. Boonphiphop BoonphengExt. Pataramon

Case
• ผู้��ป่�วยหญิงไทย อาย� 85 ป่�• Previous status: household ambulation using
walker (Parkinson’s disease)• CC: หกล้�ม เจ็�บสะโพกซ้�าย 2 hr

Present illness
• 2 hr PTA ขณะเดินเองบนพ"#นบ�าน ม$ส�น%ขมาเกะกะ พ%นขา เส$ยหล้%กสะดิ�ดิหกล้�มเอา ก�นกระแทกพ"#นใน ท)าน%*ง ศี$รษะไม)กระแทกพ"#น ไม)สล้บ จ็-าเหตุ�การณ/ไดิ�
หล้%งล้�มย"นไม)ข0#น เจ็�บสะโพกแล้ะตุ�นขาซ้�ายดิ�าน นอก ไม)ม$แผู้ล้หร"อเล้"อดิออก ไม)เจ็�บบรเวณอ"*น

Past History

Primary Survey

Physical Examination
• Vital signs: PR = 90 / min , RR = 20 /min , BP = 130/80 mmHg
• General appearance: No distress.• HEENT: not pale.• Lung: WNL• Heart: WNL

Physical examination
Right hip Left hip
- WNL
-From ASIS to medial malleolus: 71 cm
- Full ROM- Anvil: negative- Rolling: negative
- Slight external rotation- No ecchymosis. No swelling- No leg length shortening
From ASIS to medial malleolus: 70 cm- Marked tenderness at greater trochanter and lateral
leg- ROM limited in all direction due to pain- Anvil’s test: positive- Rolling test: positive- Popliteal, dorsalis pedis, posterior tibial pulse 2+- Motor power: no weakness (limited due to pain)
Upper: within normal limited both sides

Impression
• Fracture around Lt hip joint• Fracture from low-impact trauma• Osteoporosis
• Investigation:– Plain radiography of both hips: AP, lateral



Diagnosis
• Plain radiography findings:• - Intertrochanteric fracture of left hip without
displacement – Generalized osteopenia
• Final Diagnosis– Closed nondisplaced intertrochanteric fracture of
left hip– Osteoporosis

Intertrochanteric fracture
• Intertrochanteric fractures account for nearly 50% of all fractures of the proximal femur.
• Average patient age of incidence is 66 to 76 years.
• The ratio of women to men ranges from 2:1 to 8:1, likely because of postmenopausal metabolic changes in bone.
Intertrochanteric fracture
• Extracapsular fractures • occur in cancellous bone with an abundant blood supply• Low risk of nonunion/osteonecrosis but high risk of
displacement due to muscle contraction• MECHANISM OF INJURY• Intertrochanteric fractures in younger individuals are usually the
result of a high-energy injury such as a motor vehicle accident or fall from a height.
• Ninety percent of intertochanteric fractures in the elderly result from a simple fall.
• Most fractures result from a direct impact to the greater trochanteric area.
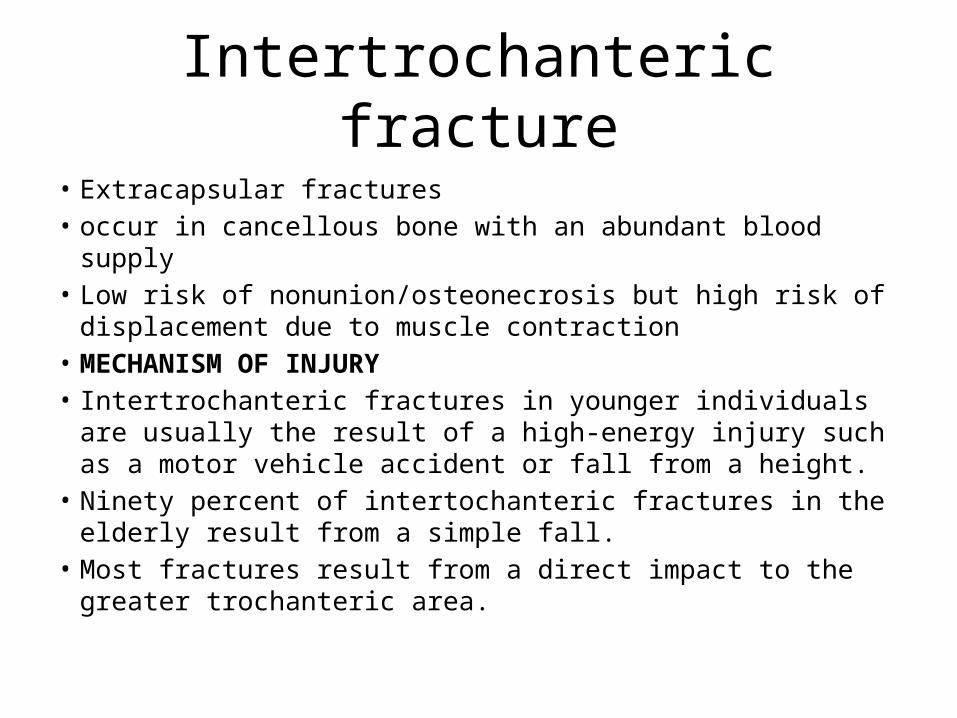
Anatomy

Evans classification

Initial management
• Pain control• Skin traction of left leg: 10 lbs• Pre-op medical consultation• Option for further management– Surgery within 72 hrs / medically stabilized– Nonoperative management– Osteoporosis management• DEXA bone mineral density measurement – baseline• Bisphosphonates / Teriparatide

Surgery
• The goal is stable internal fixation to allow early mobilization and full weight-bearing ambulation
• Most cases require surgical fixation• Fixation techniques– Sliding hip screw– Intramedullary hip screw

Nonoperative management
• Indication:– Patients at extreme medical risk for surgery– Nonambulatory patients with mild hip pain.
• Early bed to chair mobilization is important to avoid increased risks and complications of prolonged immobility
• Resultant hip deformity is both expected and accepted.
• Higher mortality rate than operative treatment.


Complication
• Loss of fixation• Nonunion• Malrotation deformity• Osteonecrosis
Related Documents