Review – Laparoscopy Transumbilical Single-Port Surgery: Evolution and Current Status David Canes *, Mihir M. Desai, Monish Aron, Georges-Pascal Haber, Raj K. Goel, Robert J. Stein, Jihad H. Kaouk, Inderbir S. Gill Center for Laparoscopic and Robotic Surgery, Department of Urology, Glickman Urological and Kidney Institute, Cleveland Clinic, Cleveland, Ohio, USA european urology 54 (2008) 1020–1030 available at www.sciencedirect.com journal homepage: www.europeanurology.com Article info Article history: Accepted July 3, 2008 Published online ahead of print on July 14, 2008 Keywords: Laparoscopy Single port NOTES Transumbilical Abstract Context: Single-port transumbilical laparoscopy, also known as embryonic natural orifice transumbilical endoscopic surgery (E-NOTES), has emerged as an attempt to further enhance cosmetic benefits and reduce morbidity of minimally invasive surgery. Within a short span, several clinical reports have emerged in the urologic literature. As this field is poised to move forward, a complete understanding of its evolution and current status is timely. Objective: To summarize and review the history of E-NOTES across surgical disciplines. This review emphasizes nomenclature, surgical technique, instru- mentation, and perioperative outcomes. Specific urological and nonurological applications of single-port surgery to date are summarized. Evidence acquisition: Using the National Library of Medicine database, the English-language literature was reviewed for the past 40 yr. Keyword searches included: scarless, scar free, single port/trocar/incision, intraumbilical, and transumbilical. Within the bibliography of selected references, additional sources were retrieved. Evidence synthesis: The gynecologic and general surgical literature includes approximately 19 papers fulfilling the search criteria, encompassing extirpative procedures only. The urologic literature contains eight published reports of single-trocar transumbilical procedures. These reports are summarized in a chronological manner and grouped by subject. No prospective studies compar- ing outcomes to standard laparoscopy have been reported. Technical feasibility has been demonstrated for a broad range of extirpative and reconstructive procedures on the upper and lower urinary tracts, including simple and radical nephrectomy, donor nephrectomy, renal cryotherapy, pyeloplasty, ileal uret- eral replacement, sacrocolpopexy, and varicocelectomy. Conclusions: E-NOTES has made its initial forays into laparoscopic surgery. Ongoing refinement in technique and instrumentation is likely to expand its future role. # 2008 Published by Elsevier B.V. on behalf of European Association of Urology. * Corresponding author. Department of Urology, Glickman Urological and Kidney Institute, 9500 Euclid Avenue, A-100, Cleveland, OH 44195, United States. Tel. +1 216 445 1530; Fax: +1 216 445 7031. E-mail address: [email protected] (D. Canes). 0302-2838/$ – see back matter # 2008 Published by Elsevier B.V. on behalf of European Association of Urology. doi:10.1016/j.eururo.2008.07.009

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

Review – Laparoscopy
Transumbilical Single-Port Surgery: Evolution and CurrentStatus
e u r o p e a n u r o l o g y 5 4 ( 2 0 0 8 ) 1 0 2 0 – 1 0 3 0
avai lable at www.sc iencedi rect .com
journal homepage: www.europeanurology.com
David Canes *, Mihir M. Desai, Monish Aron, Georges-Pascal Haber, Raj K. Goel,Robert J. Stein, Jihad H. Kaouk, Inderbir S. Gill
Center for Laparoscopic and Robotic Surgery, Department of Urology, Glickman Urological and Kidney Institute, Cleveland Clinic, Cleveland,
Ohio, USA
Article info
Article history:Accepted July 3, 2008Published online ahead ofprint on July 14, 2008
Keywords:LaparoscopySingle portNOTESTransumbilical
Abstract
Context: Single-port transumbilical laparoscopy, also known as embryonicnatural orifice transumbilical endoscopic surgery (E-NOTES), has emerged asan attempt to further enhance cosmetic benefits and reduce morbidity ofminimally invasive surgery. Within a short span, several clinical reports haveemerged in the urologic literature. As this field is poised to move forward, acomplete understanding of its evolution and current status is timely.Objective: To summarize and review the history of E-NOTES across surgicaldisciplines. This review emphasizes nomenclature, surgical technique, instru-mentation, and perioperative outcomes. Specific urological and nonurologicalapplications of single-port surgery to date are summarized.Evidence acquisition: Using the National Library of Medicine database, theEnglish-language literature was reviewed for the past 40 yr. Keyword searchesincluded: scarless, scar free, single port/trocar/incision, intraumbilical, andtransumbilical. Within the bibliography of selected references, additionalsources were retrieved.Evidence synthesis: The gynecologic and general surgical literature includesapproximately 19 papers fulfilling the search criteria, encompassing extirpativeprocedures only. The urologic literature contains eight published reports ofsingle-trocar transumbilical procedures. These reports are summarized in achronological manner and grouped by subject. No prospective studies compar-ing outcomes to standard laparoscopy have been reported. Technical feasibilityhas been demonstrated for a broad range of extirpative and reconstructiveprocedures on the upper and lower urinary tracts, including simple and radicalnephrectomy, donor nephrectomy, renal cryotherapy, pyeloplasty, ileal uret-eral replacement, sacrocolpopexy, and varicocelectomy.Conclusions: E-NOTES has made its initial forays into laparoscopic surgery.
Ongoing refinemen t in technique and instrumentation is likely to expand itsfuture role.# 2008 Published by Elsevier B.V. on behalf of European Association of Urology.
* Corresponding author. Department of Urology, Glickman Urological and Kidney Institute,9500 Euclid Avenue, A-100, Cleveland, OH 44195, United States. Tel. +1 216 445 1530;Fax: +1 216 445 7031.E-mail address: [email protected] (D. Canes).
0302-2838/$ – see back matter # 2008 Published by Elsevier B.V. on behalf of European Association of Urology. doi:10.1016/j.eururo.2008.07.009

e u r o p e a n u r o l o g y 5 4 ( 2 0 0 8 ) 1 0 2 0 – 1 0 3 0 1021
1. Introduction
Laparoscopic surgery is a well-established alterna-tive to open surgery across disciplines. Although themagnitude of impact varies by procedure, in general,the benefits of laparoscopy on postoperative pain,cosmesis, hospital stay, and convalescence arewidely recognized. Current efforts are aimed atfurther reducing the morbidity associated withminimally invasive surgery. To this end, two recentinnovations are being developed, either pure orhybrid: (1) natural orifice translumenal endoscopicsurgery (NOTES), whereby intraperitoneal access isgained through the mouth, anus, vagina, or urethraand the viscus-of-entry is perforated to reach thesurgical target; and (2) embryonic natural orificetransumbilical endoscopic surgery (E-NOTES),wherein the surgical scar is virtually concealedwithin the umbilicus, an embryonic natural orifice.
Table 1 – Nonurologic E-NOTES procedures
Procedure Year First report A
Tubal ligation 1969 Wheeless [4]
Total hysterectomy, BSO 1991 Pelosi et al [8]
Supracervical
hysterectomy, BSO
1992 Pelosi et al [9]
Appendectomy 1992 Pelosi et al [10]
Cholecystectomy 1997 Navarra et al. [13]
Ovarian cystectomy 2001 Kosumi et al [15]
Salpingectomy for ectopic
pregnancy
2005 Ghezzi et al [16]
Peritoneal dialysis catheter 2005 Blessing et al [18]
Lap-assisted
ventriculoperitoneal
shunt
2006 Goitein et al [19]
Lap-assisted gastrostomy 2006 Kawahara et al [31]
Meckel’s diverticulectomy 2007 Cobellis et al [17]
Abbreviations: E-NOTES, embryonic natural orifice transumbilical e
Percutaneous endoscopic gastrostomy.
This review seeks to place E-NOTES in its historicalcontext; describe its gynecologic, general surgical,and urologic applications to date; and describecurrent instrumentation and limitations.
2. Methods
Efforts aimed at further reductions in morbidity while
maintaining the same high standard of surgical cure are
valuable. Indirect evidence for potential benefits of E-NOTES
and NOTES already exists. For instance, a reduction in port
size decreases operative morbidity [1]. Mostafa et al compared
patients undergoing needlescopic versus conventional laparo-
scopic appendectomy [2]. The needlescopic group had shorter
hospital stay (1.3 d vs 3.2 d), reduced narcotic requirements,
and faster return to work (8 d vs 17 d) than the conventional
group. Similarly, in a randomized prospective comparison of
conventional laparoscopic cholecystectomy versus the same
procedure using downsized trocars (3.5 mm), Bisgaard et al
detected important decrements in morbidity [3]. The group
pprox no.of cases
Transumb,single trocar
Comments
>4000 U Has been performed as
outpatient procedure under
local anesthesia with sedation
1 U First case of complex
extirpative pelvic surgery
using a solitary intraumbilical
incision
4 U Concomitant intrauterine
cannula for manipulation;
offset eyepiece on
laparoscope with 5-mm
working channel; standard
lap instruments used
180 U –
1 –
1 U Performed in an infant aged
2 mo where, after grasping
the cyst through a trocar,
cyst was aspirated and
delivered through the
umbilical incision
10 U Single umbilical trocar and
percutaneous sling suture to
retract the affected tube
25 – –
7 – 5-mm periumbilical trocar with
laparoscope allowed safe
intraperitoneal placement
of catheter tip
22 – Incision and 10-mm trocar
placed at PEG site; stomach
grasped and exteriorized
with 3-mm instrument
9 U –
ndoscopic surgery; BSO, bilateral salpingo-oophorectomy; PEG,

e u r o p e a n u r o l o g y 5 4 ( 2 0 0 8 ) 1 0 2 0 – 1 0 3 01022
with downsized trocars reported less incisional pain in the
first postoperative week.
Although limiting the size and/or number of trocars is
clearly not the sole means of decreasing overall morbidity, the
effect of restricting access to the umbilicus only (E-NOTES) or
of removing transabdominal incisions completely (NOTES)
warrants further evaluation. With each procedure, the
possibility of inserting additional ports as necessary always
exists, such that surgical safety and outcomes remain
uncompromised.
2.1. Nonurologic E-NOTES procedures
A review of nonurologic E-NOTES procedures is summarized
in Table 1 and detailed in the following sections.
2.1.1. Tubal ligationClifford Wheeless first published his technique of laparoscopic
tubal ligation in 1969 [4]. He reported 2 yr later on 85 patients
who had been sterilized using his single-incision outpatient
technique [5]. Through a 1-cm, curved infraumbilical incision,
he established CO2 insufflation and inserted a laparoscope
with an offset eyepiece. The uterus itself was manipulated
externally with a tenaculum inserted through the vagina,
bringing the fallopian tubes into view. A biopsy forceps was
used to grasp and cauterize each fallopian tube. Wheeless later
updated his series, reporting on 3600 cases, 2600 of which had
one-incision tubal ligation [6]. The cosmetic benefits of this
technique were recognized by Singh, who had performed
>1000 single-trocar tubal sterilization procedures by 1977 [7].
He remarked, ‘‘Wound healing is so satisfactory that no scar is
grossly visible postoperatively.’’
2.1.2. Hysterectomy, bilateral salpingo-oophorectomyIn 1991, Pelosi et al performed total hysterectomy with bilateral
salpingo-oophorectomy (BSO), the first complex extirpative
procedure using the single-puncture technique [8]. The follow-
ing year, supracervical hysterectomy was performed for benign
uterine disease in four patients, with application of the term
minilaparocopy [9]. Similar to the technique for tubal steriliza-
tion, a laparoscope was used with an offset eyepiece and a
5-mm working channel through which standard laparoscopic
instruments were inserted. The uterus was manipulated with a
tranvaginal cannula. In their discussion, the authors high-
lighted presumed advantages of their technique: simplicity,
lower cost, decreased trocar-site-related complications,
improved cosmesis, and ability to convert to standard laparo-
scopy or open surgery when required.
2.1.3. AppendectomyPelosi also reported the first series (n = 25) of single-trocar
appendectomies in 1992 [10]. A larger series by D’Alessio et al
followed in 2001, with 116 patients undergoing one-trocar
transumbilical laparoscopic-assisted appendectomy (TULAA)
[11]. In 28 additional cases (19%), the majority of which had
inflamed retrocecal appendix, additional trocars were
inserted. Open surgery was required for six patients (4%).
This group used an 11-mm Hasson trocar and an 11-mm
laparoscope with a 5-mm working channel. The appendix was
grasped and delivered through the umbilical incision, and the
appendectomy was performed extracorporeally. Mean opera-
tive time was 35 min. The single-trocar group returned to
normal activity at 7 d compared to 10 d for the multiple trocar
group and 14 d for the open surgical cases. The authors
commented that ‘‘from an aesthetic point of view the
transumbilical incision is practically invisible.’’ In 2007, Ates
et al reported 35 patients undergoing single-port appendect-
omy [12]. They used a specialized trocar with dual 5-mm
working channels (Applied Medical, Rancho Santa Margarita,
CA, USA). A laparoscope with an offset eyepiece and 6-mm
working channel (Karl Storz, Tuttlingen, Germany) was
employed. A percutaneous sling suture through the mesoap-
pendix provided countertraction on the appendix, taking over
the role usually reserved for a second instrument through an
additional trocar.
2.1.4. CholecystectomyThe first transumbilical cholecystectomy was reported in 1997
by Navarra [13], followed shortly thereafter by Piskun in 1999
[14]. In the latter report, two separate 5-mm trocars were
placed through a single intraumbilical incision. Two intra-
abdominal stay sutures facilitated surgical manipulation. The
5-mm fasciotomies were joined for specimen extraction. No
extraumbilical incisions were required. The procedure was
successfully completed without intraoperative complication
in 10 patients.
2.1.5. Ovarian cystectomySingle-port ovarian cystectomy in an infant aged 2 mo was
reported in 2001 [15]. The 6-cm cyst was accessible through a
single 10-mm umbilical trocar grasped through the working
channel of a Wolf cerebral endoscope (Panoview telescope,
Richard Wolf, Knittlingen, Germany) and delivered to the
umbilical incision where the cyst was aspirated, decorticated,
and delivered back into the peritoneal cavity.
2.1.6. Salpingectomy for tubal ectopic pregnancyNormally a three-trocar procedure, laparoscopic salpingect-
omy through a single umbilical trocar was reported in 2005
[16]. Similar to the cases of appendectomy, these 10 cases of
salpingectomy were aided by placing a midline percutaneous
sling suture through the affected tube, suspending the
fallopian tube and obviating the need for a second trocar.
2.1.7. Meckel’s diverticulectomyIn 2007, the single-trocar transumbilical approach to Meckel’s
diverticulectomy was used in nine patients [17]. In each case,
the intestinal segment was brought out through the umbilical
incision and bowel work was performed extracorporeally. A
wide fasciotomy beneath the 10-mm skin incision was
necessary to facilitate exteriorization and reintroduction of
the ileum without inducing vascular congestion.
2.1.8. MiscellaneousApplication of a single trocar to direct placement of intraper-
itoneal drains has been described, although morbidity data are
lacking. Blessing et al elucidated their single-trocar technique
for placement of a peritoneal dialysis catheter in 2005 [18].
Goitein et al described laparoscopically assisted ventroculo-
peritoneal shunt placement in 2006 [19], avoiding the typical

Table 2 – E-NOTES urologic procedures
Procedure First author Year No. of cases Comments
Simple nephrectomy, ureterolithotomy Rane et al [22] 2007 2 R-port via extraumbilical flank
incision for nephrectomy
Simple nephrectomy, radical nephrectomy Raman et al [23] 2007 1 Multiple ports, single umbilical incision,
additional 3-mm liver retraction port
Simple nephrectomy Desai et al [24] 2008 1 Single transumbilical port exclusively
Renal cryotherapy; sacrocolpopexy Kaouk et al [25] 2008 4 Single transumbilical port exclusively
4
Pyeloplasty, ileal ureter, psoas hitch
ureteroneocystostomy
Desai et al [29] 2008 4 Single transumbilical port; 2-mm
needlescopic grasper
Live-donor nephrectomy; partial
nephrectomy
Gill et al [27] 2008 4 Single transumbilical port; 2-mm
needlescopic grasper3
Pediatric varicocelectomy Kaouk et al [28] 2008 – First experience in pediatrics
Radical prostatectomy; Radical cystectomy Kaouk et al [30] 2008 4 Single transumbilical port exclusively;
ileal conduit urinary diversion3
Abbreviations: E-NOTES, embryonic natural orifice transumbilical endoscopic surgery.
Fig. 2 – Mock intraoperative view of the Uni-X multichannel
port, where a combination of flexible and bent
instruments allows tip separation and triangulation
distally. Inset shows the port fixed in its intraumbilical
e u r o p e a n u r o l o g y 5 4 ( 2 0 0 8 ) 1 0 2 0 – 1 0 3 0 1023
small midline laparotomy incision. A periumbilical 5-mm
trocar with laparoscope was placed, allowing inspection of the
peritoneal cavity to choose an ideal site for catheter insertion.
The introducer/dilator was passed under laparoscopic vision,
and the tip was guided toward the pelvis.
2.2. Urologic E-NOTES procedures
Gettman et al recently recognized in a NOTES consensus paper
that whereas NOTES is still evolving predominantly in the lab,
single-access procedures such as E-NOTES are already being
clinically implemented [20]. A review of urologic E-NOTES
procedures is summarized in Table 2 and is detailed in the
following sections.
2.2.1. PortsRecently, two trocar options for transumbilical laparoscopy
have been reported in the urologic arena. These proprietary,
multilumen, single-trocar systems include the R-port
Fig. 1 – Intraoperative photograph of the multichannel R-
port in a transumbilical incision with a camera occupying
one 5-mm inlet and the insufflation channel attached.
position with fascial sutures. Of the three channels, the
longer camera channel with insufflation inlet is seen.
(Advanced Surgical Concepts, Wicklow, Ireland), and the
Uni-X single laparoscopic port system (Pnavel Systems,
Morganville, NJ, USA). Multilumen access through a single
intraumbilical incision can also be performed using standard
laparoscopic trocars placed through adjacent fascial punc-
tures.
The R-Port consists of two components: (1) a fascial
retractor containing an inner and an outer ring with an
intervening plastic sleeve, and (2) a multichannel valve (one at
12 mm, two at 5 mm). Each component is covered with a
thermoplastic elastomer that maintains a tight seal on
pneumoperitoneum while allowing the smooth introduction
of instruments and accessories. After making a vertical
intraumbilical incision and releasing dermis from the fascia,
a 2-cm fasciotomy is made in an open or Hasson fashion. The
inner ring is loaded within a nonbladed introducer that

Table 3 – Multichannel ports for single-port procedures
Port Manufacturer Lumens Fixation mech Valve mech
R-port Advanced Surgical Concepts,
Wicklow, Ireland
One at 12 mm,
two at 5 mm
Inner/outer ring, intervening
taut plastic sleeve
Gel elastomer
Uni-X Pnavel Systems,
Morganville, NJ, USA
Three at 5 mm Fascial sutures Rubber inlet
Table 4 – Specialized instruments
Instrument Manufacturer Size Comment
Flexible grasper, needle holder, scissors RealHand; Novare Surgical Systems,
Cupertino, CA, USA
5 mm –
Flexible laparoscopic grasper,
needle holder, scissors
Autonomy Lapro-Angle;
Cambridge Endo, Framingham, MA, USA
5 mm Bulky handle can be obstacle
with external instrument crowding
Flexible endoscope Olympus Surgical,
Orangeburg, NY, USA
5 mm Bulk of standard laparoscopic
cameras exacerbate crowding.
These streamlined digital cameras
minimize clashing
Rigid 308 endoscope
Bent laparoscopic grasper Pnavel Systems Inc,
Morganville, NJ, USA
5 mm Position of curved shaft can be
altered by rotational knob
e u r o p e a n u r o l o g y 5 4 ( 2 0 0 8 ) 1 0 2 0 – 1 0 3 01024
deploys the inner ring intraperitoneally. Slack is removed,
whereby the taut plastic sleeve effectively tents open the
fasciotomy and tightly approximates the rings to create an
effective seal. Once deployed, the retractor is reminiscent of a
miniature hand port to which the multivalve cap with
insufflation inlet is attached (Fig. 1).
The Uni-X system consists of an inverted-cone-shaped,
plastic outer unit converging on three separate 5-mm inlets.
The device is also inserted using a Hasson technique. Four
fascial sutures affixed to the device effectively create a tight
seal for pneumoperitoneum (Fig. 2). Features of the R-Port and
Uni-X systems are compared in Table 3.
2.2.2. InstrumentationIn addition to standard laparoscopic instruments, either bent
or flexible instrumentation has been used to facilitate
dissection and/or intracorporeal suturing. A list of instru-
ments can be seen in Table 4.
2.3. Animal studies
In the porcine model, Zeltser et al reported single-trocar
nephrectomy using novel magnetically anchored instru-
ments, each deployed through the 15-mm umbilical portal
of entry [21]. The relatively thin porcine abdominal wall
allowed fixation of both a camera and a robotic cautery arm
using magnetic couplers. Each of these was hardwired to
external guidance systems, and light was provided by
fiberoptic cables surrounding the umbilical trocar itself.
Standard laparoscopic graspers and the vascular stapler were
manipulated through the umbilical trocar, and tissue dissec-
tion was accomplished with the robotic arm. The specimen
was extracted through the solitary umbilical incision. As of
this writing, the use of magnetically anchored instruments to
facilitate urologic E-NOTES procedures has not been reported
in humans.
3. Results
3.1. Clinical applications
3.1.1. Nephrectomy, ureterolithotomy, pyeloplasty
The first two cases of single-port surgery in urologywere reported by Rane et al, in abstract form, at the2007 World Congress of Endourology in Cancun,Mexico [22]. The first report of single-port, non-transumbilical, simple nephrectomy described an R-port situated in a flank incision for retroperitoneo-scopy. The patient was a 36-yr-old man with a small,nonfunctioning right kidney. The second casedescribed laparoscopic transperitoneal uretero-lithotomy for an impacted 2.5-cm proximal ureteralstone, performed exclusively with an intraumbilicalR-port.
Subsequently, the first multitrocar single-inci-sion transumbilical nephrectomy was reported byRaman et al [23]. Following an initial porcinefeasibility demonstration, three human nephrec-tomies were performed: two for benign nonfunctionand one for a 4.5-cm clear-cell carcinoma. Meanoperative time was 133 min. Through a singleumbilical incision, three adjacent conventionaltrocars (one at 12 mm, two at 5 mm) were placed.The hilum was transected using an endovascularstapler through the 12-mm port. On the right side(nephrectomy for carcinoma), static liver retractionrequired an extraumbilical skin incision for a 3-mminstrument. Dissection was facilitated by flexiblelaparoscopic instruments (RealHand, Novare Surgi-cal Systems, Cupertino, CA, USA) and either an

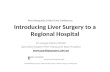
Fig. 3 – Donor allograft on the back bench demonstrates
vessel length commensurate with standard laparoscopy.
e u r o p e a n u r o l o g y 5 4 ( 2 0 0 8 ) 1 0 2 0 – 1 0 3 0 1025
angled, rigid 5-mm endoscope or a flexible-tip videoendoscope (Olympus Surgical, Orangeburg, NY, USA).
The first single-port transumbilical nephrectomywas reported by Desai et al in 2007 [24]. Specializedinstrumentation and accessories included theR-port; a 5-mm, 308 endoscope (EndoEye; OlympusMedical, Tokyo, Japan); and curved laparoscopicgrasping instruments (Advanced Surgical Concepts).The transperitoneal left nephrectomy, performedfor benign nonfunctioning kidney after failed pye-loplasty, was performed in 3.6 h without anyextraumbilical skin incisions. The endoscope occu-pied one inlet at all times, and a combination of abent grasper and straight scissors or harmonicscalpel allowed tissue presentation under tensionsufficient for precise dissection. Hemolock clips(Teleflex Medical, Research Triangle Park, NC, USA)were used for renal artery and vein control.
This same report described single-port transum-bilical pyeloplasty for primary right ureteropelvicjunction (UPJ) obstruction [24]. A 2-mm needlescopicgrasper was used through a Veres Minisite port(USSC, Norwalk, CT, USA) that had been used toestablish pneumoperitoneum in the left hypochon-drium. A 5-mm atraumatic grasper placed trans-umbilically through one of the three proprietaryinlets was used for liver retraction as needed. Thesolitary umbilical incision was used to exteriorize apenrose drain at the conclusion of the case. Nofunctional outcomes were reported.
3.1.2. Cryotherapy, kidney biopsy, sacrocolpopexy
Kaouk et al reported seven patients undergoingsingle-port transumbilical urologic laparoscopicprocedures [25]: renal cryotherapy (n = 2), wedgekidney biopsy (n = 1), and sacrocolpopexy (n = 4). Inthese cases, the Uni-X single port was used. Theseseven patients underwent transperitoneal proce-dures through the umbilicus without extraumbilicalincisions. For this series, standard laparoscopicinstruments, a flexible 5-mm endoscope (OlympusSurgical), and bent laparoscopic instruments (Pna-vel Systems) were used. Three additional patientsunderwent extraumbilical skin incisions: retroper-itoneoscopic cryotherapy (n = 2) with incision at thetip of the 12th rib, and radical nephrectomy (n = 1)with a 12-mm trocar placed through a standardGibson incision for various intraoperative manip-ulations and ultimate specimen extraction.
The first series of single port cryotherapy wasreported by Goel and Kaouk [26]. E-NOTES cryother-apy was performed in two patients undergoing atransperitoneal approach for anterior tumors, andfour patients had retroperitoneoscopic single-portcryotherapy with the multilumen port positioned at
the tip of the 12th rib for posterior tumors. Meantumor size was 2.6 cm. Although instrument clash-ing was frequent, cryotherapy was feasible withoutintraoperative complication, and mean hospital staywas 2.3 d. In these cases, an endoscope with aflexible tip allowed the assistant to change thesurgical view while leaving the external segmentstill, thereby maximizing space for the primarysurgeon’s movements.
3.1.3. Live-donor nephrectomy
Gill et al reported the initial four patients whounderwent E-NOTES live-donor nephrectomy fortransplantation [27]. Through an intraumbilical inci-sion, the novel R-Port was inserted into the abdomen.A 2-mm Veres needle port, inserted via skin needle-puncture to create pneumoperitoneum, was used toselectively insert a needlescopic grasper for tissueretraction. The vessels were controlled in identicalfashion to standard donor nephrectomy: the arterywas controlled with hemolock clips (Teleflex Medical,Research Triangle Park, NC), and the vein wascontrolled with an articulating vascular Endo-GIAstapler (US Surgical, Norwalk, CT). Excellent donorvascular and tissue dissection could be performed,and a quality donor kidney was retrieved transumbi-lically after preentrapment; median umbilical inci-sion length was 4 cm (Figs. 3 and 4). E-NOTES donornephrectomy was successful in all four patientswithout any extraumbilical skin incision or conver-sion to standard laparoscopy. Median operating timewas 3.3 h, blood loss was 50 cc, warm ischemia timewas 6.2 min, and hospital stay was 3 d. One patienthad two left renal arteries; each was controlledindividually. Median length of harvested renal arterywas 3.3 cm, renal vein was 4 cm, and ureter was15 cm. No intraoperative complications occurred.

Fig. 4 – Postoperative photograph at 2 wk following
embryonic natural orifice transumbilical endoscopic
surgery (E-NOTES) donor nephrectomy.
e u r o p e a n u r o l o g y 5 4 ( 2 0 0 8 ) 1 0 2 0 – 1 0 3 01026
Median donor visual analog scale (VAS) upondischarge was 2/10. Convalescence was completedby 2 wk, as reflected by VAS scores of 0/10 at 2 wk withno patient taking any pain medications. All allograftsfunctioned immediately upon transplantation, withearly nadir serum creatinine 0.9–1.8 mg/dl.
Since starting our E-NOTES program, we haveperformed nine consecutive E-NOTES donornephrectomies and are in the process of comparingoutcomes of E-NOTES and standard laparoscopy.E-NOTES donor nephrectomy appears to haverelevance and promise, especially for this typicallyyounger, altruistic population. Although this initialexperience is encouraging, more data and experi-ence at additional centers are necessary.
3.1.4. Pediatric E-NOTES
The first series of single port urologic laparoscopy inchildren was reported by Kaouk and Palmer, whosuccessfully performed E-NOTES varicocelectomy inthree adolescents aged 13–16 yr [28]. Each patienthad grade 3 varicoceles, and the testicular artery andvein were transected between clips. At 2-mo follow-up, no varicocele recurrence or complication hadoccurred, including hydrocele, infection, or inci-sional sequelae.
3.1.5. Unpublished data
To date at the Cleveland Clinic, complex recon-structive E-NOTES urologic procedures have beenperformed, including ileal ureteral interposition,
bilateral single-session pyeloplasty, and psoas hitchureteroneocystostomy [29]. In addition, complexextirpative procedures requiring reconstructionhave been accomplished, including E-NOTES partialnephrectomy, radical prostatectomy, and radicalcystectomy with extended pelvic lymphadenectomy[30].
4. Discussion
4.1. Technical challenges
4.1.1. Triangulation
Wide spacing of trocars is considered a tenet ofmultitrocar standard laparoscopy. Instrument trian-gulation allows proper tissue retraction, which isessential for proper dissection along anatomicaltissue planes. Placing several parallel instrumentsmakes triangulation more difficult. Using at least oneflexible or curved instrument offsets the shaftssufficiently to accomplish some degree of triangula-tion. Often this requires counterintuitive movementson the outside, where the surgeon’s instruments maycross each other. Although generally frowned uponduring standard laparoscopy, crossing instrumentsmay often be necessary in single-port access surgery.
4.1.2. Retraction
The use of fixation or sling sutures can achieveretraction that is normally accomplished by anadditional assistant trocar. These can either be staticintra-abdominal sutures affixed to the parietalperitoneum or percutaneous sutures grasped andmanipulated extracorporeally to maintain variabletractionasdissection proceeds.The general literatureshows that these techniques have proved useful forsalpingectomy [16], appendectomy [12], and chole-cystectomy [14]. In the case of pyeloplasty, suturingthe lateral cut edge of Gerota’s fascia to the lateralabdominal wall is another example of securing wideexposure of the operative field without adding ports.
4.1.3. Instrument crowding
External crowding and clashing of instruments isthe most salient and frustrating aspect of thelearning curve for these procedures. One mustchoose instruments that will set the stage forsuccess. For one, the instrument profile should beas slim as possible. A primary advantage of theEndoEye camera system (Olympus Medical) is itsstreamlined profile, whereas the standard laparo-scopic light cable enters the lens at 908 and itsinteraction with adjacent instruments is severelylimiting, even prohibitive.

e u r o p e a n u r o l o g y 5 4 ( 2 0 0 8 ) 1 0 2 0 – 1 0 3 0 1027
Using instruments of differential overall lengthsis also helpful. If one camera and two instrumentsoccupy the multichannel port, varying lengthsprevent the bulkiest portion of each instrument(the external handle) from overlapping extracor-poreally. We have found, for instance, that using astandard laparoscopic grasper and a bariatric suc-tion cannula, which is longer than the standardlength lap instruments, minimizes external clashingto some degree. In addition, a vigilant cameracontroller anticipates clashing and chooses analternate camera angle that, like a pair of scissorsopening, moves the camera away from the activesurgical instruments.
4.1.4. Inline vision
During standard laparoscopy, depth perception islost when the camera lines up with the shaft of aworking instrument. This can become an issueduring single-port surgery. The surgeon mustbecome accustomed viewing angles that wouldotherwise seem suboptimal during standard laparo-scopy. The flexible-tip endoscope ameliorates thisproblem to some degree.
4.1.5. Patient-related limitations
Using the umbilicus as the portal of entry limits theappropriate candidates for this approach. For upper-tract surgery in obese patients during standardlaparoscopy, trocars are typically shifted laterallyand are based off of bony landmarks. The umbilicusitself ceases to become a useful landmark becauseits distance to the target organ increases; for thisreason, obese patients are not suitable for E-NOTES.Similarly, the umbilicus in tall patients may be toofar from the upper pole of the kidney. Suchconsiderations would play a role in patient selection.An umbilical hernia is not a contraindicationbecause direct umbilical access affords the oppor-tunity for simultaneous hernia repair.
These challenges underscore the need for tech-nical facility and broad experience with standardmultiport laparoscopy as a prerequisite to attempt-ing E-NOTES procedures.
4.1.6. Future instrumentation
Early experience demonstrates that specific areasexist for task-specific instrument development.Currently, large external movements are requiredfor internal maneuvering, causing instrumentclashing. Robotic or motorized instruments couldaddress this problem, since fine movements wouldbe generated at the instrument tip itself. Instru-mentation with low-profile, streamlined handpieceswould also address issues of extracorporeal crowd-
ing. Flexible instrumentation must be refined;currently, force applied to the instrument tipdissipates along the flexible portion of the shaft,limiting some maneuvers during blunt dissection.
4.2. Impact on standard laparoscopy
Single-port laparoscopy has had a positive effect onstandard laparoscopy. Undoubtedly, single-portlaparoscopy, even with flexible instrumentation, istechnically more challenging than straight laparo-scopy; however, we are still in the initial learningcurve. This new technique of single-port surgery hasbrought to light various superfluous aspects ofstandard laparoscopy and seems to have facilitatedthese cases as well. Instead of routinely placingancillary assistant ports for upper-tract surgery, forexample, one may substitute a static or dynamicretraction suture or discover that lateral retractionin a given case is unnecessary.
5. Conclusions
As with many surgical leaps forward, one needssimply to look back in history to find wheels beingreinvented as themes repeat. The same is true for E-NOTES, where we now walk on a previously troddenpath. Our gynecology colleagues paved the wayalmost 40 yr ago, having performed thousands ofvirtually scar-free tubal ligations. These were indeedthe first E-NOTES procedures, complete with con-comitant manipulation of the uterus using thevaginal natural orifice—and all of this beforestandard multiple-trocar laparoscopy was even inour collective consciousness. Without mainstreamstandard laparoscopy to bolster its existence, how-ever, it would take many years for single-portsurgery to reappear in published series.
After the pioneering efforts in single-port gyneco-logic surgery, such procedures took little foothold.Instrumentation to perform complex maneuversintracorporeally did not exist. This accounts forseveral reports of single-port surgery that can bestbe regardedas hybrid reports, in which thepathologictarget organ was exteriorized through the umbilicusand extracorporeal open surgery was performed[11,15,17]. Several decades would pass before flexibleinstrumentation caught up with the surgical concept.
Currently, although the cosmetic benefit is appar-ent, the true impact of E-NOTES on perioperativepain and morbidity are not known. Patient attitudesaboutscar-free surgeryhavealso notbeen quantified.Cost differences between single- and multiple-portlaparoscopy are being studied but are not yet known.

e u r o p e a n u r o l o g y 5 4 ( 2 0 0 8 ) 1 0 2 0 – 1 0 3 01028
The incremental benefit in morbidity is not likely tomatch that seen with the jump from open toconventional laparoscopic surgery. This, however,is no justification for accepting the status quo. Aprospective multi-institutional clinical trial compar-ing E-NOTES to standard laparoscopy is essential todiscern whether incremental benefits exist.
Flexible multichannel robotic systems and stand-alone deployable miniature robots are not far off.When these technologies become widely available,both E-NOTES and NOTES procedures will advanceeven further. Currently, careful case selection isparamount so that these procedures can be exploredsafely, with a low threshold to convert to standardlaparoscopy as indicated for safety and quality ofcare.
Author contributions: David Canes had full access to all the data
in the study and takes responsibility for the integrity of the
data and the accuracy of the data analysis.
Study concept and design: Gill, Desai, Kaouk, Canes.
Acquisition of data: Canes, Goel, Aron, Stein.
Analysis and interpretation of data: Canes, Haber.
Drafting of the manuscript: Canes, Gill, Desai.
Critical revision of the manuscript for important intellectual content:
Canes, Gill.
Statistical analysis: None.
Obtaining funding: None.
Administrative, technical, or material support: None.
Supervision: None.
Other (specify): None.
Financial disclosures: I certify that all conflicts of interest,
including specific financial interests and relationships and
affiliations relevant to the subject matter or materials
discussed in the manuscript (eg, employment/affiliation,
grants or funding, consultancies, honoraria, stock ownership
or options, expert testimony, royalties, or patents filed,
received, or pending), are the following: None.
Funding/Support and role of the sponsor: None.
References
[1] Soble JJ, Gill IS. Needlescopic urology: incorporating 2-mm
instruments in laparoscopic surgery. Urology 1998;52:
187–94.
[2] Mostafa G, Matthews BD, Sing RF, Kercher KW, Heniford
BT. Mini-laparoscopic versus laparoscopic approach to
appendectomy. BMC Surg 2001;1:4.
[3] Bisgaard T, Klarskov B, Trap R, Kehlet H, Rosenberg J.
Microlaparoscopic vs conventional laparoscopic chole-
cystectomy: a prospective randomized double-blind trial.
Surg Endosc 2002;16:458–64.
[4] Wheeless CR. A rapid, inexpensive and effective method
of surgical sterilization by laparoscopy. J Reprod Med
1969;3(5):65–9.
[5] Wheeless CR. Outpatient laparoscope sterilization under
local anesthesia. Obstet Gynecol 1972;39:767–70.
[6] Wheeless Jr CR, Thompson BH. Laparoscopic sterilization.
Review of 3600 cases. Obstet Gynecol 1973;42:303–6.
[7] Singh KB. Tubal sterilization by lararoscopy. Simplified
technique. N Y State J Med 1977;77:194–6.
[8] Pelosi MA, Pelosi 3rd MA. Laparoscopic hysterectomy with
bilateral salpingo-oophorectomy using a single umbilical
puncture. N J Med 1991;88:721–6.
[9] Pelosi MA, Pelosi 3rd MA. Laparoscopic supracervical
hysterectomy using a single-umbilical puncture (mini-
laparoscopy). J Reprod Med 1992;37:777–84.
[10] Pelosi MA, Pelosi 3rd MA. Laparoscopic appendectomy
using a single umbilical puncture (minilaparoscopy).
J Reprod Med 1992;37:588–94.
[11] D’Alessio A, Piro E, Tadini B, Beretta F. One-trocar trans-
umbilical laparoscopic-assisted appendectomy in chil-
dren: our experience. Eur J Pediatr Surg 2002;12:24–7.
[12] Ates O, Hakguder G, Olguner M, Akgur FM. Single-port
laparoscopic appendectomy conducted intracorporeally
with the aid of a transabdominal sling suture. J Pediatr
Surg 2007;42:1071–4.
[13] Navarra G, Pozza E, Occhionorelli S, Carcoforo P, Donini I.
One-wound laparoscopic cholecystectomy. Br J Surg
1997;84:695.
[14] Piskun G, Rajpal S. Transumbilical laparoscopic cholecys-
tectomy utilizes no incisions outside the umbilicus.
J Laparoendosc Adv Surg Tech A 1999;9:361–4.
[15] Kosumi T, Kubota A, Usui N, Yamauchi K, Yamasaki M,
Oyanagi H. Laparoscopic ovarian cystectomy using a sin-
gle umbilical puncture method. Surg Laparosc Endosc
Percutan Tech 2001;11:63–5.
[16] Ghezzi F, Cromi A, Fasola M, Bolis P. One-trocar salpin-
gectomy for the treatment of tubal pregnancy: a ‘marion-
ette-like’ technique. BJOG 2005;112:1417–9.
[17] Cobellis G, Cruccetti A, Mastroianni L, Amici G, Martino A.
One-trocar transumbilical laparoscopic-assisted manage-
ment of Meckel’s diverticulum in children. J Laparoen-
dosc Adv Surg Tech A 2007;17:238–41.
[18] Blessing Jr WD, Ross JM, Kennedy CI, Richardson WS.
Laparoscopic-assisted peritoneal dialysis catheter place-
ment, an improvement on the single trocar technique.
Am Surg 2005;71:1042–6.
[19] Goitein D, Papasavas P, Gagne D, Ferraro D, Wilder B,
Caushaj P. Single trocar laparoscopically assisted place-
ment of central nervous system-peritoneal shunts.
J Laparoendosc Adv Surg Tech A 2006;16:1–4.
[20] Gettman MT, Box G, Averch T, et al. Consensus statement
on natural orifice transluminal endoscopic surgery and
single-incision laparoscopic surgery: heralding a new era
in urology? Eur Urol 2008;53:1117–20.
[21] Zeltser IS, Bergs R, Fernandez R, Baker L, Eberhart R,
Cadeddu JA. Single trocar laparoscopic nephrectomy
using magnetic anchoring and guidance system in the
porcine model. J Urol 2007;178:288–91.
[22] Rane A, Kommu S, Eddy B, Bonadio F, Rao P, Rao P. Clinical
evaluation of a novel laparoscopic port (R-port) and evo-
lution of the single laparoscopic port procedure (SLiPP).
J Endourol 2007;21(Suppl 1):A22–3.

e u r o p e a n u r o l o g y 5 4 ( 2 0 0 8 ) 1 0 2 0 – 1 0 3 0 1029
[23] Raman JD, Bensalah K, Bagrodia A, Stern JM, Cadeddu JA.
Laboratory and clinical development of single keyhole
umbilical nephrectomy. Urology 2007;70:1039–42.
[24] Desai MM, Rao PP, Aron M, et al. Scarless single port
transumbilical nephrectomy and pyeloplasty: first clini-
cal report. BJU Int 2008;101:83–8.
[25] Kaouk JH, Haber GP, Goel RK, et al. Single-port laparo-
scopic surgery in urology: initial experience. Urology
2008;71:3–6.
[26] Goel RK, Kaouk JH. Single port access renal cryoablation
(SPARC): a new approach. Eur Urol 2008;53:1204–9.
[27] Gill IS, Canes D, Aron M, et al. Single port transumbilical
(E-NOTES) donor nephrectomy. J Urol 2008;180:637–41.
Editorial Comment on: Transumbilical Single-Port Surgery: Evolution and Current StatusRichard ZigeunerDepartment of Urology, Medical University Graz, Graz,[email protected]
In this review article [1], the authors report onfurther progress in the rapidly evolving field oflaparoscopy. Transumbilical single-port surgery,also referred to as embryonic natural orificetransumbilical endoscopic surgery (E-NOTES), hasbeen performed only in a limited number of patientsso far; the authors’ institution is the most experi-enced. Despite this fact, the authors critically reflecton the question of true clinical advantages ofE-NOTES without exaggerated enthusiasm. Theprocedures are more technically challenging, evenin the hands of very experienced laparoscopists,which may limit the widespread use of the method.The very timely issue of cost-effectiveness com-pared to standard laparoscopy cannot currently beclarified because data are lacking; however, highercosts may be expected due to the requirement ofmore sophisticated instruments. Most importantly,because this novel method is in its infancy, we haveno information about whether technical progresswill translate into patient benefit. Using E-NOTES,separate incisions for additional trocars can bespared, but the incision must still be enlarged forkidney retrieval after nephrectomy. There is nodoubt that laparoscopy has brought relevant benefitfor patients, as proven in prospective trials in renalsurgery [2,3]. With regard to prostatectomy, theother widely used laparoscopic procedure in urol-ogy, the real clinical advantage of laparoscopy overopen surgery has not been proven [4,5]. Despite the
[28] Kaouk JH, Palmer JS. Single-port laparoscopic surgery:
initial experience in children for varicocelectomy. BJU
Int 2008;102:97–9.
[29] Desai MM, Stein RJ, Rao P, et al. E-NOTES (embryonic
natural orifice surgery) for advanced reconstruction:
initial experience. Urology. In press.
[30] Kaouk JH, Goel RK. Single port laparoscopic pelvic surgery:
a scar-less approach. Abstract presented at: Annual Meet-
ing of the Society of Gastrointestinal and Endoscopic Sur-
geons; April 9–12, 2008; Philadelphia, PA, USA. Abstract 201.
[31] Kawahara H, Kubota A, Okuyama H, et al. One-trocar
laparoscopy-aided gastrostomy in handicapped children.
J Pediatr Surg 2006;41:2076–80.
absence of any prospective randomised data prov-ing superiority of laparoscopy over the openapproach, laparoscopic and robotic prostatectomiesare increasingly performed worldwide, even againstthe background of published disadvantages regard-ing higher incontinence and readmission rates [5].Consequently, the scientific urologic communityhas to maintain critical assessment of any novelmethods, even against pressure from industry andmarketing. As the authors correctly state, prospec-tive trials comparing E-NOTES to conventionallaparoscopy are essential to prove clinical advan-tages.
References
[1] Canes D, Desai MM, Aron M, et al. Transumbilical single-
port surgery: evolution and current status. Eur Urol
2008;54:1020–30.
[2] Rassweiler J, Gumpinger R, Miller K, Holzermann F,
Eisenberger F. Multimodal treatment (extracorporeal
shock wave lithotripsy and endourology) of complicated
renal stone disease. Eur Urol 1986;12:294–304.
[3] Fornara P, Doehn C, Seyfarth M, Jocham D. Why is
urological laparoscopy minimally invasive? Eur Urol
2000;37:241–50.
[4] Jurczok A, Zacharias M, Wagner S, Hamza A, Fornara P.
Prospective non-randomized evaluation of four media-
tors of the systemic response after extraperitoneal
laparoscopic and open retropubic radical prostatec-
tomy. BJU Int 2007;99:1461–6.
[5] Touijer K, Eastham JA, Secin FP, et al. Comprehensive
prospective comparative analysis of outcomes between
open and laparoscopic radical prostatectomy conducted
in 2003 to 2005. J Urol 2008;179:1811–7.
DOI: 10.1016/j.eururo.2008.07.010
DOI of original article: 10.1016/j.eururo.2008.07.009

Editorial Comment on: Transumbilical Single-Port Surgery: Evolution and Current StatusJens RassweilerDepartment of Urology, SLK Kliniken Heilbronn,D-74076 Heilbronn, [email protected]
Canes and colleagues focus our attention on afurther modification of laparoscopic surgery: thetransumbilical single-port surgery [1]. Their histor-ical overview demonstrates clearly that this is anold technique pioneered by gynecologists in the1960s using an operative laparoscope with an offseteyepiece comparable to the rigid nephroscopesused during percutaneous renal surgery [2,3].However, in the year 2008, it seems that thingshave to be more fancy.
Whereas laparoscopists initially used the umbi-licus as an easy-to-hide entrance for the trocar, inthe era of natural orifice transluminal endoscopicsurgery (NOTES), the umbilicus has gained moreimportance, being recognized as an ‘‘embryonicnatural orifice.’’ This has resulted in the new term‘‘E-NOTES.’’
But the reader should be aware of the distinctdifferences between NOTES and the transumbilicallaparoscopic single port technique. NOTES hasbeen pioneered by gastroenterologists and sur-geons who used the technology of a flexiblegastroscope with different working channels toperforate the stomach and then to reach theperitoneal cavity. In the peritoneal cavity, complexprocedures such as appendectomy and cholecys-tectomy have been carried out using specializedflexible endoscopes and devices (ie, intraluminalclip appliers). After transoral removal of the organ,the gastric wall was closed with intraluminalsuturing techniques [4].
Single-port surgery is completely different andgoes back to the operative resectoscope developedby Buess in the 1980s for transanal endoscopicmicrosurgery [5]. This device consists of a recto-scope 40 mm in diameter with up to five ports forinsertion of the telescope and curved instruments.
The principle of this device has been modified fortransumbilical laparoscopy with three ports forinsertion of a rigid or flexible telescope and flexibleor bent instruments.
Although the necessity and importance of anoperative nephroscope, a complex gastro- orcoloscope, and an operative resectoscope has beenproven over decades for intraluminal surgery, therole of such devices for transluminal and laparo-scopic surgery remains uncertain. It is impressiveto see what type of laparoscopic procedures havebeen carried out, but in my view, there is still noargument for not using the standard trocartechnique, which provides efficient solutions tothe main problems of E-NOTES, such as triangula-tion, retraction, instrument crowding, and in-linevision. However, endoscopic surgey will definitelybenefit from the technological input (ie, flexibleinstruments, staplers) of these ‘‘new old’’ techni-ques.
References
[1] Canes D, Desai MM, Aron M, et al. Transumbilical single-
port surgery: evolution and current status. Eur Urol
2008;54:1020–30.
[2] Rassweiler J, Gumpinger R, Miller K, Holzermann F,
Eisenberger F. Multimodal treatment (extracorporeal
shock wave lithotripsy and endourology) of complicated
renal stone disease. Eur Urol 1986;12:298–304.
[3] Wheeless CR. A rapid, inexpensive and effective method
of surgical sterilization by laparoscopy. J Reprod Med
1969;5:255–7.
[4] Kalloo AN, Singh VK, Jagannath SB, Niiyama H, Hill SL,
Vaughn CA. Flexible transgastric peritoneoscopy: a
novel approach to diagnostic and therapeutic interven-
tions in the peritoneal cavitiy. Gastointest Endosc
2004;60:114–7.
[5] Buess G, Kipfmuller K, Hack D, Grussner R, Heintz A,
Junginger T. Technique of transanal endoscopic micro-
surgery. Surg Endosc 1988;2:71–5.
DOI: 10.1016/j.eururo.2008.07.011
DOI of original article: 10.1016/j.eururo.2008.07.009
e u r o p e a n u r o l o g y 5 4 ( 2 0 0 8 ) 1 0 2 0 – 1 0 3 01030
Related Documents