Translational Research For Interventional Neurologists Dileep R. Yavagal, MD Director Interventional Neurology Co-Director Endovascular Neurosurgery Jackson Memorial Hospital Associate Professor, Neurology & Neurosurgery University of Miami Miller School of Medicine Faculty, Interdisciplinary Stem Cell Institute SVIN Annual Meeting, November 8 th , 2014, Hollywood, FL

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

Translational Research For Interventional
Neurologists
Dileep R. Yavagal, MD Director Interventional Neurology
Co-Director Endovascular Neurosurgery Jackson Memorial Hospital
Associate Professor, Neurology & Neurosurgery University of Miami Miller School of Medicine Faculty, Interdisciplinary Stem Cell Institute
SVIN Annual Meeting, November 8th, 2014, Hollywood, FL

Dileep R. Yavagal, MD
Clinical Trial Steering Committee Member:
1. Recover-Stroke ( Sponsor: Cytomedix Aldagen)
2. SWIFT-PRIME ( Sponsor: EV3)
Consultant:
1. Aldagen/Cytomedix
2. EV3/Covidien
3. Stryker
Financial Disclosures

Funding
UM Endovascular Stroke Translational Research
Laboratory
• 1. Department of Neurology, University of Miami: 2008-2010
• 2.Interdepartmental Research Development Initiative (IRDI) grant: 2009-2010
• 3. Anderson Family Gift : 2009-2010, 2013-2015
• 4. Florida Biomedical New Investigator Grant: 2011-2014
• 5. CTSI NIH Grant: Jan 2013-May 2014

Synopsis
• Why Translational Research
• Personal Story
– Promise of Stem Cells in Stroke from the
Laboratory
– Translation Data on Intra-arterial MSC’s in
Stroke
– Rise in Early Clinical Trials
– RECOVER-Stroke Clinical Trial

Career Pathway
• Promise of Very Innovative Biomedical Research US Medical System
• Residency: Program Director Input on Academic Career
• Fellowship: Novel large animal model development
• J1-Waiver: No resources for Translational Research but avoid loss of focus
• University of Miami: – Small Start-up Package and Seed funding
– Non-NIH Intra-mural Grants
– NIH grant
– Industry Collaboration
– Philanthrophy

Why Translational Research

Why Translational Research
• Different things to different
people
• the “bench-to-bedside”
enterprise of harnessing
• knowledge from basic
sciences to produce new
drugs, devices,
• and treatment options for
patients.
• the interface between basic
science and clinical
• medicine
• the end point is the production
of a promising new treatment.
• “effective translation of
the new knowledge,
mechanisms, and
techniques generated
by advances in basic
science research into
new approaches for
prevention, diagnosis,
and treatment of
disease is essential for
improving health.”

Why Translatational Research
• NIH has made translational research a priority
• centers of translational research the Clinical and Translational Science Award
• (CTSA) program in 2006.
• 24 CTSA-funded academic by 2008
• By 2012, the NIH expects to fund 60 such centers with a
• budget of $500 million per year.
• foundations, industry, disease-related organizations, and
• individual hospitals and health systems have also established
• translational research
• European Commission’s €6 billion budget for health related
• research,
• United Kingdom has invested £450
• million over 5 years to establish translational research

Need for Novel Class of Stroke
Therapies
• IV tPA prevents disability in only 6/1000
patients
• Over 100 clinical trials of neuroprotection
agents in stroke have failed
• Endovascular Acute Stroke Therapy when
standard of care may only reach 20% of
ischemic stroke cases due to limited time
window

IA vs IC vs IV cell delivery: Timing of
migration and distribution of Cells

Dileep R. Yavagal, MD
Biodistribution of cells in IA vs IV delivery
Stroke 2010;41;2064-2070 Pendharkar et
al

Intra-carotid NSCs at 48 hours post
mouse hypoxia-ischemic model • Guzman et al. Stroke 2008;39;1300-1306

Acute administration of MSCs post recanalization
• If cells mediate benefit mainly through neuroprotection, acute delivery to maximize chances of tissue salvage
• Challenges: excitotoxicity, peri-infarct depolarization, reactive O2 species release

Intra-arterial delivery of Stem Cells in Stroke
Walczak et al. Stroke 2008;39;1569-1574

Methods
• Female Sprague-Dawley rats 250-300 g
• 90 min suture induced reversible MCA occlusion (rMCAO)
• At 60 min post recanalization: Intra-carotid (IC) injection of vehicle or allogenic male rat MSCs in escalating dose groups
• Continuous Laser doppler flow signal (LDFS) monitoring over ipsilateral cortex
Longa et al. Stroke 1989;20:84-
91

Ultramicrospy: IA allogenic cGFP
MSCs, day 1 post injection
Control Day 1 post IA
MSCs


May 7th, 2014

CBF worsening is normalized on dose-de-escalation to 1 x 10^5 MSCs
-80
-60
-40
-20
0
20
40
LD
FS
Re
lati
ve
Ch
an
ge
(%
), 9
5%
CI
Placebo
(n=11)
5 x 104
(n=7)
2 x 105
(n=5)
1 x 105
(n=7)
1 x 106
(n=7)
5 x 105
(n=6)
p<0.05

Cerebro-Microvascular MSC
Transport: Diapedesis
a 10 μm b c 10 μm 10 μm

Pre-Clinical Efficacy Study
Reperfusion
90’ 60’ or 24h
Post-injection
Real time laser-Doppler flowmetry (LDF)
Neurodeficit assessment At 1, 7, 14, 21 and 28 days rMCAo
Injection
A
C

4
6
8
10
12
14
16
Day 1 Day 7 Day 14 Day 21 Day 28
Me
an
ND
Sc
ore
, 9
5%
CI
IC_PBS_24h IV_MSCs_24h IC_MSCs_1h IC_MSCs_24h
p=.49
p=.02p=.01
p=.003p<.0001
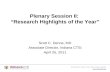
Significant Functional Benefit with
24h_IC MSC

Infarct Volume Is Significantly lower
in IC_MSC_24h
0
20
40
60
80
100
120
140
IC_PBS_24h (n=5) IC_MSCs_1h (n=5) IV_MSCs_24h (n=8) IC_MSCs_24h (n=9)
Infa
rct
volu
me
(mm
^3)
, 95%
CI
p=.01

PBS-control (n=5) MSCc-treated (n=9) Fisher’s Exact Test
Infarction frequency map and
Statistical comparison


Howells et al. J Cereb Blood Flow Metab. 2010
August; 30(8): 1412–1431

Unique Advantages of Large
Animal Studies
• Route of Cell Administration
• Cell dose finding
• Cell Tracking in a larger brain
• DTI in larger brain ?

Canine Neurovascular Anatomy

Dog CCA bifurcation

Superselective catheterization of ICA


Yavagal et al, SVIN 4th Annual Meeting
Canine Endovascular MCA occlusion
Model

MRA COW

TCD Velocities over Canine
MCA’s during IC MSC injection
34
rMCAo
Post
rMCAo
During IA
delivery
of 10 x
106
MSCs
Post IA
MSCs
LMCA RMCA RMCA LMCA

D10-009; subacute IA 10 x 106
MSCs
48 hrs post
stroke
FLAIR
29 days
post stroke
FLAIR

D10-011; subacute IA 10x 106 MSCs
48 hrs post
stroke
FLAIR
21 days
post
stroke
FLAIR

D10-002; treatment with IV
5 x 106 MSCs
3 day post
stroke T2
58 day post
stroke T2

Study/
Countr
y
Type of
stroke
Design No.
of
patie
nts
Cell type Timing of
IA
delivery
Dose Follow-
up
Mendonca
2006;
Correa
2007/Brazil
MCA
ischemic
stroke
Case
reports on
phase I,
nonrandomi
zed, open
label
2 (no
controls)
Auto BM-
MNCs
5d & 9d 1 x 108 (1
pt.) and
3 x107 (1
pt.)
2-4 mo
Battistella
2011;
Rosadode-
Castro,
2013/Brazil
MCA
ischemic
stroke
Phase I,
nonrandomi
zed,
open label
12 (no
controls)
Auto BM-
MNCs
19-89 d (mean
64.5d)
1 x 108 to 5
x108
(mean 3.1
x 108)
6 mo
Friedrich,
2012/Brazil
MCA
ischemic
stroke
Phase I/II,
nonrandomi
zed,
single-blind
(CT)
20 (no
controls)
Auto BM-
MNCs
3 -10 days
(mean 6 d)
5 .1 x 107
to 6 x108
(mean 2.2
x108)
6 mo
Moniche et
al.,
2012/Spain
MCA
ischemic
stroke
Phase I/II,
nonrandomi
zed,
single-blind
10 (10
controls)
Auto BM-
MNCs
5 -9d (mean
6.4 d)
mean 1.6 x
108
6mo
Jiang et
al., 2012/
China
MCA
ischemic
(3)
hemorrhagic
(1) stroke
Phase I,
nonrandomi
zed,
open
label
4 ( no
controls)
Allogeneic
UC-MSCs
11 to 50 days
(mean 25.5)
2 · 107 6 mo
Intra-arterial Stem Cell Clinical Trials, Published

Clinial Trial of Autologous Marrow Cell in
Stroke • Phase 1 / 2 Study of ALD-401 Via
Intracarotid Infusion in Ischemic Stroke Subjects – Randomized trial of Autologous stem cells
– 2 weeks (13-19 days) post stroke
– 100 patients
– IA delivery within 48 hours of bone marrow harvest
– Safety endpoints: Clinical AE’s and SAE’s
– Efficacy endpoints: Clinical functional recovery scales at 90 days, 6 mo and 12 months
RECOVER-Stroke:

Multistem: Stroke Stem Cell Trial
at JMH and UMH
• Double-Blind, Randomized, Placebo-Controlled Phase 2
Safety and Efficacy Trial of MultiStem® in Adults With Ischemic Stroke
• Intravenous Bone marrow stem cells from healthy donors
• Given within 48 hours of stroke symptom onset

Patient Eligibility: Key Criteria
1. 18-83 years of age
2. Cortical MCA cerebral ischemic stroke
3. NIHSS 8-20
4. Onset of Stroke must have occurred within 24-48 hours
5. Acute cortical lesion measuring ≥ 5mL and ≤ 100mL
6. Subjects who received tPA or mechanical thrombectomy are allowed
• If they do, we are happy to transfer the patient preferably before the the 24 hour mark to allow us time for enrollment procedures and infusion of the stem cells (off the shelf from healthy donors bone marrow) before 48 hours from stroke symptom onset.

Acknowledgements
Tienlong Pham, Philip Garza, BS, Baowan Lin, MD,
Dalia Milan, Ami Raval PhD, Pedro Cifuentes, MD
• Mentors:
Joshua Hare, MD
Miguel Perez-Pinzon, PhD Tanja
Rundek, MD, PhD
• Collaborator:
Ami Raval, PhD
• Biostatistics:
Chanhui Dong, PhD
• Rat and Canine MSCs:
Aisha Khan
Ian McNiece PhD,
ISCI, University of Miami

Thank you!
Related Documents