Translating Clinical Trial Data into the Community Setting: A Case-Based Approach to Metastatic Colorectal Cancer—Overview Axel Grothey, MD Professor of Oncology Department of Oncology Mayo Clinic, College of Medicine Rochester, Minnesota

Translating Clinical Trial Data into the Community Setting: A Case- Based Approach to Metastatic Colorectal Cancer—Overview Axel Grothey, MD Professor.
Dec 26, 2015
Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

Translating Clinical Trial Data into the Community Setting: A Case-Based Approach to Metastatic Colorectal Cancer—Overview
Axel Grothey, MDProfessor of Oncology
Department of OncologyMayo Clinic, College of Medicine
Rochester, Minnesota

RegimenFirst Line
Second Line
FDA Approval Year
5-FU √ √ 1962
Irinotecan (monotherapy) √ 1996
IFLa √ 2000
Capecitabine (monotherapy) √ 2001
Oxaliplatin + infusional 5-FU/LVb √ √Second line 2002
First line 2004
Cetuximab (with or without irinotecan) √ 2004
Bevacizumab + IV 5-FU-based regimensc √ √First line 2004
Second line 2006
Panitumumab (single agent) Salvage 2006
Venook A. Oncologist. 2005;10:250.
New Agents Have Significantly Improved Treatment and Patient Outcomes
More regimens provide more options formultiple lines of therapy to extend survival
a FOLFIRIb FOLFOXc IFL, FOLFIRI, FOLFOX, and FU/LV 5-FU = 5-fluorouracil; IFL = irinotecan+5-FU+leucovorin; LV = leucovorin.

NCCTG/Intergroup Trial N9741Efficacy
Goldberg RM, et al. J Clin Oncol. 2004;22:23.
15
19.5(P = .0001)
6.9
8.7(P = .0014)
0
5
10
15
20
25
IFL FOLFOX IFL FOLFOX
Med
ian
Mo
nth
s
Overall Survival Progression-Free Survival
Response rate: IFL 31%, FOLFOX 45% (P = .002)
NCCTG = North Central Cancer Treatment Group; IFL = irinotecan + 5-FU + leucovorin;FOLFOX = leucovorin + 5-FU + oxaliplatin.

Tournigand Trial (N = 220)
FOLFOXFOLFOX FOLFIRI FOLFIRI FOLFOXFOLFOX (1st line 2nd line) (1st line 2nd line)
111 69 109 81
RR 54% 4% 56%15%
Resection ofhepatic metastases 21%21% 9%
PFS (mo) 8.0 2.5 8.5 4.2
Median OS (mo) 20.6 21.5 Tournigand C, et al. J Clin Oncol. 2004;22:229.
2nd line62%
2nd line74%
No. Patients
FOLFOX = leucovorin + 5-FU + oxaliplatin; FOLFIRI = leucovorin + 5-FU + irinotecan;RR = response rate; PFC = progression-free survival; OS = overall survival.

Different Philosophies…
Piling up
Sequencing
FOLFOXIRIPACCE
FOCUSCAIRO
Courtesy of Dr. A. Grothey.

CAIRO—Trial Design
Arm A Arm B
Randomize
CapecitabineN = 397
Capecitabine +oxaliplatin
N = 143 (36%)
IrinotecanN = 251 (62%)
Capecitabine +oxaliplatin
N = 213 (53%)
Capecitabine +irinotecan
N = 398
1st line
2nd line
3rd line
Courtesy of Dr. C.J. Punt.

CAIRO—Overall Survival
Reprinted from Koopman M, et al. Lancet. 2007;370:135, with permission from Elsevier.
Median OS17.4 vs 16.3 mo

Phase III Trial of FOLFOXIRI vs FOLFIRI as First-Line Therapy of Advanced Colorectal Cancer
FOLFIRIN = 122
FOLFOXIRIN = 122
P-value
RRa (%) 34 60 <.0001
CR+PR+SDa (%) 68 81 N/A
R0 resection (%) (all patients)
6 15 .033
R0 resection (%) (liver limited)
12 36 .017
PFS (mo) 6.9 9.8 .0006
OS (mo) 16.7b 22.6 .032aExternally reviewed; b67% 2nd line FOLFOXRR= Response Rate; CR= Completed Response; PR= Partial Response; SD= Stable Disease
Falcone A, et al. J Clin Oncol. 2007;25:1670.

Concept of “All 3 Drugs”—Update 200511 Phase III Trials, 5768 Patients
OS (mo) = 13.2 + (% 3 drugs x 0.1), R^2 = .85Grothey A, Sargent D. J Clin Oncol. 2005;23:9441.
0 10 20 30 40 50 60 70 80
Infusional 5-FU/LV + irinotecanInfusional 5-FU/LV + oxaliplatinBolus 5-FU/LV + irinotecanIrinotecan + oxaliplatinBolus 5-FU/LV LV5FU2
FOLFOXIRI
CAIRO
22
21
20
19
18
17
16
15
14
13
12
Med
ian
OS
(m
o)
Patients with 3 Drugs (%)
P = .0001
First-Line Therapy
Multivariate analysis:Effect on OS P
First-line doublet .69All 3 drugs .005
2007

mAbs Target Tumor Cell-Bound EGFR
MetastasisAngiogenesis
Cell survival
Extracellular
Intracellular
Ligand
EGF-R
PI3K
Akt
Ras
Raf
MEK
MAPK
Cell motility
Proliferation
DNA
Courtesy of Dr. A. Grothey.

NCIC CTG CO.17—Cetuximab vs BSCProgression-Free Survival
CETUXIMAB + BSCCENSORED
BSCBSCCENSOREDCENSORED
Pro
po
rtio
n P
rog
ress
ion
-Fre
e
0.00.0
0.10.1
0.20.2
0.30.3
0.40.4
0.50.5
0.60.6
0.70.7
0.80.8
0.90.9
1.01.0
Months
00 33 66 99 1212 1515
HR 0.68HR 0.68 (95% CI = 0.57–0.80)
PP-value < .0001-value < .0001
Study ArmStudy Arm Med PFS Med PFS 95% CI95% CI
Cetuximab + BSCCetuximab + BSC 1.91.9 1.8–2.11.8–2.1
BSC aloneBSC alone 1.81.8 1.8–1.91.8–1.9
Reprinted from Jonker DJ, et al. N Engl J Med. 2007;357(20):2040-2048, with permission from the Massachusetts Medical Society.
OS 6.1 vs 4.6 moHR 0.77, P = .0046(NO cross-over)

CRYSTAL Study—First-Line
Patients with EFGR+ mCRCa
Randomized to
FOLFIRI FOLFIRI+ Cetuximab (n = 599) (n = 599)
Primary endpoint: PFS (independent review) Secondary endpoints: RR, DCR, OS, safety, QOL RR, DCR, OS, safety, QOL
a Stratified by region, ECOG PSVan Cutsem E, et al. ASCO; June 1-5, 2007. Abstract 4000. Courtesy of Dr. E. Van Cutsem.

CRYSTAL Trial—Primary Endpoint=PFS ITT Population Independent Review
Progression-Free Survival Time (months)
Pro
gre
ssio
n-F
ree
Su
rviv
al E
stim
ate
1.0
0.8
0.9
0.0
0.1
0.2
0.3
0.4
0.5
0.6
0.7
0 2 4 6 8 10 12 14 16 18 20
8.9 mo
8.0 mo
FOLFIRI
FOLFIRI + cetuximab
1- y PFS rate23% vs 34%
Van Cutsem E, et al. ASCO; June 1-5, 2007. Abstract 4000. Courtesy of Dr. A. Grothey.
HR = 0.851 P = .0479
RR
46.9%
38.7%
P = .0038

mAbs Target Tumor Cell-Bound EGFR
Cell survival
Extracellular
Intracellular
Ligand
EGF-R
PI3K
Akt
Raf
MEK
MAPK
Cell motility
MetastasisAngiogenesis
Proliferation
DNA
Ras
Courtesy of Dr. A. Grothey.

K-ras as Biomarker for Panitumumab Response in Metastatic CRC
Amado RG, et al. ECCO; December 8-11, 2007. Abstract 0007. Courtesy of Dr. RG Amado.
• PFS log HR significantly different depending on K-ras status (P <.0001)• Percentage decrease in target lesion greater in patients with wild-type K-ras receiving panitumumab
Patients with Mutant K-ras
Mean(Wk)
Stratified log rank test: P < .0001
115/124 (93)
Patients with Wild-Type K-ras
1.0
0.9
Pro
po
rtio
n w
ith
PF
S
0.8
0.70.60.50.4
0.3
0.20.1
00 2 4 6 8 10
Events/No. (%)Median
(Wk)
Pmab + BSCBSC alone
114/119 (96)
12.37.3
19.09.3
HR: 0.45 (95% CI: 0.34–0.59)
12 14 16 18 20 22 24 26 28 30 32 3436 38 4042 44 46 48 50 52
Weeks
Pro
po
rtio
n w
ith
PF
S
1.0
0.90.8
0.70.60.50.4
0.30.20.1
00 2 4 6 8 10 12 14 16 18 20 22 24 26 2830 32 3436 38 4042 44 46 48 50
Weeks
Pmab + BSCBSC alone Mean
(Wks)
76/84 (90)
Events/No. (%)Median(Wks)
95/100 (95)
7.47.3
9.910.2
HR: 0.99 (95% CI: 0.73–1.36)
52

Anti-VEGF Approaches andAgents—Summary
Reprinted from Kowanetz M, et al. Clin Cancer Res. 2006;12:5018-5022, with permission from the American Association for Cancer Research.
EPC recruitmentMigrationInvasion
Proliferation SurvivalMigration Permeability
LymphangiogenesisVasculogenesis
VEGFR-3VEGFR-2
VEGFR-1
MAPK
MEK
PKC
Akt/PKB
Akt
eNOS
PI3-K
Src
IMC-18F1
BevacizumabVEGF-trap
IMC-1121b
SunitinibVatalanibMotesanib
AxitinibAZD2171
Pazopanib
SunitinibVatalanibSorafenib
VandetanibMotesanib
AxitinibAZD2171
Pazopanib
SunitinibSorafenib
VandetanibMotesanib
AxitinibAZD2171
Pazopanib

Phase III Trial of IFL +/-Bevacizumab in MCRC—Survival
HR = 0.66, P = .00004
Median survival: 15.6 vs 20.3 mo
Duration of survival (mo)
Pro
po
rtio
n s
urv
ivin
g
0.2
200 10 30 400
0.8
1.0
0.4
0.6
Treatment Group
IFL + placeboIFL + bevacizumab
Reprinted from Hurwitz H, et al. N Engl J Med. 2004;350(23):2335-2342, with permission from the Massachusetts Medical Society.

BICC-C—Summary
Period 1 (No BEV) Period 2 (+ BEV)
EfficacyFOLFIRIN = 144
mIFLN = 141
CapIriN = 145
FOLFIRIN = 57
mIFLN = 60
RR (%) 46.6 41.9 38 57.9 53.3
PFS (mo) 7.6 5.9 5.8 11.2 8.3
OS 23.1 17.6 18.9 NR 19.2
G 3/4 (%)
Diarrhea 14 19 48 11 12
Dehydr. 6 7 19 5 2
MI/stroke 0.7 4.4 0 1.8 0
60-d mort. 3.4 5.1 3.5 1.8 6.8
NR = not reached.Fuchs CS, et al. J Clin Oncol. 2007;25:4779.

XELOX + placebo n = 350
FOLFOX4 + placebo n = 351
XELOX + bevacizumab
n = 350
FOLFOX4 + bevacizumab
n = 350
XELOX n = 317
FOLFOX4 n = 317
Initial 2-armopen-label study
(n = 634)
Protocol amended to 2x2 placebo-controlled design after bevacizumab
phase III data became available(n = 1401)
RecruitmentJune 2003–May 2004
RecruitmentFeb 2004–Feb 2005
XELOX vs FOLFOX +/- Bevacizumab Roche NO16966—Study Design
Cassidy J, et al. ASCO; June 1-5, 2007. Abstract 4026. Courtesy of Dr. J. Cassidy.

PFS Chemotherapy + Bevacizumab Primary Objective Met
0 5 10 15 20 25
Months
Pro
gre
ssio
n-F
ree
Su
rviv
al E
stim
ate
HR = 0.83 [97.5% CI 0.72–0.95] (ITT)P =.0023
9.48.0
1.0
0.8
0.6
0.4
0.2
0
FOLFOX+placebo/XELOX+placebo (n = 701; 547 events) FOLFOX+bevacizumab/XELOX+bevacizumab (n = 699; 513 events)
Saltz L, et al. ASCO. June 1-5, 2007. Abstract 4028. Courtesy of Dr. L. Saltz.

NO16966 Study Drug ExposureMedian Months of Treatment
FOLFOX+ Placebo
(n = 336)
FOLFOX+ Bev
(n = 341)
XELOX+ Placebo
(n = 339)
XELOX+ Bev
(n = 353)
Oxaliplatin 6.0 6.0 5.5 5.8
Fluoropyrimidine 6.3 6.7 5.6 6.3
Placebo or bev 6.3 6.0 5.5 6.0
Per protocol, patients discontinuing oxaliplatin could continue with a fluoropyrimidine + placebo or bevacizumab. Patients could also remain on a fluoropyrimidine alone or placebo or bevacizumab alone but not oxaliplatin alone.
Saltz L, et al, Proc Am Soc Clin Oncol. 2007; Abstract 4028. Courtesy of Dr. L. Saltz.

OPTIMOX Studies
OPTIMOX-1n = 620
FOLFOX 4 until TF
FOLFOX 7 FOLFOX 7
sLV5FU2
OPTIMOX-2n = 202
mFOLFOX 7 mFOLFOX 7
sLV5FU2
mFOLFOX 7 mFOLFOX 7
CFIMaindrault-Goebel F, et al. ASCO. June 1-5, 2007. Abstract 4013. Courtesy of Dr. A. Grothey.
Tournigand C, et al. J Clin Oncol. 2006; 22:229.

0 10 20 30 40 500.0
0.2
0.4
0.6
0.8
1.0
26 months
19 months
Maintenance
CFI
P = .0549
Months
OPTIMOX-2—Overall Survival
Lesson from OPTIMOX-2—Don’t stop treatment before progression
Courtesy of Dr. A. Grothey.

PACCE StudyRandomized, Open-Label, Controlled Phase 3b Trial
Stratification factors: ECOG score, prior adjuvant tx, disease site, Ox doses/Iri regimen, number of metastatic organs.
Tumor assessments: q12wk until disease progression or intolerability.
Panitumumab 6 mg/kg q2wk
Ox-CTBevacizumab
Ox-based CT(eg, FOLFOX)
N = 800Inv choice
Iri-basedCT(eg, FOLFIRI)
N = 200Inv choice
Ox-CTBevacizumab
Panitumumab Panitumumab 6 mg/kg q2wk6 mg/kg q2wk
Iri-CTIri-CTBevacizumabBevacizumab
Iri-CTBevacizumab
RANDOMIZE
1:1
1:1
SCREENING
Courtesy of Dr. J. Hecht.
PACCE = Panitumumab Advanced Colorectal Cancer Evaluation.

Months
413 267 92 21 3
410 298 96 21 1
0 5 10 15 20
Pmab+bev/Ox-CT Nbev/Ox-CT N
Patients at risk:
Limited Update of PFS—Ox-CT Cohort(Central Review, Apr 2007 Data Cutoff)
# PFS Events (%)
Median95% CI (mo)
206 (50) 9.0 (8.5–10.4)
172 (42) 10.5 (9.7–11.6)
Pmab+bev/Ox-CT
Bev/Ox-CT
HR = 1.29 (95% CI, 1.05–1.58)
Pro
po
rtio
n P
rog
ress
ion
-Fre
e 100%
90%
80%
70%
60%
50%
40%
30%
20%
10%
0%
ITT setCourtesy of Dr. J. Hecht.

PACCE—Grade 3/4 AEs of InterestOx-CT Cohort
Pmab+bev/Ox-CT, % (n = 401)
bev/Ox-CT, %(n = 392)
Adverse Effects Gr 3 Gr 4 Gr 3 Gr 4
Skin toxicity 33 <1 1 0
Diarrhea 21 2 12 1
Dehydration 14 2 4 1
Hypokalemia 8 2 3 1
Hypomagnesemia 3 1 0 0
Neutropenia 12 10 17 7
Neuropathy 9 <1 10 <1
Nausea 10 0 4 <1
Infectionsa 16 2 7 2
Deep venous thrombosis 6 0 7 0
Pulmonary embolismb 0 6 0 4MedDRA v9.0 preferred terms; Graded per NCI CTCAE v3.0aGrade 5 infections occurred in 2 (1%) pmab + bev/Ox-CT pts and 3 (1%) bev/Ox-CT pts.bGrade 5 pulmonary embolism occurred in 2 (1%) pmab + bev/Ox-CT pts.Courtesy of Dr. J. Hecht.

CALGB/SWOG Intergroup Trial 80405(n = 2289)
“Dealer’s Choice”
FOLFOX or FOLFIRI
Randomize to
Bevacizumab Cetuximab Bevacizumab+
Cetuximab
Primary endpoint: overall survivalHR 1.25 (22 vs 27.5 months)
http://www.cancer.gov protocol ID CALGB-80405

BBP(n = 642)
No BBP(n = 531)
No Post-progression
treatment(n = 253)
Evaluablepatients
(n = 1953)
1st progression(n = 1445)
BRiTE Registry—Patients withBevacizumab Beyond Progression (BBP)
BRiTEN = 1953 1445 pts with 1st progression 932 deaths (1/21/07 cut-off) Median follow-up 19.6 mo
Grothey A, et al. J Clin Oncol. 2008 (in press).
Physician decision—no randomization

BRiTE—Patient Outcome Based on Treatment Post 1st PD
BBP(n = 642)
No BBP(n = 531)
No Post-PD Treatment(n = 253)
Number of deaths (%)
168(66%)
306(58%)
260(41%)
Median OS (mo) 12.6 19.9 31.8
1-year OS rate (%)
52.5 77.3 87.7
OS after 1st PD (mo)
3.6 9.5 19.2
Grothey A, et al. J Clin Oncol. 2008 (in press).
PD = progression; BBP = bevacizumab beyond progression; OS = overall survival.

Multivariate Analysis of Pre- and Post-Treatment Variables on Survival
Grothey A, et al. J Clin Oncol. 2008 (in press).
Hazard Ratio (HR) (95% Cl) P value
Age at 1st PD (per 10 years) 1.04 (0.98, 1.11) .235
ECOG PS0 (n = 632)1 (n = 598) ≥2 (n = 87)
1.0 (reference)1.29 (1.09, 1.52)1.58 (1.20, 2.09)
.003
.001
Albumin, (per g/dL) 0.73 (0.64, 0.32) <.001
Alkaline phosphatase, per (100 U/L) 1.18 (1.12, 1.23) <.001
Site of primary tumor, %
Colon (n = 1137) Rectum (n = 293)
1.0 (reference)0.79 (0.66, 0.97) .024
Exposure to EGFR inhibitors (cetuximaband/or other EGFR monoclonal antibodies) No (n = 884) Yes (n = 542)
1.0 (reference)0.97 (0.81, 1.16) .724
Exposure to all 3 active CT agentsb
No (n = 681) Yes (n = 745)
1.0 (reference)0.93 (0.77, 1.12) .447
Time-To-1st PD, per month 0.91 (0.89, 0.93) <.001
Best 1st-line response CR (n = 156) PR (n = 468) SD (n = 488) PD (n = 314)
1.0 (reference)1.64 (1.14, 2.35)1.62 (1.13, 2.33)1.32 (0.88, 1.97)
.007
.008
.173
Post-1st progression therapy
No BBP (n = 531) BBP (n = 642) No Post-PD treatment (n = 253)
1.0 (reference)0.48 (0.41, 0.57)2.01 (1.61, 2.51)
<.001<.001

SWOG/NCCTG/NCIC 2nd-Line Trial S0600/iBET (Intergroup BEV Continuation Trial)
(FOLF)IRI/C225
MCRC pretreated with
FOLFOX + BEV or CAPOX + BEV orOPTIMOX + BEV
(FOLF)IRI/C225+ BEV 10 mg/kg
n = 1260Primary endpoint: OS (HR 1.30; 12 15.6 mo)Principal Investigators: Gold P, Grothey A
(FOLF)IRI/C225+ BEV 5 mg/kg
Open since June 2007
Courtesy of Dr. A. Grothey.

Patient Potentially Curable?
Induction Ctx (3–4 mo)Eg, FOLF?? + BEV/C225
Surgery with curative intent
“Adjuvant” Ctx
Yes
Yes
Yes
Re-evaluation of resectability
Observation
RRInduction Ctx (3–4 mo)
eg, FOLF?? + BEV
Maintenance
Re-induction Ctx
“All 5 drugs”
No
Evaluation oftumor biology
CFI ??
Time, QOL
Treatm
ent C
on
tinu
umC
ura
tive
Ap
pro
ach
Courtesy of Dr. A. Grothey.

Case Study: Stage IV Metastatic Colon Cancer in a Patient with
Ulcerative Colitis
J. Philip Kuebler, MD, PhDPrincipal Investigator
Columbus Community Clinical Oncology ProgramColumbus, Ohio


Martin
• A 71-year-old man presented with chronic abdominal pain and recent blood in his stool
• There were no changes in bowel habits • He had a history of ulcerative colitis and
associated symptoms• There was no family history of cancer• He was moderately overweight but has no other
medical problems• Physical exam revealed abdominal tenderness

Martin
• An abdominal CT scan showed a large mass in the ascending colon
• The CT scan also showed bilateral masses in his liver• Abdominal and retroperitoneal lymph nodes, as well as
pulmonary nodules, were also present • A liver biopsy was positive for metastatic adenocarcinoma
consistent with a colon primary• After being told surgery was not an option due to the extent
of his disease, he was referred to a medical oncologist

Advances in the Treatment of Colorectal Cancer
1980 1985 1990 1995 2000 2005
Therapeutic concepts
Palliative CT
Adjuvant CT
Neoadjuvant CT
CapecitabineOxaliplatin
CetuximabBevacizumab
Irinotecan5-FU
PanitumumabTargeted therapies {
5-FU = 5-fluorouracil; CT = chemotherapy.Courtesy of Dr. J. Kuebler.

6.2
4.4
6.7
4.3
7.0 6.96.5
8.78.0
8.59.0
012
3456
789
10
1112
5-FU/LVFOLFOX4 5-FU/LVFOLFIRI 5-FU/LVIFL IFL IROX FOLFOX4 FOLFOX6FOLFIRI
First-Line Chemotherapy in MCRC Phase III Trials—Progression-Free Survival
aUpdate: After a median follow-up of 4.3 years, median TTP was significantly longer in the FOLFOX arm, 9.2 mo vs 6.5 mo for IROX (P≤.001) and 6.0 mo for IFL (P≤.001); bIn first-line therapy; cP≤.001; dP≤.01. MCRC = metastatic colorectal cancer; PFS = progression-free survival; TTP = time to progression.
de Gramont A, et al. J Clin Oncol. 2000;18:2938; Douillard JY, et al. Lancet. 2000;355:1041; Goldberg RM, et al. J Clin Oncol. 2004;22:23; Saltz LB, et al. N Engl J Med. 2000;343:905; Sanoff HKK, et al. 43rd ASCO; June 1–5, 2007. Abstract 4067; Tournigand C, et al. J Clin Oncol. 2004;22:229.Courtesy of Dr. J. Kuebler.
SaltzDouillardde Gramont N9741a Tournigandb
PF
S o
r T
TP
(m
o) c
cd
d c

First-Line Bevacizumab in MCRC Progression-Free Survival
aP<.001; bP<.005; cP=.004 vs mIFL.
Fuchs CS, et al. J Clin Oncol. 2007;25:4779; Hochster HS, et al. ASCO; June 1–5, 2006. Abstract 3510; Hurwitz H, et al. N Engl J Med. 2004;350:2335; Saltz LB, et al. ASCO GI; January 17–21, 2007. Abstract 238.Courtesy of Dr. J. Kuebler.
6.2
8.0
9.4
7.6
11.2
5.9
8.3
10.6
0
2
4
6
8
10
12
IFL IFL + BevFOLFOX/CapeOxFOLFOX/CapeOxFOLFIRIFOLFIRI + BevmIFL mIFL + Bev
+ Bev
PF
S o
r T
TP
(m
o)
NO16966AVF2107g
Phase III
b
a
BICC-C
c

9.8
8.2 8.4
10.6
8.08.9b
0
2
4
6
8
10
12
FOLFOX FOLFOX + CetFOLFIRI FOLFIRI + CetFOLFIRI FOLFIRI + Cet
First-Line Cetuximab in MCRCPhase III Trials—Progression-Free Survival
a16 months’ follow-up; bP<.05.Conclusions on overall survival await further follow-up.Van Cutsem E, et al. 43rd ASCO; June 1–5, 2007. Abstract 4000; Venook A, et al. 42nd ASCO; June 2–6, 2006. Abstract 3509.Courtesy of Dr. J. Kuebler.
b
CALGB 80203a CRYSTAL
PF
S o
r T
TP
(m
o)

Correlation Between Survival and Percentage of Patients Receiving 3 Drugs*
in Phase III Trials
*3 drugs: 5-FU/LV, irinotecan, oxaliplatin.Reprinted from Grothey A, et al. J Clin Oncol. 2005;23:9441,with permission from the American Society of Clinical Oncology.
12
13
14
15
16
17
18
19
20
21
22
0 10 20 30 40 50 60 70 80
Patients receiving 3 drugs (%)
Median OS (mo)

Managing Side Effects ofChemotherapy—Diarrhea
• Treat diarrhea aggressively and promptly with antidiarrheals
• Fluid/electrolyte replacement for grade >3 diarrhea• Hospitalization/antibiotics for diarrhea with febrile
neutropenia• Delay chemotherapy until bowel function back to
grade 0–1 with no antidiarrheals• Consider dose reduction if diarrhea grade >3• Anticholinergic therapy for diarrhea due to irinotecan
Kuebler JP, et al. Cancer. 2007;110:1945.

Managing Side Effects of Chemotherapy—Neurotoxicity
• Distal paresthesias/dysethesias triggered by cold• Educate patients to breathe in warm air, drink warm fluids• Acute paresthesias tend to last longer with each cycle and may
increase as duration of infusion increases• Efficacy of calcium and magnesium still being evaluated• Evaluate neurotoxicity prior to each treatment
– Stop oxaliplatin when paresthesias begin to interfere with activities of daily living
– Residual paresthesias can last up to 2 years
Land SR, et al. J Clin Oncol. 2007;24:2205.

Managing Side Effects of Chemotherapy—Bevacizumab
• Treat hypertension (blood pressure persistently >140/90) with oral agents
• Stop chemotherapy if blood pressure uncontrolled on oral agents
• Monitor dipstick urine assays• Interrupt treatment if proteinuria >2 gm/24 hours• Risk for arterial thrombotic events greater in patients
aged >65 years or with arteriosclerosis• Mild epistaxis common, major bleeding rare• Avoid surgery 1 month prior to and 6–8 weeks after
bevacizumab• GI perforation in ~1.5% of patients
Gordon MS, Cunningham D. Oncology. 2005;69(suppl 3):25; Kozloff M, et al. ASCO GI; January 17–21, 2007. Abstract 364; Rosiak J, Sadowski L. Clin J Oncol Nurs. 2005;9:407; Scappaticci FA, et al. J Natl Cancer Inst. 2007;99:232;Ellis LM, et al. J Clin Oncol. 2005;23:4853; Sugrue M, et al. 42nd ASCO; June 2–6, 2006. Abstract 3535.

Managing Side Effects of Chemotherapy—Cetuximab
• Treat grade 1 acneiform skin rash with topical anti-inflammatory agents
• Treat pruritis with oral antihistamines• Treat grade >2 skin rash with oral tetracycline (minocycline
at 100 mg/day)• Treat paronychia with topical antiseptics/antibiotics • Due to severe infusion reactions in ~3% of patients,
premedicate with antihistamines • Monitor patients for 1 hour posttreatment
Segaert S, Van Cutsem E. Ann Oncol. 2005;16:1425.


Martin
• The patient had a marked initial response to FOLFOX + bevacizumab, documented by CT scan and drop in CEA
• After 11 cycles of chemotherapy, he was still in response, but he was beginning to have problems with fine motor control
• His wife had to help button his shirts and he had difficulty holding a pen to write his name
• He discussed options for further therapy (maintenance vs observation) with his medical oncologist
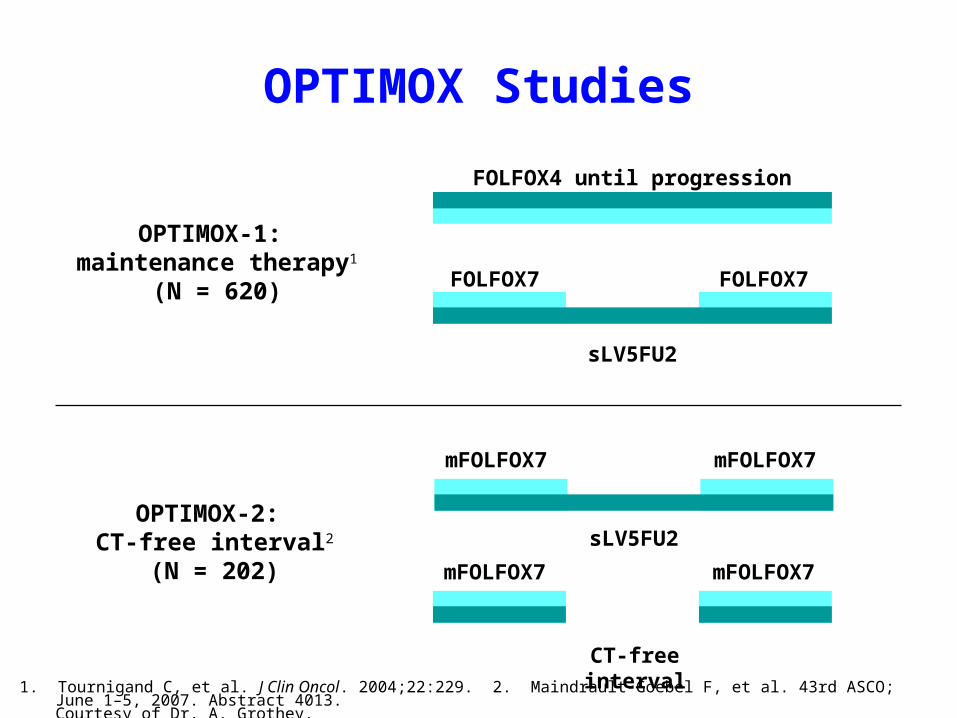
OPTIMOX Studies
OPTIMOX-1: maintenance therapy1
(N = 620)
FOLFOX4 until progression
FOLFOX7 FOLFOX7
sLV5FU2
OPTIMOX-2: CT-free interval2
(N = 202)
mFOLFOX7 mFOLFOX7
sLV5FU2
mFOLFOX7 mFOLFOX7
CT-free interval1. Tournigand C, et al. J Clin Oncol. 2004;22:229. 2. Maindrault-Goebel F, et al. 43rd ASCO; June 1–5, 2007. Abstract 4013.
Courtesy of Dr. A. Grothey.

Chemotherapy-Free Intervals of mFOLFOX in Patients With MCRC (OPTIMOX-2)—OS
MCRC = metastatic colorectal cancer; OS = overall survival.Maindrault-Goebel F, et al. 43rd ASCO; June 1–5, 2007. Abstract 4013. Courtesy of Dr. F. Maindrault-Goebel.
0
0.2
0.4
0.6
0.8
1.0
0 10 20 30 40 50
Pro
bab
ility
Months
OPTIMOX-1 (median 26 mo)OPTIMOX-2 (median 19 mo)
OS
P = .0549

Martin
• The patient was placed on maintenance treatment with infusional 5-FU + leucovorin
• The neurotoxicity improved quickly but did not resolve entirely
• After 4 months, his CEA began to rise and a follow-up CT scan confirmed progressive disease
• Options for second-line chemotherapy were discussed as the patient’s performance status had not changed

Second/Third-Line Therapy Options in MCRC
• If FOLFOX + bevacizumab used as first-line, consider FOLFIRI or irinotecan, +/- cetuximab, as second-line treatment
• IF FOLFIRI + bevacizumab used as first-line, consider FOLFOX, CAPOX or cetuximab + irinotecan as second-line
• If 5-FU/LV + bevacizumab used as first-line (not preferred), consider FOLFOX, CAPOX, FOLFIRI, or irinotecan as second-line
• For third-line therapy, consider cetuximab, panitumumab, or cetuximab + irinotecan
• Avoid single-agent bevacizumab or oxaliplatin• Consider going back to FOLFOX or FOLFIRI

FOLFIRI + Cetuximab ± Bevacizumab in Patients with Relapsed MCRC
(S0600/iBET)—Phase III Trial Design
MCRC = metastatic colorectal cancer; iBET = Intergroup Bevacizumab Continuation Trial.aPatients progressed on FOLFOX, OPTIMOX, or CAPEOX + bevacizumab as first-line regimen.http://clinicaltrials.gov/ct/show/NCT00499369?order=1. Accessed August 27, 2007.
Primary end point: Overall Survival (OS)
Secondary end point: Progression-Free Survival (PFS)
Previously treated patients with MCRCa
N = 1250
FOLFIRI + cetuximab +
bevacizumab (5 mg/kg q2w)
FOLFIRI + cetuximab +
bevacizumab (10 mg/kg q2w)
FOLFIRI + cetuximab +
placebo (q2w)
RANDOMIZATION

Summary
• First-line treatment regimen should be based on the disease and patient situation
• mFOLFOX, FOLFIRI, CAPOX, or 5-FU/LV with bevacizumab or cetuximab are all reasonable choices for first-line therapy
• Maintenance therapy after response is reasonable but there are no randomized data
• Bevacizumab is an option for maintenance and with second-line therapy
• Cetuximab plus irinotecan is an option for second- or third-line therapy
• Overall survival of patients with metastatic unresectable disease has been steadily increasing with the use of regimens in sequence or in combination (FOLFOXIRI)

Case Study: Surgically Resectable Metastatic Colorectal Cancer
Cathy Eng, MDAssistant Professor
Department of Gastrointestinal Medical OncologyThe University of Texas M. D. Anderson Cancer Center
Houston, Texas


Case Presentation—Ann• Ann is a 49-year-old female with newly diagnosed metastatic
colorectal cancer who presents for treatment recommendations• Six weeks earlier, she presented to the ER with weakness,
nausea and vomiting, and abdominal pain• She denies any prior constitutional symptoms or change in
bowel habits until the past month• Physical exam revealed a young, thin female in moderate
distress with 8/10 right-sided abdominal pain• Her ECOG PS was 1• Diagnostic studies included blood work, obstruction series, and
CT scan of the chest, abdomen, and pelvis– Findings: Hb = 10.1 g/dL, MCV = 73 fL, LFTs = WNL– Obstruction series of the abdomen demonstrated air fluid levels and
dilated small bowel loops consistent with small bowel obstruction
ER = Emergency Room; ECOG PS = Eastern Cooperative Group performance status;CT = computed tomography; Hb = hemoglobin; MCV = mean corpuscular volume;LFTs = liver function tests; WNL = within normal limits.

CT Scan at Baseline
2 coalescent lesions 4.8 cm in greatest diameter
Carcinoma of the cecum
Courtesy of Dr. C. Eng.

Case Presentation
• Preoperative carcinoembryonic antigen (CEA) = 38 ng/mL (normal, <5 ng/mL)
• No known family history of colon cancer • Emergent right hemicolectomy performed due to bowel obstruction • Palpation of the liver revealed no additional hepatic lesions, a
finding confirmed by intraoperative ultrasound • The surgeon elected to resect the hepatic lesions at a later date • Postoperative pathology revealed a moderately differentiated
adenocarcinoma of the colon penetrating through the muscularis propria, with 5 of 22 lymph nodes positive
• AJCC staging: T3N2M1 right-sided colon cancer


Case PresentationPostoperative state
• Ann has recovered fully • ECOG PS = 0
– She has only lost 5 lbs since the surgery– She has 1–2 bowel movements daily – Postoperative CEA = 16 ng/mL– LFTs: within normal limits – Postoperative CT scan reveals no new lesions
• She is anxious to initiate therapy• She desires to know what her options are to be “cancer-free” in the
future • What is the best approach to address her metastatic disease in the
liver?

Options in Management of Hepatic Metastasis from Colorectal Cancer
• Prioritize multidisciplinary discussion with the liver surgeon
• Options– Surgical resection– Neoadjuvant systemic chemotherapy– Conversion chemotherapy– Hepatic arterial infusion therapy–fallen out of favor

Immediate Hepatic Resection
• Resectable disease• Role of adjuvant chemotherapy is unknown • Duration of adjuvant chemotherapy is unknown• To date, no randomized trial of surgical resection
followed by observation vs adjuvant chemotherapy has been completed

Neoadjuvant Systemic Chemotherapy
• Majority of prior studies have been retrospective • Ideal for surgically resectable or borderline resectable
disease • Allows indirect measure of chemotherapy
responsiveness• Be wary of chemotherapy-induced hepatic toxicities
– Do not treat until best response– Radiologic complete response ≠ pathologic complete response

Phase III EORTC 40983
Perioperative FOLFOX for ResectableHepatic Metastases*
RandomizeN = 364
Surgery
FOLFOX46 cycles
(3 months)
Nordlinger B, et al. 43rd ASCO; June 1-5, 2007. Abstract LBA5.
• Primary endpoint: progression-free survival
• Eligibility criteria: < 4 liver lesions
(metachronous or synchronous),
surgically resectable, no extrahepatic disease
Surgery
*Only prospective trial to date.
FOLFOX46 cycles
(3 months)

Complications of SurgeryPeri-op CT Surgery
Postoperative complications*
40 /159 (25.2%)
27 / 170 (15.9%)
Cardiopulmonary failure 3 2
Bleeding 3 3
Biliary fistula 122 5
Includes output >100 mL/d, >10 d (9) (2)
Hepatic failure 11 8
Includes bilirubin >10 mg/dL, >3 d (10) (5)
Wound infection 4 4
Intra-abdominal infection 8 2
Needed to re-operate 5 3
Other 25
16
Includes postoperative death 1 patient 2 patients
*P = .04Courtesy of Dr. B. Nordlinger.

Final Results of EORTC 40983No. Pts
CTN Pts
SurgeryAbsolute
Differencein 3-Year PFS
(95.66% Confidence
Interval)
HazardRatio
(95.66% Confidence
Interval)
P-value
All patients (ITT)
182 182 +7.3% (28.1%–35.4%)
0.79(0.62–1.02)
P = .058
All eligiblepatients
171 171 +8.1% (28.1%–36.2%)
0.77 (0.60–1.00)
P = .041
All resectedpatients
151 152 +9.2% (33.2%–42.4%)
0.73(0.55–0.97)
P = .025*
Courtesy of Dr. B. Nordlinger.
*Statistically significant only in those patients surgically resected.

Conversion Chemotherapy
• Defined as systemic chemotherapy provided to decrease tumor burden and improve likelihood of surgical resection
• Previously conducted studies– FOLFOXIRI – CRYSTAL – NO16966

FOLFIRI vs FOLFOXIRIPhase III
(Gruppo Oncologico Nord Ovest)
Randomize untreated MCRC N=244
FOLFIRI X 12
FOLFOXIRI x 12
Falcone A, et al. J Clin Oncol. 2007;25:1670.

FOLFOXIRI vs FOLFIRIResults
FOLFIRI(n = 122)
FOLFOXIRI(n = 122)
CR* 6% 8%
PR* 35% 58%
RR* 41%[95%: 0.32-0.50]
66% [95%: 0.56-0.74]
R0 (hepatic resection)†
12% (n = 42) 36% (n = 39)P = .017
Falcone A, et al. J Clin Oncol. 2007;25:1670.
* Investigators assessment † Patients with liver metastases only

Role of Biologics in Hepatic Resection?

CRYSTAL TrialLiver Resection with Cetuximab
Courtesy of Dr. E. Van Cutsem.
4.5
9.8
0
1
2
3
4
5
6
7
8
9
10
Percentage (%)
2.5
1.5
6
4.3
0
1
2
3
4
5
6
7
Surgery withCurative Intent
No Residual TumorAfter Resection
Percentage (%)
n = 599/Group n = 599/Group n = 134/n = 122
P = .0034*
No Residual Tumor in Patients with Liver Metastases
ITT Population Liver-Metastases–Only Population
FOLFIRI Alone Cetuximab + FOLFIRI

Lucrative Points in the Management of Hepatic
Resection

Duration of Chemotherapy• Chemotherapy may induce hepatic toxicities• At a median of 4 months of chemotherapy with fluoruracil
and irinotecan or oxaliplatin, many patients developed– Sinusoidal dilatation– Steatosis– Steatohepatitis
Associated with increased 90-day postoperative mortality
• Shorter duration of chemotherapy (e.g. 2-3 months may be optimal)
• Biologic therapy– Bevacizumab recommended to be held 4-8 weeks prior to
surgical resection
Vauthey JN, et al. J Clin Oncol. 2006;24:2065.

Radiologic CR = Pathologic Cure?
• 1998–2004– 586 consecutive patients treated for up to 10 hepatic
metastases 38 patients had radiologic CR of >1 hepatic lesion Surgery was conducted 4 weeks after start of neoadjuvant
treatment
• Number of neoadjuvant cycles: 9 + 5• Types of chemotherapy
– 5-FU/LV = 9– FOLFOX = 17– FOLFIRI = 12
Nordlinger B, et al. 42nd ASCO; June 2-6, 2006. Abstract 3501.

Radiological CR = Cure?• 66 liver lesions had a radiologic CR
20 (9 pts) had macroscopic residual disease– Mean size 12 + 7 mm– Viable cancer cells at biopsy
15 (15 pts) had microscopic disease– No visible tumor was seen surgically or by IOUS– Site was resected– Viable cancer cells were seen in 12 of 15 liver mets
31 lesions in 14 pts showed no evidence of disease surgically or by IOUS
– Site was not resected– One year follow-up: 23 of 31 mets had in situ recurrences
• Findings: 55 of 66 (83%) of the lesions were not pathologically cured
• Conclusions: Consider pursuing surgical resection regardless of no radiographic evidence of disease.
Nordlinger B, et al. 42nd ASCO; June 2-6, 2006. Abstract 3501.

Case Presentation
• Ann received 5 cycles of FOLFOX + bevacizumab, followed by 1 cycle of FOLFOX without bevacizumab
• Except for mild cold hypersensitivity, she tolerated her chemotherapy well
• In the interim, genetics counseling showed that she is microsatellite-stable
• Her CEA concentration is now 7.2 ng/mL• CT of her chest, abdomen, and pelvis all showed
response to therapy • Her PET/CT scan is negative for extrahepatic disease

Postchemotherapy CT Scan
• The patient undergoes right hepatic resection without complications
• Minimal <5% steatosis was noted
• Due to her excellent response to chemotherapy, the patient opted for an additional 4–6 months of adjuvant FOLFOX + bevacizumab
Courtesy of Dr. C. Eng.

Conclusions• Multidisciplinary management is crucial for a patient with
resectable hepatic metastases • Resection of the primary tumor is patient dependent
based on presenting symptoms • Be wary of duration of neoadjuvant therapy—Do not
treat a patient to cure for hepatic metastases but treat until surgically resectable
• Radiolologic CR is not equivalent to pathologic CR and must still be evaluated if possible – Challenge: identifying the original site of disease
intraoperatively• To date, the role of biologic therapy in conjunction with
chemotherapy as neoadjuvant treatment has not been defined in a large randomized phase II or phase III trial
Related Documents











