Transfusing tiny soldiers Ramsey C. Tate, MD

Transfusing tiny soldiers Ramsey C. Tate, MD. Applying combat-derived massive transfusion protocols to pediatric trauma patients.
Dec 17, 2015
Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

Transfusing tiny soldiers
Ramsey C. Tate, MD
Applying combat-derived massive transfusion protocols to pediatric trauma patients
Case
Damage control resuscitation
Massive transfusion protocols
Pediatric massive transfusion protocols
Agenda

Case
Damage control resuscitation (DCR)
Massive transfusion protocols (MTP)
Pediatric massive transfusion protocols
Agenda


GCS 15HR
151BP 100/palp

HR 166BP
60/palp“exhibits transient loss of consciousness”
Trauma code
Emergently taken to OR “Likely to require multiple transfusions”
Grade V liver laceration
Packed red blood cells: 19 unitsFresh frozen plasma: 5 unitsApheresis platelets: 1 unitsCryoprecipitate pooled: 2 unitsRecombinant Factor VIIa: 1 dose



5 million

40%
Massive hemorrhage carries greater than 50% risk of death

Damage Control Resuscitation

Damage Control Resuscitation
Permissive hypotension
Aggressive correction of coagulopathyUse of vasopressors and blood products to maintain hemodynamics and euvolemia

Damage Control Resuscitation
Permissive hypotension
Aggressive correction of coagulopathyUse of vasopressors and blood products to maintain hemodynamics and euvolemia
Hemostatic resuscitation
Death
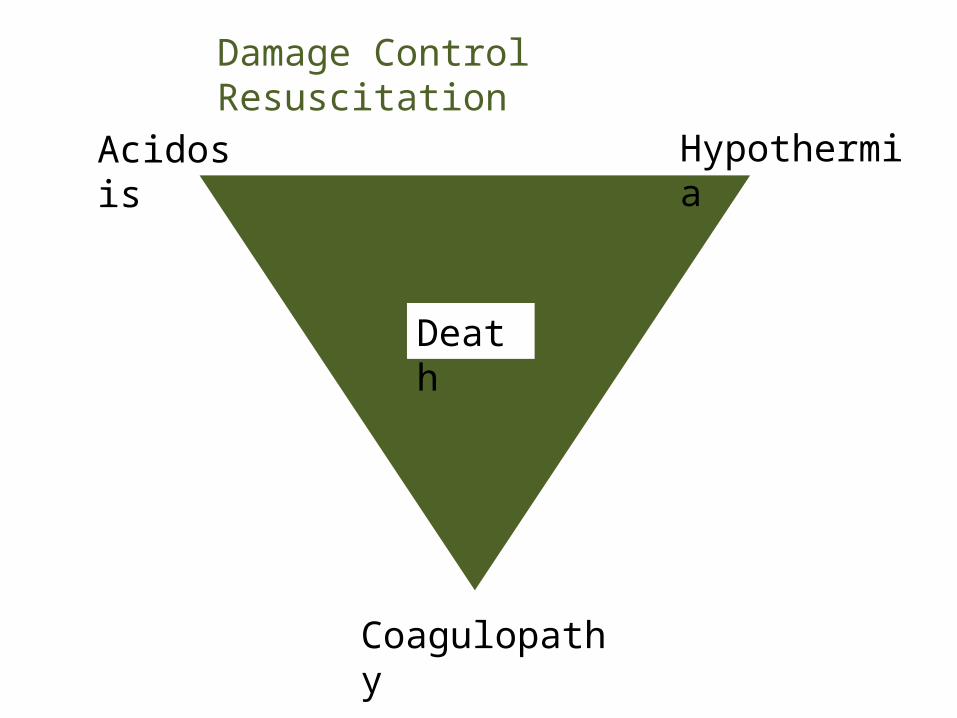
Damage Control Resuscitation
Acidosis
Hypothermia
Coagulopathy
Death
Damage Control Resuscitation
Acidosis Hypothermia
Coagulopathy
Death
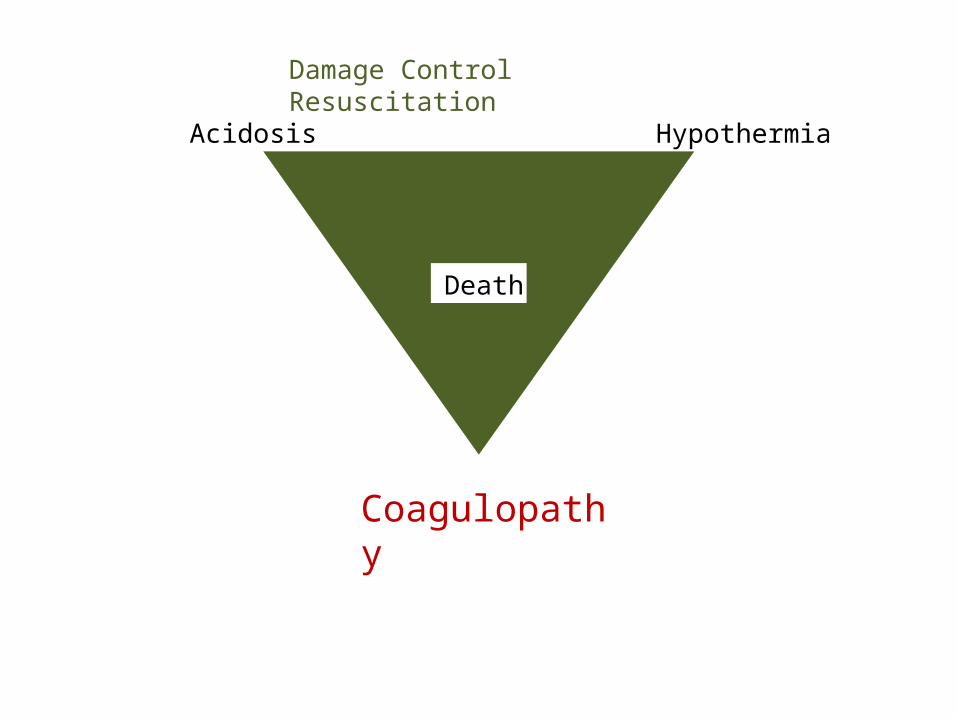
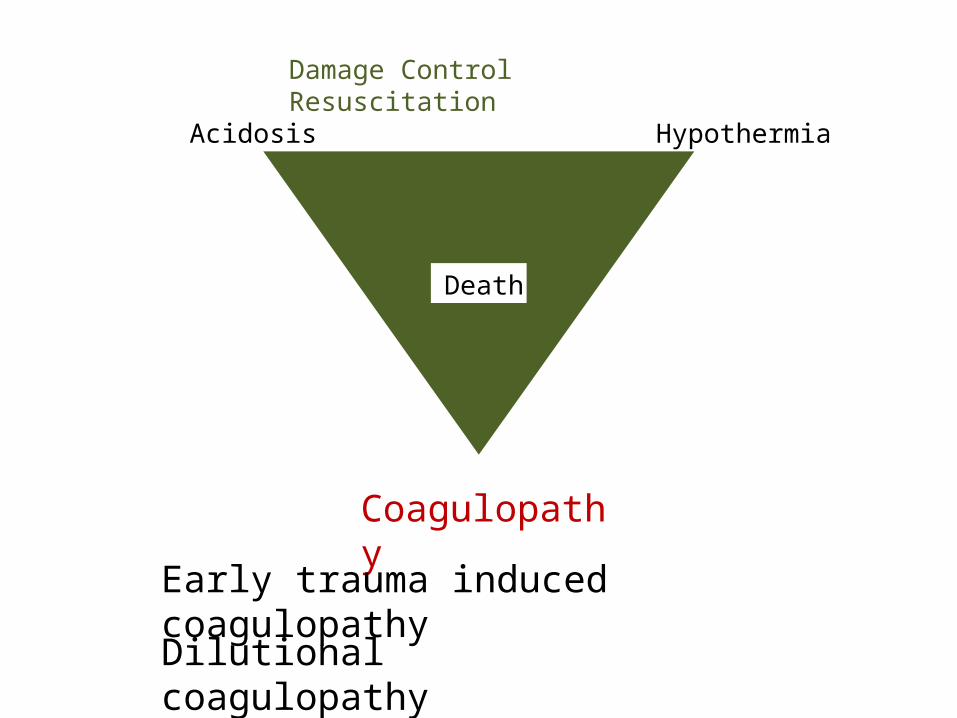
Damage Control Resuscitation
Acidosis Hypothermia
Coagulopathy
Early trauma induced coagulopathy Dilutional coagulopathy

3% of adult civilian trauma patients

3% of adult civilian trauma patients
70% of transfused blood products at trauma centers

Transfusion of more than 10 units of blood
Loss of 50% of blood volume in 3 hours
Ongoing blood loss of 150 mL/hour

5 liters
0.5 liters

5 liters
0.5 liters
Transfusion of one blood volume in 24 hours

Approaches to massive transfusion
Component therapy
Transfusion physician managementMassive transfusion protocol with predetermined blood product administration

Massive transfusion protocol with predetermined blood product administration

Fresh whole blood:
500 mLHct 33-43%Plt 130-350,000Fibrinogen 1500 mgClotting activity 86%Full platelet activityWarm

Fresh whole blood:
500 mLHct 33-43%Plt 130-350,000Fibrinogen 1500 mgClotting activity 86%Full platelet activityWarm
RBC + Platelets + FFP:
660 mLHct 29%Plt 88,000Fibrinogen 750 mgClotting activity 65%Reduced platelet activityCold

Fresh whole blood:
500 mLHct 33-43%Plt 130-350,000Fibrinogen 1500 mgClotting activity 86%Full platelet activityWarm
RBC + Platelets + FFP:
660 mLHct 29%Plt 88,000Fibrinogen 750 mgClotting activity 65%Reduced platelet activityCold
1:1:1

Key components of MTP
Resuscitation with predetermined ratios of blood components
Rapid infusion of warmed blood productsCoordination with transfusion specialists to ensure streamlined delivery of productsMonitoring of coagulation studies to determine the end-point of protocol

Key components of MTP
Resuscitation with predetermined ratios of blood components 1 RBC:1 FFP:1 PlateletRapid infusion of warmed blood productsCoordination with transfusion specialists to ensure streamlined delivery of productsMonitoring of coagulation studies to determine the end-point of protocol

Key components of MTP
Resuscitation with predetermined ratios of blood components
Rapid infusion of warmed blood productsCoordination with transfusion specialists to ensure streamlined delivery of productsMonitoring of coagulation studies to determine the end-point of protocol
Key components of MTP
Resuscitation with predetermined ratios of blood components
Rapid infusion of warmed blood productsCoordination with transfusion specialists to ensure streamlined delivery of productsMonitoring of coagulation studies to determine the end-point of protocol

Key components of MTP
Resuscitation with predetermined ratios of blood components
Rapid infusion of warmed blood productsCoordination with transfusion specialists to ensure streamlined delivery of productsMonitoring of coagulation studies to determine the end-point of protocol

MTP-associated outcomes
Mortality
Decreases in blood product consumption
Improvements in blood product delivery
Decreases in ventilator-associated pneumonia
Decreases in open abdomen days and abdominal compartment syndrome

MTP-associated outcomes
Mortality
Decreases in blood product consumption
Improvements in blood product delivery
Decreases in ventilator-associated pneumonia
Decreases in open abdomen days and abdominal compartment syndrome
All published data are retrospective!

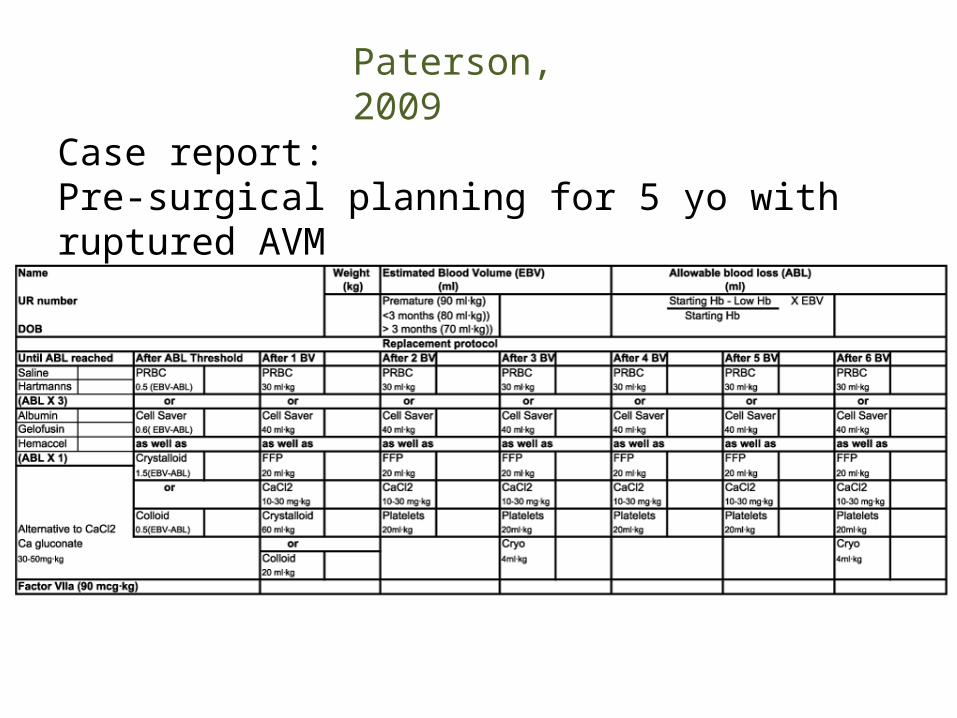
Paterson, 2009
Case report:Pre-surgical planning for 5 yo with ruptured AVM

Paterson, 2009
Case report:Pre-surgical planning for 5 yo with ruptured AVM
This might work in the OR…

… but tough to do in here.

Dehmer and Adamson, 2010
Expert opinion:Adapted Paterson’s protocol
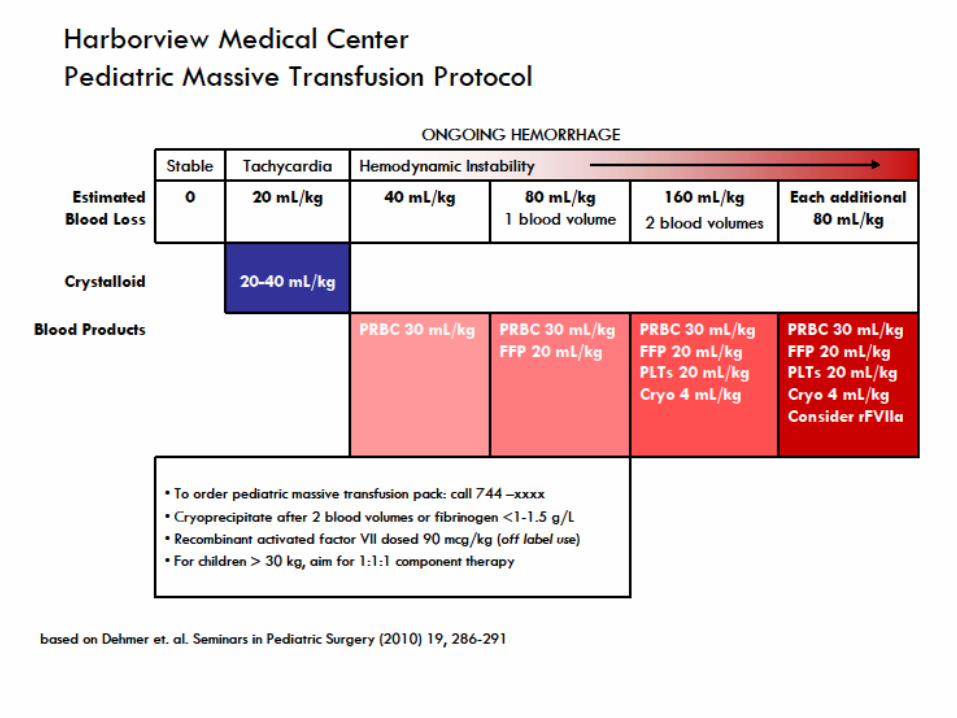
Harborview pediatric MTP
adapted by Brian Johnston

On the horizon
Pediatric MTP in development at UNM

On the horizon
Pediatric MTP in development at UNM
Introduction of ROTEM testing

On the horizon
Pediatric MTP in development at UNM
Introduction of ROTEM testing
PROMMTT Study

Questions?
Related Documents











