Order Number 9411943 Transformational leadership of clinical nutrition managers Foltz, Mary Elizabeth, Ph.D. The Ohio State University, 1993 Copyright ©1993 by Foltz, Mary Elizabeth. All rights reserved. U MI 300 N. Zeeb Rd. Ann Arbor, MI 48106

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

Order Number 9411943
Transform ational leadership o f clinical nutrition managers
Foltz, Mary Elizabeth, Ph.D.
The Ohio State University, 1993
Copyright © 1993 by Foltz, M ary E lizabeth. A ll rights reserved.
U MI300 N. Zeeb Rd.Ann Arbor, MI 48106
TRANSFORMATIONAL LEADERSHIP OF CLINICAL NUTRITION MANAGERS
DISSERTATION
Presented in Partial Fulfillment of the Requirements for the Degree Doctor of Philosophy in the
Graduate.School of The Ohio State University
By
Mary Elizabeth Foltz, B.S., M.S., R.D., L.D.
* * * * *
The Ohio State University 1993
Dissertation Committee:W.A. JohnsonV.M. Vivian M.R. SchillerS. Strasser
Approved by
Johnson Adviser
College of Human Ecology Department of Human Nutrition
and Food Management

Copyright by Mary Elizabeth Foltz
1993
To My Parents
1 1
ACKNOWLEDGMENTS
The author is deeply indebted to Virginia M. Vivian for her enduring support, guidance, and encouragement in the successful completion of the research. She has been a steady hand— giving an occasional, helpful push— since she became my advisor in the Honors Program, when I was an undergraduate. Sincere gratitude is also expressed to others involved with this research, including members of my committee: M. Rosita Schiller, for her insights and mentor- ship; Wayne A. Johnson, for his expertise and advice on my program and manuscript; and Steven Strasser for his review and suggestions on the proposal and this composition.Alan S. Ryan is also thanked for his consideration of the proposal and manuscript.
A very personal thank you goes to Jan Alloy, Daryl Yammishita, Denise Scales, and Sandy Shelly for their technical assistance with the research and this treatise. With special thanks I acknowledge the cooperation of those clinical nutrition managers who completed the survey instruments used in this investigation.
I am most grateful to an outstanding leader in our profession and my dear colleague, Susan Calvert Finn, for
her sterling example and strong personal support. Thanks to her, I also had the complete cooperation of many coworkers in the Ross Products Division of Abbott Laboratories, whose understanding and able assistance were of great import in this endeavor.
To my fiancee, Bradley M. Arensberg, I offer a loving thank you for his unyielding faith and constant encouragement, as I worked to complete the final step toward a life long goal. To my family, I say thanks again for your personal examples and continued dedication to my education
VITA
July 19, 1959 .... . Born - Alexandria, Virginia1981..................... B.S., The Ohio State
University, Columbus, Ohio1981-1982 ................ Dietetic Internship, New
England Deaconess Hospital, Boston, Massachusetts
1983 ..................... M.S., Boston UniversityBoston, Massachusetts
1983-1987 ................ Program Consultant, RossProducts Division, Abbott Laboratories, Columbus, Ohio
1987-Present ............. Manager, Nutrition ServicesRoss Products Division, Abbott Laboratories, Columbus, Ohio
PUBLICATIONSFoltz MB, ed: Nutritional Support Folio [11 volume clinical resource] Columbus, Ohio: Ross Laboratories, 1984.Hensel RD, Burris B, Foltz MB: Lights, cameras, action!Ross Labs' successful teleconference. Carina 3(1):22—4, 1984 .Kittleberger S, Foltz MB, Shields EM: Nutritional Supportin the Long-Term Care Institution. Columbus, Ohio: RossLaboratories, 1984.Foltz MB, Stephens G: Marketing food and nutritionservices. Hospital Administration Currents 29(2):7-12.1985.
v
Kittleberger S, Foltz MB, Shields EM: How to deliverspecialized nutritional support. Journal American Health Care Association 11(8): 29-36, 1985.Foltz MB, Stephens G: Use of nutritional support systemsto meet hospital marketing needs. Hospital Materiel Management Quarterly 7(3):80-90, 1985.Foltz MB, Stephens G: A marketing model for hospitals.Frontline Planning 4:9-11. 1986.Brusadin RA, Foltz MB: Enteral nutrition. NARD Journal108: 53-57, 1986.Finn SC, Foltz MB: Nutritional support of the ENT patient:Enteral formula selection. ENTechnology September:58-65,1986.Finn SC, Foltz MB, Parks SC: Challenges of the changing dietetic marketplace, in The Competitive Edge: Marketing Strategies for the Registered Dietitian. Chicago: TheAmerican Dietetic Association, 1987.Foltz MB: Workbook in Communications. How to Tell the WICSuccess Story. Columbus, OH: Ross Laboratories, 1987.Foltz MB, Ryan AS: Aging population presents marketingopportunities for dietitians. Journal of the American Dietetic Association 87(5):633-635, 1987.Ryan AS, Foltz MB, Finn SC: The role of the clinicaldietitian: I. Present professional image and recent imagechanges. Journal of the American Dietetic Association.88 (6) :671-676, 1988.Ryan AS, Foltz MB, Finn SC: The role of the clinicaldietitian: II. Staffing patterns and job functions.Journal of the American Dietetic Association, 88(6):679- 683, 1988.Foltz, MB: The American Dietetic Association House ofDelegates; Your Voice in the Association. Multi-imageprogram and video, Columbus, OH: Ross Laboratories and TheAmt?Tican Dietetic Association, 1990.Hassan S, Foltz MB: Health care innovations from theinternal marketing perspective, Journal of Hospital Marketing A <11:97-117, 1990.
Finn SC, Foltz MB, Ryan AS: Image and role of theconsultant dietitian in long-term care: Results from asurvey of three midwestern states. Journal of the American Dietetic Association. 91(7):788-792, 1991.Foltz, MB: Strategic planning: How can we chart a safecourse in shark-infested waters? Journal of the American Dietetic Association. 91(9):A152, 1991.Foltz MB: The American Dietetic Association Foundation:Silver Reflections and Future Visions. Multi-image program and video, Columbus, OH: Ross Laboratories and TheAmerican Dietetic Association, 1991.Foltz MB: Payment Power: What It Is and How DietitiansCan Get It! Columbus, Ohio: The American DieteticAssociation and Ross Laboratories, 1991.Foltz MB, ed: The Power of Persuasion. Dialogue forDollars. Columbus, Ohio: The American DieteticAssociation and Ross Laboratories, 1992.Foltz MB, ed: The Politics of Reimbursement. Columbus,Ohio: The American Dietetic Association and RossLaboratories, 1993.Foltz MB, Schiller MR, Ryan AS: Nutrition assessmentpractices. Accepted for publication, Journal of the American Dietetic Association. 1993.Schiller MR, Foltz MB, Campbell SM: Dietitians' selfperceptions: implications for leadership. Journal of theAmerican Dietetic Association. 93:868-876, 1993.
FIELDS OF STUDYMajor Field: Human Ecology
Studies in Human Nutrition. Professor EmeritusVirginia M. Vivian
Studies in Health Education. Professor Moon Chen
vii
TABLE OF CONTENTSACKNOWLEDGMENTS .......................................... iiiV I T A ......................................................... vLIST OF TABLES............................................ xiLIST OF FIGURES.......................................... xivCHAPTER
I. INTRODUCTION...................................... 1Leadership in Businesses and
Organizations ............................... 1Transformational Leadership................. 4Need for Transformational Leadership in
Healthcare and Dietetics.................... 5Purpose and Objectives of the Study.......... 7
Problem Statement ........................... 7Research Objectives of the Study.......... 8Hypotheses..................................... 9Definition of Terms ......................... 9Assuuiptjions ...i........................... 10
Scope and Significance of the Study......... 10
II. LITERATURE REVIEW ............................... 12Introduction ................................. 12
"Great Man," Situational and InteractionalTh6O3-16s ............................... 13
Style and Behavior Theories............... 16Situational or Contingency Theories ...... 19Motivational Theories ...................... 24Summary of Traditional Leadership
Theories................................. 26Transformational Leadership Theory........... 2 6Transformational Leadership Measures......... 35
Multifactor Leadership Questionnaire..... 36Leadership Practices Inventory.............. 43Leadership Behavior Questionnaire..........4 7Survey of Leadership Practices ............ 55
viii
Table of Contents (continued)Summary of Transformational Leadership
Measures 59Transformational Leadership Research.......... 61
Demographic and Experiential Variables .... 62Situational Variables...................... 68Effectiveness Outcomes ...................... 68Subordinate Beliefs...... ................. 72Leader and Subordinate Ratings......... .. 74Summary of Transformational Leadership
Research 74Healthcare Professional Leadership
Rg ssflir oh 7 5Nursing Literature......................... 75Other Health Professions Literature........ 84Dietetic Literature........................ 89Summary of Health Professions Literature . . 97
III. METHODOLOGY...................................... 99Study Design................................... 99
Populations and Sample .................... 100Survey Instruments ........................ 102
Distribution of the Survey Instruments andInstructions .............................. 104
Statistical Analysis ......................... 105
IV. RESEARCH FINDINGS .............................. IllThe Study Sample............................. 112
Demographic Profile of ClinicalNutrition Managers...... ............... 112
Demographic Profile of EmployeeEvaluators............................. 119
Transformational Leadership Qualitiesof Clinical Nutrition Managers........ 119
Description of the Clinical NutritionManager (SELF) LBQ Scores............... 119
Description of the Clinical Nutrition Manager Employee Evaluator (OTHER)LBQ S c o r e s 121
Comparison of the Clinical Nutrition Manager (SELF) LBQ Scores to the Clinical Nutrition Manager EmployeeEvaluator (OTHER) LBQ Scores .......... 123
Comparison of the Clinical Nutrition Manager LBQ Scores to the LBQ Scores from Other Samples..................... 123
ix
Table of Contents (continued)Association Between Transformational Leader
ship Qualities of Clinical Nutrition Managers and Defined Study Variables .... 125
V. INTERPRETATION AND DISCUSSION OF FINDINGS .... 127Description of Transformational Leadership
Qualities of Clinical Nutrition Managers . . 127Hypothesis 1 .............................. 127
Comparison of Transformational Leadership Qualities of Clinical Nutrition Managers as Rated by Clinical Nutrition ManagersThemselves and Employee Evaluators...... 133Hypothesis 2 133
Association Between Transformational Leadership Qualities of Clinical Nutrition Managers and DefinedStudy Variables........................... 137Hypothesis 3 .............................. 137
Limitations................................... 140General Implications of Findings . .......... 143Recommendations.............................. 151
V I . SUMMARY....................................... 157APPENDICES.......................................... 163
A. Leadership Behavior Questionaire (LBQ)Leadership Scales and Summary of Triangular Profiles Developed for the LBQ.............. 163
B. Leadership Characteristics and Activitiesof Clinical Nutrition Managers Survey ....... 168
C. Leadership Characteristics and Activities of Clinical Nutrition Managers EmployeeSurvey 175
D. Letters and Instructions to Clinical Nutrition Managers and Employee Evaluators . . 177
E « T ab l6s ........... 186F. Figures...................................... 225
LIST OF REFERENCES.................................. 231
x
LIST OF TABLES
Table Page1. Employment and educational characteristics
of clinical nutrition managers.................... 1872. Memberships in practice groups of The American
Dietetic Association held by clinical nutrition managers........................................... 189
3. Demographic characteristics of institutions where clinical nutrition managers wereemployed........................................... 190
4. Percentage of reimbursement received by institution for charges made for clinical nutrition services................................ 191
5. Size of clinical nutrition staff and number of employees directly supervised by theclinical nutrition managers....................... 192
6. Type of education program in which students supervised by clinical nutrition managerswere enrolled.......................... 194
7. Reductions and/or additions of full-time equivalent (FTE) clinical nutrition staffin the past three years .............. . 195
8. Annual percentage of staff turnover for clinical dietitians and/or dietetictechnicians........................................ 196
9. Techniques and programs used by clinical nutrition managers to enhance clinicalnutrition staff retention and development ........ 197
10. Items and programs developed by clinical nutrition managers for use in clinical nutrition continuous quality improvement......... 198
xi
List of Tables (continued)11. Clinical nutrition management programs
implemented by clinical nutrition managers ....... 19812. Methods of marketing clinical nutrition
services used by clinical nutrition managers .... 19913. Beliefs of clinical nutrition managers on the
future of the clinical nutrition manager position in their institution........................ 199
14. Items of responsibility and control by the clinical nutrition managers...................... 200
15. Budget size controlled by clinical nutrition managers.............................................200
16. Involvement of clinical managers in educational activities, publications, and research activities (outside of routine workassignments) ...................................... 201
17. Appointed/elected offices held by clinical nutrition managers in professional organizations and professional development programs attended by clinical nutrition managers inpast three years.................................. 202
18. Participation by clinical nutrition managersin leadership-related activities . ......... 202
19. Personal behaviors/actions listed by clinical nutrition managers as important for leadersin clinical dietetics ....................... 203
20. Classification of clinical nutrition managers' listing of personal behaviors/actions importantfor leaders in clinical dietetics............... 204
21. Personal characteristics/traits listed by clinical nutrition managers as important for leadership in clinical dietetics................ 206
22. Classification of clinical nutrition managers' listing of personal characteristics/traits important for leaders in clinical dietetics 207
xii
List of Tables (continued)23. How leaders in clinical dietetics should re
late to or interface with institutional goalsas described by clinical nutrition managers 209
24. Classification of clinical nutrition managers' listing of how leaders in clinical dietetics should relate to or interfacewith institutional goals......................... 210
25. Employment and educational characteristics of employee evaluators of clinical nutrition managers.......................................... 212
26. Mean of clinical nutrition manager (SELF) LBQ scores and rating on LBQ guidelines............. 214
27. Percentage of clinical nutrition manager (SELF)LBQ scores by quintiles.......................... 215
28. Mean of clinical nutrition manager employee evaluator (OTHER) LBQ scores and rating onLBQ guidelines.................................... 216
29. Percentage of clinical nutrition manager employee evaluator (OTHER) LBQ scores by quintiles............................ 217
30. Mean of clinical nutrition manager (SELF) LBQ scores compared with mean of clinical nutrition manager employee evaluator (OTHER) LBQ scores . . . 218
31. Mean of clinical nutrition manager (SELF) LBQ scores compared with mean of healthcare administrators/organizational consultants in psychological healthcare field (SELF) LBQ scores..... 219
32. Mean of clinical nutrition manager (SELF) LBQ scores compared with mean of entrepreneursin very small businesses (SELF) LBQ scores ..... 220
33. Mean of clinical nutrition manager employee evaluator (OTHER) LBQ scores compared with mean of entrepreneurs in very small businesses other evaluator (OTHER) LBQ scores..................... 221
34. Association of defined study variables with clinical nutrition manager (SELF) LBQ subscoresand totals............................. 222
xiii
I
LIST OF FIGURES
Figure Page1. Value direct supervisor has of clinical
nutrition services as rated by clinical nutrition managers........... 226
2. Self-ratings of leadership style by clinical nutrition managers .............................. 227
3. Closeness of working relationship with clinical nutrition managers as evaluated by employee evaluators .............................. 228
4. Mean of clinical nutrition manager (SELF)LBQ subscores depicted on a triangle diagram and compared to specific profiles developedfor the LBQ instrument.......................... 229
5. Mean of clinical nutrition manager employee evaluator (OTHER) LBQ subscores depicted ona triangle diagram and compared to a specific profile developed for the LBQ instrument...... 230
xiv
CHAPTER I INTRODUCTION
Leadership in Businesses and OrganizationsLeadership has been a topic of interest to
philosophers and social and political scientists for centuries. Yet, only in the past century has there been intensive study and application of leadership theory to the management of businesses and organizations. With the quickly changing and competitive business environment of today, there is renewed interest in and study of leadership.
The study of leadership is important to businesses and organizations for several reasons. First, leadership is linked to organizational success. Bass (1990) noted that leadership was often regarded as the single most critical factor to success or failure of institutions. In the workplace, it has been documented that when immediate supervisors are considered, 60% of the supervisors are the major cause of job-related stress (Clark et al 1992).
Second, leadership is viewed as an essential element for effective organizational change. This concept distinguishes leaders from managers. Specifically, when
1
2
managers implement change in an organization it is often "planned change." Managers function within the existing organizational structure. They make small changes in the process perhaps, but do not alter fundamental constructs or worker motivation. This provides for incremental but not necessarily significant organizational gains.
Leaders, on the other hand, are not typically confined by structure. They more readily make changes in organizational cultures and ultimately the workers themselves. Thus, leaders provide an opportunity for more effective change and significant organizational gains. Kotter (1990) distinguished the functions of management and leadership in this way: management helped keep an organization on time and on budget, whereas leadership produced movement through constructive or adaptive change.
Another consideration is the level at which leadership is exhibited within an organization. Often the leadership of an effective and popular chief executive officer or president is singled out as the reason for organizational success. Day and Lord (1986) noted that differences in executive leadership might have explained up to 4 5% of an organization's performance. Researchers have also documented that effective organizations have leaders not just in the executive ranks, but also at lower levels of management (Wilson et al 1990; Yammarino and Bass 1990;
3
Sashkin and Burke 1990). Current research in leadership is being redirected on how to identify and foster leadership skills at many organizational levels.
The application of leadership theories in businesses and organizations has contributed to the further development of the models used to define leadership. Businesses and organizations provide "real world" opportunities to test the practical nature of leadership models.
Most traditional leadership theories seem to define leadership along only one dimension, such as commonly identified traits or situational approaches. These theories have limited use in business and organizational contexts because the goals of the organization are not considered.
Current theories of leadership take a much broader, multidimensional approach viewing leadership not as a single factor but rather as resulting from several interacting factors. These theories reflect personal characteristics of the leader, such as power and influence, and situational or organizational contexts in which the leader and followers interact, thus accounting for the ability of the leader to impact the organization's functioning. In addition, current theories often incorporate specific interpersonal behaviors of the leaders and their actions within organizations.
4
Transformational LeadershipThe current theories of leadership are described as
"transformational" leadership. In the broad concept of transformational leadership, leaders help individuals and organizations survive in a complex world, help them master change, and help provide employees gain a greater sense of self-worth. Transformational leaders are viewed as the leaders who help develop and achieve visions to move organizations and employees ahead in the future.
The foundations of transformational leadership theory were first proposed by Weber (1947) and later more fully developed by and most frequently credited to Burns (1978). Burns (1978, p. 20) presented the paradigm of transformational leadership as leadership that "occurs when one or more persons engage with others in such a way that leaders and followers raise one another to higher levels of motivation and morality."
As the theory has been further developed, transformational leadership has been described as a process by which followers are converted into leaders and are challenged to focus on organizational goals and achieve more than they thought was possible. The transformational leader is characterized as having vision, power, and an ability to communicate broad organizational goals to followers. The transformational leader is also one who empowers followers
5
to make their own decisions and become leaders themselves. Thus, the transformational leader helps others deal more effectively with change.
Need for Transformational Leadership in Healthcare and Dietetics
Just as there is a need for transformational leaders to help businesses and organizations deal with the significant changes occurring today, there is also a need for transformational leaders in healthcare. Healthcare itself is undergoing a metamorphosis. A technological explosion has expanded medical knowledge. This trend, combined with a divergent emphasis on cost control and quality and a transition to the information age, has brought patients, employers, and private and public payers into stronger decision-making roles.
A new type of leader is needed to provide vision that will help balance the interests of the many decisionmakers, patients, payors, and providers. Specifically, transformational leaders are needed to communicate organizational goals to followers, to provide for effective change, and to empower followers to make their own effective decisions in the shifting healthcare environment.
Healthcare professional literature, particularly in nursing, but also in physical therapy and social work, has
6
reflected a growing interest in and an expressed need for leadership (McCloskey and Molen 1987; Mueller and Rose 1987; Nielson 1989). The need for leadership is also echoed in the dietetic literature, where leadership is identified as a skill of growing importance for the future of the profession and its specialty areas (Wylie-Rosett et al 1990; Huenemann 1981; Hoover 1983; Rinke and Finn 1990; Finn 1991; Dodd 1992a; Dodd 1992b; Schiller et al 1993).
Even though there appears to be significant commentary on the subject of leadership among healthcare professionals, there is little research applying leadership theory to specific healthcare practice, such as dietetics. And research on transformational leadership theory is even more limited. To develop transformational leaders in dietetics, a research base must be established that will help determine those qualities of transformational leadership exhibited by leaders in dietetics.
Clinical dietetics represents the largest specialty area of dietetic practice and can serve as an initial model for transformational leadership research. Clinical dietitians in management positions would logically engage in leadership of their employees, and thus are an appropriate group for initial research. The Clinical Nutrition Management (CNM) practice group of The American Dietetic Association (ADA) is one identifiable cadre of
7
dietitians in clinical management positions, that is, its members provide direct supervision for the delivery of clinical nutrition services.
In this study, transformational leadership qualities were identified for clinical nutrition managers who were members of the Clinical Nutrition Management practice group of the ADA. Transformational leadership qualities were measured using an existing standardized and validated transformational leadership analysis instrument developed by Sashkin (1990a), the Leadership Behavior Questionnaire (LBQ). LBQ ratings from clinical nutrition managers and their employee evaluators were compared. The data were also associated with defined demographic variables: training/degree, length of time in management, number of people supervised, income, and participation in advanced practice activities (management, research, and scholarly activities).
Purpose and Objectives of the Study Problem Statement
In its new strategic plan developed in 1992, The American Dietetic Association established leadership development as a top priority for the Association (The American Dietetic Association 1992). Specifically, the acute- and chronic-care segment of the strategic plan was focused on clinical dietetic practice and leadership
8
skills were identified as essential for building stronger relationships and linkages with physicians and other healthcare decision-makers.
A first step in developing such leadership skills for clinical dietetics is to initiate research based on current leadership theory. The present descriptive study was designed to describe transformational leadership qualities of clinical nutrition managers who are members of the Clinical Nutrition Management practice group.
Research Objectives of the StudyResearch objectives of the study were the following:1. To identify transformational leadership qualities
of clinical nutrition managers.2. To compare transformational leadership qualities
of clinical nutrition managers as rated by clinical nutrition managers themselves and as rated by their employee evaluators.
3. To associate identified transformational leadership qualities with defined variables: training/degree, length of time in management, number of people supervised, income, and participation in advanced practice activities (management, research, and scholarly activities).
HypothesesSpecific null hypotheses formulated for this
investigation were the following:1. Clinical nutrition managers do not exhibit trans
formational leadership qualities as measured by the LBQ.
2. There are no differences between the transformational leadership qualities of clinical nutrition managers as rated by clinical nutrition managers themselves and as rated by their employee evaluators.
3. There are no associations between transformational leadership qualities of clinical nutrition managers and defined study variables.
Definition of TermsTerms used in this study were defined as follows:Clinical Nutrition Manager: a full-time dietitian who
supervised one or more dietitians or dietetic technicians providing direct, clinical patient nutrition care in an acute care hospital.
Leadership: a relationship between two or more members of a group, often including a structuring or restructuring of the situation and perceptions and expectations of the members (Bass 1990). Leaders are change agents and
10
modify the motivation or competencies of others in the group (Bass 1990) .
Transformational Leadership: a type of leadership bywhich leaders can have a major impact on their organization by using power and influence to empower employees to "make real" the leader’s long-range organizational vision (Sashkin and Burke 1990). Transformational leaders enact their vision by constructing and/or modifying organizational cultures (Sashkin and Burke 1990) .
AssumptionsThe following assumptions were made for this investi
gation :1) Subjects completed the demographic survey and LBQ
to the best of their ability.2) The LBQ is a reliable and valid instrument to
ascertain transformational leadership qualities.3) Clinical nutrition managers are effective in
their management positions as perceived by their employee evaluators.
Scope and Significance of the StudyClinical dietitians face many challenges in the chang
ing healthcare environment. Transformational leaders are needed in the field to help dietitians move beyond their
11
own self-interests to contribute to the long-term success of clinical dietetics and healthcare organizations.
To help develop transformational leaders in clinical dietetics it is important to determine transformational leadership qualities of dietitians who are already practicing in leadership roles, i.e., clinical nutrition managers. The comparison of these qualities as rated by clinical nutrition managers themselves and by their employee evaluators, helped to identify their strengths in transformational leadership. The results can now be used to provide the groundwork for strategic programs that will nurture the development of transformational leaders in clinical dietetic practice.
I
CHAPTER II LITERATURE REVIEW
IntroductionThe compelling need for leadership in today's society
to deal effectively with change is evidenced by the scores of books, publications, and rhetoric on the subject.Clark et al (1992) observed that in the past 15 years articles on leadership increased at twice the rate of articles in general. In 1978, Burns (p. 1) wrote in his Pulitzer Prize winning Leadership that "One of the most universal cravings of our time is a hunger for compelling and creative leadership." The healthcare literature also reflects a growing interest in and need for leadership to help manage the changing healthcare environment (McCloskey and Molen 1987; Mueller and Rose 1987; Nielson 1989, Finn 1991; Dodd 1992a; Dodd 1992b).
Such strong interest in leadership has been paralleled by the development of new definitions and theories of leadership. Traditional leadership theories are no longer viewed as comprehensive enough to help organizations move forward and take charge of their futures. The need for a new type of leadership, transformational leadership, has
12
13
emerged. Transformational leaders broaden and elevate the interests of their followers, generate awareness and acceptance among their followers of the purposes and mission of the organization, and move their followers to transcend their own self-interests for the good of the group.
In this chapter, classic leadership theories and the development of transformational leadership theory are reviewed. In addition, instruments for identifying transformational leadership are examined. Finally, research using those instruments, as well as relevant leadership research among the health professional literature, is described.
"Great Man," Situational, and Interactional TheoriesLeadership and its development have been topics of
interest and study since early civilization. From the early writings of Confucius, Plato, Caesar, the Old and New Testaments, the Renaissance Machiavelli, to more modern authors and philosophers, the subject of leadership has been explored. However, it was not until the 20th century that experimental research began in leadership and formal theories and models of leadership evolved. A number of those theories are described below.
Early leadership theory was based on the study of "great men" of history and society and founded on the Aristotelian philosophy that some men were born to lead
14
while others were born to be led (Bernard and Walsh,1990). Such a focus was explained by Dowd (1936, p. 151): "There is no such thing as leadership by the masses. The individuals in every society possess different degrees of intelligence, energy, and moral force, and in whatever direction the masses may be influenced to go, they are always led by the superior few." The so-called "great man" theorists studied and listed many attributes and personal characteristics that they believed distinguished great leaders from their followers.
This research laid the groundwork for development of a second theory, trait theory. Using group observation, personality inventories, and other techniques, the trait theorists described leadership in terms of specific traits and attributes, such as physical.factors, skill and ability, personality characteristics, and social characteristics (Bernard 1926; Bingham 1927; Tead 1935; Page 1935; Kilbourne 1935).
However, the consensus of research reviews by Bird (1940) and Jenkins (1947) was that neither the great man nor trait theorists successfully identified universal traits or personal characteristics that could be viewed as the hallmarks of leadership. Stogdill (1948) also reached that conclusion, and publication of his work marked a turning point in leadership study. For the next 25 years, trait theory was abandoned and leadership research focused
15
almost exclusively on situation-specific and leader- behavior analyses.
There was a second tenet to the original thesis of Stogdill (1948). He specifically identified five sets of personal characteristics (capacity, achievement, responsibility, participation, and status) that he believed were consistently associated with leadership in many of the leadership research studies. The theme of common personal characteristics among leaders was lost, however, until it was revived by the work of Downton (1973), House (1977), and others in more recent years.
Criticism of the great-man and trait theories gave rise in the 1940s to the development of the situational theory of leadership. As an antecedent to trait theory, situational theory suggested that great leaders evolve because of events and circumstances. Murphy (1941) proposed that "leadership does not reside in a person, but is a function of the occasion.”
While the trait and situational theories of leadership were attempts to define leadership by a single set of circumstances, other theorists took a broader approach. Theorists such as Gibb (1947) believed leadership was relative to the situation and was determined by the goals of the group, a process of mutual stimulation by which the group's goals and the leader's characteristics interacted. This personal-situational or interactional approach made
16
both the trait and situational theories of leadership usable, for the first time linking the characteristics of the leader to the group. However, a negative aspect of interactional theory was that it did not predict outcomes or prescribe actions that could help direct leaders in their roles (Bernard and Walsh 1990).
Style and Behavior TheoriesIn the 1960s, researchers began to focus on predicting
outcomes, that is, the effectiveness of leaders in their roles, and prescribing actions and thus developing approaches that would help train leaders. They moved away from studying leadership in children's and social groups as used by earlier theorists and started to examine leadership in work groups. A number of different models were developed to describe leadership styles and behaviors.
Work by White and Lippit (1960) was focused on decision-making and control and they described a continuum of three leadership styles: autocratic, democratic, andlaissez-faire. The autocratic leader exerted a high degree of control, with minimum freedom for the group members. At the opposite end of the continuum was the laissez-faire leader, providing maximum freedom for group members and minimum leader control. The democratic leader was in the middle, with varying degrees of freedom and control. From this research two important findings were
17
identified. First, it seemed that leadership behavior directly influenced the climate and productivity of the group. A second finding was that democratic leadership was the most successful style; the democratic leader allowed participation in decision-making while supporting, guiding, and counseling the followers. Further research on transformational leadership theory has reinforced both of those findings.
Likert (1967), at the University of Michigan, also investigated leadership styles and discerned four styles based on an autocracy-democracy dimension:
1) exploitative authoritative style, in which leader exploited subordinates;2) benevolent authoritative style, in which leader was paternalistic, with authoritarian decision-making and control using direct hierarchical pressure for results;3) consultative style, in which leader maintained decision-making option, but consulted with employees;4) participative style, in which decisions were reached by group consensus and the leader gave direction.
These results were supportive of the earlier work by White and Lippit (1960), as the participative leadership style was again found to be the most effective style of leadership.
18
Differing somewhat from the investigations of leadership styles, leadership behavior was the emphasis of two parallel research programs at Harvard University and The Ohio State University. At Harvard University, Bales (1958) worked with college undergraduates and identified two important behavioral dimensions of leadership, behavior centered on task accomplishment and behavior centered on interpersonal relations. Bales found leaders typically exhibited high levels of both types of behavior.
Investigators working with The Ohio State University Leadership Studies (Fleishman 1951, 1953; Halpin and Winer 1957) identified two similar factors consistently related to leader behavior. These were characterized as consideration and initiating structure. Consideration was described as the degree of leader-follower interactions and communication including the mutual trust, respect, and warmth a leader exhibited toward followers. Initiating structure was referred to as behavior related to giving task directions, specifically the degree of organizing and defining work and establishing clear channels of communication and methods of accomplishing the group task. The Leader Behavior Description Questionnaire was developed to measure consideration and initiating structure (Stogdill 1963). That tool is still used today. Research to confirm the consideration/initiating structure theory has often yielded conflicting findings, yet leaders scoring
19
high in initiating structure and consideration seem to have many cohesive and productive followers (House 1971).
The Managerial Grid® developed by Blake and Mouton (1964) was closely related to the initiating structure and consideration model and was used to support training programs for improving managerial performance. The Blake and Mouton model centered on a task/production versus a relation/people orientation. A grid was used to plot five leadership styles:
1) authority/obedience style, maximum concern for production, minimum concern for people;2) country club management style, minimum concern for production and maximum concern for people;3) team management style, integration of production and people concerns;4) impoverished management style, minimum concern for both production and people;5) organization man management style, conforming to status quo.
The team management style was believed to be the most desirable, but continued research failed to confirm that effective leaders actually engaged in this type of leadership behavior (Larson et al 1976).
Situational or Contingency TheoriesThe above research on leadership styles and behaviors
helped describe how leaders behaved when interacting with
20
followers or potential followers. Yet, such research did not allow for variance in situations. Thus, the researchers typically assumed that leadership behavior caused or determined group or organizational outcome and did not consider, for example, the interaction of followers (Jago 1982). More complex leadership models have been developed to help explain such situational contingencies, in which different leadership traits or behaviors may be effective in different situations. These situational models contributed two important elements to leadership theory, consideration of the situation and consideration of the followers.
Fiedler's Contingency Model (Fiedler 1967; Fiedler and Chemers 1974) incorporated a situational hypothesis with personal characteristics and behaviors of leaders.Fiedler theorized that leadership effectiveness was contingent on the leader's motivational system and the degree of control or influence a leader had in a situation. Thus, there were two parts to the model.First, a questionnaire was used to rank the leader as task-motivated or relationship-motivated. The distinction between these two classifications was similar to the distinction made between considerate leader behavior and initiating structure leader behavior as identified in The Ohio State Studies (Fleishman 1951, 1953; Halpin and Winer 1957). Second, the leadership situation was characterized
21
as favorable or unfavorable in the Fiedler Contingency Model by three critical dimensions:
1) leader-follower relations, the degree of friendliness of the leader and the degree to which group members trusted/liked the leader and were willing to follow the leader's guidance;2) task structure, the degree of structure required in a job;3) position power, the degree of formal power and influence of the leader, including ability to reward/punish.
Using the motivational system and degree of control dimensions, Fiedler and Chemers (1974) then derived eight classification schemes with prescriptive suggestions for matching a leadership style with a situation.
The Fiedler Contingency Theory was unique in that it was the only theory developed at the time based on specific leadership traits and behaviors (Fiedler and Chemers 1974). Other contingency models were developed using just leader behavior as the foundation. For example, the path-goal theory developed by House (1971) was behavior based. The foundation of that theory was individual motivation. The two principles of the theory were certain behaviors resulted in achieving certain goals, and the desirability of achieving goals influenced behavior.
22
The theory of House (1971) was labeled path-goal because behavior was expressed in terms of the leader’s influence in clarifying the paths or routes followers pursued toward work and personal goal attainment. Four leadership styles were delineated:
1) directive, authoritarian;2) supportive, showed concern for others;3) participative, asked for and used suggestions;4) achievement, set goals for subordinates and showedconfidence in subordinates.
House (1971) believed leaders could use varying styles depending on two situational factors: the personalcharacteristics of subordinates and the environmental demands subordinates must cope with to accomplish goals/satisfy their needs. Thus, the path-goal theory introduced subordinates as an important variable.
The life-cycle theory (Hersey and Blanchard 1977) also considered subordinates as a factor in leadership. It predicted the most appropriate leadership style based on the level of maturity of the followers and evolved from the initiating structure and consideration model of leader behavior. Follower maturity was rated based on its relationship to a specific task. The theory had several elements:
1) capacity to set high/realistic goals for self;2) willingness and ability of follower;
23
3) education, experience, job maturity, and psychological maturity of the follower.
Hersey and Blanchard proposed that with increased follower maturity less structure and emotional support were needed.
Finally, Vroom and Yetton (1973) composed a contingency model that attempted to specify situations that would impact the effectiveness of decision-making.The decision-making process was proposed to be affected by three factors:
1) quality/rationality of decision;2) acceptance/commitment by subordinates to execute decision effectively;3) amount of time required to make decision.
Based on these factors, a decision tree was developed to guide leaders in a choice of appropriate levels of subordinate participation. Research using the model documented that a leader's willingness to use participative decision-making was affected more by the decisionmaking situation than an autocracy-democracy "style." For example, leaders were more willing to use participation in situations requiring a high quality, technically adequate solution than in situations that were trivial or had no technical component. Thus, Vroom and Yetton expanded the earlier work of White and Lippot (1960) and Likert (1967), who had considered only leadership style as a factor in evaluating leadership.
24
Motivational TheoriesThe follower was an important variable in leadership
research, as evidenced by the theories of House (1971), Hersey and Blanchard (1977) and Vroom and Yetton (1973) .To gain a better understanding of the follower, leadership researchers turned to motivational and organizational models. Those models were developed to focus on the needs and motivations of followers and to examine factors that satisfied followers or decreased their dissatisfaction.The premise of motivational theories was that satisfied employees were more productive and thus lead to more productive organizations (Barker 1990) .
One of the early theories of motivation was developed by Maslow (1943) . Maslow built his theory of human motivation on a hierarchy of human needs; physiological, safety, social, esteem, and self-actualization needs. He proposed that all needs were present in an individual, but that physiological needs were the highest priority when unsatisfied. The remaining needs followed stair-step fashion, with self-actualization becoming top priority only when all other needs were satisfied.
From a different approach, McGregor (1960) developed theories of motivation based on his view that the leader's attitude about human nature influenced leadership behavior. He proposed two theories, Theory X and Theory Y. Theory X described the past, or traditional, view of
25
direction and control: people disliked and avoided workand had to be forced to engage in goal-directed activity. Thus, Theory X leaders had to direct and control workers. Theory Y was a separate philosophy that proposed an integration of individual goals with organizational goals. Theory Y was based on the view that human beings were self-directed and would engage in goal-directed activity by choice if they agreed with the goals. Theory Y leaders provided a supportive working environment by eliminating obstacles and encouraging opportunities for growth.
Ouchi (1981) developed Theory Z as an alternative motivational approach to the Theory X and Theory Y of McGregor (1960). Theory Z referred to an organization's style rather than an individual manager's style. It evolved from Japanese management traditions and was based on the belief that involved workers are the key to better quality and productivity. Theory Z organizations created an environment where there was a commitment to mutual goals.
Another motivational theory was developed by Herzberg (1966). His motivation-hygiene theory, also known as the two-factor theory, proposed that job satisfaction and job dissatisfaction were separate but related factors.Herzberg labeled factors influenced by the job environment as hygiene factors: organizational policies, workingconditions, interpersonal relations, money, status,
security, and personal life. Factors related to the job content were labeled motivation factors: achievement,recognition, challenging work, responsibility, advancement, and growth. Herzberg documented that employees who were dissatisfied with hygiene factors had lower performance. Three motivation factors— the work itself, opportunity for advancement, and responsibility— were the most important factors for long-lasting, positive attitudes about the job.
Summary of Traditional Leadership TheoriesThe 20th century has seen the development of many new
theories of organizational leadership. Three common themes emerged (Barker 1990). First, a democratic, participatory style was one of the most effective forms of leadership. Second, it was important for leaders to support the tasks/goals of the organization and be attuned to the interpersonal needs and relationships of their followers. Finally, behaviors and attitudes of leaders affected the followers' satisfaction and productivity.
Transformational Leadership Theory None of the trait, behavior, situational, or
motivational theories seemed to fully explain and provide a model for effective leadership in the organizations of today. There were several reasons why the theories were ineffective. Most of the theories were developed from
27
research on supervisors and lower-level managers, not on top executive leaders who would have been more attuned to organizational goals (Sashkin and Burke 1990) . Furthermore, contemporary workers were no longer fulfilled only by their work and by respectful treatment (Barker 1990). They also wanted opportunities for personal growth and development. Thus, there had been a need for the development of a new theory of leadership that can help organizations be more successful and maintain enthusiasm in their workers.
The theory of transformational leadership was developed over the past decade to meet this need for a new theory of leadership. Today, it is believed to be a more effective theory for organizational leadership than previous theories because it focuses on leadership development, how individuals become leaders, as well as considers leadership within the context of the organization by focusing on achievement of organizational goals. Charisma and power have been identified as primary components of transformational leadership theory and explaining how individuals become leaders. Both charisma and power have their roots in older leadership theories.
In 1947, the German social scientist Weber (1947) identified charisma as one of three principal types of authority or leadership. The other two types identified were traditional authority (rule based on custom) and
28
rational-legal authority (rule based on law). Weber described traditional and rational-legal authority as directly related to economic activity, that is, the followers of these types of leaders were generally their paid staff. In contrast, he viewed charisma as a form of noneconomic authority because followers of charismatic leaders gave their support freely, and without pay. A further distinction Weber made (1947, p. 361) was in the actions of the leaders: "Both rational and traditionalauthority are specifically forms of everyday routine control of action; while the charismatic type is the direct antithesis of this." In summary, Weber proposed that charismatic leadership was not bound by rules.
While the theories of Weber (1947) made significant contributions to the field of sociology in his day, leadership researchers in the decades of the 1940s and 1950s were moving away from studying traits and, instead, were examining leadership behaviors and styles. Thus, the relevance of Weber's work to leadership theory was not recognized for a number of years. Downton (1973) was one of the first to focus on Weber's views on charisma. In developing his own model of "rebel leadership," Downton believed that it was important to borrow theoretical perspectives from others in related fields to help illuminate thinking about leadership and revolutionary change.
29
House (1977) also developed a theory of charismatic leadership, stemming in part from the work of Weber.House argued that while several writers had proposed that charismatic leadership existed in organizations (Runciman 1963; Shils 1965; Dow 1969; Oberg 1972), their work was almost exclusively theoretical and not based on empirical tests. House reviewed sociological and political science literature on charisma and then developed his own propositions on charismatic leadership. Sashkin (1977) commented that the review of House was one of the most significant treatments of leadership from a personality perspective since the demise of leadership trait theory.
In more recent years, House (1988) has specifically addressed the power need of effective charismatic leaders. Power was also a focus of research by McClelland (1975) and McClelland and Burnham (1976). They argued that power was an important basis for motivation and that good managers had high power needs tempered with high degrees of self-control.
The reports of Downton (1973), House (1977, 1988), and McClelland (1975) were significant in helping to lay the groundwork for the development of new models of leadership. Yet, political scientist and historian Burns (1978) was credited with the theory of transformational leadership and with bringing to the forefront the economic versus noneconomic sources of authority first defined by
30
Weber (1947). Burns developed his theory by examining profiles of historically and socially significant leaders; he described power as essential to leadership.
Burns (1978) considered several important elements in his theory. First, he addressed the relationship of leaders and followers. He described this relationship as one in which the leader recognized, appealed to, and acted on both his/her own and the followers1 values and motivations. Second, leaders had certain values, motives, and needs. Transformational leaders operated at a level of need and value higher than their followers did, but not so high that they lost perspective of their followers. Transformational leaders worked to help followers satisfy the lower level needs identified by Maslow (1943) , such as physiological, safety, and belongingness and love. After lower-level needs were satisfied, higher-level needs, including esteem and self-actualization, could emerge and be fulfilled. Thus, transformational leaders helped followers become aware of and clarify their needs, define their values, and also stimulated the followers to purposeful action.
A third element in transformational leadership was that values, motives, and needs were used in a context of competition and conflict to realize goals independently or mutually held by both leaders and followers. Conflict and competition could be viewed negatively, yet both were
31
needed to facilitate change. The role of the transformational leader was to shape conflict so it could be a source of growth, learning, and pressure for change.
The final element in the transformational theory of Burns (1978) was power. Transformational leaders had certain goals and a capacity to secure changes in both the behavior of others and in the environment by using economic, political, institutional, and personal resources. Burns also believed that a sense of purpose was crucial to power in transformational leadership and that the purpose was always in the best interest of the leaders and followers.
Burns (1978) was one of the first to make the distinction between transactional and transformational leaders and to link leadership to organizational goals.He described transactional leaders as individuals who take the initiative with followers to exchange valued things, that is, things with economic, psychological, or political benefit. Transactional leadership was described as an exchange process that satisfied the needs of the leader and the follower; while both the leader and follower may have had related purposes, they were not pursuing common goals. Specifically, he explained that under transactional leadership the exchange of rewards for services limited how much effort was given by subordinates. Transactional leadership also limited the satisfaction of
32
subordinates and their effectiveness in contributing to the goals of the organization.
On the other hand, transformational leaders engaged with followers in such a way that leaders and followers raised one another to higher levels of motivation and morality. Burns (1978) further believed that the transformational leader was able to articulate and share a realistic vision of the future, stimulate subordinates intellectually, and help them develop into leaders. Transformational leaders also paid attention to the differences among subordinates and were able to raise the level of subordinate motivation and performance to better meet organizational goals. It was proposed that transformational leaders were the ones best able to promote dramatic change within individuals, groups, and organizations.
Perhaps what best distinguished transactional leadership from transformational leadership was the nature of the goals pursued. Transactional leadership occurred when two persons exchanged goods or services to realize independent goals and objectives. Transformational leadership resulted when leaders helped shape and elevate the motives, values, and goals of followers, and thus the separate interests of leader and followers were united in the pursuit of "higher level" goals.
33
From this perspective, transactional and transformational leadership in the theory of Burns (1978) were similar to the economic and noneconomic forms of leadership described by Weber (1947). Transactional leadership was based on economic or quasi-economic exchanges between leader and followers as the transactional leader sought to fulfill current material and psychic needs. In contrast, the transformational approach was based on a noneconomic interchange, similar to the charismatic leader proposed by Weber. Transformational leaders sought to identify and develop higher-level needs such as the esteem and self- actualization needs described by Maslow (1943). By developing higher level needs the followers were engaged more fully in their work.
While similar to the economic/noneconomic premise of the theory of Weber (1947), the transformational leadership theory of Burns (1978) differed from other traditional leadership theories in several ways. First, Burns incorporated both the leader and follower interaction. Second, he considered how people became leaders and the characteristics that shaped them. Burns believed that people were not necessarily born transformational leaders. He also believed in power as a principal factor for leadership. Finally, Burns proposed the unique concept that under transformational leadership followers could be converted into leaders.
I
34
The theory of Burns (1978) has been further researched and defined. Bennis and Nanus (1985) studied successful organizational leaders and documented four strategies of transformational leaders, stressing the idea that transformational leadership is not so much the exercise of power itself but rather the empowerment of others.
Bass (1985) undertook significant research to define his own theory of transformational leadership. In expanding on the theory of Burns (1978), Bass postulated that transformational leaders did not necessarily need to move followers to higher levels of needs along the hierarchy of Maslow (1943) but rather that leaders could be transformational by broadening the current needs of the followers at their existing levels. A second significant difference was that Burns saw transformation as a process for furthering good, not evil. Bass argued that even leaders such as Hitler were transformational, despite the methods employed, because transformation occurred; Germany was indeed transformed, yet destroyed under Hitler's reign. A final difference, and perhaps the most important, was that Burns perceived transformational and transactional leadership at opposite ends of a single continuum. Bass proposed that leaders exhibited a variety of patterns of leadership but that most leaders did employ both transactional and transformational leadership in varying amounts.
r
35
Bass (1985) tested his theory by developing and validating an instrument to measure transformational and transactional leadership. Sashkin and Burke (1990) also developed a model and instrument for transformational leadership. They argued that their instrument more adequately incorporated key theoretical elements of transformational leadership, power and its use within organizations, than did the instrument of Bass. The theories and instruments of Bass, Sashkin and Burke, and others are discussed in detail in the next section of this chapter.
Transformational Leadership Measures As theories of leadership have been developed over
time, so too have the various instruments used to measure and evaluate leadership. Thus, from the simple lists of leadership qualities that once characterized the "trait" approach to leadership, the more elaborate leadership tools of today have been evolved and include many factors; leadership actions, traits and behaviors, and the roles of leaders and followers. Several tools specifically related to the measurement of transformational leadership have been described in the literature. These tools were most often described as measures of inspiration and influence (Clark and Clark 1990) and are discussed in detail below.
[
36Multifactor Leadership Questionnaire
Bass (1985) developed one of the first transformational leadership tools, the Multifactor Leadership Questionnaire (MLQ). In the past 10 years, this tool has been refined based on extensive research on leaders at various levels of management in both public and private organizations.
Three constructs were the basis of the instrument: transformational leadership, transactional leadership, and nonleadership. The following leadership behaviors associated with those constructs were assessed by using the MLQ:
1) transformational leadership: exceptional leadership, including an ability to transform individuals and organizations;
2) transactional leadership: effective leadershipused to motivate followers to achieve agreed-upon and expected levels of performance;
3) nonleadership: ineffective leadership characterized by avoidance of responsibility and action.
The MLQ was developed to provide a reliable method for differentiating between the inspirational and charismatic leader and the leader who practiced a "hands-off" style, one who only intervened when something went wrong. The MLQ is comprised of an 80-item questionnaire that identified and measured key leadership behaviors documented in prior research to be strongly associated with both
37
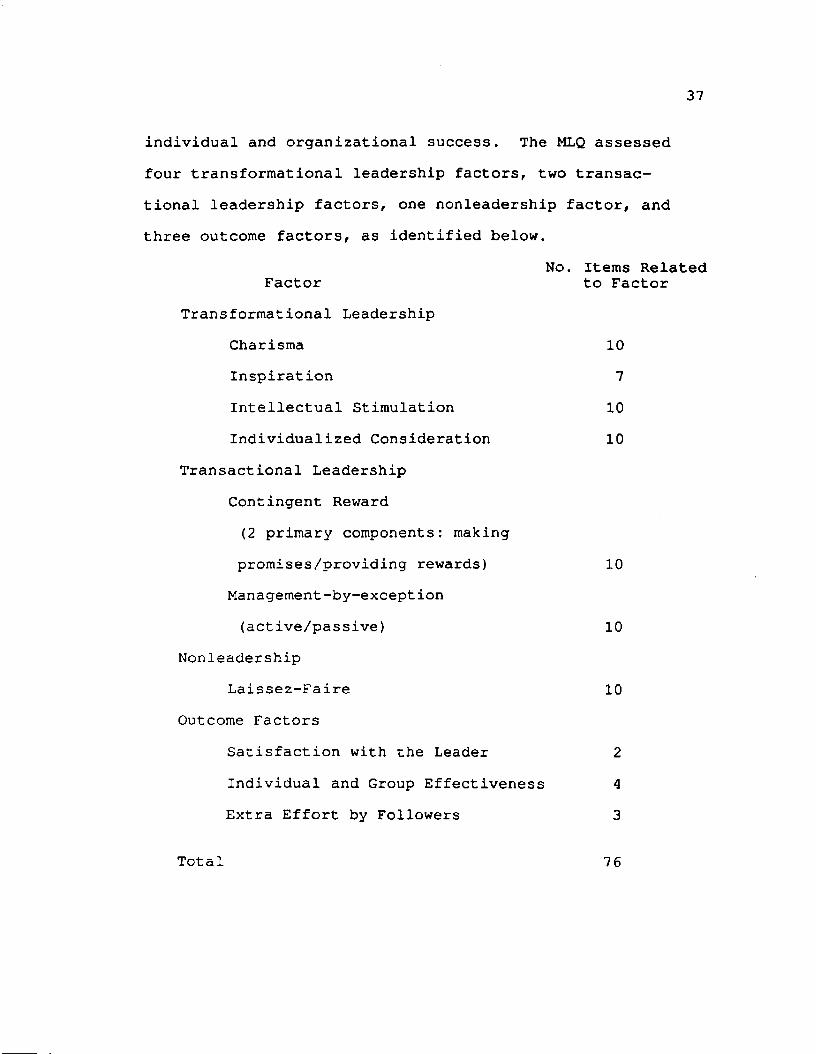
individual and organizational success. The MLQ assessed four transformational leadership factors, two transactional leadership factors, one nonleadership factor, and three outcome factors, as identified below.
No. items RelatedFactor to Factor
Transformational LeadershipCharisma 10Inspiration 7Intellectual Stimulation 10Individualized Consideration 10
Transactional Leadership Contingent Reward (2 primary components: making promises/providing rewards) 10
Management-by-except ion (active/passive) 10
NonleadershipLaissez-Faire 10
Outcome FactorsSatisfaction with the Leader 2Individual and Group Effectiveness 4
Extra Effort by Followers 3
Total 76
Four additional items on the questionnaire focused on biographical data and allowed respondents to rate the degree of confidence they had that the MLQ identified and measured the appropriate range of leadership behaviors.
Individuals completed the MLQ rater form evaluating how frequently they had observed a leader/colleague engage in specific transformational, transactional, or nonleadership behavior. Likewise, leaders completed the MLQ self-rating form, evaluating how frequently they believed they engaged in the same leadership behaviors toward supervisees/colleagues. A five-point rating scale (0-4, with 0 equal to "not at all" or "not effective") was used for both forms. Respondents marked their ratings directly on computer-scorable answer sheets which were forwarded to Consulting Psychologists Press for computer scoring.
In discussing the theoretical basis of the MLQ, Bass and Avolio (1990) commented that traditional leadership research and training were often directed toward helping leaders become more transactional to make first-order change, that is, change of degree. Such change included maintenance of quantity or quality of performance, substitution of one goal for another, shifting of attention from one action to another, and reduction in resistance to particular changes.
Transactional leadership is based on an exchange process. It is characterized by two types of leader
39
behavior: contingent reward, in which followers' needsare met if their performance measured up to their contract with their leader, and management-by-exception, in which leaders avoid transactional relationships with followers and only give (negative) feedback when performance is poor. Both types of transactional leadership behavior, contingent reward and management-by exception, are measured by the MLQ. Transactional leadership also involves the implementation of decisions within a given contextual framework, and thus the results are limited to expected effort and expected performance.
In contrast, transformational leadership represents a higher order of change in orientation that actually increases the rate at which the performance of a group improves. Higher-order changes involve significant changes in attitudes, beliefs, values, and needs. Thus, the transformational leader motivates followers to do more than they originally thought possible.
Transformational leadership is characterized by several different leader behaviors that are measured by the MLQ. The transformational leader is often viewed as charismatic by followers, wielding significant power and influence. The transformational leader is inspirational, articulating shared goals in simple ways and providing visions of what is possible and how to attain it. The transformational leader uses intellectual stimulation to
40
help followers think about old problems in new ways and to question their own beliefs and assumptions. In this way, followers learn to solve problems on their own with creativity and innovation.
Individualized consideration is another behavior important in transformational leadership that is measured by the MLQ. The transformational leader understands and shares followers' concerns and developmental needs, treating each follower uniquely. The transformational leader helps expand and elevate those needs to maximize and develop their full potential, and perhaps most importantly, links follower needs to the organization's mission. Focusing and establishing congruence between follower and organizational needs is viewed as crucial to the transformational leader's success. This success is defined in the model as heightened motivation to attain designed outcomes (extra effort) and performance beyond expectations.
An important consideration in the model is that transformational leadership does not replace transactional leadership. Instead, transformational leadership augments transactional leadership in achieving goals of the leader, follower, group, and organization. Thus, individuals completing the MLQ can score on both transformational and transactional-related factors.
The factors used in the MLQ were conceptually and empirically derived from independently conducted factor analyses (Bass 1985). First, a review of literature and an open-ended survey of 70 senior executives were used to generate 142 leadership behavior items. Those items were next reviewed and sorted into transformational, transactional, or "can't say" categories by 11 graduate students. A total of 73 items were selected and then, using data from a sample of 176 senior military officers, a factor analysis using varimax rotation was conducted (Bass 1985). Seven leadership factors emerged: charisma, inspiration,intellectual stimulation, individualized consideration, contingent reward, management-by-exception, and laissez- faire. Two subsequent replications of the original factor analyses (Hater and Bass 1988; Seltzer and Bass 1990) yielded the same factors.
The reported alpha reliability coefficients for the 10 factors measured by the MLQ Rater Form yielded a range of 0.77 to 0.95, and 0.84 to 0.94 for supervisees and coworkers, respectively (Bass and Avolio 1990). The alpha reliability coefficients for the MLQ Self-Rating Form were documented to be lower for each factor, with a range of 0.60 to 0.92 (Bass and Avolio 1990). Bass and Avolio reported one possible reason for this difference was that leaders interpreted each item with respect to multiple followers, while followers rated a single leader. Thus,
I
42
they recommended generally using the followers' descriptions of leaders for research, due to the higher reliabilities.
Test-retest reliability for the MLQ over a six-month period was computed for the Rater and Self-Rating forms using data collected on 33 middle- to upper-level managers (Bass and Avolio 1990). The test-retest reliabilities ranged from 0.44 to 0.74 for the Self-Rating Form and 0.52 to 0.85 for the Rater Form. However, those reliabilities were thought to underestimate true test-retest reliability, since the management group received team development and individual training during the six-month interval.
Several researchers have correlated the MLQ scales with outcomes. Transformational leadership scores were uniformly more strongly correlated with higher ratings of organizational effectiveness than were transactional scores (Bass and Avolio 1990). Hater and Bass (1988) showed managers labeled as high performers based on performance appraisal ratings by their superiors were independently evaluated by followers as being more transformational and possessing certain characteristics of transactional leadership (they were high in contingent reward leadership). Similar patterns have been described by Bass and Yammario (1988), Avolio et al (1988), and Onnen (1987) .
43
Leadership Practices InventoryKouzes and Posner (1991) developed the Leadership
Practices Inventory (LPI), which included components they believed important in transformational leadership. The LPI was developed to measure empirically the conceptual framework developed in case studies of managers' personal best experiences as leaders.
The LPI comprised a 30-item questionnaire that identified and measured six key leadership behaviors related to each of five main leadership practices:
1) Challenging the processa) Searching for opportunitiesb) Experimenting and taking risks
2) Inspiring a shared visiona) Envisioning the futureb) Enlisting others
3) Enabling others to acta) Fostering collaborationb) Strengthening others
4) Modeling the waya) Setting an exampleb) Planning small wins
5) Encouraging the hearta) Recognizing contributionsb) Celebrating accomplishments.
Individuals completed the LPI rater form, based on their observation and work with the leader/colleague. Leaders completed the LPI self-rating form, evaluating how frequently they believed they engaged in the same leadership behaviors toward supervisees/colleagues. A five-point rating scale (1-5, with 1 equal to "rarely") was used for both forms. Respondents marked their ratings directly on the inventory and then transferred their ratings to a scoring sheet attached to the form. Respondents returned their forms for scoring or used the LPI self-assessment and analysis to complete their own scoring.
The LPI was developed based on the belief of Posner and Kouzes (1990) that leadership was a skill distributed normally in the population and that there was a clear distinction between the process of managing and the process of leading. Managers were able to get other people to "do," but leaders were able to get other people "to want to do."
Posner and Kouzes (1987) further postulated that people use an actual pattern of behavior to lead and achieve extraordinary results. To investigate this pattern, they evaluated the times when leaders performed at their "personal best" and asked followers what they looked for or admired in a leader.
45
Posner and Kouzes (1988) collected qualitative data on what leaders did by asking managers attending a variety of public and contract management development seminars to describe a "personal best as a leader," defined as an experience in which they accomplished something extraordinary in an organization. The 12-page survey included 37 open-ended questions. Over 850 surveys were collected. A short form survey (one or two pages) was collected from an additional 450 managers.
Thirty-eight in-depth interviews with middle and senior-level managers were also conducted. The case studies from the surveys and interview notes were then content-analyzed by the authors and validated by two separate outside raters. From this analysis, the five basic leadership patterns, each consisting of two basic strategies, emerged. Greater than 80% of the behavior and strategies described in respondents' personal best case studies and interviews were accounted for by these factors (Posner and Kouzes 1990).
The LPI was then designed based on lengthy and repeated feedback from respondents and factor analyses of various sets of behaviorally based statements (Posner and Kouzes 1990). The LPI was originally completed by 120 MBA students. Feedback discussions with nine professionals in psychology, organizational behavior, and human resource management helped further refine the inventory. The
46
instrument was subsequently administered to more than 2,100 managers and their subordinates and fine-tuned based on analysis for internal reliability and construct validation through evaluating the underlying factor structure (Posner and Kouzes 1990).
More recent internal reliability data were reported for a sample of 2,87 6 managers and executives and their subordinates (Posner and Kouzes 1990). Internal reliabilities ranged from 0.77 to 0.90, with reliabilities ranging from 0.70 to 0.84 on the LPI-Self to 0.81 to 0.91 on the LPI-Other. Test-retest reliability determined from a convenience sample of 57 MBA students averaged about0.94 (Posner and Kouzes 1990). Finally, the Marlowe- Crowne Personal Reaction Inventory (Crowne and Marlowe 1960) was used to test for social desirability. The Marlowe-Crowne Personal Reaction Inventory was a scale of 33 items representing behaviors that were culturally sanctioned and approved but were improbable of occurrence. None of the correlations for a sample of 30 middle-level managers were statistically significant (Posner and Kouzes 1990) . Factor analysis of the LPI using principal factoring with iteration and varimax rotation documented that the factor structure of the LPI was consistent with the a priori conceptual model (Posner and Kouzes 1990) .
In comparisons between the LPI-Self and LPI-Other responses, frequency scores on the LPI-Self were generally
47
higher than those on the LPI-Other for all five leadership practices (Posner and Kouzes 1990). Normative data from another study of 73 senior human resource management professionals was used to compare male and female respondents. One significant difference was found: femalemanagers rated themselves as engaging in "encouraging the heart" behaviors significantly more often than did male managers (Kouzes and Posner 1991).
The LPI was also evaluated in relation to managerial effectiveness. In a study of 514 subordinates, over half of the evaluations (measured by a leadership effectiveness scale developed by the researchers) could be explained by subordinates' perceptions of the behavior of their managers along the conceptual framework of the LPI (Posner and Kouzes 1990).
Finally, preliminary research was conducted utilizing pre- and post-test administration of the LPI in relation to a week-long leadership development program. Participants showed an average 15% increase in leadership behaviors (as measured on the LPI-Other) 10 months after the program (Posner and Kouzes 1990).
Leadership Behavior QuestionnaireSashkin and Burke (1990) developed the Leadership
Behavior Questionnaire (LBQ), which, they commented, best measured transformational leadership in an organizational context. The LBQ was intended primarily for use in
48
management training and development and to raise effectively the levels of awareness of participants about the important dimensions of organizational leadership.The LBQ had fifty items, with five items forming each of 10 scales. On each scale, two items (40%) were negatively stated (this was not always obvious) and three (60%) positively stated, to help reduce social-desirability bias.
The items were rated c (completely true), m (mostly true), s (somewhat true), 1 (a little true), or n (not at all true). These letters were then transferred to numeric scores using a pressure-sensitive, sheet, with one equal to "not at all true" if the item was stated positively and five equal to "not at all true" if the item was stated negatively.
The numeric scores for the items were added to yield a scale score (Sashkin and Burke 1990). The 10 scales are:1) focused leadership, 2) communication leadership,3) trust leadership, 4) respectful leadership, 5) risk leadership, 6) bottom-line leadership, 7) empowered leadership, 8) long-term leadership, 9) organizational leadership, and 10) cultural leadership. Detailed descriptions of these scales are included in Appendix A. The scales formed three "cluster" scores. The one through five scale-scores were added to form an overall Visionary Leadership Behavior Score. Scores six, seven, and eight were added to yield an overall Visionary Leadership
49
Characteristics Score. The final two scale scores were added to yield an overall Visionary Culture Building Score.
Adding the three summary scores yielded an overall Visionary Leadership Score. The leader's Interpretive Guide (Sashkin 1990a) helped the respondent through the process of calculating these scores and provided visual representations and an explanation of the scores {Appendix A).
In developing their theoretical foundation of the LBQ, Sashkin and Burke (1990) proposed that the study of organizational leadership had been neglected in favor of a focus on "supervisory management" or the role of individuals at middle and lower levels of the organizational hierarchy. Thus, there had been a gain in knowledge about management at lower levels, but proportionately little real knowledge about leadership, the process top level leaders used to design and direct social-organizational processes.
Sashkin and Burke (1990) explained that for a comprehensive understanding of organizational leadership, it was important to go beyond earlier approaches to leadership study by incorporating three key elements: 1) theleader's personal characteristics, 2) the leader's effect on organizational functioning and culture, and 3) the
50
leader's behavior. These three key elements formed the basis of their theory.
Sashkin and Burke (1990) defined three specific personal characteristics that differentiated effective organizational leaders from others, based on the work by House (1977, 1988), McClelland (1975), and Jaques (1976, 1986). First was impact belief, the belief that one can control or affect one's environment. Power need was the second personal characteristic. Effective leaders used power to empower others so they could enact the leader's vision of the organization. The third personal characteristic was cognitive time span, meaning that effective organizational leaders at the top levels of an organization must have had relatively long time spans of vision, thus they must have thought and functioned over periods of at least a decade or two.
Sashkin and Burke (1990), citing the work of Weber (1947), Parsons (1960), and Schein (1985), believed it was also possible to assess the leader in the organizational context. Specifically, it was important to assess whether the leader had a positive impact on the organization's functioning (defined as adapting, attaining goals, coordinating or integrating the efforts of organizational members and groups, and maintaining the organization's cultures) . Another determination was whether the leader was successful in defining and inculcating within the
51
organization's culture the values that supported those functions.
The most overt aspect of Sashkin and Burke's (1990) theory of organizational leadership is the emphasis on actions taken by leaders. These actions were first defined by Bennis (1984): an ability to focus others on key points and concepts in interpersonal discussions, effective communication, actions that demonstrated others could place trust in the leader, a consistency in frequent expressions of respect and personal concern including a base of self-respect, and an ability to take risks by constructing opportunities for others to "buy in" to the leader's ideas and programs and take an ownership role in making the leader's vision real.
Finally, Sashkin and Burke's (1990) theory also incorporated visionary leadership theory, that is, that effective transformational leaders believed they could have major impact by using power and influence to empower organization members to make the leaders' long-range organizational visions real. Sashkin and Burke explained that three important factors differentiated their organizational leadership approach from other transformational leadership theories. First, they incorporated into their theory all three critical variables: personal characteristics of leaders, organizational contexts in which leaders acted, and the specific actions leaders took, both
52
organizationally and interpersonally. Second, they included a focus on the ways transformational/visionary leaders empowered followers to develop their organizational visions. Finally, they developed micromacro integration, that is, they provided an opportunity for individual-level variables to be meshed with social- organizational level factors.
The LBQ was initially developed as a 24-item research and training instrument based on the work of Bennis (1984), who had identified characteristics of exceptionally effective chief executives across a wide range of organizational settings (Sashkin 1990b). Following its publication in 1984, ongoing research with managers and graduate students helped the researchers to improve scale coherence and document reliability and provided minor wording changes. Over 20,000 managers used this original LBQ, making it one of the most widely used measures of organizational research.
Sashkin (1990b) recently undertook a major revision of the instrument. There were two reasons for the revision. First, scales six through 10 of the original instrument were often viewed as minimally useful or actually distracting from the utility of the instrument. For example, some of the scales measured traditional leadership functions, often referred to as "task" and "relationship" styles. Yet, many of the individuals using the LBQ were
53
interested in the new concepts of leadership and these scales sometimes distracted learners from a focus on visionary leadership.
A second and more important reason cited by Sashkin (1990b) for revising the original LBQ was that the theory of Bennis (1984), as well as the visionary leadership theory of the authors, had been developed further since the mid 1980s. The new LBQ reflected those changes, including measurements for personal characteristics and organizational culture in addition to leader behavior.
A number of psychometric tests regarding the LBQ were reported, and further tests have also been in progress. Stoner-Zemel (1988), using Cronbach's alpha to measure score reliability, reported scores of 0.52 to 0.75 for the first five leadership scales. More recent reliability tests yielded similar results for the first five leadership scales; for the five new scales the scores were 0.68 (scale six), 0.33 (scale seven), 0.77 (scale eight), 0.88 (scale nine), and 0.31 (scale 10) (Sashkin 1990b).Sashkin noted that the low reliability scores for scales seven and 10 were probable, given that those scales were composed of distinct elements that could be associated together. Additional tests of reliability, including test-retest reliability are being investigated (Sashkin and Burke 1990).
I
54
Validation research initially used the early edition of the LBQ, based only on the five behavior scales, but provided evidence of construct validity with LBQ scores strongly associated with bottom-line organizational performance {Major 1988) and the perceived quality of work life of organizational members (Stoner-Zemel 1988). More recent studies (Sashkin and Sashkin 1990; Endeman 1990) showed evidence that culture building activities by leaders (assessed by LBQ scales nine and 10) were related to cultural strength, adaptability, and teamwork.
Factor analytic studies documented moderate to strong support for the construct validity of the LBQ and its behavior and personal characteristic scales (Sashkin and Burke 1990). Other validation studies showed leaders scoring higher on the LBQ had more productive organizations (Major 1988; Stoner-Zemel 1988; Endeman 1990;Sashkin and Sashkin 1990) and had subordinates with more positive perceptions of their work environments and their performance (Stoner-Zemel 1988; Endeman 1990; Sashkin and Sashkin 1990).
Sashkin (1990b) reported normative data for a variety of business and public leaders, broken out by group. He noted that generally there was very little difference between self-ratings and ratings by others, and that while self-reports might be expected to be more positive, as had been true in other leadership instruments, this was not
55
borne out by normative data. Instead, normative data showed it was more common for others' reports to be slightly more positive than self-reports. More recent normative data {Sashkin et al 1992) have not consistently supported this observation.
Survey of Leadership PracticesWilson et al (1990) developed a measure of transforma
tional leadership, the Survey of Leadership Practices (SLP), that they believed described the role of the leader in an organization. It was based on the belief that leadership was one of several organizational roles that depended on skills of influencing others. To explain these roles, they developed a Task Cycle Model, a sequential process model that was used with a number of their instruments.
The most recent edition of the Survey of Leadership Practices (SLP-H) was based on the Task Cycle Model. Five phases formed the construct of the SLP-H, and several factors contributed to each of those phases, as specified below:
Phase I : Entrepreneurial VisionA. Vision/ImaginationB. Risk-Taking/Venturesomeness
Phase II: Sensing the EnvironmentC. Organizational SensitivityD. Personal Awareness
56
Phase III: Gaining CommitmentE. PersuasivenessF . Teaming
Phase IV: DriveG. Standards of PerformanceH. PerseveranceI. Push/Pressure
Phase V: ReinforcementJ. Recognition/Reinforcement
In addition, there were measures of residual impact and sources of influence, as defined below:
Residual ImpactK. Effectiveness/Outcomes L. Personal Standards M. Consistency N. Coping with Stress 0. Charisma
Sources of InfluenceP. Control of Incentives/Pay Q. Personal Connections R. Job Title/Position S. PressureT. Technical Competence U. Managerial Competence V. Teamwork with Others w. Compatible Values
57
The SLP-H comprised an 85-item questionnaire. Individuals completed the SLP-H for themselves or for a colleague or supervisor. A seven-point rating scale was used, with one meaning the statement was true to a very limited extent, never, or not at all. Respondents marked their ratings directly on computer-scorable answer sheets, which were then forwarded to Clark Wilson Publishing Company for computer scoring.
The SLP-H was based on the Task Cycle Model (Clark Wilson Publishing Company 1992). This model reflected that every task one manages or leads involved skills that follow in a specific sequence. All levels of work (not just leadership) followed a similar process, and while specifics differed from task to task, the fundamentals in the sequence did not.
The key components of the Task Cycle Model were defined as
I: clarifying the goalII: developing a plan to achieve itIII: providing the resources and training to carry
it outIV: maintaining a flow of feedback to monitor
progressV: making control adjustments if the feedback
indicated the need
VI: reinforcing positive effect (Clark WilsonPublishing Company 1992) .
Ultimately, the repeated implementation of the behavioral cycle produced an outcome and impacted the personality of the task performer or leader (Wilson et al 1990). If a leader's scores for these skills were average or above, his/her personal relations would be sound and supportive (Clark Wilson Publishing Company 1992). Thus, good interpersonal relations would be the consequence of basic operational skills and competencies.
Wilson et al (1990) believed that their theory and research went beyond investigation of the personalities or broad behavior patterns of leaders. They developed assessments that could be more readily used to train individuals in the skills and attributes that constituted leaderlike and other important influencing role behaviors. They believed that they were observing the same activities or operations as other transformational researchers but describing them in different ways and levels. Wilson et al (1990) further believed that their SLP-H reflected the skills and attributes as well as the spirit of transformational leadership, but at a more operational level. That is, they believed they captured the vision, venturesomeness, and charisma of the concept and developed the 23 amplifying skills and attributes to make the concept more trainable.
59
In summary, Wilson et al (1990) proposed that their model of transformational leadership related to the contemporary literature but differed in level of observation. They believed their tool assessed specifics of what participants actually did and then provided guidance in terminologies leaders understood.
In developing the SLP, Wilson et al (1990) first designed and validated a Survey of Management Practices to differentiate between levels of performance of the managers and their change in practices over time. The Survey of Management Practices was then used as the basis for developing the SLP.
The SLP underwent a number of revisions, and the SLP-H is the most current version. To date, the only reported validations have been normative data on two earlier versions of the SLP. In those studies, peers and superiors generally evaluated leadership of leaders with similar ratings (Wilson et al 1990).
Summary of Transformational Leadership MeasuresThe measures of transformational leadership described
have a number of similarities and several important differences. Yammarino (Clark and Clark 1990) noted that Yammarino and Bass (1990), Posner and Kouzes (1990), and Sashkin and Burke (1990) all seemed to consider similar variables in their research, specifically, emotional, intellectual, and people-based phenomena. Yammarino
60
(Clark and Clark 1990) explained that one of the primary differences in the researchers' approaches might have been their differing emphasis on levels of analysis. Specifically, Yammarino and Bass (1990) emphasized the leader and leadership, or the personal level of analysis. Posner and Kouzes (1990) placed emphasis on followers and leadership, or the group level of analysis. Sashkin and Burke (1990) focused on the organization and leadership, or the collective/ organizational level of analysis.
In contrast, Wilson et al (1990) took a much different approach. Their research was based on a process model. They believed this process model was applicable to all levels of work in an organization, not just to leadership.
Part of the difference in instruments may have been based on the contexts in which the models were developed. Posner (Clark and Clark 1990) noted that Yammarino and Bass (1990) began work with military personnel, while Posner and Kouzes (1990) developed their instrument based on data from middle- and senior-level managers. In contrast, the instrument of Sashkin and Burke (1990) was developed from work with higher level, or executive, leaders.
Finally, there were some differences in the applicability and use of the various instruments. The instrument of Yammarino and Bass (1990) could not be self-scored. While widely used in research it appeared to have limited
61
support information for training and could only be supplied to trainers meeting defined qualifications. This may have decreased its use in broad-based leadership training and development programs. The instrument of Wilson et al (1990) also could not be self-scored. It was developed for use in training, but use appeared to be tied to prearranged seminars, limiting its applicability for broad-based leadership training programs. On the other hand, the instruments of Posner and Kouzes (1990) and Sashkin and Burke (1990) could be self-scored. Detailed training and self-study materials were available for both instruments, making them applicable for use in leadership training programs.
Transformational Leadership ResearchAs previously discussed, research has been performed
on a number of the current instruments used to measure transformational leadership. In most of the published research the MLQ developed by Bass (1985) was used.
Several variables appear to be related to transformational leadership. These variables include the demographic and experiential variables of gender and training and education. In addition, situational variables, a number of effectiveness outcomes, and the beliefs of those rating the leader also appear to influence transformational leadership. Below are highlighted specific research findings related to these variables.
62
Demographic and Experiential VariablesIn examining demographic variables that may correlate
with transformational leadership, gender has been considered in several studies. Early leadership research provided limited information on gender, since until the late 197 0s most leadership research focused on men. Even since that time, men have been the majority of subjects in leadership studies using instruments such as the MLQ. One review that examined studies of gender differences concluded there were few differences between men's and women's styles and called for a moratorium on research comparing men to women (Dobbins and Platz 1986). Bass (1990), in reviewing the literature, similarly concluded that overall there were no clear differences between leadership in men and women. He stated that some individual studies did indicate differences in specific issues related to leadership, such as need for achievement, need for power, and fear of success. Yet, he explained, these differences were less distinct in men and women who had achieved status as leaders.
One study showing evidence of gender differences in specific issues related to leadership examined transformational and transactional leadership among student affairs administrators (Komives 1991) . Both the male and female hall directors held similar views of their leadership behaviors on the MLQ, with transformational factors
63
reported at an average to moderately high level. The study also examined the achieving styles of the hall directors using the L-BLA Achieving Styles Inventory instrument and Achieving Styles Inventory Form 13 (Lipman- Blumen and Leavitt 1979). Female hall directors thought their relational styles (described as vicarious, contributory, and collaborative) contributed to their transformational leadership, whereas men viewed their power-direct styles (described as taking charge, directing, or controlling) as contributing to their self-view of being transformational leaders. These results seemed to support the finding of Posner and Kouzes (1988) that female managers rated themselves as engaging in encouraging-the-heart behaviors significantly more than did male managers.
Other, more recent findings on gender and transformational leadership provided stronger evidence that there may be a gender difference. Rosener et al (1990) conducted a study for the International Women's Forum, in which they matched men and women executives based on position, type, and size of organization. Using a modified form of the MLQ, the respondents reported employing both transformational and transactional leadership styles. However, the women were found to be more transformational than their male peers. The researchers concluded that this was consistent with the belief that women feel more comfortable in empowering others and encouraging group decision-making
64
versus directing subordinates in a formal reward-in- exchange-for-performance manner.
Another study using the MLQ identified transformational leadership characteristics of nurse executives as rated both by the nurse executives themselves and by their immediate staff members (Dunham and Klafehn 1990). The group was predominantly female. Both the nurse executives and their staffs rated the nurse executives as possessing a predominantly transformational leadership style and, to a lesser degree, a transactional leadership style. Nurse executives had higher transformational leadership scores than in other studies reported by Bass (1985), again underscoring that women may have a more transformational leadership style than men.
Dunham and Klafehn (1990) also investigated other demographic and experiential variables and determined several that might be related to transformational leadership. First, individuals with advanced degrees rated themselves at higher transformational levels than those without advanced degrees. Second, it appeared that the area of study for the advanced degree made a difference. Individuals with a master's degree in nursing were more transformational than those with a master's degree in other areas. The researchers suggested that successful pursuit of a master's degree and/or a doctoral degree in
65
nursing might strengthen an individual's transformational qualities.
Dunham and Klafehn (1990) reported several demographic variables that did not seem to be related to transformational leadership. In comparing nurse executives rated as highly transformational with those rated less highly as transformational, no significant differences were found for the personal variables of age, marital status, children, tenure, or number of full-time personnel supervised.
In another study of nurses, Young (1992) investigated the type of leadership development activities identified by hospital nurse leaders as important in the development of a transformational leadership style. The study sample included 66 nurse leaders. The LBQ and a researcher- developed instrument designed to measure the importance, amount, and rank order of formal and informal education, and ethnographic interview techniques were used for data collection. The LBQ scores were used to form three groups: participants reporting high, moderate, or lowdegrees of transformational leadership behavior.
Of those nurse leaders who had completed a master's program, all were in the high transformational leadership group. The high transformational leadership group also had the highest mean leadership experience. The low transformational leadership group had the highest mean experience for years in current leadership position. In
66
examining differences in educational activities, Young (1992) reported that high transformational leadership nurse leaders reported significantly more informal education then low transformational leadership nurse leaders. The high and low transformational groups also differed significantly in the content and teaching strategies experienced. And the high transformational leadership group had significantly more formal content in their educational experiences than the moderate transformational leadership group had.
Young (1992) reported that the high transformational leadership group identified informal education experiences to be significantly more important than the low-scoring transformational leadership group. Differences in the educational importance factor were also explained by the amount of leadership experience and the type of nursing program attended. For more experienced leaders (greater than five years) formal content and formal strategies in educational experiences were significantly more important than for less experienced leaders (less than five years experience). Leaders with at least a bachelor's degree rated formal strategies in educational experiences as more important, compared to the ratings by those leaders with less than a bachelor's degree.
When asked to rank the five activities in each category (formal and informal education) making the most
67
important contribution to their development as leaders, continuing education was ranked as the most important formal education activity and on-the-job training was ranked as the most important informal education activity (Young 1992). The high transformational leadership group rated mentorship as the most important informal educational experience. When considering formal and informal education as a composite group, overall the most important activity rated was on-the-job training, followed by informal activity not previously identified on the survey, mentorship, continuing education by professional organizations, and a specific graduate nursing course in leadership.
Young (1992) interviewed 12 of the 66 nurse leaders, with three randomly selected from each of the high, moderate, and low transformational groups. High transformational leadership nurses believed they promoted staff nurse empowerment and made a difference in the work environment. And while task mastery was reported as a major source of satisfaction for the low transformational leadership group, the moderate and high transformational leadership groups verbalized that their satisfaction increased as their staff demonstrated increasing amounts of empowering behavior.
68Situational Variables
In the research by Dunham and Klafehn (1990) no significant differences were found for situational variables such as hospital size, or public versus private hospitals.In contrast, Young (1992) found nurse leaders with high transformational leadership scores as a group worked in larger hospitals on larger nursing units and supervised more employees. Other research has also documented a difference in transformational and transactional scale values and norms as related to situational variables (Bass and Avolio 1990). This difference was strongest when comparing scores from individuals in different professions or from different countries. However, Bass and Avolio did note that the transactional approach of management-by- exception would need to be practiced more in organizations where leaders had large numbers of subordinates than in those organizations where there were more limited numbers of subordinates. Finally, Schein (1985) documented that transformational leadership is more likely to occur during times of crisis or opportunistic conditions than under static or stable conditions.
Effectiveness OutcomesA third type of variable that has been linked to
transformational leadership is effectiveness outcomes. Transformational leadership has been related to a variety of effectiveness outcomes for different types of groups.
69
In their study of nurse executives, Dunham and Klafehn (1990) reported that 90% of the hospitals of nurse executives sampled had annual retention rates that were at least 85 percent. They concluded that transformational leadership could be important for nurse retention and that nurse executives could be a key force in developing transformational leaders at all levels of nursing, including the staff nurse level.
McDaniel and Wolf (1992) investigated whether transformational leadership theory applied to nurses in an entire nursing service department composed of 77 registered nurse staff, 11 mid-level nurse administrators, and one nurse executive. The researchers documented above- average work satisfaction scores and a low turnover rate among staff registered nurses at the institution. Those findings were not tested for causality, but the investigators believed they were positive outcomes of transformational leadership.
Niehoff et al (1990) also found an impact of transformational leadership on job satisfaction. In a study of 862 employees of a midwestern insurance company, the relationship between five transformational actions of top management and employee commitment, job satisfaction, and role ambiguity was examined. The researchers suggested that top-management transformational actions were strongly related to all three outcomes.
Other studies also have documented increased effectiveness among transformational leaders. Onnen (1987) had 4 54 parishioners rate their Methodist clergymen and found significant correlations of transformational but not transactional leadership with growth in church membership and worship attendance. When Avolio et al (1988) studied 27 teams of MBA students participating in a computer simulation, those teams with presidents described by the MLQ as more transformational finished the semester with higher profits and greater returns on investments.
Howell and Higgins (1990) conducted a study of the personality characteristics, leadership behaviors, and influence tactics of "champions of technological innovations." In comparing champions to nonchampions, they found that champions reported using transformational leader behaviors to a significantly greater extent than did the nonchampions. Spangler and Braiotta (1990) examined audit committee effectiveness in terms of the leadership styles of audit committee chairpersons.Results from audit committee members, external auditors, and senior management suggested that transformational leadership and active management by exception had a substantial impact on the performance of audit committees. Similarly, Keller (1992) conducted a longitudinal study of transformational leadership and the performance of project groups in three industrial research and development
71
organizations. Higher transformational leadership predicted higher project quality and budget-schedule performance ratings.
In measuring effectiveness in terms of performance ratings, Hater and Bass (1988) reported that managers described by subordinates on the MLQ as more transformational had higher performance ratings by their bosses. Yammarino and Bass (1990) likewise were able to predict superiors' fitness reports and recommendations for early promotions of a sample of 186 naval officers based on the MLQ evaluations by the subordinates of the officers.Howell and Avolio (1989) showed similar results for 76 managers in a large Canadian financial institution.
Another way to judge effectiveness has been to study the effect of transformational leadership on subordinates. If leaders were truly transformational, they should have been able to raise their subordinates to higher levels of motivation and help their subordinates become leaders.This effect was documented by Bass et al (1987). They reported that transformational bosses were more likely to have transformational subordinates. In another study of an entire nursing service department, McDaniel and Wolf (1992) reached a similar conclusion. They used the MLQ to measure transformational leadership and reported that the transformational leadership of the nurse executive and mid-level nurse administrators exhibited a cascading
72
effect: the transformational leadership scores werehighest at the top echelon.
Finally, effectiveness of transformational leadership can be measured in qualitative terms. Such analyses help describe how leaders actually use and apply the behaviors that are assessed in quantitative terms (Sashkin et al 1992). Deal and Peterson (1990) used case studies to investigate qualitatively how transformational school principals formally and informally shaped their organizational culture. The six major ways in which the principals shaped culture consisted of the following:
1) Developing a sense of what is important;2) Selecting faculty;3) Dealing with conflict;4) Setting a consistent and communicative example;5) Telling stories that communicate values;6) Using ceremonies, traditions, rituals, and
symbols as culture builders.
Subordinate BeliefsTransformational leadership research has also been
focused on the beliefs of the subordinate or follower. Waldman et al (1987) studied 256 managers in a business firm and showed that the subordinates of transformational leaders were more satisfied with their performance appraisals than were subordinates of leaders who were not transformational.
73
Singer (1985) studied transformational versus transactional leadership among 36 New Zealand company managers who rated an ideal leader and their real immediate superior. Transformational factors were found to be more highly correlated than transactional factors with subordinate job satisfaction. In addition, the ratings of the ideal leader showed that managers preferred working with leaders who were more transformational than transactional. In another study, Singer and Singer (1986) again found staff members preferred working with leaders who were more transformational.
In a further examination of leader-follower relationships, Yammarino and Bass (1990) examined transformational and transactional leadership and outcomes of leadership. They reported that followers of various leaders can be viewed as perceiving a unique interaction with their leader, independent of other followers, and that there may be "optimum" levels of transformational leadership for each subordinate. Some subordinates may require or accept higher levels of transformational behaviors from their leader than other subordinates. Yammarino and Bass concluded that transformational leadership as compared to transactional leadership is more strongly associated with individual follower effort and satisfaction and perceived leader effectiveness.
74
Leader and Subordinate RatingsOne finding that was not consistent among studies, and
seemed to vary according to the research instrument used, was how subordinate or other ratings of transformational leadership compared to the self-ratings of the leaders themselves. Bass and Avolio (1990) and Posner and Kouzes (1990) documented with their respective transformational leadership instruments the finding that leader self- ratings for transformational leadership were typically higher than transformational ratings of those same leaders made by subordinates and others. In contrast, Wilson et al (1990) and Sashkin (1990) noted that for their respective instruments transformational leadership ratings made by leaders themselves and others were generally similar. With the instrument developed by Sashkin (1990), the ratings by others tended to be slightly more positive than self-ratings.
Summary of Transformational Leadership ResearchIn summary, transformational leadership has been
related to several variables: gender, training andeducation of the leader; the location of the leader, particularly the organization and the country; and effectiveness outcomes such as organizational growth, championing innovation, higher job performance, and developing transformational subordinates. Transformational leadership was also correlated with subordinate
75
beliefs. Subordinates preferred transformational rather than transactional leaders, yet they may not rate their leaders as highly in transformational skills as their leaders rate themselves.
Healthcare Professional Leadership Research In this section, healthcare professional leadership
research, specifically in nursing, other healthcare professions, and dietetics, is reviewed. Many of the investigations summarized here used questionnaires or other methods unique to the research. Thus, in considering the findings, several problems emerged. First, such instruments appeared to have had limited testing for reliability, validity, and application in situations other than the original research protocols for which they were designed. A second issue was that comparison of the studies was difficult because of the wide differences in sample populations and methodologies. Finally, while leadership was a component in all the research reviewed, in few investigations was the theory of transformational leadership specifically addressed.
Nursing LiteratureMcCloskey and Molen (1987) reviewed the literature
regarding leadership and nursing from 1966 to 1984, identifying over 200 citations. Of these, only 58 studies
76
were found that were research-based, relevant to leadership in nursing, and written in English. Their review was conducted prior to the development and publication of the transformational leadership instruments of today. Thus, none of the studies investigated transformational leadership. However, some of the traits and behaviors now associated with transformational leadership were identified and studied in those earlier investigations.
McCloskey and Molen (1987) noted that preliminary research on leadership in nursing was primarily case-study analyses of nurses who had made substantial contributions to their profession. Some of the personal characteristics identified in those studies that could have been related to transformational leadership were being visionary, enthusiastic, energetic, risk-taking, and committed.
McCloskey and Molen (1987) also reviewed several investigations in which leadership development was considered. Characteristics in leaders that could be associated with transformational leadership, such as ambition and sensitivity to others' needs (Gilbert 1975), were identified in some studies. In other studies traits that would more likely be associated with a transactional leadership approach, such as conforming (Gluck and Charter 1980; Hanson and Chater 1983), were identified.
77
Finally, McCloskey and Molen (1987) examined a number of studies on leadership effectiveness in academic and practice settings. In these studies, the findings were consistent with the results of situational theory, that is factors such as organizational size and the nature of the work could influence leadership. Similarly, Bass and Avolio (1990) provided evidence that transformational leadership might be impacted by situational variables.Yet, other researchers (Dunham and Klafehn 1990) did not show a situational effect for transformational leadership.
McCloskey and Molen (1987) noted an important, complicating factor in the research they reviewed; the terms leadership and management were often interchanged. Such lack of definition and focus could have confounded the study of both leadership and management. Sashkin and Burke (1990) identified that such confusion existed when they defined their transformational leadership theory.They believed that much of the traditional study of "leadership” resulted in significant knowledge about management but proportionately little real knowledge about leadership. That could have been the case in the nursing literature as well.
From a review of more recent investigations than those summarized by McCloskey and Molen (1987) it was apparent that many more commentaries on nursing leadership than
78
experimental investigations have continued to be published. And surprisingly, the research on transformational leadership remained limited. The nursing studies on transformational leadership by Dunham and Klafhen (1990), McDaniel and Wolf (1992), and Young (1992) were reviewed in the previous section.
However, some other studies in current nursing literature did appear to have application to transformational leadership theory, as summarized below. Dunham and Fisher(1990) conducted in-depth, taped interviews with 85 hospital nurse executives to define excellent nurse leadership. The nurse executives participating in the study had been rated as "excellent" by nursing executives, nursing administration faculty, and other nursing administration personnel. A number of the ideas and concepts of excellent nursing leadership identified by the nurse executives related to transformational leadership. Specifically, the nurse executives believed excellent nursing leaders were creative, had a vision of what could be accomplished, and used this vision to structure goals, set direction, and empower their staffs. Excellent nursing leaders were also seen as risk-takers, charismatic, having strong value systems and then modeling these values for their staffs. The nurse executives reported that they possessed strengths similar to those they
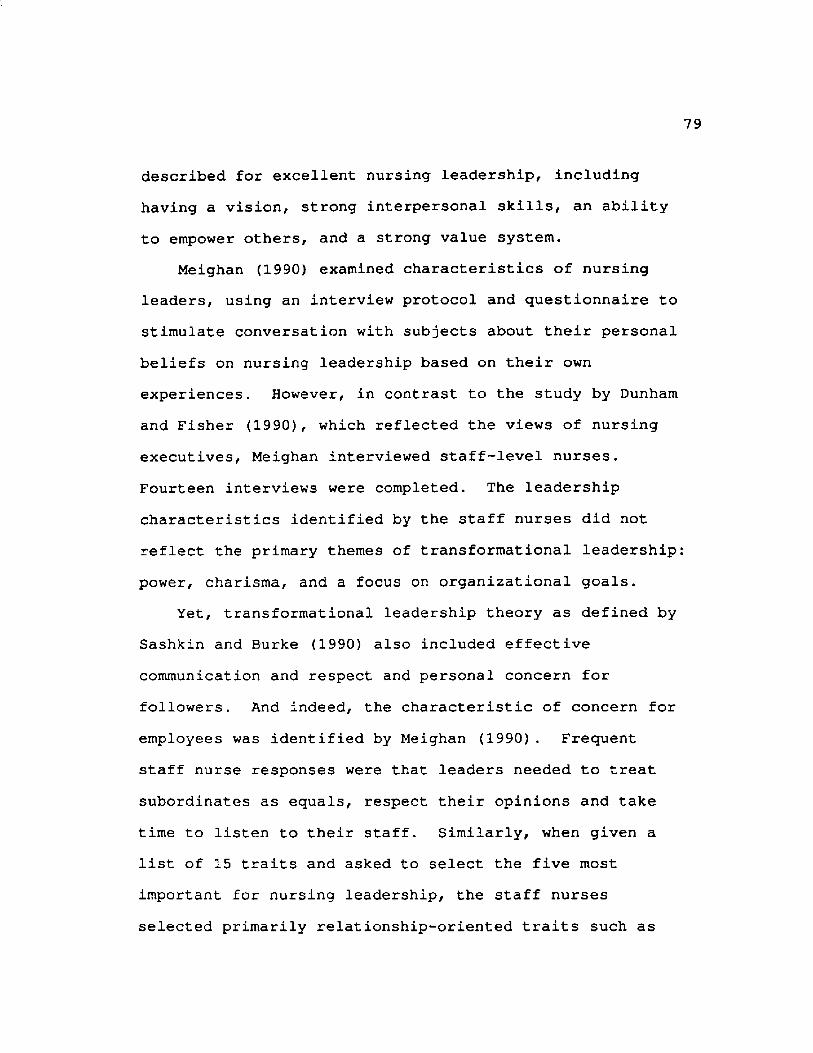
described for excellent nursing leadership, including having a vision, strong interpersonal skills, an ability to empower others, and a strong value system.
Meighan (1990) examined characteristics of nursing leaders, using an interview protocol and questionnaire to stimulate conversation with subjects about their personal beliefs on nursing leadership based on their own experiences. However, in contrast to the study by Dunham and Fisher (1990) , which reflected the views of nursing executives, Meighan interviewed staff-level nurses. Fourteen interviews were completed. The leadership characteristics identified by the staff nurses did not reflect the primary themes of transformational leadership power, charisma, and a focus on organizational goals.
Yet, transformational leadership theory as defined by Sashkin and Burke (1990) also included effective communication and respect and personal concern for followers. And indeed, the characteristic of concern for employees was identified by Meighan (1990). Frequent staff nurse responses were that leaders needed to treat subordinates as equals, respect their opinions and take time to listen to their staff. Similarly, when given a list of 15 traits and asked to select the five most important for nursing leadership, the staff nurses selected primarily relationship-oriented traits such as
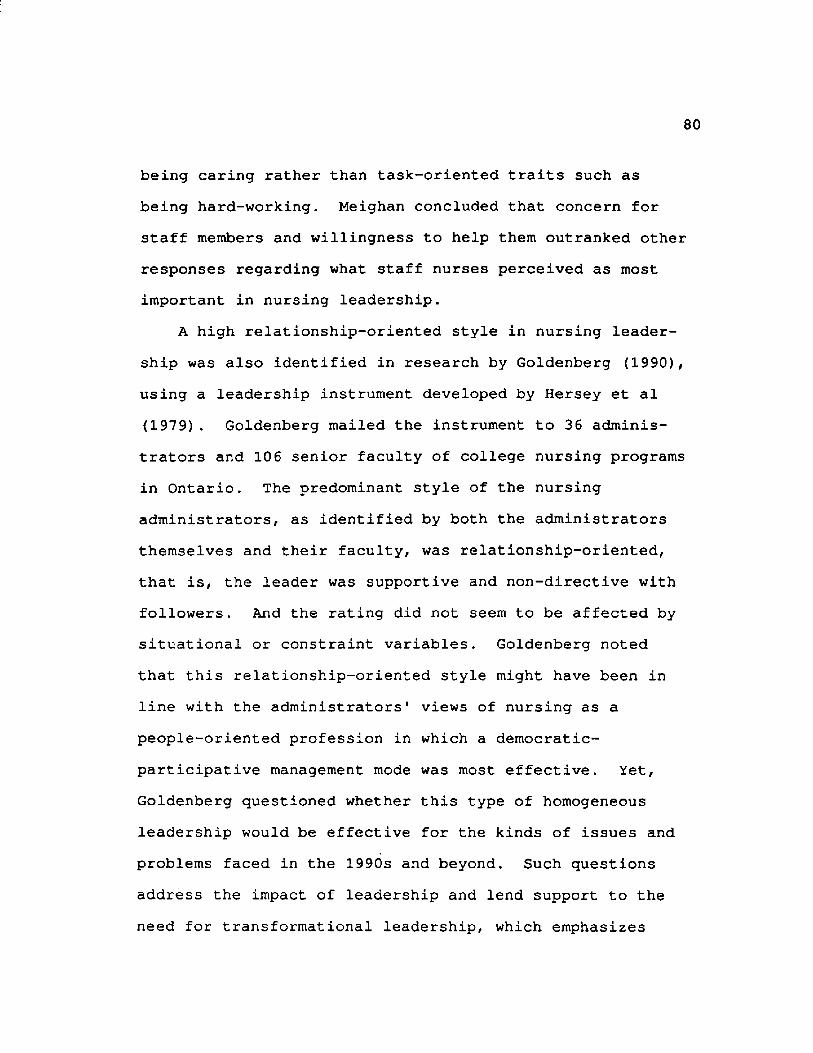
80
being caring rather than task-oriented traits such as being hard-working. Meighan concluded that concern for staff members and willingness to help them outranked other responses regarding what staff nurses perceived as most important in nursing leadership.
A high relationship-oriented style in nursing leadership was also identified in research by Goldenberg (1990), using a leadership instrument developed by Hersey et al (1979) . Goldenberg mailed the instrument to 36 administrators and 106 senior faculty of college nursing programs in Ontario. The predominant style of the nursing administrators, as identified by both the administrators themselves and their faculty, was relationship-oriented, that is, the leader was supportive and non-directive with followers. And the rating did not seem to be affected by situational or constraint variables. Goldenberg noted that this relationship-oriented style might have been in line with the administrators' views of nursing as a people-oriented profession in which a democratic- participative management mode was most effective. Yet, Goldenberg questioned whether this type of homogeneous leadership would be effective for the kinds of issues and problems faced in the 1990s and beyond. Such questions address the impact of leadership and lend support to the need for transformational leadership, which emphasizes
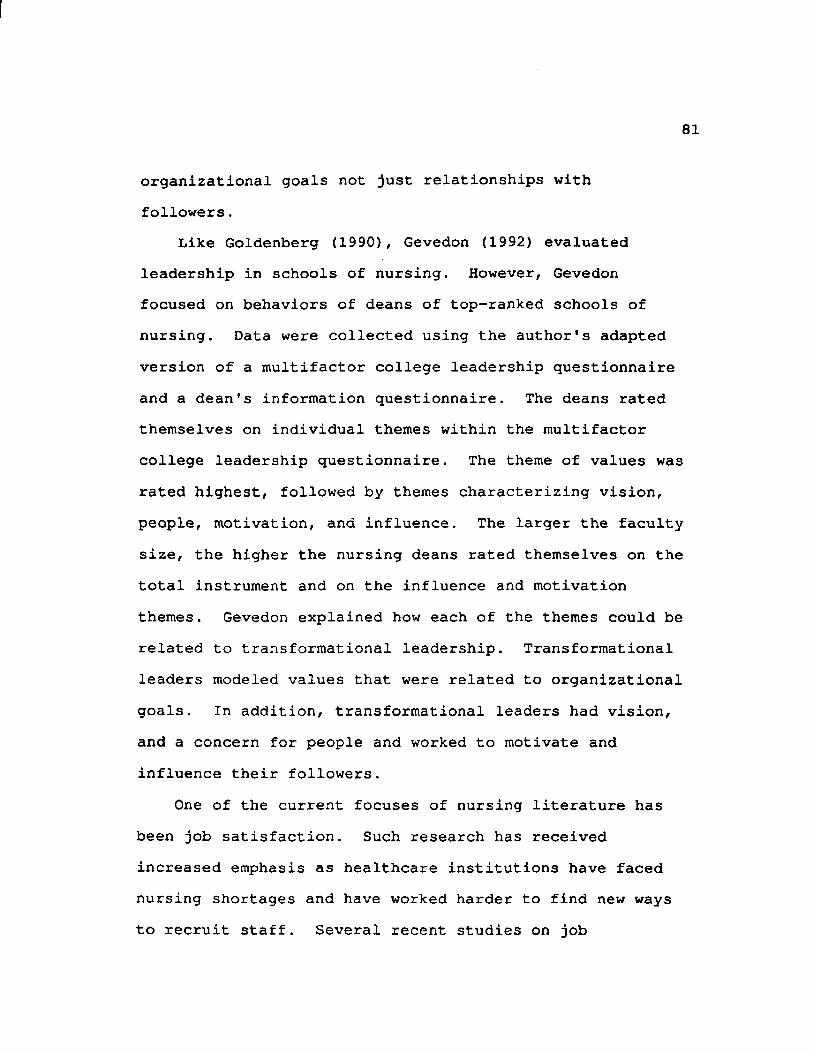
organizational goals not just relationships with followers.
Like Goldenberg (1990), Gevedon (1992) evaluated leadership in schools of nursing. However, Gevedon focused on behaviors of deans of top-ranked schools of nursing. Data were collected using the author's adapted version of a multifactor college leadership questionnaire and a dean's information questionnaire. The deans rated themselves on individual themes within the multifactor college leadership questionnaire. The theme of values was rated highest, followed by themes characterizing vision, people, motivation, and influence. The larger the faculty size, the higher the nursing deans rated themselves on the total instrument and on the influence and motivation themes. Gevedon explained how each of the themes could be related to transformational leadership. Transformational leaders modeled values that were related to organizational goals. In addition, transformational leaders had vision, and a concern for people and worked to motivate and influence their followers.
One of the current focuses of nursing literature has been job satisfaction. Such research has received increased emphasis as healthcare institutions have faced nursing shortages and have worked harder to find new ways to recruit staff. Several recent studies on job
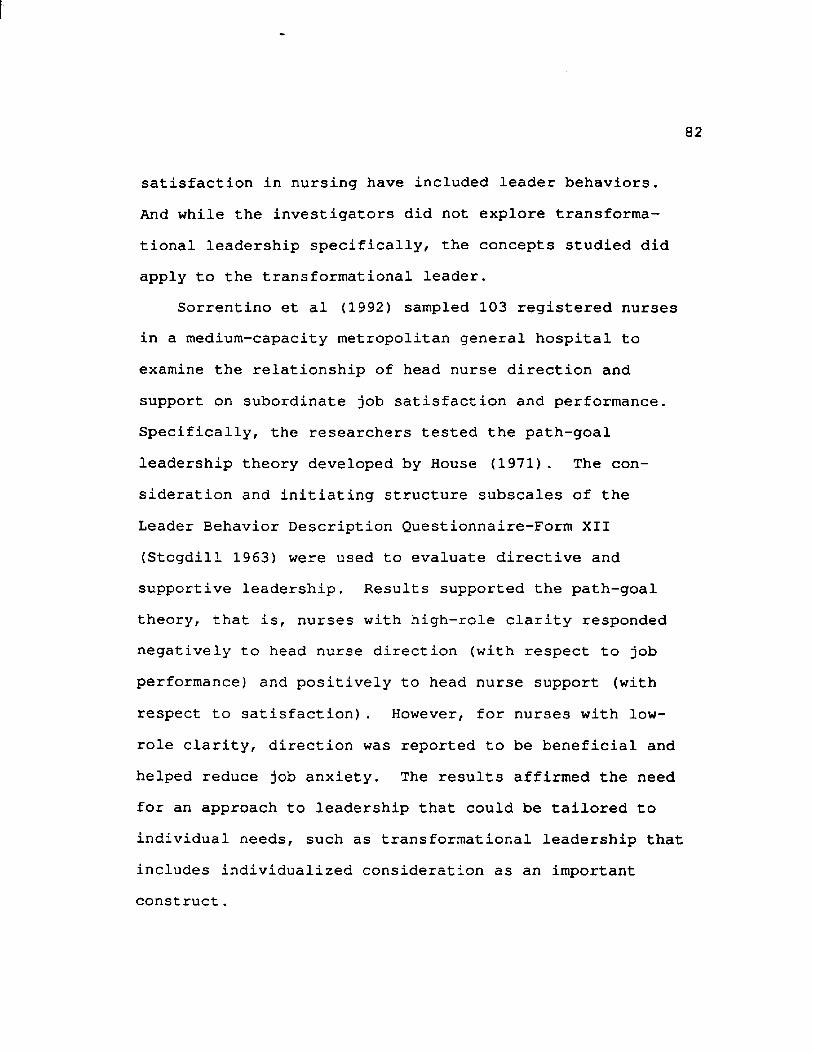
satisfaction in nursing have included leader behaviors. And while the investigators did not explore transformational leadership specifically, the concepts studied did apply to the transformational leader.
Sorrentino et al (1992) sampled 103 registered nurses in a medium-capacity metropolitan general hospital to examine the relationship of head nurse direction and support on subordinate job satisfaction and performance. Specifically, the researchers tested the path-goal leadership theory developed by House (1971). The consideration and initiating structure subscales of the Leader Behavior Description Questionnaire-Form XII (Stogdill 1963) were used to evaluate directive and supportive leadership. Results supported the path-goal theory, that is, nurses with high-role clarity responded negatively to head nurse direction (with respect to job performance) and positively to head nurse support (with respect to satisfaction). However, for nurses with low- role clarity, direction was reported to be beneficial and helped reduce job anxiety. The results affirmed the need for an approach to leadership that could be tailored to individual needs, such as transformational leadership that includes individualized consideration as an important construct.
83
In another study of head nurse leadership Garrett(1991) investigated the interactions among leadership preferences of 298 staff nurses, the perceived leader behavior of their nurse managers, and their job satisfaction. Like Sorrentino et al (1992), Garrett focused on consideration and initiating structure. The researchers used the subscales related to consideration and initiating structure of the Leader Behavior Description Question- naire-Form XII (Stogdill 1963) to measure perceived style of the leaders of the staff nurses and used the Ideal Leader Behavior Description Questionnaire Form (Stogdill 1963) to measure preferred leadership styles.Surprisingly, there was no significant relationship between job satisfaction and whether the styles of leadership preferred by the staff nurses and the actual leadership behaviors of their head nurses matched. There was a positive relationship between perceived head nurse consideration and job satisfaction, as well as a positive relationship between perceived initiating structure and job satisfaction. The finding of a positive relationship between perceived initiating structure and job satisfaction was not explored to determine if role clarity had an effect as demonstrated by Sorrentino et al (1992) .
Uliss (1991) also studied job satisfaction, but in a more specialized population of 92 evening and night shift
84
registered nurses from nine critical care units. Uliss explored the relation of critical care nurse satisfaction to two leadership dimensions: degree of task orientationand orientation to relationships. Drawing on the work of Stogdill (1974) and Hersey and Blanchard (1977), Uliss developed a leadership opinion questionnaire to describe leadership styles. Overall, critical care nurses did not significantly relate task orientation or relationship orientation to work satisfaction. However, when the factor of experience was considered, Uliss found a difference. In general, critical care nurses preferred working with a leader who delegated necessary authority and then kept a low profile. On the other hand, critical care nurses with less than two years' experience preferred leaders who would coach them into "self-confident, self- starting performances." It was possible that these less- experienced nurses had lower role clarity, and like those nurses studied by Sorrentino et al (1992), needed more direction and task orientation. These findings again underscore the need for individualized consideration as included in transformational leadership theory.
Other Health Professions LiteratureWhile the healthcare literature reviewed on leadership
was most prevalent in the nursing profession, there were publications on leadership in other health professions
85
too. Most of this literature consisted of commentaries rather than research studies. Perhaps most importantly, in the majority of the literature for other health professions, leadership was not distinguished as separate from management as it was in the more current nursing literature.
Two studies of note were published regarding leadership in the management role of physical therapists. In the first investigation, Inderrieden et al (1987) studied physical therapy managers, hospital administrators, and private organization managers. A 13-item questionnaire developed by Ghiselli (1971) was used to assess traits and characteristics usually associated with managerial success. The needs and characteristics were similar to those developed by Maslow (1943) and McClelland (1961): supervisory ability, intelligence, initiative, self-assurance, decisiveness, masculinity/femininity, maturity, working class affinity, need for occupational achievement, need for self-actualization, need for power, need for high financial reward, and need for job security. Inderrieden et al (1987) documented that gender differences existed for physical therapists, with women showing stronger managerial profiles than their male counterparts.Further, they found that the situational variables of organization and profession did not affect the ratings.
86
In general, when gender was not considered, there were few differences between the ratings for the physical therapists, hospital administrators, and business managers studied.
Lamastro and Fortin-Crosby (1980) studied the managerial roles of chiefs of physical therapy services. Forty interviews with physical therapy directors were conducted using a questionnaire developed for the study.In describing their role, the respondents generally described transactional activities, including the following: serving as manager, resource person, and coordinator. However, there was also some evidence of transformational leadership in that the chiefs of physical therapy services suggested that being a staff developer was important to their roles. In describing skills and competencies, additional transformational skills were indicated, such as an ability to identify areas for future growth and an ability to understand individual needs and motivation for work.
The chiefs of physical therapy also had a highly participative style, with almost three-fourths of those responding indicating there was a high degree of involvement by their staff in changing departmental policies that directly affected their staff (Lamastro and Fortin-Crosby 1980), In general, though, the transformational elements
of power, charisma, and a focus on organizational goals were lacking from the role descriptions of chiefs of physical therapy services.
Parrett et al (1985) conducted a survey of 570 randomly selected hospital pharmacy directors to determine their prevalent leadership styles, the association between person-oriented leadership and use of innovative services, and the association between participative management and use of innovative services. The researchers used a leadership evaluation tool developed by Hersey and Blanchard (1982) to measure leadership style. Responses indicated that the most frequent dominant leadership style was high task-high relationship. Respondents with this style also had the highest scores for subordinate participation, and a positive correlation between scores for subordinate participation and scores for innovative services was demonstrated. In addition, a significant difference in innovative services scores for directors with and without graduate degrees was found and there was a positive correlation between number of staff supervised and scores for innovative services. The findings of this study supported those of studies in nursing, that is, managers had a high concern for relationships (consideration) and task (initiating structure).
Leadership in occupational therapy was examined by Burke and DePoy (1991), who interviewed 10 master clinicians to determine the characteristics of their mastery and excellence in practice and explore the degree to which they engaged in leadership behavior. Sixteen semistructured questions were used to gather data on known constructs of mastery and leadership. Items that were differentiated included the definition of leadership and excellence as public activities, that is, that those activities could only be recognized and exercised in the presence of others. Furthermore, key characteristics differentiating leadership were found to be power, influence, and recognition. While power and influence have been used to help describe transformational leadership, the researchers did not discuss transformational leadership. And other elements, like vision, that have been traditionally related to transformational leadership by researchers such as Burns (1978) were related in this study to the areas of mastery and excellence.
Wattenberg et al (1977) compared opinions of social work administrators and hospital administrators toward specific leadership tasks performed by social workers in the hospital. Hospital and social service administrators were interviewed to determine the importance and frequency of the task. Both reported similar views on the
89
importance and frequency of tasks; they judged the tasks to be quite important but not extremely important.However, none of the tasks studied appeared to be related to transformational leadership, rather the tasks seemed to be more transactional, because they were job-related functions such as clinical teaching and participating in patient care.
In a larger sample of 252 hospital personnel in a healthcare center, Seltzer and Numeroff (1990) explored the effects of leadership behavior and task characteristics on burnout. The initiating structure and consideration subscales of the Leader Behavior Description Questionnaire (Stogdill 1963) were used to measure leadership. For supervisors scoring high in consideration there was a correlation to less burnout. This finding again underscored the importance of the individualized consideration construct of transformational leadership.
Dietetic LiteratureIn the dietetic literature, research studies on
leadership are very limited as in other healthcare fields. Most often leadership has been considered simply as one of a number of variables in the evaluation of the role and competencies of dietitians. Thus, for many of these studies leadership was not a primary focus. Among the researchers who did consider leadership were those who
[
90
studied role delineation. Specifically, several investigators focused on entry-level clinical practice and more advanced-level practice in food management and business and industry.
Snyder et al (1985) examined entry-level practice competency in administrative skills as rated by a sample of 50 administrative dietitians. The questionnaire that was developed and used focused on the areas of organization and administration, leadership and management, communications, financial management, and quality assurance services. Most of the competencies listed under the leadership and supervision area of the questionnaire were transactional in approach. Two competency statements could be considered transformational leadership:1) "relate motivational techniques to employeeproductivity/job satisfaction" and 2) "evaluate the effectof change on the individual and on the organization."These two competencies were rated slightly lower but not significantly lower than the transactional type of competencies when respondents considered their importance for career entrance. In considering the competencies needed for professional practice, however, the respondents rated the two transformational competencies similarly to the transactional competencies.
91
In another study of entry-level practitioners, Parks and Kris-Etheron (1982) identified nine areas of competency. A questionnaire was mailed to a random sample of 400 dietitians, with a response rate of about 30 percent. In one competency leadership was included in the description: "Understands the managerial process of planning,organizing, leading, evaluating, and controlling and their relationship to the management of human, material, and financial resources." The leadership competency was ranked as the least critical of all nine competencies for entry-level practitioners.
In other studies, competencies and skills of dietitians beyond entry-level practice were investigated. In examining attributes and qualities of dietitians in business and industry, skills listed that could be related to transformational leadership included communication skills (Kirk et al 1989; Boudreaux et al 1991), listening skills, organizational politics, and leadership (Boudreaux et al 1991}. Similarly, some of the competencies identified as important for hospital food and nutrition department directors, though not specifically defined as transformational leadership, did refer to some key transformational leadership elements. These included communication, political savvy (Dowling et al 1990), ability to apply motivational techniques and involve personnel in
92
decision-making (Yates et al 1987), ability to provide a motivational environment, and ability to evaluate new developments (Seal et al 1983). Coordinated dietetic program directors also had a documented role for leadership, specifically described as exhibiting leadership qualities on committees within the university setting (Nyland et al 1989).
One of the reasons that the transformational principles of power, charisma, and focus on organizational goals might not have been clearly identified in the dietetic role delineation studies discussed was that leadership has never been clearly defined as separate from management in the dietetic literature. Without such a basic distinction it is therefore logical that more specialized theories such as transformational leadership have not yet been explored. For example, in studying leadership in nutrition support Nestle (1984) surveyed health profession students in a clinical nutrition course. The students were asked who should hold primary responsibility for particular aspects of nutritional support. All of the aspects listed were task-oriented, such as "takes a diet history" or "selects enteral and parenteral formulas," and none addressed relationships or broader concepts of leadership such as power, charisma, or focus on organizational goals.
93
A second consideration was the level of responsibility of the dietitians surveyed in the various studies. Brown and Fruin (1989) studied management activities in community dietetics practice and noted that as management levels increased, the activities perceived as important changed from mostly technical activities to more human and, finally, more conceptual activities. Specifically, lower-management level dietitians rated technical activities, such as serving as a consultant, keeping current with readings, and conducting meetings, as most important for their positions. Mid-management level dietitians rated as important many aspects of personnel management, as well as activities that required human and conceptual skills. At the other end of the spectrum, upper-management level dietitians rated activities such as long-range planning, problem solving, and developing new projects and directions as most important. These activities are primarily conceptual skills. Thus, it could be expected that some transformational leadership characteristics, such as concern for employees and vision, would be less likely to be identified as important for entry- level dietetic practitioners than for advanced-level dietetic practitioners.
The identification of qualities that could be related to transformational leadership was evident in the research of Nettles et al (1993). They identified professional and educational characteristics of graduates from master's degree programs in food service management to determine the relevance of specific concepts to present professional responsibilities. In addition, they rated the quality of the master's degree educational preparation and determined whether competence was gained from sources other than from the graduate program. Of the 43 food service concepts rated as relevant to the job, several could be related to transformational leadership: strategic marketing,written/oral communication, problem-solving/decisionmaking, consulting skills, environmental screening, marketing management, and new development evaluation.
Bradley et al (1993) also investigated advanced-level dietetics, developed a model, and reported empirical results. They postulated that in addition to extraordinary technical expertise, advanced-level practitioners used intuition and feelings to achieve a holistic understanding, used a process approach that was creative and adaptive, and valued innovation and self-growth. Bradley et al determined a number of characteristics that were important for their model of advanced practice, and several characteristics could be related to
95
transformational leadership: creator/developer role,adviser role, use own curiosity, handle unfamiliar situations, preceptor role, and maintain impassioned commitment.
In contrast, in a study of specialty practice, transformational leadership concepts were very limited.Bradley et al (1993) studied specialty practice in metabolic nutrition care, pediatric nutrition, and renal nutrition. Forty-nine discriminating tasks were included in a generic model of specialty practice. None of those tasks seemed to be specifically related to transformational leadership. Of the 35 common tasks included in the generic model of specialty practice, three appeared to be somewhat related to transformational leadership: coordinate nutrition programs for groups with other services, develop a strategic plan for nutrition services in the specialty, and review market research data related to nutrition services. Thus, it seems that at the specialty practice level, job functions are still primarily task- related, with very few functions related to leadership.
One of the only studies specifically addressing leadership skills in dietetics was reported by Schiller et al (1993) . Self-perceptions of personal thought and behavior were assessed in a group of 893 clinical dietitians using the Lifestyles Inventory Level I, Self
96
Description (LSI-Level I) instrument developed by Human Synergistics (1987). While this instrument has not been typically related to transformational leadership, the researchers believed self-perception was a necessary first step for development of transformational leadership. Specifically, they proposed that dietitians needed to become aware of their professional self-concepts before they could set goals to strengthen positive traits and minimize limiting attributes for transformational leadership. The LSI-Level I rated 12 self concepts or styles:I) humanistic-helpful, 2) affiliative, 3) approval,4) conventional, 5) dependent, 6) avoidance, 7) oppositional, 8) power, 9) competitive, 10) perfectionistic,II) achievement, and 12) self actualize.
Overall, the results of the inventory were generally nondiscriminate. However, two dominant styles, dependent style and self-actualize style, were slightly (but not significantly) higher than other styles as reflected by the mean scores of respondents. In addition, these researchers documented that dietitian mean scores were higher (though not significantly) than the general population (Human Synergistics 1987) in every category except power.
Schiller et al (1993) also related self-concepts to selected demographic variables and found that dietitians
97
who scored high in achievement, self-actualize, humanistic-helpful, and affiliative styles more often had advanced degrees, published articles, held offices, lectured to medical and dietetic students, represented the department to the organization, initiated projects, participated in educational programs, and served as mentors. In contrast, dietitians who scored above the mean in self-defeating styles {styles numbered 3-10) typically had only a bachelor's degree and did not write articles, participate in educational activities, write research proposals or manage research projects. These researchers concluded that the data documents the existence of a cadre of self-actualized leaders as well as many who seek security rather than satisfaction in their daily activities. They also believed that the profession needs both leaders and followers, but that in the turbulence of healthcare today those who have achieved self- fulfillment have a responsibility to foster positive styles in other dietitians.
Summary of Healthcare Professional LiteratureThe healthcare professional literature on leadership
surveyed in this review, with the exception of a few studies (Dunham and Klafehn 1990; Young 1992; McDaniel and Wolf 1992; Schiller et al 1993) do not address transformational leadership. Therefore, the research was considered
98
as it could be applied to transformational theory and several themes were developed. First, vision and enthusiasm are recognized as important leadership characteristics by leaders, whereas subordinates are more likely to recognize interpersonal skills as important. Second, there appear to be some gender differences in managerial/leadership skills of health professionals. Third, leadership skills do not seem to be as important for entry-level practice as they are for advanced-level practice and management.
A general conclusion is that in clinical dietetics there appear to be two distinct groups of clinicians, those who practice high-level behaviors related to leadership and can perhaps be transformational leaders and those who are not secure in their leadership roles and are probably not transformational leaders. In addition, it is interesting to note that clinical dietitians in general scored low in power, which may indicate a weakness in transformational leadership. Clearly, there is a need in the dietetic literature for distinction between leadership and management as well as a need for definitions of leadership and specifically transformational leadership.
CHAPTER IIIMETHODOLOGY
This descriptive study was undertaken to describe transformational leadership qualities of clinical nutrition managers who were members of the Clinical Nutrition Management practice group of The American Dietetic Association. Specifically, transformational leadership qualities of clinical nutrition managers were identified and a comparison was made between transformational leadership qualities of clinical nutrition managers as rated by clinical nutrition managers themselves and their employee evaluators. In addition, the association of transformational leadership qualities with defined variables including training/degree, length of time in management, number of people supervised, income, and participation in advanced practice activities {management, research, and scholarly activities) was evaluated.
Study DesignThe research design included two descriptive surveys.
First, a descriptive survey was used to select the study population. A research sample was then randomly selected
99
100
from those in the study population who met defined criteria. Second, another descriptive survey, the Leadership Behavior Questionnaire (LBQ), was mailed to the study sample and used to measure transformational leadership qualities as reported by clinical nutrition managers and their employee evaluators.
Populations and SampleThe general population comprised all 1,599 members of
the Clinical Nutrition Management practice group of The American Dietetic Association in 1992. Name and address labels were purchased from The American Dietetic Association in Chicago. Ten labels were discarded because the addresses were outside the United States.
The study population of 951 members (59.8% of the general population) was defined as all members of the Clinical Nutrition Management group who responded to a descriptive survey mailed by the investigator. Because of the high cost of the LBQ instrument and its mailing, a study sample of 150 was selected from the study population. This study sample was then used to measure transformational leadership qualities.
The selection process of the study sample included two steps. First, clinical nutrition managers who met the following criteria were identified:
101
1. Current membership in the Clinical Nutrition Management practice group of The American Dietetic Association;
2. Current dietetic registration and/or licensure;3. Employment as clinical nutrition managers in
United States hospitals;4. Direct supervision of a staff of three or more
individuals (dietitians and/or dietetic technicians);
5. Consent to participate in the study and to recruit three direct-report employee evaluators (dietitians and/or dietetic technicians) to participate in the study.
The criterion of employment of clinical nutrition manager was evaluated on the basis of the reported current title, that is, only those whose titles reflected a clinical management position (clinical nutrition manager, nutrition manager, chief clinical dietitian, etc.) were included in the selection pool for the study sample. Staff size was another important criterion; it was used to ensure that three employee evaluators were available for each clinical nutrition manager. Previous research using the LBQ had established that a minimum of three questionnaires should be completed by subordinates for evaluation of a superior (Sashkin and Burke 1990). A total of 222 respondents met the defined criteria. In the next step the
102
surveys were arranged in ZIP code numerical order and every third survey was discarded to yield a final study sample of 150.
Survey InstrumentsA 60-item demographic questionnaire (Appendix B) was
used to survey the general population for the study, the U.S. membership of the Clinical Nutrition Management practice group of the ADA. Questions included topics related to the individual's employment, institution, experience, supervisory responsibilities, educational activities, publications, research, areas of professional involvement/specialization, mentoring, and leadership.
A separate, nine-item demographic survey (Appendix C) was used with the employee evaluators of the clinical nutrition managers. This survey was used to help define the working relationships of the employee evaluators with the clinical nutrition managers. The survey was given to the employee evaluators when they received the Leadership Behavior Questionnaire (LBQ).
Drafts of both demographic questionnaires were submitted to a panel of experts for review and critique. The panel was comprised of four clinical nutrition managers who had held leadership positions in the Clinical Nutrition Management practice group and four individuals with experience in mail survey design.
103
The Leadership Behavior Questionnaire (LBQ) was used to measure transformational leadership qualities using 10 different scales (Appendix A). The LBQ was developed by Sashkin and Burke (1990) and measured transformational leadership by scoring visionary leadership behavior, visionary leadership characteristics, and visionary culture-building. The LBQ is a standardized, selfadministered instrument designed for use in management training and development. The reliability and validity of the LBQ were previously reported (Stoner-Zemel 1988;Sashkin 1990b; Sashkin and Burke 1990; Major 1988; Sashkin and Sashkin 1990; Endeman 1990).
The LBQ had 50 items, with five items forming each of 10 scales. On each scale, two items (40%) were negatively stated and three (60%) were positively stated to help reduce social desirability bias. The items were rated c (completely true), m (mostly true), s (somewhat true), 1 (a little true), or n (not at all true).
The responses on the LBQ form were automatically converted to numeric scores (one to five) as subjects marked pressure-sensitive response sheets. For example, a "c" rating on a positively stated item was equal to a numeric score of five, an "n" rating on this same item was equal to a numeric score of one. When items were negatively stated, a "c" rating was equal to a numeric score of one and an "n" rating was equal to a numeric score of five. Upon
104
completion, clinical nutrition managers were instructed to return the LBQ packet to the investigator for analysis and interpretation.
Distribution of the Survey Instruments and Instructions
An explanatory cover letter, instruction sheet, coded demographic questionnaire, and coded self-addressed, stamped envelope were mailed to the 1,589 members of the Clinical Nutrition Management practice group on September 14, 1992 (Appendix D). Envelopes were coded to allow one follow-up of nonrespondents; questionnaires were coded to allow correlation with the LBQ. No attempt was made to pair names with code numbers. A follow-up letter and demographic questionnaire were sent on September 21 1992, to members of the Clinical Nutrition Management practice group who had not yet responded to the initial mailing of the demographic questionnaire (Appendix D).
The study sample of 150 clinical nutrition managers received explanatory letters, instruction sheets, sets of LBQs (one SELF and three OTHERS) three short demographic surveys, and return envelopes (Appendix D ) . These packets were mailed on October 14, 1992. The clinical nutrition managers were instructed to complete the LBQ marked SELF following the instructions and then to place the completed instrument in the enclosed envelope. The clinical nutrition managers were also instructed to provide the
105
explanatory letters, short demographic surveys, LBQs marked OTHER, and envelopes to each of three of their direct- report subordinates.
The subordinates or employee evaluators were instructed to complete the short demographic survey and LBQ following instructions, place both instruments in the enclosed envelope, seal the envelope, and return the envelope to the clinical nutrition manager (Appendix D). Clinical nutrition managers were instructed to mail in a postage-paid envelope addressed to the co-investigator their completed LBQs and the sealed envelopes containing the LBQs and short demographic surveys of their three employee evaluators. Follow-up reminder cards (Appendix D) were mailed to individuals in the study sample who did not return their survey instruments. The follow-up cards were mailed in the first and second weeks in November, 1992.
Clinical nutrition managers requesting outcomes of the study were promised a short summation of study results. Individual (SELF) LBQ scores would be mailed only when a signed release form was received (Appendix D) .
Statistical AnalysisBoth demographic instruments and the LBQ were coded and
processed at The Ohio State University Polymetrics Laboratory. Responses to questions on the demographic survey that used a nonrated scale, such as the question asking how
clinical nutrition managers believed their supervisor valued clinical nutrition services, were converted to numeric scores. The numeric value of one was assigned to the lowest or most negative ratings and the numeric value of seven was assigned to the highest or most positive ratings. For the LBQ, the 50 numeric scores were added to yield 10 scale scores (five numeric scores were added to yield each individual scale score). The 10 scale scores were 1) focused leadership, 2) communication leadership,3) trust leadership, 4) respectful leadership, 5) risk leadership, 6) bottom-line leadership, 7) empowered leadership, 8) long-term leadership, 9) organizational leadership, and 10) cultural leadership. Detailed descriptions of these 10 scales are included in Appendix A.
Calculations were made from the 10 scale scores to form the three "clusters" or subscores that defined the instrument. Specifically, the one through five scale scores were added to yield an overall Visionary Leadership Behavior subscore. Scores six through eight formed the Visionary Leadership Characteristics subscore, and the final two scale scores were added to yield an overall Visionary Culture Building subscore. Adding the three subscores provided an overall Visionary Leadership Score.
The LBQ scores were rated using the methods described by Sashkin (1990a). Specifically, for the 10 individual scales, scores were rated as follows:
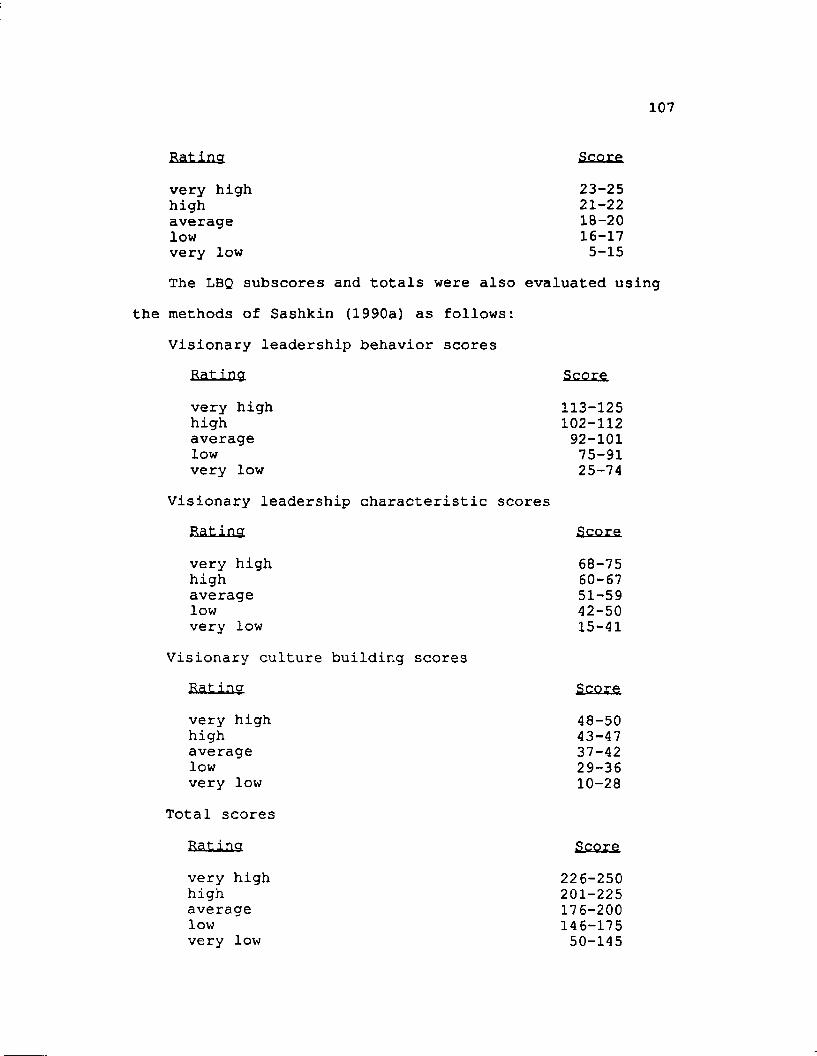
107
Eating &££££very high 23-25high 21-22average 18-20low 16-17very low 5-15The LBQ subscores and totals were also evaluated using
the methods of Sashkin (1990a) as follows:Visionary leadership behavior scores
Rating Scorevery high high average lowvery low
Visionary leadership characteristic scores
Visionary culture building scores Ratingvery high high average lowvery low
Total scoresRatingvery high high average lowvery low
113-125102-11292-10175-9125-74
Rating Scorevery high 68-75high 60-67average 51-59low 42-50very low 15-41
Score48-5043-4737-4229-3610-28
Scoxe226-250201-225176-200146-17550-145
108
Statistics were calculated using the 1989 version (6.07) of the Statistical Analysis System (SAS) software (SAS 1992) and the 1990 version of the BMDP statistical software package (Dixon 1990). Working with The Ohio State University Statistical Consulting Service, descriptive statistics were used to analyze the demographic surveys and define the demographic profiles of the subject group of clinical nutrition managers and employee evaluators and describe the frequency of distribution of responses.
The few individual missing values in the LBQ were imputed by employing a nearest-neighbor hot-deck procedure. In this procedure, an individual survey with a missing value(s) was matched to a completed survey that was closest (that is, the nearest neighbor) in terms of the pattern of ratings on the LBQ. The value(s) from the completed survey was then substituted for the missing value(s) on the incompleted survey. This procedure was used just for individual missing values and not to generate entire LBQ survey scores. Thus, for the seven clinical nutrition managers who did not return all three employee evaluator (OTHER) LBQs, only the data from the actual returned OTHER LBQ surveys were used.
Next means and standard deviations were calculated for the LBQ scale scores, subscores, and totals and were used to evaluate transformational leadership based on the rating guidelines for the LBQ developed by Sashkin (1990a). To
109
compare clinical nutrition manager (SELF) LBQ scores and clinical nutrition manager employee evaluator (OTHER) LBQ scores, the PROC MIXED repeated measures SAS procedure was used (SAS 1992) . Significance was computed using the approximate F-test.
The final step was to associate transformational leadership qualities with the defined study variables: training/degree, length of time in management, number of people supervised, income, and participation in advanced practice activities (management, research, and scholarly activities). For this analysis, clinical nutrition manager (SELF) LBQ subscores and LBQ totals were used, and the subscores and totals were first classified into three groups. For each subscore and total the low group was made up of individuals with ratings in the "very low" and "low" categories based on the rating scale developed by Sashkin (1990a). The medium group included those with a rating of "average" on the rating scale developed by Sashkin.Finally, the high group was made up of individuals in the "high" and "very high" categories as evaluated by the rating scale of Sashkin. Missing values for the LBQ were again imputed by employing a nearest-neighbor hot-deck procedure. For the defined study variables that were assessed in the demographic survey, missing values were equated to zero. The ability of the defined study variables to predict transformational leadership qualities
110
was measured by calculating X using the BMDP 4F program(Brown 1990). Specifically, using the low, medium, and high groupings of the LBQ subscores and the LBQ total, Xwas then calculated for each of the defined study variables.
CHAPTER IV RESEARCH FINDINGS
The purpose of this investigation was to describe transformational leadership qualities of clinical nutrition managers who were members of the Clinical Nutrition Management practice group of The American Dietetic Association. In this study the Leadership Behavior Questionnaire (LBQ) developed by Sashkin and Burke (1990) was used to measure transformational leadership. The selected parameters that might influence transformational leadership specifically investigated were training/degree, length of time in management, number of people supervised, income, and participation in advanced practice activities (management, research, and scholarly activities).
Findings are presented in three general sections. In the first section, demographic profiles of the sample, including clinical nutrition managers and their employee evaluators, are detailed. In the second section, the transformational leadership qualities of clinical nutrition managers are described based on the LBQ scores of the clinical nutrition managers and their employee evaluators.A comparison was made of those scores to scores in published
111
112
research. In the final section transformational leadership qualities based on the LBQ subscores were associated with the defined study variables.
The Study Sample Demographic Profile of Clinical Nutrition Managers
Although the aim was to include 150 clinical nutrition managers in the study sample, only 121 (80.0%) survey instrument sets (including the clinical nutrition manager and employee evaluator LBQs and the employee evaluator demographic surveys) were returned. One set (1.0%) was returned late and four clinical nutrition managers (2.6%) chose not to participate and returned the survey sets uncompleted. One hundred thirteen sets (75.3%) were complete; that is, they contained the SELF and three OTHER LBQs. Three sets had fewer than three OTHER LBQs but were included in the study sample. Thus, the study sample consisted of 116 clinical nutrition managers.
The clinical nutrition managers in the study sample were employed full-time in U.S. healthcare institutions, were licensed and/or registered dietitians, and were predominantly female (97.4%). The majority of the clinical nutrition managers had Master’s degrees (67.2%) or had completed work toward those degrees (7.8%). Most clinical nutrition managers who had completed their Master's degrees had selected either nutrition (57.7%) or health management
113
(10.3%) as their major emphasis. Some clinical nutrition managers had certification and/or advanced practice credentials; 17.2% were certified nutrition support dietitians, 5.2% were certified diabetes educators, and 10.3% held other certifications, such as certification through the American College of Healthcare Executives or American Society of Hospital Food Service Administrators. Additional characteristics regarding the employment and education of the clinical nutrition managers are presented in Table 1. A number of the clinical nutrition managers were members of practice groups of The American Dietetic Association in addition to the Clinical Nutrition Management Practice Group (Table 2).
The clinical nutrition managers were employed in a variety of institutions though most worked in teaching hospitals (40.5%) or community hospitals (39.7%) and most worked in hospitals with a bedsize of 250-499 beds (44.8%), as reported in Table 3. Most clinical nutrition managers worked in hospitals with over 70% occupancy of open beds (77.5%). In the majority of the institutions where the clinical nutrition managers worked, clinical nutrition services and food services were not managed as separate departments (85.3%). Most clinical nutrition managers reported to the director of food and nutrition services (42.5%), director of dietary services (11.5%), director of nutrition services (9.7%), or department head/division
114
manager (7.1%). Only 9.0% reported to individuals who did not have food- and/or nutrition-related titles; other job titles included associate director of patient services or vice president of operations.
While only about one-third (32.8%) of the institutions charged for inpatient clinical nutrition services, 81.0% charged for outpatient clinical nutrition services. About one-third (31.2%) of the institutions provided homecare clinical nutrition services and of that number 40.0% charged for those services. More than two-thirds (67.8%) of the clinical nutrition managers had initiated or were developing fee-for-clinical nutrition services programs in their current institutions or had developed such programs in other institutions. The percentage of reimbursement received varied when charges were made for clinical nutrition services. While a number of clinical nutrition managers reported not receiving reimbursement for inpatient clinical nutrition services (45.9%) and homecare clinical nutrition services (66.7%), only 18.6% did not receive reimbursement for outpatient clinical nutrition services (Table 4).
Most clinical nutrition managers supervised at least some clinical nutrition staff and 91.2% had staffs of more than five clinical nutrition FTEs. A description of the sizes of the clinical nutrition staffs and the numbers of employees directly supervised by the clinical nutrition managers is presented in Table 5. Listed in Table 6 are the
115
types of students supervised by the clinical nutrition managers, including: AP4-traineeship students (27.6%),interns (22.4%), coordinated program students (20.7%), and technician students (17.2%).
Three-fourths (75.7%) of the clinical nutrition managers had experienced personnel reductions and/or additions in full-time clinical nutrition staff in the past three years (Table 7). Most clinical nutrition managers reported turnover of two percent or less per year in clinical nutrition dietitians and dietetic technicians (Table 8).
The clinical nutrition managers reported a variety of techniques used for retention and development of clinical nutrition staff in their institutions (Table 9). The most frequently reported staff-retention techniques were assignment to specialty areas (78.4%) and/or education reimbursement (78.4%). The use of guest speakers for department meetings (72.4%) and attendance at medical rounds (70.7%) were the most frequently reported staff-development programs.
The majority (82.6%) of the clinical nutrition managers developed performance objectives with each of their clinical nutrition staff members. Ninety-six percent (96.6%) of the study sample had developed or were developing department plans for continuous quality improvement (CQI). When asked to specify from a given list what programs they had developed for use in CQI, a high percentage of clinical
116
nutrition managers had implemented all the programs listed (Table 10). These results are high because most of the programs listed are important in CQI. They also had implemented a number of management and marketing programs for clinical nutrition services (Table 11 and Table 12, respectively). The most frequently reported management program was a productivity study (62.1%) and the most frequently reported marketing program was community outreach (83.6%) .
The majority of clinical nutrition managers (73.5%) believed the position of clinical nutrition manager would continue to exist at their institution for more than 10 years (Table 13). Over one-third (36.6%) believed the position of clinical nutrition manager would be upgraded in the future, 33.0% believed the position would remain the same, 3.6% believed the position would be downgraded, and the remaining 26.8% did not know how the position would change in the future. Clinical nutrition managers were asked to rate the value they believed their immediate supervisors had of clinical nutrition services, nearly half (46.1%) reported "very valuable" (Figure 1).
Clinical nutrition managers had varying control and responsibility over departmental functions (Table 14). Most clinical nutrition managers had control of product selection (98.3%) and personnel administration (98.3%). Yet, over half (57.9%) did not control a budget (Table 15) .
117
Clinical nutrition managers had involvement in a number of selected educational activities, publications, and research studies (Table 16). Most commonly the clinical nutrition managers were involved in giving local presentations for professionals and the public and writing articles and brochures for the public. Twenty-seven percent (27.6%) of the sample had mentors for professional development. Of those listing a reason for the mentors, 54.5% cited career advancement. Half (50.4%) of the clinical nutrition managers had served as mentors, usually for their staffs (36.4%) . Most clinical nutrition managers had held offices at the local/regional level, as described in Table 17. Seventy-one percent of the managers had attended six or more workshops/seminars lasting one day or longer in the past three years (Table 17). Clinical nutrition managers participated in several other leadership-related activities (Table 18), most frequently reporting quality improvement activities (97.4%), leading department and staff meetings (96.6%), representing the department to the institution (89.7%), and initiating major projects (88.8%).
Clinical nutrition managers listed personal behaviors and actions they believed were important for leaders in clinical dietetics to display. The most often cited behavior and action was strong management skills/ professionalism/communication skills (Table 19). When the clinical nutrition manager responses on those leadership
118
behaviors and actions were categorized into the 10 classifications measured by the LBQ, the most common behaviors and actions reported were, in rank order, those related to communication leadership, respectful leadership, and focused leadership (Table 20).
Clinical nutrition managers also identified a number of characteristics they believed were important for leadership in clinical dietetics. The most often reported characteristics were professionalism and updated knowledge (Table 21). When the characteristics reported were categorized into the LBQ classifications, the most common characteristics were, in rank order, those related to risk leadership, respectful leadership, and trust leadership (Table 22).
The clinical nutrition managers identified how they believed leaders in clinical dietetics should relate to or interface with institutional goals. The most common response was development of department goals with hospital goals (Table 23). In terms of the LBQ categories, the most common responses were those related to organizational leadership (Table 24).
Finally, the clinical nutrition managers were provided with descriptions of transactional and transformational leadership and asked to rate their own leadership styles in their organizations. Most rated themselves as more transformational than transactional (Figure 2).
119
Demographic Profile of Employee EvaluatorsA total of 34 4 employee evaluator demographic surveys
were included in the study sample. The majority {88.1%) of the employee evaluators worked full-time; the remaining11.9% employee evaluators worked part-time. Of those working part-time, 61.5% worked more than 20 hours per week. The title of dietitian or nutritionist (57.1%), nutrition specialist (13.9%), dietetic technician (10.1%), or a management-level title (12.7%) were the most frequently reported titles. Specific employment and educational characteristics of the employee evaluators of the clinical nutrition managers are further detailed in Table 25. When the employee evaluators were asked how closely they worked with the clinical nutrition managers, more reported working closely than not closely at all (Figure 3).
Transformational Leadership Qualities of Clinical Nutrition Managers
Description of the Clinical Nutrition Manager (SELF) LBQ Scores
Initially, the means of the clinical nutrition manager (SELF) LBQ scores were used to evaluate the clinical nutrition managers within the guidelines for the LBQ developed by Sashkin (1990a). On six of the 10 specific leadership scales, the SELF scores were rated as average (Table 2 6) . Possible ratings were very low, low, average, high, and very high. On the remaining four specific
120
leadership scales, the SELF scores were rated as high.Those four high-rating scales were: trust leadership,respectful leadership, bottom-line leadership, and organizational leadership. When the three major subscores were considered, the SELF subscores were rated high on the visionary leadership behavior and visionary leadership characteristics scores and average on the visionary culture building score. Finally, the SELF scores were rated high on the visionary leadership total score. Thus, the clinical nutrition managers were transformational as rated by the SELF LBQ scores.
The SELF LBQ scores were separated into quintiles following the rating guidelines developed by Sashkin (1990a). Most SELF scores were in the average, high, or very high quintiles (Table 27) . For three leadership scales, over one-third of the SELF scores were in the very high quintile (Table 27). Those three leadership scales were respectful leadership, bottom-line leadership, and organizational leadership. On only three leadership scales were more than 5% of the SELF scores in the very low quintile; those were communication leadership, risk leadership, and longterm leadership (Table 27) .
The means of the three SELF LBQ subscores (visionary leadership behavior, visionary leadership characteristics, and visionary culture building) were plotted on the triangle diagram developed by Sashkin (1990a) (Figure 4). The
121
diagram provided a visual pattern of transformational leadership and a perspective on the balance among the three subscores. Based on the interpretive guidelines of Sashkin, the triangular profile of the mean SELF subscores closely resembled that of the self-actualizing leader (Figure 4) though the mean SELF subscore of visionary leadership behavior was lower than that shown in the self-actualized leader profile. The mean SELF subscores were also similar to the "organizational planner" profile identified by Sashkin, which was low in visionary leadership behavior.
Description of the Clinical Nutrition Manager Employee Evaluator (OTHER) LBQ Scores
The approach used to describe the clinical nutrition manager employee evaluator (OTHER) LBQ scores is similar to that used to describe the clinical nutrition manager (SELF) LBQ scores. Again, the first step was to consider the means of the OTHER LBQ scores. Those means were used to evaluate the OTHER LBQ scores on guidelines developed by Sashkin (1990a). On eight of the 10 specific leadership scales, the mean OTHER scores were rated as average (Table 28). On two leadership scales, respectful leadership and organizational leadership, the mean OTHER scores were rated as high (Table 28). When the three major subscores were considered, each of the OTHER subscores was rated average (Table 28).Finally, the OTHER scores were rated average on the visionary leadership total score (Table 28) . Thus, the
122
clinical nutrition managers were rated as transformational based on the OTHER LBQ scores.
The OTHER LBQ scores were broken into quintiles using the scoring guidelines developed by Sashkin {1990a). There was broad distribution of the OTHER scores among the quintiles (Table 29). Two leadership scales, respectful leadership and organizational leadership, had over one-third of the OTHER scores in the very high quintile (Table 2 9). For almost every leadership scale, at least five percent of the OTHER scores were in the very low quintile, and four leadership scales had over 15% of the OTHER scores in the very low quintile: communication leadership, risk leadership, empowered leadership, and long-term leadership (Table 2 9).
The means of the OTHER subscores (visionary leadership behavior, visionary leadership characteristics, and visionary culture building) were plotted on the triangle diagram developed by Sashkin (1990a) (Figure 5). Using the interpretive guidelines of Sashkin, the triangular profile of the mean OTHER subscores closely resembled that of the aspiring leader (Figure 5), but with a stronger visionary culture building subscore than that shown in the aspiring leader profile.
123Comparison of the Clinical Nutrition Manager (SELF) LBQ Scores to the Clinical Nutrition Manager Employee Evaluator (OTHER) LBQ Scores
The PROC MIXED, repeated measures SAS procedure (SAS 1992) was used to compare the mean clinical nutrition manager (SELF) LBQ scores to the mean clinical nutrition manager employee evaluator (OTHER) LBQ scores. All of the mean SELF LBQ scores were higher than the mean OTHER LBQ scores with the exception of the focused leadership score, which was higher for the OTHER group (Table 30). Furthermore, a number of those differences were statistically significant (Table 30). A significant difference (p<.05) was found for two leadership scales: respectful leadershipand risk leadership. A significant difference (pc.01) was also found for five other leadership scales: trust leadership, bottom-line leadership, empowered leadership, organizational leadership, and cultural leadership. Each of the subscores was significantly different: visionary leadershipbehavior (p<.05), visionary leadership characteristics (p<.01), and visionary culture building (p<.01). The visionary leadership total score was also significantly different (pc.01) for the two groups.
Comparison of the Clinical Nutrition Manager LBQ Scores to the LBQ Scores from Other Samples
Sashkin et al (1992) reported normative data for the LBQ and some of these data were compared to the clinical nutrition manager LBQ scores. Tests of statistical
124
significance were not used because different methodologies were employed among the various studies. The first comparison was made between mean clinical nutrition manager SELF LBQ scores and mean SELF LBQ scores of administrators and organizational consultants in the psychological healthcare field (Sashkin et al 1992). While the mean scores were in general similar for the two groups, there were some specific differences (Table 31). The mean communication leadership and long-term leadership LBQ scores were more than one point lower for clinical nutrition managers, compared to the psychological administrators/ consultants. In considering the mean subscores, the visionary leadership behavior and visionary leadership characteristics subscores were lower for clinical nutrition managers. However, the mean of the clinical nutrition manager SELF LBQ score for visionary culture building was higher than the mean administrator/consultant SELF LBQ subscore for the same measure. When the mean LBQ score totals were compared, clinical nutrition managers had a lower mean LBQ score total than the administrator/ consultant SELF LBQ total.
A comparison was also made between mean clinical nutrition manager (SELF and OTHER) LBQ scores and mean entrepreneurs and sole proprietors in very small businesses (SELF and OTHER) LBQ scores. First, in comparing the mean SELF LBQ scores, clinical nutrition managers (SELF) had a greater
r
125
than one point higher communication leadership score than the entrepreneurs and sole proprietors (SELF) (Table 32).The clinical nutrition managers (SELF) had a bottom-line leadership score more than one point lower than the entrepreneurs and sole proprietors (SELF). For the LBQ subscores, mean clinical nutrition manager SELF LBQ subscores were higher for visionary leadership behavior and visionary culture building and lower for visionary leadership characteristics when compared to the entrepreneurs (SELF). The mean clinical nutrition manager SELF LBQ score total was also higher than that of entrepreneurs (SELF).
When a comparison was made between the mean clinical nutrition manager employee evaluator (OTHER) LBQ scores and evaluator (OTHER) LBQ scores of entrepreneurs and sole proprietors in very small businesses, there were again only a few differences (Table 33). Clinical nutrition managers (OTHER) had a one point lower mean bottom-line leadership score compared to the entrepreneurs (OTHER). The clinical nutrition managers (OTHER) also had a lower visionary leadership characteristics subscore and total score than the entrepreneurs (OTHER).
Association Between Transformational Leadership Qualities of Clinical Nutrition Managers
and Defined Study VariablesThe 4F program of the BMDP statistical software package
(Brown 1990) was used to calculate A. as a measure of the
ability to predict transformational leadership qualities when individual defined study variables were known. Values for A were calculated using the clinical nutrition manager(SELF) LBQ subscores and totals and defined study variables training/degree, length of time in management, number of people supervised, income, and participation in advanced practice activities (management, research, and scholarly activities). The defined study variables appeared to have the strongest predictive effect, that is, A values werehighest for the visionary culture building subscore (Table 34). Specific demographic variables that appeared to have the strongest predictive effect on the visionary culture building subscore included: number of clinical technicianssupervised, implementing CQI programs, implementing management programs, public presentations radio/TV, appointment/ election to local/regional offices.
Two demographic variables also appeared to have a predictive affect, that is, A values were greater than 0.10,
for several of the subscores and the total (Table 34).These variables were appointment/election to local/regional offices and implementing techniques to enhance staff retention.
r
CHAPTER VINTERPRETATION AND DISCUSSION OF FINDINGS
In this descriptive study, the sample of clinical nutrition managers exhibited transformational leadership qualities as rated by the LBQ. However, clinical nutrition managers and employee evaluators of the clinical nutrition managers significantly differed in their LBQ scores of the transformational leadership of the clinical nutrition manager. Finally, there was some association between the defined study variables and the clinical nutrition manager LBQ subscores and total score. The specific null hypotheses developed for the investigation were not supported by the results of the study, as discussed below.
Description of Transformational Leadership Qualities of Clinical Nutrition Managers
Hypothesis 1The first hypothesis, that "clinical nutrition managers
do not exhibit transformational leadership qualities," was rejected. The basis for this rejection was the reported mean LBQ scores and quintile profiles of LBQ scores of clinical nutrition managers. All of the mean clinical nutrition manager (SELF) LBQ scores and the mean clinical
127
nutrition manager employee evaluator (OTHER) LBQ scores were rated as average or high based on the guidelines developed by Sashkin (1990a). Furthermore, when LBQ scores were broken into quintiles, more than 75% of the clinical nutrition manager (SELF) LBQ scores (with the exception of the scores on the communication leadership scale) were rated as average, high, or very high based on the guidelines developed by Sashkin. The clinical nutrition manager employee Evaluator (OTHER) LBQ scores, although lower than the SELF LBQ scores, showed a similar trend of average, high, or very high ratings when broken into quintiles. On all but three scales (communication leadership, empowered leadership, and longterm leadership), more than 70% of the OTHER LBQ scores were rated as average, high, or very highusing the guidelines developed by Sashkin.
When the mean LBQ scores (SELF and OTHER) of clinical nutrition managers were compared to the mean LBQ scores ofnormative data, additional evidence was obtained thatclinical nutrition managers exhibited transformational leadership qualities. Overall, there were few differences between mean LBQ scores (SELF and OTHER) of the clinical nutrition managers and the mean LBQ scores (SELF) of administrators/consultants in psychological healthcare and mean LBQ scores (SELF and OTHER) of entrepreneurs of small businesses.
129
Although there has been very limited research on transformational leadership in dietetics, the finding that the study sample of clinical nutrition managers exhibited transformational leadership qualities was not unexpected. There were several reasons that might account for the finding. First, transformational leadership is more likely to be found during crisis or opportunistic conditions rather than static or stable conditions (Schein 1985). In other words the impetus of change could promote transformational leadership development. And though the stability of individual institutions where the clinical nutrition managers worked was not measured in this study, healthcare institutions in general are in a state of flux today because of the impact of cost containment, healthcare reform, and other challenges.
Second, the study sample had several demographic characteristics that have been shown to be related to transformational leadership. The study sample was predominantly female. Some investigators have argued that gender does not impact transformational leadership (Bass 1981; Dobbins and Platz 1986) but others have found that women are more transformational than their male peers (Rosener et al 1990; Dunham and Klafehn 1990). Having an advanced degree has also been shown to be related to transformational leadership (Dunham and Klafehn 1990; Young
130
1992) and the majority of the clinical nutrition managers in this sample either had master's degrees or had completed some work toward those degrees.
Situational variables may have contributed to the transformational leadership exhibited by the clinical nutrition managers in this sample. The majority of the clinical nutrition managers were from institutions greater than 2 50 beds. Young <1992) found that as a group nurse leaders with high transformational leadership scores worked in larger hospitals, on larger nursing units, and supervised more employees. However, Dunham and Klafehn (1990) found no significant relationship between transformational leadership and hospital size.
Finally, personality factors might have affected the disposition of clinical nutrition managers for transformational leadership. While this investigation did not evaluate specific personality factors, some, such as power, were indirectly measured by the LBQ. On the LBQ, the "empowered leadership" scale was a measure of the use of power to influence others. Few investigations have considered the power exhibited by dietitians. In the present study, clinical nutrition managers (SELF) LBQ scores and employee evaluator (OTHER) LBQ scores of clinical nutrition managers were rated as average on empowered leadership. In contrast, Schiller et al (1993)
131
reported the mean score for power in the clinical dietitians they studied was low when compared to all other measured behavioral styles of clinical dietitians and when compared to the normative data for their study instrument. Since their data were collected from 1986 to 1989 it could be that in the current healthcare environment clinical dietitians have developed a greater appreciation of and use for power. Another and more important consideration is the definition of power on the scale used by Schiller et al: power was described as a negative trait where power managers were dogmatic, abrupt, hostile, and had little regard for others' feelings.
This negative definition of power is somewhat similar to words dietitians themselves have used to describe power. In a recent study by Mandel and Garey (1993), dietitians from the New Jersey Dietetic Association were asked to describe their concept of power. The key descriptors the dietitians used were accomplishments, control, intelligence, and connections; power was not considered a priority by respondents. In contrast, on the LBQ, empowered leadership was described positively; the empowered leader had a strong need for power but realized power and influence must be shared and thus used power to empower others. The clinical nutrition managers in the present study may have responded more positively to this new
132
definition of power versus that identified in the instrument used by Schiller et al (1993) and described by Mandel and Garey.
Overall, evidence of strong transformational leaders in clinical nutrition management was provided in the present research. This is somewhat in conflict with the results of Schiller et al (1993). These researchers documented that some clinical dietitians had a high self-actualization score which they believed indicated transformational leadership. However, they also reported that a number of dietitians had high dependency and several other "negative" scores that they concluded did not reflect transformational leadership.
There may be several reasons for the difference in strengths of transformational leadership documented in the two studies. First, the study sample of Schiller et al (1993) consisted of clinical dietitians who in general represented smaller hospitals. Smaller hospital size itself could have been a factor limiting transformational leadership as previously found by Young (1992). Also it is possible that even though the sample of Schiller et al included clinical dietitians with supervisory responsibility, there could have been a smaller number of clinical dietitians who were in true management and leadership positions. These positions could have represented low-
133
level management, which as McDaniel and Wolf (1992) documented may have weaker transformational leadership skills.
Another consideration is that the data presented by Schiller et al (1993) were collected over a four-year period, during which time healthcare was not faced with the severe pressures seen today, including downsizing, skyrocketing costs, and government regulation. In addition, the instruments used by the researchers were different from those selected for the present study. Specifically, they used the Lifestyles Inventory. That instrument was not developed to examine transformational leadership and thus did not provide a true measure of transformational leadership. Finally, their data were based exclusively on self- reports. It is not known if data from subordinates would have provided similar or conflicting results to those Schiller et al reported.
Comparison of Transformational Leadership Qualities of Clinical Nutrition Managers as Rated by
Clinical Nutrition Managers Themselves and Employee Evaluators
Hypothesis 2The second hypothesis, "there are no differences
between the transformational leadership qualities of clinical nutrition managers as rated by clinical nutrition managers themselves and as rated by their employee
134
evaluators" was rejected. With the exception of the focused leadership, communication leadership, and longterm leadership scales, mean clinical nutrition manager {SELF) LBQ scores were significantly higher for every scale when compared with the mean clinical nutrition manager employee evaluator (OTHER) LBQ scores. It was anticipated that the clinical nutrition manager SELF and OTHER LBQ scores would differ, but the finding that the SELF LBQ scores were consistently higher was unexpected. Some researchers (Bass and Avolio 1990; Posner and Kouzes 1990) have documented that with their respective transformational leadership instruments self-ratings are typically higher than ratings of the same leaders by subordinates and others. Yet the opposite has been reported for the LBQ developed by Sashkin and Burke (1990). Sashkin (1990b) stated that with the LBQ, the ratings by others tend to be slightly more positive than self-ratings. However, in the most recent normative data of Sashkin et al (1992) this does not always appear to be true.
In the field of dietetics, researchers investigating areas related to leadership, such as the image of the dietitian, reported dietitians rated themselves lower than their peers rated them in the area of image (Calvert et al 1982; Ryan et al 1988; Finn et al 1991) . Perhaps in the present study, the low score on the communication
135
leadership scale indicates that dietitians did not clearly communicate their mission, visions, and values and thus were not perceived as high in transformational leadership qualities as they themselves believed they were.
By plotting the mean LBQ subscores (visionary leadership behavior, visionary leadership characteristics, and visionary culture building) on the triangular diagram developed by Sashkin (1990a) a visual comparison of the mean clinical nutrition manager (SELF) LBQ scores and the mean clinical nutrition manager employee evaluator (OTHER) LBQ scores was provided. Visually, the difference between the mean scores of the two groups was striking. The mean SELF LBQ subscores most closely fit the "self-actualizing leader" profile described by Sashkin as the ideal profile (Figure 4). He believed that this profile provided strong evidence that the leader was currently acting as an effective leader. Sashkin explained that research shows this individual has employees who report a high quality of work life, as well as high productivity and bottom line outcomes. He described leaders in this group as self- actualizing .
In contrast, the mean clinical nutrition manager employee evaluator (OTHER) LBQ subscores formed a smaller triangle that most closely matched "the aspiring leader" (Figure 2). Sashkin (1990a) described this individual as
136
not overly focused on any one area and quite likely to have sound managerial capabilities and already looking toward the challenge of leadership. He explained, however, that this person might feel frustration. Such a leader may have some idea of what he/she is reaching for but not be able to identify a clear path or goal. Personal awareness of the nature of leadership and being able to differentiate management from leadership were suggested as beginning action steps.
Sashkin (1990a) explained that "the larger your triangle, the more likely it is that you are a visionary leader." Thus, clinical nutrition managers viewed themselves as more transformational than their employee evaluators viewed them. The clinical nutrition managers' views of themselves as transformational leaders was further underscored by the results of the demographic questionnaire distributed during the first part of this study. When given definitions of transactional and transformational leadership and asked in the demographic questionnaire to rate their own leadership style, a greater number of clinical nutrition managers rated themselves as more transformational than transactional (Figure 2).
One possible reason for the difference between the profiles of the clinical nutrition manager SELF and OTHER LBQ subscores could be related to the relatively lower
137
transformational leadership behavior subscores and lower communication leadership scores compared to the other scores measured. Specifically, it might be interpreted that the clinical nutrition managers were not able to communicate effectively their transformational leadership beliefs and behave in the manner of transformational leaders. The profile of the clinical nutrition managers to some extent fit the "organizational planner" profile outlined by Sashkin (1990a) (Figure 4). He described this individual as a person with great plans and a real vision, and who sees how these plans can fit into the organization. However, the organizational planner does not have the necessary interpersonal skills to communicate the vision to others, to excite, interest, and ultimately empower them to buy into— and own— the vision.
Association Between Transformational Leadership Qualities of Clinical Nutrition Managers
and Defined Study VariablesHypothesis 3
The third hypothesis, that "there are no associations between transformational leadership qualities of clinical nutrition managers and defined study variables," was rejected based on the X calculations used to measure the predictive ability of the defined study variables. The X
values were consistently high for the defined study variables when the culture behavior subscore was evaluated.
In addition, two study variables, appointment/election to local/regional offices and implementing techniques to enhance staff retention, had higher X values for the LBQsubscores and the LBQ total score, when those variables were compared to the other defined study variables. It was anticipated that there would be some association between the defined study variables and the LBQ subscores and the LBQ total score, since reports by other researchers (Schiller et al 1993; Dunham and Klafehn 1990; Young 1992) had indicated an association. However, the finding that the defined study variables appeared to have a closer association with one particular subscore, the visionary culture building subscore, was unexpected. An association of this type was not found in the literature.
Dunham and Klafehn (1990) and Young (1992), considered various demographic variables and the relationship of those variables to transformational leadership, but used total measures of transformational leadership and did not consider subscores. Schiller et al (1993) did consider subscores and the relation of the subscores to the characteristics of dietitians. However, the instrument used by these researchers to measure leadership, the Life Styles Inventory (LSI), did not have scales that were well- correlated with those of the LBQ.
139
The finding in the present study that only two study variables, appointment/election to local/regional offices and implementing techniques to enhance staff retention, seemed to be more predictive of transformational leadership than were other defined variables, was also unexpected. Schiller et al (1993) found an association between holding local and regional offices and the scores of dietitians on the LSI instrument used to measure leadership in their study. Yet, they also found an association between a number of other characteristics and the LSI scores of dietitians. It may be that those differences were indicative of the differences in the instruments used for the two studies. The LSI instrument was developed to measure thinking and behavioral styles, not transformational leadership. The LSI centered on concern for job satisfaction and security and concern for people and tasks. Each of the styles measured by the LSI was distinct, and some, such as the humanistic-helpful style and oppositional style, were diametrically opposed to each other. Thus, both positive and negative styles were reflected on the LSI. In contrast, the LBQ included only positive scales and the LBQ was a measure of transformational leadership. Furthermore, a number of the LBQ scores were strongly interrelated and were therefore added to form subscores. Perhaps because the LSI instrument yielded less strongly
140
interrelated scores, the association of characteristics of the dietitians with the LSI scores was more pronounced than the association documented in the present study between the defined study variables and the LBQ scores.
LimitationsAs one of the first studies to explore transformational
leadership in dietetics, this investigation had several limitations. First, the sample chosen for this research might not have been representative of clinical nutrition managers as a whole. There could be some clinical nutrition managers who were not members of the Clinical Nutrition Management practice group and thus were not surveyed in this study. In addition, those selected for inclusion in the research were from larger hospitals and supervised at least three dietitians and/or dietetic technicians.Thus, the sample might not have reflected transformational leadership qualities of clinical nutrition managers in smaller hospitals. Also, the sample included an element of self-selection. It is not known if the results of this study were reflective of clinical nutrition managers who chose not to participate in further leadership research and thus were excluded from the sample.
Another limitation was that individuals, both clinical nutrition managers and employee evaluators, might have responded on the LBQ as they believed they should have and
141
not answered truthfully. And some clinical nutrition managers could have selected those employee evaluators who the managers believed would rate them most positively.This could have accounted for some of the disparity between the clinical nutrition manager and employee evaluator LBQ scores.
There was also the limitation of nonresponse, which frequently occurs in mailed surveys. In this study there was nonresponse at two levels, when the initial demographic survey was mailed and when the LBQ was mailed. It is not known if those who chose not to respond to the initial demographic survey or the LBQ mailing would have answered differently than those who did return the demographic surveys and LBQs. There were some individual items for which there were nonresponses. For the LBQs, values were imputed for the missing data based on results from other completed LBQs. Although there were few missing values on the LBQs, the imputation could have influenced the data analysis. For the demographic surveys, nonresponses were equated with a value of zero or none. The most common variables with missing values were number of clinical technicians supervised (n = 83), professional presentations state/national (n = 103), public presentations state/ national (n = 96), public presentations radio/TV (n = 101), publication professional book chapters (n = 102),
publication professional books (n = 98) publication public book chapters (n = 97), and publication public books (n = 98) (Table 34). Since these variables are relatively discrete, it was assumed that when no number of occurrences was reported by the clinical nutrition manager it was likely that no activity occurred for that dimension. Given the nature of these variables this seemed to be a reasonable assumption. Another way of handling the missing values for demographic variables would have been to substitute a mean response. However, this was not viewed as reasonable, since it seemed that if the clinical nutrition managers had had activity related to the variables, they would have responded, since they did respond for other defined study variables. However, it is possible, though not likely, that the assumption that missing values could be equated to zero was not valid for some or all of the variables. Thus, the analysis might have again been influenced.
A fourth limitation was related to the selection of the LBQ and demographic instruments. The LBQ has been validated by previous research (Sashkin and Burke 1990; Sashkin 1990). However, it was still possible that the LBQ did not accurately evaluate all elements of transformational leadership. The demographic surveys developed for this study were reviewed by content experts but were not
143
validated. Thus, the survey instruments could have introduced some measurement error.
Another limitation was the strength of the statistics used in this investigation. To test the first hypothesis, mean LBQ scores were used that mediated the influence of individual scores. To help overcome that, LBQ scores were also grouped by quintiles, which helped delineate the range of individual scores. For the second hypothesis, inferential statistics were used; thus, there was a possibility for both type I and type II errors in interpreting significance. The third hypothesis was tested using the Xvalue, which was appropriate to test prediction but, like other tests of association, could have given evidence of no association even though the variables might not have been statistically independent.
General Implications of FindingsWith the paucity of reported research on leadership in
clinical dietetics, this study provides important implications for the profession. First, this investigation extends the work of Schiller et al (1990): 1) an instrument was used that evaluated transformational leadership specifically; 2) a defined area of dietetic practice, clinical nutrition management, was investigated; and 3) the ratings of subordinates were considered.
144
Clark et al (1992) reported that self-ratings of leadership performance have much lower correlations with performance than do ratings of leadership by others and explained, "Leaders think they are doing much better than they are." Thus, including the views of subordinates or others is critical to helping better understand the transformational leadership of clinical nutrition managers.
The present investigation also yielded valuable information regarding the transformational leadership weaknesses and strengths of clinical nutrition managers. Surprisingly, when compared to other LBQ scales, the clinical nutrition manager (SELF) LBQ scores and clinical nutrition manager employee Evaluator (OTHER) LBQ scores were lowest on the communication leadership scale. It may be that in the responsibilities and job functions of clinical nutrition managers, communication skills have limited emphasis. In the research literature, emphasis appears to be on measurement of discrete tasks and activities related to the delivery of clinical patient nutrition care and not to communication with staff and colleagues who will ultimately have the most impact on the quality of that patient nutrition care. This focus also exists at both the specialty and management levels.
For example, in a recent study conducted to help define specialty clinical practice in dietetics, only 3 of the 49
145
tasks found to be part of a generic model of specialty practice seemed to be related to communication. Most of the remaining 46 tasks were specific nutrition care tasks (Bradley et al 1993) . Interestingly, the three communication tasks were not common to each of the three specialities studied; that is, none of the communication tasks were included in the metabolic specialty practice model. However, all three communication tasks were included in the renal and pediatric practice models.
Further evidence of an emphasis on tasks related to patient care was presented in The American Dietetic Association's most recent position paper on management of healthcare food and nutrition services (American Dietetic Association 1993). That position paper described in detail the training needed in human resources, food science and safety, government regulations, and medical nutrition care to be successful as a manager. The manager was described as a professional who was "knowledgeable in identifying services required by patients and competent in managing resources and processes necessary to provide those services." Yet, only one small mention was made of the need for communication skills: "The director must be able to access this [staff] expertise and communicate effectively in order to contribute to both the facility healthcare and administrative teams."
Based on reported research of dietetics at the advanced practice level, there seems to be a decrease in emphasis on tasks, but communication skills are not necessarily viewed as primary skills. Recently, Bradley et al (1993) investigated characteristics of advanced-level dietetics practice to develop a model of advanced practice for the profession. Although some of the elements included in their model did appear to relate to transformational leadership, communication skills were not included in the model.
However, practitioners themselves appear to recognize a strong need for communication skills at an advanced practice level. Nettles et al (1993) examined the relevance of competencies to graduate education and experience in a different area of dietetic management, food service management. Problem solving/decision making, written/oral communication, and organizational skills concepts were rated by the graduates as the most relevant to management among 43 concepts listed. And when the concepts were grouped into just four factors, the organizational communication factor had the highest relevance score. Likewise, in the present study, the need for leaders to have good communication skills was identified by a number of the clinical nutrition managers surveyed (Table 22) .
It is important to identify such areas where clinical nutrition managers can sharpen skills that will enhance
147
transformational leadership. It is also helpful to consider the strengths that clinical nutrition managers might already possess in transformational leadership and what might contribute to the development of those strengths. In this study, the LBQ scores of the clinical nutrition managers were highest on the scales of respectful leadership and organizational leadership. Respectful leadership measured how the clinical nutrition managers expressed concern for others and their feelings and also measured the leaders' self-regard (Sashkin 1990b). The high rating on the respectful leadership scale is corroborated in other research. Respectful leadership is similar to the humanistic/helpful behavioral style measured in the study by Schiller et al (1993) where they found that the mean dietitian score for the humanistic/helpful behavioral style was above the normative population mean. Respectful leadership is also like the characteristic of concern for employees identified by Meighan (1990) as a key characteristic of transformational nursing leaders.
Organizational leadership as described by Sashkin (1990b) examines the degree to which a leader has a positive impact on helping organizations deal with change, achieve goals, coordinate the activities of organizational members, and maintain the system. The scale was developed based on the work of Parsons (1960) and Schein (1985), who
148
believed that effective leaders designed and developed productive organizational cultures. Such skills are of vital importance for today's healthcare leaders. The finding that the study sample of clinical nutrition managers had a high concern for developing a productive organizational culture and a high concern for people (as evidenced by their high scores on the organizational leadership and respectful leadership scales) is not unexpected. Researchers investigating leadership among other health professionals have documented that health professional leaders typically had a high concern for both tasks and relationships (Gevedon 1990; Garrett 1991; Mamastro and Fort in-Crosby 1980) . Certainly in the turbulent times healthcare faces today, transformational leaders with such skills will continue to be needed.
Given that clinical nutrition managers had several strengths in transformational leadership, specifically respectful leadership and organizational leadership, the next question was, What helped build those strengths? The present study was descriptive in nature; thus, it was not possible to determine exactly what factors, such as the defined study variables, actually contributed to the development of transformational leadership. However, the data reported could provide some insight. Some variables, such as appointment/election to local/regional offices and
149
implementing techniques to enhance staff retention, seemed to be predictive of transformational leadership and should be encouraged. It also appeared that the experiences and strengths of clinical nutrition managers in management, research, and scholarly activities had the most impact on the visionary culture building subscore, which included the organizational leadership scale. Having strength in visionary culture building is vital today. Schein (1985) identified that constructing the organization's culture might be one of the most important tasks of organizational leaders. Perhaps providing opportunities to experience management, research, and scholarly activities, such as those defined in this study, could help dietitians develop strength in visionary culture building.
In summary, the current strength in transformational leadership in clinical nutrition management appears to be similar to that described by Barker (1990) regarding leadership in nursing, where the focus was more on gaining knowledge than taking action. She stated that nurse leaders were eager to seek out information on how-to's and gather knowledge of managing change, conflict resolution, and leadership rather than to focus on experiences that put that knowledge into practice. As evidenced by this study, the clinical nutrition managers were strong in visionary organizational leadership and visionary leadership
150
characteristics. Thus the clinical nutrition managers appeared to have knowledge about what was needed to take on leadership roles in their organizations and appeared to have the characteristics needed to take on those roles.Yet, clinical nutrition managers needed to become stronger in visionary leadership behavior to help their subordinates understand the clinical nutrition managers' visions. Clinical nutrition managers needed to exhibit behaviors and take action more like transformational leaders, to actually experience transformational leadership and to learn to effectively communicate their ideas and visions to others.
Barker (1990, p. vii) explained that the emerging healthcare environment is transforming the way health professionals work and utilize available resources:
1. "People, rather than dollars, technology, equipment, or machines are seen as the most significant asset.
2. People are identified as the source of creativity, diversity, and skills.
3. People issues and influencers surface as determinants of organizational success."
Barker (1990) issued the challenge to nurses to place less emphasis on getting the task done and to make the perceptual shift to recognizing the significance of the individual as a quality factor in the practice of nursing. The same challenge could be applied to dietetics. The questions that must be raised are, How can clinical
151
nutrition managers learn to exhibit transformational leadership behaviors? What will it take to broaden their experiences in these areas and improve communication skills, to develop a stronger focus on the individual, and not just the task? Suggestions for how to address those issues are summarized in the next section.
Recommendat ionsBased on the results of this research, there are
several important recommendations for expanding transformational leadership in clinical nutrition management. First, there is a need for more basic research to define transformational leadership in the dietetic profession in general and clinical nutrition managers in particular. To date most researchers in the dietetic profession have not distinguished leadership as different from management. New studies are needed in which the distinction is clearly made between leadership and management as well as studies that will continue to investigate transformational leadership in dietetics.
The present study provided an initial profile of how a selected group of clinical nutrition managers could be rated on transformational leadership qualities. Further investigations are needed to determine how such strengths and weaknesses might be expressed in other areas of dietetic practice. In addition, there should be specific
152
research to delineate factors that could help contribute to the development of transformational leadership skills. It is important to determine how best to strengthen areas such as visionary leadership behaviors, where dietitians may need to build their skills. The current research defined only two study variables that seemed to influence visionary leadership behaviors. Perhaps there are others that could be identified and encouraged.
Beyond basic research to identify the skills clinical nutrition managers should possess and develop to become transformational leaders, there is a need to examine the outcomes of transformational leadership in the profession. Outside the profession of dietetics, the outcome level of research is becoming the mainstay of many transformational leadership investigations today. Specifically, now that researchers have defined the underlying principles of transformational leadership, they have turned their attention to documenting the results and impact of transformational leadership on issues such as 1) profitability,2) performance of work units, 3) quality of work output,4) reduction of stress in the workplace, and 5) worker satisfaction and morale. Research should be conducted in the dietetics field to determine how transformational leadership affects similar outcomes.
f
153
In addition to a focus on quantitative outcomes, it is also appropriate to investigate qualitative outcomes, to help show how leaders can model and apply transformational leadership behaviors in dietetics. Sashkin (1990b) reported that the major impact of transformational leadership is on the organizational culture. An example of how leaders might help shape organizational culture is provided by Deal and Petterson (1990, p. 80), who studied school principals and revealed six ways leaders helped shape culture:
1. "Developing a sense— rooted in history, values, and beliefs— of what the school should be;
2. Selecting staff whose values fit well with their own;
3. Facing conflict rather than avoiding it and, through conflict, resolving disputes and building unity;
4. Using one's own behavior to exemplify core values and beliefs, and reinforcing those values consistently in daily routines;
5. Telling stories that communicate shared values; and
6. Nurturing the traditions, ceremonies, rituals, and symbols that express and reinforce the school culture."
From quantitative outcome research in dietetics, similar findings may be derived.
A second recommendation is to focus on increasing the communication skills of clinical nutrition managers. It seemed that the study group of clinical nutrition managers
154
possessed the characteristics of transformational leaders (such as strong bottom-line and long-term leadership) and visionary culture building skills of organizational and cultural leadership, but were not as strong in visionary leadership behaviors, particularly communication skills. Visionary leadership behaviors are the actions that are important for followers to become excited about the leader's goals and understand how they can build the success of the organization. Based on the current study, it appears that the clinical nutrition managers already recognize the importance of those behaviors, yet lack the skill and training to implement such behaviors effectively.
To increase communication skills, a two-pronged approach is needed. First, communication and conceptual skills need to become a more recognized part of advanced practice and management jobs. Brown and Fruin (1989) identified that in community dietetics practice, upper management rated conceptual skills of long-range planning, problem solving, and developing new projects and direction as most important— but communication of those values is equally important. In addition to strengthening the role of communication in management practice, there is also a need to develop educational programs that provide training in communication skills, both at the undergraduate and continuing education levels.
With a strong base in communication skills, it would then be appropriate to develop training programs in transformational leadership. Clarke et al (1992) stated that leader behaviors are trainable and that the effects of training have been proven to persist. They believed that trained leaders outperform untrained leaders. The American Dietetic Association Professional Development Institute now being formed is an excellent beginning in leadership training for the profession. The Institute has been described as having a three-track approach (Finn and Dodd 1993).Track I will be open to all members of The American Dietetic Association (ADA) and feature programs developed for specific audiences on topics such as negotiation and innovation. Communication skills training should also be a focus at this level. Track II, open to ADA members on a limited basis, will select qualified individuals for participation in a leadership development program unique to ADA. Track III will be designed as a "train the trainer" program to foster leadership skills among young members. It will be important for ADA leaders developing this institute to keep in mind that the training programs implemented at all levels must go beyond building basic knowledge and how-to's and focus on actually modeling leadership behavior and helping members develop the skills needed to act more like transformational leaders. Through the Institute, members
156
should have exposure to hands-on leadership experiences and an opportunity to take on actual leadership roles and then have critiques of their performances.
A final recommendation is to develop programs and approaches for dietitians that will mold organizational environments to support the continued development of transformational leadership. Sashkin et al (1992) believed that it was important to develop better methods for teaching aspiring and current leaders how to think about and construct their own cultures of excellence. Those researchers further explained that organizations that encourage, model, and reward leadership training can expect increased levels of transformational leadership. Perhaps The American Dietetic Association Professional Development Institute could help dietitians learn to shape organizational cultures that reflect a commitment to leadership. Through the Institute and its programs, clinical nutrition managers and other dietitians must learn how to create a work environment that will support transformational leadership development in their subordinates. The clinical nutrition managers and other dietitians must learn to prepare the way for the transformational leaders that follow in their footsteps.
f
CHAPTER VI SUMMARY
A study was conducted to investigate transformational leadership qualities of clinical nutrition managers who were members of the Clinical Nutrition Management practice group of The American Dietetic Association (ADA). Transformational leadership qualities were measured using an existing standardized and validated transformational leadership analysis instrument developed by Sashkin and Burke (1990), the Leadership Behavior Questionnaire (LBQ). Other data were obtained from two demographic surveys developed by the investigator for use in the study. Initially, demographic surveys were mailed to the general population of 1,599 members of the Clinical Nutrition Management practice group of ADA. Surveys were returned by 951 members (59.8%). A study sample of 150 was selected from those clinical nutrition managers who returned the demographic survey and met the following criteria:
1. Current membership in the Clinical Nutrition Management practice group of ADA;
2. Current dietetic registration and/or licensure;
157
158
3. Employment as clinical nutrition managers in United States hospitals;
4. Direct supervision of a staff of three or more individuals (dietitians and/or dietetic technicians);
5. Consent to participate in the study and to recruit three direct-report employee evaluators (dietitians and/or dietetic technicians) to participate in the the study.
Explanatory letters, instruction sheets, and sets of LBQs (one SELF and three OTHERS) were mailed to the study sample and 116 (77.3%) sets were usable for data analysis.
Statistics were calculated using the 1989 version (6.07) of the Statistical Analysis System (SAS) software (SAS 1992) and the 1990 version of the BMDP statistical software package (Dixon 1990) . Descriptive statistics were used to analyze the demographic surveys and define the demographic profiles of the subject group of clinical nutrition managers and employee evaluators and to describe the frequency of distribution of responses. Means and standard deviations were calculated for the LBQ scores, subscores, and totals and were used to evaluate transformational leadership based on the rating guidelines for the LBQ developed by Sashkin (1990a). To compare clinical nutrition manager (SELF) LBQ scores and clinical nutrition manager employee evaluator (OTHER) LBQ scores the PROC
159
MIXED repeated measures SAS procedure was used (SAS 1992). Significance was computed using the approximate F-test.The ability of defined study variables to predict transformational leadership qualities was measured by calculating Xusing the BMDP 4F program (Brown 1990).
The three null hypotheses tested in the study were rejected. The first null hypothesis, that "clinical nutrition managers do not exhibit transformational leadership qualities," was rejected based on the reported mean LBQ scores and quintile profiles of the LBQ scores of clinical nutrition managers. All mean LBQ scores were rated as average or high and over 70% of the individual LBQ scores were in the average, high, or very high quintiles. The second null hypothesis rejected was that "there are no differences between the transformational leadership qualities of clinical nutrition managers as rated by clinical nutrition managers themselves and as rated by their employee evaluators." This hypothesis was rejected on the basis that the LBQ subscores, the LBQ total, and all but three mean clinical nutrition manager (SELF) LBQ scores were significantly higher when compared with the mean clinical nutrition manager employee evaluator (OTHER) LBQ scores. The final hypothesis, that "there are no associations between transformational leadership qualities of clinical nutrition managers and defined study variables,” was rejected based on the X calculations used
I.
160
to measure the predictive ability of the defined study variables. The X values were consistently high for thedefined study variables when the culture building subscore was evaluated. In addition, two study variables, appointment/election to local/regional offices and implementing techniques to enhance staff retention, seemed to be more predictive of transformational leadership than were other defined variables.
There were three specific objectives to this study:1. To identify transformational leadership qualities
of clinical nutrition managers;2. To compare transformational leadership qualities of
clinical nutrition managers as rated by clinical nutrition managers and as rated by their employee evaluators;
3. To associate identified transformational leadership qualities with defined variables: training/degree, length of time in management, number of people supervised, income, and participation in advanced practice activities (management, research, and scholarly activities).
In general these objectives were met in this descriptive study. Specifically, it was documented that the study sample of clinical nutrition managers appeared to have transformational leadership qualities. The clinical nutrition managers themselves rated their transformational
[
161
leadership qualities higher than did the clinical nutrition manager employee evaluators. The clinical nutrition managers were particularly strong in respectful leadership and organizational leadership, but were weaker in communication leadership skills. In addition, the clinical nutrition managers were stronger in visionary leadership characteristics and visionary culture building than they were in visionary leadership behaviors. Finally, there appeared to be some association between leadership and management experiences of the clinical nutrition managers and their visionary culture building skills.
Based on the results of this research, there are several important recommendations for expanding transformational leadership in clinical nutrition management. First, there is a need for more basic research to define transformational leadership in the dietetic profession in general and clinical nutrition management in particular. Specific research should also be focused on delineating factors that help contribute to the development of transformational leadership skills in clinical nutrition managers. Beyond basic research, there is a need to examine the outcomes of transformational leadership in the profession, including both quantitative and qualitative outcomes.
A second recommendation is to increase the communication skills of clinical nutrition managers. Third, it is important to develop training programs in transformational
162
leadership, with an emphasis on hands-on leadership experiences and critiques of performances. The final recommendation is to develop programs and approaches for clinical nutrition managers that will help them shape their organizational environments to foster the development of transformational leadership in their subordinates, and thus prepare the profession's transformational leaders of the future.
APPENDIX A
LEADERSHIP BEHAVIOR QUESTIONNAIRE (LBQ) SCALES AND SUMMARY OF TRIANGULAR PROFILES
DEVELOPED FOR THE LBQ
163
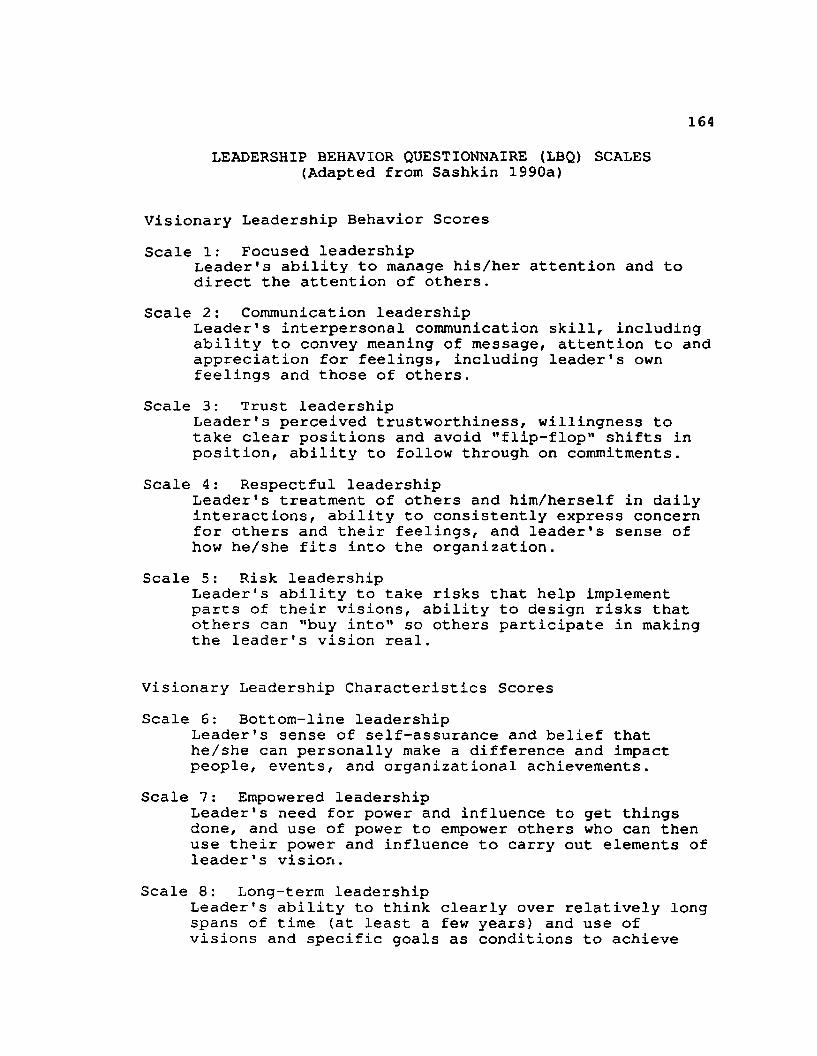
164LEADERSHIP BEHAVIOR QUESTIONNAIRE (LBQ) SCALES
(Adapted from Sashkin 1990a)
Visionary Leadership Behavior ScoresScale 1: Focused leadership
Leader's ability to manage his/her attention and to direct the attention of others.
Scale 2: Communication leadershipLeader's interpersonal communication skill, including ability to convey meaning of message, attention to and appreciation for feelings, including leader's own feelings and those of others.
Scale 3: Trust leadershipLeader's perceived trustworthiness, willingness to take clear positions and avoid "flip-flop" shifts in position, ability to follow through on commitments.
Scale 4: Respectful leadershipLeader's treatment of others and him/herself in daily interactions, ability to consistently express concern for others and their feelings, and leader's sense of how he/she fits into the organization.
Scale 5: Risk leadershipLeader's ability to take risks that help implement parts of their visions, ability to design risks that others can "buy into" so others participate in making the leader's vision real.
Visionary Leadership Characteristics ScoresScale 6: Bottom-line leadership
Leader's sense of self-assurance and belief that he/she can personally make a difference and impact people, events, and organizational achievements.
Scale 7: Empowered leadershipLeader’s need for power and influence to get things done, and use of power to empower others who can then use their power and influence to carry out elements of leader’s vision.
Scale 8: Long-term leadershipLeader's ability to think clearly over relatively long spans of time (at least a few years) and use of visions and specific goals as conditions to achieve
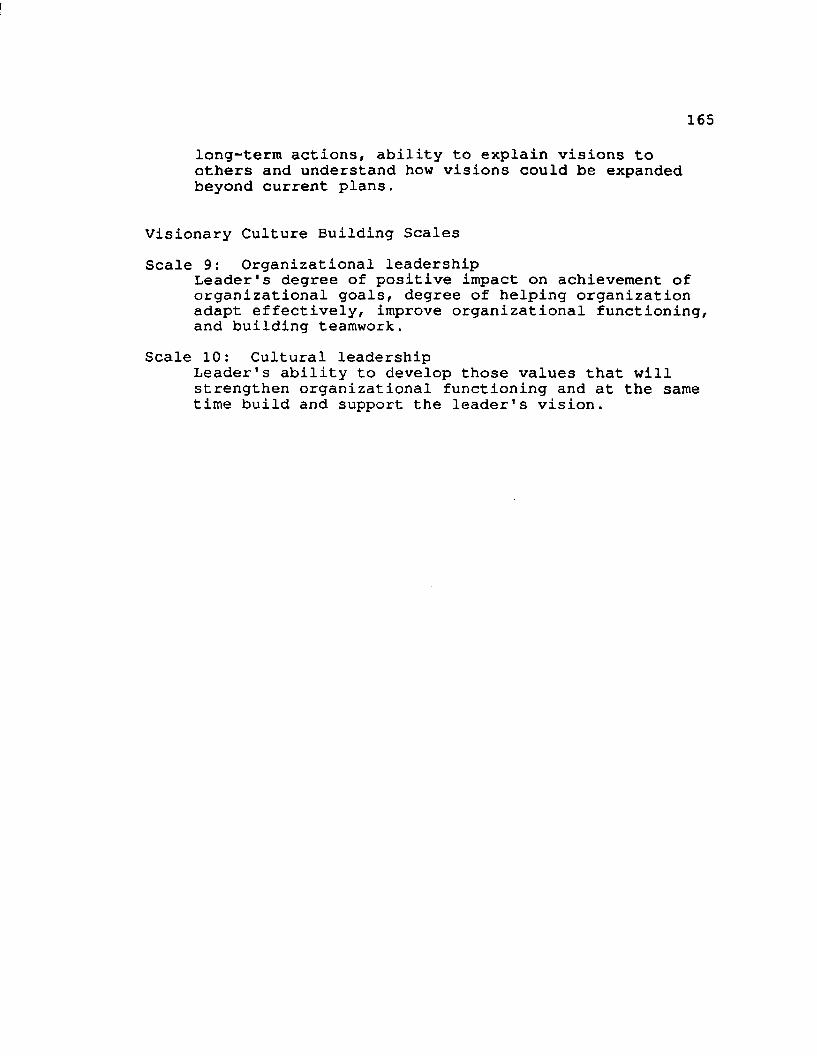
I
165long-term actions, ability to explain visions to others and understand how visions could be expanded beyond current plans.
Visionary Culture Building ScalesScale 9: Organizational leadership
Leader's degree of positive impact on achievement of organizational goals, degree of helping organization adapt effectively, improve organizational functioning, and building teamwork.
Scale 10: Cultural leadershipLeader's ability to develop those values that will strengthen organizational functioning and at the same time build and support the leader's vision.
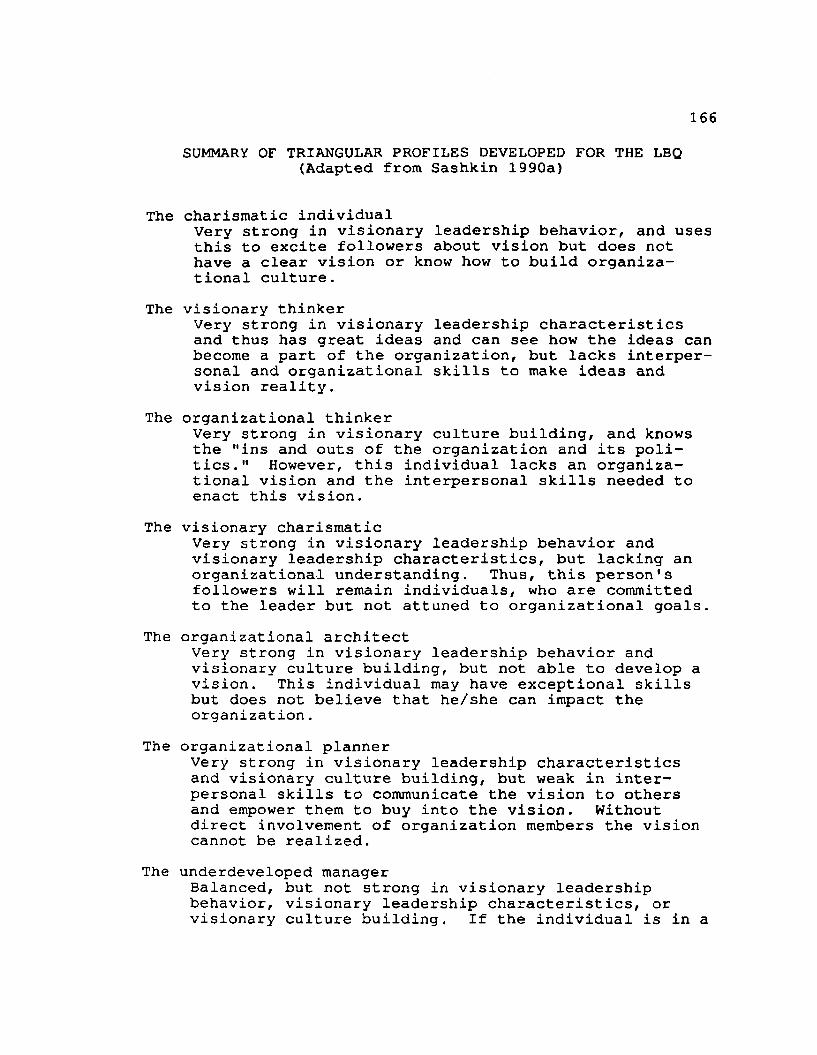
166SUMMARY OF TRIANGULAR PROFILES DEVELOPED FOR THE LBQ
(Adapted from Sashkin 1990a)
The charismatic individualVery strong in visionary leadership behavior, and uses this to excite followers about vision but does not have a clear vision or know how to build organizational culture.
The visionary thinkerVery strong in visionary leadership characteristics and thus has great ideas and can see how the ideas can become a part of the organization, but lacks interpersonal and organizational skills to make ideas and vision reality.
The organizational thinkerVery strong in visionary culture building, and knows the "ins and outs of the organization and its politics." However, this individual lacks an organizational vision and the interpersonal skills needed to enact this vision.
The visionary charismaticVery strong in visionary leadership behavior and visionary leadership characteristics, but lacking an organizational understanding. Thus, this person's followers will remain individuals, who are committed to the leader but not attuned to organizational goals.
The organizational architectVery strong in visionary leadership behavior and visionary culture building, but not able to develop a vision. This individual may have exceptional skills but does not believe that he/she can impact the organization.
The organizational plannerVery strong in visionary leadership characteristics and visionary culture building, but weak in interpersonal skills to communicate the vision to others and empower them to buy into the vision. Without direct involvement of organization members the vision cannot be realized.
The underdeveloped managerBalanced, but not strong in visionary leadership behavior, visionary leadership characteristics, or visionary culture building. If the individual is in a
167leadership position, the person should consider leadership development planning.
The aspiring leaderBalanced, and average in visionary leadership behavior, visionary leadership characteristics, and visionary culture building. This individual is in an excellent position for leadership growth and development, and quite likely to have sound management skills. Personal awareness of how leadership is different from management is suggested as a first step.
The self-actualizing leaderThe ideal profile with high scores in visionary leadership behavior, visionary leadership characteristics, and visionary culture building. Few people have this profile. Self-actualizing leaders are strong evidence of effective leadership and have been found to have employees with a high quality of work life and high productivity and bottom-line outcomes.
APPENDIX B
LEADERSHIP CHARACTERISTICS AND ACTIVITIES OF CLINICAL NUTRITION MANAGERS SURVEY
168
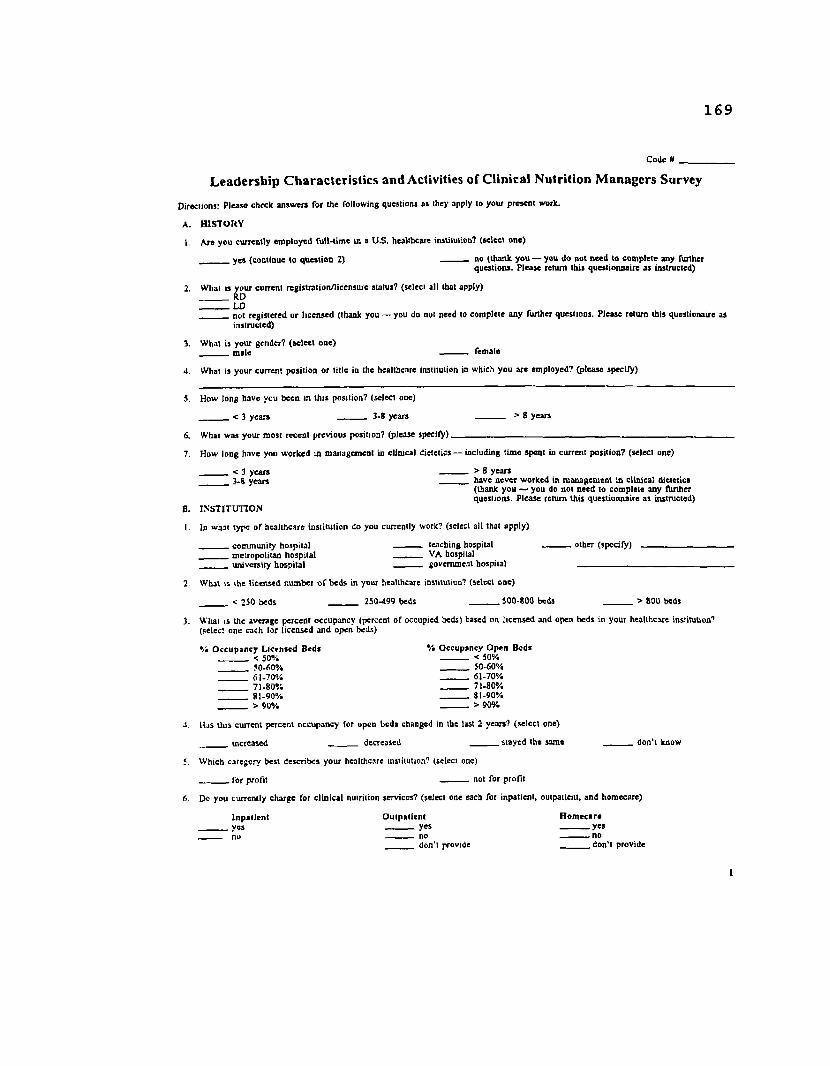
169
Code # ___________
Leadership Characteristics and Activities of Clinical Nutrition Managers Survey
Directions: P lease cheek answ ers for Ihe following queslions as they apply 10 your p resent work.
A . H IS T O R Y
1. A re you currently em ployed fu ll-tim e in a U.S. healthcare institution? (select one)
_______ y es (continue lo question 2) _______ no (thank you — you do not need to com plete any furtherquestions. P lease return this questionnaire as instructed)
2. W hat is your current reg istration/licensure status? (select all that apply) RD L D_______ not registered o r licensed (thank you — you do not need lo com plete any (Urther questions. P lease return this questionatre as
instructed)
3. W hat is you r gcndet7 (se lec t one)_______ m ale ----------- female
4. W hat is your current position o r title in the healthcare institution in which you are em ployed? (p lease specify)
5. How long have you been in th is position? (select one)
_< 3 years _______ 3-8 years _______ > 8 years
S. W hat w as your m ost recent prev ious position? (please sp ec ity )__________________ ■
7. How long have you w orked in m anagem ent in clinical dietetics — including tim e spent in current position? (select one)
< 3 years_________________________________________________ > 8 years 3.8 yea rs _______ have never w orked in m anagem ent in clin ical dietetics
(thank you —■ you do not need to com plete any furtherquestions. P lease return th is questionnaire a s instructed)8. IN S T IT U T IO N
I. In w hat type o f healthcare institu tion do you currently work? (select all that apply)
_______ com m unity hospita l --------- - teaching hospital o ther (specify)_______ m etropolitan hospita l _______ VA hospital university hosp ita l governm ent hospital ______________
W hat is the licensed num ber o f beds in your healthcare institution? (select one)
< 250 beds____________ _______ 250-499 beds____________________ $00-800 beds _______ > 800 beds
W hat is the average percent occupancy (percent o f occupied beds) based on licensed and open beds in your healthcare institution? (select one each for licensed and open beds)
*/• O ccu p an cy L icensed B eds V* O ccupancy O pen B eds < 50% _______ < 50%_______ 50-60% 50-60%_______ 61-70% 61-70%_______ 71-80% _______ 71-80%_______ 81-90% _______ 81-90% > 90% _______ > 90%
Has th is current percent occupancy for upcn beds changed in the last 2 years? (select one)
_______ increased_______________ _______ decreased _______ stayed the sam e _______ don 't know
W hich category best describes your healthcare institution? (select one)
_______ for profit _______ not for p ro fit
Do you currently charge for c lin ical nutrition services? (select one each for inpatient, outpatient, and hom ecare)
In p a t ie n t O u tp a tien t H o m ecare_______ yes yes yes_ no no no
_ _____ don‘i provide d o n 'l provide
1
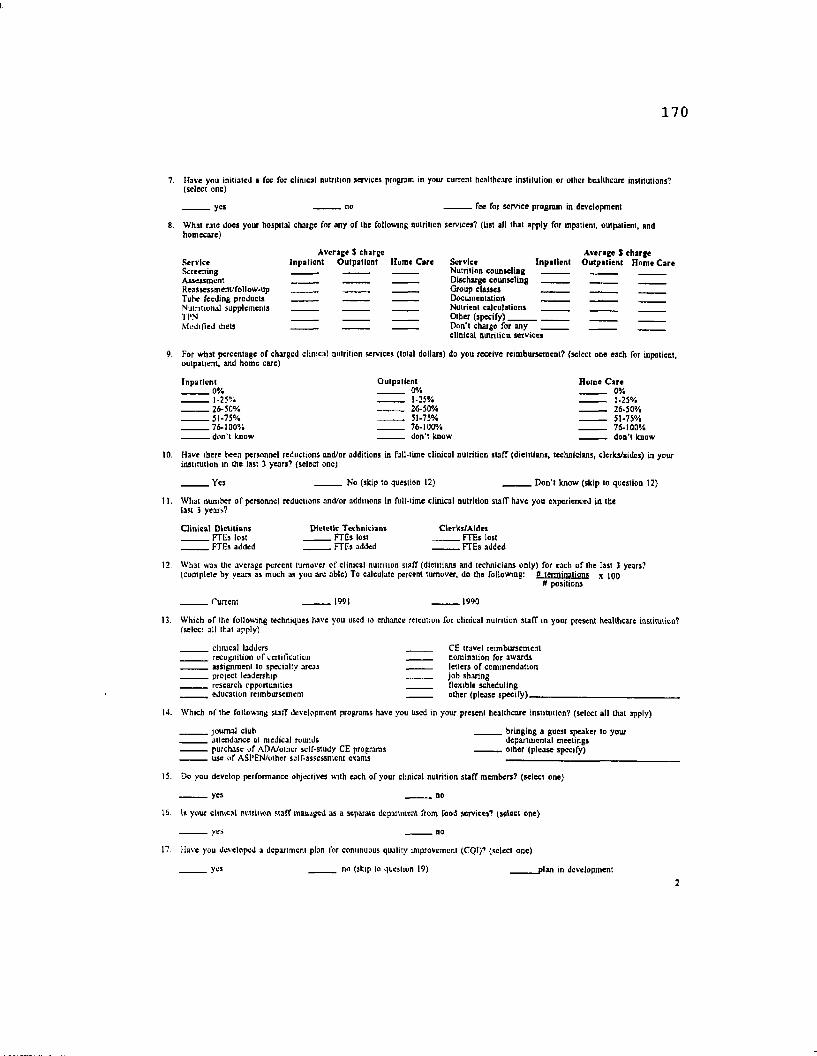
170
7. Have you initialed a fee for clinical nutrition services program in your current healthcare institution or other healthcare institutions? (select one)
yes no fee for service program in development
What rate does your hospital charge for any of the following nutriiion services? (List all that apply for inpatient, outpatient, and homecare)
Average $ charge Average $ chargeService Inpatien t O utpatient flume Care Service Inpatien t O utparient Home C areScreening » -... - ______ Nutrition counseling _______ _______Assessment — ______ Discharge counseling __________ - _______Reasiessmem/follow-up _____ __________________________ Group classes . _______Tube feeding products - — _ — Documentation - . .. .Nutritional supplements _______ _______ — Nut r i ent calculations _______TPN _______ _______ ______ Other (specify) _______ ____Modified diets_____________ _______ _______ ______ Don’t charge for any
clinical nutriiion services
For what percentage o f charged clinical nutrition services (total dollars) do you receive reimbursement? (select one each for inpatient, outpatient, and home care)
Inpatien t O utpatient Home C are 0% 0% 0% 1-25% — — - 1-25% ______ I *25% 26-50% ---------- 26-50% _______ 26*50% 51-75%_________________________________________> 51-75% 51*75% 76-100% _______ 76-100% 76-100%_______don't know _______ don't know — don’t know
Have there been personnel reductions and/or additions in full-time clinical nutrition staff (dietitians, technicians, clerks/aides) in your institution in the last 3 years? (select one)
Yes No (skip to question 12) D on 't know (skip to questioo 12)
11. What number of personnel reductions and/or additions in full-time clinical nutrition staff have you experienced in thelast 3 years?
C linical D ietitians Dietetic Technicians Clerks/Aldcs FTEs lost FTEs lost FTEs lost
... FTEs added - FTEs added_____________________FTEs added
12. What was the average percent turnover o f clinical nutriiion staff (dietitians and technicians only) for each o f the last 3 years?(complete by years as much as you are able) To calculate percent turnover, do the following: V terminations x jqq
n positions
_ Current 1991 r 1990
Which of the following techniques have you used to enhance retention for clinical nutrition staff in your present healthcare institution? (select all that apply)
clinical ladJers__________________________________ _CE travel reimbursement recognition o f certification_______________________ ______ nomination for awards assignment lo specialty areas_____________________ ______ letters of commendation project leadership______________________________________ job sharing research opportunities__________________________________ flexible scheduling
education reim bursem ent___________________________ _______ o ther /p lease sp e c ify )___
14. Which of the following stafT development programs have you used in your present healthcare institution? (select all that apply)
journal club _______bringing a guest speaker to your_______attendance at medical rounds departmental meetings purchase o f ADA/othcr self-study CE programs other (please specify) use o f ASPEN/othcr self-assessment exams_________________________________________________________ ____
15. Do you develop performance objectives with each o f your clinical nutrition stafT members? (select one)
yes no
16. h your clinical nutrition staff managed as a separate department from food services? (select one)
_______yes no
1? Have you developed a deportment plan lor continuous quality improvement (CQI)? (select one)
yes no (skip to question 19) plan in development
171
18. W hich o f the following have you devclopud for use in clinical nutrition CQ1? (select all that apply)
membership on interdisciplinary committees criteria for indicators scope o f patient care _______thresholds
. important aspects o f patient care — . data collection or monitoring toots
. quality indicators other (please speeifyi
19. Which o f the following management programs have you implemented in clinical dietetic practice in your facility? (select all thatapply)
productivity study _______programmable calculators for clinical staff use_______staffing study _ departmental strategic plao acuity level m easures for patient care _______ other (please specify)________________________ ____________ personal computers for clinical staff use ~
20. How do you market clinical nutrition services within your facility? (select all that apply)
regular updates with administration internal publications or presentations regular updates with medical staff external publications or presentations regular updates with nursing staff _______media relations regular updates with others (please specify) community outreach (including health fairs) patient surveys _______other (please sp ec ify )_______________________ other surveys (please specify )__________________ ,
21. What is the size o f the budget that you currently control? (select one)
. Don’t control budget S1Q0,00G - 300,000 5700,001 - 1,000,000
. < 5100,000 5300,001 - 700,000 - > 51,000,000
22. Do you believe that The position o f clinical nutrition manager will exist in your institution in the future? (select one)
Yes, this position w ill exist for > 10 years Yes, this position w ill exist for 5 - 10 years Yes, this position will exist for 1-4 years No, this position will be eliminated in < 1 year D on't know
23. How will (he position o f clinical nutrition manager possibly change in the future? (select one)
will be upgraded will be downgraded will remain the same don’t know
24 How docs your direct supervisor value clinical nutrition services? (circle the triangle on the following rating scale)not at all valuable very valuableA_____________ <A_____________ £ ______________ /\______________£ _______________ A_________________
C. EXPERIEN CE
1. What wos your rouie lo registration? (select one)
CUP _______AP4-trainccship___________,______ other (specify)______________________________________________internship _______MS'experience „ not registered
What is the highest academic degree you have earned or are working toward? (select one)
BS Doctorate in progress (specify a re a ) . Masters in progress (specify area)----------------------------- Doctorate (specify a re a )__---------- Masters (specify a re a ) -------------------------------------- Other (specify_area)________________
V How- long have you been practicing in dietetics? (select one)
< I year ------------1-5 years 6-10 years ---------- , 11-15 years ------------16-20 years > 20 years
4 What number o f promotions (by position) have you received in the field o f dietetics? (select one)
0 ---------- 1-2-------------------------------- ---------- 3-5 > 5
5. What is your current annual salary range (select one)
< 520.000/ycar ______ 530,001-40,000/year_________________ _______ 550,001-60,000/year S20,000-30,000/year ______ S40.00I-50,000/year _______ > 60,000/year
3
172
D. SU PERV ISO R Y RESPO N SIBILITIES
I. What is the size o f the FTE clinical nutrition staff (dietitians, technicians, clerks/aides, excluding student/interns) in your institution? (select one)
. 1-5 FTEs 11-15 FTEs _______ 21-25 FTEs
.6 -1 0 FTEs 16-20 FTEs _______ > 25 FTEs
2. How many FTE employees do you directly supervise? (complete the num ber Tor all that apply)
dietitians_________________ technicians clerks/aides other (specify ).
3. How many studenis/iniems do you personally supervise/direct annually? (select one)
0 students (skip to question 5) _______ 1-3 students 4-8 students > 8 students
4. In what type o f education programs are these students enrolled? (select all that apply)
technician________________ _______ intern other health professionals (specify )__________ _________CUP_____________________________graduate other (soecifvt AP4-trainecship
What items o f responsibility/control do you have in your cunont position? (select all that apply)
budget__________________________________ _______ capital expenditures_______________ _______ revenue generation product selection________________________ _______flexible time allocation___________________ other (specify)_____------------ personnel admin, (hiring and appraisal)-----------------------------------------------------------------------------------------
6. W ho is your direct supervisor? (please specify).
E. EDU CATION A L A C TIV ITIES (Outside o f routine work assignments)
1. What is the average number o f presentations/poster sessions you make per year to health professionals? (select one per category)
local/regional itate/national 0 0 1-2 1 -2 3-5 3-5 > 5 _______ > 5
2. W hat is the average number o f presentations you make per year to the public? (select one per category)
lucaRrcglnnal slate/national radio/TV appearances 0 0 0 1-2 1-2 1-2 3-5 ---------- 3-5 3-5 > 5 ---------- > 5 > 5
F p u b l i c a t i o n s
1 What is the total number o f publications you have authored/co-authoreo for professionals in your career? (select one per category)
articles abstractsfhonk reviews book chap ters hooks 0 ___ D____________ ___ 0__________ ___ 0 1-2 ]■: 1-2 1-2 3-5 _______ 3-5_______________________ _______ 3-5___________________________ 3-5 6-8 6-8 6-8 6-8________> 8 ________ >8__________________________________ > 8 _____________________ ________> g
2 What is the total number o f publications you have authored/co-authored for the public in your career? (select one per category)
articles brochures/m onographs book chap ters books 0 0 0 0 1-2 1-2 1-2 1-2 3-5 _______ 3-5_______________________ _______ 3-5___________________ _______ 3-5 6-8 6-8 6-8 6-8 >8 > 8 > 8 >8
G RESEARCH
I What is the total number o f approved research proposals you have authorcd'co-authorcd in your career? (select one)
0 1-2 3-5 6-8 > 8
4
173
2. What is the total number o f research studies you have managed/supported in your career? (select one)
0 _______ 1-2 3-5 6-8 > 8H. a r e a s o f p r o f e s s i o n a l i n v o l v e m e n t /s p e c i a l i z a t i o n
I. Do you have any certification and/or advanced practice credentials (exclude RD, LD, and academic degrees)? (Select all that apply)
CDE CNSD other (sp ec ify )__________________________________________________________________________________________________ _ none
2, W hat memberships do you hold in practice groups o f The American Dietetic Association other than membership in the Clinical N utrition Management Practice Group? (list all that apply)
I, M EN TO RIN G
1. Do you currently have a menior(s) for professional development?
ves
I f yes. please specify your association with the individuals) (e.g. academic, career advancement, etc.)
2. Do you currently serve as a mentor for other's professional development?
yes no
If yes, please specify your association with the individual(s)
J. LEAD ERSH IP
1. How many appointed/elected offices in professional organizations have you held in your career? (select one per category)
local/regional state/natjonal 0 0 1-2 1-2 3-5 3-5 6-8 6-8 >8 >8
2. How many different professional development programs (including workshops/seminars lasting I day or longer have you attended in the last / ’years? (select one)
n 1-2 3-5 6-8 > g
3. What is ynur routine work involvement with leadership related activities? (select all that apply)
participation in unit rounds _______ conducting quality improvement activities_______leading departmcnVstalT meetings _______ initiating major projects giving modicat/dietctic lectures _______ other (sp ec ify )__________________________ representing the department to the insiitution
4 What personal characteristics and/or traits do you believe are important for leadership in clinical dietetics? (List all that apply)
5. What personal behaviors an d u r actions do you believe are important for leaders in clinical dietetics to display? (List all that apply)
6 How do you believe leaders in clinical dietetics should relate to or interface with institutional goals? (List all that apply)
5
174
7, Leadership earl be defined in a number o f ways. One such definition describes transactional and transformational leadership as follows:
Transactional leaders operate within the framework o f an existing organisational culture, identifying present subordinate wants/needs and exchanging things lhai satisfy those needs when subordinates work toward a goal or outcome desired by the leader.
Transformational leaders seek to alter the organizational culture to change the make-up o f subordinate's wants and needs, developing avision o r whal can be, communicating this vision to others and inspiring them to achieve the vision.
Based on these descriptions, how would you describe your current overall leadership style in your organization’’ (Circle Ihe triangle on the following scale, where the far left - 100% transactional and Ihe far right » 100% transformational)
T ransactional leadership T ran sfo rm a tio n a l leadership
A________A_______ A________ A________ A_________A__________A£. Would you be billing to participate, in the next 2 months, in a survey o f leadership practices o f clinical nutrition managers, and
recruit 3 o f your direct-report staff (dietitians and technicians only) to participate also?
yes no
THANK YOU!!!
Please return this survey in ihe enclosed, postage-paid, self-addressed envelope by SEPTEMBER 30TH to:
Mary Beth Follz, MS, RD Medical Dietetics Department 1583 Perry Street The Ohio State University Columbus, OH 43210
6
APPENDIX C
LEADERSHIP CHARACTERISTICS AND ACTIVITIES OF CLINICAL NUTRITION MANAGERS EMPLOYEE SURVEY
175
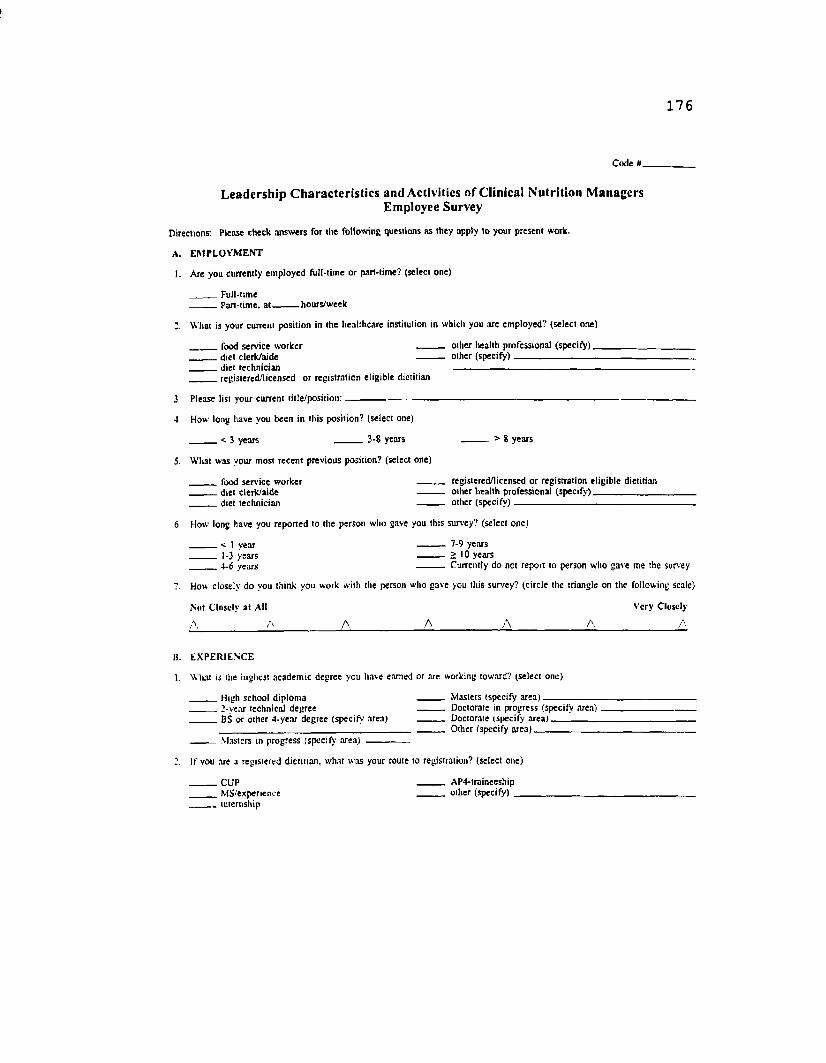
176
C ode
Leadership Characteristics and Activities of Clinical Nutrition Managers Employee Survey
D irections: P lease check an sw ers fo r th e fo llow ing questions a s they app ly lo you r p resen t w ork.
A. E M P L O Y M E N T
I. A re you cu rren tly em p loyed fu ll-tim e o r part-tim e? (select one)
F ull-tim e— P art-tim e, a t hou rs /w eek
W hat is your curren t po sitio n in Ihe hea lthca re institu tion in w hich you are em p lo y ed ? (se lec t one)
food serv ice w orker o ther health pro fessional ( s p e c ify ) d ie t c le rk /a ide o ther ( s p e c i fy ) ---------------------------------- d ie t techn ic ian --------------------------------------------------------- reg istered /licensed o r reg istra tion e lig ib le d ie titian
3 P lease list you r cu rren t ti t le /p o s it io n :--------------------------------------------------------------------------------------------------------------------------
4. H ow long h ave you been in th is position? (select one)
< 3 years 3-8 years > 8 y ea rs
5. W hat w as your m ost rece n t p rev ious p o sition? (select one)
food serv ice w o rk er _______ reg istered /licensed o r reg istra tion e lig ib le d ie titian d ie t c le rk /a ide ---------------------------------------------------- ----------- o ther hea lth p ro fessional (s p e c ify )_________________
. d ie t techn ic ian o the r ( s p e c i fy ) .
6 H ow long have you rep o rted to the person w ho gave you th is survey? (select one)
< 1 y ea r ----------- 7-9 years 1-3 yea rs ---------- i 10 years 4-6 years _______ C urren tly do not report to person w ho g ave m e the survey
7. How close ly do you th ink you w ork w ith the person w ho g ave you th is survey? (c irc le the triang le on the fo llow ing scale)
N ut C losely a t A ll V e ry C losely
A_____________________ A________A______________A _______________A________________ A
B. E X P E R IE N C E
1. W hat is the h ighest ac ad em ic d eg ree you h ave earned o r are w orking tow ard? (se lec t one)
H igh schoo l d ip lo m a M asters (specify a r e a ) ------------------------------------------------------- „ 3-vear techn ica l d eg ree D octorate in progress (specify a r e a ) _______________________ BS o r o th e r 4 -year deg ree (sp ec ify area) _______ D octorate (specify a r e a ) ____________________________________
_______________ O ther (specify a r e a ) _________________________________________M asters in p rogress (specify area )
I f vou are a reg istered d ie titian , w hat w as yo u r rou te to reg istration? (select one)
C U P _______ A P4-traineeship M S/experience _______ o th e r (specify) ___ in ternship
APPENDIX D
LETTERS AND INSTRUCTIONS FOR CLINICAL NUTRITION MANAGERS AND EMPLOYEE EVALUATORS
177
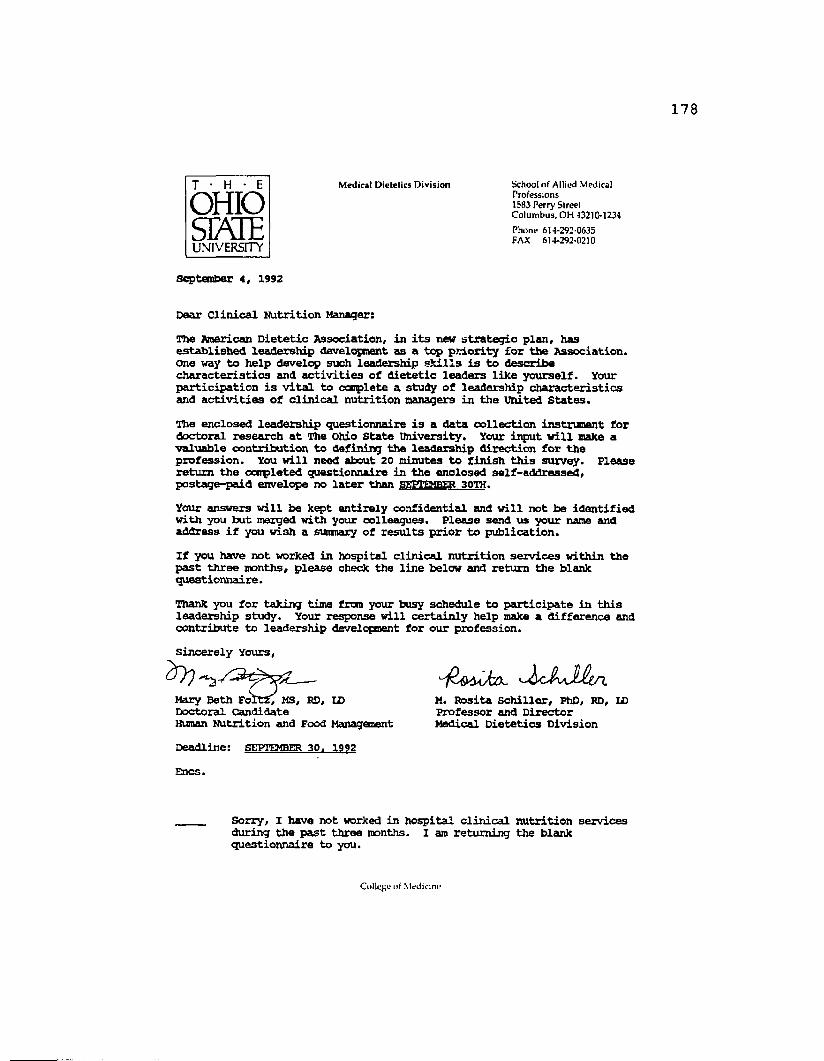
T • H • E M ed ic a l D ie te tics D iv is io n School o f A llied M edical P ro fessions 1583 P erry S tree t C o lu m b u s , O H 43210-1234OHIO
SPvIE P h o n e 614-292-0635 FAX 614-292-0210UNIVERSITY
September 4, 1992
Dear Clinical Nutrition Manager:
The American Dietetic Association, in its new strategic plan, has established leadership development as a top priority for the Association. One way to help develop such leadership shills is to describe characteristics and activities of dietetic leaders like yourself. Your participation is vital to complete a study of leadership characteristics and activities of clinical nutrition managers in the united States.
The enclosed leadership questionnaire is a data collection instrument for doctoral research at The Ohio State University. Your input will make a valuable contribution to defining the leadership direction for the profession. You will need about 20 minutes to finish this survey. Please return the completed questionnaire in the enclosed self-addressed, postage-paid envelope no later than SEPTEMBER 30TH.
Your answers will be kept entirely confidential and will not be identified with you hut merged with your colleagues. Please send us your name and address if you wish a sumnary of results prior to publication.
If you have not worked in hospital clinical nutrition services within the past three months, please check the line below and return the blank questionnaire.
Thank you for taking time fran your busy schedule to participate in this leadership study. Your response will certainly help make a difference and contribute to leadership development for our profession.sincerely Yours,
M. Rosita Schiller, PhD, RD, ID Professor and Director Medical Dietetics Division
Doctoral CandidateHuman Nutrition and Food ManaganentDeadline: SEPTEMBER 30. 1992Encs
Sorry, I have not worked in hospital clinical nutrition services during the past three months. I am returning the blank questionnaire to you.
C ollege of SledidrL*
179
T • H • E M ed ica l D ie te tic s D iv is io n School o f A llied M edical P ro fessions 1583 P erry S tree t C o lu m b u s, O H 43210-1234
OHIOSME P hone 614-292-0635 FAX 614-292-0210UNIVERSITY
September 21, 1992
Dear Clinical Nutrition Manager:A few weeks ago you received a questionnaire about leadership characteristics and activities of clinical nutrition managers. This study is critical to the development of leadership skills within our profession.As a leader, your response to this questionnaire is very important. If you have already responded to the questionnaire— THANK YOU! If you have not had time to ccnplete the questionnaire, please take a few minutes to conpleta it. A second copy of the questionnaire is enclosed for your convenience. Please return your ocnpleted questionnaire in the enclosed self-addressed, postage-paid envelope by SEPTEMBER 30TH.Again, let me assure you that your responses will not be identified with you but will be combined with those of your colleagues. Please send us your name and address if you wish a summary of results prior to publication.if you have not worked in hospital clinical nutrition services within the past three months, check the line belcw and return the blank questionnaire.Your participation in this dissertation research is essential so that valid results can be drawn from the data. We again thank you for your help as a leader in our profession.Sincerely Yours,
Sorry, I have not worked in hospital clinical nutrition services during the past three months. I am returning the blank questionnaire to you.
M. Rosita Schiller, PhD, RD, ID Professor and Director Medical Dietetics Division
Doctoral CandidateHuman Nutrition and Food Managem entDeadline: SEPTEMBER 30. 1992Encs
C ollege o l M edicine
T • H • E M e d ic a l D ie te t ic s D iv is io n S choo l o f A llie d M ed ic a l Professions 1583 P e rry S tre e t C o lu m b u s , O H 43210*1234OHIOSEME P h o n e 614-292-0635 FAX 614-292-0210UNIVERSITY
October 14, 1992
Dear Clinical Nutrition Manager;
Thank you for agreeing to participate in our study of leadership characteristics and activities of clinical nutrition managers. As a leader you will play a valuable role in helping define effective leadership strategies for success in healthcare today and into the future.
To evaluate leadership behaviors, we are using a special Iieadership Behavior Questionnaire developed by Marshall Sashkin, PhD. This Questionnaire is to be completed by yourself and three of your direct-report subordinates— dietitians and/or dietetic technicians.
Please follow the attached instructions and return all octnpleted forms in the enclosed self-addressed, postage-paid envelope by No v e m b e r 13TH.
Information will only be reported in aggregate. If you would like a copy of these group results, please send us your name and address.
Again, thank you so much for you. help and participation in this study.Sincerely Yours,
Mary Beth Foltz, MS, RD, IDDoctoral CandidateHuman Nutrition and Food Management
M. Rosita Schiller, PhD, RD, ID Professor and Director Medical Dietetics Division
Deadline: NOVEMBER 13. 1992
Co!U’j*o o f M ed ic in e
181
LEADERSHIP CHARACTERISTICS AMD BEHAVIORS OF CLINICAL NUTRITION MANAGERS
Leadership Behavior Questionnaire Instructions
To ccnplete an accurate assessment of your leadership characteristics, it is important that we receive a profile from you and 3 dietitians and/or dietetic technicians reporting to you. Enclosed are 4 Leadership Behavior Questionnaires for the visionary leader:
1 marked SELF (printed in purple and blue)3 narked OTHER (printed in green and blue).
in addition, there are 3 copies of an introductory letter and short survey. Please ccnplete, distribute, and return these materials as follows:1. Complete the SELF Leadership Behavior Questionnaire (printed in purple
and blue) as instructed on the instrument. Please do not separate or score the form. The Questionnaire should take 15-20 minutes to ccnplete.
2. Distribute 1 copy of each of the following materials to 3 dietitians and/or dietetic technicians who directly report to you. Each of the 3 dietitians and/or dietetic technicians should receive:
1 introductory letter1 abort demographic survey (printed on green paper)1 OTHER Leadership Behavior Questionnaire (printed in green £ blue) 1 manila envelope.
Ask each subordinate to oanpleta the survey and questionnaire as truthfully as possible. Remind him/her that the results of the survey and questionnaire will be kept confidential and will not affect performance evaluations or job security. Instruct each subordinate not to separate or score the surveys or questionnaires.Ask each subordinate to place the completed survey and questionnaire (subordinates should not have separated or scored the forms) in the envelope provided. Have him/her seal the envelope before returning it to you.Please collect the sealed envelopes from each subordinate within one week after you distributed the questionnaires and surveys. Thank each subordinate for his/her participation.
3. Place the following in the enclosed self-addressed, postage-paid envelope:
Your oanpletad leadership Behavior Questionnaire (return the entire instrument— do not separata or score the form)3 sealed envelopes frcm your subordinates.
4. Please return all instruments by NPTOtBER 13TH to:Mary Beth Foltz, MS, RD Medical Dietetics Department 1583 Ferry Street The Ohio State University Columbus, OH 43210THANK YOU again for your participation in this important research!!
182
BEQUEST FOR RELEASE OF INDIVIDUAL LEADERSHIP BEHAVIOR QUESTIONNAIRE RESULTS
Data for this study of leadership characteristics and activities of clinical nutrition managers will be reported only in aggregate. If you would like a copy of these group results when they are published, please send me your name and address.It is possible for you to receive the soores fran your individual Leadership Behavior Questionnaire (IBQ) and guidelines to interpret than. However, to release these data, confidentiality cannot be maintained, if you wish to receive the soores Iron your Individual ISQ, you must sign, date, and return this letter with the enclosed survey. Results cannot be released until this research study has been oonpleted. Therefore, your individual results will not be mailed until about one year from this date.
I, _______________________ , request that individual Leadership Behavior[Name]
Questionnaire soores as rated by myself be provided to me. I understand that by making this request, I release the investigators fran their obligation to maintain the confidentiality of my LBQ soores.
[Signature] [Date]
NameAddressCity State Zip
183
UNIVERSITY
M edical D ietetics D ivision School of A llied M edicalProfessions 1383 Perry Street C olum bus, O H -I32HM234
Phone 614-292-0635 FAX 614-292-0210
October 14, 1992
Dear Biployee,Your supervisor is participating in a study on leadership in dietetics.To provide a reliable reflection of his/her work within your institution, we need your help.Please complete, as accurately as possible, the enclosed questionnaire which asks you questions about certain qualities and characteristics of your supervisor, please also ccnplete the green survey sheet. It should take about 20 minutes to oarplete these forms.To assure that your responses remain anonymous, please place the oonqpleted questionnaire and green survey in the attached envelope. Seal the envelope and return it to your supervisor within l week.We want you to know that individual responses will not be identified in any way. The results of the survey and questionnaire will be kept confidential and will not affect performance evaluations or job security.Thank you for your help in this valuable study.Sincerely Yours,
Mary Beth Poltz, MS, HD, la m. Rosita Schiller, PhD, RD, LDDoctoral Candidate Professor and DirectorHuman Nutrition and Food Management Medical Dietetics Division
Deadline: REPLY WITHIN 1 WEEK
E n c s .
C |>I \ k d U :IK'
184
November 2, 1992
Dear Clinical Nutrition Manager:Thank you for agreeing to participate in a study an leadership characteristics of clinical nutrition managers. A few weeks ago, you received a special mailing with leadership evaluation instruments. To ensure the validity of our sample, it is very important that you and 3 of your direct-report subordinates— dietitians and/or dietetic technicians— ccnplete these questionnaires.If you have already returned your questionnaires— THANK YOT. if you hove not had time to ccnplete the questionnaires, please take a few minutes and work with your subordinates to ccnplete the questionnaires. If you did not receive the mailing or have misplaced the questionnaires, please contact me i m m e d iately at (614) 624-3065.Please return all completed questionnaires by MUVtMiEK 13TH to:
Mazy Beth Poltz, MS, RD, ID Medical Dietetics Division 1583 Perry street The Ohio State University Coltmbus, CH 43210
Thank you again for your participation in this study.sincerely Yours,
Mazy Beth Poltz, MS, RD Deadline: wnvrawEft 13. 1992Doctoral CandidateHuman Nutrition and Food Management
November 11, 1992
Dear Clinical Nutrition Manager:H u n k you for agreeing to participate In a study on leadership characteristics of clinical nutrition managers. By now, you should hove received a special mailing with leadership evaluation instruments. We need to include your data in our study to ensure our results are valid, ve hope to hear from you soon.If you have already returned your questionnaires— THANK you. If you have been unable to couplets the questionnaires, please take a few minutes and work with your subordinates to complete the questionnaires, or return them unanswered to me. If you did not receive a mailing, or have misplaced the questionnaires please contact me immediately at (614) 624-3065.Please return all completed questionnaires by November 20th to:
Mary Beth Foltz, MS, RD Medical Dietetics Division 1583 Perry street The Ohio State university OolUDbUS, OS 43210
Thank you again for taking the time to participate in this study.Sincerely Yours,
Deadline: tctemrbp 2 0. 1992Doctoral CandidateHuman Nutrition and Food Management
APPENDIX E
TABLES
186
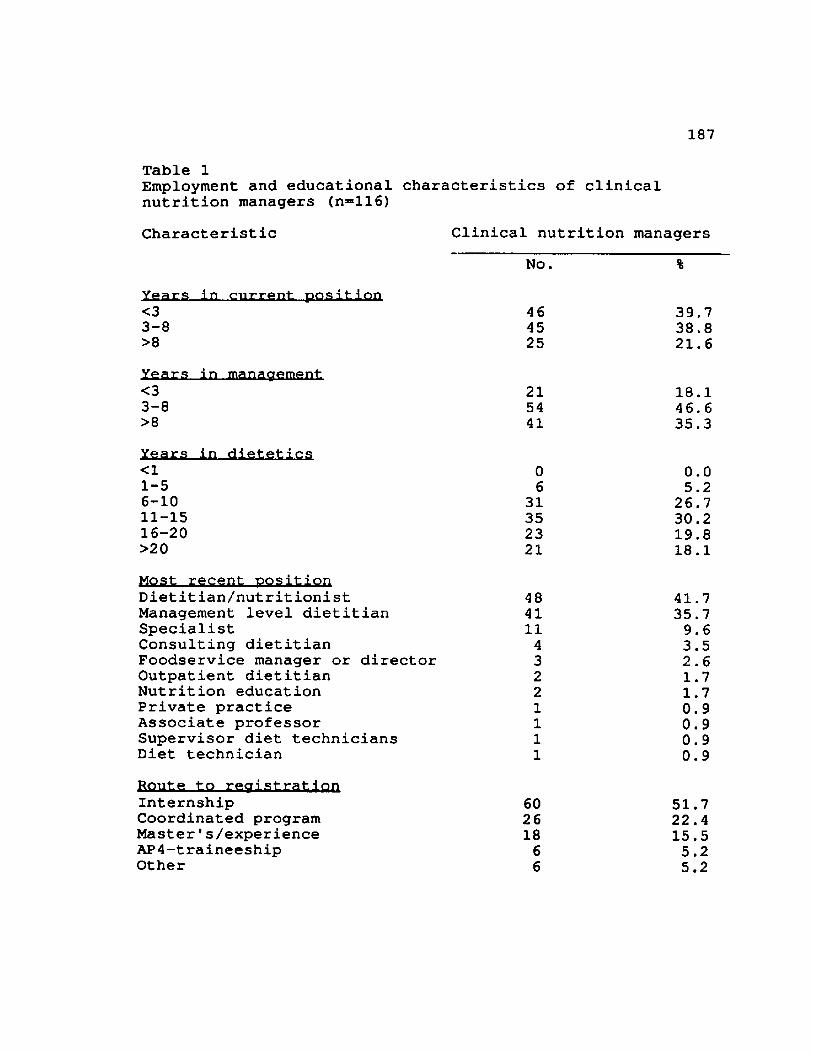
187
Table 1Employment and educational characteristics of clinical nutrition managers (n=116)Characteristic Clinical nutrition managers
No. %Years in current position<3 46 39.73-8 45 38.8>8 25 21.6Years in management<3 21 18.13-8 54 46.6>8 41 35.3Years in dietetics<1 0 0.0I-5 6 5.26-10 31 26.7II-15 35 30.216-20 23 19.8>20 21 18.1Most recent positionDietitian/nutritionist 48 41.7Management level dietitian 41 35.7Specialist 11 9.6Consulting dietitian 4 3.5Foodservice manager or director 3 2.6Outpatient dietitian 2 1.7Nutrition education 2 1.7Private practice 1 0.9Associate professor 1 0.9Supervisor diet technicians 1 0.9Diet technician 1 0.9Route to registration Internship Coordinated program Master's/experience AP4-traineeship Other
60 51.726 22.418 15.56 5.26 5.2
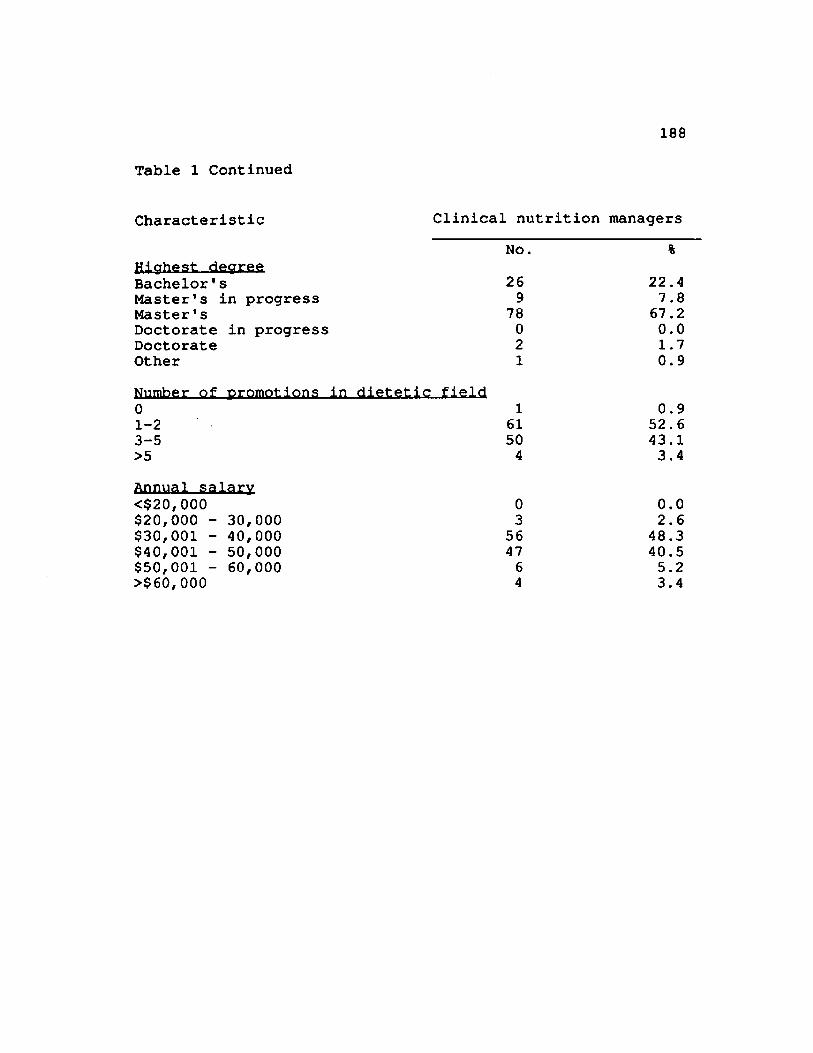
188
Table 1 Continued
Characteristic Clinical nutrition managersNo. %
Highest decreeBachelor's 26 22.4Master's in progress 9 7.8Master's 78 67.2Doctorate in progress 0 0.0Doctorate 2 1.7Other 1 0.9Number of promotions in dietetic field0 1 0.91-2 61 52.63-5 50 43.1>5 4 3.4Annual salary<$20,000 0 0.0$20,000 - 30,000 3 2.6$30,001 - 40,000 56 48.3$40,001 - 50,000 47 40.5$50,001 - 60,000 6 5.2>$60,000 4 3.4
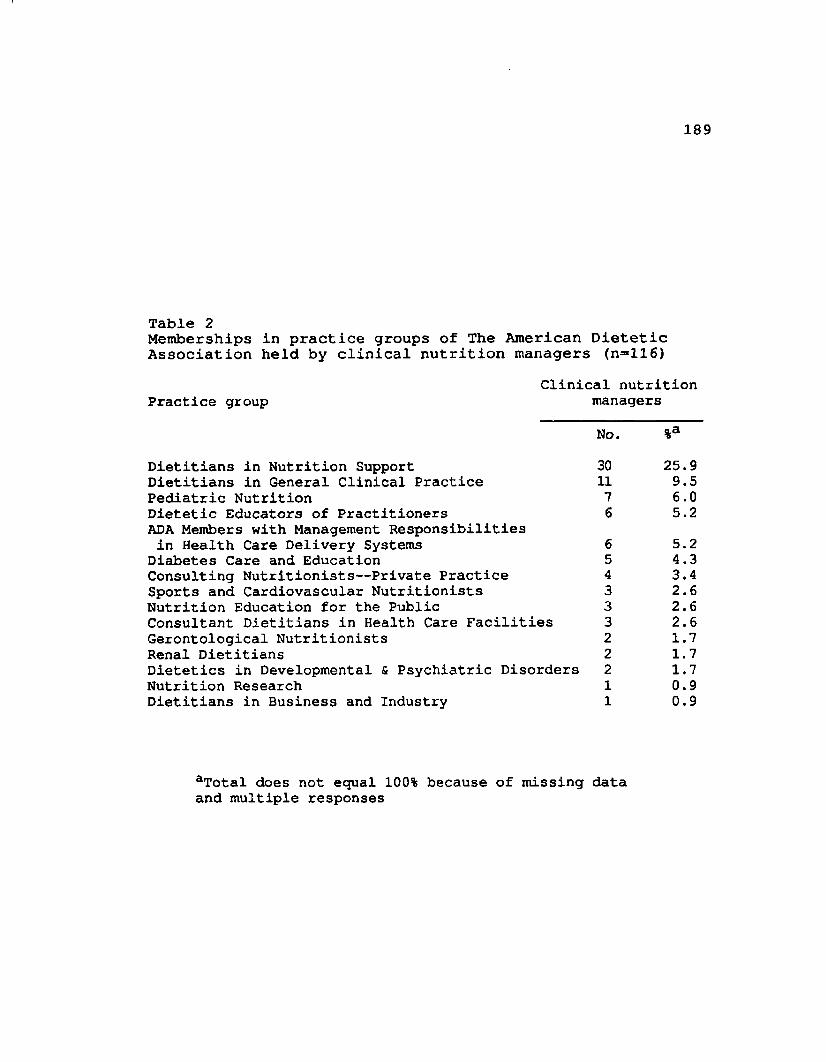
189
Table 2Memberships in practice groups of The American Dietetic Association held by clinical nutrition managers (n=ll6)
Clinical nutrition Practice group managers
No. %aDietitians in Nutrition Support 30 25.9Dietitians in General Clinical Practice 11 9.5Pediatric Nutrition 7 6.0Dietetic Educators of PractitionersADA Members with Management Responsibilities
6 5.2in Health Care Delivery Systems 6 5.2
Diabetes Care and Education 5 4.3Consulting Nutritionists— Private Practice 4 3.4Sports and Cardiovascular Nutritionists 3 2.6Nutrition Education for the Public 3 2.6Consultant Dietitians in Health Care Facilities 3 2.6Gerontological Nutritionists 2 1.7Renal Dietitians 2 1.7Dietetics in Developmental & Psychiatric Disorders 2 1.7Nutrition Research 1 0.9Dietitians in Business and Industry 1 0.9
aTotal does not equal 100% because of missing data and multiple responses
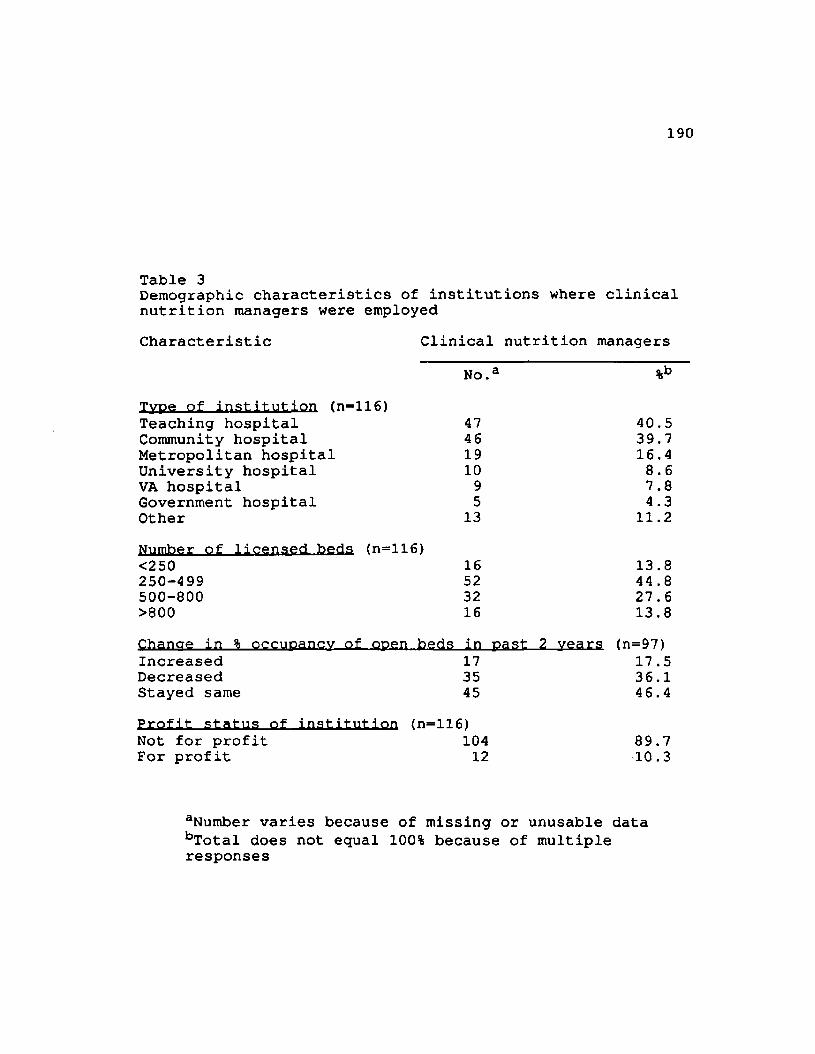
190
Table 3Demographic characteristics of institutions where clinical nutrition managers were employedCharacteristic Clinical nutrition managers
No.a %bType of institution (n=116)Teaching hospital 47 40.5Community hospital 46 39.7Metropolitan hospital 19 16.4University hospital 10 8.6VA hospital 9 7.8Government hospital 5 4.3Other 13 11.2Number of licensei beds. (n=116)<250 16 13.8250-499 52 44 .8500-800 32 27.6>800 16 13.8Chancre in % occuDancv of ooen.beds in past 2 vears (n=97)Increased 17 17.5Decreased 35 36.1Stayed same 45 46.4Profit status of institution <n=116>Not for profit 104 89.7For profit 12 10.3
aNumber varies because of missing or unusable data bTotal does not equal 100% because of multiple responses
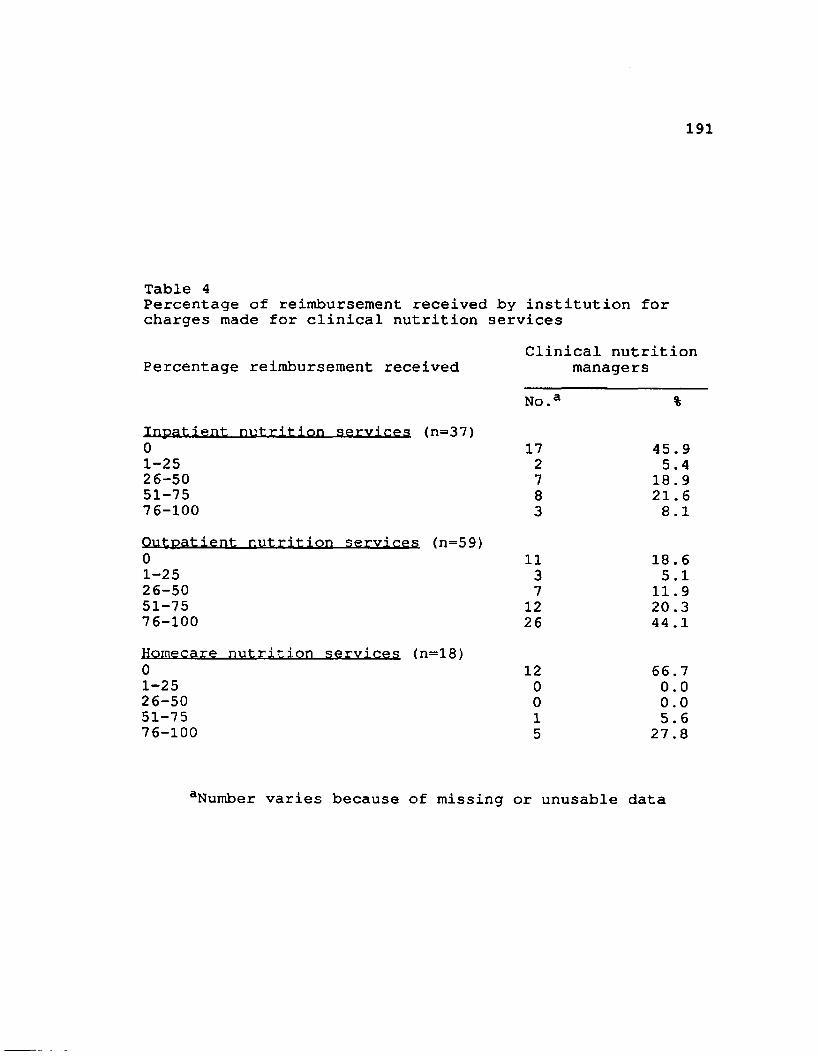
191
Table 4Percentage of reimbursement received by institution for charges made for clinical nutrition services
Clinical nutrition Percentage reimbursement received managers
No.a %Inpatient nutrition services <n=37)0 17 45.91-25 2 5.426-50 7 18.951-75 8 21.676-100 3 8.1Outpatient nutrition services (n=59)0 11 18.61-25 3 5.126-50 7 11.951-75 12 20.376-100 26 44.1Homecare nutrition services (n=18)0 12 66.71-25 0 0.026-50 0 0.051-75 1 5.676-100 5 27.8
aNumber varies because of missing or unusable data
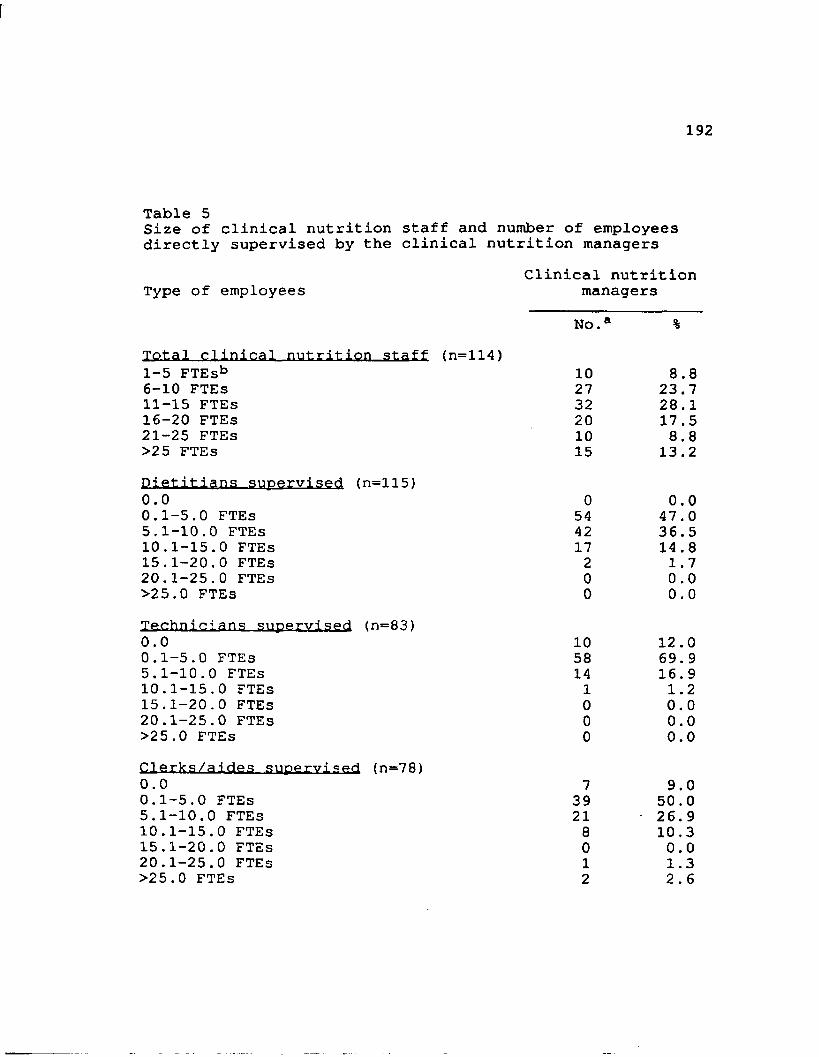
192
Table 5Size of clinical nutrition staff and number of employees directly supervised by the clinical nutrition managers
Clinical nutrition Type of employees managers
N o . %Total clinical nutrition staff (n=114)I-5 FTEsb 10 8.86-10 FTEs 27 23.7II-15 FTEs 32 28.116-20 FTEs 20 17.521-25 FTEs 10 8.8>25 FTEs 15 13.2Dietitians supervised (n=115)0.0 0 0.00.1-5.0 FTEs 54 47.05.1-10.0 FTEs 42 36.510.1-15.0 FTEs 17 14.815.1-20.0 FTEs 2 1.720.1-25.0 FTEs 0 0.0>25.0 FTEs 0 0.0Technicians supervised (n=83)0.0 10 12.00.1-5.0 FTEs 58 69.95.1-10.0 FTEs 14 16.910.1-15.0 FTEs 1 1.215.1-20.0 FTEs 0 0.020.1-25.0 FTEs 0 0.0>25.0 FTEs 0 0.0Clerks/aides supervised (n=78)0.0 7 9.00.1-5.0 FTEs 39 50.05.1-10.0 FTEs 21 26.910.1-15.0 FTEs 8 10.315.1-20.0 FTEs 0 0.020.1-25.0 FTEs 1 1.3>25.0 FTEs 2 2.6
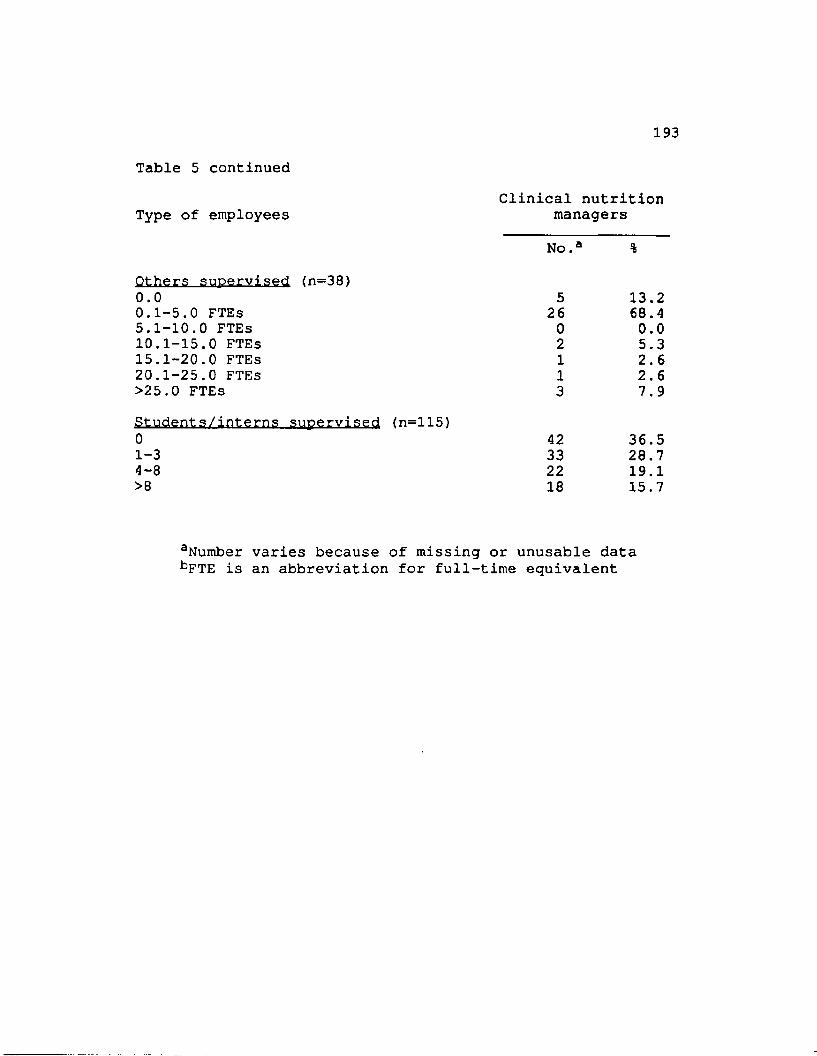
193Table 5 continued
Clinical nutrition Type of employees managers
No.a %Others supervised (n=38)0.0 5 13.20.1-5.0 FTEs 2 6 68.45.1-10.0 FTEs 0 0.010.1-15.0 FTEs 2 5.315.1-20.0 FTEs 1 2.620.1-25.0 FTEs 1 2.6>25.0 FTEs 3 7.9Students/interns supervised (n=115)0 42 36.51-3 33 28.74-8 22 19.1>8 18 15.7
aNumber varies because of missing or unusable data bFTE is an abbreviation for full-time equivalent
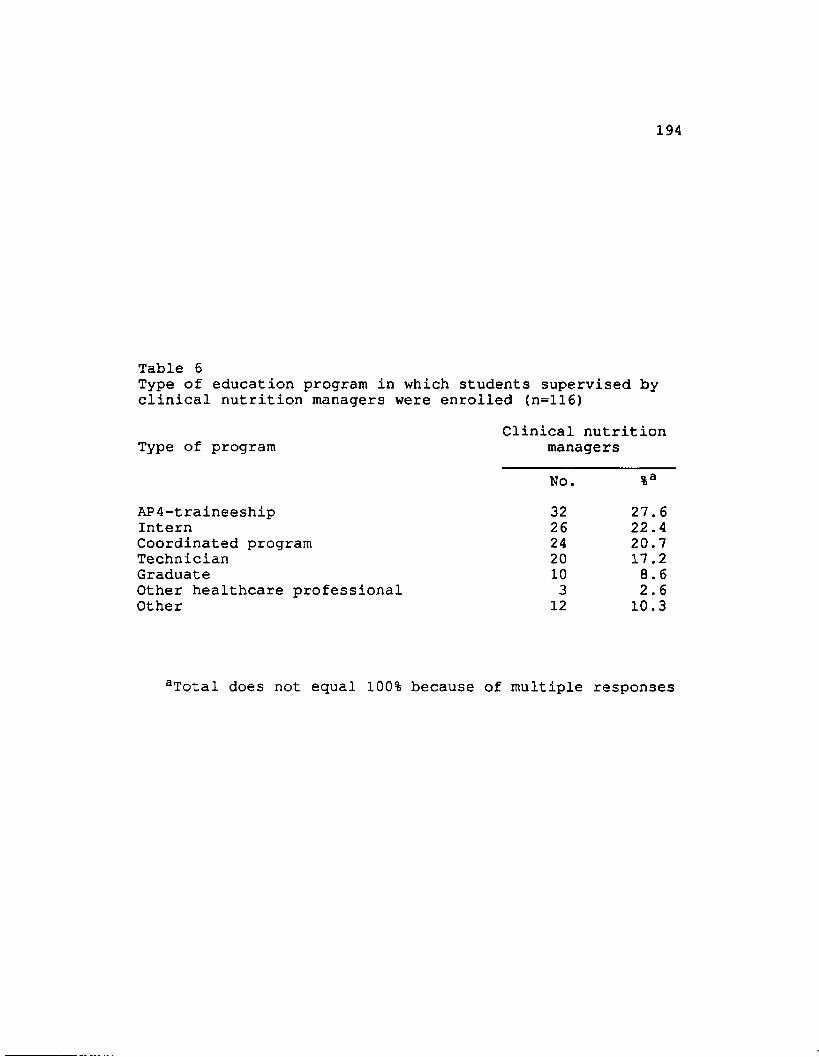
194
Table 6Type of education program in which students supervised by clinical nutrition managers were enrolled (n=116)
Clinical nutrition Type of program managers
No. %aAP4-traineeship 32 27.6Intern 26 22.4Coordinated program 24 20.7Technician 20 17.2Graduate 10 8.6Other healthcare professional 3 2.6Other 12 10.3
aTotal does not equal 100% because of multiple responses
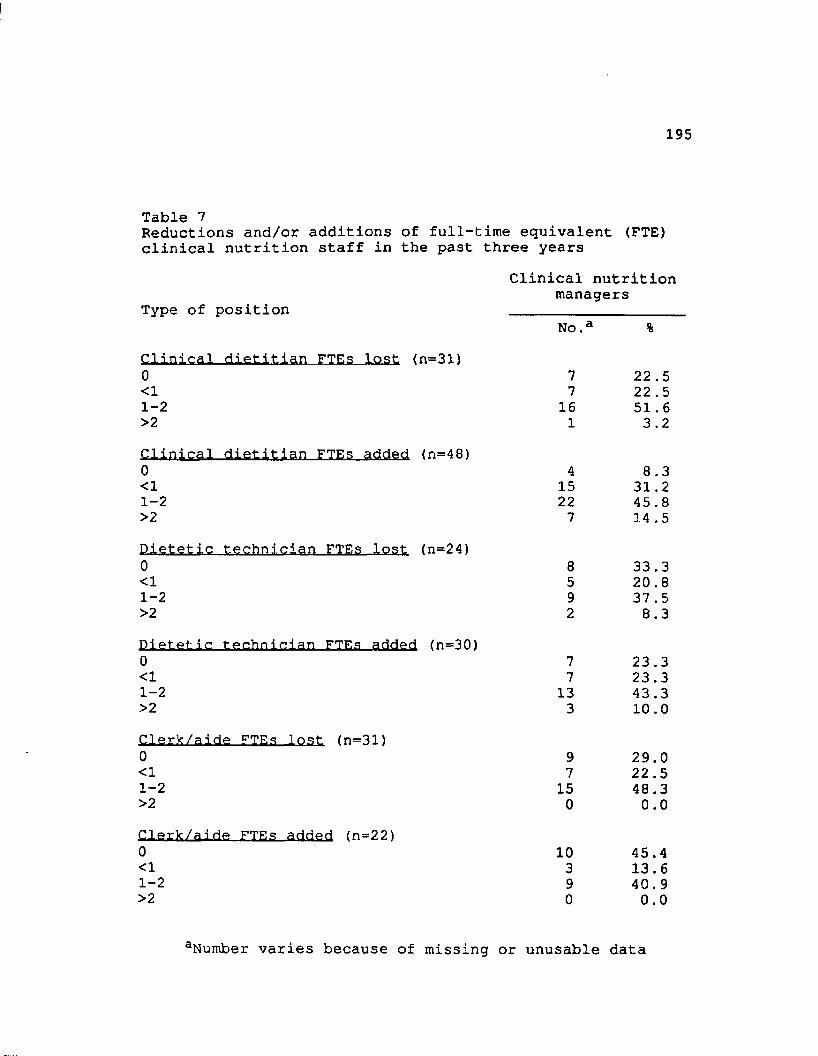
195
Table 7Reductions and/or additions of full-time equivalent (FTE) clinical nutrition staff in the past three years
Clinical nutrition managers
Type of position ___________________No.a %
Clinical dietitian FTEs lost (n=31)0<11-2>2Clinical dietitian FTEs added (n=48>
77
161
22 .5 22 .5 51.6 3.2
0 4 8.3<1 15 31.21-2 22 45 .8>2 7 14 .5Dietetic technician FTEs lost (n=24)0 8 33.3<1 5 20.81-2 9 37 .5>2 2 8.3Dietetic technician FTEs added (n=30)0 7 23.3<1 7 23.31-2 13 43.3>2 3 10.0Clerk/aide FTEs lost (n=31»0 9 29.0<1 7 22 .51-2 15 48.3>2 0 0.0Clerk/aide FTEs added (n=22)0 10 45 .4<1 3 13.61-2 9 40.9>2 0 0.0
aNumber varies because of missing or unusable data
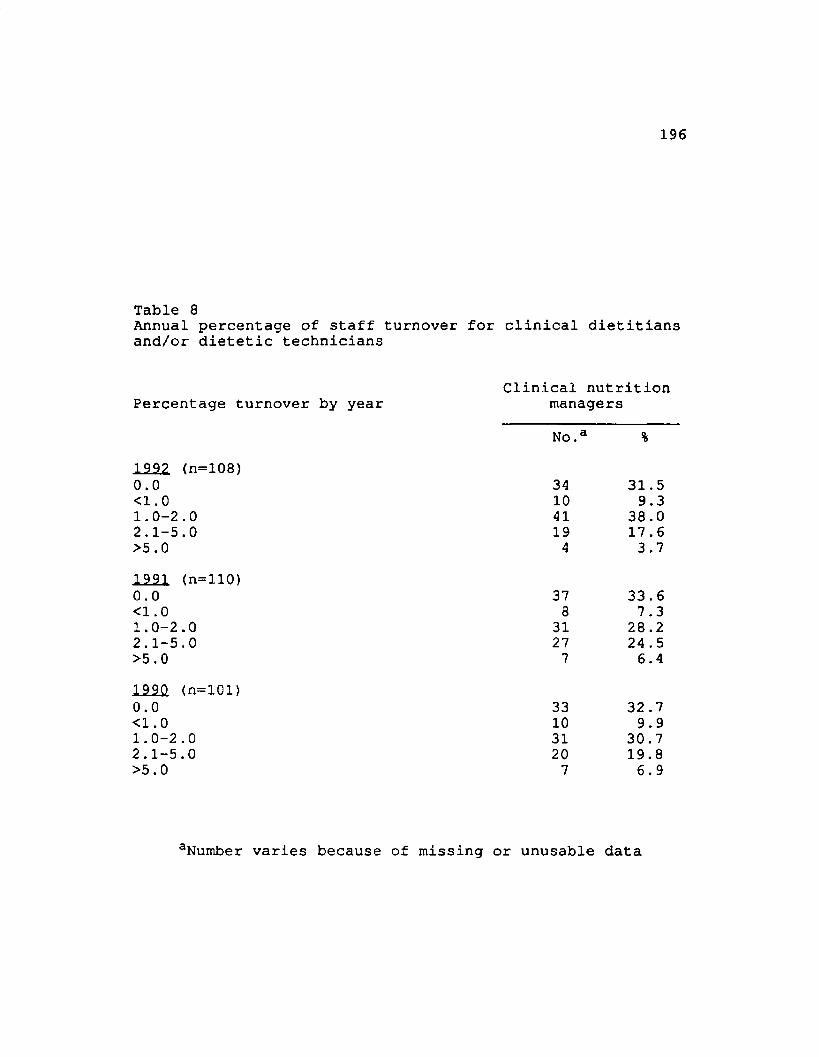
196
Table 8Annual percentage of staff turnover for clinical dietitians and/or dietetic technicians
Clinical nutrition Percentage turnover by year managers
No.a %1992 (n=108)0.0 34 31.5<1.0 10 9.31.0-2.0 41 38.02.1-5.0 19 17 .6>5.0 4 3.71991 (n=110)0.0 37 33.6<1.0 8 7.31.0-2.0 31 28.22.1-5.0 27 24 .5>5.0 7 6.41990 (n=101)0.0 33 32 .7<1.0 10 9.91.0-2.0 31 30.72.1-5.0 20 19.8>5.0 7 6.9
aNumber varies because of missing or unusable data
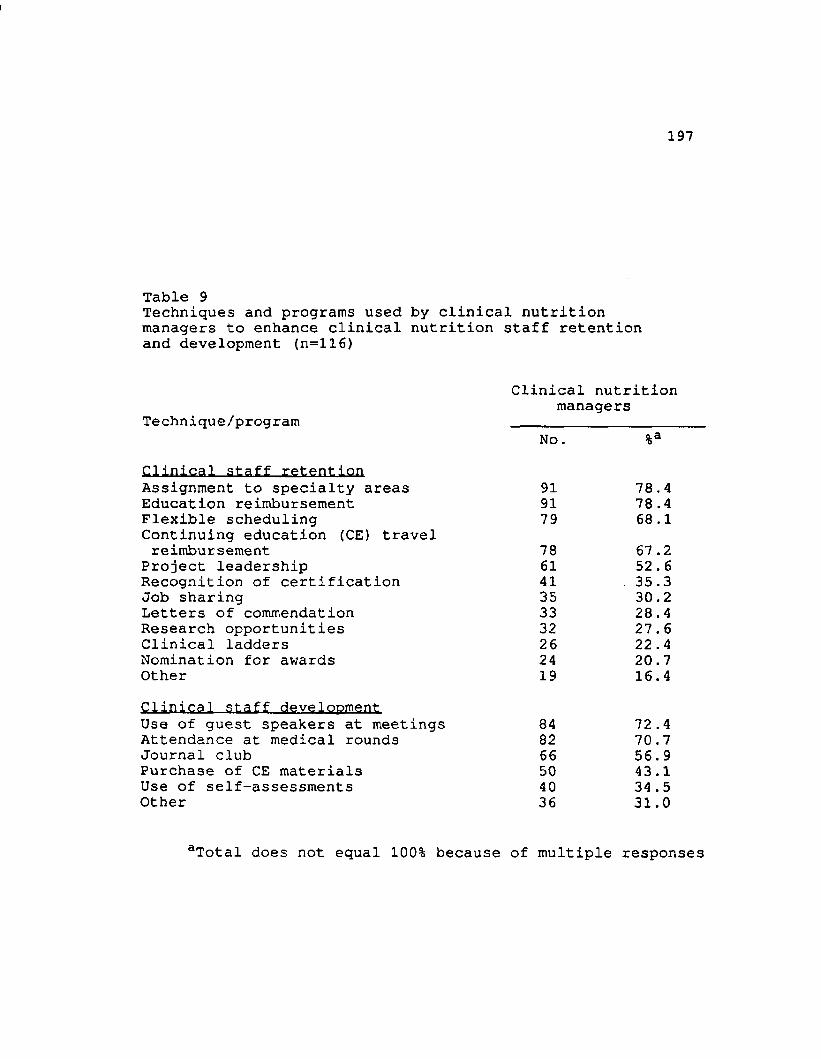
197
Table 9Techniques and programs used by clinical nutrition managers to enhance clinical nutrition staff retention and development (n=ll6)
Clinical nutrition managers
Technique/program ___________________No. %a
Clinical staff retentionAssignment to specialty areas 91 78.4Education reimbursement 91 78 .4Flexible scheduling 79 68.1Continuing education (CE) travel reimbursement 78 67 .2
Project leadership 61 52.6Recognition of certification 41 35.3Job sharing 35 30.2Letters of commendation 33 28.4Research opportunities 32 27.6Clinical ladders 26 22 .4Nomination for awards 24 20.7Other 19 16.4Clinical staff developmentUse of guest speakers at meetings 84 72 .4Attendance at medical rounds 82 70.7Journal club 66 56.9Purchase of CE materials 50 43.1Use of self-assessments 40 34 .5Other 36 31.0
aTotal does not equal 100% because of multiple respon
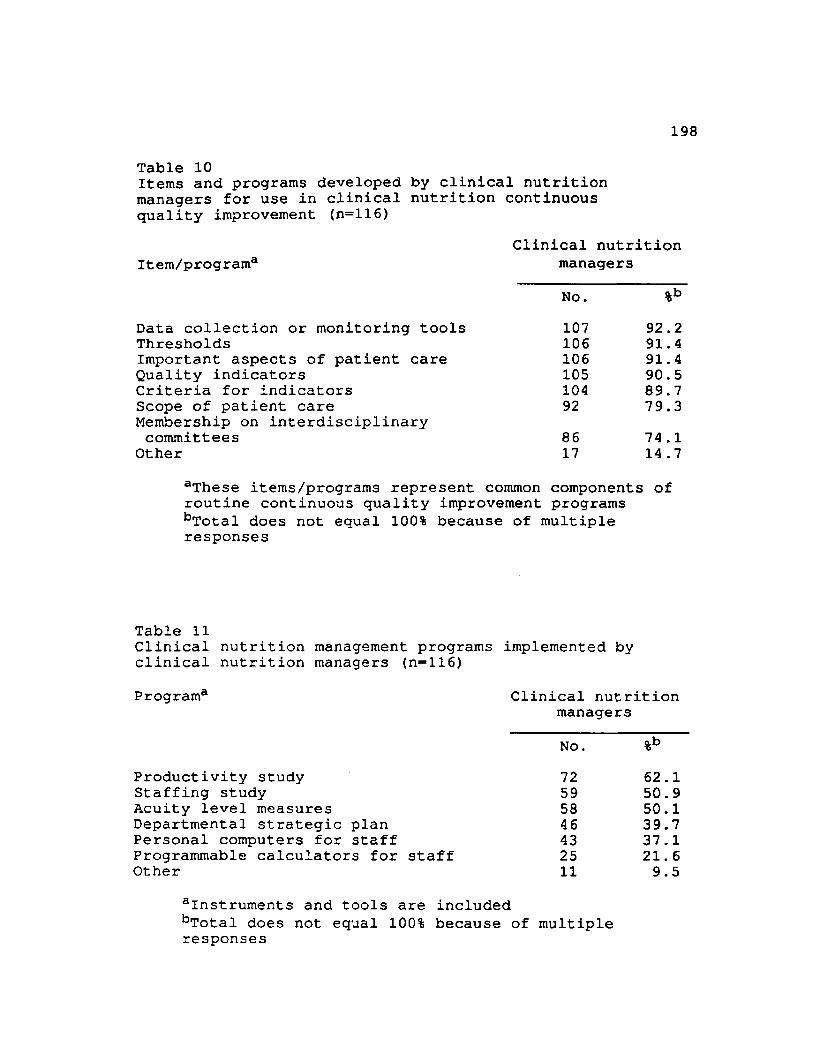
198
Table 10Items and programs developed by clinical nutrition managers for use in clinical nutrition continuous quality improvement (n=116)
Clinical nutrition Item/program3 managers
No. %bData collection or monitoring tools 107 92 .2Thresholds 106 91.4Important aspects of patient care 106 91.4Quality indicators 105 90.5Criteria for indicators 104 89.7Scope of patient care Membership on interdisciplinary
92 79.3committees 86 74 .1
Other 17 14 .7aThese items/programs represent common components of routine continuous quality improvement programs bTotal does not equal 100% because of multiple responses
Table 11Clinical nutrition management programs implemented byclinical nutrition managers Program3
Productivity study Staffing study Acuity level measures Departmental strategic plan Personal computers for staff Programmable calculators for Other
(n-116)Clinical nutrition
managersNO. %b72 62.159 50. 958 50.146 39.743 37.125 21. 611 9.5
instruments and tools are includedbTotal does not equal 100% because of multipleresponses
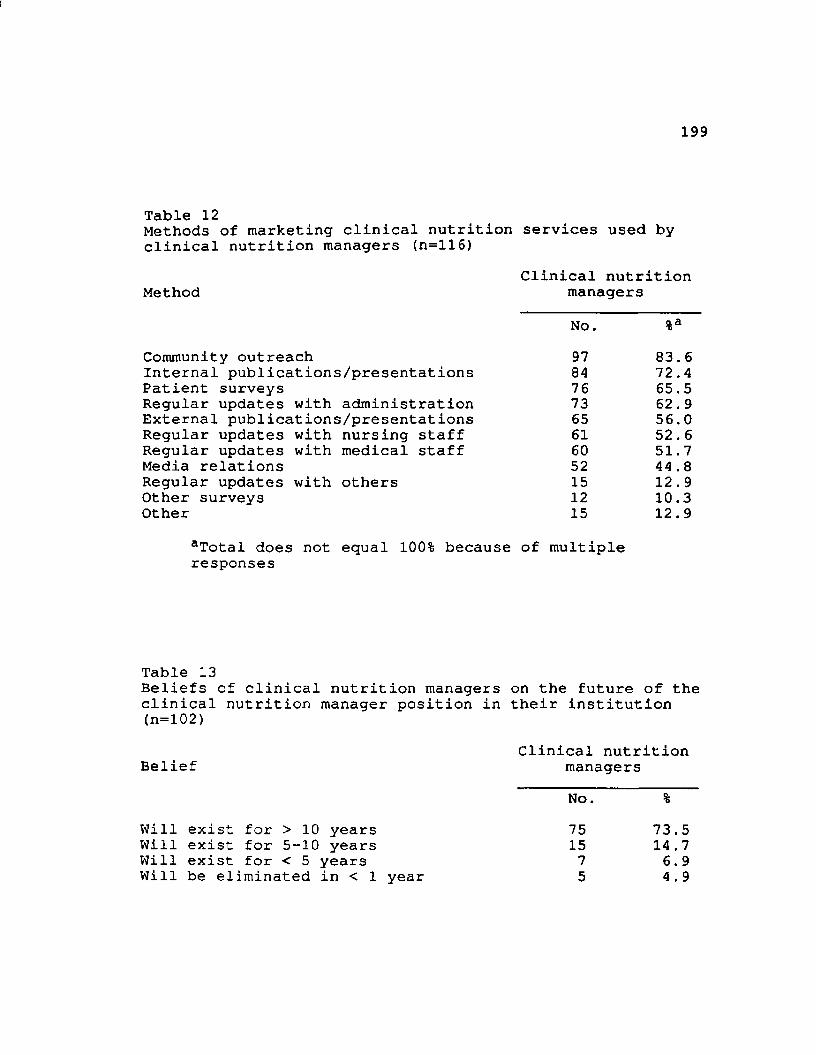
199
Table 12Methods of marketing clinical nutrition services used by clinical nutrition managers (n=116)
Clinical nutrition Method managers
No. %aCommunity outreach 97 83. 6Internal publications/presentations 84 72 .4Patient surveys 76 65.5Regular updates with administration 73 62. 9External publications/presentations 65 56.0Regular updates with nursing staff 61 52.6Regular updates with medical staff 60 51.7Media relations 52 44 .8Regular updates with others 15 12.9Other surveys 12 10.3Other 15 12.9
aTotal does not equal 100% because of multiple responses
Table 13Beliefs of clinical nutrition managers on the future of the clinical nutrition manager position in their institution (n=l02)
Clinical nutrition Belief managers
No. %Will exist for > 10 years 75 73.5Will exist for 5-10 years 15 14.7Will exist for < 5 years 7 6.9Will be eliminated in < 1 year 5 4.9
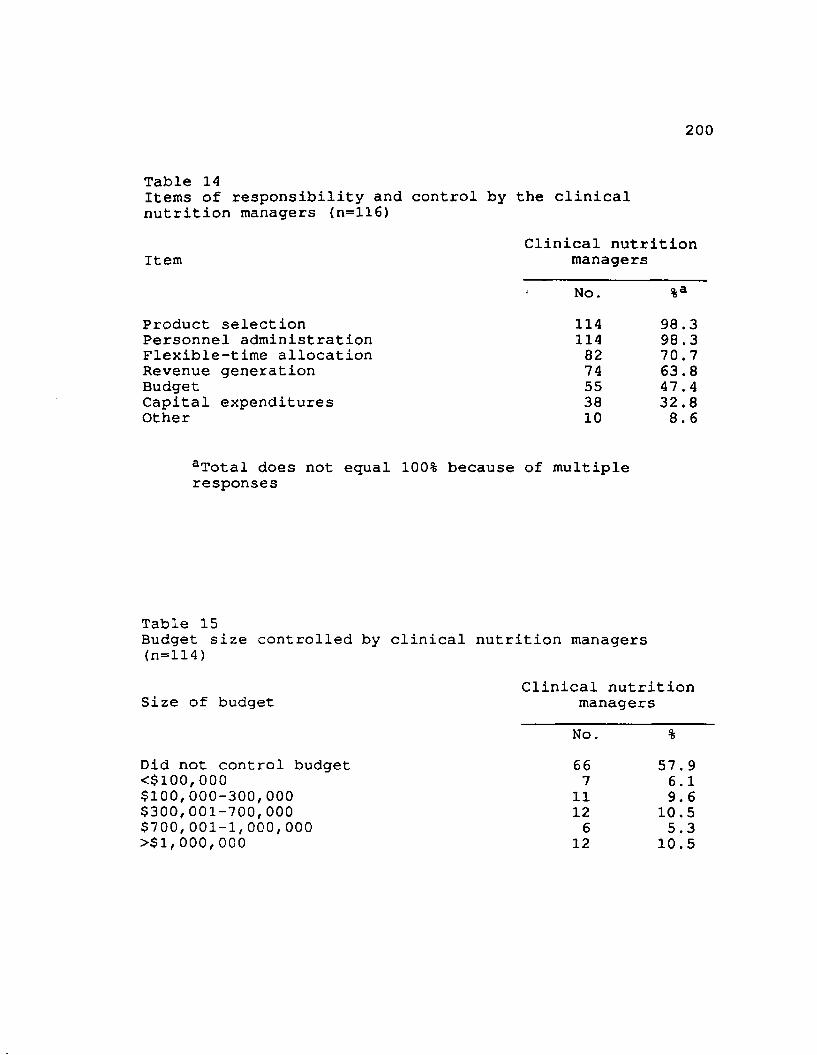
200
Table 14Items of responsibility and control by the clinical nutrition managers <n=116)
Clinical nutrition Item managers
No. %aProduct selection 114 98.3Personnel administration 114 98 .3Flexible-time allocation 82 70.7Revenue generation 74 63.8Budget 55 47.4Capital expenditures 38 32.8Other 10 8.6
aTotal does not equal 100% because of multipleresponses
Table 15Budget size controlled by clinical nutrition managers (n=114)
Clinical nutrition Size of budget managers
No. %Did not control budget 66 57. 9<$100,000 7 6.1$100,000-300,000 11 9.6$300,001-700,000 12 10.5$700,001-1,000,000 6 5.3>$1,000,000 12 10.5
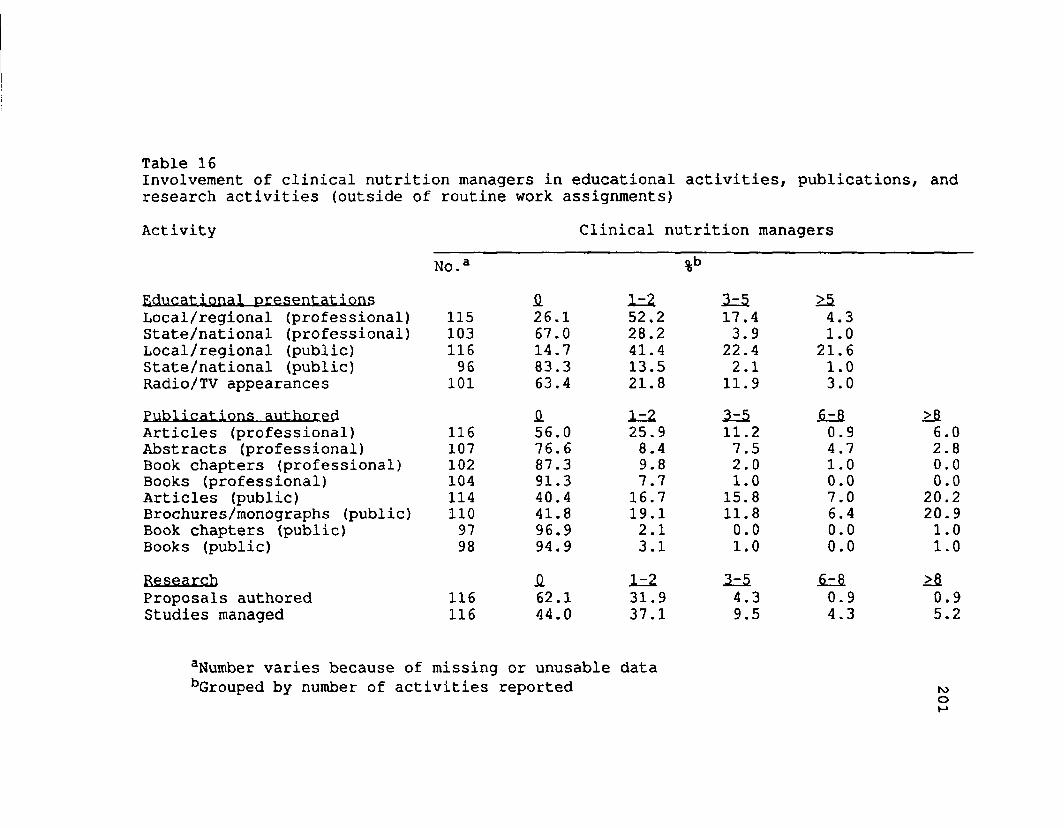
Table 16Involvement of clinical nutrition managers in educational activities, publications, and research activities (outside of routine work assignments)Activity
Educational presentations Local/regional (professional) State/national (professional) Local/regional (public) State/national (public) Radio/TV appearancesPublications authored Articles (professional) Abstracts (professional)Book chapters (professional) Books (professional)Articles (public) Brochures/monographs (public) Book chapters (public)Books (public)ResearchProposals authored Studies managed
aNumber varies because of bGrouped by number of act
Clinical
No.a0. 1 = Z
115 26.1 52,2103 67.0 28.2116 14.7 41.496 83.3 13.5
101 63.4 21.8£ 1 = 1
116 56.0 25.9107 76.6 8.4102 87.3 9.8104 91.3 7.7114 40.4 16.7110 41.8 19.197 96.9 2.198 94.9 3.1
H 1 = 1116 62.1 31.9116 44.0 37.1
missing or unusable data vities reported
managers
> 217.4 4.33.9 1.0
22.4 21.62.1 1.0
11.9 3.0I z S 2 = 2 >fi11.2 0.9 6.07.5 4.7 2.82.0 1.0 0.01.0 0.0 0.0
15.8 7.0 20.211.8 6.4 20.90.0 0.0 1.01.0 0.0 1.0
2 = 5 . 2 = 2 >fl4.3 0.9 0.99.5 4.3 5.2
r o
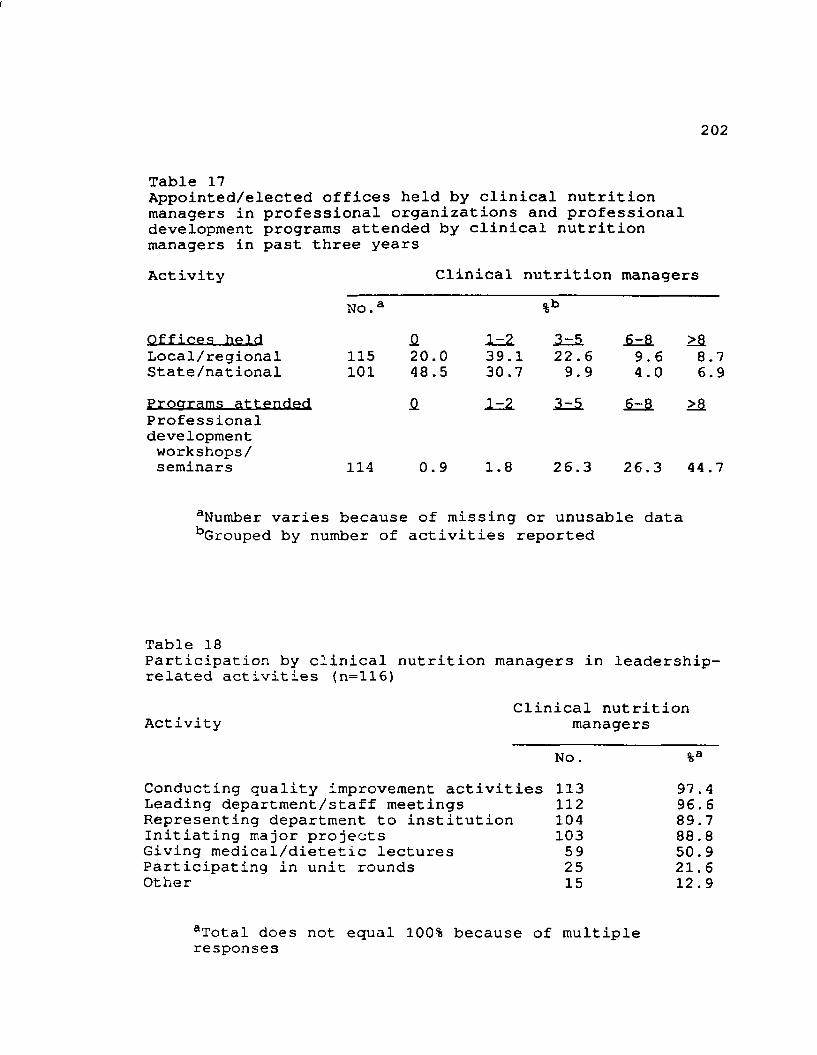
202
Table 17Appointed/elected offices held by clinical nutrition managers in professional organizations and professional development programs attended by clinical nutrition managers in past three yearsActivity Clinical nutrition managers
Offices heldNo.a
Q. 1=2.
%b3-5 >a
Local/regional 115 20.0 39.1 22.6 9.6 8.7State/national 101 48.5 30 .7 9.9 4.0 6.9Procrrams attended £ 1-2 3-5 6-8 >&Professionaldevelopmentworkshops/seminars 114 0.9 1.8 26.3 26.3 44.7
aNumber varies because of missing or unusable data bGrouped by number of activities reported
Table 18Participation by clinical nutrition managers in leadership- related activities (n=116)
Clinical nutrition Activity managers
N o . %aConducting quality improvement activities 113 97 .4Leading department/staff meetings 112 96. 6Representing department to institution 104 89.7Initiating major projects 103 88.8Giving medical/dietetic lectures 59 50.9Participating in unit rounds 25 21.6Other 15 12 . 9
aTotal does not equal 100% because of multipleresponses
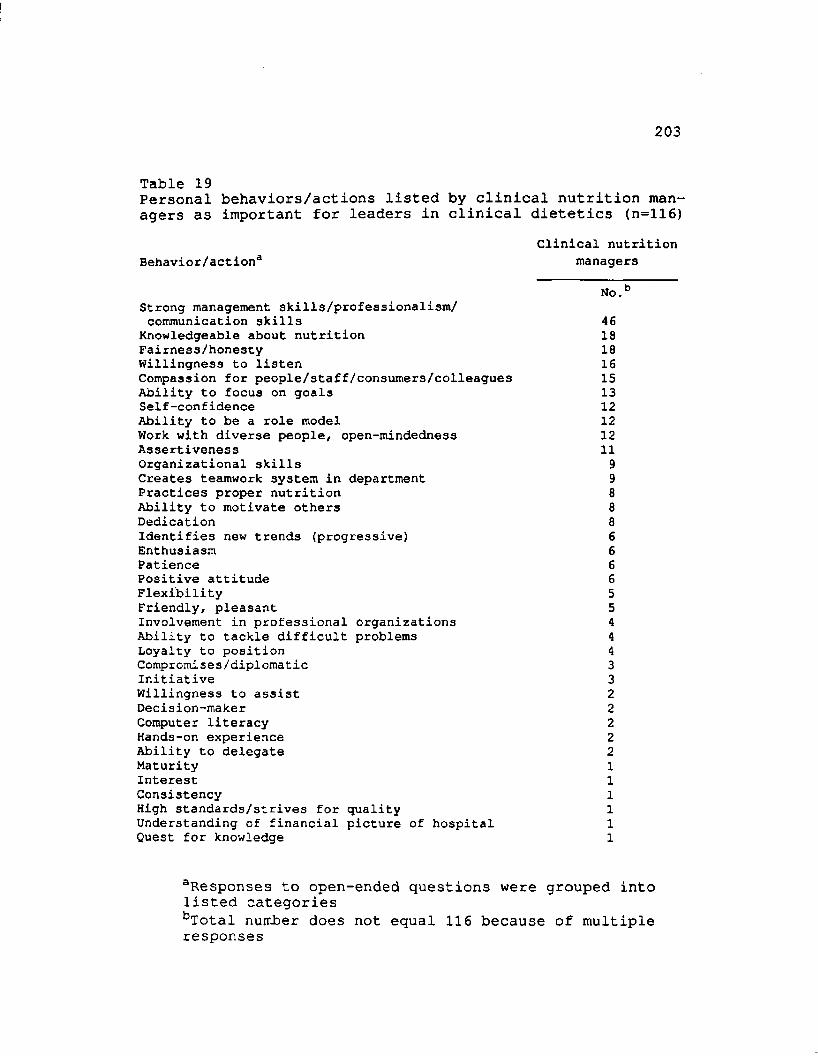
I
203
Table 19Personal behaviors/actions listed by clinical nutrition managers as important for leaders in clinical dietetics (n=116)
Clinical nutritionBehavior/action3 managers
No.bStrong management skills/professionalism/ communication skills 46
Knowledgeable about nutrition 18Fairnes3/honesty 18Willingness to listen 16Compassion for people/staff/consumers/colleagues 15Ability to focus on goals 13Self-confidence 12Ability to be a role model 12Work with diverse people, open-mindedness 12Assertiveness 11Organizational skills 9Creates teamwork system in department 9Practices proper nutrition 8Ability to motivate others 8Dedication 8Identifies new trends (progressive) 6Enthusiasm 6Patience 6Positive attitude 6Flexibility 5Friendly, pleasant 5Involvement in professional organizations 4Ability to tackle difficult problems 4Loyalty to position 4Compromises/diplomatic 3Initiative 3Willingness to assist 2Decision-maker 2Computer literacy 2Hands-on experience 2Ability to delegate 2MaturityInterestConsistencyHigh standards/strives for quality Understanding of financial picture of hospital Quest for knowledge
aResponses to open-ended questions were grouped into listed categoriesbTotal number does not equal 116 because of multiple responses
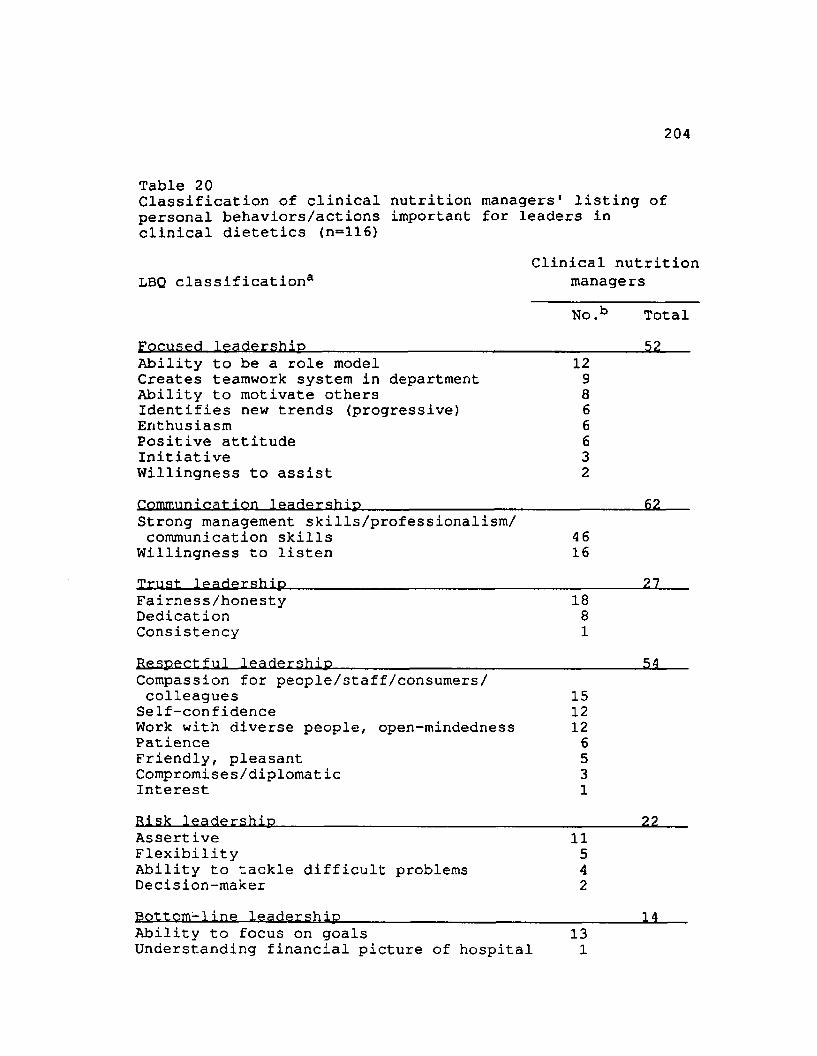
204
Table 20Classification of clinical nutrition managers' listing of personal behaviors/actions important for leaders in clinical dietetics (n=116)
Clinical nutritionLBQ classification3
Focused leadership
managers No.b Total
52Ability to be a role model 12Creates teamwork system in department 9Ability to motivate others 8Identifies new trends (progressive) 6Enthusiasm 6Positive attitude 6Initiative 3Willingness to assist 2Communication leadership 62Strong management skills/professionalism/ communication skills 46
Willingness to listen 16Trust leadership 27Fairness/honesty 18Dedication 8Consistency 1Respectful leadership 54Compassion for people/staff/consumers/ colleagues 15
Self-confidence 12Work with diverse people, open-mindedness 12Patience 6Friendly, pleasant 5Compromises/diplomatic 3Interest 1Risk leadership 22Assertive 11Flexibility 5Ability to tackle difficult problems 4Decision-maker 2Bottom-line leadership 14Ability to focus on goals 13Understanding financial picture of hospital 1
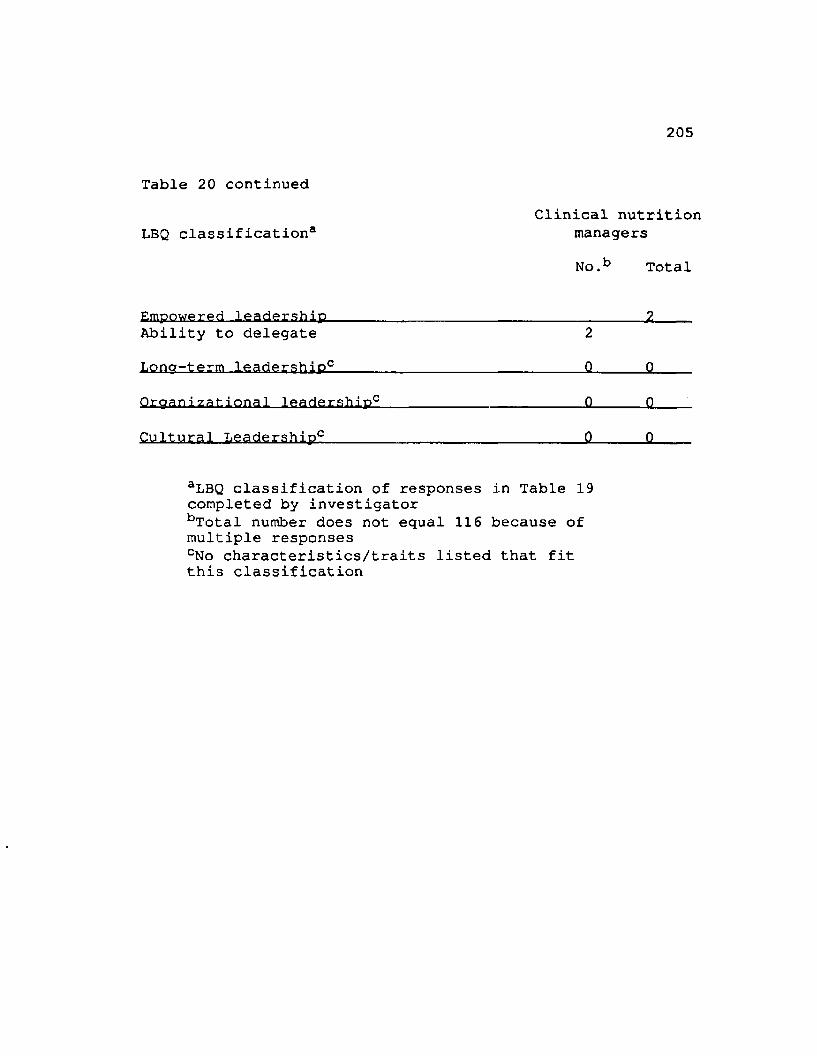
205
Table 20 continuedClinical nutrition
LBQ classification3 managers
Empowered leadership
No.b Total
2Ability to delegate 2Lona-term leadership0 0 0Oraanizational leadership0 0 0Cultural Leadership0 0 0
aLBQ classification of responses in Table 19 completed by investigatorbTotal number does not equal 116 because of multiple responsescNo characteristics/traits listed that fit this classification
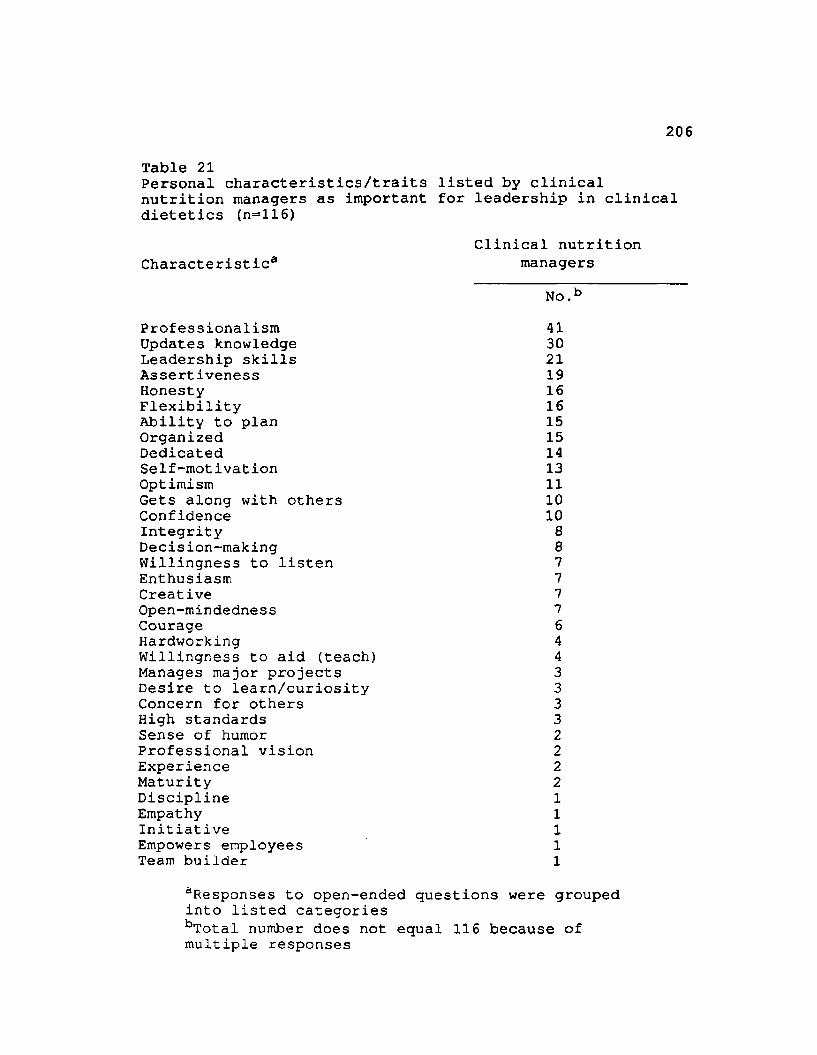
206
Table 21Personal characteristics/traits listed by clinical nutrition managers as important for leadership in clinical dietetics (n=116)
Clinical nutrition Characteristic® managers
ProfessionalismNo.41
Updates knowledge 30Leadership skills 21Assertiveness 19Honesty 16Flexibility 16Ability to plan 15Organized 15Dedicated 14Self-motivation 13Optimism 11Gets along with others 10Confidence 10Integrity 8Decision-making 8Willingness to listen 7Enthusiasm 7Creative 7Open-mindedness 7Courage 6Hardworking 4Willingness to aid (teach) 4Manages major projects 3Desire to learn/curiosity 3Concern for others 3High standards 3Sense of humor 2Professional vision 2Experience 2Maturity 2Discipline 1Empathy 1Initiative 1Empowers employees 1Team builder 1
aResponses to open-ended questions were grouped into listed categoriesbTotal number does not equal 116 because of multiple responses
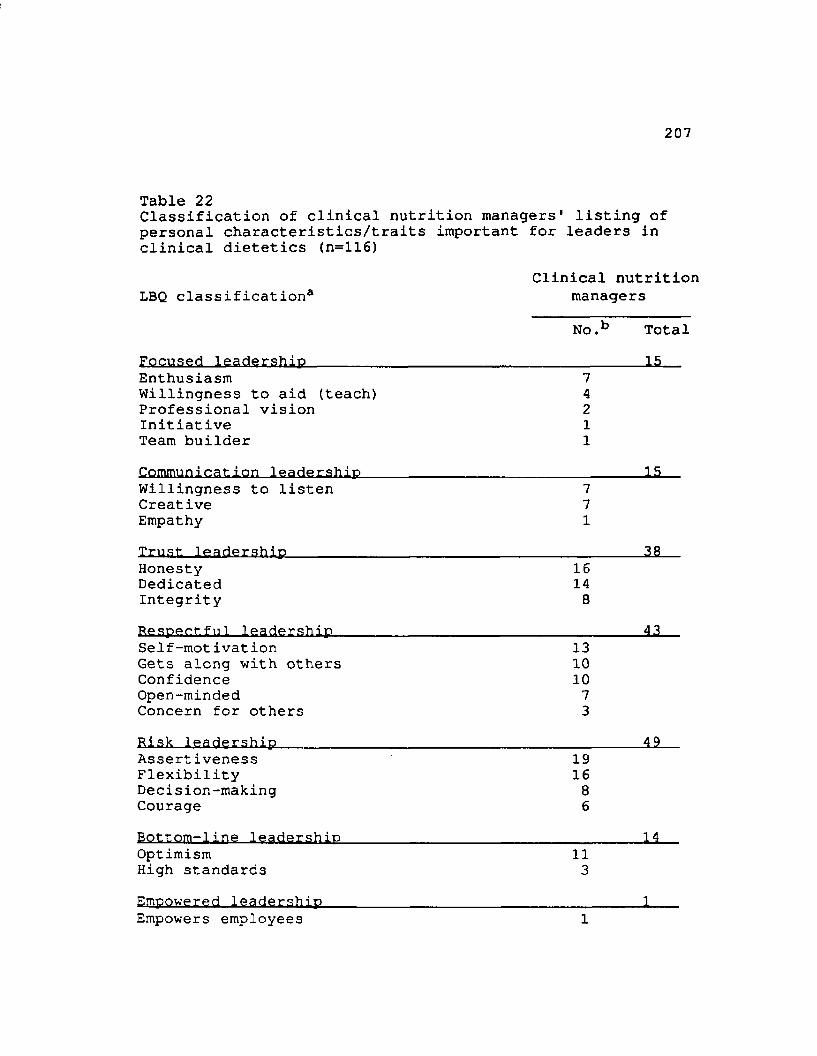
207
Table 22Classification of clinical nutrition managers' listing of personal characteristics/traits important for leaders in clinical dietetics (n=116)
Clinical nutrition LBQ classification3 managers
No.b TotalFocused leadership______________________________________ liEnthusiasm 7Willingness to aid (teach) 4Professional vision 2Initiative 1Team builder 1Communication leadership 15Willingness to listen 7Creative 7Empathy 1Trust leadership 38Honesty 16Dedicated 14Integrity 8Resoect fu1 leadership 43Self-mot ivation 13Gets along with others 10Confidence 10Open-minded 7Concern for others 3Risk leadership 49Assertiveness 19Flexibility 16Decision-making 8Courage 6Bottom-line leadership 14Optimism 11High standards 3Empowered leadership Empowers employees 1
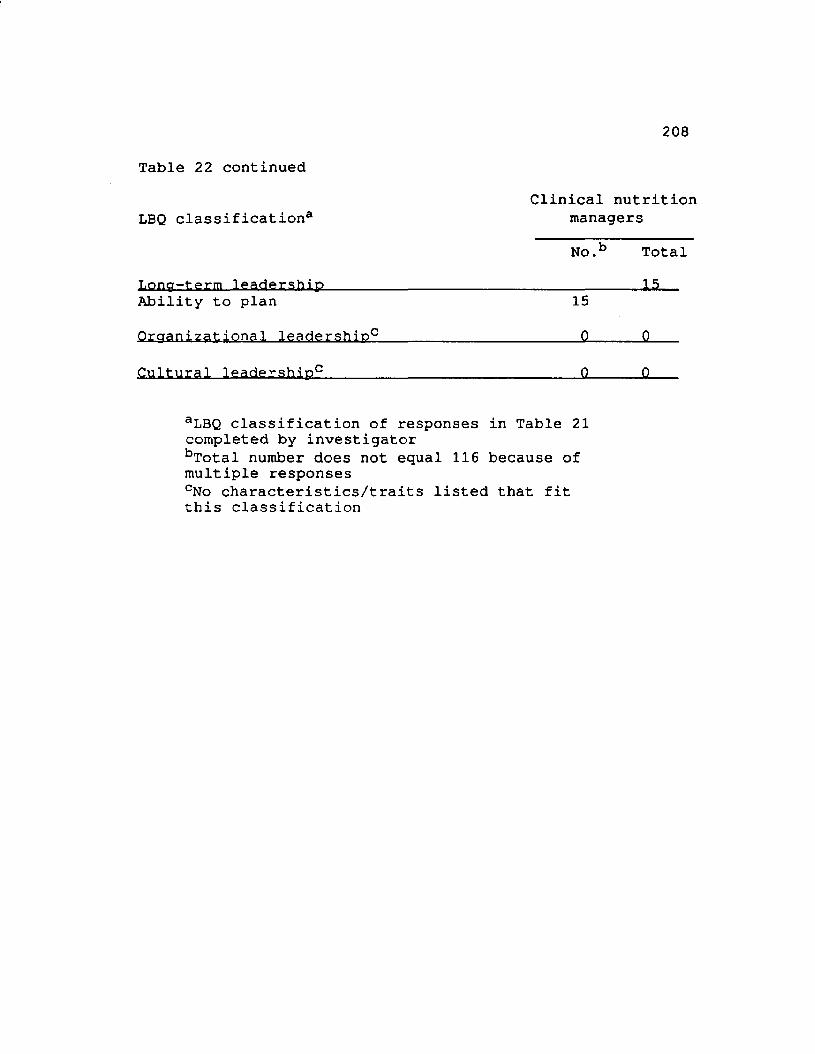
208
Table 22 continuedClinical nutrition
LBQ classification3 managersNo .b Total
L o n g - t e r m leaaersnip Ability to plan 15Qrcranizational leadership0 0 0
Cultural leadership0 0 0
aLBQ classification of responses in Table 21 completed by investigatorbTotal number does not equal 116 because of multiple responsescNo characteristics/traits listed that fit this classification
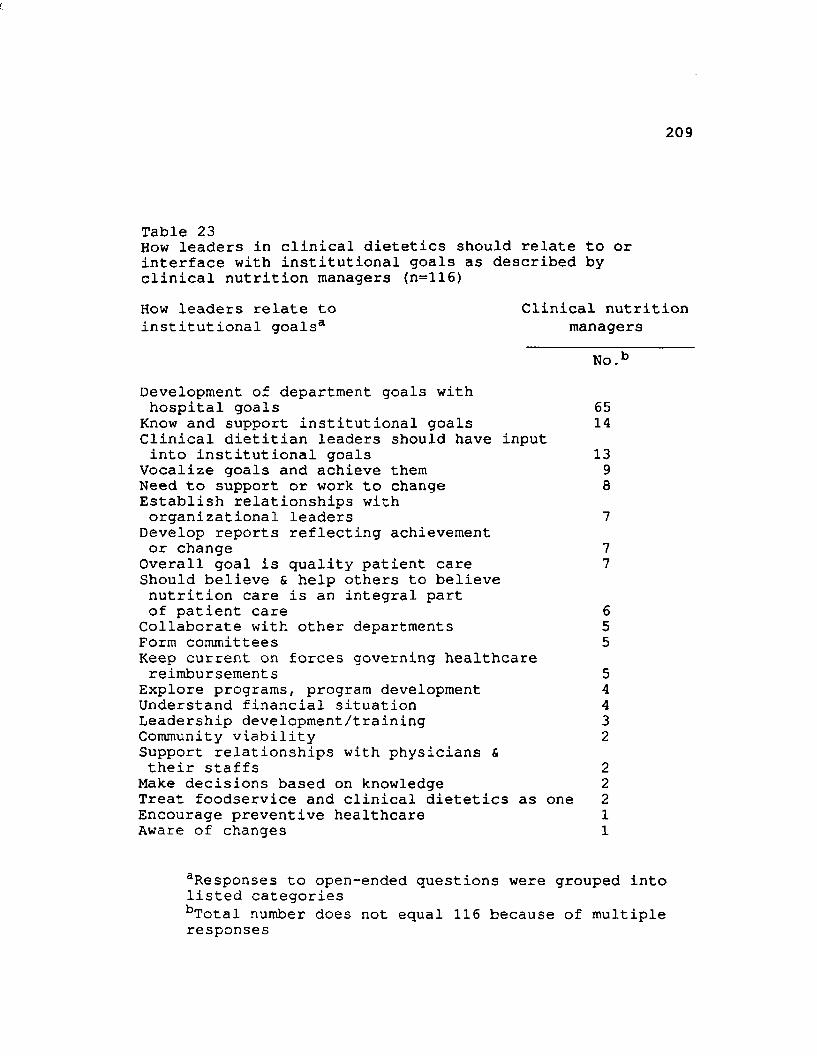
209
Table 23How leaders in clinical dietetics should relate to or interface with institutional goals as described by clinical nutrition managers (n=116)How leaders relate to institutional goals3
Clinical nutrition managers
No.1Development of department goals with hospital goals
Know and support institutional goals Clinical dietitian leaders should have input into institutional goals
Vocalize goals and achieve them Need to support or work to change Establish relationships with organizational leaders
Develop reports reflecting achievement or change
Overall goal is quality patient care Should believe & help others to believe nutrition care is an integral part of patient care
Collaborate with other departments Form committeesKeep current on forces governing healthcare reimbursement s
Explore programs, program development Understand financial situation Leadership development/training Community viabilitySupport relationships with physicians & their staffs
Make decisions based on knowledge Treat foodservice and clinical dietetics as one Encourage preventive healthcare Aware of changes
65141398
77
6555443222211
aResponses to open-ended questions were grouped into listed categoriesbTotal number does not equal 116 because of multiple responses
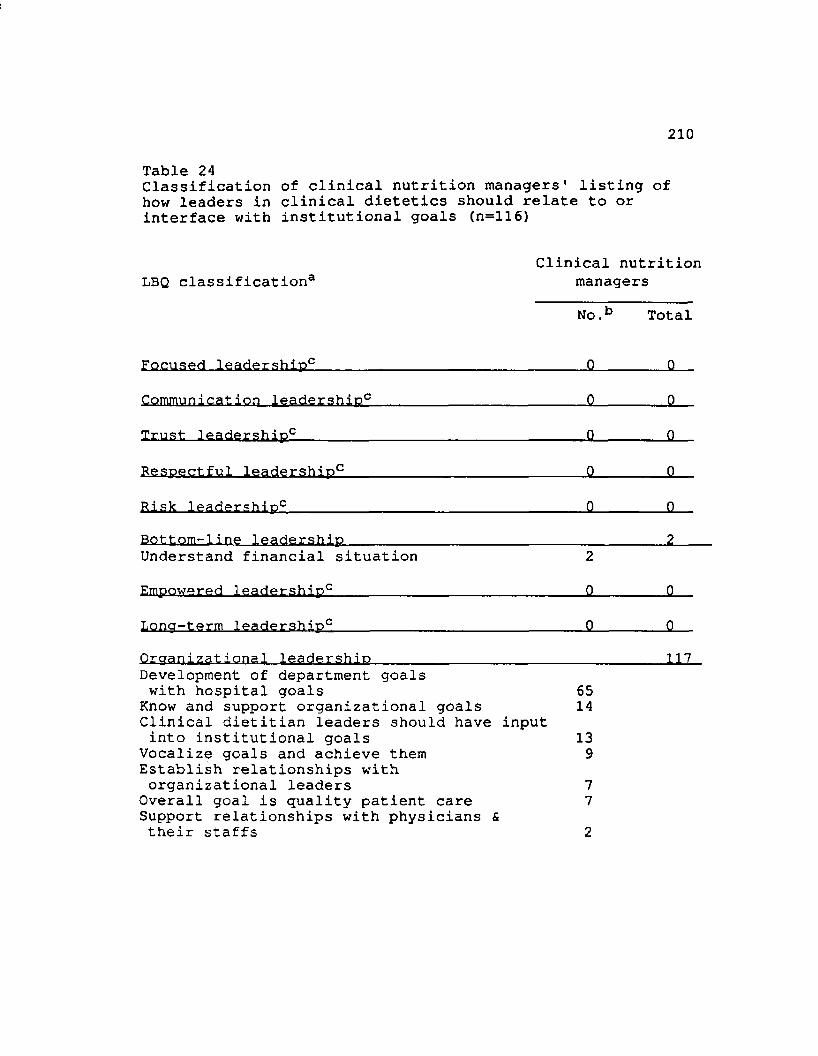
210
Table 24Classification of clinical nutrition managers' listing of how leaders in clinical dietetics should relate to or interface with institutional goals (n=116)
LBQ classification*Clinical nutrition
managersNo.b Total
Focused leadership0 0 0Communication leadership0 0 .. . . 0Trust leadership0 0 Q
Respectful leadership0 0 0Risk leadership0 0 0Bottom-line leadership 2Understand financial situation 2EmDowered leadership0 0 0
Loncr-term leadership0 0 0Orcranizational leadership .... 117Development of department goals with hospital goals
Know and support organizational goals Clinical dietitian leaders should have input into institutional goals
Vocalize goals and achieve them Establish relationships with organizational leaders
Overall goal is quality patient care Support relationships with physicians & their staffs
6514139772
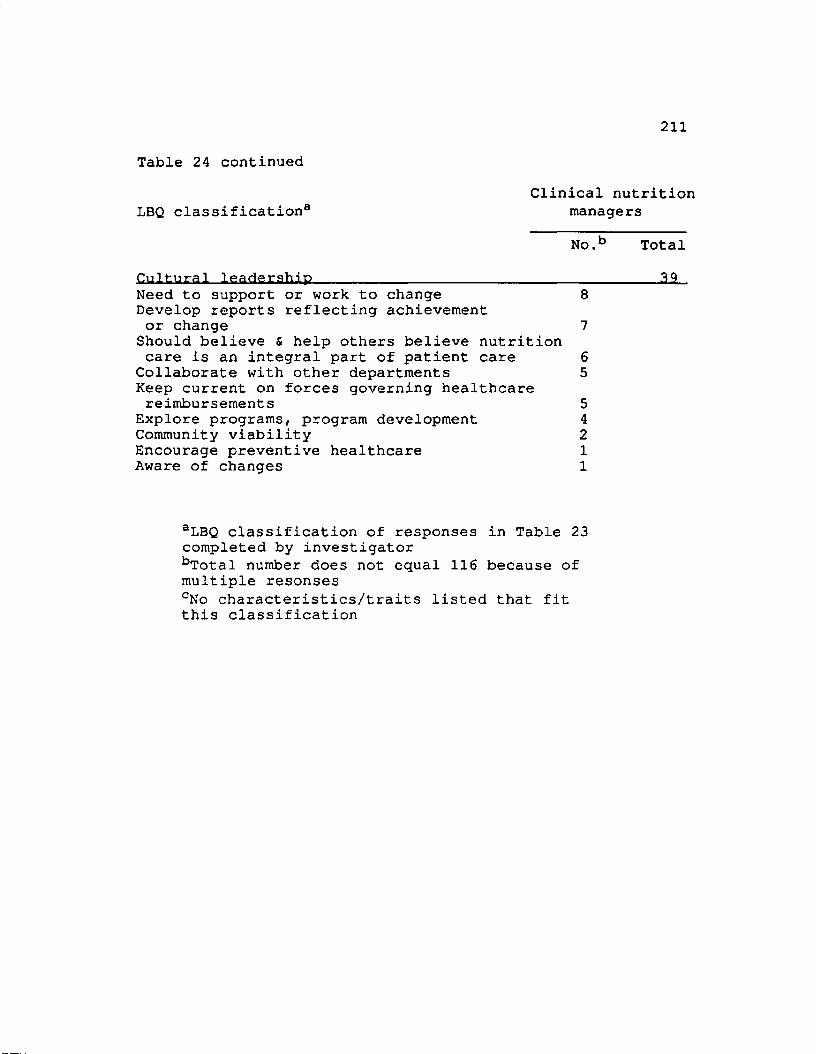
211
Table 24 continuedClinical nutrition
LBQ classification3 managersNo.b Total
Cultural leadership_______________________________________ 12_Need to support or work to change 8Develop reports reflecting achievement or change 7
Should believe & help others believe nutrition care is an integral part of patient care 6
Collaborate with other departments 5Keep current on forces governing healthcare reimbursements 5
Explore programs, program development 4Community viability 2Encourage preventive healthcare 1Aware of changes 1
aLBQ classification of responses in Table 23 completed by investigatorbTotal number does not equal 116 because of multiple resonsescNo characteristics/traits listed that fit this classification
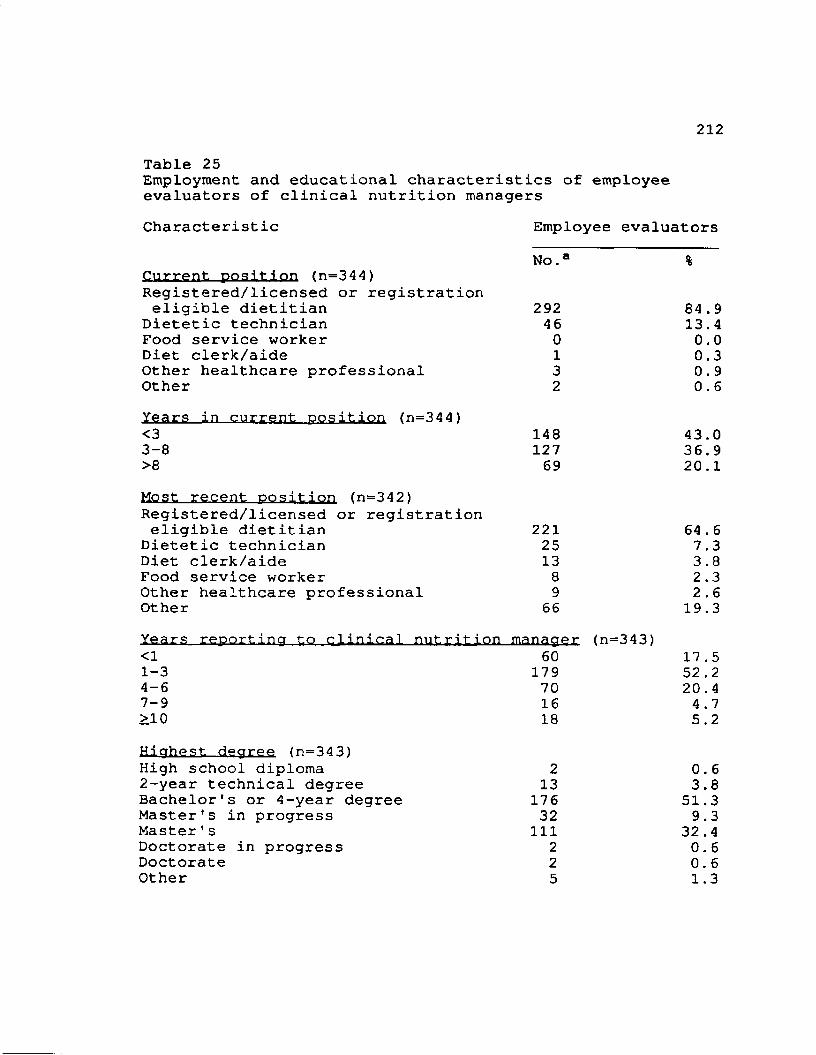
212Table 25Employment and educational characteristics of employee evaluators of clinical nutrition managersCharacteristic Employee evaluators
N o . %Current position (n=344)Registered/licensed or registration eligible dietitian 292 84.9
Dietetic technician 46 13.4Food service worker 0 0.0Diet clerk/aide 1 0.3Other healthcare professional 3 0.9Other 2 0.6Years in current position (n=344)<3 148 43.03-8 127 36.9>8 69 20.1Most recent position (n=342)Registered/licensed or registration eligible dietitian 221 64.6
Dietetic technician 25 7.3Diet clerk/aide 13 3.8Food service worker 8 2.3Other healthcare professional 9 2.6Other 66 19.3Years reporting to clinical nutrition manager <n=343)<1 60 17.51-3 179 52.24-6 70 20.47-9 16 4.7>10 18 5.2Highest degree (n=343)High school diploma 2 0.62-year technical degree 13 3.8Bachelor's or 4-year degree 176 51.3Master's in progress 32 9.3Master's 111 32.4Doctorate in progress 2 0.6Doctorate 2 0.6Other 5 1.3
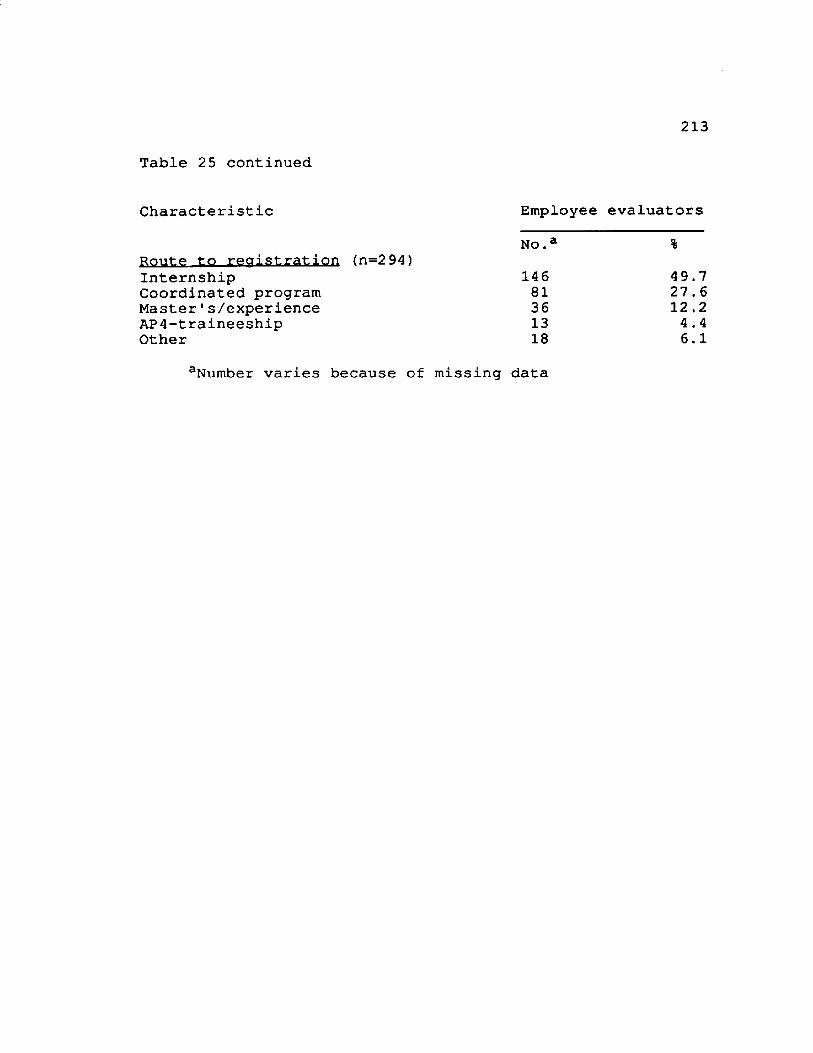
213
Table 25 continued
Characteristic Employee evaluators
Route to reoistration (n=2 94)No.a %
Internship 146 49.7Coordinated program 81 27.6Master's/experience 36 12 .2AP4-traineeship 13 4 . 4Other 18 6.1
aNumber varies because of missing data
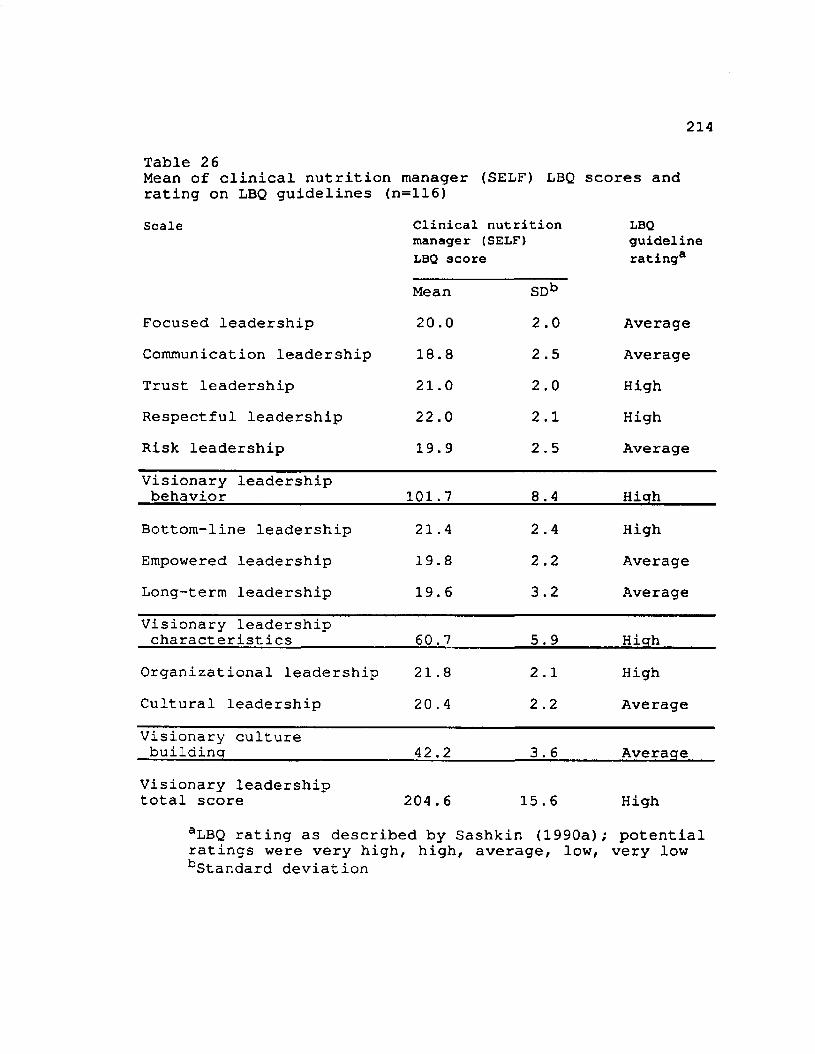
214
Table 2 6Mean of clinical nutrition manager (SELF) LBQ scores and rating on LBQ guidelines (n=116)Scale Clinical nutrition
manager (SELF)LBQ score
LBQguidelinerating3
Mean S D b
Focused leadership 20.0 2.0 AverageCommunication leadership 18.8 2.5 AverageTrust leadership 21.0 2.0 HighRespectful leadership 22.0 2.1 HighRisk leadership 19.9 2.5 AverageVisionary leadership behavior 101.7 8.4 Hiqh
Bottom-line leadership 21.4 2.4 HighEmpowered leadership 19.8 2.2 AverageLong-term leadership 19.6 3.2 AverageVisionary leadership characteristics 60.7 5.9 Hiqh
Organizational leadership 21.8 2 .1 HighCultural leadership 20 . 4 2.2 AverageVisionary culture buildina 42 .2 3 . 6 Average
Visionary leadershiptotal score 204.6 15.6 High
aLBQ rating as described by Sashkin (1990a); potential ratings were very high, high, average, low, very low bStandard deviation
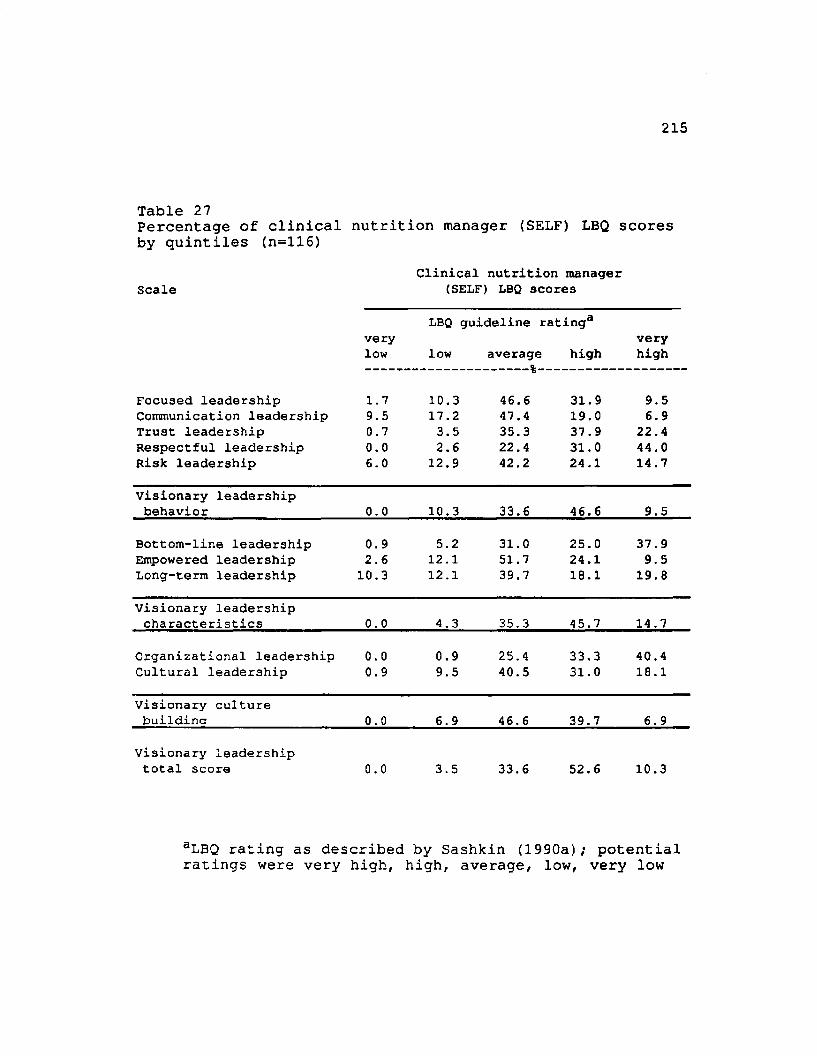
215
Table 27Percentage of clinical nutrition manager (SELF) LBQ scores by quintiles (n=116)
ScaleClinical nutrition manager
(SELF) LBQ scores
LBQ guideline rating3very verylow low average high high
%
Focused leadership 1.7 10.3 46.6 31.9 9.5Communication leadership 9.5 17.2 47.4 19.0 6.9Trust leadership 0.7 3.5 35.3 37.9 22.4Respectful leadership 0.0 2.6 22.4 31.0 44.0Risk leadership 6.0 12.9 42.2 24.1 14.7
Visionary leadershipbehavior 0.0 10.3 33.6 46.6 9.5
Bottom-line leadership 0.9 5.2 31.0 25.0 37.9Empowered leadership 2.6 12.1 51.7 24.1 9.5Long-term leadership 10.3 12.1 39.7 18.1 19.8
Visionary leadershipcharacteristics 0.0 4.3 35.3 45.7 14.7
Organizational leadership 0.0 0.9 25.4 33.3 40.4Cultural leadership 0.9 9.5 40.5 31.0 18.1
Visionary culturebuildina 0.0 6.9 46.6 39.7 6.9
Visionary leadershiptotal score 0.0 3.5 33.6 52.6 10.3
aLBQ rating as described by Sashkin (1990a); potential ratings were very high, high, average, low, very low
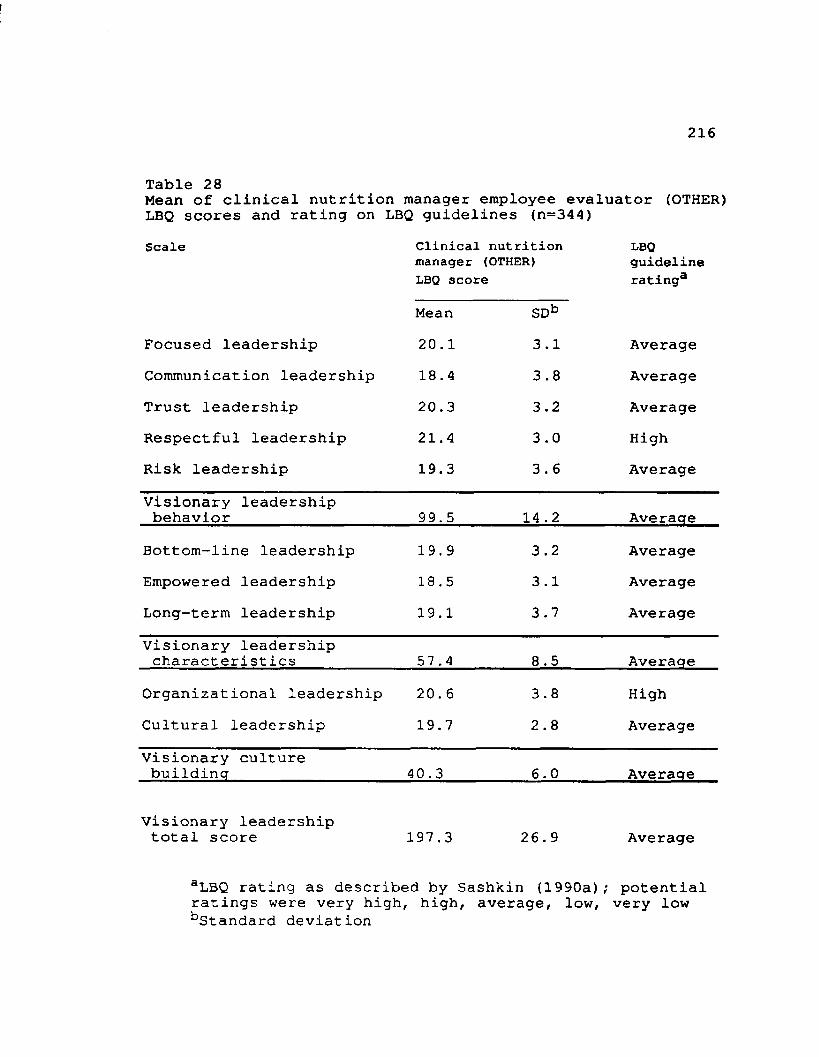
216
Table 28Mean of clinical nutrition manager employee evaluator (OTHER) LBQ scores and rating on LBQ guidelines (n=34 4)Scale Clinical nutrition
manager (OTHER)LBQ score
LBQguidelinerating3
Mean SDbFocused leadership 20.1 3.1 AverageCommunication leadership 18.4 3.8 AverageTrust leadership 20.3 3.2 AverageRespectful leadership 21.4 3.0 HighRisk leadership 19.3 3.6 AverageVisionary leadership behavior 99.5 14 .2 Average
Bottom-line leadership 19.9 3.2 AverageEmpowered leadership 18 . 5 3.1 AverageLong-term leadership 19.1 3.7 AverageVisionary leadership characteristics 57 .4 8.5 Average
Organizational leadership 20. 6 3.8 HighCultural leadership 19.7 2.8 AverageVisionary culture buildinq 40.3 6.0 Average
Visionary leadership total score 197.3 26.9 Average
aLBQ rating as described by Sashkin (1990a); potential ratings were very high, high, average, low, very low ^Standard deviation
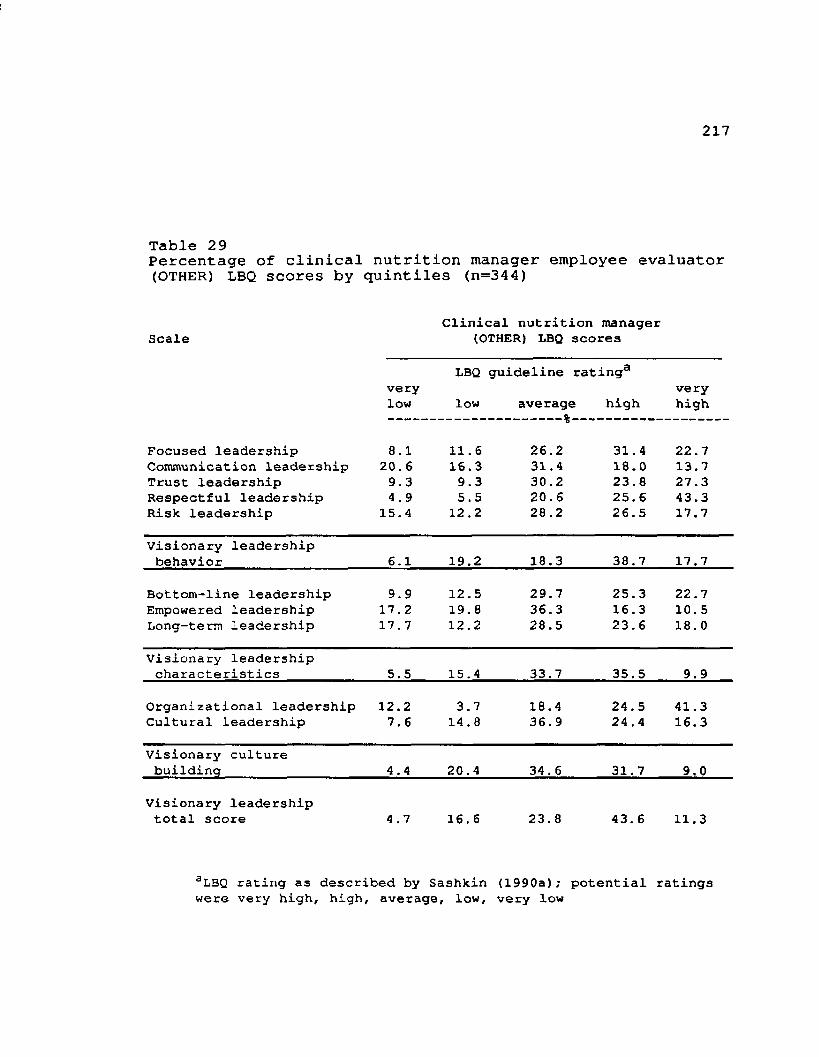
217
Table 2 9Percentage of clinical nutrition manager employee evaluator (OTHER) LBQ scores by quintiles (n=344)
Clinical nutrition manager Scale (OTHER) LBQ scores
LBQ guideline rating3very verylow low average high high
%
Focused leadership 8.1 11.6 26.2 31.4 22.7Communication leadership 20. 6 16.3 31.4 18.0 13.7Trust leadership 9.3 9.3 30.2 23.8 27.3Respectful leadership 4.9 5.5 20.6 25.6 43.3Risk leadership 15.4 12.2 28.2 26.5 17. 7
Visionary leadershipbehavior 6.1 19.2 18.3 38.7 17.7
Bottom-line leadership 9.9 12.5 29.7 25.3 22.7Empowered leadership 17.2 19.8 36.3 16.3 10.5Long-term leadership 17 . 7 12.2 28.5 23.6 18. 0
Visionary leadershipcharacteristics 5.5 15.4 33.7 35.5 9.9
Organizational leadership 12.2 3.7 18.4 24.5 41.3Cultural leadership 7.6 14.8 36.9 24.4 16.3
Visionary culturebuilding 4.4 20.4 34. 6 31.7 9.0
Visionary leadership total score 4.7 16.6 23.8 43.6 11.3
aLBQ rating as described by Sashkin (1990a); potential ratings were very high, high, average, low, very low
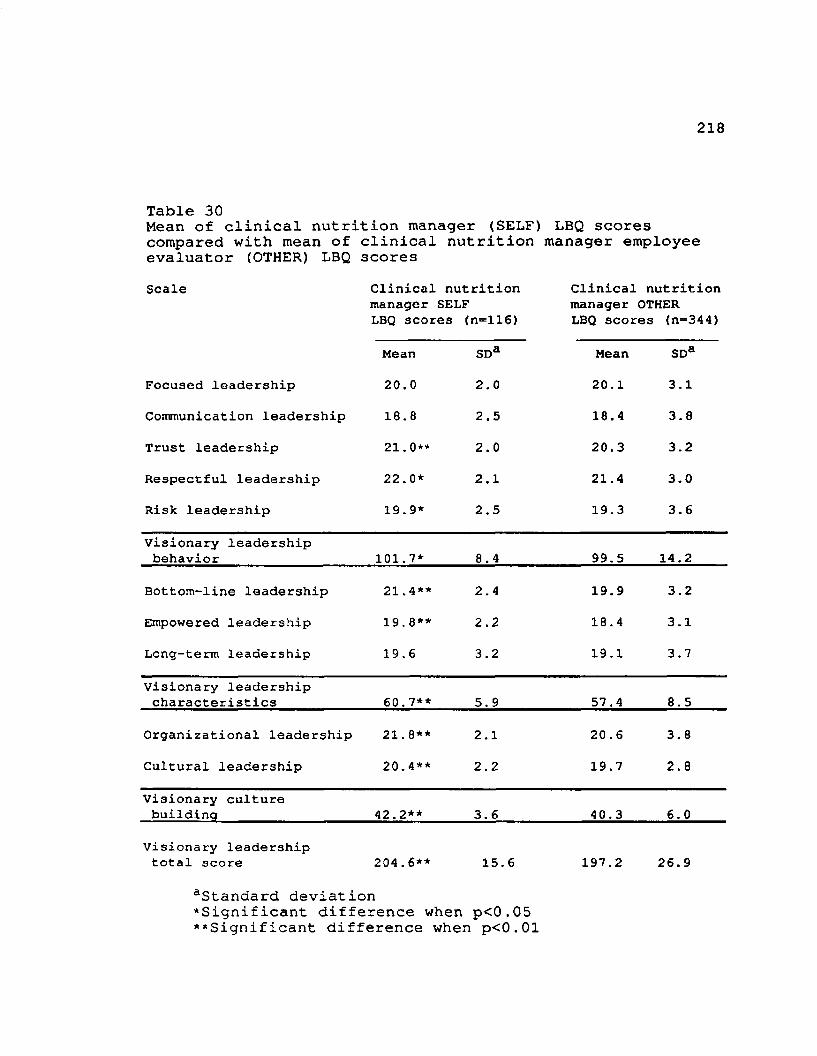
218
Table 30Mean of clinical nutrition manager (SELF) LBQ scores compared with mean of clinical nutrition manager employee evaluator (OTHER) LBQ scoresScale Clinical nutrition Clinical nutrition
manager SELF manager OTHERLBQ scores (n=116) LBQ scores (n=344)
Mean SDa Mean SDa
Focused leadership 20.0 2.0 20.1 3.1
Communication leadership 18.8 2.5 18.4 3.8
Trust leadership 21.0** 2.0 20.3 3.2
Respectful leadership 22.0* 2.1 21.4 3.0
Risk leadership 19.9* 2.5 19.3 3.6
Visionary leadership behavior 101.7* 8.4 99.5 14.2
Bottom-line leadership 21.4** 2.4 19.9 3.2
Empowered leadership 19.8** 2.2 18.4 3.1
Long-term leadership 19.6 3.2 19.1 3.7
Visionary leadership characteristics 60.7** 5.9 57.4 8.5
Organizational leadership 21. 8** 2.1 20 . 6 3.8
Cultural leadership 20.4** 2.2 19.7 2.8
Visionary culture buildinq 42.2** 3.6 40.3 6.0
Visionary leadership total score 204.6** 15.6 197.2 26.9
aStandard deviation‘Significant difference when p<0.05 **Significant difference when p<0.01
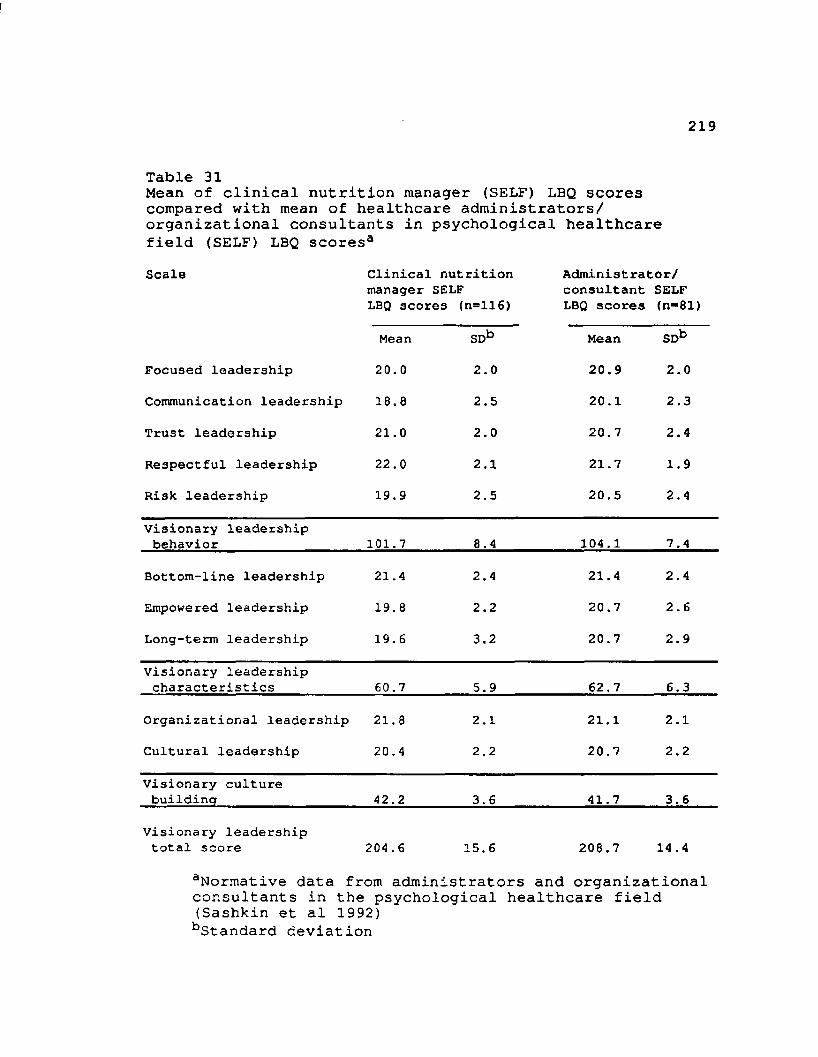
219
Table 31Mean of clinical nutrition manager (SELF) LBQ scores compared with mean of healthcare administrators/ organizational consultants in psychological healthcare field (SELF) LBQ scores3Scale Clinical nutrition
manager SELF LBQ 3core3 (n=116)
Administrator/ consultant SELF LBQ scores (n**81)
Mean SDb Mean SDb
Focused leadership 20.0 2.0 20.9 2.0
Communication leadership 16.8 2.5 20.1 2.3
Trust leadership 21.0 2.0 20.7 2.4
Respectful leadership 22.0 2.1 21.7 1.9
Risk leadership 19.9 2.5 20.5 2.4
Visionary leadership behavior 101.7 8.4 104.1 7.4
Bottom-line leadership 21.4 2.4 21.4 2.4
Empowered leadership 19.8 2.2 20.7 2.6
Long-term leadership 19.6 3.2 20.7 2.9
Visionary leadership characteristics 60.7 5.9 62.7 6.3
Organizational leadership 21.8 2.1 21.1 2.1
Cultural leadership 20.4 2.2 20.7 2.2
Visionary culture buildinq 42.2 3.6 41.7 3.6
Visionary leadership total score 204 .6 15.6 208.7 14.4
aNormative data from administrators and organizational consultants in the psychological healthcare field (Sashkin et al 1992) bStandard deviation
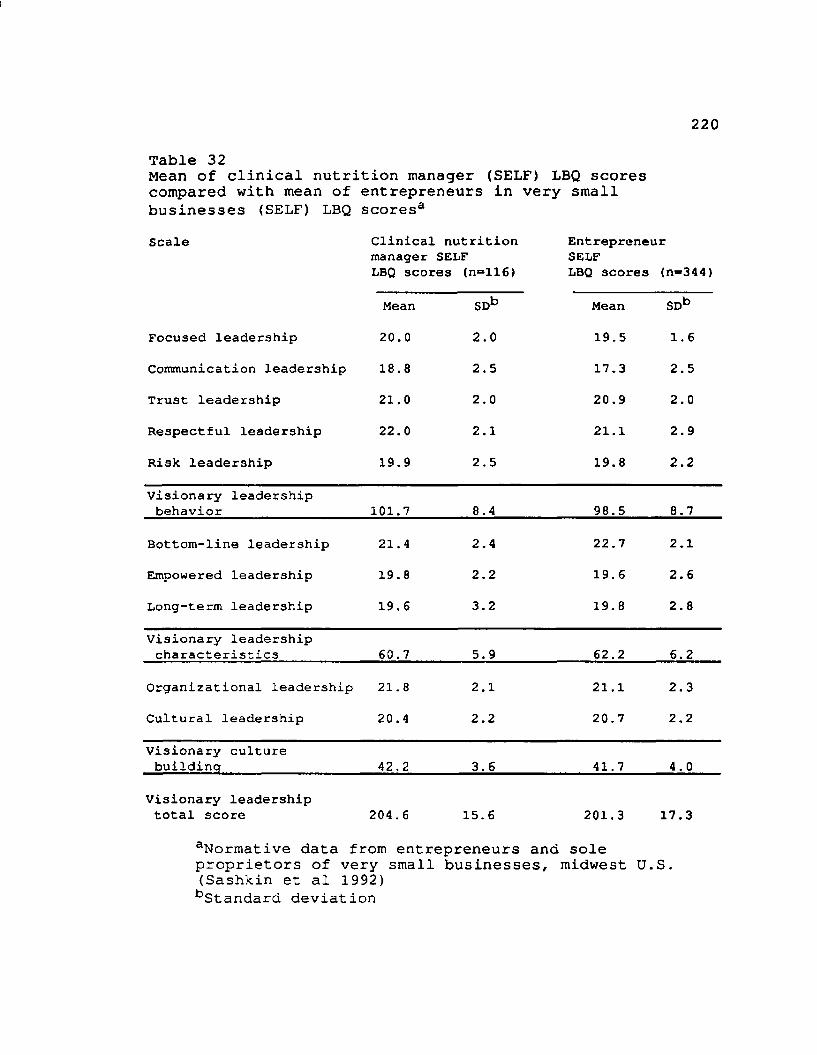
220
Table 32Mean of clinical nutrition manager (SELF) LBQ scores compared with mean of entrepreneurs in very small businesses (SELF) LBQ scores3Scale Clinical nutrition
manager SELF LBQ scores (n=116)
EntrepreneurSELFLBQ scores (n~344)
Mean SDb Mean SDb
Focused leadership 20.0 2.0 19.5 1.6
Communication leadership 18.8 2.5 17.3 2.5
Trust leadership 21.0 2.0 20.9 2.0
Respectful leadership 22.0 2.1 21.1 2.9
Risk leadership 19.9 2.5 19.8 2.2
Visionary leadership behavior 101.7 8.4 98.5 8.7
Bottom-line leadership 21.4 2.4 22.7 2.1
Empowered leadership 19.8 2.2 19.6 2.6
Long-term leadership 19. 6 3.2 19.8 2.8
Visionary leadership characteristics 60.7 5.9 62.2 6.2
Organizational leadership 21. 8 2.1 21.1 2.3
Cultural leadership 20.4 2.2 20.7 2.2
Visionary culture building 42.2 3.6 41.7 4.0
Visionary leadership total score 204.6 15.6 201.3 17.3
Normative data from entrepreneurs and sole proprietors of very small businesses, midwest U.S. (Sashkin et al 1992) bStandard deviation
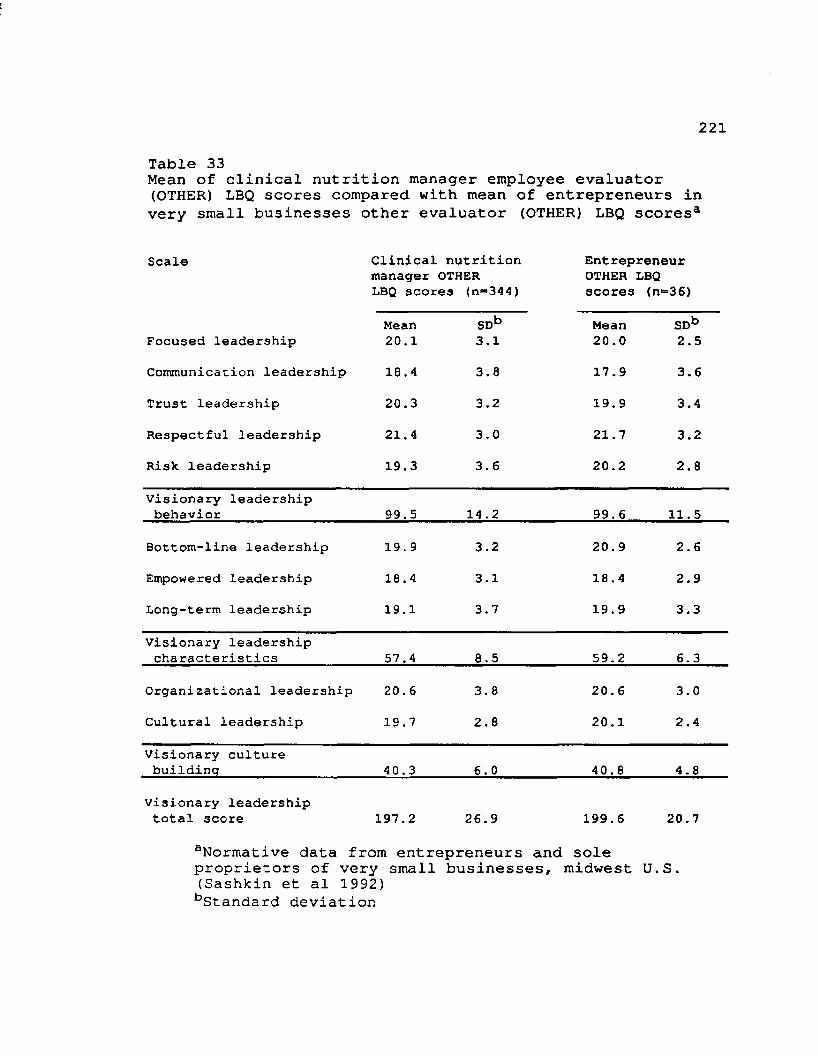
221
Table 33Mean of clinical nutrition manager employee evaluator (OTHER) LBQ scores compared with mean of entrepreneurs in very small businesses other evaluator (OTHER) LBQ scores3
Scale Clinical nutrition manager OTHER LBQ scores <n=344)
Entrepreneur OTHER LBQ scores (n=36)
Focused leadershipMean20.1
SDb3.1
Mean20.0
SDb2.5
Communication leadership 18.4 3.8 17.9 3.6
Trust leadership 20.3 3.2 19.9 3.4
Respectful leadership 21.4 3.0 21.7 3.2
Risk leadership 19.3 3.6 20.2 2.8
Visionary leadership behavior 99.5 14.2 99.6 11.5
Bottom-line leadership 19. 9 3.2 20. 9 2.6
Empowered leadership 18.4 3.1 18.4 2.9
Long-term leadership 19.1 3.7 19.9 3.3
Visionary leadership characteristics 57.4 8.5 59.2 6.3
Organizational leadership 20.6 3.8 20.6 3.0
Cultural leadership 19.7 2.8 20.1 2.4
Visionary culture building 40.3 6.0 40.8 4.8
Visionary leadership total score 197.2 26.9 199.6 20.7
aNormative data from entrepreneurs and sole proprietors of very small businesses, midwest U.S. (Sashkin et al 1992) bStandard deviation
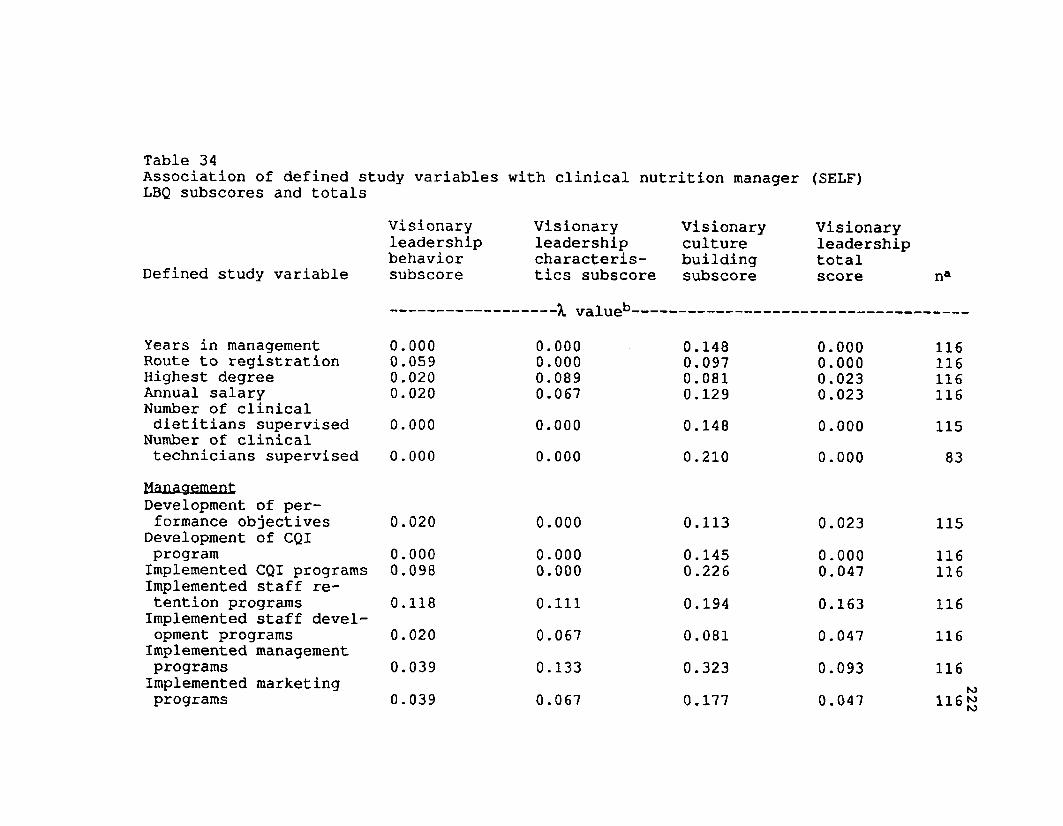
Table 34Association of defined study variables LBQ subscores and totals
Visionaryleadershipbehavior
Defined study variable subscore
Years in management 0.000Route to registration 0.059Highest degree 0.020Annual salary 0.020Number of clinical dietitians supervised 0.000
Number of clinical technicians supervised 0.000Management Development of performance objectives 0.020
Development of CQI program 0.000Implemented CQI programs 0.098Implemented staff retention programs 0.118Implemented staff development programs 0.020Implemented management programs 0.039Implemented marketing programs 0.039
with clinical nutrition manager (SELF)
Visionary leadership characteristics subscore
Visionaryculturebuildingsubscore
Visionaryleadershiptotalscore
valueb-0.0000.0000.0890.067
0.0,0,0,
148097081129
0.0000.0000.0230.023
0.0000.000
0.1480.210
0.0000.000
0.000 0.113 0.0230.000 0.145 0.0000.000 0.226 0.0470.111 0.194 0.1630.067 0.081 0.0470.133 0.323 0.0930.067 0.177 0.047
na
11611611611611583
115116 116116116116116
222
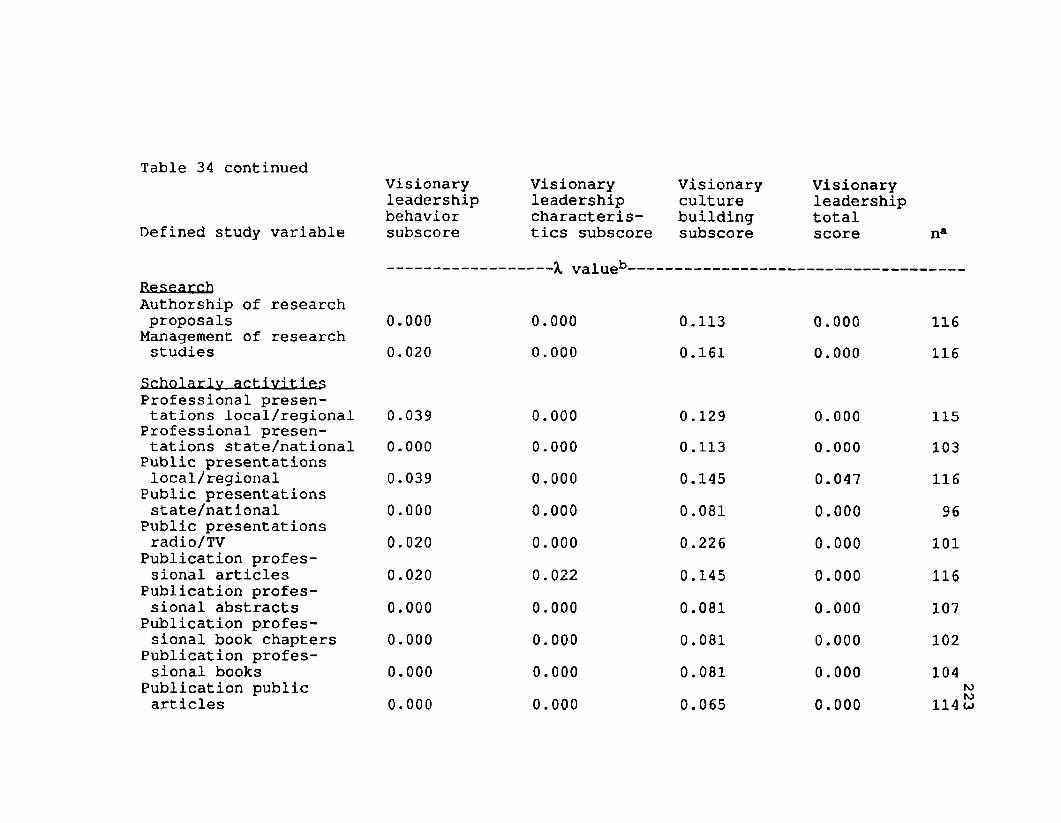
Table 34 continuedVisionaryleadershipbehavior
Defined study variable subscore
ResearchAuthorship of research proposals 0.000
Management of research studies 0.020
Scholarly activities Professional presentations local/regional 0.039
Professional presentations state/national 0.000
Public presentations local/regional 0.039
Public presentations state/national 0.000
Public presentations radio/TV 0.020
Publication professional articles 0.020
Publication professional abstracts 0.000
Publication professional book chapters 0.000
Publication professional books 0.000
Publication public articles 0.000
Visionary leadership characteristics subscore
X valueb--
0.0000.000
0.0000.0000.0000 . 0 0 0
0 . 0 0 0
0 . 0 2 2
0 . 0 0 0
0 . 0 0 0
0 . 0 0 0
0.000
Visionaryculturebuildingsubscore
0.1130.161
0.1290.1130.1450.0810.2260.1450.0810.0810.0810.065
Visionaryleadershiptotalscore
0.0000.000
0.0000.0000.0470.0000.0000.0000.0000.0000.0000.000
na
116116
115103116 96
101116107102104 114
223
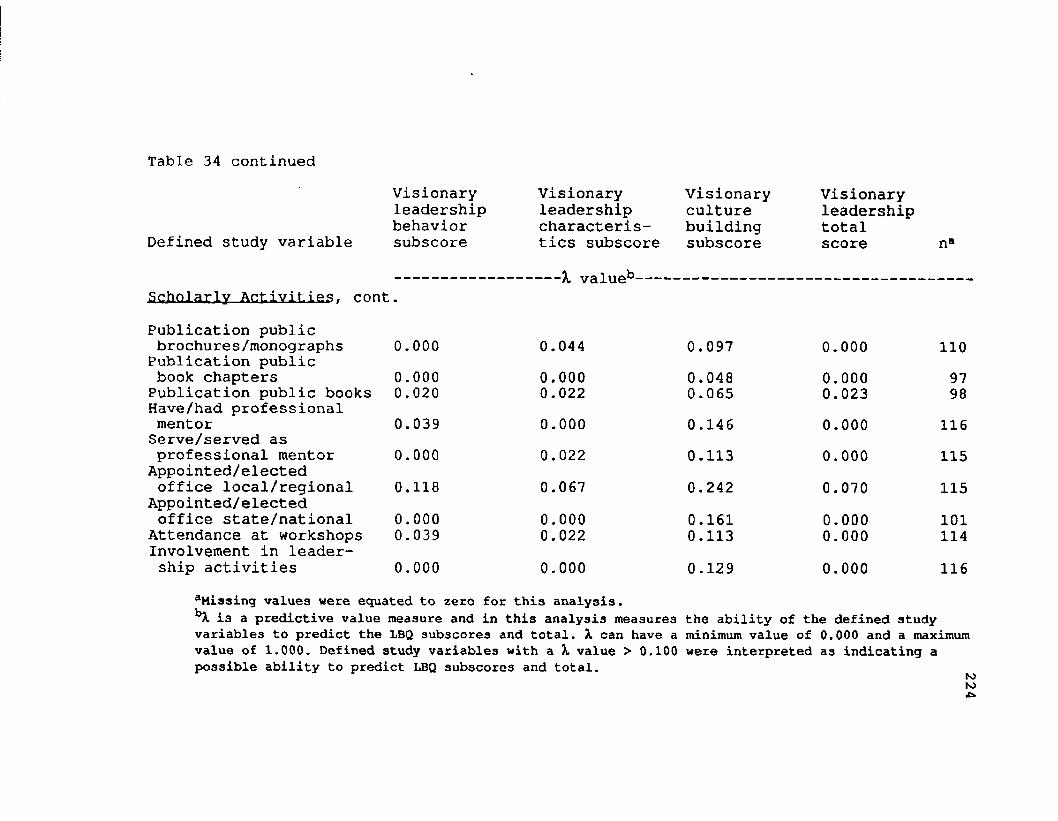
Table 34 continued
Defined study variable
Visionaryleadershipbehaviorsubscore
Visionary leadership characteristics subscore
Visionaryculturebuildingsubscore
Visionaryleadershiptotalscore n*
-X valueb-Scholarly Activities, contPublication public brochures/monographs 0.000 0.044 0.097 0.000 110Publication public book chapters 0.000 0.000 0.048 0.000 97Publication public books 0.020 0.022 0.065 0.023 98Have/had professional mentor 0.039 0.000 0.146 0.000 116Serve/served as professional mentor 0.000 0.022 0.113 0.000 115
Appointed/elected office local/regional 0.118 0.067 0.242 0.070 115
Appointed/elected office state/national 0.000 0.000 0.161 0.000 101
Attendance at workshops 0.039 0.022 0.113 0.000 114Involvement in leadership activities 0.000 0.000 0.129 0.000 116
aMiasing values were equated to zero for this analysis.bX is a predictive value measure and in this analysis measures the ability of the defined study variables to predict the LBQ subscores and total. X can have a minimum value of 0.000 and a maximum value of 1 .0 0 0 . Defined study variables with a X value > 0.100 were interpreted as indicating a possible ability to predict LBQ subscores and total. toto•c>
APPENDIX F FIGURES
225
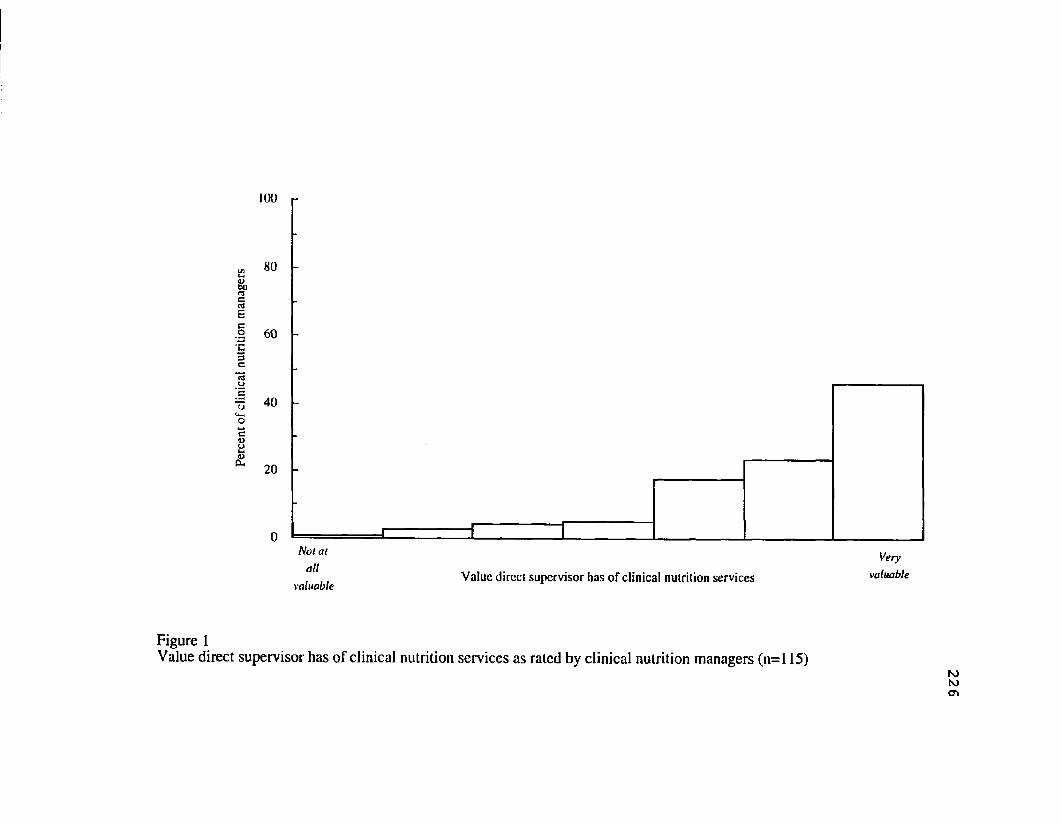
Notal Very
, ,, Value direct supervisor has of clinical nutrition services valuablevaluable
Figure 1Value direct supervisor has o f clinical nutrition services as rated by clinical nutrition managers (n=l 15)
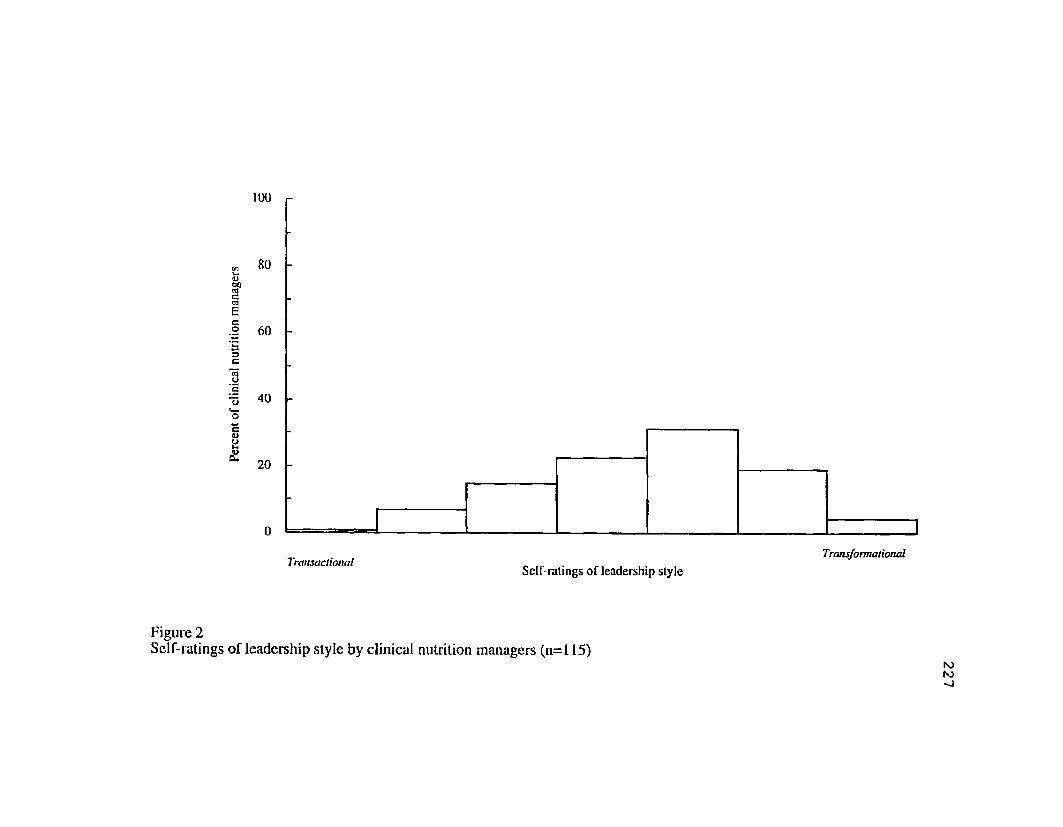
100
80
.2 60 '53clCJr, 40eu2ua. 20
TransactionalTransformational
Self-ratings ofleadership style
Figure 2Self-ratings ofleadership style by clinical nutrition managers (n=115) 227
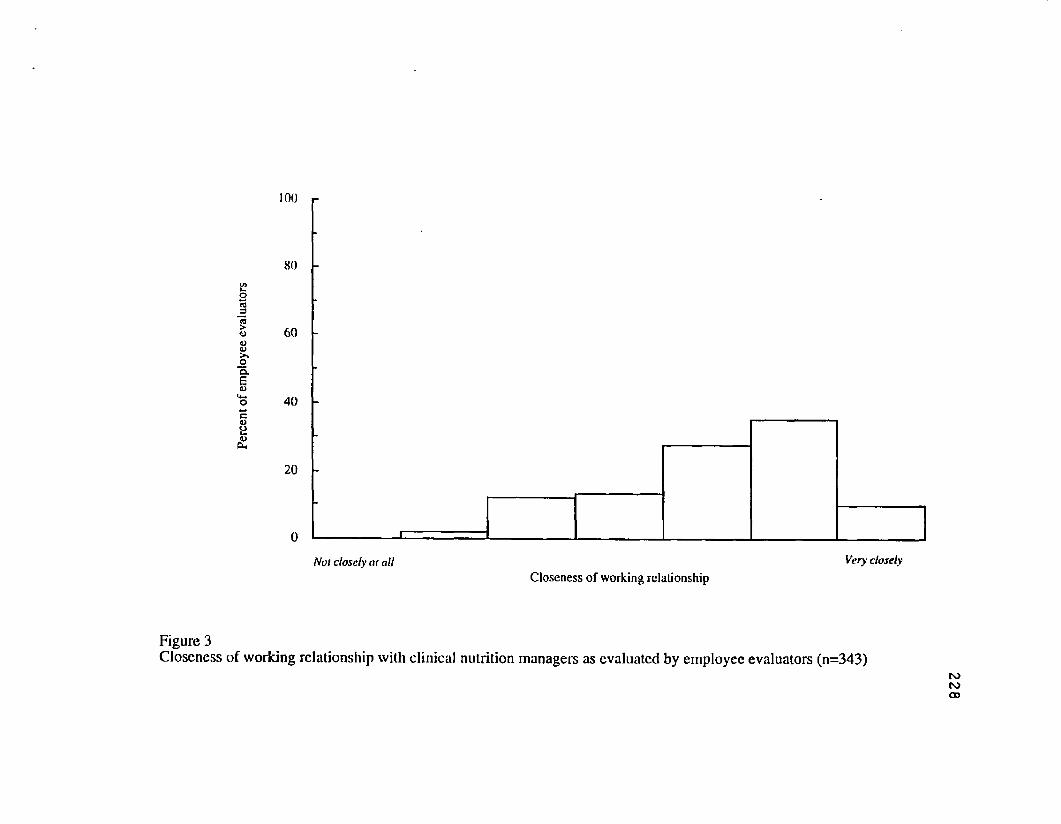
100
80oj3>CJUCJ>%O
60
cua£X
40
20
Not closely at all Very closelyCloseness of working relationship
Figure 3Closeness o f working relationship with clinical nutrition managers as evaluated by employee evaluators (n=343)
228
PLEASE NOTE
Copyrighted materials in this document have not been filmed at the request of the author. They are available for consultation, however,
in the author’s university library.
229-230,Triangle diagram and profiles for the
LBQ instrument
University Microfilms International
LIST OF REFERENCES
The American Dietetic Association. Achieving Competitive Advantage Strategic Thinking Initiative. Chicago, IL:The American Dietetic Association; 1992.The American Dietetic Association. Position of The American Dietetic Association: Management of health care food and nutrition services. Journal of the American Dietetic Association. 1993; 93: 914-915.Avolio BJ, Waldman DA, Einstein WO. Transformational leadership in a management simulation: Impacting thebottom line. Group and Organization Studies. 1988; 13:59-80.Bales RF. Task roles and social roles in problem-solving groups. In Maccoby EE, Newcomb TM, Harley EL, eds. Readings in Social Psychology. 3rd ed. New York, NY:Holt, Rinehart & Winston; 1958.Barker AM. Transformational Nursing Leadership. A Visionfor the Future. Baltimore, MD: Williams & Wilkins; 1990.Bass BM. Bass & Stoodill's Handbook of Leadership.Theory. Research & Managerial Applications. 3rd ed. New York, NY: The Free Press; 1990.Bass BM. Leadership and Performance Bevond Expectations. New York, NY: Free Press, 1985;Bass BM, Avolio BJ. Transformational Leadership Development., Manual for the Multifactor Leadership Questionnaire . Palo Alto, CA: Consulting Psychologists Press,Inc; 1990.Bass BM, Waldman DA, Avolio BM, Bebb M. Transformational leadership and the falling dominoes effect. Group and Organization Studies. 1987; 12:73-87.Bass BM, Yammarino FJ. Forecasting Transformational Leadership Among Naval Academy Midshipmen and Graduates.
231
232Annual Report No. 88-1. Binghamton, NY: State Universityof New York, Center for Leadership Studies; 1988.Bennis WG. The four competencies of leadership. Training and Development Journal. 1984; 38:15-18.Bennis WG, Nanus B. Leaders. The Strategies for TakingCharge. New York, NY: Harper & Row; 1985.Bernard LL. An Introduction to Social Psychology. New York, NY: Holt; 1926.Bernard LA and Walsh M. Leadership the Key to Professionalization of Nursing. St. Louis, MO: The C.V. MosbyCompany; 1990.Bingham WV. Leadership. In Metcalf H.C. The Psychological Foundations of Management. New York, NY: Shaw; 1927.Bird C. Social Psychology. New York, NY: Appleton-Century, 1940.Blake RR, Mouton JS. The Managerial Grid. Houston, TX: Gulf Publishing Company; 1964.Boudreaux LJ, Shanklin CW, Johnson JT. Factors influencing success of dietitians employed in business and industry. Journal of The American Dietetic Association. 1991; 91:1227-1232.Bradley RT, Young WY, Ebbs P, Martin J. Characteristics of advanced-level dietetics practice: A model and empirical results. Journal of The American Dietetic Association. 1993; 93:196-202.Brown LM, Fruin MF. Management activities in community dietetics practice. Journal of The American Dietetic Association. 1989; 89:373-377.Brown MB. 4F Program. In Dixon WJ, ed. BMDP Statistical Software Manual Volume 1. Berkeley, CA: University of California Press, 1990.Burke JP, DePoy E. An emerging view of mastery, excellence, and leadership in occupational therapy practice.The American Journal of Occupational Therapy. 1991;45:1027-1032.Burns JM. Leadership. New York, NY: Harper and Row; 1978.
233Calvert S, Parish HY, Oliver K. Clinical dietetics:Forces shaping its future. Journal of The American Dietetic Association. 1982; 80:350-354.Clark KE, Clark MB, eds. Measures of Leadership. West Orange, NJ: Leadership Library of America, Inc; 1990.Clark KE, Clark MB, Campbell DP, eds. Impact of Leadership . Greensboro, NC: Center for Creative Leadership;1992.Clark Wilson Publishing Company. Task Cycle Update.Silver Spring, MD: Clark Wilson Publishing Company; 1992.Crowne DP, Marlowe D. A new scale of social desirability independent of psychopathology. Journal of Consulting Psychology. 1960; 14:349-354.Day DV, Lord RG. Executive leadership and organizational performance: Suggestions for a new theory and methodology. Journal of Management. 1988; 14:453-464.Deal TE, Peterson KD. The Principal's Role in Shaping School Culture. Washington, DC: U.S. Government PrintingOffice; 1990.Dixon WJ, ed. BMDP Statistical Software Manual Volume 1. Berkeley, CA: University of California Press, 1990.Dobbins GH, Platz SJ, Sex differences in leadership: Howreal are they? Academy of Management Review. 1986;11:118-127.Dodd J. The leadership challenge. Journal of The American Dietetic Association. 1992a; 92:225-226.Dodd J. The words of leadership. Journal of The American Dietetic Association. 1992b; 92:1006.Dow TE. The theory of charisma. Sociological Quarterly.1969; 10:306-18.Dowd J. Control in Human Societies. New York, NY:Appleton-Century; 1936.Dowling RA, Lafferty LJ, McCurley M. Credentials and skills required for hospital food and nutrition department directors. Journal of The American Dietetic Association. 1990; 90:1535-1540.
234Downton JV. Rebel Leadership:__ Commitment and Charisma Inthe Revolutionary Process. New York, NY: Free Press;1973.Dunham J, Klafehn K. Transformational leadership and the nurse executive. Journal of Nursing Administration.1990; 20:28-34.Dunham M, Fisher E. Nurse executive profile of excellent nursing leadership. Nursing Administration Quarterly. 1990; 15:1-8.Endeman JL. Leadership and culture: Superintendents anddistricts. Paper presented at the annual meeting of the American Educational Research Association, Boston, MA, April 1990.Fiedler FE. A Theory of Leadership Effectiveness. New York, NY: McGraw-Hill; 1967.Fiedler FE, Chemers MM. Leadership and Effective Management . Glenview, IL: Scott Foresman; 1974.Finn SC. The decade of the dietitian: Leadership canmake it happen. Topics in Clinical Nutrition. 1991; 6:1— 7.Finn SC, Dodd J. President's page: Institute for Professional Enhancement positions tomorrow's leaders. Journal of The American Dietetic Association. 1993; 93:916.Finn SC, Foltz MB, Ryan AS. Image and role of the consultant dietitian in long-term care: Results from a survey of three midwestern states. Journal of The American Dietetic Association. 1991; 91 (7) :788-792.Fleishman EA. Leadership Climate and Supervisory Behavior. Personnel Research Board. Columbus, OH: OhioState University; 1951.Fleishman EA. The description of supervisory behavior. Journal of Applied Psychology. 1953; 37:1-6.Garrett BH. The relationship among leadership preferences, head nurse leader style, and job satisfaction of staff nurses. Journal of the American Nurses Association. 1991; 22:11-14.
235Gevedon SL. Leadership behaviors of deans of top ranked schools of nursing. Journal of Nursing Education. 1992; 31:221-224.Ghiselli E. Explorations in Managerial Talent. Pacific Palisades, CA: Goodyear Publishing Co; 1971.Gibb CA. The principles and traits of leadership. Journal of Abnormal and Social Psychology. 1947; 42:267-284.Gilbert MA. Personality profiles and leadership potential of medical-surgical and psychiatric nursing graduate students. Nursing Research. 1975; 24:125-130.Goldenberg D. Nursing education leadership. Effect of situational and constraint variables on leadership style. Journal of Advanced Nursing. 1990; 15:132 6-1334.Gluck M, Charter R. Personal qualities of nurses implying need for continuing education to increase interpersonal and leadership effectiveness. The Journal of Continuing Education in Nursing. 1980; 11:29-36.Halpin AW, Winer BJ. A factorial study of the leader behavior descriptions. In Stogdil RM, Coons AE, eds. Leader Behavior, Its Description and Measurement.Columbus, OH: Ohio State University, Bureau of BusinessResearch; 1957.Hanson HA, Chater S. Role selection by nurses: managerial interests and personal attibutes. Nursing Research. 1983; 32:48-52.Hater JJ, Bass BM. Superiors' evaluations and subordinates' perceptions of transformational and transactional leadership. Journal of Applied Psychology. 1988; 73:695- 702.Hersey P, Blanchard KH. Management of Organizational Behavior: Utilizing Human Resources. 3rd ed. Englewood Cliffs, NJ: Prentice-Hall; 1977.Hersey P, Blanchard KH. Management of OrganizationalBehavior; utilizing Human Resources. 4 th ed. EnglewoodCliffs, NJ: Prentice-Hall; 1982.Hersey P, Blanchard KH, Hambleton R. Leadership Stvle Analysis— Self and Other. Amherst, MA: Center forLeadership Studies and Psychometric and Evaluative Research Services; 1979,
236
Herzberg F. Work and the Nature of Man. New York, NY: World Publishing; 1966.Hoover LW. Enhancing managerial effectiveness in dietetics. Journal of the American Dietetic Association. 1983; 82:58-61.House RJ. Leadership research: Some forgotten, ignored,or overlooked findings. In Hunt JG, Baliga BR, Dachler HP, Schriesheim CA, eds. Emerging Leadership Vistas. Lexington, MA; Lexington Books; 1988.House RJ. A 1976 theory of charismatic leaderhip. InHunt JG, Larson LL, eds. Leadership; The Cutting Edge.Carbondale, IL: Southern Illinois University Press; 1977.House RJ. A path goal theory of leadership effectiveness. Administrative Science Quarterly. 1971; 16:321-338.Howell JM, Avolio BJ. Locus of Control Leadership and Support for Innovation: Key Predictors of Business UnitPerformance. Unpublished manuscript; 1989.Howell JM, Higgins CA. Champions of technological innovation. Administratrive Science Quarterly. 1990; 35:317-341.Huenemann RL. Leadership and quality in nutritional care: our role in today's world. Journal of the American Dietetic Association. 1981; 78:124-128.Human Synergistics. Life Styles Inventory-Level I:__Self-Development Guide. Plymouth, MI: Human Synergistics;1987.Inderrieden EJ, Nosse LJ, Allen DE. An investigation of managerial characteristics of health care managers: Acomparison study. Journal of Allied Health. 1987;August:237-24 6.Jago AG. Leadership: Perspectives in theory andresearch. Management Science. 1982; 28:315-336.Jaques E. A General Theory of Bureaucracy. London, UK: Heinemann; 1976.Jaques E. The development of intellectual capability. Journal of Applied Behavioral Science. 1986; 22:361-383.
237Jenkins WO. A review of leadership studies with particular reference to military problems. Psychological Rnl1etin. 1947; 44:54-79.Keller RT. Transformational leadership and the performance of research and development groups. Journal of Management■ 1992; 18:489-501.Kilbourne CE. The elements of leadership. Journal of Coast Artillery. 1935; 78:437-439.Kirk D, Shanklin CW, Gorman, MA. Attributes and qualifications that employers seek when hiring dietitians in business and industry. Journal of The American Dietetic Association. 1989; 89:494-498.Komives SR. Gender differences in the relationship of hall directors' transformational and transactional leadership and achieving styles. Journal of College Student Development. 1991; 32:155-165.Kotter JP. A Force for Change. How Leadership Differs From Management. New York, NY: The Free Press; 1990, 4-5.Kouzes JM, Posner BZ. The Leadership Challenge. How to Get Extraordinary Things Done in Organizations. San Francisco, CA: Jossey-Bass Publishers; 1991.Lamastro JA, Fortin-Crosby P. An analysis of the managerial roles of the chief of physical therapy services.1980; AART. Spring:17-19.Larson LL, Hunt JG, Osborn RN. The great hi-hi leader behavior myth: A lesson from Occam's Razor. Academy ofManagement Journal. 1976; 19:628-641.Likert R. The Human Organization:__ Its Management andValues. New York, NY: McGraw Hill; 1967.Lipman-Blumen J, Leavitt HJ. L-BLA Achievement Styles Inventory, Form 13. Bethesda, M D : L-BLA Associates;1979.Major KD. Dogmatism. Visionary Leadership and Effectiveness of Secondary Principals. Unpublished doctoral dissertation, University of la Verne, California; 1988.Mandel ED, Garey JG. Perception of power among dietitians. Journal of the American Dietetic Association. 1993; 93: 423-428.
238
Maslow A. A theory of motivation. Psychology Review. 1943; 50:370-396.McClelland D. The Achieving Society. Princeton, NJ:D. VanNostrand Company, Inc. 1961.McClelland DC. Power:__The Inner Experience. New York,NY: Irvington; 1975.McClelland DC, Burnham DH. Power is the great motivator. Harvard Business Review. 1976; 54:100-110.McCloskey JC, Molen MT. Leadership in nursing. Annual Reviews in Nursing Research. 1987; 5:177-202.McDaniel C, Wolf GA. Transformational leadership in nursing services, a test of theory. Journal of Nursing Administration. 1992; 22:60-65.McGregor D. The Human Side of Enterprise. New York, NY: World Publishing; 1966.Meighan MM. The most important characteristics of nursing leaders. Nursing Administration Quarterly. 1990; 15:63- 39 .Mueller MJ, Rose SJ. Physical therapy director as professional value setter. Physical Therapy. 1987; 62:1389- 1392.Murphy AJ. A study of the leadership process. American Sociological Review. 1941; 6:674-687.Nestle M. Leadership in clinical dietetics: Meeting thechallenge to roles in nutrition support. Journal of the American Dietetic Association. 1984; 84:134 9-1353.Nettles MF, Gregoire MB, Partlow CG. Relevance of competencies to graduate education and experience in food- service management. Journal of the American Dietetic Association. 1993; 93:877-880.Niehoff BP, Enz CA, Grover RA. The impact of top management actions on employee attitudes and perceptions. Group and Organization Studies. 1990; 15:337-352.Nielson SK. Administration: Getting the right thingsdone. Social Work Health Care. 1989; 12:59-69.
239Nyland NK, Spears MC, Myers EF. Activities of coordinated dietetic program directors compared by educational background. Journal of The American Dietetic Association. 1989; 89:1822-1826.Oberg W. Charisma, commitment, and contemporary organization theory. Business Topics. 1972; 20:18-31.Onnen M K . The Relationship of Clergy and Leadership Characteristics to Growing or Declining Churches. Unpublished doctoral dissertation, University of Louisville,KY; 1987.Ouchi W G . How American Business Can Meet the Japanese Challenge. Reading, MA: Addison-Wesley; 1981.Page DP. Measurement and prediction of leadership. American Journal of Sociology. 1935; 41:31-42.Parks SC, Kris-Etherton PM. Practitioners view dietetic roles for the 1980s. Journal of The American Dietetic Association. 1982; 80:574-576.Parrett EE, Hurd PD, Northcraft G, McGhan WF, Bootman JL. Leadership styles of hospital pharmacy directors. American Journal of Hospital Pharmacy. 1985; 42:1069-1073.Parsons T. Structure and Process in Modern Societies. New York, NY: Free Press; 1960.Posner BZ, Kouzes JM. Development and validation of the Leadership Practices Inventory. Educational and Psychological Measurement. 1988; 48:483-496.Posner BZ, Kouzes JM. Leadership practices: An alternative to the psychological perspective. In Clark KE, Clark MB, eds. Measures of Leadership. West Orange, NJ: Leadership Library of America, Inc; 1990.Rinke WJ, Finn SC. Winning strategies to excel in dietetics. Journal of The. ■American Dietetic Association. 1990; 90:935-938.Rosener JB, McAllister DJ, Stephens GK. Leadership Study. International Women's Forum. Unpublished report from the University of California, Irvine Graduate School of Management; 1990.
240Runciman WG. Charismatic legitimacy and one-party rule in China. Archives Europeenes de Sociologic. 1963; 4:148- 65.Ryan AS, Foltz MB, Finn SC. The role of the clinical dietitian: I. Present professional image and recent image changes. Journal of The American Dietetic Association. 1988; 88(6):671-676.SAS Technical Report P-229. SAS/STAT Software: Changes and Enhancements. Release 6107. Cary, NC: SAS Institute, Inc; 1992 .Sashkin M. The structure of charismatic leaderhip. InHunt JG, Larson LL, eds. Leadership:__The Cutting Edge.Carbondale, IL: Southern Illinois University Press; 1977.Sashkin M. The Visionary Leader. Leader Behavior Questionnaire. 3rd ed. (SELF). King of Prussia, PA: Organization Design and Development, Inc; 1990a.Sashkin M. The Visionary Leader Trainer Guide, 3rd ed. King of Prussia, PA: Organization Design and Development,Inc; 1990b.Sashkin M, Burke WW. Understanding and assessing organizational leadership. In Clark KE, Clark MB, eds. Measures of Leadership. West Orange, NJ: Leadership Library ofAmerica, Inc; 1990; 297-326.Sashkin M, Rosenbach WE, Deal TE, Peterson K D . Assessing transformational leadership and its impact. In Clark KE, Clark MB, Campbell DP. Impact of Leadership. Greensboro, NC: Center for Creative Leadership; 1992; 131-148.Sashkin M, Sashkin MG. Leadership and culture building in schools: Quantitative and qualitative understandings.Paper presented at the annual meeting of the American Educational Research Association, Boston, MA, April 1990.Schein EH. Organizational Culture and Leadership:__&Dynamic View. San Francisco, CA: Jossey-Bass; 1985.Schiller MR, Foltz MB, Campbell S. Dietitians' selfperceptions: Implications for leadership. Journal ofThe American Dietetic Assoctiation. 1993; 93:868-876.Seal MJ, Spears MC, Vaden AG, Hoyt DP. Graduate education in food service systems management: Clarifying the focus.
241Journal of The American Dietetic Association. 1983;83:661-663.Seltzer JA, Bass BM. Transformational leadership: Beyondinitiation and consideration. Journal of Management.1990; 16:693-703.Seltzer J, Numerof RA. Exploring the effects of leadership behavior and task characteristics on burnout in a healthcare center. Journal of Health and Human Resources Administration. 1990; 13:155-165.Shils EA. Charisma, order, and status. American Sociological Review. 1965; 30:199-213,Singer MS. Transformational vs transactional leadership:A study of New Zealand company managers. Psychological Reports. 1985; 57:143-146.Singer MS, Singer A E . Relation between transformational vs transactional leadership preference and subordinates' personality: an exploratory study. Perceptual and MotorSkills. 1986; 62:775-780.Snyder JR, Schiller MR, Smith JL. A comparison of career- entry administrative competencies with skills required in practice: Implications for continuing education. Journalof The American Dietetic Association. 1985; 85:934-938.Sorrentino EA, Nalli B, Schriesheim C. The effect of head nurse behaviors on nurse job satisfaction and performance. Hospital and Health Services Administration. 1992;37:103-113.Spangler WD, Braiotta L. Leadership and corporate audit committee effectiveness. Group and Organization Studies. 1990; 15:134-157.Stein F. Anatomy of Research in Allied Health. New York, NY: John Wiley & Sons; 1980.Stogdill RM. Handbook of Leadership: A Survey of Theoryand Research. New York, NY: Free Press, 1974.Stogdill RM. Manual for the Leader Behavior Description Questionnaire Form XII. Columbus, OH: Ohio StateUniversity, 1963.
242Stogdill RM. Personal factors associated with leadership: A survey of literature. Journal of Psychology. 1948; 25:35-71.Stoner-Zemel MJ. Visionary Leadership. Management, and Hlah Performance Work Units. Unpublished doctoral dissertation, University of Massachusetts; 1988.Task Cycle Update. Silver Spring, MD: Clark WilsonPublishing Company; 1992.Tead 0. The Art of Leadership. New York, NY: McGraw-Hill; 1935.Uliss D. What leadership style best suits critical care nurses? Nursing Management. 1991; 22:56D-P.Vroom VH, Yetton PW. Leadership and Decision-making. Pittsburgh, PA: University of Pittsburgh Press; 1973.Waldman DA, Bass BM, Einstein WO. Leadership and outcomes of the performance appraisal process. Journal of Occupational Psychology. 1987; 60, 177-186.Wattenberg SH, Orr MM, O'Rourke TW. Comparison of opinions of social work administrators and hospital administrators toward leadership tasks. Social Work in Health Care. 1977; 2:285-293.Weber M. The Theory of Social and Economic Organization. Henderson AM, Parsons T, trans; Parsons T. ed. New York, NY: Free Press; 1947. (Original work published in 1924.)White RK, Lippit R. Autocracy and Democracy: An Experimental Inquiry. New York, NY: Harper; 1960.Wilson CL, O'Hare D, Shipper F. Task cycle theory: Theprocesses of influence. In Clark KE, Clark MB, eds. Measures of Leadership. West Orange, N J : LeadershipLibrary of America, Inc; 1990.Wylie-Rosett J, Wheeler M, Krueger K, Halford B. Opportunities for research-oriented dietitians. Journal of the American Dietetic Association. 1990; 90:1531-1534.Yammarino FJ, Bass BM. Long-term forecasting of transformational leadership and its effects among naval officers: Some preliminary findings. In Clark KE, Clark MB, eds. Measures of Leadership. West Orange, NJ: LeadershipLibrary of America, Inc; 1990.
243
Yammarino F, Bass BM. Transformational leadership and multiple levels of analysis. Human Relations. 1990; 43:975-995.Yates SC, Shanklin CW, Gorman MA. Competencies of food- service directors/managers required in health care operations. Journal of The American Dietetic Association. 1987; 87:1636-1643.Young SW. Educational experiences of transformational nurse leaders. Nursing Administration Quarterly. 1992; 17:25-33.
Related Documents











