Review ArticleTransumbilical laparoendoscopic single-site surgery in urology John E Humphrey and David Canes Department of Urology,Tufts University School of Medicine, Lahey Clinic Institute of Urology, Burlington, Massachusetts, USA Abbreviations & Acronyms CL = conventional laparoscopy DVT/PE = deep venous thrombosis/pulmonary embolus EBL = estimated blood loss E-NOTES = embryonic natural orifice transumbilical endoscopic surgery Lap = laparoscopic LESS = laparoendoscopic single-site surgery LOS = length of hospital stay MAG3 = technetium-99m mercaptoacetyltriglycine MOT = mean operative time OPUS = one port umbilical surgery SIL = single incision laparoscopy SILS = single port laparoscopy SPA = single port access SPL = single port laparoscopy Correspondence: David Canes M.D., Department of Urology, Tufts University School of Medicine, Lahey Clinic Institute of Urology, 41 Mall Road, Burlington, MA 01805, USA. Email: [email protected] Received 18 October 2011; accepted 4 January 2012. Online publication 15 February 2012 Abstract: Laparoendoscopic single-site surgery has seen a dramatic rise in the uro- logical community. With the advent of new techniques and instrumentation, laparoen- doscopic single-site surgery has become more accessible for a wide variety of applications. The majority have been carried out through a transumbilical incision in order to effectively hide the scar within the umbilicus. Here, we review the history and clinical applications for transumbilical laparoendoscopic single-site surgery within urology. The current scope is broad, and great strides have been made, but the overall benefit appears to be predominantly cosmetic. Diffusion of laparoendoscopic single-site surgery techniques from tertiary referral centers to the community urologist remains unknown. This review demonstrates the feasibility of transumbilical laparoendoscopic single-site surgery as shown in the urological literature. Key words: laparoendoscopic single-site surgery, minimally invasive, review, transumbilical. Introduction Rise of minimally invasive surgery Single-port surgery, like many advances in medicine, is the result of constant fine-tuning of prior techniques, and questioning how they can be improved on. The initial impetus driving towards minimally invasive surgery was the morbidity from an open laparotomy incision. The pain, recovery time and inherent wound complications, such as infection and incisional hernias, as well as the cosmetic nature of open surgery drove us to push the field towards laparoscopic surgery, and subsequently its robotic counterpart. The subsequent evolution of technique, ability and technology has led to the development of transumbilical single-port surgery. This is thought to be the next natural step in accomplishing safe, effective proce- dures while limiting the morbidity and cosmetic consequences of large and/or several incisions. Assumptions that surgical morbidity is simply linearly related to the sum-total of incision length(s), however, have not held under scrutiny in the past.The present review is focused on the urological experience with single-port surgery specifically using a transumbilical approach. The umbilicus provides a location in which the resultant scar can be at least partially hidden from view, enhancing the benefit of improved cosmesis with single-port surgery. The application of transumbilical single-port surgery in urology is ever growing, and herein we describe the worldwide use of this technique to date. The term now used to describe single-port surgery in the urological literature is LESS. This was developed to incorporate and standardize the various previous terms used to describe one overall concept of minimally invasive operations performed through a single incision using conventional laparoscopic or newer instrumentation such as fixed pre-bent or deflectable flexible instruments. 1 Previous terms included E-NOTES, SILS, OPUS, SPA, SPL and SIL, among others. The first transumbilical urological LESS procedure described was by Raman et al. where three nephrectomies were carried out, each using a single incision with multiple trocars. 2 Since that time, the clinical experience has increased International Journal of Urology (2012) 19, 416–428 doi: 10.1111/j.1442-2042.2012.02963.x 416 © 2012 The Japanese Urological Association

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

Review Articleiju_2963 416..428
Transumbilical laparoendoscopic single-site surgeryin urologyJohn E Humphrey and David CanesDepartment of Urology, Tufts University School of Medicine, Lahey Clinic Institute of Urology, Burlington, Massachusetts, USA
Abbreviations & AcronymsCL = conventionallaparoscopyDVT/PE = deep venousthrombosis/pulmonaryembolusEBL = estimated blood lossE-NOTES = embryonicnatural orificetransumbilical endoscopicsurgeryLap = laparoscopicLESS = laparoendoscopicsingle-site surgeryLOS = length of hospitalstayMAG3 = technetium-99mmercaptoacetyltriglycineMOT = mean operativetimeOPUS = one port umbilicalsurgerySIL = single incisionlaparoscopySILS = single portlaparoscopySPA = single port accessSPL = single portlaparoscopy
Correspondence: David CanesM.D., Department of Urology,Tufts University School ofMedicine, Lahey Clinic Instituteof Urology, 41 Mall Road ,Burlington, MA 01805, USA.Email: [email protected]
Received 18 October 2011;accepted 4 January 2012.Online publication 15 February2012
Abstract: Laparoendoscopic single-site surgery has seen a dramatic rise in the uro-logical community. With the advent of new techniques and instrumentation, laparoen-doscopic single-site surgery has become more accessible for a wide variety ofapplications. The majority have been carried out through a transumbilical incision inorder to effectively hide the scar within the umbilicus. Here, we review the history andclinical applications for transumbilical laparoendoscopic single-site surgery withinurology. The current scope is broad, and great strides have been made, but the overallbenefit appears to be predominantly cosmetic. Diffusion of laparoendoscopic single-sitesurgery techniques from tertiary referral centers to the community urologist remainsunknown. This review demonstrates the feasibility of transumbilical laparoendoscopicsingle-site surgery as shown in the urological literature.
Key words: laparoendoscopic single-site surgery, minimally invasive, review,transumbilical.
Introduction
Rise of minimally invasive surgery
Single-port surgery, like many advances in medicine, is the result of constant fine-tuning ofprior techniques, and questioning how they can be improved on. The initial impetus drivingtowards minimally invasive surgery was the morbidity from an open laparotomy incision.The pain, recovery time and inherent wound complications, such as infection and incisionalhernias, as well as the cosmetic nature of open surgery drove us to push the field towardslaparoscopic surgery, and subsequently its robotic counterpart. The subsequent evolution oftechnique, ability and technology has led to the development of transumbilical single-portsurgery. This is thought to be the next natural step in accomplishing safe, effective proce-dures while limiting the morbidity and cosmetic consequences of large and/or severalincisions.
Assumptions that surgical morbidity is simply linearly related to the sum-total of incisionlength(s), however, have not held under scrutiny in the past. The present review is focusedon the urological experience with single-port surgery specifically using a transumbilicalapproach. The umbilicus provides a location in which the resultant scar can be at leastpartially hidden from view, enhancing the benefit of improved cosmesis with single-portsurgery. The application of transumbilical single-port surgery in urology is ever growing,and herein we describe the worldwide use of this technique to date.
The term now used to describe single-port surgery in the urological literature is LESS.This was developed to incorporate and standardize the various previous terms used todescribe one overall concept of minimally invasive operations performed through a singleincision using conventional laparoscopic or newer instrumentation such as fixed pre-bent ordeflectable flexible instruments.1 Previous terms included E-NOTES, SILS, OPUS, SPA,SPL and SIL, among others. The first transumbilical urological LESS procedure describedwas by Raman et al. where three nephrectomies were carried out, each using a singleincision with multiple trocars.2 Since that time, the clinical experience has increased
bs_bs_banner
International Journal of Urology (2012) 19, 416–428 doi: 10.1111/j.1442-2042.2012.02963.x
416 © 2012 The Japanese Urological Association

dramatically and LESS has cemented itself as an excellenttechnique for a broad range of urological procedures.
Early history
The first description of a true LESS procedure, evident nowonly in retrospect, was in the field of gynecology for tuballigation in 1972.3 A 1-cm infraumbilical incision was made,through which a laparoscope was inserted to visualize andthen cauterize each fallopian tube. The fallopian tubes wereexposed using an external tenaculum placed on the uterusfrom the vagina. The cosmetic benefit of the technique wasimmediately evident, and eventually led gynecologists toexplore similar techniques for larger procedures, includingtotal abdominal hysterectomy and bilateral salpingo-oophorectomy by 1991.4
General surgeons also began to explore the use oftransumbilical LESS surgery for appendectomy andcholecystectomy.5–7 During this process, a new techniquewas developed in 1999 for use in cholecystectomy, by whicha single skin incision is made, but two fascial incisions areused to accommodate 5-mm trocars within this commonskin incision.8 This allows more ports for instrumentswithout compromising the cosmetic benefit.
Initial urological applications
Although LESS procedures were being developed in theseother arenas, the evolution from open to laparoscopic andfinally robotic surgery was taking place in urology. Thebenefits realized during this transition included less bleed-ing, fewer complications and shorter hospital stays leadingto faster convalescence.9 It was thus inevitable that urolo-gists would also begin exploring the single-port system.
Although we focus here on transumbilical LESS, in2007, the first case in urology used a flank incision forplacement of an R-port (Advanced Surgical Concepts,Wicklow, Ireland) to complete a nephrectomy on a small,non-functioning kidney.10 This technique has also beenused for radical nephrectomy with a 7-cm paramedian inci-sion just lateral to the rectus muscle for placement of aGelPort (Applied Medical, Rancho Santa Margarita, CA,USA).11 Another case report described a 4-cm flank inci-sion with a GelPort to carry out retroperitoneal radicalnephrectomy for renal cell carcinoma in a dialysis patient.12
The pfannenstiel incision has also been explored as a focalpoint for LESS. In one report, a 7.5-cm pfannenstiel inci-sion was used to carry out both nephrectomy and neph-roureterectomy, using a GelPort as an access device.13
These approaches proved to be feasible options utilizingnon-umbilical incisions. However, the majority of urologi-cal single-site experience, as described here, has been withtransumbilical access.
Benefits of LESS
The transition from CL to LESS creates inherent technicalchallenges. In order for the urological community at large toembrace LESS, clear benefits of LESS over CL must beshown rigorously and scientifically. This has been difficult,as the salient advantage is improved cosmesis, a variable forwhich there is a paucity of objective measures. An earlycomparison between LESS and CL among patients under-going nephrectomy showed a subjective cosmetic advan-tage, while also showing comparable outcomes for operativetime, analgesic use, hospital stay and complication rate.14
Similar subjective outcomes have been reproduced withvarious procedures,15–18 but a recent study by Park et al. usedan objective measure to quantify the cosmetic advantage.19
This group used a body image questionnaire to comparepatient satisfaction after kidney surgery. Although the scalewas non-validated, it does represent the first objectivemeasure of improved cosmesis with LESS. As rigorous datacontinues to accumulate, by preliminary observation itseems clear that at least from the surgeon’s perspective,cosmesis is excellent after umbilical LESS surgery. Figure 1shows the immediate intraoperative cosmetic result of apatient in our own group undergoing a LESS left renal cystdecortication. For this procedure, a 4-cm vertical intraum-bilical incision was made, with the result as shown at6 weeks postoperatively in Figure 2.
Other theoretical benefits of LESS include decreasedpostoperative pain and fewer postoperative wound compli-cations (infection, hernia). Jeong et al. presented dataamong patients undergoing adrenalectomy (9 LESS, 17 CL)showing significantly lower postoperative pain in the LESScohort.17 However, most comparison series have not hadlong enough follow up or were powered with sample sizesnecessary to show a meaningful difference in woundcomplications.
Fig. 1 LESS renal cyst decortication immediate cosmeticresult.
Transumbilical LESS in urology
© 2012 The Japanese Urological Association 417

Technique and instruments
As with any new surgical platform, LESS has been associ-ated with unique ergonomic challenges to overcome andinherent difficulties, which continue to be present. Multiportlaparoscopic surgery with strategically placed trocarsachieves triangulation for improved tissue retraction andonly rare instrument clashing. Triangulation and instrumentcrowding becomes even more difficult during LESS,whereby bulky instrument handles clash in preciouslylimited external “real estate”. These difficulties have put theonus not only on the surgeon to creatively overcome theselimitations given current instruments, but also on industry todesign purpose-built access devices and instrumentation.The technical and equipment challenges with LESS havepreviously been described by Sawyer and Ponsky.20 Theynote the rapid innovation seen with LESS and highlight theobstacles that are inherent to single-port surgery. Twoapproaches are described: (i) a coaxial approach in whichinstruments are used in parallel; or (ii) a novel platform. Thecoaxial approach leads to limited visual perspective, asinstruments are in line with the operator’s vision. The tran-sition to novel platforms to overcome this challenge isdescribed below.
Before the current devices were created, surgeons firstexperimented by using existing laparoscopic instrumentsthrough a single skin incision and multiple fascial incisions.This “keyhole” technique (as described above as the firsturological transumbilical LESS procedure) was used tocomplete three nephrectomies (two for chronic infection,one for a 4.5-cm enhancing renal mass) with three adjacenttrocars in an umbilical incision.2 Articulating graspers, stan-dard endoshears and a 45° 5-mm rigid laparoscope or 5-mmdeflectable tip laparoscope were used. The authors citedinternal and external instrument collision as a constant chal-lenge, as well as a difficult learning curve. Similarly, adrena-
lectomy has been carried out using a 2-cm incision withadjacent trocars through multiple fascial punctures.21 Thefascial incisions were connected in these cases for specimenextraction. The three challenges noted were limited maneu-verability with tearing of port site fascia, difficult visualiza-tion and potential difficulty with vascular control. In order tomeet these challenges, new access platforms were createdthat depended on only one fascial incision with the potentialto accommodate up to three or four instruments at a time(such as with Triport and QuadPort; Advanced SurgicalConcepts). The main concept behind new platforms is toprovide access for multiple instruments through one incisionwhile limiting device profile. One solution is provided by theGelPOINT Advanced Access Platform (Applied Medical),which allows the surgeon to place multiple trocars throughany location in the device. Table 1 shows current accessdevices and instrumentation for LESS procedures. Figure 3shows an intraoperative view of the GelPOINT AdvancedAccess Platform being used for the aforementioned LESSleft renal cyst decortication.
One notable addition is that of mini-laparoscopic orneedlescopic instruments, which have been and continue tobe used as adjuncts during LESS procedures. For certainprocedures, in addition to the transumbilical single-port, asmall 2- or 3-mm port has been used for a retracting device,requiring no skin suturing and virtually no scar. This adjunctwas embraced as a way to bridge the gap between standardlaparoscopy and LESS in the consensus statement on LESSin 2010.22
Applications
As described earlier, nephrectomy was the initial procedurereported for transumbilical LESS in 2007. Since that timein only 4 years, an impressive array of procedures havebeen successfully completed using a transumbilical LESSapproach, spanning almost the full urological surgical arma-mentarium for intra-abdominal procedures. We summarizethe literature here, including only those procedures com-
Fig. 2 Cosmetic result 6 weeks after LESS renal cystdecortication.
Fig. 3 GelPOINT Advanced Access Platform intraoperatively.
JE HUMPHREY AND D CANES
418 © 2012 The Japanese Urological Association

pleted through the umbilicus. We have extracted such datafrom series in which multiple techniques and access siteswere included. As the literature is ever growing, this is notintended to be a comprehensive summary. We hope to givethe reader the current scope of the clinical applicationsutilizing transumbilical LESS. Currently-reported transum-bilical LESS applications by organ systems are detailedbelow.
Kidney
Raman first described nephrectomy using three trocarsthrough a single umbilical incision.2 Kidney surgery com-prises the majority of transumbilical LESS surgery to date.It is therefore instructive to subdivide kidney proceduresinto the following categories: oncology, reconstructive,donor nephrectomy and other. Oncological procedures with
a LESS approach must be able to be completed withoutcompromising cancer outcomes. This began by demonstra-tion of renal mass cryoablation using a 3.8-mm cryoprobe(Endocare, Irvine, CA, USA) through a Uni-X accessdevice.23 The authors described this method with both tran-sumbilical and retroperitoneal approaches. The utility of thismethod was confirmed later in a review of a single-center’stransumbilical LESS experience.24
Extirpative oncological surgery has also been shown to befeasible. Aron et al. reported five partial nephrectomies in200825 using the R-Port access device. An extra 2-mm portwas used for a grasper, and one patient needed an additional5-mm port for liver retraction. The R-Port was again usedwhen carried out on six patients in an overall review ofseveral LESS procedures by Desai.26 Other devices havebeen used for partial nephrectomy including the Uni-X27 andGelPort,28 as well as standard trocars through a single inci-
Table 1 Current devices and instrumentation for LESS (alphabetical order)
Company Design Currentlyavailable
Access devicesAirseal Surgiquest, Orange, CT, USA Maximize movement with small incision
by using oval cannulaYes
GelPOINT AdvancedAccess Platform
Applied Medical, Rancho SantaMargarita, CA, USA
1.5–7-cm incisions with self-retainingports for 5–10-mm diameterinstruments
Yes
Quadport Advanced Surgical Concepts, Wicklow,Ireland
Accommodates up to 4 instruments(1 ¥ 5 mm, 2 ¥ 10 mm, 1 ¥ 15 mm indiameter)
Yes
SILS Port Covidien, Dublin, Ireland Accommodates up to 3ports/instruments of variable sizes
Yes
Triport Advanced Surgical Concepts, Wicklow,Ireland
Accommodates up to 3 instruments(12 mm and two 5 mm in diameter)
Yes
Uni-X Pnavel Systems, Brooklyn, NY, USA Three 5-mm diameter ports/instruments NoX-cone Storz, Tuttlingen, Germany Reusable, accommodates 3 working
channels (5 or 12.5 mm in diameter)Yes
Camera systemsEndocameleon Storz, Tuttlingen, Germany 10-mm diameter with adjustable angle
0° to 120°Yes
Endoeye LTF Olympus, Center Valley, PA, USA Deflectable tip 5–10-mm diameter scope YesExtra long Storz, Tuttlingen, Germany 5-mm diameter with 30° lens YesEyemax Richard Wolf Medical Instruments
Corporation, Vernon Hills, IL, USA5–10-mm diameter with 0–30° digital
lensYes
Ideal Eyes HD Stryker, Kalamazoo, MI, USA 5-mm diameter articulating scope YesInstruments
Roticulator Covidien, Dublin, Ireland 5-mm diameter instruments YesPrebent Various companies Basic curved instruments YesReal Hand Novare, Cupertino, CA, USA 5-mm instruments NoAutonomy laparo-angle Cambridge Endo, Framingham, MA, USA 5-mm articulating instruments Yes
Devices are presented in alphabetical order.
Transumbilical LESS in urology
© 2012 The Japanese Urological Association 419

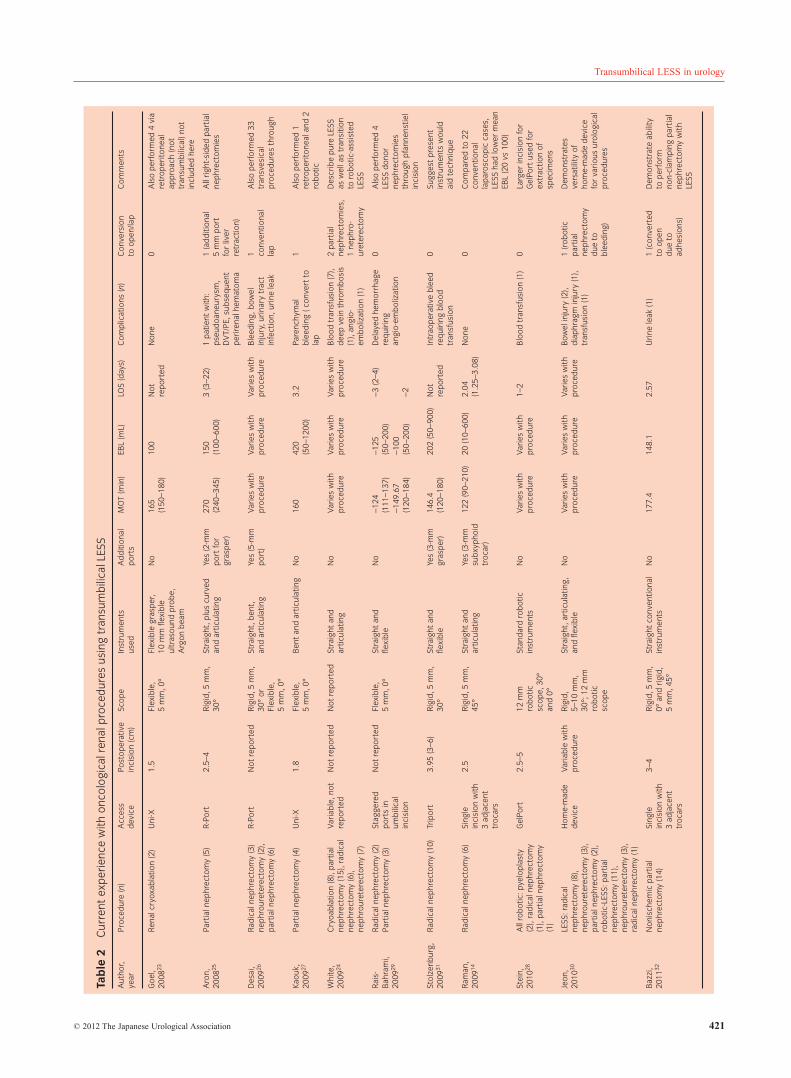
sion29 and homemade access devices.30 Radical nephrec-tomy has also seen broad use in several series.14,24,26,28–31 Acommon practice for right-sided nephrectomy has been theaddition of a small 2–3-mm port to aid with liver retraction.This gives the surgeon a technical advantage while not sac-rificing the cosmetic benefit of LESS. A more recent serieshas shown that non-ischemic partial nephrectomy is safe andfeasible with LESS.32 Table 2 details LESS kidney surgeryfor malignancy.
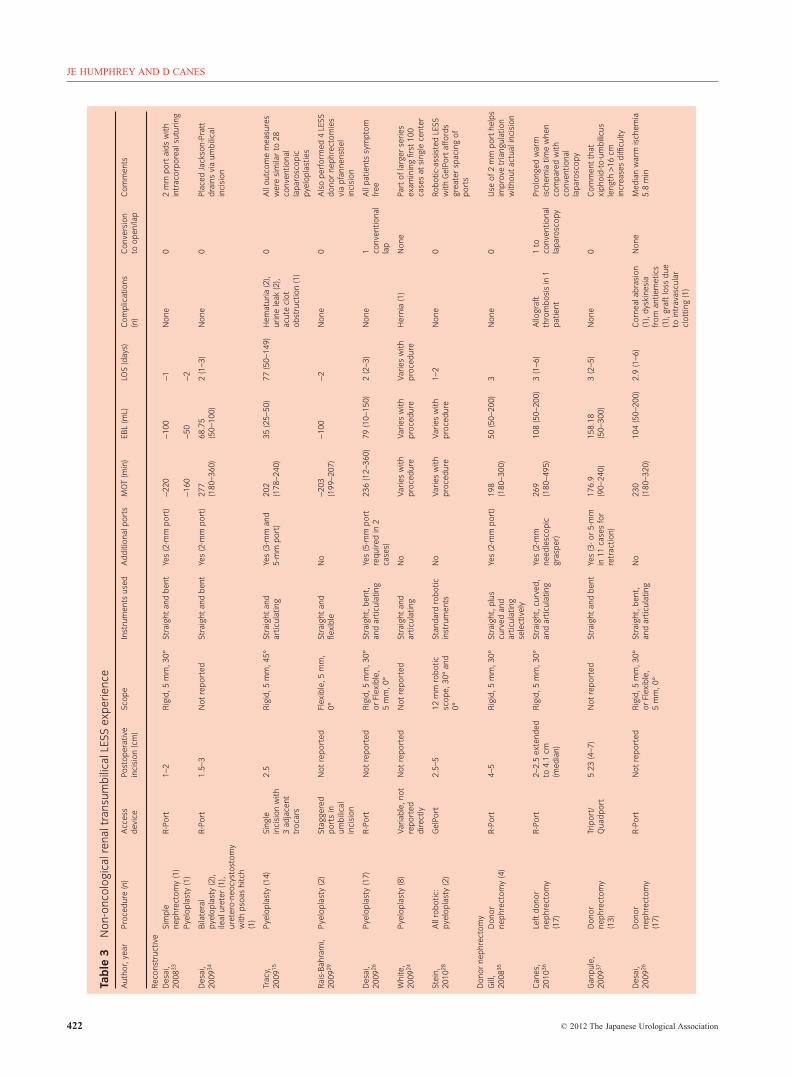
The full cosmetic benefit of transumbilical LESS can berealized with reconstructive renal procedures. Unlike withmany oncological indications, these do not require extensionof the original incision for specimen extraction. Desai et al.reported the first pyeloplasty using the R-Port with an addi-tional 2-mm port for a grasper and to aid with intracorporealsuturing.33 A similar technique was described for simplenephrectomy in a patient with a poorly functioning leftkidney. The same group later published results with single-session bilateral pyeloplasty in two patients, as well as anileal ureter and a ureteroneocystostomy with a psoas hitch.34
This shows the evolution of transumbilical LESS techniquesto more complex procedures. When compared with conven-tional laparoscopic pyeloplasty, transumbilical LESS pyelo-plasty has been found to have similar immediate outcomes,including length of hospital stay, morphine equivalents, andminor and major complications.15 Surprisingly, they alsofound that median operative times and median estimatedblood loss were lower in patients undergoing LESS. Thismight represent increased attending involvement with LESSinherent at teaching institutions with new techniques.
The transplantation arena has been fertile ground forLESS application and investigation. Transumbilical LESSdonor nephrectomy provides the patient cosmetic benefitand potentially faster recovery time with decreased periop-erative pain compared with conventional laparoscopic andopen donor nephrectomy. The first experience with LESSdonor nephrectomy used the R-Port, as well as a 2-mm portwithout an incision to aid in retraction.35 A comparison withconventional laparoscopy has shown that there is an associ-ated quicker convalescence with LESS patients, includingdays on oral pain medication, days off work and days to100% recovery.36
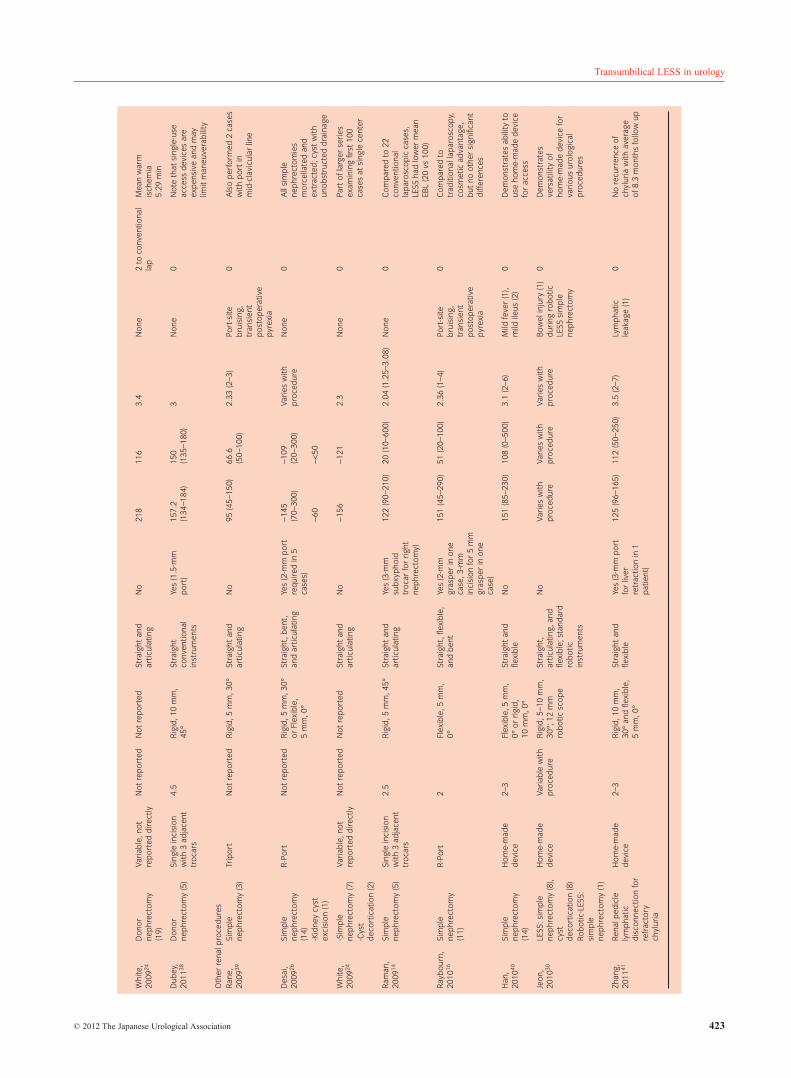
Other miscellaneous renal procedures have been com-pleted successfully with transumbilical LESS. These includesimple nephrectomy for benign indications and cyst decor-tication. See Table 3 for experience with these procedures,as well as the reconstructive and donor nephrectomyexperience.
Adrenal
A rare application of transumbilical LESS has been foradrenalectomy, perhaps because retraction is so crucial toexpose the gland. Several series have been published to
date,26,30 including the largest that includes a matched case–control study comparing conventional laparoscopic withtransumbilical LESS adrenalectomy.17 Nine LESS proce-dures were compared with 17 conventional laparoscopicadrenalectomies matched to age, sex, surgical indicationsand tumor size. The indications for the LESS procedureswere benign adenoma (n = 3), Cushing’s Syndrome (n = 1)and pheochromocytoma (n = 5). Tumor size differed signifi-cantly between groups, with an average size of 2.8 cm(1–5.4 cm) in the LESS cohort compared with 4.3 cm (2.5–6.0 cm) in the CL group. However, the techniques weresimilar in terms of conversion rate, operative time, estimatedblood loss, complications and hospital stay. The LESS groupdid have a shorter duration of patient controlled anesthesia(0.9 days vs 1.9 days). Table 4 summarizes the current lit-erature in regard to transumbilical LESS adrenalectomy.
Ureter
One of the theoretical advantages of the umbilicus as aportal-of-entry is the ability to operate in all quadrants. Asthe ureter encompasses such a long path, ureteral pathologypresents a potential opportunity to capitalize on the versa-tility of umbilical LESS. The variety of ureteral proceduresspans oncology, reconstructive and stone diseases. Table 5describes current literature for LESS ureteral surgeriesacross this spectrum.
The series of ureterolithotomy described by Lee et al. is thelargest report.42 Here, 30 transumbilical LESS ureterolitho-tomies were carried out successfully with no conversions toconventional laparoscopy. A homemade device was used foraccess using a 2–3-cm umbilical incision. Patient satisfactionwas analyzed and the authors found that 28 out of 30 patients(93.3%) were satisfied with their postoperative outcomes.
Bladder
Current LESS experience with bladder procedures includesthose listed in Table 6. Procedures accomplished to datethrough a LESS approach include radical and partial cystec-tomy, augmentation enterocystoplasty, sacral colpopexy andvesicovaginal fistula repair. Of note, a comparative studycarried out by White et al. looking at sacral colpopexy foundsimilar efficacy and improved cosmesis for transumbilicalLESS versus laparoscopic and robotic techniques.18 Therewere no conversions and no immediate complications. Thepatients showed prolapse reduction at 6 months follow up,and were overall satisfied with the outcomes. The authorsstate that they are exploring this technique robotically toovercome the learning curve associated with the procedure.
Prostate
With tremendous experience in minimally invasive (laparo-scopic and robotic) prostatectomy, it is not surprising that
JE HUMPHREY AND D CANES
420 © 2012 The Japanese Urological Association
Tab
le2
Cur
rent
exp
erie
nce
with
onco
logi
calr
enal
pro
ced
ures
usin
gtr
ansu
mb
ilica
lLES
S
Aut
hor,
year
Pro
ced
ure
(n)
Acc
ess
dev
ice
Post
oper
ativ
ein
cisi
on(c
m)
Scop
eIn
stru
men
tsus
edA
dd
ition
alp
orts
MO
T(m
in)
EBL
(mL)
LOS
(day
s)C
omp
licat
ions
(n)
Con
vers
ion
toop
en/la
pC
omm
ents
Goe
l,20
0823
Ren
alcr
yoxa
bla
tion
(2)
Uni
-X1.
5Fl
exib
le,
5m
m,0
°Fl
exib
legr
asp
er,
10m
mfle
xib
leul
tras
ound
pro
be,
Arg
onb
eam
No
165
(150
–180
)10
0N
otre
por
ted
Non
e0
Als
op
erfo
rmed
4vi
are
trop
erito
neal
app
roac
h(n
ottr
ansu
mb
ilica
l)no
tin
clud
edhe
re
Aro
n,20
0825
Part
ialn
ephr
ecto
my
(5)
R-P
ort
2.5–
4R
igid
,5m
m,
30°
Stra
ight
,plu
scu
rved
and
artic
ulat
ing
Yes
(2-m
mp
ort
for
gras
per
)
270
(240
–345
)15
0(1
00–6
00)
3(3
–22)
1p
atie
ntw
ith:
pse
udoa
neur
ysm
,D
VT/
PE,
sub
seq
uent
per
iren
alhe
mat
oma
1(a
dd
ition
al5
mm
por
tfo
rliv
erre
trac
tion)
All
righ
t-si
ded
par
tial
nep
hrec
tom
ies
Des
ai,
2009
26R
adic
alne
phr
ecto
my
(3)
nep
hrou
rete
rect
omy
(2),
par
tialn
ephr
ecto
my
(6)
R-P
ort
Not
rep
orte
dR
igid
,5m
m,
30°
orFl
exib
le,
5m
m,0
°
Stra
ight
,ben
t,an
dar
ticul
atin
gYe
s(5
-mm
por
t)V
arie
sw
ithp
roce
dur
eV
arie
sw
ithp
roce
dur
eV
arie
sw
ithp
roce
dur
eB
leed
ing,
bow
elin
jury
,uri
nary
trac
tin
fect
ion,
urin
ele
ak
1 conv
entio
nal
lap
Als
op
erfo
rmed
33tr
ansv
esic
alp
roce
dur
esth
roug
h
Kaou
k,20
0927
Part
ialn
ephr
ecto
my
(4)
Uni
-X1.
8Fl
exib
le,
5m
m,0
°B
ent
and
artic
ulat
ing
No
160
420
(50–
1200
)3.
2Pa
renc
hym
alb
leed
ing
(con
vert
tola
p
1A
lso
per
form
ed1
retr
oper
itone
alan
d2
rob
otic
Whi
te,
2009
24C
ryoa
bla
tion
(8),
par
tial
nep
hrec
tom
y(1
5),r
adic
alne
phr
ecto
my
(6),
nep
hrou
rete
rect
omy
(7)
Var
iab
le,n
otre
por
ted
Not
rep
orte
dN
otre
por
ted
Stra
ight
and
artic
ulat
ing
No
Var
ies
with
pro
ced
ure
Var
ies
with
pro
ced
ure
Var
ies
with
pro
ced
ure
Blo
odtr
ansf
usio
n(7
),d
eep
vein
thro
mb
osis
(1),
angi
o-em
bol
izat
ion
(1)
2p
artia
lne
phr
ecto
mie
s,1
nep
hro-
uret
erec
tom
y
Des
crib
ep
ure
LESS
asw
ella
str
ansi
tion
toro
bot
ic-a
ssis
ted
LESS
Rai
s-B
ahra
mi,
2009
29
Rad
ical
nep
hrec
tom
y(2
)St
agge
red
por
tsin
umb
ilica
lin
cisi
on
Not
rep
orte
dFl
exib
le,
5m
m,0
°St
raig
htan
dfle
xib
leN
o-1
24(1
11–1
37)
-125
(50–
200)
-3(2
–4)
Del
ayed
hem
orrh
age
req
uiri
ngan
gio-
emb
oliz
atio
n
0A
lso
per
form
ed4
LESS
don
orne
phr
ecto
mie
sth
roug
hp
fann
enst
iel
inci
sion
Part
ialn
ephr
ecto
my
(3)
-149
.67
(120
–184
)-1
00(5
0–20
0)-2
Stol
zenb
urg,
2009
31R
adic
alne
phr
ecto
my
(10)
Trip
ort
3.95
(3–6
)R
igid
,5m
m,
30°
Stra
ight
and
flexi
ble
Yes
(3-m
mgr
asp
er)
146.
4(1
20–1
80)
202
(50–
900)
Not
rep
orte
dIn
trao
per
ativ
eb
leed
req
uiri
ngb
lood
tran
sfus
ion
0Su
gges
tp
rese
ntin
stru
men
tsw
ould
aid
tech
niq
ue
Ram
an,
2009
14R
adic
alne
phr
ecto
my
(6)
Sing
lein
cisi
onw
ith3
adja
cent
troc
ars
2.5
Rig
id,5
mm
,45
°St
raig
htan
dar
ticul
atin
gYe
s(3
-mm
sub
xyp
hoid
troc
ar)
122
(90–
210)
20(1
0–60
0)2.
04(1
.25–
3.08
)N
one
0C
omp
ared
to22
conv
entio
nal
lap
aros
cop
icca
ses,
LESS
had
low
erm
ean
EBL
(20
vs10
0)
Stei
n,20
1028
All
rob
otic
:pye
lop
last
y(2
),ra
dic
alne
phr
ecto
my
(1),
par
tialn
ephr
ecto
my
(1)
Gel
Port
2.5–
512
mm
rob
otic
scop
e,30
°an
d0°
Stan
dar
dro
bot
icin
stru
men
tsN
oV
arie
sw
ithp
roce
dur
eV
arie
sw
ithp
roce
dur
e1–
2B
lood
tran
sfus
ion
(1)
0La
rger
inci
sion
for
Gel
Port
used
for
extr
actio
nof
spec
imen
s
Jeon
,20
1030
LESS
:rad
ical
nep
hrec
tom
y(8
),ne
phr
oure
tere
ctom
y(3
),p
artia
lnep
hrec
tom
y(2
),ro
bot
ic-L
ESS:
par
tial
nep
hrec
tom
y(1
1),
nep
hrou
rete
rect
omy
(3),
rad
ical
nep
hrec
tom
y(1
)
Hom
e-m
ade
dev
ice
Var
iab
lew
ithp
roce
dur
eR
igid
,5–
10m
m,
30°;
12m
mro
bot
icsc
ope
Stra
ight
,art
icul
atin
g,an
dfle
xib
leN
oV
arie
sw
ithp
roce
dur
eV
arie
sw
ithp
roce
dur
eV
arie
sw
ithp
roce
dur
eB
owel
inju
ry(2
),d
iap
hrag
min
jury
(1),
tran
sfus
ion
(1)
1(r
obot
icp
artia
lne
phr
ecto
my
due
tob
leed
ing)
Dem
onst
rate
sve
rsat
ility
ofho
me-
mad
ed
evic
efo
rva
riou
sur
olog
ical
pro
ced
ures
Baz
zi,
2011
32N
onis
chem
icp
artia
lne
phr
ecto
my
(14)
Sing
lein
cisi
onw
ith3
adja
cent
troc
ars
3–4
Rig
id,5
mm
,0°
and
rigi
d,
5m
m,4
5°
Stra
ight
conv
entio
nal
inst
rum
ents
No
177.
414
8.1
2.57
Uri
nele
ak(1
)1
(con
vert
edto
open
due
toad
hesi
ons)
Dem
onst
rate
abili
tyto
per
form
non-
clam
pin
gp
artia
lne
phr
ecto
my
with
LESS
Transumbilical LESS in urology
© 2012 The Japanese Urological Association 421
Tab
le3
Non
-onc
olog
ical
rena
ltra
nsum
bili
calL
ESS
exp
erie
nce
Aut
hor,
year
Pro
ced
ure
(n)
Acc
ess
dev
ice
Post
oper
ativ
ein
cisi
on(c
m)
Scop
eIn
stru
men
tsus
edA
dd
ition
alp
orts
MO
T(m
in)
EBL
(mL)
LOS
(day
s)C
omp
licat
ions
(n)
Con
vers
ion
toop
en/la
pC
omm
ents
Rec
onst
ruct
ive
Des
ai,
2008
33Si
mp
lene
phr
ecto
my
(1)
R-P
ort
1–2
Rig
id,5
mm
,30°
Stra
ight
and
ben
tYe
s(2
-mm
por
t)-2
20-1
00-1
Non
e0
2m
mp
ort
aid
sw
ithin
trac
orp
orea
lsut
urin
gP
yelo
pla
sty
(1)
-160
-50
-2
Des
ai,
2009
34B
ilate
ral
pyel
opla
sty
(2),
ileal
uret
er(1
),ur
eter
o-ne
ocys
tost
omy
with
pso
ashi
tch
(1)
R-P
ort
1.5–
3N
otre
por
ted
Stra
ight
and
ben
tYe
s(2
-mm
por
t)27
7(1
80–3
60)
68.7
5(5
0–10
0)2
(1–3
)N
one
0P
lace
dJa
ckso
n-P
ratt
dra
ins
via
umb
ilica
lin
cisi
on
Trac
y,20
0915
Pye
lop
last
y(1
4)Si
ngle
inci
sion
with
3ad
jace
nttr
ocar
s
2.5
Rig
id,5
mm
,45°
Stra
ight
and
artic
ulat
ing
Yes
(3-m
man
d5-
mm
por
t)20
2(1
78–2
40)
35(2
5–50
)77
(50–
149)
Hem
atur
ia(2
),ur
ine
leak
(2),
acut
ecl
otob
stru
ctio
n(1
)
0A
llou
tcom
em
easu
res
wer
esi
mila
rto
28co
nven
tiona
lla
par
osco
pic
pyel
opla
stie
s
Rai
s-B
ahra
mi,
2009
29P
yelo
pla
sty
(2)
Stag
gere
dp
orts
inum
bili
cal
inci
sion
Not
rep
orte
dFl
exib
le,5
mm
,0°
Stra
ight
and
flexi
ble
No
-203
(199
–207
)-1
00-2
Non
e0
Als
op
erfo
rmed
4LE
SSd
onor
nep
hrec
tom
ies
via
pfa
nnen
stie
lin
cisi
on
Des
ai,
2009
26P
yelo
pla
sty
(17)
R-P
ort
Not
rep
orte
dR
igid
,5m
m,3
0°or
Flex
ible
,5
mm
,0°
Stra
ight
,ben
t,an
dar
ticul
atin
gYe
s(5
-mm
por
tre
qui
red
in2
case
s)
236
(12–
360)
79(1
0–15
0)2
(2–3
)N
one
1 conv
entio
nal
lap
All
pat
ient
ssy
mp
tom
free
Whi
te,
2009
24P
yelo
pla
sty
(8)
Var
iab
le,n
otre
por
ted
dir
ectly
Not
rep
orte
dN
otre
por
ted
Stra
ight
and
artic
ulat
ing
No
Var
ies
with
pro
ced
ure
Var
ies
with
pro
ced
ure
Var
ies
with
pro
ced
ure
Her
nia
(1)
Non
ePa
rtof
larg
erse
ries
exam
inin
gfir
st10
0ca
ses
atsi
ngle
cent
er
Stei
n,20
1028
All
rob
otic
:py
elop
last
y(2
)G
elPo
rt2.
5–5
12m
mro
bot
icsc
ope,
30°
and
0°
Stan
dar
dro
bot
icin
stru
men
tsN
oV
arie
sw
ithp
roce
dur
eV
arie
sw
ithp
roce
dur
e1–
2N
one
0R
obot
ic-a
ssis
ted
LESS
with
Gel
Port
affo
rds
grea
ter
spac
ing
ofp
orts
Don
orne
phr
ecto
my
Gill
,20
0835
Don
orne
phr
ecto
my
(4)
R-P
ort
4–5
Rig
id,5
mm
,30°
Stra
ight
,plu
scu
rved
and
artic
ulat
ing
sele
ctiv
ely
Yes
(2-m
mp
ort)
198
(180
–300
)50
(50–
200)
3N
one
0U
seof
2m
mp
ort
help
sim
pro
vetr
iang
ulat
ion
with
out
actu
alin
cisi
on
Can
es,
2010
36Le
ftd
onor
nep
hrec
tom
y(1
7)
R-P
ort
2–2.
5ex
tend
edto
4.1
cm(m
edia
n)
Rig
id,5
mm
,30°
Stra
ight
,cur
ved
,an
dar
ticul
atin
gYe
s(2
-mm
need
lesc
opic
gras
per
)
269
(180
–495
)10
8(5
0–20
0)3
(1–6
)A
llogr
aft
thro
mb
osis
in1
pat
ient
1to
conv
entio
nal
lap
aros
copy
Pro
long
edw
arm
isch
emia
time
whe
nco
mp
ared
with
conv
entio
nal
lap
aros
copy
Gan
pul
e,20
0937
Don
orne
phr
ecto
my
(13)
Trip
ort/
Qua
dp
ort
5.23
(4–7
)N
otre
por
ted
Stra
ight
and
ben
tYe
s(3
-or
5-m
min
11ca
ses
for
retr
actio
n)
176.
9(9
0–24
0)15
8.18
(50–
300)
3(2
–5)
Non
e0
Com
men
tth
atxi
pho
id-t
o-um
bili
cus
leng
th>1
6cm
incr
ease
sd
ifficu
lty
Des
ai,
2009
26D
onor
nep
hrec
tom
y(1
7)
R-P
ort
Not
rep
orte
dR
igid
,5m
m,3
0°or
Flex
ible
,5
mm
,0°
Stra
ight
,ben
t,an
dar
ticul
atin
gN
o23
0(1
80–3
20)
104
(50–
200)
2.9
(1–6
)C
orne
alab
rasi
on(1
),d
yski
nesi
afr
oman
tiem
etic
s(1
),gr
aft
loss
due
toin
trav
ascu
lar
clot
ting
(1)
Non
eM
edia
nw
arm
isch
emia
5.8
min
JE HUMPHREY AND D CANES
422 © 2012 The Japanese Urological Association
Whi
te,
2009
24D
onor
nep
hrec
tom
y(1
9)
Var
iab
le,n
otre
por
ted
dir
ectly
Not
rep
orte
dN
otre
por
ted
Stra
ight
and
artic
ulat
ing
No
218
116
3.4
Non
e2
toco
nven
tiona
lla
pM
ean
war
mis
chem
ia5.
29m
in
Dub
ey,
2011
38D
onor
nep
hrec
tom
y(5
)Si
ngle
inci
sion
with
3ad
jace
nttr
ocar
s
4.5
Rig
id,1
0m
m,
45°
Stra
ight
conv
entio
nal
inst
rum
ents
Yes
(1.5
-mm
por
t)15
7.2
(134
–184
)15
0(1
35–1
80)
3N
one
0N
ote
that
sing
le-u
seac
cess
dev
ices
are
exp
ensi
vean
dm
aylim
itm
aneu
vera
bili
ty
Oth
erre
nalp
roce
dur
esR
ane,
2009
39Si
mp
lene
phr
ecto
my
(3)
Trip
ort
Not
rep
orte
dR
igid
,5m
m,3
0°St
raig
htan
dar
ticul
atin
gN
o95
(45–
150)
66.6
(50–
100)
2.33
(2–3
)Po
rt-s
iteb
ruis
ing,
tran
sien
tp
osto
per
ativ
epy
rexi
a
0A
lso
per
form
ed2
case
sw
ithp
ort
inm
id-c
lavi
cula
rlin
e
Des
ai,
2009
26Si
mp
lene
phr
ecto
my
(14)
R-P
ort
Not
rep
orte
dR
igid
,5m
m,3
0°or
Flex
ible
,5
mm
,0°
Stra
ight
,ben
t,an
dar
ticul
atin
gYe
s(2
-mm
por
tre
qui
red
in5
case
s)
-145
(70–
300)
-109
(20–
300)
Var
ies
with
pro
ced
ure
Non
e0
All
sim
ple
nep
hrec
tom
ies
mor
cella
ted
and
extr
acte
d;c
yst
with
unob
stru
cted
dra
inag
e-K
idne
ycy
stex
cisi
on(1
)-6
0-<
50
Whi
te,
2009
24-S
imp
lene
phr
ecto
my
(7)
Var
iab
le,n
otre
por
ted
dir
ectly
Not
rep
orte
dN
otre
por
ted
Stra
ight
and
artic
ulat
ing
No
-156
-121
2.3
Non
e0
Part
ofla
rger
seri
esex
amin
ing
first
100
case
sat
sing
lece
nter
-Cys
td
ecor
ticat
ion
(2)
Ram
an,
2009
14Si
mp
lene
phr
ecto
my
(5)
Sing
lein
cisi
onw
ith3
adja
cent
troc
ars
2.5
Rig
id,5
mm
,45°
Stra
ight
and
artic
ulat
ing
Yes
(3-m
msu
bxy
pho
idtr
ocar
for
righ
tne
phr
ecto
my)
122
(90–
210)
20(1
0–60
0)2.
04(1
.25–
3.08
)N
one
0C
omp
ared
to22
conv
entio
nal
lap
aros
cop
icca
ses,
LESS
had
low
erm
ean
EBL
(20
vs10
0)
Ray
bou
rn,
2010
16Si
mp
lene
phr
ecto
my
(11)
R-P
ort
2Fl
exib
le,5
mm
,0°
Stra
ight
,flex
ible
,an
db
ent
Yes
(2-m
mgr
asp
erin
one
case
,3-m
min
cisi
onfo
r5
mm
gras
per
inon
eca
se)
151
(45–
290)
51(2
0–10
0)2.
36(1
–4)
Port
-site
bru
isin
g,tr
ansi
ent
pos
top
erat
ive
pyre
xia
0C
omp
ared
totr
aditi
onal
lap
aros
copy
,co
smet
icad
vant
age,
but
noot
her
sign
ifica
ntd
iffer
ence
s
Han
,20
1040
Sim
ple
nep
hrec
tom
y(1
4)
Hom
e-m
ade
dev
ice
2–3
Flex
ible
,5m
m,
0°or
rigi
d,
10m
m,0
°
Stra
ight
and
flexi
ble
No
151
(85–
230)
108
(0–5
00)
3.1
(2–6
)M
ildfe
ver
(1),
mild
ileus
(2)
0D
emon
stra
tes
abili
tyto
use
hom
e-m
ade
dev
ice
for
acce
ss
Jeon
,20
1030
LESS
:sim
ple
nep
hrec
tom
y(8
),cy
std
ecor
ticat
ion
(8)
Hom
e-m
ade
dev
ice
Var
iab
lew
ithp
roce
dur
eR
igid
,5–1
0m
m,
30°;
12m
mro
bot
icsc
ope
Stra
ight
,ar
ticul
atin
g,an
dfle
xib
le;s
tand
ard
rob
otic
inst
rum
ents
No
Var
ies
with
pro
ced
ure
Var
ies
with
pro
ced
ure
Var
ies
with
pro
ced
ure
Bow
elin
jury
(1)
dur
ing
rob
otic
LESS
sim
ple
nep
hrec
tom
y
0D
emon
stra
tes
vers
atili
tyof
hom
e-m
ade
dev
ice
for
vari
ous
urol
ogic
alp
roce
dur
esR
obot
ic-L
ESS:
sim
ple
nep
hrec
tom
y(1
)
Zhan
g,20
1141
Ren
alp
edic
lely
mp
hatic
dis
conn
ectio
nfo
rre
frac
tory
chyl
uria
Hom
e-m
ade
dev
ice
2–3
Rig
id,1
0m
m,
30°
and
flexi
ble
,5
mm
,0°
Stra
ight
and
flexi
ble
Yes
(3-m
mp
ort
for
liver
retr
actio
nin
1p
atie
nt)
125
(96–
165)
112
(50–
250)
3.5
(2–7
)Ly
mp
hatic
leak
age
(1)
0N
ore
curr
ence
ofch
ylur
iaw
ithav
erag
eof
8.3
mon
ths
follo
wup
Transumbilical LESS in urology
© 2012 The Japanese Urological Association 423

Tab
le4
Ad
rena
lpro
ced
ures
usin
gtr
ansu
mb
ilica
lLES
S
Aut
hor,
year
Pro
ced
ure
(n)
Acc
ess
dev
ice
Post
oper
ativ
ein
cisi
on(c
m)
Scop
eIn
stru
men
tsus
edA
dd
ition
alp
orts
MO
T(m
in)
EBL
(mL)
LOS
(day
s)C
omp
licat
ions
(n)
Con
vers
ion
toop
en/la
pC
omm
ents
Jeon
g,20
0917
Ad
rena
lect
omy
(9)
Hom
e-m
ade
dev
ice
2Fl
exib
le,5
mm
,0°
Stra
ight
and
artic
ulat
ing
No
169.
2(8
9–28
9)17
7.8
(50–
400)
3.2
(2–4
)Se
rosa
ltea
r(1
)0
Mat
ched
toco
nven
tiona
lla
par
osco
pyw
ithco
mp
arab
lere
sults
Des
ai,2
00926
Ad
rena
lect
omy
(1)
R-P
ort
Not
rep
orte
dR
igid
,5m
m,3
0°or
Flex
ible
,5
mm
,0°
Stra
ight
,ben
t,an
dar
ticul
atin
gYe
s(2
-mm
por
t)15
035
03
Ble
edin
gw
ithri
ght
rena
lvei
nin
jury
,su
bse
que
ntre
nal
vein
thro
mb
us(1
)
1to
conv
entio
nal
lap
aros
copy
Onl
yca
sew
asco
nver
ted
due
tori
ght
rena
lvei
nin
jury
Jeon
,201
030A
dre
nale
ctom
y(2
)H
ome-
mad
ed
evic
eN
otre
por
ted
Rig
id,5
–10
mm
,30
°;12
mm
rob
otic
scop
e
Stra
ight
,ar
ticul
atin
g,an
dfle
xib
le
N0
260
125
3N
one
0D
emon
stra
tes
vers
atili
tyof
hom
e-m
ade
dev
ice
for
vari
ous
urol
ogic
alp
roce
dur
es
Tab
le5
Ure
tera
lpro
ced
ures
usin
gtr
ansu
mb
ilica
lLES
S(e
xclu
din
gne
phr
oure
tere
ctom
y)
Aut
hor,
Year
Pro
ced
ure
(n)
Acc
ess
dev
ice
Post
oper
ativ
ein
cisi
on(c
m)
Scop
eIn
stru
men
tsus
edA
dd
ition
alp
orts
MO
T(m
in)
EBL
(mL)
LOS
(day
s)C
omp
licat
ions
(n)
Con
vers
ion
toop
en/la
pC
omm
ents
Des
ai,2
00933
Ileal
uret
er(1
),ur
eter
o-ne
ocys
tost
omy
with
pso
ashi
tch
(1)
R-P
ort
1.5–
3N
otre
por
ted
Stra
ight
and
ben
tYe
s(2
-mm
por
tfo
rgr
asp
er,n
otr
uein
cisi
on)
277
(180
–360
)68
.75
(50–
100)
2(1
–3)
Non
e0
Pla
ced
Jack
son-
Pra
ttd
rain
svi
aum
bili
cali
ncis
ion
Des
ai,2
00926
-Ure
tera
lre
imp
lant
(2)
R-P
ort
Not
rep
orte
dR
igid
,5m
m,3
0°or
Flex
ible
,5
mm
,0°
Stra
ight
,ben
t,an
dar
ticul
atin
gYe
s(2
-mm
por
t)-1
75(1
40–2
10)
-175
(100
–250
)-4
Ana
stom
otic
leak
(1)
0Pa
rtof
larg
erse
ries
exam
inin
gfir
st10
0ca
ses
atsi
ngle
cent
er-Il
ealu
rete
r(3
)-3
30(3
00–3
60)
-170
(90–
250)
-2
Whi
te,2
00924
Ure
tera
lre
imp
lant
(1)
Not
rep
orte
dN
otre
por
ted
Not
rep
orte
dSt
raig
htan
dar
ticul
atin
gN
o18
010
03
Non
e0
MA
G3
norm
al
Jeon
,201
030-U
rete
rect
omy
(1)
Hom
e-m
ade
dev
ice
Not
rep
orte
dR
igid
,5–1
0m
m,
30°;
12m
mro
bot
icsc
ope
Stra
ight
,ar
ticul
atin
g,an
dfle
xib
le
No
-80
-150
-3N
one
0U
rete
rect
omy
for
dup
licat
ion,
ecto
pic
uret
er-U
rete
rolit
hoto
my
(1)
-2-3
10-2
10-6
Lee,
2011
42U
rete
rolit
hoto
my
(30)
Hom
e-m
ade
dev
ice
2–3
Rig
id,1
0m
m,0
°St
raig
ht,fl
exib
le,
and
artic
ulat
ing
Yes
(tra
nscu
tane
ous
por
tfo
ron
ep
atie
nt,s
ize
not
rep
orte
d)
110.
4361
.17
3.40
Feve
r(2
),m
ildile
us(1
)1
Use
fuli
fur
eter
osco
pyor
shoc
kwav
elit
hotr
ipsy
not
avai
lab
le
JE HUMPHREY AND D CANES
424 © 2012 The Japanese Urological Association

Tab
le6
Bla
dd
erP
roce
dur
esus
ing
tran
sum
bili
calL
ESS
Aut
hor,
year
Pro
ced
ure
(n)
Acc
ess
dev
ice
Post
oper
ativ
ein
cisi
on(c
m)
Scop
eIn
stru
men
tsus
edA
dd
ition
alp
orts
MO
T(m
in)
EBL
(mL)
LOS
(day
s)C
omp
licat
ions
(n)
Con
vers
ion
toop
en/la
pC
omm
ents
Nog
uera
,200
943A
ugm
enta
tion
ente
rocy
stop
last
y(1
)
Qua
dp
ort
5Fl
exib
le,5
mm
,0°
Stra
ight
and
flexi
ble
No
300
<100
6N
one
0B
owel
rese
ctio
nan
dan
asto
mos
isp
erfo
rmed
extr
acor
por
eally
Whi
te,2
00918
Sacr
alco
lpop
exy
(10)
Uni
-X1.
8Fl
exib
le,5
mm
,0°
Stra
ight
and
artic
ulat
ing
No
162
47.5
1.5
Cys
toce
le(1
),st
ress
inco
ntin
ence
(2)
0Si
ngle
-por
tco
mp
arab
lein
seri
esto
mat
ched
lap
aros
cop
ican
dro
bot
icca
ses
Whi
te,2
00924
Rad
ical
cyst
ecto
my
(3)
Var
iab
le,n
otre
por
ted
dir
ectly
Not
rep
orte
dN
otre
por
ted
Stra
ight
and
artic
ulat
ing
No
-315
-216
-6.6
Non
e0
Cys
tect
omy
lym
ph
nod
eyi
eld
=16
Sacr
alco
lpop
exy
(13)
-182
-46.
9-1
.6
Kaou
k,20
1044
Rad
ical
cyst
ecto
my
(3)
Uni
-X4.
5–5
(1.8
cmb
efor
eex
trac
tion)
Flex
ible
,5m
m,
0°St
raig
htan
dfle
xib
leN
o31
5(2
85–3
60)
217
(200
–250
)6
(5–7
)N
one
0O
per
ativ
etim
ed
ecre
ased
from
first
toth
ird
pat
ient
Jeon
,201
030Pa
rtia
lcy
stec
tom
y(1
)H
ome-
mad
ed
evic
eV
aria
ble
with
pro
ced
ure
Rig
id,5
–10
mm
,30
°;12
mm
rob
otic
scop
e
Stra
ight
,ar
ticul
atin
g,an
dfle
xib
le
No
175
504
Non
e0
Dem
onst
rate
sve
rsat
ility
ofho
me-
mad
ed
evic
efo
rva
riou
sur
olog
ical
pro
ced
ures
Ab
del
-Kar
im,
2011
45V
esic
ovag
inal
fistu
lare
pai
r(5
)Tr
ipor
t2
Flex
ible
,5m
m,
0°B
ent
Yes
(inal
lcas
es,
5-m
mp
ort
add
edfo
rsu
turi
ngan
dtr
iang
ulat
ion)
198
(170
–240
)90
(70–
120)
2N
one
0Le
ssp
ain
and
shor
ter
hosp
ital
stay
than
sam
egr
oup
’sco
nven
tiona
lla
par
osco
pic
case
s
Transumbilical LESS in urology
© 2012 The Japanese Urological Association 425

LESS prostatectomy would ultimately be cautiouslyexplored. This has been described both laparoscopically andwith robotic LESS. Robotic instruments with articulatingtips provide the surgeon with better dexterity when operat-ing through the LESS avenue. The largest series described20 patients undergoing robotic LESS prostatectomy withreasonable mean operative time (187.6 min), estimatedblood loss (128.8 mL) and average length of stay(2.5 days).46 They concluded that robotic assistance“reduces or eliminates instrument crossing, has superiorergonomics, and instrument tip articulation significantlyfacilitates suturing.” Their series is compared with otherLESS prostate series in Table 7.
Robotic LESS
Use of robotics for assistance with LESS procedures wasintended to bring increased dexterity to offset some of thefrustrations with standard laparoscopic LESS surgery. Theda Vinci robotic system (Intuitive Surgical, Sunnyvale, CA,USA) has been used successfully through a single transum-bilical port in a variety of procedures. In 2009, Rane et al.discussed the use of robotics with LESS and its implicationsfor future directions.49 They described how robotics can aidLESS with superior visualization of the operative field,enhanced surgical dexterity and excellent ergonomics.
However, the original da Vinci robotic system was notdesigned specifically for single-site surgery, and thereforehas its own limitations. First, the external size and straightshape of the robotic arms lead to external clashing over asingle port. Second, the original robotic instrument shaftsthemselves do not articulate, and therefore intracorporealclashing can occur as well.
To this end, the newer da Vinci Si surgical system hasbeen modified to be more amenable to single-site surgery.There has been development of VeSPA surgical instruments(Intuitive Surgical) to overcome the aforementioned limita-tions. These instruments are inserted through curved cannu-lae and allow multiple ports through one incision while stillallowing intra-abdominal triangulation. The feasibility ofthis technique was shown in a porcine model in 2010, inwhich the authors completed various kidney procedures(pyeloplasty, partial nephrectomy, nephrectomy) showingimproved ergonomics and minimal instrument clashing.50
Disadvantages
Transumbilical LESS does have difficulties associated withit that the surgeon must weigh with the cosmetic benefit. Asaforementioned, in general utilizing a LESS technique willlead to either no true triangulation or a reliance on curved orbent instruments in order to create triangulation. Thus, thereis a learning curve to LESS that might dissuade communityurologists from accepting LESS into their practice. Another Ta
ble
7P
rost
ate
pro
ced
ures
usin
gtr
ansu
mb
ilica
lLES
S
Aut
hor,
year
Pro
ced
ure
(n)
Acc
ess
dev
ice
Post
oper
ativ
ein
cisi
on(c
m)
Scop
eIn
stru
men
tsus
edA
dd
ition
alp
orts
MO
T(m
in)
EBL
(mL)
LOS
(day
s)C
omp
licat
ions
(n)
Con
vers
ion
toop
en/la
pC
omm
ents
Kaou
k,20
0847
Rad
ical
pro
stat
ecto
my
(4)
Uni
-X2–
3Fl
exib
le,5
mm
,0°
Flex
ible
shea
rs,
curv
edan
dar
ticul
atin
g
No
285
(240
–300
)28
7(1
50–4
00)
2.5
(2–3
)R
ecto
uret
hral
fistu
la0
Flex
ible
-tip
scop
ehe
lps
limit
inst
rum
ent
clas
hing
Whi
te,2
00924
Rad
ical
pro
stat
ecto
my
(6)
Var
iab
le,n
otre
por
ted
dir
ectly
Not
rep
orte
dN
otre
por
ted
Stra
ight
and
artic
ulat
ing
No
270
250
2.3
Fist
ula
(1)
03
foca
llyp
ositi
vem
argi
ns
Bar
ret,
2009
48R
obot
ic-a
ssis
ted
rad
ical
pro
stat
ecto
my
(1)
Sing
lein
cisi
ons
with
3ad
jace
nttr
ocar
s
412
mm
rob
otic
scop
eSt
and
ard
rob
otic
inst
rum
ents
Yes
(5-m
mri
ght
low
erab
dom
inal
por
tfo
rsu
ctio
nan
dco
unte
rtr
actio
n)
150
500
Not
Rep
orte
dN
one
0U
sed
5m
mad
diti
onal
por
tfo
rhe
lpin
tran
sitio
nto
sing
le-p
ort
surg
ery
Whi
te,2
01046
Rob
otic
-ass
iste
dra
dic
alp
rost
atec
tom
y(2
0)
SILS
3–4.
512
mm
rob
otic
scop
eSt
and
ard
rob
otic
inst
rum
ents
Yes
(tw
oca
ses
with
8-m
mro
bot
icp
ort
due
toex
cess
ive
exte
rnal
clas
hing
)
187.
6(1
20–3
00)
128.
8(5
0–35
0)2.
5(1
–6)
Ileus
(1),
blo
odtr
ansf
usio
n(1
),p
ulm
onar
yem
bol
us(1
),ur
osep
sis
(1)
1(t
ost
and
ard
rob
otic
-ass
iste
dla
par
osco
pic
pro
stat
ecto
my)
Rob
otic
sre
duc
esin
stru
men
tcr
ossi
ng,
imp
rove
ssu
turi
ngab
ility
JE HUMPHREY AND D CANES
426 © 2012 The Japanese Urological Association

important aspect of incorporating transumbilical LESS isthe potential cost of newer instruments and access devices. Itmight not be worth both the training and cost associatedwith LESS for the urologist who only has a limited use forLESS. However, there has been no dedicated analysis of costassociated with LESS to this date.
Conclusion
The progression of minimally invasive surgery has ledurologists to explore LESS. Born out of a desire forimproved cosmesis, and the potential for reduced operativetrauma, decreased postoperative pain and complications,transumbilical LESS has successfully been implementedinto the urologist’s armamentarium. However, the futurerole of LESS is still uncertain. Although large specialtycenters have described LESS for virtually all urologicallaparoscopic procedures, it is unclear whether LESS willdiffuse beyond select centers. The majority of data availableare based on non-randomized series, whereby selection biasmight play a significant role. However, a randomized pro-spective trial would be very difficult to complete comparingLESS to conventional laparoscopy. It does seem evident thatthe cosmetic benefit from LESS is real and reproducible, butany incremental benefit apart from cosmesis seems unlikelyto match the leap previously witnessed from open surgery tolaparoscopy.
Surgical device companies have responded by developingaccess devices, scopes and instruments more specificallyaimed towards LESS. As technology improves, this will nodoubt continue to make the transition to LESS easier for moresurgeons. Currently-available LESS training courses shouldbe considered for surgeons interested in LESS techniques tobenefit from the collective experience of early adopters.
The urological transumbilical LESS experience is rapidlygrowing, but many questions remain. Whether the benefits ofLESS truly outweigh its technical challenges is currently un-known. We also cannot predict whether LESS in some formwill become a permanent fixture in our arsenal, or a historicalfootnote. For now, LESS surgery remains the subject ofintense scrutiny, and is a laudable example of surgical cre-ativity aimed at minimizing surgical trauma for our patients.
Conflict of interest
None declared.
References
1 Box G, Averch T, Cadeddu J et al. Nomenclature ofNatural Orifice Transluminal Endoscopic Surgery(NOTES™) and Laparoendoscopic Single-Site Surgery(LESS) procedures in urology. J. Endourol. 2008; 22:2575–81.
2 Raman JD, Bensalah K, Bagrodia A, Stern JM, CadedduJA. Laboratory and clinical development of single keyholeumbilical nephrectomy. Urology 2007; 70: 1039–42.
3 Wheeless CR. Outpatient laparoscope sterilization underlocal anesthesia. Obstet. Gynecol. 1972; 39: 767–70.
4 Pelosi MA, Pelosi MA III. Laparoscopic hysterectomy withbilateral salpingo-oophorectomy using a single umbilicalpuncture. N. J. Med. 1991; 8: 721–6.
5 Pelosi MA, Pelosi MA III. Laparoscopic appendectomyusing a single umbilical puncture (minilaparoscopy). J.Reprod. Med. 1992; 37: 588–94.
6 D’Alessio A, Piro E, Tadini B, Beretta F. One-trocartransumbilical laparoscopic-assisted appendectomy inchildren: our experience. Eur. J. Pediatr. Surg. 2002; 12:24–7.
7 Navarra G, Pozza E, Occhionorelli S, Carcoforo P, DoniniI. One-wound laparoscopic cholecystectomy. Br. J. Surg.1997; 84: 695.
8 Piskun G, Rajpal S. Transumbilical laparoscopiccholecystectomy utilizes no incisions outside the umbilicus.J. Laparoendosc. Adv. Surg. Tech. A 1999; 9: 361–4.
9 Kercher KW, Heniford BT, Matthews BD et al.Laparoscopic vs open nephrectomy in 210 consecutivepatients. Surg. Endosc. 2003; 17: 1889–95.
10 Rane A, Kommu S, Eddy B, Bonadio F, Rao P, Rao P.Clinical evaluation of a novel laparoscopic port (R-port)and evolution of the single laparoscopic port procedure(SLiPP). J. Endourol. 2007; 21 (Suppl 1): A22–23.
11 Ponsky LE, Cherullo EE, Sawyer M, Hartke D. Singleaccess site laparoscopic radical nephrectomy: initial clinicalexperience. J. Endourol. 2008; 22: 663–5.
12 Nomura T, Sato F, Takahashi M, Sumino Y, Mimata H.Laparoendoscopic single-site (LESS) retroperitoneal radicalnephrectomy in a patient with renal cell carcinomareceiving hemodialysis. Case Report Med 2011;doi:10.1155/2011/506032.
13 Ponsky LE, Steinway ML, Lengu IJ, Hartke DM, VourgantiS, Cherullo EE. A pfannenstiel single-site nephrectomyand nephroureterectomy: a practical application oflaparoendoscopic single-site surgery. Urology 2009; 74:482–5.
14 Raman JD, Bagrodia A, Cadeddu JA. Single-incision,umbilical laparoscopic versus conventional laparoscopicnephrectomy: a comparison of perioperative outcomes andshort-term measures of convalescence. Eur. Urol. 2009; 55:1198–206.
15 Tracy CR, Raman JD, Bagrodia A, Cadeddu JA.Perioperative outcomes in patients undergoing conventionallaparoscopic versus laparoendoscopic single-sitepyeloplasty. Urology 2009; 74: 1029–35.
16 Raybourn JH III, Rane A, Sundaram CP. Laparoendoscopicsingle-site surgery for nephrectomy as a feasible alternativeto traditional laparoscopy. Urology 2010; 75: 100–3.
17 Jeong BC, Park YH, Han DH, Kim HH. Laparoendoscopicsingle-site and conventional laparoscopic adrenalectomy. J.Endourol. 2009; 23: 1957–60.
18 White WM, Goel RK, Swartz MA, Moore C, Rackley RR,Kaouk JH. Single-port laparoscopic abdominal sacral
Transumbilical LESS in urology
© 2012 The Japanese Urological Association 427

colpopexy: initial experience and comparative outcomes.Urology 2009; 74: 1008–12.
19 Park SK, Olweny EO, Best SL, Tracy CR, Mir SA,Cadeddu JA. Patient-reported body image and cosmesisoutcomes following kidney surgery: comparison oflaparoendoscopic single-site, laparoscopic, and opensurgery. Eur. Urol. 2011; 60: 1097–104;doi:10.1016/j.eururo.2011.08.007.
20 Sawyer MD, Ponsky LE. Technical and equipmentchallenges for laparoendoscopic single-site surgery andnatural orifice transluminal endoscopic surgery. BJU Int.2010; 106: 892–6.
21 Castellucci SA, Curcillo PG, Ginsberg PC et al. Single portaccess adrenalectomy. J. Endourol. 2008; 22: 1573–6.
22 Gill IS, Advincula AP, Aron M et al. Consensus statementof the consortium for laparoendoscopic single-site surgery.Surg. Endosc. 2010; 24: 762–8.
23 Goel RK, Kaouk JH. Single port access renal cryoablation(SPARC): a new approach. Eur. Urol. 2008; 53: 1204–9.
24 White WM, Haber GP, Goel RK, Crouzet S, Stein RJ,Kaouk JH. Single-port urological surgery: single-centerexperience with the first 100 cases. Urology 2009; 74:801–4.
25 Aron M, Canes D, Desai MM et al. Transumbilicalsingle-port laparoscopic partial nephrectomy. BJU Int.2008; 103: 516–21.
26 Desai MM, Berger AK, Brandina R et al. Laparoendoscopicsingle-site surgery: initial hundred patients. Urology 2009;74: 805–13.
27 Kaouk JH, Goel RK. Single-port laparoscopic and roboticpartial nephrectomy. Eur. Urol. 2009; 55: 1163–70.
28 Stein RJ, White WM, Goel RK, Irwin BH, Haber GP,Kaouk JH. Robotic laparoendoscopic single-site surgeryusing GelPort as the access platform. Eur. Urol. 2010; 57:132–7.
29 Rais-Bahrami S, Montag S, Atalla MA, Andonian S,Kavoussi LR, Richstone L. Laparoendoscopic single-sitesurgery of the kidney with no accessory trocars: an initialexperience. J. Endourol. 2009; 23: 1319–24.
30 Jeon HG, Jeong W, Oh CK et al. Initial experience with 50laparoendoscopic single site surgeries using a homemade,single port device at a single center. J. Endourol. 2010;183: 1866–72.
31 Stolzenburg JU, Kallidonis P, Hellawell G et al. Techniqueof laparoscopic-endoscopic single-site surgery radicalnephrectomy. Eur. Urol. 2009; 56: 644–50.
32 Bazzi WM, Allaf ME, Berkowitz J, Atalah HN, ParekattilS, Derweesh IH. Multicenter experience with nonischemicmultiport laparoscopic and laparoendoscopic single-sitepartial nephrectomy utilizing bipolar radiofrequencyablation coagulator. Diagn Ther Endosc 2011; DOI:10.1155/2011/636537.
33 Desai MM, Rao PP, Aron M et al. Scarless single porttransumbilical nephrectomy and pyeloplasty: first clinicalreport. BJU Int. 2008; 101: 83–8.
34 Desai MM, Stein R, Rao P et al. Embryonic Natural OrificeTransumbilical Endoscopic Surgery (E-NOTES) for
advanced reconstruction: initial experience. Urology 2009;73: 182–7.
35 Gill IS, Canes D, Aron M et al. Single port transumbilical(E-NOTES) donor nephrectomy. J. Urol. 2008; 180:637–41.
36 Canes D, Berger A, Aron M et al. Laparo-EndoscopicSingle Site (LESS) versus standard laparoscopic left donornephrectomy: matched-pair comparison. Eur. Urol. 2010;57: 95–101.
37 Ganpule AP, Dhawan DR, Kurien A et al.Laparoendoscopic single-site donor nephrectomy: asingle-center experience. Urology 2009; 74: 1238–40.
38 Dubey D, Shrinivas RP, Srikanth G. Transumbilicallaparoendoscopic single-site donor nephrectomy: Withoutthe use of a single port access device. Indian J. Urol. 2011;27: 180–4.
39 Rane A, Ahmed S, Kommu SS, Anderson CJ, RimingtonPD. Single-port “scarless” laparoscopic nephrectomies: theUnited Kingdom experience. BJU Int. 2009; 104: 230–3.
40 Han WK, Park YH, Jeon HG et al. The feasibility oflaparoendoscopic single-site nephrectomy: initialexperience using home-made single-port device. Urology2010; 76: 862–5.
41 Zhang Y, Ye J, Wu G et al. Transumbilicallaparoendoscopic single-site renal pedicle lymphaticdisconnection for refractory chyluria. J. Endourol. 2011;25: 1337–41.
42 Lee JY, Han JH, Kim TH, Yoo TK, Park SY, Lee SW.Laparoendoscopic single-site ureterolithotomy for upperureteral stone disease: the first 30 cases in a multicenterstudy. J. Endourol. 2011; 25: 1293–8.
43 Noguera RJS, Astigueta JC, Carmona O et al. Laparoscopicaugmentation enterocystoplasty through a single trocar.Urology 2009; 73: 1371–4.
44 Kaouk JH, Goel RK, White MA et al. LaparoendoscopicSingle-site Radical Cystectomy and Pelvic Lymph NodeDissection: Initial Experience and 2-Year Follow-up.Urology 2010; 76: 857–61.
45 Abdel-Karim AM, Moussa A, Elsalmy S. Laparoendoscopicsingle-site surgery extravesical repair of vesicovaginalfistula: early experience. Urology 2011; 78: 567–71.
46 White MA, Haber GP, Autorino R et al. Roboticlaparoendoscopic single-site radical prostatectomy:technique and early outcomes. Eur. Urol. 2010; 58: 544–50.
47 Kaouk JH, Goel RK, Haber GP, Crouzet S, Desai MM,Gill IS. Single-port laparoscopic radical prostatectomy.Urology 2008; 72: 1190–3.
48 Barret E, Sanchez-Salas R, Kasraeian A et al. A transitionto laparoendoscopic single-site surgery (LESS) radicalprostatectomy: human cadaver experimental and initialclinical experience. J. Endourol. 2009; 23: 135–40.
49 Rane A, Tan GY, Tewari AK. Laparo-endoscopicsingle-site surgery in urology: is robotics the missing link?BJU Int. 2009; 104: 1041–3.
50 Haber GP, White MA, Autorino R et al. Novel Robotic daVinci instruments for laparoendoscopic single-site surgery.Urology 2010; 76: 1279–82.
JE HUMPHREY AND D CANES
428 © 2012 The Japanese Urological Association
Related Documents











