INTRODUCTION Toxoplasmosis is a parasitic zoonotic infection found throughout the world, commonly carried by cats and other animals (Asad et. al., 2006), it is caused by a zoonotic obligate intracellular protozoan parasite; Toxoplasma gondii, which has the capacity to infect all warm-blooded animals. Generally, T. gondii is among the most prevalent parasites in the global human population, Generally, it is estimated that about one third of the World’s population is infected with T. gondii (Tenter, et. al., 2000; Dubey and Jones, 2008; Swai and, Schoonman, 2009). T. gondii is an opportunistic parasitic infection in immune compromised hosts (Ferreira and Borges, 2002). Geographical Distribution Prevalence of the infection varies widely, depending on social and cultural habits, geographic factors, climate, and transmission route. It has been reported that the prevalence is higher in warm and humid areas (Studeničová, et. al., 2006) and in areas where raw or undercooked meat is traditionally eaten.

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript
INTRODUCTION
Toxoplasmosis is a parasitic zoonotic infection found
throughout the world, commonly carried by cats and other
animals (Asad et. al., 2006), it is caused by a zoonotic obligate
intracellular protozoan parasite; Toxoplasma gondii, which has the
capacity to infect all warm-blooded animals. Generally, T. gondii
is among the most prevalent parasites in the global human
population, Generally, it is estimated that about one third of
the World’s population is infected with T. gondii (Tenter, et. al.,
2000; Dubey and Jones, 2008; Swai and, Schoonman, 2009). T.
gondii is an opportunistic parasitic infection in immune
compromised hosts (Ferreira and Borges, 2002).
Geographical Distribution
Prevalence of the infection varies widely, depending on social
and cultural habits, geographic factors, climate, and
transmission route. It has been reported that the prevalence
is higher in warm and humid areas (Studeničová, et. al., 2006)
and in areas where raw or undercooked meat is traditionally
eaten.
High prevalence of the infection have been reported among
pregnant women and women of childbearing age from different
foci in Latin America, parts of Eastern/Central Europe, the
Middle East, parts of south-east Asia and Africa (Pappas et. al.,
2009). However, the prevalence of T. gondii in pregnant women in
China was less than 10% (Gao, et. al., 2012). In Africa, overall
seroprevalence rate as high as 92.5% has been reported (Ayi,
et. al., 2009). Most pregnant women infected with T. gondii are
chronically infected while few acquire the infection during
pregnancy (Nowakowska et. al., 2006). Pregnant women with acute
infection during pregnancy are at risk of congenitally
transmitting the infection to the foetus. Felids play a
crucial role in the epidemiology of this parasitic disease
because they are the only definitive hosts, shedding and
excreting millions of infective oocysts in a short period of
time in their faeces (Dubey, and prowell, 2013).
In most adults it does not cause serious illness, however,
blindness and mental retardation can be caused in congenitally
infected children and severe diseases in those with
compromised immunity. A recent study indicated that infection
with T. gondii is associated with abdominal hernia (Alvarado-
Esquivel and Estrada-Martínez, 2011).
Congenital Toxoplasmosis
T. gondii infection acquired by pregnant women during gestation
and its transmission to the foetus continue to be the cause of
tragic yet preventable disease in the offspring (Remington et.
al., 2006). It has been estimated that 500–5000 infants each
year are born with congenital toxoplasmosis in the United
States (Roberts and Frenkel, 1990). Although the majority of
infants appear to be healthy at birth, significant long-term
sequelae may become obvious only months or years later. Most
pregnant women with acute acquired infection do not experience
obvious symptoms or signs (Remington, et. al., 2006; Boyer,
et. al., 2005). A minority may experience malaise, low-grade
fever, and lymphadenopathy. Rarely, pregnant women will
present with visual changes due to toxoplasmic chorioretinitis
(Garweg et. al., 2005). Congenital toxoplasmosis (CT) occurs
in infants following maternal transmission. It can result in
foetal death and abortion and in syndromes that include
neurologic and neurocognitive deficit One of the late sequelae
of congenital toxoplasmosis is chorioretinitis (Al-Azawi et al.,
2013). It could also cause mental retardation, blindness,
epilepsy, and death (Petersen, 2007).
Toxoplasmosis could be severe and life-threatening during
pregnancy, and to foetuses, and new born babies (Robert-
Gangneux et al., 2009).
Toxoplasmosis in Immuno-compromised people
Among the immuno-competent people, toxoplasmosis is usually
asymptomatic, subclinical or benign, and can be classified as
congenital, acquired or ocular (Oyibo et al., 2009). It could
result in the chronic persistence of cysts within host
tissues; the cysts normally lie dormant, probably for life
(Malla, et. al., 2005). However, it can be severe and life-
threatening to immune-compromised patients (Robert-Gangneux et
al., 2009), causing severe encephalitis through acute infection
or reactivation of latent infection (Innes, 2010; Hang et al.,
2007). It may precursor spontaneously resolved symptoms such
as fever, malaise, and lymphadenopathy, indicating symptomless
latent infection (Montoya and Liesenfield, 2004). Immune
compromised patients such as in HIV infections, subjects are
at risk of developing acute toxoplasmosis due to reactivation
of the organism if their CD4+ T-cell count decreases below 200
cells/μL (Martinez, et. al., 2002; Jayawardena, et. al.,
2008). Since the pandemic of HIV infection has spread
throughout the world, toxoplasmosis has been implicated as one
of the most important opportunistic infections in HIV/AIDS
patients (Nissapatorn, et. al., 2002; Montoya and Remington,
2000; Walker and Zunt, 2005). Moreover, in up to 10% of HIV
infected immune competent individuals, it causes cervical
lymphadenopathy or ocular disease (Walker and Zunt, 2005).
Ocular Toxoplasmosis
This occurs when the parasite enters the eyes. If parasites
reach an eye and they yield a focus of inflammation, the
lesion is progressed to retinitis and involves the choroid
secondarily. Immune responses of the host appear to induce
conversion of the parasitic forms, from tachyzoites to
bradyzoites and their encystment. The cyst may remain inactive
in the scar or nearby for a long time. However, when the cyst
ruptures with release of organisms into the surrounding
retina, retinitis may be reactivated. The reactivation of
retinitis is known to develop at the border of old scars and
is attributed to the rupture of tissue cysts which are located
within old lesions. Sometimes, however, new lesions are found
at locations distant from old scars. Some studies have
suggested a possible route of infection from the brain to the
eye through the optic nerve; however, now ocular infection is
most likely mediated via the bloodstream (Park and Nam, 2013)
Immunity
Both cellular and humoral immune responses are associated with
toxoplasmosis. Acute infections produce IgA and IgM. The
occurrence of IgG in individuals indicates prior infection
with T. gondii. IgE antibodies severe infection (Otubanjo, 2013).
Diagnosis
Diagnosis is usually achieved by the following methods
Serology: Serological tests involves detecting specific
antibodies like IgM and IgG through ELISA.,
The Sabin-Feldman dye test
Tissue cysts may be observed in stained biopsy specimens.
Diagnosis of congenital infections can be achieved by
detecting T. gondii
Ploymerase chain reaction (PCR): DNA in amniotic fluid, cerebrospinal fluids, blood samples etc. can be detected using PCR
Treatment
Treatment is with combination of sulfadiazine and pyrimethamine.
TRANSMISSION OF T. gondii
T. gondii exists in 3 forms, all of which are possible to infect
hosts as a form of zoonosis. These forms are:
1. Tachyzoites; which can infect almost all nucleated cells
through a process of active invasion,
2. Tissue cysts (containing bradyzoites); which are formed
primarily in the brain and skeletal muscles during the chronic
phase of infection, and
3. Oocysts which are produced during the sexual cycle that
takes place in the intestine of acutely infected felines
(Tenter, et. al., 2000)
The routes of infection are therefore:
By ingestion of tissue cysts from undercooked or raw meat
(primarily pork and lamb) (Dubey, 2004; Dubey, 2010;
Dehkordi et. al., 2013) .
Direct contact with cats and owning of pets. This will
increase the proximity of humans to the cats (which
excrete oocysts with their faeces) and pets like dogs
have been found to be transport hosts of the parasite.
Consumption of water or food contaminated by oocysts
excreted in the faeces of infected cats (Montoya and
Liesenfeld, 2004).
Recently, T. gondii has been reported in many marine
mammals, suggesting the possibility that the
contamination of seawater with T. gondii may be more common
than realized (Dubey et al., 2003b).
Congenital infection; this may occur following maternal
infection during pregnancy.
Oocysts in soil can be spread mechanically by flies,
cockroaches, dung beetles, and earthworms.
Humans may also acquire toxoplasmosis by petting dogs
that have rolled over in infected cat faeces (Frenkel et
al., 1995; Lindsay et al., 1997). T. gondii infection in dogs
are important because the infection can cause serious
illness in dogs. It is important to note that dogs can
also be transport hosts for T. gondii oocysts and dog meat
is consumed by humans in several countries (Liu, et. al.,
2012).
Through organ transplant; Organ transplant recipients can
develop toxoplasmosis due to transmission of the parasite
with the transplanted organ from a Toxoplasma-seropositive
donor to a Toxoplasma-seronegative recipient. Heart
transplantation is the most common type of organ
transplantation procedure when this occurs, as cysts form
in the cardiac muscles (Martina et al. 2011; Derouin and
Pelloux 2012). However, toxoplasmosis is an uncommon
outcome from organ transplantation as only 5% of human
pathogenic parasites have reportedly caused significant
illness in transplant recipients (Barsoum 2006). It is
also possible that parasite transmission could occur as
the result of blood transfusion or haematopoietic stem
cell transplantation. The chance of either of these
occurring is very low and could only occur if the donor
was recently infected with T. gondii and so had tachyzoites
present in their blood and bone marrow (Derouin and
Pelloux 2012).
There is also pseudo-vertical transmission through the
milk, and sexual transmission through the sperm (Dubey,
2010; House, et. al., 2011; Dass, et. al., 2011).
LIFE CYCLE OF T. gondii
The organism undergoes both schizogonic and sexual cycles
typical of coccidians. It consists of two cycles which are the
intra-intestinal (enteric) cycle and Extra-Intestinal (exo-
enteric) cycle.
The Intra-intestinal cycle is characterized by a direct,
monoxenous life cycle in the intestine of the natural feline
definitive host, the domestic cat, and other feline host of
the genera; Felis and Lynx. This involves several schizogonic
cycle followed by gametogony (sexual reproduction. Sexual
reproduction occurs only in the cat.
The Extra-intestinal cycle is a heteroxenous cycle, involving
other mammalian hosts as intermediate hosts and also, the
feline host with strictly asexual reproduction. It involves
oocysts, sporozoites and tissue cysts bradyzoites.
Infection of the feline definitive host occurs when a cat
consumes an intermediate host (such as a mouse or bird)
infected with tissue cysts. Upon ingestion of a tissue cyst by
a susceptible cat, the walls of the cyst are digested by
proteolytic enzymes and bradyzoites are released. The
bradyzoites undergo asexual reproduction followed by sexual
reproduction in intestinal epithelial cells to produce
microgametocytes and macrogametocytes. The microgametocytes
fertilise the macrogametocytes, leading to the production of
zygotes. The zygotes differentiate into unsporulated oocysts
and are shed in the faeces of the definitive host (Ortega
2007; Jones and Dubey 2010).
After a prepatent period of up to 10 days following primary
infection with tissue cysts, a cat may shed more than 100
million oocysts into the environment over a 2-3 week period
(Tenter et al. 2000).
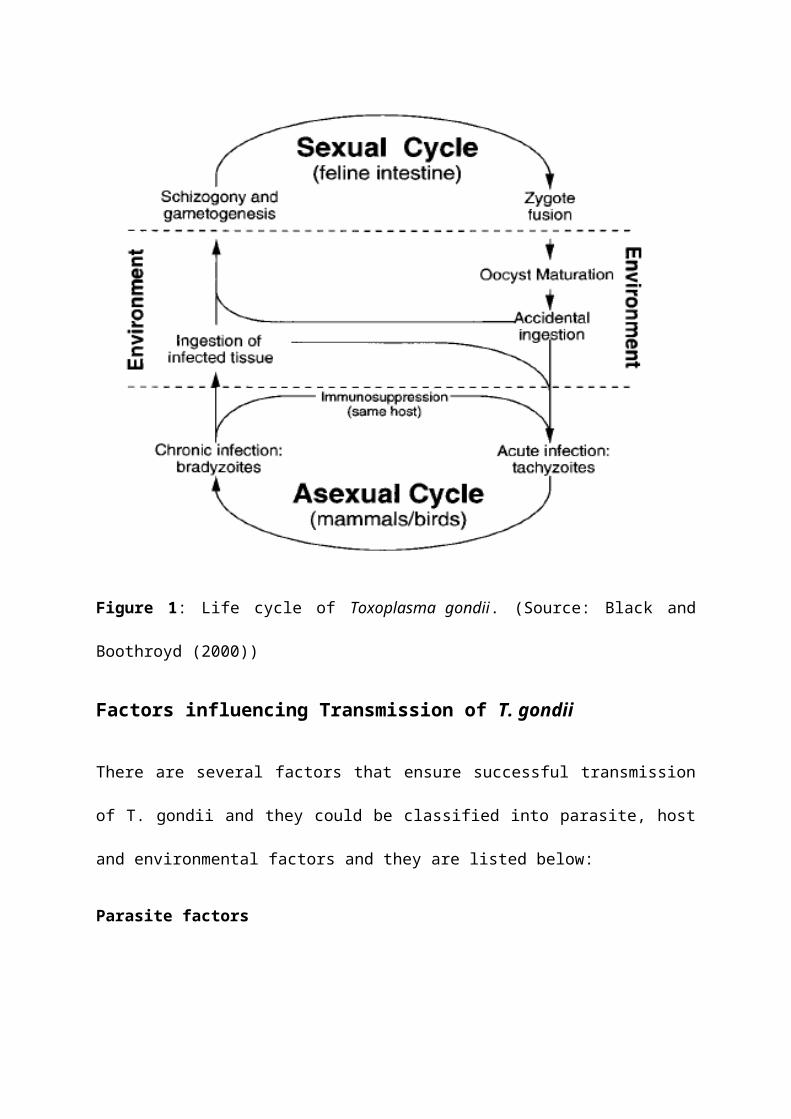
Figure 1: Life cycle of Toxoplasma gondii. (Source: Black and
Boothroyd (2000))
Factors influencing Transmission of T. gondii
There are several factors that ensure successful transmission
of T. gondii and they could be classified into parasite, host
and environmental factors and they are listed below:
Parasite factors
Toxoplasma gondii is considered as one of the most successful
parasites in the world.
This success is first illustrated by the worldwide
distribution of the parasite, from arctic to hot desert
areas, including isolated islands and in cities (Dubey,
2010).
The parasite also has the ability to affect host’s
behaviour. Infected rats are less fearful of the scent of
cats, thus making them readily available for predation by
the feline hosts. Infected humans are also prone to
behaviour changes such as hallucinations and reckless
behaviour (Otubanjo, 2013).
The parasite is able to infect, or be present in, the
highest number of host species: any warm-blooded animal
may act as an intermediate host, and oocysts may be
transported by invertebrates such as filtrating mussels
and oysters (Dubey, 2010; Miller, et.al., 2008).
Millions of infective oocysts can be shed and excreted
in a short period of time in the faeces of the cat (which
is the only definitive host) (Dubey, and prowell, 2013).
The ability of oocysts to survive for long periods.
Oocysts are known to survive on fruits and vegetables for
long periods (Kniel et al., 2002). Also, Sporulated oocysts
may survive during several years and may disperse through
water movements, soil movements and microfauna
High Infectivity of the parasite. Ingesting a single
sporulated oocyst may be sufficient to infect an
Intermediate Host and begin the asexual reproduction
phase (Dubey, 2010). This classical life cycle thus
relies on a prey predator relationship and on
environmental contamination, like other parasites
(Deplazes, et. al., 2004).
Host Factors
The presence of proteolytic enzymes in the gut of the cat
that helps to digest the walls of the cysts to release
the tissue cyst bradyzoites.
Predatory behaviour of cats, that is, cats could become
infected when they feed on rats whose tissues contain
tissue cysts (bradyzoites).
Socio-cultural practices of humans, that is, the practice
of eating raw or poorly cooked meat. It has been reported
that the prevalence is higher in areas where raw or
undercooked meat is traditionally eaten.
Owning pets like cats and dogs.
Maintaining poor personal hygiene, such as the habit of
not washing hands after handling pets.
The physiological state of the host. Studies have shown
that people most at risk of developing clinical symptoms
include immune-compromised individuals, pregnant women
who acquire (or have a reactivation of) the infection
during gestation, foetuses that are congenitally infected
and individuals who have previously been infected in utero
(Tenter et al. 2000; Jones et al. 2003; Montoya and
Liesenfeld 2004; ESR 2010).
Environmental Factors
The following conditions have been seen to affect the length
of time required for sporulation to occur,
Temperature and
High farm density.
Poor environmental sanitary conditions.
Temperature: It has been reported that the prevalence is
higher in warm and humid areas (Studeničová, et. al., 2006) and
in areas where raw or undercooked meat is traditionally eaten.
Studies have shown that lower temperatures slow the
sporulation rate (Lindsay et al. 2002; Jones et al. 2003; Hill et
al. 2007). A study conducted by Lindsay (2002) demonstrated
that unsporulated oocysts can survive in the environment at
4°C and retain their ability to sporulate for at least 3
months. Sporulated oocysts are more resilient than
unsporulated oocysts. Once sporulated, oocysts maintain
infectivity in moist soils for up to 18 months and in water
and seawater for several years at 4°C (Lindsay and Dubey
2009). The duration of infectivity, however, decreases with
increasing temperatures. Infectivity is maintained for at
least 200 days in the temperature range of 10–25°C, for 1
month at 35°C, for 1 day at 45°C and sporulated oocysts become
non-infective after 1 minute at 60°C (Dubey 1998a).
Unsporulated oocysts die within 24 hours when stored at 37°C,
whereas sporulated oocysts can survive for over a month at
35°C and 9 days at 40°C (Lindsay et. al. 2002). Constant freezing
at -21°C kills unsporulated and sporulated oocysts within 1
and 28 days, respectively (ESR 2010). T. gondii tissue cysts
remain viable in infected meat stored at refrigeration
temperatures of 4°C for up to 19 days. Cooking infected meat
to internal temperatures of 67°C or higher inactivates the
tissues cysts (Dubey 2004). Freezing meat at -10°C for 3 days
or -20°C for 2 days or treatment with gamma irradiation at a
dose of 75 krad is also sufficient to kill tissue cysts (El-
Nawawi et al. 2008). Tachyzoites that may be found in the milk
of intermediate hosts are inactivated by pasteurisation
(Tenter et al. 2000). Studies have shown that farming areas
and weather conditions such as cool and wet winters are
associated with increased T. gondii seroprevalence in cats. As
cat infection determines the environmental contamination by
oocysts, climate and landscape characteristics should be taken
into account to improve the risk analysis and prevention of T.
gondii (Afonso, et. al., 2013).
High farm density: Research has shown that areas with high
farm density are high risk places for the prevalence of T. gondii
because farms are favourable areas for the presence of
domestic cats (Turner and Bateson, 2000).
Poor Environmental Sanitary Condition: Environmental
condition such as contamination of the environment with
faeces of cats containing oocysts increase the chance of
infection.
REFERENCES
Afonso, E., Germain, E., Poulle, M., Ruette, S., Devillard,S., Say, L., Villena, I., Aubert, D., and Gilot-Fromont, E.(2013). Environmental Determinants of Spatial and TemporalVariations in the Transmission of Toxoplasma gondii in itsDefinitive Hosts. International Journal for Parasitology: Parasites andWildlife 2:278–285
Al-Azawi, A.K.A., Al-Rawe, I.H.A., and Al- Bayati, R.Y.J.(2013). Seroprevalance of Toxoplasmic chorioretinitis inBaghdad Province. International Journal of Science and Nature 4(1),68-71.
Alvarado-Esquivel, C., and Estrada-Martínez, S. (2011).Toxoplasma gondii Infection and Abdominal Hernia: Evidence of aNew Association. Parasit Vectors 4:112
Asad, Y., Abuodeh, M.D., Basem, S., and Hattar, M.D. (2006).Concurrent Malaria and Toxoplasmosis: A Case Report. JRMS;13(1): 48-50.
Ayi, I., Edu, A., Apea-Kubi, K., Boamah, D., Bosompem, K., andEdoh, D. (2009). Sero-epidemiology of Toxoplasmosis amongstPregnant Women in the Greater Accra Region of Ghana. Gh MedJ, 43:107-114
Berenreiterova, M., Flegr, J., Kubena, A.A.,and Nemec, P.(2011). The Distribution of Toxoplasma gondii Cysts in theBrain of a Mouse with Latent Toxoplasmosis: Implicationsfor the Behavioral Manipulation Hypothesis. PLoS One 6:e28925.
Black, M.W., and Boothroyd, J.C. (2000). Life Cycle ofToxoplasma gondii. Microbiol. Mol. Biol. Rev. 2000, 64(3):607.
Boyer, K.M., Holfels, E., Roizen, and N., (2005). Risk Factorsfor Toxoplasma gondii Infection in Mothers of Infants with
Congenital Toxoplasmosis: Implications for Pre-natalManagement and Screening. Am J Obstet Gynecol. 192:564–71.
Dass, S.A.H., Vasudevan, A., Dutta, D., Soh, L.J.T., Salposky,R.M, and Vyas, A. (2011). Protozoan Parasite Toxoplasma gondiiManipulates Mate Choice in Rats by Enhancing Attractivenessof Males. PLoS ONE 6: 27229.
Deplazes, P., Hegglin, D., Gloor, S., and Romig, T. (2004).Wilderness in the City: The Urbanization of Echinococcusmultilocularis. Trends parasitol 20: 77-84.
Dubey JP (1998a) Toxoplasma gondii Oocyst Survival Under Defined Temperatures. Journal of Parasitology 84(4):862–865.
Dubey, J.P., Zarnke., R., Thomas, N.J., Wong, S.K., Van Bonn,W., Davis, J.W., Ewing, R., Mense, M., Kwok, O.C.H.,Beckmen, K.B., Romand, S., and Thulliez, P., (2003b).Toxoplasma gondii, Neospora caninum, Sarcocystis neurona, andSarcocystis canis-like Infections in Marine Mammals. Vet. Parasitol.116, 275–296.
Dubey, J.P. (2010). Toxoplasmosis of animals and humans, 2ndedition. Boca Raton: CRC Press. 313 p.
Dubey, J.P., and Jones, J.L. (2008). Toxoplasma gondii Infectionin Humans and Animals in the United States. Int J Parasitol.38:1257-1278
Dubey, J.P., and Prowell, M., (2013). Ante-mortem Diagnosis,Diarrhoea, Oocyst Shedding, Treatment, Isolation andGenetic Typing of Toxoplasma gondii Associated with ClinicalToxoplasmosis in a Naturally Infected Cat. J. Parasitol.99(1):158-160).
El-Nawawi, F.A., Tawfik, M.A., and Shaapan, R.M. (2008)Methods for Inactivation of Toxoplasma gondii cysts in Meat andTissues of Experimentally Infected Sheep. Foodborne Pathogensand Disease 5(5):687–690
ESR (2010) Toxoplasma gondii. Ministry for Primary Industries, New Zealand.
Ferreira, S.M., and Borges, S.A.(2002). Some Aspects ofProtozoan Infections in Immune Compromised Patients – Areview. BioLine Int System, 97(4):443–457.
Gao, X.J., Zhao, Z.J., He, Z.H., Wang, T., Yang, T.B., Chen, X.G., Shen, J.L., Wang, Y., Lv, F.L., Hide, G., and Lun, Z.R. (2012). Toxoplasma gondii Infection in Pregnant Women in China. Parasitology, 139:139-147
Gilot-Fromont, E., Lélu, M., Dardé, M.L., Richomme, C.,Aubert, .D., Afonso, E., Mercier, A., Gotteland, C., andVillena, I. (2012). The Life Cycle of Toxoplasma gondii in theNatural Environment.
Hill, D.E., Sreekumar, C., Jones, J., and Dubey, J.P. (2007) Toxoplasma gondii. Ch 12 In: Simjee S (ed) Foodborne diseases.Humana Press, Totowa, p. 337–353
House, P.K., Vyas, A., and Sapolsky, R. (2011). Predator CatOdours Activate Sexual Arousal Pathways in Brains ofToxoplasma gondii Infected Rats. PLoS ONE 6: 23277.
Innes, E.A. (2010). A brief history and overview of Toxoplasmagondii. Zoon Pub Heal. 57, 1–7.
Jayawardena, S., Singh, S., Burzyantseva, O., and Clarke, H.(2008): Cerebral Toxoplasmosis in Adult patients with HIVinfection. Clin Med J Resid Hosp Physician 44(7):17–24.
Jones, J., Lopez, A., and Wilson, M. (2003). Congenital Toxoplasmosis. American Family Physician 67(10):2131–2138.
Lindsay, D.S., and Dubey, J.P. (2009). Long-term Survival of Toxoplasma gondii Sporulated Oocysts in Seawater. Journal of Parasitology 95(4):1019–1020
Lindsay, D.S., Blagburn, B.L., and Dubey, J.P. (2002) Survivalof Non-sporulated Toxoplasma gondii Oocysts Under RefrigeratorConditions. Veterinary Parasitology 103(4):309–313.
Malla, N., Sengupta, C., Dubey, M.L., Sud, A., and Dutta, U:(2005). Antigenaemia and Antibody Response to Toxoplasmagondii in Human Immuno deficiency Virus Infected Patients. BrJ Biomed Sci 28:104–109.
Martinez, E., Mago, H., Rocha, R., and Pacheco, M. (2002):Epidemiological findings and Prevalence of Toxoplasma gondiiantibodies in HIV-positive patients in a Venezuelanhospital. Valencia Int Conf AIDS . 7–12:14.
Miller, M.A., Miller, W.A., Conrad, P.A., James, E.R., Melli,A.C., Leutenegger, C.M., Dabritz, H.A., Packham, A.E.,Paradies, D., Harris, M., Ames, J., Jessup, D.A.,Worcester, K., and Grigg, M.E. (2008). Type X Toxoplasmagondii in a Wild Mussel and Terrestrial Carnivores fromCoastal California: New Linkages between TerrestrialMammals, Runoff and Toxoplamosis of sea otters. Int. j. parasitol58: 928-937.
Montoya, J.G., and Remington, J.S. (2000): Toxoplasma gondii. InPrinciples and Practice of
Infectious diseases. 5th ed. Edited by Mandell, G.E.,Beneth, J.E., Dolin, R.Odon: Churchill Livingstone;2000:2858–2888.
Montoya, J.G., and Liesenfeld, O. (2004). Toxoplasmosis.Lancet, 363:1965–1976.
Nissapatorn, V., Kamarulzaman, A., Init, I., Tan, L.H.,Rohela, M., Norliza, A., Chan, L.L.,
Latt, H.M., Anuar, A.K., and Quek, K.F. (2002):Seroepidemiology of Toxoplasmosis among HIV- infectedPatients and Healthy Blood Donors. Med J Malaysia, 57(3):304–310.
Nowakowska, D., Stray-Pedersen, B., Spiewak, E., Sobala, W.,Małafiej, E., and Wilczyński, J. (2006). Prevalence andEstimated Incidence of Toxoplasma infection Among PregnantWomen in Poland: a decreasing trend in the youngerpopulation. Clin Microbiol Infect 12:913-917
Otubanjo, O., (2013). Elements of Parasitology, Panaf Publishers,Inc., Nigeria, Pp. 169-171
Oyibo, W.A., Oladosu, O.O., Agomo, C.O., Ojuromi, O.T.,Anunobi, C.C., and Soyebi, K. (2009). CongenitalToxoplasmosis: A Review of its Pathology, Immune Response
and Current Treatment Options. Sierra Leone J Biomed Res 1 (1),9-20,
Pappas, G., Roussos, N., Falagas, and M. E.(2009).Toxoplasmosis Snapshots: Global Status of Toxoplasma gondiiSeroprevalence and Implications for Pregnancy andCongenital Toxoplasmosis. Int J Parasitol 39: 1385-94
Park, Y.H., and Nam, H.W. (2013). Clinical Features andTreatment of Ocular Toxoplasmosis. Korean J Parasitol. 51(4):393–399.
Petersen, E. (2007). Toxoplasmosis. Semin Fetal Neonatal Med, 12,214–223.
Qing-Xin, L., Shuai, W., Li-Qun, W., Jun, X., Wen-Jue, G.,Guo-Fang, L., Bin, Z., Hai-Bin, Z., and Li-Hua, G. (2014).Seroprevalence of Toxoplasma gondii Infection in Dogs and Catsin Zhenjiang City, Eastern China. Asian Pac J. Trop Biomed 4(9):725-728
Remington, J.S., McLeod, R., Thuilliez, P., and Desmonts, G.,(2006). Toxoplasmosis. In: Remington, J.S., Klein, J.O.,Wilson, C.B., and Baker, C., (eds.). Infectious Diseases ofthe Foetus and New-born Infant. 6th ed. Philadelphia:Elsevier Saunders, 947–1091.
Robert-Gangneux, F., Year, H., D'Herve, D., Guiguen, C.(2009). Congenital Toxoplasmosis after a Preconceptional orPericonceptional Maternal Infection. Pediatr Infect. Dis. J. 28,660-661
Studeničová, C., Benčaiová, G., and Holková., R. (2006).Seroprevalence of Toxoplasma gondii Antibodies in a healthypopulation from Slovakia. Eur J Intern Med . 17:470–473.
Swai, E.S., and Schoonman, L. (2009). Seroprevalence ofToxoplasma gondii Infection Amongst Residents of TangaDistrict in North-East Tanzania. Tanz J Hth Res, 11(4):205–209.
Tenter, A.M., Heckeroth, A.R., and Weiss, L.M. (2000).Toxoplasma gondii: From Animals to Humans. Int. j. parasitol. 30:1217-1258.
Turner, D.C., and Bateson, P.B., (2000). The Domestic Cat. TheBiology of its Behaviour.
Cambridge University Press, Cambridge.
Walker, M., and Zunt, J.R. (2005): Parasitic central nervoussystem infections in Immunocompromised hosts. Clin Inf Dis40:1005–1015.
Related Documents