Data on burden of pneumonia in the country is limited

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript
Data on burden of pneumonia in the country is limited

Top Killer of Children: Pneumonia
Maria Rosario Z. Capeding, M.D.Research Institute for Tropical Medicine

Pneumonia remains to be a major cause of morbidity and mortality among Filipino children.

Region I: 400Region II: 600
Region III: 250
Region IV-A: 700
Region IV-B: 350
Region V: 3200
Region VI: 900Region VII: 800
Region VIII: 1400
Region IX: 650
Region X: 600
Region XI: 1300
Region XII: 1200
NCR: 450
CAR: 1750
CARAGA: 450
ARMM:
Pneumonia Morbidity Rate by RegionRate per 100,00 population
2008
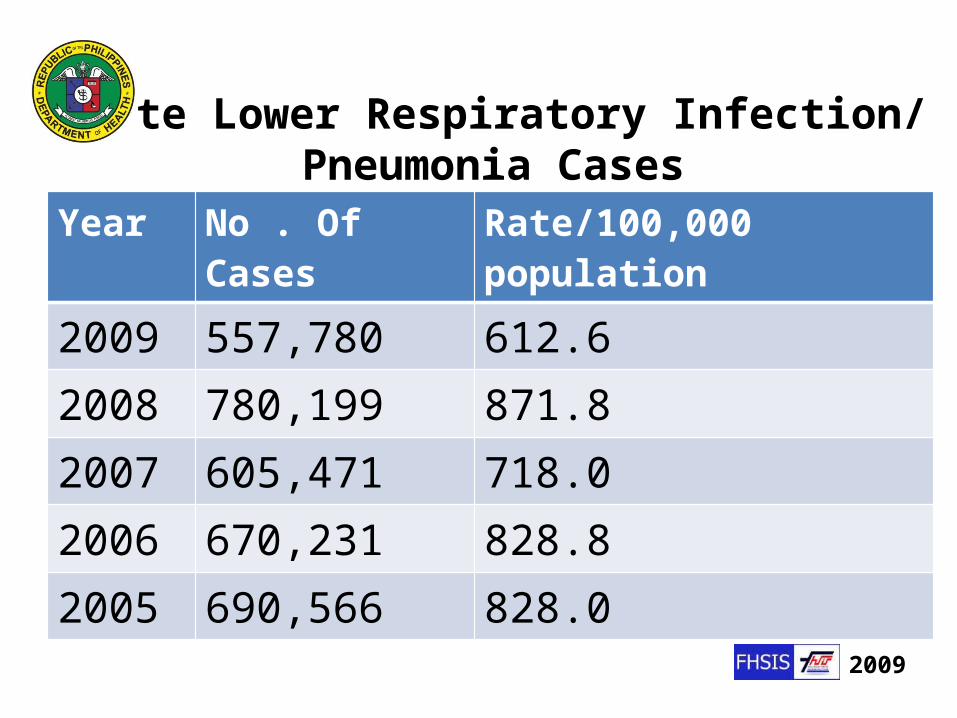
Acute Lower Respiratory Infection/Pneumonia Cases
Year No . Of Cases Rate/100,000 population2009 557,780 612.62008 780,199 871.82007 605,471 718.02006 670,231 828.82005 690,566 828.0
2009
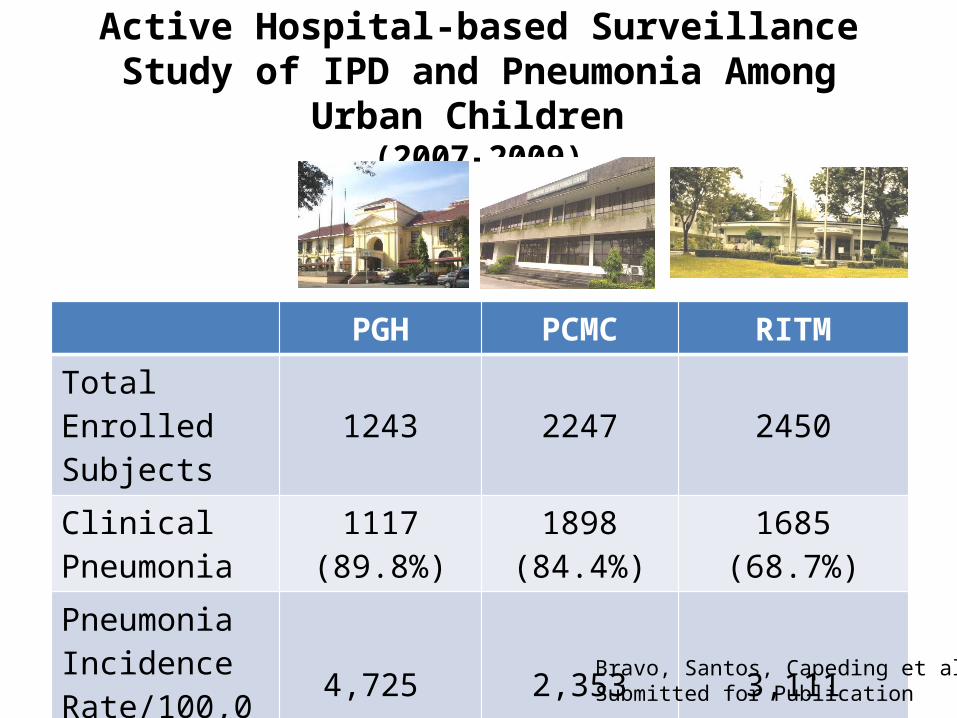
Active Hospital-based Surveillance Study of IPD and Pneumonia Among Urban Children
(2007-2009)
PGH PCMC RITMTotal Enrolled Subjects 1243 2247 2450
Clinical Pneumonia
1117 (89.8%)
1898 (84.4%)
1685(68.7%)
PneumoniaIncidence Rate/100,000
4,725 2,353 3,111
Bravo, Santos, Capeding et al Submitted for Publication

Younger Children Bore the Greatest Burden of Pneumonia
< 1 yr 1-4 yrs 5-14 yrs 15-49 yrs 50-64 yrs > 65 yrs0
50000
100000
150000
200000
250000
300000
350000
Pneumonia and LRTI
No.
of c
ases
2008

Risk factors for Pneumonia:
Definite Likely Possible
Malnutrition Low birth weight Non-exclusive breastfeeding (1st 4 mos of life)Lack of measles immunizationIndoor air pollutionCrowding
Parental smoking Zinc deficiency Mother’s experience as caregiver Concomitant diseases (diarrhea, heart dis, asthma)
Mother's education Day-care attendance Rainfall (humidity) High altitude (cold air) Vit. A deficiency Birth order Outdoor air pollution
Rudan et al. WHO Bulletin 2008 May 2008, vol 86 no 5; Pneumonia: The Forgotten Killer of Children Unicef/WHO 2006

Outcome of Childhood Pneumonia EVRMC 2008-2011
Died TotalPneumonia, neonatal 1 (4.7%) 21Pneumonia 9 (6.5%) 137Pneumonia, severe 20 (2.4%) 817Pneumonia, very severe 78 (12.8%) 605Mortality Rate 26.4% 1,580
Lupisan et al Asia-Africa Congress on Emerging and Re-emerging Infections Kobe, Japan January 2012

Lucero, et al. Reviews Inf Dis 1990
Pre Hib/PCV Era
S. pneumo15%Mixed
Viral/bacterial23%
Hinfluenzae
21%
Styphi14%
Others17%
RSV37%
Adenov 13%
Parainfluenza17%
Etiology of Pneumonia in <5 Years Old 1984-1986, RITM, N=537

Etiology of Pneumonia in <5 Years Old 1990-1992, RITM, N=332
Bacterial11%
Viral 19%
No Pathogens Found
62%S. Pneumo
4.4%
H. in-fluenzae
4.0%
Others2.6%
Bacterial Pathogens
Adenovirus6.0%
RSV19%
Others2.6%
Viral Pathogens
S. aureusK. pneumoniaeS. viridansA. anitratum
ParainfluenzaInfluenza A and B
Pre Hib/PCV Era
Capeding et al. Etiology of ALRI in Filipino Children under 5 yearsSoutheast Asian J Trop Med Public Health, Dec. 1994

Etiology of Pneumonia in <5 Years Old 2008-2011, EVRMC N=1582
Bacteria6 %
Vi-ral 38%No Pathogens
Found56%
Hib/PCV Era S. pneumoniaeH. influenzaeOthersS. aureusMRSAS. typhi
RSV 14%Rhino-A 7%Rhino-C 6%hMPV* 3.3%OthersInfluenza A (H1N1)Influenza A/BAdenovirus Parainfluenza
Lupisan et al Asia-Africa Congress on Emerging and Re-emerging Infections Kobe, Japan January 2012
Determining Bacterial Etiology in Childhood Pneumonia is Challenging
• Use of conventional bacterial culture considered as gold standard but with low sensitivity
• Bacteria (S. pneumoniae, H. influenzae) are fastidious organisms
• High percentage of antibiotic usage prior to hospitalization

Mortality Rate by Case Definitions EVRMC
Pneumonia, neonatal
0.9%Pneumonia
8.3%
Pneu-monia, severe 18.5%
Pneu-monia,
very severe72.2%
Total number of cases = 108
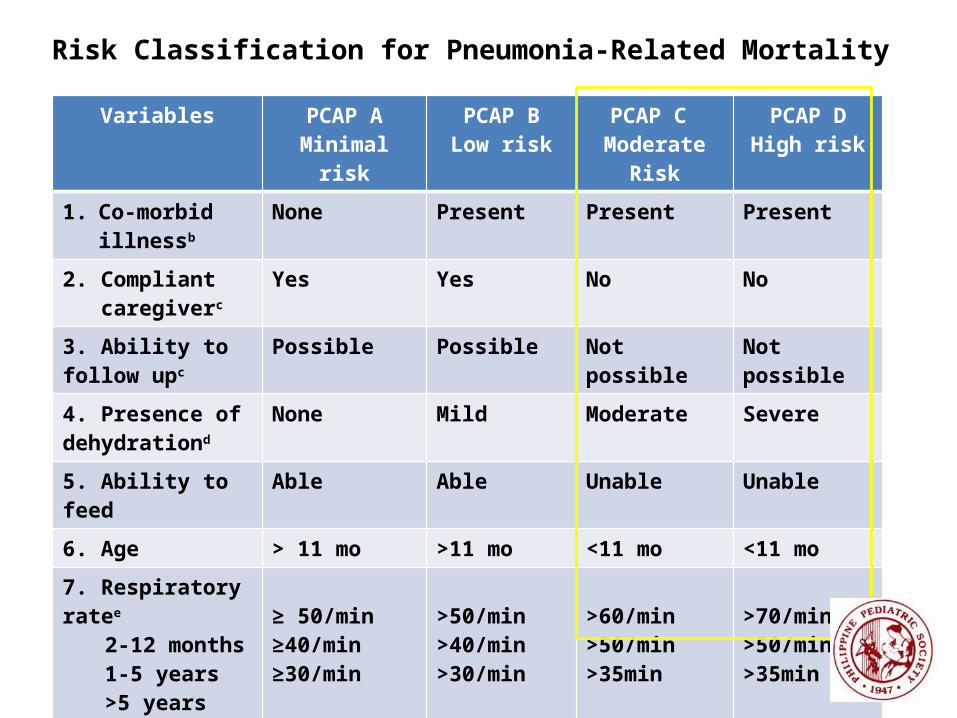
Variables PCAP AMinimal risk
PCAP BLow risk
PCAP C Moderate Risk
PCAP DHigh risk
1. Co-morbid illnessb
None Present Present Present
2. Compliant caregiverc
Yes Yes No No
3. Ability to follow upc
Possible Possible Not possible Not possible
4. Presence of dehydrationd
None Mild Moderate Severe
5. Ability to feed Able Able Unable Unable
6. Age > 11 mo >11 mo <11 mo <11 mo
7. Respiratory ratee 2-12 months1-5 years>5 years
≥ 50/min≥40/min≥30/min
>50/min>40/min>30/min
>60/min>50/min>35min
>70/min>50/min>35min
Risk Classification for Pneumonia-Related Mortality
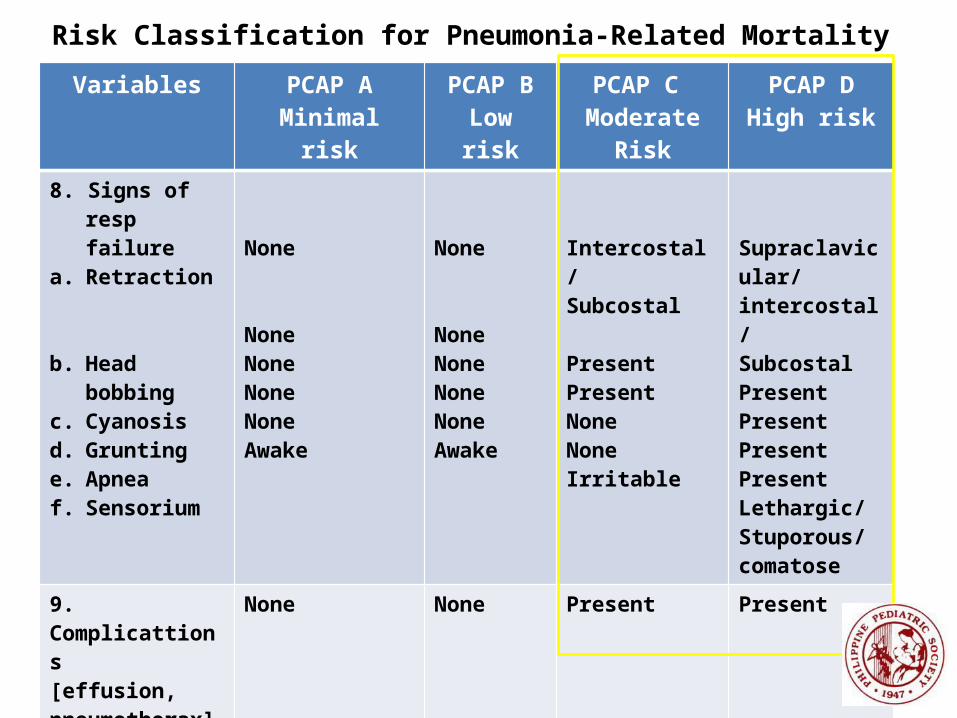
Risk Classification for Pneumonia-Related MortalityVariables PCAP A
Minimal riskPCAP BLow risk
PCAP C Moderate Risk
PCAP DHigh risk
8. Signs of resp failure
a. Retraction
b. Head bobbingc. Cyanosisd. Gruntinge. Apneaf. Sensorium
None
NoneNoneNoneNoneAwake
None
NoneNoneNoneNoneAwake
Intercostal/Subcostal
PresentPresentNoneNoneIrritable
Supraclavicular/intercostal/SubcostalPresentPresentPresentPresentLethargic/Stuporous/comatose
9. Complicattions[effusion, pneumothorax]
None None Present Present
ACTION PLAN OPDF
Follow-up at the end of treatment
OPDF
Follow-up after 3 days
Admit to regular ward
Admit to a critical care unit Refer to Specialist

Empiric Antibiotic Treatment
1. PCAP A or B without previous antibiotic Oral amoxicillin, drug of choice
2. PCAP C without previous antibiotic and complete Hib vaccination.
Penicillin G, drug of choice
3. PCAP C with incomplete Hib vaccination Ampicillin IV
4. PCAP D Refer to Specialist
CPG, In the Evaluation and Management of Pediatric Community Acquired Pneumonia
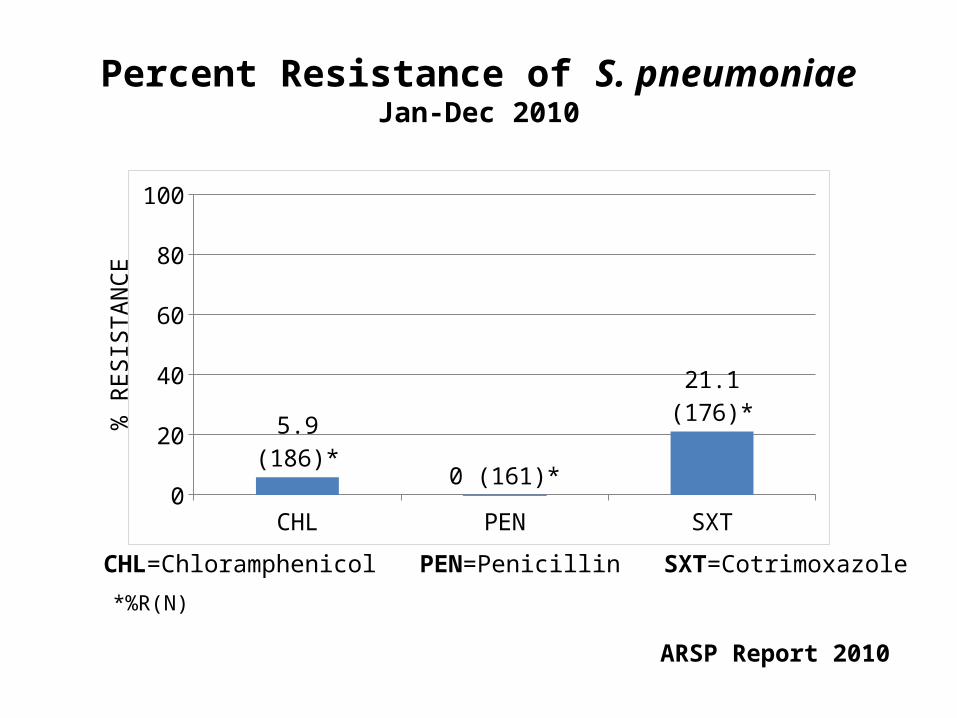
Percent Resistance of S. pneumoniaeJan-Dec 2010
CHL PEN SXT0
20
40
60
80
100
5.9 (186)*0 (161)*
21.1 (176)*% R
ESIS
TAN
CE
CHL=Chloramphenicol PEN=Penicillin SXT=Cotrimoxazole
*%R(N)
ARSP Report 2010

Clinical Management of Viral Etiology
1. In laboratory confirmed influenza A or B virus infection.
a. Influenza A: amantadine for 3-5 days, an option to discontinue within 24-48 hours after resolution of symptoms
b. Influenza A or B: oseltamivir for 5 days 2. Both drugs should be administered within 48
hours of onset of symptoms, ineffective against respiratory viruses other than influenza, not recommended for children below 1 year old
CPG, In the Evaluation and Management of Pediatric Community Acquired Pneumonia

Burden of Pneumonia Over the Past Decades
• Pneumonia is the most common presentation of IPD in children.
• Most commonly affects the very young • S. pneumoniae, H. influenzae and RSV
consistently are the most frequently detected pathogens
• Pneumonia is the top killer of Filipino children <5 years old, accounts for 34% of deaths
the90’s
Related Documents



![Pneumonia and Respiratory Tract Infections in Children[1]](https://static.cupdf.com/doc/110x72/577d27341a28ab4e1ea34b0a/pneumonia-and-respiratory-tract-infections-in-children1.jpg)


![Community acquired pneumonia [cap] in children](https://static.cupdf.com/doc/110x72/5454e4c4af795946778b8712/community-acquired-pneumonia-cap-in-children.jpg)




