Trauma Top 10 2014-15 @EMManchester

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript
Trauma Top 10 2014-15
@EMManchester


@EMManchester


10



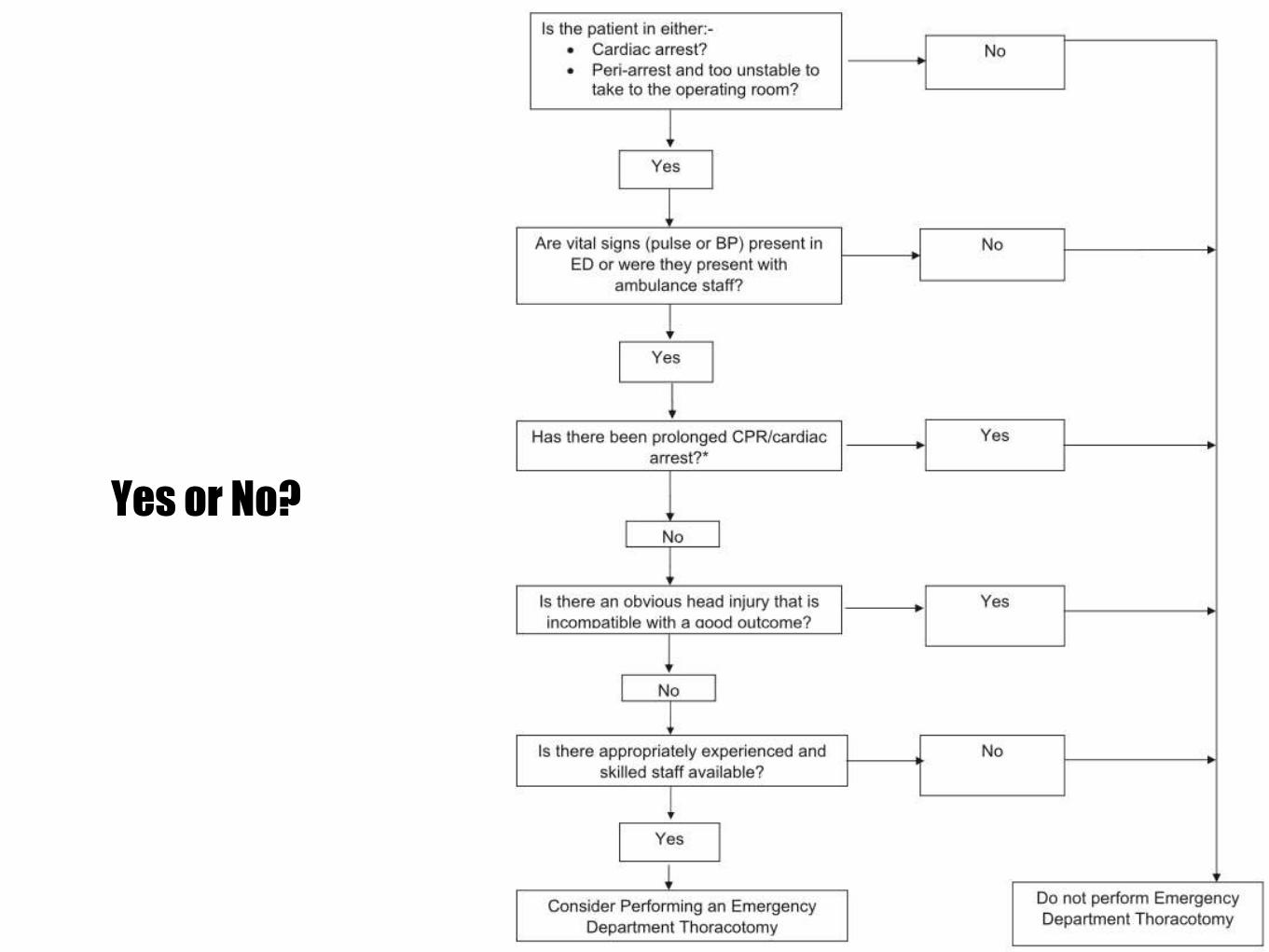
Yes or No?

9


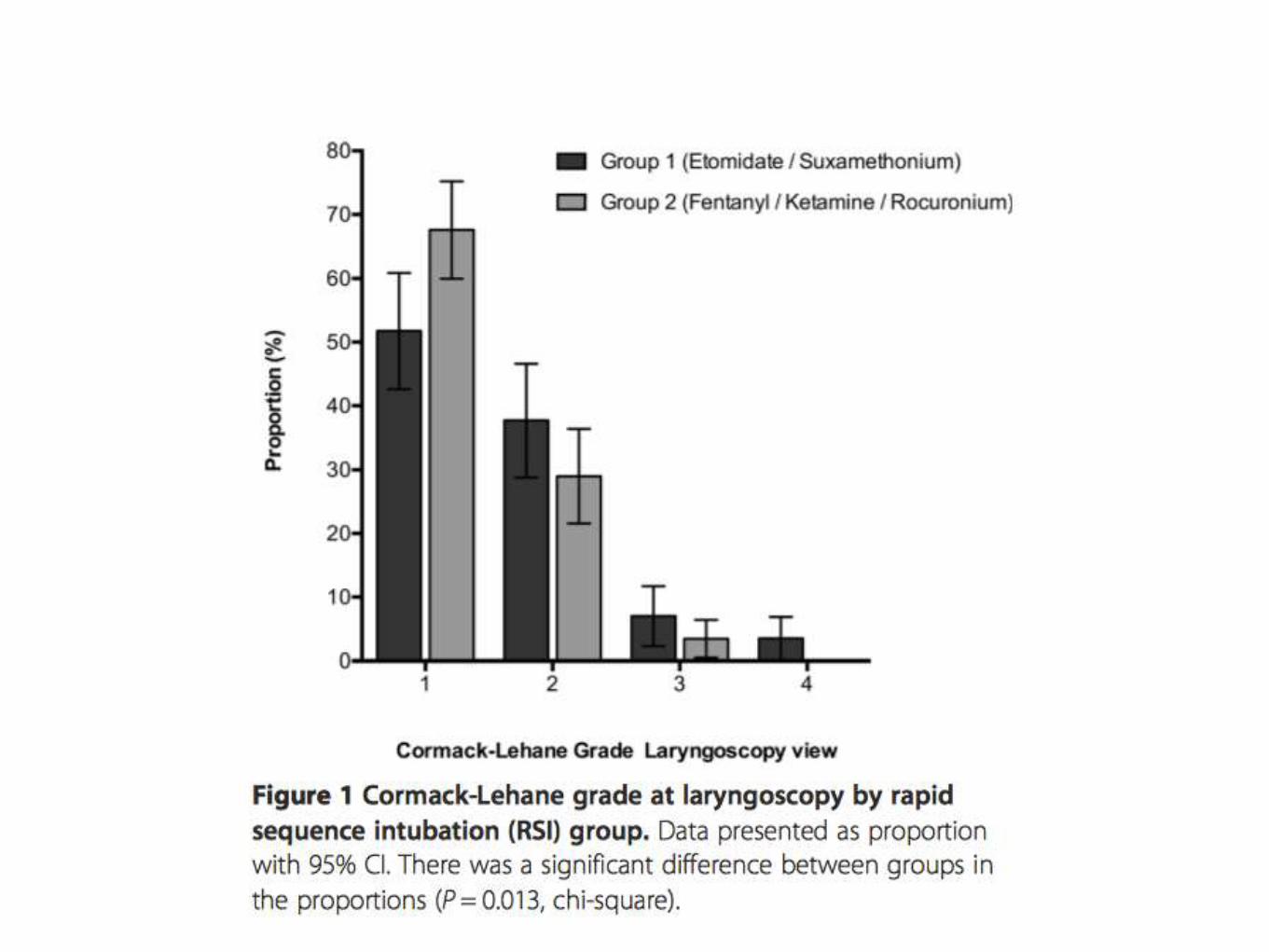
Gp 1. 0.3mg/Kg Etomidate + 1.5mg/Kg Suxamethonium
Gp2a. 3mcg/Kg Fentanyl + 2mg/Kg Ketamine + 1mg/Kg Rocuronium
Gp2b. 1mcg/Kg Fentanyl + 1mg/Kg Ketamine + 1mg/Kg Rocuronium

Screenshot 2015-04-18 10.04.48

8

http://www.sciencedirect.com/science/article/pii/S0020138314006731

10 Trauma Centres
Patients surviving >30 mins and who received blood
966 patients included
23% received major transfusion
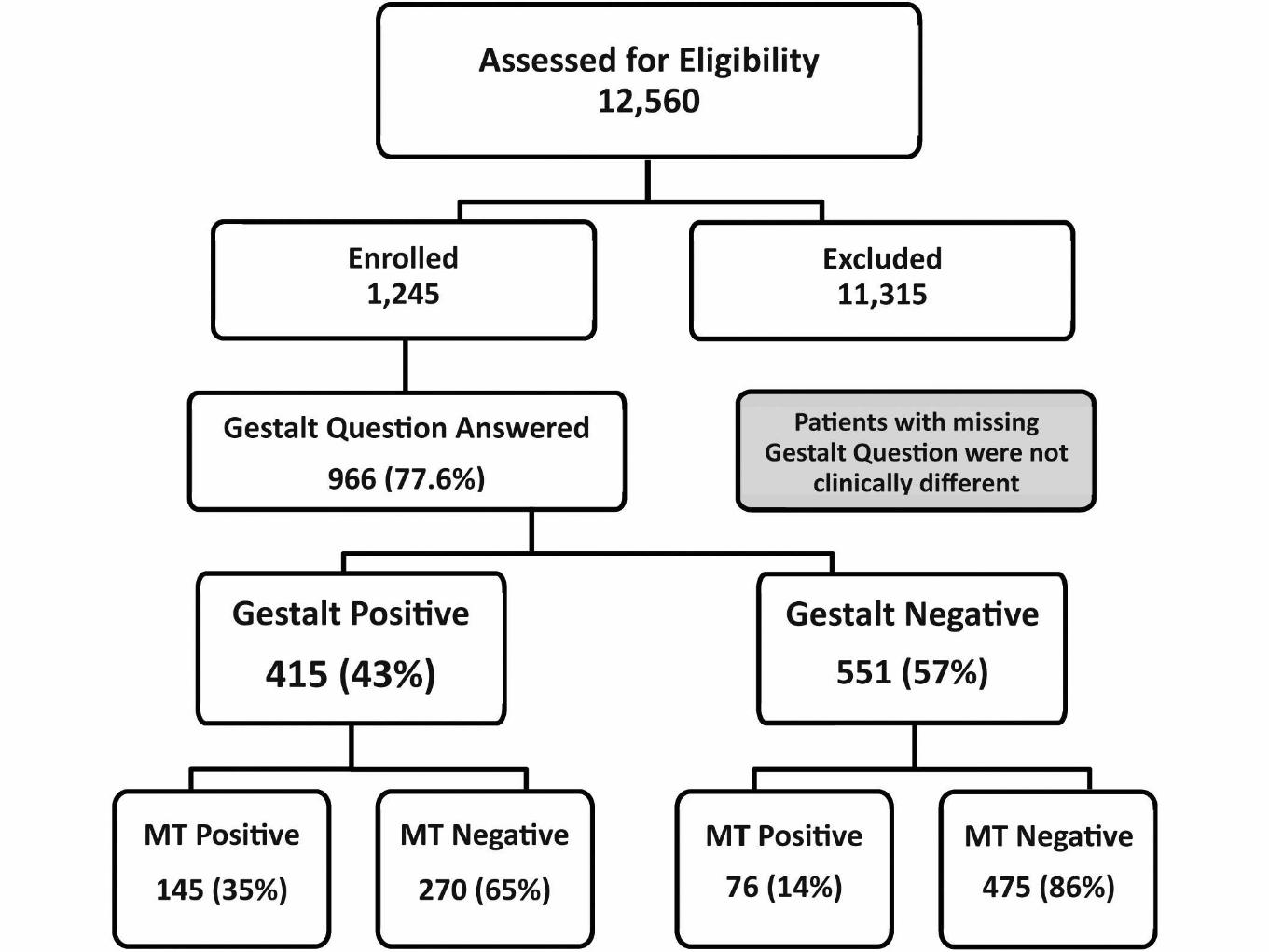

Sensitivity 65.6%
Specificity 63.8%
7

http://www.nejm.org/doi/full/10.1056/NEJMoa1404304

http://www.nejm.org/doi/full/10.1056/NEJMoa1404304
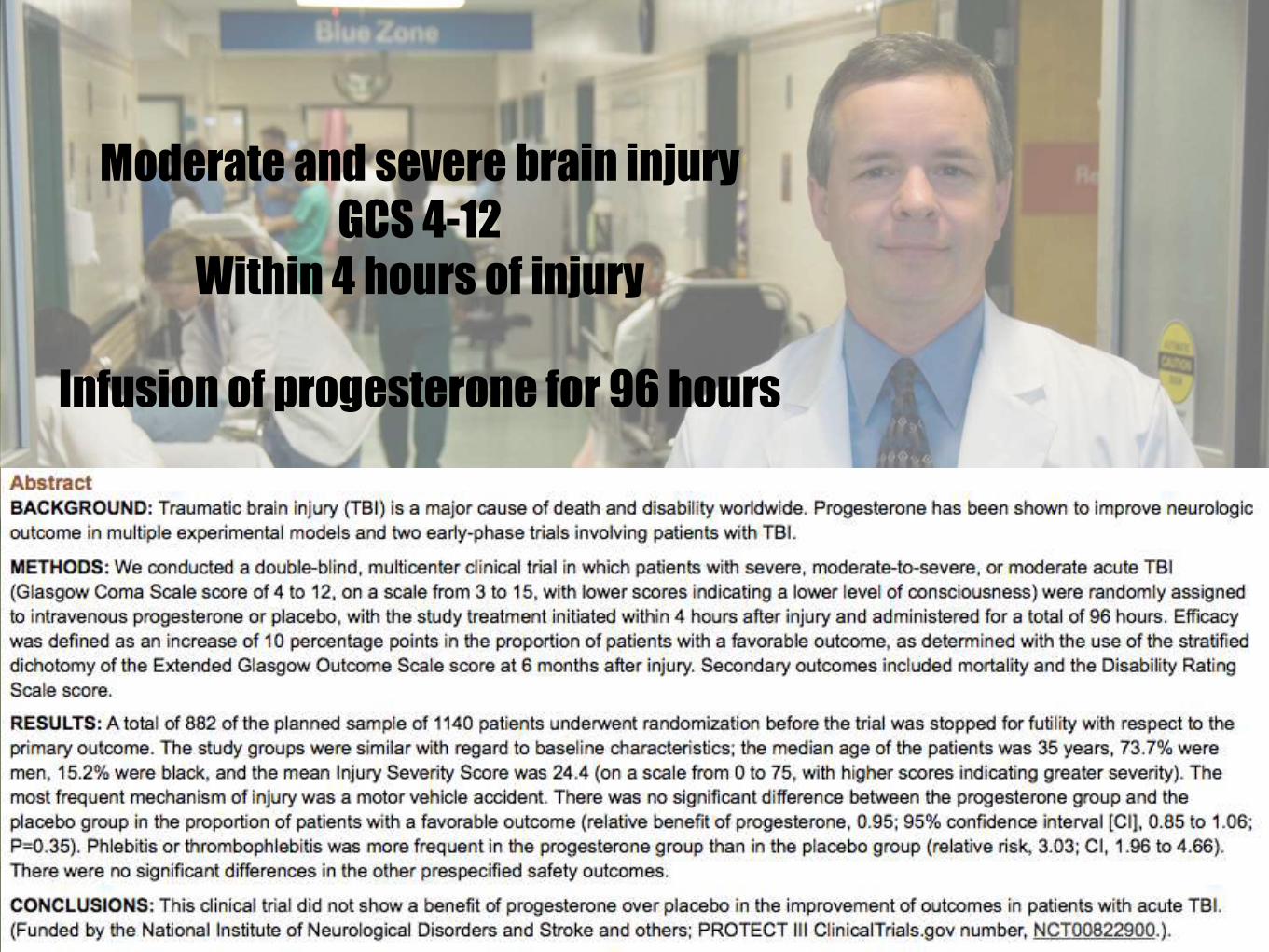
Moderate and severe brain injury
GCS 4-12
Within 4 hours of injury
Infusion of progesterone for 96 hours


6


5




4


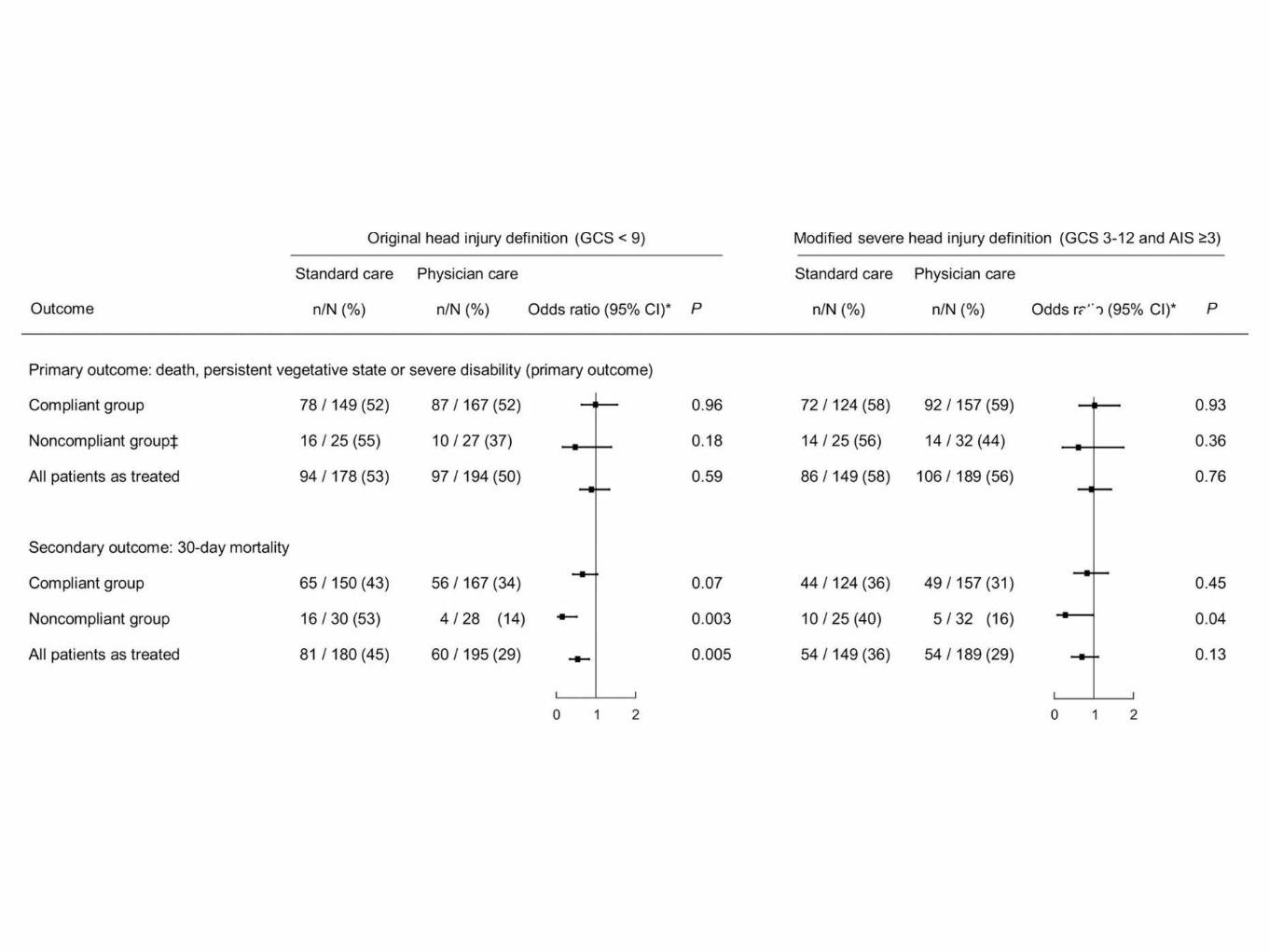
http://prehospitalmed.com/2015/03/24/a-response-to-the-hirt-trial/
Method
Protocols
Time
Reproducibility

3

http://emj.bmj.com/content/early/2014/11/09/emermed-2014-204260.full.pdf+html

e


2

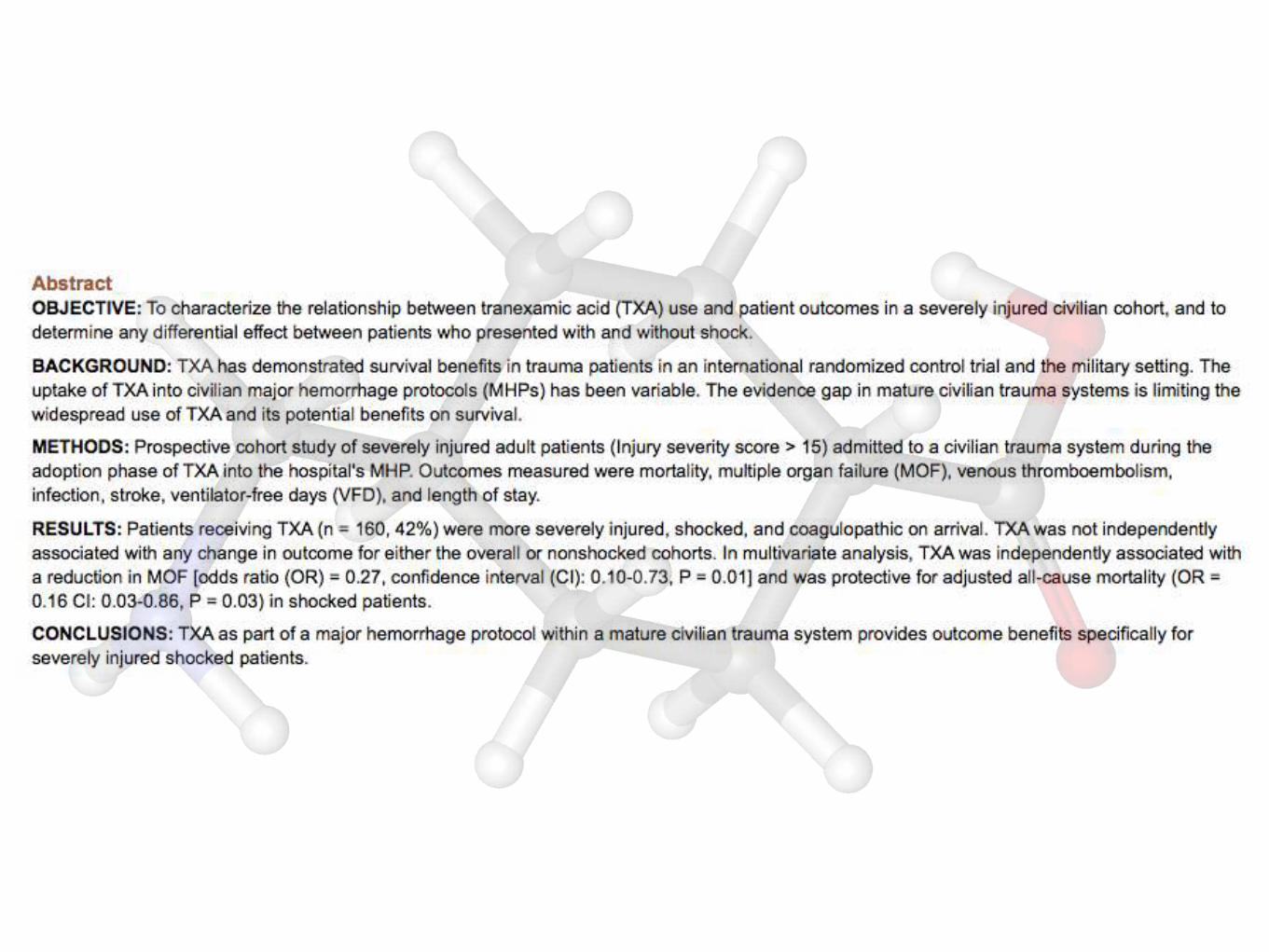
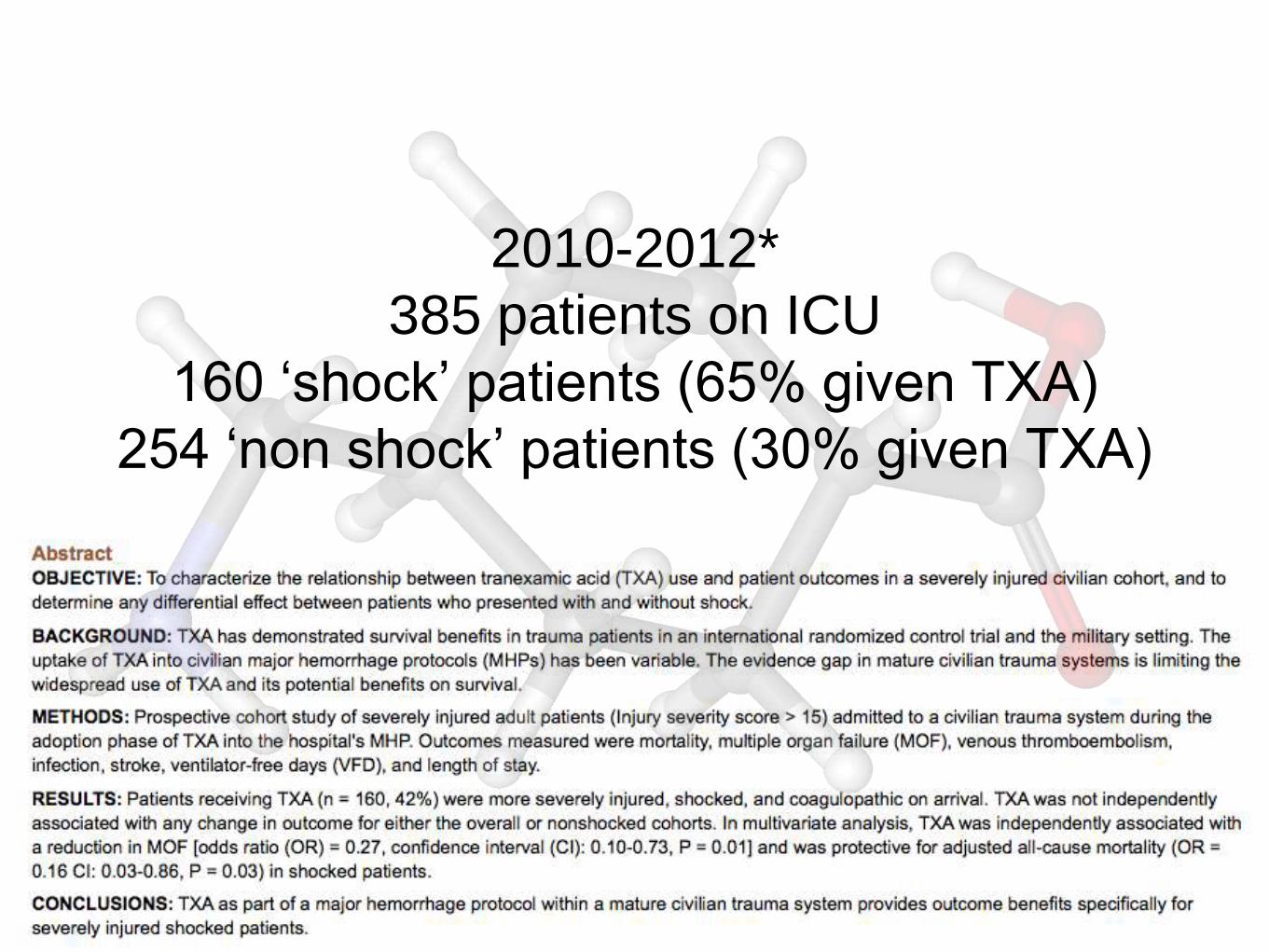
2010-2012*
385 patients on ICU
160 ‘shock’ patients (65% given TXA)
254 ‘non shock’ patients (30% given TXA)


1
http://jama.jamanetwork.com/article.aspx?articleid=2107789

http://jama.jamanetwork.com/article.aspx?articleid=2107789



http://www.wessexics.com/The_Bottom_Line/Review/index.php?id=7495881379650332408
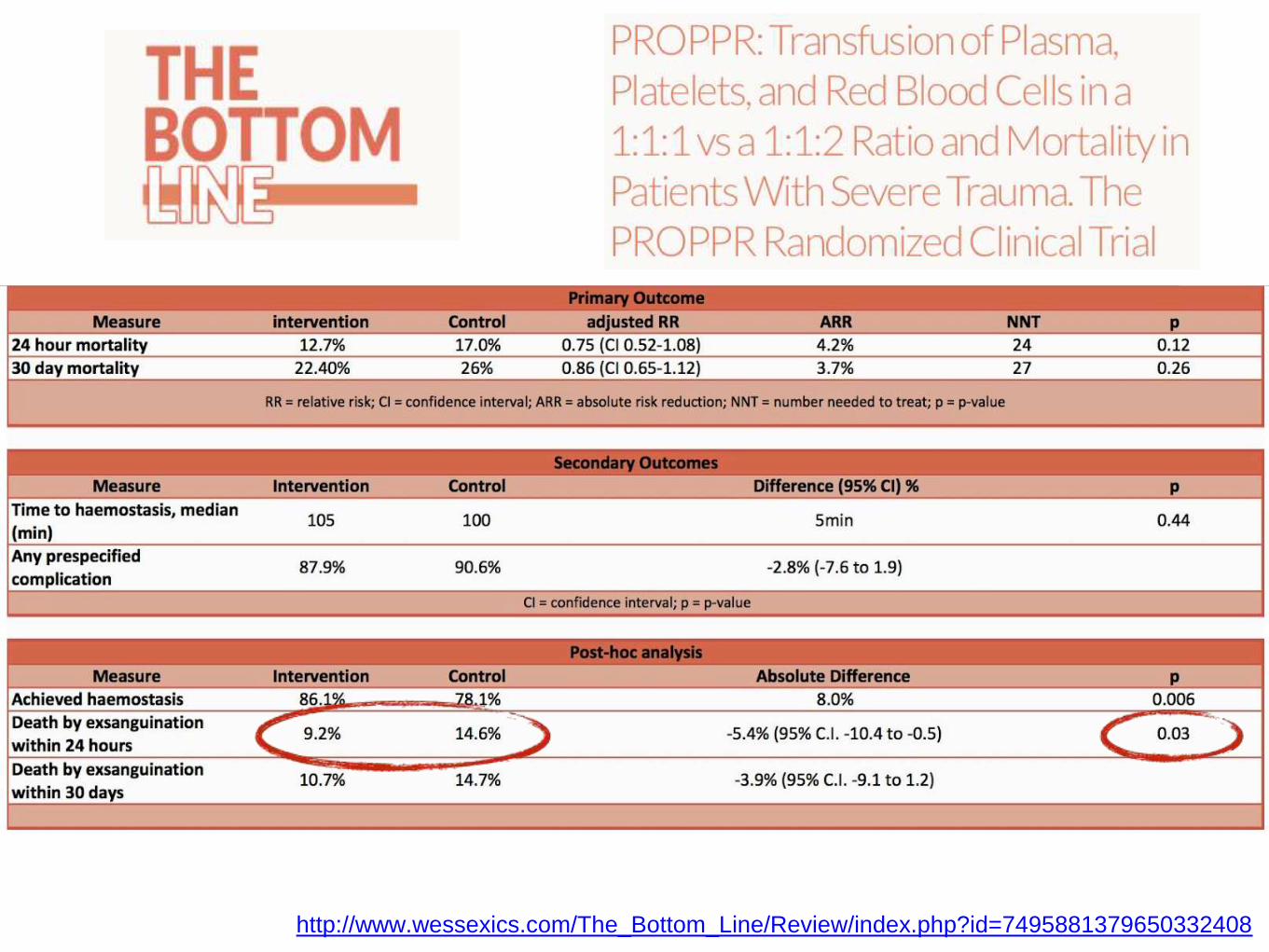
http://www.wessexics.com/The_Bottom_Line/Review/index.php?id=7495881379650332408

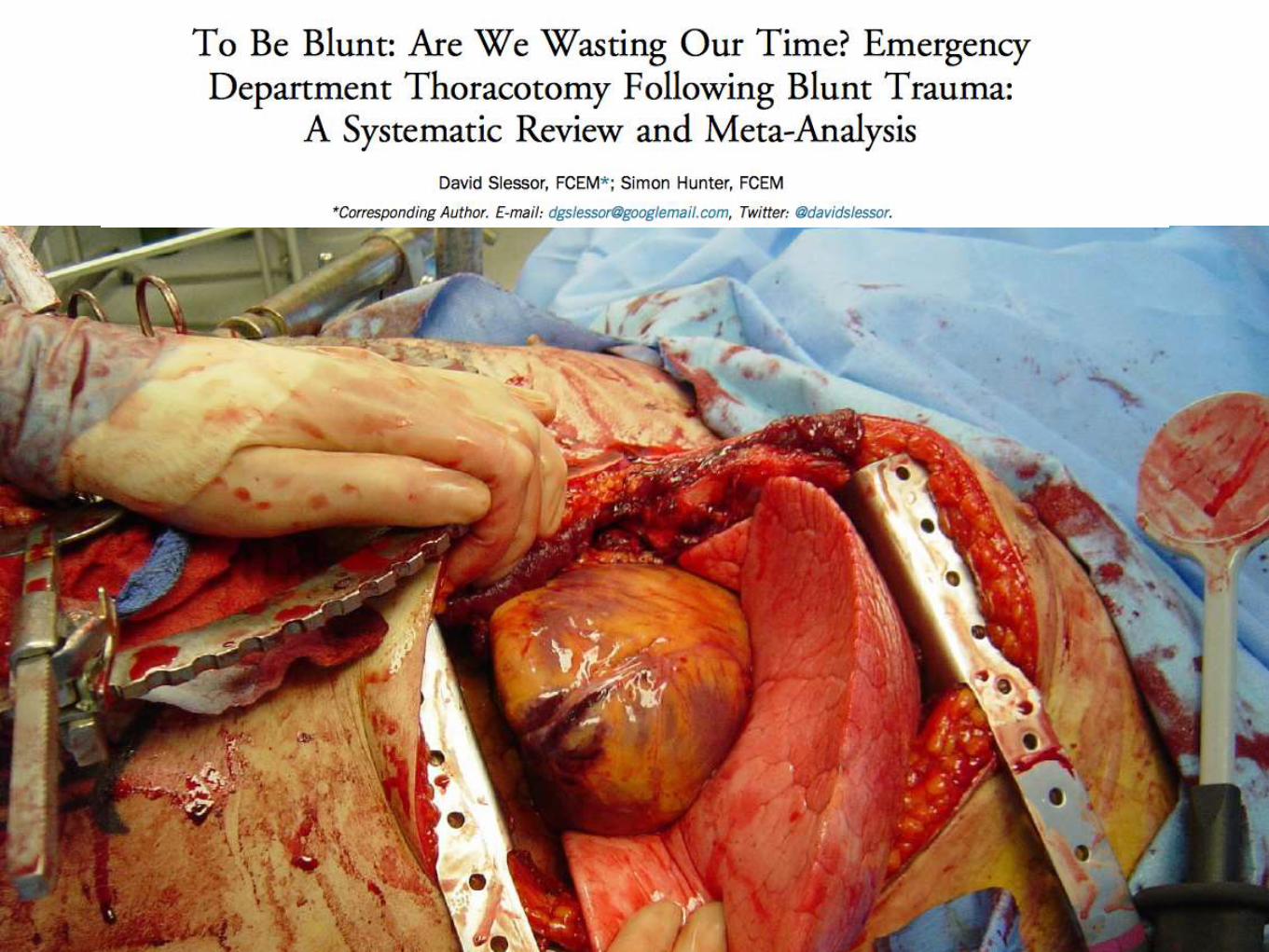
Be (very) selective in blunt thoracotomy
Use Ket/Roc/Fent for trauma RSI
You’re rubbish at determining need for MHPs
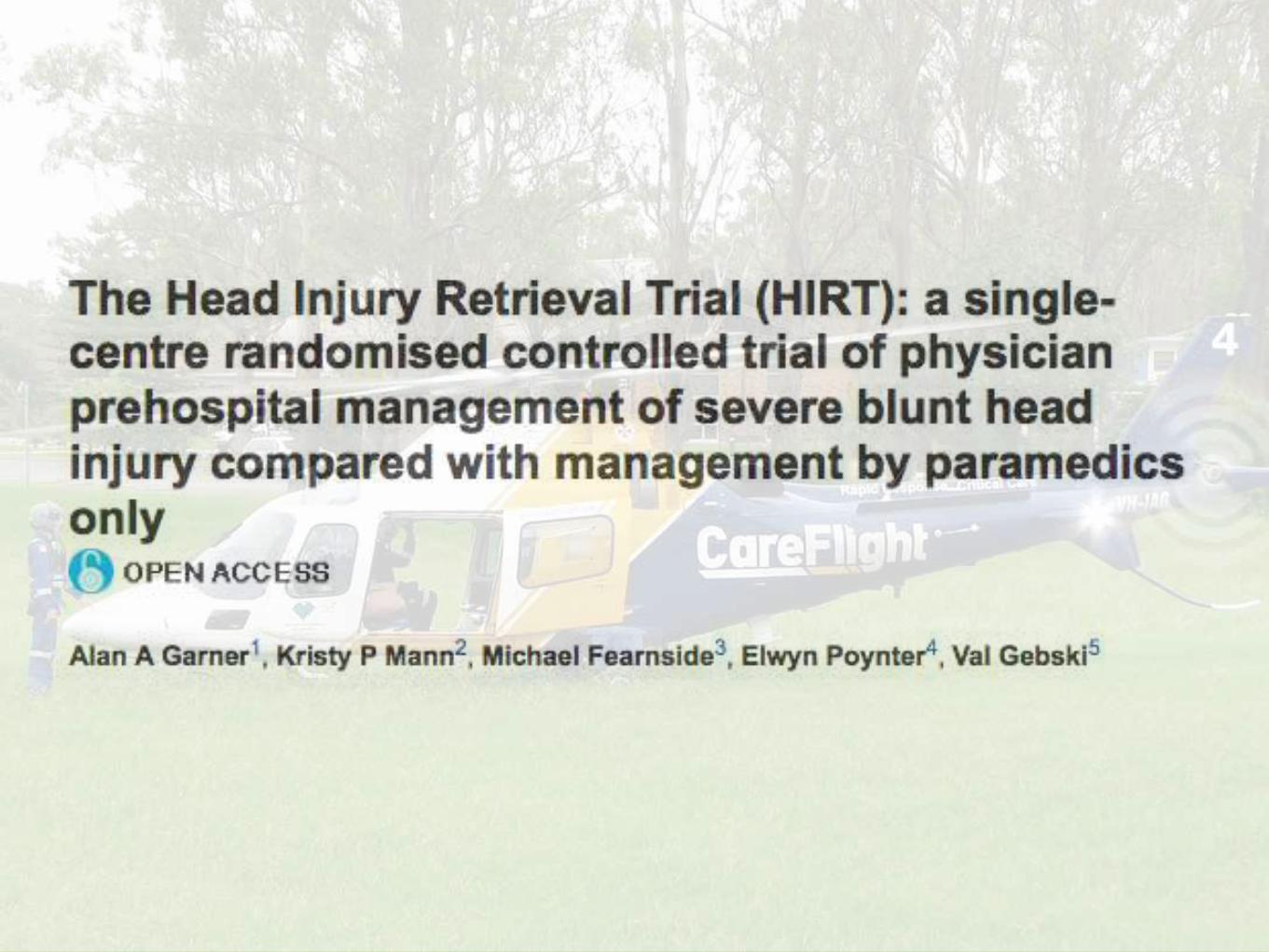
Don’t make head injuries sexy
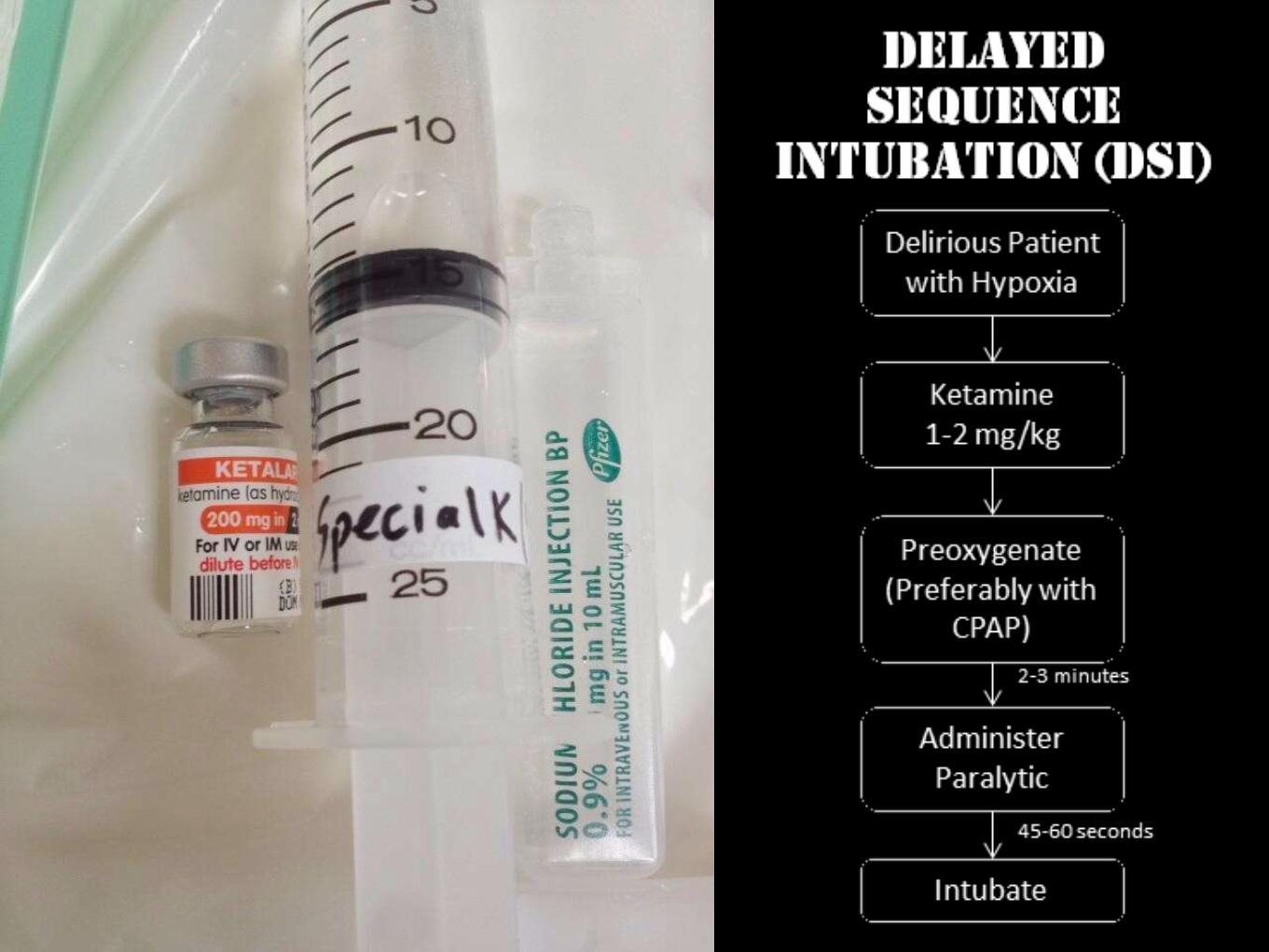
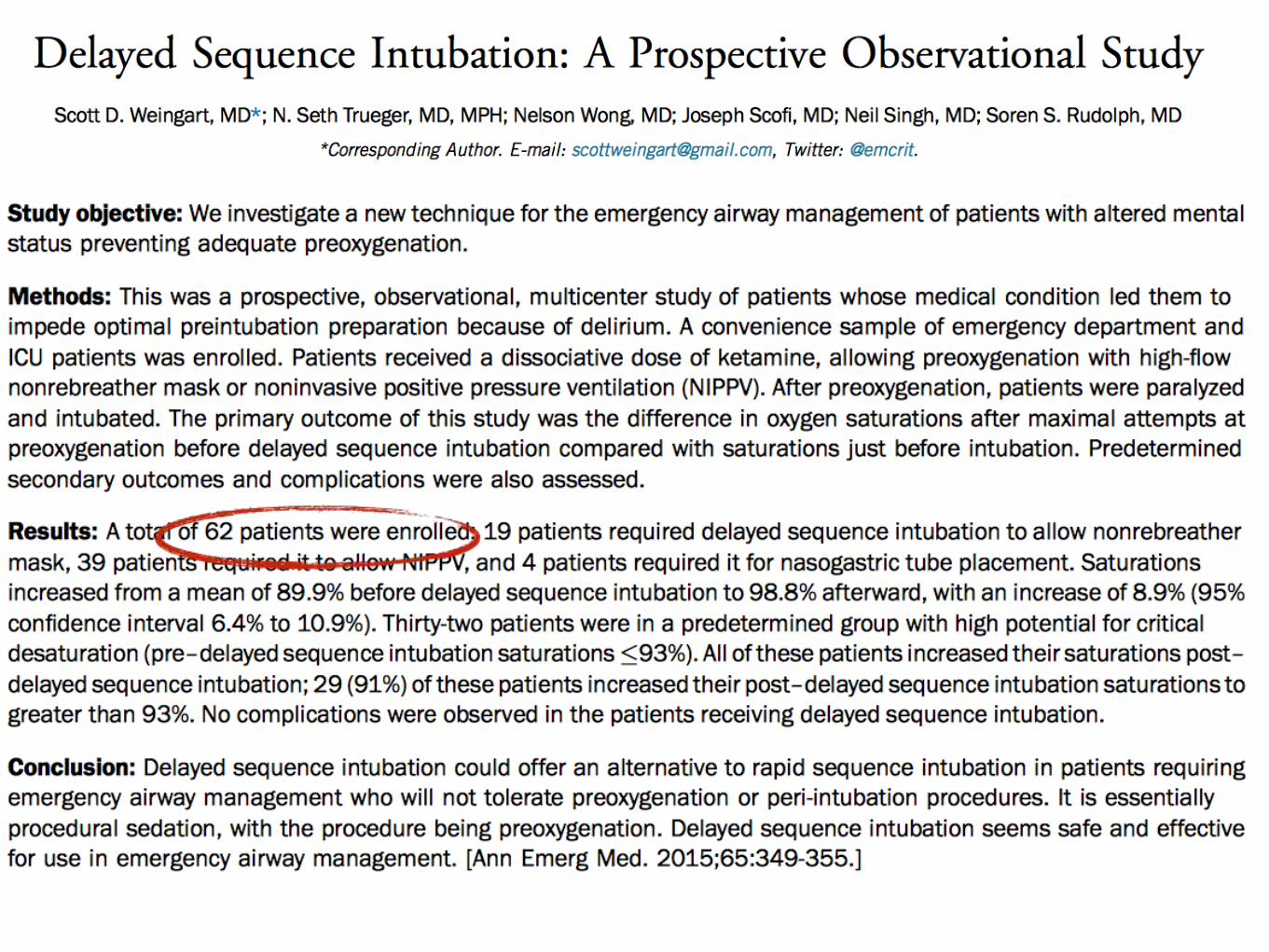
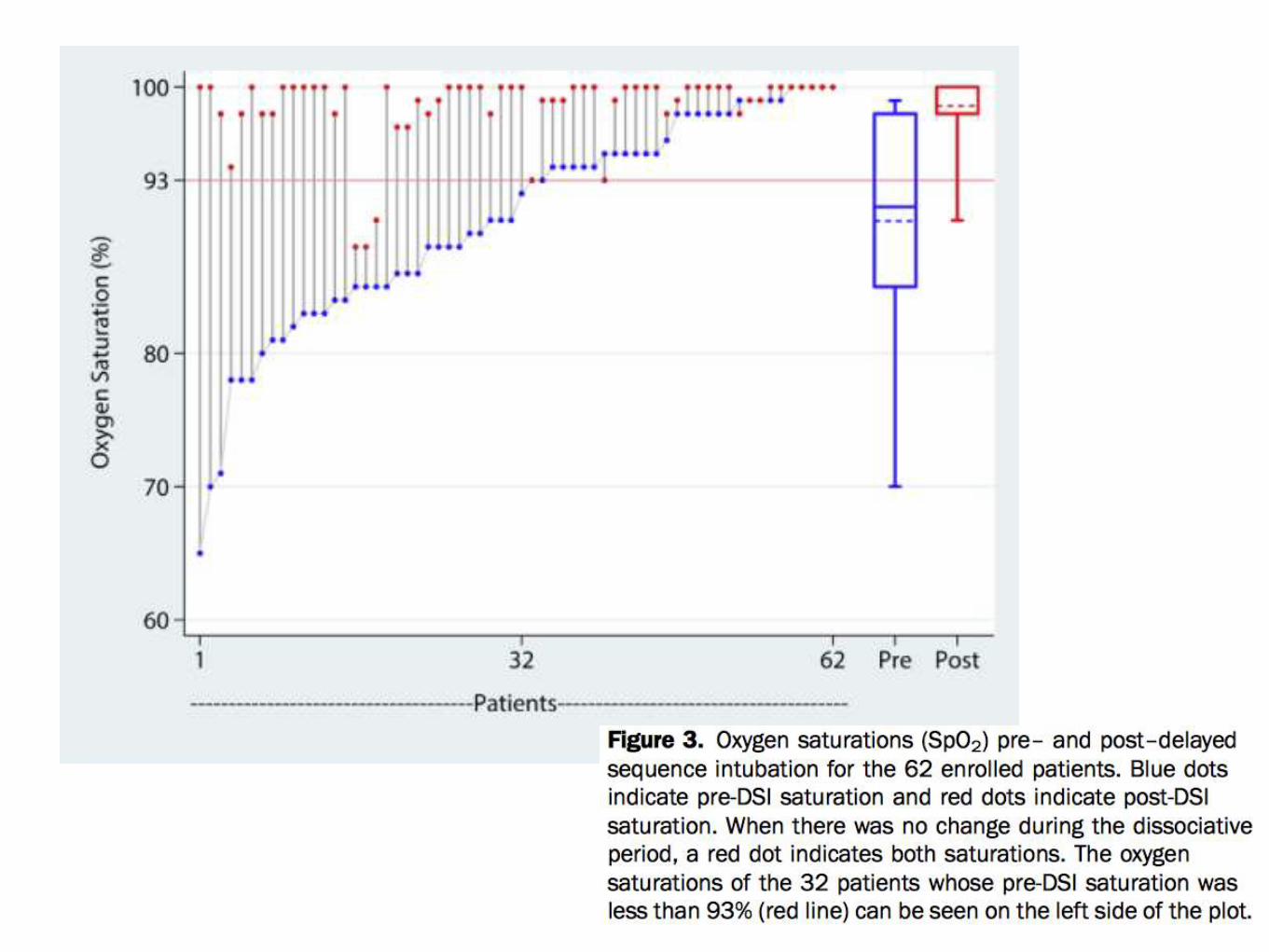
DSI you’re combative hypoxic patients
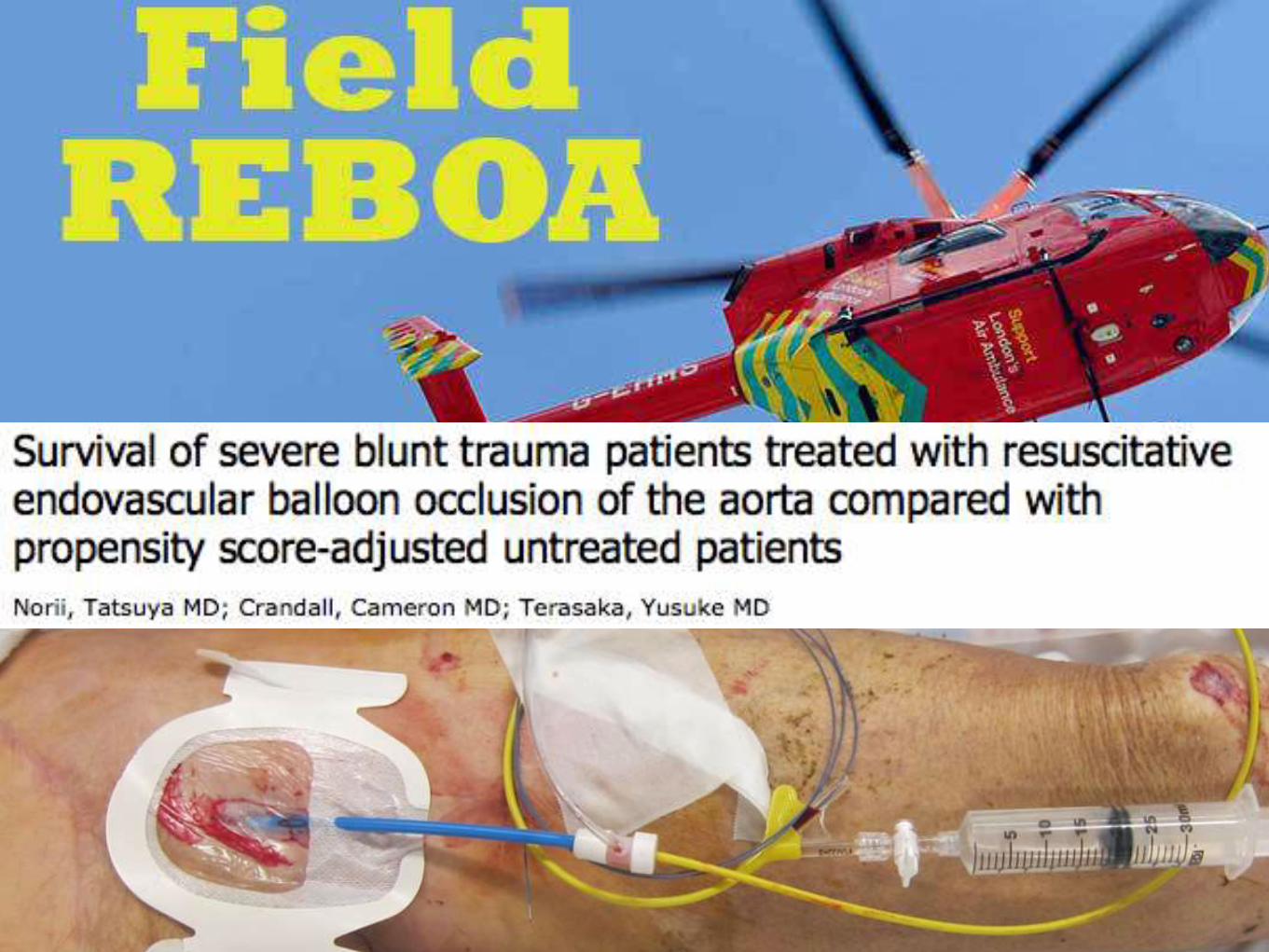
REBOA may not be all that it seems
RCTs in pre-hospital care are tricky
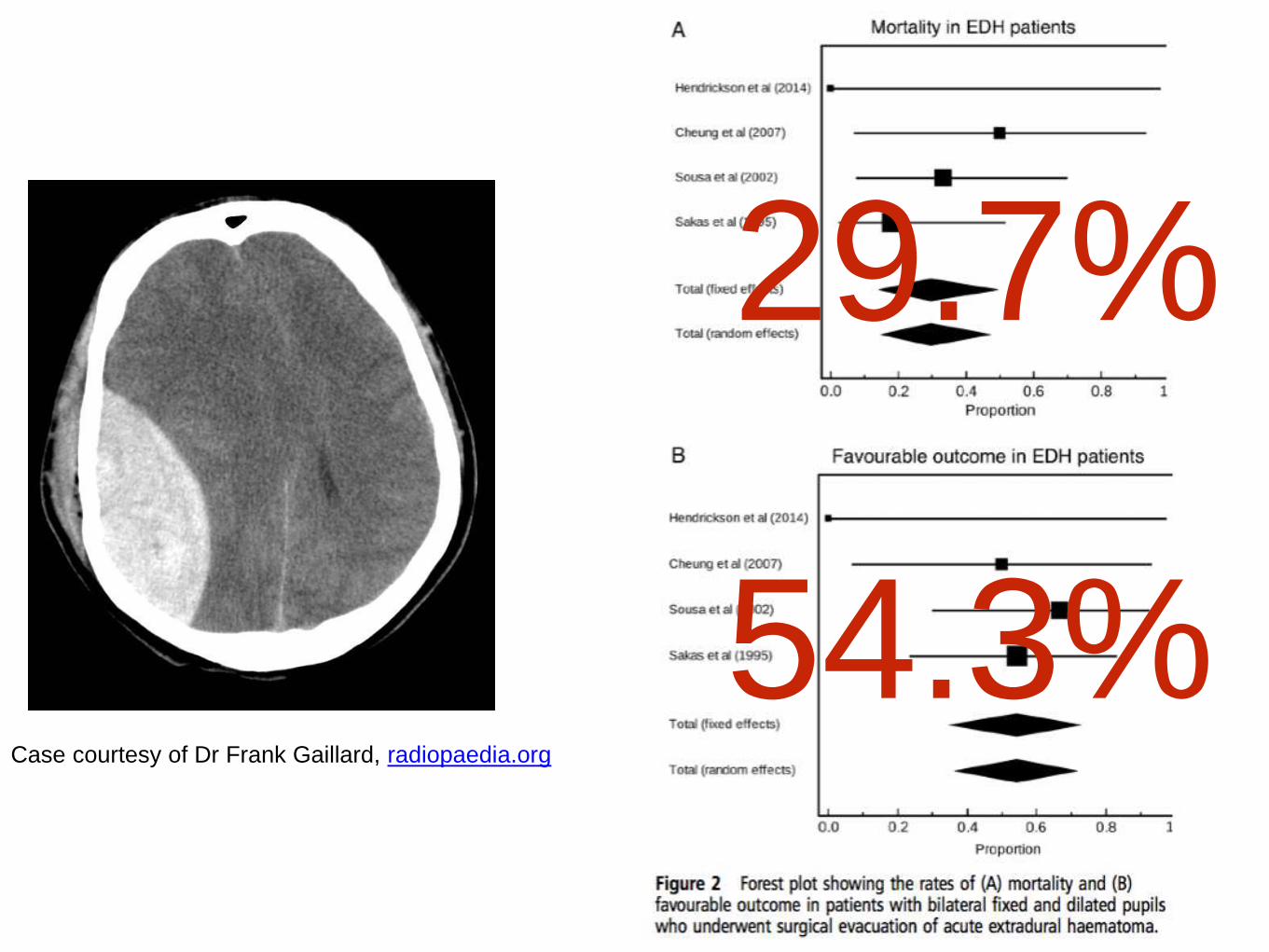
Don’t give up on the dilated head injury
TXA benefits the sickest patients
Use 1:1:1 blood, plasma, platelets in trauma


Related Documents
![15. [BIC 2015] NINETEEN - TOP 15](https://static.cupdf.com/doc/110x72/587c3d6b1a28ab5a1d8b57df/15-bic-2015-nineteen-top-15.jpg)










