JTCM | www. journaltcm. com April 15, 2020 | Volume 40 | Issue 2 | Online Submissions: http://www.journaltcm.com J Tradit Chin Med 2020 April 15; 40(2): 188-196 [email protected] ISSN 0255-2922 © 2020 JTCM. All rights reserved. SYSTEMATIC REVIEW Tonifying kidney therapy for stable chronic obstructive pulmonary disease: a systematic review Gao Zhen, Liu Yingying, Xu Yizhe, Dong Jingcheng aa Gao Zhen, Department of Integrative Medicine, Huashan Hospital, Fudan University, Shanghai 200040, China; Nation- al Clinical Research Base of Traditional Chinese Medicine, Traditional Chinese Medicine Hospital Affiliated to Xinjiang Medical University, Urumqi 830000, China Liu Yingying, Xu Yizhe, Dong Jingcheng, Department of Integrative Medicine, Huashan Hospital, Fudan University, Shanghai 200040, China Supported by Tianshan Innovation Team Plan of Xinjiang: Traditional Chinese Medicine Research Team on Prevention and Treatment of Chronic Obstructive Pulmonary Disease (No. 2017D14013) Correspondence to: Dong Jingcheng, Department of Inte- grative Medicine, Huashan Hospital, Fudan University, Shanghai 200031, China. [email protected] Telephone: +86-21-52888301 Accepted: October 15, 2019 Abstract OBJECTIVE: To evaluate the efficacy and safety of tonifying kidney therapy (Bushen, TK) for stable chronic obstructive pulmonary disease (COPD). METHODS: Randomized controlled trials (RCTs) of TK use for treatment of stable COPD were searched in four databases including PubMed, the Cochrane Library, Chinese Biomedical Literature Database, and China National Knowledge Infrastructure Data- base from inception to December 2017. Two re- viewers independently screened the literature, ex- tracted the data, and assessed the risk of bias in the included studies. RevMan 5.3 software was used for the Meta-analysis. RESULTS: Eight RCTs involving 809 patients with stable COPD were included. Compared with the conventional Western Medicine (CWM) group, the TK group (TK combined with CWM) showed signifi- cant improvements in the effectiveness rates (RR = 1.37, 95% CI 1.22 to 1.53, P < 0.000 01) and 6-min walk distance in meters (MD 11.92, 95% CI 3.52 to 20.32, P = 0.005), this study also showed that the TK group can decrease The Traditional Chinese Medi- cine Syndrome Score (MD -8.01, 95% CI - 12.89 to -3.13, P = 0.001). The lung function [forced expira- tory volume in one second% (FEV1% ), FEV1/forced vital capacity] showed no difference between the TK and control groups. CONCLUSION: For patients with stable COPD, TK can improve the clinical effectiveness and exercise capacity but fail to improve the patient's symp- toms. Because of the low methodological quality of the included trials, additional high-quality and large-scale RCTs are required. © 2020 JTCM. All rights reserved. Keywords: Pulmonary disease, chronic obstructive; Reinforcing kidney; Review; Randomized con- trolled trial INTRODUCTION Chronic obstructive pulmonary disease (COPD) is cur- rently the fourth leading cause of death worldwide 1 but is projected to be the third leading cause of death by 2020. A recent survey reported an estimated COPD prevalence of 6.2% in seven Asian-Pacific countries (China, Indonesia, Malaysia, the Philippines, Singa- pore, Thailand, and Vietnam). 2 COPD is one of the main contributors to the global burden of disease, and the COPD burden in China is high in terms of eco- 188

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript
JTCM |www. journaltcm. com April 15, 2020 |Volume 40 | Issue 2 |
Online Submissions: http://www.journaltcm.com J Tradit Chin Med 2020 April 15; 40(2): [email protected] ISSN 0255-2922
© 2020 JTCM. All rights reserved.
SYSTEMATIC REVIEW
Tonifying kidney therapy for stable chronic obstructive pulmonarydisease: a systematic review
Gao Zhen, Liu Yingying, Xu Yizhe, Dong Jingchengaa
Gao Zhen, Department of Integrative Medicine, HuashanHospital, Fudan University, Shanghai 200040, China; Nation-al Clinical Research Base of Traditional Chinese Medicine,Traditional Chinese Medicine Hospital Affiliated to XinjiangMedical University, Urumqi 830000, ChinaLiu Yingying, Xu Yizhe, Dong Jingcheng, Department ofIntegrative Medicine, Huashan Hospital, Fudan University,Shanghai 200040, ChinaSupported by Tianshan Innovation Team Plan of Xinjiang:Traditional Chinese Medicine Research Team on Preventionand Treatment of Chronic Obstructive Pulmonary Disease(No. 2017D14013)Correspondence to: Dong Jingcheng, Department of Inte-grative Medicine, Huashan Hospital, Fudan University,Shanghai 200031, China. [email protected]: +86-21-52888301Accepted: October 15, 2019
AbstractOBJECTIVE: To evaluate the efficacy and safety oftonifying kidney therapy (Bushen, TK) for stablechronic obstructive pulmonary disease (COPD).
METHODS: Randomized controlled trials (RCTs) ofTK use for treatment of stable COPD were searchedin four databases including PubMed, the CochraneLibrary, Chinese Biomedical Literature Database,and China National Knowledge Infrastructure Data-base from inception to December 2017. Two re-viewers independently screened the literature, ex-tracted the data, and assessed the risk of bias in theincluded studies. RevMan 5.3 software was used forthe Meta-analysis.
RESULTS: Eight RCTs involving 809 patients withstable COPD were included. Compared with the
conventional Western Medicine (CWM) group, theTK group (TK combined with CWM) showed signifi-cant improvements in the effectiveness rates (RR =1.37, 95% CI 1.22 to 1.53, P < 0.000 01) and 6-minwalk distance in meters (MD 11.92, 95% CI 3.52 to20.32, P = 0.005), this study also showed that the TKgroup can decrease The Traditional Chinese Medi-cine Syndrome Score (MD -8.01, 95% CI -12.89 to-3.13, P = 0.001). The lung function [forced expira-tory volume in one second% (FEV1% ), FEV1/forcedvital capacity] showed no difference between theTK and control groups.
CONCLUSION: For patients with stable COPD, TKcan improve the clinical effectiveness and exercisecapacity but fail to improve the patient's symp-toms. Because of the low methodological quality ofthe included trials, additional high-quality andlarge-scale RCTs are required.
© 2020 JTCM. All rights reserved.
Keywords: Pulmonary disease, chronic obstructive;Reinforcing kidney; Review; Randomized con-trolled trial
INTRODUCTIONChronic obstructive pulmonary disease (COPD) is cur-rently the fourth leading cause of death worldwide1 butis projected to be the third leading cause of death by2020. A recent survey reported an estimated COPDprevalence of 6.2% in seven Asian-Pacific countries(China, Indonesia, Malaysia, the Philippines, Singa-pore, Thailand, and Vietnam).2 COPD is one of themain contributors to the global burden of disease, andthe COPD burden in China is high in terms of eco-
188

Gao Z et al. / Systematic Review
JTCM |www. journaltcm. com April 15, 2020 |Volume 40 | Issue 2 |
nomic burden and quality of life.3 Patients who sufferfrom COPD may experience cough, dyspnea, chesttightness, and wheezing.4,5 Chronic cough, sputum pro-duction, and decreased forced expiratory volume inone second (FEV1) have been shown to be indepen-dently associated with an increased risk of frequent ex-acerbations and hospitalizations.6 Therefore, Each phar-macologic treatment regimen should be individualizedand guided by the severity of symptoms, risk of exacer-bations, side effects, comorbidities, drug availabilityand cost, and the patient's response, preference, andability to use various drug delivery devices.7
Many clinical guidelines recommended pharmacologi-cal therapies for COPD, but acute exacerbation still oc-curs frequently and is significantly associated with mor-bidity and mortality.8 In China, Traditional ChineseMedicine (TCM) has been used for thousands of yearsfor the treatment of respiratory disease. TCM is a prev-alent treatment for COPD and is widely prescribed asan adjunct to Western medicine to manage stableCOPD in clinical guidelines. Although TCM is not amainstream method for treating COPD, it has becomeincreasingly accepted as a form of complementary med-icine in Western countries.9 Studies have shown thatTCM combined with routine pharmacotherapy hasshown promising benefits for clinical symptoms andquality of life compared with routine pharmacotherapyalone.10 Furthermore, tonifying kidney therapy (TK)formulas are a type of basic therapy for stable COPDin TCM. Stable COPD is divided into four TCM syn-dromes: lung (Fei) Qi deficiency, lung (Fei) and spleen(Pi) Qi deficiency, lung (Fei) and kidney (Shen) Qi de-ficiency, and lung (Fei), kidney (Shen) Qi and Yin defi-ciency.11 The four TCM therapies that include TK for-mulas for treatment of stable COPD are as follows:tonifying kidney (Shen), tonifying kidney (Shen) andlung (Fei), tonifying kidney (Shen) and spleen (Pi),and tonifying kidney (Shen), lung (Fei) and spleen(Pi). In this study, TK indicates that the main functionof the formulas is tonifying the kidney (Shen) (tonify-ing kidney therapy or tonifying kidney therapy plus in-vigorating the blood circulation or resolving phlegm);main effects including tonifying the lung or/and spleenwere not included.TK often serves as a principal medicine in formulas forstable COPD. However, the quality of these studieshas not been evaluated systematically, and some reportsof the effects of TK are conflicting. Therefore, we con-ducted this systematic review to compare TK com-bined with pharmacotherapy to determine their rela-tive effectiveness and safety for the treatment of stableCOPD.
MATERIALS AND METHODS
RegistrationThe study protocol was registered in the International
Prospective Register of Systematic Reviews (PROSPE-RO). The PROSPERO study registration number of isCRD 42018090328, and this protocol was publishedin Medicine.12
Inclusion and exclusion criteriaRandomized Control Trials (RCTs) reporting the appli-cation of TK for the treatment of stable COPD wereincluded. There were no limitations on publication sta-tus. The inclusion criteria were as follows: (a) articlespublished in the English or Chinese language; (b) ran-domized or quasi-randomized clinical trials; (c) studiesincluding patients diagnosed with stable COPD; (d)studies including patients treated according to syn-drome differentiation (TCM).The exclusion criteria were as follows: (a) randomizedcrossover trials, case reports, case series, reviews, qual-itative studies, or animal experiments; (b) stableCOPD interventions combined with external TCMtherapy.
Intervention typesRCTs that examined the effects of TK combined withthe conventional Western Medicine (CWM) andCWM were identified. Patients in the treatment groupwere given TK combined with CWM, while patientsin control group were treated only with CWM. Pa-tients were excluded when the RCTs included externalTCM therapy. We did not set limitations on dosagesand course of treatment.
Outcome measuresThe primary outcomes analyzed in this Meta-analysiswere the effectiveness, TCM Syndrome Score,13 COPDhealth status (COPD Assessment Test ™, CAT),14 andexercise capacity (6-min walk distance in meters,6mWD).15 The secondary outcomes analyzed for thisMeta-analysis were lung function including forced expi-ratory volume in one second% (FEV1% ) and FEV1/forced vital capacity (FVC).
Literature search strategyTwo Chinese language databases and two English lan-guage databases were widely searched for all relevant re-sults until December 2017. The Chinese language data-bases were the China National Knowledge Infrastruc-ture Database and Chinese Biomedical Literature Data-base. The two English language databases werePubMed and the Cochrane Library.The search strategy was as follows: #1 Bushen; #2 Bushen; #3 Yishen; #4 nourishing the kidney; #5 tonify-ing the kidney; #6 Yi shen; #7 tonifying shen; #8 toni-fying kidney; #9 nourishing kidney; #10 nourishingshen; #11 reinforcing the kidney; #12 reinforcing kid-ney; #13 reinforcing shen; #14 invigorating the kid-ney; #15 invigorating kidney; #16 invigorating shen; #17 kidney-reinforcin; #18 kidney reinforcing; #19Shen reinforcing; #20 Shen-reinforcing; #21 kidney-In-
189

JTCM |www. journaltcm. com April 15, 2020 |Volume 40 | Issue 2 |
Gao Z et al. / Systematic Review
vigorating; #22 kidney Invigorating; #23 Shen-Invigo-rating; #24 kidney-tonifying; #25 Shen-tonifying; #26kidney tonifying; #27 Shen tonifying; #28 Shen Invigo-rating; #29 Invigorating Shen; #30 #1 or #2 or #3 or #4 or #5 or #6 or #7 or #8 or #9 or #10 or #11 or #12reinforcing kidney or #13 or #14 or #15 or #16 or #17or #18 or #19 or #20 or #21or #22 or #23 or #24 or #25 or #26 or #27 or #28 or #29; #31 COPD; #32chronic obstructive pulmonary disease; #33 #31 or #32; #34 #30 and #33.
Data extraction and managementData were independently extracted by two reviewers.After extraction, any disagreements were resolved byconsulting a third reviewer. All of the data were record-ed using a data collection form. The form contentswere as follows: (a) title, authors, source, and time ofpublication; (b) basic characteristics (sample, gender,age, diagnostic criteria, course of disease, intervention,course of treatment, main outcomes, and specific de-tails); (c) methods (study design, total study duration,sequence generation, allocation sequence concealment,blinding, and other concerns about bias). The collectedoutcome data were inputted into Review Manager 5.3(RevMan 5.3).
Assessment of risk of biasCriteria for judging the risk of bias were taken fromthe "risk of bias" assessment tool in The CochraneHandbook for Systematic Reviews of Interventions5.1.0.16 This judgement was independently evaluatedby two reviewers, and disagreements were resolved byconsulting a third reviewer.
Data synthesisRevMan 5.3 was used for the statistical analysis. Theextracted data were divided into dichotomous and con-tinuous variables. Data are summarized using the rela-tive risk (RR) and 95% confidence intervals (CI) for di-chotomous outcomes; the mean difference (MD) withthe 95% CI is presented for continuous outcomes. Co-chrane's P values and I 2 test values were determined toexamine the level of heterogeneity among trials. A ran-dom-effects model was used to evaluate the effects ofTK on stable COPD if I 2 > 50% or P < 0.1. Other-wise, a fixed-effects model was utilized. A value ofP < 0.01 was considered statistically significant. Datawere subjected to Meta-analysis using RevMan 5.3(Cochrane Community, London, United Kingdom,2014).
RESULTSResults of the searchIn total, 560 potential records (507 records from Chi-nese databases and 53 records from English databases)were obtained. Among these, 418 records were left forfurther screening after the duplicates were removed. A
total of 171 studies were read and analyzed in detail,and eight studies17-24 were finally included in the system-atic review. This screening process is summarized in aflow diagram (Figure 1).
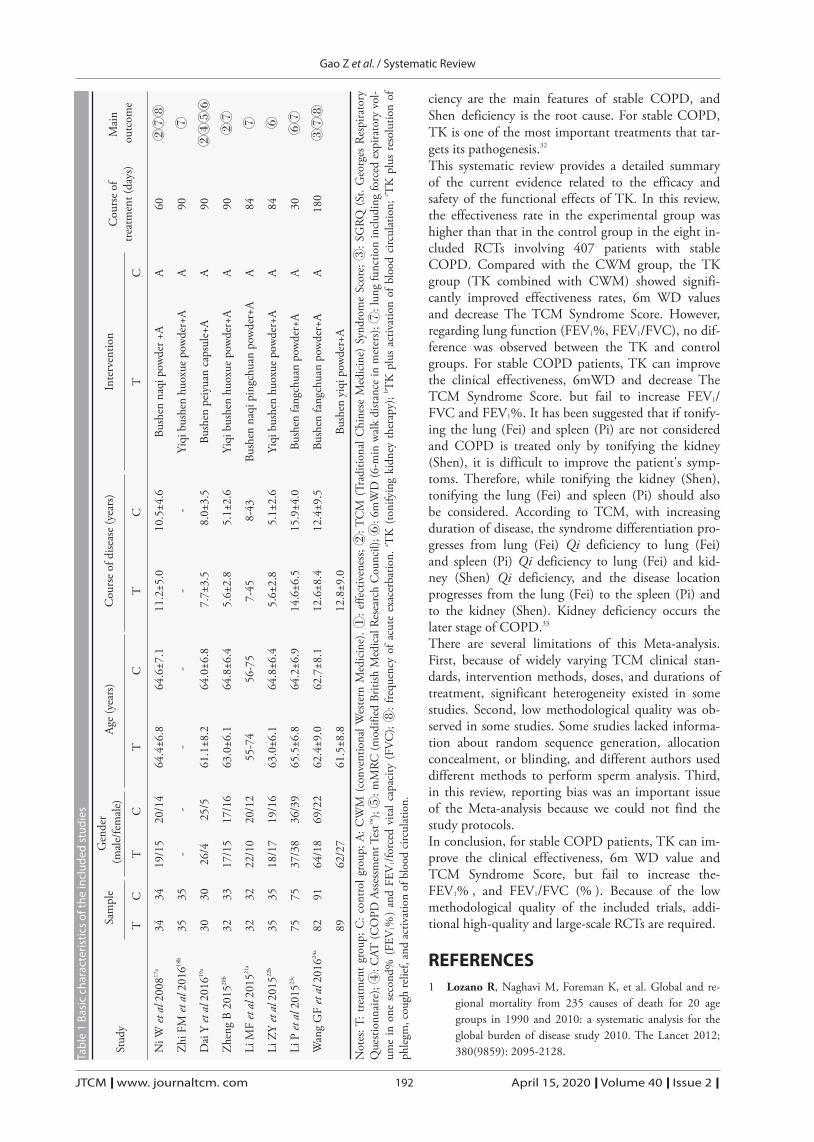
Study characteristicsAmong eight studies,17-24 809 patients with COPDwere included. The control group received CWM,while the experimental group received TK combinedwith CWM. The study characteristics are shown inTable 1.
Composition of the Herbal Formulas for COPD inthis reviewPatients in the treatment group were treated with TK.Herbal medicines in the included studies are presentedin Table 2.
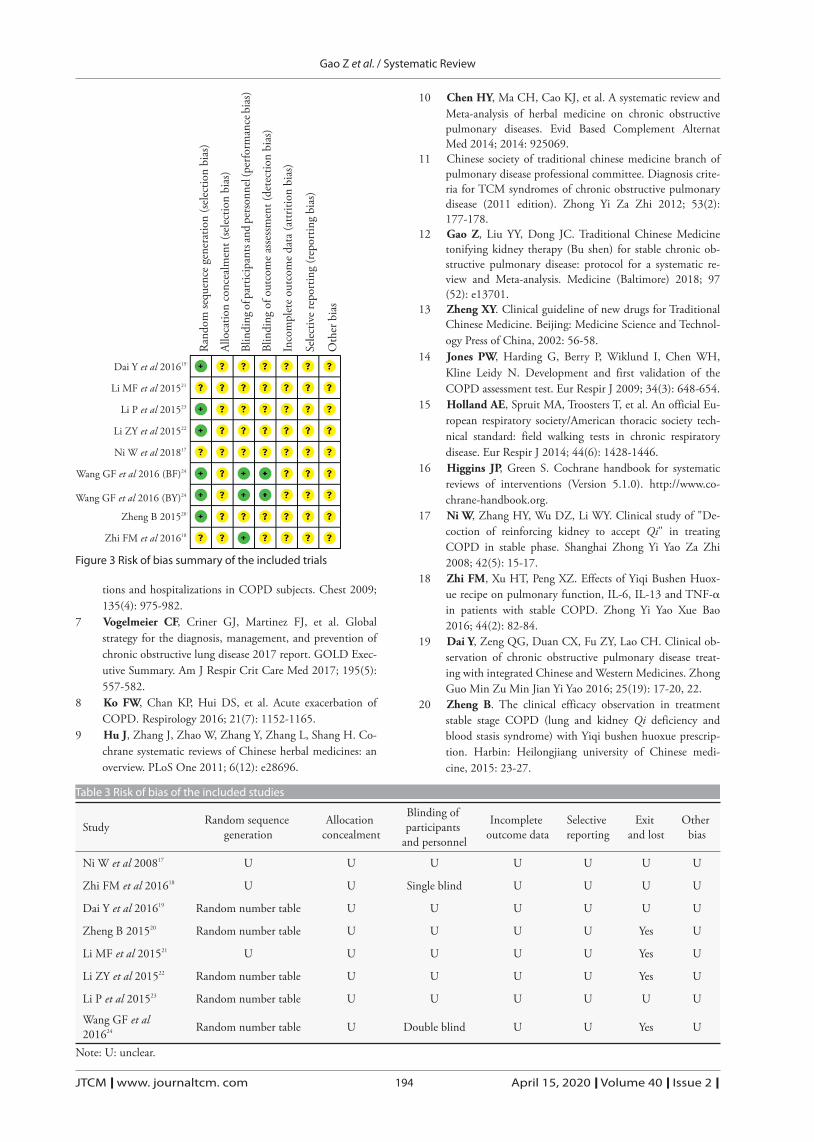
Risk of bias assessmentEight17-24 of the included articles described the specificmethod of randomization (five19,20,22-24 used randomnumber tables). None of the studies described the allo-cation concealment method. One study24 used a dou-ble-blind method, and one18 used a single-blind meth-od. It is not known whether the trails are relevant be-cause of incomplete outcome data and selective report-ing (Figures 2 and 3 and Table 3).
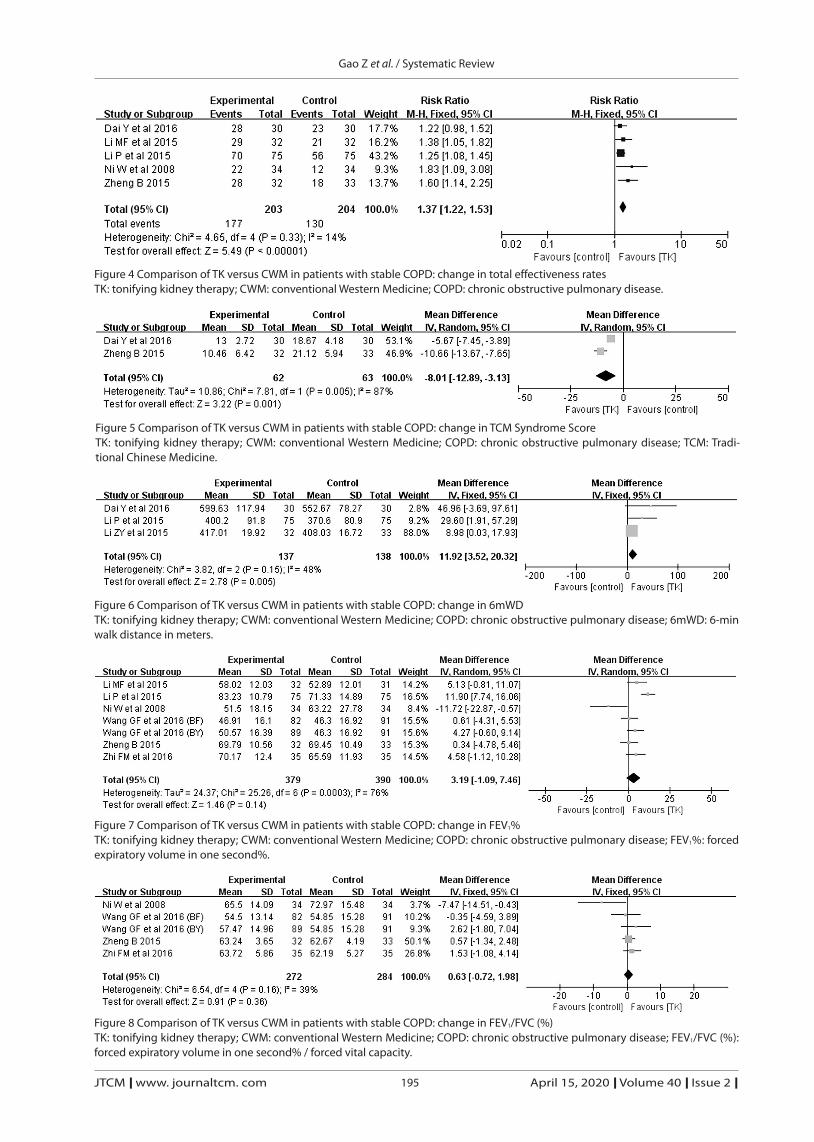
Meta-analysisThe Meta-analysis was performed according to a ran-dom effects statistical model. In addition, all of thestudies included treatment group patients (treated withTK combined with CWM) and control patients (treat-ed with CWM).The total effectiveness rates of TK were analyzed infive studies, 17,19-21,23 including 203 treatment group pa-tients (TK + CWM) and 204 controls (CWM). Ouranalysis revealed that TK combined with CWMshowed increased effectiveness (RR = 1.37, 95% CI1.22 to 1.53, P < 0.000 01). A fixed-effects model wasused (Figure 4).The TCM Syndrome Score of TK was evaluated intwo studies 19,20 (60 treatment group patients and 62controls). Our analysis revealed that TK can decreaseThe TCM Syndrome Score (MD - 8.01, 95% CI-12.89 to -3.13, P = 0.001) (Figure 5).The exercise capacity (6mWD) was evaluated in threestudies,19,22,23 including 137 treatment group patientsand 138 controls. Our analysis revealed that TK can in-crease 6mWD (MD 11.92, 95% CI 3.52 to 20.32, P =0.005). A fixed-effects model was used (Figure 6).Lung function (FEV1%) was assessed in six studies17,18,
20-24 (379 treatment group patients and 299 controls).Our analysis revealed no difference between the TKand control group (MD = 3.19, 95% CI - 1.09 to7.46, P = 0.14) (Figure 7).Lung function (FEV1/FVC, % ) was assessed in fourstudies17,18,20,24 (272 treatment group patients and 193
190

Gao Z et al. / Systematic Review
JTCM |www. journaltcm. com April 15, 2020 |Volume 40 | Issue 2 |April 15, 2020 |Volume 40 | Issue 2 |
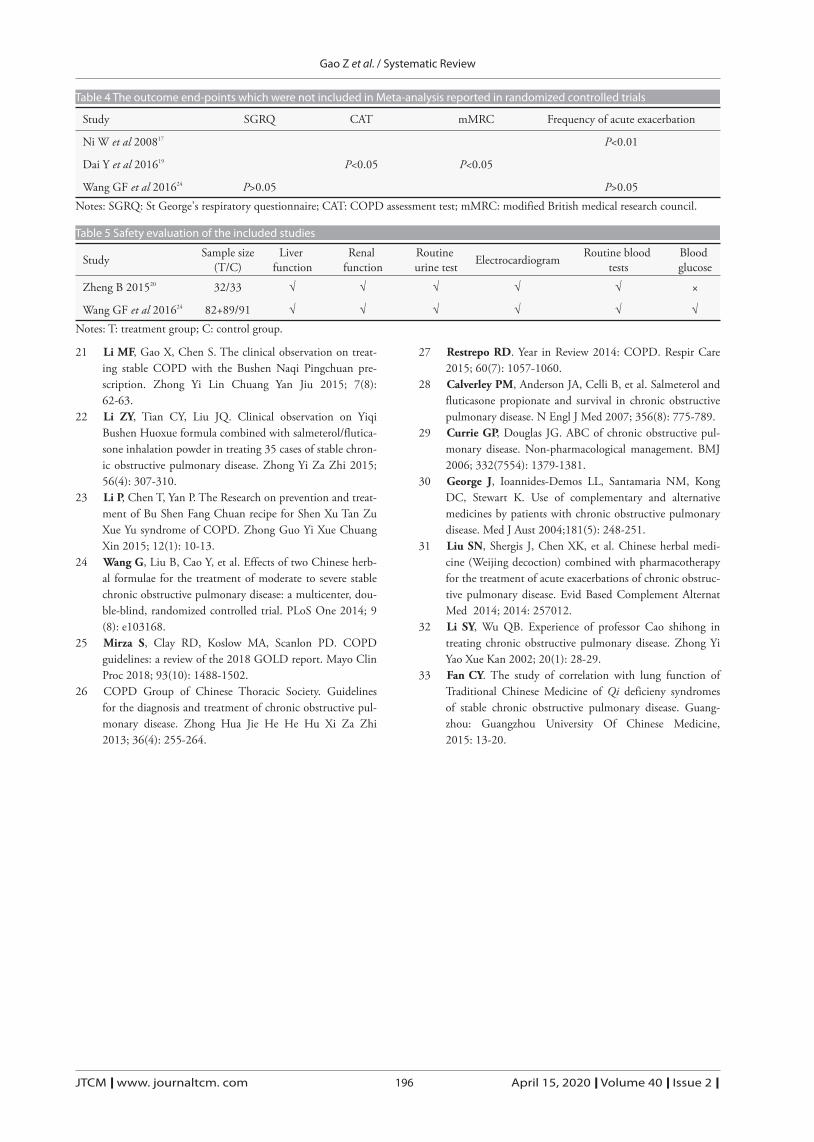
controls). Our analysis revealed no difference betweenthe TK and control groups (MD = 0.63, 95% CI-0.72 to 1.98, P = 0.36) (Figure 8).The Table shows important outcomes endpoints thatwere not included in the Meta-analysis of the RCTs(Table 4).
Safety and adverse eventsAmong 8 17-24 included RCTs, only two RCTs20,24 (in-cluding 327 participants) mentioned safety evaluation(Table 5), while one RCT24 (including 262 partici-pants) provided adverse events associated with TCM.The percentage of patients with adverse events was13.54% , 14.14% and 16.50% in Bushen fangchuantablets group, Bushen yiqi granule group and placebogroup, respectively. There were no differences amongthe three groups. No serious adverse event was report-ed in this study.24
DISCUSSIONMany guidelines have been developed,25,26 and oral sys-temic corticosteroids, such as theophylline, and someclasses of long-acting inhaled therapeutic agents, suchas long-acting β-agonists plus inhaled corticosteroids,are commonly used in the treatment of COPD.27 How-ever, difficulties still exist in helping patients controltheir symptoms as well as eliminating medication-in-duced side effects or adverse events.28 In China, COPDpatients seek TCM management when CWM is notsufficient to maintain their quality of daily work andlife. There has been increasing interest in complementa-ry and alternative medicine for the treatment ofCOPD, especially the use of Chinese herbal medi-cines,29, 30 and many complementary and alternativemedicines have been assessed with promising results.31
According to TCM, Fei (lung) and Shen (kidney) defi-
Records identified through 4 databasesearching (n = 560)
CNKI (n = 359), CBM (n = 148),Pubmed (n = 35), Cochrane (n = 18)
Additional records identified throughother sources (n = 0)
Records after duplicates removed(n = 418)
Records screened(n = 418)
After reading the titles andabstracts records excluded
(n = 247)
Full-text articles assessed for eligibility(n = 171)
Full-text articles excluded,with reasons (n = 163):
not RCTs (n = 8);Not targeted disease or
syndrome (n = 82);Invalid comparison (n = 55);
Other reasons (n = 18)
Studies included in qualitative synthesis(n = 8)
Studies included in qualitative synthesis(Meta-analysis)
(n = 8)
Iden
tific
atio
nSc
reen
ing
Elig
ibili
tyIn
clud
ed
Figure 1 Flow chart of the trial selection processCNKI: Chinese national knowledge infrastructure; RCTs: randomized controlled trials.
191
JTCM |www. journaltcm. com April 15, 2020 |Volume 40 | Issue 2 |
Gao Z et al. / Systematic Review
ciency are the main features of stable COPD, andShen deficiency is the root cause. For stable COPD,TK is one of the most important treatments that tar-gets its pathogenesis.32
This systematic review provides a detailed summaryof the current evidence related to the efficacy andsafety of the functional effects of TK. In this review,the effectiveness rate in the experimental group washigher than that in the control group in the eight in-cluded RCTs involving 407 patients with stableCOPD. Compared with the CWM group, the TKgroup (TK combined with CWM) showed signifi-cantly improved effectiveness rates, 6m WD valuesand decrease The TCM Syndrome Score. However,regarding lung function (FEV1%, FEV1/FVC), no dif-ference was observed between the TK and controlgroups. For stable COPD patients, TK can improvethe clinical effectiveness, 6mWD and decrease TheTCM Syndrome Score. but fail to increase FEV1/FVC and FEV1%. It has been suggested that if tonify-ing the lung (Fei) and spleen (Pi) are not consideredand COPD is treated only by tonifying the kidney(Shen), it is difficult to improve the patient's symp-toms. Therefore, while tonifying the kidney (Shen),tonifying the lung (Fei) and spleen (Pi) should alsobe considered. According to TCM, with increasingduration of disease, the syndrome differentiation pro-gresses from lung (Fei) Qi deficiency to lung (Fei)and spleen (Pi) Qi deficiency to lung (Fei) and kid-ney (Shen) Qi deficiency, and the disease locationprogresses from the lung (Fei) to the spleen (Pi) andto the kidney (Shen). Kidney deficiency occurs thelater stage of COPD.33
There are several limitations of this Meta-analysis.First, because of widely varying TCM clinical stan-dards, intervention methods, doses, and durations oftreatment, significant heterogeneity existed in somestudies. Second, low methodological quality was ob-served in some studies. Some studies lacked informa-tion about random sequence generation, allocationconcealment, or blinding, and different authors useddifferent methods to perform sperm analysis. Third,in this review, reporting bias was an important issueof the Meta-analysis because we could not find thestudy protocols.In conclusion, for stable COPD patients, TK can im-prove the clinical effectiveness, 6m WD value andTCM Syndrome Score, but fail to increase the-FEV1% , and FEV1/FVC (% ). Because of the lowmethodological quality of the included trials, addi-tional high-quality and large-scale RCTs are required.
REFERENCES1 Lozano R, Naghavi M, Foreman K, et al. Global and re-
gional mortality from 235 causes of death for 20 agegroups in 1990 and 2010: a systematic analysis for theglobal burden of disease study 2010. The Lancet 2012;380(9859): 2095-2128.Ta
ble
1Ba
sic
char
acte
ristic
sof
the
incl
uded
stud
ies
Stud
y
NiW
etal
2008
17a
Zhi
FMet
al20
1618
b
Dai
Yet
al20
1619
a
Zhe
ngB
2015
20b
LiM
Fet
al20
1521
a
LiZY
etal
2015
22b
LiP
etal
2015
23c
Wan
gG
Fet
al20
1624
a
Sam
ple
T 34 35 30 32 32 35 75 82 89
C 34 35 30 33 32 35 75 91
Gen
der
(mal
e/fe
mal
e)
T
19/1
5
-
26/4
17/1
5
22/1
0
18/1
7
37/3
8
64/1
8
62/2
7
C
20/1
4
-
25/5
17/1
6
20/1
2
19/1
6
36/3
9
69/2
2
Age
(yea
rs)
T
64.4
±6.8
-
61.1
±8.2
63.0
±6.1
55-7
4
63.0
±6.1
65.5
±6.8
62.4
±9.0
61.5
±8.8
C
64.6
±7.1
-
64.0
±6.8
64.8
±6.4
56-7
5
64.8
±6.4
64.2
±6.9
62.7
±8.1
Cou
rse
ofdi
seas
e(y
ears
)
T
11.2
±5.0
-
7.7±
3.5
5.6±
2.8
7-45
5.6±
2.8
14.6
±6.5
12.6
±8.4
12.8
±9.0
C
10.5
±4.6
-
8.0±
3.5
5.1±
2.6
8-43
5.1±
2.6
15.9
±4.0
12.4
±9.5
Inte
rven
tion
T
Bush
enna
qipo
wde
r+A
Yiqi
bush
enhu
oxue
pow
der+
A
Bush
enpe
iyua
nca
psul
e+A
Yiqi
bush
enhu
oxue
pow
der+
A
Bush
enna
qipi
ngch
uan
pow
der+
A
Yiqi
bush
enhu
oxue
pow
der+
A
Bush
enfa
ngch
uan
pow
der+
A
Bush
enfa
ngch
uan
pow
der+
A
Bush
enyi
qipo
wde
r+A
C A A A A A A A A
Cou
rse
oftre
atm
ent(
days
)
60 90 90 90 84 84 30 180
Mai
nou
tcom
e
②⑦⑧ ⑦
②④⑤⑥ ②⑦ ⑦ ⑥ ⑥⑦ ③⑦⑧
Not
es:T
:tre
atm
ent
grou
p;C
:con
trolg
roup
;A:C
WM
(con
vent
iona
lWes
tern
Med
icin
e).①
:effe
ctiv
enes
s;②:
TC
M(T
radi
tiona
lChi
nese
Med
icin
e)Sy
ndro
me
Scor
e;③:
SGRQ
(St.
Geo
rges
Resp
irato
ryQ
uesti
onna
ire);④:
CAT
(CO
PDAs
sess
men
tTes
t™);⑤:
mM
RC(m
odifi
edBr
itish
Med
ical
Rese
arch
Cou
ncil)
;⑥:6
mW
D(6
-min
wal
kdi
stanc
ein
met
ers)
;⑦:l
ung
func
tion
incl
udin
gfo
rced
expi
rato
ryvo
l-um
ein
one
seco
nd%
(FEV
1%)
and
FEV
1/for
ced
vita
lcap
acity
(FV
C);
⑧:fre
quen
cyof
acut
eex
acer
batio
n.a T
K(to
nify
ing
kidn
eyth
erap
y);b T
Kpl
usac
tivat
ion
ofbl
ood
circ
ulat
ion;
c TK
plus
reso
lutio
nof
phle
gm,c
ough
relie
f,an
dac
tivat
ion
ofbl
ood
circ
ulat
ion.
192

Gao Z et al. / Systematic Review
JTCM |www. journaltcm. com April 15, 2020 |Volume 40 | Issue 2 |
2 Lim S, Lam DC, Muttalif AR, et al. Impact of chronic ob-structive pulmonary disease (COPD) in the Asia-Pacific re-gion: the EPIC Asia population-based survey. Asia PacFam Med 2015; 14: 4.
3 Zhu B, Wang Y, Ming J, Chen W, Zhang L. Disease bur-den of COPD in China: a systematic review. Int J ChronObstruct Pulmon Dis 2018; 13: 1353-1364.
4 Barnes PJ, Celli BR. Systemic manifestations and comor-
bidities of COPD. Eur Respir J 2009; 33(5): 1165-1185.
5 Stockley RA. Progression of chronic obstructive pulmo-nary disease: impact of inflammation, comorbidities andtherapeutic intervention. Curr Med Res Opin 2009; 25(5):1235-1245.
6 Burgel PR, Nesme-Meyer P, Chanez P, et al. cough andsputum production are associated with frequent exacerba-
Random sequence generation (selection bias)Allocation concealment (selection bias)
Blinding of participants and personnel (performance bias)Blinding of outcome assessment (detection bias)
Incomplete outcome data (attrition bias)Selective reporting (reporting bias)
Other bias
0% 25% 50% 75% 100%
Low risk of bias Unclear risk of bias High risk of bias
Figure 2 Risk of bias graph of the included trials
Table 2 Herbal medicines in the included studies
Study (reference)
Ni W et al 200817
Zhi FM et al 201618
Dai Y et al 201619
Zheng B 201520
Li MF et al 201521
Li ZY et al 201522
Li P et al 201523
Wang GF et al 201624
Composition of formulaBuguzhi (Fructus Psoraleae) 30 g, Yinyanghuo (Herba Epimedii Brevicornus) 30 g, Fupenzi (Fructus Rubi Chin-
gii) 12 g, Wuweizi (Fructus Schisandrae Chinensis) 9 g
Dangshen (Radix Codonopsis), Huangqi (Radix Astragali Mongolici), Banxia (Rhizoma Pinelliae), Kuxingren(Semen Armeniacae Amarum), Yinyanghuo (Herba Epimedii Brevicornus), Dilong (Pheretima Aspergillum),Sumu (Lignum sappan), Chenpi (Pericarpium Citri Reticulatae), Baizhu (Rhizoma Atractylodis Macrocephalae),
et al
Not given
Dangshen (Radix Codonopsis) 20 g, Huangqi (Radix Astragali Mongolici) 20 g, Buguzhi (Fructus Psoraleae) 15 g,Shudihuang (Radix Rehmanniae Praeparata) 15 g, Wuweizi (Fructus Schisandrae Chinensis) 15 g, Yinyanghuo(Herba Epimedii Brevicornus) 15 g, Ziwan (Radix Asteris Tatarici)15 g, Kuandonghua (Flos Farfarae) 15 g,Zisuzi (Fructus Perillae Argutae) 15 g, Banxia (Rhizoma Pinelliae) 10 g, Shanzhuyu (Fructus Corni) 15 g,Sumu (Lignum sappan) 10 g, Huangjing (Rhizoma Polygonati Sibirici) 15 g, Gancao (Radix Glycyrrhizae) 5 g
Rougui (Cortex Cinnamomi Cassiae) 6 g, Fuzi (Typhonii Rhizoma, to be decocted first) 6 g, Shudihuang (Ra-dix Rehmanniae Praeparata) 15 g, Shanzhuyu (Fructus Corni) 10 g, Shanyao (Rhizoma Dioscoreae Oppositae)10 g, Chuanniuxi (Radix Cyathulae) 10 g, Gejie (Gecko) 3 g, Huangqi (Radix Astragali Mongolici) 30 g, Ful-ing(Poria)10 g, Mudanpi (Cortex Moutan Radicis) 10 g, Zexie (Rhizoma Alismatis) 10 g, Chenxiang (Lig-num Aquilariae Resinatum) 3 g, Zisuzi (Fructus Perillae Argutae) 10 g, Jiegeng (Radix Platycodi) 10 g, Kuxin-
gren (Semen Armeniacae Amarum) 10 g, Wuweizi (Fructus Schisandrae Chinensis) 6 g
Huangqi (Radix Astragali Mongolici) 20 g, Dangshen (Radix Codonopsis) 20 g, Shudihuang (Radix Rehmanni-ae Praeparata) 15 g, Buguzhi (Fructus Psoraleae) 15 g, Wuweizi (Fructus Schisandrae Chinensis) 15 g,Huangjing (Rhizoma Polygonati Sibirici) 15 g, Banxia (Rhizoma Pinelliae) 10 g, Kuandonghua (Flos Farfarae)15 g, Ziwan (Radix Asteris Tatarici) 15 g, Zisuzi (Fructus Perillae Argutae) 15 g, Yinyanghuo (Herba EpimediiBrevicornus) 15 g, Sumu (Lignum Sappan) 10 g, Shanzhuyu (Fructus Corni) 15 g, Gancao (Radix Glycyrrhi-
zae) 5 g
Nuzhenzi (Fructus Ligustri Lucidi) 15 g, Mohanlian (Herba Ecliptae prostratae) 15 g, Dangshen (Radix Co-donopsis) 20 g, Huangqi (Radix Astragali Mongolici) 15 g, Chenpi (Pericarpium Citri Reticulatae) 12 g, Zhiq-iao (Fructus Aurantii Submaturus) 10g, Banxia (Rhizoma Pinelliae) 10g, Fuling (Poria) 15 g, Jiegeng (RadixPlatycodi) 10 g, Tinglizi (Semen Lepidii Apetali) 10 g, Danshen (Radix Salviae Miltiorrhizae) 15 g, Danggui(Radix Angelicae Sinensis) 12 g, Ziwan (Radix Asteris Tatarici) 10 g, stir-frying with liquid adjuvant Gancao
(Radix Glycyrrhizae) 6 g
Bushen Yiqi granule: Huangqi (Radix Astragali Mongolici), Yinyanghuo (Epimedium brevicornum Maxim),Dihuang (Radix Rehmanniae Recens)
Bushen Fangchuan Tablet: Yinyanghuo (Herba Epimedii Brevicornus), Dihuang (Radix Rehmanniae), Fuzi(Radix Aconiti Lateralis Preparata), Buguzhi (Fructus Psoraleae), Tusizi (Semen Cuscutae), Shudihuang (Radix
Rehmanniae Praeparata), Shanyao (Rhizoma Dioscoreae Oppositae), Chenpi (Pericarpium Citri Reticulatae)
193
JTCM |www. journaltcm. com April 15, 2020 |Volume 40 | Issue 2 |
Gao Z et al. / Systematic Review
tions and hospitalizations in COPD subjects. Chest 2009;135(4): 975-982.
7 Vogelmeier CF, Criner GJ, Martinez FJ, et al. Globalstrategy for the diagnosis, management, and prevention ofchronic obstructive lung disease 2017 report. GOLD Exec-utive Summary. Am J Respir Crit Care Med 2017; 195(5):557-582.
8 Ko FW, Chan KP, Hui DS, et al. Acute exacerbation ofCOPD. Respirology 2016; 21(7): 1152-1165.
9 Hu J, Zhang J, Zhao W, Zhang Y, Zhang L, Shang H. Co-chrane systematic reviews of Chinese herbal medicines: anoverview. PLoS One 2011; 6(12): e28696.
10 Chen HY, Ma CH, Cao KJ, et al. A systematic review andMeta-analysis of herbal medicine on chronic obstructivepulmonary diseases. Evid Based Complement AlternatMed 2014; 2014: 925069.
11 Chinese society of traditional chinese medicine branch ofpulmonary disease professional committee. Diagnosis crite-ria for TCM syndromes of chronic obstructive pulmonarydisease (2011 edition). Zhong Yi Za Zhi 2012; 53(2):177-178.
12 Gao Z, Liu YY, Dong JC. Traditional Chinese Medicinetonifying kidney therapy (Bu shen) for stable chronic ob-structive pulmonary disease: protocol for a systematic re-view and Meta-analysis. Medicine (Baltimore) 2018; 97(52): e13701.
13 Zheng XY. Clinical guideline of new drugs for TraditionalChinese Medicine. Beijing: Medicine Science and Technol-ogy Press of China, 2002: 56-58.
14 Jones PW, Harding G, Berry P, Wiklund I, Chen WH,Kline Leidy N. Development and first validation of theCOPD assessment test. Eur Respir J 2009; 34(3): 648-654.
15 Holland AE, Spruit MA, Troosters T, et al. An official Eu-ropean respiratory society/American thoracic society tech-nical standard: field walking tests in chronic respiratorydisease. Eur Respir J 2014; 44(6): 1428-1446.
16 Higgins JP, Green S. Cochrane handbook for systematicreviews of interventions (Version 5.1.0). http://www.co-chrane-handbook.org.
17 Ni W, Zhang HY, Wu DZ, Li WY. Clinical study of "De-coction of reinforcing kidney to accept Qi" in treatingCOPD in stable phase. Shanghai Zhong Yi Yao Za Zhi2008; 42(5): 15-17.
18 Zhi FM, Xu HT, Peng XZ. Effects of Yiqi Bushen Huox-ue recipe on pulmonary function, IL-6, IL-13 and TNF-αin patients with stable COPD. Zhong Yi Yao Xue Bao2016; 44(2): 82-84.
19 Dai Y, Zeng QG, Duan CX, Fu ZY, Lao CH. Clinical ob-servation of chronic obstructive pulmonary disease treat-ing with integrated Chinese and Western Medicines. ZhongGuo Min Zu Min Jian Yi Yao 2016; 25(19): 17-20, 22.
20 Zheng B. The clinical efficacy observation in treatmentstable stage COPD (lung and kidney Qi deficiency andblood stasis syndrome) with Yiqi bushen huoxue prescrip-tion. Harbin: Heilongjiang university of Chinese medi-cine, 2015: 23-27.
Figure 3 Risk of bias summary of the included trials
Ran
dom
sequ
ence
gene
ratio
n(s
elec
tion
bias
)
Allo
catio
nco
ncea
lmen
t(se
lect
ion
bias
)
Blin
ding
ofpa
rtic
ipan
tsan
dpe
rson
nel(
perfo
rman
cebi
as)
Blin
ding
ofou
tcom
eas
sess
men
t(de
tect
ion
bias
)
Inco
mpl
ete
outc
ome
data
(attr
ition
bias
)
Sele
ctiv
ere
port
ing
(rep
ortin
gbi
as)
Oth
erbi
as
Dai Y et al 201619
Li MF et al 201521
Li P et al 201523
Li ZY et al 201522
Ni W et al 201817
Wang GF et al 2016 (BF)24
Wang GF et al 2016 (BY)24
Zheng B 201520
Zhi FM et al 201618
Table 3 Risk of bias of the included studies
Study
Ni W et al 200817
Zhi FM et al 201618
Dai Y et al 201619
Zheng B 201520
Li MF et al 201521
Li ZY et al 201522
Li P et al 201523
Wang GF et al201624
Random sequencegeneration
U
U
Random number table
Random number table
U
Random number table
Random number table
Random number table
Allocationconcealment
U
U
U
U
U
U
U
U
Blinding ofparticipantsand personnel
U
Single blind
U
U
U
U
U
Double blind
Incompleteoutcome data
U
U
U
U
U
U
U
U
Selectivereporting
U
U
U
U
U
U
U
U
Exitand lost
U
U
U
Yes
Yes
Yes
U
Yes
Otherbias
U
U
U
U
U
U
U
U
Note: U: unclear.
194
Gao Z et al. / Systematic Review
JTCM |www. journaltcm. com April 15, 2020 |Volume 40 | Issue 2 |
Figure 4 Comparison of TK versus CWM in patients with stable COPD: change in total effectiveness ratesTK: tonifying kidney therapy; CWM: conventional Western Medicine; COPD: chronic obstructive pulmonary disease.
Figure 5 Comparison of TK versus CWM in patients with stable COPD: change in TCM Syndrome ScoreTK: tonifying kidney therapy; CWM: conventional Western Medicine; COPD: chronic obstructive pulmonary disease; TCM: Tradi-tional Chinese Medicine.
Figure 6 Comparison of TK versus CWM in patients with stable COPD: change in 6mWDTK: tonifying kidney therapy; CWM: conventional Western Medicine; COPD: chronic obstructive pulmonary disease; 6mWD: 6-minwalk distance in meters.
Figure 7 Comparison of TK versus CWM in patients with stable COPD: change in FEV1%TK: tonifying kidney therapy; CWM: conventional Western Medicine; COPD: chronic obstructive pulmonary disease; FEV1%: forcedexpiratory volume in one second%.
Figure 8 Comparison of TK versus CWM in patients with stable COPD: change in FEV1/FVC (%)TK: tonifying kidney therapy; CWM: conventional Western Medicine; COPD: chronic obstructive pulmonary disease; FEV1/FVC (%):forced expiratory volume in one second% / forced vital capacity.
195
JTCM |www. journaltcm. com April 15, 2020 |Volume 40 | Issue 2 |
Gao Z et al. / Systematic Review
21 Li MF, Gao X, Chen S. The clinical observation on treat-ing stable COPD with the Bushen Naqi Pingchuan pre-scription. Zhong Yi Lin Chuang Yan Jiu 2015; 7(8):62-63.
22 Li ZY, Tian CY, Liu JQ. Clinical observation on YiqiBushen Huoxue formula combined with salmeterol/flutica-sone inhalation powder in treating 35 cases of stable chron-ic obstructive pulmonary disease. Zhong Yi Za Zhi 2015;56(4): 307-310.
23 Li P, Chen T, Yan P. The Research on prevention and treat-ment of Bu Shen Fang Chuan recipe for Shen Xu Tan ZuXue Yu syndrome of COPD. Zhong Guo Yi Xue ChuangXin 2015; 12(1): 10-13.
24 Wang G, Liu B, Cao Y, et al. Effects of two Chinese herb-al formulae for the treatment of moderate to severe stablechronic obstructive pulmonary disease: a multicenter, dou-ble-blind, randomized controlled trial. PLoS One 2014; 9(8): e103168.
25 Mirza S, Clay RD, Koslow MA, Scanlon PD. COPDguidelines: a review of the 2018 GOLD report. Mayo ClinProc 2018; 93(10): 1488-1502.
26 COPD Group of Chinese Thoracic Society. Guidelinesfor the diagnosis and treatment of chronic obstructive pul-monary disease. Zhong Hua Jie He He Hu Xi Za Zhi2013; 36(4): 255-264.
27 Restrepo RD. Year in Review 2014: COPD. Respir Care2015; 60(7): 1057-1060.
28 Calverley PM, Anderson JA, Celli B, et al. Salmeterol andfluticasone propionate and survival in chronic obstructivepulmonary disease. N Engl J Med 2007; 356(8): 775-789.
29 Currie GP, Douglas JG. ABC of chronic obstructive pul-monary disease. Non-pharmacological management. BMJ2006; 332(7554): 1379-1381.
30 George J, Ioannides-Demos LL, Santamaria NM, KongDC, Stewart K. Use of complementary and alternativemedicines by patients with chronic obstructive pulmonarydisease. Med J Aust 2004;181(5): 248-251.
31 Liu SN, Shergis J, Chen XK, et al. Chinese herbal medi-cine (Weijing decoction) combined with pharmacotherapyfor the treatment of acute exacerbations of chronic obstruc-tive pulmonary disease. Evid Based Complement AlternatMed 2014; 2014: 257012.
32 Li SY, Wu QB. Experience of professor Cao shihong intreating chronic obstructive pulmonary disease. Zhong YiYao Xue Kan 2002; 20(1): 28-29.
33 Fan CY. The study of correlation with lung function ofTraditional Chinese Medicine of Qi deficieny syndromesof stable chronic obstructive pulmonary disease. Guang-zhou: Guangzhou University Of Chinese Medicine,2015: 13-20.
Table 4 The outcome end-points which were not included in Meta-analysis reported in randomized controlled trials
Study
Ni W et al 200817
Dai Y et al 201619
Wang GF et al 201624
SGRQ
P>0.05
CAT
P<0.05
mMRC
P<0.05
Frequency of acute exacerbation
P<0.01
P>0.05Notes: SGRQ: St George's respiratory questionnaire; CAT: COPD assessment test; mMRC: modified British medical research council.
Table 5 Safety evaluation of the included studies
Study
Zheng B 201520
Wang GF et al 201624
Sample size(T/C)
32/33
82+89/91
Liverfunction
√
√
Renalfunction
√
√
Routineurine test
√
√
Electrocardiogram
√
√
Routine bloodtests
√
√
Bloodglucose
×
√Notes: T: treatment group; C: control group.
196
Related Documents











