Tobacco Control/Underserved Populations Secondhand Smoke Exposure Among Hispanics/ Latinos Living in Multiunit Housing: Exploring Barriers to New Policies Lourdes A. Baezconde-Garbanati, PhD, MPH; Kimberly Weich-Reushe ´, MPH; Lilia Espinoza, PhD; Cecilia Portugal, MPH; Rosa Barahona, BA; James Garbanati, PhD; Faatima Seedat, BA; Jennifer B. Unger, PhD Abstract Purpose. Despite a high prevalence of voluntary home smoking bans and laws protecting Californians from exposure to secondhand smoke (SHS) in the workplace, many Hispanic/Latino (H/L) residents of multiunit housing (MUH) are potentially exposed to SHS from neighboring apartments. An advocacy/ policy intervention was implemented to reduce tobacco-related health disparities by encouraging H/L living in MUH to implement voluntary policies that reduce exposure to SHS. This article presents findings from qualitative and quantitative data collected during development of the intervention, as well as preliminary results of the intervention. Design, Setting, and Subjects. MUH residents in Southern California participated in focus groups (n 5 48), door-to-door surveys (n 5 142), and a telephone survey (n 5 409). Measures. Exposure to SHS, attitudes toward SHS, and attitudes toward policies restricting SHS in MUH were assessed. Results. H/L MUH residents reported high levels of exposure to SHS and little ability to protect themselves and their families from SHS. Respondents expressed positive attitudes toward adopting antismoking policies in MUH, but they also feared retaliation by smokers. The cultural values of familismo, respeto, simpatı ´a, and personalismo influenced their motivation to protect their families from SHS as well as their reluctance to ask their neighbors to refrain from smoking. Nonsmokers were more likely to favor complete indoor and outdoor smoking bans in MUH, whereas smokers were more likely to favor separate smoking areas. The Regale Salud advocacy/policy intervention, implemented to reduce SHS exposure, prompted the passage of seven voluntary policies in apartment complexes in Southern California to prevent smoking in MUH. Conclusions. H/L in California support voluntary policies, local ordinances, and state laws that prevent exposure to SHS in MUH, especially those that are consistent with H/L cultural values and norms for interpersonal communication. (Am J Health Promot 2011;25[5 Supplement]:S82–S90.) Key Words: Tobacco, Secondhand Smoke, Hispanic, Latino, Multiunit Housing, Apartment, Prevention Research. Manuscript format: research; Research purpose: descriptive, program evaluation; Study design: nonexperimental; Outcome measure: cognitive, behavioral; Setting: local community; Health focus: smoking control; Strategy: policy; Target population age: adults; Target population circumstances: low income, Hispanic/Latino, California PURPOSE California has been a natural labo- ratory and an exemplar for antismok- ing policies in the United States and around the world. 1–3 Although much progress has been made in the United States and California in reducing to- bacco prevalence, exposure to second- hand smoke (SHS) still impacts more than 126 million nonsmoking Ameri- cans. 4 Disproportionate exposure to SHS among minority groups, including Hispanic(s)/Latino(s) (H/L), could exacerbate tobacco-related health dis- parities. SHS Exposure in the H/L Community The H/L community is the largest minority population in the United States, and nearly one-third of U.S. H/L live in California. 5 Although the prevalence of smoking among H/L adults in California is relatively low compared with that of other ethnic groups, 6 H/L are disproportionately exposed to SHS in the workplace. California’s Smoke-Free Workplace Law (Law 6404.5 of the California State Labor Code) prohibits smoking in all indoor workplaces with more than five employees. 7 However, many H/L workers are not covered by this law. A disproportionately high number of H/L have jobs in small-service occupa- tions with only a few employees (e.g., automotive shops, employment within a private home), where California’s smoke-free workplace laws do not apply. Between 1990 and 2008, H/L nonsmokers have consistently reported the highest amount of exposure to Lourdes Baezconde-Garbanati, PhD; Cecilia Portugal, MPH; Rosa Barahona, BA; Faatima Seedat, BA; and Jennifer B. Unger, PhD, are with the Institute for Health Promotion and Disease Prevention Research, Department of Preventive Medicine; Lilia Espinoza, PhD, is with the Department of Family Medicine; and James Garbanati, PhD, is with the California School of Professional Psychology, Alliant International University, Alhambra, California. Kimberly Weich-Reushe ´, MPH, is with the Center for Tobacco Policy and Organizing, American Lung Association, Sacramento, California. Send reprint requests to Lourdes Baezconde-Garbanati, PhD, Institute for Health Promotion and Disease Prevention Research, Department of Preventive Medicine, University of Southern California Keck School of Medicine, 1000 South Fremont, Unit 8, Alhambra, CA 91803; [email protected]. This manuscript was submitted June 28, 2010; revisions were requested October 18, 2010; the manuscript was accepted for publication December 14, 2010. Copyright E 2011 by American Journal of Health Promotion, Inc. 0890-1171/11/$5.00 + 0 DOI: 10.4278/ajhp.100628-QUAL-219 S82 American Journal of Health Promotion May/June 2011, Vol. 25, No. 5 Supplement

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript
Tobacco Control/Underserved Populations
Secondhand Smoke Exposure Among Hispanics/Latinos Living in Multiunit Housing: ExploringBarriers to New PoliciesLourdes A. Baezconde-Garbanati, PhD, MPH; Kimberly Weich-Reushe, MPH; Lilia Espinoza, PhD;Cecilia Portugal, MPH; Rosa Barahona, BA; James Garbanati, PhD; Faatima Seedat, BA;Jennifer B. Unger, PhD
AbstractPurpose. Despite a high prevalence of voluntary home smoking bans and laws protecting Californians
from exposure to secondhand smoke (SHS) in the workplace, many Hispanic/Latino (H/L) residents ofmultiunit housing (MUH) are potentially exposed to SHS from neighboring apartments. An advocacy/policy intervention was implemented to reduce tobacco-related health disparities by encouraging H/L livingin MUH to implement voluntary policies that reduce exposure to SHS. This article presents findings fromqualitative and quantitative data collected during development of the intervention, as well as preliminaryresults of the intervention.
Design, Setting, and Subjects. MUH residents in Southern California participated in focus groups (n5 48), door-to-door surveys (n 5 142), and a telephone survey (n 5 409).
Measures. Exposure to SHS, attitudes toward SHS, and attitudes toward policies restricting SHS inMUH were assessed.
Results. H/L MUH residents reported high levels of exposure to SHS and little ability to protectthemselves and their families from SHS. Respondents expressed positive attitudes toward adoptingantismoking policies in MUH, but they also feared retaliation by smokers. The cultural values offamilismo, respeto, simpatıa, and personalismo influenced their motivation to protect their families fromSHS as well as their reluctance to ask their neighbors to refrain from smoking. Nonsmokers were more likelyto favor complete indoor and outdoor smoking bans in MUH, whereas smokers were more likely to favorseparate smoking areas. The Regale Salud advocacy/policy intervention, implemented to reduce SHSexposure, prompted the passage of seven voluntary policies in apartment complexes in Southern Californiato prevent smoking in MUH.
Conclusions. H/L in California support voluntary policies, local ordinances, and state laws thatprevent exposure to SHS in MUH, especially those that are consistent with H/L cultural values and normsfor interpersonal communication. (Am J Health Promot 2011;25[5 Supplement]:S82–S90.)
Key Words: Tobacco, Secondhand Smoke, Hispanic, Latino, Multiunit Housing,Apartment, Prevention Research. Manuscript format: research; Research purpose: descriptive,program evaluation; Study design: nonexperimental; Outcome measure: cognitive,behavioral; Setting: local community; Health focus: smoking control; Strategy: policy; Targetpopulation age: adults; Target population circumstances: low income, Hispanic/Latino,California
PURPOSE
California has been a natural labo-ratory and an exemplar for antismok-ing policies in the United States andaround the world.1–3 Although muchprogress has been made in the UnitedStates and California in reducing to-bacco prevalence, exposure to second-hand smoke (SHS) still impacts morethan 126 million nonsmoking Ameri-cans.4 Disproportionate exposure toSHS among minority groups, includingHispanic(s)/Latino(s) (H/L), couldexacerbate tobacco-related health dis-parities.
SHS Exposure in the H/L CommunityThe H/L community is the largest
minority population in the UnitedStates, and nearly one-third of U.S.H/L live in California.5 Although theprevalence of smoking among H/Ladults in California is relatively lowcompared with that of other ethnicgroups,6 H/L are disproportionatelyexposed to SHS in the workplace.California’s Smoke-Free WorkplaceLaw (Law 6404.5 of the California StateLabor Code) prohibits smoking in allindoor workplaces with more than fiveemployees.7 However, many H/Lworkers are not covered by this law. Adisproportionately high number ofH/L have jobs in small-service occupa-tions with only a few employees (e.g.,automotive shops, employment withina private home), where California’ssmoke-free workplace laws do notapply. Between 1990 and 2008, H/Lnonsmokers have consistently reportedthe highest amount of exposure to
Lourdes Baezconde-Garbanati, PhD; Cecilia Portugal, MPH; Rosa Barahona, BA; Faatima Seedat, BA;and Jennifer B. Unger, PhD, are with the Institute for Health Promotion and Disease Prevention Research,Department of Preventive Medicine; Lilia Espinoza, PhD, is with the Department of Family Medicine; andJames Garbanati, PhD, is with the California School of Professional Psychology, Alliant InternationalUniversity, Alhambra, California. Kimberly Weich-Reushe, MPH, is with the Center for Tobacco Policyand Organizing, American Lung Association, Sacramento, California.
Send reprint requests to Lourdes Baezconde-Garbanati, PhD, Institute for Health Promotion and DiseasePrevention Research, Department of Preventive Medicine, University of Southern California Keck Schoolof Medicine, 1000 South Fremont, Unit 8, Alhambra, CA 91803; [email protected].
This manuscript was submitted June 28, 2010; revisions were requested October 18, 2010; the manuscript was accepted for publicationDecember 14, 2010.
Copyright E 2011 by American Journal of Health Promotion, Inc.0890-1171/11/$5.00 + 0DOI: 10.4278/ajhp.100628-QUAL-219
S82 American Journal of Health Promotion May/June 2011, Vol. 25, No. 5 Supplement

SHS in indoor work areas, comparedwith other ethnic and racial groups.8,9
Because of their lower average so-cioeconomic status, H/L in Californiaare more likely than non-Hispanics tolive in multiunit housing complexes(MUH; 46% of H/L vs. 37% of non-Hispanics).10 MUH are apartmentbuildings, townhouses, or condomini-ums that share common walls and/orcommon areas such as hallways, laun-dry rooms, parking garages, stairwells,or courtyards. Although most H/Lhouseholds have complete or partialsmoking bans to protect children fromSHS exposure,9,11 H/L residents livingin MUH are at risk for exposure to SHSfrom neighboring units. California’sSmoke-Free Workplace Law does applyto MUH complexes that employ five ormore workers, including managers andmaintenance workers. The law requiresthat all enclosed common areas, in-cluding lobbies, halls, laundry rooms,stairways, elevators, recreation rooms,and the manager’s office, in a MUHcomplex be smoke-free.12 However, thelaw does not protect the residents inMUH from being exposed to SHS fromsmoke drifting into their units fromneighboring units or outdoor areas.The California Division of Occupa-tional Safety and Health reported that‘‘tobacco smoke travels from its pointof generation in a building to all otherareas of the building…through lightfixtures, through ceiling crawl spaces,and into and out of doorways.’’13 InCalifornia’s warm climate, windowsand doors are often open, allowingunimpeded flow of smoke. Althoughlevels of exposure to SHS have de-creased by 70% between the late 1980sand 2002,14 protection from SHS in theH/L community remains a priority inCalifornia’s H/L health agenda.
Voluntary PoliciesAlthough most California house-
holds have complete or partial smok-ing bans,7,15 voluntary policies to pro-tect MUH residents from SHS fromneighboring units or outdoor areas arerare. Voluntary smoking bans in MUHcould be useful not only in protectingnonsmokers from SHS exposure butalso in supporting smokers in theirquit attempts, helping them to contin-ue refraining from smoking, and pre-venting youth from initiating smok-
ing.7,16,17 According to a statewideCalifornia survey in 2004 to 2005,18 themajority of apartment residents andowner/managers favored a law requir-ing all apartment buildings to offernonsmoking sections. Nearly one-halfof the apartment owners and managershad received complaints from tenantsabout SHS exposure.
Regale Salud—An Advocacy/PolicyIntervention to Reduce Exposure to SHSin Predominantly H/L MUH
Regale Salud (Give the Gift of Health)is an intervention that uses the envi-ronmental change model to reducetobacco-related health disparities byencouraging voluntary policies to con-trol SHS exposure among H/L MUHresidents. This intervention has beendesignated a model program by theCenters for Disease Control’s NationalLatino Tobacco Control Network andis being implemented in Californiaand several other states. To the au-thors’ knowledge, it is the only SHSprevention program specifically target-ed toward H/L MUH residents.
The Regale Salud intervention incor-porates and addresses H/L culturalvalues, which have been described indetail elsewhere.19,20 Some of thesecultural values may make individualsreluctant to ask others not to smoke,such as respeto—a norm of treating otherswith respect or admiration and notinterfering with their personal deci-sions; personalismo—relating to others ona personal, friendly level; and simpatıa—maintaining agreeable social relation-ships and avoiding direct confrontation.These cultural values may make H/Lresidents feel that it is not appropriate toask their neighbors to change theirsmoking habits or that doing so mightjeopardize their relationships withneighbors who smoke. Other culturalvalues emphasize the importance of theimmediate and extended family over theindividual, which includes the responsi-bility to protect children from SHS. Themost salient of these values is familismo—respect, loyalty, and unity within theimmediate and extended family, in-cluding the responsibility to take care offamily members. These cultural valuesare common to most H/L groups, butsome are endorsed more strongly thanothers depending on acculturation,personality, and individual differences.
The Regale Salud program attempts toeducate all apartment residents, man-agers, and owners about the problem ofSHS so that they can implement volun-tary policies in a collectivist mannerrather than waiting for individual resi-dents to initiate confrontations.
Regale Salud calls for individuals inthe H/L community to advocate forand adopt voluntary nonsmoking pol-icies to protect workers, residents, andfamilies beyond the parameters of theCalifornia Smoke-Free Workplace Law.The premise is that health is a gift thatcan be given by anyone, includingsmokers who want to protect othersfrom the dangers of SHS. The inter-vention consists of multiple phases(outlined briefly in Table 1).
An essential element of Regale Saludinvolves convincing apartment ownersthat their tenants really are bothered bySHS and would support smoke-freepolicies. To gather evidence to supportthis claim, we conducted three phasesof research, using mixed quantitativeand qualitative methods. A community-based participatory research model wasused, involving community membersand local stakeholders throughout theprocess. The qualitative portion of theresearch consisted of focus groups toexplore the issue of SHS in the homeamong H/L MUH tenants. The focusgroup findings were used to inform thedevelopment of a door-to door inter-cept survey and a telephone survey toassess attitudes toward implementingvoluntary antismoking policies in MUH.These two survey methodologies wereused to increase representativeness andgeneralizability of the sample; door-to-door intercept surveys are more expen-sive and typically cover more limitedgeographical areas, whereas telephonesurveys can cover wider areas but arelimited to residents who have landlinetelephones and are listed in telephonedirectories. After describing the find-ings from the three data collectionphases, we present preliminary out-comes of the implementation of theRegale Salud intervention.
METHODS
All data collection methods de-scribed below were approved by theinstitutional review board.
American Journal of Health Promotion May/June 2011, Vol. 25, No. 5 Supplement S83
Phase 1: Focus Groups
Method. In 2005 to 2007, five focusgroups were conducted with H/L inLos Angeles County, Riverside County(southeast of Los Angeles), San Ber-nardino County (east of Los Angeles),and Fresno County (in central Califor-nia, northwest of Los Angeles). Theseareas were selected because of theirlarge and rapidly growing H/L popu-lations and because they include urbanand suburban areas. The apartmentcomplexes selected consisted of at least93% residents of Mexican origin andhad no smoking restrictions currentlyin place.
The protocol and focus group guidewere developed by staff from the H/LTobacco Education Network and pilottested with one group of H/L MUHresidents. Questions assessed residents’self-reported SHS exposure, opinionsabout the extent of the problem ofSHS, perceptions of the effects of SHS,willingness to take action in favor ofvoluntary policies, and perceptions ofpotential advantages and disadvantagesof voluntary policies. Verbal assent wasreceived from each participant. Thefocus groups were audio-recorded, anda Spanish-speaking staff member re-corded notes. Participants receivededucational pamphlets about tobaccoand small token gifts worth approxi-
mately $5 (e.g., hats, tote bags, writingpads, water bottles imprinted with theRegale Salud logo).
Analyses. Audio-recordings were tran-scribed verbatim by a trained Spanish-speaking staff member. Two bilingualstaff members translated the Spanishtext into English independently, com-pared their translations, and agreed ona final English version. Focus groupdata were coded and analyzed themat-ically using Nud*ist qualitative soft-ware, and responses were collapsedaccordingly by two senior researcherswho served as focus group raters.
Phase 2: Door-to-Door Intercept Surveys
Method. To obtain a broader under-standing of the feasibility of imple-menting voluntary policies in MUH, weconducted a door-to-door interceptsurvey of 142 apartment residents inLos Angeles and Riverside Counties in2007. Apartment complexes were se-lected based on their high proportionsof low-income H/L residents. Of the18 apartment complexes approached,7 agreed to participate. Surveys wereconducted on weekends to maximizeparticipation. The survey was conduct-ed by three pairs of bilingual datacollectors, who knocked on every otherdoor of the selected complexes. Thedata collectors delivered an introduc-
tory script, obtained consent, andadministered the 12-minute survey inthe respondent’s preferred language.Participants received educationalpamphlets about tobacco and smalltoken gifts worth approximately $5(e.g., hats, tote bags, writing pads,water bottles imprinted with the RegaleSalud logo).
Survey questions were developedfrom the focus group findings andfrom existent surveys endorsed byCalifornia’s Clean Air Project of theAmerican Lung Association and othermaterials available through the Cali-fornia Tobacco Control Program eval-uation technical assistance provider.Two bilingual staff members indepen-dently translated the survey into Span-ish and then compared their transla-tions to create a final Spanish versionof the survey. The Spanish survey waspilot-tested with several Spanish-speak-ing adults in Los Angeles to identifyany ambiguous wording or unfamiliaridioms. Questions assessed residents’perceived harm of SHS, whether andwhere they had been exposed to SHS,and how much SHS bothered them.We also asked about their support forvoluntary smoking bans in their apart-ment complex.
Analyses. Frequencies were calculatedand compared with the focus group
Table 1Phases of the Regale Salud Intervention
Phase Objective Specific Activities
1 Establish objectives and gather baseline data Survey residents of specific apartment complexesDetermine extent of problem and level of support
2 Determine level of capacity buildingnecessary to implement program
Identify leaders in community; identify people, organizations, coalitions, and othergroups that could be involved; assess their capacity and readiness to act
3 Identify allies and opposing forces Determine level of support for advocacy/policy campaignPartner with other service providers such as California Smokers’ HelplineOffer to provide information and technical assistance
4 Identify participants and develop materials Form committees of residents, managers, owners, and business patronsEstablish framework of mutual respect and equityDevelop materials that are culturally acceptable and language appropriatePilot-test the materials
5 Implement intervention Establish effective communication systems, acknowledging culture, language, andeducational levels
Educate residents, managers, and owners about voluntary policiesEncourage policy adoption and enforcement
6 Recognize efforts Capitalize on local media opportunities to publicize program and acknowledgeparticipants
Place ads in local mediaDocument results with formal evaluation
S84 American Journal of Health Promotion May/June 2011, Vol. 25, No. 5 Supplement

findings to detect similarities anddifferences.
Phase 3: Telephone Survey
Method. In partnership with the Centerfor Policy and Organizing, we con-ducted a telephone survey to assessknowledge and attitudes about smoke-free MUH among H/L MUH residentsin 2006. The sample was obtained froma commercially available listing ofapartment renters with H/L surnameswho were listed in the telephonedirectory. Because some people withH/L surnames are not H/L, theinterviewer verified that the partici-pants self-identified as H/L beforeproceeding with the survey. Questionsfocused on living conditions, type ofdwelling, household composition, SHSexposure, and attitudes about policiesto prohibit smoking in MUH. Twobilingual staff members independentlytranslated the survey into Spanish andthen compared their translations tocreate a final Spanish version of thesurvey. The Spanish survey was pilot-tested with several Spanish-speakingadults in Los Angeles to identify anyambiguous wording or unfamiliar idi-oms. The 30-minute survey was ad-ministered by a bilingual call center.Respondents were not compensatedfor their participation.
Analyses. Frequencies and univariatestatistics were calculated. Attitudes to-ward SHS and smoking bans werecompared between smokers and non-smokers with x2 tests.
RESULTS
Phase 1: Focus GroupsA total of 48 participants attended
the focus groups, with six to eightparticipants per group. More than halfof the participants (53.6%) were fromRiverside County. Sixty-five percent ofthe participants were female, and 35%were male. Almost half of the partici-pants (46%) were between the ages of26 and 40 years, and almost one-third(29%) of the participants were 55 yearsand older. All participants weremonolingual Spanish speakers.
All participants knew that SHS hadharmful health effects. Most of theparticipants (71%) reported being
exposed to SHS at home or work, and65% felt that SHS was a problem wherethey lived. Participants reported beingexposed to SHS from neighbors smok-ing in their units or in common areas.Some were exposed to the smell ofcigarette smoke when family memberscame home after smoking or being withsmokers. Participants expressed con-cern about the effects of SHS onchildren. Most (85%) did not have awritten or verbal policy prohibitingsmoking in their building, but 71%believed that it would be possible toobtain support for a written voluntarypolicy prohibiting smoking in commonareas. Participants, including smokers,expressed support for the establish-ment of smoke-free policies in commonareas, with appropriate signage.
Three broad themes emerged: (1)impact of SHS exposure in MUH, 2)protection of themselves and theirfamilies from SHS exposure, and (3)attitudes toward the implementation ofvoluntary policies that protect resi-dents from SHS exposure.
Theme 1: Impact of Exposure to SHS.Several questions focused on how SHSaffected MUH residents. Participants’responses centered on how the smokepenetrated the apartment units, re-gardless of whether the smoker wasindoors or outdoors. They also ex-pressed hesitancy about asking peoplenot to smoke because they value theirfriendship. The value of simpatıa wasevident. One participant expressed herconflict between disliking smoke andnot wanting to offend her neighbors:
‘‘It affects me a lot because I don’tsmoke. When I open the door I cansmell the cigarette. The smoker isalways happy, but I’m not. See, thereare three neighbors that are alwayssmoking, but they are good people,and I like them very much. But theysmoke too much. Although they aresmoking outdoors the smell stillcomes inside my apartment.’’
Theme 2: Protecting Themselves and TheirFamilies From SHS Exposure. Whenasked about what they have done toavoid exposure to SHS, respondentsmentioned several strategies. However,these strategies were not sufficient toprotect them completely:
‘‘We close the doors. We placetowels or a cloth under the doors.But it doesn’t matter; it is as if wehad not done anything.’’‘‘Sometimes we need to sleep withour windows open. Every night myhusband opens all the windows sowe can get some air because that isthe only time that we can get someclean air so keep the windows openall night.’’‘‘Whatever comes in stays in and itdoes not leave. Not even with the airconditioner.’’
Respondents believed that it wouldbe beneficial to educate smokers andothers about SHS, but they also believedthat the smokers really did not care.Respondents were reluctant to ask theirneighbors not to smoke because theneighbors were paying to live there andthey did not want to interfere with theirdecisions. Therefore, they felt disem-powered and hopeless. Although thenonsmokers had tried to use the valueof familismo to convince smokers not tosmoke near children, these efforts hadnot been effective. Participants believedthat these efforts need to be supportedby something more formal, such as aclause in the rental contract and signson the property:
‘‘It should be in the contract beforeyou move in.’’‘‘Put up signs to remind peopleabout the dangers of smoking.’’
Theme 3: Attitudes TowardVoluntary Policies. Most respondentshad never heard of voluntary policiesto regulate SHS exposure in commonliving areas. Some expressed doubtsabout whether such a policy would belegal and whether it would be discrim-inatory. After we explained that volun-tary policies were legal and that smok-ing was not a fundamental right, theparticipants were positive about thepotential benefits of such a policy,highlighting the collective benefits:
‘‘There would be benefits for every-one…and also for the childrenbecause I was going to let my childgo outside and instead we went backinside because they were smokingoutside.’’
American Journal of Health Promotion May/June 2011, Vol. 25, No. 5 Supplement S85

Although respondents generally fa-vored voluntary policies, some residentswere reluctant to challenge the statusquo because of their respeto values:
‘‘Even for the older people thatdon’t listen this would be good,but they are older and who am I totell them what to do?’’‘‘We need to educate everyone in arespectful way.’’‘‘There is an apartment availablenext door. I am glad that person leftbecause it was a smoker but I hope Idon’t get another smoker. Depend-ing on who he/she is I don’t know ifI can ask them not to smoke.’’
Respondents listed some potentialbarriers to a voluntary policy. Theywere concerned about angering thesmokers:
‘‘Those that smoke might get an-gry.’’‘‘We would be lost if the ownersmoked because they might attackus.’’
Some respondents were also con-cerned that owners would not supportthe policy because it would make itmore difficult to fill their vacantapartments, although others disagreed:
‘‘Many of the owners don’t havethose rules because they rent theplaces more easily…all the ownerscare is to have money and they don’twant to lose anything.’’‘‘I think it would be the oppositebecause people would then see thatthe place does not smell bad and it ismuch cleaner so people would bemuch happier in living in a cleanarea. The building would not lookdirty.’’
Respondents had mixed views aboutthe extent to which their fellow resi-dents would support a policy. Ingeneral, they believed that nonsmokerswould support the policy, but smokerswould not:
‘‘Although they would like to behelpful they can’t because they lovecigarettes.’’‘‘I think there would not (be muchsupport)…because they smoke all
over the place…in the garage, out-side, inside, everywhere.’’
Respondents believed that it wouldbe easier to pass a voluntary policy forcommon areas such as patios andlaundry rooms, but that this would notsolve the SHS problem completely:
‘‘Common areas, because I wouldfeel bad if someone came to tell meyou can’t smoke in your apart-ment.’’‘‘It does not matter if it is indoors oroutdoors. The smoke still comes ineither way.’’
When asked if they would be willingto write a note to tell the owner abouttheir concerns regarding SHS expo-sure and a possible voluntary policy asa solution, respondents were not yetready to take action:
‘‘It would not matter because we arethe minority; they only listen to themajority.’’‘‘At least now I don’t think manywould speak up. Look at this group,it is small compared to all thepeople that live here.’’
Phase 2: Door-to-Door Intercept SurveysA total of 142 residents participated
in the survey, with an 86% participationrate. Slightly more than one-half (56%)of the respondents were female; and29% were aged 18 to 30 years, 27% were31 to 40 years, 33% were 41 to 64 years,and 11% were 65 years or older.
Nearly all respondents (97%) be-lieved that SHS is harmful, and themajority (68%) believed that SHS candrift into their units from the outside.Respondents reported that SHS haddrifted into their units from outside(35%) or from other units (20%).Respondents were asked if they hadbeen exposed to SHS in specific indoorand outdoor common areas. The mostspecific locations of SHS exposurewere the lobby/entrance (24%), bal-cony/patio (23%), and stairs/hallway(20%). Other areas included recrea-tional areas and the garage/parkingstructure. Two-thirds of the respon-dents (66%) stated that they had been‘‘somewhat’’ bothered or bothered ‘‘alot’’ by SHS in their apartments.
Only 35% said they had taken actionto address the issue of SHS. Theseactions included moving away from theperson, asking the person to stopsmoking or move away, and closingdoors and windows. Among those whodid not take action, reasons for nottaking action included issues of dis-empowerment (‘‘Because I cannot doanything,’’ ‘‘I did not know that I cando something about it,’’ ‘‘I can’tcontrol other’s actions’’) and discom-fort with confrontation (‘‘I didn’t feelcomfortable telling them,’’ ‘‘I don’twant to look for trouble or problems,’’‘‘People might get mad,’’ ‘‘Tooscared’’).
We also asked about preferences forsmoke-free MUH. Most respondentsstated that they would like to live in anonsmoking section of an apartmentbuilding (82%) or in a completelysmoke-free building (80%). The ma-jority (63%) believed that a tenantshould be required to move if theycontinue to smoke after signing anonsmoking agreement.
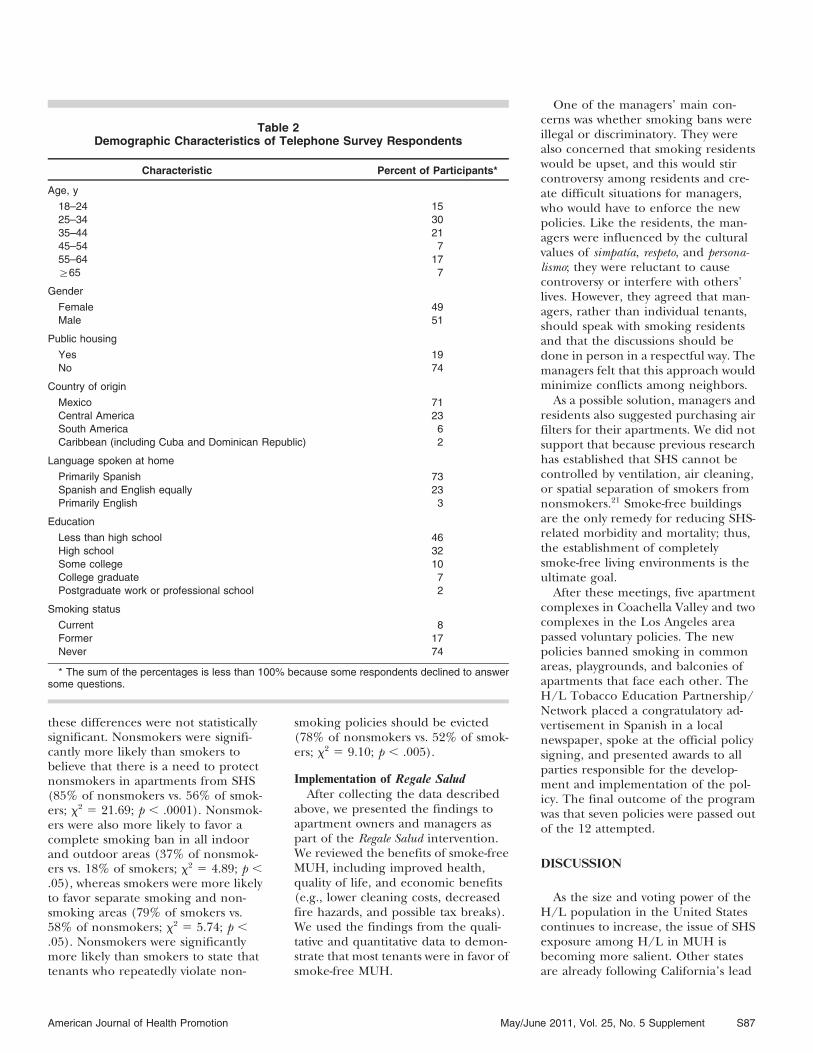
Phase 3: Telephone SurveyA total of 409 H/L adult renters in
California participated in the tele-phone survey. Table 2 shows the de-mographic characteristics of the re-spondents. Participants ranged in agefrom 18 to 89 years (mean, 38.7 years;SD, 14.6 years). The median numberof people living in their units (includ-ing the respondent) was 5, and themedian number of bedrooms was 2.Most lived in small- to medium-sizedapartment buildings: 40% lived inbuildings with 10 or fewer units, and24% lived in buildings with 11 to50 units. Only 8% of the respondentshad smoked in the past week (13% ofthe men and 4% of the women), but17% had a smoker in the household.Nearly all (95%) had banned smokinginside their own units. Only 26%reported that their current apartmentbuildings restricted smoking in indoorcommon areas, and only 19% reportedsmoking restrictions in outdoor com-mon areas.
Table 3 compares attitudes towardSHS and smoke-free policies betweensmokers and nonsmokers. In general,nonsmokers had stronger beliefs aboutthe negative effects of SHS and itsability to drift into apartments, but
S86 American Journal of Health Promotion May/June 2011, Vol. 25, No. 5 Supplement
these differences were not statisticallysignificant. Nonsmokers were signifi-cantly more likely than smokers tobelieve that there is a need to protectnonsmokers in apartments from SHS(85% of nonsmokers vs. 56% of smok-ers; x2 5 21.69; p , .0001). Nonsmok-ers were also more likely to favor acomplete smoking ban in all indoorand outdoor areas (37% of nonsmok-ers vs. 18% of smokers; x2 5 4.89; p ,.05), whereas smokers were more likelyto favor separate smoking and non-smoking areas (79% of smokers vs.58% of nonsmokers; x2 5 5.74; p ,.05). Nonsmokers were significantlymore likely than smokers to state thattenants who repeatedly violate non-
smoking policies should be evicted(78% of nonsmokers vs. 52% of smok-ers; x2 5 9.10; p , .005).
Implementation of Regale SaludAfter collecting the data described
above, we presented the findings toapartment owners and managers aspart of the Regale Salud intervention.We reviewed the benefits of smoke-freeMUH, including improved health,quality of life, and economic benefits(e.g., lower cleaning costs, decreasedfire hazards, and possible tax breaks).We used the findings from the quali-tative and quantitative data to demon-strate that most tenants were in favor ofsmoke-free MUH.
One of the managers’ main con-cerns was whether smoking bans wereillegal or discriminatory. They werealso concerned that smoking residentswould be upset, and this would stircontroversy among residents and cre-ate difficult situations for managers,who would have to enforce the newpolicies. Like the residents, the man-agers were influenced by the culturalvalues of simpatıa, respeto, and persona-lismo; they were reluctant to causecontroversy or interfere with others’lives. However, they agreed that man-agers, rather than individual tenants,should speak with smoking residentsand that the discussions should bedone in person in a respectful way. Themanagers felt that this approach wouldminimize conflicts among neighbors.
As a possible solution, managers andresidents also suggested purchasing airfilters for their apartments. We did notsupport that because previous researchhas established that SHS cannot becontrolled by ventilation, air cleaning,or spatial separation of smokers fromnonsmokers.21 Smoke-free buildingsare the only remedy for reducing SHS-related morbidity and mortality; thus,the establishment of completelysmoke-free living environments is theultimate goal.
After these meetings, five apartmentcomplexes in Coachella Valley and twocomplexes in the Los Angeles areapassed voluntary policies. The newpolicies banned smoking in commonareas, playgrounds, and balconies ofapartments that face each other. TheH/L Tobacco Education Partnership/Network placed a congratulatory ad-vertisement in Spanish in a localnewspaper, spoke at the official policysigning, and presented awards to allparties responsible for the develop-ment and implementation of the pol-icy. The final outcome of the programwas that seven policies were passed outof the 12 attempted.
DISCUSSION
As the size and voting power of theH/L population in the United Statescontinues to increase, the issue of SHSexposure among H/L in MUH isbecoming more salient. Other statesare already following California’s lead
Table 2Demographic Characteristics of Telephone Survey Respondents
Characteristic Percent of Participants*
Age, y
18–24 1525–34 3035–44 2145–54 755–64 17§65 7
Gender
Female 49Male 51
Public housing
Yes 19No 74
Country of origin
Mexico 71Central America 23South America 6Caribbean (including Cuba and Dominican Republic) 2
Language spoken at home
Primarily Spanish 73Spanish and English equally 23Primarily English 3
Education
Less than high school 46High school 32Some college 10College graduate 7Postgraduate work or professional school 2
Smoking status
Current 8Former 17Never 74
* The sum of the percentages is less than 100% because some respondents declined to answersome questions.
American Journal of Health Promotion May/June 2011, Vol. 25, No. 5 Supplement S87

in implementing smoke-free apart-ment initiatives. Support for suchpolicies needs to be supplementedwith local action and incentives forbuilding owners to implement smoke-free policies.
Overcoming Barriers to Smoke-FreeEnvironments in MUH
This study identified some potentialbarriers to implementing smoke-freehousing policies. The cultural values ofrespeto, personalismo, and simpatıa madesome residents hesitant to ask theirneighbors not to smoke. Many re-spondents empathized with the smok-ers, mentioning how inconvenient itwould be for the smokers to be forcedto refrain from smoking in commonareas. Respondents also stated that itwould be inappropriate and difficultfor a younger person to ask an elderlyperson not to smoke. This indicatesthat voluntary policies initiated bytenants might be difficult to enforce.However, if apartment owners ormanagers initiated the policy andreinforced it with signage, residentswould feel more empowered to askpeople not to smoke. This indicatesthat smoke-free policies should beinitiated and enforced by authorityfigures such as managers, apartmentowners, or city ordinances.
Although some cultural values couldbe barriers to enforcement of volun-
tary policies, other cultural values mayempower residents to protect theirfamilies from SHS. For example, thevalue of familismo made residents quiteconcerned about the effects of SHS ontheir family members. Familismo mayempower residents to insist on smoke-free environments for the entire fam-ily, especially the children, the elderly,and those with chronic illnesses. Resi-dents also could reframe the roles ofrespeto and simpatıa to shift the focusfrom protecting the smokers frominconvenience to protecting the healthof the whole community.
The owners’ and managers’ barriersto implementing policies were theirconcerns that nonsmoking policiesmight be discriminatory or illegal andthat they would be unable to fill theirvacant apartments. It is important toeducate landlords that smoke-free pol-icies are legal and that the majority oftenants actually favor smoke-freeapartments. The present findings in-dicate that once landlords understandthat their own tenants favor nonsmok-ing policies, they are more receptive tothe idea. We recommend collectingdata from the residents of the land-lords’ own apartment complexes toconvince landlords that their tenantssupport nonsmoking policies. Ourexperience suggests that landlords andtenants each have unique roles increating and maintaining smoke-free
MUH: the tenants need to voice theirpreference for smoke-free MUH andthe landlords need to create an envi-ronment where tenants feel safe andempowered to voice their preferenceswithout fear of reprisal. As a result,tenants and landlords will be moresatisfied and healthy.
The current findings in the Califor-nia H/L community are consistentwith findings from previous studies inother demographic groups in otherstates. Surveys of MUH residents inMinnesota22–24 found that substantialproportions of residents were botheredby SHS entering their units. Most ofthese respondents reported that theircurrent buildings did not have smoke-free policies, but they would prefer tolive in a building with smoke-freepolicies. Moreover, although residentswere bothered by SHS, very few hadtalked to owners, managers, or thesmokers about their concerns. This isvery similar to our findings from thedoor-to-door intercept survey. A studyof low-income MUH residents in sub-sidized housing in Oregon25 foundstrong support for smoke-free MUHpolicies among nonsmokers but muchweaker support among smokers. This isconsistent with the results from ourtelephone survey, although we foundthat the vast majority of residents(smokers and nonsmokers) were infavor of some type of policy to protect
Table 3Comparison of Attitudes Toward SHS and No-Smoking Policies Between Smokers and Nonsmokers!
Attitude/Belief
Percent Who Agreed
x2
OverallSample
(N = 409)Nonsmokers
(n = 375)Smokers(n = 34)
SHS is harmful 98 98 97 5.02SHS can drift from one apartment to another 86 86 79 1.97SHS can drift from outside an apartment building into an apartment 82 83 76 2.86Have experienced SHS drifting into your apartment 63 64 53 1.79There is need for laws to protect nonsmokers in apartments from SHS 82 85 56 21.69***Strongly favor law limiting smoking in outdoor common areas of apartment buildings 78 79 68 5.56Favor a complete smoking ban in all indoor and outdoor areas 35 37 18 4.89*Favor separate smoking and nonsmoking areas 60 58 79 5.74*Favor law requiring all apartment buildings to offer sections that are completely nonsmoking 86 86 85 3.64Tenants should be evicted for repeat violations of no-smoking policies 76 78 52 9.10**
! SHS indicates secondhand smoke; Smoker, smoked in the past week; and nonsmoker, did not smoke in the past week.* p , 0.05.** p , 0.005.*** p , 0.0005.
S88 American Journal of Health Promotion May/June 2011, Vol. 25, No. 5 Supplement

nonsmokers from SHS. The maindifference between the smokers andnonsmokers in our study was that thenonsmokers favored a complete in-door and outdoor smoking ban,whereas the smokers favored separatesmoking areas. The consistency ofthese findings across states with diversedemographic characteristics suggeststhat there is widespread support forsmoke-free MUH.
Our findings from apartment ownersand managers are also consistent withthose documented in other states. Asurvey of apartment owners and man-agers in New York26 found that fewowners and managers had implement-ed smoke-free policies, but most werereceptive to the idea. Their mainperceived barrier to implementationwas concern about vacancy rates. In aMinnesota study,23 owners and manag-ers were aware of SHS, but they werereluctant to implement smoke-freepolicies because they were concernedabout increasing their vacancy rates,being accused of discriminatingagainst smokers, or incurring addi-tional responsibilities to enforce thepolicies. However, owners who hadalready implemented smoke-free poli-cies reported neutral or positive effectson vacancies, apartment turnover, andmanagement workload. It is under-standable that apartment owners andmanagers are worried about the effectof smoke-free policies on their abilityto rent out their apartments, but theevidence suggests that these policies infact will not adversely affect theiroccupancy rates and are not overlyburdensome.
LimitationsAlthough Regale Salud focuses on
voluntary policy development, the H/LTobacco Education Partnership/Net-work also collaborated with smoke-freehousing coalitions in California toencourage the passage of city-levelordinances to give priority to develop-ers who would build smoke-free afford-able housing. This could have influ-enced support for smoke-free housing.Another limitation of this study is thatencouraging the passage of policies forsmoke-free common areas (indoors andoutdoors) does not address the prob-lem of smoke drifting from neighbor-ing units because such a policy would
drive smokers back into their homesand expose their families and neigh-bors to SHS. Therefore, we favor totalsmoking bans rather than partial bans.The Regale Salud intervention needs toevolve its advocacy and policy workfurther to reflect and acknowledge thedisadvantages of partial vs. completevoluntary policies. Also, it is importantto work with apartment owners inaddition to managers and residents.Owners can establish permanent poli-cies that can survive after managers andresident advocates leave.
Although we attempted to obtain themost comprehensive and representa-tive data possible by using mixedqualitative and quantitative methodsand using two different samplingmethodologies for the quantitativesurveys, our method does have severallimitations. Sampling for the focusgroup portion of the project was onlyperformed with two MUH facilities;thus, generalizability to other MUHfacilities is limited. The door-to-doorintercept surveys were limited to resi-dents who were at home and agreed toparticipate. Thus, residents who spendmuch of their time away from homewere likely underrepresented. Thetelephone survey was limited to peoplewith Hispanic surnames who hadlandline phones and were listed in thetelephone directory. Thus, cell phone–only households and Hispanics withoutobvious Hispanic surnames were un-derrepresented. Although each meth-odology has inherent limitations, webelieve that the similar findings acrossthe three phases of data collectionsupport the validity of the findings.
Because we did not ask participantsto divulge their smoking status in thefocus group and door-to-door inter-cept surveys, we were unable to analyzedifferences between smokers and non-smokers. The telephone survey resultsrevealed some similarities and somedifferences between smokers and non-smokers; respondents generally agreedthat SHS smoke was harmful andshould be avoided, but nonsmokersfavored more restrictions on smoking.In future studies, it would be useful toascertain all participants’ smoking sta-tus, if this can be done withoutcompromising participation rates.
Because of budgetary constraints,this project was unable to collect data
on the sustainability of the Regale Saludintervention or its long-term effects onSHS exposure among MUH residents.Longitudinal studies are needed toassess these important outcomes.
RecommendationsBased on the three phases of data
gathering described in this article andthe preliminary outcomes of the RegaleSalud intervention, we offer severalrecommendations to promote smoke-free choices in MUH. At the policylevel, we encourage municipalities topass ordinances that prohibit smokingin all new and existing residences thatshare walls or common areas. Outdoorcommon areas should be smoke-freeexcept for designated smoking areas.Rental clauses should specify wheresmoking is allowed and the conse-quences of smoking in units or com-mon areas. Involuntary exposure toSHS in residential housing should bedeclared a public nuisance, especiallywhen it impacts children and theelderly.
Until such policies are widespread,we encourage individual apartmentowners and managers to implementand enforce policies to protect theirresidents from SHS. The findings ofthis study indicate that most residents,even smokers, acknowledge the harmassociated with SHS and favor at leastminimal restrictions. If apartmentowners are unsure about their tenants’preferences, we encourage them to askthe tenants, confidentially or anony-mously if possible. We expect that theywill find that protecting their residentsfrom SHS will actually result in moresatisfied, loyal, long-term tenants,rather than increased vacancies.
Although some MUH residents mayfeel powerless to avoid SHS, they canbecome empowered. MUH residentscan form partnerships with communi-ty-based organizations involved in thehousing industry (e.g., affordablehousing); health organizations; andcity, county, or state agencies thatpromote smoke-free housing. Coali-tions of residents can educate theirlandlords about the hazards of SHSand the health, safety, and economicbenefits of smoke-free housing. If acritical mass of tenants demandssmoke-free environments, voluntaryand formal policies will follow.
American Journal of Health Promotion May/June 2011, Vol. 25, No. 5 Supplement S89
CONCLUSIONS
In California, apartment residents,managers, and owners are passingvoluntary policies to prohibit smokingindoors and in outdoor communalareas of MUH complexes. Policies thatprohibit smoking in communal areasare capable of surviving most legalchallenges because smoking is notconsidered a fundamental right. Asstate and local ordinances and volun-tary policies in MUH gain momentum,it is our hope that the option to chooseto live in smoke-free environments willbecome the norm.
Acknowledgments
The authors thank Jeannette Noltenious (National LatinoTobacco Control Network), Pebbles Fagan (TReND
Network), and Paul Goodwin (Goodwin Simon VictoriaResearch Group). This research was supported by theCalifornia Department of Health Services, Tobacco ControlProgram.
References
1. Centers for Disease Control and Prevention(CDC), State-specific smoking-attributablemortality and years of potential life lost—United States, 2000–2004. MMWR.2009;58:29–33.
2. Roeseler A, Burns D. The quarter thatchanged the world. Tob Control.2010;19(suppl 1):i3–i15.
3. Tang H, Abramsohn E, Park HY, et al.Using a cessation-related outcome index toassess California’s cessation progress at thepopulation level. Tob Control. 2010;19(suppl1):i56–i61.
4. Centers for Disease Control andPrevention, Smoking and tobacco use:2006 Surgeon’s General Report—thehealth consequences of involuntaryexposure to tobacco smoke. Available at:http://www.cdc.gov/tobacco/data_statistics/sgr/2006/. AccessedDecember 27, 2010.
5. US Census Bureau, State & countyquickfacts. Available at: http://quickfacts.census.gov/qfd/states/06000.html.Accessed May 27, 2010.
6. California Dept of Public Health, CaliforniaTobacco Control Program, CaliforniaTobacco Control Update 2009: 20 Years ofTobacco Control in California. Sacramento,Calif: California Dept of Public Health;2009.
7. Gilpin EA, White M, Farkas A, Pierce JP.Home smoking restrictions: which smokershave them and how they are associated withsmoking behavior. Nicotine Tob Res.1999;1:153–162.
8. Cook DM, Lee WL, Yang W. Factorsassociated with total restrictions onsmoking at work and at home: a studyamong populations in multiple US statesand the US Virgin Islands. Int J OccupEnviron Health. 2009;15:392–401.
9. Shavers VL, Fagan P, Alexander LA, et al.Workplace and home smoking restrictionsand racial/ethnic variation in theprevalence and intensity of currentcigarette smoking among women bypoverty status, TUS-CPS 1998–1999 and2001–2002. J Epidemiol Community Health.2006;60(suppl 2):34–43.
10. US Census Bureau, American factfinder:profile of selected housing characteristics,2000. Available at: http://factfinder.census.gov/servlet/QTTable?_bm5y&-geo_id504000US06&-qr_name5DEC_2000_SF4_U_DP4. Accessed October7, 2010.
11. Americans for Nonsmokers’ Rights,Latino/Hispanic community andsecondhand smoke. Available at: http://www.no-smoke.org/pdf/latino.pdf.Accessed December 27, 2010.
12. California Legislative Counsel Opinion,Legal Opinions: Smokefree CommonAreas: What Does the California Smoke-Free Workplace Law Require? CaliforniaLegislative Counsel Opinion, September
23, 1999. http://www.smokefreeapartments.org/general_03.html.
13. Schoenmarklin S. Legal Options forCondominium Owners Exposed to SecondhandSmoke. St. Paul, Minn: Tobacco ControlLegal Consortium; 2006.
14. Centers for Disease Control andPrevention, Disparities in secondhandsmoke exposure—United States, 1988–1994-and 1999–2004. MMWR.2008;57:744–747.
15. Al-Delaimy WD, White MM, Gilmer T, et al.The California Tobacco Control Program: CanWe Maintain the Progress? Results from theCalifornia Tobacco Survey, 1990–2005. LaJolla, Calif: University of California, SanDiego; 2008.
16. Martinez-Donate AP, Johnson-Kozlow M,Hovell MF, Gonzalez Perez GJ. Homesmoking bans and secondhand smokeexposure in Mexico and the US. Prev Med.2009;48:207–212.
17. Messer K, Mills AL, White MM, Pierce JP.The effect of smoke-free homes onsmoking behavior in the U.S. Am J PrevMed. 2008;35:210–216.
18. Center for Tobacco Policy and Organizing,American Lung Association of California,Survey of apartment owners and managers.Available at: http://www.center4tobaccopolicy.org/_files/_files/5387_CAOwnersManagersSummaryofFindings_4.pdf. Accessed May 27,2010.
19. Marın G, Marın BV. Research With HispanicPopulations. Applied Social ResearchMethods Series, Vol 23. London,United Kingdom: Sage Publications;1991.
20. Chong N, Baez F. Latino Culture: A DynamicForce in the Changing American Workplace.London, United Kingdom: InterculturalPress Inc; 2005.
21. Drope J, Bialous SA, Glantz SA. Tobaccoindustry efforts to present ventilation as analternative to smoke-free environments inNorth America. Tob Control. 2004;13(suppl1):i41–i47.
22. Hennrikus D, Pentel PR, Sandell SD.Preferences and practices among rentersregarding smoking restrictions inapartment buildings. Tob Control.3003;12:189–194.
23. Hewett MJ, Sandell SD, Anderson J,Niebuhr M. Secondhand smoke inapartment buildings: renter and owner ormanager perspectives. Nicotine Tob Res.2007;9(suppl 1):S39–S47.
24. King BA, Cummings KM, Mahoney MC, etal. Multiunit housing residents’experiences and attitudes toward smoke-free policies. Nicotine Tob Res.2010;12:598–605.
25. Drach LL, Pizacani BA, Rohde KL,Schubert S. The acceptability ofcomprehensive smoke-free policies to low-income tenants in subsidized housing. PrevChronic Dis. 2010;7:A66.
26. King BA, Travers MJ, Cummings KM, et al.Prevalence and predictors of smoke-freepolicy implementation and support amongowners and managers of multiunit housing.Nicotine Tob Res. 2010;12:159–163.
SO WHAT? Implications for HealthPromotion Practitioners andResearchersWhat is already known on this topic?Many Hispanic/Latino residents ofmultiunit housing in California arepotentially exposed to secondhandsmoke from neighboring apart-ments.What does this article add?Secondhand smoke exposure isprevalent among Hispanic/Latinosin multiunit housing. There is highsupport for policies to reduce sec-ondhand smoke exposure, but cer-tain traditional cultural values maderesidents hesitant to ask their neigh-bors not to smoke. Apartment own-ers and managers were also con-cerned about negative consequencesof implementing policies. The RegaleSalud intervention prompted thepassage of several anti-smoking pol-icies in housing units.What are the implications for healthpromotion practice or research?Municipalities should pass ordi-nances to prohibit smoking in mul-tiunit housing and common areas.In the meantime, it is important tocontinue to educate landlords andmanagers about secondhand smokeand encourage them to implementvoluntary policies. This could re-duce health disparities in second-hand smoke exposure among His-panic/Latinos.
S90 American Journal of Health Promotion May/June 2011, Vol. 25, No. 5 Supplement

Editor in ChiefMichael P. O’Donnell, PhD, MBA, MPH
Associate Editors in ChiefMargaret Schneider, PhDJennie Jacobs Kronenfeld, PhDShirley A. Musich, PhDKerry J. Redican, MPH, PhD, CHESSECTION EDITORSInterventionsFitness
Barry A. Franklin, PhDMedical Self-Care
Lucy N. Marion, PhD, RNNutrition
Karen Glanz, PhD, MPHSmoking Control
Michael P. Eriksen, ScDWeight Control
Kelly D. Brownell, PhDStress Management
Cary Cooper, CBEMind-Body Health
Kenneth R. Pelletier, PhD, MD (hc)Social Health
Kenneth R. McLeroy, PhDSpiritual Health
Larry S. Chapman, MPH
StrategiesBehavior Change
James F. Prochaska, PhDCulture Change
Daniel Stokols, PhDPopulation Health
David R. Anderson, PhD, LP
ApplicationsUnderserved Populations
Antronette K. (Toni) Yancey, MD, MPHHealth Promoting Community Design
Bradley J. Cardinal, PhDThe Art of Health Promotion
Larry S. Chapman, MPH
ResearchDatabase
Leslie Spenser, PhDFinancial Analysis
Ron Z. Goetzel, PhDMeasurement Issues
Shawna L. Mercer, MSc, PhD
The Wisdom of Practiceand the Rigor of Research
“ The American Journal of Health Promotion provides a forum for that rare commodity— practical and intellectual exchange between researchers and practitioners. ”
Kenneth E. Warner, PhDDean and Avedis Donabedian Distinguished University Professor of Public HealthSchool of Public Health, University of Michigan
“ The contents of the American Journal of Health Promotion are timely, relevant, andmost important, written and reviewed by the most respected researchers in our field. ”
David R. Anderson, PhD, LPSenior Vice President & Chief Health Officer, StayWell Health Management
Subscribe today...ANNUAL SUBSCRIPTION RATES: (Available 1/1/11. Good through 12/31/11)
INDIVIDUAL INSTITUTIONPrint + Online Print Online Print + Online
U.S. $139 $184 $359 $359
Canada and Mexico $148 $193 $359 $368
Other Countries $157 $202 $359 $377
Call 800-783-9913 (U.S. only) or 818-760-8520
Definition of Health Promotion“Health Promotion is the art and science of helpingpeople discover the synergies between their corepassions and optimal health, enhancing their motivationto strive for optimal health, and supporting them inchanging their lifestyle to move toward a state of optimalhealth. Optimal health is a dynamic balance of physical,emotional, social, spiritual, and intellectual health.Lifestyle change can be facilitated through acombination of learning experiences that enhanceawareness, increase motivation, and build skills and, mostimportant, through the creation of opportunities that openaccess to environments that make positive health practicesthe easiest choice.”
(O’Donnell, American Journal of Health Promotion, 2009, 24,1,iv)
DIMENSIONS OFOPTIMAL HEALTH
fOnline
subscriptionsnow available
Check out our new online format:http://www.HealthPromotionJournal.com/online.htm
ADfpSUB_2011:ADfp 9/17/10 8:40 AM Page 1
Related Documents