TO TREAT OR NOT TO TREAT THAT IS THE QUESTION Dr. Ruth Kandel Director, Infection Control Hebrew SeniorLife

TO TREAT OR NOT TO TREAT THAT IS THE QUESTION Dr. Ruth Kandel Director, Infection Control Hebrew SeniorLife.
Dec 22, 2015
Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript
TO TREAT OR NOT TO TREATTHAT IS THE QUESTION
Dr. Ruth KandelDirector, Infection Control
Hebrew SeniorLife
Objectives
• Define whether to screen for or treat asymptomatic bacteriuria in an elderly population
• Review complications of antibiotic use • Define symptomatic urinary tract infections• Review challenges of diagnosis in the elderly
2

Clinical Infectious Disease 2005;40:643-654
3

What is Asymptomatic Bacteriuria?

Asymptomatic Bacteriuria (ASB)
5

Pyuria
• Pyuria (> 10 WBC / high-power field) is evidence of inflammation in the genitourinary tract
• Pyuria is commonly found with ASB• Elderly institutionalized residents 90% (Infect Dis Clin North Am 1997;11:647-62)
• Short-term (< 30 days) catheters 30-75% (Arch IM 2000;160:673-82)
• Long-term catheters 50-100% (Am J Infect Control 1985;13:154-60)
6

Treatment for ASB Indicated
• Pregnant women– Increased risk for adverse outcomes
• Urologic interventions• TURP• Any urologic procedure with potential mucosal
bleeding
7

Treatment for ASB Not Indicated
8

Prevalence of ASB
9

No Benefit Treating ASB in the Elderly
10

Prospective Randomized StudiesTreatment vs. No Treatment ASB
Authors Subjects Intervention Outcome
Nicolle LE, et al. NEJM 1983;309:1420-5
Men, NH, median age 80
Treated 16Not treated 20Duration 2 years
No difference mortality or infectious morbidity 2 groups
Nicolle LE, et al. Am J Med 1987;83:27-33
Women, NH, median age 83
Treated 26Not treated 24Duration 1 year
No difference mortality/GU morbidity. Increase drug reactions and AB resistance treated group.
Abrutyn E, et al.Ann Intern Med1994;120:827-33
Women, ambulatory and NHMean age 82
Treated 192Not treated 166Duration 8 years
No survival benefit from treatment
Ouslander JGAnn Intern Med1995;122:749-54
Women and menNHMean age 85
Treated 33Not treated 38Duration 4 weeks
No difference chronic urinary incontinence
11

Cohort Studies
Authors Subjects Observation Outcome
JAGS 1990;38:1209-14
Men, Ambulatory, > 65 years
29 Subjects
Duration 1-4.5 years
No adverse outcomes attributed to no treatment
NEJM 1986;314:1152-6
Population based Swedish men and women
Duration 5 years No association between bacteriuria and survival
Gerontology1986;32:167-71
Population based Finnish men and women > 85 years
Duration 5 years No association between bacteriuria and survival
12

Proportion of Women with Diabetes Who Remained Free of Symptomatic Urinary Tract Infection, According to Whether They Received Antimicrobial Therapy or Placebo at Enrollment.
Harding GK et al. N Engl J Med 2002;347:1576-1583.
13

IDSA Recommendations
14

Any Problems
Just Treating Anyway?

16

CDC Website17

Antibiotic misuse adversely impacts
patients - resistance• Getting an antibiotic increases a
patient’s chance of becoming colonized or infected with a resistant organism.

Antibiotic Resistance
19

Antibiotic Resistance
20

Antibiotic resistance increases mortality

Mortality associated with carbapenem resistant (CR) vs susceptible (CS)
Klebsiella pneumoniae (KP)
0
10
20
30
40
50
60
Overall Mortality Attributable Mortality
Pe
rce
nt o
f s
ub
jec
ts
CRKP
CSKP
Patel G et al. Infect Control Hosp Epidemiol 2008;29:1099-1106
OR 3.71 (1.97-7.01)
OR 4.5 (2.16-9.35)
p<0.001
p<0.001

Mortality of resistant (MRSA) vs. susceptible
(MSSA) S. aureus• Mortality risk associated with MRSA
bacteremia, relative to MSSA bacteremia: OR: 1.93; p < 0.001.1
• Mortality of MRSA infections was higher than MSSA: relative risk [RR]: 1.7; 95% confidence interval: 1.3–2.4).2
1. Clin. Infect. Dis.36(1),53–59 (2003). 2. Infect. Control Hosp. Epidemiol.28(3),273–279 (2007).

CDC: Get Smart About Antibiotics
24

CDC: Get Smart About Antibiotics
• Antibiotic resistance is one of the world’s most pressing public threats.
• Antibiotic resistance in long-term care increases risk– Hospitalization– Death– Cost of treatments
25

Antibiotic misuse adversely impacts
patients- resistance• Increasing use of antibiotics
increases the prevalence of resistant bacteria in hospitals.

Reservoir for Spread of Antibiotic Resistant Pathogens
Clinical Infections
Colonized (asymptomatic)
Patients
27

Antibiotic Resistant Bacteria Travels‐
Journal of the American Geriatrics Societypages 242-246, 12 JUL 2002 http://onlinelibrary.wiley.com/doi/10.1046/j.1532-5415.50.7s.5.x/full#f1
28

And Another Reason Not To Treat

Clostridium Difficile Infection
30
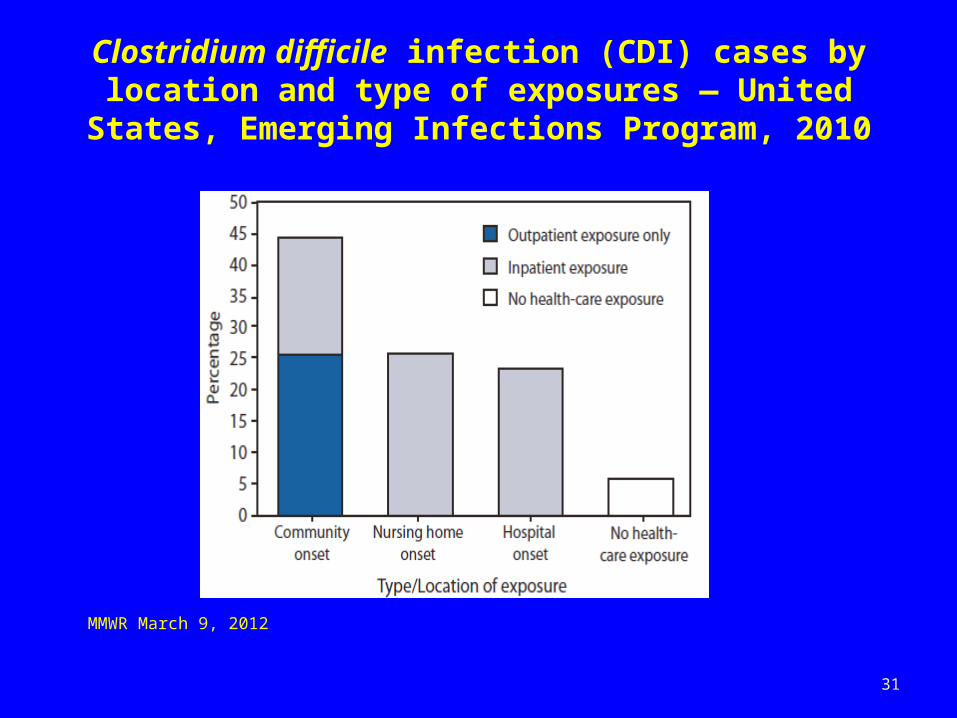
Clostridium difficile infection (CDI) cases by location and type of exposures — United States, Emerging Infections Program, 2010
MMWR March 9, 2012
31
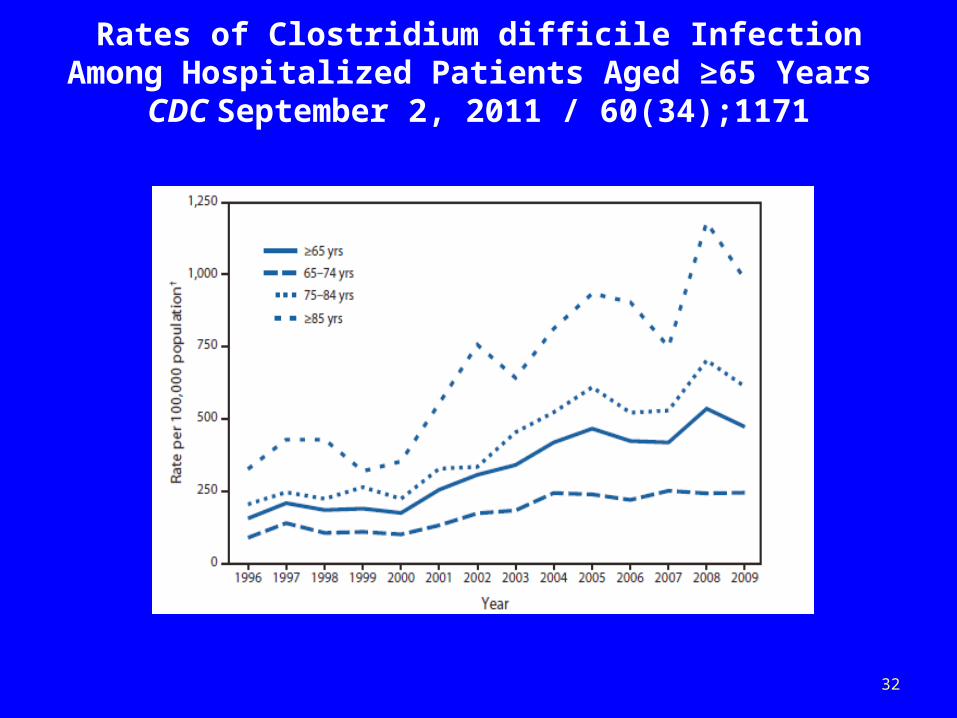
Rates of Clostridium difficile Infection Among Hospitalized Patients Aged ≥65 Years
CDC September 2, 2011 / 60(34);1171
32

Heron et al. Natl Vital Stat Rep 2009;57(14). http://www.cdc.gov/nchs/data/nvsr/nvsr57/nvsr57_14.pdf
Background: ImpactAge-Adjusted Death Rate* for
Enterocolitis Due to C. difficile, 1999–2006
*Per 100,000 US standard population
0
0.5
1.0
1.5
2.0
2.5
1999 2003
Rate
2000 20042001 20052002 2006Year
MaleFemaleWhiteBlackEntire US population
33

Deaths from Gastroenteritis DoubleC. difficile and norovirus are the leading causes
34

Background: Epidemiology
Risk Factors
• Antimicrobial exposure• Acquisition of C. difficile • Advanced age• Underlying illness• Immunosuppression• Tube feeds• Gastric acid suppression FDA Drug Safety Communication:
Clostridium difficile infection can be associated with stomach acid drugs known as proton pump inhibitors (PPIs) February 2012
Main modifiable risk factors
35

When to TreatUrinary Tract Infections
Long Term Care

Challenges
• Comorbid illnesses may result in symptoms similar to UTIs.
• Cognitive impairment may make reporting of symptoms difficult.
• Older individuals can have atypical presentations for infections.
• There is a lack of evidenced based guidelines for symptomatic UTIs.
37
Criteria for Surveillance, Diagnosis and Treatment
• Based on consensus group recommendations
• Modified by – Recent clinical practice guidelines– Current research
38

Criteria for Surveillance, Diagnosis and Treatment
39

McGeer CriteriaNo Indwelling Catheter
• At least three of the following– Fever* or chills– New or increased dysuria,
frequency or urgency– New flank or suprapubic pain
or tenderness– Change in character of urine– Worsening of mental or
functional status
Chronic Indwelling Catheter
• At least two of the following– Fever* or chills– New flank or suprapubic pain
or tenderness– Change in character of urine– Worsening of mental or
functional status
*Fever > 100.4° F
Am J Infect Control 1991;19:1-7
40

Loeb Minimal CriteriaInitiating Antibiotics
No Indwelling Catheter• Acute dysuria Or• Fever* + new or worsening
(must have at least one of following)– Urgency– Frequency– Suprapubic pain– Gross hematuria– Costovertebral angle
tenderness– Urinary incontinence
Chronic Indwelling CatheterMust have at least one of the
following• Fever*• New costovertebral angle
tenderness• Rigors (shaking chills)• New onset delirium
*Fever > 100° or 2.4° F above baselineICHE 2001;22:120-124
41

Criteria for Surveillance, Diagnosis and Treatment
Clinical Practice Guidelines• Infectious Disease Society of America (IDSA)
Clinical Practice Guidelines Fever and Infection Long-Term Care Facilities 2008 CID 2009;48:149-171
• IDSA Clinical Practice Guidelines Catheter-Associated Urinary Tract Infections Adults 2009 CID 2010;50:625-663
• IDSA Guidelines Asymptomatic Bacteriuria CID 2005;40:643-654
42

Criteria for Surveillance, Diagnosis and Treatment Current Research
Diagnostic algorithm for ordering urine cultures for NH residents in intervention arm
Loeb M et al. BMJ 2005;331:669
©2005 by British Medical Journal Publishing Group43

Treatment algorithm for prescribing antimicrobials to NH residents in intervention arm
Loeb M et al. BMJ 2005;331:669
©2005 by British Medical Journal Publishing Group44

Monthly rates of antimicrobial prescriptions for urinary indications in intervention and usual care nursing homes.
Loeb M et al. BMJ 2005;331:669
©2005 by British Medical Journal Publishing Group45
Collecting Urine Samples
46

Role of Urine Analysis and Dipstick Testing in the Evaluation of Urinary Tract Infection in Nursing Home Residents
47

Urine Culture
• A urine culture should always be obtained when evaluating SYMPTOMATIC infections.
• Urine cultures will assist in appropriate antibiotic selection.
• A negative urine culture obtained prior to initiation of antibiotics excludes routine bacterial urinary infection
48

At least one of the following that are new or increased □ Fever (> 100°F or 2.4°F > baseline)
□ Costovertebral angle tenderness
□ Rigors (shaking chills)
□ Delirium □ Flank pain* or pelvic discomfort* □ Acute hematuria* □ Malaise or lethargy with no other cause**CID 2010;50:625-663
Acute dysuria alone ORFever (> 100°F or 2.4°F > baseline) AND at least one of the following that is new or increased
□ Urgency Frequency□ □ Suprapubic pain □ Gross hematuria □ Costovertebral angle tenderness □ Urinary incontinence □ Change in mental status* □ Rigors (shaking chills)*
If accompanied only by fever, rule out other causes *CID 2012;54:973-978 BMJ 2005;331:669
49

Key Points• Routine screening for and treatment of ASB is not
recommended – In older individuals in the community– In elderly residents in LTCFs
• Get Smart About Antibiotics– Antibiotic resistance is one of the world’s most pressing public
threats.– Clostridium difficile infections are on the rise and are associated
with increased mortality especially among the elderly• Treat only symptomatic urinary tract infections in the
elderly– Refer to clinical guidelines to assist in making a diagnosis
50
Related Documents