UNIVERSITY OF GLASGOW Orthodontics, TMD & TMJ Ankylosis Personal notes Mohammed Almuzian ……… …..

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript
UNIVERSITY OF GLASGOW
Orthodontics, TMD & TMJ Ankylosis
Personal notes
Mohammed Almuzian
………
…..

Contents
Introduction................................................................................................1
Anatomy of TMJ........................................................................................2
Physiology of the TMJ's.............................................................................4
Disorders of the TMJ's...............................................................................5
Temporomandibular Dysfunction (TMD)..................................................7
Aetiology....................................................................................................7
Incidence of TMD......................................................................................8
Measurement of TMD................................................................................9
Examination of TMD.................................................................................9
Evidences of the Relationship between TMD, Orthodontics, occlusal
interferences & malocclusion...................................................................10
Problems with TMJ research....................................................................13
Orthodontist’s role in the management of TMD......................................13
BOS guidelines for management of TMD...............................................16
What are the main treatments available for TMD?..................................16
Limited mouth opening (Trismus)...........................................................22
Presentation of Ankylosis.........................................................................22
Diagnosis of for ankylosed TMJ..............................................................23
Mohammed Almuzian, University of Glasgow, 2013 1
Treatment Choices....................................................................................23
Surgical Approach and preparation..........................................................25
Complications...........................................................................................25
Mohammed Almuzian, University of Glasgow, 2013 2
Orthodontics, TMD & TMJ Ankylosis
Introduction
Interest was aroused in 1987 following litigation in America; the case
was that of Brimm vs. Malloy and is described in more detail, by an
attorney in: Pollack B. Cases of note: Michigan jury awards $850,000 on
orthodontic case: a tempest in a teapot. (Am J Orthod Dentofacial Orthop
1988; 94: 358-60). A patient developed symptoms of a
temporomandibular disorder (TMD) during orthodontic treatment and the
case went against the orthodontist, resulting in almost a million dollars
being paid out.
At the BOS Spring Meeting in 1997, the well-known American academic
Lysle Johnston explained that originally the claim was that the patient
had not received appropriate management when TMD symptoms had first
started in treatment and that there had been inadequate pre-treatment
documentation of the patient's TMD status. Ultimately however, the
orthodontic treatment itself was blamed for causing the patient's TMD.
One of the main reasons for this was the lack of evidence to suggest that
orthodontics had not caused the problem (Giannelly, 1989).
This was confirmed by Reynders (1990) who reviewed relevant studies
spanning the period 1966 - 1988 and found that of 91 relevant papers, 55
were view point articles, 30 were case reports but only 6 were sample
studies. Worse still, half of the case reports were written by one author
and these were published in one journal - of which that author was the
editor.
Mohammed Almuzian, University of Glasgow, 2013 3

It is better to start with some introduction before going ahead and
discuss this topic in details.
Anatomy of TMJ
The TMJs are the only freely movable (synovial) articulations in the skull
apart from the joints between the ossicles of the middle ear.
The TMJ consists of:
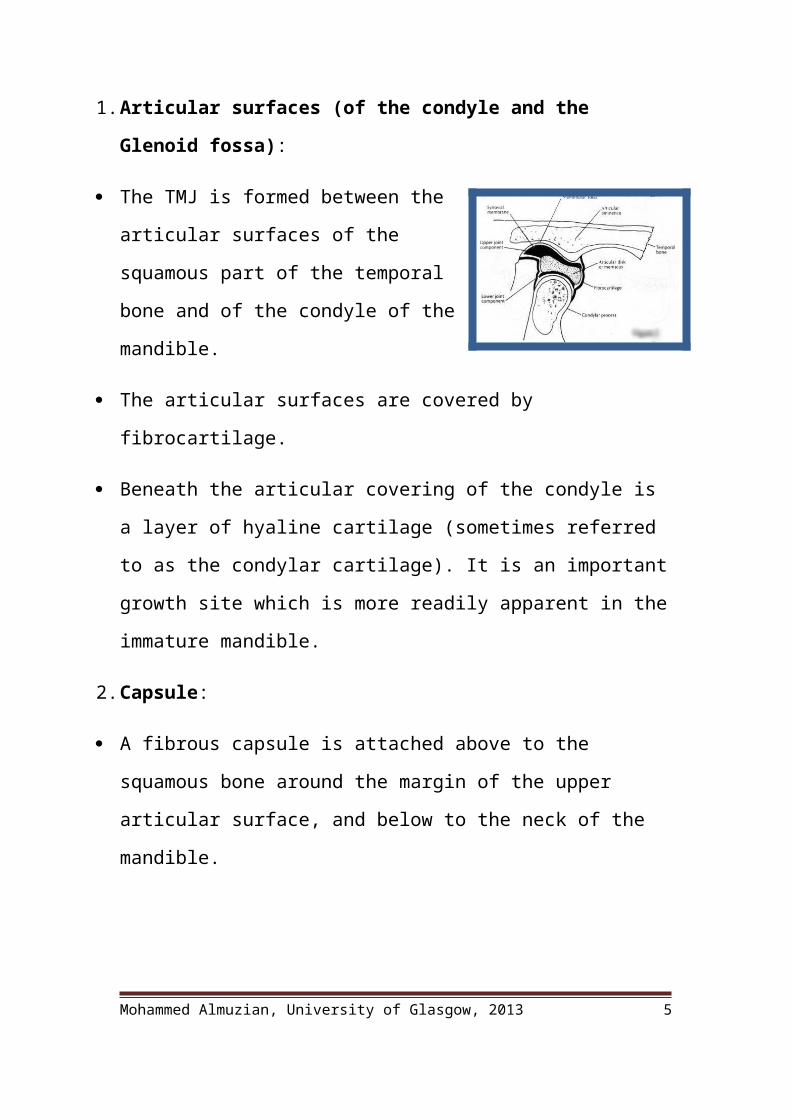
1. Articular surfaces (of the condyle and the Glenoid fossa):
The TMJ is formed between the articular
surfaces of the squamous part of the temporal
bone and of the condyle of the mandible.
The articular surfaces are covered by
fibrocartilage.
Beneath the articular covering of the condyle is a layer of hyaline
cartilage (sometimes referred to as the condylar cartilage). It is an
important growth site which is more readily apparent in the immature
mandible.
2. Capsule:
A fibrous capsule is attached above to the squamous bone around the
margin of the upper articular surface, and below to the neck of the
mandible.
The capsule is slack between the articular disc and the squamous bone but
much tighter between the disc and the neck of the mandible.
Mohammed Almuzian, University of Glasgow, 2013 4
The lateral pterygoid muscle is inserted, in part, into the anterior surface
of the capsule.
3. Articular disc:
It is a plate of fibrocartilage which in the majority of cases completely
divides the joint cavity into upper and lower compartment.
Laterally and medially the disc blends with the capsule of the joint.
In front, it is attached to the capsule and the lateral pterygoid muscle.
Posteriorly the disc is divided into two layers. The upper layer is attached
to the anterior margin of the squamotympanic fissure while the lower
layer is attached to the posterior surface of the neck of the mandible.
The upper surface of the disc is slightly concave anteriorly and markedly
convex posteriorly. The under surface is concave over its whole extent.
The disc is not uniform thickness. The central part is the thinnest and is
relatively avascular
4. Ligaments:
The capsule is strengthened laterally by a thick band of fibrous tissues,
the lateral temporomandibular ligament.
The sphenomandibular and stylomandibular ligament are described as
accessory ligaments of the TMJ.
5. Synovial membrane:
The internal aspect of the capsule, the non-articular surfaces of the
mandibular neck and to a variable extent, the peripheral areas of the
Mohammed Almuzian, University of Glasgow, 2013 5
articular disc is covered with a layer of the synovial membrane which
provide nourishment for the joint structures.
6. Nerve and Blood supply:
The deep temporal and masseteric branches of the maxillary artery and
the branches of the superficial temporal artery, which arise from the
external carotid artery, supply the TMJ.
Venous drainage is via the superficial temporal, maxillary, and pterygoid
plexus of veins.
The capsule of the TMJ is innervated from a large branch of the
auriculotemporal nerve. The anterior region of the joint is innervated
from the masseteric nerve and from the posterior deep temporal nerve.
The articular cartilage and the central part of the disk contain no nerves
Physiology of the TMJ's
There are two basic movements of the TMJ's:
Hinge movement occurs in the first stages of opening. Here the condylar
head remains in the glenoid fossa.
Translation occurs as the condylar head moves down the articular
eminence. It relies on coordinated movement between the condyle and
the disc. In some TMJ conditions the disc and condyle do not move
together for example in anterior disc displacement
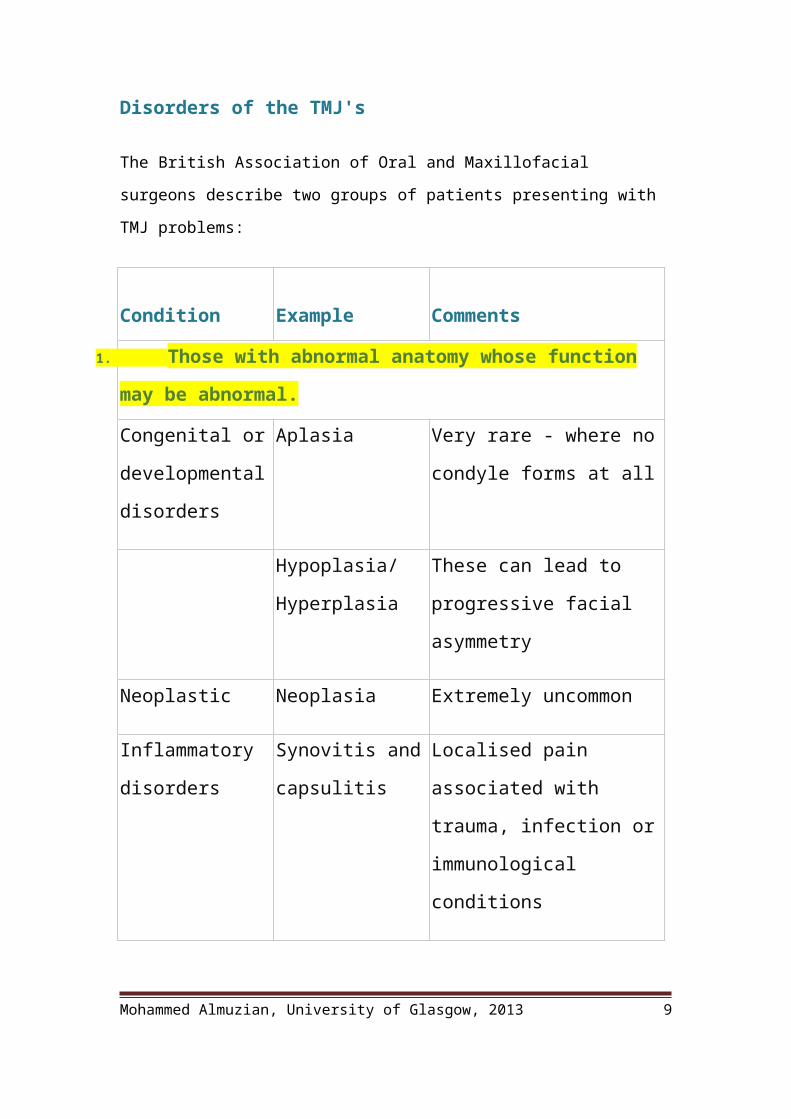
Disorders of the TMJ's
The British Association of Oral and Maxillofacial surgeons describe two groups of
patients presenting with TMJ problems:
Mohammed Almuzian, University of Glasgow, 2013 6
Condition Example Comments
Those with abnormal anatomy whose function may be
abnormal.
Congenital or
developmental
disorders
Aplasia Very rare - where no condyle
forms at all
Hypoplasia/
Hyperplasia
These can lead to progressive
facial asymmetry
Neoplastic Neoplasia Extremely uncommon
Inflammatory
disorders
Synovitis and
capsulitis
Localised pain associated with
trauma, infection or
immunological conditions
Rheumatoid
arthritis and other
auto immune
diseases
Systemic conditions affecting
the TMJ's
Degenerative or
Age related
problems
Osteoarthritis Degenerative joint disease,
leads to abrasion of the joint
surfaces and remodeling.
Characterised by crepitation.
Traumatic Ankylosis Long term sequela of trauma
Fracture Caused by trauma
Mohammed Almuzian, University of Glasgow, 2013 7
TMJ dislocation:
Acute or chronic.
The chronic type is associated
in most of the cases with some
degenerative disorders acute
dislocation occurs when the
patient is hit with the mouth
open
Those with normal anatomy but abnormal function
Dysfunctional Disc displacement
with reduction
Where the disc clicks back
into place part way through
translation
Disc displacement
without reduction
Where the disc remains
permanently displaced
anteriorly
Temporomandibula
r Dysfunction
(TMD).
See below
Mohammed Almuzian, University of Glasgow, 2013 8
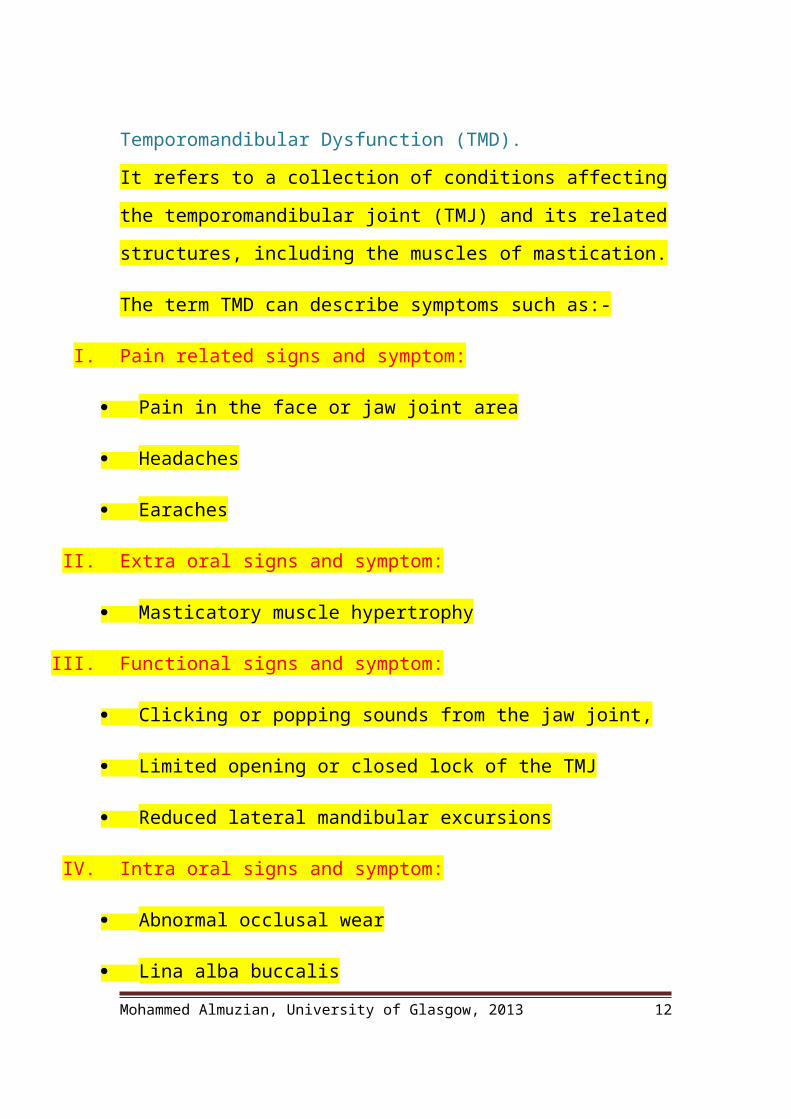
Temporomandibular Dysfunction (TMD).
It refers to a collection of conditions affecting the temporomandibular
joint (TMJ) and its related structures, including the muscles of
mastication.
The term TMD can describe symptoms such as:-
I. Pain related signs and symptom:
Pain in the face or jaw joint area
Headaches
Earaches
II. Extra oral signs and symptom:
Masticatory muscle hypertrophy
III. Functional signs and symptom:
Clicking or popping sounds from the jaw joint,
Limited opening or closed lock of the TMJ
Reduced lateral mandibular excursions
IV. Intra oral signs and symptom:
Abnormal occlusal wear
Lina alba buccalis
Mohammed Almuzian, University of Glasgow, 2013 9

AetiologyA. Old theories regarding the aetiological factors that may cause TMD
independently
1. Factors within the central nervous system: as the emotional stresses.
2. Social conditions: an increased level of anxiety, which may lead to
increased muscle tension.
3. Occlusal interference: such as anterior open bite, crossbites, reverse
overjet, parafunctional activity…etc.
4. Trauma.
5. Internal joint pathology eg disc displacement / destruction. Proffit, 1993
6. Orthodontic treatment: such as changing the condyle position and
changing vertical face height.
7. Orthognathic surgery.
B. New philosophy: Mohlin & Thilander, 1984 described the new opinion
about the aetiology of TMD. It is Multifactorial reason:
1. Psychological
2. Dysfunctional
3. Inflammatory
4. Degenerative
5. Idiopathic
Incidence of TMD
A. Proffit (2002) suggests levels of between 5-30% depending on the
symptoms examined for TMD.(this variation because the studies have no
standardization in their method of assessment)
Mohammed Almuzian, University of Glasgow, 2013 10

B. It has also be noted that TMD increases with age, Egermark-Ericson et al
(1983) suggesting an increase in the prevalence of symptoms from 30%
to 60% (two times) between the age of 20 and 45 years.
C. Females have higher prevalence due to (Warren and Fried, 2001):
Physiological differences
Anatomical differences
Behavioural differences
Genetic differences.
Measurement of TMD
Studies investigating TMD have used indices:
1. Helkimo Clinical Dysfunction Index. (HCDI) The following are
scored:
TMJ sounds,
Symptoms of reduced movement capacity
Locking or luxation of the mandible,
Deviation on opening,
Pain on movement,
Muscle and TMJ tenderness.
Each symptom is judged according to a three grade scale. Problems with
the use of this index are described (Van der Weele and Dibbets 1987)
including insufficient evidence to support or to document the validity of
this index. This index contains useful elements and should be adapted
rather than replaced to improve its' validity
Mohammed Almuzian, University of Glasgow, 2013 11
2. Craniomandibular index CMI (Fricton and Schiffman, 1987)
Index has had little use in the orthodontic literature but it addresses the
problems of validity and reproducibility associated with Helkimo Index.
Examination of TMD
History:
Before any clinical examination, the patient should be asked about
symptoms such as pain, clicking, crepitus or locking of the jaw.
Ask the patient about any previous treatment that he/she had for the
TMJ such as medications, splints, occlusal adjustments, physical therapy
or surgery.
Clinical Examination:
The joint should be palpated simultaneously by placing the middle finger
over the condylar head whilst the patient is instructed to open and close
and to move laterally. Any clicks, crepitus, and locking should be
recorded. It is probably prudent to record any negative findings as well.
The muscles of mastication should also be examined for areas of
tenderness.
Special Tests:
1. Mounted study models
2. Radiographs
3. If problems persist MRI and arthrogram may be considered
Mohammed Almuzian, University of Glasgow, 2013 12

Note: Subjects with removable dental prostheses will be examined with the
prostheses in their mouth Bite plates and other appliances that do not replace teeth are to be removed for
the examination. Vertical incisal overlap, and midline deviation, is included so corrections to
measurements of mandibular range of motion can be done to determine actual values of openings and excursions. Therefore, to determine the actual amount of opening, the amount of vertical incisor overlap should be added to the recorded opening measurements. If midline deviation is greater than 0, this measurement should be added to one side of the lateral excursion and subtracted from the other side (For example: If a subject has a 2 mm deviation to the right, then subtract 2 mm from the value given to the right lateral excursion
and add 2 mm to the value given to the left lateral excursion).
Evidences of the Relationship between TMD, Orthodontics, occlusal
interferences & malocclusion
With Against
A. Correlation between occlusal interference, malocclusion and TMD
There are weak evidences by
(Thilander et al., 2002) regarding
the association between TMD and
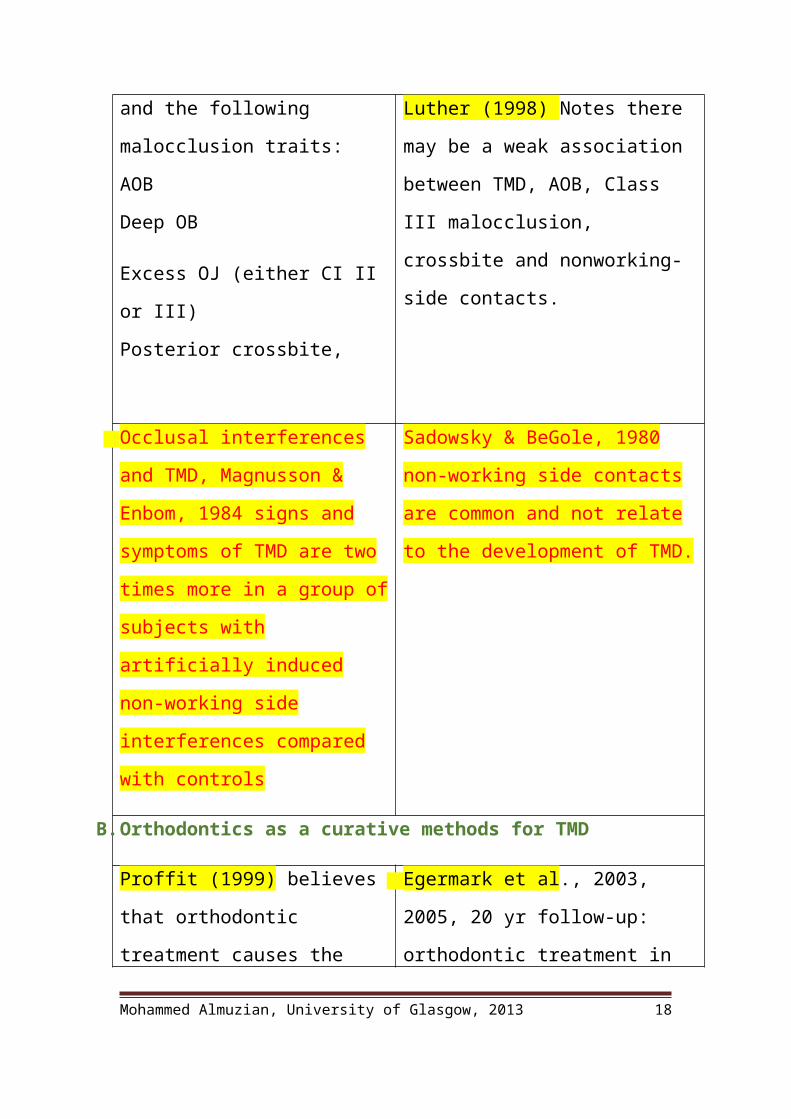
the following malocclusion traits:
AOB
Deep OB
Excess OJ (either CI II or III)
Posterior crossbite,
Proffit (2002) only 5-30% of
individuals have TMD yet 50-75% has
at least a moderate malocclusion.
Luther (1998) Notes there may be a
weak association between TMD, AOB,
Class III malocclusion, crossbite and
nonworking-side contacts.
Occlusal interferences and TMD,
Magnusson & Enbom, 1984 signs
Sadowsky & BeGole, 1980 non-
working side contacts are common and
Mohammed Almuzian, University of Glasgow, 2013 13

and symptoms of TMD are two
times more in a group of subjects
with artificially induced non-
working side interferences
compared with controls
not relate to the development of TMD.
B. Orthodontics as a curative methods for TMD
Proffit (1999) believes that
orthodontic treatment causes the
periodontal ligament to become
temporarily painful which reduces
any bruxing habits and therefore
rests the TMJs, in turn this reduces
the TMD symptoms.
TMD reduced in patients having
fixed appliances (Sadowsky and
BeGole, 1980). This reduction was
not statistically significant.
Egermark et al., 2003, 2005, 20 yr
follow-up: orthodontic treatment in
childhood does not reduce the risk of
developing TMD.
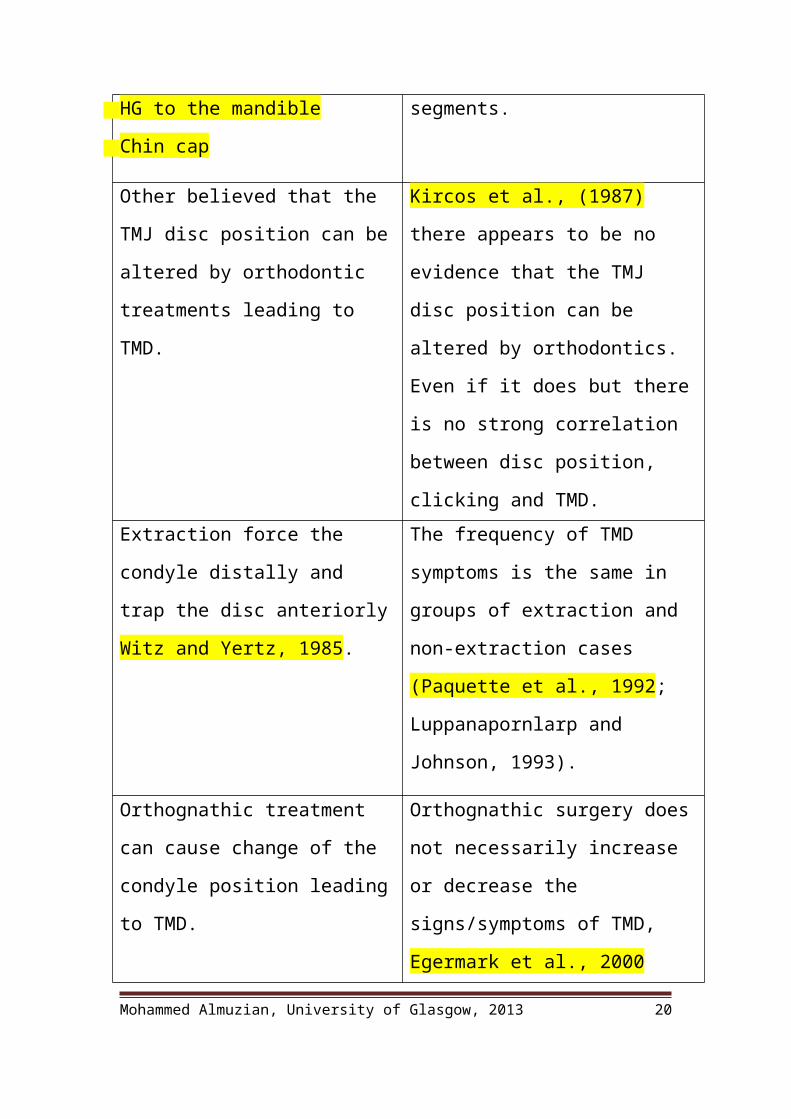
C. Orthodontics as a causative factor for TMD
Roth, 1973 thought that condylar
position can be altered with the aid
of some mechanics:
Elastics
Retraction of the ULS
HG to the maxilla
HG to the mandible
Johnston & Luecke, 1992 orthodontic
treatment does not force the condyle
distally, in fact it moves temporarily
forwards 0.7mm (in 70%), movement
due to loss of anchorage in buccal
segments.
Mohammed Almuzian, University of Glasgow, 2013 14
Chin cap
Other believed that the TMJ disc
position can be altered by
orthodontic treatments leading to
TMD.
Kircos et al., (1987) there appears to
be no evidence that the TMJ disc
position can be altered by
orthodontics. Even if it does but there
is no strong correlation between disc
position, clicking and TMD.
Extraction force the condyle distally
and trap the disc anteriorly Witz and
Yertz, 1985.
The frequency of TMD symptoms is
the same in groups of extraction and
non-extraction cases (Paquette et al.,
1992; Luppanapornlarp and Johnson,
1993).
Orthognathic treatment can cause
change of the condyle position
leading to TMD.
Orthognathic surgery does not
necessarily increase or decrease the
signs/symptoms of TMD, Egermark et
al., 2000
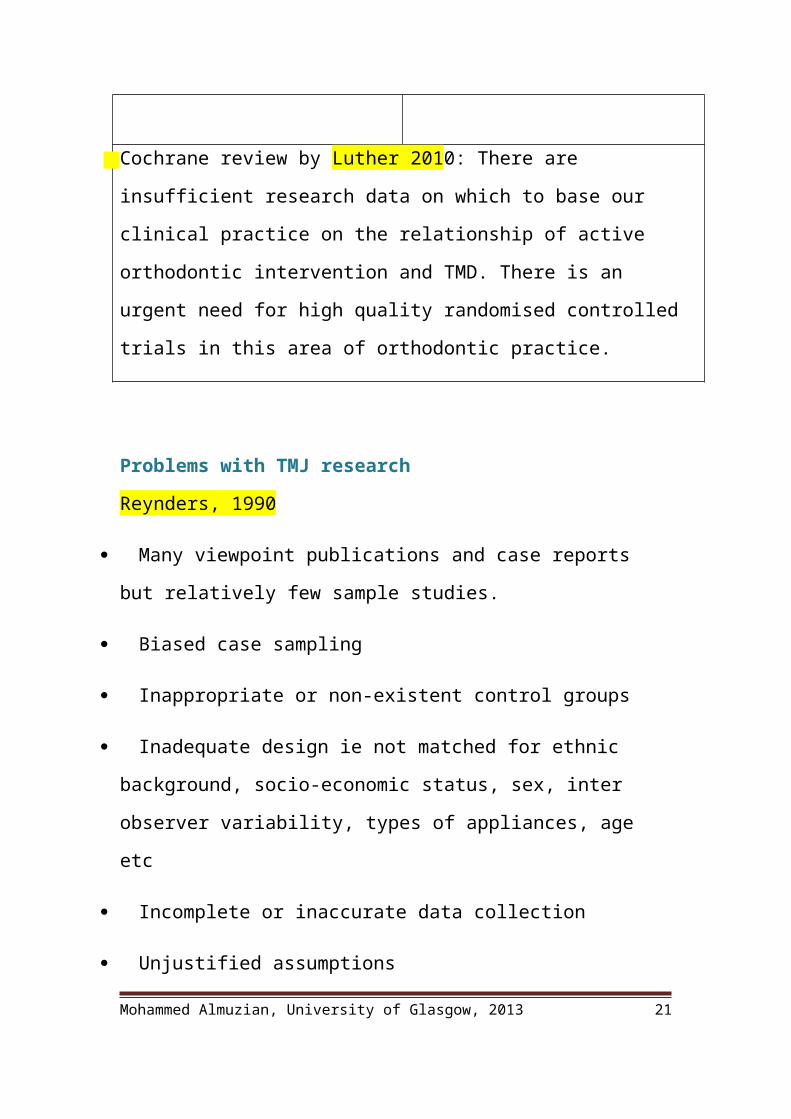
Cochrane review by Luther 2010: There are insufficient research data on
which to base our clinical practice on the relationship of active orthodontic
intervention and TMD. There is an urgent need for high quality randomised
controlled trials in this area of orthodontic practice.
Problems with TMJ research
Reynders, 1990
Many viewpoint publications and case reports but relatively few
sample studies.Mohammed Almuzian, University of Glasgow, 2013 15

Biased case sampling
Inappropriate or non-existent control groups
Inadequate design ie not matched for ethnic background, socio-
economic status, sex, inter observer variability, types of appliances, age
etc
Incomplete or inaccurate data collection
Unjustified assumptions
Faulty interpretation
Orthodontist’s role in the management of TMD
Also the evidence seems to suggest that orthodontics has no effect on
TMJ, but TMD could be present or appear during treatment, therefore
certain protocols should be followed.
Pre-treatment. 1. Full history.
2. Any signs or symptoms of TMD should be noted
3. If the patient already has a TMD, then the patient
informed that orthodontic treatment has no
influences according to the evidence based
literatures.
4. If the condition is sever and acute it is better not
to commence orthodontic treatment until the
Mohammed Almuzian, University of Glasgow, 2013 16

condition is stabilized by a specialist.
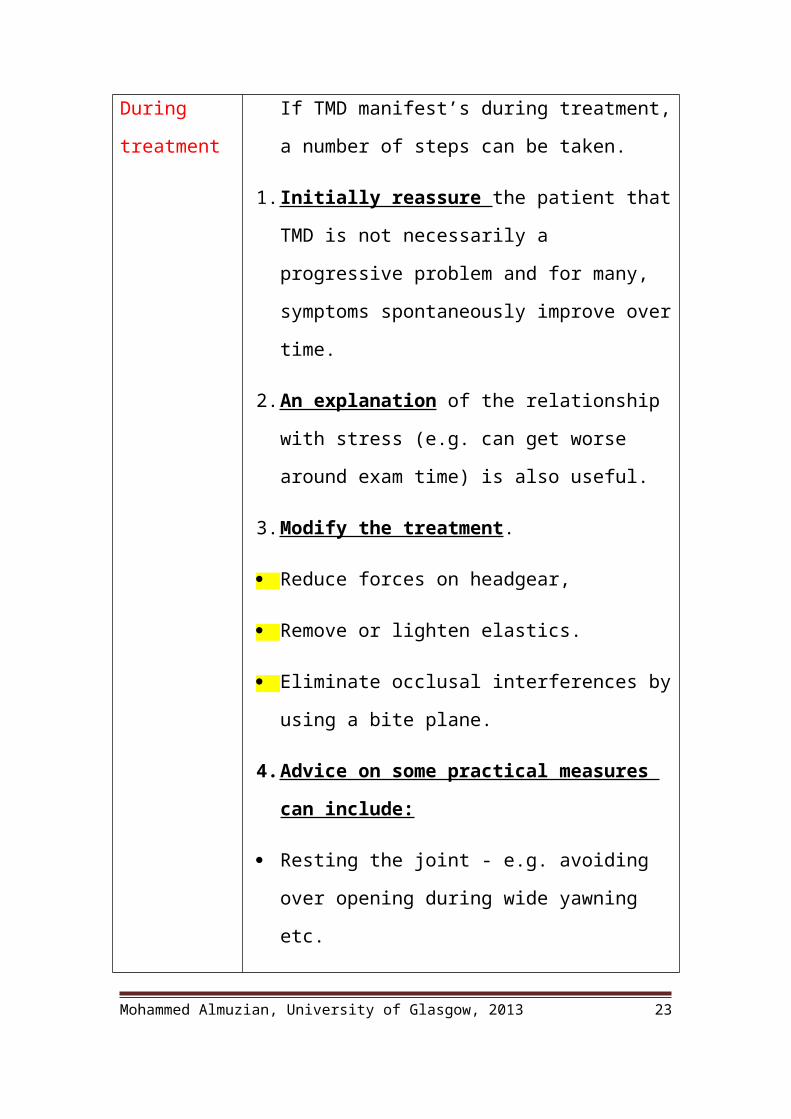
During
treatment
If TMD manifest’s during treatment, a number of
steps can be taken.
1. Initially reassure the patient that TMD is not
necessarily a progressive problem and for many,
symptoms spontaneously improve over time.
2. An explanation of the relationship with stress (e.g.
can get worse around exam time) is also useful.
3. Modify the treatment .
Reduce forces on headgear,
Remove or lighten elastics.
Eliminate occlusal interferences by using a bite
plane.
4. Advice on some practical measures can include:
Resting the joint - e.g. avoiding over opening during
wide yawning etc.
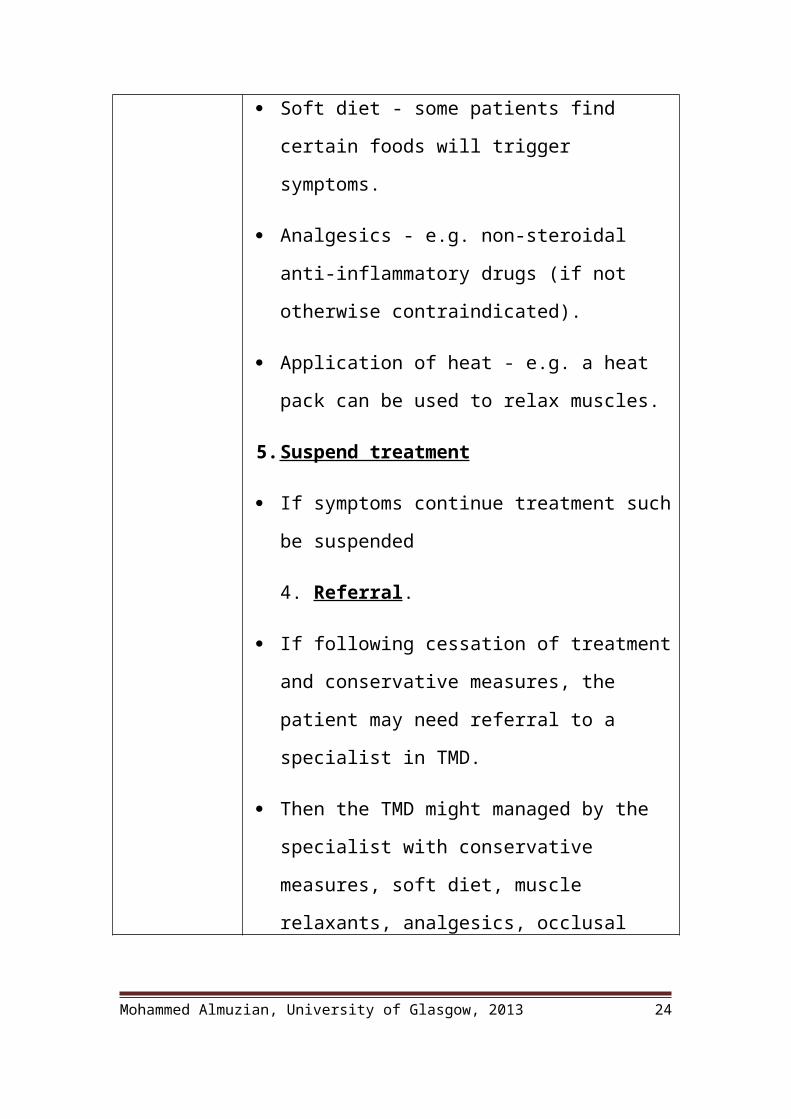
Soft diet - some patients find certain foods will
trigger symptoms.
Analgesics - e.g. non-steroidal anti-inflammatory
drugs (if not otherwise contraindicated).
Application of heat - e.g. a heat pack can be used to
relax muscles.
Mohammed Almuzian, University of Glasgow, 2013 17
5. Suspend treatment
If symptoms continue treatment such be suspended
4. Referral.
If following cessation of treatment and conservative
measures, the patient may need referral to a
specialist in TMD.
Then the TMD might managed by the specialist
with conservative measures, soft diet, muscle
relaxants, analgesics, occlusal splint or surgery.
Post treatment The patient should be monitored through out
retention for the signs and symptoms of TMD.
Mohammed Almuzian, University of Glasgow, 2013 18

BOS guidelines for management of TMD
What are the main treatments available for TMD?
Mohammed Almuzian, University of Glasgow, 2013 19
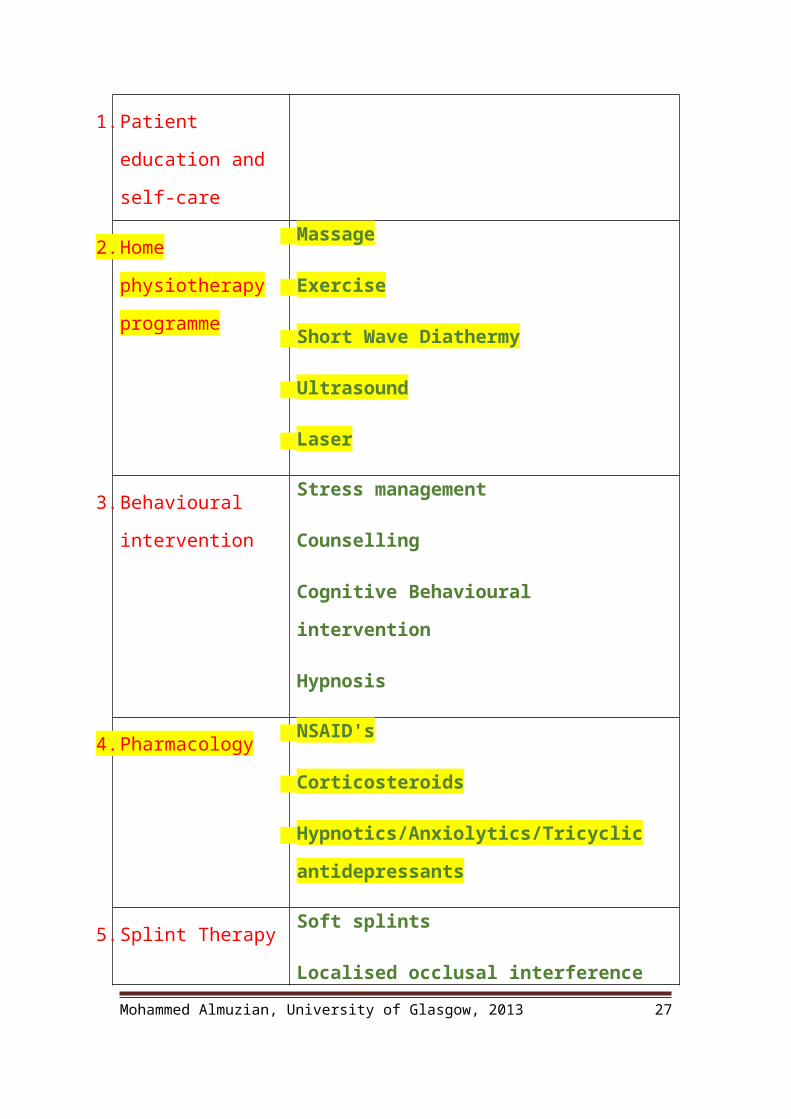
1. Patient education and
self-care
2. Home physiotherapy
programme
Massage
Exercise
Short Wave Diathermy
Ultrasound
Laser
3. Behavioural
intervention
Stress management
Counselling
Cognitive Behavioural intervention
Hypnosis
4. PharmacologyNSAID's
Corticosteroids
Hypnotics/Anxiolytics/Tricyclic
antidepressants
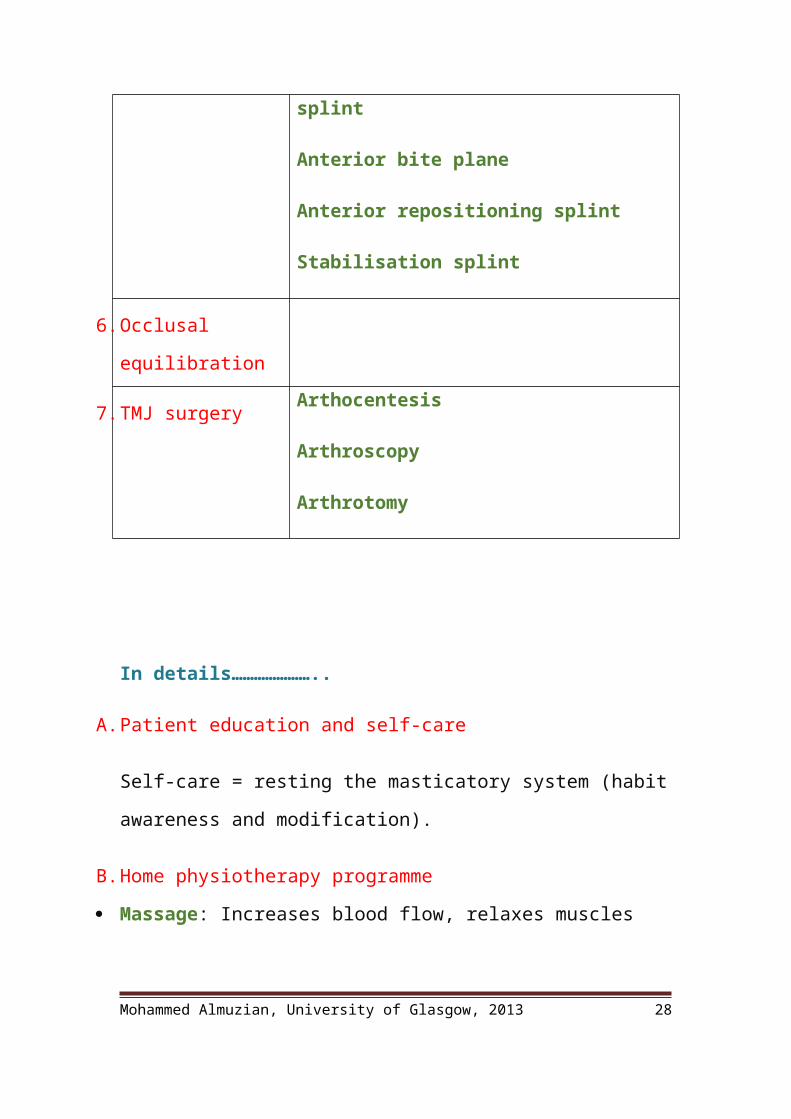
5. Splint TherapySoft splints
Localised occlusal interference splint
Anterior bite plane
Anterior repositioning splint
Stabilisation splint
Mohammed Almuzian, University of Glasgow, 2013 20
6. Occlusal
equilibration
7. TMJ surgeryArthocentesis
Arthroscopy
Arthrotomy
In details…………………..
A. Patient education and self-care
Self-care = resting the masticatory system (habit awareness and
modification).
B. Home physiotherapy programme
Massage: Increases blood flow, relaxes muscles
Exercise: Mobilisation can be used when there is decreased range of
motion due to muscle contracture, disc displacement without reduction or
fibrous adhesions in the joint
Short Wave Diathermy: Thermal stimuli increased blood flow to
increase oxygenation and metabolite removal.
Ultrasound: The sound waves produce pressure waves in the tissue
resulting in micro massage
Mohammed Almuzian, University of Glasgow, 2013 21

Laser: Laser treatment does not increase the tissue temperature but is
thought to increase capillary permeability and stimulate fibroblast
production
C. Cognitive Behavioural intervention
Stress management
Counselling
Hypnosis
D. Pharmacology
Analgesics like (NSAID's)
Corticosteroids, these are not usually prescribed for systemic use in TMD
treatment because of their side effects. The exception is for acute
generalised muscle and joint inflammation associated with
polkyarthrides. Intracapsular steroid injections have been recommended
on a limited basis in cases of severe joint pain where conservative
treatment has been unsuccessful.
Hypnotics/Anxiolytics/Tricyclic antidepressants have been shown to be
effective for short-term management (1-2 weeks) especially for bruxism.
E. Splint Therapy
Splints are the widely used as a treatment in the UK.
Types of splints:
Soft splints
Localised occlusal interference splint
Mohammed Almuzian, University of Glasgow, 2013 22
Anterior bite plane
Anterior repositioning splint
Stabilisation splint
In details …..
1. Soft splints - these are usually made of a vacuum formed polyvinyl
material. They can be thought of as a simple emergency treatment for
patients with symptoms of TMD e.g. the student with an acute pain
around exam time. Their mode of action is unclear - they may simply be a
habit breaker but there is a risk that it can induce more parafunctional
activity.
2. Localised occlusal interference splint - this is an acrylic splint with
ball clasps that deliberately places the entire occlusal load on 4 teeth so as
to overload the proprioceptive fibres and break clenching or grinding
habits. It is meant to be worn by grinders at night or at other times when
they may parafunction e.g. whilst driving.
3. Anterior bite plane (Lucia jig). This is a deprogramming splint,
made at the chairside for emergency (short-term) treatment of patients
with acute muscle spasm and pain. The aim is to provide ideal anterior
guidance and to dis-occlude the posterior teeth.
4. Anterior repositioning splint - a hard acrylic splint fitted on the
lower teeth used to treat anterior displacement with reduction. The
mandible is postured forwards (a little like a functional appliance) which
keeps the disc in the correct position on the condylar head in order to
achieve 'click free' opening and closing. Short term these can work well
in reducing symptoms, but one questions how they can work long-term?
Mohammed Almuzian, University of Glasgow, 2013 23
5. Stabilisation splint (Tanner appliance, Fox appliance, Michigan
Splint, Centric Relation Appliance) - a hard acrylic splint constructed on
a semi adjustable articulator and ground in in the mouth. This splint is
intended to provide a temporary ideal functional occlusion. It is likely
that like all other splints it is a habit breaker. Some clinicians consider the
success of a stabilisation splint to be an indication that orthodontic
treatment or occlusal equilibration may be successful.
Cochrane review by Al Ani 2009 found no evidence regarding the
advantage of splint in treatment of TMD
F. Occlusal equilibration
It has long been recommended for the treatment of TMD
This is the is the removal of non-working side contacts by selective
grinding
Cochrane review by Koh 2009 Occlusal adjustment cannot be
recommended for the management or prevention of TMD
G. TMJ surgery
Non-invasive measures are preferred to surgery for the treatment of
TMD.
Surgery may be considered if conservative measures fail or if pathology
e.g. neoplasia is suspected.
The surgeries include: Arthocentesis, Arthroscopy and Arthrotomy
Type of
Surgery
What does it
involve?
When is it used? Is it Successful?
Mohammed Almuzian, University of Glasgow, 2013 24
Arthocentesi
s
Intra-articular
irrigation with or
without steroids.
Often used with
joint mobilisation
For intra-articular
joint restrictions
Thought to be
equally as
effective as
arthroscopy in
anterior disc
displacement
without reduction
Arthroscopy Insertion of a
camera into the
joint (usually upper
joint space). Allows
direct observation
and can then also
irrigate, debride,
incise minor
adhesions and take
biopsies.
As above Further research
needed but no
better than physio
in improving
range of
movement or
decreasing pain.
Arthrotomy Open surgical
intervention
E.g.: discoplasty,
discal repositioning,
discectomy (with or
without
replacement),
arthroplasty
(recontouring of the
Bony or fibrous
ankylosis,
neoplasia, severe
chronic
dislocations,
persistent painful
disc derangement,
severe
osteoarthritis, Less
commonly -
Variable success.
Alloplastic disc
replacements are
now
contraindicated
and it has actually
been
recommended that
all Proplast
implants are
Mohammed Almuzian, University of Glasgow, 2013 25
articular surfaces
with or without
removal of the
disc), high
condylectomy
displaced condylar
fractures
actually removed
Limited mouth opening (Trismus)
There are many causes of limited mouth opening which may be classified
as follows.
1. Intra-articular (intracapsular)
Functional: Anterior displacement of the meniscus without reduction.
Trauma: Osseous or fibro-osseous ankylosis, secondary to trauma
Inflammatory: Ankylosing spondylitis, juvenile rheumatoid arthritis.
Infection in the joint.
Tumour of the joint structures.
2. Extra-articular (extracapsular)
Muscle trismus.
Disuse muscle atrophy, contractures secondary to intra-articular
ankylosis or psychogenic trismus.
Post-radiotherapy and thermal scarring.
Post-traumatic scarring.
Mohammed Almuzian, University of Glasgow, 2013 26
Oral submucous fibrosis.
Infection or inflammation of the masticatory muscle
Anatomical like Eagle syndrome.
Presentation of Ankylosis
If developed at early age:
Ankylosis in children produces impaired mandibular growth with
bilateral deformity in all dimensions.
This deformity is asymmetrical in unilateral cases with a straight small
hemi-mandible on the ankylosed side, and a marked contralateral bowing
deformity.
Retrognathia and retrogenia become more apparent with age.
This produces an occlusal cant down to the normal side.
In rare bilateral cases the mandible is short but symmetrical.
In all cases the inter-incisal opening can be up to 10 mm even with total
bony fusion reflecting the bone elasticity within the masticatory system.
Diagnosis of for ankylosed TMJ
History and clinical examination
Imaging techniques including:
1. OPG.
2. True lateral skull.
3. PA
Mohammed Almuzian, University of Glasgow, 2013 27
4. CT scan with 3D reconstruction.
5. Standard orthognathic photographic series.
Treatment Choices
Resection of the ankylosis should be carried out as early as possible to
enable normal growth and avoid secondary deformity.
There are many treatment strategies depending on the age of the patient
the duration of the deformity and degree of secondary deformity.
A. Ankylosis presenting in childhood or Ankylosis presenting during or post
adolescence
1. Excision of the condyle
2. Insertion of an interpositional temporalis myofascial peninsular flap
3. Bilateral coronoidectomies (coronoidotomies) to free temporalis
contractures
4. Costochondral growth centre to restore function and ramus growth with
or without Distraction osteogenesis.
NB: The anteroposterior deficiency and asymmetry in childhood is
usually self-corrected with catch-up growth.
B. Ankylosis presenting after the completion of facial growth.
1. Excision of the condyle
2. Insertion of an interpositional temporalis myofascial peninsular flap
3. Bilateral coronoidectomies (coronoidotomies) to free temporalis
contractures
Mohammed Almuzian, University of Glasgow, 2013 28

4. Reconstruction of the condyle with or without distraction osteogenesis.
5. In addition to one of these:
Genioplasty
BSS or inverted L osteotomy.
The maxillary procedure can be done to correct secondary problems
C. Very late ankylosis in adults with no interference with facial growth.
Exactly as B but in addition to 7-day pre- and 2-month postoperative
course of bisphosphonate, which is currently alendronic acid 10 mg a day
in the morning to avoid the localised fibrodysplasia ossificans .
Surgical Approach and preparation
The preoperative preparation differs from the standard orthognathic
workup in several respects.
1. The anaesthetist must be skilled in fibre optic intubation and
tracheostomy or submental approach.
2. The temporal area must be shaved and cleaned before the patient is
taken into theatre.
Complications
1. Scar
2. Damage to the orbital and frontal branches of the facial nerve.
3. Frey’s syndrome
4. Damage to parotid salivary gland
Mohammed Almuzian, University of Glasgow, 2013 29
5. Limited opening due to
Inadequate bone removal
Failure to do a bilateral coronoidectomies.
Postoperative fibrodysplasia ossificans
Fusion of the graft with re-ankylosis
6. Failure of the costochondral graft to grow.
7. Excess growth of the graft
8. Pneumothorax.
Mohammed Almuzian, University of Glasgow, 2013 30
Related Documents