endodontics Editor: SAMUEL SELTZER, DDS Department of Endodontology School of Dentistry Temple University 3223 North Broad Street Philadelphia, Pennsylvania 19140 Tissue reaction to endodontic materials: Methods, criteria, assessment, and observations Elizeu Alvaro Pascon, DDS, ~IcC~D,~ Mario Roberto Leonardo, DDS,b Kamran Safavi, DMD. MEd,a and Kaare Langeland, DDS, PhD,C Farmington, Corm. SCHOOL OF DENTAL MEDICINE, UNIVERSITY OF CONNECTICUT HEALTH CENTER The purpose of this study was to develop methods and criteria for the testing of the biocompatibility of endodontic materials. One hundred twenty-one teeth from 12 baboons (Papio anubis) were used to test three sealers: AH26, Kerr pulp canal sealer, and Kloroperka N.8. Gutta-percha cones were used as solid core in all cases. Under disinfected conditions, access preparation was performed, and with working length approximately 1 .O mm short of the foramen, the instrumentation of the root canal was started, using sodium hypochlorite (1%) for irrigation. After the root canals were cleaned and shaped, they were obturated with gutta-percha cones and the sealer, and by lateral condensation technique. Histologic periapical reactions were evaluated at 1, 7, 30, 365, 730, and 1095 days. The methods and criteria used were adequate for ranking of the biocompatibility of the tested materials in the short and long periods. At short observation periods (1 to 7 days) AH26 caused severe reactions, and Kerr pulp canal sealer and Kloroperka N.0., moderate and mild reactions, respectively. At 2- and 3-year observation periods the ranking was AH26, mild; Kerr pulp canal sealer, moderate; and Kloropercha N.0.. severe. (ORAL SURC ORAL MED ORAL PATHOL 1991;72:222-37) T he periradicular tissue reaction after root canal treatment depends on the cumulative effect of all in- volved factors: the preexisting diseasele3; the elimina- tion of disintegrating pulp tissue by meticulous access preparation, debridement, and shaping of the root canal system4-6; the distance from the apical foramen Supported by National Institutes of Health grant 2 ROI DE04096/ 07A3. aAssistant Professor, Department of Restorative Dentistry and Endodontology. bVisiting Professor, Department of Restorative Dentistry and Endodontology. CProfessor Emeritus, Department of Restorative Dentistry and EndodontoIogy. 7/15/16976 222 (or foramina); and the physical adequacy and bio- compatibility of the obturation materials.7-10 Davis” was the first to point out the importance of the integrity of the apical/periapical tissues in endo- dontic therapy. Nygaard-@stby12 produced the ex- perimental evidence for Davis’ clinically based obser- vation and called attention to the need for biocom- patible endodontic materials. Valuable information may be obtained from stud- ies that involve root canal treatment failure-s,13-‘5 but they do not meet the requirements of objective non- biased testing, because the original endodontic ther- apy would not have been controlled experimentally. Therefore it is necessary to apply an animal model, step by step, imitating the actual clinical situation, to test the biocompatibility of endodontic materials.

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript
endodontics
Editor:
SAMUEL SELTZER, DDS
Department of Endodontology School of Dentistry Temple University 3223 North Broad Street Philadelphia, Pennsylvania 19140
Tissue reaction to endodontic materials: Methods, criteria, assessment, and observations Elizeu Alvaro Pascon, DDS, ~IcC~D,~ Mario Roberto Leonardo, DDS,b Kamran Safavi, DMD. MEd,a and Kaare Langeland, DDS, PhD,C Farmington, Corm.
SCHOOL OF DENTAL MEDICINE, UNIVERSITY OF CONNECTICUT HEALTH CENTER
The purpose of this study was to develop methods and criteria for the testing of the biocompatibility of endodontic materials. One hundred twenty-one teeth from 12 baboons (Papio anubis) were used to test three sealers: AH26, Kerr pulp canal sealer, and Kloroperka N.8. Gutta-percha cones were used as solid core in all cases. Under disinfected conditions, access preparation was performed, and with working length approximately 1 .O mm short of the foramen, the instrumentation of the root canal was started, using sodium hypochlorite (1%) for irrigation. After the root canals were cleaned and shaped, they were obturated with gutta-percha cones and the sealer, and by lateral condensation technique. Histologic periapical reactions were evaluated at 1, 7, 30, 365, 730, and 1095 days. The methods and criteria used were adequate for ranking of the biocompatibility of the tested materials in the short and long periods. At short observation periods (1 to 7 days) AH26 caused severe reactions, and Kerr pulp canal sealer and Kloroperka N.0., moderate and mild reactions, respectively. At 2- and 3-year observation periods the ranking was AH26, mild; Kerr pulp canal sealer, moderate; and Kloropercha N.0.. severe. (ORAL SURC ORAL MED ORAL PATHOL 1991;72:222-37)
T he periradicular tissue reaction after root canal treatment depends on the cumulative effect of all in- volved factors: the preexisting diseasele3; the elimina- tion of disintegrating pulp tissue by meticulous access preparation, debridement, and shaping of the root canal system4-6; the distance from the apical foramen
Supported by National Institutes of Health grant 2 ROI DE04096/ 07A3. aAssistant Professor, Department of Restorative Dentistry and Endodontology. bVisiting Professor, Department of Restorative Dentistry and Endodontology. CProfessor Emeritus, Department of Restorative Dentistry and EndodontoIogy. 7/15/16976
222
(or foramina); and the physical adequacy and bio- compatibility of the obturation materials.7-10
Davis” was the first to point out the importance of the integrity of the apical/periapical tissues in endo- dontic therapy. Nygaard-@stby12 produced the ex- perimental evidence for Davis’ clinically based obser- vation and called attention to the need for biocom- patible endodontic materials.
Valuable information may be obtained from stud- ies that involve root canal treatment failure-s,13-‘5 but they do not meet the requirements of objective non- biased testing, because the original endodontic ther- apy would not have been controlled experimentally. Therefore it is necessary to apply an animal model, step by step, imitating the actual clinical situation, to test the biocompatibility of endodontic materials.
Volume 72 Number 2
Apical and periapical tissue reaction 223
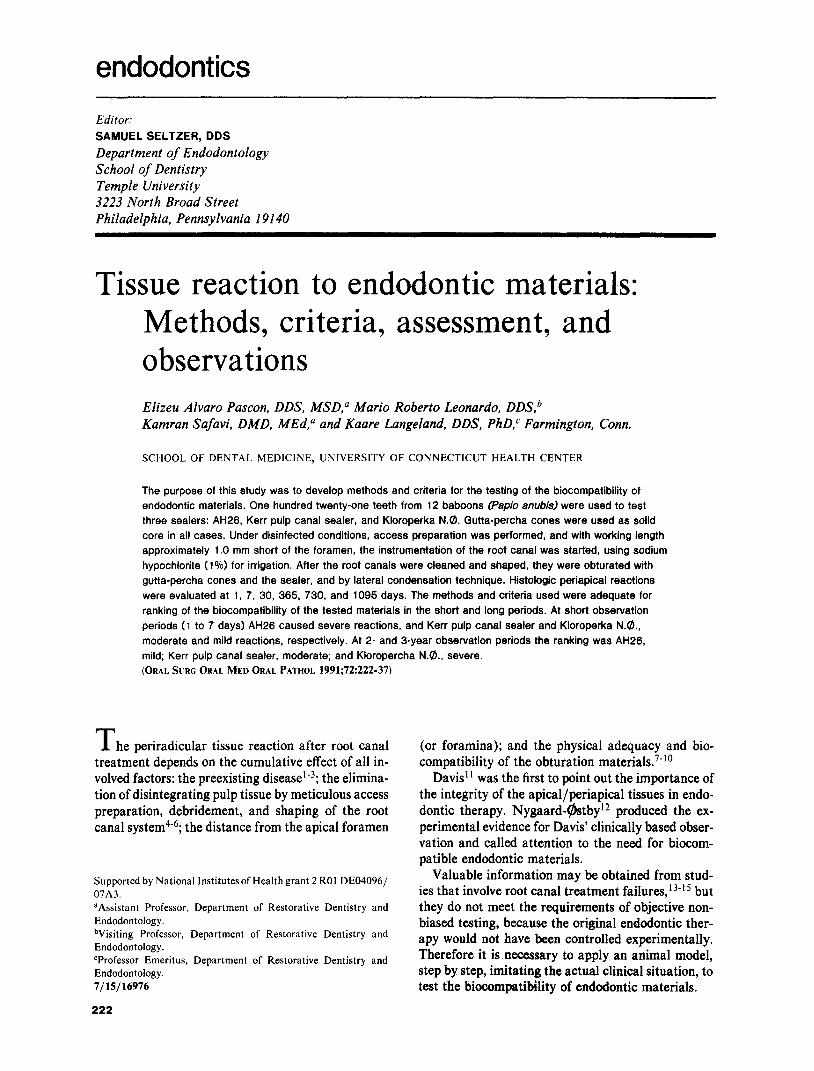
Fig. 1. Tooth 3.6, distal root, Kerr sealer, 1 day. A, Preoperative radiograph. B, Final radiograph. C, Root tip with debris in canal, transition zone between debris and periapical tissue. Note effect of earlier root re- sorption. (Hematoxylin-eosin stain; original magnification, X44.) D, Debris and sealer from the canal. (He- matoxylin-eosin stain; original magnification, X 1250.) E, Contact zone between debris and vital tissue con- taining numerous neutrophilic leukocytes. (Hematoxylin-eosin stain: original magnification, X 1200.)
Erausquin and Muruzabal16 used root canals of the maxillary molars of rats for evaluation of endodontic materials, which represented an attempt at standard- ization. However, because of the lack of similarity of the rat and human teeth and their root canal systems, these tests should be considered implantation tests in mechanically damaged bone tissue through an artifi- cially produced canal rather than a usage test. The required apical perforation causes an inflammatory foreign body reaction, which causes a less favorable prognosis. Therefore it should not be used for testing materials.
Snyder et a1.17 and Holland18 employed dog teeth for the usage test. However, the extensive apical rami- fications of dogs’ teeth impair proper instrumenta- tion.19
Testing in nonhuman primates provides the best model. The anatomy of the teeth and the supporting structures are sufficiently similar to those in human
Table I. Distribution of 121 cases according to the observation periods and materials
Root canal sealers Observation
period (days) Group I Group II Group III
1 5 9 9 7 9 7 5
30 8 11 13 365 12 9 6 730 2 5 5
1095 2 -! 2 Total 39 41 41
beings and allows commonly available endodontic in- struments for human teeth (e.g., rubber dam clamps, and files and reamers) and obturation materials to be used without modification. This is particularly appli-
224 Pascon et al. 0~4~ SURG ORAL MED ORAL PATHCII August I99 I
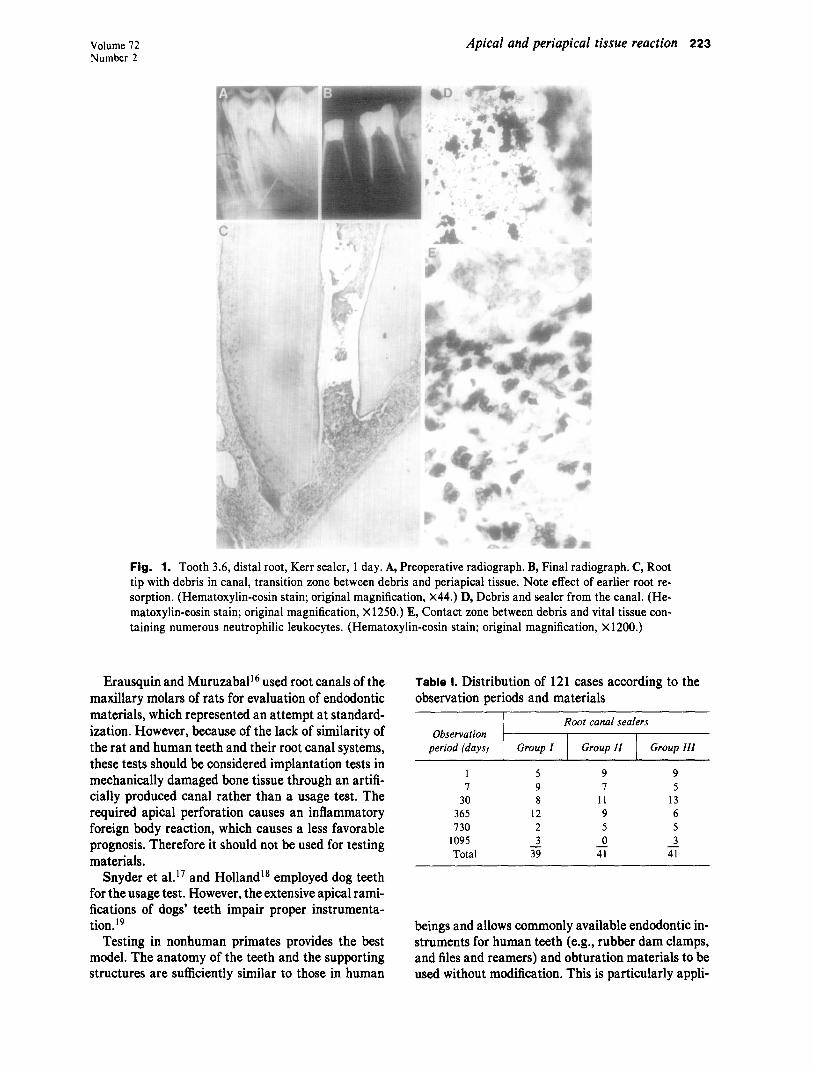
Fig. 2. Tooth 4.1, AH26, 7 days. A, Preoperative radiograph. B, Final radiograph. C, Root tip with debris in apical part of canal and minor concentration of cells in periapical tissue. (Hematoxylin-eosin stain; orig- inal magnification, x20.) D, Vital tissue from transition zone with chronic inflammatory cells and macro- phages with sealer particles. (Hematoxylin-eosin stain; original magnification, X1250.) E, From concentra- tion of cells in periapical tissue, macrophages with sealer particles. (Hematoxylin-eosin stain; original mag- nification, X 1250.)
cable to baboon teeth because of the similarity to the size of human teeth. Thus a major variable is eliminated.20q 2’
The long-term prognosis studies clearly confirm the validity of Davis’ principle to leave the periapical tis- sue undisturbed,’ 1, 22 because in all cases where a for- eign material is forced into the periapical tissue, a foreign body reaction will occur.s-‘o
The purpose of this study was to further develop and refine methods for the testing of endodontic ma- terials and to refine the criteria for evaluation of their biologic acceptability with the long-range goal of im- proving biologic standards and specifications. An at- tempt was made to establish a correlation between the results of usage test and earlier implant tests.
MATERIAL AND METHODS Material
Group I: Kloroperka N.@ (Union Broach Corp., Long Island City, N.Y.). The composition according
to manufacturer is zinc oxide (48.9%), gutta-percha alba (19.6%), resina canadense (17-O%), and resina colophonium (14.0%), when mixed with 0.5 gm of chloroform. This material was chosen to represent gutta-percha products used as a sealer.
Group ZZ: Kerr pulp canal sealer (Rickert modi- fied, Sybron/Kerr, Romulus, Mich.). Composition according to manufacturer is as follows: the base contains zinc oxide (34%), oleoresin (30%), radio- paque agent (25%), and dithymol diiodide (11%). Equal parts of the base and the catalyzer are mixed immediately before use. This product was chosen to represent sealers that have a zinc oxide-eugenol base.
Group ZZZ: AH26 (De Trey Dentsply, Zurich, Switzerland). Composition according to manufac- turer is as follows: the powder contains bismuth tri- oxide (60%), silver powder (lo%), hexamethylene- tetramine (25%), and titanium dioxide (5%). The fluid phase is a bisphenol diglycidyl ether ( 100%). For this experiment 1 gm of powder was mixed with 0.5
Volume 72 Number 2
Apical and periapical tissue reaction 225
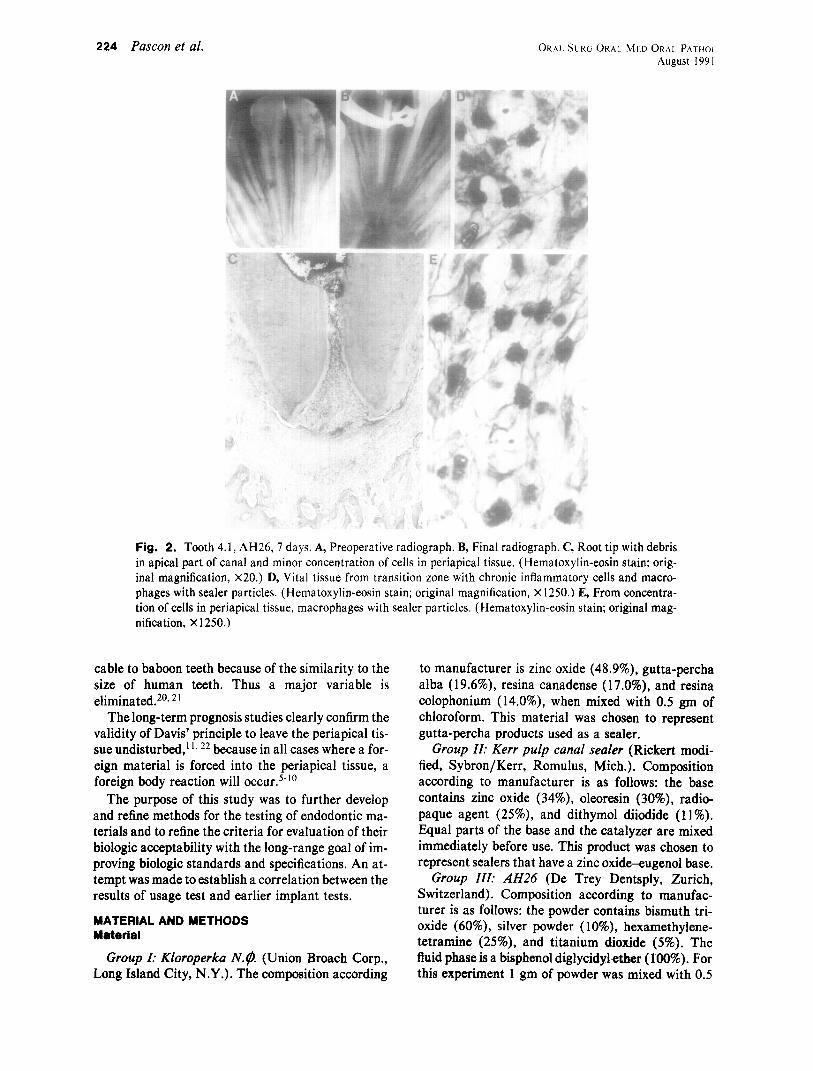
Fig. 3. Tooth 4.5, mesial root, AH26, 7 days. A, Preoperative radiograph. B, Final radiograph showing termination of obturation flush with apex. C, Root tip with debris and material in canal and material beyond the apex in periapical lesion. (Hematoxylin-eosin stain; original magnification, X22.) D, Contact zone between material/tissue with material particles on surface and deeper in tissue; mostly neutrophilic leukocytes, fibro- blasts, and chronic inflammatory cells. (Hematoxylin-eosin stain; original magnification, X750.) E, Disinte- grating foreign body cells with material particles and adjacent fibroblasts. (Hematoxylin-eosin stain; original magnification, X900.)
gm of catalyst fluid. AH26 was chosen to represent resin materials.
Gutta-percha cones (Premier, Norristown, Pa.) were used as a solid core for obturation. Composition of gutta-percha cones was not supplied by the manu- facturers.
Animals
Twelve baboons (Papio anubis) were used in this study. The observation periods were 1,7, and 30 days, and 1, 2, and 3 years. The animals were not fed the evening before experimentation. While caged, the animals were given a mixture of ketamine hydro- chloride (5 to 7.5 mg/kg) and acepromazine male- ate (2 to 4 mg/kg) by intramuscular injection, followed by subcutaneous injection of atropine (0.04 mg/kg), which was effective for 1 l/z hours. If needed, half the original dose was given to maintain anesthe- sia.
Root canal treatment
The treatment was performed in all anterior teeth, premolars, and first molars of the maxilla and man- dible. After prophylaxis, rubber dam was applied and the tooth, rubber dam, and clamp were disinfected with 30% hydrogen peroxide and 5% tincture of iodine.23 Access preparation was performed. Before we entered the pulp chamber, the tooth was redisin- fected and new sterile instruments were used.
Radiographs were taken to establish the working length approximately 1.0 to 1.5 mm short of the ra- diographic apex, and the pulpectomy was performed accordingly. Copious amounts of 1% sodium hypo- chlorite were used for irrigation. After proper shap- ing and debridement, the canals were dried with ster- ile paper cones.
Obturation was performed with the use of stan- dardized gutta-percha cones as the solid core together with the sealers and accessory cones, in a lateral con-
226 Pascon et al. ORAL SLRG ORAL MED ORAL PATHOL.
August 199 I
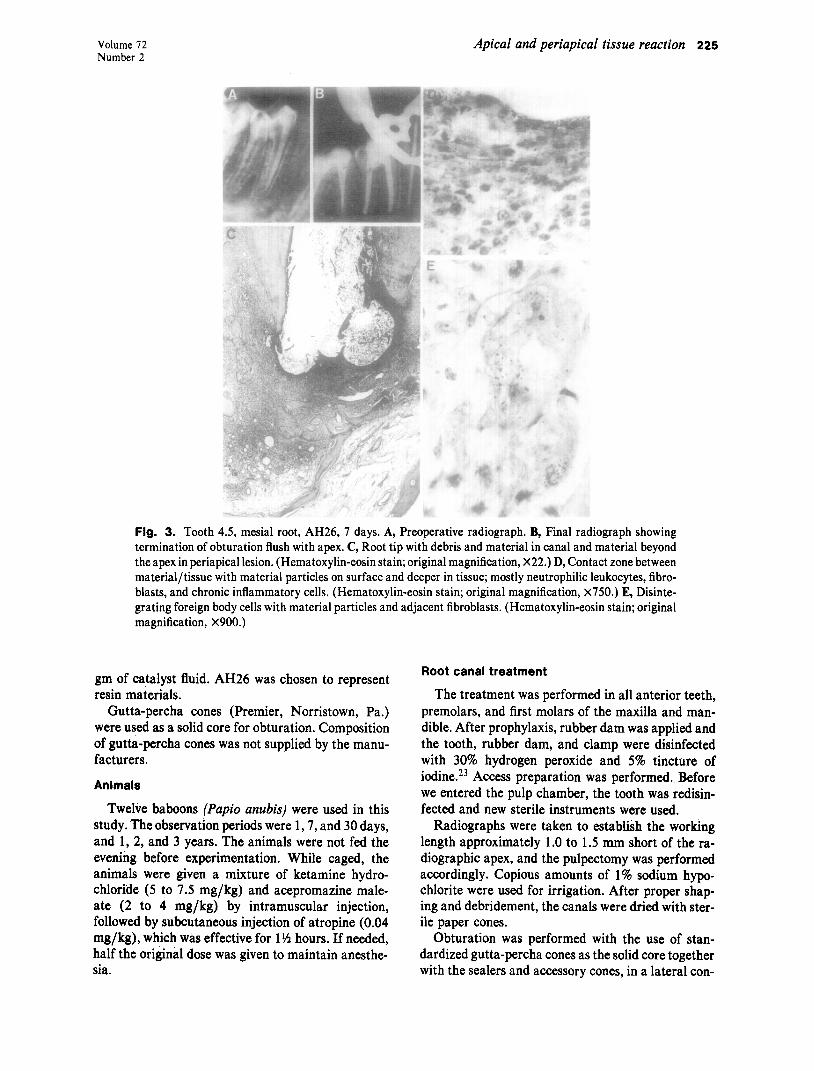
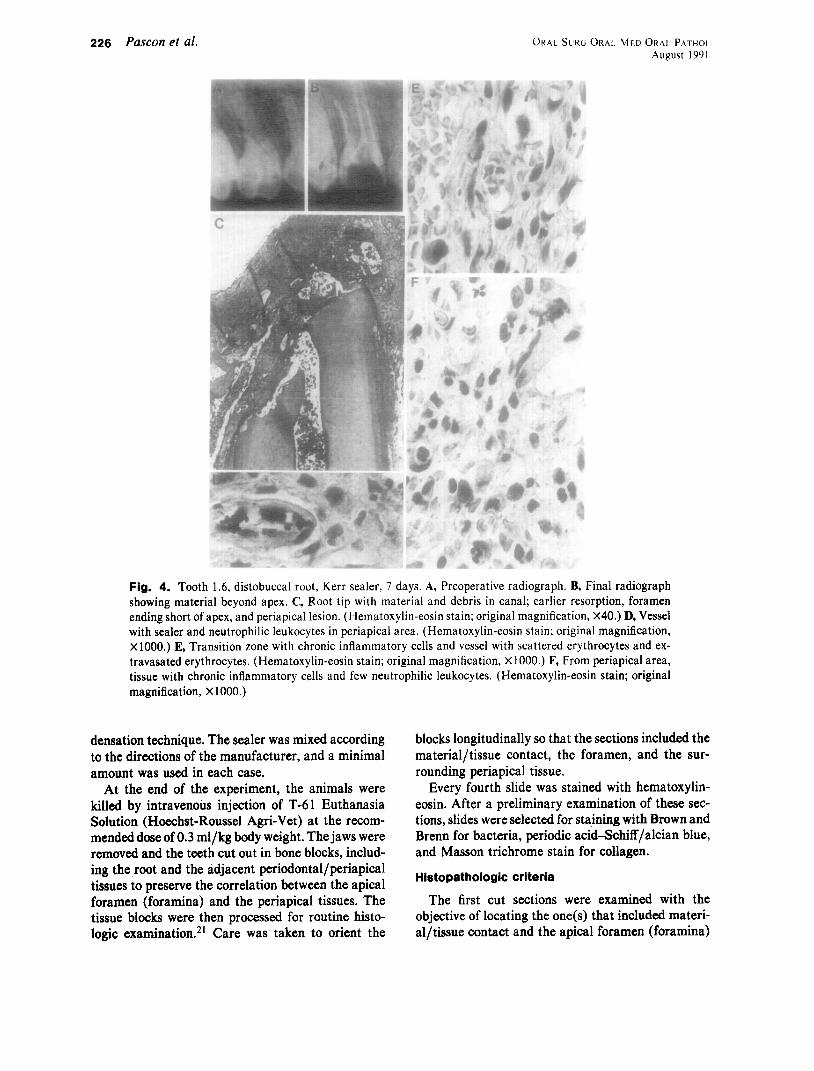
Fig. 4. Tooth 1.6, distobuccal root, Kerr sealer, 7 days. A, Preoperative radiograph. B, Final radiograph showing material beyond apex. C, Root tip with material and debris in canal; earlier resorption, foramen ending short of apex, and periapical lesion. (Hematoxylin-eosin stain; original magnification, X40.) D, Vessel with sealer and neutrophilic leukocytes in periapical area. (Hematoxylin-eosin stain; original magnification, x1000.) E, Transition zone with chronic inflammatory cells and vessel with scattered erythrocytes and ex- travasated erythrocytes. (Hematoxylin-eosin stain; original magnification, X1000.) F, From periapical area, tissue with chronic inflammatory cells and few neutrophilic leukocytes. (Hematoxylin-eosin stain; original magnification, X 1000.)
densation technique. The sealer was mixed according blocks longitudinally so that the sections included the to the directions of the manufacturer, and a minimal material/tissue contact, the foramen, and the sur- amount was used in each case. rounding periapical tissue.
At the end of the experiment, the animals were killed by intravenous injection of T-61 Euthanasia Solution (Hoechst-Roussel Agri-Vet) at the recom- mended dose of 0.3 ml/kg body weight. The jaws were removed and the teeth cut out in bone blocks, includ-
Every fourth slide was stained with hematoxylin- eosin. After a preliminary examination of these sec- tions, slides were selected for staining with Brown and Brenn for bacteria, periodic acid-Schiff/alcian blue, and Masson trichrome stain for collagen.
ing the root and the adjacent periodontal/periapical tissues to nreserve the correlation between the apical foramen iforamina) and the periapical tissues.-The tissue blocks were then processed for routine histo- logic examination. 21 Care was taken to orient the
Histopathologic criteria
The first cut sections were examined with the objective of locating the one(s) that included materi- al/tissue contact and the apical foramen (foramina)
Volume 72 Number 2
Apical and periapical tissue reaction 227
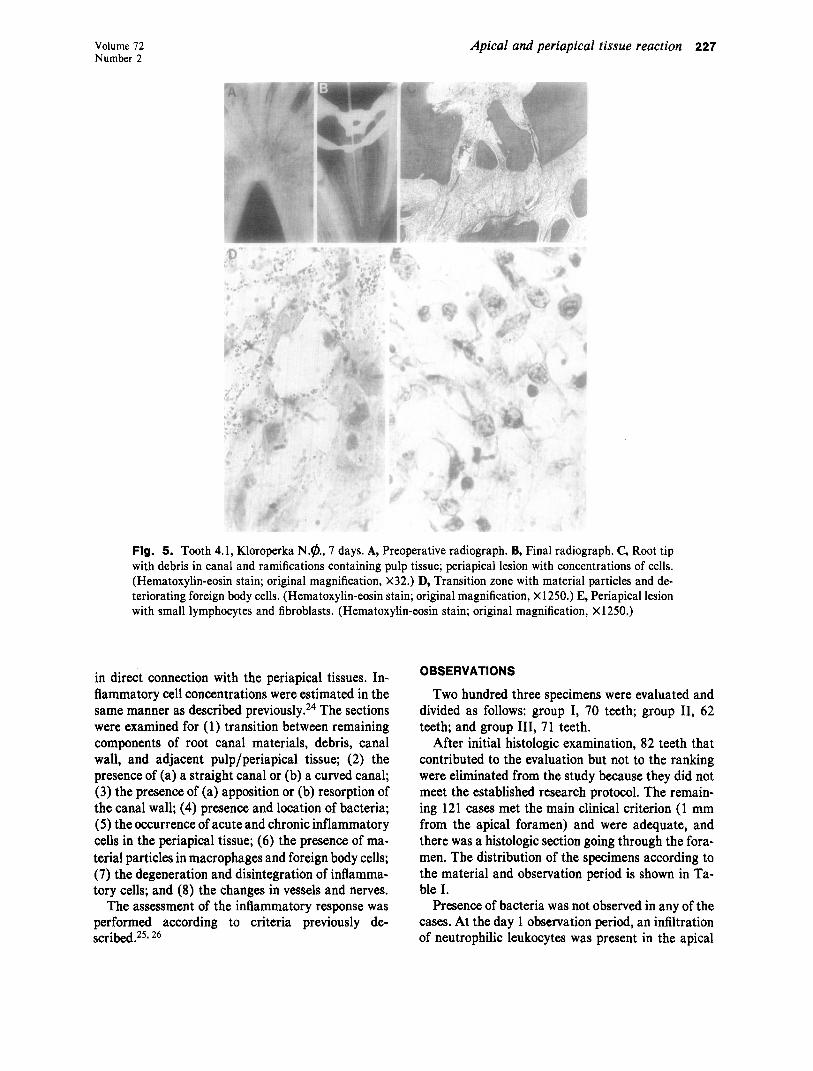
Fig. 5. Tooth 4.1, Kloroperka N.@., 7 days. A, Preoperative radiograph. B, Final radiograph. C, Root tip with debris in canal and ramifications containing pulp tissue; periapical lesion with concentrations of cells. (Hematoxylin-eosin stain; original magnification, X32.) D, Transition zone with material particles and de- teriorating foreign body cells. (Hematoxylin-eosin stain; original magnification, X 1250.) E, Periapical lesion with small lymphocytes and fibroblasts. (Hematoxylin-eosin stain; original magnification, X1250.)
in direct connection with the periapical tissues. In- flammatory cell concentrations were estimated in the same manner as described previously.24 The sections were examined for (1) transition between remaining components of root canal materials, debris, canal wall, and adjacent pulp/periapical tissue; (2) the presence of (a) a straight canal or (b) a curved canal; (3) the presence of (a) apposition or (b) resorption of the canal wall; (4) presence and location of bacteria; (5) the occurrence of acute and chronic inflammatory cells in the periapical tissue; (6) the presence of ma- terial particles in macrophages and foreign body cells; (7) the degeneration and disintegration of inflamma- tory cells; and (8) the changes in vessels and nerves.
The assessment of the inflammatory response was performed according to criteria previously de- scribed.25* 26
OBSERVATIONS
Two hundred three specimens were evaluated and divided as follows: group I, 70 teeth; group II, 62 teeth; and group III, 71 teeth.
After initial histologic examination, 82 teeth that contributed to the evaluation but not to the ranking were eliminated from the study because they did not meet the established research protocol. The remain- ing 12 1 cases met the main clinical criterion (1 mm from the apical foramen) and were adequate, and there was a histologic section going through the fora- men. The distribution of the specimens according to the material and observation period is shown in Ta- ble I.
Presence of bacteria was not observed in any of the cases. At the day 1 observation period, an infiltration of neutrophilic leukocytes was present in the apical
228 Pascon et al. ORAL SURG 0~.41. MED ORAL PATHOL August I 99 1
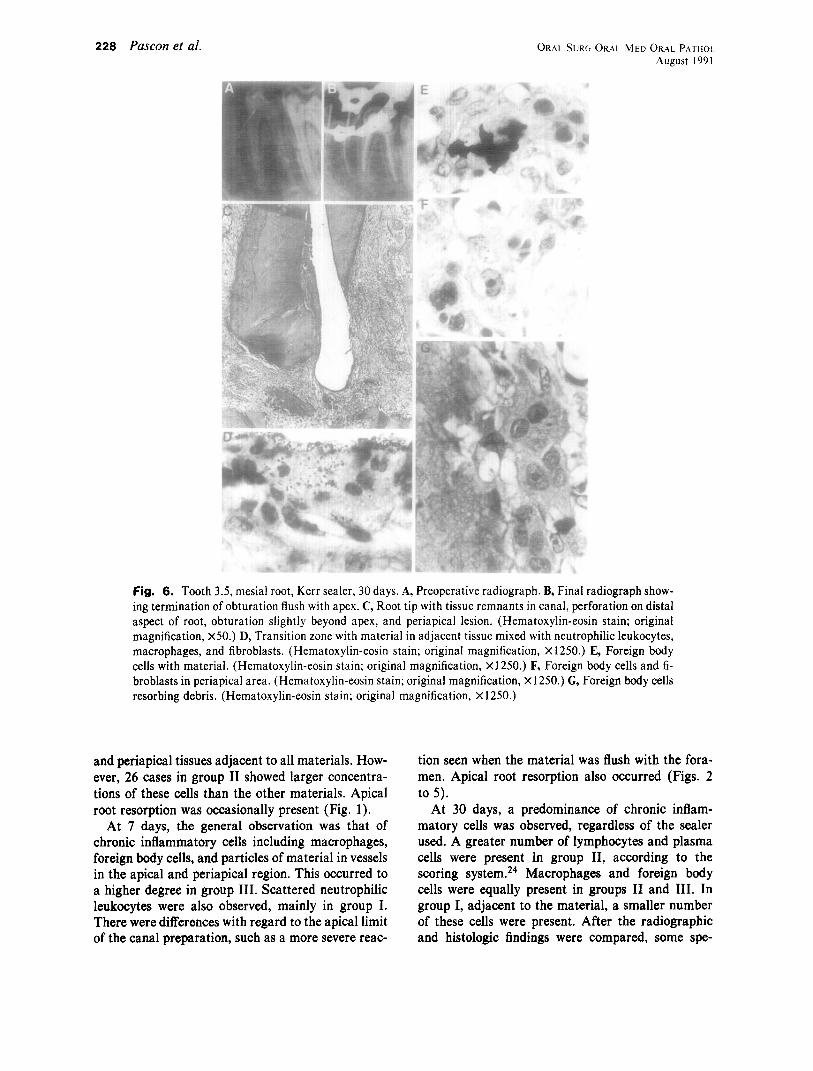
Fig. 6. Tooth 3.5, mesial root, Kerr sealer, 30 days. A, Preoperative radiograph. B, Final radiograph show- ing termination of obturation flush with apex. C, Root tip with tissue remnants in canal, perforation on distal aspect of root, obturation slightly beyond apex, and periapical lesion. (Hematoxylin-eosin stain; original magnification, X50.) D, Transition zone with material in adjacent tissue mixed with neutrophilic leukocytes, macrophages, and fibroblasts. (Hematoxylin-eosin stain; original magnification, X 1250.) E, Foreign body cells with material. (Hematoxylin-eosin stain; original magnification, x 1250.) F, Foreign body cells and fi- broblasts in periapical area. (Hematoxylin-eosin stain; original magnification, x 1250.) G, Foreign body cells resorbing debris. (Hematoxylin-eosin stain; original magnification, X 1250.)
and periapical tissues adjacent to all materials. How- ever, 26 cases in group II showed larger concentra- tions of these cells than the other materials. Apical root resorption was occasionally present (Fig. 1).
At 7 days, the general observation was that of chronic inflammatory cells including macrophages, foreign body cells, and particles of material in vessels in the apical and periapical region. This occurred to a higher degree in group III. Scattered neutrophilic leukocytes were also observed, mainly in group I. There were differences with regard to the apical limit of the canal preparation, such as a more severe reac-
tion seen when the material was flush with the fora- men. Apical root resorption also occurred (Figs. 2 to 5).
At 30 days, a predominance of chronic inflam- matory cells was observed, regardless of the sealer used. A greater number of lymphocytes and plasma cells were present in group II, according to the scoring system.24 Macrophages and foreign body cells were equally present in groups II and III. In group I, adjacent to the material, a smaller number of these cells were present. After the radiographic and histologic findings were compared, some spe-
Volume 72 Number 2
Apical and periapical tissue reaction 229
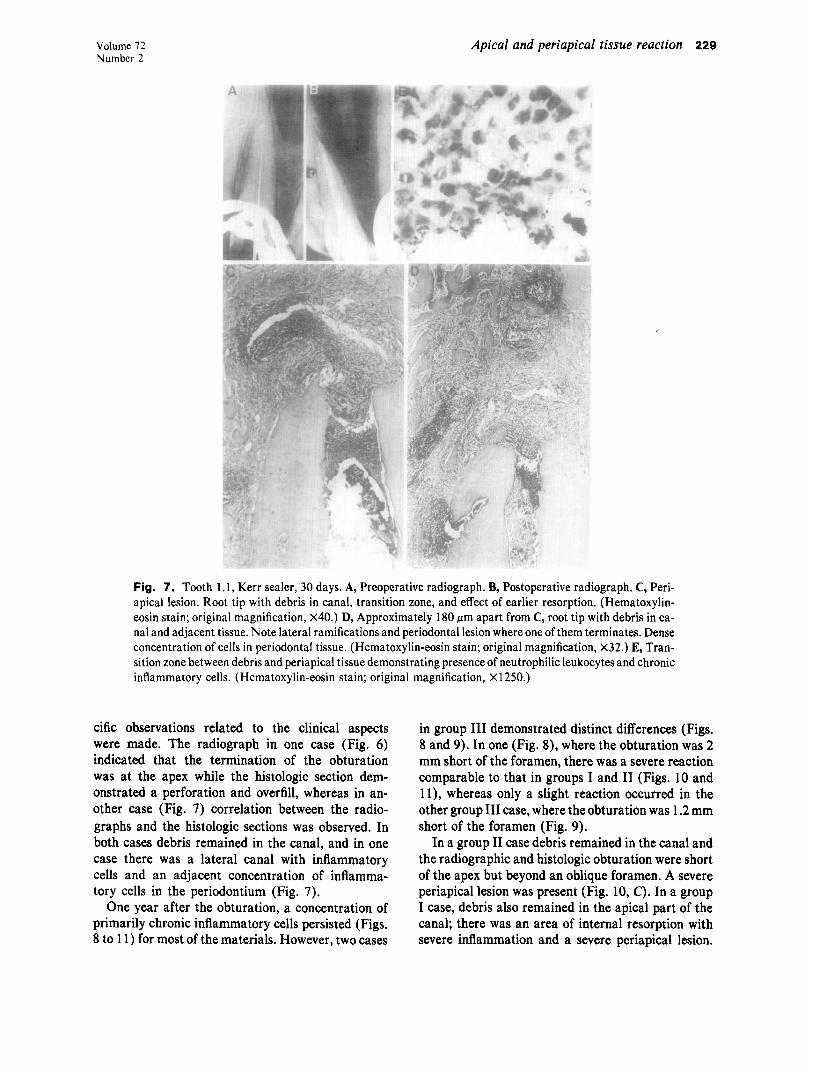
Fig. 7. Tooth 1.1, Kerr sealer, 30 days. A, Preoperative radiograph. B, Postoperative radiograph. C, Peri- apical lesion. Root tip with debris in canal, transition zone, and effect of earlier resorption. (Hematoxylin- eosin stain; original magnification, X40.) D, Approximately 180 Km apart from C, root tip with debris in ca- nal and adjacent tissue. Note lateral ramifications and periodontal lesion where one of them terminates. Dense concentration of cells in periodontal tissue. (Hematoxylin-eosin stain; original magnification, X32.) E, Tran- sition zone between debris and periapical tissue demonstrating presence of neutrophilic leukocytes and chronic inflammatory cells. (Hematoxylin-eosin stain; original magnification, X1250.)
cific observations related to the clinical aspects were made. The radiograph in one case (Fig. 6) indicated that the termination of the obturation was at the apex while the histologic section dem- onstrated a perforation and overfill, whereas in an- other case (Fig. 7) correlation between the radio- graphs and the histologic sections was observed. In both cases debris remained in the canal, and in one case there was a lateral canal with inflammatory cells and an adjacent concentration of inflamma- tory cells in the periodontium (Fig. 7).
One year after the obturation, a concentration of primarily chronic inflammatory cells persisted (Figs. 8 to 11) for most of the materials. However, two cases
in group III demonstrated distinct differences (Figs. 8 and 9). In one (Fig. 8), where the obturation was 2 mm short of the foramen, there was a severe reaction comparable to that in groups I and II (Figs. 10 and 1 l), whereas only a slight reaction occurred in the other group III case, where the obturation was 1.2 mm short of the foramen (Fig. 9).
In a group II case debris remained in the canal and the radiographic and histologic obturation were short of the apex but beyond an oblique foramen. A severe periapical lesion was present (Fig. 10, C). In a group I case, debris also remained in the apical part of the canal; there was an area of internal resorption with severe inflammation and a severe periapical lesion.
230 Pascon et al. ORAL SURG ORAL MED ORRL PATHCX August 1991
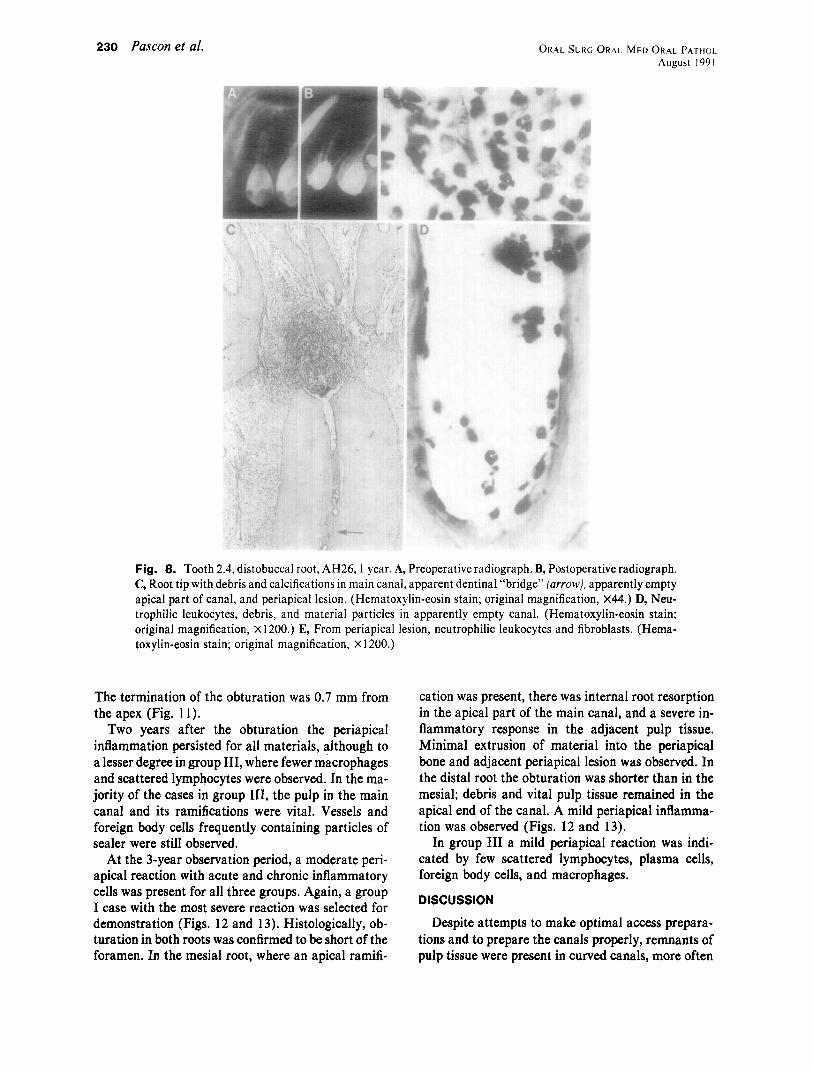
Fig. 8. Tooth 2.4, distobuccai root, AH26, I year. A, Preoperative radiograph. B, Postoperative radiograph. C, Root tip with debris and calcifications in main canal, apparent dentinal “bridge” farrowj, apparently empty apical part of canal, and periapical lesion. (Hematoxylin-eosin stain; original magnification, ~44.) D, Neu- trophilic leukocytes, debris, and material particles in apparently empty canal. (Hematoxylin-eosin stain; original magnification, X 1200.) E, From periapical lesion, neutrophilic leukocytes and fibroblasts. (Hema- toxylin-eosin stain; original magnification, X 1200.)
The termination of the obturation was 0.7 mm from the apex (Fig. 11).
Two years after the obturation the periapical inflammation persisted for all materials, although to a lesser degree in group III, where fewer macrophages and scattered lymphocytes were observed. In the ma- jority of the cases in group III, the pulp in the main canal and its ramifications were vital. Vessels and foreign body cells frequently containing particles of sealer were still observed.
At the 3-year observation period, a moderate peri- apical reaction with acute and chronic inflammatory cells was present for all three groups. Again, a group I case with the most severe reaction was selected for demonstration (Figs. 12 and 13). Histologically, ob- turation in both roots was confirmed to be short of the foramen. In the mesial root, where an apical ramifi-
cation was present, there was internal root resorption in the apical part of the main canal, and a severe in- flammatory response in the adjacent pulp tissue. Minimal extrusion of material into the periapical bone and adjacent periapical lesion was observed. In the distal root the obturation was shorter than in the mesial; debris and vital pulp tissue remained in the apical end of the canal. A mild periapical inflamma- tion was observed (Figs. 12 and 13).
In group III a mild periapical reaction was indi- cated by few scattered lymphocytes, plasma cells, foreign body cells, and macrophages.
DISCUSSION
Despite attempts to make optimal access prepara- tions and to prepare the canals properly, remnants of pulp tissue were present in curved canals, more often
Volume 72 Number 2
Apical and periapical tissue reaction 231
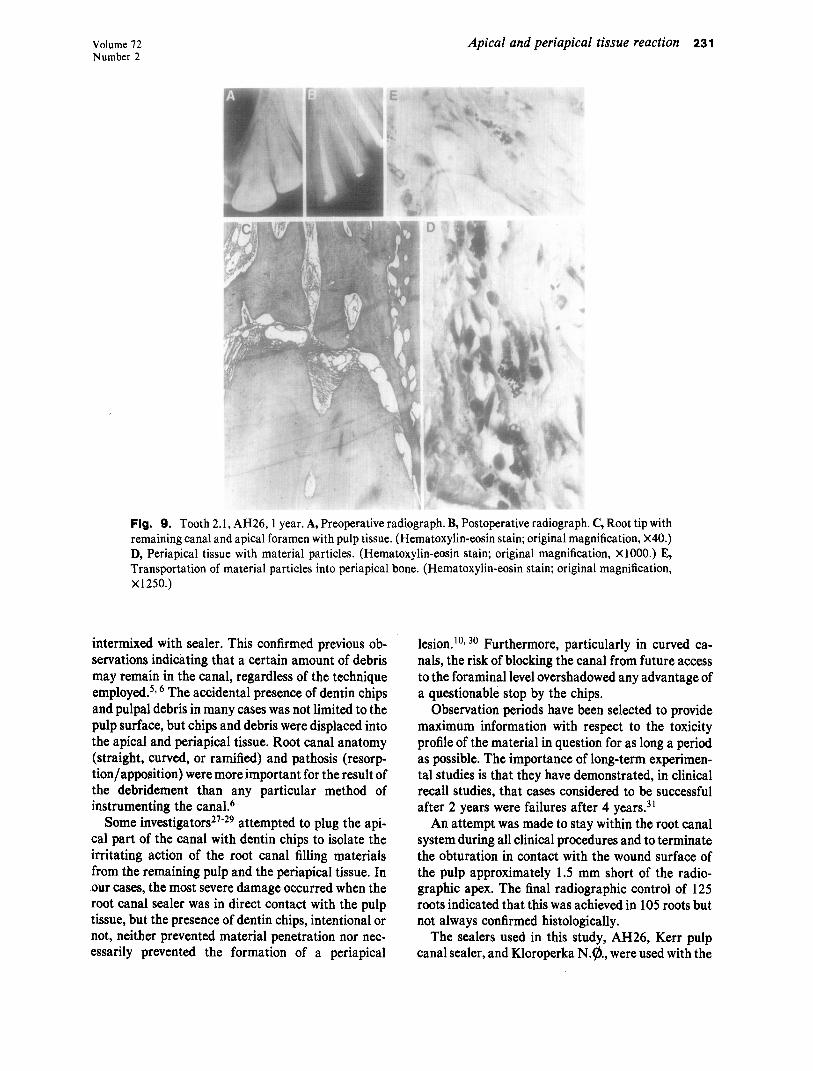
Fig. 9. Tooth 2.1, AH26,l year. A, Preoperative radiograph. B, Postoperative radiograph. C, Root tip with remaining canal and apical foramen with pulp tissue. (Hematoxylin-eosin stain; original magnification, X40.) D, Periapical tissue with material particles. (Hematoxylin-eosin stain; original magnification, X1000.) E, Transportation of material particles into periapical bone. (Hematoxylin-eosin stain; original magnification, x1250.)
intermixed with sealer. This confirmed previous ob- servations indicating that a certain amount of debris may remain in the canal, regardless of the technique employed. 5* 6 The accidental presence of dentin chips and pulpal debris in many cases was not limited to the pulp surface, but chips and debris were displaced into the apical and periapical tissue. Root canal anatomy (straight, curved, or ramified) and pathosis (resorp- tion/apposition) were more important for the result of the debridement than any particular method of instrumenting the canal.6
Some investigators27-29 attempted to plug the api- cal part of the canal with dentin chips to isolate the irritating action of the root canal filling materials from the remaining pulp and the periapical tissue. In our cases, the most severe damage occurred when the root canal sealer was in direct contact with the pulp tissue, but the presence of dentin chips, intentional or not, neither prevented material penetration nor nec- essarily prevented the formation of a periapical
lesion.lO, 3o Furthermore, particularly in curved ca- nals, the risk of blocking the canal from future access to the foraminal level overshadowed any advantage of a questionable stop by the chips.
Observation periods have been selected to provide maximum information with respect to the toxicity profile of the material in question for as long a period as possible. The importance of long-term experimen- tal studies is that they have demonstrated, in clinical recall studies, that cases considered to be successful after 2 years were failures after 4 years31
An attempt was made to stay within the root canal system during all clinical procedures and to terminate the obturation in contact with the wound surface of the pulp approximately 1.5 mm short of the radio- graphic apex. The final radiographic control of 125 roots indicated that this was achieved in 105 roots but not always confirmed histologically.
The sealers used in this study, AH26, Kerr pulp canal sealer, and Kloroperka N.@., were used with the
232 Pascon et al. ORAL SURC ORAL MED ORAL Aug1
PP ust
(THOL 1991
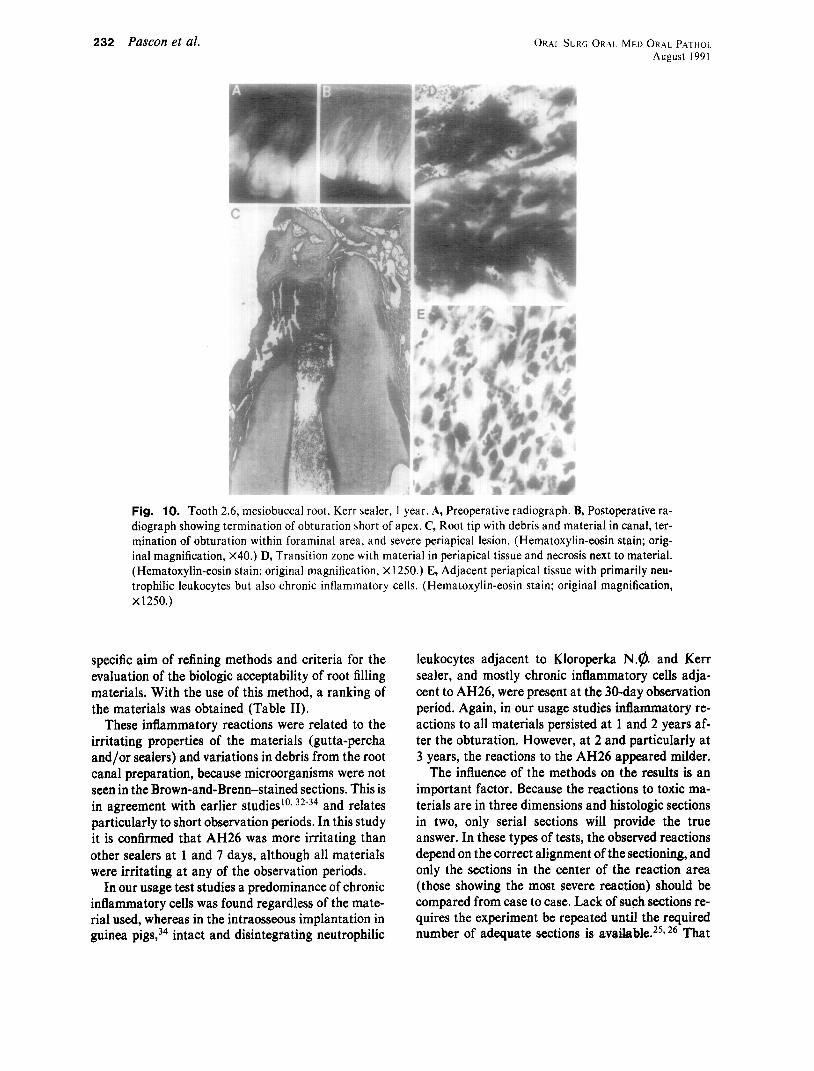
Fig. 10. Tooth 2.6, mesiobuccal root, Kerr sealer, 1 year. A, Preoperative radiograph. B, Postoperative ra- diograph showing termination of obturation short of apex. C, Root tip with debris and material in canal, ter- mination of obturation within foraminal area, and severe periapical lesion. (Hematoxylin-eosin stain; orig- inal magnification, X40.) D, Transition zone with material in periapical tissue and necrosis next to material. (Hematoxylin-eosin stain; original magnification, X 1250.) E, Adjacent periapical tissue with primarily neu- trophilic leukocytes but also chronic inflammatory cells. (Hematoxylin-eosin stain; original magnification, x1250.)
specific aim of refining methods and criteria for the evaluation of the biologic acceptability of root filling materials. With the use of this method, a ranking of the materials was obtained (Table II).
These inflammatory reactions were related to the irritating properties of the materials (gutta-percha and/or sealers) and variations in debris from the root canal preparation, because microorganisms were not seen in the Brown-and-Brenn-stained sections. This is in agreement with earlier studiesroT 32-34 and relates particularly to short observation periods. In this study it is confirmed that AH26 was more irritating than other sealers at 1 and 7 days, although all materials were irritating at any of the observation periods.
In our usage test studies a predominance of chronic inflammatory cells was found regardless of the mate- rial used, whereas in the intraosseous implantation in guinea pigs,34 intact and disintegrating neutrophilic
leukocytes adjacent to Kloroperka N.9. and Kerr sealer, and mostly chronic inflammatory cells adja- cent to AH26, were present at the 30-day observation period. Again, in our usage studies inflammatory re- actions to all materials persisted at 1 and 2 years af- ter the obturation. However, at 2 and particularly at 3 years, the reactions to the AH26 appeared milder.
The influence of the methods on the results is an important factor. Because the reactions to toxic ma- terials are in three dimensions and histologic sections in two, only serial sections will provide the true answer. In these types of tests, the observed reactions depend on the correct alignment of the sectioning, and only the sections in the center of the reaction area (those showing the most severe reaction) should be compared from case to case. Lack of such sections re- quires the experiment be repeated until the required number of adequate sections is available.25y 26 That
Volume 72 Number 2
Apical and periapical tissue reaction 233
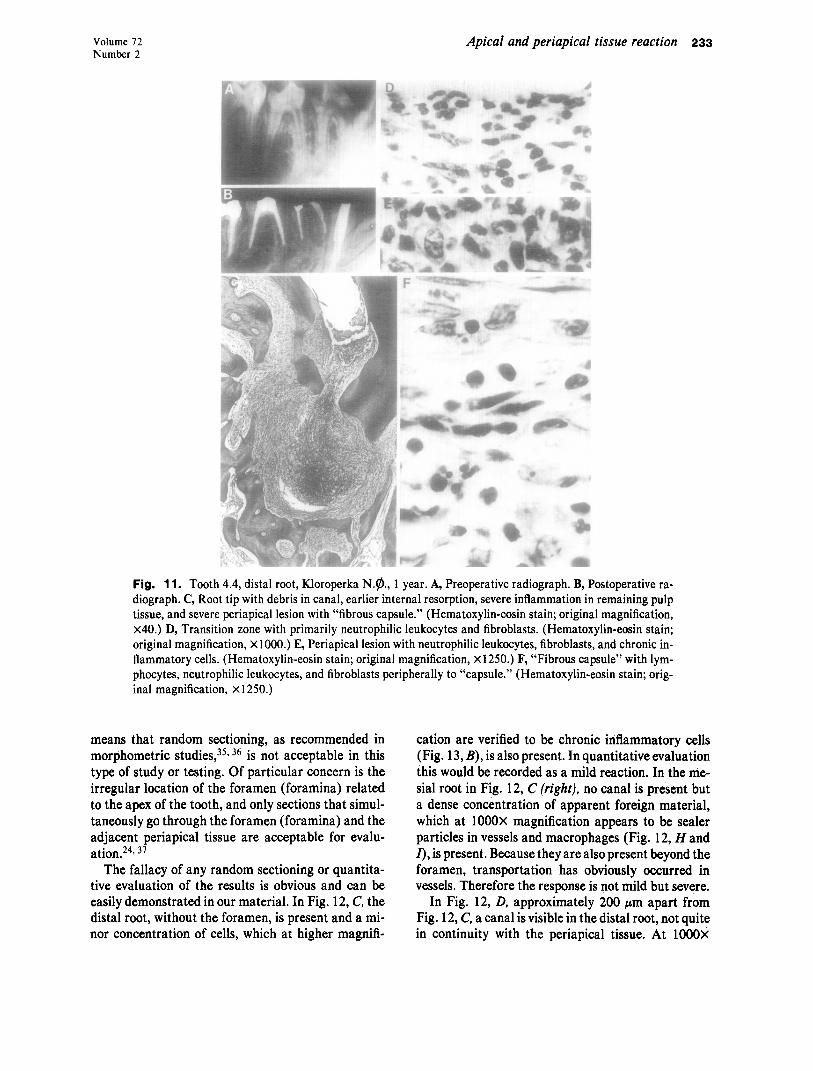
Fig. 11. Tooth 4.4, distal root, Kloroperka N.@, 1 year. A, Preoperative radiograph. B, Postoperative ra- diograph. C, Root tip with debris in canal, earlier internal resorption, severe inflammation in remaining pulp tissue, and severe periapical lesion with “fibrous capsule.” (Hematoxylin-eosin stain; original magnification, x40.) D, Transition zone with primarily neutrophilic leukocytes and fibroblasts. (Hematoxylin-eosin stain; original magnification, X 1000.) E, Periapical lesion with neutrophilic leukocytes, fibroblasts, and chronic in- flammatory cells. (Hematoxylin-eosin stain; original magnification, X1250.) F, “Fibrous capsule” with lym- phocytes, neutrophilic leukocytes, and fibroblasts peripherally to “capsule.” (Hematoxylin-eosin stain; orig- inal magnification, X 1250.)
means that random sectioning, as recommended in morphometric studies,35, 36 is not acceptable in this type of study or testing. Of particular concern is the irregular location of the foramen (foramina) related to the apex of the tooth, and only sections that simul- taneously go through the foramen (foramina) and the adjacent periapical tissue are acceptable for evalu- ation.24, 37
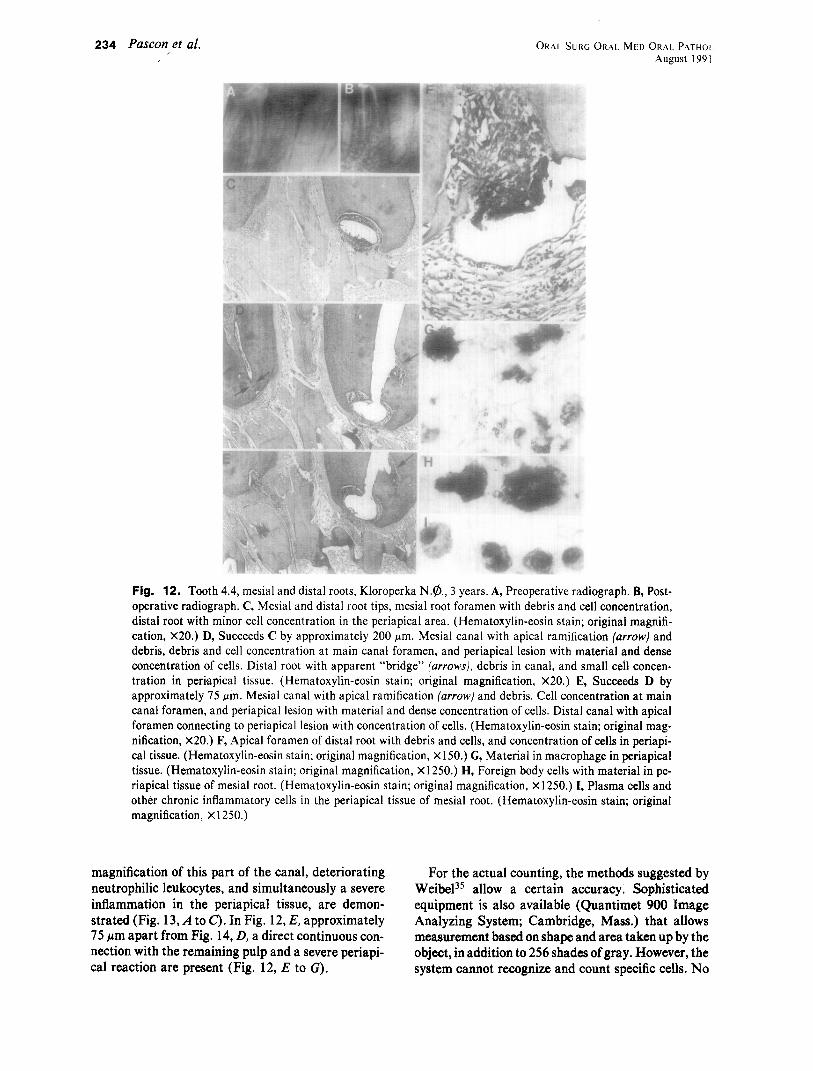
The fallacy of any random sectioning or quantita- tive evaluation of the results is obvious and can be easily demonstrated in our material. In Fig. 12, C, the distal root, without the foramen, is present and a mi- nor concentration of cells, which at higher magnifi-
cation are verified to be chronic inflammatory cells (Fig. 13, B), is also present. In quantitative evaluation this would be recorded as a mild reaction. In the me- sial root in Fig. 12, C (right). no canal is present but a dense concentration of apparent foreign material, which at 1000X magnification appears to be sealer particles in vessels and macrophages (Fig. 12, H and I), is present. Because they are also present beyond the foramen, transportation has obviously occurred in vessels. Therefore the response is not mild but severe.
In Fig. 12, D, approximately 200 pm apart from Fig. 12, C, a canal is visible in the distal root, not quite in continuity with the periapical tissue. At 1000X
ORAL SURG ORAL MED ORAL PATHOI August I99 1
234 Pascon et al. I
Fig. 12. Tooth 4.4, mesial and distal roots, Kloroperka N.@, 3 years. A, Preoperative radiograph. B, Post- operative radiograph. C, Mesial and distal root tips, mesial root foramen with debris and cell concentration, distal root with minor cell concentration in the periapical area. (Hematoxylin-eosin stain; original magnifi- cation, X20.) D, Succeeds C by approximately 200 pm. Mesial canal with apical ramification (arrow) and debris, debris and cell concentration at main canal foramen, and periapical lesion with material and dense concentration of cells. Distal root with apparent “bridge” (arrows), debris in canal, and small cell concen- tration in periapical tissue. (Hematoxylin-eosin stain; original magnification, X20.) E, Succeeds D by approximately 75 pm. Mesial canal with apical ramification (arrow) and debris. Cell concentration at main canal foramen, and periapical lesion with material and dense concentration of cells. Distal canal with apical foramen connecting to periapical lesion with concentration of cells. (Hematoxylin-eosin stain; original mag- nification, X20.) F, Apical foramen of distal root with debris and cells, and concentration of cells in periapi- cal tissue. (Hematoxylin-eosin stain; original magnification, X 150.) G, Material in macrophage in periapical tissue. (Hematoxylin-eosin stain; original magnification, X 1250.) H, Foreign body cells with material in pe- riapical tissue of mesial root. (Hematoxylin-eosin stain; original magnification, X 1250.) I, Plasma cells and other chronic inflammatory cells in the periapical tissue of mesial root. (Hematoxylin-eosin stain; original magnification, X 1250.)
magnification of this part of the canal, deteriorating For the actual counting, the methods suggested by neutrophilic leukocytes, and simultaneously a severe WeibeP5 allow a certain accuracy. Sophisticated inflammation in the periapical tissue, are demon- equipment is also available (Quantimet 900 Image strated (Fig. 13, A to c). In Fig. 12, E, approximately Analyzing System; Cambridge, Mass.) that allows 75 I.tm apart from Fig. 14, D, a direct continuous con- measurement based on shape and area taken up by the nection with the remaining pulp and a severe periapi- object, in addition to 256 shades of gray. However, the cal reaction are present (Fig. 12, E to G). system cannot recognize and count specific cells. No
Volume 72 Number 2
Apical and periapical tissue reaction 235
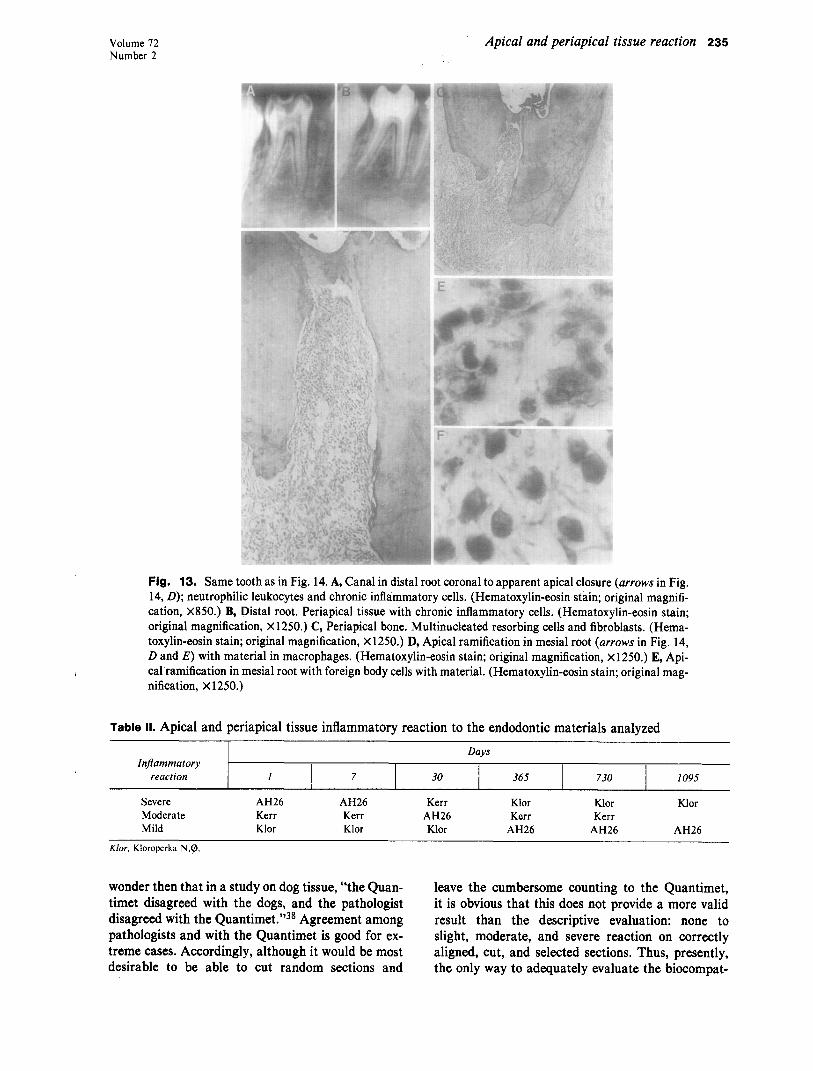
Fig. 13. Same tooth as in Fig. 14. A, Canal in distal root coronal to apparent apical closure (arrows in Fig. 14, D); neutrophilic leukocytes and chronic inflammatory cells. (Hematoxylin-eosin stain; original magnifi- cation, X850.) B, Distal root. Periapical tissue with chronic inflammatory cells. (Hematoxylin-eosin stain; original magnification, X1250.) C, Periapical bone. Multinucleated resorbing cells and fibroblasts. (Hema- toxylin-eosin stain; original magnification, X 1250.) D, Apical ramification in mesial root (arrows in Fig. 14, D and E) with material in macrophages. (Hematoxylin-eosin stain; original magnification, x 1250.) E, Api- cal ramification in mesial root with foreign body cells with material. (Hematoxylin-eosin stain; original mag- nification, X 1250.)
Table II. Apical and periapical tissue inflammatory reaction to the endodontic materials analyzed
Injammatory reaction I 7 30
Days
365 730 1095
Severe AH26 AH26 Kerr Klor Klor Moderate Kerr Kerr AH26 Kerr Kerr Mild Klor Klor Klor AH26 AH26
Klor
AH26
K/or, Kloroperka NQ
wonder then that in a study on dog tissue, “the Quan- leave the cumbersome counting to the Quantimet, timet disagreed with the dogs, and the pathologist it is obvious that this does not provide a more valid disagreed with the Quantimet.“38 Agreement among result than the descriptive evaluation: none to pathologists and with the Quantimet is good for ex- slight, moderate, and severe reaction on correctly treme cases. Accordingly, although it would be most aligned, cut, and selected sections. Thus, presently, desirable to be able to cut random sections and the only way to adequately evaluate the biocompat-
236 Pascon et al. ORAI. %RG ORAL MED ORAL PATHOS August 199 1
ibility of an endodontic material is the hard way in a full usage test:
1. An adequate access preparation and correct longitudinal alignment of the sectioning with the canal allows for the evaluation of com- plete canal preparation.
2. Only sections that include (a) the apical part of the canal and its ramifications, (b) the material/tissue interface, and (c) the remain- ing pulp tissue extending through the foramen to the periapical tissue are valid.
3. For measurement, until something better than the present equipment is developed, photomi- crographs of serial sections demonstrating the conditions in the third dimension (Fig. 7, C and D, 180 pm apart, and Fig. 12, C to E, 200 and 275 pm apart) are required.
In addition, sufficiently high magnification allow- ing the identification of cells and particles must be used. Photomicrographs demonstrate this better than a thousand words and graphics.
CONCLUSIONS
A direct correlation between the results of this usage test study and earlier implant test studies could not be established. Adherence to strict clinical and histologic meth- ods allows differentiation between severely irri- tating and nonirritating materials. It is not possible to rank materials in the inter- mediary range.
REFERENCES
1. Lin LM, Langeland K. Light and electron microscopic study of teeth with carious pulp exposures. ORAL SURG ORAL MED ORAL PATHOL 1981;51:292-316.
2. Lin LM, Shovlin F, Skribner J, Langeland K. Pulp biopsies from the teeth associated with periapical radiolucency. J En- dod 1984; 10:436-48.
3. Langeland K. Tissue response to dental caries. Endod Dent Traumatol 1987;3:149-71.
4. Schilder H. Cleaning and shaping the root canal. Dent Clin North Am 1974; 18:269-96.
5. Turek T, Langeland K. A light microscopic study of the efficacy of the telescopic and the Giromatic preparation of root canals. J Endod 1982;8:436-43.
6. Langeland K, Liao K, Pascon EA. Work-saving devices in en- dodontics: efficacy of sonic and ultrasonic techniques. J Endod 1985;11:499-510.
7. Langeland K, Guttuso J, Langeland LK, Tobon G. Methods in the study of biologic responses to endodontic materials: tis- sue response to N2. ORAL SURG ORAL MED ORAL PATHOL 1969;27:522-42.
8. Leonardo MR. Contribuicao para a reparacao apical e peri- apical pas-tratamento de canais radiculares [Thesis]. SLo Paulo, Brazil: Fat Farm Odont Araraquara, 1973.
9. Langeland K. Root canal sealants and pastes. Dent Clin North Am 1974;18:309-27.
10. Langeland K, Olsson B, Pascon EA. Biological evaluation of Hydron. J Endod 1981;7:196-204.
Il.
12.
13.
14.
15.
16.
17.
18.
19.
20.
21.
22.
23.
24.
25.
26.
27.
28.
29.
30.
31.
32.
33.
Davis WC. Pulpectomy vs. pulp-extirpation. Dent Items Interest 1922;44:8 l-100. Nygaard-@stby B. i;‘ber die Gewebsveranderungen im apikalem paradentium des Menschen nach verschiedenartigen Eingriffen in den Wurzelkannalen. Det Norske Videnskaps- Akademi i Oslo 1939;4:211. Block R, Bushel1 A, Rodrigues H, et al. A histopathologic, histobacteriologic, and radiographic study of periapical endo- dontic surgical specimens. ORAL SURC ORAL MED ORAL PATHOL 1976;42:656-78. Langeland K, Block RM, Grossman Ll. A histopathologic and histobacteriologic study of 35 periapical endodontic surgical specimens. J Ended 1977;3:8-23. Block RM. Pascon EA. Laneeland K. Paste techniaue retreat- ment study: a clinical, histoibgic, and radiographic evaluation of 50 cases. ORAL SURC ORAL MED ORAL PATHOL 1985;60: 76-93. Erausquin J, Muruzabal M. Root canal filling with zinc-oxide eugenol cement in the rat molar. ORAL SURG ORAL MED ORAL PATHOL 1967;24:547-58. Snyder E, Seltzer S, Moodnik R. Effects of N2 in experimen- tal endodontic therapy. ORAL SURG ORAL MED ORAL PATHOL 1966;2 11635-56. Holland R. Process0 de reparo do coto pulpar e dos tecidos pe- riapicais apes biopulpectomia e obturacao de canal radicular corn hidroxido de calcio ou oxide de zinco e eugenol. Estudo histologic0 em dentes de cles [Thesis]. Aracatuba, SQo Paulo, Brazil: Fat Odont, 1975. Block RM, Lewis RD. Hirsch J, Coffey J, Langeland K. Sys- temic distribution of N2 paste containing t4C paraformalde- hyde following root canal therapy in dogs. ORAL SURG ORAL MED ORAL PATHOL 1980;50:350-60. Langeland K. The histopathologic basis in endodontic treat- ment. Dent Clin North Am 1967:491-520. Pascon EA, lntrocaso JH, Langeland K. Development of a predictable periapical lesion monitored by subtraction radiog- raphy. Endod Dent Traumatol 1987;3:192-208. Kerekes K, Tronstad L. Long-term results of endodontic treatment performed with a standardized technique. J Endod 1979;5:83-90. Miiller AJR. Microbiological experimentation of root canals and periapical tissues of human teeth: methodological studies. Odontol Tidskr 1966;74(suppl):l-380. Safavi KS, Pascon EA, Langeland K. Evaluation of tissue re- action to endodontic materials. J Endod 1983;9:421-9. Stanford J. FDI Technical Report No. 9: recommended stan- dard practices for biological evaluation of dental materials. Int Dent J 1980;30: 140-88. American National Standards Institute/American Dental Association specification No. 41 for biological evaluation of dental materials. Approved Jan 4, 1982. Tronstad L. Tissue reactions following apical plugging of the root canal with dentin chips in monkey teeth subjected to pulpectomy. ORAL SURG ORAL MED ORAL PATHOL 1978; 45~297-304. Petersson K, Hasselgren G, Petersson A, Tronstad L. Clinical experience with the use of dentin chips in pulpectomies. Int Endod J 1982;15:161-7. Kuttler Y. A precision and biologic root canal filling technique. J Am Dent Assoc 1958;56:38-50. Safavi K, H$rnsted P, Pascon EA, Langeland K. Biological evaluation of the apical dentin chip plug. J Endod 1985;11:18- 24. Strindberg LZ. The dependence of the results of pulp therapy on certain factors. Acta Odontol Stand 1956;14(suppl 21):1- 175. Olsson B, Sliwkowski A, Langeland K. Subcutaneous implan- tation for the biological evaluation of endodontic materials. J Endod 1981;7:355-69. Leonardo MR, Pascon EA, Langeland K. Tissue reaction to endodontic materials: a morphometric approach. J Dent Res 1984;63:286.

Volume 72 Number 2
34.
35.
36.
31.
38.
Olsson B, Sliwkowski A, Langeland K. Intraosseous implan- tation for biological evaluation of endodontic materials. J En- dod 1981;7:253-65. Weibel ER. Stereological methods. Practical methods for bi- ological morphometry; vol 1. New York: Academic Press,
39.
Apical and periapical tissue reaction 237
Kilpatrick SJ. Statistical principles in the health care information. 2nd ed. Baltimore: University Park Press, 1977:l.
1979:128. Warfvinge J. Dental pulp inflammation: experimental studies in human and monkey teeth. Swed Dent J (Suppl) 1986;39: I 1L
Reprint requests: Elizeu A. Pascon, DDS, MSD Assistant Professor
I-JO.
Walton RE, Langeland K. Migration of materials in the den- tal pulp of monkeys. J Endod 1978;4:167-77. Nicolson WL. Application of statistical methods in quantita- tive microscopy. J Microscopy 1978;113:223-39.
Department of Restorative Dentistry and Endodontology School of Dental Medicine University of Connecticut Health Center Farmington, CT 06032
Related Documents











