Tintinalli's Emergency Medicine: A Comprehensive Study Guide, 7e > Chapter 25. Approach to the Patient in Shock FIGURE 25-1. Ronny M. Otero; H. Bryant Nguyen; Emanuel P. Rivers Epidemiology The exact number of cases of shock that present to the ED in the U.S. is difficult to ascertain due to the insensitivity of clinical parameters, current definitions, and lack of a central database repository. Previous estimates propose that approximately 1 million cases of shock are seen in the ED each year in the U.S. 1 These estimates are largely based upon the assumption that hypotension, defined as a systolic blood pressure <90 mm Hg is consistent with shock in adults. Based upon a low blood pressure, the incidence of hypotension that present to American EDs is approximately 5.6 million cases/year. 2 Mortality The mortality attributed to clinical shock varies depending on the inciting event. Septic shock has an estimated mortality of 40% to 60%. Cardiogenic shock has an estimated mortality of 36% to 56%. 3 Approximately 30% to 45% of patients with septic shock and 60% to 90% of patients with cardiogenic shock die within 1 month of presentation. 3,4 With a greater recognition and improved treatment, mortality from neurogenic shock has been reduced significantly. 5 The definition and treatment of shock continues to evolve, but the general approach to a patient in the initial stages of shock follows similar principles regardless of the inciting factors or etiology. Pathophysiology Shock is circulatory insufficiency that creates an imbalance between tissue oxygen supply (delivery) and oxygen demand (consumption). This physiologic state leads to a reduction in effective tissue perfusion with its attendant biochemical, bioenergetic, and subcellular sequelae. Reduction in effective perfusion can be global or local, and the result is suboptimal substrate use at the cellular or subcellular level. 6 Knowledge of the principles of oxygen delivery and consumption is important for understanding shock. Arterial oxygen content is the amount of oxygen bound to hemoglobin plus the amount dissolved in plasma. Oxygen is delivered to the tissues by the pumping function [cardiac output (CO)] of the heart. This is dependent upon the interplay of cardiac inotropy (speed and shortening capacity of myocardium), chronotropy (heart contraction rate), and lusitropy (ability to relax and fill heart chambers). Determinants of inotropy include autonomic input from sympathetic activation, parasympathetic inhibition, circulating catecholamines, and short-lived responses to an increase in afterload (Anrep effect) or heart rate (Bowditch effect). 7 Increases in inotropic state help to maintain stroke volume at high heart rates. 7 Under certain conditions, such as shock states, higher levels of epinephrine will be produced and reinforce adrenergic tone. Epinephrine levels are significantly elevated during induced hemorrhagic shock, then are subsequently reduced to almost normal levels after normal blood pressure is restored. 8 Furthermore, previous studies have also shown that an acidotic milieu as may be found in shock further compromises ventricular contractile force and blood pressure. 9 Both chronotropy and lusitropy are both influenced by sympathetic input. Norepinephrine interacts with cardiac β 1 -receptors, resulting in increased cyclic adenosine monophosphate. This leads to a process of intracellular signaling with an increased heart rate (chronotropy) and sequestration of calcium, leading to myocardial relaxation. 7 Systemic oxygen delivery (DO 2 ) is the product of the arterial oxygen content and CO (Tables 25-1 and 25-2). Systemic oxygen consumption (V̇ O 2 ) comprises a sensitive balance between supply and demand. Normally, the tissues consume approximately 25% of the oxygen carried on hemoglobin, and venous blood returning to the right heart is approximately 75% saturated [mixed venous oxygen saturation (pulmonary artery) (SmvO 2 )]. When oxygen supply is insufficient to meet demand, the first compensatory mechanism is an increase in CO. If the increase in CO is inadequate, the amount of oxygen extracted from hemoglobin by the tissues increases, which decreases SmvO 2 . See Chapter 20, Blood Gases. Table 25-1 Definitions of Abbreviations (a-v)CO 2 Arterial-central venous carbon dioxide difference CaO 2 Arterial oxygen content CmvO 2 Mixed venous oxygen content CI Cardiac index (cardiac output/body surface area) CO Cardiac output CPP Coronary perfusion pressure CVP Central venous pressure DO 2 Systemic oxygen delivery DBP Diastolic blood pressure Hb Hemoglobin MAP Mean arterial pressure MODS Multi-organ dysfunction syndrome OER Oxygen extraction ratio PaCO 2 Arterial carbon dioxide pressure http://accessmedicine.mhmedical.com.pbidi.unam.mx:8080/content.aspx... 1 de 13 07/03/2015 07:35 p. m.

Tintinalli shock.pdf
Oct 04, 2015
Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript
-
Tintinalli's Emergency Medicine: A Comprehensive Study Guide, 7e >
Chapter 25. Approach to the Patient inShock
FIGURE 25-1.Ronny M. Otero; H. Bryant Nguyen; Emanuel P. Rivers
EpidemiologyThe exact number of cases of shock that present to the ED in the U.S. is difficult to ascertain due to the insensitivity of clinical parameters, current definitions, and lack of a central
database repository. Previous estimates propose that approximately 1 million cases of shock are seen in the ED each year in the U.S.1 These estimates are largely based upon theassumption that hypotension, defined as a systolic blood pressure
-
PaO2 Arterial oxygen pressure
PAOP Pulmonary artery occlusion (wedge) pressure
SaO2 Arterial oxygen saturation
ScvO2 Central venous oxygen saturation
SmvO2 Mixed venous oxygen saturation (pulmonary artery)
SIRS Systemic inflammatory response syndrome
SVR Systemic vascular resistance
VO2 Systemic oxygen consumption
Table 25-2 Oxygen Transport and Utilization Components
Arterial oxygen content CaO2= 0.0031 PaO2+ 1.38 Hb SaO2
CaO2 is the amount of O2 within 100 mL blood. Oxygen is contained within blood in two forms: dissolved in plasma and chemically combined withhemoglobin. Assuming 15 grams hemoglobin per 100 mL blood and an oxygen saturation of 97%, the representative normal value of CaO2 is 20.1 mL/100mL blood (vol%).
Central venous/mixed venous oxygen saturation ScvO2 or SmvO2
SmvO2 reflects physiologic efforts to meet tissue O2 demands. Normal SmvO2 is 65% to 75%. When the SmvO2 falls below 50%, the bodys limits tocompensate have been reached and O2 availability for tissue metabolism will be compromised, leading to lactic acidosis.
Central venous/mixed venous oxygen content CmvO2 = 0.0031 PmvO2 + 1.38 Hb SmvO2
CmvO2 is the amount of oxygen content returning to the heart. Normal CmvO2 is 15 mL/100 mL blood (vol%).
Systemic oxygen extraction ratio (OER) OER = C(a-v)O2/ CaO2
The amount of O2 taken out of the blood by the tissues is the systemic OER. It is described as a percentage. Normal OER is about 25%. Lactic acidproduction, an indicator of anaerobic metabolism, usually accompanies an OER of >50%.
Oxygen delivery DO2= CO CaO2 10
DO2 is the amount of O2 delivered to the tissues per minute. Assuming a normal cardiac output of 5 L/min and a CaO2 of 20.1 (vol%), a normal value for O2delivery would be 1000 mL O2 per minute.
Oxygen consumption VO2 = CO Hb 1.38 (SaO2 SmvO2) 10
The amount of O2 consumed by tissues each minute is equal to the difference in O2 delivered to tissues and the O2 returning from tissues. The normal valueis about 250 mL O2 per minute. Note that this formula ignores the small contribution from dissolved oxygen.
Oxygen affinity
Shifts in the oxyhemoglobin dissociation curve affect the release of O2 in the peripheral circulation. Increased pH, decreased temperature, decreased carbondioxide concentration (PCO2), and decreases in 2,3-diphosphoglycerate levels all result in a shift of the oxyhemoglobin curve to the left. Thus, for anyparticular value of PaO2, the O2 saturation will be higher. This increased affinity of hemoglobin for O2 makes O2 loading easier, but release of O2 in theperipheral tissues is impaired. The reverse is true with a decreased pH, increased temperature, increased PCO2, and increased 2,3-diphosphoglycerate:there is a shift of the oxyhemoglobin dissociation curve to the right resulting in a decreased affinity of hemoglobin for O2.
Note: See Table 25-1 for abbreviation definitions.
When compensatory mechanisms fail to correct the imbalance between tissue supply and demand, anaerobic metabolism occurs, resulting in the formation of lactic acid. Lactic acid israpidly buffered, resulting in the formation of measured lactate. Normal lactate levels are 0.5 to 1.5 mmol/L. An elevated lactate level is often associated with decreased SmvO2. Mostcases of lactic acidosis are a result of inadequate oxygen delivery, but lactic acidosis occasionally can develop from an excessively high oxygen demand; for example, in statusepilepticus. In other cases, lactic acidosis occurs because tissue oxygen utilization is impaired. Examples of impaired tissue oxygen utilization include septic shock or thepostresuscitation phase of cardiac arrest, in which a normal SmvO2 and an elevated lactate may be encountered. Elevated lactate is a marker of impaired oxygen delivery and/orutilization and correlates with short-term prognosis of critically ill patients in the ED. SmvO2 can also be used as a measure of the balance between tissue oxygen supply and demand.SmvO2 is obtained from the pulmonary artery catheter, but similar information can be from central venous oxygen saturation (ScvO2). ScvO2 correlates well with SmvO2, and ScvO2 is
easier to obtain in the ED setting.10
Shock provokes a myriad of autonomic responses, many of which serve to maintain perfusion pressure to vital organs. Stimulation of the carotid baroreceptor stretch reflex activatesthe sympathetic nervous system leading to (1) arteriolar vasoconstriction, resulting in redistribution of blood flow from the skin, skeletal muscle, kidneys, and splanchnic viscera; (2) anincrease in heart rate and contractility that increases CO; (3) constriction of venous capacitance vessels, which augments venous return; (4) release of the vasoactive hormonesepinephrine, norepinephrine, dopamine, and cortisol to increase arteriolar and venous tone; and (5) release of antidiuretic hormone and activation of the renin-angiotensin axis toenhance water and sodium conservation to maintain intravascular volume.
http://accessmedicine.mhmedical.com.pbidi.unam.mx:8080/content.aspx...
2 de 13 07/03/2015 07:35 p. m.
-
These compensatory mechanisms attempt to maintain DO2 to the most critical organsthe heart and brainbut blood flow to other organs such as the kidneys and GI tract may becompromised.
The cellular response to decreased DO2 is adenosine triphosphate depletion, leading to ion-pump dysfunction, influx of sodium, efflux of potassium, and reduction in membrane restingpotential. As shock progresses, lysosomal enzymes are released into the cells with subsequent hydrolysis of membranes, deoxyribonucleic acid, ribonucleic acid, and phosphateesters. As the cascade of shock continues, the loss of cellular integrity and the breakdown in cellular homeostasis result in cellular death. These pathologic events give rise to themetabolic features of hemoconcentration, hyperkalemia, hyponatremia, prerenal azotemia, hyper- or hypoglycemia, and lactic acidosis.
In the early phases of septic shock, these physiologic changes produce a clinical syndrome called the systemic inflammatory response syndrome or SIRS (Table 25-3).
Table 25-3 Clinical Feature of Systemic Inflammatory Response Syndrome (SIRS)54
Two or more of the following features are required to make a diagnosis of SIRS:
Temperature >38C (100.4F) or 90 beats/min
Respiratory rate >20 breaths/min
White blood cell count >12.0 109/L, 10% immature forms or bands
Reproduced with permission from American College of Chest Physicians/Society of Critical Care Medicine consensus
conference: definitions for sepsis and organ failure and guidelines for the use of innovative therapies in sepsis. Crit Care
Med 20: 864, 1992.
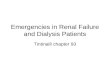
As SIRS progresses, shock ensues, followed by multi-organ dysfunction syndrome manifested by myocardial depression, adult respiratory distress syndrome, disseminatedintravascular coagulation, hepatic failure, or renal failure. The fulminant progression from SIRS to multi-organ dysfunction syndrome is determined by the balance ofanti-inflammatory and proinflammatory mediators or cytokines that are released from endothelial cell disruption11 (Figure 25-1).
FIGURE 25-1.
The pathophysiology of shock, systemic inflammatory response syndrome (SIRS), and multi-organ dysfunction syndrome (MODS).
Clinical Features
http://accessmedicine.mhmedical.com.pbidi.unam.mx:8080/content.aspx...
3 de 13 07/03/2015 07:35 p. m.
-
History and Comorbidities
Often, the presence of shock and the underlying cause will be quite apparentsuch as acute myocardial infarction, anaphylaxis, or hemorrhage. Some patients may be in shock withfew symptoms other than generalized weakness, lethargy, or altered mental status. Symptoms that suggest volume depletion include bleeding, vomiting, diarrhea, excessive urination,insensible losses because of fever, or orthostatic light-headedness. Ask about a history of cardiovascular disease, episodes of chest pain, or symptoms of congestive heart failure.Underlying neurologic disease can render patients more susceptible to complications from hypovolemia. Consider the possibility of an anaphylactic reaction to a new medication orcardiovascular depression from a drug. Some medications can cause volume depletion (e.g., diuretics) and others depress myocardial contractility (e.g., -blockers and calciumchannel blockers).
Physical Examination
Shock is usually, but not always, associated with systemic arterial hypotensionsystolic blood pressure 1.0) indicates an impaired left ventricular function(as a result of blood loss and/or cardiac depression) and carries a high mortality rate.13
Central nervoussystem
Acute delirium or brain failure, restlessness, disorientation, confusion, and coma secondary to decrease in cerebral perfusion pressure(mean arterial pressure intracranial pressure). Patients with chronic hypertension may be symptomatic at normal blood pressures.
Skin Pallor, pale, dusky, clammy, cyanosis, sweating, altered temperature, and decreased capillary refill.
CardiovascularNeck vein distention or flattening, tachycardia, and arrhythmias. An S3 may result from high-output states. Decreased coronaryperfusion pressures can lead to ischemia, decreased ventricular compliance, increased left ventricular diastolic pressure, andpulmonary edema.
Respiratory Tachypnea, increased minute ventilation, increased dead space, bronchospasm, hypocapnia with progression to respiratory failure,and adult respiratory distress syndrome.
Splanchnic organs Ileus, GI bleeding, pancreatitis, acalculous cholecystitis, and mesenteric ischemia can occur from low flow states.
Renal Reduced glomerular filtration rate, renal blood flow redistributes from the renal cortex toward the renal medulla leading to oliguria.Paradoxical polyuria can occur in sepsis, which may be confused with adequate hydration status.
Metabolic Respiratory alkalosis is the first acid-base abnormality. As shock progresses, metabolic acidosis occurs. Hyperglycemia,hypoglycemia, and hyperkalemia.
Diagnosis
http://accessmedicine.mhmedical.com.pbidi.unam.mx:8080/content.aspx...
4 de 13 07/03/2015 07:35 p. m.
-
Clinical Criteria
The result of shock is global tissue hypoperfusion and is associated with a decreased venous oxygen content and metabolic acidosis (lactic acidosis). Shock is classified into fourcategories by etiology (Table 25-5). Clinically, shock usually presents with signs and symptoms of hypovolemia, but as the shock state persists or progresses to irreversible end-organdamage, other pathophysiologic mechanisms become operative.15
Table 25-5 Classification of Shock
Type Comment
Hypovolemic Caused by inadequate circulating volume
Cardiogenic Caused by inadequate cardiac pump function
Obstructive Caused by extra cardiac obstruction to blood flow
Distributive Metabolic derangements that impair cellular respiration such as cyanide toxicity, sepsis.
Laboratory Evaluation
The clinical presentation and the presumptive etiology of shock dictate the use of ancillary studies. A battery of standard hematologic, coagulation, and biochemical tests usuallyprovides an assessment of the patients general physiologic condition and occasionally detects an abnormality that requires specific treatment (Table 25-6). A wide range of laboratoryabnormalities may be encountered in shock, but most abnormal values merely point to the particular organ system that is either contributing to, or being affected by, the shock state.No single laboratory value is sensitive or specific for shock.
Table 25-6 Ancillary Studies in Shock
Basic evaluation
Complete blood count: white blood cell count and differential, hemoglobin and hematocrit, platelet count
Electrolytes, glucose, calcium, magnesium, phosphorus
Blood urea nitrogen, creatinine
Prothrombin time, partial thromboplastin time
Urinalysis
Chest radiograph
ECG
Moderate physiologic assessment
Arterial blood gas (measured oxygen saturation)
Serum lactate
Fibrinogen, fibrin split products, D-dimer
Hepatic function panel
Noninvasive hemodynamic assessment
End-tidal CO2
Noninvasive cardiac output measurement
Echocardiogram
Invasive hemodynamic assessment
Filling pressures: CVP, PAOP
Cardiac output
Central venous oxygen saturation ScvO2
Calculation of hemodynamic values: SVR, CO, DO2, VO2
As clinically indicated to define etiology or detect complications
Blood, sputum, urine, and pelvic cultures
CT of head and sinuses
Lumbar puncture
http://accessmedicine.mhmedical.com.pbidi.unam.mx:8080/content.aspx...
5 de 13 07/03/2015 07:35 p. m.
-
Culture suspicious wounds
Cortisol level
Pregnancy test
Acute abdominal series
Abdominal or pelvic US
Abdominal or pelvic CT
Note: See Table 25-1 for abbreviation definitions.
Imaging
Chest X-Ray
The portable anteroposterior-view chest roentgenogram (CXR) is often used in the evaluation of unstable patients to avoid transporting the patient during resuscitation. The CXR can
shed light on the etiology of shock and may aid in assessment of volume status in the critically ill.16 However, the accuracy of determining volume status is 70% compared withpulmonary artery occlusion pressure >18 mm Hg. The likelihood ratio of CXR determining volume status using objective vascular pedicle width and cardiothoracic ratio is 3.1 [95% CI
(1.9% to 6.0%)].17
US
The use of ultrasonography in the assessment of patients with suspected shock manifesting as symptomatic hypotension has been advocated.18
US evaluation can help narrow diagnostic considerations.18 The following are helpful in this assessment: subcostal cardiac view, inferior vena cava view, parasternal long-axis cardiac
view, apical four-chamber cardiac view, right upper quadrant abdominal view, pelvic view, and abdominal aorta view.18 Emergency physician determination of left ventricular function
can be comparable to the assessment performed by a cardiologist in hypotensive patients.19
Hemodynamic MonitoringHemodynamic monitoring helps assess the severity of shock and the response to treatment. Monitoring capabilities vary from institution to institution, but if possible should includepulse oximetry, electrocardiographic monitoring, continuous noninvasive but preferably intra-arterial blood pressure monitoring, end-tidal CO2 monitoring, and central venous pressure
(CVP) and ScvO2 monitoring.20 Average access time, number of attempts, and mechanical complications are reduced when an US-assisted approach to central access is
used.21Figure 25-1 outlines a systematic approach to the evaluation of the patient in shock.
Treatment
Early Intervention
The benefit of timely ED intervention in nontraumatic critical illness is significant. Comprehensive and timely ED care can significantly decrease the predicted mortality of critically ill
patients in as little as 6 hours of treatment.22,23 Application of an algorithmic approach to optimize hemodynamic end points with early goal-directed therapy in the ED reduces
mortality by 16% in patients with severe sepsis or septic shock.23 Early goal-directed therapy has been validated in both septic and nonseptic populations.24 The ABCDE tenets ofshock resuscitation are establishing Airway, controlling the work of Breathing, optimizing the Circulation, assuring adequate oxygen Delivery, and achieving End points of resuscitation.
Establishing Airway
Airway control is best obtained through endotracheal intubation for airway protection, positive pressure ventilation (oxygenation), and pulmonary toilet. Sedatives used to facilitateintubation may cause arterial vasodilatation, venodilation, and myocardial suppression and result in hypotension. Positive pressure ventilation reduces preload and CO. Thecombination of sedative agents and positive pressure ventilation can lead to hemodynamic collapse. Consider volume resuscitation or application of vasoactive agents beforeintubation and positive pressure ventilation.
Controlling the Work of Breathing
Control of breathing is required when tachypnea accompanies shock. Respiratory muscles are significant consumers of oxygen during shock and contribute to lactate production.Mechanical ventilation and sedation allow for adequate oxygenation, improvement of hypercapnia, and assisted, controlled, synchronized ventilationall of which decrease the work ofbreathing and improve survival. Arterial oxygen saturation should be restored to >93% and ventilation controlled to maintain a PaCO2 of 35 to 40 mm Hg. Normalizing pHabove 7.3 by hyperventilation is not beneficial. Neuromuscular blocking agents should be considered to further decrease respiratory muscle oxygen consumption and preserve DO2 tovital organs.
Optimizing the Circulation
Circulatory or hemodynamic stabilization begins with intravascular access through large-bore peripheral venous lines. The Trendelenburg position does not improve cardiopulmonaryperformance compared with the supine position. It may worsen pulmonary gas exchange and predispose to aspiration. Passive leg raising above the level of the heart with the patient
supine25 can be effective. If passive leg raising results in an increase in blood pressure or CO, fluid resuscitation will be helpful.25
Central venous access aids in assessing volume status (preload) and monitoring ScvO2. It is the preferred route for the long-term administration of vasopressor therapy and providesrapid access to the heart if pacemaker placement is required.
Fluid resuscitation begins with isotonic crystalloid. The amount and rate of infusion are determined by an estimate of the hemodynamic abnormality. Most patients in shock have eitheran absolute or relative volume deficit. The exception is the patient in cardiogenic shock with pulmonary edema. Administer fluid rapidly, in set quantities of 500 or 1000 mL normalsaline, and reassess the patient after each bolus. Patients with a modest degree of hypovolemia usually require an initial 20 mL/kg of isotonic crystalloid. More fluids are needed forprofound volume deficits.
http://accessmedicine.mhmedical.com.pbidi.unam.mx:8080/content.aspx...
6 de 13 07/03/2015 07:35 p. m.
-
Vasopressor agents are used when there has been an inadequate response to volume resuscitation or if there are contraindications to volume infusion.26 Vasopressors are mosteffective when the vascular space is full and least effective when the vascular space is depleted. However, vasopressors may be necessary early in the treatment of shock, beforevolume resuscitation is complete, to prevent potentially lethal consequences of prolonged systemic arterial hypotension. This is especially important in elderly patients with significantcoronary and cerebrovascular disease. Rapidly restoring the MAP (Formula 25-2) to 60 mm Hg or systolic pressure to 90 mm Hg may avoid the coronary and cerebral complicationsof decreased blood flow.
Formula 25-2
Diastolic blood pressure + [pulse pressure/3]
Mean arterial blood pressure (maintain 60 mm Hg or higher).
Vasopressor agents have variable effects on the -adrenergic, -adrenergic, and dopaminergic receptors (Table 25-7). Although vasopressors improve perfusion pressure in the largevessels, they may decrease capillary blood flow in certain tissue beds, especially the GI tract. Vasopressors will falsely elevate intracardiac filling pressures (i.e., CVP). If multiplevasopressors are used, they should be simplified as soon as the best therapeutic agent is identified.
Table 25-7 Commonly Used Vasoactive Agents
Drug Dose (Mixture)* Action CardiacStimulation Vasoconstriction VasodilationCardiacOutput
Side Effects andComments
Dopamine
0.525.0micrograms/kg/min(400milligrams/250 mL)
, , anddopaminergic
++ at 510micrograms/kg/min
++ at 10micrograms/kg/min
+ at 0.55.0micrograms/kg/min
Usuallyincreases
Tachydysrhythmias;increasesmyocardial O2consumption; acerebral,mesenteric,coronary, and renalvasodilator at lowdoses
Norepinephrine212micrograms/min (4milligrams/250 mL)
Primarily 1,some 1
++ ++++ 0 Slightdecrease
Dose-related, reflexbradycardia; usefulwhen loss of venoustone predominates;spares the coronarycirculation
Phenylephrine
100200micrograms/min,taper as drugtakes effect (10milligrams/250 mL)
Pure 0 ++++ 0 Decrease
Reflex bradycardia,headache,restlessness,excitability, rarelyarrhythmias; idealfor patients in shockwith tachycardia orsupraventriculararrhythmias
Ephedrine
5- to 25-milligramIV bolus; mayrepeat at 5- to10-min intervals upto 150 mg in 24 h
and +++ ++ + Increases
Causes palpitations,hypertension,cardiac arrhythmias;an indirect-actingcentral nervoussystem stimulant;limited long-termvalue as therapy forshock
Vasopressin0.010.04units/min (200units/250 mL)
++++
Primarilyvasoconstriction;outcome data fromits use are lacking;infusions of 0.04unit/min may lead toadverse,vasoconstriction-mediated events
Epinephrine210micrograms/min (4milligrams/250 mL)
and ++++ at 0.030.15micrograms/kg/min++++ at 0.150.30micrograms/kg/min +++ Increases
Causestachydysrhythmia,leukocytosis;increasesmyocardial oxygenconsumption
Dobutamine
2.020.0micrograms/kg/min(250milligrams/250 mL)
1, some 2and 1 inlargedosages
++++ + ++ Increase
Causestachydysrhythmia,occasional GIdistress, increases
http://accessmedicine.mhmedical.com.pbidi.unam.mx:8080/content.aspx...
7 de 13 07/03/2015 07:35 p. m.
-
Drug Dose (Mixture)* Action CardiacStimulation Vasoconstriction VasodilationCardiacOutput
Side Effects andComments
myocardial oxygenconsumption,hypotension involume depletedpatient; has lessperipheralvasoconstrictionthan dopamine; cancause fewerarrhythmias thanisoproterenol
Isoproterenol
0.010.05micrograms/kg/min(1 milligram/250mL)
1 and some2
++++ 0 ++++ Increases
Causestachydysrhythmia,facial flushing,hypotension inhypovolemicpatients; increasesmyocardial oxygenconsumption; neveruse alone in shock
Note: 0 = no effect; + = mild effect; ++ = moderate effect; +++ = marked effect; ++++ = very marked effect.
*Individual drugs may be diluted in 5%dextrose in water or normal saline, and may be diluted in larger volumes or
concentrated into smaller volumes according to the fluid needs of the individual patient.
Assuring Adequate Oxygen Delivery
Once blood pressure is stabilized through optimization of preload and afterload, DO2 can be assessed and further manipulated. Restore arterial oxygen saturation to physiologic 93%
to 95%. In shock state, transfusion of packed red blood cells should be considered to maintain hemoglobin 10 grams/dL.26 If CO can be assessed, it should be increased usingvolume infusion and inotropic agents in incremental amounts until venous oxygen saturation (SmvO2 or ScvO2) and lactate are normalized.
Control of VO2 is important in restoring the balance of oxygen supply and demand to tissues. A hyperadrenergic state results from the compensatory response to shock, physiologicstress, pain, and anxiety. Shivering frequently results when a patient is unclothed for examination and then left inadequately covered in a cold resuscitation room. The combination ofthese variables increases systemic oxygen consumption. Pain further suppresses myocardial function, thus impairing DO2 and VO2. Providing analgesia, muscle relaxation, warmcovering, anxiolytics, and even paralytic agents, when appropriate, decreases this inappropriate VO2.
Tissue oxygen extraction assesses adequacy of the resuscitation in meeting the oxygen needs of the tissues. Sequential examination of lactate and SmvO2 or ScvO2 is a method to
assess adequacy of tissue oxygen extraction. Continuous measurement of SmvO2 or ScvO2 through fiberoptic technology can be used in the ED.10 A variety of technologic tools may
be used to assess tissue perfusion during resuscitation.2636 The advantages and disadvantages of these measures are summarized in Table 25-8.
Table 25-8 Tools for Hemodynamic Monitoring
Tool Comments
Invasive blood pressure monitoring
Intra-arterial pressure measurement is preferable because vasoactive drugs may cause rapid swings in bloodpressure, and multiple blood samplings will typically be required.
Radial artery pressure may underestimate central pressure in hypotensive septic patients receiving high-dosevasopressor therapy and may lead to excessive vasopressor administration.27
Pulse pressure variation and pulsecontour analysis of stroke volumevariation
Measures of stroke volume variation using arterial pulse contour analysis estimates cardiac output and candemonstrate fluid responsiveness if cardiac output increases after volume loading during positive pressureventilation.29
CVP
May not reliably reflect the left ventricular filling pressure in clinical states that produce pulmonary hypertensionor compliance changes in the right or left heart.
Common iliac venous pressure can approximate CVP.30
Static measures of fluid responsiveness
Central venous or right atrial pressure, wedge, or pulmonary artery occlusion pressure, right ventricularend-diastolic volume index, left ventricular end-diastolic area, global end-diastolic volume, and intrathoracic bloodvolume.
One of the disadvantages of this diagnostic approach in unstable patients is that it is definitive in only 50% ofsuch patients.20,28
http://accessmedicine.mhmedical.com.pbidi.unam.mx:8080/content.aspx...
8 de 13 07/03/2015 07:35 p. m.
-
Tool Comments
Central and mixed venous oximetry(ScvO2 and SmvO2)
ScvO2 closely approximates mixed venous O2 saturation (SmvO2) and can be monitored continuously usinginfrared oximetry.
Enables the clinician to detect clinically unrecognized global hypoperfusion in the treatment of myocardialinfarction, general medical shock, trauma, hemorrhage, septic, hypovolemic, end-stage heart failure, cardiogenicshock during and after cardiopulmonary arrest.10
Systemic arterial-venous CO2 difference
Increased arterial-mixed venous carbon dioxide gradients or (a-v)CO2 are seen in acute circulatory failure, andinversely correlate with the cardiac index.
Central venous and pulmonary artery CO2 values can be interchanged to determine cardiac index.31
Gastric tonometry and sublingualcapnography
Serial measurements of gastric and sublingual mucosal blood flow are based on hydrogen ion diffusion and CO2elimination.
Inadequate visceral perfusion as evidenced by persistently low intramucosal pH or increased sublingual CO2concentration after resuscitation is associated with subsequent organ dysfunction and death.32,33
Pulmonary artery catheterization
Can measure left-sided heart filling, pulmonary artery occlusion pressure, cardiac output, and mixed venousoxygen saturation.
Enables calculation of hemodynamic and oxygen transport variables.
Special catheters can measure right ventricular end-diastolic volume index calculated from right ventricularejection fraction.
US and echocardiography
Intracardiac, vena caval diameters, left ventricular end-diastolic area after a fluid challenge or passive leg raisingmay be used to assess volume status.
Controlled-compression sonography measures venous pressure in peripheral veins and allows reliable indirectassessment of CVP.
US can also be used to assist in line placement.19,21
Noninvasive cardiac outputCardiac output can be measured by pulse pressure variation, pulse contour analysis, transesophageal Doppler(esophageal Doppler monitor), thoracic cutaneous bioimpedance, lithium dilution, or transpulmonarythermodilution.34
NIRS
Patients with severe sepsis have lower StO2; StO2 recovery slope, tissue hemoglobin index, and total tissuehemoglobin increase on venous occlusion.
Patients with severe sepsis had longer StO2 recovery times and lower NIRS-derived local oxygen consumption
values versus healthy volunteers.35
Orthogonal polarization spectral
Disordered microcirculatory flow is associated with systemic inflammation, acute organ dysfunction, andincreased mortality.
New technologies that directly image microcirculatory blood flow will help define the role of microcirculatorydysfunction in oxygen transport and circulatory support in severe sepsis.36
Abbreviations: CVP = central venous pressure; NIRS = near-infrared spectroscopy; StO2 = tissue oxygen saturation.
End Points of Resuscitation
The goal of resuscitation is to maximize survival and minimize morbidity using objective hemodynamic and physiologic values to guide therapy. No therapeutic end point is universally
effective, and only a few have been tested in prospective trials, with mixed results.37 Hypotension at ED presentation is associated with poor outcomes.38 Noninvasive parameters,such as blood pressure, heart rate, and urine output, may underestimate the degree of remaining hypoperfusion and oxygen debt, so use of additional physiologic end points may be
informative (Table 25-8).37,39,40 A goal-directed approach of urine output >0.5 mL/kg/h, CVP 8 to12 mm Hg, MAP 65 to 90 mm Hg, and ScvO2 >70% during ED resuscitation
of septic shock significantly decreases mortality.23
Troubleshooting a Persistently Hypotensive Patient
Table 25-9 lists important issues to consider if hypotension and shock persist.
Table 25-9 Troubleshooting Persistent Shock or Hypotension
Equipment and monitoring
Is the patient appropriately monitored?20
Has the early use of vasopressors falsely elevated the central venous pressure and masked persistent hypovolemia?
http://accessmedicine.mhmedical.com.pbidi.unam.mx:8080/content.aspx...
9 de 13 07/03/2015 07:35 p. m.
-
Is there an equipment malfunction, such as dampening of the arterial line or disconnection from the transducer?
Is the IV tubing into which the vasopressors are running connected appropriately?
Are the vasopressor infusion pumps working?
Are the vasopressors mixed adequately and in the correct dose?
Patient assessment
Do mentation and clinical appearance match the degree of hypotension?
Is the patient adequately volume resuscitated?
Does the patient have a pneumothorax after placement of central venous access?
Has the patient been adequately assessed for an occult penetrating injury (a bullet hole or stab wound)?
Is there hidden bleeding from a ruptured spleen, large vessel aneurysm, or ectopic pregnancy?
Does the patient have adrenal insufficiency? The incidence of adrenal dysfunction can be as high as 30% in this subset of patients.55
Is the patient allergic to the medication just given or taken before arrival?
Is there cardiac tamponade in the dialysis patient or cancer patient?
Is there associated acute myocardial infarction, aortic dissection, or pulmonary embolus?
Controversies of Treatment
Fluid Therapy
Rapid restoration of fluid deficits modulates inflammation and decreases the need for subsequent vasopressor therapy, steroid administration, and invasive monitoring (pulmonary
artery catheterization and arterial line placement) if the condition progresses to shock.26,30 Although there is general agreement that volume therapy is an integral component of earlyresuscitation, there is a lack of consensus for the type of fluid, standards of volume assessment, and end points. Table 25-10 compares the most commonly used fluid therapies.
Table 25-10 Fluid Therapy
Fluid Comments
Crystalloids
NSSlightly hyperosmolar solution containing 154 mEq/L of both sodium and chloride.
Risk of inducing hyperchloremic metabolic acidosis when given in large amounts due to relatively high chloride concentration.42
LR
Lactate can accept a proton and subsequently be metabolized to CO2 and water by liver, leading to release of CO2 in the lungs andexcretion of water by the kidneys. LR results in a buffering of the acidemia that is advantageous over NS.
Risk of inducing hyperkalemia in patients with renal insufficiency or renal failure due to small potassium content (very small amount).
D-isomer of LR causes immune activation and induction of cellular injury. Replacement of the lactate with ethyl pyruvate or-hydroxybutyrate or using only the L-isomer of lactate in Ringers solution decreases this adverse effect.42,43
Colloids
Albumin
Derived from human plasma.
Available in varying strengths from 4% to 25%.
The Saline versus Albumin Fluid Evaluation (SAFE) study compared fluid resuscitation with albumin or saline on mortality and found similar28-day mortalities and secondary outcomes in each arm. However, a subset analysis of septic patients resuscitated with albumin showed adecrease in mortality, although statistically it was insignificant. There was an increase in mortality in trauma patients complicated by headinjury.44
Hydroxyethylstarch
Hydroxyethyl starch should be avoided in sepsis.4547
Synthetic colloid derived from hydrolyzed amylopectin.
Many harmful effects: renal impairment at recommended doses and impairing long-term survival at high doses,45 coagulopathy andbleeding complications from reduced Factor VIII and von Willebrand factor levels, impaired platelet function.
DextranArtificial colloids/glucose polymers synthesized by Leuconostoc mesenteroides bacteria grown in sucrose media.
Used to lower blood viscosity.
http://accessmedicine.mhmedical.com.pbidi.unam.mx:8080/content.aspx...
10 de 13 07/03/2015 07:35 p. m.
-
Fluid Comments
Can cause renal dysfunction, anaphylactoid reactions.
Gelatin
Produced from bovine collagen.
Small molecular weight limits effectiveness of plasma volume expansion.
Less expensive than other plasma volume expanders.41,42,46
Can cause renal impairment, allergic reactions.
Not currently available in the U.S.
Abbreviations: LR = lactated Ringers solution; NS =normal saline.
Colloids are high-molecular-weight solutions that increase plasma oncotic pressure. Colloids can be classified as either natural (albumin) or artificial (starches, dextrans, and gelatins).Due to their higher molecular weight, colloids stay in the intravascular space significantly longer than crystalloids. The intravascular half-life of albumin is 16 hours versus 30 to 60
minutes for normal saline and lactated Ringers solution.4144 Resuscitation with crystalloids requires two to four times more volume than colloids.41 The outcome advantage
between crystalloid and colloids continues to remain unresolved in sepsis.4148
The issue of liberal versus conservative fluid resuscitation in the face of lung injury is also unsettled.4951 The Fluids and Catheters Treatment Trial demonstrated no difference in60-day mortality between the two strategies but did reveal significantly improved lung and central nervous system function and a decreased need for sedation, mechanical ventilation,
and intensive care unit care in patients who received conservative fluid resuscitation.52 Other trials comparing early liberal fluid resuscitation strategy with more conservative strategies
failed to demonstrate an increased need for mechanical ventilation.49
Bicarbonate Use in Shock
Bicarbonate administration shifts the oxygen-hemoglobin dissociation curve to the left, impairs tissue unloading of hemoglobin-bound oxygen, and may worsen intracellular acidosis.There is no evidence that bicarbonate administration reverses myocardial depression or improves sensitivity to endogenous catecholamines.
Many clinicians remain uncomfortable withholding bicarbonate if metabolic acidosis is severe. A compromise position is to partially correct the metabolic acidosis over time, asillustrated in Formula 25-3. Correct only to arterial pH 7.25.
Formula 25-3
1. Calculate the bicarbonate deficit.
[(normal HCO3 the patients HCO3) 0.5 body weight (kg)]
2. Slowly infuse one half of the calculated deficit.
3. Infuse the remainder over 6 to 8 hours.
4. Stop bicarbonate when arterial pH = 7.25.
1.
Slow and partial correction of metabolic acidosis with HCO3.
Disposition and Transition to the Intensive Care UnitDocument and communicate all steps of ED resuscitation to the critical-care team. Even when resuscitation is systematic and thoughtful, miscommunication can undo the benefits ofinitial ED treatment. Ideally, verbally communicate and document a system-oriented problem list with an assessment and plan, including all procedures and complications, before
transfer. For prolonged or boarded ED stays, provide appropriately timed notations regarding patient status, diagnostic and therapeutic interventions, and sentinel events.22
PrognosisSome clinical variables are associated with poor outcome, such as severity of shock, temporal duration, underlying cause, preexisting vital organ dysfunction, and reversibility. Direct
noninvasive measurement of VO2 is predictive of outcome in patients who developed cardiogenic shock secondary to myocardial infarction and after cardiac arrest.10 Persistent
elevated lactate levels are prognostic in trauma, septic shock, and after cardiac arrest.12 Base deficit is also correlated with the development of multisystem organ failure in trauma.36
Outcome predictions using physiologic scoring systems in the ED are still being studied.53
References1. McCaig LF, Ly N: National hospital ambulatory medical care survey: 2000 emergency department summary. Adv Data 326: 1, 2002.2. Nawar EW, Niska RW, Xu J: National Hospital Ambulatory Medical Care Survey: 2005 emergency department summary. Adv Data 386: 1, 2007. [PubMed: 17703794]3. Moscucci M, Bates ER: Cardiogenic shock. Cardiol Clin 13: 391, 1995. [PubMed: 7585775]4. Angus DC, Linde-Zwirble WT, Lidicker J, et al: Epidemiology of severe sepsis in the United States: analysis of incidence, outcome, and associated costs of care. Crit Care Med 29:1303, 2001. [PubMed: 11445675]5. Stevens RD, Bhardwaj A, Kirsch JR, Mirski MA: Critical care and perioperative management in traumatic spinal cord injury. J Neurosurg Anesthesiol 15: 215, 2003. [PubMed:12826969]6. Kumar A, Parillo JE: Shock: Classification, Pathophysiology, and Approach to Management in Critical Care Medicine: Principles of Diagnosis and Management in the Adult 3rd ed.Philadelphia, PA, Mosby Inc., p. 379, 2008.7. Opie LH: Mechanisms of cardiac contraction and relaxation, in Braunwalds E, Libby P, Bonow RO, et al: Heart Disease: A Textbook of Cardiovascular Medicine, 8th ed.Philadelphia, PA, Saunders Elsevier, p. 530, 2008.8. Greever CJ, Watts DT: Epinephrine levels in the peripheral blood during irreversible hemorrhagic shock in dogs. Circ Res 7: 192, 1959. [PubMed: 13629815]9. Thrower WB, Darby TD, Aldinger EE: Acid base derangements and myocardial contractility. Arch Surg 82: 56, 1961. [PubMed: 13776757]
http://accessmedicine.mhmedical.com.pbidi.unam.mx:8080/content.aspx...
11 de 13 07/03/2015 07:35 p. m.
-
Copyright McGraw-Hill GlobalEducation Holdings, LLC.
All rights reserved.
10. Rivers EP, Ander DS, Powell D: Central venous oxygen saturation monitoring in the critically ill patient. Curr Opin Crit Care 7: 204, 2001. [PubMed: 11436529]11. Karimova A, Pinsky DJ: The endothelial response to oxygen deprivation: biology and clinical implications. Intensive Care Med 27: 19, 2001. [PubMed: 11280633]12. Rady MY, Rivers EP, Nowak RM: Resuscitation of the critically ill in the ED: responses of blood pressure, heart rate, shock index, central venous oxygen saturation and lactate.Ann Emerg Med 14: 218, 1996. [PubMed: 8924150]13. Rady MY, Nightingale P, Little RA, et al: Shock index: a re-evaluation in acute circulatory failure. Resuscitation 23: 227, 1992. [PubMed: 1321482]14. Birkhahn RH, Gaeta TJ, Terry D, et al. Shock index in diagnosing early acute hypovolemia. Am J Emerg Med 23: 323, 2005. [PubMed: 15915406]15. Nguyen HB, Rivers EP, Havstad S, et al: Critical care in the emergency department: a physiologic assessment and outcome evaluation. Acad Emerg Med 7: 1354, 2000.[PubMed: 11099425]16. Miller RR, Ely EW: Radiographic measures of intravascular volume status: the role of vascular pedicle width. Curr Opin Crit Care 12: 255, 2006. [PubMed: 16672786]17. Ely EW, Smith AC, Chiles C, et al: Radiologic determination of intravascular volume status using portable, digital chest radiography: a prospective investigation in 100 patients. CritCare Med 29: 1502, 2001. [PubMed: 11505116]18. Jones AE, Tayal VS, Sullivan DM, et al: Randomized controlled trial of immediate versus delayed goal-directed ultrasound to identify the cause of nontraumatic hypotension inemergency department patients. Crit Care Med 32: 1703, 2004. [PubMed: 15286547]19. Moore CL, Rose GA, Tayal VS, et al: Determination of left ventricular function by emergency physician echocardiography of hypotensive patients. Acad Emerg Med 9: 186, 2002.[PubMed: 11874773]20. Boldt J: Clinical review: hemodynamic monitoring in the intensive care unit. Crit Care 6: 52, 2002. [PubMed: 11940266]21. Karakitsos D, Labropoulos N, DeGroot E, et al: Real-time ultrasound-guided catheterisation of the internal jugular vein: a prospective comparison with the landmark technique incritical care patients. Crit Care 10: R162, 2006.22. Institute Of Medicine: IOM report: the future of emergency care in the United States health system. Acad Emerg Med 13: 1081, 2006.23. Rivers E, Nguyen B, Havstad S, et al: Early goal-directed therapy in the treatment of severe sepsis and septic shock. N Engl J Med 345: 1368, 2001. [PubMed: 11794169]24. Sebat F, Musthafa AA, Johnson D, et al: Effect of a rapid response system for patients in shock on time to treatment and mortality during 5 years. Crit Care Med 35: 2568, 2007.[PubMed: 17901831]25. Monnet X, Rienzo M, Osman D, et al: Passive leg raising predicts fluid responsiveness in critically ill patients. Crit Care Med 34: 1402, 2006. [PubMed: 16540963]26. Dellinger RP, Levy MM, Carlet JM, et al: Surviving Sepsis Campaign: international guidelines for management of severe sepsis and septic shock: Crit Care Med 36: 296, 2008.[PubMed: 18158437]27. Dorman T, Breslow MJ, Lipsett PA, et al: Radial artery pressure monitoring underestimates central arterial pressure during vasopressor therapy in critically ill surgical patients. CritCare Med 26: 1646, 1998. [PubMed: 9781720]28. Pinsky MR, Payen D: Functional hemodynamic monitoring. Crit Care 9: 566, 2005. [PubMed: 16356240]29. Michard F, Lopes M, Auler JO: Pulse pressure variation: beyond the fluid management of patients with shock. Crit Care 11: 131, 2007. [PubMed: 17521454]30. Packman MI, Rackow EC: Optimum left heart filling pressure during fluid resuscitation of patients with hypovolemic and septic shock. Crit Care Med 11: 165, 1983. [PubMed:6831886]31. Cuschieri J, Rivers EP, Donnino MW, et al: Central venous-arterial carbon dioxide difference as an indicator of cardiac index. Intensive Care Med 31: 818, 2005. [PubMed:15803301]32. Weil MH, Nakagawa Y, Tang W, et al: Sublingual capnometry: a new noninvasive measurement for diagnosis and quantitation of severity of circulatory shock. Crit Care Med 27:1225, 1999. [PubMed: 10446813]33. Marik PE: Regional carbon dioxide monitoring to assess the adequacy of tissue perfusion. Curr Opin Crit Care 11: 245, 2005. [PubMed: 15928474]34. Prentice D, Sona C: Esophageal Doppler monitoring for hemodynamic assessment. Crit Care Nurs Clin North Am 18: 189, x, 2006.35. Skarda DE, Mulier KE, Myers DE, et al: Dynamic near-infrared spectroscopy measurements in patients with severe sepsis. Shock 27: 348, 2007. [PubMed: 17414414]36. Verdant C, De Backer D: How monitoring of the microcirculation may help us at the bedside. Curr Opin Crit Care 11: 240, 2005. [PubMed: 15928473]37. Porter JM, Ivatury RR: In search of the optimal end points of resuscitation in trauma patients: a review. J Trauma 44: 908, 1998. [PubMed: 9603098]38. Jones SE, Stiell IG, Nesbitt LP, et al: Nontraumatic out-of-hospital hypotension predicts inhospital mortality. Ann Emerg Med 43: 106, 2004. [PubMed: 14707949]39. Rutherford EJ, Morris JA Jr, Reed GW, Hall KS: Base deficit stratifies mortality and determines therapy. J Trauma 33: 417, 1992. [PubMed: 1404512]40. Lind L: Veno-arterial carbon dioxide and pH gradients and survival in critical illness. Eur J Clin Invest 25: 201, 1995. [PubMed: 7781668]41. American Thoracic Society: Evidence-based colloid use in the critically ill: American Thoracic Society Consensus Statement. Am J Respir Crit Care Med 170: 1247, 2004.42. Rackow EC, Falk JL, Fein IA, et al: Fluid resuscitation in circulatory shock: a comparison of the cardiorespiratory effects of albumin, hetastarch, and saline solutions in patients withhypovolemic and septic shock. Crit Care Med 11: 839, 1983. [PubMed: 6194934]43. Vincent JL, Gerlach H: Fluid resuscitation in severe sepsis and septic shock: an evidence-based review. Crit Care Med 32: S451, 2004.44. Finfer S, Bellomo R, Boyce N, et al: A comparison of albumin and saline for fluid resuscitation in the intensive care unit. N Engl J Med 350: 2247, 2004. [PubMed: 15163774]45. Brunkhorst FM, Engel C, Bloos F, et al: Intensive insulin therapy and pentastarch resuscitation in severe sepsis. N Engl J Med 358: 125, 2008. [PubMed: 18184958]46. Wiedermann CJ: Systematic review of randomized clinical trials on the use of hydroxyethyl starch for fluid management in sepsis. BMC Emerg Med 8: 1, 2008. [PubMed:18218122]47. Sriskandan S, Altmann DM: The immunology of sepsis. J Pathol 214: 211, 2008. [PubMed: 18161754]48. Vincent JL, Weil MH: Fluid challenge revisited. Crit Care Med 34: 1333, 2006. [PubMed: 16557164]49. Rivers EP, Kruse JA, Jacobsen G, et al: The influence of early hemodynamic optimization on biomarker patterns of severe sepsis and septic shock. Crit Care Med 35: 2016, 2007.[PubMed: 17855815]50. Estenssoro E, Gonzalez F, Laffaire E, et al: Shock on admission day is the best predictor of prolonged mechanical ventilation in the ICU. Chest 127: 598, 2005. [PubMed:15706002]51. Rivers EP: Fluid-management strategies in acute lung injuryliberal, conservative, or both? N Engl J Med 354: 2598, 2006. [PubMed: 16714769]52. Wiedemann HP, Wheeler AP, Bernard GR, et al: Comparison of two fluid-management strategies in acute lung injury. N Engl J Med 354: 2564, 2006. [PubMed: 16714767]53. Nguyen HB, Banta JE, Cho TW, et al: Mortality predictions using current physiologic scoring systems in patients meeting criteria for early goal-directed therapy and the severesepsis resuscitation bundle. Shock 30: 23, 2008. [PubMed: 18323748]54. American College of Chest Physicians/Society of Critical Care Medicine consensus conference: definitions for sepsis and organ failure and guidelines for the use of innovativetherapies in sepsis. Crit Care Med 20: 864, 1992.55. Rivers EP, Blake HC, Dereczyk B, et al: Adrenal dysfunction in hemodynamically unstable patients in the emergency department. Acad Emerg Med 6: 626, 1999. [PubMed:10386680]
Useful Web Resources
Critical Care Medicine Tutorials (SHOCK)http://ccmtutorials.com, http://ccmtutorials.com/cvs/index.htmCritical Care Archiveshttp://ccforum.com
http://accessmedicine.mhmedical.com.pbidi.unam.mx:8080/content.aspx...
12 de 13 07/03/2015 07:35 p. m.
-
Your IP address is 132.248.9.8
The pathophysiology of shock, systemic inflammatory response syndrome (SIRS), and multi-organ dysfunction syndrome (MODS).
http://accessmedicine.mhmedical.com.pbidi.unam.mx:8080/content.aspx...
13 de 13 07/03/2015 07:35 p. m.
Related Documents