Time Interval Between Concussions and Symptom Duration WHAT’S KNOWN ON THIS SUBJECT: Although concussion is increasingly being diagnosed in the pediatric population, little is known about what factors lead to prolonged postconcussive symptoms in children. In particular, the effect of previous history of concussion on recovery from a repeat injury is unclear. WHAT THIS STUDY ADDS: Children with a history of previous concussion, particularly recent or multiple concussions, are at increased risk for prolonged symptoms after concussion. This suggests that repeat concussion, particularly within a vulnerable time window, may lead to longer duration of symptoms. abstract OBJECTIVE: To test the hypothesis that children with a previous his- tory of concussion have a longer duration of symptoms after a repeat concussion than those without such a history. METHODS: Prospective cohort study of consecutive patients 11 to 22 years old presenting to the emergency department of a children’ s hospital with an acute concussion. The main outcome measure was time to symptom resolution, assessed by the Rivermead Post- Concussion Symptoms Questionnaire (RPSQ). Patients and providers completed a questionnaire describing mechanism of injury, associated symptoms, past medical history, examination findings, diagnostic studies, and the RPSQ. Patients were then serially administered the RPSQ for 3 months after the concussion or until all symptoms resolved. RESULTS: A total of 280 patients were enrolled over 12 months. Patients with a history of previous concussion had a longer duration of symp- toms than those without previous concussion (24 vs 12 days, P = .02). Median symptom duration was even longer for patients with multiple previous concussions (28 days, P = .03) and for those who had sustained a concussion within the previous year (35 days, P = .007) compared with patients without those risk factors. In a multivariate model, previous concussion, absence of loss of consciousness, age $13, and initial RPSQ score .18 were significant predictors of pro- longed recovery. CONCLUSIONS: Children with a history of a previous concussion, particularly recent or multiple concussions, are at increased risk for prolonged symptoms after concussion. These findings have direct implications on the management of patients with con- cussion who are at high risk for repeat injuries. Pediatrics 2013;132:8–17 AUTHORS: Matthew A. Eisenberg, MD, John Andrea, BS, William Meehan, MD and Rebekah Mannix, MD, MPH Division of Emergency Medicine, Boston Children’ s Hospital, Harvard Medical School, Boston, Massachusetts KEY WORDS brain concussion, emergency medicine, pediatrics, postconcussion syndrome, traumatic brain injury ABBREVIATIONS ADHD—attention-deficit/hyperactivity disorder ED—emergency department LOC—loss of consciousness mTBI—mild traumatic brain injury RPSQ—Rivermead Post-Concussion Symptoms Questionnaire Dr Eisenberg was responsible for study conception and design, data acquisition and analysis, and drafting and review of the article; Mr Andrea was responsible for data acquisition and analysis, and drafting and review of the article; Dr Meehan was responsible for study conception, study design, and article review; Dr Mannix was responsible for study conception, study design, data analysis, and article review; and all authors approved the final version of this manuscript. www.pediatrics.org/cgi/doi/10.1542/peds.2013-0432 doi:10.1542/peds.2013-0432 Accepted for publication Mar 27, 2013 Address correspondence to Matthew A. Eisenberg, MD, Division of Emergency Medicine, Boston Children’ s Hospital, 300 Longwood Ave, Boston, MA 02115. E-mail: matthew.eisenberg@childrens. harvard.edu PEDIATRICS (ISSN Numbers: Print, 0031-4005; Online, 1098-4275). Copyright © 2013 by the American Academy of Pediatrics FINANCIAL DISCLOSURE: The authors have indicated they have no financial relationships relevant to this article to disclose. FUNDING: No external funding. Expenses related to use of research coordinators were paid by the Division of Emergency Medicine, Boston Children’ s Hospital. 8 EISENBERG et al by guest on April 11, 2017 Downloaded from

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript
Time Interval Between Concussions and SymptomDuration
WHAT’S KNOWN ON THIS SUBJECT: Although concussion isincreasingly being diagnosed in the pediatric population, little isknown about what factors lead to prolonged postconcussivesymptoms in children. In particular, the effect of previous historyof concussion on recovery from a repeat injury is unclear.
WHAT THIS STUDY ADDS: Children with a history of previousconcussion, particularly recent or multiple concussions, are atincreased risk for prolonged symptoms after concussion. Thissuggests that repeat concussion, particularly within a vulnerabletime window, may lead to longer duration of symptoms.
abstractOBJECTIVE: To test the hypothesis that children with a previous his-tory of concussion have a longer duration of symptoms after a repeatconcussion than those without such a history.
METHODS: Prospective cohort study of consecutive patients 11 to 22years old presenting to the emergency department of a children’shospital with an acute concussion. The main outcome measure wastime to symptom resolution, assessed by the Rivermead Post-Concussion Symptoms Questionnaire (RPSQ). Patients and providerscompleted a questionnaire describing mechanism of injury,associated symptoms, past medical history, examination findings,diagnostic studies, and the RPSQ. Patients were then seriallyadministered the RPSQ for 3 months after the concussion or untilall symptoms resolved.
RESULTS: A total of 280 patients were enrolled over 12 months. Patientswith a history of previous concussion had a longer duration of symp-toms than those without previous concussion (24 vs 12 days, P = .02).Median symptom duration was even longer for patients with multipleprevious concussions (28 days, P = .03) and for those who hadsustained a concussion within the previous year (35 days, P = .007)compared with patients without those risk factors. In a multivariatemodel, previous concussion, absence of loss of consciousness, age$13, and initial RPSQ score .18 were significant predictors of pro-longed recovery.
CONCLUSIONS: Children with a history of a previous concussion,particularly recent or multiple concussions, are at increasedrisk for prolonged symptoms after concussion. These findingshave direct implications on the management of patients with con-cussion who are at high risk for repeat injuries. Pediatrics2013;132:8–17
AUTHORS: Matthew A. Eisenberg, MD, John Andrea, BS,William Meehan, MD and Rebekah Mannix, MD, MPH
Division of Emergency Medicine, Boston Children’s Hospital,Harvard Medical School, Boston, Massachusetts
KEY WORDSbrain concussion, emergency medicine, pediatrics,postconcussion syndrome, traumatic brain injury
ABBREVIATIONSADHD—attention-deficit/hyperactivity disorderED—emergency departmentLOC—loss of consciousnessmTBI—mild traumatic brain injuryRPSQ—Rivermead Post-Concussion Symptoms Questionnaire
Dr Eisenberg was responsible for study conception and design,data acquisition and analysis, and drafting and review of thearticle; Mr Andrea was responsible for data acquisition andanalysis, and drafting and review of the article; Dr Meehan wasresponsible for study conception, study design, and articlereview; Dr Mannix was responsible for study conception, studydesign, data analysis, and article review; and all authorsapproved the final version of this manuscript.
www.pediatrics.org/cgi/doi/10.1542/peds.2013-0432
doi:10.1542/peds.2013-0432
Accepted for publication Mar 27, 2013
Address correspondence to Matthew A. Eisenberg, MD, Division ofEmergency Medicine, Boston Children’s Hospital, 300 LongwoodAve, Boston, MA 02115. E-mail: [email protected]
PEDIATRICS (ISSN Numbers: Print, 0031-4005; Online, 1098-4275).
Copyright © 2013 by the American Academy of Pediatrics
FINANCIAL DISCLOSURE: The authors have indicated they haveno financial relationships relevant to this article to disclose.
FUNDING: No external funding. Expenses related to use ofresearch coordinators were paid by the Division of EmergencyMedicine, Boston Children’s Hospital.
8 EISENBERG et alby guest on April 11, 2017Downloaded from

Approximately 144 000 children pres-ent each year to US emergency depart-ments (EDs) with concussion,1,2 andmillions more are treated by athletictrainers, primary care doctors, oroutpatient specialists.3 Despite in-creasing scientific research into con-cussion, however, relatively little isknown about what factors lead toprolonged postconcussive symptomsin children. This lack of prognosticdata has led to significant uncertaintyamong patients, families, and healthcare providers as to which patientswould benefit from specialist follow-up,extended academic accommodations,prolonged abstinence from athleticparticipation, and even permanentcessation of high-risk activity.
Although a large and expanding body ofliterature has examined concussion inadults,4–6 the data that exist on pediatricconcussion is composed primarily ofsmaller case series and retrospectivestudies.7–9 Few studies have examinedrisk factors for prolonged symptomduration in children,10–14 and they havegenerated conflicting results on themodifying effect of previous concussion.Supporting an association betweenprevious history of concussion and pro-longed symptom duration, Moser et al7
showed that high school athletes withmultiple previous concussions had per-sistent neurocognitive deficits indis-tinguishable from those in the acuterecovery phase of concussion. Similarly,in an analysis of 119 children with mildtraumatic brain injury (mTBI), Ponsfordet al15 demonstrated that previous headinjury was predictive of persistent con-cussive symptoms 3 months after theinjury. However, 2 larger studies, a sec-ondary analysis of an mTBI cohortpresenting to a pediatric ED and a pro-spective study of concussed high schoolathletes, found no association betweenprevious concussion and duration ofpostconcussive symptoms.16,17
Animal models of mTBI offer a possibleexplanation for this variation, sug-gesting that both timing and number ofinjuries modify the effects of previousinjury. In particular, several studies inrodents suggest that the effect ofmultipleconcussions iscumulative,andthat the time elapsed between con-cussions to allow for return of normalphysiologic function may be the key tothe course of recovery.18–22
Despite this, no clinical study hascharacterized the vulnerable windowduringwhichrepeat concussionresultsin worse outcome among children, orthe critical number of injuries thatconfers increased risk of prolongedrecovery. If reinjury within a window ofvulnerabilityconfershigherriskof long-term neurocognitive deficits, then ab-stinence from at-risk activities mayultimately improve outcomes. Theobjective of this study was to charac-terize the effect of previous concussionon recovery from concussion amongchildren presenting to an ED. We hy-pothesized that those with a previoushistory of concussion would havea longer time to symptom resolutionthan those without such a history, andthat those who sustained a concussionwithin the previous year would havea longer time to symptom resolutionthan those with more remote injuries.
METHODS
Study Design
We conducted a prospective cohortstudy of consecutive patients aged 11 to22 years who presented to the ED ofa tertiary care children’s hospitalwithin 72 hours of a concussion fromSeptember 1, 2011, to August 31, 2012.
Definition
Concussion was defined as a blunt in-jury to the head resulting in either (1)alteration in mental status or (2) any ofthe following symptoms that started
within4hoursof the injuryandwerenotpresent before the injury: headache,nausea, vomiting, dizziness/balanceproblems, fatigue, drowsiness, blur-red vision, memory difficulty, or diffi-culty concentrating in the absence ofindications for head imaging orwithoutintracranial hemorrhagewhen imagingwas obtained. Although there has beencontroversy regarding the definition ofconcussion for clinical research,23–26
we chose this broad definition so as toinclude both those who had alterationof consciousness and those who pre-sented with typical postconcussivesymptoms following a head injury.6,27,28
Patientswereexcluded from the study ifany of the following were present: (1)Glasgow Coma Score,13 on arrival tothe ED, (2) coexisting skull or long-bonefracture, (3) coexisting injury to intra-abdominal or intrathoracic organ orspinal cord, (4) cognitive or develop-mental disability preventing patientfrom completing the questionnaire, or(5) involvement of either law enforce-ment or ED social workers for victimsof an assault. These criteria were de-signed to distinguish postconcussivesymptoms from symptoms related toother injuries or psychological stressesrelated to major trauma or assault.
Primary Outcome
The primary outcome was time to res-olution of postconcussive symptomsassessed via the Rivermead Post-Concussion Symptoms Questionnaire(RPSQ), a 16-item concussion symptominventory checklist.29 The RPSQ hasbeen used extensively in both adult andpediatric studies of mTBI,10,30,31 showna high degree of interrater and test-retest reliability,29,32 and been shownto be valid and unbiased in youngchildren.31,33 The questionnaire wasavailable to study participants in bothEnglish and Spanish. Patients wereconsidered symptom-free when all in-ventories of the RPSQ were scored
ARTICLE
PEDIATRICS Volume 132, Number 1, July 2013 9by guest on April 11, 2017Downloaded from
a 0 (symptom not present) or 1 (symp-tom present at preinjury baseline).Patients filled out the survey indepen-dently or with assistance of parents atthe discretion of the patient and family.
Enrollment and Consent
Study participants were enrolled dur-ing their ED visit by trained researchcoordinators after informed consent(and assent for patients ,18 years)was obtained. Eligible patients whowere not contacted during their ED visitwere offered enrollment the followingday if they were still within 72 hours ofthe injury. On enrollment, patientscompleted an electronic questionnaireasking for demographic information(including self-reported race andethnicity), mechanism of injury, asso-ciated symptoms, such as loss of con-sciousness (LOC) and amnesia, relevantpast medical history, and the RPSQ.Providers completed a questionnairewith physical examination findings, di-agnostic studies, and information oninterventions, disposition, and dis-charge instructions.
Follow-up
An online follow-up questionnaire con-taining theRPSQwassent electronicallytopatients1, 2, 4, 6, 8, and12weeksaftertheir ED visit or until they met criteriafor symptom resolution. Patients whoreported resolution of symptoms wereprompted to provide the last date onwhich symptoms occurred. Patientswith incomplete or inconsistent datawere called to resolve these issues.Patients were considered lost to follow-up if they failed to respond to 2 con-secutive questionnaires. Study datawere collected and managed usingREDCap (Research Electronic DataCapture, Nashville, TN) electronic datacapture tools hosted at Boston Child-ren’s Hospital.34
Statistical Analysis
Statistical analysis was performed byusing PASW Statistics 18 (IBM SPSSStatistics, IBMCorporation, Chicago, IL).We estimated that 250 patients wouldbe required to demonstrate a 5-daydifference in time to resolution ofsymptoms between those with andwithout previous concussion, usinga 2-tailed a of 0.05 and power of 90%.
Data were analyzed by Student’s t-testor Wilcoxon Rank Sum test as appro-priate. Our primary outcome, time tosymptom resolution, was assessed asa continuous variable ranging from0 to 90 days. Potential predictors thatwere continuous in nature were di-chotomized before analysis accordingto their median value. The only excep-tion to this was age; 13 years or olderwas chosen rather than the median asa proxy for pubertal status.
In univariate analysis of time to symp-tom resolution, Kaplan-Meier analysiswith log-rank tests of significance wasused to best account for censored data.To adjust for confounders, we con-structed a multivariate Cox regression
model using predictors with P ,.05 on univariate screening. WhereKaplan-Meier analysis was performed,“median” refers to median survivaltime (where “survival” signifies per-sistence of symptoms), a measure thattakes into account expected duration ofsymptoms for censored patients. Val-ues were considered statistically sig-nificant if P , .05. The institutionalreview board approved this study be-fore onset of data collection.
RESULTS
Study Population
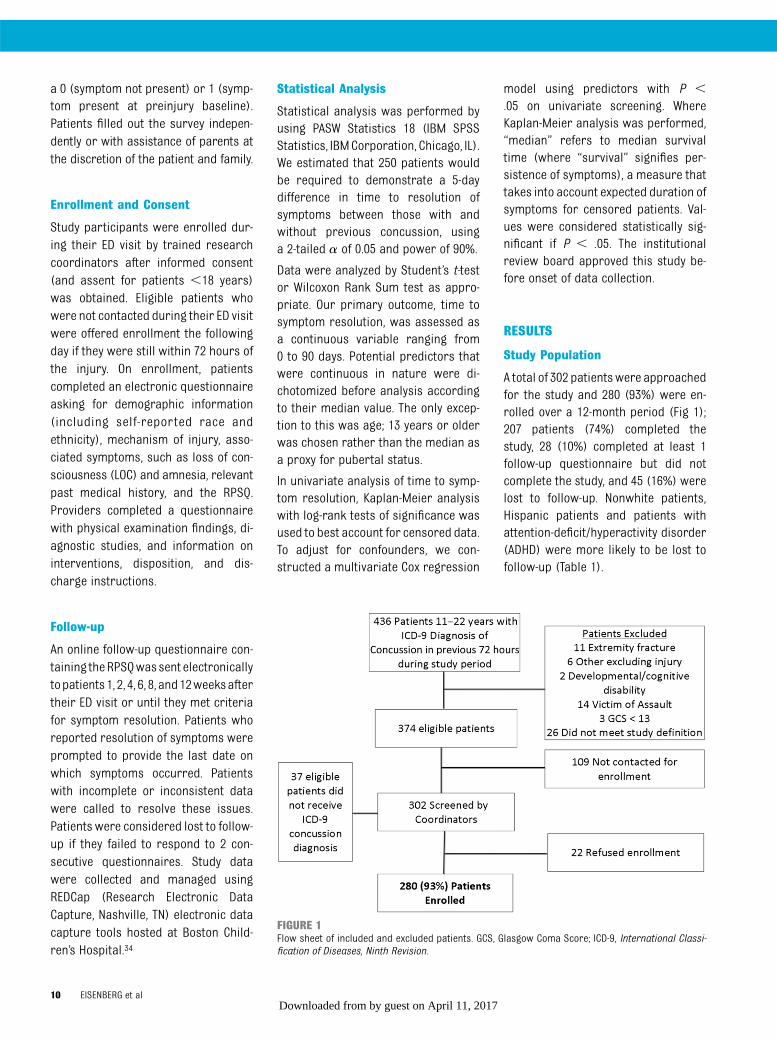
A total of 302 patientswere approachedfor the study and 280 (93%) were en-rolled over a 12-month period (Fig 1);207 patients (74%) completed thestudy, 28 (10%) completed at least 1follow-up questionnaire but did notcomplete the study, and 45 (16%) werelost to follow-up. Nonwhite patients,Hispanic patients and patients withattention-deficit/hyperactivity disorder(ADHD) were more likely to be lost tofollow-up (Table 1).
FIGURE 1Flow sheet of included and excluded patients. GCS, Glasgow Coma Score; ICD-9, International Classi-fication of Diseases, Ninth Revision.
10 EISENBERG et alby guest on April 11, 2017Downloaded from

Patient Presentation
Most patients (66.0%) were enrolled inthe study on the day their concussionoccurred, with 24.7% enrolled the fol-lowing day, 7.2% enrolled 2 days later,and 1.7% 3 days later.
A majority of (63.8%) patients wereinjured playing a sport, with the mostcommon sports being hockey (14%),soccer (9.4%), football (8.5%), andbasketball (8.1%). The most commonpresenting symptoms (RPSQ score $
2) were headache (85.1%), fatigue(64.7%), and dizziness (63.0%). An ab-normal physical finding was noted in10.6% of patients, with the most com-mon abnormalities being altered gaitor balance (4.3%) and altered mentalstatus (2.4%). Among the 20.8% ofpatients who had neuroimaging per-formed, there were no abnormalitiesidentified related to trauma. On dis-charge, 65.9% of patients were pre-scribed a period of cognitive rest,92.4% were recommended to take timeoff from athletics, and 63.8% were ad-vised to follow-up with their primarycare doctor, 45.5% in a sports concus-sion clinic, and 6.2% with anotherspecialist.
Time to Recovery
Median time to symptomresolution andpercentage of patients symptomatic 7,28, and 90daysafter the concussionare
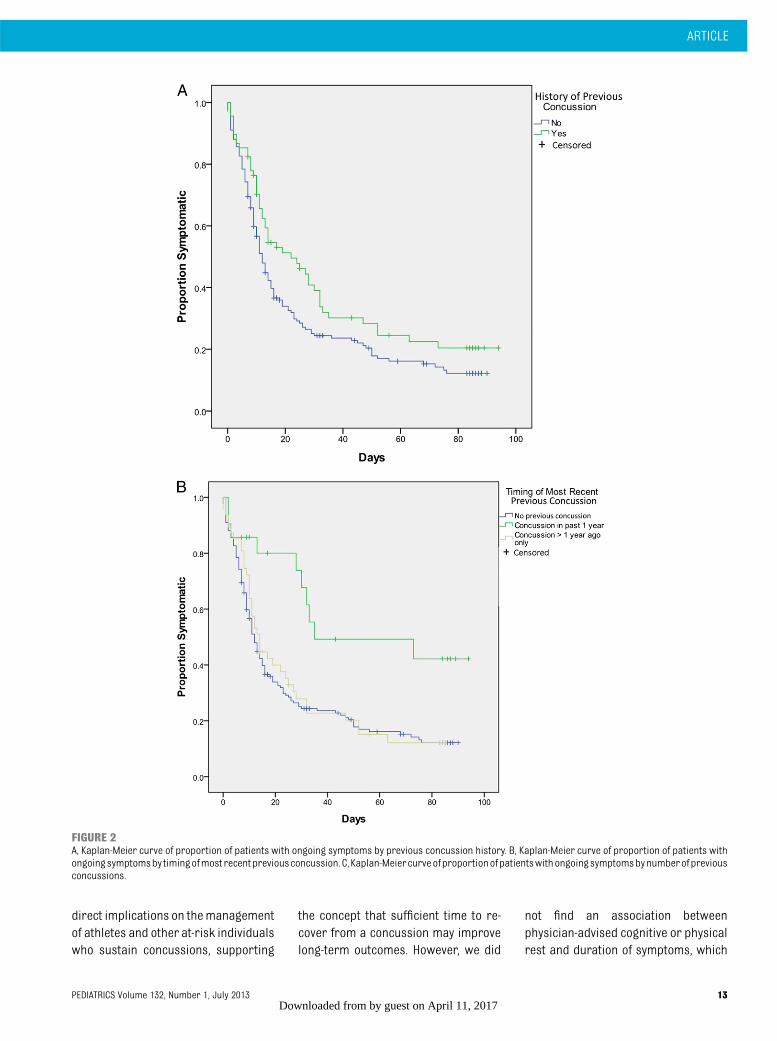
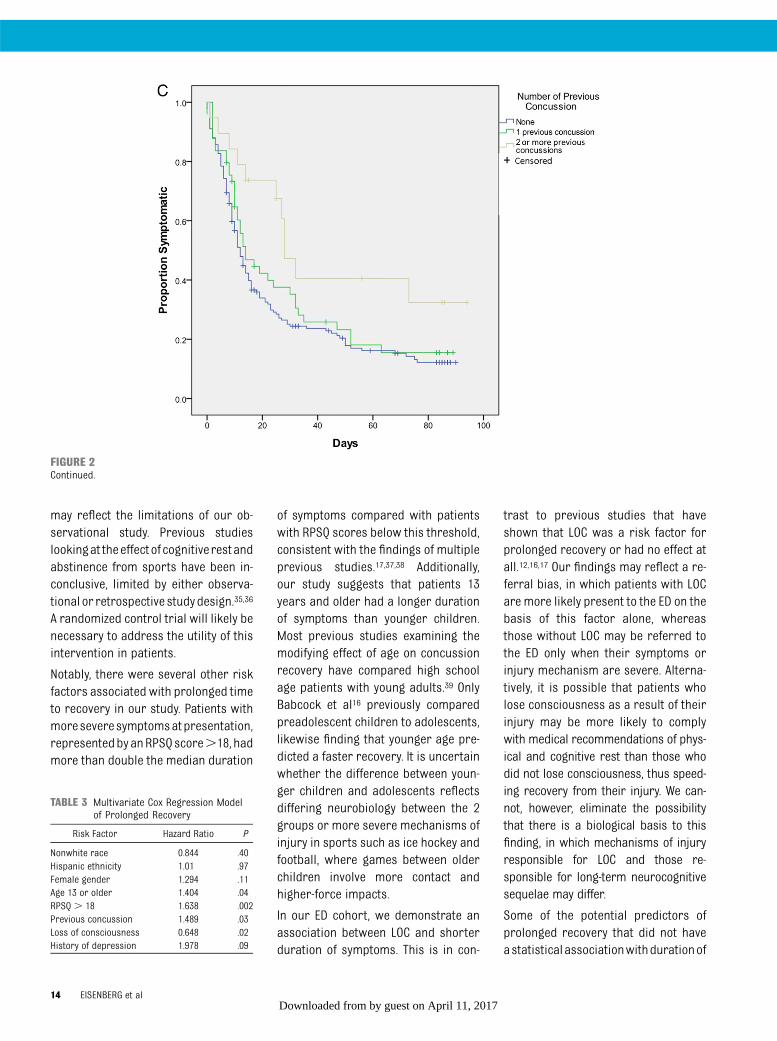
shown in Table 2. In univariate analysis,history of previous concussion (Fig 2A),age $13, initial RPSQ score .18, fe-male gender, history of depression,absence of LOC, and abnormal neuro-logic examination on presentationwere all predictive of a longer time tosymptom resolution (Table 2). Amongpatients with a previous concussion,those who had a concussion in the pastyear had nearly 3 times the medianduration of symptoms compared withthose who had no previous concussionor whose most recent concussion oc-curred .1 year previous (Fig 2B).Similarly, patients with 2 or more pre-vious concussions had more thandouble the median symptom durationcompared with patients with 0 or 1previous concussion (Fig 2C).
In the multivariate model, patients witha history of previous concussion, ab-sence of LOC, age$13, and RPSQ score.18 had significantly longer symptomduration than patients without theserisk factors (Table 3).
DISCUSSION
Our study demonstrates that previousconcussion is predictive of a longertime to symptom resolution after pe-diatric concussion. Importantly, wefound that the effect of previous con-cussion on symptom duration wasstrongly influenced by both the number
of previous concussions and the timeelapsed since the most recent previousconcussion. Both study participantswithmultipleprevious concussionsandthose who had sustained a concussionwithin thepreviousyearhadamarkedlygreater duration of symptoms thanthose with no previous concussion.Conversely, patients who had onlya single previous concussion that oc-curred more than a year before theircurrent injury had no statistical dif-ference in duration of symptoms fromchildrenwithoutapreviousconcussion.These findings, which suggest bothtemporal vulnerability and a dose-response effect of previous injuries,support previous research in animalmodels of concussive brain injury.18–22
Previous studies in rodents have dem-onstrated cumulative effects of repet-itivemild head injuries.19,21 Additionally,several of these studies suggest atemporal window of vulnerability where-in the repeat trauma has a more pro-nounced effect. One study observedthat whereas mice concussed atmonthly intervals performed similarlyto noninjured mice on tests of learningand memory, animals concussed atweekly and daily intervals developedpersistent cognitive deficits, with thedaily concussion group showing ongo-ing effects up to 1 year after the injurycompared with controls.22 Other ani-mal models have offered possible bi-ological mechanisms for this temporalvulnerability. Longhi et al18 showed ev-idence of axonal injury and cytoskeletaldamage that was significantly greaterin mice that received a second con-cussion within 3 to 5 days of an initialhead injury than those who had beensubjected to only a single concussion.Vagnozzi et al20 found a similar effectin rats and correlated it to reversibleimpairments in mitochondrial enzymes.
Ourstudydemonstrates this temporallysensitive effect of previous concussionfor the first time in humans. This has
TABLE 1 Characteristics of Patients With and Without Follow-up Data
Included in Study, n = 235 Lost to Follow-up, n = 45 P
Mean age 14.3 13.6 .05Male gender, n (%) 135 (57.4) 28 (62.2) .55Nonwhite race, n (%) 50 (21.3) 19 (42.2) .003Hispanic ethnicity, n (%) 20 (8.5) 10 (22.2) .005Sports-related concussion, n (%) 150 (63.8) 23 (51.1) .11LOC, n (%) 52 (22.1) 10 (22.2) .97Amnesia, n (%) 101 (43.0) 15 (33.3) .22Previous concussion, n (%) 68 (28.9) 11 (24.4) .54PMH migraine, n (%) 29 (12.3) 9 (20.0) .17PMH LD, n (%) 30 (12.8) 5 (11.1) .75PMH ADHD, n (%) 35 (14.9) 13 (28.9) .02PMH depression, n (%) 15 (6.4) 5 (11.1) .34PMH anxiety, n (%) 21 (8.9) 5 (11.1) .58Mean total RPSQ score 18.83 18.13 .75
LD, learning disability; PMH, previous medical history.
ARTICLE
PEDIATRICS Volume 132, Number 1, July 2013 11by guest on April 11, 2017Downloaded from
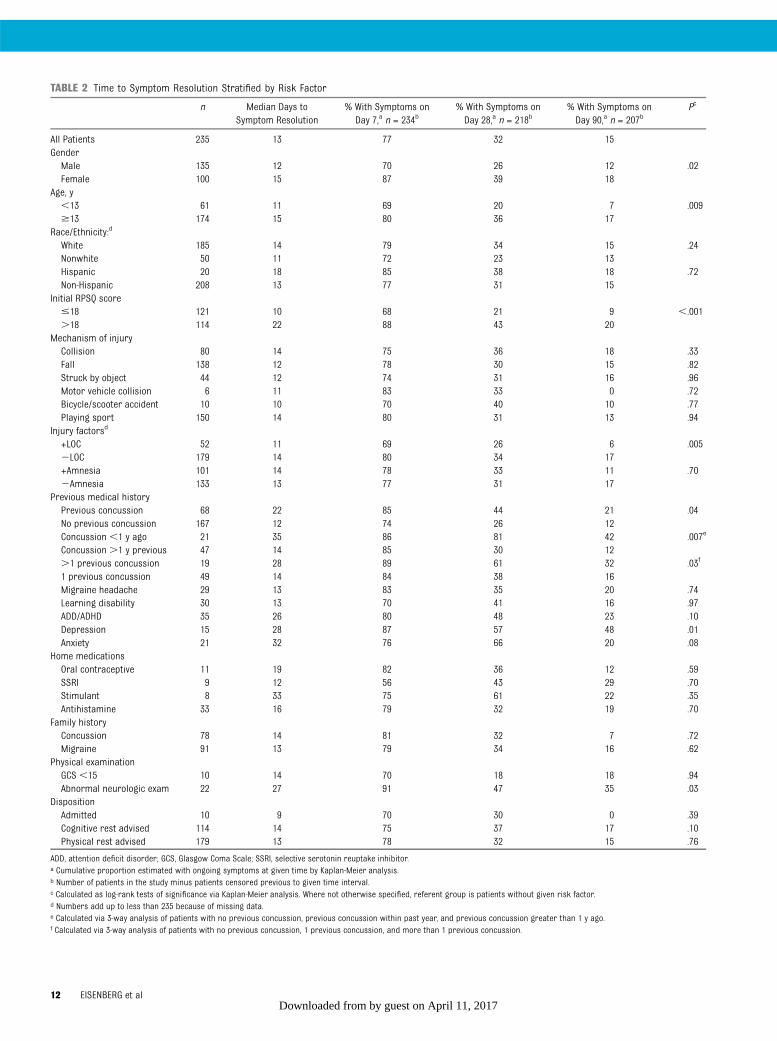
TABLE 2 Time to Symptom Resolution Stratified by Risk Factor
n Median Days toSymptom Resolution
% With Symptoms onDay 7,a n = 234b
% With Symptoms onDay 28,a n = 218b
% With Symptoms onDay 90,a n = 207b
Pc
All Patients 235 13 77 32 15GenderMale 135 12 70 26 12 .02Female 100 15 87 39 18
Age, y,13 61 11 69 20 7 .009$13 174 15 80 36 17
Race/Ethnicity:d
White 185 14 79 34 15 .24Nonwhite 50 11 72 23 13Hispanic 20 18 85 38 18 .72Non-Hispanic 208 13 77 31 15
Initial RPSQ score#18 121 10 68 21 9 ,.001.18 114 22 88 43 20
Mechanism of injuryCollision 80 14 75 36 18 .33Fall 138 12 78 30 15 .82Struck by object 44 12 74 31 16 .96Motor vehicle collision 6 11 83 33 0 .72Bicycle/scooter accident 10 10 70 40 10 .77Playing sport 150 14 80 31 13 .94
Injury factorsd
+LOC 52 11 69 26 6 .0052LOC 179 14 80 34 17+Amnesia 101 14 78 33 11 .702Amnesia 133 13 77 31 17
Previous medical historyPrevious concussion 68 22 85 44 21 .04No previous concussion 167 12 74 26 12Concussion ,1 y ago 21 35 86 81 42 .007e
Concussion .1 y previous 47 14 85 30 12.1 previous concussion 19 28 89 61 32 .03f
1 previous concussion 49 14 84 38 16Migraine headache 29 13 83 35 20 .74Learning disability 30 13 70 41 16 .97ADD/ADHD 35 26 80 48 23 .10Depression 15 28 87 57 48 .01Anxiety 21 32 76 66 20 .08
Home medicationsOral contraceptive 11 19 82 36 12 .59SSRI 9 12 56 43 29 .70Stimulant 8 33 75 61 22 .35Antihistamine 33 16 79 32 19 .70
Family historyConcussion 78 14 81 32 7 .72Migraine 91 13 79 34 16 .62
Physical examinationGCS ,15 10 14 70 18 18 .94Abnormal neurologic exam 22 27 91 47 35 .03
DispositionAdmitted 10 9 70 30 0 .39Cognitive rest advised 114 14 75 37 17 .10Physical rest advised 179 13 78 32 15 .76
ADD, attention deficit disorder; GCS, Glasgow Coma Scale; SSRI, selective serotonin reuptake inhibitor.a Cumulative proportion estimated with ongoing symptoms at given time by Kaplan-Meier analysis.b Number of patients in the study minus patients censored previous to given time interval.c Calculated as log-rank tests of significance via Kaplan-Meier analysis. Where not otherwise specified, referent group is patients without given risk factor.d Numbers add up to less than 235 because of missing data.e Calculated via 3-way analysis of patients with no previous concussion, previous concussion within past year, and previous concussion greater than 1 y ago.f Calculated via 3-way analysis of patients with no previous concussion, 1 previous concussion, and more than 1 previous concussion.
12 EISENBERG et alby guest on April 11, 2017Downloaded from
direct implications on themanagementof athletes and other at-risk individualswho sustain concussions, supporting
the concept that sufficient time to re-cover from a concussion may improvelong-term outcomes. However, we did
not find an association betweenphysician-advised cognitive or physicalrest and duration of symptoms, which
FIGURE 2A, Kaplan-Meier curve of proportion of patients with ongoing symptoms by previous concussion history. B, Kaplan-Meier curve of proportion of patients withongoingsymptomsby timingofmost recentpreviousconcussion. C,Kaplan-Meiercurveofproportionofpatientswithongoingsymptomsbynumberof previousconcussions.
ARTICLE
PEDIATRICS Volume 132, Number 1, July 2013 13by guest on April 11, 2017Downloaded from
may reflect the limitations of our ob-servational study. Previous studieslookingat theeffectof cognitiverestandabstinence from sports have been in-conclusive, limited by either observa-tional or retrospective studydesign.35,36
A randomized control trial will likely benecessary to address the utility of thisintervention in patients.
Notably, there were several other riskfactors associated with prolonged timeto recovery in our study. Patients withmoreseveresymptomsatpresentation,representedbyanRPSQscore.18, hadmore than double the median duration
of symptoms compared with patientswith RPSQ scores below this threshold,consistent with the findings of multipleprevious studies.17,37,38 Additionally,our study suggests that patients 13years and older had a longer durationof symptoms than younger children.Most previous studies examining themodifying effect of age on concussionrecovery have compared high schoolage patients with young adults.39 OnlyBabcock et al16 previously comparedpreadolescent children to adolescents,likewise finding that younger age pre-dicted a faster recovery. It is uncertainwhether the difference between youn-ger children and adolescents reflectsdiffering neurobiology between the 2groups or more severe mechanisms ofinjury in sports such as ice hockey andfootball, where games between olderchildren involve more contact andhigher-force impacts.
In our ED cohort, we demonstrate anassociation between LOC and shorterduration of symptoms. This is in con-
trast to previous studies that haveshown that LOC was a risk factor forprolonged recovery or had no effect atall.12,16,17 Our findings may reflect a re-ferral bias, in which patients with LOCare more likely present to the ED on thebasis of this factor alone, whereasthose without LOC may be referred tothe ED only when their symptoms orinjury mechanism are severe. Alterna-tively, it is possible that patients wholose consciousness as a result of theirinjury may be more likely to complywith medical recommendations of phys-ical and cognitive rest than those whodid not lose consciousness, thus speed-ing recovery from their injury. We can-not, however, eliminate the possibilitythat there is a biological basis to thisfinding, in which mechanisms of injuryresponsible for LOC and those re-sponsible for long-term neurocognitivesequelae may differ.
Some of the potential predictors ofprolonged recovery that did not haveastatisticalassociationwithdurationof
FIGURE 2Continued.
TABLE 3 Multivariate Cox Regression Modelof Prolonged Recovery
Risk Factor Hazard Ratio P
Nonwhite race 0.844 .40Hispanic ethnicity 1.01 .97Female gender 1.294 .11Age 13 or older 1.404 .04RPSQ . 18 1.638 .002Previous concussion 1.489 .03Loss of consciousness 0.648 .02History of depression 1.978 .09
14 EISENBERG et alby guest on April 11, 2017Downloaded from

symptoms in our study are also note-worthy. In the multivariate analysis, fe-male gender did not predict prolongedrecovery, although there appeared tobe a difference between the genders inunivariate analysis. This is nearly iden-tical to the results of Babcock et al,16 andlikely because female patients had moresevere symptoms at presentation in ourstudy (mean initial RPSQ 21.3 vs 17.0 inmale patients,P= .02), thus representinga confounding variable. Whether thisfinding is indicative of the fact that fe-male patients have more severe symp-toms from concussion in general, assuggested in several previous studies,40–42
or is due to referral bias in which fe-male individuals preferentially presentto the ED when symptoms are moresevere than male counterparts cannotbe ascertained from our data.
We also observed that patients witha history of migraine headaches, de-pression,ADHD,andanxietydidnothaveprolonged symptoms after concussion;however, small sample size limits ourability to detect relationships in thesespecific patient populations.
Patients in our study had a longerduration of symptoms than most pre-vious reports in the literature, whichhave frequently shown symptoms re-solvingby7to10daysafter the injury.5,17,43
This may be because of differences instudy populations, as children pre-senting to an ED may represent a moresevere subset of concussed patientsthan the outpatient cohorts previouslystudied. The RPSQ may also be moresensitive to ongoing symptoms thanthe self-assessment tools or neuro-cognitive testing used in many otherstudies.
There are several limitations to ourstudy. Although we enrolled 93% ofpatients approached to participate,there were additional patients whowere not contacted by the researchcoordinators. The most common rea-sons for this were arrival to the EDduring a time when no research co-ordinator was available and shortlength of ED stay, leading to dischargebefore the patient could be contactedabout enrollment. Second, by usingsurvival analysis to best account forcensored data, we assumed that therewas no difference between patientswhowerecensoredandthosewhowerenot. Although this assumption appearsto be valid based on similar de-mographics and symptom scores ofcensored versusnoncensoredpatients,it is possible that patients ultimatelyfailed to complete the study because ofmore bothersome symptoms or, con-versely, more rapid symptom resolu-tion. A final limitation is the accuracy ofself-reported symptoms: certain sub-groups of the population, notably ath-letes, may have had an incentive toreport symptom resolution to expeditereturn-to-play; others may report symp-toms that are no longer present to avoidschoolwork; still others may have a diffi-cult time understanding the questions ofthe RPSQ.
Despite these limitations, our study hadseveral strengths, including a largesample size and prospective methodol-ogy. We enrolled a high percentage ofeligible patients and most patientscontinued participation until symptomresolution. By serially surveying patientsat short time intervals andasking for thespecific date of symptom resolutionwithin that interval, our estimates of
symptom duration are likely to be moreaccurate than if we used a single follow-upquestionnairemonthsafter theinjury.
Finally, unlike previous studies thatfocused on particular subgroups ofpatients, such as participants in a par-ticular sport, our study examined alleligible patients who presented toa tertiary care ED. As a result, westudiedadiversegroup in termsof bothdemographics and mechanisms of in-jury, potentially making our studymoregeneralizable to medical providerspracticing in the primary care and EDsettings than samples of selectedpopulations.
CONCLUSION
Children with a history of a previousconcussion, particularly those withrecent or multiple concussions, are atincreased risk for prolonged symptomsafter concussion. These findings havedirect implications on themanagementof concussion patients, particularlythose at high risk for future concussiveinjuries, such as athletes.
ACKNOWLEDGMENTSMichaelMonutaeux, ScD, provided sta-tistical guidance and support. RichBachur, MD, and Mark Neuman, MD,provided mentorship and manuscriptreview. Chris Landrigan, MD, assistedwith manuscript review. Mark Berry,MA, provided programming and ad-ministrative support. The research co-ordinator team (Elizabeth Paulsen, BS,Lucy Abernethy, BA, Kaitlin Morris, BA,Hillary Chu, BA, and Jessica LeSage,BS) enrolled and followed up withpatients and provided administrativesupport.
REFERENCES
1. Meehan WP III, Mannix R. Pediatric con-cussions in United States emergency
departments in the years 2002 to 2006. JPediatr. 2010;157(6):889–893
2. Guerriero RM, Proctor MR, Mannix R,Meehan WP III. Epidemiology, trends,
ARTICLE
PEDIATRICS Volume 132, Number 1, July 2013 15by guest on April 11, 2017Downloaded from

assessment and management of sport-related concussion in United States highschools. Curr Opin Pediatr. 2012;24(6):696–701
3. Meehan WP III, d’Hemecourt P, ComstockRD. High school concussions in the 2008-2009 academic year: mechanism, symp-toms, and management. Am J Sports Med.2010;38(12):2405–2409
4. Jacobs B, Beems T, Stulemeijer M, et al.Outcome prediction in mild traumatic braininjury: age and clinical variables arestronger predictors than CT abnormalities.J Neurotrauma. 2010;27(4):655–668
5. McCrea M, Guskiewicz KM, Marshall SW,et al. Acute effects and recovery time fol-lowing concussion in collegiate footballplayers: the NCAA Concussion Study. JAMA.2003;290(19):2556–2563
6. Ropper AH, Gorson KC. Clinical practice.Concussion. N Engl J Med. 2007;356(2):166–172
7. Moser RS, Schatz P, Jordan BD. Prolongedeffects of concussion in high school ath-letes. Neurosurgery. 2005;57(2):300–306;discussion 300–306
8. Blinman TA, Houseknecht E, Snyder C, WiebeDJ, Nance ML. Postconcussive symptoms inhospitalized pediatric patients after mildtraumatic brain injury. J Pediatr Surg. 2009;44(6):1223–1228
9. Iverson G. Predicting slow recovery fromsport-related concussion: the new simple-complex distinction. Clin J Sport Med. 2007;17(1):31–37
10. Barlow KM, Crawford S, Stevenson A,Sandhu SS, Belanger F, Dewey D. Epidemi-ology of postconcussion syndrome in pedi-atric mild traumatic brain injury. Pediatrics.2010;126(2). Available at: www.pediatrics.org/cgi/content/full/126/2/e374
11. Blume HK, Vavilala MS, Jaffe KM, et al.Headache after pediatric traumatic braininjury: a cohort study. Pediatrics. 2012;129(1). Available at: www.pediatrics.org/cgi/content/full/129/1/e31
12. Yeates KO, Taylor HG, Rusin J, et al. Longi-tudinal trajectories of postconcussivesymptoms in children with mild traumaticbrain injuries and their relationship toacute clinical status. Pediatrics. 2009;123(3):735–743
13. Zemek RL, Farion KJ, Sampson M, McGahernC. Prognosticators of persistent symptomsfollowing pediatric concussion: a system-atic review. JAMA Pediatr 2013;167(3):259–265
14. Kutcher JS, Eckner JT. At-risk populations insports-related concussion. Curr SportsMed Rep. 2010;9(1):16–20
15. Ponsford J, Cameron P, Fitzgerald M, GrantM, Mikocka-Walus A, Schonberger M. Pre-dictors of postconcussive symptoms 3 monthsafter mild traumatic brain injury. Neuropsy-chology. 2012;26(3):304–313
16. Babcock L, Byczkowski T, Wade SL, Ho M,Mookerjee S, Bazarian JJ. Predicting post-concussion syndrome after mild traumaticbrain injury in children and adolescentswho present to the emergency department.JAMA Pediatr. 2013;167(2):156–161
17. McCrea M, Guskiewicz K, Randolph C, et al.Incidence, clinical course, and predictorsof prolonged recovery time following sport-related concussion in high school andcollege athletes. J Int Neuropsychol Soc.2013;19(1):22–33
18. Longhi L, Saatman KE, Fujimoto S, et al.Temporal window of vulnerability to re-petitive experimental concussive brain in-jury. Neurosurgery. 2005;56:364–374; discussion364–374
19. Shitaka Y, Tran HT, Bennett RE, et al. Re-petitive closed-skull traumatic brain injuryin mice causes persistent multifocal axonalinjury and microglial reactivity. J Neuro-pathol Exp Neurol. 2011;70(7):551–567
20. Vagnozzi R, Tavazzi B, Signoretti S, et al.Temporal window of metabolic brain vul-nerability to concussions: mitochondrial-related impairment—part I. Neurosurgery.2007;61(2):379–388; discussion 388–389
21. Weber JT. Experimental models of re-petitive brain injuries. Prog Brain Res.2007;161:253–261
22. Meehan WP III, Zhang J, Mannix R, WhalenMJ. Increasing recovery time betweeninjuries improves cognitive outcome afterrepetitive mild concussive brain injuries inmice. Neurosurgery. 2012;71(4):885–891
23. Meehan WP III, d’Hemecourt P, Collins CL,Comstock RD. Assessment and manage-ment of sport-related concussions inUnited States high schools. Am J SportsMed. 2011;39(11):2304–2310
24. McCrory P, Meeuwisse W, Johnston K, et al.Consensus statement on concussion insport 3rd International Conference onConcussion in Sport held in Zurich, No-vember 2008. Clin J Sport Med 2009;19:185–200
25. McCrory P, Meeuwisse W, Johnston K, et al.Consensus statement on concussion insport: the 3rd International Conference onConcussion in Sport held in Zurich, No-vember 2008. Br J Sports Med. 2009;43(suppl 1):i76–i90
26. International Symposium on Concussion inSport. Abstracts. Br J Sports Med. 2001;35(5):367–377
27. Halstead ME, Walter KD; Council on SportsMedicine and Fitness. American Academyof Pediatrics. Clinical report—sport-relatedconcussion in children and adolescents. Pe-diatrics. 2010;126(3):597–615
28. Meehan WP III, Bachur RG. Sport-relatedconcussion. Pediatrics. 2009;123(1):114–123
29. King NS, Crawford S, Wenden FJ, Moss NE,Wade DT. The Rivermead Post ConcussionSymptoms Questionnaire: a measure ofsymptoms commonly experienced afterhead injury and its reliability. J Neurol.1995;242(9):587–592
30. Faux S, Sheedy J, Delaney R, Riopelle R.Emergency department prediction of post-concussive syndrome following mild trau-matic brain injury—an international cross-validation study. Brain Inj 2011;25(1):14–22
31. Gagnon I, Swaine B, Friedman D, Forget R.Exploring children’s self-efficacy related tophysical activity performance after a mildtraumatic brain injury. J Head TraumaRehabil. 2005;20(5):436–449
32. Eyres S, Carey A, Gilworth G, Neumann V,Tennant A. Construct validity and reliabilityof the Rivermead Post-Concussion Symp-toms Questionnaire. Clin Rehabil. 2005;19(8):878–887
33. Lannsjo M, Borg J, Bjorklund G, Af Geijer-stam JL, Lundgren-Nilsson A. Internal con-struct validity of the Rivermead Post-Concussion Symptoms Questionnaire. JRehabil Med 2011;43(11):997–1002
34. Harris PA, Taylor R, Thielke R, Payne J,Gonzalez N, Conde JG. Research electronicdata capture (REDCap)—a metadata-drivenmethodology and workflow process forproviding translational research informaticssupport. J Biomed Inform. 2009;42(2):377–381
35. McCrea M, Guskiewicz K, Randolph C, et al.Effects of a symptom-free waiting period onclinical outcome and risk of reinjury aftersport-related concussion. Neurosurgery.2009;65(5):876–882; discussion 882–883
36. Moser RS, Glatts C, Schatz P. Efficacy ofimmediate and delayed cognitive andphysical rest for treatment of sports-related concussion. J Pediatr. 2012;161(5):922–926
37. Stulemeijer M, van der Werf S, Borm GF,Vos PE. Early prediction of favourable re-covery 6 months after mild traumatic braininjury. J Neurol Neurosurg Psychiatry. 2008;79(8):936–942
38. De Kruijk JR, Leffers P, Menheere PP,Meerhoff S, Rutten J, Twijnstra A. Predictionof post-traumatic complaints after mildtraumatic brain injury: early symptoms and
16 EISENBERG et alby guest on April 11, 2017Downloaded from

biochemical markers. J Neurol NeurosurgPsychiatry. 2002;73(6):727–732
39. Field M, Collins MW, Lovell MR, Maroon J.Does age play a role in recovery fromsports-related concussion? A comparisonof high school and collegiate athletes. JPediatr. 2003;142(5):546–553
40. Broshek DK, Kaushik T, Freeman JR,Erlanger D, Webbe F, Barth JT. Sex differ-
ences in outcome following sports-related
concussion. J Neurosurg. 2005;102(5):856–
863
41. Colvin AC, Mullen J, Lovell MR, West RV,
Collins MW, Groh M. The role of concussion
history and gender in recovery from soccer-
related concussion. Am J Sports Med. 2009;37
(9):1699–1704
42. Preiss-Farzanegan SJ, Chapman B, WongTM, Wu J, Bazarian JJ. The relationshipbetween gender and postconcussionsymptoms after sport-related mild trau-matic brain injury. PM R 2009;1(3):245–253
43. Frommer LJ, Gurka KK, Cross KM, IngersollCD, Comstock RD, Saliba SA. Sex differencesin concussion symptoms of high schoolathletes. J Athl Train. 2011;46(1):76–84
REMOTE MONITORING: At our University, all students taking an examination mustbe monitored by a proctor who is physically present in the room in which theexamination is being given. Although somewhat cumbersome, the system workswhen all students take the exam together in one place. However, the policy beginsto break down when several students need to take exams at different times, orhave accommodations allowing extra time to complete the exam. Suddenly, we donot have enough proctors. The situation is even more complex when one con-sidersmassive open online courses (MOOC) which can have enrollments of 40,000or more students. Historically not for credit, more MOOC courses are offeringexaminations and course credits, and monitoring students for cheating whiletaking a test in an MOOC is challenging. Requiring students to take examinationsin a regional testing center is often unrealistic and too costly for most. However,a few companies now offer electronic surveillance of MOOC test-takers (using thekind of gadgetry one might expect someone like James Bond, not an onlinecourse, to need). This surveillance is just as good as, if not better than, using liveproctors in traditional courses. As reported in The New York Times (Technology:March 3, 2013), test-taker identity can be confirmed remotely by checking photoIDs and signatures – and, in a new twist, by comparing typing styles (e.g., howlong individual keys are depressed while typing a specified phrase) to those onrecord. Techniques to detect cheating include video monitoring, keystroke sur-veillance, screen sharing, and the use of sophisticated computer algorithms.Students can be monitored in real time, or sessions can be recorded and thenreplayed later (at high speed) in order to detect any aberrations. The costs tomonitor the examination are often borne by the student, and range from around$15 to $100 (depending on the class and type of monitoring). A number of uni-versities already make use of the programs offered by these companies, andreport high satisfaction. While many of these techniques have been designed forMOOC, there is no reason they cannot be applied to examinations given in tra-ditional classes at “brick and mortar” universities. While some complain thata webcam is intrusive, so is an exam monitor. I personally hope we can moveaway from sit-down exams at a specified time with a proctor, and move to a moreopen system where students take the exam when ready, where ready, using thesame proctor-free technology being used in MOOCs.
Noted by WVR, MD
ARTICLE
PEDIATRICS Volume 132, Number 1, July 2013 17by guest on April 11, 2017Downloaded from

DOI: 10.1542/peds.2013-0432; originally published online June 10, 2013; 2013;132;8Pediatrics
Matthew A. Eisenberg, John Andrea, William Meehan and Rebekah MannixTime Interval Between Concussions and Symptom Duration
ServicesUpdated Information &
/content/132/1/8.full.htmlincluding high resolution figures, can be found at:
References
/content/132/1/8.full.html#ref-list-1at:This article cites 34 articles, 10 of which can be accessed free
Citations /content/132/1/8.full.html#related-urls
This article has been cited by 18 HighWire-hosted articles:
Subspecialty Collections
/cgi/collection/concussion_subConcussion
/cgi/collection/sports_medicine:physical_fitness_subSports Medicine/Physical Fitness
/cgi/collection/neurology_subNeurologythe following collection(s):This article, along with others on similar topics, appears in
Permissions & Licensing
/site/misc/Permissions.xhtmltables) or in its entirety can be found online at: Information about reproducing this article in parts (figures,
Reprints /site/misc/reprints.xhtml
Information about ordering reprints can be found online:
rights reserved. Print ISSN: 0031-4005. Online ISSN: 1098-4275.Grove Village, Illinois, 60007. Copyright © 2013 by the American Academy of Pediatrics. All and trademarked by the American Academy of Pediatrics, 141 Northwest Point Boulevard, Elkpublication, it has been published continuously since 1948. PEDIATRICS is owned, published, PEDIATRICS is the official journal of the American Academy of Pediatrics. A monthly
by guest on April 11, 2017Downloaded from
DOI: 10.1542/peds.2013-0432; originally published online June 10, 2013; 2013;132;8Pediatrics
Matthew A. Eisenberg, John Andrea, William Meehan and Rebekah MannixTime Interval Between Concussions and Symptom Duration
/content/132/1/8.full.html
located on the World Wide Web at: The online version of this article, along with updated information and services, is
of Pediatrics. All rights reserved. Print ISSN: 0031-4005. Online ISSN: 1098-4275.Boulevard, Elk Grove Village, Illinois, 60007. Copyright © 2013 by the American Academy published, and trademarked by the American Academy of Pediatrics, 141 Northwest Pointpublication, it has been published continuously since 1948. PEDIATRICS is owned, PEDIATRICS is the official journal of the American Academy of Pediatrics. A monthly
by guest on April 11, 2017Downloaded from
Related Documents











